
Frequencies of CYP3A5*1/*3 Variants in a Moroccan Population and Effect...
4
Frequencies of CYP3A5*1/*3 Variants in a Moroccan Population and Effect on Tacrolimus Daily Dose Requirements in Renal Transplant Patients Mustapha Elmachad, 1,2, * Driss Elkabbaj, 3, * Fatiha Elkerch, 2 Fatima Zahra Laarabi, 2 Amina Barkat, 4 Zouhir Oualim, 3 and Abdelaziz Sefiani 1,2 The cytochromes P450 are a superfamily of oxidative enzymes, which are implicated in the metabolism of a large number of endogenous substances as well as exogenous chemicals. The cytochrome P450 (CYP3A5) appears to play an important role in drug metabolism activity. The most frequent mutation in the CYP3A5 gene, affecting its activity, consists of a G6986A transition within intron 3. In this study, we determined the allelic frequency of CYP3A5*3 in a Moroccan population, consisting of 108 individuals including 10 renal transplant patients. About 8.33% (9/108) of the subjects were homozygous wild-type (CYP3A5*1/*1), 37.04% (40/108) were heterozygous (CYP3A5*1/*3), and 54.63% (59/108) were homozygous (CYP3A5*3/*3). Therefore, CYP3A5*3 variant was the most frequent allele detected at 73.15%. In the second part of this work, we assessed the influence of the CYP3A5 polymorphism on tacrolimus doses required for 10 renal transplant patients who are receiving tacrolimus as immunosuppressive therapy. Our results showed that, during the first 3 months after kidney transplantation, the tacrolimus daily requirements for heterozygous patients (CYP3A5*3/*1) were higher compared with ho- mozygous patients (CYP3A5*3/*3) (0.133 – 0.026 vs. 0.21 – 0.037 mg/kg/day). After the third month the differ- ence was also observed, whereby the mean of tacrolimus daily requirements for patients with CYP3A5*3/*3 and CYP3A5*1/*3 was 0.053 – 0.013 and 0.08 – 0.014 mg/kg/day, respectively. This first study in Morocco pro- vides genetic data related to the frequency of genetic polymorphisms of CYP3A5 and opens the perspective to develop other pharmacogenetic studies. Introduction T he cytochromes P450 are a superfamily of oxidative enzymes, which are implicated in the metabolism of a large number of endogenous substances as well as exogenous chemicals (Thompson et al., 2004). The cytochromes P450s are involved in the oxidation of *40%–60% of commonly used drugs. CYP3A4 and CYP3A5 are two major isoforms of CYP3A subfamily expressed in adult human tissues. CYP3A4 is found in the liver and small intestine, whereas CYP3A5 is polymorphically expressed in the liver, small intestine, kid- ney, and other organs (Murray et al., 1999; Paine et al., 2006). These isoforms represent the predominant functional forms of human CYP3A (Lin et al., 2002). Many studies have been focused on the identification of sequence variation affecting enzyme activity in the CYP3A5 gene. The most frequent mutation in this gene consists of a G6986A transition within intron 3 (CYP3A5*3). This mutation creates an alternative splice site resulting in a frame shift and truncation of the protein (Kuehl et al., 2001; Lamba et al., 2002). Individuals who are carrying two copies of a CYP3A5*3 allele show a markedly reduced level of CYP3A5 protein expression and activity (Kuehl et al., 2001). Many reports suggested that the CYP3A5*3 mutant allele may play an important role in interindividual dif- ferences of response to drug therapy (Ingelman-Sundberg et al., 1999; Tsuchiya et al., 2004). The association between tacrolimus, an immunosuppressive agent for preventing or treating graft rejection in organ transplantation, and CYP3A5 polymorphism was largely investigated in several studies. It has been demonstrated that renal transplant patients who are CY3A5 expressors (CYP3A5*1) required a higher dose of tacrolimus to achieve therapeutic trough concentration than nonexpressors (CYP3A5*3) (Thervet 1 Centre de Ge ´nomique Humaine, Faculte ´ de Me ´decine et de Pharmacie, Universite ´ Mohammed V Souissi, Rabat, Morocco. 2 De ´partement de Ge ´ne ´tique Me ´dicale, Institut National d’Hygie `ne, Rabat, Morocco. 3 Service de Ne ´phrologie Dialyse et Transplantation Re ´nale, Hopital Militaire d’instruction Mohammed V, Rabat, Morocco. 4 Centre National de Re ´fe ´rence en Ne ´onatologie et en Nutrition, Rabat, Morocco. *These authors contributed in the same way to the realization of this work. GENETIC TESTING AND MOLECULAR BIOMARKERS Volume 16, Number 6, 2012 ª Mary Ann Liebert, Inc. Pp. 644–647 DOI: 10.1089/gtmb.2011.0240 644
Transcript of Frequencies of CYP3A5*1/*3 Variants in a Moroccan Population and Effect...
Frequencies of CYP3A5*1/*3 Variantsin a Moroccan Population and Effect on Tacrolimus
Daily Dose Requirements in Renal Transplant Patients
Mustapha Elmachad,1,2,* Driss Elkabbaj,3,* Fatiha Elkerch,2 Fatima Zahra Laarabi,2
Amina Barkat,4 Zouhir Oualim,3 and Abdelaziz Sefiani1,2
The cytochromes P450 are a superfamily of oxidative enzymes, which are implicated in the metabolism of a largenumber of endogenous substances as well as exogenous chemicals. The cytochrome P450 (CYP3A5) appears toplay an important role in drug metabolism activity. The most frequent mutation in the CYP3A5 gene, affectingits activity, consists of a G6986A transition within intron 3. In this study, we determined the allelic frequency ofCYP3A5*3 in a Moroccan population, consisting of 108 individuals including 10 renal transplant patients. About8.33% (9/108) of the subjects were homozygous wild-type (CYP3A5*1/*1), 37.04% (40/108) were heterozygous(CYP3A5*1/*3), and 54.63% (59/108) were homozygous (CYP3A5*3/*3). Therefore, CYP3A5*3 variant was themost frequent allele detected at 73.15%. In the second part of this work, we assessed the influence of the CYP3A5polymorphism on tacrolimus doses required for 10 renal transplant patients who are receiving tacrolimus asimmunosuppressive therapy. Our results showed that, during the first 3 months after kidney transplantation,the tacrolimus daily requirements for heterozygous patients (CYP3A5*3/*1) were higher compared with ho-mozygous patients (CYP3A5*3/*3) (0.133 – 0.026 vs. 0.21 – 0.037 mg/kg/day). After the third month the differ-ence was also observed, whereby the mean of tacrolimus daily requirements for patients with CYP3A5*3/*3and CYP3A5*1/*3 was 0.053 – 0.013 and 0.08 – 0.014 mg/kg/day, respectively. This first study in Morocco pro-vides genetic data related to the frequency of genetic polymorphisms of CYP3A5 and opens the perspective todevelop other pharmacogenetic studies.
Introduction
The cytochromes P450 are a superfamily of oxidativeenzymes, which are implicated in the metabolism of a
large number of endogenous substances as well as exogenouschemicals (Thompson et al., 2004). The cytochromes P450s areinvolved in the oxidation of *40%–60% of commonly useddrugs. CYP3A4 and CYP3A5 are two major isoforms ofCYP3A subfamily expressed in adult human tissues. CYP3A4is found in the liver and small intestine, whereas CYP3A5 ispolymorphically expressed in the liver, small intestine, kid-ney, and other organs (Murray et al., 1999; Paine et al., 2006).These isoforms represent the predominant functional forms ofhuman CYP3A (Lin et al., 2002).
Many studies have been focused on the identification ofsequence variation affecting enzyme activity in the CYP3A5gene. The most frequent mutation in this gene consists of a
G6986A transition within intron 3 (CYP3A5*3). This mutationcreates an alternative splice site resulting in a frame shift andtruncation of the protein (Kuehl et al., 2001; Lamba et al., 2002).Individuals who are carrying two copies of a CYP3A5*3 alleleshow a markedly reduced level of CYP3A5 protein expressionand activity (Kuehl et al., 2001).
Many reports suggested that the CYP3A5*3 mutantallele may play an important role in interindividual dif-ferences of response to drug therapy (Ingelman-Sundberget al., 1999; Tsuchiya et al., 2004). The association betweentacrolimus, an immunosuppressive agent for preventingor treating graft rejection in organ transplantation, andCYP3A5 polymorphism was largely investigated in severalstudies. It has been demonstrated that renal transplantpatients who are CY3A5 expressors (CYP3A5*1) required ahigher dose of tacrolimus to achieve therapeutic troughconcentration than nonexpressors (CYP3A5*3) (Thervet
1Centre de Genomique Humaine, Faculte de Medecine et de Pharmacie, Universite Mohammed V Souissi, Rabat, Morocco.2Departement de Genetique Medicale, Institut National d’Hygiene, Rabat, Morocco.3Service de Nephrologie Dialyse et Transplantation Renale, Hopital Militaire d’instruction Mohammed V, Rabat, Morocco.4Centre National de Reference en Neonatologie et en Nutrition, Rabat, Morocco.*These authors contributed in the same way to the realization of this work.
GENETIC TESTING AND MOLECULAR BIOMARKERSVolume 16, Number 6, 2012ª Mary Ann Liebert, Inc.Pp. 644–647DOI: 10.1089/gtmb.2011.0240
644
et al., 2003; Haufroid et al., 2004; Macphee et al., 2005;Quteineh et al., 2008).
In this study, we aimed to determine the allelic frequency ofCYP3A5*3 in the Moroccan population. Moreover, we as-sessed the impact of this polymorphism on the daily doserequired for 10 renal transplant patients undergoing treat-ment with tacrolimus.
Materials and Methods
Subjects
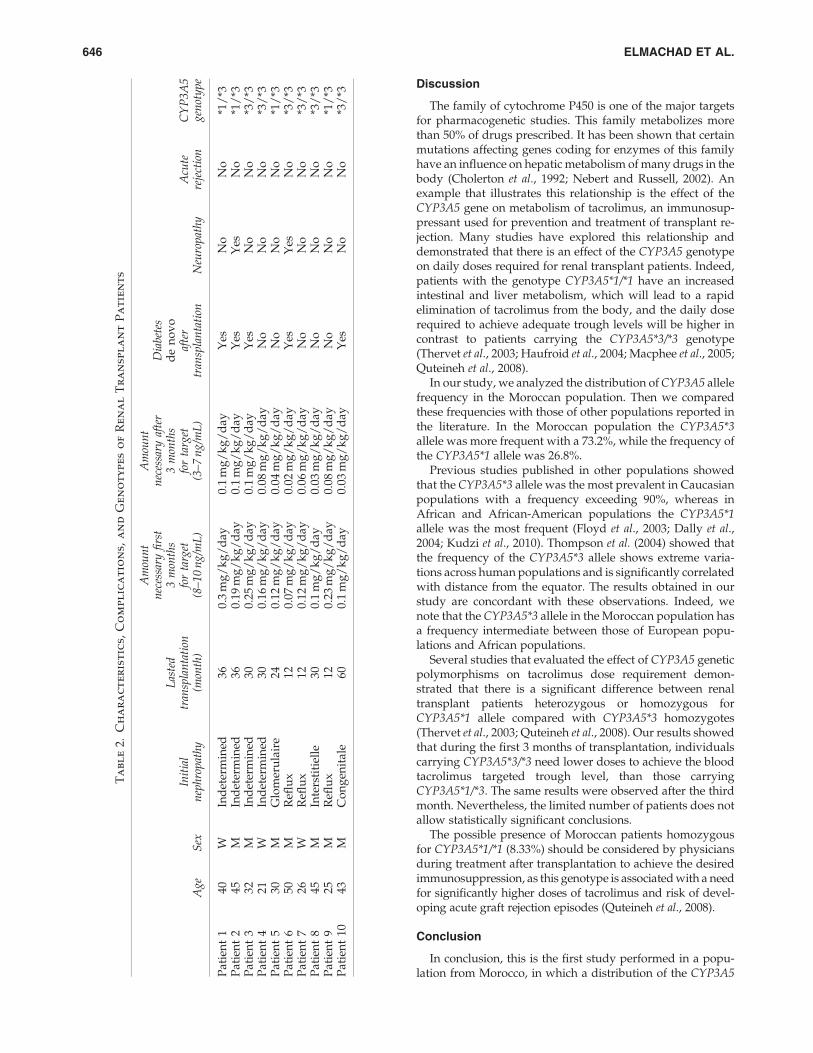
In this study we have genotyped a group of 108 individu-als, including 98 healthy newborn infants and 10 renaltransplant patients (7 men and 3 women). Newborn infantsare from different regions of Morocco and the Moroccan ori-gin of their parents and grandparents was confirmed. All re-nal transplant patients received tacrolimus as their mainimmunosuppressant; the characteristics of patients are shownin Table 2. Informed consent for DNA analysis was obtainedfrom patients and parents of newborns.
DNA samples and polymerase chainreaction conditions
Genomic DNA was extracted from peripheral blood sam-ples, using a salt extraction method. The concentration ofgenomic DNA was determined by measuring the absorbanceby NanoDrop ND-2000 (Nanodrop Technologies). DNA wasstored at - 20�C before use. One hundred nanograms of ex-tracted DNA was amplified in a final volume of 50 mL. Thepolymerase chain reaction (PCR) mixture contained 10mL of5 · buffer (2 mM MgCl2), 0.1 mM each of the deoxynucleotidetriphosphates, 1.5 U of Go Taq (Promega), and 0.6 mM of eachprimer.
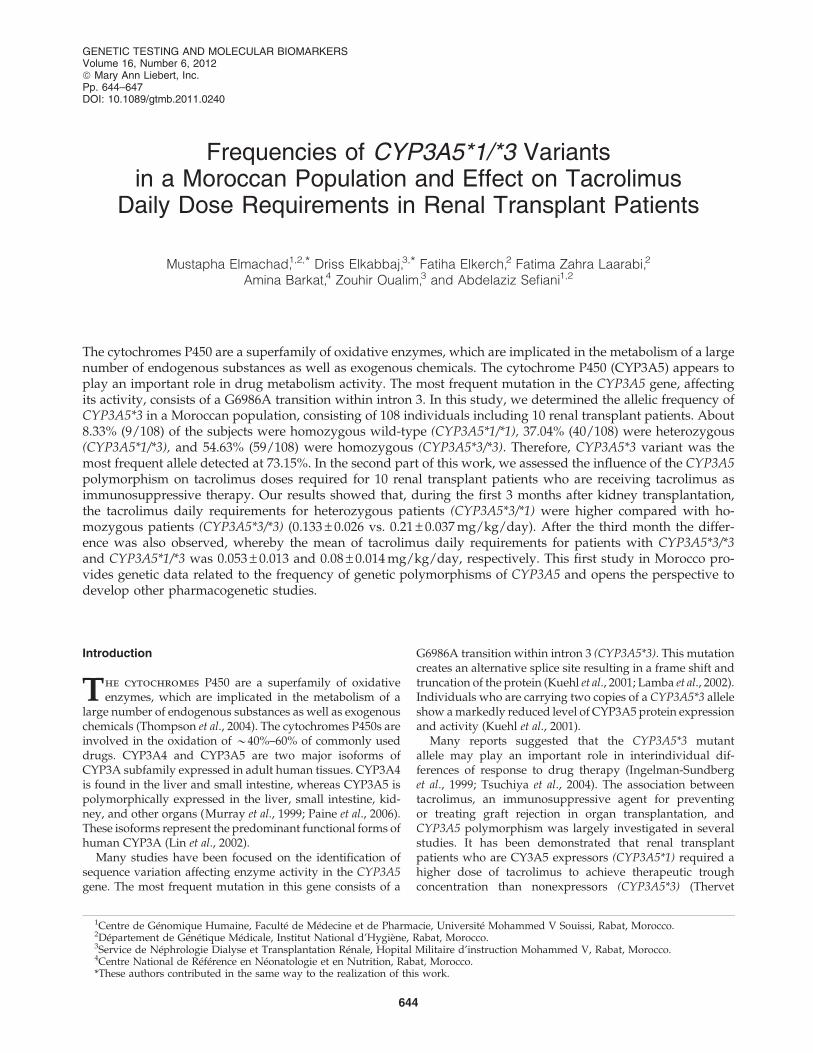
The forward primer was 5¢aaacatataaaacattatggagagtgg3¢and reverse primer was 5¢cacacccaggaagccagact3¢. The PCRconditions were 1 min denaturation at 95�C; 35 cycles of 15 s at95�C, 15 s at 59�C, and 30 s at 72�C; and a final extension stepat 72�C for 7 min. Two microliters of purified product wasamplified using a Big Dye kit (Applied Biosystems) as indi-cated in the manufacturer’s protocol in a final volume of13 mL. The PCR consisted of an initial denaturation step at96�C for 10 s, 25 cycles at 96�C for 10 s, 50�C for 5 s, and 60�Cfor 4 min. The final product was sequenced using an Abi-Prism 310 sequencer (Applied Biosystems) (Fig. 1).
Results
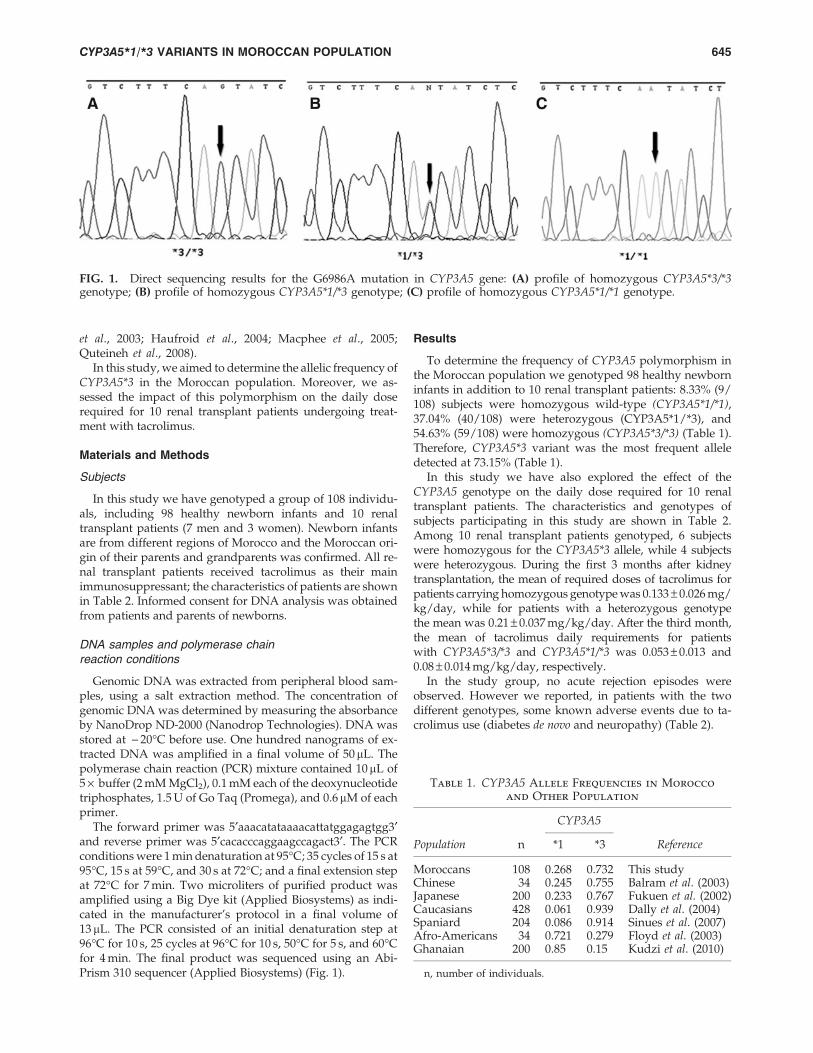
To determine the frequency of CYP3A5 polymorphism inthe Moroccan population we genotyped 98 healthy newborninfants in addition to 10 renal transplant patients: 8.33% (9/108) subjects were homozygous wild-type (CYP3A5*1/*1),37.04% (40/108) were heterozygous (CYP3A5*1/*3), and54.63% (59/108) were homozygous (CYP3A5*3/*3) (Table 1).Therefore, CYP3A5*3 variant was the most frequent alleledetected at 73.15% (Table 1).
In this study we have also explored the effect of theCYP3A5 genotype on the daily dose required for 10 renaltransplant patients. The characteristics and genotypes ofsubjects participating in this study are shown in Table 2.Among 10 renal transplant patients genotyped, 6 subjectswere homozygous for the CYP3A5*3 allele, while 4 subjectswere heterozygous. During the first 3 months after kidneytransplantation, the mean of required doses of tacrolimus forpatients carrying homozygous genotype was 0.133 – 0.026 mg/kg/day, while for patients with a heterozygous genotypethe mean was 0.21 – 0.037 mg/kg/day. After the third month,the mean of tacrolimus daily requirements for patientswith CYP3A5*3/*3 and CYP3A5*1/*3 was 0.053 – 0.013 and0.08 – 0.014 mg/kg/day, respectively.
In the study group, no acute rejection episodes wereobserved. However we reported, in patients with the twodifferent genotypes, some known adverse events due to ta-crolimus use (diabetes de novo and neuropathy) (Table 2).
FIG. 1. Direct sequencing results for the G6986A mutation in CYP3A5 gene: (A) profile of homozygous CYP3A5*3/*3genotype; (B) profile of homozygous CYP3A5*1/*3 genotype; (C) profile of homozygous CYP3A5*1/*1 genotype.
Table 1. CYP3A5 Allele Frequencies in Morocco
and Other Population
CYP3A5
Population n *1 *3 Reference
Moroccans 108 0.268 0.732 This studyChinese 34 0.245 0.755 Balram et al. (2003)Japanese 200 0.233 0.767 Fukuen et al. (2002)Caucasians 428 0.061 0.939 Dally et al. (2004)Spaniard 204 0.086 0.914 Sinues et al. (2007)Afro-Americans 34 0.721 0.279 Floyd et al. (2003)Ghanaian 200 0.85 0.15 Kudzi et al. (2010)
n, number of individuals.
CYP3A5*1/*3 VARIANTS IN MOROCCAN POPULATION 645
Discussion
The family of cytochrome P450 is one of the major targetsfor pharmacogenetic studies. This family metabolizes morethan 50% of drugs prescribed. It has been shown that certainmutations affecting genes coding for enzymes of this familyhave an influence on hepatic metabolism of many drugs in thebody (Cholerton et al., 1992; Nebert and Russell, 2002). Anexample that illustrates this relationship is the effect of theCYP3A5 gene on metabolism of tacrolimus, an immunosup-pressant used for prevention and treatment of transplant re-jection. Many studies have explored this relationship anddemonstrated that there is an effect of the CYP3A5 genotypeon daily doses required for renal transplant patients. Indeed,patients with the genotype CYP3A5*1/*1 have an increasedintestinal and liver metabolism, which will lead to a rapidelimination of tacrolimus from the body, and the daily doserequired to achieve adequate trough levels will be higher incontrast to patients carrying the CYP3A5*3/*3 genotype(Thervet et al., 2003; Haufroid et al., 2004; Macphee et al., 2005;Quteineh et al., 2008).
In our study, we analyzed the distribution of CYP3A5 allelefrequency in the Moroccan population. Then we comparedthese frequencies with those of other populations reported inthe literature. In the Moroccan population the CYP3A5*3allele was more frequent with a 73.2%, while the frequency ofthe CYP3A5*1 allele was 26.8%.
Previous studies published in other populations showedthat the CYP3A5*3 allele was the most prevalent in Caucasianpopulations with a frequency exceeding 90%, whereas inAfrican and African-American populations the CYP3A5*1allele was the most frequent (Floyd et al., 2003; Dally et al.,2004; Kudzi et al., 2010). Thompson et al. (2004) showed thatthe frequency of the CYP3A5*3 allele shows extreme varia-tions across human populations and is significantly correlatedwith distance from the equator. The results obtained in ourstudy are concordant with these observations. Indeed, wenote that the CYP3A5*3 allele in the Moroccan population hasa frequency intermediate between those of European popu-lations and African populations.
Several studies that evaluated the effect of CYP3A5 geneticpolymorphisms on tacrolimus dose requirement demon-strated that there is a significant difference between renaltransplant patients heterozygous or homozygous forCYP3A5*1 allele compared with CYP3A5*3 homozygotes(Thervet et al., 2003; Quteineh et al., 2008). Our results showedthat during the first 3 months of transplantation, individualscarrying CYP3A5*3/*3 need lower doses to achieve the bloodtacrolimus targeted trough level, than those carryingCYP3A5*1/*3. The same results were observed after the thirdmonth. Nevertheless, the limited number of patients does notallow statistically significant conclusions.
The possible presence of Moroccan patients homozygousfor CYP3A5*1/*1 (8.33%) should be considered by physiciansduring treatment after transplantation to achieve the desiredimmunosuppression, as this genotype is associated with a needfor significantly higher doses of tacrolimus and risk of devel-oping acute graft rejection episodes (Quteineh et al., 2008).
Conclusion
In conclusion, this is the first study performed in a popu-lation from Morocco, in which a distribution of the CYP3A5
Ta
bl
e2.
Ch
ar
ac
te
rist
ic
s,
Co
mp
lic
at
io
ns,
an
dG
en
ot
yp
es
of
Re
na
lT
ra
nsp
la
nt
Pa
tie
nt
s
Ag
eS
exIn
itia
ln
eph
rop
ath
y
Las
ted
tran
spla
nta
tion
(mon
th)
Am
oun
tn
eces
sary
firs
t3
mon
ths
for
targ
et(8
–1
0n
g/m
L)
Am
oun
tn
eces
sary
afte
r3
mon
ths
for
targ
et(3
–7
ng
/mL
)
Dia
bete
sd
en
ov
oaf
ter
tran
spla
nta
tion
Neu
rop
ath
yA
cute
reje
ctio
nC
YP
3A
5g
enot
yp
e
Pat
ien
t1
40W
Ind
eter
min
ed36
0.3
mg
/k
g/
day
0.1
mg
/k
g/
day
Yes
No
No
*1/
*3P
atie
nt
245
MIn
det
erm
ined
360.
19m
g/
kg
/d
ay0.
1m
g/
kg
/d
ayY
esY
esN
o*1
/*3
Pat
ien
t3
32M
Ind
eter
min
ed30
0.25
mg
/k
g/
day
0.1
mg
/k
g/
day
Yes
No
No
*3/
*3P
atie
nt
421
WIn
det
erm
ined
300.
16m
g/
kg
/d
ay0.
08m
g/
kg
/d
ayN
oN
oN
o*3
/*3
Pat
ien
t5
30M
Glo
mer
ula
ire
240.
12m
g/
kg
/d
ay0.
04m
g/
kg
/d
ayN
oN
oN
o*1
/*3
Pat
ien
t6
50M
Refl
ux
120.
07m
g/
kg
/d
ay0.
02m
g/
kg
/d
ayY
esY
esN
o*3
/*3
Pat
ien
t7
26W
Refl
ux
120.
12m
g/
kg
/d
ay0.
06m
g/
kg
/d
ayN
oN
oN
o*3
/*3
Pat
ien
t8
45M
Inte
rsti
tiel
le30
0.1
mg
/k
g/
day
0.03
mg
/k
g/
day
No
No
No
*3/
*3P
atie
nt
925
MR
eflu
x12
0.23
mg
/k
g/
day
0.08
mg
/k
g/
day
No
No
No
*1/
*3P
atie
nt
1043
MC
on
gen
ital
e60
0.1
mg
/k
g/
day
0.03
mg
/k
g/
day
Yes
No
No
*3/
*3
646 ELMACHAD ET AL.

variants was investigated in a group of newborn infants. Ourresults showed that frequency of the CYP3A5*1 variant seemsto be higher as compared with the Caucasians and lower thanis found in black Africans. Furthermore, comparison of dosesrequired for 10 renal transplant patients showed a differencebetween patients homozygous for CYP3A5*3 and those whowere heterozygous; this difference needs to be explored byincreasing the number of cases, even if many previous studiesshowed a statistically significant difference only betweenCY3A5*1/*1 and CY3A5*3/*3 genotypes.
Disclosure Statement
No competing financial interests exist.
References
Balram C, Zhou Q, Cheung YB, Lee EJ (2003) CYP3A5*3 and *6single nucleotide polymorphisms in three distinct Asianpopulations. Eur J Clin Pharmacol 59:123–126.
Cholerton S, Daly AK, Idle JR (1992) The role of individualhuman cytochromes P450 in drug metabolism and clinicalresponse. Trends Pharmacol Sci 13:434–439.
Dally H, Bartsch H, Jager B, et al. (2004) Genotype relationshipsin the CYP3A locus in Caucasians. Cancer Lett 207:95–99.
Floyd MD, Gervasini G, Masica AL, et al. (2003) Genotype-phenotype associations for common CYP3A4 and CYP3A5variants in the basal and induced metabolism of midazolam inEuropean- and African-American men and women. Pharma-cogenetics 13:595–606.
Fukuen S, Fukuda T, Maune H, et al. (2002) Novel detectionassay by PCR-RFLP and frequency of the CYP3A5 SNPs,CYP3A5*3 and *6, in a Japanese population. Pharmacogenetics12:331–334.
Haufroid V, Mourad M, Van Kerckhove V, et al. (2004) The effectof CYP3A5 and MDR1 (ABCB1) polymorphisms on cyclo-sporine and tacrolimus dose requirements and trough bloodlevels in stable renal transplant patients. Pharmacogenetics14:147–154.
Ingelman-Sundberg M, Oscarson M, McLellan RA (1999) Poly-morphic human cytochrome P450 enzymes: an opportunityfor individualized drug treatment. Trends Pharmacol Sci20:342–349.
Kudzi W, Dodoo AN, Mills JJ (2010) Genetic polymorphisms inMDR1, CYP3A4 and CYP3A5 genes in a Ghanaian popula-tion: a plausible explanation for altered metabolism of iver-mectin in humans? BMC Med Genet 11:111.
Kuehl P, Zhang J, Lin Y, et al. (2001) Sequence diversity inCYP3A promoters and characterization of the genetic basis ofpolymorphic CYP3A5 expression. Nat Genet 27:383–391.
Lamba JK, Lin YS, Schuetz EG, Thummel KE (2002) Geneticcontribution to variable human CYP3A-mediated metabolism.Adv Drug Deliv Rev 54:1271–1294.
Lin YS, Dowling AL, Quigley SD, et al. (2002) Co-regulationof CYP3A4 and CYP3A5 and contribution to hepatic andintestinal midazolam metabolism. Mol Pharmacol 62:162–172.
Macphee IA, Fredericks S, Mohamed M, et al. (2005) Tacrolimuspharmacogenetics: the CYP3A5*1 allele predicts low dose-normalized tacrolimus blood concentrations in whites andSouth Asians. Transplantation 79:499–502.
Murray GI, McFadyen MC, Mitchell RT, et al. (1999) CytochromeP450 CYP3A in human renal cell cancer. Br J Cancer 79:1836–1842.
Nebert DW, Russell DW (2002) Clinical importance of the cy-tochromes P450. Lancet 360:1155–1162.
Paine MF, Hart HL, Ludington SS, et al. (2006) The human in-testinal cytochrome P450 ‘‘pie’’. Drug Metab Dispos 34:880–886.
Quteineh L, Verstuyft C, Furlan V, et al. (2008) Influence ofCYP3A5 genetic polymorphism on tacrolimus daily dose re-quirements and acute rejection in renal graft recipients. BasicClin Pharmacol Toxicol 103:546–552.
Sinues B, Vicente J, Fanlo A, et al. (2007) CYP3A5*3 and CY-P3A4*1B allele distribution and genotype combinations: dif-ferences between Spaniards and Central Americans. TherDrug Monit 29:412–416.
Thervet E, Anglicheau D, King B, et al. (2003) Impact of cyto-chrome p450 3A5 genetic polymorphism on tacrolimus dosesand concentration-to-dose ratio in renal transplant recipients.Transplantation 76:1233–1235.
Thompson EE, Kuttab-Boulos H, Witonsky D, et al. (2004)CYP3A variation and the evolution of salt-sensitivity variants.Am J Hum Genet 75:1059–1069.
Tsuchiya N, Satoh S, Tada H, et al. (2004) Influence of CYP3A5and MDR1 (ABCB1) polymorphisms on the pharmacokineticsof tacrolimus in renal transplant recipients. Transplantation78:1182–1187.
Address correspondence to:Mustapha Elmachad, Ph.D.
Departement de Genetique MedicaleInstitut National d’Hygiene
27, Avenue Ibn BatoutaB.P. 11400 Rabat
Morocco
E-mail: [email protected]
CYP3A5*1/*3 VARIANTS IN MOROCCAN POPULATION 647


















