for people with Neuropathic Pain - Squarespace · Traumatic spinal cord injury 8. Multiple...
24
1 © 2006 Angela Mailis-Gagnon, MD, MSc, FRCPC (Physical Medicine) Comprehensive Pain Program, Toronto Western Hospital, ON Canada Endorsed by the following organizations: for people with Neuropathic Pain and The Canadian Pain Coalition
Transcript of for people with Neuropathic Pain - Squarespace · Traumatic spinal cord injury 8. Multiple...

1
© 2006 Angela Mailis-Gagnon, MD, MSc, FRCPC (Physical Medicine)Comprehensive Pain Program, Toronto Western Hospital, ON Canada
Endorsed by the following organizations:
for people with Neuropathic Pain
and
The Canadian Pain Coalition

1
Non Medical Version

During the past 23 years that I have practiced exclusively in the area of chronic pain management, neuropathic pain has puzzled, confused and often frustrated me as it is more difficult to treat than musculoskeletal pain. Over the years, I have seen thousands of patients with common and rare diseases and injuries of the peripheral and central nervous system. The Atlas of Neuropathic Pain Syndromes is an effort to disseminate some basic information about neuropathic pain syndromes in a handy pocket size illustrated reference. While there is a version suitable for physicians and other health professionals, the booklet you have in your hands tries to convey the same information in a simple language that can be understood by patients, their families and the public in general. Given the success of the first edition (2005), I have been able to add more neurological syndromes in 2006, making this version complete.
My first step was to team up with a group of talented 3D artists (Norm Gagnon and Martin Mayer) who have spent many many hours creating images of what my patients experience and what I find on neurological examination. Case histories are summaries of true patient cases. To preserve patient confidentiality simulated patients and computer altered or generated images have been used. For each topic I used information from recent scientific literature (details of which can be found in the medical version).
This project would not have been possible without the generous support of Pfizer, Merck Frosst and Bayer, while the Canadian Pain Society and the University of Toronto Centre for the Study of Pain have endorsed the booklet in terms of its scientific content.
Angela Mailis-Gagnon, MD, MSc, FRCPC(Physical Medicine)Director, Comprehensive Pain Program, Senior Investigator, Krembil Neuroscience CentreToronto Western Hospital, University Health Network, Professor, Dept. of Medicine, University of Toronto Centre for the Study of Pain, Ontario, Canada
January 2006
FOREWORD
1

2
1. Foreword
2. Table of contents
3. Glossary
4. The circuits of pain
5. Introduction
6. Central post-stroke pain
7. Traumatic spinal cord injury
8. Multiple sclerosis
9. Syringomyelia
10. Failed back surgery syndrome
11. Traumatic brachial plexus injury
12. Post amputation pain
13. Diabetic neuropathy
14. Complex Regional Pain Syndrome type I (CRPS I)
15. Self-induced CRPS (like) disorders
16. Traumatic and compressive nerve injuries
17. Nerve tumours
18. Trigeminal neuralgia
19. Post herpetic neuralgia
20. Pain after breast surgery
21. Chest pain after cardiac bypass surgery
22. References/ Abbreviations
TABLE OF CONTENTS

Pain: The International Association for the Study of Pain (IASP) accepts the following definition (paraphrased): Pain is an unpleasant sensory and emotional experience which occurs in the presence of actual or potential damage to our bodies or described in terms of such damage (in the absence of tissue injury). The definition acknowledges three im-portant concepts: 1) pain is always subjective defined by the person who experiences it; 2) pain is unpleasant, so the definition includes how a person feels, and 3) in this defin-ition pain is NOT tied to a specific stimulus.
Neuropathic pain is pain initiated or caused by a primary injury or dysfunction in the peripheral or central nervous system (consisting of our nerves or the spinal cord and brain respectively). Neuropathic pain is “pathological or abnormal pain” in contrast to Nociceptive pain, which is the result of activation of nociceptors, i.e., our pain receptors in muscles, bones, ligaments, the gut, the heart etc. Nociceptive pain is “normal pain” in the sense that it is the pain we feel normally when the nervous system is intact.Allodynia: A medical term meaning pain evoked by a stimulus that does not normally cause pain, for example pain upon touch.Hyperalgesia: The term means unusually intense pain to a stimulus which is normally painful (for example pin prick).Hyperesthesia: Increased sensitivity to stimulation (it is a more general term and in-cludes both allodynia and hyperalgesia). Hypoesthesia or anesthesia means decreased sensation and complete lack of sensation respectively.Paresthesia: An abnormal sensation which occurs on its own (spontaneous) or is gener-ated by touch, prick or pressure, but is not unpleasant. It contrasts to the term Dyses-thesia, which means that this abnormal sensation is unpleasant.Deafferentation pain is a term often used to indicate pain felt in a body part lacking sensation (as in brachial plexus injury, spinal cord injury etc).
GLOSSARY
3

4
THE CIRCUITS OF PAIN
Cerebral cortex
VPLthalamus
Pons
Medulla
Mid brain(Cerebral peduncles)
The diagram shows neural tracts that pass through several levels of the spinal cord to the cor-tex (outer shell of the brain). The inserts show details of a spinal cord segment (bottom left) and the trigeminal nerve with its 3 branches innervating the face (top right). These pathways are the “posterior or dorsal funiculus” responsible for fine touch sensations and perception of move-ment, and the “anterolateral or ventral funiculus” for pain, temperature, gross touch and deep pressure. The ventral funiculus consists of the lateral (red) and anterior (blue) spinothalamic tract which end at a specialized thalamic structure called VPL and finally to the cortex allowing the person to understand the body part from where a stimulus comes. Another pathway (not shown) is involved in attaching emotions and colouring to our pain perception. Furthermore, many other influences from the cortex to the spinal cord change the original stimulus at many levels.
Trigeminalganglion
Trigeminal innervation
Cervicalspinal cord
Lateral spinothalamic tract
Anterior (ventral) spinothalamic tract
Posterior funiculus(dorsal columns)
Dorsal (spinal) root ganglion
Proprioception, position sense
Touch,pressure,vibration
Pain, temperature

Neuropathic pain occurs in some but not all people with injury or dysfunction of the peripheral or central nervous system. It is poorly understood by doctors, patients and the public in general. In case of injury to nervous tissue, all parts of the nervous system may undergo changes within milliseconds which may last indefinitely. Specifically, when peripheral nerves get injured, they may fire abnormally generating “ectopic impulses” at the site of injury and becoming supersensitive to multiple neurochemicals. This phe-nomenon is called “peripheral nociceptor sensitization”. Similarly the spinal cord and the brain undergo changes after damage to the peripheral nerves or after spinal cord injury or stroke (“central sensitization”). Some of these abnormalities include pain seemingly com-ing from body areas larger than the original injury site or generated by stimuli that are nor-mally painless, for example pain on mere touch. Our understanding of neuropathic pain has dramatically increased over the past few years with the invention of neuroimaging, an ingenious way to visualize brain activity in awake people. It is used exclusively for research and has shown many changes in brain activation patterns, even when our every-day tests fail to show abnormalities. Typical neuropathic symptoms include pain (burning, shooting, stabbing, shock-like etc), occurring spontaneously or generated by touch, pin prick, pressure or movement; paresthesiae and dysesthesiae, numbness, pins and needles sensations and motor dys-function (weakness, difficulty starting or performing movements etc). Neuropathic signs may include abnormal sensations, weakness, atrophy, changes in colour, temperature or sweating patterns and flickering of the muscles, stiffness or bizarre posturing. Many treatments exist, but they do not work in all people. Drugs over the counter are not very useful, while those prescribed by doctors include TCAs (amitriptyline, desip-ramine etc); antiepileptics (carbamazepine, valproic acid, gabapentin, pregabalin etc); local anesthetic type of drugs (e.g. mexiletine); anti-inflammatory drugs (usually not very effective), opioids (morphine and similar drugs), and a recently approved buccal spray derived from marijuana. Non drug treatments are nerve, root and spinal cord blocks; lo-cal heat, cold or TENS, acupuncture and exercises; and finally surgery (spinal stimulators or implanted pumps and sometimes procedures like cutting or burning nerves). Chronic pain takes its toll on a patient’s emotional and mental state, creating depression, sleep problems, isolation, loss of work and pride and problems with loved ones. The best way to treat chronic pain in general is a “whole person” approach and may require combina-tion of medical and non medical treatments (like counseling, relaxation and cognitive/be-havioural techniques).
INTRODUCTION
5

6
58 year old man with a stroke in the right side of the brain and complaints of left sided burning dysesthetic pain appearing within two weeks after the stroke. Notice hypersensi-tivity to touch and pin prick across the left face, arm and torso.
In one study CPSP developed in 8% of stroke victims. Burning was the commonest de-scriptor of pain, while most patients had more than one kind of pain (continuous pain, sudden spells of pain and pains when touched or moved). The pain was rated moderate to severe at least in 50% of the stroke victims. It appears immediately after stroke in more than 1/3 of patients, days to 12 months later in half of the patients, 2 years in 9.5% and more than 2 yrs in 4.5%. The motor and sensory abnormalities in CPSP are variable. Examples of sensory abnormalities are hypoesthesia, hyperesthesia, paresthesiae or dysesthesiae. CPSP seems to arise from brain lesions that damage the connections that carry messages from the spine to the brain (spino-thalamo-cortical pathways). Traditional neuropathic pharmacotherapy and opioids as well as deep brain stimulators in the most severe cases have limited success. Usually the patients require more than one drug in order to obtain some relief.
CENTRAL POST-STROKE PAIN
Allodynia Hyperalgesia

Allodynia Hyperalgesia Hypoesthesia Hypoalgesia
7
TRAUMATIC SPINAL CORD INJURY (TSCI)
63 year old man with fractures of the spine and complete paralysis after a car accident. Ayear after the injury he developed hypersensitivity at the level of the broken back bonesand can not even bear his shirt in contact with his skin. Below the hypersensitive zone hehas dense anesthesia and paralysis, while he still complains of burning leg pains.According to many studies, pain occurs in 40-75% of people with TSCI. It is moderate tosevere, often associated with depression and/or anxiety and impairs function and enjoymentof life. Pain after TSCI can be a) neuropathic occurring at the level of the injury (oftendue to damage of the nerve roots at the site of trauma as in the case above) or below thelevel of the injury (called central or deafferentation pain); b) musculoskeletal pain above orbelow the injury level and c) visceral pain (from the bladder or the bowels). Neuropathicpain can also occur as a consequence of TSCI (for example due to development of a syrinxor cavity within the spinal cord). A recent literature review showed that there is limitedor no success with different pharmacological and other treatments. In practice, traditionalneuropathic drugs, opioid analgesics, physical modalities, acupuncture, relaxation techniquesand rarely surgery are tried, but with limited success.

8
MULTIPLE SCLEROSIS
The diagram shows acute (in yellow) and subacute/chronic (in white) pain syndromes in MS.
MS is a disease that attacks the brain and spinal cord by causing inflammation and dam-age to the protective myelin covering of the CNS. In recent studies up to 65% of MS patients have been reported to have pain (usually in more than one site). The pain is a) directly related to the disease, b) may arise from musculoskeletal reasons (painful muscle contractures, stiff joints, back pain etc) or c) originate from MS treatments (steroids and interferon). The commonest chronic pain syndrome seems to be dysesthetic leg pains, while common acute pain conditions are neuralgias, optic neuritis and brief painful tonic spasms. Pain management in MS is complex as the doctor must take in account multiple symptoms (bladder problems, spasticity, depression, fatigue etc) and many medications the patient takes at the same time. Certain rehabilitation approaches may be helpful (to correct body mechanics or for reconditioning). Medications for pain have variable and often limited effects (NSAIDS and acetaminophen, antispasticity drugs, anticonvulsants, antidepressants, opioids and oral cannabinoids). A buccal spray containing extracts of natural cannabis has been recently approved by Health Canada to assist in the treatment of neuropathic pain in MS. However, more studies are needed to confirm the clinical benefits that some early research has shown.
Tic like or burning extremity pains
Painful tonic seizures
Steroid orimmunosuppressant
induced complications (osteoporosis, vertebral fractures, hemorrhagic
cystitis)
Lhermitte`s sign
Optic neuritis
Painful leg spasms
Dysestethic continu-ous burning extremity pain
Visceral pains
Back pain
Painful compressive neuropaties
Trigeminal Neuralgia
Headaches

9
A1: Chiari malformation associated with a cervical cord syrinx. Pain affects both flanks while hypoesthesia involves the whole right hemibody; A2: Multiple small cavities in arachnoiditis affecting members of one family with complete paralysis below the waist. Pain affects the arms while the hypoesthesia is confined below the level of paralysis.
Syringomyelia (cavitations within the spinal cord) is rare. It may be “communicating” (as-sociated with “Chiari malformation”) or “non-communicating” (running in families, after spinal cord trauma, spinal tumour etc). A survey of the Canadian Syringomyelia Network participants during their 1996 convention found that 97.5% of the responders had pain. In a recent study pain was the only symptom at the beginning of syringomyelia in 59% of the patients and the primary cause of disability in 69% of the sufferers. Most patients had more than one type of pain involving multiple body areas. Pain was rated as moder-ate in 70% of the patients and severe in 11%. Interestingly, the sensory abnormalities with hypoesthesia to touch, pin prick and cold were covering large areas of the body and only partially matched the areas of pain. While a surgical procedure called shunting of the syrinx may improve balance and bladder problems, it usually does not improve pain. Traditional neuropathic pharmacotherapy and opioids have variable success.
SYRINGOMYELIA
A1 A2
Pain Hypoalgesia

10
42 year old with persistent back and left leg pain, both worse after spinal surgery. Notice sensory hypoesthesia in the distribution of L5 and S1 roots, while the left ankle jerk is absent.
The term FBSS refers to patients who have persistent pain and disability after spinal surgery. Despite the high cost and frequency of surgery, the results are poor in 10 to 40% of patients. There are many reasons for failure. Psychological factors include cer-tain personality characteristics and faulty coping mechanisms, anxiety or depression etc. Factors relating to the surgery itself are failure to completely remove the disc or other pathology, excessive surgery, damage already done by a big disc, root injury during surgery and (most common of all) operating on a patient who has nothing that warrants surgery. After the surgery, recurrent disc herniation or “epidural fibrosis” known as scar tissue could be sources of continuous pain. Epidural scar forms 6 weeks to 6 months postoperatively in 10-75% of the patients, but the vast majority do NOT have symptoms. Epidural steroid injections are widely performed, but their value is questionable. Drugs include NSAIDs, antidepressants, anticonvulsants and opioids. Spinal stimulators and intrathecal opioid pumps may be used in patients resistant to conventional therapy. Ther-apy should not focus only on medical/surgical management as chronic pain management programs seem to be more effective.
FAILED BACK SURGERY SYNDROME (FBSS)
Hypoesthesia
Hypoalgesia
L5
S1

TRAUMATIC BRACHIAL PLEXUS INJURY
30 year old man with detachment of left C7, 8 and T1 roots of the brachial plexus (which innervates the shoulder, arm and hand) after an MVA with complaints of constant burn-ing and paroxysmal shooting hand pain. The left forearm/ hand has no feeling at all to touch, pinch or pressure, while the hand is weak and wasted with profound coldness and profuse sweating.
More than 80% of patients with avulsion of one or more brachial plexus roots suffer from serious constant, burning or crushing pain often coming in very brief spells (paroxysms) of agonizing intensity and lasting for seconds. Most patients are young men involved in traumatic accidents. Extremes of temperature and emotional stress aggravate the pain, while it is relieved by distraction (when the patient’s attention is switched to other things than pain). Two thirds of the patients seem to experience some improvement within 3 years, while in the remaining 1/3 the pain may steadily get worse with age. Treatments like traditional neuropathic medications (TCAs and antiepileptics), opioids, supportive therapy etc. provide limited relief or no relief at all. The two most helpful interventions at the opposite ends of the technological and medical spectrum include distraction tech-niques (for example imagery) and DREZ lesions of the avulsed roots (a surgical procedure performed by neurosurgeons).
11

12
44 year old man with traumatic amputation below the elbow. Artistic interpretation of his complaints of shock-like, burning and squeezing pain in the missing “ghost” limp, while he feels his fingers rigidly twisted.
The feeling of a missing limb can be painless (phantom sensation) or painful (phantom pain). Phantom limb pain can follow amputation of any body part including limb, breast, tooth or rectum and occurs within the first week after amputation at least in 50-75% of the patients, but also any time after it. Several PNS and CNS abnormalities may account for phantom limp pain. Recent neuroimaging studies show changes in activity, size and location of brain tructures appearing within hours from the loss of the body part. Unfortu-nately, the existing studies in the literature do not tell the difference between phantom pain and stump pain (the latter more often caused by focal neuroma, a form of sensitive knot at the site of the cut nerves). Pain is described as squeezing, burning, shooting or aching, often associated with abnormal movements/posture of the phantom. Treatments are numerous with generally poor results, including non surgical therapies (TENS, acu-puncture, relaxation techniques, neuropathic medications and opioids), while surgical techniques include stump revision with neuroma implantation within deep tissues, DREZ surgery and spinal cord or brain stimulation.
POST AMPUTATION PAIN

13
Hypoesthesia Hypoalgesia
DIABETIC NEUROPATHY
65 year old woman with 4 year history of poorly controlled diabetes and 2 year history of painful foot numbness (the boot-like distribution of the sensory deficit is marked only in the right foot while the abnormalities are bilateral).
Diabetic polyneuropathy affects primarily the nerves of feet and hands in both insulin and non-insulin dependent diabetes. Single nerves can also be affected either due to lack of blood supply (ischemic mononeuropathy) or because they become vulnerable to compression (an example is a pinched nerve in the wrist that causes carpal tunnel syndrome). The commonest forms of painful neuropathy are ischemic mononeuropathy and distal polyneuropathy. In the latter, patients may experience gradual onset of aching, burning and/or shooting pain, numbness and dysesthesiae in their feet and feel out of balance. While proper sugar control can slow the progression of polyneuropathy, it may do little to control pain. Antiepileptics (particularly gabapentin and pregabalin) and less so TCAs have been shown to work in many people. Opioids may be used as adjuncts in certain cases. A cream containing capsaicin, the ingredient of hot chilli peppers, has been reported in some studies to offer relief but many patients find it intolerable due to the burning it produces. Proper foot care and regular activity are a must.

14
COMPLEX REGIONAL PAIN SYNDROME I (CRPS I)(also known as Reflex Sympathetic Dystrophy/RSD)
A1 A2
A1: 45 year old woman with right leg CRPS after heel injury. Notice the brownish discolor-ation of dead skin, as she has not washed the leg for a year due to severe allodynia; A2: 36 year old man with cold, sweaty, swollen and allodynic foot after a fracture of a small foot bone. Both cases were resistant to all treatments.
As the 1994 IASP criteria proved to diagnose CRPS in a lot more people than they should, the most recently proposed clinical criteria are: • Continuingpainoutofproportiontoanytraumaticevent. • At least reporting by the patient of one symptom in 3 of the 4 following categories and observation by the health practitioner of one sign in 2 or more of the follow- ing: 1) abnormal sensation (hyperesthesia and/or allodynia); 2) temperature and/ or colour changes or asymmetry; 3) sweating and/or edema abnormalities, and 4) decreased range of movement and/or motor dysfunction and/or trophic changes. • Nootherdiagnosisbetterexplainsthesignsandsymptoms.
The cornerstone of treatment is physiotherapy with mobilization. Sympathetic blocks may help, but the role of SNS has been downplayed as large numbers of patients respond to sham blocks. Traditional neuropathic pharmacotherapy, opioids and spinal stimulators may be of help, while sympathectomy is not advocated due to multiple complications.

37 year old woman with documented knee CRPS. Once she became depressed after a dispute with her insurance, she developed symmetrical wounds exud-ing puss (C) in the anterior leg that failed to respond to dressing changes and surgery, but healed when she was told that the doctors believed she was creating the wounds herself.
In one pain clinic, self inflicted lesions were found in 5-8% of all CRPS referrals. One should suspect self-injury in the case of a) bizarre, migrating, symmetrical or well demarcated lesions, b) ligature sign, c) a woman who is emotionally distraught or displays bizarre indif-ference to her problem, and d) lesions healing when the patient is placed in a cast or confronted. Such wounds may be occasionally superimposed on underlying nerve injury or even CRPS.
21 year old woman diagnosed with CRPS. See grotesque swell-ing of the hand (A1) and “ligature marks” after tying the elbow with a tight bandage (A2). The hand normalized once the bandage was re-moved.
SELF INDUCED (“CRPS” like) DISORDERS
31 year old woman diag-nosed as CRPS after surgery. When the pain doctor noticed purplish lines on her pants (B1), she wiped unexpect-edly the patient’s purple forearm (B2) with a wet cloth. The patient admit-ted to using dark make up to colour the limb.
A1 A2
B1 B2
C
15

16
43 year old man with radial nerve injury after a deep laceration in the forearm. He com-plains of spontaneous burning and paroxysmal electric shock-like pains while he has areas of increased or decreased sensitivity across the forearm and hand.
When a nerve is cut, the surgeons must work quickly to reattach it. When, however, the nerve is injured but not transected, it usually recovers on its own and surgeons will wait for 2-3 months. Common chronic neuropathies due to trauma or compression in the up-per extremities, are carpal tunnel at the wrist and ulnar nerve entrapment at the elbow; in the chest wall, intercostobrachial nerve injury after breast surgery (see page 16) and inter-costal nerve damage after cardiac bypass surgery (see page 17); in the abdominal wall, genitofemoral and ilioinguinal nerve damage; in the perineum, pudendal neuropathy; and in the lower extremities, lateral femoral cutaneous nerve of the thigh entrapment (meral-gia paresthetica), sciatic nerve injury (e.g. after hip fractures), tibial nerve compression in the inside part of the ankle, peroneal nerve injury just below the outside of the knee, sural nerve compression behind the knee, or entrapment of small nerves in between the toes (Morton’s neuroma). Treatment includes neuropathic medications, opioids, spinal or peripheral nerve stimulation and occasionally surgery (neurectomy, neuroma implanta-tion within deep tissues etc).
TRAUMATIC AND COMPRESSIVE NERVE INJURIES

17
NERVE TUMOURS49 year old woman with a 9 year history of intermittent sharp stabbing and elec-tric shock-like pain across the right calf, aggravated by walking. She failed to re-spond to traditional neuro-pathic treatments and opioid analgesics. MRI of the leg showed a spindle-shaped tumour attached to the pos-terior tibial nerve. During surgery a benign tumour was removed completely from the nerve (a and b), with disappearance of her symp-toms.
Peripheral nerve tumours are rare. Benign tumours arising spontaneously from the cov-er of a nerve (nerve sheath) are usually schwannomas and neurofibromas. Other types of nerve tumours are neuromas created by trauma (traumatic neuromas) by c o m p r e s s i o n _ ( M o r t o n ’ s neuroma in between the toes often due to tight shoes). Schwannomas involve most frequently the nerve respon-sible for our hearing (acous-tic neuroma), and surgery to remove such a tumour may produce damage to the pa-tient’s hearing. Neurofibro-mas can occur as isolated nerve tumours or be part of neurofibromatosis, a gen-etic disease, which occurs in 1/3,000 births. Patients with neurofibromatosis may have variable presentation: a few pigmented skin spots of no clinical significance or a devastating disease with multiple tumours in many or-gans which tend to turn into cancer.
A
B

18
42 year old man with one year history of paroxysmal agonizing electric shock-like pains in the distribution of the 2nd branch of the trigeminal nerve in the cheek, triggered by light touch, chewing or an air draft.
Most cases of trigeminal neuralgia (TN) or tic douloureux are of unknown origin. Oc-casionally, however, TN occurs in multiple sclerosis (MS) or facial trauma. Roughly TN affects 5.7 women and 2.5 men in 100,000 people every year in the USA. TN occurs in spells in the trigeminal nerve territory (one side of the forehead, cheek or jaw) in about 95% of the cases. Pain in both sides of the face may occur years later, particularly in patients with MS. The paroxysms come in clusters and last minutes or seconds followed by brief pain free periods and occur rarely at night. Touch, shaving, washing, air drafts, chewing etc. can generate outbursts of pain. 50% of patients identify a trigger zone and occasionally complain that their nose drips or their eye tears. Neurological examination is normal but sophisticated testing may show minor sensory loss. The patients may be free of pain days to months or years. Carbamazepine (an antiepileptic) seems to be the first line treatment. In case of failure or intolerant side effects, newer antiepileptics (e.g. gabapentin or others) may be helpful. Compression of the trigeminal nerve inside the brain by abnormal arteries or veins can be relieved surgically.
TRIGEMINAL NEURALGIA

19
POST HERPETIC NEURALGIA (PHN)
66 year old man with persistent burning and itching pain a year after “shingles”. The discoloured areas of the skin are insensitive alternating with areas of hypersensitivity to touch and pin prick.
PHN is the most frequent debilitating complication of Herpes Zoster or shingles (after reactivation of the dormant VZV virus in the sensory ganglia). In 36.6% of patients older than 60 years and 47.5% of those older than 70, pain lasts more than a year. Patients are at greater risk for PHN as they get older, if they experience intense pain during acute shin-gles, if the original rash was severe or they had serious emotional stressors at the onset of shingles. Antiviral therapy reduces severity and duration of shingles and may prevent PHN, but not in all cases. Available treatments shown to work for some patients are topical lidocaine patch 5% (not available in Canada), gabapentin, TCAs, opioids and the recently approved drug in Canada for neuropathic pain (pregabalin). Nerve blocks, cut-ting nerves or use of spinal stimulators have unproven effectiveness. A recently published study of 38,000 adults older than 60 years of age tested a special vaccine (Oka/Merck VZV vaccine) and showed that it works quite well in reducing the severity of shingles and the occurrence of PHN. The vaccine is not yet available in USA or Canada.

54 year old woman with burning pain and hypersensitivity to touch and pinprick in her armpit after bilateral mastectomy for breast cancer, followed by radiotherapy and breast reconstruction. The skin graft of the reconstructed breast is anesthetic and painless, while the shaded area of pain and hypersensitivity correspond to the area of the skin innervated by the intercostobrachial nerve (a long skin nerve in the chest wall and the underarm area).
A quarter or more of women who have breast surgery report pain a year later. Specific-ally, pain after breast surgery for cancer is not a simple syndrome as several entities have been described: phantom breast pain, nerve injury pain (as in the case reported here), brachial plexus neuropathy due to infiltration by cancer or due to scarring after radiother-apy, cervical radiculopathy, shoulder inflammation etc. Breast pain can also occur after non-cancer surgeries as in the case of breast implants or breast reduction. It is not easy to separate and understand the different mechanisms of pain after breast surgery and the pain is not well recognized and managed by physicians. Traditional treatments for neuropathic pain (pharmacological and local) as well as non opioid and opioid analgesics have variable success
PAIN AFTER BREAST SURGERY
Allodynia Hyperalgesia
20
21
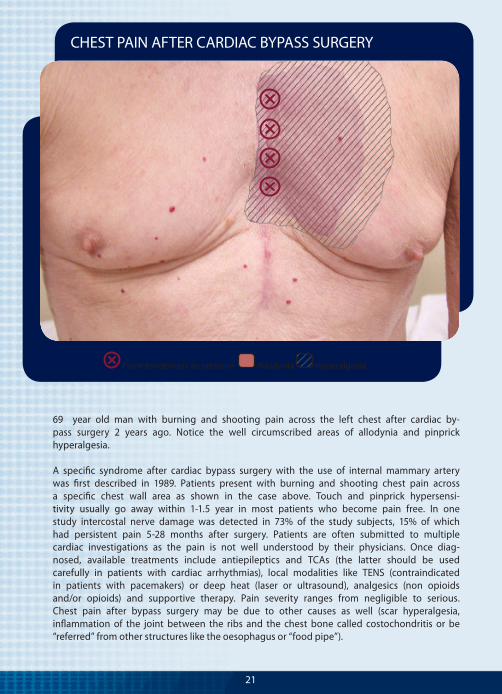
69 year old man with burning and shooting pain across the left chest after cardiac by-pass surgery 2 years ago. Notice the well circumscribed areas of allodynia and pinprick hyperalgesia. A specific syndrome after cardiac bypass surgery with the use of internal mammary artery was first described in 1989. Patients present with burning and shooting chest pain across a specific chest wall area as shown in the case above. Touch and pinprick hypersensi-tivity usually go away within 1-1.5 year in most patients who become pain free. In one study intercostal nerve damage was detected in 73% of the study subjects, 15% of which had persistent pain 5-28 months after surgery. Patients are often submitted to multiple cardiac investigations as the pain is not well understood by their physicians. Once diag-nosed, available treatments include antiepileptics and TCAs (the latter should be used carefully in patients with cardiac arrhythmias), local modalities like TENS (contraindicated in patients with pacemakers) or deep heat (laser or ultrasound), analgesics (non opioids and/or opioids) and supportive therapy. Pain severity ranges from negligible to serious. Chest pain after bypass surgery may be due to other causes as well (scar hyperalgesia, inflammation of the joint between the ribs and the chest bone called costochondritis or be “referred” from other structures like the oesophagus or “food pipe”).
CHEST PAIN AFTER CARDIAC BYPASS SURGERY
Point tenderness to pressure Allodynia Hyperalgesia

22
REFERENCES
The scientific information used in this Atlas is listed in detail in the medical version for professionals (Mailis Gagnon A. Pocket Atlas of Neuropathic Pain Syndromes, 2006).
ABBREVIATIONS
CNS: Central Nervous System; CRPS: Complex Regional Pain Syndrome; DREZ: Dorsal Root Entry Zone; IASP: International Association for the Study of Pain; MS: Multiple Sclerosis; MVA: motor vehicle accident; NMDA: N-methyl-D-aspartate; PHN: postherpetic neuralgia; PNS: Peripheral Nervous System; RCT: randomized controlled trial; ROM: range of movement: RSD: Reflex Sympathetic Dystrophy: SNS: Sympathetic Nervous System; TCAs: tricyclic antidepressants; TENS: transcutaneous electrical nerve stimulation; TN: trigeminal neuralgia; TSCI: traumatic spinal cord injury.
REFERENCES / ABBREVIATIONS