FOUNDATION OF NURSING STUDIES IDENTIFYING A PAIN ... Reports... · FOUNDATION OF NURSING STUDIES...
19
FOUNDATION OF NURSING STUDIES IDENTIFYING A PAIN ASSESSMENT TOOL FOR PATIENTS WITH COGNITIVE IMPAIRMENT IN ACUTE CARE 7/4/2011 Royal Bolton Hospitals NHS Foundation Trust Project Lead: Julie Gregory, Acute Pain Nurse Specialist Key words: pain assessment, acute care, cognitive impairment and dementia, participatory action research, practice development E-mail. [email protected]
Transcript of FOUNDATION OF NURSING STUDIES IDENTIFYING A PAIN ... Reports... · FOUNDATION OF NURSING STUDIES...

FOUNDATION OF NURSING STUDIES IDENTIFYING A PAIN ASSESSMENT TOOL FOR PATIENTS WITH COGNITIVE IMPAIRMENT IN ACUTE CARE 7/4/2011 Royal Bolton Hospitals NHS Foundation Trust Project Lead: Julie Gregory, Acute Pain Nurse Specialist
Key words: pain assessment, acute care, cognitive impairment and dementia, participatory action research, practice development
E-mail. [email protected]

Identifying a pain assessment tool for patients with cognitive impairment Page 2
CONTENTS
PAGE NO. SUMMARY 3
Introduction 4
Background 4
Aim and objectives of the project 5
Methods and approaches 5
Action cycle one 5
Audit 6
Literature review 6
Action cycle two 8
Workshops 8
Claims, concerns and issues 8
Action cycle three 9
Trial of assessment tools 9
Evaluation 9
Final evaluation 10
Discussion 10
Conclusion 11
References 13
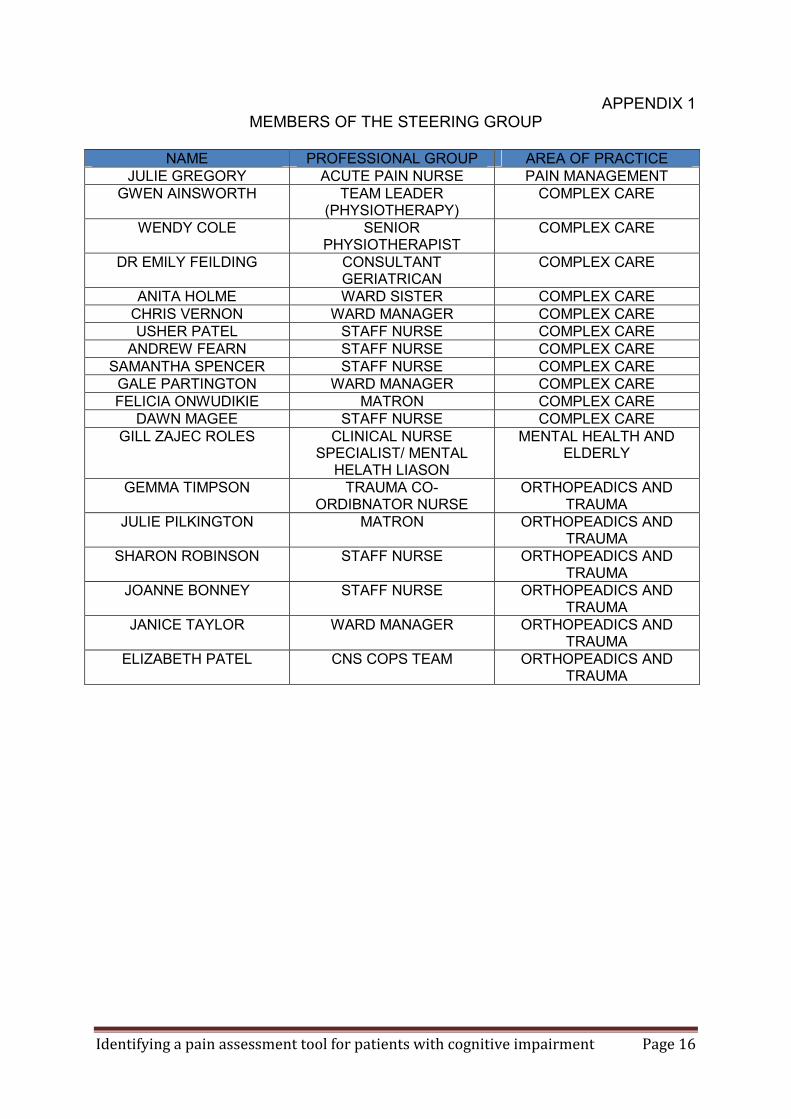
Appendix 1 members of the steering group 15
Appendix 2 the evaluation tool 16
Appendix 3 Bolton Pain Assessment Scale 17

Identifying a pain assessment tool for patients with cognitive impairment Page 3
Summary:
This project aimed to identify a pain assessment tool sensitive to the cognitively
impaired patient in acute care settings to ensure good pain control and improved
outcomes for this group of patients.
Funding was obtained from the Foundation of Nursing Studies and General Nursing
Council Trust to support the project. A steering group comprising of members of the
pain team, representatives from the complex care and trauma unit and the mental
health liaison team for older people was formed. The purpose of the group was to
provide expert advice, to set mile stones and to meet regularly to ensure project kept
to the set targets.
The method and approaches used were based on participatory action research
methodology. Using a collaborative and participatory approach and incorporating
cycles of assessment, planning, action, evaluation and reflection the clinicians
involved examined and evaluated established behavioural pain assessment tools
within practice.
None of the behavioural pain assessment tools trialled was ideal and therefore the
group have devised their own pain assessment tool which has recently been
introduced into practice and will be evaluated by the clinical team.
Identifying a pain assessment tool for patients with cognitive impairment Page 4
INTRODUCTION Pain is a common symptom associated with injuries and surgery with up to 79% of hospitalised patients experiencing pain (Clinical Standards Advisory Group [CSAG] 1999, Strong et al 2002, Donovan et al 1987). Good pain management improves function, reduces complications and the duration of hospitalisation (Murdock and Larsen 2004).The recognition, assessment and treatment of pain should be conducted routinely for all patients. Unfortunately this does not always occur and in older people, pain is often under reported and frequently under treated (Murdock and Larsen (2004). There is evidence that there is even less treatment in cognitively impaired patients who cannot self-report pain (Warden et al 2003, Murdock and Larsen 2004). Self report is considered the most reliable way of assessing pain due to its subjective nature and based on the definition “pain is what the experiencing person says it is, existing whenever he/she says it does” McCaffery and Pasero (1999, p17). The patient needs to describe the sensation, its impact and its meaning for them as an individual. However there are groups of patient who cannot interpret, describe and communicate their experience of pain to clinicians. This project examined the pain assessment tools available for the recognition and assessment of pain for patients with cognitive impairment. BACKGROUND Following a pain management course, nurses and therapists from the complex care unit reflected on and critically examined their practice and as a result they identified specific difficulties with pain assessment in patients with cognitive impairment and/or dementia. The staff realised that this group of patients cannot always express or describe their pain and they felt that the number of patients admitted to the complex care wards with cognitive impairment appears to have increased. As a result of the National Dementia Strategy (2009) there is an increased awareness of the specific care needs for this group of patients. Some of the observations made by members of staff from the complex care wards and trauma unit included, for example, problems in mobilising the patient as they may resist, when the physiotherapist attempted to move them. This may indicate pain, but without an assessment tool or confirmation from the patient it was difficult to verify this. Members of the team contacted the physiotherapists on the elderly psychiatric unit and discovered that they did not use an assessment tool for their client group; they used an ‘instinctive feeling’ that relies on their knowledge of patients over a prolonged period of time. The pain assessment tool currently used within the hospital is a simple verbal descriptor tool which depends on an individual expressing pain when asked. A brief examination of assessment tools for cognitively impaired people by members of the care team did not identify a tool suitable for acute care. The project involved members of the healthcare teams on the complex care wards and the trauma unit where they had recognised this problem for many of their patients.

Identifying a pain assessment tool for patients with cognitive impairment Page 5
AIM: To identify and implement a pain assessment tool sensitive to the cognitively impaired patient in acute care settings to ensure good pain control and improved outcomes for this group of patients. OBJECTIVES:
• To develop individual practitioner’s skills in collecting and analysing data from a number of sources, examining evidence and changing practice
• To examine current pain assessment practice for this specific group by observation, interviewing relatives, holding staff focus groups and examining documented care
• To carry out a review of the literature and tools available on pain assessment in dementia with clinical practitioners and choose tools to trial
• To analyse the range of assessment tools to evaluate their effectiveness and efficacy for all members of the healthcare team and relatives to use in clinical practice
• To disseminate the findings of the teams • To produce our own assessment tool if required
METHODS AND APPROACHES The method and approaches used were based on participatory action research methodology. Participatory action research (PAR) removes the distinction between practitioner and researcher. The researcher or project leader (in this project the Acute Pain Nurse Specialist) undertakes the role of a process facilitator to help participants (Fox, Martin and Green 2007). This involves using a cyclical process and including as many stakeholders as possible in the activities and decisions made during the project. A participatory approach was chosen to involve those responsible for pain assessment practice, to broaden the range of evaluation and to include them in decision making relating to the project. A multi-professional steering group was formed and included the project lead (the Acute Pain Nurse Specialist), the Nurse Specialist from the mental health liaison team for older people, medical staff, nurses and physiotherapists from the complex care and trauma wards A full list of members of the steering group is available in Appendix 1. The purpose of the steering group was to provide expert advice, set mile stones and meet regularly to ensure the project kept to the targets. ACTION CYCLE 1 Audit of current practice An audit of current practice was undertaken using a variety of approaches. This involved observing practice using audit tools produced by the steering group and was conducted by nurses and therapists on each of the wards. The data obtained from five wards compared cognitively intact patients with those that appeared to have some cognitive impairment. A total of forty five patients were observed, see table 1 for results. The observations suggest that cognitively impaired patients were less likely to be asked about pain and there were issues about recording a pain score for both groups of patients.

Identifying a pain assessment tool for patients with cognitive impairment Page 6
Table 1: Results of the observational audit Number of patients 35 cognitively intact 19 cognitively impaired Asked about pain 30 ( 86%) 15 (79%) Pain recorded 23 (66%) 9 (47%) An attempt to undertake an assessment of the context was made at this time using Context Assessment Index (McCormack et al 2009) but just a few nurses completed the assessment. The feedback obtained to explain this poor response from the nursing staff was that the questionnaire appeared too long and complex and the physiotherapists who attempted the questions found it difficult because they work on a number of wards. The context assessment index examines elements of a context to ensure there is person centred practice and it can help identify areas of strength and weakness to develop practice towards person centred care (McCormack et al 2009). Literature An examination of the literature relating to pain assessment tools and cognitive impairment and dementia was conducted by a one of the geriatricians, a physiotherapist and nursing staff, with the help of the hospital librarian. A total of 17 behavioural pain assessment tools were identified. The abstracts for many of the assessment tools were examined and inclusion/exclusion criteria agreed upon prior to examining the specific assessment tools. Table 2: Inclusion and exclusion criteria for the literature review INCLUSION EXCLUSION The tool needs to have been validated Used on patients Used in the acute care setting Be easy to use (subjective) Clear appearance
If the tool has not been validated or used on real patients Used in long-term care facilities only Appears complex and difficult to use Requires a lot of instruction/education
As a result of this activity, the audit of practice and examination of literature, we confirmed that assessment of pain was a problem on the complex care and trauma wards and that there were a large number of behavioural assessment tools have been produced. An assessment tool for cognitively impaired patients was not used within the six wards involved in the project. This may be because there is no pain behavioural assessment tool that has strong reliability and validity that can be recommended for adoption in clinical practice (Herr et al 2006). The results of the audit and examination of literature were presented and discussed at a meeting of the steering group. The literature search had identified seven assessment tools and the steering group examined them and rated the appropriateness of the tools for use in practice. Three assessment tools obtained a higher rating and these are highlighted in table 3.

Identifying a pain assessment tool for patients with cognitive impairment Page 7
Table 3: Summary of literature examined for pain assessment tool SCALE
REFERENCE COMMENTS INITAIL RATING
ABBEY Pain Scale
Abbey et al (2004) the abbey scale: a 1 minute numerical indicator for people with end stage dementia. International Journal of Palliative Nursing, 10(1), 6-13.
Validated Long-term care and relies on previous knowledge of patient Easy to use
Rated by group as 5-6 / 10
Checklist of nonverbal pain indicators (CNPI) observation score
Feldt KS (2000) The checklist of nonverbal pain indicators. Pain management Nursing 1 (1) 13-21
Used on hip fracture patients(n=88) Not pain specific, no grading of pain Scores on movement and on rest. But the scoring system confusing
Rated by group as 7 / 10
PADE Pain assessment for the dementing elderly
Villaneuva MR et al (2003) Pain assessment for the dementing elderly reliability and validity of a new measure. Journal of the American medical directors association January/ February 4:1-8
2 studies involving 25 and then 40 residents over 10 day period Long-term care and extended amount of time required. Lots of questions i.e. 23 and over 2 pages long
Rated by group as 1/10
PACSLAC Pain assessment checklist for seniors with limited ability to communicate
Fuchs-Lacelle S and Hadjistavropolous T (2004) development of and preliminary validation of the Pain assessment checklist for seniors with limited ability to communicate. Pain Management Nursing 5(1) 37-49
List of 60 items with yes no responses. No measure of degree of pain. Long-term care and relies on knowledge of patients Not validated- relied on care givers providing a list of behaviours relating to pain
Rated by group as 3/10
PAINAID Pain assessment IN advanced dementia
Warden V et al (2003) development and psychometric evaluation of the Pain assessment in advanced dementia. Journal of the American directors Association January / February 4: 9-15
Small sample size all male and white. Tested in nursing homes and specialist dementia care units. Complicated to use and misleading but we liked some aspects of the tool
Rated by group as 5/10
PATCOA pain assessment tool in confused older adults
Decker SA and Paerry AG (2003) the development and testing of the PATCOA to assess pain in confused older adults. Pain management nursing 4 (2) 77-86
Validated using 116 post surgical (orthopaedic) patients. Statistically analyzed results 22 behaviours identified by tool. Looked complicated for use.
Rated by group as 2/10
MOBID Mobilization-Observation-Behaviour-Intensity-
Husebo, B. S., et al (2007). Mobilization-observation-behaviour-intensity-dementia pain scale (MOBID): Development and validation
Used in nursing homes and validated with just 26 patients. Suitable for long-term care, chronic pain and muscular
Rated by group as 2/10

Identifying a pain assessment tool for patients with cognitive impairment Page 8
Dementia of a nurse-administered pain assessment tool for use in dementia. Journal of Pain and Symptom Management, 34(1), 67-80.
skeletal pain. Identifies three pain behaviours and difficult to elicit an intensity score
ACTION CYCLE 2 Workshops Two workshops were held, participants included Registered Nurses, Physiotherapists, Health Care Assistants (HCAs) and Student Nurses. Information about cognitive impairment, delirium and dementia, pain assessment and the management of pain for older people was presented. The workshop groups then carried out a ‘claims, concerns and issues’ exercise in relation to assessing pain in patients with cognitive impairment. This exercise is based on fourth generation evaluation to enable a focus on different stakeholders and leads to mutual understanding between stakeholders (Guba and Lincoln 1989). See table 4. Table 4: Summary of claims, concerns and Issues
Claims Concerns Issues That we do recognise pain in patients with cognitive impairment Recognise that dementia patients do feel pain
That pain in dementia patients is ignored or not recognised
Why do patients with cognitive impairment not get appropriate assessment in regards to pain
Talking and discussing pain assessment for dementia patients
Pre-judgement by health professionals that people with dementia do not experience pain and so do not address this
How to get doctors to recognise patients are in pain How to make sure the pain does not get ignored
Pain is recognised in dementia patients by visual rather than by asking them Recording if in any pain
That we cannot get doctors to recognise this and to prescribe regular analgesia
How to improve pain management in the elderly
Discuss how we can improve the management of pain for individuals with cognitive impairment with their families/carers
Doctors not willing to prescribe opiates for elderly confused patients
Recognising pain in people with dementia and cognitive impairment Tools for dementia patients to assess pain needed
This exercise was very useful and resulted in the identification of the workshop participants’ desire to recognise and assess pain. It also recognised the need for an assessment tool to provide consistent assessments in patients with cognitive impairment and dementia. This assessment would identify pain and assist in overcoming the problem of prescribing analgesia. The seven behavioural pain assessment tools were also examined by workshop participants to identify a suitable tool to use in practice. They identified three as suitable for trial within the clinical area which were the same scales that were identified by the steering group.

Identifying a pain assessment tool for patients with cognitive impairment Page 9
The assessment tools chosen for the trial were: The Abbey Scale, Pain Assessment in Advanced Dementia (PAINAD) and Checklist for Non Verbal Indicators (CNVI). Figure 1 presents the main features of the assessment tools. Figure 1: main features of the pain assessment tools
Scale Abbey CNVI PAINAD Vocalisation √ √ √ Facial grimace √ √ √ Body language √ √ √ Behavioural changes √ Restless/rubbing √ Physiological changes √ X X Physical changes √ Breathing X (Consolability)
ACTION CYCLE 3 Six wards were involved in the project, four from the complex care, medical division and two trauma, surgical wards, therefore two wards trialled one of the three assessment tools. A practitioner or ‘champion’ from each ward who had attended the workshop and demonstrated an interest volunteered to explain how to use the behavioural pain assessment tool to staff and to promote its use within their ward. Evaluation A sheet to evaluate each assessment tool was produced and approved by the steering group (Appendix 2). Six weeks after introducing the behavioural pain assessment tools the staff on each ward were invited to evaluate their assessment tool. This included ease of use, time taken to complete and any action taken as a result of their assessment. They were asked to rate the assessment tool out of a possible score of ten and to add any comments they wished. Staff (HCAs, Assistant Practitioners, Registered Nurses, Student Nurses and Physiotherapists) from four of the six wards completed and returned the evaluations. All three scales were evaluated as understandable, easy to use and took between one and five minutes to administer. The overall mean rating for each scale The evaluation asked practitioners to score the assessment tools out of 10 and the average score obtained and comments are presented in table 5. Table 5: Initial evaluation of three pain assessment tools
Assessment Tool PAINAD Abbey CNVI Mean Score (up to 10)
6.3
6.5
7
Comments Easy to follow and completed fast, Good to use especially in those who cannot communicate
Gives prompts, it is effective and helps justify analgesia
Useful if analgesia insufficient

Identifying a pain assessment tool for patients with cognitive impairment Page 10
Other comments included: ‘Difficult to assess if patient has pain or dementia’ ‘Pain assessment in dementia is hard because they are shouting; it doesn’t mean they are in pain’. ‘Find it hard to read body language’ ‘I would like more education’ ‘Assessment tool is not to be relied on, only as a guidance tool’ The evaluations were discussed by the steering group. The assessment tools had been positively accepted but the overall rating was similar for all three. It was generally felt ‘something was better than nothing!’ There was a need to evaluate the tools further to establish if any one tool was appropriate. A second trial was suggested and involved asking the wards to use a different assessment tool to enable a comparison between the behavioural tools. The ward staff agreed and the champions on each ward ensured that a different tool was trialled on the wards. Evaluation The same evaluation sheet was used and completed six weeks after trialling the tools for a second time. The Abbey and PAINAD were again rated as understandable and easy to use by 100% of respondents. The CNVI was found to be understandable by 100%, but just 44% found it easy to use during the second evaluation, compared to 100% initially. The time taken to carry out the assessments was between one and ten minutes for all three tools. Table 4: Final evaluation of three pain assessment tools
Assessment Tool PAINAD Abbey CNVI Score (up to 10)
7.75
7.4
4.2
Comments A very good pain assessment tool, easy to use. Remove the ‘Cheyne stoke’
like the documentation effective and justifies analgesia’
It is not clear what the numerical scores should actionP.would need several sheets per day if patient on regular observations’. no clear guidance as when to action giving pain relief’ Nowhere to document findings
Many practitioners asked for Cheyne stokes to be removed from the PAINAD because Cheyne Stokes is a term used when an individual’s breathing is very slow and irregular with temporary cessation and is not associated with pain.

Identifying a pain assessment tool for patients with cognitive impairment Page 11
During the trial period relatives of patients with dementia / cognitive impairment identified pain that had not been found using the assessment tool being trialled. The individual patient did not appear to be in obvious pain and the assessment tools failed to identify pain behaviour for a small number of patients. This indicated that pain behaviour can be very individual and the literature describes this issue of attempting to categorise behaviours that may indicate pain. For example Fuchs-Lacelle and Hadjistavropolous (2004) identified 60 items and Decker and Paerry (2003) 22 items. The assessment tool therefore helps to indicate pain, but is not to be relied on entirely. DISCUSSION The project leader was the Acute Pain Nurse Specialist who could have examined the literature and decided on a pain assessment tool from this literature and then told practitioners to use it. This would be a conventional way of introducing a change to practice using a linear or technical practice development approach. The outcomes of the project are decided in advance by the facilitator and the staff are the instrument through which practice is to be improved (Manley and McCormack 2004). The focus is usually to apply new knowledge, or skills, behaviour and attitudes to improve performance or productivity. There is an assumption that the change will be unproblematic, linear and rational (Parkin 2009).This approach has been found to result in limited changes in practice. This project used an emancipatory practice development approach where collaboration and participation with as many stakeholders as possible was encouraged and the practitioners themselves shared the responsibility of introducing the pain assessment tools (Manley and McCormack 2004). They examined the literature and decided themselves which pain assessment tools to trial. This was more successful than traditional models of change because the responsibility for the change lies with the workplace team rather than policy makers who tend to be far removed from the situation (Hall 2006). In this project the group itself defined the issues, instigated, implemented and assessed actions for change in a collaborative manner (Parkin 2009). Practitioners and managers usually wish to improve their own service and they tend to feel more confident to say something about their own situation and own the changes. Using a collaborative approach to the change was viewed as less specialised or threatening for the clinicians involved (Fox, Green and Martin 2009). Participation was sustained by members of the ward teams who introduced and explained the assessment tool to their colleagues. Because they were members of the individual wards involved, they understood its context and at the same time it increased their responsibility and ownership of the use of the assessment tool (Manley 2004). It also demonstrated that the proposed assessment tools did not require specialised training by the nurse specialist. As a result of working through the action cycles members of the steering group and practitioners from the wards developed a variety of skills including: literature searching, analysis of the information obtained from the audit, the literature review and the production of an evaluation sheet. Involvement of the clinical teams led to an understanding of pain assessment and its difficulty, as indicated by some of the

Identifying a pain assessment tool for patients with cognitive impairment Page 12
comments made during the workshops and the evaluation of the tools. The practitioners involved had also increased their knowledge and critical skills as a result of examination and comparison of the various tools. The CNVI assessment tool was originally devised for use in acute care whereas the majority of tools were introduced for long-term care. Simply examining the literature would have identified this tool (CNVI) as suitable for use in acute care. By conducting the trials in clinical practice the project demonstrates how this tool was not as easy to use as the other assessment tools. As a result of conducting trials within practice and comparing the assessment tools the rating for the CNVI was lower than the initial evaluation. The PAINAD and the Abbey scales were rated equally. The Abbey Pain scale provides a scoring system that is compatible with the pain score used within the hospital. It was found to be subjective; there is little guidance to define the difference between mild, moderate or severe changes in behaviour. Without previous experience of caring for the individual this may cause different ratings. The PAINAD does provide clearer guidance about rating but suggests that severe pain is indicated by Cheyne Stokes respiration, which none of the steering group or clinicians agreed with. There were some patients where the scales failed to identify pain, but their relatives did describe pain problems to nursing staff. The family or usual carer have not been included in previous pain assessment scales and it was felt by everyone involved in the project that this was an important factor. As a result of the project a combination of the Abbey scale and the PAINAD was produced and included a rating by a member of their family or usual care giver. A chart to document the scoring system has also been produced. The ‘Bolton Pain Assessment Tool’ is now under trial on all six wards (Appendix 3). CONCLUSION There are a large number of behavioural pain assessment tools available, but they are not used in everyday practice. Using a participatory approach and involving clinical staff led to three pain tools actually being used in practice. The clinicians evaluated and became critical of the scales and provided suggestions for improvement.
From the literature, the CNVI assessment tool appeared to be suitable for acute care (devised in acute trauma specialities) but in practice and when compared to other tools it was not useful. None of the established tools were ideal and at times failed to identify pain. The need to produce an assessment tool specifically for acute care was identified. Ideally the pain assessment should involve relatives and/or established carers.
We have produced an assessment tool which combines two established scales. Behavioural pain assessment should always be used with other information and ideally with someone who knows the individual well.

Identifying a pain assessment tool for patients with cognitive impairment Page 13
ACKNOWLEDGEMENTS As the project lead I would like to express my gratitude to Theresa Shaw and the Foundation of Nursing Studies for their support during the project. The clinicians involved in this project have demonstrated a real desire to improve their practice, have been enthusiastic and collaboratively contributed towards it. I would like to say a massive THANK YOU to all the members of the steering group, especially Dr Emily Feilding for her support and critical appraisal and the ward ‘Champions’ who have encouraged their colleagues to use the various assessment tools and then evaluate them.
Identifying a pain assessment tool for patients with cognitive impairment Page 14
REFERENCES Abbey, J.A., Piller, N., DeBellis, A, Esterman, A., Parker, D., Giles, L. & Lowcay, B. (2004). The Abbey Pain Scale. A 1-minute numerical indicator for people with late-stage dementia. International Journal of Palliative Nursing, 10(1), 6-13. Clinical Standards Advisory Group (CSAG) (1999) Services for patients with pain. London Clinical Standards Advisory Group. Department of Health (2009) Living well with dementia: A national Strategy. London. Department of Health. Donovan M Dillon P and Mc Guire L (1987) Incidence and characteristics of pain in a sample of medical-surgical patients Pain. 30 69-78. Feldt, K. S. (2000) The Checklist of Nonverbal Pain Indicators (CNPI). Pain Management Nursing, 1(1) Fox M, Martin P, and Green G (2007) Doing Practitioner Research London Sage Fuchs-Lacelle S, Hadjistavropoulos T (2004), Development and preliminary validation of the pain assessment checklist for seniors with limited ability to communicate (PACSLAC) Pain Management Nursing. Vol.5: pp37–49. Guba EG and Lincoln YS (1989) Fourth generation evaluation. Newbury Park. Sage publication Hall (2006) Hall JE (2006) Professionalizing action research – a meaningful strategy for modernizing services? Journal of Nursing Management. 14, 195-200. In Parkin P (2009).Managing Change in Healthcare Using Action Research. London. Sage Publications. Herr K, Coyne PJ, Key T, et al (2006) Pain assessment in the nonverbal patient: a position statement with clinical practice recommendations. Pain Management Nursing 7 (2) 44-52 Kaasalainen S and Crook J (2004) An exploration of seniors’ ability to report pain. Clinical Nursing Research. 13, 2 , 199-215. Manley K (2004) Transformational culture. A culture of Effectiveness. Chp 4 in McCormack B, Manley K and Garbett R (editors) (2004) Practice Development in Nursing. Oxford Blackwell Publishing. Manley K. and Mc Cormack B.(2004) Practice Development Purpose ,Methodology, Facilitation and Evaluation. Chapter 3 in Mc Cormack B, Manley K and Garbett R (Eds) (2004) Practice Development in Nursing. Oxford Blackwell Publishing. McCaffery M and Pasero C (1999) PAIN: clinical manual. (Second edition) St Louis, Mosby.
Identifying a pain assessment tool for patients with cognitive impairment Page 15
McCormack, B., McCarthy, G., Wright, et al (2009) Development and testing of the Context Assessment Index (CAI) Worldviews on Evidence Based Nursing. Vol. 6. No. 1. pp27-25 Murdock J and Larsen D (2004) Assessing pain in cognitively impaired older adults. Nursing Standard 18 (38) 33-39 Parkin P (2009).Managing Change in Healthcare Using Action Research. London. Sage Publications. Strong J, Unruh A M, Wright A, Baxter DG (2002) Pain. A text book for Therapists. Edinburgh, Churchill Livingstone. Villanueva, M. R., Smith, T. L., Erickson, J. S., Lee, A. C., & Singer, C. M. (2003). Pain assessment for the Dementing Elderly (PADE): Reliability and validity of a new measure. Journal of the American Medical Directors Association, 4(1), 1-8 Warden, V., Hurley, A.C., Volicer, L. (2003). Development and psychometric evaluation of the Pain Assessment in Advanced Dementia (PAINAD) Scale. Journal of the American Medical Directors, Jan/Feb, 9-15. Zwakhalen SMG, Dongen KAJ, Hamers JPH, ABU-Saad HH (2004) Pain assessment in intellectually disabled people: non-verbal indicators. Journal of Advanced Nursing 45 (3) 236-245.
Identifying a pain assessment tool for patients with cognitive impairment Page 16
APPENDIX 1 MEMBERS OF THE STEERING GROUP
NAME PROFESSIONAL GROUP AREA OF PRACTICE
JULIE GREGORY ACUTE PAIN NURSE PAIN MANAGEMENT GWEN AINSWORTH TEAM LEADER
(PHYSIOTHERAPY) COMPLEX CARE
WENDY COLE SENIOR PHYSIOTHERAPIST
COMPLEX CARE
DR EMILY FEILDING CONSULTANT GERIATRICAN
COMPLEX CARE
ANITA HOLME WARD SISTER COMPLEX CARE CHRIS VERNON WARD MANAGER COMPLEX CARE USHER PATEL STAFF NURSE COMPLEX CARE
ANDREW FEARN STAFF NURSE COMPLEX CARE SAMANTHA SPENCER STAFF NURSE COMPLEX CARE
GALE PARTINGTON WARD MANAGER COMPLEX CARE FELICIA ONWUDIKIE MATRON COMPLEX CARE
DAWN MAGEE STAFF NURSE COMPLEX CARE GILL ZAJEC ROLES CLINICAL NURSE
SPECIALIST/ MENTAL HELATH LIASON
MENTAL HEALTH AND ELDERLY
GEMMA TIMPSON TRAUMA CO-ORDIBNATOR NURSE
ORTHOPEADICS AND TRAUMA
JULIE PILKINGTON MATRON ORTHOPEADICS AND TRAUMA
SHARON ROBINSON STAFF NURSE ORTHOPEADICS AND TRAUMA
JOANNE BONNEY STAFF NURSE ORTHOPEADICS AND TRAUMA
JANICE TAYLOR WARD MANAGER ORTHOPEADICS AND TRAUMA
ELIZABETH PATEL CNS COPS TEAM ORTHOPEADICS AND TRAUMA

Identifying a pain assessment tool for patients with cognitive impairment Page 17
APPENDIX 2 EVALUATION OF PAIN ASSESSMENT TOOL
FOR COGNITIVELY IMPAIRED / DEMENTIA PATIENTS
Ward You are? Reg Nurse
Assistant Practitioner
Physiotherapist Occupational therapist
HCA doctor Other, please state
1. Did you understand how to use the assessment tool? YES/ NO 2. Was it easy to complete? 3. How long did it take to assess the pain/Complete the tool? ------------ 4. Did the use of this assessment tool prompt you to act? YES /NO If yes, what action did you take? 5. Do you feel there is anything that needs to be added to the pain assessment tool? Is there anything that is not required? 6. Overall how would you rate this pain assessment tool? (Indicate on the scale 1= Not useful and 10 = very useful) 1 2 3 4 5 6 7 8 9 10
Can you please explain your rating? Any other comments: Thank you

BOLTON PAIN ASSESSMENT SCALE NAME OF PATIENTPPPPPPPPPPPPPPPPPPPPPPPP. NAME AND DESIGNATION OF PERSON COMPLETING SCORE:PPPPPPPPPPPPPPPPPP DATE AND TIMEPPPPPPPPPPPPPPPPPP
SCORE ABSENT 0 MILD 1 MODERATE 2 SEVERE 3 SCORE VOCALISATION
none
Occasional moan or groan
Low level speech with a negative or disapproving quality
Repeatedly crying out, loud moaning or crying
FACIAL EXPRESSION e.g.
Smiling or relaxed
Looking tense,
Sad Frowning,
Grimacing and looks frightened
CHANGE IN BODY LANGUAGE
None
Tense, fidgeting
Guarding part of the body,
Withdrawn, rigid, fists clenched. Knees pulled up
BEHAVIOURAL CHANGE
None
Increased confusion
Refusing to eat, alterations in usual pattern
Pulling or pushing away, striking out
PHYSIOLOGICAL CHANGE
Normal
Occasional laboured breath, increased heart rate
Hyperventilation, increased heart rate and BP
Change in pulse BP, respiratory rate and perspiring, flushed or pallor
PHYSICAL CHANGES
None
Skin tears
Pressure sores, arthritis
Post surgery, trauma,
Comments by family or usual care givers
Pain on movement/ physiotherapy
0-2 = no pain (0)
3-7 = mild pain (1)
9-13 = moderate pain (2)
14+ severe pain (3)
© Royal Bolton Hospital NHS Foundation Trust 2011. All rights reserved. Not to be reproduced in whole or in part without the permission of the copyright owner.

Identifying a pain assessment tool for patients with cognitive impairment Page 2


![Transcultural Nursing Lei Wangccftp.scu.edu.cn/Download/20191225084457219.pdfTranscultural Pain Management: Theory, Practice, and Nurse-Client Partnerships[J]. Pain Management Nursing*,](https://static.fdocuments.in/doc/165x107/5f8030ffe94d5811d861700a/transcultural-nursing-lei-transcultural-pain-management-theory-practice-and-nurse-client.jpg)