Forum on TB and migrants final 6sept2013 (final) · 6 Format (See Annex 3 for complete agenda) The...
52
1 Forum on international migration and health in Thailand: status and challenges to controlling TB Bangkok, 4‐6 June 2013
Transcript of Forum on TB and migrants final 6sept2013 (final) · 6 Format (See Annex 3 for complete agenda) The...

1
Forum on international migration and health in
Thailand: status and challenges to controlling TB Bangkok, 4‐6 June 2013
2
ACRONYMS
AEC ASEAN Economic CommunityART Antiretroviral Treatment ASEAN Association of Southeast Asian Nations CCSDPT Committee for Coordination of Services to Displaced Persons in Thailand DHO District Health OfficeDOT Directly Observed Treatment DOTS The basic package that underpins the Stop TB Strategy EPTB Extra Pulmonary Tuberculosis HIV Human Immunodeficiency VirusIEC Information, Education and Communication IDC Immigration Detention Center IO International Organization IOM M+/M‐
International Organization for MigrationSmear positive/smear negative
MDG Millennium Development Goal MDR‐TB Multidrug‐resistant Tuberculosis (resistance to, at least, isoniazid and rifampicin) MoH/MoPH Ministry of Health/Ministry of Public HealthMoU Memorandum of Understanding NGO Non‐governmental organization NTP National TB Control Program PHO Provincial Health OfficePU‐AMI Premier Urgence‐Aide Medicale InternationaleRTG Royal Thai Government TB Tuberculosis TB‐RAM TB Reduction Among non‐Thai MigrantsTTBI Tak TB Border Initiative ProjectWHO World Health Organization
Acknowledgements
The forum was funded with support from the European Union, WHO, and the US Centers for Disease
Control. Staff from WHO/Thailand and the Bureau of TB provided highly efficient administrative
support. Grateful thanks to all participants for their active inputs, and especially to presenters,
chairs, group facilitators and rapporteurs; and to Dr. Virginia Macdonald, overall rapporteur.

3
Executive Summary
WHO Thailand and the Bureau of Tuberculosis (BTB) of the Royal Thai Government’s Ministry of
Public Health (MoPH) collaborated to organize a forum from 4‐6 June 2013 in Bangkok to address
key issues surrounding the challenges of controlling TB among migrants in Thailand. The objective
was to provide a systematic overview of relevant epidemiology and to examine control efforts from
both patient centered and public health systems approaches. The 114 meeting participants
(representing the Thai government at the national, regional, and provincial levels ; TB programs
from Cambodia, Lao PDR and Myanmar; TB clinicians; non‐governmental organizations;
international organizations; and donors), provided updates on their efforts and developed key
recommendations for further action.
In 2011, there were an estimated 110,000 ongoing TB cases and 86,000 new TB cases in Thailand,
yielding an estimated prevalence rate of 161/100,000 and an incidence rate of 124/100,000 (see
table 2). However, preliminary results (excluding Bangkok) from the 2012 Thailand National TB
Prevalence Study indicate that the national prevalence of TB may be higher than these estimates.
Still, the prevalence in Thailand is considerably lower than the latest available estimated prevalence
rates for Cambodia (817/100,000), Myanmar (506/100,000), and Lao PDR (570/100,000), which are
all considered high burden countries in the world. Additionally, available evidence presented at the
forum indicates that TB prevalence in provinces bordering Thailand for all these three countries is
generally above their respective national averages. This epidemiologic situation has direct
implications for Thailand due to the large number (estimated at 2+ million) migrants from these
surrounding countries who have crossed the border to live and work in Thailand.
Surveillance gaps may lead to under‐reporting of TB among the non‐Thai population, but data
available at the national level indicates a total of 2268 TB cases of all types were reported among
this group in Thailand in 2011. The estimated range of new TB cases with MDR‐TB for non‐Thais is 1‐
4% compared to the latest drug resistance survey among Thai patients which indicates that
national average was 1.9% in 2011. Provincial level epidemiologic data provided by four provinces
(Tak, Kanchanaburi, Samut Sakhon, and Sa Kaeo) showed that newly reported M+ TB cases among
the Thai population were lower than the estimated national incidence rate for all provinces. The
overall incidence rates for migrants could not be determined due to lack of denominator data;
however, health screening in Samut Sakorn in 2011 showed an incidence of 201/100,000 among
migrants seeking health insurance. The four provinces reported that the cure rates for the latest
cohort of M+ Thai TB patients ranged from 75‐84% compared to 65‐75% for non‐Thai patients.
Default rates are consistently higher among non‐Thai TB patients.
In addition to TB detection and treatment facilities at provincial hospitals, numerous NGOs and IOs
provide services to migrants and special populations in displaced person shelters and detention
centers. Identifying TB among migrants primarily relies on passive case detection. Data on migrant
TB cases is entered into the Thai national data base; however, obtaining a comprehensive national
assessment of TB among migrants through routine surveillance or even prevalence surveys remains
a challenge. Funding to support TB drugs for both first and second line treatments for migrants is
available through Global Fund support. However, providing DOTS for mobile populations remains
particularly problematic. Follow‐up and referral mechanisms are a key challenge, particularly for
undocumented migrants or those who cross the border into Thailand seeking medical care.

4
Extensive services for TB control are available in displaced person camps but providers in these
settings can have additional challenges in sustaining care and linking to other national program
efforts. There is only limited information available about health services available in detention
centers.
There was a common underlying conclusion that the key barrier to controlling TB among migrants is their limited access to health services due to relatively poor socio‐economic status, lack of health insurance, high mobility, language barriers, and real or perceived stigma and discrimination. Beyond addressing core systemic gaps in providing health services to migrants, key recommendations for strengthening TB control among migrants include: expand active case detection among migrant populations, develop a common cross‐border referral mechanism‐‐ including multi‐language referral forms and patient ID cards, provide HIV testing for all confirmed TB cases, and ensure relevant guidelines for migrants’ treatment are widely distributed to PHOs and hospitals and well understood by their program staff responsible for TB. All four countries represented agreed on the need to expand cross border collaboration and to develop a multi‐country funding proposal (possibly to the Global Fund) to address gaps in the response to TB control and treatment among migrants.

5
Forum on international migration and health in Thailand: status and
challenges to controlling TB
With financial support from the European Union, WHO, and the US CDC, WHO Thailand and the
Bureau of Tuberculosis (BTB) of the Royal Thai Government’s Ministry of Public Health collaborated
to organize a forum from 4‐6 June 2013 in Bangkok to address key issues surrounding the challenges
of controlling TB among migrants in Thailand. The forum was designed to follow‐up the status of
implementation of the 2009 recommendations made by the Strategy and Planning Cluster of the BTB
to address this same concern and to provide input on the condition of TB among migrants to the
Thai National TB Programme review being conducted by a Joint Monitoring Mission in August 2013.
Discussions were put in the context of Thailand’s Border Health Development Master Plan and the
increasing focus on border and migrant issues in the Greater Mekong Sub‐region (GMS)1.
There were 114 meeting participants representing the Thai government from the national level, 5
regional offices, and 12 provincial health offices and hospitals; national TB programs from Cambodia,
Lao PDR, and Myanmar; TB clinicians and private hospitals; non‐governmental organizations;
international organizations; donors; and other stakeholders. (See Annex 2 for complete list of
participants.)
Objectives
1. To raise awareness among key stakeholders and public health policy makers about the
challenges and importance of addressing infectious diseases among border and migrant populations;
2. To provide an update on the status of TB in Thailand, including epidemiology, current
national programme implementation, and technical guidelines;
3. To learn about specific challenges of combating TB in border areas of Myanmar, Cambodia,
and Lao PDR, and provide an opportunity for establishing a process of collaboration for cross‐border
activities;
4. To provide a systematic overview, identify gaps, and recommend priority actions for the
current programs directed to diagnosing and treating TB among border and migrant populations
(e.g. health systems approach), and,
5. To provide an opportunity to raise and address technical questions, exchange ideas, and
develop new approaches to address the challenges of diagnosing and treating TB patients among
border and migrant populations (e.g. patient centered approach)
1 The Greater Mekong Sub‐region includes Myanmar, Thailand, Cambodia, Lao PDR, Vietnam, and the Yunnan province of the Republic of China. This forum concentrated on the issues of migrants in Thailand and contiguous countries.

6
Format (See Annex 3 for complete agenda)
The forum provided a global and regional update on migration and TB issues to provide a context for
the overlap between these two subject areas. Representatives from Thailand, Myanmar, Cambodia,
and Lao PDR summarized the current status of their national TB programs with a focus on migrant
specific data. Because circumstances and required diagnostic and treatment approaches may differ
among migrant sub‐groups, working groups discussed three separate migrant population
categories: 1) labor migrants—both documented and undocumented; 2) cross‐border migrants; and
3) special settings—including displaced persons in temporary shelters, those seeking re‐settlement,
and migrants in detention centers. For each population category, participants reviewed a) specific
diagnostic and treatment requirements; and b) the health system impact and requirements for
addressing TB. The framework for the health system discussion followed the 2010 WHO/IOM
Global Consultation on the Health of Migrants recommended priority action areas: a. monitoring
migrant health, b. policy and legal frameworks, c. migrant sensitive health systems, and d.
partnerships, networks, and multi‐country frameworks2.
Context
Global and regional tuberculosis situation
Globally, there has been significant progress in tuberculosis (TB) control and treatment. The Millennium Development Goal (MDG) to halt and reverse the TB epidemic by 2015 has already been achieved, with a decrease in new cases of TB over several years and also decreasing TB mortality. However, TB still affects great numbers of people: in 2011 there were an estimated 8.7 million incident cases of TB (the majority of these occurring in Asia) and 1.4 million people died of TB3. Over 1 million (or 13%) of incident TB cases were HIV positive. While the prevalence rate has fallen by 36% globally since 1990, there were still an estimated 12 million people around the world living with TB in 20114. In 2011 National TB control programs (NTPs) were notified of 5.8 million newly diagnosed cases of TB or only about two thirds of the estimated total incident cases. The global treatment success rate among newly diagnosed cases was 85%5; however, there were an estimated 310,000 cases of multi‐drug resistant TB (MDR‐TB) among notified TB cases. Progress in responding to MDR‐TB remains slow6. The Global Stop TB Strategy is the World Health Organization’s (WHO’s) currently recommended approach to TB control and treatment with a goal to dramatically reduce the global burden of TB by 2015. The strategies advocated for include:
Pursue high‐quality DOTS7 expansion and enhancement;
Address TB‐HIV, MDR‐TB, and the needs of poor and vulnerable populations;
Contribute to health system strengthening based on primary health care;
Engage all care providers;
2 WHO/IOM. Health of Migrants—the Way Forward. Report of a global consultation, Madrid, Spain, 3‐5 March 2010. 3 Global Tuberculosis Report 2012 (2012) World Health Organisation 4 Ibid 5 Ibid 6 Ibid 7 Directly Observed Treatment, the basic package that underpins the Stop TB Strategy

7
Empower people with TB, and communities through partnership, and,
Enable and promote research.
In terms of TB incidence, the South East Asian region accounts for 40% of the global burden of TB and India and China together account for 40% of the world’s TB cases8. There were an estimated 3.5 million incident TB cases and a prevalence of 5 million in South‐East Asia in 2011. Excluding those with HIV‐TB, an estimated 480,000 people died of TB in South‐East Asia in 2012, most of these in Bangladesh, India, Indonesia, Thailand and Myanmar9
In South‐East Asia in 2011 32% of TB patients had known HIV status, among them 7.2% were found to be HIV positive and 59% of HIV‐positive TB cases were on antiretroviral therapy (ART)10. Levels of MDR‐TB among newly diagnosed TB patients are still low at 3%11. All countries in the region have sustained country‐wide access to DOTS and treatment success has remained above 85% since 200512.
Migration in the Greater Mekong Sub‐region (GMS)
Internal and international migration is unprecedented throughout Asia, and, as in most parts of the world, will likely grow. Factors stimulating population movement include increasing levels of political and economic cooperation, increasingly free movement across borders and rapid development of the transport sector, leading to new socio‐economic opportunities. In the South East Asian region there is also a high demand for low‐skilled and inexpensive workers in more developed counties. Further, with increasing connectivity, other issues such as human trafficking and transnational crime are additional factors that need to be effectively managed. The ASEAN Economic Community (AEC) is the goal of Asian regional economic integration by 2015. As stated by ASEAN, AEC is expected to “transform ASEAN into a region with free movement of goods, services, investment, skilled labor and freer flow of capital”13. The result of AEC will be more movement across borders into Thailand and has potentially far‐reaching implications for the control of TB in border areas and the rest of Thailand. Governments in South East Asia are facing the challenge of integrating the health needs of migrants into national plans, policies and strategies taking into account the human rights of these individuals, including their right to health. Not doing so creates marginalized groups in society, is an infringement of human rights and constitutes poor public health practice. Income disparities in the region have provided incentives for migrants to find work in Thailand to the extent that Thailand is now considered one of the top destination countries for migrants in Asia. Economic development in Thailand has attracted foreign investors to the manufacturing sectors that employ both highly skilled and low‐skilled migrant workers. Myanmar, Cambodia and Lao PDR are the biggest groups of migrants in Thailand; at least 70% of migrants in Thailand are from Myanmar (see Table 1). The majority of migrants enter Thailand voluntarily but many lack full documentation which increases the risk for trafficking, labor exploitation, and health vulnerabilities.
8 Tuberculosis Control in South East Asia Region: Annual TB report 2013 (2013) WHO South‐East Asian Region Office (SEARO) 9 Global Tuberculosis Report 2012 (2012) World Health Organisation 10 Tuberculosis Control in South East Asia Region: Annual TB report 2013 (2013) WHO South‐East Asian Region Office (SEARO) 11 Ibid 12 Ibid
13 Accessed 24
th June 2013 www.asean.org/communities/asean‐economic‐community

8
Table 1. Migrants in Thailand, 2011
Country of
origin
Population Data on Migrants in
Thailand
Most common occupation of migrants
in Thailand
Cambodia 181,579 documented, 80,000
undocumented migrants
Fisherman, agriculture, mill workers,
construction workers, low cost laborers
Lao PDR Estimated 181,614 documented, 80,000
undocumented (no reliable statistics)
Truck drivers, factory workers,
agriculture workers, construction
workers, sex workers, domestic workers
and livestock workers.
Myanmar 1.5 million documented migrants, 70%
of total migrant population in Thailand.
140,000 displaced persons in 9
temporary shelters along Myanmar
border
Factory workers, sex workers,
fisherman and seafood processers, farm
workers and domestic workers.
Source: Ministry of Labour, 2011
Policy context: TB and Migration in Thailand and the Region In 2009, the Strategy and Planning Cluster of the Thailand Bureau of TB convened a meeting of key stakeholders to review the status of TB among migrant in Thailand and to propose strategic areas for TB control programs aimed at this vulnerable population14. The meeting had the following recommendations for controlling of TB in migrants and in border areas: • Improve case detection/treatment; • Develop short, medium, and long term management plans; • Establish coordination among Mekong countries on trans‐nation TB control and MDR‐TB; • Cleary determine the roles of key actors on TB control at local level; • Improve monitoring and reporting; • Develop policy at central and provincial level; • Increase training, particularly for directly observed treatment (DOT) “watchers”
The RTG MoPH has made comprehensive efforts to address the public health needs specific to border and migrant populations. Broad policies to address migrants’ health, including health insurance schemes to cover financing of these services, have been drafted. Other efforts have targeted the particular health requirements of populations in border areas. In August 2011, the Minister of Public Health released the Border Health Development Master Plan for 2012 to 2016 15 which proposed four key strategies: • Develop a quality health service system; • Promote access to basic health services; • Strengthen collaboration and participation in all sectors, and, • Provide an effective administrative system
14 See Ministry of Labour, 2011 15 Bureau of Policy and Strategy, RTG MoPH. Border Health Development Master Plan 2012‐2016. August
2011.

9
On a regional level, WHO’s Western Pacific Regional Office (WPRO) has collaborated with multiple
national TB programs and stakeholders to draft broad guidelines‐‐ Tuberculosis Control in Migrant
Populations: Guiding Principles and Proposed Actions. Although initially developed for countries in
the Western Pacific region, the document has applicability for Thailand and the GMS in general.
Update on TB epidemiology and programs in Thailand and border countries
The selected TB indicators for Thailand, Cambodia, Lao PDR and Myanmar shown in Table 2 clearly
show disparity of TB prevalence among these countries, with TB prevalence higher in all the
bordering countries than it is in Thailand. As described above there is ever increasing and fluid
migration into Thailand from these countries, highlighting the importance of addressing TB control
and treatment in migrants and in border communities for Thailand’s national response to TB.
Table 2. Select TB indicators for Cambodia, Myanmar, Thailand and Lao PDR, 201116
Prevalence rate (includes HIV+TB) *
Incidence rate (includes HIV+TB)*
Incidence HIV+TB rate *
Mortality rate 2011 (excludes HIV/TB)*
Case detection, all forms, 1000’s (%,
Treatment success rate 2010 (%, new smear +ve &/or culture +ve)
% new TB patients with MDR‐TB
Cambodia 817 (690‐954)
424 (364 – 489)
22 (18‐25)
63 (29‐111)
64 (55‐74)
94 1.4 (0.7‐2.5)
Myanmar 506 (390‐637)
381 (326‐439)
38 (31‐45) 48 (22‐84) 74 (64‐87) 86 4.2 (3.1‐5.6)
Thailand 161 (73‐282)
124 (102‐147)
18 (15‐22)
14 (6.1‐25)
76 (64‐93)
85 1.7 (1.0‐2.6)
Lao PDR 540 (353‐767)
213 (131‐313)
7.4 (4.2‐12)
11 (6.9‐17)
32 (22‐52)
91 4.9
* Rates per 100,000 population with 95% Confidence Interval Source: Global Tuberculosis Report 2012 (2012), World Health Organization
Thailand
Thailand is one of 22 “high‐burden” countries as listed in the WHO Global TB report for 2012. There
are an estimated 110,000 ongoing TB cases in Thailand and 86,000 new cases in 2011, yielding an
estimated prevalence rate of 161/100,000 and an incidence rate of 124/100,000 (see table 2).
However, preliminary results (excluding Bangkok) from the 2012 Thailand National TB Prevalence
Study indicate that the national prevalence of TB may be higher than previously estimated.
Case notification data from the Thai Bureau of TB Control shows little change in the number of
notified TB cases in Thailand over the past decade with 58,270 notified TB cases in 2012 of which
30,576 were new smear positive TB cases. However, there has been improvement in the case
detection rate up from 56% in 2009 to 76% in 201117. There has also been steady improvement in TB
treatment outcomes over the last 12 years, from a treatment success rate of 69% in 2001 to 85% in
2012, mainly because of decreasing numbers of defaulters and treatment failures. Preliminary data
from the 4th Surveillance Study of TB Drug Resistance in Thailand (2012) show that the percentage of
16 Global Tuberculosis Report 2012 (2012), World Health Organization
17 Ibid
10
new TB cases with MDR‐TB in Thailand in 2011 is low at 1.9%, however, the percentage of
retreatment cases with MDR‐TB, at 16.6%, is high.
In Thailand DOTS and TB services are available for free at any public hospital for the Thai population
under multiple national health insurance schemes. Accessing these services is more problematic for
migrants, especially for those who are undocumented and lack insurance. Global Fund support is
available to provide TB drugs to all migrants through both government and non‐governmental
organization (NGO) programs; however, many migrants are reluctant to present to health facilities
for a variety of reasons.
Table 3 provides data available at the national level for TB among the non‐Thai population. The
‘non‐Thai’ category primarily includes migrant populations, but may also include some cases among
‘stateless’ populations who have resided in Thailand for generations but do not yet have Thai
citizenship. Surveillance gaps may lead to under‐reporting for the non‐Thai population and the lack
of denominator data precludes determining prevalence rates. The latest published data on MDR‐TB
among new migrant TB cases in one border province was 1‐4%, but more recent national data is
sparse18. In any case, given the higher prevalence of TB among countries on its border, Thailand
remains concerned about the implications of increased travel and migration that could accompany
the initiation of the ASEAN Economic Community in 2015.
Table 3. TB among non‐Thai population in Thailand, 2009‐2011
Fiscal Year New M+ Relapse New M‐ EPTB Total
2011 1182 44 789 253 2268
2010 1028 27 652 220 1927
2009 933 38 804 168 1943
Source: Bureau of TB, Ministry of Public Health, Thailand
Cambodia
Cambodia has the highest reported TB prevalence rate (817 per 100,000) and mortality rate (63 per
100,000) in the world19 with a TB incidence rate of 424 per 100,000 for 2012. Even so, Cambodia has
successfully reached the 2015 MDG target of halving TB mortality and prevalence rates. The
treatment success rate in Cambodia continues to be high in 2011 at 94%20. Five percent of TB
patients tested for HIV were HIV positive in 2011 and the majority of these are receiving ART21. The
percentage of newly diagnosed TB cases with MDR‐TB was 1.4 in 201122 (see table 2).
In collaboration with the International Organization for Migration, the Cambodian Ministry of Public
Health initiated active case finding for TB in Banteay Meanchey Province among Cambodia migrants
being deported from Thailand. Banteay Meanchey Province is a key crossing point on the Thai‐
Cambodian border for the 71,000 documented and estimated 180,000 undocumented Cambodians
migrating into Thailand for work. TB incidence as well as treatment and default rates in the
18 P Hemhongsa, et al. (2008) TB, HIV‐associated TB and multidrug‐resistant TB on Thailand’s border with Myanmar, 2006‐2007. Tropical Medicine and International Health. 13, 1288‐1296 19 Global Tuberculosis Report 2012 (2012) World Health Organisation 20 Ibid 21 Ibid
22 Ibid

11
province are higher than the national average. From 1 February 2012 to 30 January 2013, the
project screened 6,680 Cambodian migrants upon deportation and detected 127 TB cases by Gene
Xpert. The estimated prevalence rate among this migrant population was 1,150/100,000—slightly
above the already high national rate. Figure 2 shows the wide age range and gender balance among
the deportees detected with TB.
Figure 1. Age and sex of Cambodian migrants deported from Thailand detected with MTB by
GeneXpert, February 2012 until Jan 2013, (n = 126)
Source: IOM‐TB Reach Program, Cambodia, 2013

12
Lao PDR
In 2011 the TB prevalence rate in Lao
PDR was 540 per 100,000 and
incidence rate (for new and relapse
cases of TB) was 213 per 100,00023.
There was a low case detection rate of
32% in 201124. The treatment success
rate in 2011 was 82%25. MDR‐TB rates
in 2011 were 4.9% among TB patients
never treated before and 23% among
previously treated26.
Although there is high coverage of
DOTS in the community and at health
centres in Lao PDR, there is still low
access to TB care due to a lack of TB
awareness, remoteness, costs of
transportation and limited medical
insurance. There is also limited
capacity (human resource and
equipment) for diagnosis and care of
TB in peripheral health system. Seven
of the 12 provinces bordering Thailand
reported higher than the national
average for notification of new smear
position patients in 2012. (See Table 4)
23 Global Tuberculosis Report 2012 (2012) World Health Organisation 24 Ibid 25 Ibid
26 Lao PDR Ministry of Health
CROSS BORDER COLLABORATION BETWEEN LAO PDR
AND THAILAND
Collaboration for TB control between TB programmes
in Vientiane Capital in Lao PDR and Nong Khai in
Thailand started in 2006.
This specific collaboration for TB control and
treatment (under a memorandum of understanding
for communicable diseases) works within the public
hospital system in both countries and consists of
regular exchange of information on registered TB
patients from both sides with quarterly meetings held
in either Nong Khai or Vientiane. Hospitals are able to
follow‐up patients (by phone) as per the agreement
between the hospitals. This is useful particularly if the
patient is absent or late for treatment.
Lao patients have to pay for TB drugs in Thai private
clinics and public hospitals and often revert to Lao
NTP due to resources limitations. The agreement also
allows referral and transfer of TB patients from the
Thai NTP to hospitals in Lao PDR.

13
Table 4. Notification of new smear + TB cases per 100,000 population, by province, Lao PDR,
2006‐2012
Province on the border with Thailand Source: Lao PDR National TB Center
Myanmar
Myanmar is one of 22 high burden countries as described in the WHO’s 2012 Global TB Report. The
TB prevalence (including HIV+TB) in 2011 was 506 per 100,000 population; this has decreased over
the last decade. However, the incidence rate has remained steady over the last five years (2011—
381 per 100,000 population). The treatment success rate was 86% in 2010 and the mortality rate in
2011 was 48 per 100,000 population (see table 2)27. In 2012, 147,984 new TB cases were notified to
the NTP in Myanmar and 4% of these were in the 16 townships bordering Thailand.
While the number of cases in border townships represents only a small proportion of the total
national TB cases, the prevalence of TB in the key townships with border crossing points is higher
than the national average. Figure 2 shows consistently higher case notifications rates for new smear
positive TB cases in Tachileik—bordering Chiang Rai Province in Thailand, Myawaddy—bordering Tak
Province, and Kawthaung—bordering Ranong Province, than for the country as a whole.
27 Ibid

14
In 2012, treatment success rates for these townships averaged only 80% compared to the national
average of 87%. However, there are special efforts being made to strengthen programme efforts at
the border areas, including quarterly evaluation meeting for improvement of case finding and case
holding, health talks at rural health centers to increase community awareness, annual border health
committee meeting.
Figure 2 – Case Notification Rate for New Smear Positive TB cases in Myawady, Kawthaung, and Tachileik Townships vs. National average, 2008‐2012.
Source: MoH Myanmar
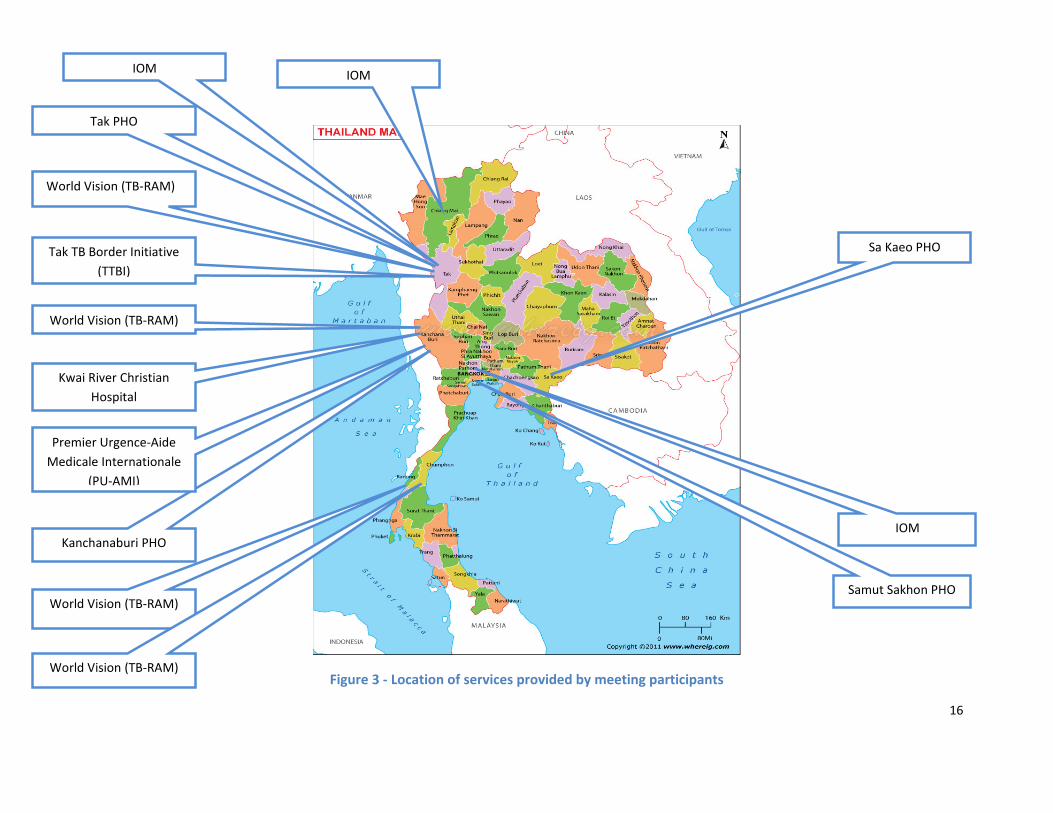
Update on migrant TB programs in border areas in Thailand
Presentations from both government and NGOs provided updated epidemiologic data on TB among migrants in different provinces of Thailand and demonstrated programming strategies for, and common challenges in, addressing TB control and treatment in different migrant groups. (See Figure 3 for location of providers who presented at the forum). Provincial level epidemiologic data was provided by four provinces (Tak, Kanchanburi, Samut Sakhon, and Sa Kaeo. Newly reported M+ TB cases among the Thai population were lower than the estimated national incidence rate for all provinces. The overall incidence rates for migrants could not be determined due to lack of denominator data; however, health screening in Samut Sakorn in 2011 showed an incidence of 201/100,000 among migrants seeking health insurance. Cure rates for the latest cohort of M+ Thai TB patients ranged from 75‐84% compared to 65‐75% for non‐Thai patients. Default rates were consistently higher among non‐Thai TB patients. (More complete epidemiologic data by province is shown in Annex 1). Programmatic updates were presented according to several migrant categories. For the purpose of this meeting, types of migrants in Thailand were categorized as:

15
• Labour migrants: Persons (and dependents) who cross an international border to seek work for more than 6 months. This includes both documented and undocumented migrants.
• Causal cross‐border migrants: Persons (and dependents) who cross an international border for a limited period of time (less than 6 months) to seek work, obtain health care, visit relatives, etc.
• Special settings: Persons residing in displaced person temporary shelters or in detention centers (regardless of length of stay).
These categories are not inclusive of all international migrants; others include tourists, students and retirees; and some migrants may float between the groups at different times. Differentiation of migrant classifications may help identify specific targeted programme approaches for controlling TB. Yet, presentations from both government and NGOs demonstrated a high degree of overlap between programmes for labour and causal cross‐border migrants. Nevertheless, there do appear to be specific issues relevant for irregular or undocumented migrants due to their relative lack of access to health care services. Activities in special settings still appear to require more targeted interventions. TB programmes for labor and casual cross border migrants
Tak Provincial Health Office ‐ Tak province in Thailand shares a long border with Myanmar. The
Provincial Health Office (PHO) in Tak estimates that there are around 27,000 registered and more
than 200,000 undocumented migrants from Myanmar working in Tak. The following joint activities
are planned between Tak and Myawaddy township in Myanmar: sharing of disease surveillance
information; Mae Sot hospital in Tak will support TB sputum culture tests coming from Myawaddy
with diagnosis provided within 24 hours, and collaboration on TB outbreak control. There is a one‐
stop TB clinic service available at all public hospitals in Tak province and DOT is provided with the
majority of observers being family members. Sputum culture tests and TB detection using GeneXpert
platform are provided at Mae Sot provincial hospital.
Case finding reports from Tak province show that 83.9% of confirmed TB cases among non‐Thai
patients are undocumented migrants. They also note a high defaulter rate among non‐Thai patients.
TB Reduction Among non‐Thai Migrants (TB‐RAM) project of World Vision Foundation ‐ In
response to estimated higher prevalence among non‐Thai migrants than in the Thai population and
limited access to health care and TB medicine among this migrant population, World Vision works at
four border and adjacent provinces along the Thai‐Myanmar border (Tak, Kanchanaburi, Chumphon,
Ranong) as well as Phang Nga and Phuket under the TB Reduction Among non‐Thai Migrants (TB‐
RAM) project. Through collaborative activities and regular meetings with provincial level
organisations (PHOs, hospitals and NGOs) TB‐RAM works as an advocate for the health of the non‐
Thai population. They work with migrant health volunteers to provide health information and
counselling and use information and education materials developed in Myanmar. They provide TB
diagnosis and treatment (DOT), nutrition, transportation and psychosocial support.
16
Figure 3 ‐ Location of services provided by meeting participants
Tak PHO
Sa Kaeo PHO
Samut Sakhon PHO
World Vision (TB‐RAM)
World Vision (TB‐RAM)
World Vision (TB‐RAM)
Kwai River Christian
Hospital
Kanchanaburi PHO
Tak TB Border Initiative
(TTBI)
World Vision (TB‐RAM)
Premier Urgence‐Aide
Medicale Internationale
(PU‐AMI)
IOM IOM
IOM

17
Samut Sakhon Provincial Health Office Samut Sakhon province is located in the
central part of Thailand and only 30km
from Bangkok. Of an estimated total
population of 722,152 in Samut Sakhon,
213,340 (30%) are migrants. Most (97%)
of migrants are from Myanmar, Lao PDR
and Cambodia. Although 155,599
migrants enrolled in the MOPH
Compulsory Migrant Health Insurance
Scheme (CMHIS) in 2009, the number
sharply dropped to only 19,429 in 2012.
The latest data from 2011 found 284 TB
cases among 134,860 migrants screened
for work permits (incidence of
210/100,000).
Tak TB Border Initiative Project (TTBI)
The Tak TB Border Initiative Project (TTBI)
aims to improve migrant health in Tak
province, on the Thai/Myanmar border. It
is a consortium of NGO, UN and
government partners responding to a
fragmented a TB control program,
ooverloaded Thai Hospitals, lless
attention given to TB in the casual cross
border migrant population and difficult
terrain to access to the TB program in
Myawaddy in Myanmar. They work in 5
sites on the Thai side of the border and at
the time of the forum had been
operating for 5 months.
TTBI works to improve case finding
activities and diagnostic capacity of both
TB and MDR‐TB through introduction of
the GeneXpert system and systematic
culture and drug susceptibility testing for
all GeneXpert positive cases. They also
provide treatment for TB and TB/HIV co‐
infection and MDR‐TB through
community and home‐based DOTS and
operate a residential TB treatment centre.
ACTIVE CASE FINDING THROUGH DEPORTATION
CHANNELS IN CAMBODIA
Poipet in Banteay Meanchey province in Cambodia
is a major return channel for casual cross border
migrants who have travelled to Thailand for work
without documentation and subsequently been
detained and deported by Thai immigration
authorities. About 98,000 casual cross border
migrants are deported through Cambodian Border
Immigration Centre each year. For many, a period of
stay in a detention center will increase their risk of
TB exposure due to crowded conditions.
The IOM TB‐REACH project, in partnership with the
Cambodian NTP, provincial health and immigration
authorities, targets migrants returning to Cambodia
through the border immigration center.
Migrants are separated into two groups based on
more than one month (Group A) or less than one
month (Group B) detention history. Group A are
referred directly to the hospital by the project van.
For Group B those that show or indicate any TB
symptoms are referred to the hospital by the project
van. At the border hospital, all referred migrants
receive a detailed TB symptom and chest X‐ray
screening using a diagnostic screening ticket.
The doctors and radiologists evaluate the screening
tickets for eligibility for sputum collection. For Group
A eligibility is based on a either a cough more than
two weeks or an abnormal chest X‐ray, or both. For
Group B eligibility for GeneXpert is only based on
the abnormal chest X‐ray indicative of active TB. All
migrant TB suspects provide one sputum sample for
the GeneXpert MTB/R assay.
Actively screening migrants upon return via
immigration is an opportunity for early TB detection
and treatment initiation and the rapid turnaround
time of GeneXpert is appropriate for highly mobile
cross‐border migrants

18
Sa Kaeo Provincial Health Office – Sa Kaeo province shares a 165km border with Cambodia. The Sa
Kaeo PHO employs both active and passive case finding among Thai and non‐Thai populations. They
provide TB treatment via home based care teams and village health volunteers. Registered migrants
are eligible for treatment in Thailand, funded either through employers or Global Fund support. For
undocumented migrants, the PHO will provide advice and refer patients back to Cambodia for
treatment.
Kanchanaburi Provincial Health Office ‐ Kanchanaburi province shares a 370km border with
Myanmar and is only 130km from Bangkok. Of a population of around 950,000, 11% are migrants.
The PHO supervises and monitors all TB control activities and employs both active and passive case
finding and screening, particularly in migrant workers in the large factories in the province. They
provide education for high risk groups through community health volunteers and TB treatment with
home visits to support DOT.
Kwai River Christian hospital ‐ The Kwai River Christian hospital operates in Kanchanaburi province
on the Thai/Myanmar border and serves poor migrants from Myanmar. They operate a TB house
where patients can live for the duration of their treatment with shelter and food. They also provide
DOT through mobile health teams and clinics that travel by motorbike or boat where necessary to
reach patients. They have extended their DOTS programme into Myanmar and also employ health
workers in neighbouring Myanmar towns.
TB programmes in special settings
Premier Urgence‐Aide Medicale Internationale (PU‐AMI) ‐ PU‐AMI operates at three temporary
shelters which house displaced people in Tak province (Mae La, Umpiem Mai and Nu Po). After
initially conducting passive case finding in the camps, in 2013 PU‐AMI has expanded to conduct
active case finding in each shelter. TB treatment is provided at Mae La camp and those in Umpiem
and Nu Po are referred to local hospitals for treatment. Community DOT is provided in all three
shelters. They also provide diagnosis and treatment of HIV co‐infection for camp residents. Patients
reside in the TB “village” or wards for a period of 1‐2 months and then are supported through a
community DOTS programme. Patients are also supported with supplementary feeding, care
packages and food support, pre‐treatment and adherence counselling, and livelihood and social
inclusion activities.
International Organization of Migration (IOM) – Migration health assessments are a statutory
requirement for entry to many destination countries for displaced people in Thailand. Part of these
assessments is the detection of communicable diseases, including TB. The IOM operates 3 Biosafety
Level 3 laboratories which perform sputum microscopy and cultures, drug susceptibility testing and
molecular analysis. Within the resettlement programmes active case detection is conducted with a
low threshold for referral for sputum tests (10% of all screened) and high sensitivity of testing using
sputum culture. The prevalence of culture‐positive pulmonary TB among refugees for the US re‐
settlement programme has remained steady for the last three years at around 550 per 100,000.
Thai Department of Disease Control – Many people enter Thailand illegally or overstay their visas and are arrested for confinement in immigration detention centres in Thailand. Most of them are migrant workers, victims of human trafficking, asylum seekers or refugees and the majority come from Cambodia. In general, between 50 and 100 people are detained in each cell with an area of 114

19
to 156 square meters. TB screening at the detention centres consists of physical exam and history and chest X‐ray and those suspected to have TB infection are referred to the hospital for further investigation and treatment.
Discussion and conclusions on status of TB control among migrant populations
The objective of further discussion was to address specific questions on the overall status and required interventions to control TB among migrants in Thailand. Several working groups focusing on a health care systems approach examined four key priority action areas: monitoring migrant health, migrant sensitive health systems, policy and legal frameworks, and partnerships/networks/multi‐country frameworks. Other groups took a clinical approach focusing on the health of the migrant patient from the perspective of case detection and diagnosis, treatment, and follow‐up and referral.
There was a common underlying conclusion for all working groups that the key barrier to controlling TB among migrants is their limited access to health services due to relatively poor socio‐economic status, lack of health insurance, high mobility, language barriers, and real or perceived stigma and discrimination. Even the minority of migrants who do have Compulsory Migrant Health Insurance face systemic challenges which may preclude actively seeking care.

20
Monitoring migrant health (surveillance, data availability)
Key question: To what extent does the health information we collect, routinely and through surveys, help us plan and measure progress TB control?
Labour Migrants Casual Cross border Migrants Special Settings
Displaced Person Shelters Detention Centers (IDC)
Status Migrant TB patients detected at hospitals and migrant screenings are entered into the Thai national data base using Form TB01 (the same as used for Thai patients) which collects demographic data, country of origin, length of stay, contact information, reference person, etc.
TB programs are monitored through key indicators (e.g. # of new smear + cases, cure rate, default rate, HIV determination, etc.); however data may not be routinely analyzed separately for migrants in all areas
Data collected by NGO medical staff and sent to PHO using BoE/CCSDPT forms.
Analysis by NGOs and CCSDPT
In some case, migrants
screened on arrival or
after 2 months detained (a
case of Suan Plu IDC) and
sent to PHO or Royal Thai
Police if TB is suspected.
Gaps and
Challenges
Challenge to obtain comprehensive national assessment of TB among migrants through routine surveillance or even prevalence surveys
Data collection depends on the skill and language capacity of the interview staff.
Often difficult to obtain information from un‐documented migrants and those who casually cross the border to seek health care. These categories of migrants also do not have official numbers which would facilitate registration or tracking.
Lack of general data on migrant populations precludes determination of overall incidence/prevalence rates
Cross border sharing of TB data is highly dependent on local circumstances.
NGOs may have only informal or indirect links to National TB programme which limits data analysis and feedback
Small number of cases precludes extensive analysis
Uncertain whether TB data
is available for detention
center cases

21
Migrant Sensitive Health System (Service delivery, Human Resources, Medicines)
Key questions: • To what extent are there good quality services being delivered and taken up by the people who need them? • To what degree do we have the right drugs available, distributed where and when they are needed? • To what extent are there the right levels of staff, with the right levels of training and support, in posts where they are needed?
Labour Migrants Casual Cross border migrants Special settings
Displaced Person Shelters Detention Centers (IDC)
Status TB diagnostic services are available for migrants through initial work permit screenings or in public hospitals.
In general, diagnostic capacity and first line treatment (with Global Fund support) appears to be adequate but may not be readily available in all locations.
Most migrant TB cases are still identified in hospitals through passive case finding; however, some active case finding efforts, including use of community migrant health volunteers, are ongoing with Global Fund support and recent initiative from TTBI.
NGOs provide TB
diagnosis and treatment
services, including long
term stay facilities in some
shelters
Suspect cases are referred to
PHO.
Gaps and
Challenges
Undocumented and casual cross border migrants in particular do not readily access the health system.
Language barriers for medical staff can hamper patient care and IEC materials are not always available in the appropriate language
HIV testing of new TB patients is not conducted for migrants in all areas due to limited access to ARV treatment
Challenge to sustain and expand active case finding
Follow‐up and referral systems are not in place to track migrants across the border
Few employers understand the implications of TB or are involved in
supporting health services for their employees
High turn‐over rate of medical staff
Absence of
guidelines for active
case finding
Availability of services,
including screening beyond
initial arrival, is unknown.
22
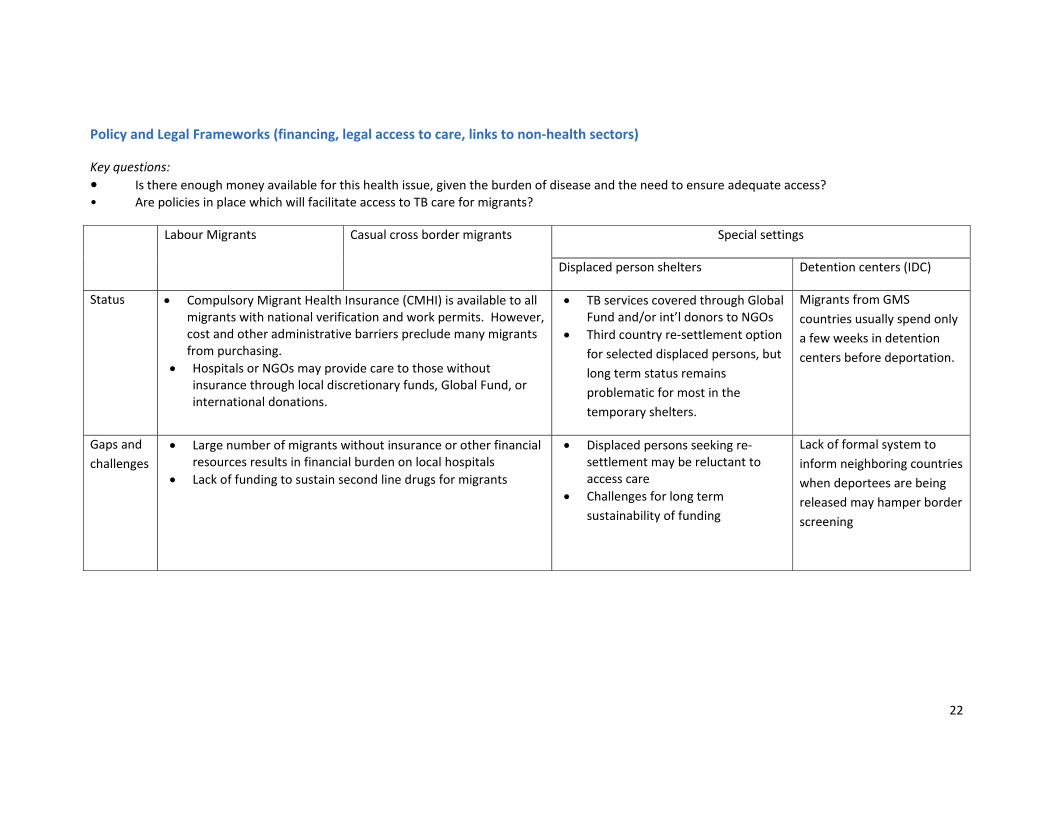
Policy and Legal Frameworks (financing, legal access to care, links to non‐health sectors)
Key questions:
• Is there enough money available for this health issue, given the burden of disease and the need to ensure adequate access? • Are policies in place which will facilitate access to TB care for migrants?
Labour Migrants Casual cross border migrants Special settings
Displaced person shelters Detention centers (IDC)
Status Compulsory Migrant Health Insurance (CMHI) is available to all migrants with national verification and work permits. However, cost and other administrative barriers preclude many migrants from purchasing.
Hospitals or NGOs may provide care to those without insurance through local discretionary funds, Global Fund, or international donations.
TB services covered through Global Fund and/or int’l donors to NGOs
Third country re‐settlement option
for selected displaced persons, but
long term status remains
problematic for most in the
temporary shelters.
Migrants from GMS
countries usually spend only
a few weeks in detention
centers before deportation.
Gaps and
challenges
Large number of migrants without insurance or other financial resources results in financial burden on local hospitals
Lack of funding to sustain second line drugs for migrants
Displaced persons seeking re‐settlement may be reluctant to access care
Challenges for long term
sustainability of funding
Lack of formal system to
inform neighboring countries
when deportees are being
released may hamper border
screening

23
Partnerships, Networks, Multi‐country frameworks (stakeholders, leadership, X border communication)
Key question: To what extent is the necessary leadership, policy, planning and organizational support in place to adequately address TB control among
migrants?
Labour Migrants Casual cross border migrants Special settings
Displaced person shelters Detention centers
Status Thailand has national level bi‐lateral MOUs supporting communicable disease control, including TB, with neighboring GMS countries. Some data sharing occurs through platform of the Mekong Basin Disease Surveillance System (MBDS).
Sub‐national collaborations (e.g. ‘twin‐cities) are active in some
border areas, but degree of cross border communication may depend
on personal relationships and informal mechanisms rather than
agreed protocols and standards.
NGOs involved with TB care are
linked through the CCSDPT.
No information available
Gaps and
challenges
Lack of formal or informal mechanisms to engage private sector and employers in TB control among migrants. Employers have no incentive to support TB control due to high mobility among migrants.
Perhaps due to chronic nature of TB and challenges with diagnosis,
there appears to be less regional mechanisms or forums or
collaborations on TB than some other key diseases (e.g. HIV, malaria).
Limited opportunities for
engagement among NGOs,
academics, government, and IOs
to discuss TB issues

24
Patient care dimension
Key question: From the perspective of the clinician, what are the key challenges that are specific to controlling TB among migrants compared to the general
Thai population?
Labour Migrants Casual cross border migrants Special settings
Displaced person shelters Detention centers
Case
detection and
diagnosis
Due to fear of retribution from their employers if they are found to be TB infected, migrants are often reluctant to seek health care at all, or until symptoms are far progressed. Health providers perceive that, in general, migrants have a low level of trust towards the health system.
While documented migrants may receive check‐ups each year through the hospitals holding contract with MOPH when they apply for health insurance, additional active case detection through outreach program is required to seek out TB cases among undocumented migrants and others reluctant to come to government hospitals.
Active case detection is expensive but often better in rural provinces than urban areas due to lack of support from large employers.
While TB diagnostic services (sputum and CXR) are generally available, GeneXpert is only utilized in a few areas. Migrants and other border populations in isolated areas may have to travel long distances at great personal expense to seek care.
Due to shortage of staff, public hospitals face a challenge to track suspected TB patients to collect sputum samples‐‐especially for migrants in isolated areas.
National protocols and guidelines for providing TB diagnosis and care to migrant populations are not always clear to local clinicians. Specifically need additional guidance on specimen transport for drug sensitivity testing and HIV testing.
Primarily rely on passive case detection but camp residents do not present due to fear that diagnosis of TB will be a barrier to resettlement
Absence of funding as well as clear guidelines for active case finding for both new comers as well as long term shelter residents
Need to improve communication and feedback mechanism between NGOs and referral hospitals for diagnostic results
HIV+ cases are routinely
tested for TB and vice
versa.
No information available

25
Treatment DOTS compliance is sporadic among migrants and may be similar to Thai patients in some areas; however, difficult to identify DOT provider for those who live far from a health facility.
Default rates are high (20‐40% on Thai‐Myanmar border) ‐‐‐especially in casual cross border and undocumented migrants; dropout rates among MDR patients in these groups may be even higher.
Patients previously treated for TB in other countries often lack proper records or documentation of prior drugs used.
Supplies of 1st and 2nd line TB drugs are generally sufficient.
Since migrants are not part of the Thai Universal Health Care
Coverage, supplies of ART are inadequate.
Widespread use of DOTs following Thai National treatment guidelines, including proper isolation mechanisms
1st line drugs are readily available; but challenges to obtain 2nd line drugs. Sometime shortages of pediatric dose preparations.
Referral and
follow‐up
There is a referral system in place in some twin cities; however, this system could be expanded to more areas and more frequent meetings between health officials on both sides of the border to share patient information.
Patients are difficult to track due to high mobility, language barriers, lost treatment/ID cards, lack of mobile phone numbers.
Treatment/referral cards are only be in a single language, this is
considered as a limitation on information sharing and referral to
cross‐border patients
DST and regular patient monitoring is available for patients in the camps
Patients who leave the
camps are often lost to
follow‐up, especially if
they cross the border

26
Key recommendations
Monitoring migrant health 1. Improve data collection through recruitment and training of more migrant health volunteers/workers in health facilities, use of unique ID number for migrants (regardless of documentation status), and use of standard multi‐language data collection forms and data collection protocols in all countries. Primary responsibility: BTB, PHOs, hospitals, in collaboration with other NTPs
2. Improve information sharing about TB situation/burden through designation of staff in each hospital and PHO with responsibility to track migrant data and provide quarterly analysis and feedback to BTB, DHO, and other stakeholders. All private hospitals, academics, or NGOs providing health care to migrants should regularly provide standardized data to the relevant PHO. Primary responsibility: BTB, PHOs, hospitals, other health care providers
Migrant Sensitive Health System 3. Promote expansion of active case finding for TB cases among all migrant populations. Primary responsibility: BTB, PHOs, IOs, NGOs, donors 4. Scale up the effort in developing appropriate IEC materials on TB targeting migrants in multiple languages, including languages of ethnic minorities, and make the information widely available at TB testing and treatment sites and for use in community outreach programs. Primary responsibility: BTB, NGOs 5. Update TB treatment advice and guidelines for controlling TB among migrants and disseminate widely to all government, NGO, and private health facilities. Provide training to ensure these guidelines and policies are well understood by all health care providers. Primary responsibility: BTB, PHO 6. Develop innovative ways of tracking mobile patients both across borders and within migrant communities. Establish a common cross‐border referral mechanism, including multi‐language referral forms and patient ID cards. Review experience on the Thai‐Laos border for applicable lessons learned which could be scaled up. Primary responsibility: BTB, NTPs, NGOs, IOs 7. Develop a regional clearinghouse for migrant health information and resource for notification of available health care facilities providing TB care in the region. Primary responsibility: BTB along with other NTPs, IOM, WHO 8. Undertake relevant operational research on controlling TB among migrants, including studies on cost benefit analysis of TB program options (e.g. active case finding), and migrants’ health seeking behaviors and treatment adherence. Primary responsibility: BTB, Research Institutes, WHO, IOM, NGOs 9. Intensify TB control in immigration detention centers through further review of the current status of TB care in detention centers, including infection control practices, case finding, treatment and referral mechanisms between detention centers and counter parts across the border. Primary responsibility: BTB, DDC

27
Policy and Legal frameworks 10. Scale up policy to integrate HIV testing and treatment for migrants in all TB programs and link with advocacy to secure sustainable funding for ART in migrant patients. Primary responsibility: BTB, PHOs, IOs, NGOs 11. Develop regional guidelines and principles for TB control among migrants as part of more comprehensive frameworks for migrant health care in the GMS. Primary responsibility: NTPs, WHO, IOM,
Partnerships, Networks, Multi‐country frameworks 12. Formalize relationships between TB programs and services across borders with regularly scheduled meetings at PHO and DHO level. Primary responsibility: PHO/DHO with support from BTB links to other NTPs, WHO 13. Expand partnerships with employers in both industry wide organizations as well as individual factories to reach out to migrants and advocate for friendly workplace policy for controlling TB among migrant workers. Primary responsibility: PHO, DHO, NGOs (with the support from BTB) 14. As a short‐medium term measure, Thailand, Myanmar, Cambodia and Lao PDR should develop a multi‐country funding proposal (possibly to the Global Fund to fight AIDS, TB and Malaria) to address gaps in the response to TB control and treatment in the borders between these four countries. Primary responsibility: BTB, PR‐DDC, WHO, NTPs

28
Annex 1 – Epidemiologic data on TB among migrants provided by Provincial Health Offices
1. Tak Provincial Health Office
Tak province in Thailand shares a long border with Myanmar. The Provincial Health Office (PHO) in
Tak estimates that there are around 27,000 registered and more than 200,000 undocumented
migrants from Myanmar working in Tak, these numbers are added to another 605,431 Thais
registered in the province. There is a one‐stop TB clinic service available at all public hospitals in Tak
province and DOTS is provided with the majority of observers being family members. Sputum culture
tests and TB detection using GeneXpert platform are provided at Mae Sot provincial hospital.
Presentation from Tak‐PHO demonstrated almost equal number of TB reported cases from Thais and
Non Thais. (See Table 1) Interestingly 83.9% (743/885) of TB cases among migrants reported are
uninsured migrants. (See Table 2) Among total 8 administrative districts of Tak province, the highest
proportion of TB cases reported from Mae Sot district. MDR‐TB seems to be the biggest problem in
Mae Sot district as well.
In term of treatment outcomes (M+), overall success rates are still < 85% (81% and 75% in 2011 and
20121 respectively) and default rates are > 3% (6.5% and 7.8% in 2011 and 2012 respectively).
Figures in 2011 suggested that success rate is a bit higher in migrant group (Thai 79.5% and migrant
82.5%) and success rates of the two population groups have decreased to around 75% in 2012. The
occurrence of high dead rate, particular among Thai TB patients (13.9% and 16.8% in 2011 and 2012
respectively) perhaps could explain this phenomenon. Presentation also highlights that default rate
is higher in migrant group (2011: Thai 1.6% and migrant 8.9%, 2012: Thai 2.2% and migrant 12.7%).
Key challenges mentioned by PHO‐Tak included
High death rate in Thai TB patients
High default rate in Non‐Thai TB patient
Increasing number of MDR cases (particularly among non‐Thais)
DOT watchers are mainly patients’ family member, not health care workers or village health
volunteer
Table 1. Number of TB cases (Thai and Non Thai) by district in Tak province
District
2011 2012 2013(Q1+Q2)
Thai Non‐
Thai
Total
(%)
Thai Non‐
Thai
Total
(%)
Thai Non‐
Thai
Total
(%)
Mueang 115 10 125(16.3)
112 2 114(14.9)
54 2 56(17.9)
Ban Tak 23 2 25
(3.3)
36 1 37
(4.8)
10 0 10
(3.2)
Sam
Ngao
23 0 23
(2.9)
25 0 25
(3.3)
10 0 10
(3.2)

29
Mae Sot 140 250 390
(50.9)
106 215 321
(42.2)
50 55 105
(33.5)
Mae
Ramat
31 14 45
(5.8)
33 10 43
(5.6)
9 8 17
(5.4)
Thasong
Yang
27 17 44
(5.7)
45 20 65
(8.5)
30 5 35
(11.2)
Phob Pra 20 52 72
(9.4)
32 49 81
(10.6)
12 27 39
(12.5)
Umphang 4 39 43
(5.7)
9 68 77
(10.1)
2 39 41
(13.1)
Total 383 384 767
(100)
398 365 763
(100)
177 136 313
(100)
Table 2. Cumulative number of TB cases among Non‐Thais by district from 2011‐ 2013 (Q1+Q2)
District Total Insured migrant Uninsured migrant
n % n %
Mueang 14 10 71.4 4 28.6
Ban Tak 3 3 100 0 0
Sam Ngao 0 0 0 0 0
Mae Sot 520 71 13.7 449 86.3
Mae Ramat 32 2 6.3 51 93.7
Thasong Yang 42 0 0 42 100
Phob Pra 128 53 41.4 75 58.1
Umphang 146 3 2.1 143 97.9
Total 885 142 16.1 743 83.9

30
Table 3. TB treatment outcomes in Thai TB cases (M+)
Treatment outcomes
2011 2012
N % N %
No. of TB patients received treatment 195 ‐ 190 ‐
Success 155 79.5 143 75.2
Failed 6 3.0 6 3.2
Died 27 13.9 32 16.8
Defaulted 6 1.6 4 2.2
Transferred out 0 0 5 2.6
Note: Treatment outcomes analysis is based on TB cases with complete record only
Table 4 TB treatment outcomes in Non‐Thai TB cases (M+)
Treatment outcomes
2011 2012
N % N %
No. of TB patients received treatment 256 ‐ 220 ‐
Success 211 82.5 166 75.5
Failed 12 4.8 10 4.5
Died 5 1.9 13 5.9
Defaulted 23 8.9 28 12.7
Transferred out 5 1.9 3 1.4
Figure 1. Number of Reported MDR‐TB cases in Mae Sot district, 2007‐2013 (Q1+Q2)
0
2
4
6
8
10
12
14
16
2007 2008 2009 2010 2011 2012 2013
Thai
Non-Thai

31
Figure 2. Outcomes of MDR‐TB treatment in Thai patients
Figure 3. Outcomes of MDR‐ TB treatment in Non‐Thai patients
2. Kanchanaburi Province
PHO‐ Kanchanaburi province shares a 370km border long with Myanmar and is only 130km from
Bangkok. Of a population of around 950,000, 11% (110,296) are migrants. The PHO supervises and
monitors all TB control activities and employs both active and passive case finding and screening,
particularly in migrant workers in the large factories in the province based on the national
guidelines. They provide education for high risk groups through community health volunteers and TB
treatment with home visits to support DOT.
Constraints identified on TB control programme include:
Staff issue include under staff and high staff turn over
0
10
20
30
40
50
60
70
80
90
100
2007 2008 2009 2010 2011 2012 2013
On treatmentDiedDefaultedCured
0
10
20
30
40
50
60
70
80
90
100
2007 2008 2009 2010 2011 2012 2013
On treatmentDiedDefaultedCured

32
Inadequate budget on programme management
Capture highly mobile population as cross‐border patients are highly mobile (moving from
one district to another district and across the province)
Key concerns are on controlling of MDR TB particularly in the context of AEC which will be effect in
2015 and how to enhance participation of community organization in TB control programme.
Table 5. TB case notification in Thai population in 2009‐2013
Total M+ M‐ Extra
pulmonary
Relapse
2009 729 382 203 124 20
2010 806 406 211 159 30
2011 674 362 165 121 26
2012 697 378 193 110 16
2013(Q1+Q2) 371 200 104 56 11
Table 6. TB case notification in non‐Thai population in 2009‐2013
Total
(all forms)
M+ M‐ Extra
pulmonary
Relapse
2009 202 112 66 21 3
2010 226 137 67 21 1
2011 207 125 60 22 0
2012 263 148 95 18 2
2013(Q1+Q2) 71 36 22 12 1
Figure 4. Treatment Outcomes in Thai TB cases in 2009‐2012

33
Figure 5. Treatment Outcomes in non‐Thai TB cases in 2009‐2012
3. Samut Sakhon Province
Samut Sakhon province is located in the central part of Thailand and only 30km far from Bangkok. Of
a total populations around 722,152 (Thais 508,812, Non Thais 213,340) residing in Samut Sakhon, 30
% are migrants. Most of migrants (97%) are from Myanmar, Lao PDR and Cambodia. (Source: PHO
SSK, 28 Feb 2013) Presentation showed that the highest number of migrants enrolled in the MOPH
health insurance scheme occurred in 2009, in which 155,599 migrants were enrolled in CMHI, and
then the number has slightly declined to 134,860 in 2011 and sharply dropped in 2012 to 19,429
only. The latest TB data from Health Check‐up in 2011 suggested 284 TB cases from 134,860 persons
checked (0.21%).
The following are the TB programme goals set by PHO‐SSK
Detection rate > 75%
Success rate (New M+) > 90%
Mortality rate < 6%
Default rate < 3%
Based on SSK‐PHO Cohort TB Reporting system in 2012, of total 1,347 TB (all forms) reported cases
74.5% (n=1,003) are Thais and 25.5% (n=344) are migrants. The presentation also suggested that all
detected M+ cases (both Thais and migrants) were not enrolled in the TB treatment programme.
There are only 28.9% (143/495) for Thais and 3.6 % for migrants (7/194) enrolled in TB programme.
PHO‐SSK TB programme data shown the success rates (M+) is 79% (113/143 cases) in Thai patients
and 71% among migrant patients (5/7 cases). It is also noted that default rate is higher among
migrants (28%:2/7 cases) than Thais (11%:16/143 cases). Referral systems both within the country
(between private and public hospitals) and between country to country are the key challenges that
SSK TB Programme faced.

34
Table 7. Number of TB cases detected in 2012
Population
Sputum +
Sputum ‐
Extra
pulmonary TB
Total New Relapse
Thai 465 30 354 154 1,003
Non‐Thai 186 8 111 39 344
Total 651 38 462 193 1,347
Table 8. Outcomes of TB treatment (M+) in 2012
Population
No. M+
enrolled
Success Failed died defaulted
n % n % n % n %
Thai 143 113 79.0 2 1.4 0 0 16 11.2
Non‐Thai 7 5 71.4 0 0 0 0 2 28.6
4. Sa Kaeo Provincial Health Office
Sa Kaeo province shares a 165km border with Cambodia. The Sa Kaeo PHO employs both active and
passive case finding among Thai and non‐Thai populations. They provide TB treatment via home
based care teams and village health volunteers. Registered migrants are eligible for treatment in
Thailand, for some the employer bears the cost of treatment and for other’s treatment cost if
supported through a Global Fund donation. For undocumented migrants, the PHO will provide
advice and refer patients back to Cambodia for treatment.
Figure 6. Number of TB cases reported in 2011‐2013 (Q1+Q2)
35
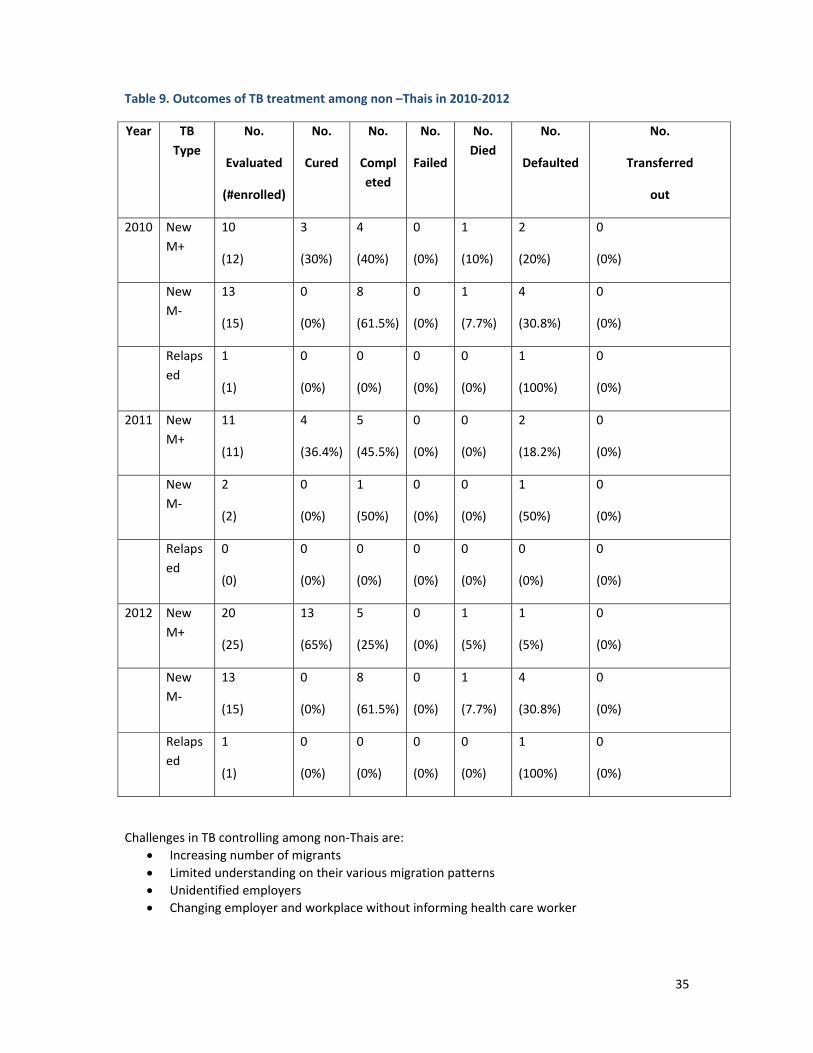
Table 9. Outcomes of TB treatment among non –Thais in 2010‐2012
Year TB
Type
No.
Evaluated
(#enrolled)
No.
Cured
No.
Compl
eted
No.
Failed
No.
Died
No.
Defaulted
No.
Transferred
out
2010 New
M+
10
(12)
3
(30%)
4
(40%)
0
(0%)
1
(10%)
2
(20%)
0
(0%)
New
M‐
13
(15)
0
(0%)
8
(61.5%)
0
(0%)
1
(7.7%)
4
(30.8%)
0
(0%)
Relaps
ed
1
(1)
0
(0%)
0
(0%)
0
(0%)
0
(0%)
1
(100%)
0
(0%)
2011 New
M+
11
(11)
4
(36.4%)
5
(45.5%)
0
(0%)
0
(0%)
2
(18.2%)
0
(0%)
New
M‐
2
(2)
0
(0%)
1
(50%)
0
(0%)
0
(0%)
1
(50%)
0
(0%)
Relaps
ed
0
(0)
0
(0%)
0
(0%)
0
(0%)
0
(0%)
0
(0%)
0
(0%)
2012 New
M+
20
(25)
13
(65%)
5
(25%)
0
(0%)
1
(5%)
1
(5%)
0
(0%)
New
M‐
13
(15)
0
(0%)
8
(61.5%)
0
(0%)
1
(7.7%)
4
(30.8%)
0
(0%)
Relaps
ed
1
(1)
0
(0%)
0
(0%)
0
(0%)
0
(0%)
1
(100%)
0
(0%)
Challenges in TB controlling among non‐Thais are:
Increasing number of migrants
Limited understanding on their various migration patterns
Unidentified employers
Changing employer and workplace without informing health care worker

36
Key recommendations include
Early detection is a key to control TB among migrants
Systematic TB treatment should be provided to migrants and diagnosis should be in‐line with national TB guidelines
Employers and village health volunteers can be key agents to assist heal official to provide
DOT
5. Immigration Detention Center
There are approx. 880‐1,000 detained in the Bangkok Suan Plu Immigration Detention Center, with
an area of 114‐156 square meters per 50‐11 persons or approx. 3 square meters per person. TB
screening through chest radiography is carried out with more than 2 months detainees. If CXR found
abnormal and suggestive of TB cases then they are referred to (Royal Thai police or contracted)
hospital.
Since 2011, 591 (M=309, F=282) detainees were screened with CXR. Majority of them are North
Korean (32%) and Myanmar (25.2%). Of total screen cases, 9.8% (58 cases) found with abnormal CXR
result and of those abnormal CXR 25.8% was diagnosed as TB cases by medical doctor at the
referred hospitals. Royal Thai Policy hospital then provides TB treatment to TB detainees.
It is noted that number of detainees screened seem to be relatively small compare to number of
detainees recorded in 2012. (See table 10) Of total 591 cases screened, 2.5 % was detected as TB
cases during 2011‐2013. Budget constraint and rapid movement of detainees, particularly a case of
Cambodian detainees are factors contributing to low screening rate among detainees at IDC‐Suan
Plu.
Table 10. Number of detainees in 2012
Nationality No. arrested No. released
Cambodia 21,167 (53.3%) 20,959
Myanmar 5,728 (15%) 5,686
Laos 4,333 (11.3%) 4,341
Others 7,015 (18.3%) 7,327
Total 38,243 38,313
Note: No. released is more than No. arrested due to some case was detained crossed a year
Figure 7. Proportion of detainees screened with CXR (2011‐2013) by nationality
nationality
80
73
69
32
149188
North Korean
Myanmar
Vietnamese
Srilankan
pakistani
others
37
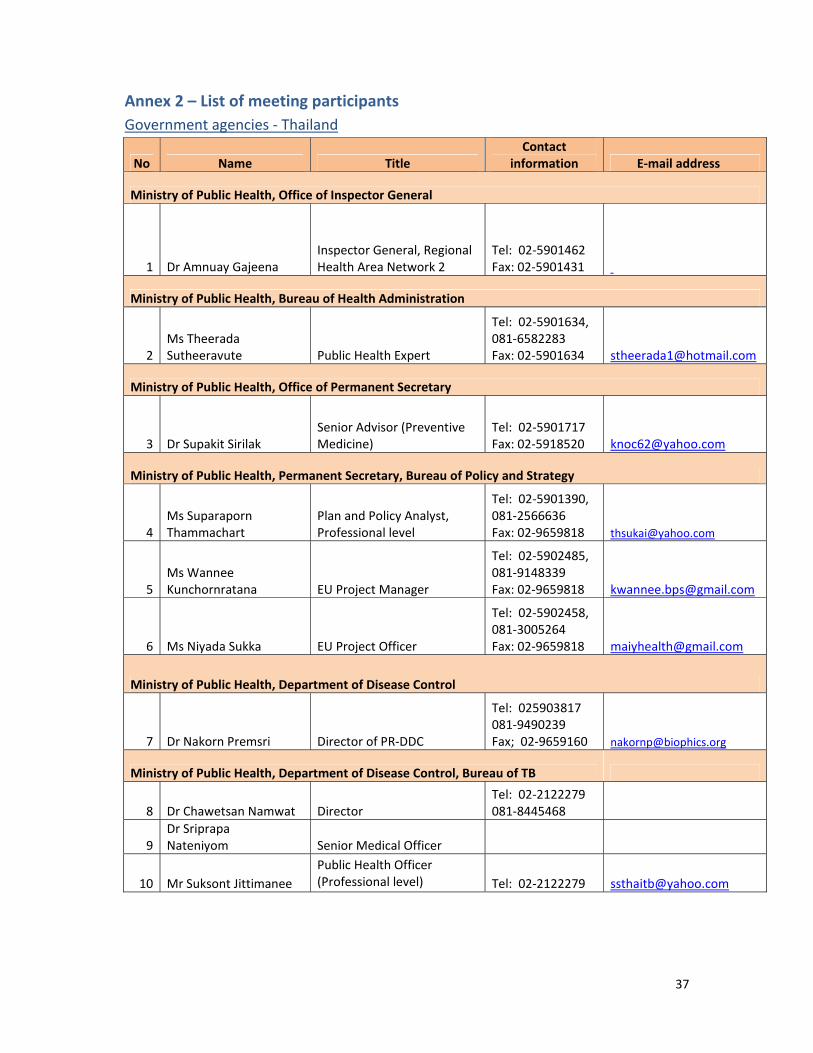
Annex 2 – List of meeting participants
Government agencies ‐ Thailand
No Name Title Contact
information E‐mail address
Ministry of Public Health, Office of Inspector General
1 Dr Amnuay Gajeena Inspector General, Regional Health Area Network 2
Tel: 02‐5901462 Fax: 02‐5901431
Ministry of Public Health, Bureau of Health Administration
2 Ms Theerada Sutheeravute Public Health Expert
Tel: 02‐5901634, 081‐6582283 Fax: 02‐5901634 [email protected]
Ministry of Public Health, Office of Permanent Secretary
3 Dr Supakit Sirilak Senior Advisor (Preventive Medicine)
Tel: 02‐5901717 Fax: 02‐5918520 [email protected]
Ministry of Public Health, Permanent Secretary, Bureau of Policy and Strategy
4 Ms Suparaporn Thammachart
Plan and Policy Analyst, Professional level
Tel: 02‐5901390, 081‐2566636 Fax: 02‐9659818 [email protected]
5 Ms Wannee Kunchornratana EU Project Manager
Tel: 02‐5902485, 081‐9148339 Fax: 02‐9659818 [email protected]
6 Ms Niyada Sukka EU Project Officer
Tel: 02‐5902458, 081‐3005264 Fax: 02‐9659818 [email protected]
Ministry of Public Health, Department of Disease Control
7 Dr Nakorn Premsri Director of PR‐DDC
Tel: 025903817 081‐9490239 Fax; 02‐9659160 [email protected]
Ministry of Public Health, Department of Disease Control, Bureau of TB
8 Dr Chawetsan Namwat Director Tel: 02‐2122279 081‐8445468
9 Dr Sriprapa Nateniyom Senior Medical Officer
10 Mr Suksont Jittimanee
Public Health Officer (Professional level) Tel: 02‐2122279 [email protected]
38
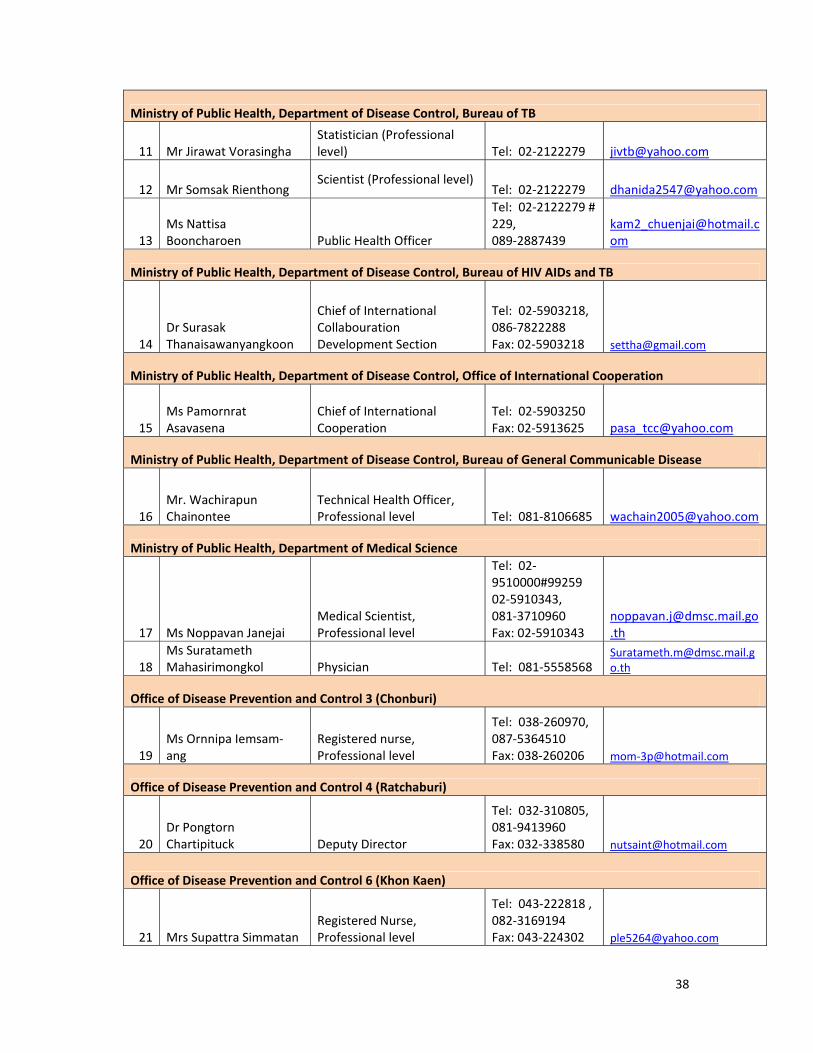
Ministry of Public Health, Department of Disease Control, Bureau of TB
11 Mr Jirawat Vorasingha Statistician (Professional level) Tel: 02‐2122279 [email protected]
12 Mr Somsak Rienthong Scientist (Professional level)
Tel: 02‐2122279 [email protected]
13 Ms Nattisa Booncharoen Public Health Officer
Tel: 02‐2122279 # 229, 089‐2887439
Ministry of Public Health, Department of Disease Control, Bureau of HIV AIDs and TB
14 Dr Surasak Thanaisawanyangkoon
Chief of International Collabouration Development Section
Tel: 02‐5903218, 086‐7822288 Fax: 02‐5903218 [email protected]
Ministry of Public Health, Department of Disease Control, Office of International Cooperation
15 Ms Pamornrat Asavasena
Chief of International Cooperation
Tel: 02‐5903250 Fax: 02‐5913625 [email protected]
Ministry of Public Health, Department of Disease Control, Bureau of General Communicable Disease
16 Mr. Wachirapun Chainontee
Technical Health Officer, Professional level Tel: 081‐8106685 [email protected]
Ministry of Public Health, Department of Medical Science
17 Ms Noppavan Janejai Medical Scientist, Professional level
Tel: 02‐9510000#99259 02‐5910343, 081‐3710960 Fax: 02‐5910343
18 Ms Suratameth Mahasirimongkol Physician Tel: 081‐5558568
Office of Disease Prevention and Control 3 (Chonburi)
19 Ms Ornnipa Iemsam‐ang
Registered nurse, Professional level
Tel: 038‐260970, 087‐5364510 Fax: 038‐260206 mom‐[email protected]
Office of Disease Prevention and Control 4 (Ratchaburi)
20 Dr Pongtorn Chartipituck Deputy Director
Tel: 032‐310805, 081‐9413960 Fax: 032‐338580 [email protected]
Office of Disease Prevention and Control 6 (Khon Kaen)
21 Mrs Supattra Simmatan Registered Nurse, Professional level
Tel: 043‐222818 , 082‐3169194 Fax: 043‐224302 [email protected]

39
Office of Disease Prevention and Control 9 (Phitsanulok)
22 Dr Sakchai Chaimahapurk Director
Tel: 055‐214615 081‐7276572 Fax: 055‐321241 [email protected]
Office of Disease Prevention and Control 10 (Chiang Mai)
23 Dr Witaya Liewsaree Director
Tel: 053‐140767, 081‐9808849 Fax: 053‐140773 [email protected]
Chiang Rai, Chiang Rai Provincial Health Office
24 Dr Chamnarn Hansudewechakul Chief Medical Office
Tel: 053‐910300, 081‐1643838 Fax: 053‐910345 [email protected]
Kanchanaburi, Kanchanaburi Provincial Health Office
25 Ms Ketruetai Settakorn Public Health Officer, Professional level
Tel: 034‐622982 Fax: 034‐514598
26 Ms Nattita Keecharoensuk TB Information Officer
Tel: 034‐622982 Fax: 034‐514598
Kanchanaburi, Sangklaburi District Health Office
27 Ms Pannapa Vuttikasatekit
Public Health Officer, Professional level
Tel: 034‐595035, 091‐7169385 Fax: 034‐595035 [email protected]
Mae Hong Son, Mae Hong Son Provincial Health Office
28 Dr Walairat Chaifoo Deputy Chief Medical Officer
Tel: 053‐611281, 081‐8318537 Fax:053‐611322 [email protected]
29 Mr Woraphan Amrarong Public Health Officer, Professional level
Tel: 053‐611281, 081‐6713257 Fax: 053‐611322 [email protected]
Nong Khai, Nong Khai Provincial Health Office
30 Mr Thapon Tiawsirichaisakul
Public Health Officer, Professional level
Tel: 042‐465067#70, 081‐9756115 Fax: 042‐412650 [email protected]

40
Ratchaburi, Ratchaburi Provincial Health Office
31 Ms Nisachon Sriring Public Health Officer, Professional level
Tel: 032‐326270#141, 088‐9017345 Fax: 032‐325225 [email protected]
Ratchaburi, Tham Hin Health Promoting Hospital
32 Mr Apisit Wechasart Director Tel: 081‐9413676 Fax: 032‐395155 [email protected]
Ranong, Ranong Provincial Health Office
33 Dr Suriya Guharat Chief Medical Office
Tel: 077‐812679, 086‐3009520 Fax: 077‐811584
Rayong, Rayong Provincial Health Office
34 Ms Jongdee Intrasub Public Health Officer, Professional level
Tel: 038‐967415‐7, 081‐6836159 Fax: 038‐620976 [email protected]
Rayong, Rayong hospital
35 Dr Bralee Suntiwut Pulmonologist, Professional level
Tel: 038‐611104, 081‐8806580 Fax: 038‐611104#2140 [email protected]
36 Ms Jaruwan Iamsa‐ard Registered Nurse Tel: 086‐6055482 [email protected]
Sa Kaeo, Sa Kaeo Provincial Health Office
37 Ms Dararat Howong Public Health Officer, Senior Professional Level
Tel: 037‐425141#104, 081‐9837675 Fax: 037‐425147 [email protected]
38 Ms Wanwimon Surinsak Public Health Officer, Professional Level
Tel: 037‐425141#104, 084‐3625243 Fax: 037‐425147 [email protected]
39 Ms Sukanya Songsang Public Health Officer
Tel: 037‐425141#104, 084‐8663204 Fax: 037‐425147
Samutsakhon, Samutsakhon Provincial Health Office
40 Ms Sudarat Seehabona Public Health Officer Tel: 081‐2798013 Fax: 034‐842513
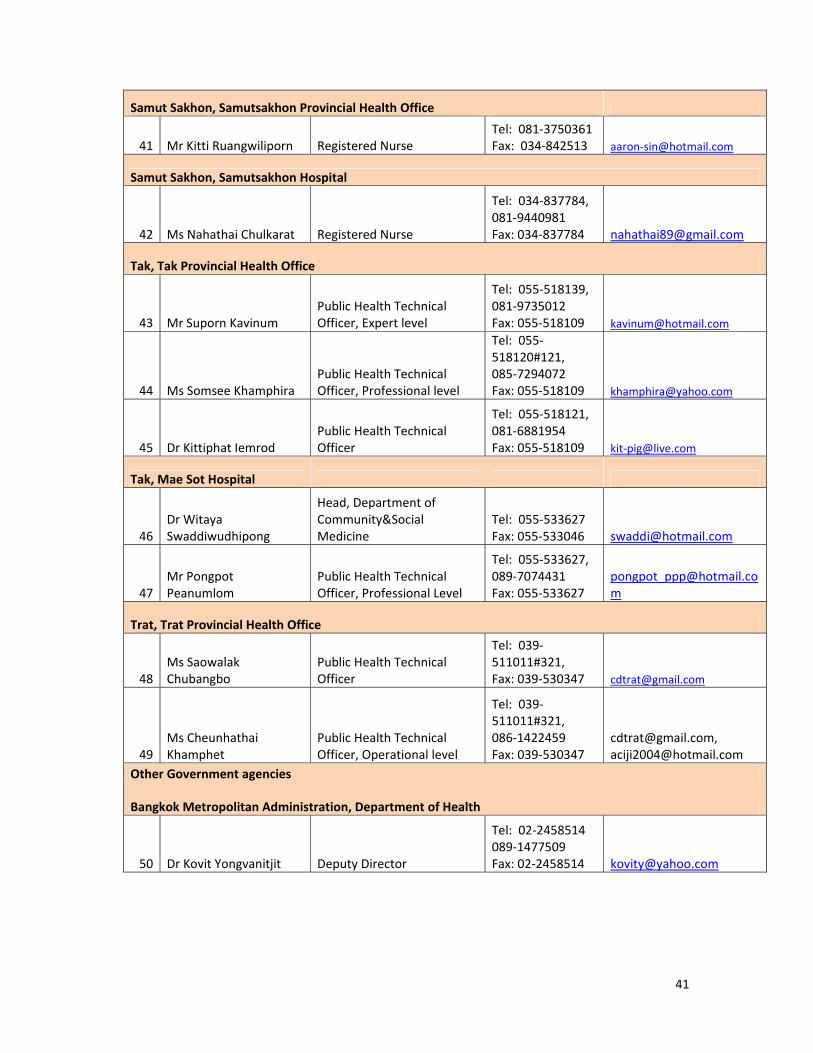
41
Samut Sakhon, Samutsakhon Provincial Health Office
41 Mr Kitti Ruangwiliporn Registered Nurse Tel: 081‐3750361 Fax: 034‐842513 aaron‐[email protected]
Samut Sakhon, Samutsakhon Hospital
42 Ms Nahathai Chulkarat Registered Nurse
Tel: 034‐837784, 081‐9440981 Fax: 034‐837784 [email protected]
Tak, Tak Provincial Health Office
43 Mr Suporn Kavinum Public Health Technical Officer, Expert level
Tel: 055‐518139, 081‐9735012 Fax: 055‐518109 [email protected]
44 Ms Somsee Khamphira Public Health Technical Officer, Professional level
Tel: 055‐518120#121, 085‐7294072 Fax: 055‐518109 [email protected]
45 Dr Kittiphat Iemrod Public Health Technical Officer
Tel: 055‐518121, 081‐6881954 Fax: 055‐518109 kit‐[email protected]
Tak, Mae Sot Hospital
46 Dr Witaya Swaddiwudhipong
Head, Department of Community&Social Medicine
Tel: 055‐533627 Fax: 055‐533046 [email protected]
47 Mr Pongpot Peanumlom
Public Health Technical Officer, Professional Level
Tel: 055‐533627, 089‐7074431 Fax: 055‐533627
Trat, Trat Provincial Health Office
48 Ms Saowalak Chubangbo
Public Health Technical Officer
Tel: 039‐511011#321, Fax: 039‐530347 [email protected]
49 Ms Cheunhathai Khamphet
Public Health Technical Officer, Operational level
Tel: 039‐511011#321, 086‐1422459 Fax: 039‐530347
[email protected], [email protected]
Other Government agencies
Bangkok Metropolitan Administration, Department of Health
50 Dr Kovit Yongvanitjit Deputy Director
Tel: 02‐2458514 089‐1477509 Fax: 02‐2458514 [email protected]
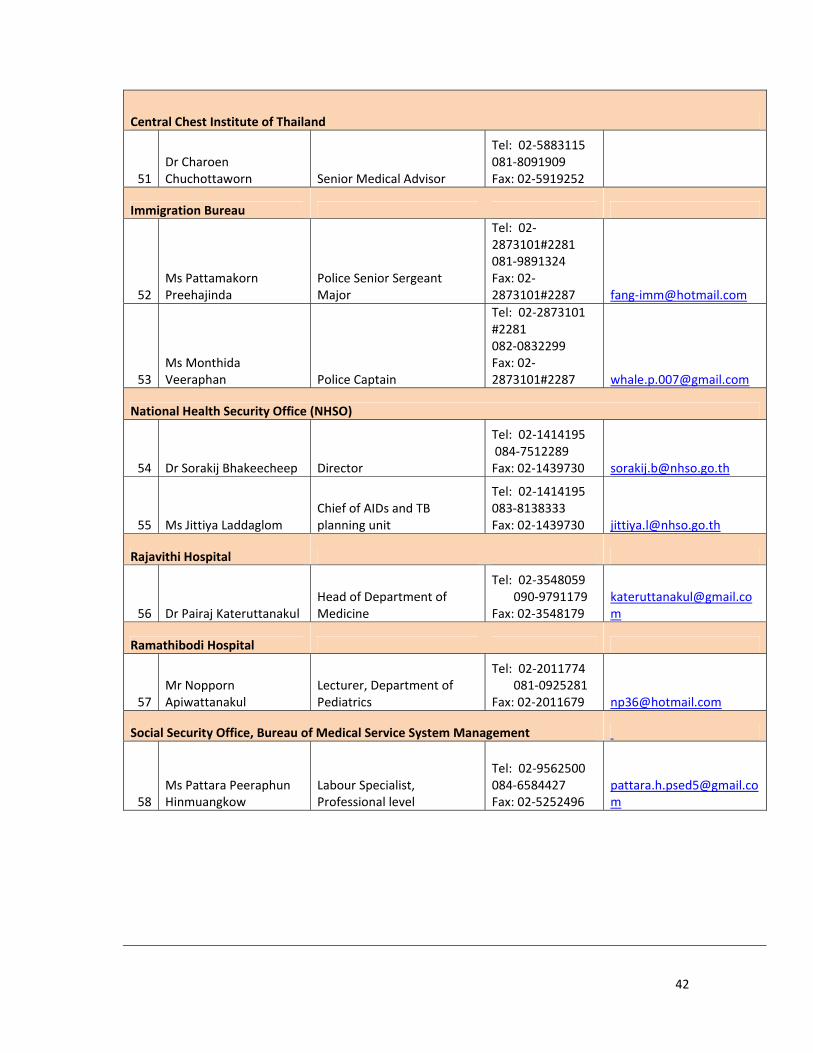
42
Central Chest Institute of Thailand
51 Dr Charoen Chuchottaworn Senior Medical Advisor
Tel: 02‐5883115 081‐8091909 Fax: 02‐5919252
Immigration Bureau
52 Ms Pattamakorn Preehajinda
Police Senior Sergeant Major
Tel: 02‐2873101#2281 081‐9891324 Fax: 02‐2873101#2287 fang‐[email protected]
53 Ms Monthida Veeraphan Police Captain
Tel: 02‐2873101 #2281 082‐0832299 Fax: 02‐2873101#2287 [email protected]
National Health Security Office (NHSO)
54 Dr Sorakij Bhakeecheep Director
Tel: 02‐1414195 084‐7512289 Fax: 02‐1439730 [email protected]
55 Ms Jittiya Laddaglom Chief of AIDs and TB planning unit
Tel: 02‐1414195 083‐8138333 Fax: 02‐1439730 [email protected]
Rajavithi Hospital
56 Dr Pairaj Kateruttanakul Head of Department of Medicine
Tel: 02‐3548059 090‐9791179 Fax: 02‐3548179
Ramathibodi Hospital
57 Mr Nopporn Apiwattanakul
Lecturer, Department of Pediatrics
Tel: 02‐2011774 081‐0925281 Fax: 02‐2011679 [email protected]
Social Security Office, Bureau of Medical Service System Management
58 Ms Pattara Peeraphun Hinmuangkow
Labour Specialist, Professional level
Tel: 02‐9562500 084‐6584427 Fax: 02‐5252496

43
Government agencies ‐ Cambodia
Ministry of Health, Banteay Mean Chey Province
59 Dr Kimsorth Heng
Chief of Tuberculosis Programme in Banteay Mean Chey Province +855 17 351111 [email protected]
Ministry of Health, Oddor Meanchey Province
60 Dr Kham Samphos Chief of Ternical Bureau and RRT Manager +855 12 499192 [email protected]
Ministry of Health, Preah Vihear Province
61 Dr Saomony Chhay
Deputy Director, Preah Vihear Provincial Health Department +855 12 955693 [email protected]
Government agencies – Lao PDR
Ministry of Health
62 Dr Phouvang Vangvichit Department Director National TB Center [email protected]
63 Dr Soth Bounmala Project Coordinator National TB Center [email protected]
Government agencies – Myanmar
Ministry of Health
64 Dr Cho Cho San
Assistant Director (TB), National TB Control Programme Department of Health, Naypyitaw
65 Dr Win Naing
State TB Control Officer TB Control Programme, Mon State, Mawlamyaing [email protected]
66 Dr Lwin Lwin Mon
Team Leader TB Control Programme, Taninthayi Region, Myeik [email protected]

44
NGOs and INGOs
No Name Title Contact
information E‐mail address
Kanchanaburi,Kwai River Christian Hospital
1 Mrs Lalida Murray
Public Health Nurse, Assistant to Business Manager
Tel: 034‐688001 082‐2930109 Fax: 034‐688003 [email protected]
2 Ms Laongdao Sankawiram Health Promotion Officer
Tel: 034‐688001 087‐1586285 Fax: 034‐688003 [email protected]
American Refugee Committee International (ARC)
3 Dr Gary Dahl Country Director
Tel: 02‐2525186 081‐8463548 Fax: 02‐2532899 [email protected]
4 Dr Aye Aye Moe Medical Coordinator
Tel: 034‐595580 080‐2165548 Fax: 034‐595177
[email protected] [email protected]
Committee for Coordination of Service to Displaced Persons in Thailand (CCSDPT)
5 Dr Thet Win Health Information System Coordinator
Tel: 02‐2557025 081‐9351722 Fax: 02‐2557022 [email protected]
European Union (EU)
6 Ms Priya Waeohongsa Programme Officer Tel: 02‐3052752 Fax: 02‐2559113
7 Ms Khobkhul Inieam Operations Assistant Tel: 02‐3052746 Fax: 02‐2559113
European Commission DG for Humanitarian Aid and Civil Protection (ECHO)
8 Ms Piriyada Vessuwon Regional Programme Assistant Tel: 081‐8411527
FHI 360
9 Dr Anh L. Innes Chief of Party, FHI
Tel: 02‐2632300#180 081‐9318621 ainnes@fhi360@org
10 Dr Yuthichai Kasetcharoen Advisor to FHI Tel: 089‐6591878 [email protected]

45
Global Fund
11 Dr Philippe Creac'h Fund Portfolio Manager Tel: +41 79 2217830
International Organization of Migration (IOM) Regional office, Bangkok
12 Dr Jaime Calderon Regional Migration Health Adviser
Tel: 02‐3439448 081‐8326900 Fax: 02‐3439499 [email protected]
13 Dr Montira Inkochasan Senior Regional Migration Health Assistant
Tel: 02‐3439416 080‐5364242 Fax: 02‐3439499 [email protected]
14 Ms Jacqueline Weekers
Senior Regional Health Assessment Programme Coordinator
Tel: 02‐3439462 081‐9183482 [email protected]
15 Mr Iain Mclellan [email protected]
Cambodia Country Office
16 Dr Brett Dickson Project Coordinator, TB REACH funded project
Tel: +855 12 222132 Fax: +855 23 216423 [email protected]
Myanmar Country Office
17 Mr Greg Irving Programme Manager ‐Migration Health
Tel: +95 1 254008#5005 +95 94 3170624 Fax: +95 1 252560#5010 [email protected]
Thailand Country Office
18 Dr Olga Gorbacheva Chief Medical Officer
Tel: 02‐3439300#9367 081‐3762058 Fax: 02‐3439399 [email protected]
19 Ms Valentina Parr Lab Manager/MHP Coordination
Tel: 02‐3439362 081‐3766171 [email protected]
International Rescue Committee
20 Dr Aung Than Lin Clinical Medical Officer, Tham Hin Ratchaburi
Tel: 032‐364448#103 084‐2738724 Fax: 032‐364357 [email protected]

46
International Rescue Committee
21 Dr Nyi Wynn Soe Health Coordinator, Mae Hong Son programme
Tel: 053‐611626 081‐9606160 Fax: 053‐611404
[email protected], [email protected]
Malteser International
22 Dr Susanne Rastin Medical Coordinator
Tel: 053‐621559 086‐1858603 Fax: 053‐681575
susanne.rastin@malteser‐international.org
Premier Urgence‐Aide Medicale Internationale (PU‐AMI)
23 Dr Kyaw Zaw Myat Deputy Programme Coordinator
tha.deputyprogrames@pu‐ami.org
24 Dr Htun Myint TB Manager tha.tbmanger@pu‐ami.org
25 Dr Carole Deglise Health Advisor‐Asia Tel: 090‐4520994 cdeglise@pu‐ami.org
Rak Thai Foundation
26 Mr Promboon Panitchpakdi Executive Director
Tel: 02‐2656888 081‐8107089 Fax: 02‐2714467 [email protected]
27 Ms Wanna Buthasane Project Manager
Tel: 02‐2656888 089‐7123597 Fax: 02‐2714467 [email protected]
28 Ms Ruangtong Chantichai Programme Assistant‐TB
Tel: 02‐2656888#29 081‐8406116 Fax: 02‐2714467
[email protected] [email protected]
Shoklo Malaria Research Unit (SMRU)
29 Dr Sein Sein Thi TB Doctor Tel: 055‐545020 085‐6030563 seinseinthi@shoklo‐unit.com
Thailand Business Coalition on AIDS (TBCA)
30 Dr Anthony Pramualratana Executive Director Tel: 081‐5579626
31 Dr Brohmsek Yen‐ura Operations Director
Tel: 02‐6438080 081‐8201951 Fax: 02‐6438089 [email protected]

47
Thailand Business Coalition on AIDS (TBCA)
32 Dr Peeraporn Weruwanaruk Operations Team Leader
Tel: 02‐6438080081‐8201951 Fax: 02‐6438089 [email protected]
Thailand MOPH US‐CDC Collabouration (TUC)
33 Dr Christina Phares [email protected]
34 Dr Luis Ortega Programme Director
Tel: 02‐5800669 084‐8742166 Fax: 02‐5912909 [email protected]
35 Dr Nuttapong Wongjindanon Epidemiologist
Tel: 02‐5800669#571 085‐4870227 Fax: 02‐5912909 [email protected]
36 Dr Sara Whitehead Tel: 02‐5800669 Fax: 02‐5912909 [email protected]
World Vision
37 Dr Sarmphong Nang M&E Coordinator and Technical Support
Tel: 02‐3818863 084‐6782176 Fax: 02‐3814923 [email protected]
Rapporteur
38 Ms Virginia MacDonald Tel: 089‐0551774
[email protected] [email protected]
Simultaneous Translation
39 Mr Kanok Suwannasit
40 Mr Suraphan Virojanadul
Conference organizer
World Health Organization WCO Cambodia
1 Dr Miwako Kobayashi Professional Officer [email protected]

48
WCO Myanmar
2 Dr Eva Nathanson Technical Officer
Tel: +951 241932 +951 241933 Fax: +951 241836 [email protected]
WCO Thailand
3 Dr Yonas Tegegn WR Representative Tel: 02‐5918198 Fax: 02‐5918199
4 Dr Monirul Islam Tel: 02‐5918198 Fax: 02‐5918199 [email protected]
5 Dr Brenton Burkholder Border and Migrant Health Programme Coordinator
Tel: 02‐5918198 089‐8908061 Fax: 02‐5918199 [email protected]
6 Ms Aree Moungsookjareoun
Border and Migrant Health Officer
Tel: 02‐5918198 081‐8106816 Fax: 02‐5918199 [email protected]
7 Ms Benja Sae‐Seai Programme Assistant
Tel: 02‐5918198 081‐8087145 Fax: 02‐5918199 [email protected]
8 Ms Wilawan Tanyavutti Programme Assistant
Tel: 02‐5918198 084‐6630673 Fax: 02‐5918199 [email protected]
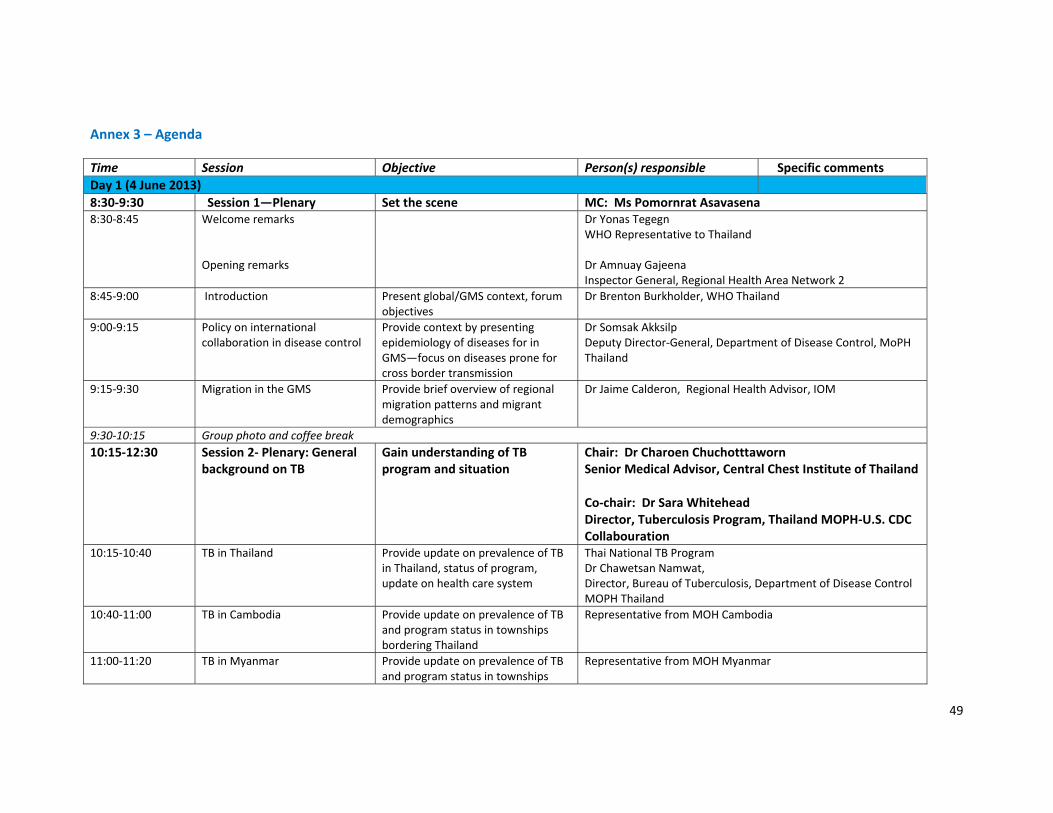
49
Annex 3 – Agenda
Time Session Objective Person(s) responsible Specific comments
Day 1 (4 June 2013)
8:30‐9:30 Session 1—Plenary Set the scene MC: Ms Pomornrat Asavasena8:30‐8:45 Welcome remarks
Opening remarks
Dr Yonas TegegnWHO Representative to Thailand Dr Amnuay Gajeena Inspector General, Regional Health Area Network 2
8:45‐9:00 Introduction Present global/GMS context, forum objectives
Dr Brenton Burkholder, WHO Thailand
9:00‐9:15 Policy on international collaboration in disease control
Provide context by presenting epidemiology of diseases for in GMS—focus on diseases prone for cross border transmission
Dr Somsak Akksilp Deputy Director‐General, Department of Disease Control, MoPH Thailand
9:15‐9:30 Migration in the GMS Provide brief overview of regional migration patterns and migrant demographics
Dr Jaime Calderon, Regional Health Advisor, IOM
9:30‐10:15 Group photo and coffee break
10:15‐12:30 Session 2‐ Plenary: General background on TB
Gain understanding of TB program and situation
Chair: Dr Charoen Chuchotttaworn Senior Medical Advisor, Central Chest Institute of Thailand Co‐chair: Dr Sara Whitehead Director, Tuberculosis Program, Thailand MOPH‐U.S. CDC Collabouration
10:15‐10:40 TB in Thailand Provide update on prevalence of TB in Thailand, status of program, update on health care system
Thai National TB Program Dr Chawetsan Namwat, Director, Bureau of Tuberculosis, Department of Disease Control MOPH Thailand
10:40‐11:00 TB in Cambodia Provide update on prevalence of TB and program status in townships bordering Thailand
Representative from MOH Cambodia
11:00‐11:20 TB in Myanmar Provide update on prevalence of TB and program status in townships
Representative from MOH Myanmar

50
Time Session Objective Person(s) responsible Specific commentsbordering Thailand
11:20‐11:40 TB in Lao PDR Provide update on prevalence of TB and program status in townships bordering Thailand
Representative from MOH Lao PDR
11:40‐12:30 Comments and discussion Provide academic and program perspective
Chair/co‐chair Provide comments on the 4 national programs
12:30n‐13:30 Lunch
13:30‐17:00 (coffee break from 15:45‐16:15)
Session 3‐ Panels: Target populations
Provide experience on current operational challenges/ identification, diagnosis, treatment for TB control among various target populations and provide examples of creative program strategies
Chair: Dr Supakit Sirilak,Senior Advisor (Preventive Medicine), Permanent Secretary Office, MOPH Thailand Co‐chair: Dr Eva Nathanson, Technical Officer, WHO Myanmar
13:30‐14:30 Labour migrants (documented + irregular migrants)— in Thailand for >6months
Update on TB among longer stay migrants in both urban and border areas
1.“TB reduction among non‐Thai migrants: a NGO perspective”—World Vision 2.”Controlling TB in a border province:”— Tak PHO 3. “Controlling TB in an urban area:”— Samut Sakhorn PHO
14:30‐15:45 Causal Cross‐border migrants –in Thailand for <6 months
Update on TB among short term migrants, those crossing the border to seek health care, and outreach across the border
1. “Initial progress of the Tak TB Initiative (TTBI)”—SMRU2. “Controlling TB in a border province:”— Sa Kaeo PHO 3. “Providing DOTS to migrant populations”—Kwai River Christian Hospital 4. “Controlling TB in a border province:”— Kanchanaburi PHO
15:45‐16:15 Coffee break
16:15‐17:00 Special settings: Displaced persons (including those seeking re‐settlement) and Detention Centers
Update on TB among those in temporary shelters, those seeking re‐settlement, and those in detention centers
1.”Controlling TB in displace person temporary shelters”‐PU‐AMI 2. “TB screening among displaced persons seeking resettlement”—IOM/Thailand 3. “TB screening among migrants in detention centers”—Mr Wachiarapun Chaimoontee, Bureau of General Communicable Disease, DDC, MOPH Thailand
17:00‐17:30 Chair and Co‐chair provide comments and open for panel discussion

51
Day 2 (5 June 2013)
8:30‐12.00 (coffee break 10:‐10:30)
Session 4: Working Groups (6) Two work groups for each of the three target populations
A. Health system impact and requirements
B. Health of the migrant
To further share experiences and provide opportunity to develop concrete suggestions to strengthen implementation.
For all group A: Provide a programmatic overview relevant to the target population by assessing status and gaps for each of the 4 priority action areas* For all group B: Provide an assessment of key challenges and possible suggestions by technical area (diagnosis, treatment, follow‐up/referral)
Facilitators/rapporteurs: Labour A: TBD Labour B: TBD Casual A: TBD Casual B: TBD Special setting A: TBD Special setting B: TBD
Divide into 6 working groups (w/ max of 15 persons + designated facilitator). 2 rounds—participants can switch groups after first round if they choose
8:30 Provide summary of Day 1 and Introduction to Group Work
Ms Virginia Macdonald, Rapporteur Dr Brenton Burkholder, WHO Thailand
9:00‐10.00 Working Groups: round 1 All
10:00‐10:30 Coffee break
10:30 Work Groups: round 2 All
12.00‐13:30 Lunch
13:30‐16:30 (coffee break 15:‐15:30
Session 5: Report from each work group
Share findings and recommendations
Reports (10 min) from each working group followed by group discussion
16:30‐17:00 Closing Dr Chawetsan Namwat,Bureau of Tuberculosis, DDC, Thailand MoPH Dr Brent Burkholder WHO Thailand
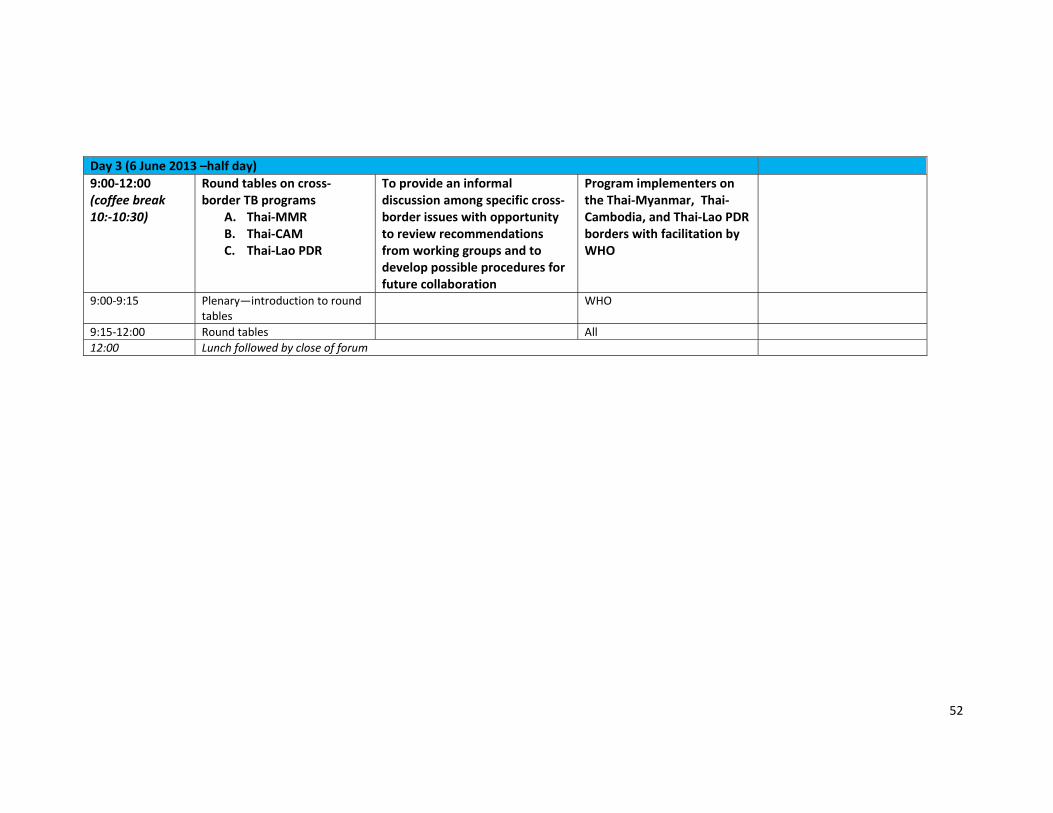
52
Day 3 (6 June 2013 –half day)
9:00‐12:00 (coffee break 10:‐10:30)
Round tables on cross‐border TB programs
A. Thai‐MMR B. Thai‐CAM C. Thai‐Lao PDR
To provide an informal discussion among specific cross‐border issues with opportunity to review recommendations from working groups and to develop possible procedures for future collaboration
Program implementers on the Thai‐Myanmar, Thai‐Cambodia, and Thai‐Lao PDR borders with facilitation by WHO
9:00‐9:15 Plenary—introduction to round tables
WHO
9:15‐12:00 Round tables All
12:00 Lunch followed by close of forum