Focus on on Cochlear Cochlear Implants Implants · deaf children beginning school have a cochlear...
60
MAGAZINE March 2005 ISSN 1366-0799 Focus on Cochlear Implants Focus on Cochlear Implants MAGAZINE
Transcript of Focus on on Cochlear Cochlear Implants Implants · deaf children beginning school have a cochlear...

MAGAZINEMarch 2005
ISSN 1366-0799
Focus on Cochlear ImplantsFocus on Cochlear Implants
MAGAZINE
53955-BatodMarch05 8/3/05 9:18 am Page 1
creo

website: www.BATOD.org.ukOur email addresses are easy to remember.They all end @BATOD.org.uk So the Magazine will be:
[email protected](check your spelling so you don’t fall into the black hole!)
Phoning 01964 544243BATOD Magazine, Publications & Advertising?
if no-one makes it to the phone to respond
....PLEASE SPEAK
(don’t sigh and hang up!)
LEAVE A MESSAGE
or send a fax
or even email [email protected]
Visit our web pages www.BATOD.org.ukarticles should be emailed to
Need to contact BATOD?talk to
BATOD Secretary Paul Simpson email: [email protected]/fax 01494 464190
From your editorThis Magazine has no minutes or reports from the last NEC (December) meeting as these appeared in January’s Magazine and the next
NEC is held in conjunction with the March Conference and AGM. This is probably just as well as there have been many articles both about
the focus topic and also shorter items of interest that BATOD members have sent in. My thanks to Pauline Cobbold who has gathered all
the articles in.
The Cochlear Implant focus of this Magazine presented a challenge in that we wanted as many Implant teams as possible to have the
opportunity to contribute. This may have resulted in a bit of overlap of information but you should have a good overview of what is going
on in the Cochlear Implant world.
The BATOD website now has an on-line magazine folder in ‘Publications’ and the articles from January’s focus on models of deaf
education are available. Visitors are asked to submit information about their area/national provision. There will be a similar folder for
cochlear implants and everyone is invited to submit more news, information and to share good practice. Items for submission should be
sent to [email protected] at any time.
Do remember that the BATOD website is continually being supplemented with items of interest and articles on various issues.
Use this as a resource and send in items that can be shared. The quality and content of information is reliant on what BATOD members
share with each other through the media of the Magazine and the website.
As the steering group at NEC is now considering a replacement editor for me, the format, style and content of the
Magazine will be considered. If you have constructive ideas please share them with Paul Simpson, or indeed, think
about becoming an editor yourself.
Cover PictureToby and his mum road test materials for review in the BATOD Magazine.
MMaaggaazziinnee eeddiittoorr
CONTENTSCochlear Implants in children: past, present and future ........ 2BCIG ...................................................................................... 4Guidelines for ToDs working with CI children ....................... 5Cochlear Implantation and the future ..................................... 6One size fits all? ..................................................................... 7Categorising hearing loss for those with cochlear implants .. 9Phonological awareness ........................................................ 11Cochlear Implants International ............................................. 12FM systems with cochlear implant speech processors ......... 14Generic trouble shooting of CI system .................................. 17Cochlear implantation and cued speech ............................... 18Listening boxes ...................................................................... 20CI in children with complex needs ....................................... 22Bringing deafblind cochlear implant users together .............. 23CIs in an oral environment .................................................... 24Growing up, moving on ......................................................... 25Management of CIs in a bilingual special school ..................... 26Working with teenagers ......................................................... 28www.ci-4teenz.com ............................................................... 29Manchester adolescent CI programme ................................. 30Cochlear Implants - a guide for families ............................... 31Teenage programme at Southampton .................................. 31Keeping the links working ..................................................... 32After early diagnosis - early implantation? ............................ 35A tactile audiogram for deafblind pupils ................................ 37Regular items and general informationMechlen CI Course ............................................................... 4NEAP (Resource Review) ..................................................... 33Challenges - DCCAP ............................................................. 36New BSL on-line glossaries of signs ..................................... 38This and that ........................................................................ 41Educational achievement, measurement and perspective .. 44EARS ..................................................................................... 46Sharing information - Dyslexia .............................................. 48Obituary Melanie Dix 1965-2004 .......................................... 48Ear Foundation website ........................................................ 50Noticeboard ........................................................................... 51Abbreviations in this Magazine .............................................. 52ICT for teachers ..................................................................... 53
Association Business:....thoughts from my potting shed .......................................... 1Children’s FM working group meeting .................................. 21BATOD archives .................................................................... 45‘At the heart of inclusion’ synopsis ........................................ 46Educational Maintenance Allowance ..................................... 50Subscription rates 2004-5 ....................................................... 55I’ve moved... notification form ................................................. 55
Advertising rates .................................................................... 37Calendar - Meetings and training to know about .................. 56Officers of Regions and Nations............................ inside back cover
53955-BatodMarch05 8/3/05 9:18 am Page 2

©BATOD Magazine March 05 1
Whilst potting up African violet cuttings in mypotting shed, I was thinking about this articleand realised that many of the things that arecurrent are those I have mentioned in myprevious article. I thought perhaps I could justrevisit my previous 'thoughts' and see if anyoneother than Ann and her team of proof readerswould notice! This made me realise thatsometimes things do move slowly so this will bean update of on-going business.
On 18 January 2005 BATOD was involved in afurther meeting regarding the future of trainingcourses for Teachers of the Deaf. Again therewere representatives from the training courses,RNID and NDCS. There were responses toWendy McCracken's proposals from groupsand members across the UK. I think it hasbeen heartening that there were responsesfrom across the country as all areas will beaffected. These responses are being collatedand put together with statistics of numbers ofdeaf children and numbers (and age profile) ofTeachers of the Deaf. The DfES recognises theneed for increased numbers of Teachers of theDeaf as they have produced, with theinvolvement of many organisations includingBATOD, a leaflet promoting recruitment. Thusit is hoped that when the case for tackling theconcerns around the future of the trainingcourses is made, they will appreciate itsimportance. The next meeting for this group isat the end of April and by that time allconcerned will have a clearer idea of whatproposals we are taking to the DfES.
Another on-going issue is the review andrevamping of the BATOD survey. As previouslymentioned, BATOD has been in negotiationwith the Scottish survey - ADPS (the
Achievements of Deaf Pupils in Scotland).ADPS have an up-to-date data base andsurvey format that has been based on theBATOD survey. Sadly Dr Mary Brennan fromEdinburgh University has been taken seriouslyill and as she heads up ADPS things havecome to a temporary halt. Hopefully next timeI will have good progress reports on both Maryand the survey modernisation.
Accurate and robust statistics are vital for manyaspects of our work including submissions tothe DfES (eg on the need for Teacher of theDeaf training courses) so it is really important tocontinue to collect the data across the UK.There are also many other good reasons forthe data collection as there is a need to havedetailed research into all aspects of deafnessand deaf education. A reliable source of data isessential for credibility.
In the last few weeks I have had considerabledifficulties with the exam arrangements forGCSE. Changes have been put in placewithout consultation or real announcement. Ifcandidates are being presented this year weneed them to be sitting mock exams under thesame conditions as the real exams. This hasbeen a shock for some pupils as well as theteachers as they try to sort out thesearrangements. BATOD and many of itsmembers have been pursuing this with both theJoint Council of Qualifications and the individualAwarding Bodies. More information aboutreasonable adjustments in examinations 2004-2005 is available about this on our website atwww.BATOD.org.uk and followHome/Articles/Reasonableadjustments/Concerns.
...... thoughts from my potting shedCarole Torrance, President
CCaarroollee
53955-BatodMarch05 8/3/05 11:58 am Page 3

2 ©BATOD Magazine March 05
Apart from the changes in numbers, the proceduresand criteria have changed over the years. Initiallyonly those children with near total hearing losseswere implanted; now children with some residualhearing are receiving implants. Children with aidedthresholds of 50dB and even less, will routinely beconsidered for implantation; through their implantthey are likely to receive sound in the region of 30dBacross the speech frequencies, receiving useful highfrequency information. Many children successfullyhave an implant in one ear and wear a hearing aidin the other. In some countries bilateral implantationis becoming the norm, giving benefits of localisationand of listening in noise.
In addition to children with some residual hearingbeing considered for implantation, the age of thoseimplanted has also changed. Following an earlierdiagnosis of hearing loss, children are being referredearlier for implantation and being implanted earlier.
Cochlear implants in children: past, present and future?Sue Archbold, Education Co-ordinator, The Ear Foundation
Currently, the youngest child to be implanted in theUK was an infant of six months. On the other hand,increasing numbers of teenagers are requestingimplants for themselves; these are likely to be thosewho are using their residual hearing well and usespoken language but who would receive more of thespeech signal through an implant. Increasingnumbers of children with complex needs are alsoreceiving implants. This requires a great deal ofcareful assessment, particularly to ensure that thereis a definitive assessment of the levels of hearing.Up to 40% of deaf children are likely to have anotherdifficulty and one which an implant may not help.Interestingly, more deaf children of deaf parents arenow receiving implants - in order to give them bothspoken and sign language.
The procedure of implantation itself has nowchanged – the stay in hospital is likely to be one dayand there will be minimal hair shave (if any) and asmall scar behind the ear. The technology haschanged over the years, enabling tuning of theexternal system to take place more easily withobjective measures taken. In addition the externalsystems are smaller with ear level processors muchmore commonly used.
Cochlear implantation has been shown to be safeand devices largely reliable. In a series of 500operations over 15 years on children at theNottingham Cochlear Implant Programme, therehave been 18 failed devices, all successfully
This edition of BATOD magazine is focussed on cochlearimplantation – an intervention for deaf children whichbegan in the UK in 1989, amidst much controversy. In theyears since then, the numbers have grown rapidly – in theUK, there are currently about 2,400 children who havereceived implants. As can be seen from the graph(www.ihr.mrc.ac.uk) the numbers implanted on an annualbasis have also grown over the years, until about 300children per year are now implanted. The implication forTeachers of the Deaf is that now over half the profoundlydeaf children beginning school have a cochlear implantand in some educational settings the children with implantsoutnumber those with hearing aids. Now that we have alarge group of children with implants, some who have hadtheir implants for some time and are growing to adulthood,what have we learnt and what has changed?
53955-BatodMarch05 8/3/05 9:18 am Page 4

replaced, three cases of infection and three devicesremoved for other reasons. In the same group ofchildren, the usage rate remains high, with over90% of children continuing to choose to wear theirimplant systems all or most of the time, five yearsafter implantation.
Although results from implantation can be veryvariable, we do know that age at implantation has astrong effect on outcomes. If we look at changes ina child’s ability to use hearing to understand spokenlanguage, five years after implantation, over 80% ofchildren implanted under three can understandconversation without lipreading. If we look atspeech intelligibility, we see a similar pattern, with40% of children implanted below the age of threehaving speech with normal intelligibility, five yearsafter implantation.
What have been the changes we have seeneducationally? With regard to educationalplacement of children with implants, significantlymore children implanted before the age of five go tomainstream schools and significantly fewer toschools for the deaf, when compared with a likegroup of children with hearing aids. When we lookat communication and use of spoken language, wecan see changes after implantation over time. In astudy looking at the effect of communication modeon progress after implantation, those children usingoral language at three years after implantationoutscored those using sign language. However,when those who had always used oral languagewere compared with those who began using signlanguage and had changed to oral language afterthree years, there was no significant differencebetween them. A current research study, funded byNDCS, is looking at the pattern of changes incommunication after implantation. Although the aimof cochlear implantation is to provide hearing forspeech, for some children sign language has a roleand the issue of cochlear implantation and signlanguage clearly needs investigation. The large UKstudy led by Quentin Summerfield (formerly of IHR)and in which many Teachers of the Deafparticipated, has shown that children with implantsare performing as children who are less deaf.
With this growing experience of implantation, whatare the major issues?� complexity of monitoring the device functioning� complexity of device programming � implementation of changes in technology over
time� management of device and technology difficulties
©BATOD Magazine March 05 3
� length of time taken for progress – often yearsnot months
� flexibility of educational support required:placement, levels of support and communicationmay change over time
� medical risks associated with implantation.
There are three other issues emerging as we gainmore experience. � It may be that implants sometimes work too well!
Levels of intelligibility are sometimes such that itmay appear to a non-specialist that the child hasno difficulty in accessing the curriculum; this is anaïve view. These remain profoundly deafchildren but function as less deaf than beforeimplant.
� There are other children who do not do as wellas one might have predicted. It is likely thatthese children have learning difficulties notidentifiable prior to implantation, which now canbe more readily identified when they have someuseful hearing.
� Another recurring theme in discussion aboutimplantation is the management of those withimplants as they grow through adolescence,maintaining and developing implant use throughthese challenging times and supporting them indeveloping a secure identity as a deaf personwith an implant.
In order to maximise the benefits of implantation,teachers need to know about:� the differences between cochlear implants and
hearing aids� appropriate candidature� expectations from implantation for different
populations� the fundamentals of an implant system� the basics of the tuning process� monitoring the system’s functions and trouble-
shooting� monitoring the child’s progress.
These are some of the everyday knowledge andskills required; however, for them to be put in placeand utilised effectively, there may need to be someorganisational changes. Educational services needto look at how they:� organise their services to provide effective,
trained support in the classroom for those inmainstream
� provide placement and communication choicesas children’s needs change
� meet the challenges of sign-bilingualism andbilingualism and cochlear implants
53955-BatodMarch05 8/3/05 9:18 am Page 5

4 ©BATOD Magazine March 05
� provide appropriate education for those for whoman additional language difficulty may becomeapparent after implantation
� provide support for the implant system and theamount of hearing it provides in the demandingenvironment of secondary or high school
� implement changes in technology and supportthem throughout the child’s educational life
� provide for the psycho-social needs of thechildren as they grow to independence.
With growing numbers of children receiving implantsat earlier ages, including those with complex needs,it is vital that teachers receive regular updates in themanagement of this rapidly changing technology.The developments are far from finished: bilateralimplants, implants with electrical and acousticstimulation, wholly implantable devices and thosepromoting hair cell regeneration are some of thetechnical developments which will be in use in ourclassrooms over the next ten years. At the EarFoundation the education programme provides abridge between the clinic-based services, home andschool where the children actually use thetechnology.
As the Teacher of the Deaf of the first child toreceive an implant, I find an entry in my diary from1987: “will all this come to anything and be worth the effort?”
Mechlen CI courseRehabilitation specialists from Europe gathered inMechlen, Belgium at the Cochlear Training andEducation Centre for the first Nucleus FoundationCourse.
The two and a half day course was attended byeducational practitioners including Teachers of theDeaf (ToDs) from four UK Cochlear Implant Centres:Cambridge, Kilmarnock, Nottingham and South ofEngland and also Teachers of the Deaf fromSwitzerland, Belgium and Denmark. As well as theformal training sessions there was the opportunityfor the twelve ToDs on the course to network, shareand discuss working with deaf children acrossEurope. Cochlear Corporation regularly providessuch courses.
BCIGIn 1989, Graham Fraser formed a group calledBritish Cochlear Implant Group (BCIG) to bringtogether those working in the implant field, whatevertheir profession, to promote good practice.
It is a professional body with members includingclinicians working in cochlear implant centres acrossthe UK, experts and scientists working in the field,manufacturers of cochlear implant equipment andother professionals and members of the public withan interest in cochlear implantation.
BCIG aims to provide information in the field ofcochlear implantation to patients, prospectivepatients, families, carers, educators and otherinterested parties.
All cochlear implant centres in the UK are members(there is a map on the website) and contact detailscan be found on www.bcig.org
With NDCS, BCIG has published Quality Standardsfor cochlear implantation - and the revised version isabout to be launched at the BCIG meeting inBirmingham in April 2005.
BCIG also publishes guidelines for Teachers of theDeaf working with children with implants. Theseexamples of good practice are unique in the world inendeavouring to cross professional and institutionalboundaries in the support of these children.
Taking time out on the Variety Club bench at The Ear Foundation.
The outcomes we are seeing in many children arefar beyond what we expected then, when we feltsome deafened children may be able to hearenvironmental sounds and perhaps have an aid tolipreading. Who knows what the next ten years willbring?
53955-BatodMarch05 8/3/05 9:18 am Page 6
creo

©BATOD Magazine March 05 5
IntroductionAs both the benefits and responsibilities ofpaediatric implantation have become clear, theimportance of the collaboration between educationsupport services and cochlear implant professionalsis being increasingly recognised and documentedworld-wide. Educators will provide long-termsupport and management and be responsible forsupporting parents and children.
As more Teachers of the Deaf are working oncochlear implant teams, we need to share andpromote consistency of practice, in consideration of:� selection of appropriate candidates� amount/nature of support that is necessary for
each implanted child� access of implant team professionals to children
in different schools� responsibilities of implant centre Teachers of the
Deaf� responsibilities of class teachers and local
Teachers of the Deaf� long-term effects of implantation on educational
management and attainments� long-term need for maintenance of the device
and how this is best provided.
The guidelines cover:� the roles and responsibilities of Teachers of the
Deaf on implant teams� access to schools and children by implant team
professionals� minimum standards of support� direct contact� indirect contact� aims of outreach visits by implant centre
teachers� support needs: management of device� information for local Teachers of the Deaf and
class teachers.
The aim is to promote consistency of practicethroughout the UK and a recognition of the needs ofchildren with cochlear implants. They were drawnup bearing in mind that other professionals, forexample, speech and language therapists, will beworking with implanted children and the roles mayoverlap.
RationaleThe guidelines are based on the following premises.� The aim of cochlear implantation is (unless there
are other major difficulties for the child) to
provide access to spoken language throughhearing, which was not possible for that childwith hearing aids.
� The demand for, and incidence of, paediatricimplantation is continuing to grow. The group willinclude:
- very young children- adolescents- children with complex needs- deaf children of deaf parents.
� Many young children, without other significantlearning difficulties, are able with appropriatesupport to acquire spoken language throughaudition after implantation. Some of thesechildren are now in mainstream schools.
� Benefits are only seen in the long-term andcontinue to develop in the years postimplantation.
� Long-term maintenance and management is vitalin order to maximise these benefits.
� Monitoring long-term outcomes is essential.
Definitions� Implant Centre Teacher of the Deaf (ICTOD) - the
Teacher of the Deaf based at an implant centre� local Teacher of the Deaf - Teacher of the Deaf
local to child whether peripatetic or class teacher� class teacher - where not Teacher of the Deaf� keyworker - as defined in BCIG/NDCS Quality
Standards document
The Guidelines booklet was included with a BATODmagazine mailing but if you cannot trace your copyor want to have more to hand out to colleaguesplease contact the BATOD Publications Manager([email protected]) or download a copyfrom the BCIG website www.BCIG.org
In the Audiology Focus Magazine (September 2003page 18) Jane Frew described a ‘sister’ publicationto the BCIG booklet as the RNID EducationalGuidelines Project launched ‘Working with childrenwith cochlear implants’. The publication is broad-based, addressing the development needs ofchildren of different ages, using a range ofcommunication approaches and in a variety ofeducational settings.
As well as background information about cochlearimplants the publication provides practical advice,recommended activities and strategies to encouragethe effective use of cochlear implants by deafchildren of different ages and at different stages ofdevelopment. It includes sources of informationavailable for families and professionals.
Guidelines for Teachers of the Deaf working withchildren with cochlear implants
53955-BatodMarch05 8/3/05 9:18 am Page 7

6 ©BATOD Magazine March 05
The field of cochlear implantation has evolvedsubstantially over the past three decades such thatmore young children are receiving implants andindividuals with more residual hearing can accessthis technology. When one quickly reviews the past,it becomes apparent that this technology is not onlyhere to stay but will continue to improve. Thechallenges that face the industry are still the sameas they were decades ago; to ensure that severe toprofoundly deaf individuals receive high qualitysound and that they function effectively in thepresence of background noise. Towards that goalthere are numerous possibilities that can beconsidered as one looks at the future of thistechnology.
The first and foremost issue facing researchers inthis field is to improve the overall speech perceptionabilities of the recipients. This requires the futurespeech processors to select the best speechfeatures to pass through the implant and presentthis information at optimal rates. The best rate maybe different for each implant recipient and thereforeflexibility in processing the sound will be required.Once the parameters that are necessary to makesound more understandable are identified, the abilityto reproduce the coding of the sound moreeffectively must be realised. Additionally, the abilityto code different types of signals, such as music,needs further investigation.
Delivery of the information via the electrodeinterface will also change. The proximity of theelectrodes to the modiolus (the centre of thecochlear that contains the neural elements to bestimulated) will continue to improve. The number ofelectrode contacts and the use of nanotechnology(the ability to build machines on the scale of humancells) will allow more stimulation sites along thenerve. Electrode arrays that grow directly into thenerve may also be possible. Surgical techniqueswill continue to evolve as the demand for moreprecise electrode placement grows.
The ability to provide better perception in noisyenvironments will be the focus of attention as theperformance continues to improve. Hybrid devicesthat combine both electrical and acousticalinformation are now being investigated. This will notonly increase the potential number of candidateswho can benefit from implant technology but it willalso provide individuals who have severe highfrequency hearing loss with better signal input.
Bilateral cochlear implants have been introduced inthe past two years and the data continues to supporttheir utility in both the areas of sound localisationand improved hearing in noise. The benefit this willhave on children in classrooms has not yet beenrealised as the number of children with thisconfiguration is still rather small. Clearly, the noisyclassroom environment poses challenges forchildren learning under the best circumstances andtherefore bilateral cochlear implants may provide theadded signal boost that can be the differencebetween understanding and misunderstanding. Theuse of dual microphones in speech processors mayalso provide some relief from noise. These arepresently being used in hearing aid technology withgreat success.
The development of the totally implantable cochlearimplant system has reached the manufacturers'laboratories and shows great promise for the nextdecade. The challenge of developing a system thatuses a microphone that can sustain moisture on aregular basis still remains the biggest hurdle.Methods of using the normal anatomy of the ear toprovide this function are being investigated. Inconjunction with these studies, those that areinvestigating hair cell regeneration are also beingestablished. The combination of regenerating haircells through a system that delivers a neural growthhormone in the ear may provide the best approach.How these new technologies and therapies will betranslated for the later implanted adult or child is stillunknown.
Finally, the role that the professional will play will notonly be crucial but will require an additional set ofskills that will increase in due course. Programmingspeech processors remotely may become morerealistic as the technology changes. Deliveringtherapy over the internet or via interactive videolessons has already begun and will continue todevelop over time. For the teacher in the classroomwireless FM technology that is used today may bereplaced by classrooms that can deliver sound tothe entire class in a more effective manner.
One thing remains clear. Cochlear implantation hashad a profound impact on the way that we treatchildren and adults with severe to profound hearingloss. As the technology evolves we can lookforward to a future that will provide deaf children andadults with the best method of accessing spokenlanguage in the most natural manner.
Cochlear implantation and the futurePatricia M Chute, Ed.D; Helen C Buhler, Ph.D, Mercy College, Dobbs Ferry, NY
53955-BatodMarch05 8/3/05 9:18 am Page 8

©BATOD Magazine March 05 7
Sixteen years ago when my profoundly deaf sonwas just six months old I was told that his firstlanguage would be BSL and that he would needspecial education - a sweeping statement. At thattime, however, it has to be said that both predictionswere likely to be true.
How different things are today! With the advent ofcochlear implants things have swung the other way.Profoundly deaf children are having cochlearimplants and parents are being told that normalspeech and mainstream education are theexpectation - another sweeping statement.
Yes, technology is a wonderful thing and clearly thebenefits of cochlear implantation can be enormousbut in advising parents of newly diagnosed deafbabies that implants are available and can makespeech and mainstream education possible, someparents, obviously greatly relieved by this news, willnever fully accept that their child is and will alwaysbe deaf. They are desperate for their child to be inmainstream education because that indicates'normality' - whatever that means. Some are lookingfor what they want for their child rather than whatthat child actually needs.
As the parent of a deaf child and the Co-ordinator ofCICS*, I would like to make not a sweeping but acommon sense statement regarding education: it isnot possible to compartmentalise any group ofchildren, especially if they are deaf or have otherspecial needs, into one type of educationalprovision.
Outcomes from paediatric cochlear implantation varyenormously and will continue to do so in the futureespecially as children are being implanted youngerand younger before the existence of other difficultieshas been identified. Cochlear implantation is not amiracle that immediately gives access tomainstream education for all children. Undoubtedlyit provides this for some but even within this groupthe amount of support necessary will depend on theindividual child. Other children will need moresupport and will be better suited to placement in aHearing-Impaired Unit ('Unit') where more specialisthelp is available and others will need placement in aspecial school.
Amongst the population of deaf children, with orwithout cochlear implants, some will need signsupport, others are oral (to varying degrees), somewill need very little support, others will need a great
deal; and some will have additional difficulties. It is clear that the needs of deaf children are far toodiverse to be met in any one type of educationalplacement.
Inclusion sounds like a great idea and for some deafchildren it works well. Placement in a local schoolgives the opportunity for friends and socialopportunities close to home and, for the child andthe parents, avoids the stress of a journey to a Unitor school for the deaf which may be some distancefrom home. If a mainstream setting is a small classwith good acoustics, a competent teacher andappropriate support available if needed, thenobviously an able deaf child will stand a goodchance of accessing the curriculum and keeping up.Unfortunately, however, in the real world, a classcan be around thirty children, acoustics are poor anda good deal of a teacher's energy is taken up inkeeping control rather than teaching. In a class ofthirty there will be a wide range of abilities toaddress. The last thing a mainstream teacherneeds is to spend time making sure a deaf child hasunderstood the content of a lesson and to deal withany equipment that the child may have.
There are about 40% of deaf children with additionaldifficulties and of the other 60% there will be manywho will only thrive in a mainstream setting with asignificant amount of support but will they get it and,if they do, will the Classroom Assistant have hadappropriate and sufficient training to work effectivelywith deaf pupils? In many cases this scenario ismerely an excuse for cost-cutting. Placing a deafchild in a mainstream school with limited support isthe cheap option; but if there is little, or no support,it requires immense concentration and is exhaustingfor the child to understand and keep up with theteacher, let alone catch the incidental comments oftheir hearing peers throughout the school day.Inclusion? Perhaps, but at what cost to the deafpupil?
If, in the other extreme, a child has and is totallyreliant upon full-time, one-to-one support in order toaccess the curriculum this will exclude that pupilfrom learning from the class teacher with the hearingpupils. A full-time Classroom Assistant is unlikely tobe a qualified teacher and faces the difficult task ofeffectively translating a lesson into language thatcan be understood by a deaf pupil who may befunctioning at a lower linguistic level than hearingpeers in the class. How can this be described asinclusion?
One size fits all?Tricia Kemp, Co-ordinator of CICS
53955-BatodMarch05 8/3/05 9:18 am Page 9

8 ©BATOD Magazine March 05
The danger of blanket inclusion is that it actuallyleads to total exclusion, leaving some deaf childrenunable to manage socially with hearing peers andunable to keep up with the pace of learning, thusfalling behind and failing to reach their potential.Some Hearing-Impaired Units are able to provide anappropriate mixture of specialist teaching in smallgroups for specific subjects and support duringintegration into mainstream classes but more andmore of these provisions are becoming mainstreambased rather than Unit based, resulting in childrenstruggling to keep up in a setting that is notspecifically designed to meet their needs, iemainstream with support, as opposed to the morestructured and supportive environment provided by aUnit.
It is vital to have good early intervention to enabledeaf children to build the foundations for learning ata later stage. At secondary school the pace oflearning picks up enormously. A deaf child mayalready have a language delay and will simply notmanage to keep up with the vast amount of newvocabulary presented to pupils at this stage of thecurriculum, resulting in an ever-increasing languagegap making it extremely difficult, if not impossible forthe child to access the curriculum at an ageappropriate level.
Delayed communication causes problems outside,as well as inside, the classroom. Goodcommunication skills are vital if a deaf child is todevelop real friendships with hearing peers. If theydon't possess these skills at a young age and theproblem is not addressed by appropriate input at anearly stage, they will simply not catch up, especiallythose who have additional difficulties; and withoutgood communication skills, deafness leads toisolation. Poor communication can lead deafchildren to be left out of games at a young age andto be excluded from social chit-chat as they getolder. In a mainstream setting there may only beone deaf child in the school and unless s/he canfully integrate s/he is likely to feel isolated and mayeven be a target for bullying just because s/he isdifferent. In the short term this may lead to poorself-esteem and even behaviour difficulties and tomental health issues in later life.
The standard and choices of educational provisionfor deaf children need to be improved. Whilst it isclear that the Government's policy for inclusionworks well for some children, it certainly does notwork for all of them and it is important to ensure thatthere is a choice of high quality provision in allareas. Mainstream education with support, which issometimes inadequate, is merely a cheap option for
the local authority and one cannot help wonderinghow much this is a factor in what they offer toparents as an appropriate provision for their child. Itis no good having a child in mainstream education ifthat child's needs are not being fully met. Thismerely represents a short-term saving for the LocalAuthority with long-term adverse consequences forthe child.
The role of a Teacher of the Deaf, whether in aspecial school or as a support in mainstream,remains vital for deaf children. More needs to bedone to encourage teachers to enter this specialisedfield, perhaps by changing the structure of theexisting lengthy training. There will always be aneed for special schools but the number of thesehas been reduced to a dangerously low level. It istime for a re-think. More, not less special schoolsare required, spread appropriately across thecountry and research must be carried out to look atways in which these schools can work effectivelywith mainstream schools to provide pupils with thebest of both worlds. (A role model for this is alreadyin existence in Hertfordshire.)
There is a real danger that the current generation ofdeaf children will be let down by a lack of investmentin their education. In the right setting they willachieve but, without enough support and specialistteaching, many of them don't stand a chance.The ‘system’ must be made to work for, rather thanagainst, deaf children.
Even with the tremendous benefits that technologycan provide, life will be hard enough for deafchildren as they become young adults. If they are tobecome independent, well adjusted members ofsociety able to take their place and compete in thehearing world, they need an individually tailorededucational programme to ensure that they reachtheir potential.
The danger of a blanket inclusion policy is that manydeaf children will simply not be able to meet theirpotential because the system has let them down bylooking at cost rather than individual needs.
‘One size fits all’ simply isn't good enough.
* Cochlear Implanted Children’s Support (CICS)is a voluntary group, run by parents forparents, providing contact, information andsupport for families whose children havecochlear implants and for those who areconsidering an implant for their deaf child.
53955-BatodMarch05 8/3/05 9:18 am Page 10
©BATOD Magazine March 051 9
Background to the projectThe Achievements of Deaf Pupils in Scotland(ADPS) project has been collecting annual datarelating the education of deaf children and youngpeople in Scotland since November 2000. Theproject is based within the University of Edinburghand is funded by the Scottish Executive.
Teachers of deaf children all over Scotland provideinformation for ADPS, much in the same way as forthe BATOD survey. Readers may remember a four-page insert about the project, which appeared in theBATOD magazine of February 2003. We haveworked closely with BATOD and, in 2003, wearranged to collect and share relevant data onScotland. This meant that teachers weren't asked tocomplete two survey returns in one year.
We have now collected four year’s worth of data.As you would expect, one of the key types ofinformation we ask for is hearing loss level. Thismeans that we can report differences betweengroups of children with profound, severe, moderateand mild hearing loss levels. Can, or should,cochlear implanted children be described as'profoundly deaf'? That is a question which we havedebated since the beginning of the project. Thefollowing story describes the way our thinking hasdeveloped.
Ascertaining hearing loss levels: year 1In the first year of the survey, we asked teachers togive us the calculated audiometric descriptor foreach ear (unaided and aided), rather than individualthreshold readings at each frequency. In otherwords, we asked them to say whether the child hada profound, severe, moderate or mild loss in eachear, by averaging the hearing threshold levelsacross all frequencies. We used the BATOD-approved audiometric descriptor system asrecommended by the British Society of Audiology(BATOD, 2004). Where a child had a cochlearimplant, teachers mostly classified the children asprofoundly deaf in the unaided level options; one ortwo classified as severely deaf and others did notspecify an unaided level.
Ascertaining hearing loss levels: year 2 onwardsIn the second year of the survey, we had theopportunity to ask for more detail about hearing losslevels. So, from then onwards we have asked forspecific readings at each frequency and have
calculated the average thresholds automatically -both for unaided and aided levels. This means thatwe have the capacity to categorise hearing losslevels in more detailed ways where this may beuseful in the future. We have come across anumber of examples where a child technically fallsinto one category but could be seen to fitfunctionally into a different category. For example, apupil who is categorised as severely deaf whenusing the audiometric descriptor formula but isprofoundly deaf in one ear and has a profound lossin the high frequencies in the other ear. There arelikely to be more sophisticated formulas developedover time to take account of functionality. Forexample, Educational Audiologist Russell Brettargues that an 'Articulation Index' based on resultsof a relatively complex formula applied to aidedhearing loss audiograms (Brett, 2003) is an effectivealternative when assessing spoken language accessservices for a school pupil.
However, in line with the BATOD survey, for themoment at least, we continue to use the traditionalaudiometric descriptors when reporting findings bylevels of hearing loss - using unaided levels.
Where did this leave children and young peoplewith cochlear implants?A lot of teachers provided detailed unaidedaudiogram information for children/young peoplewith implants, based on the last unaided readingstaken pre-implantation. A number of teachersphoned to ask for advice where this meant givinginformation that was a few years old - and a sizableproportion gave no threshold information at all.
We consulted with cochlear implant specialists andhad long discussions about the 'common sense' aswell as the technical aspects of the situation. If youview the implant as a very sophisticated hearing aidthen, despite its intended permanency, you wouldstill consider the hearing loss level of an implantedchild as being profound. If the implant isdisconnected, then the child is profoundly deaf.
So, in co-operation with an implant centre, we firstconsidered the option of entering flat, high readingsacross all frequencies, where no thresholds hadbeen provided for implanted children. This wouldhave meant that all these children wouldautomatically be categorised as profoundly deaf.However, we were uneasy about contriving any
Categorising hearing loss for those with cochlear implantsMarian Grimes Research Associate
Achievements of Deaf Pupils in Scotland Project
53955-BatodMarch05 8/3/05 9:18 am Page 11

information, however pragmatic. In particular, wewere aware that a small number of the pre-implantunaided thresholds provided actually put the childwithin the severely rather than profoundly deafcategory. So, it was not right to make theassumption of profound deafness in all cases.
We also considered using the aided thresholds butwe would then need to categorise all children byaided rather than unaided thresholds, which wouldcause all manner of complications.
So the only option left was to simply categorise allcochlear implanted children as a distinct group. Themain disadvantage is that it further splits the wholegroup, thus potentially reducing statisticalsignificance when analysing against a number ofother factors. However, weighing everything up, thisis what we have decided to do, with the expectationthat we will be able to see statistically significantpatterns emerging over time - the benefit oflongitudinal study. So, from 2001/02 findingsonwards, when we show statistics broken down byhearing loss level, we now categorise children as'profound', 'severe', 'moderate', 'mild' and 'cochlearimplanted'. As with so many things, we don'tnecessarily see this as the end of the story, as it'sstill an issue for debate. Watch this space. http://www.education.ed.ac.uk/ADPS
Do visit our website to see basic descriptivefindings, as well as other details about the project. www.education.ed.ac.uk/ADPS
BATOD (2004) ‘Audiometric Descriptors’Information Sheet [on-line]. Available from:http://www.batod.org.uk/ follow articles, audiology,audiometric-descriptors
Brett, R. (2003) 'Allocation of support levels tohearing-impaired children - moving away fromusing audiometric descriptors'. Deafness andEducation International, 5(3), 167-183.
Have you seen the newConnevans Catalogue?Our new catalogue offers an unrivalled range ofproducts, a wealth of helpful information, innovativeideas and practical solutions for deaf and hearingimpaired people.Visit www.connevans.com to view our onlinecatalogue plus extended product information, helpfullinks and useful ideas. Join our mailing list online tokeep up to date with what’s new. Shop online fromour secure website at www.deafequipment.co.ukQuantities of literature are available for distribution – contact customer services
EQUIPMENT FOR DEAF AND HEARING IMPAIRED PEOPLE IN EDUCATION, EMPLOYMENT, THE HOME & LEISURE
CONNEVANS LLIMITED54 Albert Road North, Reigate, Surrey RH2 9YRCUSTOMER SERVICES: 01 737 247571 Text: 01 737 243134 Fax: 01 737 223475www.connevans.com [email protected] www.DeafEquipment.co.uk
53955-BatodMarch05 8/3/05 9:18 am Page 12
creo

©BATOD Magazine March 05 11
The first study of phonological awareness in childrenwith cochlear implants was conducted for mydoctoral dissertation which was supervised byProfessor Usha Goswami at the Institute of ChildHealth. We collaborated with Great Ormond StreetHospital, the Institute of Sound and VibrationResearch in Southampton and many schools andunits in the South of England.
The main aims of the study were to: a) find out if phonological awareness in severely
and profoundly deaf children developed in thesame sequence as hearing children (syllable,rhyme, phoneme);
b) assess whether children with cochlear implantshad equivalent phonological awareness to thatof profoundly and/or severely deaf children whoused hearing aids;
c) investigate whether phonological awarenesswas related to reading in deaf children.
The essential elements of the theoreticalbackground to the study are shown in Figure 1 andsummarised below.� The way words are stored in the mental lexicon
gradually changes during childhood. � Words start off being stored, or represented, as
whole word units but over time the size of therepresentational unit becomes smaller. Thelarger units of syllable and rhyme emerge beforethe phoneme which is the smallest unit.
� Re-organisation of word storage is caused bylexical development and learning to read.
� In hearing children there is a strong associationbetween phonological awareness at the rhymeand phoneme level with reading.
Testing phonological awareness in deaf childrenposes particular challenges. Firstly, in order to besure that the test does indeed test phonologicalawareness and not general language knowledge,the words used in the tests should be highly familiar
to the child. Secondly, we know from past researchthat deaf children are likely to use knowledge of thespelling of words (ie orthographic knowledge) tomake phonological judgements even when picturesare presented. So phonological awareness tests fordeaf children need to assess the extent to whichdeaf children use orthographic knowledge to makephonological judgements. For example, comparethe skills that are required to make a judgementabout the similarity of the initial sounds in the paircomb/cat with the pair queen/kite.
Nineteen children with cochlear implants took part inthe study (mean age 8;4). They were seen twiceover a twelve month period. Two groups of deafchildren using hearing aids were also tested; elevenprofoundly deaf (mean age 9;5) and ten severelydeaf children (mean age 7;4). All the children werecongenitally deaf, they were all rated as good usersof their devices and they all had normal non-verbalreasoning skills. A new battery of computerisedtests was designed to investigate syllable, rhymeand phoneme awareness. Each test required asimilarity judgement (see Figure 2). The child madea choice out of three items as to which item had thesame number of syllables, the same rhyme, or thesame initial phoneme, as a cue item. The words inthe tests were highly familiar and known to beacquired within the first three years of childhood.Each test was designed to examine the extent towhich orthographic knowledge influencedphonological judgements. All words were presentedas simple black and white line drawings. The writtenwords were not presented.
Phonological awarenessDr Deborah James, Newcastle University
Figure 1
Figure 2 Example from the Rhyme TestTrial items are, hair, pear, tie, bow. Participants made theirselection by pressing a colour coded key on a button box. In thisexample, the participant had to choose the item that rhymed withthe cue item at the top of the screen (ie hair). The correct choicein this trial was pear.
53955-BatodMarch05 8/3/05 9:18 am Page 13

7
12 ©BATOD Magazine March 05
The results showed that:� Phonological awareness developed over time in
the cochlear implant users and in the samesequence as that found in hearing children (seeFigure 3). Syllable and rhyme awarenessdeveloped before phoneme awareness. Childrenmade most progress in rhyme awarenessbetween the first and second data collectiontimes.
� The cochlear implant users and the group ofchildren with profound hearing impairment usinghearing aids relied on orthographic knowledge tomake phonological judgements to a far greaterextent than children with severe hearingimpairment.
� The performance of the cochlear implant userswas similar to the performance of the profoundlydeaf children with hearing aids but syllableawareness in the cochlear implant group wasequivalent to the severely deaf group.
� There was no significant relationship betweenphonological awareness and reading after theeffect of vocabulary knowledge was controlled.
Figure 3 Percentage Correct on Phonological Awareness Tasks in theCochlear Implant GroupNote: Scores above 50% were significantly above chance,syllable and rhyme awareness were above chance but phonemeawareness was not.
Implications for PracticeBased on my interpretation of the research findingsand my experience as a speech and languagetherapist, I have summarised the main pedagogicalimplications for those who adopt a phonologicalapproach to language and literacy development.
� Make sure you know the true level ofphonological awareness of the child. If the childis at the syllable level and you are working on astrategy that involves the identification ormanipulation of single sounds then the strategyis not likely to be effective.
� Promote phonological awareness development inthe following sequence; syllable, onset/rhyme,phoneme.
� When working on phonological awareness, usevocabulary that you think the child will know orwill easily learn.
� Use the written form of words to help develop thechild’s understanding of the internal phonologicalunits.
Cochlear Implants International Visit www.whurr.co.uk/Cii/Jump_Fr.htmlISSN: 1467 0100Editor: John Graham, Consultant Otolaryngologist,
Royal National Throat, Nose and Ear Hospital, Grays Inn Rd, London, WC1X 8DA
Deputy Editor: Huw CooperHearing Assessment and RehabilitationCentre, Birmingham, B29 6JD
Assistant Editor: Jonathan Osborne, ENT DepartmentYsbyty Glan Clwyd, Clwyd, LL18 5UJ
Cochlear Implants International is a new journal,published biannually, aimed at all those involvedwith cochlear implants: surgery, pre- and post-operative care, research or manufacture of theimplants themselves. The journal will provide aforum for the exchange of the most recent andrelevant information and ideas concerning cochlearimplants. Work from all the disciplines associatedwith cochlear implants is welcomed.
This new interdisciplinary journal will be of interest toaudiologists, audiological physicians, speech andlanguage therapists, otolaryngologists, nurses,neuro-otologists, Teachers of the Deaf, hearingtherapists, cochlear implant manufacturers andothers involved with hearing-impaired and deafindividuals.
Cochlear Implants International is the official journalof the British Cochlear Implant Group. Members ofBCIG will receive the journal as part of theirmembership.Whurr Publishers, 19b Compton TerraceLondon N1 2UNTel: 020 7359 5979 Fax: 020 7226 5290
Theo, Aaron and Sian with teacher Sarah Tate
53955-BatodMarch05 8/3/05 11:58 am Page 14

53955-BatodMarch05 8/3/05 9:18 am Page 15

14 ©BATOD Magazine March 05
frequency filters were fitted into the lead at thespeech processor end of the connecting cable. Thenew lead was tested and it was found that the rangewas increased to an acceptable level of between 15to 20 metres.
Later speech processors use a higher transmissionfrequency and as a consequence are less likely togenerate radio frequency harmonics in thefrequency region used by the radio microphones,even to the extent that it has not been necessary touse radio frequency filters in the lead in somecases.
Can all Radio Aids be fitted with all cochlearimplant speech processors?Connecting leads or a connecting adaptor areavailable to connect all commonly used FM systemsin the UK to the three cochlear implantmanufacturers’ speech processors.
Successful use of FM systems with cochlear implant speech processors
Elizabeth Wood South of England Cochlear Implant CentreJohn Popplestone Connevans Ltd.
Rationale and Background Cochlear implants and FM Radio Aid systems havenow been in successful use for a number of years.In the past there were problems associated withcombining the two systems and there was thereforea tendency for people to feel that trying to use themwas not worth the potential problems. From anaudiological perspective we need to remindourselves that the microphone used to input soundinto the cochlear implants is very similar to that of ahearing aid and suffers from the same deteriorationof signal to noise ratio over distance. In other wordsif the cochlear implant user is not within a metre ofthe sound source they are going to have difficultiesin distinguishing wanted sounds from backgroundnoise. Providing the user is able to report signalquality, so that any problems that may occur can bedealt with, the use of radio microphones in thesecircumstances can provide the same real benefits asfor hearing aid users.
When radio microphones were first used withcochlear implant systems they were connected tothe speech processor using a simple lead suitablyattenuated for the input socket on the speechprocessor. It was found that the radio microphonesworked with the cochlear implant but suffered fromvery poor range and tended to cut in and out. Aninvestigation was carried out by Connevans Ltd andCochlear UK Ltd and subsequently with Medel andAdvanced Bionics (Boyle P et al 1997).
Understanding the performanceSpeech ProcessorsThe speech processors of multi channel digitalcochlear implant systems generate radio frequencyenergy during operation. This energy is present onthe leads connected to the speech processor andalso emanates from the case of the speechprocessor. Speech processors operate at a rate ofbetween 2.5MHz and 49MHz depending on theparticular system. The speech processor cangenerate frequency harmonics in the frequencyregion used by radio microphone systems. It wasfound that some of the radio frequency energygenerated by the speech processor was present onthe connecting lead. As this was also the aerial ofthe receiver this interference could block the wantedsignal from the radio microphone transmitterresulting in poor range. To solve this, radio
transmitter
53955-BatodMarch05 8/3/05 9:18 am Page 16
©BATOD Magazine March 05 15
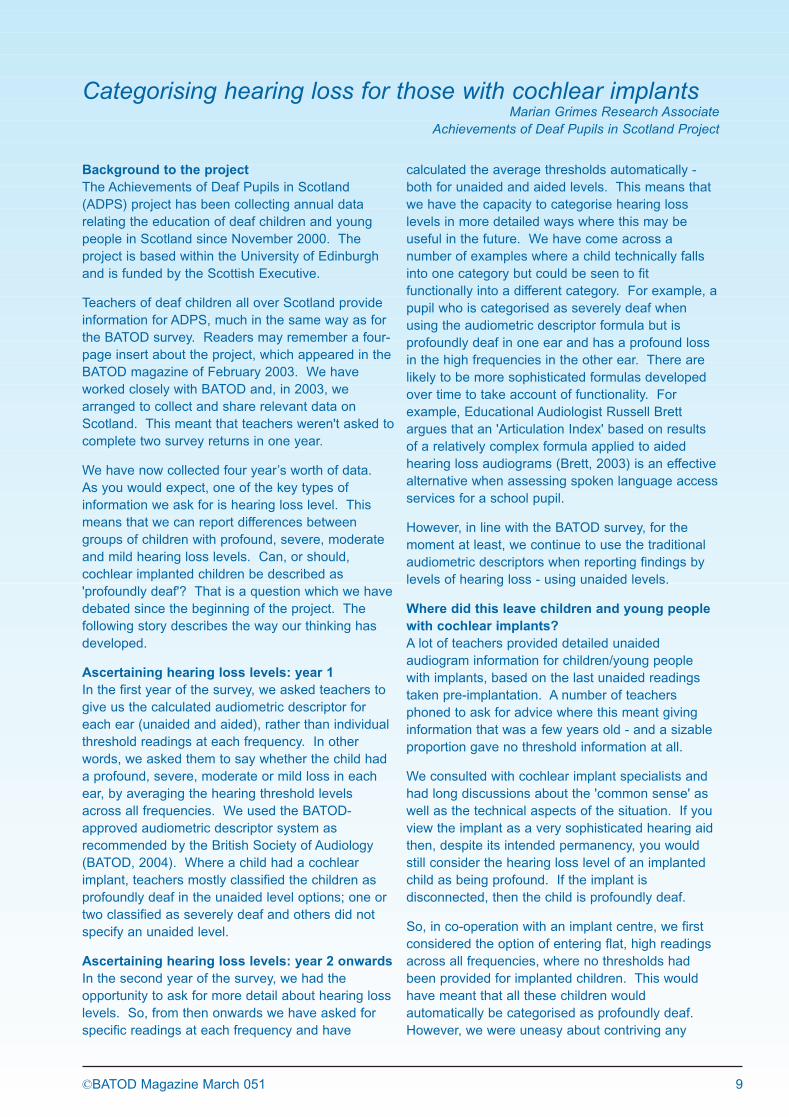
The majority of the children who do not use FM arethose who are in their first year post implant.
Gaining the Benefits of a radio microphonesystemThe following notes are a guide to those who lookafter Radio Aid equipment being used with cochlearimplant speech processors.
The initial set up of the Radio Aid is usually carriedout by the Cochlear Implant centre so that the inputinto the Speech Processor is at the correct level andthe results can be validated. If the level is not set
Research findings from studies carried out at theSouth of England Cochlear Implant Centre (SOECIC)between 1999 and 2005 have establishedcompatibility and benefit for the main UK Radio Aidswith all Nucleus Cochlear Implant speechprocessors (including most recently using thePhonak MicroLink MLxS with the ESPrit 3G).
Research rationaleOlder children and adults who are able to report onsound quality listened to a speech discriminationtask in pink noise for these studies. We also testedthe systems at distances of up to 10 metres tosimulate classroom conditions. An adapted versionof The McCormick Automated Toy Test (Ousey et al1989, McCormick 1997) was used.
Use of FM with cochlear implants in the UKA survey carried out by SOECIC (Wood et al 2000)established that 33% of all children in the UK whohad received a cochlear implant were using an FMsystem. This survey is currently being updated andresults are due to be presented in July 2005.
Radio Aids fitted at the South of EnglandCochlear Implant Centre (SOECIC)January 2005 N=145 children
correctly it will probably be either too low with theresult that the user will not obtain adequate benefitwith the Radio system, or too high with a danger ofsaturating the input of the Speech Processor. Thiswill affect the clarity of the signal which would not beat a comfortable level for extended listening. If theuser reports high levels of background noise whenthere is no input into the microphone of the RadioAid then it is likely that the output from the Radio Aidreceiver has been set too high and requiresadjustment.
All Radio Aid receivers have a muting device thatturns off the audio in the absence of a radio signal.There are occasions when the radio energyemanating from the processor can be sufficient toopen the mute resulting in the user reporting ‘whitenoise’ type shushing noises. The solution is to keepthe transmitter on all the time and to mute themicrophone of the transmitter when the teacher isnot talking to the cochlear implant user. This facilityis built into some systems, on others it can beachieved by putting a switch in the externalmicrophone lead.
Because of the masking effect of the radioemissions from the processor all transmitters shouldbe used on their long range setting. On somesystems the transmission power is already set tothis and cannot be altered.
Fitting considerationsAs with hearing aids, it is important that the settingof a radio aid is validated. This can be done byinformal testing (eg by asking the user to repeatwords at an appropriate distance) and by usingmonitor earphones, by a speech discrimination task(preferably in noise) or by objective testing (eg in atest box).
At the initial Radio Aid fitting at the implant centrewe validate the volume setting by using theMcCormick ATT speech discrimination task and byinformal checking and observation. Work is inprogress in the UK by members of the NDCS FMWorking Party to develop a method of objectivetesting using a test box.
A child must have a stable map and be a reliableuser of their implant before a Radio Aid is fitted. Asan extra piece of equipment is being issued it isimportant that the user can report on faults or anyextraneous noises so that if there are any issueswith interference they can quickly report the problemto an adult. Good lines of communication are vitalbetween the implant centre and local professionals.
53955-BatodMarch05 8/3/05 9:18 am Page 17

16 ©BATOD Magazine March 05
Soundfield FMSoundfield systems are becoming more commonlyused in school, either a classroom amplificationsystem or a portable desktop system. Researchevidence (Wood et al 2002) suggests that thesesystems can give benefit, however it is importantthat the room itself has had some acoustictreatment, otherwise the child will receive a poorcombined signal.
In our experience the following combinations givevarying degree of performance if the distance fromthe sound source is greater than one metre. Wehave rated them in the order of best to worst.� Cochlear implant connected to a Radio Aid within
an acoustically treated classroom fitted with aSoundfield System.
� Cochlear implant connected to a Radio Aid.� Cochlear implant with a personal Soundfield
System directly in front of the user.� Cochlear implant in a classroom fitted with a
Soundfield System� Cochlear implant on its own.
ConclusionsAn increasing number of children with a cochlearimplant are being fitted with an FM system and theyare successfully using the combined system toaccess the curriculum in an educationalenvironment. More training programmes are beingdeveloped to enable professionals to enhance theirskills and increase their understanding of the issuesinvolved in the successful use of FM systems withcochlear implants.
ReferencesBoyle P et al 1997 Compatibility of the Clarion cochlear implantwith the Connevans CRM-220 ENTJournal vol. 76 no 6Ousey et al 1989 The IHR/McCormick Toy Discrimination Test –description and initial evaluation. British Journal of Audiology 23, 245-251McCormick B 1997The Toy Discrimination Test Public Health London 91Wood EJ and Flynn SL 2000 A survey investigating the use of FM Radio Aidsystems and cochlear implant users in the UK19
thInternational Congress on Education of the Deaf
Wood EJ Harriott MM Shann J 2002An investigation into the use of an FM Radio Aidin a classroom/hall with a soundfield system. 6
thEuropean Symposium on Paediatric Cochlear
Implantation
Fitting notes� A young child is likely to need approximately one
year until their ‘map’ is stable, before a Radio Aidis fitted.
� Advice may need to be given with reference tothe ‘best transmitting frequency’ to use.
� It is important to follow the ‘connecting andswitching on sequence’ (this is particularlyimportant when using the Nucleus ESPrit 3G). ✓✓Check the FM system is working.✓✓Switch off the speech processor.✓✓Connect the FM cable to the speech.
processor then the FM receiver.✓✓Switch on the FM transmitter.✓✓Switch on the FM receiver.✓✓Switch on the speech processor.✓✓The sensitivity of the speech processor should
be turned down to a minimum setting to checkthe user is receiving the FM signal, then turn itback to its usual setting. (Lowering thesensitivity effectively reduces the input fromthe speech processor microphone).
✓✓Turn off in the reverse order.� For the Nucleus ESPrit 3G the monitor
earphones need to be switched off on theprogramme used for FM when using the speechprocessor with a Phonak MicroLink MLx orMLxS. (The monitor earphones take power fromthe batteries in ESPrit 3G which can result inpoor performance in normal use). The otherprogramme can be used to check the combinedsignal with the earphones if required).
� If you don’t think the Radio Aid is working tryswitching the processor off and on again.
Elizabeth Wood and John Popplestonewould like to acknowledge the invaluableassistance from all their co-workers.
53955-BatodMarch05 8/3/05 9:18 am Page 18
creo
©BATOD Magazine March 05 17
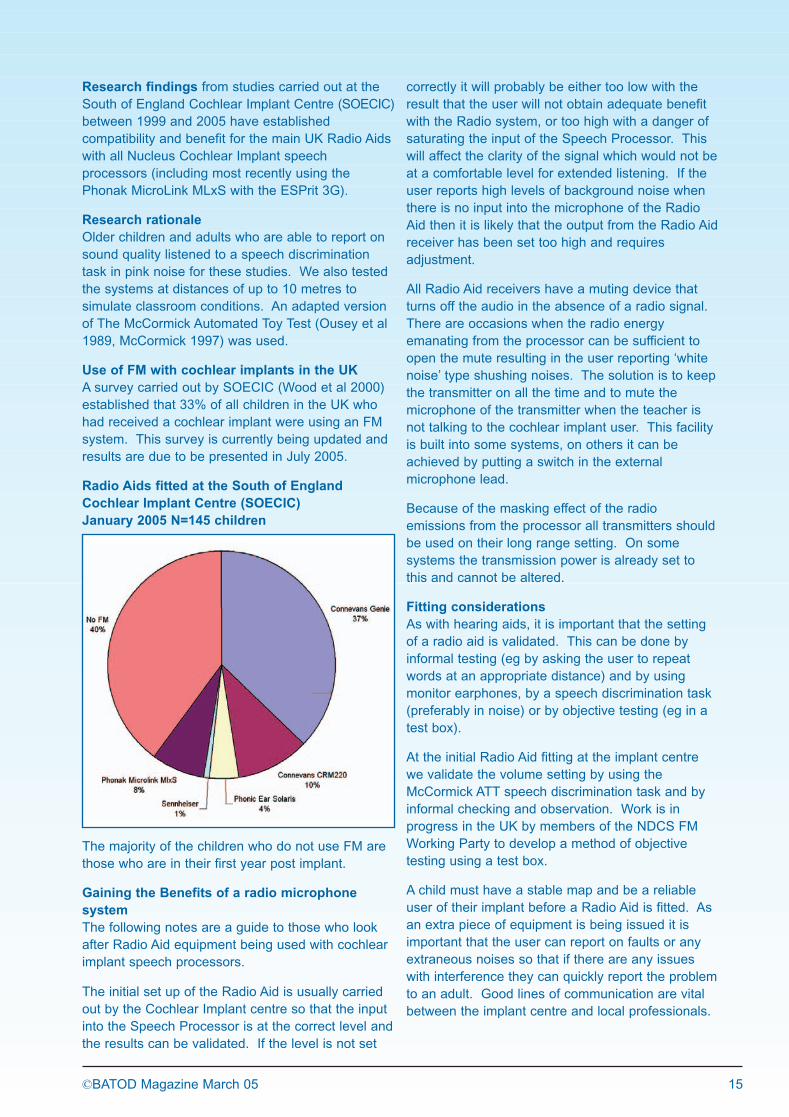
External components of a cochlear implantTroubleshootingIf a problem is suspected with a child's CI then theexternal components of the CI need to besystematically checked and the faulty componentreplaced. If the cables, battery or transmitting coilare faulty then these can be replaced in class, thechild may have a spare, or there may be spareequipment in the school. Should there be a problemwith the processor, microphone or internal devicethen the child's implant centre should be contacted.In systematically checking a CI's external equipmentit needs to be remembered that there may be morethan one faulty component and that the fault may beintermittent.
Checking the batteriesAre they fully charged?Are they correctly inserted into the processor?Is there any corrosion on the battery contacts?Processors may have indicator lights or a displaysymbol to show the charge status of the battery.Some processors can have an audible alarmenabled to indicate when the battery is running out.
Generic troubleshooting of a cochlear implant systemRichard Hughes, Clinical Specialist, Advanced Bionics UK Ltd
microphone soundprocessor
battery
With the number of children with cochlear implantsincreasing, management of cochlear implant (CI)equipment in the classroom is becoming moreimportant. Existing troubleshooting guides for CIsfocus on the reported problems/solutions and are forspecific devices (see final paragraph). In this articlea complementary approach is taken with the focuson systematically checking the components of a CI.This approach has the advantage that therecommendations, though general, are applicable toall CI devices.
Cochlear ImplantsCochlear implants consist of both internal andexternal components. The internal componentsconsist of the implantable stimulator electronics andthe electrode array. Determining if there is aproblem with the internal component of a CI requiresspecialised testing at the child's implant centre.When problems do occur with a CI it tends to bedue to a problem with the external equipment.Therefore, the remainder of the article will focus onthe external components of a CI which are shown inthe diagram below.
transmittingcoil
Checking the microphoneUse listening earphones provided by the implantmanufacturer to test the microphone. Again, indicator lights on the processor can indicatethat the microphone is detecting sounds. If themicrophone is suspected to be faulty, then using adevice specific auxiliary/lapel microphone with theprocessor might confirm a faulty microphone andprovide a short-term solution.
Checking the sound processor Is the processor switched on?Is the correct programme location selected?Is the volume setting correct?Is the sensitivity setting correct?The display lights on the processor can show ifthere is a problem with the electronics of theprocessor or if a programme location has beencorrupted by static electricity.
Checking the cablesAre the cables twisted, frayed or broken?Particular weak points are at the ends of the cablewhere it attaches to the processor and thetransmitting coil. With body-worn processorsanother way to check the integrity of the cable is touse the listening earphones. Listen to themicrophone and check that the signal doesn'tbecome intermittent.
Checking the transmitting coilUse a signal check accessory that is provided by themanufacturer. In some devices, processor display lights andaudible alarms indicate that the coil is not correctlytransmitting information to the internal device.
Checking the whole system - Ling SoundsThe quickest way to see if a CI is working is tocheck that the implanted child can detect or identifythe Ling sounds (oo,ah,m,ee,sh,ss) using auditionalone. In this way the whole system, both internaland external, can be checked. When the test isdone on a regular basis the teacher develops anawareness of a child's typical performance with theimplant and deviations from this can be quicklynoted and troubleshooting initiated.
Troubleshooting guidesFurther information regarding troubleshooting can befound at the following websites:Advanced Bionics deviceswww.bionicear.com/professionals/tools.aspCochlear deviceswww.cochlear.com/149.aspMed-el deviceshttp://download.medel.com/daten/pdf/MKT3029E_r10.pdfLing Sound Testwww.audiologyonline.com/articles/arc_disp.asp?id=728www.ncpublicschools.org/docs/ec/sixsoundtest.pdf
53955-BatodMarch05 8/3/05 9:18 am Page 19

18 ©BATOD Magazine March 05
How can we ensure that implanted children reachtheir potential? Research and case studies fromEurope and America suggest that the early andconstant use of Cued Speech by family membersand professionals can significantly improve thechildren’s ability to benefit from the implant.
Cued Speech and Cochlear Implantation arefrequently described as ‘perfect partners’ becauseCued Speech gives sound-by-sound access tospoken language by visual means, perfect foroptimising language development prior toimplantation and for supporting the child in the earlyyears post implantation.
A French study1
shows that children who had fulland consistent exposure to Cued Speech prior toimplantation performed considerably better in anumber of tests than children brought up aurally orwith French Sign Language. Tests showed that boththree and five years after implantation Cued Speechchildren had significantly better: � perception of words in open lists � speech intelligibility (measured on the
Nottingham scales).
In Spain Cued Speech is the norm in some cochlearimplant centres with several specifically recommendingits use. In addition, the Complemented Oral Model(Modelo Oral Complementada, MOC) project insouthern Spain uses Cued Speech within an oralprogramme and many of the children in theprogramme are implanted (at present they have 20children between 11 and 18 months). The aim is notjust to provide first class support for the children butalso to publish research. The programme has nowbeen running for over twelve years and early resultsare outstanding, with some areas of linguisticdevelopment better than age appropriate.
2
From America Jane Smith writes: ‘For nearly 20years, I have been a communication specialist withdeaf children who have cochlear implants (CIs).The vast majority of these deaf children use CuedSpeech.
Although CIs have been an amazing breakthroughfor the deaf, outcomes differ from child to child.I would not take the chance of denying a child avisual representation of spoken language until I wassure that they were learning everything throughlistening. Cued Speech helps clarify and verify whatis heard; it actually accelerates the learning oflanguage and listening.
Many deaf children who receive CIs perceiveenvironmental sounds but progress in the perceptionof speech is much slower. Deaf children who useCued Speech perceive speech more quickly.
Until recently, most of my students were receivingCIs after age three - after they had acquiredlanguage. I observed that children who used CuedSpeech had a ‘phonological grid’ already internalisedwhen they began to listen with their CIs. They wereable to learn auditorily what they had internalisedvisually already. Progress in learning to listen camequickly because they already had this internal grid ofphonemes. Cued Speech helps children interpretthe sounds they are hearing via electrical stimulationas the same sounds they are seeing through CuedSpeech.
For children aged three and under who learn CuedSpeech at the same time as they get their implant,Cued Speech is also a huge benefit. Cued Speechdevelops an internal phonological model of speechand language that facilitates reading later. The childnot only hears but also sees syllables and stresspatterns. A child can see morphological structuresthat are difficult to hear - plurals, possessives andtenses for example.
After a certain amount of time - which varies for allkids, Cued Speech children learn vocabulary andacademic information through listening alone. Manyparents drop the use of Cued Speech at home(except at bath time or at the pool) but continue tohave their child use it in school in the mainstreamvia a Cued Speech transliterator. This is becauseCochlear Implants have not conquered the obstaclesof noise, distance and the speed and amount ofinformation delivered in an academic classroom.
Most of my CI/Cued Speech kids have advancedlanguage, vocabulary and listening abilities.Examples include: a second grader who receivedthe highest score in her grade on a standardisedstate test in a high-performing elementary schoollast spring and a first grader who is the best readerin her class.
These examples are outstanding but unusual fordeaf children (or any child for that matter). Theirsuccess can be attributed to their innate talent andpossibly more importantly to the use of CuedSpeech with their cochlear implant.’
3
Cochlear implantation and cued speech internationallyAnne Worsfold, Executive Director, Cued Speech Association UK
53955-BatodMarch05 8/3/05 9:18 am Page 20

©BATOD Magazine March 05 19
In England successful case studies includeAlexandra who had very delayed language until herparents started to cue. Over the next two years shequickly caught up and prior to the implant hermother wrote that ‘professionals recognised that herreceptive language with Cued Speech appeared tobe age appropriate and questions were raised as towhether Alexandra might have become sodependent on this form of communication that shemight experience difficulty in adjusting. In fact, thetransition from cueing to fully oral communicationhappened completely smoothly. After as little asthree months, the clarity of her speech improvedsignificantly and other people started to understandher. Cued Speech continued to be valuable inlanguage acquisition for some months to come,reinforcing the links between the language she knewvisually and the new sounds she was hearing. Evennow it is still invaluable in noisy situations, when theimplant is not in use and in breaking down thesounds in words which hearing children also finddifficult!
‘It is now 41/2 years since we learned how to Cueand 21/2 years since Alexandra received herCochlear Implant. Her progress has beeneverything we could have hoped for. Her readingage and vocabulary are both above herchronological age and her personality has becomemore settled. Deafness has ceased to be aninsurmountable problem. The only regrets we haveare that she didn’t receive the benefits of CuedSpeech and her Cochlear Implant much earlier.’
At Alexandra’s twelve month post implantassessment her Teacher of the Deaf wrote: ‘In my30 years experience of working with profoundly deafchildren, I have never witnessed the remarkableprogress that Alexandra and her parents have madethroughout this year, following implant. In myopinion, Alexandra is a little girl who is now totallyoral/aural, in her ability to develop speech andlanguage and shows listening levels which onewould not normally anticipate until at least two orthree years of wearing her processor’.
Why is Cued Speech so successful? Hearingpeople use their knowledge of the sounds of Englishwhen they learn to cue. Deaf children brought upwith Cued Speech work in the opposite way. Theyacquire an internal model of sound-based Englishthrough Cued Speech - even if they can’t hear it.Once the implant gives them access to speechsounds these can be plotted onto the model ofsound-based English they have already internalised.Belgian research - and many case studies -demonstrates that children brought up with CuedSpeech can think in sound-based language.
4
It is this visual access to sound-based language thatenables a deaf child to acquire an understanding ofspoken language without delay pre-implant and alsouniquely primes the child for the acquisition ofspoken language when it becomes available postimplant. As Jane Smith, with her 20 yearsexperience, said: ‘Cued Speech helps clarify andverify what is heard; it actually accelerates thelearning of language and listening’.
By Anne Worsfold with grateful thanks to MaureenBrenton and Pat Cove for their translations of sourcedocuments.
For details about cueing in the UK contact:Cued Speech Association UK 9 Duke Street Dartmouth Devon TQ6 9PYTelephone (voice and text) 01803 832 784Fax 01803 835 311 email [email protected] www.cuedspeech.co.uk
References1 Study produced by Nadine Cochard, Marie-
Noelle Calmels, Geraldine Pavia, ChristineLandron, Helene Husson, Anne Honegger,Bernard Fraysse. Text by Nadine Cochard(Paediatric Unit of cochlear implants -CHU/CESDA Toulouse)
2 MOC website www.uma.es/moc or email Prof. Santiago Torres [email protected].
3 First published in the magazine of the NationalCued Speech Association (USA.)
4 Various research including: Leybaert, J. & Charlier, B. (1996), ‘Visual Speech in the Head: The Effect ofCued Speech on Rhyming, Rememberingand Spelling. Journal of Deaf Studies and DeafEducation, Vol. 1, pp. 234-248.
Cued Speech is a method of clarifying all the sounds ofspoken language visually in real-time, using simplehandshapes in different positions near the mouth toclarify ambiguous or invisible lip patterns. It can be usedwith different spoken languages (in Spain and in French-speaking countries Cued Speech is known as LPC orPC) and within a range of different educational modelsfrom sign bilingual to its more common role supportingoral/aural practices.
Proofreading - a thankless task?Without the support of Alison Weaver, CorindaCarnelley, Gill Wilding, John Edge, Paul Simpsonand occasionally John Bannister the Magazinewould be full of typos, spelling mistakes, unclearsentences and unanswered questions. My sincere thanks to this team for theirefficient use of ‘Track Changes’ in Wordand advice about articles.
53955-BatodMarch05 8/3/05 9:18 am Page 21

20 ©BATOD Magazine March 05
Listening Boxes evolved from Listening Bags, anidea used by various CI Centres and Educationteams to provide parents with structured activities toassist the development of listening skills. The boxesare used as part of the rehabilitation programme forchildren who have had cochlear implants.
What are Listening Boxes?Listening Boxes are sturdy, stackable, portable,easily recognisable and contain specific activities,targeting a range of particular listening skills. Thecontents always include toys to reinforce a particularskill, usually the words to a song or rhyme forparents to sing with their children (remembering theimportance of developing pitch, rhythm andintonation) and a book for shared reading. Thecontents are listed on laminated sheets whichprovide advice and step by step instructions on howto use the items effectively.
Why were they developed?Listening Boxes were developed to build upchildren's listening skills and to give parents specificideas on how to support their child's listeningdevelopment. Each box provides ideas on howchildren can experience sound in a meaningful andfun way. Before parents leave the Centre the ideascontained in the box are explained, along withsuggestions for how the box could be used at home.An underlying aim is to encourage parents andfamilies to spend regular 'quality' time at homereinforcing the skills between visits from centre staff.
When are Listening Boxes used?Listening Boxes are particularly useful at earlystages of development, to demonstrate to parentshow to work with their child on listening skills. EachBox has a specific reference to a listening stage:� auditory detection (knowing there is sound
present); � auditory discrimination (knowing that there are
different types of sound); � identification (knowing what the sound represents
eg doorbell); � comprehension (knowing that words/sounds
have meaning and acting on that). The activities are used to reinforce listening skills ona 1:1 basis whilst integrating meaningful concepts ina fun way.
How are they used?A simple step-by-step laminated instruction sheet isincluded on how to use the Listening Boxes. Thespecific purpose and goals for the box are on thefront. From the front of the box, parents and
professionals can quickly and easily see the specificlistening intent of each box.
A box developed to encourage auditory detectionmay simply have 'responding to sound' and 'turntaking' as its specific goals. The box may onlycontain a drum and a ball with instructions on howthese may be used to develop the skill of auditorydetection. The advice may include;a) banging the drum while encouraging the child to
'listen'; b) soft and loud banging;c) marching to the beat of the drum; d) playing the 'Wake Up' game - taking turns to be
asleep and waking up when the drum is banged;e) throwing the ball when they hear the beat of the
drum; f) playing a simple hide and seek game with the
drum.
A more complex Listening Box may involvedeveloping the skills of auditory identification orcomprehension, including activities in, for example, auditory selection, turn-taking, auditory memory,singing, role play and language building.
A 'loan card' system ensures a record of who hasborrowed the box and the date of return.
ConclusionIt is fun collecting items and making Listening Boxesand the production reaps rewards and goodfeedback from both the children and their parents.The boxes are widely used and they are aninvaluable tool in assisting parents in thedevelopment of their children's listening.
Parent Comments on Listening Boxes:☺ 'Very inspirational.' ☺ 'Interesting with lots of variety.' ☺ 'Inspires parents to have confidence to work
with their child'.☺ 'I like the suggested activity and how it's broken
down.'☺ 'Captures my child's attention.'
Listening BoxesBarb Hay SOECIC
53955-BatodMarch05 8/3/05 9:18 am Page 22

Soundfield and Related IssuesProf Julie Dockrell, Head of the School ofPsychology and Human Development at TheInstitute of Education, gave an update on currentresearch looking at the use of soundfield systems inHertfordshire schools.
The project will report on how soundfield systemscan be used effectively. Preliminary findings fromthe three-year project showed that over 70% ofteachers were using soundfield and almost 70% ofchildren recognised the benefit the system.
To ensure optimum installation it is important thatteachers are consulted about how they use theirclassroom space. It was also clear from the FMGroup that Soundfield systems are used moreeffectively when teachers feel trained and supportedin their use of the system (and its connectivity toauxiliary audiovisual devices).
Cochlear Implants and Personal FM SystemsElizabeth Wood, of the South of England PaediatricCochlear Implant Centre and Riaan Rottier,
Technical Support Specialist at Cochlear Europe,lead a discussion on the verification and evaluationof FM systems with cochlear implants.
Behavioural testing with speech in quiet conditionsand in noise was discussed. An FM advantage of10dB can be measured using soundfield levels of35dB with FM and 45dB without FM. However,testing in realistic conditions will mean the automaticgain control (AGC) engages and the true FMadvantage will be unknown. When a 70dB speechsignal in noise fluctuating to 80dB is presented, theAGC of the implant processor is activated. If the coilsensitivity is turned down to avoid AGC (not UKprocedure), then access to environmental sounds isreduced.
The Group agreed that if ToDs were undertakingelectroacoustic tests in the field for ongoingcomparative purposes (with a stable map and allleads, coil and setting the same) then a 65dB signalshould be used with the implant.
Children's FM Working Group MeetingNovember 2004, chaired by the NDCS
Report by Stuart Whyte, A&ICT Committee
53955-BatodMarch05 8/3/05 9:18 am Page 23
creo
22 ©BATOD Magazine March 05
Children with complex needsChildren referred for assessment fall into three maingroups:1 those who have been diagnosed prior to referral 2 those who are diagnosed with additional
difficulties as part of the assessment process3 those whose additional difficulties only become
apparent following cochlear implantation.
Diagnosis prior to referral These children usually have an identified aetiologyeg a syndrome or collection of identifiable features,or they may have a difficult birth history.
The children may have very clear needs eg dualsensory impairment and an appropriately modifiedassessment protocol will be implemented. Somechildren will have significant developmental delaywhich will also influence the way in which they areassessed.
At Great Ormond Street Hospital (GOSH), some ofthese children may have been attending otherdepartments for some time prior to referral. In anumber of cases the issues are purely medical egcan the child be safely anaesthetised for four hoursto undergo a CI operation? Can the child have a CIand a shunt on the same side of the head?
Those who are diagnosed with additionaldifficulties as part of the assessment processA surprising number of children continue to comethrough for assessment with very little priorinvestigation beyond an initial assessment ofhearing loss.
Once referred, these children will have an in-depthmedical/aetiological work up and this may throw upan unexpected diagnosis. For example most of thechildren on the GOSH Cochlear Implant Programme(CIP) with Usher syndrome (significant hearing losswith gradual loss of peripheral vision, leading totunnel vision) were diagnosed as part of the CIassessment process.
As most teams are now assessing very youngchildren, it is rare for a child to arrive with adiagnosis of autistic spectrum disorder which tendsto be identified at a later stage. However a numberof these children are picked up during the secondstage of assessment with speech therapists, clinicalpsychologists and Teachers of the Deaf.
Those whose additional difficulties only becomeapparent following cochlear implantation
Many children are now being implanted at aroundtheir second birthday or even younger. It can beextremely difficult to pick up children with emerginglanguage or communication disorders at this youngage and often these will only become apparent later.
CIP professionals now have greater experience ofwatching children develop through the system so weare getting better at spotting the warning signswhich may prompt us to refer on for furtherspecialist assessment and enable us to counselparents regarding the likely range of outcomes.
I find one of the most difficult issues to get acrosswhen counselling parents regarding expectations ofcochlear implantation is the difference betweenproviding a child with an improved range of soundsensations and enabling them to make sense of it.Cochlear implants are very good at providingdetection of sound across the normal frequencyrange of speech but interpretation andcomprehension of this auditory information isanother matter entirely. This is usually the primaryissue when deciding on a recommendation to offer acochlear implant.
Ultimately, having a diagnosis or clear understandingof a child's additional needs may help us to makethis decision, based on our known outcomes. Wehave certain clear predictors of outcomes egdevelopment of pre-linguistic skills, earlydevelopment/cognitive functioning, which apply to allchildren. In addition to this we must take intoaccount the way in which the child's additionaldifficulties may have affected their development; forexample a deaf-blind child will probably present with'developmental delay' but we need to assesswhether the child has made - or is capable ofmaking - the degree of progress that would beexpected from a child suffering from a high level ofsensory deprivation. Sometimes we find thatchildren are much more capable than had beenpreviously supposed.
Our results show us that some children with similaraetiologies tend to show similar outcomes. Forexample young 'Usher' children often progressslowly in the initial period post-implant, particularly interms of the development of their expressivelanguage skills (sign as well as oral) but may wellcatch up later. (This is possibly linked to delayed
Cochlear implants in children with complex needsAlex Wheeler Great Ormond Street Hospital
53955-BatodMarch05 8/3/05 9:18 am Page 24

©BATOD Magazine March 05 23
motor milestones/myelination). We find that childrenwith Waardenburg's Syndrome are more likely todevelop an additional language disorder followingimplantation.
More controversially, it is our experience thatchildren on the autistic spectrum (but possiblyexcluding Aspergers) do not make much progresswith learning to use the sound information providedby a cochlear implant, even with aided thresholds at35-40dBA. It is likely that they have an associatedauditory processing disorder. However other implantprogrammes may have different experiences.
'Quality of Life' is a much debated issue. Should wesometimes implant children who are multiplyhandicapped, for whom the development of orallanguage skills is not a realistic outcome but whomight benefit from enhanced environmentalawareness and an increased sense of'connectedness' with the outside world?
With a severely disabled child there is always thedanger that the hearing loss is seen as somethingwhich can be 'fixed' by a cochlear implant whenother disabilities are untreatable. These families areoften inundated with information from a wide rangeof professionals, many of whom will not have directexperience of deafness. Ultimately all thoseconcerned with the child, families and professionals,have to decide whether a cochlear implant is likelyto enhance the child's quality of life or will simplyprove an additional distraction, taking time andresources from other areas of the child'sdevelopment for very little benefit.
In conclusion I believe it is very important not tomake assumptions about what children with complexneeds are able to achieve both with hearing aidsand potentially with a cochlear implant. This grouphas a right to an assessment which defines andthen takes into account particular abilities anddisabilities and seeks to provide an objectivejudgement on the likely balance of benefit. Inpractice this is one of the most challenging tasksthat I have faced in my career to date.
Bringing teenagedeafblind cochlear implantusers together
Louisa Booth, Advanced Bionics UK
Sense, the organisation for deafblind people, hascollaborated with The Ear Foundation and throughthem with cochlear implant centres across the UK,to bring deafblind teenagers with cochlear implantstogether for the first time. It is tough for deafteenagers to acknowledge increasing visualdifficulties, so we were pleased to see teenagers,accompanied by family members, attending from asfar afield as Belfast, Aberdeen, Nottingham andLondon. Two young deafblind adults, Emma andClare, from the UCL cochlear implant programme,also attended to act as role models.
Connor, from Belfast, has KID Syndrome and theother teenagers have Usher Syndrome and theyface the knowledge that although they can seesomething at present, their vision may deteriorate.It was therefore great for them to meet Emma andClare, who talked honestly and enthusiasticallyabout work, social life and their extensive travels.Emma, asked what she liked best about her implant,thought it was probably the fact that it had saved herlife. One night, while she was travelling alone, in SriLanka, she was walking back to her hotel andsimply did not see it. She walked straight past thehotel, down a road that led into the wilds and thensuddenly heard the noise of someone shoutingbehind her. The sound made her turn and noticethe hotel she had missed. As she talked, horizonsopened up for the teenagers and, indeed, for all theadults. Deb Wilson, from The Ear Foundation, andLouisa Booth, from Advanced Bionics, then led adiscussion amongst the teenagers. What becameincreasingly clear is that whilst, understandably, theparents were concerned, the teenagers themselveswere keen to face the world, preferablyindependently.
The day was sponsored by Advanced Bionics,Cochlear and MedEL and also by Pizza Express,who generously donated a room to meet and lunch,thus giving the teens a taste of ordering food in arestaurant. After lunch there was a London Busride, a walk along the Thames and a trip on theLondon Eye. Altogether, it was a really good dayand we urge anyone working with a teenagecochlear implant user with visual difficulties tocontact Sense, The Ear Foundation or AdvancedBionics about the next meeting (contact details inopposite column).
Visual difficulties? Make contact...
Advanced Bionics UKTel: +44 (0) 1223 847 888 Fax: +44 (0) 1223 847 898email: [email protected] www.bionicear-europe.com
The Ear FoundationTel: + 44 (0)115 942 1985 ( V&t) Fax: +44 (0)115 924 9054 email: [email protected] www.earfoundation.org.uk
SenseTel: +44 (0)20 7272 7774 Text: +44 (0)20 7272 9648 fax: +44 (0)20 7272 6012email: [email protected] www.sense.org.uk
53955-BatodMarch05 8/3/05 9:18 am Page 25

24 ©BATOD Magazine March 05
Over the last five years Mary Hare has seen a rapidgrowth in the numbers of pupils with CochlearImplants entering year 7 and in those who areimplanted whilst they are at the school, up to andincluding year 13.
On entry, some pupils have long experience ofcochlear implant use. The level of supportcontinues and sometimes includes counsellingduring the re-implantation process. A late decisionto have an implant is often after many years ofconsideration or it may be a decision made as theresult of a sudden or gradual deterioration inhearing. Other pupils make the decision afterseeing the success of their peers eg in use of thetelephone. We also offer support to pupils and theirfamilies when a CI is not recommended.
Currently, 30% of the school population have CIs -a total of 66 pupils from thirteen centres across theUK and one centre in Australia!
As an oral school the effective use and managementof personal and educational amplification isfundamental to our philosophy and teaching. Theuse of a cochlear implant is regarded as just anothertype of personal amplification by both staff andpupils.
Whilst the development of individual listening skillsis crucial, we also focus on the skills of listeningwithin a group and this is something that all teachersof the school promote in their teaching style.Additional help in this area is the focus of two CIgroups which meet weekly.
How audiological needs are met� All staff are familiar with the range of cochlear
implant types and their appropriate managementeg checking function, battery management etc.
� Regular updates are provided through staffmeetings.
� All staff have copies of the safety guidelinesproduced by the BCIG. Risks are assessed andappropriate action is taken eg all CI pupils havea huggie or an earmould to secure their implantduring PE.
� The Audiology team continues to assess CIpupils in conjunction with the CI centres.Management of the non-implanted ear is just asimportant as that of the implanted ear.
� Form teachers retain information on the type ofimplant and CI centre in an Audiology file.
� Form teachers have a checking kit ie signalchecker and monitor earphones.
� Group hearing aids are adapted to allow directinput into the system. The adapted interfacemakes use of the direct input facility on the CIand a lapel microphone.
� Spare parts and accessories are kept stockedand replaced as used. Each centre is asked tosupply spare external parts to be kept at school.
� At each centre we have a named person as apoint of reference.
� Liaison and exchange of information with implantteams through telephone calls/emails/ teamvisits.
� Continued information exchange with the pupils'families.
How speech and language therapy needs are met� Collaborative work with audiology eg listening
groups, sharing reports. � Collaborative work with CI teams on planning
eg on target setting following assessment.� Cochlear implant groups for different language
levels but based on developing listening skills.� All sessions begin with a warm up activity which
includes the Ling five sounds and activities toidentify individual sounds, minimal pairs etc.
� Copying intonation patterns and emphasis,deriving meaning from intonation patterns, workon dynamic range of voice, meaningful sentencecompletion, collecting information around thegroup in order to solve puzzles etc.
� Individual therapy for some pupils as individualneeds require eg if there are additional needssuch as speech dyspraxia, specific work ongrammar or rate of speech, voice pitch ordynamic range.
As the pupils are teenagers the approach is verymuch one of partnership. Older pupils will managetheir own spare parts for their CI and inform theAudiologist when replacements are required,thereby fostering independence. Appointment timesfor listening groups are flexible to allow for othercommitments eg music lessons.
The pupils effectively counsel and support otherswho are considering having a cochlear implant.Such pupils attend a CI group session and have theopportunity to question the group and participate.This allows them to see that work has to continueafter a CI and what is possible.
In partnership with the CI centres, we recognise anddiscuss with pupils that there is no guarantee ofsuccess. However, staff members are committed tohelping each pupil achieve his or her maximumpotential whether their personal amplification isthrough a CI, hearing aids or a combination of both.
Working with pupils with CIs in an oral environmentPat Tufnell, Vivien Ogg Mary Hare Grammar School
53955-BatodMarch05 8/3/05 9:18 am Page 26

©BATOD Magazine March 05 25
Adolescence is such a time of change and transitionand we need to hold in mind the aspects of theyoung person that are still rather child-like and thosethat have the maturity of a young adult. Theseaspects fluctuate repeatedly throughout theassessment period and the progression from a childand family-centred to an adult-oriented healthcareservice. Importantly, we recognise that hearing loss,cochlear implants and transition in healthcare areonly part of the wider transition from dependent childto independent adult.
The Birmingham Children's and the Midlands AdultCochlear Implant Programmes services for youngpeople have developed to meet the needs of agrowing population of teenagers who were giventheir cochlear implants as children as well as thoseyoung people who are referred to the teams asteenagers. The emphasis is on joint team working.The services are integrated into the multidisciplinaryteams of the two programmes to ensure anassessment and transition process that is ageappropriate, developmentally appropriate andcomprehensive. This flexible approach, involvingstaff who work on both programmes, takesdevelopmental and psychosocial readiness intoaccount and links to other social transitions in theyoung person's life to provide continuous levels ofcare. Emphasis is on young people themselvesbeing increasingly involved in the planning anddelivery of the service according to theircommunication, social and cultural circumstances.
Key elements� Members of staff with particular experience in
working with young people take the role of keyworkers.
� Dedicated adolescent-friendly environments witha range of appropriate resources.
� Young people themselves are increasinglyinvolved in the planning and delivery of theservices according to their own perspectives,
communication, social and culturalcircumstances.
� Comprehensive adult assessment servicesenabling the young person to make informeddecisions with appropriate support from carersand team staff.
� Scheduling appointments and surgery to takeinto account the young person's educationalcareer.
� Provision of planned therapy programmes tomeet the individual needs of each young person.
� Addressing needs and providing support forparents/carers whose role is evolving at this timein the young person's life and health care.
� Offering psychosocial support for the youngperson and family members in relation toemotional well being.
� Promoting functional communication and lifeskills through discussion and real-lifeexperiences.
� Educational and social events with our teenagegroup.
� Active encouragement and support for the youngperson to self-advocate and to learn to takeincreased responsibility in decision making andfor their own clinical healthcare.
� Mediation between parents/carers and the youngperson with issues surrounding cochlear implantuse.
� Liaison with local support professionals andagencies with reference to further education,employment and lifestyle issues.
� Continuous programmes of care with a seamlesstransition to adult services.
For further information, please contactEileen McSporran or Kate HanveyBirmingham Children's Cochlear Implant ProgrammeAston Academy of Life Sciences, Aston UniversityBirmingham B4 7ETTel: 0121 204 3830 Fax: 0121 204 3840email: [email protected]
Growing Up, Moving OnEileen McSporran
Birmingham Children's Cochlear Implant Programme
Checking Coichlear Implants and hearing aids at Mary Hare School The Group Hearing Aid adapted for Cochlear Implantusers at Mary Hare School
53955-BatodMarch05 8/3/05 9:18 am Page 27
creo

26 ©BATOD Magazine March 05
The management of children with cochlear implantswithin any special school or unit involves managingrelatively large numbers of children with differingneeds. This requires organisation, communicationand negotiation with teaching and support staff andimplant centres. At RSD Derby we have theadditional factors of residential care staff, severalimplant centres and the delivery of the curriculum inBSL.
We have nine children with cochlear implants and adiverse group in terms of age, ability (from the veryable to those with additional learning difficultiesincluding autistic spectrum disorder and specificlanguage difficulties), social and emotional needs,attitude to implant, age at implantation, length oftime post implant and benefits gained from theimplant.
In many ways the management of a child with acochlear implant in school is no different from themanagement of a child with hearing aids. Morepeople are involved with the child so communicationis more important and there are a lot moremeetings! The practical issues of checking,promoting independence in management by thechild and prompt repairs remain the same. Thecrucial difference is that of the child's greatersensitivity to sound and different auditorydevelopment needs.
Practical issuesLarge numbers and a residential situation bringadditional practical issues.� Processor serial numbers need to be noted -
especially with the ear level processors whichcan come off so easily and all look the same.
� Well labelled spares available in school andresidence (many look the same but are not).
� Efficient systems for fault reporting within schooland good follow up with the many implantcentres need to be established.
� Communication with parents needs to be efficient.
Auditory developmentWhere the curriculum is delivered in BSL, theattention to development of auditory awarenessneeds an additional focus and individual tailoring foreach child. Again, communication is the key.Communication between the families, speech andlanguage therapists, audiologists and Teachers ofthe Deaf in school and on the implant teams - not aneasy task!
In the Nursery and Key Stage 1 curriculum,appropriate listening situations can easily be wovenin to the lesson plans and the rest of the classroomactivities. Both Deaf and hearing staff are in everyclass. Involvement of educational audiologist andSLT in the classroom ensure all potential listeningsituations are exploited.
At Key Stage 2 and beyond, when the demands ofthe curriculum become more prescriptive, the needsof the child with a cochlear implant need to beremembered and included in the planning. Everyone working with the child needs to know theirsensitivity to sound and need for varied and relevantspoken language as well as BSL. Listeningopportunities outside the classroom need to beprovided.
The child's attitude to the implantChildren’s attitudes to the implant can varytremendously and are often dependent on thebenefits they feel it gives them. Within our groupthere is a child accessing mainstream Frenchclasses who is extremely distressed by anyprocessor problem, a child who has progressed towearing the harness and processor but will nottolerate the coil on her head and a child who hastotally rejected the implant and is back with ahearing aid. Each situation needs to be carefullymanaged in conjunction with the child's family andimplant centre.
At the end of the day we are dealing with children.They will always come up with a new way to test ourmanagement of any situation. Would we have itotherwise?
Management of cochlear implants within a specialschool where the curriculum is delivered in BSL
Frances PyeEducational Audiologist, RSD Derby
Maastricht (The Netherlands)
53955-BatodMarch05 8/3/05 9:18 am Page 28

53955-BatodMarch05 8/3/05 9:18 am Page 29

28 ©BATOD Magazine March 05
In the light of a small amount of research and inorder to support teenagers with cochlear implants ina social setting, Nottingham Cochlear ImplantProgramme, in collaboration with the EarFoundation, runs residential programmes during thesummer. Young people have the opportunity tomeet and make new friends in a social setting.
These programmes are divided into three ageranges, 11-12 years, 13-14 years and 15-16 years tofit in with appropriate age divisions within theeducation system and to allow for maximumintegration within the age ranges.
The courses are of three days duration with a two-night residential stay. Activities are organisedaccording to the needs of the individuals attendingand include educational and recreational elements.Each course has a theme and the activities arearranged around the theme. For example in 2004one group had tennis as its theme. Focus of thesessions included gaining tennis skills, team workand group co-operation. Activities on this coursealso included going for a meal in a local restaurantwhere the individuals had to order, eat and pay fortheir own meal as well as behave appropriately in apublic place. A further activity to encourage thedevelopment of social skills was an expedition intoNottingham City Centre. Participants were dividedinto small groups and had three tasks to complete inthe centre; the purchase of a drink, the gathering ofinformation with a view to purchase a mobile phoneand to find out what was showing at the cinema andthe cost of tickets. A session on audiology wasarranged to inform the Teenz about the technologyof their cochlear implant and provide up to dateinformation on the accessories available to them.One of the surgeons from the Nottinghamprogramme spoke to the young people about thesurgery itself. All the teenagers were very interestedin how the implant got into their heads, how it worksand they asked some very detailed questions, quiterightly. For many teenagers their parents made thedecision about implantation when they were young.The teenagers need to understand the technologyand its risks themselves and come to own thedecision for themsleves.
One of the main aims of the course is to provide apeer group for these Teenz with cochlear implants,many of whom are educated in a mainstream settingand may never see another deaf teenager on aregular basis.
Living together for three days allows friendships todevelop - email addresses and phone numbers areexchanged at the end of the course. Feedback fromthe Teenz themselves indicates the value of the
courses. Approximately 80% of the participantsreturn for a second course and the friendships whichbegin on the summer programmes continuethroughout the year.
Teenz UnitedFive times each year Teenz United meets. This is aSaturday meeting to encourage teenagers withcochlear implants to get together. The name waschosen by the Teenz themselves. Meetings are heldat the Ear Foundation in Nottingham and also atoutside venues. In previous years meetings havebeen held in London, usually in January and inBirmingham. On these occasions, Teenz from otherprogrammes have the opportunity to travel to thevenue with their group and meet up with otherteenagers with cochlear implants from elsewhere inthe country. This provides the opportunity for theTeenz to meet and make new friends and again thecontacts are generally maintained. Activities onthese days are aimed at giving the Teenzexperience of an activity they may not have had theopportunity to experience eg bridge swinging andcanoeing, whilst encouraging discussion betweenTeenz about the issues which matter to them.
Teenz United produces a magazine three timeseach year aimed at keeping the Teenz informed oftechnology, activities and forthcoming events. Thismagazine is distributed to all who have attended theEar Foundation, each cochlear implant centre andthe manufacturers.
Attendance on the Summer residential programmesand at Teenz United Saturdays is open to all Teenzwith a cochlear implant regardless of where theywere implanted. Professionals wishing to supportthe group are also welcomed. Contributions to theTeenz United magazine are welcomed from Teenzwherever they live and at whatever level they wishto contribute. email [email protected]
Working with teenagersElizabeth Beadle
Teacher of the Deaf/Young people's coordinatorNottingham Cochlear Implant Programme/The Ear Foundation
fun at the launch of the ci-4teenz website
53955-BatodMarch05 8/3/05 9:18 am Page 30

A website providing up-to-date and independentinformation about cochlear implants for teenagers went on-line in September 2002. It was a multi-centre project involving teenagers from Nottingham,Oxford, St Thomas’ and UCL Cochlear ImplantProgrammes. Teenagers need accurate, teenage-friendlyinformation about cochlear implants. Furthermore, sincethey are often geographically isolated, and face pressurefrom peers without implants, hearing about otherteenagers with implants is important. The teenagers’website was created to meet these needs. (Fig.1)
The objective of this study was to establish whether the website is being used, and by whom, and to evaluateits effectiveness as a means of conveying information toteenagers. Particular consideration has been paid as towhether teenagers themselves enjoyed using it and foundthe material interesting, accessible and helpful.
MethodCochlear implant centre professionals, educators, andteenage cochlear implant users from across the UnitedKingdom were mailed a questionnaire consisting of openand closed questions to ascertain website use and value.Information was also collected from website administrationdata.
ResultsWebsite administration data indicated that in the yearsince launch in September 2002, the website wasaccessed by teenagers, their families and educators via computers in North America, mainlandEurope and the United Kingdom. As of October 2003, the website had received over 58,000 hits.
Fifty-six questionnaires were returned, including 25 fromteenage cochlear implant users aged between 10.5 to 17years, 1 from a 15 year old considering implantation, 1 from a 12 year old hearing sibling and 29 from adultsworking with teenagers. The majority (40/56) hadaccessed the website between 1 and 5 times, while 13had accessed the site over 5 times. All except onerespondent liked what they saw. The teenager who gavea negative response nevertheless commented that certainsections of the website were interesting, and had enjoyedreading other people’s views and how they felt.
The returned questionnaires indicated that teenagers: • enjoyed using the website• were comfortable with its interactive content • found the material accessible and informative• used the site for teaching purposes, to explain
to friends, family and teachers about deafness and cochlear implants
• were glad to read about the experiences of peers with cochlear implants.
Adults commented that the site also had a wider appealto younger children and some adults who appear to beattracted by the vivid graphics used to convey complexinformation without undue reliance on the written word.
Website preferencesRespondents were asked to identity their favourite sectionof the website, the section they did not like and the mosthelpful section of the website. Responses can be seen infigures 2 (teenagers) and 3 (adults). Data appearsincomplete because 17/22 teenagers did not identify anyof the website as disliked, while 7/29 adults said they liked everything.
What is your favourite bit of the website?
Evidence from Fig.2 and 3 suggests that the section ‘Who wears a cochlear implant?’ (Fig.4) was thefavourite for both teenagers and adults.
Typical comments from teenagers on this section include:
Adults were also interested in the individual experiences, saying for instance:
What bit of the website is most helpful?
‘Living with a cochlear implant-Fact Files’ (Fig.5) wasmost helpful to both groups, with ‘How a cochlear implantworks’ coming a close second for the teenagers.
The teenagers liked ‘Living with a cochlear implant’because:
Adults commented:
The teenagers, who are already experienced implantwearers, liked ‘How a cochlear implant works’ (Fig.6)because:
What bit of the website don’t you like?Most respondents gave no answer, stating they liked it all.One adult had difficulty accessing News and Views from ahome computer, while 4 teenagers just found it ‘notinteresting’, although 4 others chose it as their favouritesection.
ConclusionTeenagers use the www.ci-4teenz website to increasetheir own understanding of their implant and also toexplain things to friends and family. Those isolated inmainstream settings with no deaf peer group find thechance to read about the experiences of others especiallyrewarding. Adults find the website useful with both deafand hearing students for teaching and counsellingpurposes, and as a tool to support the national curriculumand GCSE science. We conclude that the website isfulfilling its brief and meeting a need.
Our thanks to the teenagers, families, educators and clinicians who took part in this project. We have appreciated their whole-hearted enthusiasm and support. Thanks also to The Ear Foundation for hosting the teenagers’meetings and to Advanced Bionics for their financialsupport.
www.ci-4teenz.comElizabeth Beadle
1, Louisa Booth2, Rachel England1, Sarah Evans2, Wendy Horler3 and Pete Sedgwick4
Fig.1 Home Page
Fig.2 Teenager Website Preferences
Fig.3 Adult Website Preferences
Fig.4 Who wears a cochlear implant?
Fig.5 Living with a cochlear implant – Fact Files
Fig.6 How a cochlear implant works
53955-BatodMarch05 8/3/05 9:20 am Page 31
creo

30 ©BATOD Magazine March 05
In the summer of 1997 the Centre developed aprogramme to support adolescent cochlear implantusers. This population is too old to be supportedwithin a paediatric environment but still needsregular one-to-one intervention and intensive schoolsupport. By providing a specialised service for thisage group, the Manchester Programme is able tooffer the support necessary for these cochlearimplant users to gain maximum benefit from theirdevices. A total of 96 young people are supportedby the adolescent cochlear implant programme.
Criteria for referral to the adolescent programmeCriteria are selected according to evidence-basedpractice and experience. They are set to ensurethat patients who receive a cochlear implant aremost likely to obtain benefit from the device. Noneof the criteria outlined below exclude patients withadditional physical disabilities or learning difficulties.
For adolescent patients, it is important that thepatients themselves are involved at every stage ofthe assessment process and receive all of theinformation they need to reach their ownconclusions about the cochlear implant as apotential option for them.
The Adolescent Cochlear Implant Programmeaccepts referrals for assessment of patients over theage of 10 years who are still receiving support froman educational department or school and fit into oneof the following groups.� Patients who were born with hearing and have
recently acquired a profound hearing loss. Achild with a suspected hearing loss followingmeningitis should, of course, be referred forassessment immediately so that cochlear implantsurgery can be fast-tracked in the event of anyossification of the cochlea.
� Patients who have had some benefit fromappropriately fitted hearing aids in the past butwhose hearing has deteriorated to the pointwhere powerful hearing aids are no longerhelpful.
� Patients who were born with a profound hearingloss, have received some benefit of spokenlanguage learning through consistent use ofappropriately fitted amplification but who mightreceive significantly more auditory informationfrom a cochlear implant.
� Additional factors which need to be consideredas part of the evaluation include the patient'smode of communication in the homeenvironment and an educational setting where
the curriculum is delivered through speech,evidence of auditory processing and learningthrough oral/aural communication and supportservices in place for the patient post-implant.
� MRI scan indicates that there are no radiologicalcontra-indications and that the patient’s cochleais suitable to receive an electrode array.
Post Implant careThe aim is to minimise the period of time betweenthe adolescent receiving their implant and the initialprogramming session. The initial programmingsession is offered 10-14 days following surgery.Patients are offered an initial series of fourprogramming and habilitation appointments over aperiod of two to three weeks, with furtherappointments as required. Appointments are offeredon a twice monthly basis for the first three monthsand monthly for the following three months, withfurther support as agreed with the implant user.
The habilitation package is tailored to the individualand offers regular appointments at the implantcentre, outreach visits to home, school or college toliaise with local support professionals and provisionof training and information to schools/colleges asrequested. Training and support is also provided onuse of assistive listening devices with the cochlearimplant and using the telephone. The habilitationpackage is customised to take into account theindividual needs and preferences of eachadolescent. The aim is to encourage the individualto exploit the potential of their equipment and toadvise on techniques to develop auditory processingskills. Specific activities are provided for practiceand carryover.
Adolescents are also offered the opportunity to meetand share experiences with other adolescent implantusers on the activity days run by the programme.Previous outings have included ten-pin bowling, atrip to the BBC Manchester news studios, an AfricanDrumming workshop and an art workshop.
Audiological appointments are offered to adolescentsat 3, 6 and 9 months within the first 12 months,followed by 18 months and then at 24 months andannually following.
On transition to the adolescent programme from thepaediatric programme, local services are contactedand offered support and training to suit their needs;this may include INSET to the new educationalplacement.
Manchester adolescent cochlear implant programmeChristine Anderson
Co-ordinator Manchester Adolescent Cochlear Implant Programme
53955-BatodMarch05 8/3/05 9:20 am Page 32

©BATOD Magazine March 05 31
Cochlear Implants - aguide for families A new booklet from The National DeafChildren's Society
Teenage programme atSouthampton
Sarie CrossWorking with teenagers can be a joy and achallenge. The South of England Cochlear ImplantCentre (SOECIC) is a combined adult and children'sprogramme and we see deaf children and adultsfrom eight months to eighty years of age. Webenefit enormously from dealing with clients of allages as it helps to shape the ways in which wemeet the needs of all our implant users. At theSouth of England Cochlear Implant Centre we haveforty young people, aged between 13 and 18, withcochlear implants.
There are four groups of teenagers at SOECIC.Young people who:• were implanted as young children and are now
adolescents• would not have been considered suitable
candidates for a cochlear implant when they were younger but changing criteria in respect of degree of hearing loss now means that a cochlear implant may be beneficial
• have progressive hearing losses which have deteriorated to the level such that an implant has become appropriate for them
• have been deafened suddenly.
The first three groups will have had someexperience of deafness and the deaf world, unlikethe final group. This group may experience a greatrange of feelings and have specific needs in comingto terms with their deafness, as well as undergoingthe operation and rehabilitation for a cochlearimplant.
We recognised the challenges that working withthese young people can pose and we thereforeintroduced protocols and procedures to meet theirchanging needs and attitudes.
One of our aims is to ensure that we are giving theyoung people the opportunity to manage their ownneeds in relation to the cochlear implant. The youngperson is encouraged to increase their knowledge oftheir hearing loss and to manage their ownequipment. All of the young people have theopportunity to attend at least part of the appointmentwithout the presence of a parent and sign languageinterpreters are provided where appropriate.
A peer group is very important in the teenage yearsand SOECIC invites the young people to attendsocial activities. We join with the nationalorganisation Teenz United for an annual outing andwe also have a social event for teenagers atSOECIC. Additionally, a newsletter is sent out twicea year, which includes contributions from the youngpeople.
The NDCS has produced a brand new booklet forparents - ‘Cochlear Implants - a guide for families’.
It has been written, with support from the EarFoundation, to give families clear, balancedinformation about cochlear implants, at the pointwhere they are making a decision to go ahead withthe assessment.
The first half of the booklet is a factual introductionto cochlear implants and an overview of theassessment process, surgery and follow-up care.Although the booklet is an overview, families whowant to do more research are given contacts andrecommended website links to find out more.
The second half of the booklet features families'stories, in their own words. Families explain howthey felt about the assessment process and thesurgery and how they came to make the decisionabout whether or not to go ahead. They alsoexplain more about their child's life with an implant.The booklet has been awarded the Plain Englishcrystal mark from the Plain English Campaign.
The book will be available from the end of March.If you wish to be put on our mailing list for a copy,email us at [email protected], order on-line atwww.ndcs.org.uk or write to us at:Information teamNDCS15 Dufferin StreetLondonEC1Y 8UR
The booklet is free to families and professionals.Professional ordering more than three copies willasked to pay a small postage charge. Pleasecontact NDCS for more details.
53955-BatodMarch05 8/3/05 9:20 am Page 33
creo

32 ©BATOD Magazine March 05
implants under this protocol and the team ismonitoring the outcomes closely.
The Cochlear Implant Team has been active ininviting leading professionals to Belfast to speak ona variety of topics relating to sensori-neural hearingloss and cochlear implantation. These seminarshave been of interest and benefit to our localTeachers of the Deaf, Speech and LanguageTherapists and Audiologists. Recent events hostedby the team have included the British CochlearImplant Group AGM: a workshop by ProfessorWarren Estabrooks on Auditory Verbal Therapyapproaches to habilitation of deaf children; and aseminar by Dr Josephine Marriage on the SensoryProcessing Disorders associated with Autism.
In January 2005 the Team hosted the annual'Listening to Learn' conference, which is sponsoredby Cochlear Europe Ltd, at the Ramada Hotel inBelfast. This year's theme was 'From New BornHearing Screening to success at school'. The keyspeaker, Professor Carol Flexor, from the Universityof Akron Ohio USA, gave an inspirational andstimulating presentation entitled ‘Issues that need tobe considered for successful Inclusion’. Another keyspeaker at the event was Dr Kai Uus MD Phd fromthe Audiology and Deafness Research Group,University of Manchester. Dr Uus presented an'Evaluation of the Newborn Hearing ScreeningProgramme in England'. The delegates, a mixtureof parents and professionals, came from all over theUK and Ireland, as well as Malta, Poland, theUkraine and the Czech Republic.
Keeping the links workingCecilia McAnallen
Deputy Director/Senior Speech & Language TherapistRegional Cochlear Implant Centre, Belfast City Hospital Trust
Contact details for the Cochlear ImplantTeam at Belfast City Hospital:Regional Cochlear Implant CentreMiddle Dufferin, Belfast City Hospital Trust, Lisburn Road,Belfast BT9 7AB Tel: 02890 263 603Email: [email protected] [email protected]
Editor’s noteWe hope to receive an article about bilateral implantationin children from RCIC for publication in a futureMagazine and on the website.
The Regional Cochlear Implant Centre (RCIC),Belfast City Hospital Trust, was established in 1992and both the Paediatric and Adult CochlearProgrammes are based in the same Centre. Thisprovides a continuity of service for our growingPaediatric Cochlear Implant recipients, some ofwhom have already progressed to tertiary educationand employment. Altogether 90 adults and 90children from all over Northern Ireland, as well assome from the South of Ireland, have receivedimplants at the Centre.
The Cochlear Implant Team currently consists of aDirector/Consultant Otolaryngologist, twoAudiologists, two Speech and Language Therapists,an Advisory Teacher of the Deaf, an Administratorand a part-time secretary. The team's AdvisoryTeacher, Joanne Clarke Lyttle, provides a linkbetween the Cochlear Implant Team and the localteaching professionals. She visits a wide variety ofnurseries, schools, hearing-impaired units andcolleges, liaising with the teachers of the childrenwho have received implants in Belfast City Hospital.
Recent developments at the Belfast CochlearImplant Centre have included the bilateralimplantation of children who have suffered hearingloss as the result of meningitis. Bilateralimplantation circumvents the possible problem ofossification in both cochleas which may preventfuture implant placement in either ear. It also hasthe added benefit of capturing the ‘better ear’ inthese cases and may provide additional benefits insound localisation and speech discrimination innoise. Four children have already received bilateral
Dr Kai Uus at the 'Listening to Learn' conference
53955-BatodMarch05 8/3/05 9:20 am Page 34
creo
©BATOD Magazine March 05 33
Title: Nottingham Early AssessmentPackage
Publisher The Ear FoundationDate of Publication: July 2004ISBN No: CD ROMPrice: £30Available from
The Ear Foundation, Marjorie Sherman House83 Sherwin Road, Lenton, NottinghamNG7 2FB
Reviewer: Corinda M CarnelleyPeripatetic Teacher of the Deaf
The Nottingham Early Assessment Package (NEAP)was developed for the assessment of deaf infantswithin a cochlear implant programme with staff fromNottingham Cochlear Implant Programme. Thepackage was produced with support from CochlearEurope.
The assessments used in the areas ofcommunication, the development of auditory skillsand speech production are now available on CDRom.
As a peripatetic teacher of pre-school children, I findrecording progress to be an ongoing conundrum -both in providing parental information and forreports to the service and other professionals.Whilst I acknowledge that testing deaf children ofany age is never easy, at least standardised testscores can show progress (or not!) Showing (andproving) progress in the under-threes has alwaysbeen a challenge.
I have been on one of the Nottingham trainingcourses for NEAP and returned feeling full ofenthusiasm and confident in my abilities. Myreports were going to be better than ever (!) - full ofincredibly useful information so that I could showthe amazing progress of some of my caseload. Ifiled all the papers in my personal developmentfolder ………. and that's where they still are.
Frankly, there were just too many of them and I feltoverwhelmed by the acronyms - LiP; ILiP; CAP;MAIS; SNAP etc.
However, this new CD has all of the tests, in aneasy to access format. They are divided into threeareas; Auditory Perception; Communication andLanguage Development; and Speech ProductionDevelopment. The individual tests (all nine of them)are all there, under their relevant area.
Each test is introduced in a five section format.
1 What does it measure?2 Why use it?3 Assessment guide4 Examples - and here there are some really
interesting video clips5 Test yourself/guidelines
Suddenly, it all becomes quite clear and, on loadingthe CD into the computer and having a look, I felt asfull of enthusiasm as I had on my return from thecourse. Somehow, it all seems so much easier -there are helpful pointers throughout and even themost technophobic amongst us would be able touse the CD to access the information required. For assessing the skills and abilities of young deafchildren and for monitoring their development, thisis an absolutely essential purchase - everything youcould ever need, in an easy to access format.It could also be useful in nursery/infant units as abaseline and far more relevant than the FoundationStage Profile. I highly recommend it.
LiP Listening Progress ProfileCAP Categories of Auditory PerformanceILiP Infant Listening Progress ProfileMAIS Meaningful Auditory Integration ScaleSNAP Story Narrative Assessment Procedure
☺☺☺☺☺ Quality
☺☺☺☺☺ Value for money
☺☺☺☺☺ Educational usefulness
☺☺☺☺☺ Overall
The Ear Foundation does have some trainingcourses planned for the Nottingham EarlyAssessment Package. From the BATODcalendar - 23 June 2005 and Peter Ring,Education Administrator, tells me that anothercourse is being planned for December (therewas one last December).
editor’s note
honest
ly!
53955-BatodMarch05 8/3/05 9:20 am Page 35
creo

Phonak multi-frequency FM technology
MLxS receiver� World’s only miniaturised multi-frequency FM receiver� Automatic and direct wireless frequency synchronisation � Compatible with both Phonak BTEs and BTEs from other
manufacturers
SmartLink SX� The new benchmark in FM communication� Incorporates advanced FM technology, hearing instrument remote
control and a Bluetooth link for mobile phone use� Crystal clear sound thanks to the highly advanced DSP processing
package
Campus S� Direct wireless frequency synchronisation � Ultimate flexibility in multi-classroom applications � Various microphone options
WallPilot� Automatic wireless frequency synchronisation � Best solution for educational environments with maximum
convenience for teachers� Allows full freedom of movement between classrooms
www.phonak.co.uk
Phonak FM technology –still one step ahead!
With its unique digital Synthesisertechnology, Phonak once again setsthe benchmark in FM communication.
The new multi-frequency MicroLinkreceivers are a breakthrough inflexibility and convenience for multipleclassroom situations as it can bewirelessly synchronised not only to theclassroom frequency but also to groupor individual frequencies.
For further information speak to ournew FM product manager; Tony Murphy on 0800 9800747.
53955-BatodMarch05 8/3/05 9:20 am Page 36
creo

©BATOD Magazine March 05 35
Now that we have early diagnosis of hearing loss inthe UK and we know that those children implantedearly do better - so we can just get on and do it can'twe???
Well perhaps we can't - to quote David Luterman,"when emotions are high, cognition is low" and whenone is feeling vulnerable may not be the best time tomake a major, irrevocable decision such asimplanting your infant. On the other hand, you can'twait too long either and parents clearly feel underpressure. One of the things we can do is to makesure that parents have up-to-date unbiasedinformation as soon as possible.
As part of the Early Support Pilot Programme, TheEar Foundation developed an information video andDVD, signed, subtitled and translated into otherlanguages, and a Frequently Asked Questionssection on their website to ensure that parents, inthe early stages of thinking about implantation, hadclear and objective information on the process tohelp them decide whether they wished to explorethe option further. The video and DVD were sentout to all educational services and it is still availablefrom The Ear Foundation.
The new technology can be quite daunting, followinga major operation on your child:"It was like having a new baby. At first I was terrifiedI would break something or do something wrong.After a little while I realised that the equipment wasquite straightforward and strong. I relaxed a lotmore once I realised that Robert had learnt enoughto show me very quickly if something wasn't quiteright."
After early diagnosis - early implantation?Sue Archbold
Practical Issues has now been reprinted and a DVDof the STEPS - from hearing to talking - is beingmade for families. Further details are available atwww.earfoundation.org.uk
A further book, Cochlear Implants for Deaf Babiesand Young Children, Practical Issues, was alsoproduced as part of ESPP and gives practical advicefor those parents of deaf infants who have decidedto proceed with implantation for their child. It's athoroughly realistic book, written by parents forparents, addressing the issues that parents face inthe early stages.
53955-BatodMarch05 8/3/05 9:20 am Page 37

36 ©BATOD Magazine March 05
Challenges There is an increasing number of cochlear implantedpupils referred to CAP by Teachers of the Deaf asmany of these profoundly deaf youngsters needsome additional help with language development.In many ways they are no different from all the otherdeaf pupils referred to DCCAP however, one or twohave presented us with challenges.
One DCCAP client was able to freeze the screen onthe television just by touching it, because of the 3Gprocessor in his Cochlear Implant! It is importantthat the screen on a laptop or PC is anti-static.Most modern screens come with this feature but it ispossible to buy products to reduce the staticelectricity from companies that sell computers. Anti-static sprays and wipes are the most commonsolutions. If you are not sure it is best to seekadvice from the supplier of the implant and computerequipment. This is especially true if the child hasaccess to a touch-screen such as a Tablet PC or aVoice Output Communication Aid (VOCA).
What's so different about a computer? Why notjust give them a paper and pencil?MotivationJust look at this picture! Here is pure enjoyment and
motivation. Tom hassevere learning difficultiesand can achieve muchmore on a computer thanhe can otherwise. HisCSW was surprised when amaths task that, on paper,would have demotivatedTom, had his fullconcentration and he wascompletely focussed for 11/2
hours. The only reason hestopped was because it was home time! As Tom isalso Dyspraxic, pencil and paper have been suchhard work. In spite of hours of practice it is stilldifficult for him to produce legible handwriting.Hopefully he will soon be able to complete all hiswritten work on a laptop. He is keen to use'Communicate in Print' from Widgit.
Different ways of recording assignmentsFor some pupils producing a mind map can be aschallenging as writing two sides of A4 is for others.Would you be happy if a student with a high non-verbal IQ but extremely poor literacy skills created aset of digital photographs or a short video film for apiece of work? This is something that we should beworking towards - alternative presentations todemonstrate ability.
Recording skillsChildren who are educated with British SignLanguage as their first language may have problemswriting in English. Simon was issued with apredictive software package called Co:Writer 4000by Don Johnston which follows English grammarpatterns to give him the clue as to what the nextword might be. He is getting started withPowerPoint which can be used as an excitingeducational tool to animate work, create booklets aswell as for presentations. The visual learningprogram 'Inspiration' allows him to plan his thoughts,draft his assignment and produce a well organisedessay at the end.
Building on strengths and interestsWhen a Year 6 pupil was observed in the classroom,he appeared to be totally disinterested in what wasgoing on by making noises; playing with theequipment and copying inappropriate behaviourfrom another pupil. He likes cartoons and comics.He was shown a programme called 'Story Maker 2'by Spa Software. There are opportunities to choosea background and place characters to make up astory. Once shown what to do he did not need to bereminded. He quickly formulated three imaginativestory pages and asked, “Can I do this every day?”
This pupil also has physical problems with writing.After Clicker4 grids were demonstrated he wroteabout the food he liked. The grids can have singlewords or phrases supported (or not) by pictures,either prepared earlier or else whilst the pupil andteacher or classroom support person discuss thepossible words and phrases. With pen and paper itwould have taken him at least half an hour. He wasamazed when it was pointed out that he had writtenthree sentences in a couple of minutes..Building up ideas using pictures and words in amind mapping programme is a fun way to planstories and think out ideas. The graphics in
Paul Bonsor and Marian Nash
53955-BatodMarch05 8/3/05 9:20 am Page 38

©BATOD Magazine March 05 37
'Kidspiration' reminded a pupil to add elements to astory map which is easily expanded. Although thepicture shows on the mindmap, in the writing viewthe words appear. This helps the pupil who has theideas but not the ability to record them easily.
ICT can motivate, inspire, raise standards and helpdeaf pupils to be successful, so raising self-esteemand confidence. It is not just the pupil who benefits,the teacher can see progress and has tangibleevidence that looks attractive. Parents can proudlyshow well-presented work using modern technologythat demonstrates progress where previously therewas frustration.
Websites for softwareMany suppliers of software have websites with anarea where teachers can contribute templates andgrids that they have prepared. There are oftenlesson plans and ideas available (though some mayfit an American curriculum!). Visit these websites todownload examples that can reduce yourpreparation time.
There are free courses on the Microsoftoffice site forMicrosoft Office 2003 programs only. Courses areself-paced, interactive and focused on particularfeatures or activity areas. Courses contain audiotracks, illustrations and practice sessions using theprograms they teach. On-line courses are a quick,easy way to gain valuable expertise and becomemore productive and they are FREE!
Communicate in Print - www.widgit.comCo: Writer 4000 - www.donjohnston.co.ukPowerPoint - www.MicrosoftofficeInspiration/Kidspiration - www.inspiration.comStory Maker 2 - www.spasoft.co.ukClicker 4 - www.cricksoft.com
Have you been to our website recently? If youhaven't received the flier about the training eventssoon to be in a place near you, then look at Trainingon
www.dccap.org.ukwww.blueskiesproject.org.uk
BATOD Association Magazine
ADVERTISING RATES circulation 1,900: Teachers of the Deaf and associated
professionals, readership estimate 7,000 Format A4 portrait width x height
Black & White:Full page .................. £260 170mm x 270mm Half Page .................. £150 170 x 125 or 80 x 270mmQuarter Page ............ £ 88 83mm x125mmFull Colour: Back Cover .............. £550 170mm x 270mm Full Page .................. £440 170mm x 270mm Half Page ................. £220 170 x 125 or 80 x 270mmJoin a Course .......... £33 - £55
Job Advertisements also appear on our websiteEntries to the website only............. £150.00(Entry from receipt to deadline date, live email link)
Courses
Information and registration forms plus a calendar entry £260.00 plus VAT
Loose Inserts with Magazine mailing
Supplied (1900 copies) ................. £200
Duplicated from master ................. £250
Electronic copy should be supplied wherever possible (eg: eps, highquality pdf, tiff).Confirmation of space requirements should be in writing as far inadvance as possible.
Please contact the Advertising Manager for further details:41 The Orchard, Leven, BeverleyEast Yorkshire HU17 5QA
(tel 01964 544243 answerphone and fax)(email: [email protected])
Contact DCCAPPaul Bonsor Tel/Fax 01295 [email protected] Nash Tel/Fax/Text 0870 770 [email protected]
Simon gets to grips with PowerPoint
Registered Charity No: 1068077
At the award-winning Jubilee Campus, University of Nottingham
Our annual opportunity for all professionals who work with children with cochlear
implants to explore current issues in both multi-and uni-professional groups.
This year’s course, in modern new facilities, will enable you to be updated on the
latest trends and technologies and to develop new skills.
Topics to be covered include:
• Assessment of very young, borderline and complex children• Audiological assessment and management• Medical and surgical issues • Multi-professional working and decision making• Educational issues• Communication, language and speech assessment of deaf
infants and those with additional needs• Young people with cochlear implants• Parent and family issues• Outcome measures of benefit• Health-economic issues• Future challenges
Residential – £320 Non-Residential – £270
Call today for more information or to reserve your space – early booking
advised – international speakers, including Leo De Raeve, Geoff Plant and
members of the Nottingham Cochlear Implant Programme
For information contact Peter Ring
Tel: +44(0)115 942 1985 · Fax: +44(0)115 924 9054 · e-mail: [email protected]
The Ear Foundation, Marjorie Sherman House, 83 Sherwin Road, Nottingham NG7 2FB
Website: www.earfoundation.org.uk
REGISTER ON THE WEBSITE
Our normal cancellation policy applies
53955-BatodMarch05 8/3/05 9:20 am Page 39
creo

38 ©BATOD Magazine March 05
Linden Lodge is a unique school in Wandsworth,South-West London. It is an inclusive special schoolfor children with a visual impairment and for childrenwho have additional special educational needs.
The school promotes a multi-agency approach andperipatetic teachers for Hearing-Impaired pupils arepart of the team. Pupils have varying types anddegrees of hearing loss and twelve pupils have apermanent dual sensory impairment.
The idea for a tactile audiogram developed from theincreasing need for deafblind children to haveaccess to information. Observing children in theirlessons, I saw other tactile resources used, eg raised maps in history, showing the routes ofarmies across Europe, and graphs in maths. Thisimpressed me. I was already using a smiley facereward sheet for hearing aid battery checks andhearing aid care using ‘Wikki Stix’ and I saw thepotential of ‘swell paper’.
At Annual Reviews, in my role as the peripateticToD, I explain to families and other professionals the‘shape’ of the pupils' audiograms; what can andcannot be heard. In mainstream schools, childrendiscuss their audiograms so they become familiarwith audiological terms. How could children atLinden Lodge School become equally independent?We look at the model of the ear but the audiogrampresents a problem.
The Learning Resource Department at LindenLodge prepares resources to support teaching and
learning and I discussed the idea of developing atactile audiogram with Jane Overton, TeachingAssistant. Jane has a special interest in deafblindchildren, (she has the CACDP DeafblindCommunicator Guide, Makaton, Braille and Moonqualifications and BSL Stage 2). Jane wanted tomake the audiograms in Braille or Moon as simpleas possible, yet containing all the auditoryinformation. We discussed each child's needs andlevel of understanding and Jane familiarised herselfwith each child's audiogram.
The process used to produce a tactile audiogramtakes several stages:� On A4 paper, the audiogram outline frame is
drawn and photocopied onto ‘Swell’ paper.(Paper that raises the outline/shape under heat.)
� This paper is put through a heat fusing machinewhich raises the outline to make the imagetactile.
� Jane writes in print for the sighted peopleworking with the children and puts Braille orMoon over this for the children to read.
� Along the top horizontal axis are the approximatephonic sounds: 'a, e, b, ch, th,s' which replacethe usual frequencies.
� Down the left side are the decibels, 0 to 120 (-10and -20 are complications at this stage).Decibels are described as levels of loudness.
� A dotted line across at 20dB marks the normalthreshold of hearing.
A tactile audiogram for deafblind pupilsMarion Brushett, Wandsworth Hearing-Impaired Service
53955-BatodMarch05 8/3/05 9:20 am Page 40
creo

� Down the right side are the descriptors ofhearing levels: normal, mild, moderate, severe,profound.
� The amount and type of information given varieswith each child's needs.
� A key indicates the left and right ear thresholds,using different textures: felt for the left, raffia forthe right.
� The materials are plotted according to theindividual child's hearing levels.
Using his audiogram, Nathan, who is 16 years oldand describes himself, "I have a visual and hearingdisability," he says, “It shows how good or bad myhearing is. There is a key for the different textures.The left is soft, like carpet. The right is plastic bagtype. At the top, there are letters like the differentsounds they send through the headphones athospital. Down the left side, I've got numbers likegrades of how low the hearing is. There are namesof the sections, 0 to 20 is normal hearing and themore down it goes, the worse it is.”"My hearing is in the 'moderate' section, 50 to 70and some in the 'severe' section, 70 to 90. Onehundred and twenty dB is called 'profound' andpeople with this hearing loss may use signlanguage." Once he leaves Linden Lodge School,Nathan can use the audiogram to explain to otherpeople at college, work experience, or family andfriends, about his level of hearing.
It may be that another teacher has already prepareda similar audiogram. I would like to share myexperience because I have found the tactileaudiogram has fulfilled its purpose, which is for abledeafblind children to have greater understanding oftheir hearing loss. If you have children who maybenefit from access to audiological information, talkto teachers in your local Visual Impairment servicefor help with the special techniques in the productionof the audiogram. My thanks to Linden LodgeSchool staff and children.
©BATOD Magazine March 05 39
New BSL on-lineGlossaries of SignsEver wanted to know how to sign 'atomic mass' or'escape velocity' in BSL? Well now you can - thanksto the launch of two new on-line glossaries aimed atassisting d/Deaf science, engineering andconstruction students and their interpreters.
In 2002 the University of Wolverhampton wasawarded funding from the Higher Education FundingCouncil to complete the glossary projects collectivelyentitled 'SignsOnline'. The project has taken twoyears to complete and aimed to produce two newBSL websites, for science and engineering andconstruction as well as updating the artsigns websitewhich has been available since October 2002.
Creating the new websites involved interviewingmany Deaf scientists, engineers, construction andart professionals to find out the signs they use intheir professional life and during their studies. Theinterviews took place all over the UK. Additionally,hours of footage of BSL on the television wereanalysed to find commonly used existing signs.
After analysing and comparing the signs used indifferent regions a panel of 'critical friends' wasasked to evaluate the signs to determine if theywere culturally and contextually appropriate. Thispanel was made up of Frances Elton, John Hay,Mark Heaton, Tessa Padden and Helen Phillips.
The glossary is presented by Niki Stratton andTessa Padden acted as the BSL monitor during thefilming of the signs.
The websites use high quality videos, optimised forthe web and the websites are fast and easy to use.They can be seen at www.sciencesigns.ac.uk andwww.engineeringsigns.ac.uk They are completelyfree of charge and can be accessed by anyone withan internet connected computer. Altogether thesites contain nearly 2,500 BSL sign videos.
Geneva
14-16 October 2005
Deaf children from ethnic minorities
Each BATOD region has £100 to be used to support a regional delegate
(or more) to the congress
53955-BatodMarch05 8/3/05 9:20 am Page 41

Hearing impairment, not to mention difficult listen-ing environments, of any type and degree can sabotage a child's learning of language and their ability to acquire knowledge. In a classroom, there istypically a poor signal noise ratio as a result of noise(up to 70 dBA), distance from the speaker, and pooracoustics leading to rever-beration.An FM system cou-pled with adequate amplifi-cation is the only means toovercome these problemsfor hearing impaired chil-dren thus allowing them fullaccess to language.
Oticon has recently con-ducted a study evaluatingFM advantage in the realclassroom environment,using the new Lexis digitalFM system coupled with dif-ferent hearing aids fitted tochildren with a variety ofhearing losses. The goal wasto establish whether the use
of a personal FM system provided improved speechperception in the classroom compared to using ahearing aid only.The Neale Analysis of Reading Comprehension wasadministered using live voice in the pupil's classroom, with and without the FM system. Three
questionnaires for teachers,pupils, and parents were alsoadministered in order togain their input.
The results of this FM studyshowed a significantimprovement in the stu-dent's speech perceptionwhen fitted with the FM sys-tem in the "Real" classroom.A perceived improvement invarious listening environ-ments both at home and atschool was also demonstrated.Most importantly, the FMsystem also had a positiveinfluence on behaviour andconfidence.
FM Advantage in the Real Classroom
A recent study conducted in the UK by Mark Flynn, Traci Schmidtke and Melanie Harvey(2004)
For a copy of the full OticonFM Study please contactOticon UK on 01883 331720
01883 331720 Tel.01883 331729 Fax
Oticon Limited3rd Floor, Quadrant House
33-45 Croydon RoadCaterham, Surrey
CR3 6PG ENGLAND
53955-BatodMarch05 8/3/05 9:20 am Page 42

©BATOD Magazine March 05 41
The National Maritime Museum, together withMorgan Stanley, is offering an interactive study dayfor deaf students to explore the compelling story of aman who overcame the odds and led his men tostunning naval victories, including the Battle ofTrafalgar. Through Nelson, students will examinemanagement styles, leading in a crisis and teambuilding skills, among others. The programme willbe supported by the major exhibition Nelson &Napoleon, which commemorates the bicentenary ofNelson's death. Each study day will also offerstudents the opportunity to discuss with arepresentative from Morgan Stanley the challengesand skills involved in modern business leadership.A practical and beautifully designed classroomresource will accompany the course.Date: Thursday 29 September 2005 Free of chargeTo book: tel 020 8312 6608 fax 020 8312 [email protected] Tania Dain, Education Officer,National Maritime Museum, 0208 312 8551www.nmm.ac.uk/learning
Live Science: The Cocktail Party EffectUntil early April 2005 the Science Museum isrecruiting 3,000 visitors for research into aphenomenon known as 'The Cocktail Party Effect'.As part of the Museum's Live Science initiative,visitors have a unique chance to help scientistsinvestigate aspects of selective hearing - such asthe way that a listener can tune in to only one ofseveral competing conversations when in a noisyenvironment such as a cocktail party. Admission free
Margaret Glasgow MBE! We know that she is a bit'embarrassed' by the award but certainly Margaretdeserves some public acclaim for all the time andeffort that she has dedicated to deaf children. Thecitation for Margaret's MBE is on the BATODwebsite and BATOD offers sincere congratulations.Whilst Margaret was on the NEC she wasresponsible for many of the A&ICT articlesappearing in the Magazine, especially the muchacclaimed ‘Audiology refreshers’ which are soon(honestly!) to be available on CD and also thebooklet about testing children with complex needs.
Deaf Connections, the West of Scotland Charity forDeaf and hard of hearing people, has launched anew revolutionary electronic translation service. Text Connect can be used as either an electronictranslation service or as an electronic note takingservice. Using laptops and specially developed
software, it is a communication device to enableDeaf people to access information at meetings,conferences and lecture environments etc. Theelectronic translation service allows Deaf people tobecome actively involved at an interactive event toask or answer questions, take part in debates orgeneral discussions and receive a live account ofproceedings, via an operator, onto a computerscreen in front of them.
Electronic note-taking is a more advanced systemthan the previous handwritten note-taking service.Text Connect customers will receive all notes/minutes via floppy disk, CD or email after the event.
Update on Palantype: Deaf and hard of hearingpeople who rely on Palantype, a machine to providea real-time verbatim transcript of meetings, have inrecent months, had their communications supportthreatened with the announcement that productionof Palantype equipment could be halted.
In January 2005 Possum Controls Limited confirmedthat it will be closing its Palantype division.However, RNID, the largest charity representing thenine million deaf and hard of hearing people in theUK, has announced that it will ensure Palantypistsare still able to purchase new machines.
Mark Downs, Director of Technology and Enterpriseat RNID says: "RNID is delighted that followingdiscussions with us, Possum Controls have putarrangements in place to ensure the future ofPalantype. Possum Controls' decision to ceasefurther production of Palantype equipment isdisappointing but is understandable given theincreasingly limited demand for new equipment. Itwill be a concern for the many deaf and hard ofhearing people, who rely on this technology tofacilitate a more inclusive life and Palantypeprofessionals, who provide this invaluable service."
Possum Controls have donated the technicaldrawings for the Palantype equipment to RNID toensure future production and maintenance of theequipment remains possible.
Fast-track residential BSL course at WelshCountry ManorPeople interested in learning sign language nowhave the option of fast-tracking themselves to LevelOne standard in a week. A new one-week, intensiveLevel One course in BSL will be held in the scenicsurroundings of Pembrokeshire this July. Thecourse will be run by Sense-Ability, a Wales-basedbusiness owned by two deaf people, Martin McLeanand Anna Lickley. The course will be held atClynfyw, a large manor house on a working farmnear Cardigan. The cost of the course includes full-board accommodation for one week, from 15-22July 2005. When booking the course, people will be
This and that...
53955-BatodMarch05 8/3/05 9:20 am Page 43

42 ©BATOD Magazine March 05
given the option of enrolling for the sign languageexam, to be held on the final day. For further detailsabout the course look up the Sense-Ability websiteat www.sense-ability.co.uk or phone 0151 651 1053(voice) or 01239 851 984 (textphone).
CODPUK.ORG.UKA new organisation was launched on 29 January.Children of Deaf Parents UK has been establishedto provide networking opportunities for children ofdeaf parents and support to deaf parents. At thelaunch party the CODPUK.ORG.UK logo, designedby students at Kensington and Chelsea College,was launched by Teresa May MP, Shadow Secretaryof State for the Family. For further details visit thewebsite at www.codpuk.org.uk or [email protected]
After reading the November Magazine focussing oncreativity, Ros Way, Headteacher at ElmfieldSchool for Deaf Children, Bristol wrote in to sharethe news that the school received the ArtsmarkAward. This award is presented by Arts CouncilEngland to schools offering opportunities across therange of arts.
These include creating work in art, music, BSLpoetry as well as taking part in dance and dramaperformances at the school and in the localcommunity. The pupils are taught by highly skilledand experienced specialist and enthusiastic non-specialist secondary and primary staff. Activitiesenjoyed by pupils include workshops with theTravelling Light Theatre Company and Bristol HNDdance students, theatre visits to BSL- interpretedperformances as well as links with local deaf andhearing artists. Last year the school again took partin a gala dance performance at Bristol Hippodromeas part of Stages 2004 regional schools event. The school was one of twenty-five chosen fromaround one hundred mainstream and specialschools.
The award follows the school's success last year inachieving the Basic Skills Quality Mark, the firstschool for deaf children to do so. The award by thebasic skills agency, recognises the school's raisingawareness of numeracy, literacy and communicationskills.
Be part of a ground-breaking British SignLanguage survey Most ToDs know that BritishSign Language (BSL) has regional dialects. Thesigns used across the UK, from Aberdeen to theChannel Islands, are very different. BSL users willhave the opportunity to take part in an interactivesurvey about the signs they use.
Over the coming months researchers at BristolUniversity's Centre for Deaf Studies are collectingdata, using signs from as many UK cities as
possible to compile the first-ever comprehensivesurvey of BSL variation covering the whole of theBritish Isles. The survey is part of a wider BBCproject, Voices, which is looking at the impact oflanguage on society as a whole.
Regular BSL users can help the Bristol researchersincrease what is known about BSL variation bytelling them which signs they use or know. Signshave already been collected from eight UK cities.Taking part in the survey will enable the researchersto identify where these signs are used. There isalso an opportunity to send or email a video clip ofsigns used or known, which aren't part of the survey.The results will be available in July 2005.To take part in the survey go towww.bbc.co.uk/voices and click on 'take part now'.
Mentioned in dispatches!The Royal School for the Deaf and CommunicationDisorders Manchester is one of only two specialschools to be mentioned among the 23 schools inGreater Manchester identified by the Inspector asbeing shining examples of education in his annualreport which highlighted more than 390 schools andcolleges which were drawn from those inspectedduring the academic year 2003/2004.
The Inspector, David Bell, named the outstandingschools and said that they 'stand out as having doneparticularly well on virtually all fronts or as havingachieved highly against the odds'. He congratulatedthe headteacher, staff and governors and pupils orstudents of all the successful schools and collegesnamed, on their success and hard work in deliveringsuch a high standards of education.
www.BATOD.org.ukIn between all the various demands of BATOD andthe BATOD Magazine Paul Simpson and AnnUnderwood met together at the end of January toreview the BATOD website. Discussion followingsome queries led the changes in the folder and fileorganisation on the site and it should now be easierto find some items.
Articles have been regrouped for easy referenceand in the coming months it is hoped to providefolders of articles from the Magazine and othersources to ensure that everyone can accessinformation. The exciting development of an ‘on-line’ magazine is beginning to take shape startingwith the focus of January’s Magazine ‘Models ofDeaf Education’. Changes and additions are madeto the site continually and these are flagged up ifyour computer has ‘cookies’ enabled. This makes iteasy to find the items quickly.
Go and have a look!
53955-BatodMarch05 8/3/05 9:20 am Page 44

53955-BatodMarch05 8/3/05 9:20 am Page 45
creo

44 ©BATOD Magazine March 05
In July 2004, along with their peers, three studentswith profound hearing losses completed thesecondary phase of their education. The threestudents in question attended a mainstreamsecondary school, with an inclusive unit. Over fiveyears these students made extraordinary progress.Children, regardless of the mode of communicationor educational setting, do not all start from the samebaseline, for a variety of complex reasons. Despitethese reasons and despite the baseline from whichthey start, it is our job to support these children andtheir families in the achievement of their educationalpotential. Having only few word utterances in Year7, by the time they left they were all routinely holdingconversations with staff and peers alike. They allsuccessfully completed a two-week work experienceplacement, with one of them going on to win a part-time job in the placement that they attended. Theybecame confident, independent members of theschool and social community. They went on toFurther Education placements of their choice: an ITBTEC; a vocational challenge course; and BTECDesign Course. Academically, they gained resultsranging from an A* to an entry-level certificate inEnglish. And all of this with language levels onstandardised tests of less than nine years old. Theyhad become happy, confident young adults; and weand their families wanted to celebrate thisachievement. Such a story has probably beenplayed out throughout the UK within the educationsystem.
Unfortunately, however, this is not how the educationsystem sees it, represented by Form Four. Becausethese were the only children within the LEA who fellinto the category of leaving school with a profoundor severe hearing loss and because none of thesestudents achieved five A-C GCSE results, the LEA'srecord this year for this attainment target is zero. Tocompound this point Ofsted is looming for the LEA.From this perspective, the zero attainment for thisparticular target looks ominous. But the perspectivefrom which Ofsted operates draws a picture whichmay be grimmer still.
The Hearing Impairment Team that the LEAoperates, if judged by GCSE A-C outcomes, ishardly likely to appear good value for money,especially if analysed alongside statisticalneighbours who had either a good GCSE year fromthe population of children that falls into this category,or the statementing process is different allowing a
superficially similar but actually rather distinct groupof children to be compared. This is something thatForm Four does not account for. There are, in fact,a number of points that the Form Four perspectivefails to see; and we would now like to draw yourattention to them.
The most obvious point is that the sample fromwhich a judgement about attainment can be drawnis statistically too small to make any such judgementmeaningful, even if comparisons are made withstatistical neighbour LEAs. If an LEA has only onechild within the profound or severe hearing losscategory who nevertheless leaves school with fiveGCSEs in the A-C range, their attainment for thisparticular target reaches 100%. The reason for thevacuousness of judgements based on this limitedstatistical evidence is that other factors can skewoutcomes beyond a level that could be factored outfrom a statistically salient sample. Secondly, theLEA that we work for only attaches statements tochildren, regardless of the level of hearing loss, ifthey have additional or complex problems beyond asensory impairment. By definition, this means thatthe children that form the category that Form Four isinterested in will be the children who face thegreatest challenges to educational achievement.Whilst we feel that this policy is correct, it doesmean that other children within the LEA who mayhave a profound or severe hearing loss but who arenot Statemented because they are performingeducationally on a par with their mainstream peers,will not be seen from the Form Four perspective.This brings us to the third point that the perspectivetaken by Ofsted and others fails to recognise: as faras we can tell, no standard criteria exist that canaccount for such key factors as educationalattainment and curriculum access in relation tolanguage level. It isn't simply that the effects ofsuch factors as significantly reduced levels oflanguage on curriculum access and educationalattainment have not been considered, we areunaware of any work that has attempted to discoverif this factor can be standardised within and acrosssubject areas. Nevertheless, the point isindisputable that a child with a reduced languagelevel will find it much more difficult to perform inpublic examinations and access the curriculum aseffectively as children who have language levelscommensurate with their chronological age. Otherfactors, too, such as aided thresholds, speechdiscrimination skills, age of diagnosis, whether or
Educational achievement, measurement and perspectivePaul Moran, Gwen Morris, Caz Conaghan, Sandy Rees
53955-BatodMarch05 8/3/05 9:20 am Page 46

©BATOD Magazine March 05 45
not English is the second language of the home,levels of language that children are exposed tooutside school, will inevitably have an impact uponeducational attainment and currently aredisregarded from the Ofsted perspective.
But what attention is given to more general andmore specific levels of attainment, also notconsidered by Ofsted? For example, factors suchas confidence, independence, levels of social,conversational, peer and pragmatic linguisticinclusion, levels of independent learning (given levelof language acquired) and language progress (notmeasurable according to Attainment Targetsbecause progress has been so incremental butnevertheless real and, for a specific child, thoroughlysignificant). What of progress in these areas?What if these areas are for specific children themost important areas of their educationalexperience? They are not, as far as we can tell,viewable from the Ofsted perspective; entiregeographies of potential achievement, unrecorded,un-regarded, not considered.
We come, finally, to the point about cost. Perhaps itwould be possible to obtain very similar GCSEresults for the category of profoundly and severelydeaf children with fewer resources, possiblysignificantly fewer resources. But such aperspective, as we have delineated above, is unableto perceive anything about the quality of educationalexperience for such children: a quality that dependsupon high levels of audiological skills; teachers whoare committed to encouraging communicativeconfidence; staff whose goals are not determined bythe narrow perspective of Ofsted criteria forsuccess. This alternative perspective is, however,expensive. There must be a way of measuringachievement from this alternative perspective. Atleast, we think it is worth investigating, if only toprove that our celebration of the achievement of thethree students who left this year was justified.
Editor’s noteJenny Baxter has represented BATOD and deafpupils for many years in the Examinations arena.She too has been putting forward similar ideas formany years and she fully endorses this cogentlyargued article. BATOD NEC Educational Issuescommittee will be following through and pointing outto the DfES that this article speaks on behalf ofhundreds of deaf school-leavers and their ToDs.Many students demonstrate the progress cited in thearticle and to a significant extent the mainstreamschool's ethos and teaching contributes to thesuccess.
The BATOD Archive should be more accuratelydescribed as an archive of BATOD and the bodiesthat preceded it. The archive is kept in the library(archives) at the University of Birmingham.
BATOD has developed through a series ofamalgamations between individual colleges,unfortunately not all of which are represented in ourarchive.
The material is arranged chronologically and dividedinto four main categories, one for each stage ofdevelopment.
The first section consists of material relating to theCollege of Teachers of the Deaf and Dumb (CTDD)and covers the period from its establishment in 1885to 1918, when it merged with National Association ofTeachers of the Deaf (NATD), to form the NationalCollege of Teachers of the Deaf (NCTD).
The second section contains the records of the JointExamination Board (JEB). This was established in1907 through co-operation between CTDD, theSociety for Training Teachers of the Deaf and theAssociation for Oral Instruction of the Deaf andDumb, in order to oversee a single diploma offeredby all the colleges. The archive does not containinformation about these other organisations. Itappears that the JEB was absorbed into the NCTDon its establishment in 1918.
The third section is the National College of Teachersof the Deaf (NCTD) and covers the period 1918-1979.The NCTD was established through a mergerbetween the CTDD and the NATD but there is nomaterial on NATD. This section contains extensivedocumentation on the working of the NCTD.However the formation in 1959 of a breakawayorganisation, the Society of Teachers of the Deaf(STD) is not represented.
The final section contains material relating toBATOD as the organisation that exists today.BATOD was formed in 1979 by the re-unification ofthe NCTD and the STD.
Each section of the archive consists ofcorrespondence and financial matters. The fourthsection also contains some journals and magazines.
I am continually collecting material for archiving, soif you or your local committee have any interestingitems relating to BATOD, which are more than fiveyears old, please contact me. I would be particularlypleased to receive any materials relating to thebodies mentioned above about which we have nodocumentation at all. ([email protected])
BATOD ArchiveFiona Mackenzie
53955-BatodMarch05 8/3/05 11:58 am Page 47

46 ©BATOD Magazine March 05
BATOD warmly welcomes the publication by theRNID of its report entitled "At the heart of inclusion:the role of specialist support for deaf pupils".
The report will be of great interest to all BATODmembers - particularly to those working in specialistsupport services.
The report was drawn up as a result of visits to tenLEAs. Interviews were carried out with the head ofthe support service and/or head of any hearingimpairment team (where applicable), a number ofperipatetic teachers individually and Teachers of theDeaf working in resource base provision (whereapplicable).
In total, 37 individuals were interviewed - 22 from anLEA advisory or support service and 15 from aresource base setting.
The LEAs were selected to represent a geographicalspread across England - both rural and urban areas,large LEAs and small unitary authorities.
The RNID produced five key messages 1 There is a postcode lottery of provision,
especially in London. In London, the ratios ofTeachers of the Deaf to the school populationranged from 1:9,500 to 1:38,000.
2 Forty four per cent of resource bases did nothave fully qualified staff. Twenty-five per centhad staff with no qualifications and not intraining. Problems were raised in therecruitment and retention of Teachers of theDeaf and there were concerns around theavailability of the mandatory qualification.
3 Professionals expressed concerns aroundfunding issues, in particular, the potential threatto delegated services. Fifty per cent of resourcebases had been delegated and 30% of heads ofresource bases did not know their budgets.Forty per cent of services had their budgets cutor restricted.
4 The lack of expertise of Ofsted inspectors to beable to evaluate provision for deaf pupils was aconcern.
5 Multi-agency working - the willingness andeffectiveness of Teachers of the Deaf to workwith other agencies was evident but problemswere being created by the lack of joint workingwith social services. Fifty per cent of LEAs reported problems whenliaising with social services.
There are five key recommendations.1 National criteria on access and entitlement to
LEA hearing impairment support.2 Training bursaries for Teachers of the Deaf.3 Improved data collection on the achievements of
deaf pupils in mainstream settings.4 Ofsted inspector training: specific training on the
teaching and learning needs of deaf pupils inschools and colleges.
5 LEAs should collect statistics on deaf children'sattainment in national curriculum tests andpublic examinations.
One disappointing aspect of the report is that it talksof delegation but really only refers to the delegationof resource bases (which is widespread) rather thansupport services (which is not) and the prospect ofwhich raises very real concerns.
However, the overall message very much underlinesthe points we make in our discussions with the DfESand other bodies and gives us much neededsupport. This is particularly important becauseRNID is independent from Teachers of the Deaf andcannot therefore be accused of vested interest.
Finally, we particularly welcome the proposal withinthe report for thirty bursaries for teachers under 30for three years as a very important contribution tothe problem of recruitment Teachers of the Deaf andthe funding of their training.
The full report is available on the RNID website at:www.rnid.org.uk/pdfs/support_us/heart_of_inclusion.pdf
RNID report entitled: 'At the heart of inclusion: therole of specialist support for deaf pupils'
Paul Simpson
EARSDonna Carkeet
Paediatric Audiologist and EARS board member
Do you know about EARS inc? This charity groupworks in developing countries to train and equiplocal people to fit hearing aids. Local people aretrained in the repair of hearing aids - it is no goodhaving hearing aids provided and no service forrepairs or ear moulds. EARS establishes theservices as soon as possible. We have run projectsand helped clinics in countries such as Cambodia,Vietnam, Ethiopia, India, Papua New Guinea,Dominican Republic, Indonesia and Vanuatu.
We are now looking to create an audiologicaltraining school in the Dominican Republic. This willbe a big challenge and we will need the support ofmany groups and organisations. If you have anyquestions please feel free to ask. [email protected]
53955-BatodMarch05 8/3/05 9:20 am Page 48

Siemens Hearing Instruments • www.siemens.co.uk/hearing
• Simple test routinesFonix Press&Go is a Windows-based easy-to-use, intuitive computer program thatremotely controls your FP35 or FP40 hearing aid analyser. It’s as easy as pressing a buttonto start the automatic test routine as per current protocols. Up to 4 measurements can besaved in each test and it also allows comparison with previous frequency response curves.
• Less trainingOptional Test Wizards with detailed instructionsand pictures on how to set up the analyser,hearing aids and FM system are provided for eachmeasurement, making it easy to get acquaintedwith the system.
• Saves timeThe Auto Test feature allows you to run throughthe four pre-set frequency responsemeasurements of a test without any intervention.Just push the start button and relax!
Measuring hearing aids and FM performance has never been easier.
Do you have problems remembering test protocols?…
Use Fonix Press&Go™ Software
For further informationplease call 01293 423700
53955-BatodMarch05 8/3/05 9:20 am Page 49
creo

48 ©BATOD Magazine March 05
Chance' and subsequently teachers have beentrained all over Ireland, the UK and abroad.Movement programmes are not a new phenomenonby any means but the difference with thisprogramme appears to lie in the way in which it istied to the fundamental, neurological systems whichinfluence the secondary language systems ofreading and writing.
Any attempt to look at the causes, incidence andremediation of dyslexia in both deaf and hearingchildren must surely include this programme.
Theory aside the proof of the pudding as they say isin the eating or as in this case it is for me the factthat my child has gone from being a non-reader to aregular library user, a daily reading for pleasureteenager with a reading quotient which during thecourse of the programme leapt from well belowaverage to above average. I have used theprogramme to great effect with my group of deafchildren again experiencing very significantimprovements in reading and writing. The parentsof these deaf children have also remarked on thechanges in their children, in particular their ability tocomplete home work and concentrate on tasks.
As I stated at the outset my main aim in writing tothe magazine is to make teachers and parentsaware of the existence of the programme. It hasmade my life and my children's lives so much easier.School has changed from being a dread, somethingwhich was inflicted on the whole family to arewarding positive experience, a challenge which isno longer beyond my children's grasp.
www.primarymovement.org
Sharing information - DyslexiaPatricia Mullan (Teacher of the Deaf)
Over recent months I have become very aware ofwhat a useful asset the BATOD magazine is forteachers, always providing up to date information,ideas and resources and now there is an opportunityfor me to make a small contribution of my own. In arecent edition of the magazine my eyes fell upon abulletin giving details of a study day to be held ondeafness and dyslexia. I felt so pleased that agroup of people have started to address the notionthat if a percentage of the hearing population sufferfrom dyslexia then it must follow that a percentageof the deaf population might be similarly affected, adouble wammy!
As I have been a Teacher of the Deaf for the pastsixteen years and the parent of five dyslexic childrenI feel that I have a foot in both camps. I also feelthat the experiences that I have had over these pastyears and what I have learned from them might beof some interest to other teachers and parentsstruggling with these two demons.
Having gone through various remediationprogrammes with my own children to help themcope with the effects of dyslexia, all of whichinvolved a lot of hard work and heartache, I have atlast stumbled upon the nearest thing to a cure as Ican imagine.
A programme of movements linked to the humanreflex system, has been devised by a researcher atQueen's University in Belfast. Martin McPhillips haspointed to a link between retained reflexes inchildren and problems with reading, writing and insome cases with co-ordination and balance.
'The Primarymovement Programme' was introducedto the public in a BBC documentary 'A Second
Melanie Dix (nee Marks)1.02.65 - 29.12.04
My dear friend Melanie Dix died on 29th December 2004 after her brave battle against cancer. BATODmembers will know her from Birmingham where we trained in 1991 and her teaching practice at Longwillschool for the Deaf in Birmingham. Melanie worked as a Teacher of the Deaf for twelve years as a periin Gloucestershire, mainly primary. She was dedicated to deaf children, she made everyone she camein contact with feel special - adults and children alike - she cared about everyone.
Melanie had exceptional qualities as a Teacher of the Deaf and as a colleague. I had the utmostrespect for her and learnt a lot. We had great fun together with everyone back in 1991 on the BPhilcourse with Brian Fraser, Steve Powers and Paul Simpson. I think everyone who remembers Melaniewill agree she was very lovable, kind, funny, hard-working and special.
I remained a good friend of hers when we left college and got to know her family and children well. Sheleaves behind her husband Mark and her children Lauren and Sam. We must celebrate her life but shewill be greatly missed by all.
Karen Smith
53955-BatodMarch05 8/3/05 9:20 am Page 50

How can I give my children bettersound quality in the classroom,
the playground and at home?
Give them a L EXIS™FMcommunication system.
Quiet circuitry and processorIndustry-leading +50dB signal-to-noise ratioincreases the available dynamic range, greatlybenefiting students with mild to moderatehearing loss.
Impressive 8.5dB AI-DIFive microphones and digital signalprocessing produce outstandingdirectionality for better speechunderstanding in noise.
Manually adjustable± 7dB gain controlReceiver can be quickly and easily adjustedfor FM balancing.
have you heard it?
AUDIOLOGY HOUSE, 45 NIGHTINGALE LANE, LONDON SW12 8SP
TELEPHONE: 020 8772 2700 FAX: 020 8772 2701 EMAIL: [email protected] WEB: www.pcwerth.co.uk
53955-BatodMarch05 8/3/05 9:20 am Page 51
creo

50 ©BATOD Magazine March 05
Educational MaintenanceAllowance
Elizabeth Mackinder
The educational maintenance allowance (EMA)begins after compulsory education and paymentsare usually for two years. Exceptionally, a third yearof payments may be made upon application.Students who continue in further education and wholive in a household with an annual income of £30Kor less, are paid up to £30 a week. Money is paiddirectly into their bank accounts in return for regularattendance on their courses.
EMA has been introduced to ease the financialpressures experienced by young people staying onin further education and reduce the drop-out rateamong 16-year-olds. The weekly EMA payment isintended to help cover the day-to-day costs studentshave to meet when staying on at school or college,such as travel expenses, books and courseequipment.
Young people enrolling on short courses fromJanuary 2005 may also benefit from the allowance.Students who take vocational courses such asNVQs, as well as those studying A levels at schoolor college, can apply for the allowance at any timethroughout the academic year.
Young people who were born between 1 September1987 and 31 August 1988 are eligible for paymentsif they engage in at least twelve hours a week ofguided learning on further education courses inschool sixth forms, sixth-form colleges and FEcolleges.
Once enrolled, the student must attend all coursesessions and sign an EMA contract with their schoolor college. The contract sets out what is expectedin terms of attendance, coursework and progress.
Students interested in applying for the scheme canlog on to the website at www.ema.dfes.gov.ukEMA helpline on 080 810 16219. Minicom helplines 0800 056 2811 for colleges and schools0808 101 6219 for parents and students
www.earfoundation.org.uk
Ear Foundation website
Have you had a look at The Ear Foundation'swebsite recently? It has had a complete makeover,which has brought many advantages to those of uswho visit it:� To help the partially-sighted, level Double-A
conformance to web content accessibilityguidelines has been achieved. You can click onto Large Text if you wish.
� The Home Page now has three topicshighlighted, which may interest visitors to the site- and by clicking on the picture, you can readmore about the topic.
� There is a Search button on all the pages, whichsearches the whole site - whether (for example)it's in the Frequently Asked Questions section orin Courses.
� More questions are being added to theFrequently Asked Questions page, as they arereceived from parents and professionals. In viewof the numbers of FAQs, they are nowcategorised into different sections - but try usingthe search facility if you know exactly what youwant to know.
� Go to ‘Contact Us’ and it has maps, address andtelephone numbers. There is also an easy touse Enquiry Form so that you can contact any ofThe Ear Foundation team.
� If you click on Courses, you can select the onesappropriate for (say) Teachers of the Deaf. It isthen possible to book courses on-line - and payfor them if you wish!
� The Ear Foundation is collaborating with otherorganisations (like BATOD) and they are beingadded to the website as Associates.
� There are now many reciprocal links with otherwebsites - so if you need to have a look at awebsite but don't know the address, have a lookat the Useful Links page.
If you have any comments about this website,please feel free to send an email [email protected]
53955-BatodMarch05 8/3/05 9:20 am Page 52
creo

Cued Speech uses eight handshapes in four positions near the mouth to clarify
the lip patterns of normal speech
Learn Cued Speech at our informal
Summer School in beautiful
Exeter, August 1 - 5
Tuition fee £60, low cost accommodation
Cued Speech can be used from babyhood and gives literacy skills equal to hearing children
Free information:
Cued Speech Association UKTel (v & t): 01803 83 27 84 email: [email protected] web: www.cuedspeech.co.ukRegistered charity no. 279523
MSc in HumanCommunicationThis programme provides in depth teaching on currenttheoretical and service issues related to speech andlanguage therapy and deaf studies. It is delivered byleading researchers and clinical practitioners. The flexiblemodular structure allows students to tailor their owncurriculum and pace of study. Current modules include:acquired cognitive communication impairments; acquiredlanguage impairments; clinical management; deaf studies;developmental language impairments; dysphagia;evidence based practice; habilitative audiology; identityinclusion and living with disability; language learningand development; research design and statistics; signlinguistics; speech acoustics and speech perception;speech and language therapy with deaf people.
This programme is ideal for practitioners seeking toprogress their careers within the Knowledge and SkillsFramework (Agenda for Change).
Programme fee for 2005–06: £4,300 (home/EU students);£2,150 (home/EU part-time students); £10,000 (overseasstudents); £5,000 (overseas part-time students)
For application forms contact: Admissions Office, School of Allied Health Sciences, City University, London EC1V OHB. Or call them on 020 7040 4194. Email: [email protected] information on the programme content contact: Jane Marshall, 020 7040 4668. Email:[email protected] date: 17th June 2005.
Institute ofHealth Sciences
NO
TIC
EB
OA
RD
NO
TIC
EB
OA
RDATTENTION Course Organisers
Bring your course to the notice of all our readers viathis page. An advert on this page costs £33-£55 perentry, including an entry onto the Calendar. Copymust be available five weeks preceding publication.Space should be reserved as soon as possible. Details to:Mrs Ann Underwood, Magazine Editor41 The Orchard, Leven, Beverley, HU17 5QA☎/fax 01964 544243email: [email protected]
THE BURWOOD PARK FOUNDATION FOR THE DEAF
seeks requests forMODEST GRANTS
to enhance the education of deaf children
We have about £50,000 per annum to spend.The Trustees meet twice yearly normally in May and November
Applications should be made in writing andsent toThe AdministratorThe Burwood Park Foundation for the DeafInce Castle, Saltash, Cornwall. PL12 4RA
Searching for a QToD?Job vacancies can be advertised on the
BATOD website at a cost of £150.00
Teaching Section - Situations Vacant
www.BATOD.org.uk
one of our most popular pages - especially ona Monday with hundreds of ‘hits’!!!
email your Word file to [email protected] instructions about invoicing and your advertshould appear very soon afterwards AND REMAINVISIBLE until after the deadline! If you put in anemail contact this will be an active link so potentialapplicants can contact you directly. Embeddedlogos should be sent as additional .jpg or .gif files aswell.
Value for money advertising
OORRGGIIVVAA,, SSOOUUTTHHEERRNN SSPPAAIINNA choice of charming holiday cottages with pools
in a beautiful valley surrounded by mountains
an hour south of Granada
Sleeping 2-10 from £210 pwk
www.elrosalholidays.com
email: [email protected]
or phone Hermione Bromley 0034 958 785657
©BATOD Magazine March 05 51
www.batod.org.uk
53955-BatodMarch05 8/3/05 4:24 pm Page 53
creo

52 ©BATOD Magazine March 05
A&ICT(C)Audiology and ICT Committee (BATOD NEC)ADPS Achievements of Deaf Pupils in ScotlandAGC Automatic Gain ControlAGM Annual General MeetingAIDS Acquired Immune Deficiency SyndromeATT Automated Toy TestBATOD British Association of Teachers of the DeafBBC British Broadcasting CorporationBCCIP Birmingham Children's CI ProgrammeBCIG British Cochlear Implant GroupBecta British Educational Communication technology AgencyBETT British Educational Technology for TeachersBSL British Sign LanguageBTEC Business and Technician Education CouncilCACDP Council for the Advancement of Communication with Deaf People CAP Communication Aids Project CAP Categories of Auditory PerformanceCD ROM Compact Disk Read Only Memory (also CD)CD Compact DiskCHU/CESDA Paediatric Unit of cochlea implants - ToulouseCI Cochlear ImplantCICS Cochlear Implanted Children’s SupportCIP Cochlear Implant ProgrammeCODPUKChildren of Deaf Parents UKCSW Communication Support WorkerCTDD College of Teachers of the Deaf and DumbCUP Cambridge University PressdB decibeldBA decibel A scale (soundfield measurement)DCCAP Deaf Children's Communication Aids ProvisionDfES Department for Education and Skillsdpi dots per incheg for exampleEI(C) Education Issues Committee (BATOD NEC)EMA Education Maintenance AllowanceEMAP East Midlands Associated PressENT Ear, Nose and Throateps encapsulated post scripFAQs Frequently Asked QuestionsFE Further EducationFEAPDA European Federation of Teachers of the Deaf.FFSB Federation Francophone des Sourds de Belguiquefm frequency modulationGCSE General Certificate of Secondary Education gif Graphic Interchange Format (file name extension)GOSH Great Ormond Street Hospital HI Hearing-ImpairedHIV Human Immunodeficiency VirusHND Higher National Diplomahtm hyper text markup language (html)http hyper text transfer protocolICED International Congress on the Education of the DeafICT Information Communications TechnologyICTOD Implant Centre Teacher of the Deaf IHR Institute of Hearing ResearchILiP Listening Progress ProfileILP Individual Learning ProgrammeInc IncorporatedIQ Intelligence QuotientISBN International Standard Book NumberingISSN International Standard Serial NumberJCQ The Joint Council for QualificationsJEB Joint Examination Boardjpg Graphics file type/extension (Joint Photographic Experts Group)KID Keratitis-Ichthyosis-Deafness syndromekg kilogramLEA Local Education AuthorityLiP Listening Progress ProfileLPC Cued Speech in France/SpainLSA Learning Support AssistantM&FC Membership and Finance CommitteeMAIS Meaningful Auditory Integration ScaleMBE Member of the British EmpireMOC Modelo Oral Complementada (Spain)MP Member of ParliamentMRC Medical Research CouncilMRI Magnetic Resonance ImagingNAACE National Association of Advisers for Computers in EducationNATD National Association of Teachers of the DeafNATED National Association for Tertiary Education with Deaf people
Ab
bre
via
tio
ns
a
nd
Ac
ro
ny
ms
u
se
d in
th
is M
ag
az
ine
NCTD National College of Teachers of the DeafNDCS National Deaf Children's SocietyNEAP Nottingham Early Assessment PackageNEC National Executive Council (of BATOD)NVQ National Vocational QualificationNY New Yorkorg organisationP&PC Publications and Publicity Committee (BATOD NEC)PC Cued Speech in France/SpainPC Personal ComputerPD(C) Professional Development (Committee)pdf portable document format (for Acrobat Reader)PE Physical EducationPhD Doctor of Philosophypwk per weekQTOD Qualified Teacher of the DeafRCIC Regional Cochlear Implant CentreRNID Royal National Institute for Deaf peopleRSD Royal School for the Deaf RSDCD Royal Schools for the Deaf and Communication DisordersSEN Special Educational NeedsSLT Speech and Language Therapist (also S<)SMS Short Message ServiceSNAP Story Narrative Assessment ProcedureSOECIC South of England Cochlear Implant Centre STD Society of Teachers of the DeafTES Times Education SupplementTHRASS Teaching Handwriting Reading And Spelling Skillstif Tagged Image File (file name extension)ToD Teacher of the DeafTS (Mary Hare) Training ServicesUCL University of Central LondonUK United KingdomUSA United States of America USB Universal Serial Busv/f voice/faxVOCA Voice Output Communication AidVSO Voluntary Service Overseaswww world wide webIf you have found an acronym in the Magazine that isn't explained inthis list.... then use www.acronymfinder.com to help you work it out!
��Free 64 page colour catalogue��Over 1,000 titles always in stock ��Immediate despatch��Fast and friendly service��Professional advice service�All major credit cards ac-cepted �Official orders accepted
The New Building Ellwood Road, MilkwallColeford, Gloucestershire England, GL16 7LE Tel: 01594 833858 (voice/minicom)Videophone: 01594 810637 email: [email protected]
Specialists in Books, Videos, CD-ROMs about Deafness, Deaf Issues and
Deaf Education
Web shopping:
NEW CATALOGUE
FEBRUARY 2004
NNEEWW CCAATTAALLOOGGUUEE
FFEEBBRRUUAARRYY 22000055
53955-BatodMarch05 8/3/05 11:58 am Page 54
creo

©BATOD Magazine March 05 53
BETT 2005This year's trip to the BETT exhibition proved to bemore of a personal high spot than in previous yearsand a little nerve wracking, as I was presented withKnightsfield School's Naacemark Award. Originallythe acronym Naace stood for National Association ofAdvisers for Computers in Education, anorganisation which was established in 1984.However Naace now welcomes anyone who isinterested in advancing education through theappropriate use of information and communicationstechnology.
The Naacemark has been developed in associationwith Becta and is a quality mark award whichrecognises a school's success in developing andimplementing a strategic approach to ICT. It provides a framework for using ICT to enhanceteaching and learning and provides opportunities forthe school community to develop ICT capability.The scheme was launched for mainstream schoolsin 2003, with special needs criteria following in 2004.There are now 270 schools across 84 LEAs thathave achieved the Naacemark, of these just over aquarter are secondary schools and about 5% arespecial schools. Knightsfield's assessment for theNaacemark took place in November, against thesecondary school criteria, as these proved to bemore appropriate than those for special schools. It was very exciting to be presented with the awardat BETT, especially when Steve Bacon, generalsecretary of Naace, confirmed that this was the firstaward for a school for deaf children.
The Naace website gives details of how schools cangain the award and their assessment framework isan excellent tool which schools can use as atemplate for their ICT development plans. There arevarious aspects, including using ICT to facilitateinclusion, outreach and partnership activities andlinks with parents. www.naace.org.uk
Another in the BETT awards was the 'LearningAssistance - Secondary and Post 16/LifelongLearning' category. Roy Schumann is LearningSupport Assistant, responsible for ResourceDevelopment at West Cheshire College, Cheshire.
Since joining the CollegeRoy has expressed anactive interest in using ICTto increase the accessibility
to resources and promote deaf awareness.
Roy sees his role as taking the hard work out ofmaking education accessible for pupils, families andfriends in the deaf community and supports pupilsfrom 16-80+ years at the college. Roy recentlydeveloped a package from scratch using PowerPointto create a very simple but effective way to teachsign language through visual explanations, usingdigital images and video clips to describe and playout each sign.
This bespoke package is being used as a teachingtool within the college to allow students at thecollege to learn sign language but it is also helpingteachers within the college to learn and be moreopen and approachable for deaf people.
The exhibition was again huge this year and theresimply was not time to look at everything.
Although not really looking for new computers, I gotquite excited about Apple's new Mac Mini which isonly about the size of a pack of serviettes! As akeen user of iMovie and digital video, the idea ofbeing able to buy Macs at under £350 seriouslyappealed, especially as the computer can useexisting peripherals such as monitors and USBkeyboards and mice. Personally I would like aniPhoto so I can carry around all my digitalphotographs and bore the relatives with the latestholiday snaps, not by printing them out as I currentlydo but by simply plugging the gadget into their TV.www.apple.co.uk
Kudlian have released a number of excellent lookingtools and plug-ins to use with iMovie. EssentialTools for iLife provides a number of resourcesincluding a chroma key facility has to be a 'musthave' item for all iMovie users. The idea of beingable to place a photo, graphic image or moviebehind a subject that has been filmed in front of achroma key backdrop not only gives the possibility
ICT for teachers Sharon Pointeer
Welcome to this edition of the ICT Newspage. If you would like to contribute anythingto this page, please contact Sharon Pointeer, the ICT Newspage [email protected]
53955-BatodMarch05 8/3/05 9:20 am Page 55

54 ©BATOD Magazine March 05
of exciting locations for pupils acting but couldprobably allow sign language interpretation to beadded to a digital video. Other iMovie/iDVD plug-insare provided by Charting and Graphing, WeatherReporting and Geography and Times Gone By.They have also produced On-Camera which givesyour Mac teleprompting and titling ability. Thebrochure says that movies can be published with asubtitle track which can be turned on and off.Kudlian have also produced I Can Animate, aflexible animation package, which is available for PCand Mac. It allows a variety of techniques to beemployed including use of digital images, drawing orpainting. There is also Slide Show, a newpresentation package which allows pupils very easilyto display pictures, create presentations and stories.Suitable for PC or Mac, the finished work can beexported as a QuickTime movie for sharing orputting on a web page. www.kudlian.net
For those of you who do not use Apple Macs butwant easy to use digital video editing Logotron havecome up with Revelation Sight and Sound. Thepackage has been developed specifically forchildren, although the facilities it provides wouldkeep many adult ‘Steven Spielberg wannabes’ morethan happy. It uses chunky, easy to understandicons and comes with an extensive activity guidecontaining structured, differentiated activitiesdesigned to develop understanding of digital video.At £55 for a single user pack, this has to be a verycost effective way into digital video. Typical of allLogotron's software you can be confident that it hasbeen extensively tested prior to release and it will doexactly what it says in the brochure. Logotron werealso demonstrating a number of other new packagesat BETT, including Thinking with Pictures - a mindmapping tool, Junior Simulation Insight - a computermodelling tool and Visual Fractions which is suitablefor using on a classroom whiteboard.www.logo.com
Teaching sensing and control with control boxes anda variety of sensors is great but few schools havesufficient kit for all the pupils to be hands-on for allactivities. I was excited therefore to find theLogiblocs stand where for a modest price it waspossible to purchase a kit containing plug togethermodules to make a number of simplesensing/control circuits and a remote control buggy.The sets come with a teacher’s guide andinstruction cards for pupils and cover aspects ofboth the ICT and the Design and Technologyprogrammes of study. As an added bonus £50 ofthe cost can be offset against e-learning credits andthere is also a software package which simulatesthe blocks on a computer. www.logiblocs.com
Similar kit, although possibly aimed more at Scienceand Electronics, comes from Cambridge BrainBox.Their kits contain easy to use colour codedcomponents which are assembled on a base boardusing press-studs. The kits vary from a simplePrimary kit which has instructions for 100experiments costing £14.99 through to theSecondary Explorer kit with instructions for over1200 experiments costing £49.99. At these pricesthe kits would also make excellent presents, as theycome with step by step instructions.www.cambridgebrainbox.com
There were lots of stands selling books, worksheets,posters and other non-ICT resources. Companieslike Prime-Ed, Hopscotch and Keynote have lots ofphotocopiable resources, at different levels fordifferent ages and abilities. New out from Prime-Edwere their Internet Challenges, which are aimed at8-12 year olds but could easily be used with olderpupils. These consist of single page worksheetsposing questions deigned to give pupils a purpose touse the Internet and fine-tune their research skills.Some of the worksheets to encourage pupilscritically to question and evaluate the informationthey find on the Internet, which has to be a goodthing. A number of companies are now selling theirresources on CD-ROM for people to print outthemselves, which often means they can be boughtwith e-learning credits. Daydream Education sellposters for all subject areas, the posters are alsoavailable as A5 size booklets which are great forrevision and some of the posters are now availablein an enhanced form for use on interactivewhiteboards.www.prim-ed.com
www.hopscotchbooks.comwww.e-worksheets.comwww.daydreameducation.co.uk
For those wanting portable word processing devicesthere were a number on offer, including the familiarAlphaSmart 3000, Neo and Dana which range froma fairly straightforward word processor through tosomething which is more or less a portablenotebook computer. The CalcuScribe Duo is similarbut has the added advantage of a built-in Mathsprocessor which easily allows the writing ofmathematical expressions as part of the work. Alsoon view was the QuickPAD which comes completewith a pre-installed typing tutor. With prices startingat £140 they are worth considering for pupils withwritten language difficulties. These devices areavailable from a variety of sources such as InclusiveTechnology and Keytools, both of whom specialisein equipment for special educational needs.www.inclusive.co.uk www.keytools.com
53955-BatodMarch05 8/3/05 9:20 am Page 56

This subscription can be claimed against income tax: for those who pay tax at 40% this means a saving of approximately£20.00 pa and for those members in the lower band a saving of some £10.00. You do not normally need a receipt forthis; just put it on your income tax form. A list of previous subscription details can be found on the BATOD website:follow BATOD/BATOD membership/back-subscriptions information.
For those retired members who no longer wish to receive the Journal there is a concession to pay a reducedsubscription. This concession also applies to associate members who are employed as Teaching Assistants or in similarroles who do not wish to receive the Journal.
Retired members who reach the age of 80 are entitled to free membership of the Association. Members who reach thismilestone are invited to contact the Membership Secretary.
Full and associate members who are entitled to a reduced subscription should notify the Membership Secretary of theircircumstances by 30 June for the following year’s membership, to enable the necessary paperwork to be completed.
Anyone with a change in circumstances (eg changing to retired status) should inform the Membership Secretary as soonas they are able. Cheque payers will be sent a reminder about payment in June. Direct Debits will be alteredautomatically for payments in August and beyond.
Members are reminded that membership of the Association is only open to individuals. There is no category for Serviceor School membership. We are aware that some members have their subscription paid for them and that some havetheir mailing to their work address. Only the named individual is the member and no other person at that address canclaim any benefits of membership.Any enquiries should be made to:
email: [email protected] Membership Secretary112 Deas AvenueDingwallRoss-shire IV5 9RJ
Membership subscription ratesMembership subscription ratesdue 1 AugustAnnual Quarterly Cheque
Direct Debit Direct DebitFull members in employment £ 55.00 £ 14.50 £ 60.00Associate members in employment £ 55.00 £ 14.50 £ 60.00Full members taking a career break £ 27.50 £ 7.25 £ 30.00Associate members - unwaged £ 27.50 £ 7.25 £ 30.00Retired members £ 27.50 £ 7.25 £ 30.00
2004 - 2005
©BATOD Magazine January 05 55
All members are reminded that the Membership Secretary MUST be notified of any change ofaddress to ensure that labels are changed and Magazines and Journals reach the new address.
Name changed to:
Address changed to:
Post code Post code:
Telephone:email:
53955-BatodMarch05 8/3/05 9:20 am Page 57

If you know about, or are organising, an event that you think other Teachers of the Deaf may be interested in please email the details that can beadded to the calendar to [email protected] (date, organiser, title, venue). Remember to decode the acronym so we know who is theorganiser! There are already entries on the website Calendar for 2006. The Calendar on the BATOD website is edited as soon as we know about meetings.Additional information about courses and registrations forms may also be linked to the calendar entries.
Date Organisation Meeting Topic Venue
March 2005 1 Ear Foundation Introductory programming for the Advanced Bionics
Cochlear Implant System Ear Foundation, Nottingham1 DCCAP ICT training courses for Teachers of the Deaf: 2005 Exeter2 Early Support Early Support Monitoring Protocol Training Bury St Edmunds2 DCCAP ICT training courses for Teachers of the Deaf: 2005 Bristol2 Seabrook Audiology BSA Certificate in Otoscopy & Impression Taking Gloucester2 Ear Foundation Trouble-shooting cochlear implants Ear Foundation, Nottingham3 DCCAP ICT training courses for Teachers of the Deaf: 2005 Birmingham3 Deafworks Programme for Deaf Professionals. Want a new job? Clerkenwell, London4 Ear Foundation Implantation in under-one deaf infants University of Nottingham5 Mildmay Infant & Junior School Essex working together day (free entry) Chelmsford, Essex8 DCCAP Communication Books and how to make them Bristol
10 Early Support Early Support Monitoring Protocol Training Dorset10 UKCoD Health Promotion for Deaf Communities Conference London11 DCCAP DCCAP Assessor Training Day Reading11 Ear Foundation Fitting young children with hearing aids Ear Foundation, Nottingham11 Deafworks Deaf Awareness Clerkenwell, London12 BATOD Conference Reasonable Adjustments and AGM Hinckley, Leics13 BATOD NEC Association Business Birmingham14 Ear Foundation Supporting children with CIs at 2dry level; LSAs; course 3 Ear Foundation, Nottingham15 DCCAP DCCAP Assessor Training Day Manchester15 Early Support Early Support Monitoring Protocol Training Morden15 BATOD CPD Deafness & Dyslexia: identification, assessment, practicalities Newbury16 Ear Foundation PALS; CI children and families from multi-lingual backgrounds Ear Foundation, Nottingham
15 - 16 THRASS The use of THRASS in the education of the Deaf Gillitts, Durban,17 Deafworks Programme for Deaf Professionals Boost your interview skills Clerkenwell, London17 Mary Hare TS & Burwood Centre Musicality and deaf children. Practical music and dance
activities for pre-school and primary aged deaf children Newbury18 Early Support Early Support Monitoring Protocol Training Coalville, Leicestershire
11 - 18 Deafworks Getting ready for Level 2 assessment (3 day course) Clerkenwell, London17 - 19 EMAP & TES Education Show NEC Birmingham
22 DCCAP ICT training courses for Teachers of the Deaf: 2005 Cambridge23 DCCAP ICT training courses for Teachers of the Deaf: 2005 London24 DCCAP ICT training courses for Teachers of the Deaf: 2005 Southampton
21 - 25 Cued Speech Association UK Cued Speech Easter Course, Foundation Level. . Exeter, Devon.April
2 Deafworks How should hearing people teach Deaf Awareness? Clerkenwell, London4 Deafworks Level Two Clerkenwell, London5 Deafworks Level One (every Tuesday for 15 weeks) Clerkenwell, London6 Healthy Deaf Minds Topic to be announced Euston
6 - 7 Independent Living, Scotland Independent Living Scotland 2005 (free admission) Glasgow9 Deafworks Training the Trainers in Deaf Awareness (1 of 4) Clerkenwell, London
11 Ear Foundation Deaf professionals and cochlear implantation Ear Foundation, Nottingham11 SOECIC Cochlear Implant workshop Southampton University14 Deafworks How to be a Time Management Expert Clerkenwell, London15 THRASS Teaching Handwriting Reading And Spelling Skills Suffolk
14 - 16 Ear Foundation Advanced Seminar for CI Professionals University of Nottingham16 - 17 Deafworks Between BSL One and Two (2 day course) Clerkenwell, London
18 Seabrook Audiology CPD course on the Hearing Aid Council Code of Practice Gloucester19 Mary Hare TS & Burwood Centre Prematurity and Deafness Newbury19 NDCS Radio Aids Workshop London
20 - 21 Ear Foundation Tait Video analysis Ear Foundation, Nottingham25 DCCAP ICT training courses for Teachers of the Deaf: 2005 Manchester26 Ear Foundation Making multi-agency work happen with young deaf children Ear Foundation, Nottingham26 DCCAP ICT training courses for Teachers of the Deaf: 2005 Newcastle27 DCCAP ICT training courses for Teachers of the Deaf: 2005 Lancaster
21 - 28 Deafworks A Two Day Introduction to BSL Clerkenwell, London28 Ear Foundation SNAP Dragons (two days 28/04/05 and 16/06/05) Ear Foundation, Nottingham
28 - 29 Mary Hare TS & Burwood Centre Using the Reynell developmental Language Scales Version III NewburyMay
5 THRASS Teaching Handwriting Reading And Spelling Skills Oldham LEA5 - 6 Deafworks Getting ready for Level 2 assessment (2 day course) Clerkenwell, London5 - 6 Deafworks Getting ready for Level 2 assessment (2 day course) Clerkenwell, London
6 DCCAP DCCAP Assessor Training Day Reading7 BATOD Scotland Audiology Update (half day meeting) Donaldson's College, Edinburgh
10 DCCAP DCCAP Assessor Training Day Manchester10 Seabrook Audiology CPD course on Masking in Audiometry Gloucester10 Ear Foundation Working with teenagers with CIs Ear Foundation, Nottingham11 Ear Foundation Teachers working with parents Ear Foundation, Nottingham11 Seabrook Audiology BSA Certificate in Otoscopy & Impression Taking Gloucester12 Mary Hare TS & Ewing Foundation Supporting thinking & learning skills: the primary aged deaf child Newbury12 Deafworks Polish up your work presentations Clerkenwell, London13 Mary Hare TS & Ewing Foundation Supporting thinking and learning skills at Key Stages 3 & 4 Newbury14 Deafworks Being a Good BSL Tutor Clerkenwell, London
Meetings and training to know about Calendar
56 © BATOD Magazine January 05
Item
s no
ted
on t
his
Cal
enda
r m
ay h
ave
been
adv
ertis
ed w
ithin
the
Mag
azin
e or
the
info
rmat
ion
repo
rted
by
tele
phon
e.
BA
TO
D is
not
nec
essa
rily
the
orga
nisi
ng b
ody.
Ple
ase
con
tact
th
e O
rgan
isin
g b
od
y (c
olu
mn
2)
for
det
ails
of
con
fere
nce
s, N
OT
th
e E
dit
or
of
this
Mag
azin
e.
53955-BatodMarch05 8/3/05 9:20 am Page 58
creo

Officers of nations and regionsBATOD contacts and Magazine Distribution
Northern IrelandChairperson: Sue McCrum, 6 Millhill Drive, Ballynahinch, County Down BT24 8LLSecretary: Wendy Martin, 15 Ballyholme Esplanade, Bangor BT20 5LZTreasurer: Paula McCaughey, Tullynacree Road, Crossgar BT30 9AHScotlandChairperson: Fiona Mackenzie, 112 Deas Avenue, Dingwall, Rosshire IV15 9RJSecretary: Margaret Highet, 26 Sinclair Drive, Largs, Ayrshire KA30 9BLTreasurer: Ann Dykes, 4 Grieve Croft, Silverwood, Bothwell, Glasgow G71 8LUWalesChairperson: Maggie Denholm, Gowanlea, Hoel y Delyn, Camarthen SA31 1EESecretary: Marian Williams, ‘Ty’r Grofften’, 19 Pen y Graig, Alltwen, Pontardwe SA8 3BSTreasurer: Norma Moses, 28 Pen y Groes, Groesfaen, Pont y Clun, Mid Glamorgan CF7 8PAMidland Chairperson: Jo Butler, 222 The Avenue, Acocks Green, Birmingham B27 6NRSecretary: Ursula Walker, 207 Bentley’s Lane, Walsall WS2 8SPTreasurer: Robert Miller, 13 Derby Close, The Meadows, Broughton Astley, Leics LE9 6BENorthChairperson: Colin Peake, 17 Vickers Close, Hawarden, Clwyd CH5 3HUSecretary: post vacantTreasurer: Laverne Smare, 6 Dentdale, Daleside, Mount Pleasant, Houghton-le-Spring DH4 7QQSouth Chairperson: Angie Reese, 9 Wychwood Close, Canons Park, Edgware, Middlesex HA8 6TESecretary: Sheila Smith, 26 Lyndhurst Gardens, Finchley, London N3 1TBTreasurer Cindy Paulding, Primary Hearing Centre, Kingsley Primary School, Chapman Road, Croydon CR0 3NXSouth West Chairperson: Sue Barnsley, 100 Uppleby Road, Parkstone, Poole, Dorset BH12 3DFSecretary: Lorna Warden, 57 Sunrising Estate, East Looe, Cornwall PL13 1NDTreasurer: John Shaw, School House, Weirfield Road, Exeter, Devon EX2 4DN
BATOD Magazine distribution from:Royal Schools for the Deaf, Stanley Road, Cheadle Hulme, Cheshire SK8 6 RQ
Association Magazine ISSN 1366-0799Published by The British Association of Teachers of the Deaf, 41 The Orchard, Leven, Beverley HU17 5QA
Printed by White Horse Press, 1 Hambridge Lane, Newbury, Berkshire RG14 5TU
Articles, information, contributions andadvertisements for the Association Magazineshould be sent to:
Mrs Ann UnderwoodBATOD Magazine Editor41 The OrchardLeven, BeverleyEast YorkshireHU17 5QA
tel/fax 01964 544243email [email protected]
Association information, general queries and allmatters not connected with the Magazine or theJournal should be addressed to:
BATOD SecretaryMr Paul Simpson175 Dashwood AvenueHigh WycombeBuckinghamshireHP12 3DB
tel/fax 01494 464190email [email protected]
Submissions to the Journal ‘Deafness and Education International’ should besent to:
Dr Clare Gallawayc/o Whurr Publisher Ltd 19a Compton TerraceLondon N1 2UN
email [email protected]
DISCLAIMER
The Editors and the Association do not necessarily
endorse items or the contents of advertisements
published in the Magazine and cannot accept
responsibility for any inaccuracies.
Please note that items from this Magazine may not
be reproduced without the consent of BATOD and
must acknowledge the source.
Photocopying items may breach copyright.
53955-BatodMarch05 8/3/05 9:20 am Page 59
creo

For more information please contact
BioAcoustics LimitedPO Box 1153LutonLU1 2WWTel: 01582 431000www.BioAcoustics.com
53955-BatodMarch05 8/3/05 9:20 am Page 60
creo