Four New Cases and Review of the Literaturewilliams.medicine.wisc.edu/schnitzler.pdf ·...
14
Introduction The Schnitzler syndrome is defined by a unique and particular constellation of clinical and biologic signs including chronic urticaria, intermittent fever, bone pain, arthralgia or arthritis, and a monoclonal IgM gammopathy. The syndrome was described by Schnitzler, a French dermatologist, in 1972 (42) and since then more than 40 other patients have been re- ported. The syndrome is often underdiagnosed, and the delay to diagnosis is more than 5 years in most cases. Because of the variety of clinical signs, this syndrome is of concern to the dermatologist, the in- ternist, the rheumatologist, and the hematologist. Many patients have seen all these specialists before the diagnosis is established. In this study, we report 4 new patients with this syndrome and review all cases in the English, German, and French literature. Patients and Methods We report here 4 new cases and the results of a literature review of the Schnitzler syndrome. A MEDLINE (National Library of Med- icine, Bethesda, MD) search was performed using the key words “urticaria” and “monoclonal gammopathy”; “urticaria” and “IgM”; “urticaria” and “macroglobulinemia”; and “Schnitzler syndrome.” The search period was 1966–2000. Both English and non-English literature were retrieved. Only patients with chronic urticaria and a monoclonal IgM gammopathy, in the absence of any other dis- ease that might explain these findings, were included. Case Reports From 1992 to 2000, we investigated 4 patients with the Schnitz- ler syndrome. None of these patients have been reported previ- ously. Two of these patients were followed in the dermatology de- partment of a university hospital (Patients 1 and 2), 1 in the inter- nal medicine department of a university hospital (Patient 3), and 1 in the dermatology department of a military hospital (Patient 4). Patient 1 A 67-year-old man had a 6-year history of persistent, antihista- mine-resistant urticaria. He had been examined already by 5 physi- cians, including dermatologists and hematologists, but no diagnosis had been established. Usually, individual lesions resolved within 24–48 hours. They consisted of moderately pruritic rose macules or maculopapules with varying topography (Figures 1 and 2). The face, the soles, and the palms were spared. He never experienced an- gioedema. Concomitant with the urticaria, he had experienced arthralgia affecting the shoulders and recurrent episodes of fever. The fever, which could reach 39 C, was well tolerated, and was ac- companied by an exaggeration of the skin rash. Alcohol ingestion also aggravated the skin rash. He reported occasional night sweats. On examination, he had a widespread, edematous, maculopapular rash, as well as palpable inguinal and axillary lymph nodes. Histologic examination of a biopsy from an urticarial lesion showed edema and a perivascular infiltrate of neutrophils and eosinophils in the papillary dermis. Fibrinoid deposits were seen around dilated superficial blood vessels. However, fibrinoid necro- sis, the hallmark of fully developed leukocytoclastic vasculitis, was not seen. Immunofluorescence studies were negative. Laboratory investigations showed a moderately increased ery- throcyte sedimentation rate (ESR) of 32 mm/h; C reactive protein level was 17.8 mg/dL. Interleukin (IL)-6 level was increased to 97.1 pg/mL (normal 20 pg/mL), IL-2 receptor level was slightly in- creased to 230 pg/mL (normal 190 pg/mL), while tumor necrosis factor (TNF) and IL-8 levels were within normal range. Serum pro- tein electrophoresis demonstrated a monoclonal IgM component with kappa light chains on immunofixation. No Bence-Jones pro- teinuria was detectable. Total IgM was 5.4 g/L (normal, 0.4–3.1 g/L); IgG, IgA, IgD, complement hemolytic assay (CH) 50, C3, C4, and C1- inh were in normal range. There were no antinuclear antibodies, cold agglutinins, cryofibrinogen, or cryoglobulins. Antibodies to myelin glycoprotein were absent. An IgM anti-IgG rheumatoid fac- tor was present at 30.8 U/mL (normal 11 U/mL). Hepatitis C was excluded. Creatinine, complete blood count, and serum calcium were in normal range. Skeletal X-rays were normal. Bone marrow aspirates and histology showed no abnormality. The histologic ex- amination of an axillary lymph node showed inflammatory hyper- plasia. Cerebral and thoracic scans and abdominal sonography were normal. 0025-7974/01/8001-0037/0 MEDICINE ® 80: 37-44, 2001 Vol. 80, No. 1 Copyright © 2001 by Lippincott Williams & Wilkins, Inc. Printed in U.S.A. The Schnitzler Syndrome Four New Cases and Review of the Literature DAN LIPSKER, YOLANDE VERAN, FABIENNE GRUNENBERGER, BERNARD CRIBIER, ERNEST HEID, AND EDOUARD GROSSHANS 37 From Clinique Dermatologique (DL, BC, EH, EG) and Service de Médecine Interne (FG), Hôpitaux Universitaires, Strasbourg, and Hôpital d’Instruction des armées Legouest (YV), Metz, France. Address reprint requests to: D. Lipsker, Clinique Derma- tologique, 1, Place de l’hôpital, F-67091 Strasbourg Cedex, France. Fax: 33 3 88 11 60 40; e-mail: [email protected]. Lipsker-MD-0106-01/01 12/21/2000 2:14 PM Page 37 (Black plate)
Transcript of Four New Cases and Review of the Literaturewilliams.medicine.wisc.edu/schnitzler.pdf ·...

Introduction
The Schnitzler syndrome is defined by a uniqueand particular constellation of clinical and biologicsigns including chronic urticaria, intermittent fever,bone pain, arthralgia or arthritis, and a monoclonalIgM gammopathy. The syndrome was described bySchnitzler, a French dermatologist, in 1972 (42) andsince then more than 40 other patients have been re-ported. The syndrome is often underdiagnosed, andthe delay to diagnosis is more than 5 years in mostcases. Because of the variety of clinical signs, thissyndrome is of concern to the dermatologist, the in-ternist, the rheumatologist, and the hematologist.Many patients have seen all these specialists beforethe diagnosis is established. In this study, we report4 new patients with this syndrome and review allcases in the English, German, and French literature.
Patients and Methods
We report here 4 new cases and the results of a literature reviewof the Schnitzler syndrome. A MEDLINE (National Library of Med-icine, Bethesda, MD) search was performed using the key words“urticaria” and “monoclonal gammopathy”; “urticaria” and “IgM”;“urticaria” and “macroglobulinemia”; and “Schnitzler syndrome.”The search period was 1966–2000. Both English and non-Englishliterature were retrieved. Only patients with chronic urticaria anda monoclonal IgM gammopathy, in the absence of any other dis-ease that might explain these findings, were included.
Case Reports
From 1992 to 2000, we investigated 4 patients with the Schnitz-ler syndrome. None of these patients have been reported previ-
ously. Two of these patients were followed in the dermatology de-partment of a university hospital (Patients 1 and 2), 1 in the inter-nal medicine department of a university hospital (Patient 3), and 1in the dermatology department of a military hospital (Patient 4).
Patient 1
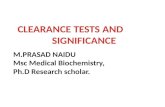
A 67-year-old man had a 6-year history of persistent, antihista-mine-resistant urticaria. He had been examined already by 5 physi-cians, including dermatologists and hematologists, but no diagnosishad been established. Usually, individual lesions resolved within24–48 hours. They consisted of moderately pruritic rose macules ormaculopapules with varying topography (Figures 1 and 2). The face,the soles, and the palms were spared. He never experienced an-gioedema. Concomitant with the urticaria, he had experiencedarthralgia affecting the shoulders and recurrent episodes of fever.The fever, which could reach 39 �C, was well tolerated, and was ac-companied by an exaggeration of the skin rash. Alcohol ingestionalso aggravated the skin rash. He reported occasional night sweats.On examination, he had a widespread, edematous, maculopapularrash, as well as palpable inguinal and axillary lymph nodes.
Histologic examination of a biopsy from an urticarial lesionshowed edema and a perivascular infiltrate of neutrophils andeosinophils in the papillary dermis. Fibrinoid deposits were seenaround dilated superficial blood vessels. However, fibrinoid necro-sis, the hallmark of fully developed leukocytoclastic vasculitis,was not seen. Immunofluorescence studies were negative.
Laboratory investigations showed a moderately increased ery-throcyte sedimentation rate (ESR) of 32 mm/h; C reactive proteinlevel was 17.8 mg/dL. Interleukin (IL)-6 level was increased to 97.1pg/mL (normal � 20 pg/mL), IL-2 receptor level was slightly in-creased to 230 pg/mL (normal � 190 pg/mL), while tumor necrosisfactor (TNF) � and IL-8 levels were within normal range. Serum pro-tein electrophoresis demonstrated a monoclonal IgM componentwith kappa light chains on immunofixation. No Bence-Jones pro-teinuria was detectable. Total IgM was 5.4 g/L (normal, 0.4–3.1 g/L);IgG, IgA, IgD, complement hemolytic assay (CH) 50, C3, C4, and C1-inh were in normal range. There were no antinuclear antibodies,cold agglutinins, cryofibrinogen, or cryoglobulins. Antibodies tomyelin glycoprotein were absent. An IgM anti-IgG rheumatoid fac-tor was present at 30.8 U/mL (normal � 11 U/mL). Hepatitis C wasexcluded. Creatinine, complete blood count, and serum calciumwere in normal range. Skeletal X-rays were normal. Bone marrowaspirates and histology showed no abnormality. The histologic ex-amination of an axillary lymph node showed inflammatory hyper-plasia. Cerebral and thoracic scans and abdominal sonographywere normal.
0025-7974/01/8001-0037/0MEDICINE® 80: 37-44, 2001 Vol. 80, No. 1Copyright © 2001 by Lippincott Williams & Wilkins, Inc. Printed in U.S.A.
The Schnitzler Syndrome
Four New Cases and Review of the Literature
DAN LIPSKER, YOLANDE VERAN, FABIENNE GRUNENBERGER, BERNARD CRIBIER, ERNEST HEID, AND EDOUARD GROSSHANS
37
From Clinique Dermatologique (DL, BC, EH, EG) and Servicede Médecine Interne (FG), Hôpitaux Universitaires, Strasbourg,and Hôpital d’Instruction des armées Legouest (YV), Metz, France.
Address reprint requests to: D. Lipsker, Clinique Derma-tologique, 1, Place de l’hôpital, F-67091 Strasbourg Cedex, France.Fax: 33 3 88 11 60 40; e-mail: [email protected].
Lipsker-MD-0106-01/01 12/21/2000 2:14 PM Page 37 (Black plate)

Lipsker-MD-0106-01/01 12/21/2000 2:14 PM Page 38 (Cyan plate)

Lipsker-MD-0106-01/01 12/21/2000 2:14 PM Page 38 (Magenta plate)

Lipsker-MD-0106-01/01 12/21/2000 2:14 PM Page 38 (Yellow plate)

His symptoms proved difficult to control. Antihistamines (lorata-dine, terfenadine, dexchlorpheniramine, hydroxyzine), colchicine (1mg/d), dapsone (100 mg/d), aspirin (3 g/d), and ibuprofen (1,200mg/d) were ineffective. Psoralens and ultraviolet A (PUVA) therapyallowed moderate improvement of the rash.
This patient was followed for 7 years and still had a daily rash. IgMlevels increased steadily from 2.55 g/L in 1993 to 11 g/L in 2000, butthe monoclonal spike remained stable about 7 g/L in the last 3 years.
Patient 2
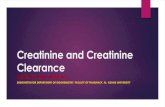
A 41-year-old woman was admitted for chronic urticaria. Theeruption began 3 years earlier and consisted of a daily, mildly pru-ritic rash involving mainly the trunk (Figure 3), but also the face onoccasion. Two years earlier, she had been hospitalized elsewhere toinvestigate the rash and inflammatory arthralgia of the hands andknees. An extensive workup was negative at that time, except for aslightly increased ESR of 22 mm/h and the presence of traces of amonoclonal IgM� gammopathy. No diagnosis was established. Re-cently, she developed intermittent fever, night sweats, and chillsand was therefore referred to us. She was in good general condition,and skin examination revealed numerous red pale macules andmaculopapules mainly on the trunk. Individual lesions resolved
within 24 hours. Fever reached as high as 40 �C. Otherwise, exami-nation was unremarkable except for a single left palpable axillarylymph node.
A skin biopsy showed edema of the upper dermis with an in-flammatory infiltrate rich in neutrophils, which was consistentwith the diagnosis of neutrophilic urticaria. Direct skin immuno-fluorescence studies were negative.
Laboratory investigations showed an elevated ESR of 121 mm/h.IL-6 level was increased to 50.6 pg/mL (normal � 20 pg/mL), IL-2 re-ceptor level was increased to 249 pmol/L (normal � 190 pmol/L),and TNF� level was within normal range. Blood count revealedleukocytosis of 21.69 � 109/L with 18.63 � 109/L neutrophils, slighteosinophilia of 0.58 � 109/L, thrombocytosis of 559 � 109/L, and ane-mia (hemoglobin 99 g/L). Serum protein electrophoresis demon-strated a monoclonal IgM component with kappa light chains onimmunofixation. No Bence-Jones proteinuria was detectable. Themonoclonal component was estimated at 6.1 g/L. Total IgM was 5.35g/L (normal, 0.4–3.1 g/L); IgG, IgA, IgD, CH 50, C3, C4, and C1-inhwere in normal range. There were no antinuclear antibodies, rheu-matoid factor, cold agglutinins, cryofibrinogen, or cryoglobulins.Hepatitis C was excluded. Creatinine and serum calcium were innormal range. Skeletal X-rays were normal. Bone marrow aspiratesand histology showed slight plasmacytosis (8%). Abdominal andthoracic scans were normal.
Antihistamines (cetirizine, hydroxyzine), aspirin (3 g/d), and di-clofenac (150 mg/d) did not alleviate the skin rash. PUVA therapypartly improved the skin rash. Naprosyn (1 g/d) controlled thejoint pain but did not prevent the fever or the skin rash. An in-crease in intensity and duration of the inflammatory symptoms(fever and arthralgia) and a symptomatic inflammatory anemia(6.5 g Hb/dL) necessitated immunosuppressive treatment withchlorambucil (4 mg/d) and dexamethasone 20 mg/d for 5 daysevery 3 weeks. Although this treatment corrected the anemia, andpartially the fever, it did not control skin rash or joint pain. Thispatient was followed for 6 years and still had a daily rash. IgM lev-els steadily increased from 5.35 g/L in 1994 to 17.9 g/L in 2000. Themonoclonal component increased more slightly during the last 3years from 6.1 g/L to 8.1 g/L.
Patient 3
A 74-year-old man had an erythematous widespread eruption of3 years’ duration. Individual lesions resolved within 24–48 hours.
38 LIPSKER ET AL
FIG. 1. Patient 1. Moderately pruritic rose macules and macu-lopapules with varying topography that usually resolved within24–48 hours.
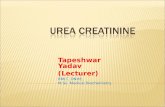
FIG. 2. Patient 1. Pale rose macules and maculopapules.
FIG. 3. Patient 2. Daily, mildly pruritic rash involving mainly thetrunk.
Lipsker-MD-0106-01/01 12/21/2000 2:15 PM Page 38 (Black plate)

Lipsker-MD-0106-01/01 12/21/2000 2:15 PM Page 39 (Cyan plate)

Lipsker-MD-0106-01/01 12/21/2000 2:15 PM Page 39 (Magenta plate)

Lipsker-MD-0106-01/01 12/21/2000 2:15 PM Page 39 (Yellow plate)

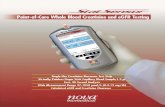
They consisted of rose pale macules or maculopapules with vary-ing topography (Figure 4). The face, the palms, and the soles werenot affected by the eruption, which was not pruritic until recently.He never experienced angioedema. The patient concomitantly de-veloped recurrent fever with peaks above 39.5 �C, and he had lost7 kg in the past 7 months. He complained about morning stiffnessaffecting the hands and feet. On examination, he had bilateral pal-pable axillary lymph nodes.
A cutaneous biopsy showed neutrophilic urticaria rich in eos-inophils. Direct cutaneous immunofluorescence studies showedgranular IgM deposits in the papillary dermis. Laboratory investi-gations showed a moderately increased ESR of 40 mm/h; C reac-tive protein level was 47.7 mg/dL. Serum levels of IL-6, IL-8 andTNF� were in normal range, but the level of the IL-2 receptor wasincreased to 460 pmol/L (normal � 190 pmol/L). Serum proteinelectrophoresis demonstrated a monoclonal IgM component withkappa light chains on immunofixation. No Bence-Jones protein-uria was detectable. The monoclonal IgM spike was 2.6 g/L (nor-mal, 0.4–3.1 g/L); IgG and IgA were in normal range. An undosableIgM� monoclonal spike had been detected 2 years earlier. CH 50,C3, C4, and C1-inh were in normal range. Ferritin and IgD levelswere in normal range. There were no cold agglutinins, cryofib-rinogen, or cryoglobulins. An IgM anti-IgG rheumatoid factor waspresent at 43.5 U/mL (normal � 11 U/mL). The search for antinu-clear antibodies was positive at 1:320. Hepatitis C was excluded.Creatinine and serum calcium were in normal range. Completeblood count revealed moderate anemia. Bone marrow aspiratesand histology showed medullary hypoplasia. Skeletal X-rays werenormal. Morphologic studies of the thorax, abdomen, and pelvisrevealed no abnormality.
Prednisone (20 mg/d), chlorambucil (4 mg/d), ketoprofen (300mg/d), cetirizine (10 mg/d), and hydroxyzine (50 mg/d) proved in-effective to control his symptoms.
This patient was followed for 4 years and still had a daily rash.His monoclonal IgM gammopathy slightly increased about 0.5 g/Levery 6 months in the last 3 years.
Patient 4
A 49-year-old man was referred for a rash of 2 years’ duration.His eruption started 2 years ago and consisted of erythematous,nonpruritic, slightly elevated red plaques. Individual lesions ap-
peared daily, lasted about 12 hours, and resolved without sequel.The eruption involved the whole body, including the face, but thepatient never experienced angioedema. The patient noticed thatthe rash was triggered when he ingested alcohol and spicy food. Afew months after the eruption started, other clinical signs ap-peared. He developed fever about twice a week, up to 39.8 �C, of-ten preceded by chills as well as inflammatory arthralgia of theknees and ankles and pain in both tibias. His examination was oth-erwise unremarkable except for a xanthelasma at the right eyelid.
A cutaneous biopsy showed neutrophilic urticaria. Direct cuta-neous immunofluorescence studies revealed no immunoglobulinor complement deposition. Laboratory investigations showed anincreased ESR of 66 mm/h; C reactive protein level was 53 mg/L.Serum level of TNF� was in normal range, but the level of the IL-2 receptor was increased to 514 pmol/L (normal � 190) and IL-6level was increased to 41 pg/mL (normal � 20 pg/mL). Serum pro-tein electrophoresis demonstrated a monoclonal IgM componentwith kappa light chains on immunofixation. No Bence-Jones pro-teinuria was detectable. The monoclonal IgM spike was 5.3 g/L(normal, 0.4–3.1 g/L); IgG and IgA levels were moderately in-creased to 16.4 g/L and 4.79 g/L, respectively. An undosable IgM�
monoclonal spike had been detected 2 years earlier. CH 50, C3, C4,and C1-inh were normal. Ferritin level was increased to 424 ng/mL(normal � 284 ng/mL), and IgD level was in normal range. Therewere no cold agglutinins, cryofibrinogen, or cryoglobulins. No an-tinuclear antibodies were detected. Hepatitis C was excluded. Cre-atinine and serum calcium were in normal range. Complete bloodcount revealed a moderate anemia (10.5 g Hb/dL) and leukocyto-sis (11.41 � 109/L leukocytes, 8 � 109/L neutrophils), and throm-bocytosis (442 � 109/L). Bone marrow aspirates and histologywere normal. Skeletal X-rays were normal. Morphologic studies ofthe thorax, abdomen, and pelvis revealed no abnormality.
Prednisone (20 mg/d) and ibuprofen (800 mg/d) proved inef-fective to control his symptoms. This patient was followed for 2years and still had a daily rash.
Discussion
The Schnitzler syndrome is a rare and probably un-derdiagnosed disorder. Including the 4 patients re-ported here, 52 patients with this syndrome havebeen reported to date (1–9, 10–26, 29–32, 35–40,42–44, 46–50). The mean delay to diagnosis was 5.4years (SD 4.9 yr). Mean age at diagnosis was 60 years(SD 12 yr) and the male to female ratio is 1.45. Ofnote, most cases were reported in Europe, mainly inFrance and Spain. Only 3 North American patientswith this syndrome have been reported so far (6, 26).
Clinical signs
The nature and frequency of the different clinicalsigns reported in patients with the Schnitzler syn-drome are shown in Table 1. The presence of the skinrash and the monoclonal IgM component, which de-fine this syndrome, are constant, although the possi-bility of the Schnitzler syndrome without rash hasbeen advocated in a patient with bone pain, bonedensification, and a monoclonal IgM� component
THE SCHNITZLER SYNDROME 39
FIG. 4. Patient 3. Pale rose macules and maculopapules withvarying topography. Individual lesions resolved within 24–48hours.
Lipsker-MD-0106-01/01 12/21/2000 2:15 PM Page 39 (Black plate)

(45). The other 2 most characteristic clinical signsare fever and joint and/or bone pain.
Rash
The rash of the syndrome is distinctive. In the 4 pa-tients we had the opportunity to follow, it consisted ofpale rose, slightly elevated, papules and plaques (seeFigures 1–4). Individual lesions measure 0.5 to 2 or 3cm in diameter. The rash is monomorphic and lesionscan be confluent. New lesions appear daily. They last12–24 hours and then disappear without sequel. Thepresence of purpura within the plaques was reportedin 1 patient (40), but this is an exceptional finding.Short periods ranging from 1 to 2 weeks without erup-tion are possible. In the beginning of the disease, pru-ritus is usually absent. After 3 or 4 years, lesionsbecome mildly pruritic in 29% of patients according tothe review of the literature, although this is not a majorcomplaint. Trunk and limbs are most frequently af-fected and the head and neck area is usually spared.Angioedema is possible, though exceedingly rare. Twoof the patients we followed reported edema of the lipsat 1 occasion. In some patients, the rash is triggered byalcohol ingestion. One of the characteristics of the skinrash is that it is difficult to treat. Antihistamines,steroids, colchicine, dapsone, nonsteroidal antiinflam-matory drugs (NSAIDs), and immunosuppressiveagents have all been tried and gave inconstant results,although they were often effective in controlling othersigns of the syndrome.
Histopathologic examination of the lesions usuallyreveals neutrophilic urticaria. de Castro et al (11) re-viewed 25 skin biopsy specimens from 15 of the orig-inally reported patients and showed that neutrophilic
urticaria is the most common histopathologic find-ing. The 4 patients we followed had neutrophilic ur-ticaria. Fully developed vasculitis is rare (only 2patients in the review by de Castro et al), and there-fore this syndrome should not be classified with theurticarial vasculitides. When immunofluorescencestudies were performed, deposition of immunoreac-tants, mainly IgM, could be found around the super-ficial dermal vessels in about 30% of patients (1, 6, 8,9, 32). In a few noteworthy observations, IgM de-posits were found along the dermal-epidermal junc-tion (21, 35, 37). We recently demonstrated, by meansof immunoelectron microscopic studies and immu-noblotting on epidermal and dermal skin extracts,that IgM-skin interactions play a major role in thepathophysiology of the skin lesion (27). Indeed, anti-skin IgM autoantibodies of the same isotype as theirmonoclonal gammopathies can be present in theserum of some patients with the Schnitzler syn-drome. These IgM autoantibodies seem to deposit invivo in the epidermis and at the dermal-epidermaljunction, in the region of the anchoring fibrils, andthey could thus trigger a local inflammatory responsethat could induce the skin lesions (27).
Fever
Intermittent fever, with peaks over 40 �C, is presentin 90% of patients and is a cardinal feature of the dis-ease. The fever is usually well tolerated and chills arerare. In most patients, there is no relation between thefever and the skin rash. Fever usually responds toNSAIDs or to steroids. The pathophysiology of thefever and of the syndrome in general remain unclear.The presence of anti-IL-1 antibodies was reportedwith increased frequency in this syndrome by Sauratet al (41), but this finding was not confirmed subse-quently by other investigators (19, 31, 32, 37). Wefound elevated IL-6 and/or IL-2 receptor levels in the 4patients reported here, but TNF� and IL-8 levels werein normal range. Although IL-6 is an essential plasmacell growth factor, it is also an acute phase reactantand its increase during a systemic illness is thereforenot surprising. Thus, it remains to be established if theclonal IgM proliferation is primary in nature or the re-sult of a continuous antigenic stimulation. It also re-mains to be established if the IgM plays a role in thesystemic features of the disease, although IgM de-posits in the skin seem to be involved in the patho-physiology of the rash (27).
Musculoskeletal involvement
Musculoskeletal involvement is another cardinalfeature of the disease, affecting 80% of patients. Bonepain (59% of patients) is the most characteristic find-ing, but arthralgia and sometimes fully developed
40 LIPSKER ET AL
TABLE 1. Frequency of clinical findings in 52 patientswith the Schnitzler syndrome
Frequency in % (% of Sign Patients in whom this
Information was Reported)
Skin rash 100/100Pruritus 29/79Fever 90/92Arthralgia and/or arthritis 59/94Bone pain 59/79Liver and/or spleen enlargement 33/83Palpable lymph nodes 50/85Elevated ESR (�30 mm/h) 98/87Leukocytosis (�10 � 109/L) 89/85Monoclonal IgM component 100/100Kappa light chain 89/87Abnormalities in IgG and/or IgA levels 26/67Bence-Jones proteinuria 44/62IgM �10 g/L 33/87IgM deposition in skin 35/71Abnormal bone marrow findings 20/79Abnormal bone morphology 56/79
Abbreviations: ESR erythrocyte sedimentation rate.
Lipsker-MD-0106-01/01 12/21/2000 2:15 PM Page 40 (Black plate)

arthritis are also common (59% of patients). Joint de-struction and/or deformities have not been reportedso far. Bone pain affects mostly the iliac bone and thetibia. Femur, spine, forearm, and clavicle were less of-ten involved. Lecompte et al (26) reviewed the bone in-volvement in this syndrome and its differentialdiagnosis. Bone densification is the most frequent ra-diologic finding. Lytic lesions were reported in 2 pa-tients (17, 22), and 2 patients had periosteal apposition(18, 26). Radiologic differential diagnosis is broad andincludes mastocytosis, POEMS syndrome, Erdheim-Chester disease, Camurati-Englemann or Van Buchemdisease, Buschke-Ollendorf syndrome, osteopetrosis,melorheostosis, ribbing disease, and hypertrophic os-teoarthropathy. Bone technetium scanning reveals hy-perfixation in the areas of radiologic involvement (26).Magnetic resonance imaging was performed in 3 pa-tients (18, 26, 50) and showed medullary bone in-volvement and marrow infiltration without space-occupying features in the affected areas in 2 patients(26, 50). A bone biopsy was performed in 9 patients (4,10, 14, 19, 29, 36, 37, 44, 50). It was normal in 3 patients(14, 42, 48) and showed a nonspecific inflammation in5 patients (4, 10, 19, 29, 36), sometimes associatedwith hyperactive osteoblasts. One patient had histo-logic evidence of osteosclerosis (37).
Palpable lymph nodes and hepatic or splenic enlargement
Palpable lymph nodes are found in 50% of patientsand hepatic or splenic enlargement occurs in 33% ofpatients. Palpable lymph nodes are found in the ax-illa and inguinal sites and sometimes in the cervicalregion. Those lymph nodes can be multiple, persis-tent, and up to 2 or 3 cm large and therefore suggestthe diagnosis of lymphoma, but biopsy shows non-specific inflammation.
Monoclonal IgM component
The monoclonal IgM component is a defining fea-ture of the syndrome. In 89% of patients, it is associ-ated with a kappa light chain. Usually, when diagnosisof the syndrome is made, IgM levels are low (�10 g/Lin 67% of patients). IgM levels can remain stable or in-crease progressively at a rate of about 0.5–1.0 g/L peryear. High IgM levels should raise suspicion of Wal-denström disease. When patients are seen at the verybeginning of the disease, monoclonal IgM componentcan be present at very low (trace) levels. Nashan et al(33) reported a patient with urticaria, fever, arthralgia,elevated ESR, and a monoclonal IgG component andsuggested that their observation could be a variant ofthe Schnitzler syndrome. We reported a patient inwhom urticaria seemed to be related to a myeloma-tous IgA monoclonal spike, but this patient was lack-
ing the other features of the Schnitzler syndrome (28).Bence-Jones proteinuria was reported in 44% of pa-tients. In about 26% of patients, lowered levels of IgGor IgA can be found. At the time of diagnosis, exami-nation of bone marrow is normal in 80% of patients. Inthe remaining 20%, unspecific, polyclonal, lympho-cytic, or plasmocytic infiltrates were reported.
Laboratory findings and differential diagnosis
During the course of the disease, elevated ESR is aconstant feature. Complement levels are normal or in-creased in patients with this syndrome. When comple-ment levels are lowered, another diagnosis must beconsidered and the possibility of a genetic deficiencyof C4 should be addressed, since 2 patients with theSchnitzler syndrome had a C4a deficiency (39). Throm-bocytosis and an inflammatory anemia are present inabout 10% of patients. In 2 patients, inflammatory ane-mia was severe and symptomatic (6). One of these 2 pa-tients is reported here (Patient 2), and anemia was sosevere that this patient had to be treated with steroidsand an alkylating agent, to which the anemia re-sponded well. It is noteworthy that persistent leukocy-tosis (�10 � 109/L), in the absence of any treatment,occurred in 90% of patients. In this regard, both adult-onset Still disease and the Schnitzler syndrome can beassociated with a skin rash, fever, palpable lymphnodes, spleen and liver enlargement, arthralgia, andleukocytosis (46). However, ferritin levels are usuallymore elevated in the former while a monoclonal IgMcomponent is present in the latter.
Other diseases that should be considered in the dif-ferential diagnosis of this syndrome are shown in Table2. There is no biologic marker for this disease. Thus, di-agnosis requires a combination of clinical, biologic,and radiologic findings as well as exclusion of otherdiseases. In Table 3, we suggest a combination of cri-teria that can be used to diagnose the Schnitzler syn-drome. Although the criteria are useful for the positivediagnosis of the syndrome, they are not intended to dis-tinguish the Schnitzler syndrome from other diseasesthat can closely mimic this syndrome. Therefore, ex-clusion of other diseases, mainly cryoglobulinemia,hypocomplementic urticarial vasculitis, acquired C1inhibitor deficiency, hyper IgD syndrome, and adult-onset Still disease, remains essential.
Associated findings included pseudoxanthum elas-ticum in 2 patients (29, 49), peripheral neuropathywith the presence of monoclonal IgM with anti-MAG(myelin-associated glycoprotein) in 1 patient (25), C4deficiency in 2 patients (39), and nodular regenera-tive hyperplasia of the liver in 1 patient (24).
Course and treatment
The disease pursues a chronic course. Sponta-neous or treatment-induced remissions have not
THE SCHNITZLER SYNDROME 41
Lipsker-MD-0106-01/01 12/21/2000 2:15 PM Page 41 (Black plate)

been reported. Although the disease features chronicinflammation and a monoclonal component, to ourknowledge no patient has developed systemic amy-loidosis. Nevertheless, amyloidosis should be con-sidered as a possible complication of the syndrome.The prognosis of the Schnitzler syndrome dependson the possible evolution into a lymphoproliferativedisorder, either a lymphoma, including lymphoplas-macytic lymphoma, lymphoma of the Richter type,IgM myeloma, or Waldenström disease. Fifteen per-cent of the patients reported with this syndrome de-veloped lymphoproliferative disorders (1, 9, 20, 30,38, 39, 47, 48). However, the number of patients withthe syndrome who will eventually develop lympho-proliferative disorder is probably much higher, sincethe reports of most patients were published shortlyafter diagnosis, and therefore follow-up was tooshort to draw any conclusion about long-term out-come. Lymphoma or Waldenström disease appearsmore than 10–20 years after the beginning of the firstsigns of the syndrome in most cases. Schnitzler’soriginal patient died from diffuse lymphoplasmacytic
infiltration of the liver and bone marrow 23 years af-ter the first signs of the disease (47). However, in rarecases, Waldenström disease was revealed by theSchnitzler syndrome (9). There is no specific predic-tive factor of the development of a lymphoprolifera-tive disorder. Thus, initial workup of a patient withthis syndrome should include an examination ofbone marrow, immunoelectrophoresis of serum andurinary proteins, and dosage of immunoglobulin sub-types. The 2 latter examinations can then be used tofollow-up those patients on a biannual basis. Lymphnodes should be biopsied when they enlarge.
Treatment of the Schnitzler syndrome is difficultand disappointing. No treatment is constantly effec-tive in treating the skin rash. NSAIDs, most notablyibuprofen (3 � 400 mg/d), should be tried first (15),but in most patients those drugs will ameliorate theskin rash only briefly or not at all (3, 7, 21, 23, 29, 32,36, 50). Antihistamines do not control the skin rash (5,7, 6, 21, 26), and, as the rash is not pruritic in most pa-tients, they are not indicated. The use of inhibitors ofneutrophil migration like colchicine or dapsone ap-pears to be logical in this syndrome characterized byleukocytosis and neutrophilic urticaria, but resultswere inconstant (7, 8, 18, 21, 29, 32, 35, 40). Hydroxy-chloroquine and chloroquine also proved ineffective(6, 21, 36). Steroids and immunosuppressive drugsare not indicated to treat the rash and they are not ef-fective at acceptable dosages (3, 5, 6, 8, 13, 14, 17, 18,22, 31, 32, 35, 36, 37); plasmapheresis (6, 31, 35) andintravenous immunoglobulins (25) also are not effec-tive. Even chemotherapeutic regimens that were pre-scribed to treat the associated hematologic disordersdid not relieve the skin rash. PUVA therapy did reducethe intensity of the skin rash in 2 of the patients re-ported here, and this has been reported (31). Fever,although intermittent, can be disabling. NSAIDs, and
42 LIPSKER ET AL
TABLE 2. Differential diagnosis of the Schnitzler syndrome
Disease Distinguishing Features
Adult-onset Still disease Absence of monoclonal IgM; elevated, low-glycosylated ferritin levels
Hypocomplementemic urticarial vasculitis Cutaneous biopsy shows vasculitis; low complement levels; lupuserythematosous is often associated
Acquired C1 esterase inhibitor deficiency, especially in the setting Usually angioedema; low C4 levels, low functional C1-inh levelsof lymphoma and/or paraproteinemia
Cryoglobulinemia Temperature-dependency of clinical signs, presence of cryo-globulins
Hyper IgD syndrome Elevated IgD levelsErythema marginatum Preceding streptococcal infection; elevated anti-streptococcal
antibodiesSystemic lupus erythematosus Clinical findings suggestive of lupus erythematosus; presence of
antinuclear antibodiesCINCA syndrome* Begins in childhood; neurologic involvement; joint deformitiesMuckle-Wells syndrome Deafness and amyloidosis; absence of monoclonal component;
family historyLymphoma, Waldenström disease Lymph node biopsy, bone marrow biopsy
*CINCA (chronic infantile neurologic cutaneous and articular syndrome) is also called NOMID (neonatal onset multisystem inflam-matory disease).
TABLE 3. Diagnostic criteria for the Schnitzler syndrome*
Urticarial skin rash, monoclonal IgM component, and at least 2of the following criteria:
FeverArthralgia or arthritisBone painPalpable lymph nodesLiver or spleen enlargementElevated erythrocyte sedimentation rateLeukocytosisAbnormal findings on bone morphologic investigations
*Another cause must be eliminated in all cases (see Table 2 fordifferential diagnosis), most notably hyper IgD syndrome, adult-onset Still disease, hypocomplementemic urticarial vasculitis, ac-quired C1 inhibitor deficiency, and cryoglobulinemia.
Lipsker-MD-0106-01/01 12/21/2000 2:15 PM Page 42 (Black plate)

sometimes steroids or immunosuppressive agents (3,7, 13, 14, 17, 21, 23, 29, 32, 35, 36, 37, 50), alleviate it.Bone pain and arthralgia most often respond well toshort treatments with NSAIDs (3, 7, 21, 23, 29, 32, 36,50). Pramidorate was reported to be an effectivetreatment of bone pain in 1 patient (34). Thus, treat-ment depends on the nature and intensity of symp-toms. NSAIDs are the first choice in most patients andcan be associated with colchicine or dapsone. Ster-oids and immunosuppressive agents are only indica-ted when systemic symptoms like fever or arthralgiaare disabling and do not respond to the first-line treat-ments. (When symptoms do not respond to first-linetreatments but are tolerable, those agents should notbe used.) In rare cases, disabling inflammatory ane-mia can necessitate introduction of steroids and alky-lating agents (6).
Summary
The Schnitzler syndrome is characterized by achronic urticarial eruption with a monoclonal IgMgammopathy. The other signs of the syndrome includeintermittent elevated fever, joint and/or bone pain withradiologic evidence of osteosclerosis, palpable lymphnodes, enlarged liver and/or spleen, elevated erythro-cyte sedimentation rate, and leukocytosis. The meandelay to diagnosis is more than 5 years, and this syn-drome is of concern to internists and many medicalspecialists. Patients with this syndrome are often ini-tially considered to have lymphoma or adult-onset Stilldisease, which are the main differential diagnoses.However, hypocomplementic urticarial vasculitis, sys-temic lupus erythematosus, cryoglobulinemia, ac-quired C1 inhibitor deficiency, hyper IgD syndrome,chronic infantile neurologic cutaneous and articular(CINCA) syndrome, and Muckle-Wells syndromeshould also be excluded, because diagnosis relies on acombination of clinical and biologic signs and there isno specific marker of the disease. The disease pursuesa chronic course, and no remissions have yet been re-ported. Disabling skin rash, fever, and musculoskele-tal involvement are the most frequent complications.Severe anemia of chronic disease is another seriouscomplication. The most harmful complication, how-ever, is evolution to an authentic lymphoplasmacyticmalignancy, which occurs in at least 15% of patients.This hematologic transformation can occur more than20 years after the first signs of the disease, thus pa-tients deserve long-term follow-up. Treatment is symp-tomatic and unsatisfactory. The skin rash is un-responsive to treatment, and nonsteroidal antiinflam-matory drugs, antihistamines, dapsone, colchicine,and psoralens and ultraviolet A (PUVA) therapy giveinconstant results. Fever, arthralgia, and bone pain of-ten respond to nonsteroidal antiinflammatory drugs.
In some patients, these symptoms and/or the presenceof severe inflammatory anemia require steroids and/orimmunosuppressive treatment, which ameliorate in-flammatory symptoms but do not change the course ofthe skin rash.
References
1. Altmeyer P, Welke S. Makroglobulinamie Waldenstrom, assoziiert miteinem chronisch rezidivierenden urtikariellen Exanthem. Akt Derma-tol 3: 71–76, 1977.
2. Aractingi S, Flageul B, Caux F, Rybojad M, Andre C, Brouet JC, Fer-mand JP. Immunofluorescence cutanee directe et indirecte au cours devascularites urticariennes associees aux IgM monoclonales. Ann Der-matol Venereol 122(S): 132–33, 1995.
3. Baleva M, Vulcheva T, Nikolov K. Vascularite urticarienne et macroglob-ulinemie (syndrome de Schnitzler) apres une sinusite maxillaire severeet une septicemie fongique: A propos d’une observation. Nouv Dermatol14: 53–54, 1995.
4. Barriere H, Schnitzler L, Moulin G, Grolleau Y. Lesions urticarienneschroniques et macroglobulinemie. A propos de cinq observations. SemHop Paris 52: 221–27, 1976.
5. Baty V, Hoen B, Hudziak H, Aghassian C, Jeandel C, Canton P. Schnitz-ler’s syndrome: Two case reports and review of the literature. MayoClin Proc 70: 570–72, 1995.
6. Berdy SS, Bloch KJ. Schnitzler’s syndrome: A broader clinical spec-trum. J Allergy Clin Immunol 87: 849–54, 1991.
7. Bonnetblanc JM, Drouet M, Laplaud P, Bedane C, Bernard P. Urticariawith macroglobulinaemia: Disease activity associated alterations inimmunoglobulins profile and bone marrow hypodiploidy. Dermatolog-ica 181: 41–43, 1990.
8. Borradori L, Rybojad M, Puissant A, Dallot A, Verola O, Morel P. Ur-ticarial vasculitis associated with a monoclonal IgM gammopathy:Schnitzler’s syndrome. Br J Dermatol 123: 113–18, 1990.
9. Carlioz R, Haas C, Jaubert F, Allouche C, Lowenstein W, Le Jeunne C,Durand H. Maladie de Waldenstrom avec lymphome diffus a grandescellules immunoblastiques et urticaire chronique. Ann Med Interne140: 51–78, 1989.
10. Clauvel JP, Brouet JC, Danon F, Leibowitch M, Seligmann M. Chronicurticaria with monoclonal IgM: A report of five cases. Clin Immunol Im-munopathol 25: 348–53, 1982.
11. de Castro FR, Masouye I, Winkelmann RK, Saurat JH. Urticarial pathol-ogy in Schnitzler’s (hyper-IgM) syndrome. Dermatology 193: 94–99,1996.
12. de Kleijn EM, Telgt D, Laan R. Schnitzler’s syndrome presenting asfever of unknown origin (FUO). The role of cytokines in its systemicfeatures. Neth J Med 51: 140–42, 1997.
13. De Saint-Pierre V, Ehrhart A, Baron D, Plantin P, Le Goff P. Urticairesystemique, osteopathie condensante, gammapathie monoclonale (syn-drome de Schnitzler): A propos d’un cas. Rev Rhum Mal Osteoartic 59:288–92, 1992.
14. Doutre MS, Beylot C, Bioulac P, Bezian JH. Monoclonal IgM andchronic urticaria: Two cases. Ann Allergy 58: 413–14, 1987.
15. Doutre MS, Beylot C. Chronic urticaria and monoclonal IgM: Treat-ment with ibuprofen [letter]. J Am Acad Dermatol 22: 143–44, 1990.
16. Dupuy O, Pinede L, Coppere B, Duhaut P, Pasquier J, Ninet J. Syn-drome de Schnitzler d’evolution stable sur une periode de 18 ans: Uneobservation. Presse Med 24: 1402, 1995.
17. Ferrando FJ, Pujol J, Hortells JL, Navarro M, Pinol J, Carapeto FJ.Schnitzler’s syndrome: Report of a case with bone osteolysis. J InvestAllergol Clin Immunol 4: 203–5, 1994.
18. Germain P, Fach J, Bui N, Traissac T, Delbrel X, Bras ML, Longy-Bour-sier M. Syndrome de Schnitzler: Une cause rare d’urticaire systemique.Rev Med Interne 21: 285–89, 2000.
19. Goupille P, Pizzuti P, Diot E, Jattiot F, Guilmot JL, Valat JP. Schnitzler’ssyndrome (urticaria with macroglobulinemia) dramatically improvedwith corticosteroids. Clin Exp Rheumatol 13: 95–98, 1995.
20. Govindaraju S, Brochot P, Ringot AC, Paternotte L, Morrone A, Es-chard JP, Etienne JC. Urticaire chronique-macroglobulinemie (syn-drome de Schnitzler): Evolution vers un myelome a IgM. A propos d’uncas. Rev Med Interne 14: 780–83, 1993.
21. Janier M, Bonvalet D, Blanc MF, Lemarchand F, Cavelier B, RibriouxA, Aguenier B, Civatte J. Chronic urticaria and macroglobulinemia(Schnitzler’s syndrome): Report of two cases. J Am Acad Dermatol 20:206–11, 1989.
THE SCHNITZLER SYNDROME 43
Lipsker-MD-0106-01/01 12/21/2000 2:15 PM Page 43 (Black plate)

22. Lambert D, Legoux A, Chapuis JL, Benoit JP, Putelat R. Urticairechronique et macroglobulinemie. Nouv Presse Med 11: 1948, 1982.
23. Lautenschlager S, Itin P. Das Schnitzler Syndrom. Hautarzt 44: 781–84,1993.
24. Lauwers A, Chouvy V, Mosnier JF, Misery L, Alexandre C. A case ofSchnitzler’s syndrome with nodular regenerative hyperplasia of theliver. Rev Rhum Engl Ed 66: 281–83, 1999.
25. Lebbe C, Rybojad M, Klein F, Oksenhendler E, Catala M, Danon F,Morel P. Schnitzler’s syndrome associated with sensorimotor neu-ropathy. J Am Acad Dermatol 30: 316–18, 1994.
26. Lecompte M, Blais G, Bisson G, Maynard B. Schnitzler’s syndrome.Skeletal Radiol 27: 294–96, 1998.
27. Lipsker D, Spehner D, Drillien R, Schmitt P, Cribier B, Heid E, HumbelRL, Grosshans E. Schnitzler syndrome: Heterogeneous immunopatho-logical findings involving IgM-skin interactions. Br J Dermatol 142:954–59, 2000.
28. Lipsker D, Cribier B, Maloisel F, Heid E, Grosshans E. Chronic ur-ticaria and IgA myeloma. Acta Derm Venereol (Stockh) 78: 395, 1998.
29. Machet L, Vaillant L, Machet MC, Esteve E, De Muret A, Khallouf R, Ar-beille B, Muller C, Lorette G. Schnitzler’s syndrome (urticaria andmacroglobulinemia) associated with pseudoxanthoma elasticum. ActaDerm Venereol (Stockh) 72: 22–24, 1991.
30. Machet L, Vaillant L, Machet MC, Reisenleiter M, Goupille P, Lorette G.Schnitzler’s syndrome (urticaria and macroglobulinemia): Evolutionto Waldenstrom’s disease is not uncommon. Acta Derm Venereol(Stockh) 76: 413, 1996.
31. Modiano P, Barbaud A, Laveine E, Cabut S, Weber M, Schmutz JL. Ef-ficacite de la PUVAtherapie dans un syndrome de Schnitzler. NouvDermatol 14: 362–63, 1995.
32. Morita A, Sakakibara S, Yokota M, Tsuji T. A case of urticarial vasculi-tis associated with macroglobulinemia (Schnitzler’s syndrome). J Der-matol 22: 32–35, 1995.
33. Nashan D, Sunderkotter C, Bonsmann G, Luger T, Goerdt S. Chronicurticaria, arthralgia, raised eythrocyte sedimentation rate and IgGparaproteinaemia: A variant of Schnitzler’s syndrome? Br J Dermatol133: 132–34, 1995.
34. Oborilova A, Adam Z. Schnitzler’s syndrome. Vnitr Lek 44: 423–27, 1998.35. Olsen E, Forre O, Lea T, Langeland T. Unique antigenic determinants
(idiotypes) used as markers in a patient with macroglobulinemia ur-ticaria: Similar idiotypes demonstrated in the skin and on peripheralblood lymphocytes. Acta Med Scan 207: 379–84, 1980.
36. Paulin P, Cusset C, Jaquelin L, Pages JM, Chapalain JC. Syndrome deSchnitzler: Une nouvelle observation. Presse Med 21: 1758–61, 1992.
37. Puddu P, Cianchini G, Girardelli CR, Colonna L, Gatti S, De Pita O.Schnitzler’s syndrome: Report of a new case and review of the litera-ture. Clin Exp Rheumatol 15: 91–95, 1997.
38. Pujol RM, Barnadas MA, Brunet S, de Moragas JM. Urticarial dermato-sis associated with Waldenstrom’s macroglobulinemia. J Am AcadDermatol 20: 855–57, 1989.
39. Rybojad M, Moraillon I, Cordoliani F, Lebbe C, Baccard M, Flageul B,Weiss L, Morel P. Syndrome de Schnitzler avec deficit genetique en C4:Deux observations. Ann Dermatol Venereol 120: 783–85, 1993.
40. Sanmartin O, Febrer I, Botella R, Grau M, de la Cuandra J, Aliaga A. Ur-ticarial lesions and monoclonal IgM gammopathy. Arch Dermatol 130:1193–98, 1994.
41. Saurat JH, Schifferli J, Steiger G, Dayer JM, Didierjean L. Anti-interleukin-1 alpha autoantibodies in humans: Characterization, isotype distribution,and receptor-binding inhibition—higher frequency in Schnitzler’s syn-drome (urticaria and macroglobulinemia). J Allergy Clin Immunol 88:244–56, 1991.
42. Schnitzler L. Lesions urticariennes chroniques permanentes (erythemepetaloide?) Cas cliniques, no. 46 B. Journee Dermatologique d’Angers,28 octobre 1972.
43. Schnitzler L, Schubert B, Boasson M, Gardais J, Tourmen A. Urticairechronique, lesions osseuses, macroglobulinemie IgM: Maladie de Wal-denstrom? 2nd presentation. Bull Soc Fr Dermatol Syphil 81: 363, 1974.
44. Schnitzler L, Hurez D, Verret JL. Urticaire chronique-osteocodensa-tion-macroglobulinemie. Cas princeps. Etude sur 20 ans. Ann Derma-tol Venereol 116: 547–50, 1989.
45. Soubrier M, Dubost JJ, Jouanel P, Tridon A, Flori B, Leguille C, RistoriJM, Bussiere JL. Multiples complications d’une IgM monoclonale. RevMed Interne 15: 484–86, 1994.
46. Tomkova H, Shirafuji Y, Arata J. Schnitzler’s syndrome versus adult on-set Still’s disease. Eur J Dermatol 8: 118–21, 1998.
47. Verret JL, Leclech C, Rousselet MC, Hurez D, Schnitzler L. Syndromede Schnitzler et maladie de Waldenstrom. Evolution terminale du casprinceps. Ann Dermatol Venereol 120: 459–60, 1993.
48. Welsh B, Tate B. Schnitzler’s syndrome: Report of a case with pro-gression to Waldenstrom’s macroglobulinaemia. Australas J Dermatol40: 201–3, 1999.
49. Wilhelmi ML, Ocana Wilhelmi J, Ocana Sierra J. Schnitzler’s syndromeand pseudoxanthoma elasticum. 3rd Congress of EADV, 26–30 Sep-tember 1993, Copenhagen, Abstract FC20, 159, 1993.
50. Winckelmann G, Nagel HG, Maier R, Reuther G. Schnitzler-Syndrom alsUrsache eines rezidivierenden Fiebers unbekannter Ursache. DtschMed Wschr 121: 860–64, 1996.
44 LIPSKER ET AL
Lipsker-MD-0106-01/01 12/21/2000 2:15 PM Page 44 (Black plate)