Folien SvenStreit - palliativebern.ch · insulin (sliding scale) dronedarone metoclopramide...
6
27/08/2019 1 wie lange gebe ich welche Medikamente noch weiter? Prof. Dr. med. Dr. phil. Sven Streit Berner Institut für Hausarztmedizin (BIHAM), Universität Bern Hausarzt in Konolfingen Vorbemerkungen Finanzielle Unterstützung: Interessenskonflikte: Herr K, 82jährig Aspirin 100 mg 1-0-0-0 Atorvastatin 40 mg 0-0-1-0 Enalapril 10 mg 1-0-0-0 Amlodipin 5 mg 1-0-0-0 Paracetamol 1 g 1-1-1-0 Tramadol 50 mg 1-0-1-0 Pantoprazol 20 mg 1-0-0-0 Palliative Care? 50% Überleben von 6 Monaten (Mitchell Index) Inhalt Einleitung Herausforderungen Definition Deprescribing Deprescribing in Palliative Care LESS Studie Was halten Ärzte von Deprescribing? Was halten Patienten von Deprescribing? Was können wir tun? In unserer Praxis? In der Forschung? Hintergrund 1: Herausforderungen liegen vor uns • Alter – Multimorbidität – Polypharmazie – ungeeignete Medikamente 1 United Nations 2012 2 Barnett Lancet 2012 3 Carroll JAMA Int Med 2017 4 Jadad JAMA 2011 Herr Meier, 82
Transcript of Folien SvenStreit - palliativebern.ch · insulin (sliding scale) dronedarone metoclopramide...

27/08/2019
1
wie lange gebe ich welche Medikamente noch weiter?
Prof. Dr. med. Dr. phil. Sven Streit
Berner Institut für Hausarztmedizin (BIHAM), Universität Bern
Hausarzt in Konolfingen
Vorbemerkungen
Finanzielle Unterstützung:
Interessenskonflikte:
Herr K, 82jährig
Aspirin 100 mg 1-0-0-0Atorvastatin 40 mg 0-0-1-0Enalapril 10 mg 1-0-0-0Amlodipin 5 mg 1-0-0-0Paracetamol 1 g 1-1-1-0 Tramadol 50 mg 1-0-1-0Pantoprazol 20 mg 1-0-0-0
Palliative Care?50% Überleben von 6 Monaten(Mitchell Index)
Inhalt
Einleitung Herausforderungen
Definition Deprescribing
Deprescribing in Palliative Care
LESS StudieWas halten Ärzte von Deprescribing?Was halten Patienten von Deprescribing?
Was können wir tun?In unserer Praxis?
In der Forschung?
Hintergrund 1: Herausforderungen liegen vor uns
• Alter – Multimorbidität – Polypharmazie – ungeeignete Medikamente1 United Nations 20122 Barnett Lancet 2012
3 Carroll JAMA Int Med 20174 Jadad JAMA 2011
Herr Meier, 82

27/08/2019
2
Hintergrund 2: “Deprescribing” – die Lösung?
Risiko/Nutzen individueller Patientenwunsch
• Was sind Gründe für/gegen Deprescribing?1 Scott JAMA IM, 20152 Page Br J Clin Pharm 2016
3 Gnjidic Clin Geriat Med 20124 Mantelli BMC Fam Pract 2018
Hintergrund 3: Deprescribing in Palliative Care (PC)?• USA 1
• UK 2
• Auslöser für Deprescribing oft der Sterbeprozess (reaktiv) und nicht die Prognose (proaktiv)
1 McNeil J Pain Symp Manag 20162 Doré BMJ Supp Pall Care 2019 (Poster)
Was denken Ärzte zu Deprescribing?LESS-Studie
• Umfrage• Fallvignette:
• Medikamente:
• Bereitschaft Gründe
Mantelli BMC Fam Pract 2018
Resultate von 157 ÄrztenMedikament (Dosis/Tag)
% für Deprescribing aller Hausärzte Gründe (am meisten genannt)
Atorvastatin 40 mg 100% Zu wenig Benefit
Pantoprazol 20 mg 88% Keine Indikation
Aspirin 100 mg 74% Keine Indikation
Tramadol 100 mg 71% Nebenwirkungen
Amlodipin 5 mg 44% Keine Indikation
Paracetamol 3g 29% Tiefere Dosis probieren
Enalapril 10 mg 24% Keine Indikation
Mantelli BMC Fam Pract 2018
Was ist Ärzten wichtig bei Deprescribing?
• Risiko und Nutzen• Lebensqualität • Lebenserwartung • Patientenwunsch -präferenzen• Kosten/Nutzen

27/08/2019
3
Und in Europa? Hohe Bereitschaft für Deprescribing bei Ärzten
• Breite Unterstützungfür Deprescribing in Europa und anderenLändern
Jungo et al. , Manuskript in VorbereitungDanke EGPRN !
Was denken Patienten zu Deprescribing?LESS-Studie
Bereitschaft für Deprescribing
• Die Gründe für/gegen • Zusammenhänge
• 300 Patienten, mittleres Alter 79.1 (SD 5.7)
Resultate 2: Polypharmazie und Bereitschaft
Polypharmazie
8 Medikamente
Bereitschaft für Deprescribing
wenn ihr Hausarzt sagt es ist möglich
Rozsnyai et al. Manuscript in Vorbereitung
Resultate 3: Häufig genannte Gründe
Gegen Deprescribing
Für Deprescribing
Rozsnyai et al. Manuscript in Vorbereitung
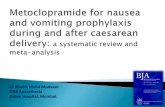
Aber
• Erste Resultate: 53% PIM, einige sogar bis 7/Patient
0 10 20 30 40 50 60
antispasmodicsmineral oil
antispasmodicsfirst-generation antihistamines
est rogens *opioids in combinat ion with benzodiazepines *
digoxininsulin (sliding scale)
dronedaronemetoclopr amide
nifedipinewar farin in combination with NSAIDs
any combination of ≥3 CNS-active drugs *opioids in combinat ion with gabapentin or pregabalin
NSAIDswar farin in combination with amiodar one
sulfonylureas (long acting)nonbenzodiazepines (Z-dr ugs) *
antidepressant speripheral alpha- 1 blockers with loop diuretics *
benzodiazepines *proton-pump inhibit ors
Most frequent potentially inappropriate medication by gender
Fe male
Mal e
Erste ResultateAchterhof, in preparation
CAVE Benzodiazepine besonders bei Frauen
und in Kombination mit Opiaten

27/08/2019
4
Was denken Patienten in anderen Ländern?
• Kanada1
• Italien2
• Australien3
• Australien4
• USA5
1Sirois Res Social Adm Pharm, 20172Galazzi Int J Clin Pharm, 2016
3Qi Int J Clin Pharm 20154Reeve BJGP, 2016
5Reeve JAMA IM, 2018
Was können wirin der Praxis tun?Tipps & Tools
Bern, 6.6.2018
1. Deprescribing – wann? 2. Deprescribing – wie?
Scott JAMA IM, 2015
Framework für Deprescribing in Palliative Care
1. Shared decision-making is also about prescribing medications
2. Not prescribing a medication should be presented as a reasonable
alternative for patients late in life, when appropriate
3. Deprescribing is part of prescribing
4. Prescribers have to embrace uncertainty
5. Difficult discussions now will simplify difficult decisions in the future Todd Int J Clin Pharm. 2015
Tools für Deprescribing in Palliative Care
Lindsay et al 2015
Was? Wann?Aspirin PrimärpräventionStatine Alle IndikationenAntihypertensiva Bei milder/moderatere HypertoniePPI Alle Indikationen ausser GERD, Steroide, NSARAntidiabetika Milde HyperglykämieOsteoporose Ausser bei HypercalcämieVitamine Alle Indikationen

27/08/2019
5
Deprescribing ToolsBeispiel Schweiz
Algorithmus von Garfinkel1:
1Garfinkel Arch Intern Med 2010
Deprescribing GuidelinesBeispiel Kanadawww.deprescribing.org
Proton Pump Inhibitor (PPI) Deprescribing Algorithm �ļäļĭĴ 201ź
Farrell B, Pottie K, Thompson W, Boghossian T, Pizzola L, Rashid J, Rojas-Fernandez C, Walsh K, Welch V, Moayyedi P. (2015). Evidence-based clinical practice guideline for deprescribing proton pump inhibitors. Unpublished manuscript.
© Use freely, with credit to the authors. Not for commercial use. Do not modify or translate without permission.This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Contact [email protected] or visit deprescribing.org for more information.
Recommend Deprescribing
Monitor at 4 and 12 weeks
or consult gastroenterologist if considering deprescribing
If unsur t if history of endoscopy, if ever hospitalized for bleeding ulcer or if taking because of chronic NSAID use in past, if ever had heartburn or dyspepsia
Mild to moderate esophagitis or GERD treated x 4-8 weeks (esophagitis healed, symptoms controlled)
Peptic Ulcer Disease treated x 2-12 weeks (from NSAID; H. pylori)Upper Gl symptoms without endoscopy; asymptomatic for 3 consecutive days ICU stress ulcer prophylaxis treated beyond ICU admission Uncomplicated H. pylori treated x 2 weeks and asymptomatic
Avoid meals 2-3 hours before bedtime; elevate head of bed; address if need for weight loss and avoid dietary triggers
If verbal: Heartburn Regurgitation
DyspepsiaEpigastric pain
If non-verbal: Loss of appetite Agitation
Weight loss
(evidence suggests no increased risk in return of symptoms compared to continuing higher dose), or
(daily until symptoms stop) (1/10 patients may have return of symptoms)
Barrett’s esophagusChronic NSAID users with bleeding riskSevere esophagitisDocumented history of bleeding GI ulcer
����
����
��
� �
�
��
��
�
��
Why is patient taking a PPI? Indication still
unknown?
Continue PPIStop PPIDecrease to lower dose
Stop and use on-demand
Strong Recommendation (from Systematic Review and GRADE approach)
If symptoms persist x 3 – 7 days and interfere with normal activity: 1) Test and treat for H. pylori2) Consider return to previous dose
If symptoms relapse:Use non-drug approachesOver-the-counter antacid, H2RA, PPI, alginate prn (ie. Tums®, Rolaids®, Zantac®, Olex®, Gaviscon®)H2RA daily (weak recommendation – GRADE; 1/5 patients may have symptoms return)
Manage occasional symptoms
Farrell B, Pottie K, Thompson W, Boghossian T, Pizzola L, Rashid FJ, et al. Deprescribing proton pump inhibitors. Evidence-based clinical practice guideline. Can Fam Physician 2017;63:354-64 (Eng), e253-65 (Fr).
Was können wir in der Forschung tun?Die OPTICA-Studie• Hauptziel:
• Nebenziele:
Implementierung
elektronischer Krankengeschichten
Jungo et al. BMJ open, in press
Software STRIP
• Systematic Tool to Reduce Inappropriate Prescribing (STRIP)
1OPERAM (PI Rodondi), operam—2020.eu
Herausforderungen
vulnerable Personen
GCP-Kurses
Schnittstellen
Jungo et al. Primary Hospital Care, in Print
Zusammenfassung
Medikamente stoppen/reduzieren (Deprescribing)
98% der Ärzte sind motiviert
80% der Patienten sind bereit, wenn von Ärzten empfohlen
Gute Beziehung zum Arzt, Studien und sicheres Gefühl bei Deprescribing unterstützen Deprescribing.
Dagegen sprechen schlechte Erfahrungen mit Deprescribing und unsicher sein, wie Deprescribing umgesetzt werden soll (Beispiel PPI)
Deprescribing-Studien am erfolgreichsten wenn Intervention durch Ärzte/Apotheker
Forschung: MIT gebrechlichen Patienten MIT Ärzten MIT Einbeziehen des Patientenwunsches (z.B. OPTICA Studie und viele weitere)
Praxis: Regelmässig Medikamentenlisten durchsehen, Guidelines sind am Entstehen

27/08/2019
6
individual clinical expertise best available external evidence
individual patient
David L Sackett, BMJ 1996
Danke für Ihre Aufmerksamkeit
Spezieller Dank an:
Prof. Dr. med. Dr. phil. Sven Streit
www.biham.unibe.ch
Twitter @Sven_Streit