Forest cover associated with improved child health and nutrition: … · 2014-08-19 · ing...
12
ORIGINAL ARTICLE Forest cover associated with improved child health and nutrition: evidence from the Malawi Demographic and Health Survey and satellite data Kiersten B Johnson, a Anila Jacob, b Molly E Brown c In Malawi, net forest cover loss over time is associated with reduced dietary diversity and consumption of vitamin A-rich foods among children. Greater forest cover is associated with reduced risk of diarrheal disease. These preliminary findings suggest that protection of natural ecosystems could play an important role in improving health outcomes. ABSTRACT Healthy forests provide human communities with a host of important ecosystem services, including the provision of food, clean water, fuel, and natural medicines. Yet globally, about 13 million hectares of forests are lost every year, with the biggest losses in Africa and South America. As biodiversity loss and ecosystem degradation due to deforestation continue at unprecedented rates, with concomitant loss of ecosystem services, impacts on human health remain poorly understood. Here, we use data from the 2010 Malawi Demographic and Health Survey, linked with satellite remote sensing data on forest cover, to explore and better understand this relationship. Our analysis finds that forest cover is associated with improved health and nutrition outcomes among children in Malawi. Children living in areas with net forest cover loss between 2000 and 2010 were 19% less likely to have a diverse diet and 29% less likely to consume vitamin A-rich foods than children living in areas with no net change in forest cover. Conversely, children living in communities with higher percentages of forest cover were more likely to consume vitamin A-rich foods and less likely to experience diarrhea. Net gain in forest cover over the 10-year period was associated with a 34% decrease in the odds of children experiencing diarrhea (P5.002). Given that our analysis relied on observational data and that there were potential unknown factors for which we could not account, these preliminary findings demonstrate only associations, not causal relationships, between forest cover and child health and nutrition outcomes. However, the findings raise concerns about the potential short- and long-term impacts of ongoing deforestation and ecosystem degradation on community health in Malawi, and they suggest that preventing forest loss and maintaining the ecosystems services of forests are important factors in improving human health and nutrition outcomes. INTRODUCTION F orests provide critical resources and processes that benefit human populations, known as ecosystem services, including food, clean water, fuel, natural medicines, and pollination. More than 1.5 billion people worldwide rely on forest products for their livelihoods. 1 Yet globally, about 13 million hectares of forests are lost every year, primarily due to agricultural expansion, extraction of natural resources, and human settlement. 2 Deforestation is a major driver of biodi- versity loss, which continues unabated despite global efforts to stem this loss. 3 According to the Board of the Millennium Ecosystem Assessment, loss of ecosystem services poses a considerable barrier to achieving the Millennium Development Goals to reduce poverty, hunger, and disease. 4 (The United Nations Secretary- General called for the Millennium Ecosystem Assessment in 2000 to assess the consequences of ecosystem change on human well-being.) Although all populations fundamentally depend on the natural environment, people living in rural areas of the developing world are most directly dependent on a ICF Macro, Beltsville, MD, USA b U.S. Agency for International Development, Forestry and Biodiversity Office, Washington, DC, USA c NASA, Biospheric Sciences Branch, Greenbelt, MD, USA Correspondence to Kiersten Johnson (mailto:[email protected]). Global Health: Science and Practice 2013 | Volume 1 | Number 2 1 https://ntrs.nasa.gov/search.jsp?R=20140010157 2020-06-08T06:15:27+00:00Z
Transcript of Forest cover associated with improved child health and nutrition: … · 2014-08-19 · ing...

ORIGINAL ARTICLE
Forest cover associated with improved child health andnutrition: evidence from the Malawi Demographic andHealth Survey and satellite dataKiersten B Johnson,a Anila Jacob,b Molly E Brownc
In Malawi, net forest cover loss over time is associated with reduced dietary diversity and consumption ofvitamin A-rich foods among children. Greater forest cover is associated with reduced risk of diarrhealdisease. These preliminary findings suggest that protection of natural ecosystems could play an importantrole in improving health outcomes.
ABSTRACTHealthy forests provide human communities with a host of important ecosystem services, including the provision of food,clean water, fuel, and natural medicines. Yet globally, about 13 million hectares of forests are lost every year, with thebiggest losses in Africa and South America. As biodiversity loss and ecosystem degradation due to deforestationcontinue at unprecedented rates, with concomitant loss of ecosystem services, impacts on human health remain poorlyunderstood. Here, we use data from the 2010 Malawi Demographic and Health Survey, linked with satellite remotesensing data on forest cover, to explore and better understand this relationship. Our analysis finds that forest cover isassociated with improved health and nutrition outcomes among children in Malawi. Children living in areas with netforest cover loss between 2000 and 2010 were 19% less likely to have a diverse diet and 29% less likely to consumevitamin A-rich foods than children living in areas with no net change in forest cover. Conversely, children living incommunities with higher percentages of forest cover were more likely to consume vitamin A-rich foods and less likely toexperience diarrhea. Net gain in forest cover over the 10-year period was associated with a 34% decrease in the oddsof children experiencing diarrhea (P5.002). Given that our analysis relied on observational data and that there werepotential unknown factors for which we could not account, these preliminary findings demonstrate only associations, notcausal relationships, between forest cover and child health and nutrition outcomes. However, the findings raise concernsabout the potential short- and long-term impacts of ongoing deforestation and ecosystem degradation on communityhealth in Malawi, and they suggest that preventing forest loss and maintaining the ecosystems services of forests areimportant factors in improving human health and nutrition outcomes.
INTRODUCTION
F orests provide critical resources and processes thatbenefit human populations, known as ecosystem
services, including food, clean water, fuel, naturalmedicines, and pollination. More than 1.5 billionpeople worldwide rely on forest products for theirlivelihoods.1 Yet globally, about 13 million hectares offorests are lost every year, primarily due to agricultural
expansion, extraction of natural resources, and humansettlement.2 Deforestation is a major driver of biodi-versity loss, which continues unabated despite globalefforts to stem this loss.3 According to the Board of theMillennium Ecosystem Assessment, loss of ecosystemservices poses a considerable barrier to achieving theMillennium Development Goals to reduce poverty,hunger, and disease.4 (The United Nations Secretary-General called for the Millennium EcosystemAssessment in 2000 to assess the consequences ofecosystem change on human well-being.)
Although all populations fundamentally depend onthe natural environment, people living in rural areas ofthe developing world are most directly dependent on
a ICF Macro, Beltsville, MD, USAbU.S. Agency for International Development, Forestry and Biodiversity Office,Washington, DC, USAcNASA, Biospheric Sciences Branch, Greenbelt, MD, USA
Correspondence to Kiersten Johnson (mailto:[email protected]).
Global Health: Science and Practice 2013 | Volume 1 | Number 2 1
https://ntrs.nasa.gov/search.jsp?R=20140010157 2020-06-08T06:15:27+00:00Z

ecosystems services to meet their basic needs.5 Asbiodiversity loss and ecosystem degradationcontinue at unprecedented rates, there is increas-ing concern about potential public healthimpacts, especially among the world’s mostvulnerable populations.
Research on the links between human healthand deforestation is limited, but a handful ofstudies suggest that ecosystem degradation hasnegative impacts on public health. For example,a Nepal study from the 1980s showed thatdeforestation increased women’s time spentgathering essential forest products (such as fuelwood and fodder for livestock) that was sig-nificant enough to reduce the amount of timethey spent on agricultural production, foodpreparation, and breastfeeding.6 Researchers inMadagascar showed, through modeling, thatanemia incidence in children would increase by29% if they no longer had access to wildlife as afood source, either due to species extinction orstrict enforcement of conservation policies.7
Among the poorest children, anemia cases wouldtriple. In a study of 54 health districts in theBrazilian Amazon, researchers found that a 4%increase in deforestation rates was associatedwith a 48% increase in malaria incidence.8
To better understand the potential health andnutrition impacts of deforestation, we conducteda case study of Malawi using 2010 Demographicand Health Survey (DHS) data linked, viageographic information system (GIS) points,with satellite remote sensing data on forest coverand change in forest cover over a decade’s time.
HYPOTHESIS
We hypothesized that deforestation and lowerpercentages of forest cover (proxies for degradedenvironments) result in declining ecosystemservices, which then open pathways to childundernutrition and poor health.
Ecosystem services are defined as the short-and long-term benefits people obtain fromecosystems, comprising:
N Provisioning goods and services (the pro-duction of basic goods such as food, water,fish, fuels, timber, and fiber)
N Regulating services (such as flood protection,purification of air and water, waste absorp-tion, disease control, and climate regulation)
N Cultural services (spiritual, aesthetic, andrecreational benefits)
N Supporting services necessary for the pro-duction of all other ecosystem services(including soil formation, production ofoxygen, crop pollination, carbon sequestra-tion, photosynthesis, and nutrient cycling)
Conversely, we hypothesized that more bio-diverse environments, represented by higherpercentages of forest cover, have comparativelybetter capacity to provide essential ecosystemservices, which then translate into improvedhuman nutrition and health outcomes.
Our outcomes of interest include children’sdietary diversity, consumption of vitamin A-rich foods, stunting, and experience of diar-rheal disease. We expect these outcomes to beassociated particularly with the level andquality of provisioning and regulating ecosystemservices.
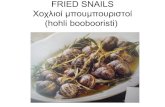
A comprehensive description of the complexand nonlinear relationships between the envir-onment and human health outcomes is beyondthe scope of this paper. However, our conceptualframework provides a simple illustration of the 3hypothesized relationships that we explore inthis analysis: (a) between forest cover andnutritional outcomes; (b) between forest coverand health outcomes; and (c) the mediatingfunction of women’s time on the relationshipbetween forest cover and nutritional outcomes(Figure 1).
Hypothesized Pathways Between ForestCover and Nutritional OutcomesProvisioning services provided by forests are animportant source of food for the rural poor, whooften rely on bushmeat and other non-timberforest products (NTFPs) for their protein andmicronutrients. In the Congo Basin, bushmeatprovides about half of people’s protein intake.9 Ina recent study of rural households in westernGhana, researchers found that residents routi-nely consumed a variety of forest foods, includ-ing bushmeat, plants, fruits, and snails.10
Residents of poorer households consumed theseitems more often than residents of wealthierhouseholds—on average, 5 days a week com-pared with 3 days a week, respectively.Furthermore, many households also sold variousNTFPs at local markets, generating additionalincome that improved food security. In ruralMalawi, researchers found that food from forestsprovided a safety net during times of crop failure;study participants reported that, on average,
More than 1.5billion peopleworldwide rely onforest products fortheir livelihoods,but 13 millionhectares of forestsare lost everyyear.
Ecosystemsprovide severalbenefits to people,such as food,water, floodprotection, wasteabsorption, andcrop pollination.
Poor, ruralresidents oftenrely on forestfoods for theirnutrients.
Forest cover, health, and nutrition in Malawi www.ghspjournal.org
Global Health: Science and Practice 2013 | Volume 1 | Number 2 2

more than 50% of their meals were derived fromforests during times of famine.11
These studies demonstrate reliance onNTFPs, particularly among the rural poor, andprovide a strong basis for the hypothesis thatdeforestation results in decreased availability offorest foods, which in turn can lead to compara-tively poorer nutritional outcomes among chil-dren as well as adults.
Hypothesized Pathways Between ForestCover and Health OutcomesPopulations living near intact forest ecosystemsare closer to forest plants and insect life thatnaturally decompose human and animal wasteand convert it to energy (a regulating ecosystemservice). Forest degradation reduces these func-tions, which in turn degrade the ability of insectlife to process animal waste.12
In Indonesia, a study found that residents ofhouseholds living downstream from protectedforested watersheds were less likely to experiencediarrhea than those living downstream from
unforested watersheds, demonstrating the reg-ulating services of forests in improving quality ofdrinking water.13 Similarly, we hypothesize thatchildren living in households close to forest coverwill experience reduced odds of diarrheal diseasecompared with children not living close to forestcover.
Hypothesized Mediating Function ofWomen’s Time on the RelationshipBetween Forest Cover and NutritionalOutcomesThe Nepal study6 demonstrated a negativeassociation between deforestation and women’stime allocation on nutrition-related functionssuch as food preparation and breastfeeding,subsequently limiting women’s ability to providenutrition to their children. Although we cannottest the role of women’s time allocation inmediating the hypothesized relationship betweenforest cover and child health and nutritionoutcomes in this study, we believe it is importantto represent this mediating function in the
Forests help toimprove thequality of drinkingwater.
FIGURE 1. Conceptual Framework of Pathways Between Biodiverse Environments and HumanHealth and Nutrition Outcomes
We hypothesize that biodiverse environments are better able to produce ecosystem services, such as food and clean water,which, in turn, improve the quantity and quality of food consumption by children and reduce diseases, leading ultimately tobetter health and nutrition outcomes. Mother’s time acts as a mediating factor between biodiversity and child health andnutrition outcomes.
Forest cover, health, and nutrition in Malawi www.ghspjournal.org
Global Health: Science and Practice 2013 | Volume 1 | Number 2 3

conceptual model, given the well-demonstratedcentrality of women’s role in ensuring childhealth and nutrition outcomes.
DATA AND METHODS
Study Site SelectionWe selected Malawi as our study country givenits very high rates of deforestation, child under-nutrition, and child mortality, as well as thedirect dependence of the majority of the popula-tion on ecosystem services. Malawi has lostalmost 600,000 hectares of primary forestbetween 1990 and 2005, with regional deforesta-tion rates as high as 3.4% per year.14 Over 80% ofMalawi’s population is rural and highly depen-dent on natural resources for food, fuel, andmaintenance of livelihoods.14–15 Forty-seven per-cent of children are stunted, and the under-5mortality rate is 112 deaths per 1,000 livebirths.16
DataDemographic and Health Surveys DataWe obtained nutritional status and dietaryconsumption data, as well as other individual-level characteristics, from the 2010 Malawi DHS.
The DHS are a key source of comparativequantitative data across developing countries ondemographic and health indicators, including forreproductive health, maternal and child health,and nutritional status of women and children.They are nationally and sub-nationally represen-tative household surveys with large sample sizesand detailed data obtained by interviewingwomen of reproductive age (15–49 years old) toobtain information about their children andother household members. The data also includeinformation on household and other socioeco-nomic characteristics of sampled women andtheir households.
The DHS are implemented using a stratified2-stage cluster sampling design. In Malawi, morethan 23,000 households participated in the 2010survey (household response rate: 98%; individualwomen’s response rate: 97%).16 For more infor-mation about the DHS, see www.measuredhs.com.
Satellite Remote Sensing DataWe used 2 types of satellite remote sensingvariables in this analysis: the VegetationContinuous Fields (VCF) product17 and theNormalized Difference Vegetation Index
(NDVI).18 A full technical description of thesatellite remote sensing data sets used in thisanalysis is available in the supplementaryAppendix; the variables are described below.
GPS Data and DisplacementDuring DHS fieldwork activities, surveyors col-lected the GPS coordinates for the center of thepopulated area surveyed (cluster centroid) usinghandheld GPS units. Of importance to this analysisis that the GPS coordinates are displaced to ensurerespondent confidentiality.16 The displacement israndomly applied so that rural points contain aminimum of 0 km and a maximum of 5 km ofpositional error. Urban points contain a minimumof 0 km and a maximum of 2 km of error. Afurther 1% of the rural sample points are offset aminimum of 0 km and a maximum of 10 km.
We overlaid DHS data with average NDVIdata derived from NASA’s Moderate ResolutionImaging Spectroradiometer (MODIS) (a keysatellite instrument that views the Earth’s sur-face) at each DHS cluster centroid for 2010. Weused a similar procedure with the VCF product tolink the percent forest cover variable and thechange in forest cover variable to the 2010Malawi DHS data set.
We chose to aggregate the satellite data to5 km resolution to ensure that even afterdisplacement of DHS GPS coordinates, environ-mental variability and tree cover were accuratelyrepresented for each DHS cluster. Displacementerrors were below the spatial resolution of thesatellite remote sensing.
Variable DefinitionsDependent VariablesOur analysis explored 4 dependent, dichotomousvariables: severe stunting, dietary diversity, con-sumption of vitamin A-rich foods, and diarrhea.
1. Severe stunting: The height, weight, andage of all children under age 5 were collectedduring DHS fieldwork using UNICEF SECAweight scales and Shorr height boards; thesedata were then used to calculate measures ofchild stunting. Stunting, or height-for-age,reflects the long-term nutritional status of achild, indicating impacts of both nutritionaldeficiencies and bouts with illnesses.Children with height-for-age z-scores thatare less than -3 standard deviations from themedian of the reference population areconsidered to be severely stunted. We coded
Forest cover, health, and nutrition in Malawi www.ghspjournal.org
Global Health: Science and Practice 2013 | Volume 1 | Number 2 4

severely stunted children with a ‘‘1’’ and allremaining children with a ‘‘0.’’
2. Dietary diversity: The DHS instrumentcollects 24-hour recall data on dietary
consumption for the most recently born child
under the age of 3. Our definition of dietary
diversity was based on the Minimum Dietary
Diversity indicator19 defined by an expert
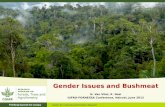
Map of Malawi showing 2010 forest cover overlaid with sampling clusters from the 2010 Malawi DHS.
Forest cover, health, and nutrition in Malawi www.ghspjournal.org
Global Health: Science and Practice 2013 | Volume 1 | Number 2 5

working group led by the World HealthOrganization–that is, the proportion of chil-dren 6–23 months of age who receive foodsfrom 4 or more of the following food groups:(a) grains, roots, and tubers; (b) legumes andnuts; (c) dairy products (milk, yogurt, andcheese); (d) flesh foods (meat, fish, poultry,and liver/organ meats); (e) eggs; (f) vitamin-A rich fruits and vegetables; and (g) otherfruits and vegetables. For our definition, wealso included breast milk as one of the foodgroups, given its importance as a source ofnutrition for children and that breastfeedingpractices are likely to be impacted by defor-estation. We also included all children underage 3 in our analysis, given that manychildren are given foods other than breastmilk prior to 6 months of age, despite therecommendation that infants be exclusivelybreastfed until that age. We coded childrenwho consumed foods from 4 or more foodgroups with a ‘‘1’’ and all remaining childrenwith a ‘‘0.’’
3. Consumption of vitamin-A rich foods:Data on consumption of vitamin-A rich foodswere also drawn from the 24-hour recall dataon dietary consumption for the most recentlyborn child under the age of 3, describedabove. All children under age 3 were includedin the analysis, and we coded children whoconsumed vitamin-A rich foods (fruits orvegetables) with a ‘‘1’’ and all remainingchildren with a ‘‘0.’’
4. Diarrhea: In DHS surveys, mothers ofchildren under age 5 are asked whether theirchildren have experienced a bout of diarrheain the past 2 weeks. We coded children whosemothers reported in the affirmative with a‘‘1’’ and all remaining children with a ‘‘0.’’
Independent Variables of InterestWe calculated our key independent variablesfrom the remotely sensed VCF data productmentioned earlier. The VCF contains propor-tional estimates for vegetative cover types; itshows how much of a land cover, such as‘‘forest’’ or ‘‘grassland,’’ exists on the landsurface.
The VCF product was averaged to 5 km andwas used to generate 2 independent variables:
1. Percentage of forest cover associated witheach DHS sampling cluster (0–9%, 10–19%,
20–29%, 30–39%, 40–49%, and 50–59% forestcover)
2. Another categorical variable reflectingchanges in forest cover over a decade (nochange, net forest loss, and net forest gain)for the sampled DHS cluster
The variable reflecting decadal change inforest cover leverages the longitudinal nature ofthe satellite remote sensing data. Adding thistemporal dimension to the analysis strengthenedour study considerably over using only a staticmeasure of forest cover taken at the time of thesurvey, allowing us to test, in effect, the relation-ship between forest change over time (loss orgain) and our outcomes of interest.
Control VariablesVariables controlled for in the analysis includechild’s age (grouped into 6-month categories),mother’s education (none, primary, secondary orhigher), urban or rural residence, householdwealth quintiles, number of years resident inthe current location, and a remotely sensedvegetation index (NDVI). The model for diarrheaincludes whether the household has access to asafer toilet facility and water source. Selection ofvariables was driven in part by data availability,given that we are analyzing secondary sourcedata.
The variable on mother’s education is a self-reported measure reflecting the mother’s highesteducation level achieved at the time of thesurvey. Respondents are asked to report the levelof highest achievement and the grade achievedwithin that level. Our analysis used a recodedcategorical variable that reflects attainment of:no education, primary education, and secondaryeducation or higher. Mother’s education isrelated to a child’s height-for-age20: motherswho are better-educated may be more knowl-edgeable about nutrition and optimal child carebehaviors, enabling them to improve healthoutcomes for their children.
Relative household wealth is measured usingan asset-based index: data on household assetownership collected during the DHS householdinterview are dichotomized (yes/no to indicateownership of each asset) and entered into astatistical procedure known as principal compo-nents analysis (PCA) that assigns a weight toeach asset. The asset values for each householdare then summed taking into consideration theweights, and a total household score is given. The
Forest cover, health, and nutrition in Malawi www.ghspjournal.org
Global Health: Science and Practice 2013 | Volume 1 | Number 2 6

household population is then divided intoquintiles on the basis of the score given to theirhousehold.21
The NDVI is a satellite remote sensingvariable that quantifies the concentrations ofgreen leaf vegetation on the ground, providing anintegrated estimate of vegetation health and ameans of monitoring changes in vegetation overtime. We used NDVI as a proxy control for thegrowing conditions of the area during thegrowing season immediately prior to adminis-tration of the DHS survey; it is the average NDVIfor December, January, and February prior toDHS implementation (June through November2010). When vegetation is brown because it isthe dry season, or because the climate isunusually dry, the NDVI is low. When theclimate is wet, and the grass, trees, and otherland cover is green, the NDVI is high. There is 1NDVI measurement associated with each DHSsampling cluster.
Statistical MethodsWe conducted multivariate analyses usingunweighted binomial logistic regressions toexamine the correlation between our indepen-dent variables of interest (forest cover or decadalchange in forest cover) and our selected dichot-omous outcome variables (severe stunting, diet-ary diversity, consumption of vitamin-A richfoods, and experience of diarrhea), while con-trolling for confounding factors for which datawere available. Logistic regression does notimpose restrictive normality assumptions onpredictors. The results are expressed in oddsratios that indicate the associations between theindependent and dependent variables withoutattributing causality.
Only the most recent birth for each motherinterviewed was included in the analysis to avoidintra-household correlations in the selected out-comes. The unweighted number of cases con-tributing to each analysis was as follows: dietarydiversity (n59,166), consumption of vitaminA-rich foods (n59,166), experience of diarrhea(n512,831), and stunting (n53,173).
RESULTS
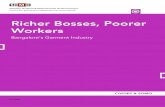
We found that children living in DHS clusterswith a net loss of forest cover over the pastdecade were 19% less likely to have a diverse dietand 29% less likely to consume vitamin A-richfoods than children living in clusters with no net
change in forest cover (Figure 2). These differ-ences were statistically significant.
Conversely, children living in communitieswith higher percentages of forest cover weremore likely to consume vitamin A-rich foods andless likely to experience diarrhea (Figure 3).Children living in clusters with a net gain inforest cover from 2000 to 2010 were 34% lesslikely to experience diarrhea (P5.002). Nostatistically significant associations were foundbetween the percentage of forest cover variableand child stunting, but there was a marginallystatistically significant association between netgain of forest cover and stunting (P5.058). Oddsratios are presented in the Table.
The health and nutrition outcomes we foundto be associated with variation in forest coverhave serious implications for children’s growthand development. Dietary diversity is often usedas an indicator of adequate dietary intake ofmicronutrients.22 Inadequate intake of vitamin Acan lead to deficiency, which is estimated toimpact 60% of young children in Malawi.23
Vitamin A deficiency is associated with poorvision and increased susceptibility to infectiousdiseases such as malaria and diarrhea, withconsequent mortality.23–24 Diarrhea in childrenin developing countries is a leading cause ofmortality; a recent study estimated that up to25% of deaths in young children in Africa can beattributable to the disease.25
DISCUSSION
Our results demonstrate an association betweenforest cover and selected nutrition-related out-comes. A study in 3 villages in southern Malawifound that, on average, almost two-thirds ofhouseholds sampled consumed wild fruit, vege-tables, and mushrooms from the forest, andalmost one-quarter consumed bushmeat tosupplement their diets.26 Nearly 70% of studyparticipants were dependent on wood collectedfrom forests for cooking.
The dependence of these rural populations onforest products is consistent with our findingthat dietary diversity and consumption of vita-min A-rich foods decrease with net decadal lossin forest cover. With respect to increased forestcover over time, we did not find a positiveassociation with dietary diversity and actuallyfound a marginally significant positive relation-ship with severe stunting. It is our understand-ing, based on expert observations from Malawi,
Children living inareas with a netloss of forest coverwere significantlyless likely to havea diverse dietand to consumevitamin-A richfoods thanchildren living inareas with no netchange in forestcover.
Forest cover, health, and nutrition in Malawi www.ghspjournal.org
Global Health: Science and Practice 2013 | Volume 1 | Number 2 7

that reforested areas tend to be plantations withmonocultures of non-native trees. Such areasmay not provide the same diversity of animal andvegetable nutrition as native forests.Additionally, access of local populations toreforested areas tends to be more restricted thanto native forests. Such reforested areas usuallyare privately held (for example, in the case of teaplantations) or strictly controlled by a villagecommittee or individual. In contrast, nativeforests are tightly regulated by law, but, inpractice, are heavily accessed and used.Reduction in access to NTFPs from such refor-ested areas could also lead to poorer nutritionaloutcomes for nearby communities. Furtherresearch is needed to support these hypotheses,however.
Our results also demonstrate an associationbetween forest cover and reduced child diarrhealdisease, supporting the hypothesis that forests
play an important provisioning role, specificallyin terms of water availability and/or quality, 2factors that impact diarrheal risk in developingcountries.27 Forests help to maintain healthywatersheds, prevent soil erosion, and filterimpurities from water, all of which positivelyimpact water availability and quality.28 Ourfinding that an increase in decadal forest coverreduces diarrhea risk suggests that tree planta-tions, which are the primary source of increasingforest cover in Malawi, may be as effective asolder forests with regard to this particular healthoutcome.
In 2008, the Maternal and ChildUndernutrition Study Group estimated that co-exposure of nutrition-related factors, such asvitamin A and iron deficiency, were togetherresponsible for about 35% of child deaths world-wide and for 11% of the total global diseaseburden.29 The authors noted that the evidence
FIGURE 2. Logistic Regression Results: Net Loss of Forest Cover Reduces the Odds That a ChildWill Consume Vitamin A-Rich Foods and Have a Diverse Diet
1.00
0.81
0.71
0.00
0.20
0.40
0.60
0.80
1.00
1.20
No net change in forest cover
(reference)
Net loss in forest cover:
Odds of consuming vitamin A-rich foods
(P<.05)
Net loss in forest cover:
Odds of consuming a diverse diet
(P<.05)
Odd
s Ra
�o
Forest cover issignificantlyassociated withreduced childdiarrheal disease.
Forest cover, health, and nutrition in Malawi www.ghspjournal.org
Global Health: Science and Practice 2013 | Volume 1 | Number 2 8

makes a compelling case for the urgent imple-mentation of interventions to reduce the variousforms of undernutrition or to ameliorate theirconsequences.
Our results provide preliminary evidencesuggesting that an equitable, sustainable, andeffective way to improve child nutrition—andhence, survival—outcomes could include ensur-ing the integrity of natural ecosystems. Such anintegrated approach would result in ecosystemsthat are healthy enough to deliver the servicesthat local communities depend on, includingfoods with high nutrient bioavailability andclean water, which is essential in preventingdiarrheal disease.
Given the limitations of the currently avail-able data, it was possible to demonstrate onlyassociations, not causal relationships, in thisanalysis. To establish the causal pathways andmechanisms responsible for the demonstrated
associations between forest cover and childhealth and nutrition outcomes in Malawi,further research is needed, involving collectionof accurately geo-referenced, longitudinal popu-lation and health data and women’s timeallocation data, as well as concomitant collectionand testing of water samples for quality and useof newly available 30 meter remote sensing data.
Acknowledgments: This research was primarily supported by theForestry and Biodiversity Office, Bureau for Economic Growth,Education and the Environment (E3 Bureau), at the United StatesAgency for International Development (USAID), with additionalsupport provided by the Famine Early Warning System Network(FEWS NET) program at USAID’s Office of Food for Peace. We wouldlike to thank USAID’s Global Health Bureau for their assistance withthis project. The views expressed in this article are the authors’ onlyand do not necessarily represent those of the United States Agency forInternational Development or the U.S. Government. We are indebtedto Mark Carroll for preparing the forest cover and deforestation datafor this analysis. This paper has benefited from discussions withMonica Kothari on the use of the minimum dietary diversity indicator.We thank Richard Mantovani for his review of a prior draft of ourmanuscript. We are grateful to the USAID Biodiversity team and allUSAID staff who generously shared their insights and expertise,
FIGURE 3. Logistic Regression Results: Greater Forest Cover Increases the Odds That a ChildWill Consume Vitamin A-Rich Foods and Decreases the Odds That the Child Will ExperienceDiarrhea
* P,.05 (statistically significant).
Protecting naturalecosystems couldbe a sustainableand effective wayto improve childnutrition andhealth.
Forest cover, health, and nutrition in Malawi www.ghspjournal.org
Global Health: Science and Practice 2013 | Volume 1 | Number 2 9

TABLE.
LogisticRe
gression
Results:AdjustedOdd
sRa
tiosforChild
Hea
lthan
dNutritio
nOutcomes
AssociatedW
ithFo
restCover,Malaw
i2010
Forest
cover-related
indep
enden
tva
riables
Severe
Stun
tinga
Dietary
Diversity
bVita
min
A-RichFo
odsb
Diarrhe
ab
Mod
el1
Mod
el2
Mod
el1
Mod
el2
Mod
el1
Mod
el2
Mod
el1
Mod
el2
PValue
OR
PValue
OR
PValue
OR
PValue
OR
PValue
OR
PValue
OR
PValue
OR
PValue
OR
Deforestatio
n,2000–2
010
(ref:n
ochang
e)
.16
.14
––
.002
––
.003
––
Net
loss
offorestcover
.64
1.113
––
.049
.813
––
.003
.708
––
.06
.822
––
Net
gain
offorestcover
.058
1.647
––
.56
.930
––
.16
1.201
––
.002
.658
––
Forest
cover
(ref:0–9
%)
.47
––
.13
––
.01
––
,.001
10–1
9%
––
.58
1.080
––
.52
.961
––
.13
1.106
––
.008
.854
20–2
9%
––
.25
1.283
––
.08
1.188
––
.006
1.328
––
.003
.748
30–3
9%
––
.14
1.665
––
.34
1.177
––
.03
1.459
––
,.001
.487
40–4
9%
––
.58
.700
––
.75
.908
––
.15
1.562
––
.008
.358
50–5
9%
––
––
––
.08
1.736
––
.02
2.046
––
,.001
.079
Abb
reviations:OR,
Odd
sRa
tio.
Pvalues
#.05wereco
nsidered
statisticallysign
ifica
nt.
aCon
trolsinclud
edchild’sag
e,previous
birth
interval,mother’s
education,
urba
nreside
nce,
householdwea
lth,migrationstatus,an
dNormalized
Difference
Vege
tationInde
x(N
DVI).
bCon
trolsinclud
edchild’sag
e,mother’s
education,
urba
nreside
nce,
householdwea
lth,migrationstatus,an
dNDVI.
Forest cover, health, and nutrition in Malawi www.ghspjournal.org
Global Health: Science and Practice 2013 | Volume 1 | Number 2 10

including Brent McCusker, Richard Volk, Sharon Murray, MaryRowen, Cynthia Gill, Diane Adams, and Rochelle Rainey. Finally, wethank the reviewers for their insightful comments, and the editors ofGlobal Health: Science and Practice for their generous contributionsof time and expertise.
Competing Interests: None declared.
REFERENCES1. Aerts R, Honnay O. Forest restoration, biodiversity and
ecosystem functioning. BMC Ecol. 2011;11:29. CrossRef.Medline
2. Food and Agriculture Organization (FAO), United Nations.Global forests resources assessment 2010: main report. Rome:FAO; 2010. Available from: http://www.fao.org/docrep/013/i1757e/i1757e.pdf
3. Butchart SH, Walpole M, Collen B, van Strien A, ScharlemannJP, Almond RE, et al. Global biodiversity: indicators of recentdeclines. Science. 2010;328(5982):1164–1168. CrossRef.Medline
4. Millennium Ecosystem Assessment. Living beyond our means:natural assets and human well-being (statement from the board).United Nations Environment Programme; 2005. Available from:http://www.unep.org/maweb/en/boardstatement.aspx
5. Palmer C, Di Falco SD. Biodiversity, poverty, and development.Oxf Rev Econ Policy. 2012;28(1):48–68. CrossRef
6. Kumar SK, Hotchkiss D. Consequences of deforestation forwomen’s time allocation, agricultural production, and nutrition inhill areas of Nepal. Washington, DC: International Food PolicyResearch Institute; 1988. Available from: http://www.ifpri.org/sites/default/files/publications/rr69.pdf
7. Golden CD, Fernald LCH, Brashares JS, Rasolofoniaina BJ,Kremen C. Benefits of wildlife consumption to child nutrition in abiodiversity hotspot. Proc Natl Acad Sci USA.2011;108(49):19653–19656. CrossRef. Medline
8. Olson SH, Gangnon R, Silveira GA, Patz JA. Deforestation andmalaria in Mancio Lima County, Brazil. Emerg Infect Dis.2010;16(7):1108–1115. CrossRef. Medline
9. Fa JE, Currie D, Meeuwig J. Bushmeat and food security in theCongo Basin: linkages between wildlife and people’s future.Environ Conserv. 2003;30(1):71–78. CrossRef
10. Ahenkan A, Boon E. Improving nutrition and health through non-timber forest products in Ghana. J Health Popul Nutr.2011;29(2):141–148. CrossRef. Medline
11. Fisher M, Chaudhury M, McCusker B. Do forests help ruralhouseholds adapt to climate variability? Evidence from southernMalawi. World Dev. 2010;38(9):1241–1250. CrossRef.
12. Spector S, Nichols E, Gomez A. Dysfunctional hotspots? Pan-tropical changes in dung beetle communities and decliningecosystem functions. Presented at: Annual Meeting of theInternational Congress for Conservation Biology; 2008 Jul 10;Chattanooga, TN.
13. Pattanayak SK,Wendland KJ. Nature’s care: diarrhea, watershedprotection, and biodiversity conservation in Flores, Indonesia.Biodivers Conserv. 2007;16(10):2801–2819. CrossRef
14. Berry N, Utila H, Clunas C, Viergever K, Tipper R. Avoidingunplanned mosaic degradation and deforestation in Malawi.Blantyre, Malawi: Plan Vivo; 2009.
15. United Nations (UN), Department of Economic and SocialAffairs, Population Division. World urbanization prospects, the2011 revision. Country profile: Malawi. New York: UN; 2011.Available from: http://esa.un.org/unup/Country-Profiles/country-profiles_1.htm
16. National Statistical Office (NSO); ICF Macro. MalawiDemographic and Health Survey 2010. Zomba, Malawi, andCalverton, MD: NSO and ICF Macro; 2011. Available from:http://www.measuredhs.com/pubs/pdf/FR247/FR247.pdf
17. Hansen MC, DeFries RS, Townshend JRG, Carroll M, Dimiceli C,Sohlberg RA. Global percent tree cover at a spatial resolution of500 meters: first results of the MODIS Vegetation ContinuousFields algorithm. Earth Interact. 2003;7(10):1–15. CrossRef
18. Justice CO, Vermote E, Townshend JRG, DeFries R, Roy DP, HallDK, et al. The Moderate Resolution Imaging Spectroradiometer(MODIS): land remote sensing for global change research. IEEETrans Geosci Rem Sens. 1998;36(4):1228–1249. CrossRef.
19. World Health Organization (WHO). Indicators for assessinginfant and young child feeding practices: part 2 measurement.Geneva: WHO; 2010. Available from: http://whqlibdoc.who.int/publications/2010/9789241599290_eng.pdf
20. Rutstein SO. Factors influencing the nutritional status of mothersand children in sub-Saharan Africa: an analytical report basedon the Demographic and Health Surveys. Calverton, MD: MacroInternational Inc.; 1996.
21. Rutstein SO, Johnson K. The DHS wealth index. Calverton, MD:ORC Macro; 2004. DHS Comparative Reports No. 6. Availablefrom: http://www.measuredhs.com/pubs/pdf/CR6/CR6.pdf
22. Steyn NP, Nel JH, Nantel G, Kennedy G, Labadarios D. Foodvariety and dietary diversity scores in children: are they goodindicators of dietary adequacy? Public Health Nutr.2006;9(5):644–650. CrossRef. Medline
23. SanJoaquin MA, Molyneux ME. Malaria and vitamin Adeficiency in African children: a vicious circle? Malar J.2009;8:134. CrossRef. Medline
24. Maziya-Dixon BB, Akinyele IO, Sanusi RA, Oguntona TE, NokoeSK, Harris EW. Vitamin A deficiency is prevalent in children lessthan 5 y of age in Nigeria. J Nutr. 2006;136(8):2255–2261.Medline.
25. Walker CL, AryeeMJ, Boschi-Pinto C, Black RE. Estimating diarrheamortality among young children in low and middle incomecountries. PLoS One. 2012;7(1):e29151. CrossRef. Medline
26. Fisher M, Shively G. Can income programs reduce tropical forestpressure? Income shocks and forest use in Malawi. World Dev.2005;33(7):1115–1128. CrossRef.
27. Moe CL, Rheingans R. Global challenges in water, sanitation andhealth. J Water Health. 2006;4 Suppl 1:41–57. Medline
28. Hamilton LS. Forests and water: a thematic study prepared in theframework of the Global Forest Resources Assessment 2005.Rome: Food and Agricultural Organization, United Nations;2008. Available from: http://www.fao.org/docrep/011/i0410e/i0410e00.htm
29. Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis M, Ezzati M,et al; Maternal and Child Undernutrition Study Group. Maternaland child undernutrition: global and regional exposures andhealth consequences. Lancet. 2008;371(9608):243–260.CrossRef. Medline
Forest cover, health, and nutrition in Malawi www.ghspjournal.org
Global Health: Science and Practice 2013 | Volume 1 | Number 2 11

______________________________________________________________________Peer Reviewed
Received: 2013 Apr 28; Accepted: 2013 Jul 5; First Published Online: 2013 XX XX
Cite this article as: Johnson KB, Jacob A, Brown ME. Forest cover associated with improved child health and nutrition: evidence from the MalawiDemographic and Health Survey and satellite data. Glob Health Sci Pract. 2013;1(2):1-12. http://dx.doi.org/10.9745/GHSP-D-13-00055.
� Johnson et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricteduse, distribution, and reproduction in any medium, provided the original author and source are properly cited. To view a copy of the license, visithttp://creativecommons.org/licenses/by/3.0/______________________________________________________________________
Forest cover, health, and nutrition in Malawi www.ghspjournal.org
Global Health: Science and Practice 2013 | Volume 1 | Number 2 12