KneeKnee. The Views AP Lateral Internal Oblique External Oblique.
Upload
dorian-freemanCategory
view
58download
0description

FOURTH NERVE / SUPERIOR OBLIQUE PALSY FNP / SOP
LIONEL KOWALRVEEH / CERAMELBOURNE

Types of apparent FNP / SOPAll of these LOOK THE SAME
1. Definite SOPOnly true HALF the time that it is diagnosed!
2. Possible SOP or Resolved SOP 3. Idiopathic oblique dysfunction &
othersynonyms for …“CycloVertical Dysfunction of uncertain
cause” = CVDMostly due to minor anatomical ‘errors’
4. Pulley heterotopy radiological diagnosis 5. Something quite different Graves’,
old fracture, other vertical rectus disease, post ret-det surgery, …

Definite SOP / Possible SOP / CVD / pulley heterotopy ….. can all
Vertical misalignment Disrupt horizontal fusion & horizontal misalignment
Head tilts Vertical greater to one side Apparent IO OA, SO UA CLINICAL PICTURE CAN BE THE SAME IN ALL THESE TYPES OF SOP & PSEUDO - SOP

Is it important to differentiate? Lumpers vs splitters
LUMPERSTraditional UK approachAll SOPs get similar treatment
SPLITTERSPost 1950’s US approachIndividualise treatmentto specific subtype ofSOP

Lumpers If it looks / smells / sounds … a bit like SOP, then call it SOP.
‘Congenital SOP’ label used with NO evidence of true palsy
Rx: inf obl weakening IO-Some lumpers: one size fits all. Some : 2-3
different ops Nucci: Milan, EJO sectional editor, trained Italy & Chicago, 62 articles in PubMed,…

Splitters Knapp: important to split7 different types based on detailed measurements and versions
Later subclassified further by others some pts do well with IO- others will do better with SO plication or SR weakening……
Selection bias: strabismus specialist tends to see pts with inadequate results after IO-
LK: a splitter

Lumpers vs Splitters & EBM
21st Century: issues resolved by randomised prospective trial - still waitingEminence based medicine Loudest most forceful & charismatic medical conference personality defines clinical practice. MOST strabismus specialists are splitters

Splitting……
1. Careful measurements in cardinal positions
Allows classification into Knapp types [or more modern variants] and likely surgical solution

Splitting……
2. Radiology:Is it a True SO atrophy: More likely to have floppy SO?less likely to respond to IO-
?more likely to need SO+

MRI X-sectional area of SO segregates SOP from normal SO
When strabismus specialists made clinical diagnosis of SOP, they were wrong 50% of the time!!

Splitting……3. Reserve final surgical plan until intra-operative FDT
If SR is tight, more likely to need SR-
If SO floppy,….If IO is tight,…If IR is tight,…
Need a MUCH larger surgical repertoire than Lumpers

R SOP
HEAD TILT TO LEFT

R IO OA
R SO UA
TIGHT RSR RIR ‘UA’
CORE DEFECT
ADAPTATION TO WEAK SO
ADAPTATION TO CHRONICHYPERTROPIA
ADAPTATIONS MAY DOMINATE THE CLINICALPICTURE

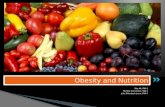
SOP image
LSO OK RSO ?absent

Case #1 Atrophic SO SO UA IO OA SOUA > IO OA IR UA [presumed tight SR from having had a ‘chronic hypertropia’]
LUMPERS : Inf obl weakening SPLITTERS : Final decision after FDT

Splitters Atrophic SO and SO UA:More likely to find floppy SOMore likely to need SO plication Apparent IR UAProbably tight SRNeeds SR- or will have DG diplopia If FDT on SO & SR are OK: IO-

Principles of treatment
Acquired SOP : 12 mo [can Rx earlier if getting worse]
Long standing: Acquired suppression makes it harder to characterise
SPLITTERS:Usually have to treat the
muscular consequences of the SOP rather than the SOP itself

Principles of treatment
1. Make it better - don’t over correct
2. Trauma: look for bilateral SOP3. Accurate measurements SPLITTERS1. Tighten floppy muscles2. Recess tight muscles

Principles of treatment : IO-
Parks’ IO Rc for 10-15 ∆ height in PP
≈ 20 ∆ To lateral edge IR≈ 25 ∆ 2mm ant to edge IR

Principles of treatmentTight SR
‘Chronic hypertropia’ may tight SR, spread of comitance & [apparent] IR UA wch may come to dominate the clinical picture.
SR Rc requiredRecessing SR will increase
extorsion unless it is
temporally transposed

TREATMENT EXPECTATIONS
LK audit early 90’s n=450
Unilateral SOP [all sorts]: 1.3 surgeries 90+% Very Good to excellent

SOPDifficult area of strabismusLumpers vs Splitters : unresolved
Splitters more likely to see the more complex pts & believe that a more complicated approach is the correct one

The contralateral inferior rectus
Lumpers 1st op: inf obl 2nd op: c/l inf rectusSplitters Consider c/l inf rectus if tight or if SO UA without SO floppiness

The contralateral inferior rectus
• MRI of the Functional Anatomy of the Inferior Rectus Muscle in Superior Oblique Muscle Palsy.Jiang L, Demer JL.UCLA Ophthalmology. November 2008.
• PURPOSE: Biomechanical modeling consistently indicates that SO muscle weakness alone is insufficient to explain the large hypertropia often observed in SOP. MRI : to investigate if any size or contractility changes in IR may contribute.
• 17 pats with unilateral SOP and 18 orthotropic controls.
• Diagnosis of SOP based on clinical presentations, subnormal contractility & small SO muscle size

The contralateral inferior rectus
•OUTCOME MEASURES: X-sectional areas of IR & SO.
•RESULTS: Patients had 16+/-7∆ of central gaze hypertropia and exhibited ipsilesional SO muscle atrophy and subnormal contractility.
•CONCLUSIONS: ..the contralesional IR is larger and more contractile than the ipsilesional IR, reflecting likely neurally mediated changes that augment the relatively small hypertropia resulting from SOP.
•Recession of the hyperfunctioning contralesional IR in SOP is a physiologic therapy.