Frequency analysis of the peripheral pulse wave detected in the finger with a photoplethysmograph
5
IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING. VOL. 37, NO. 3, MARCH 1990 313 Communications Frequency Analysis of the Peripheral Pulse Wave Detected in the Finger with a Photoplethysmograph M. H. SHEREBRIN AND R. Z. SHEREBRIN Abstract-A photoelectric plethysmograph is described that per- forms a frequency analysis of the peripheral volume pulse wave using a portable computer. It was used to determine how the pulse shape varied with age using 54 subjects in three age groups, 10-29, 30-59, and 60-89 years. The youngest group had a larger power in the second harmonic, (normalized to the fundamental), with p < 0.05 than the older two groups. The decrease of power in the harmonics of the pe- ripheral pulse wave with age may be a useful noninvasive measure of aging and vascular disease. INTRODUCTION The photoplethysmograph is a noninvasive device for detecting blood volume changes in living tissue by optical means and was first described more than 50 years ago by Hertzman [ 11. The device consists of a light source, photodetector, and ac amplifier and can be used to detect flow variations in the periphery during the cardiac cycle. Weinman et al. [2] have studied the optical signal of the photoplethysmograph in the reflective mode using an in vitro model and they concluded that scattering, reflection, absorption, and movement of the vessel wall all play a role in producing the signal. Nijboer et al. [3] have described many applications of the method and have discussed the influence of nonlinearity in the detector when comparing amplitude changes. Despite the complex source of the signal and problems of measurement, the photoplethysmo- graph has been widely used for a variety of applications including monitoring of digital arterial pressure and compliance in man [4], and detecting anxiety [5]. The electrical signal from the photodetector is related to blood volume changes in tissue. This signal provides a means of deter- mining properties of the vascular tree during the cardiac cycle and changes with aging and disease. It is important to emphasize that it yields only a qualitative description of blood pressure or flow because variables such as blood volume and vessel size which in- fluence the signal may also change with pressure. Our long-term objective is to measure the elastic properties of the vascular tree noninvasively in human subjects as a function of aging and disease using the shape of the peripheral pulse wave. However, the shape of the pulse wave depends upon the thickness of the blood vessels and contractility of the heart as well as the state of the vascular smooth muscle in the vessel wall. This makes the analysis of the problem much more complex. An interesting approach was reported recently by Shimazu et al. [6], who utilize a cuff and photoplethysmograph to calculate the volume elastic modulus of arteries in the finger. METHOD The instrument we constructed is illustrated in Fig. 1. The source consists of two 935 nm infrared light emitting diodes (LED) sep- arated by 12 mm and the detector of the reflected and scattered light Manuscript received March 3, 1988; revised August 9, 1989. This work was supported by Grant A-6016 from the National Sciences and Engineer- ing Research Council of Canada and in part by Grant MA-91 19 from the Medical Research Council of Canada. The authors are with the Department of Medical Biophysics, Faculty of Medicine, University of Western Ontario, London, Ont., Canada N6A 5C1. IEEE Log Number 8933067. is a phototransistor between the LED's. Changing the angle of the axis of the LED's relative to the phototransistor from 0 to 45" had a negligible effect on the response probably because the skin sur- face touched the lens of the both the diodes and phototransistor and scattered the light. Because of the scattering by the skin we chose the simplest arrangement and set the optical axes of the diodes and phototransistor parallel to each other. The index finger near the middle of the third phalanx is placed on the emitter detector array with sufficient pressure to dimple the skin yet not large enough to occlude the flow. The output of the phototransistor is passed through the band pass filter (single pole multiple feedback) with a center frequency of 1 .O Hz and a Q of 0.05 to provide a measure of base line stability and a minimum of attenuation (-3 dB) of the frequencies of interest between 0.1 and 10 Hz. The waveform is displayed on a chart re- corder (Dynograph, Beckman Instruments, Schiller Park, IL) or recorded on a ferric oxide audio cassette tape using equalization of 120 ps and low bias position on one channel of a model PMD 360 stereo cassette recorder (Marantz Co. Inc., Chatsworth, CA). A voltage-to-frequency converter was used for recording and a fre- quency-to-voltage converter for playback. The pulse waveform can be analyzed directly or upon playback of the cassette tape using a portable computer, (Model 100, Tandy Electronics, Fort Worth, TX), which uses a 80C85 microprocessor with 24 kb of random access memory and a data acquisition system, (Model PL-100, Elexor Associates, Moms Plains, NJ) with a 8 bit A/D converter having a minimum conversion time of 125 ps. A 20 Hz low-pass filter with a 6 dB per octave attenuation was used to prevent alias- ing when digitizing. A fast Fourier transform (FFT) written for integer arithmetic in Assembly language for the 8080 and 8085 family of microprocessors [7] provides the power spectrum of the 256 point sampled waveform in about 6 s. The main program is written in Basic and Assembly language subroutines are used to control the A/D converter and to perform the FFT. A flow chart of the program is provided in Fig. 2. The computer program displays the incoming waveform on the 64 by 240 pixels of the liquid crystal screen of the computer or on the printer. The period of the pulse wave is measured between the maxima by the program which then calculates the sampling interval between each of the 256 points. The minimum and maximum threshold values used for the period determination are selected by the operator on the basis of the displayed waveform, shown in Fig. 3, but this step could readily be incorporated into the program. The power spectrum which is the square of the Fourier amplitude for each harmonic can then be displayed on the computer screen or printed. The young and middle aged subjects were normal high school and university students and staff. The older subjects were members of a retirement club. All were asked to answer a questionnaire con- cerning physical activity, heart disease, and any drugs that they were taking although this information was not used to exclude data from the present analysis. The results were not different between sexes at a level of significance o f p = 0.05 so the data were pooled. Because the shape of the pulse wave is influenced by respiration, temperature, and psychological factors such as anxiety and fear, we took extra care to control these factors. The room was kept warm (about 23°C) to ensure that there was peripheral vasodilation and we tried to arrange a relaxed atmosphere. Finger temperature above 32°C is a good index of vasodilation and this was confirmed using an electronic thermometer. RESULTS The power spectrum of each person is normalized by dividing the power at each harmonic by that of the fundamental. The relative 0018-9294/90/0300-03 13$01 .OO 0 1990 IEEE
Transcript of Frequency analysis of the peripheral pulse wave detected in the finger with a photoplethysmograph

IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING. VOL. 37, NO. 3, MARCH 1990 313
Communications Frequency Analysis of the Peripheral Pulse Wave
Detected in the Finger with a Photoplethysmograph
M. H . SHEREBRIN AND R. Z. SHEREBRIN
Abstract-A photoelectric plethysmograph is described that per- forms a frequency analysis of the peripheral volume pulse wave using a portable computer. It was used to determine how the pulse shape varied with age using 54 subjects in three age groups, 10-29, 30-59, and 60-89 years. The youngest group had a larger power in the second harmonic, (normalized to the fundamental), with p < 0.05 than the older two groups. The decrease of power in the harmonics of the pe- ripheral pulse wave with age may be a useful noninvasive measure of aging and vascular disease.
INTRODUCTION The photoplethysmograph is a noninvasive device for detecting
blood volume changes in living tissue by optical means and was first described more than 50 years ago by Hertzman [ 11. The device consists of a light source, photodetector, and ac amplifier and can be used to detect flow variations in the periphery during the cardiac cycle. Weinman et al. [2] have studied the optical signal of the photoplethysmograph in the reflective mode using an in vitro model and they concluded that scattering, reflection, absorption, and movement of the vessel wall all play a role in producing the signal. Nijboer et al. [3] have described many applications of the method and have discussed the influence of nonlinearity in the detector when comparing amplitude changes. Despite the complex source of the signal and problems of measurement, the photoplethysmo- graph has been widely used for a variety of applications including monitoring of digital arterial pressure and compliance in man [4], and detecting anxiety [ 5 ] .
The electrical signal from the photodetector is related to blood volume changes in tissue. This signal provides a means of deter- mining properties of the vascular tree during the cardiac cycle and changes with aging and disease. It is important to emphasize that it yields only a qualitative description of blood pressure or flow because variables such as blood volume and vessel size which in- fluence the signal may also change with pressure.
Our long-term objective is to measure the elastic properties of the vascular tree noninvasively in human subjects as a function of aging and disease using the shape of the peripheral pulse wave. However, the shape of the pulse wave depends upon the thickness of the blood vessels and contractility of the heart as well as the state of the vascular smooth muscle in the vessel wall. This makes the analysis of the problem much more complex. An interesting approach was reported recently by Shimazu et al. [6], who utilize a cuff and photoplethysmograph to calculate the volume elastic modulus of arteries in the finger.
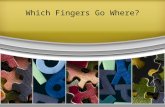
METHOD The instrument we constructed is illustrated in Fig. 1. The source
consists of two 935 nm infrared light emitting diodes (LED) sep- arated by 12 mm and the detector of the reflected and scattered light
Manuscript received March 3, 1988; revised August 9 , 1989. This work was supported by Grant A-6016 from the National Sciences and Engineer- ing Research Council of Canada and in part by Grant MA-91 19 from the Medical Research Council of Canada.
The authors are with the Department of Medical Biophysics, Faculty of Medicine, University of Western Ontario, London, Ont., Canada N6A 5C1.
IEEE Log Number 8933067.
is a phototransistor between the LED's. Changing the angle of the axis of the LED's relative to the phototransistor from 0 to 45" had a negligible effect on the response probably because the skin sur- face touched the lens of the both the diodes and phototransistor and scattered the light. Because of the scattering by the skin we chose the simplest arrangement and set the optical axes of the diodes and phototransistor parallel to each other. The index finger near the middle of the third phalanx is placed on the emitter detector array with sufficient pressure to dimple the skin yet not large enough to occlude the flow.
The output of the phototransistor is passed through the band pass filter (single pole multiple feedback) with a center frequency of 1 .O Hz and a Q of 0.05 to provide a measure of base line stability and a minimum of attenuation (-3 dB) of the frequencies of interest between 0.1 and 10 Hz. The waveform is displayed on a chart re- corder (Dynograph, Beckman Instruments, Schiller Park, IL) or recorded on a ferric oxide audio cassette tape using equalization of 120 ps and low bias position on one channel of a model PMD 360 stereo cassette recorder (Marantz Co. Inc., Chatsworth, CA). A voltage-to-frequency converter was used for recording and a fre- quency-to-voltage converter for playback. The pulse waveform can be analyzed directly or upon playback of the cassette tape using a portable computer, (Model 100, Tandy Electronics, Fort Worth, TX), which uses a 80C85 microprocessor with 24 kb of random access memory and a data acquisition system, (Model PL-100, Elexor Associates, Moms Plains, NJ) with a 8 bit A/D converter having a minimum conversion time of 125 ps. A 20 Hz low-pass filter with a 6 dB per octave attenuation was used to prevent alias- ing when digitizing. A fast Fourier transform (FFT) written for integer arithmetic in Assembly language for the 8080 and 8085 family of microprocessors [7] provides the power spectrum of the 256 point sampled waveform in about 6 s.
The main program is written in Basic and Assembly language subroutines are used to control the A/D converter and to perform the FFT. A flow chart of the program is provided in Fig. 2.
The computer program displays the incoming waveform on the 64 by 240 pixels of the liquid crystal screen of the computer or on the printer. The period of the pulse wave is measured between the maxima by the program which then calculates the sampling interval between each of the 256 points. The minimum and maximum threshold values used for the period determination are selected by the operator on the basis of the displayed waveform, shown in Fig. 3, but this step could readily be incorporated into the program. The power spectrum which is the square of the Fourier amplitude for each harmonic can then be displayed on the computer screen or printed.
The young and middle aged subjects were normal high school and university students and staff. The older subjects were members of a retirement club. All were asked to answer a questionnaire con- cerning physical activity, heart disease, and any drugs that they were taking although this information was not used to exclude data from the present analysis. The results were not different between sexes at a level of significance o f p = 0.05 so the data were pooled.
Because the shape of the pulse wave is influenced by respiration, temperature, and psychological factors such as anxiety and fear, we took extra care to control these factors. The room was kept warm (about 23°C) to ensure that there was peripheral vasodilation and we tried to arrange a relaxed atmosphere. Finger temperature above 32°C is a good index of vasodilation and this was confirmed using an electronic thermometer.
RESULTS The power spectrum of each person is normalized by dividing
the power at each harmonic by that of the fundamental. The relative
0018-9294/90/0300-03 13$01 .OO 0 1990 IEEE

314
- CASSETTE RECORDER AMPLIFIER -C "/F
IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING. VOL. 37. NO. 3, MARCH 1990
F/V - -
12 rnrn
k -3 'W TopView
?-- AhlPLlFIEH
G
CHART RECORDER
COhlPUTER ANTI ALIAS
Fig. 1. Block diagram of the measuring system. Inset shows the positions of the LED's and the phototransistor PT in the emitteddetector assem- bly. The finger was placed on this assembly at the location shown by the arrows. The PT was on the center of the whorl of the fingerprint.
FLO\\ CHART OF BASIC PROGRAM \\ ITH MACHINE LANGUAGE SUBROUrlNES
I. SELECT THRESHOLD
2. MEASURE PERIOD OF PULSE
3. CALCULATE PERIOD FOR SAMPLING
1. DIGITIZE ONE PULSE
5. PERFORhl MACHINE LANGUAGE FAST FOURIER TRANSFORhl
6 . CHOOSE DISPLAY OPTION,
ON COhlPUTER SCREEN
ON PRINTER
ON BOTH SCREEN AND PRINTER
7. RETURN FOR NEXT COMhlAND
Fig. 2. Flow chart of analysis program
power of each harmonic from the second to the ninth is shown in Fig. 4 for the subjects divided into three age groups, 10-29, 30- 59, and 60-89 years with 18 individuals in each group. The test group was made up of 25 females and 29 males not matched in age. The results are shown in Fig. 4. Since the power falls off with harmonic number very rapidly we tried to fit the experimental data using an exponential decay. The results of a least squares fit for n = 9 data points are as follows:
y = 1.17 exp ( - ,763 * n); r 2 = 0.940 for the youngest group; y = 1.85 exp (-.997 * x ) ; r 2 = 0.977 forthe middle age group; y = 0.775 exp (-.877 * x ) ; r 2 = 0.919 for the oldest group;
where r is the coefficient of correlation, y the power, and n the harmonic number (1 to 9). Power for the eighth and ninth harmon- ics in the oldest group and for the ninth harmonic in the middle age group were estimated by extrapolation as they were below the res- olution of our measurements.
Fig. 4 illustrates the influence of age on how rapidly the power of the harmonics falls off in the pulse waveform for subjects at rest. Exercise also influences the pulse shape and spectrum because the increase in heart rate and blood pressure changes the impedance throughout the vascular system. The changes after strenuous phys- ical exercise of running up and down four flights of stairs for one 18-year-old female subject are illustrated in Fig. 5. The resting frequency was 1.23 Hz rising to 1.98 Hz during the first exercise and to 1.78 Hz during the second. The pulse rate was allowed to return to the resting value between the two sets of exercise.
DISCUSSION
The shape of the peripheral pulse wave depends on environmen- tal temperature, respiration, posture, exercise, hormone levels, heart function, and even mental state. If the waveforms are to be compared in a meaningful way these factors must be controlled. We were primarily interested in the effect of age on the pulse shape so we attempted to maintain the other variables constant. For ex- ample, the amplitude of the pulse wave changes with the depth, frequency, and phase of respiration due to the influence of intra-

IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 37. NO. 3. MARCH 1990 315
ln I-
W a
z ln
SUBJECT A03 AGE 18, MALE FREO- 1.41 Hz
1 ' 1 ~ 1 ~ 1 . l ' I ~ I
- SUBJECT G O 6 AGE 71,FEMALE . FREQ-0.69 H I
-
-
0 0.2 0.4 0.6 0.8 I 1.2 1.4 TIME,S
(b)
Fig. 3. Comparison of the photoplethysmograph signals on rectilinear co- ordinates, (a) for a male age 18 and (b) a female age 71. Reproduction of curvilinear chart recordings for (c) a male age 18, (d) a female age 71, (e) a male age 87, and ( f ) a female age 17. The slower chart speed in ( f ) allows changes in amplitude due to respiration to be seen.
1 0.25 0,3El. 10-29 YEARS
1 3 0 - 5 9 Y E A R S
1 6 0 - 8 9 YEARS
E 0.2 N
2 0.15 z 0
0.1
0.05
n " 2 3 4 5 6 7 8 9
nmmotw NUMBER
Fig. 4. Power spectrum of the waveform with respect to the fundamental for three age categories 10-29, 30-59, and 60-89 years. The flags are the standard error of the mean.
thoracic pressure on venous return. In order to keep the breathing regular we suggested that the subject relax and inhale regularly but not deeply. We noted the well known intense peripheral vasocon- striction that occurs with breath holding. Even a sigh was sufficient to cause an excursion from the base line and we excluded any such anomalous waveforms from our analysis.
Fig. 4 shows a decrease in harmonic content of the pulse wave shape with age. There was often a large variation in shape between individuals within any an age group. To compare the variation in
pulse shape in one individual and in a group of nine of similar age we calculated the mean and standard error of the mean (SEM) for the second harmonic of nine pulse waves from one 18-year-old male, (0.384 k 0.034) and compared this with the mean and SEM for nine individuals in the same age range (10-19y) of both sexes, (0.309 & 0.067). Since the variance is proportional to the square of the SEM we can conclude from this calculation that about one quarter of the variance of the sample group is due to variation within each individual. Considering the similarity of the nine pulses from

3 16 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING. VOL. 37. NO. 3. MARCH 1990
TABLE I SIGNIFICANCE OF DIFFERENCE BETWEEN GROUPS
P Value
Harmonic AB-CDE AB-FGH CDE-FGH
2 0.041* 0.01* 0.20 3 0.32 0.063 0.148 4 0.505 0.196 0.608 5 0.531 0.076 0.087 6 0.134 0.025* 0.11
*Statistically significant difference at > 95 % confidence level. Group AB ages 10-29 years, n = 18; Group CDE ages 30-59 years,
n = 18; Group FGH ages 60-89 years, n = 18.
a W
I a
3 a
0 W
a 0 z
12
I
0.8
0.6
0.4
0.2
0 2
I !
3 4 5
T 1
HARMONIC NUMBER
Fig. 5. Comparison of the power spectrum of one 18-year-old female sub- ject at rest and directly following the strenuous physical exercise of run- ning up and down four flights of stairs. The results are the average power spectrum analyzing four separate waveforms from each experiment. Ex- ercise trial 2 followed trial 1 after the pulse rate had returned to the preexercise resting value. It is obvious from the results that other phys- iological variables had not yet returned to their initial values. Flags are the standard error of the mean.
the one individual we were impressed with the sensitivity of the method for detecting small variations in shape.
We selected the three age groups of 10-29, 30-59, and 60-89 years since we have noted in our other experiments [8] that there was a marked decrease in extensibility in human aortas above the age of 30 years and a minimal change beyond about 60 years. The histogram of Fig. 4 shows a drop in power in the second and third harmonics as a function of increasing age. Differences in the power for the second to sixth harmonic between each age group was com- pared using a t test. Three measurements were significant statisti- cally a t p < 0.05 as shown in Table I. The second harmonic power was significantly different between the youngest and both older groups. The sixth harmonic was significantly different between the youngest and oldest group. The power present in harmonics higher than the sixth was too small to compare. The sample size and range in age within each group is responsible in part for the large vari- ance. We have also observed a wide variation in elastic properties and wall thickness of the aorta from autopsy samples of similar age. The important result noted here is the highly significant de- crease in the relative power of the second harmonic with age.
Because the pulse frequency varies both within and between sub- jects, the fundamental frequency used in the analysis is normalized using the instantaneous frequency of the individual pulse. We rec- ognize that this can introduce errors because impedance is a func- tion of frequency but the pulse rate at rest does not vary much. It may be important to consider the absolute frequency during exer- cise although we did not do so in the example presented here.
While the main objective was to determine how the pulse shape changes as a function of age we were also interested in the quali- tative influence of heart rate and blood pressure. To examine these factors, one subject was tested at rest and after performing two periods of strenuous exercise which increase both the blood pres- sure and heart rate. The results in Fig. 5 show marked changes with exercise and suggest that we did not allowed sufficient time be- tween the first and second test for all relevant variables to return to the resting state. It also reveals the sensitivity of the spectral analysis of the peripheral pulse shape to changes with exercise.
The peripheral pulse detected by the photoplethysmograph has a steep rise and a notch (the dicrotic notch) on the falling slope in the younger subjects. In most older subjects there was a more grad- ual rise and fall and no pronounced dicrotic notch. The photopleth- ysmogram closely resembles the shape of the arterial pressure wave recorded with a catheter. Typical waveforms of the plethysmogram are shown in Fig. 3(a) for an 18-year-old male, and in (b) for a 71- year-old female redrawn on a rectilinear scale to emphasize the differences in shape. Fig. 3(c) and (d) show reproductions for (a) and (b) on the curvalinear chart to illustrate the shape uniformity from pulse to pulse. Fig. 3(e) is from a 87-year-old male while (f) is for a 17-year-old female at a slower chart speed to illustrate the amplitude variations with respiration. In some tracings there is a short distortion in the time scale due to inertia of the chart drive when the speed was changed. Anomalous waveforms due to move- ment or irregular breathing were rejected from the analysis.
The difference in shape of the peripheral pulse wave and the

IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING. VOL. 37. NO. 3. MARCH 1990 317
disappearance of the dicrotic notch with age has been explained [9] by reduced wave reflection. The dicrotic notch on the falling phase of the pulse is due to reflections at bifurcations of the arterial tree [lo]. The notch was the most noticeable feature that changed with age.
If we consider the genesis of the dicrotic notch in terms of re- flections from discontinuities, the energy that is reflected depends upon the change in vessel impedance primarily at bifurcations. The energy reflected RF according to McDonald 11 11 is given by
RF = (Zt - zO)/(Zf + ZO)
where Zf and Zo are the terminating and characteristic impedances of the vessel, respectively. The energy reflected at each disconti- nuity of the vascular tree can increase or decrease with age de- pending on how Zr and Zo change. Clinical results show that the dicrotic notch tends to disappear with age and the pulse recorded distal to an obstruction lacks a dicrotic notch and is more rounded in shape [12]. The change in reflected energy would explain how stenoses and plaque accumulations that develop with age could cause the dicrotic notch to disappear. Farrar er al. [13] using pri- mates on an atherogenic diet showed an increase in aortic stiffness due to wall thickening and a doubling of the pulse wave velocity but no increase in the incremental Young’s modulus. They also noted that the femoral pulse wave recorded with a catheter showed a decrease in the amplitude of the dicrotic notch that was similar to what we observe in the periphery. Avolio et al. 1141 and Kelly et al. [ 151 have observed similar disappearance of the dicrotic notch in the arterial pressure pulse waveform in the carotid, radial, and femoral arteries using tonometry.
The peripheral pulse can be considered as the output waveform where the driving function is the pressure at the aortic valve and the transmission line is the vascular tree. The transfer function is then a measure of the elastic properties and geometry of the blood vessels. The waveform depends on the location where it is de- tected. We measured the pulse in a capillary bed of a finger tip but other investigators have used the toe or vessels in the forehead or arm. There is a slight difference in shape dependent on the location where the pulse is measured.
Fourier analysis of the pulse pressure has been used previously to characterize pulse shape in terms of its frequency components by McDonald 1111, Milnor 1161, and Strandness 1171. Spectral analysis using the discrete FFT provides equivalent results. While further tests in a clinical environment are necessary to classify var- ious pathological conditions with the frequency spectrum of the photoplethysmogram, we believe that this type of analysis can pro- vide a simple, inexpensive, and noninvasive means for studying changes in the elastic properties of the vascular system with age and disease.
ACKNOWLEDGMENT We thank L. Rigutto for his assistance in the design and con-
struction of the photoplethysmograph and to all the individuals who participated in the study. We also wish to thank Dr. C. P. S . Taylor and Dr. M. R. Roach and the anonymous referees for their con- structive comments.
REFERENCES
[ I ] A. B. Hertzman, “The blood supply of various skin areas as esti- mated by the photoelectric plethysmograph,” Amer. J . Physiol., vol.
[2] J . Weinman, A. Hayat, and G. Raviv, “Reflection plethysmography of arterial-blood volume pulses.” Med. Biol. Eng. Comput., vol. 15, no. 1, pp. 22-31, 1977.
[3] J . A. Nijboer, J . C. Dorlas, and H. F. Mahieu, “Photoelectric pleth- ysmography-Some fundamental aspects of the reflection and trans- mission method,” Clin. Phys. Physiol. Meas. , vol. 2 , no. 3, pp. 205- 215. 1981.
[4] R. Nakayama and T . Azuma, “Noninvasive measurements of digital arterial pressure and compliance in man,” Amer. J . Physiol., vol.
124, pp. 328-340, 1938.
233, pp. H168-HI79. 1977.
[5] L. J . Bloom, “An evaluation of finger pulse volume as a psychophy- siological measure of anxiety.” Psychophysiol., vol. 13, pp. 40-42, 1976.
[6] H . Shimazu, K.-I. Yamakoshi, and A. Kamiya, “Noninvasive mea- surement of the volume elastic modulus in finger arteries using pho- toelectric plethysmography,” IEEE Trans. Biomed. Eng., vol. BME-
A. Roxburgh, “Fast Fourier comes back,” Byte, vol. 6 , pp. 458- 461, May, 1981. M. H.Sherebrin, H. A. Bernans, and M. R. Roach, “Extensibility changes of calcified soft tissue strips from human aorta,” Can. J . Physiol. Pharmacol., vol. 65, pp. 1878-1883, 1987. J . Iriuchijima, Curdiovasculur Physiology: Nerve, Flow and Pres- sure. M. F. O’Rourke, “Principles of arterial hemodynamics,” in Me- chanics of the Circulation, H.E.D.J. Ter Keurs and J .V. Tyberg, Dordrecht: Martinus Nijhoff, 1987, p. 240. D. A. McDonald, Blood Flow in Arreries, 2nd ed. London: Edward Arnold, 1974, ch. 7 . D. S . Sumner, “Mercury strain-gauge plethysmography,” Noninva- sive Diagnostic Techniques in Vascular Disease, 2nd ed., E. F. Bem- stein, Ed. D. J . Farrar, H. D. Green, M. G . Bond, W. D. Wagner, and R. A. Gobbee, “Aortic pulse wave velocity, elasticity and composition in a nonhuman primate model of atherosclerosis,” Circ. Res. , vol. 43,
A. Avolio, R. Kelly, D . Hayward, D. Winter, and M. O’Rourke, “Noninvasive registration of the arterial pressure pulse waveform using high fidelity applanation tonometry,” Fed. Amer. Soc. Exp. Bioi. J . , vol. 2 , no. 4 , p. A116, 1988. R. Kelly, C. Hayward, D. Winter, A. Avolio, and M. O’Rourke, “Noninvasive determination of aging changes in the arterial pulse,” Fed. Amer. Soc. Exp. Biol., vol. 2 , no. 4 , p. A125, 1988. W. R. Milnor, Hemodynamics. Baltimore, MD: Williams and Wil- kins, 1982. D. E. Strandness and D. S. Sumner, Hemodynamics for Surgeons. New York: Grune and Stratton, 1975, pp. 226-228.
33, pp. 795-798, 1986.
Tokyo: Igaku Shoin. 1972, ch. 8.
St. Louis: Mosby 1982, p. 128.
pp. 52-62, 1978.
The Influence of Stimulation Pulse Frequency on the Generation of Joint Moments in the Upper Limb
ROGER NATHAN A N D MOSHE TAVI
Absfruef-Six muscles of the upper limb were stimulated transcuta- neously. This communication reports the influence of the stimulation pulse frequency on the isometric joint moment generated by each mus- cle. A lower frequency of stimulation, the critical fusion frequency, was found for each muscle at which contractions ceased to be tetanic. This fusion frequency was correlated with muscle function. The mag- nitude of the joint moment was examined as a function of the stimu- lation pulse frequency for the six muscles tested. Parabolic curves were found to hest fit this relationship; the magnitude of the moment reach- ing a maximum at typically 50 Hz, and often decreasing at higher fre- quencies. The slope of the linear portion of the relationship between the generated joint moment and the stimulation current intensity was shown to be a function of the stimulation pulse frequency. This func- tion was found to be similar to the form of the joint moment versus pulse frequency curve. Fatigue curves were plotted at different stim- ulation frequencies; demonstrating reduced fatigue at lower stimula- tion frequencies. A model was presented of the fatigue curve as an exponential function of time. We conclude that a stimulation frequency of 15 Hz is optimal for the upper limb muscles with a working range of 15-50 Hz where stimulation frequency is one of the parameters used to modulate the muscle contraction force.
INTRODUCTlON Modulation of force generation can be achieved in general by
varying the total electrical charge per unit time passing through the
Manuscript received March 14, 1988; revised June 26, 1989. The authors are with the Department of Mechanical Engineering, Ben
IEEE Log Number 8933068. Gurion University of the Negev, Beer Sheva, 84105 Israel.
001 8-9294/90/0300-03 17$01 .OO 0 1990 IEEE