FOCUS ON ENDOCRINE NEOPLASIA Neuroendocrine Tumors FAUSTO BOGAZZI University of Pisa Department of...
49
FOCUS ON ENDOCRINE NEOPLASIA Neuroendocrine Tumors FAUSTO BOGAZZI University of Pisa Department of Endocrinology and Metabolic Disease Rome, 10 July 2010
-
Upload
tracey-watson -
Category
Documents
-
view
218 -
download
2
Transcript of FOCUS ON ENDOCRINE NEOPLASIA Neuroendocrine Tumors FAUSTO BOGAZZI University of Pisa Department of...

FOCUS ON ENDOCRINE NEOPLASIA
Neuroendocrine Tumors
FAUSTO BOGAZZIUniversity of Pisa
Department of Endocrinology and Metabolic Disease Rome, 10 July 2010

Neuroendocrine TumorsThe origins
1897Identification of enterochromaffin cells Kulchitsky 1856-1925
1948 Isolation of serotonin (5-HT) Rapport M.
Foregut
Midgut
Hindgut
1953 Evidence of 5-HT in carcinoid tumors Lembeck F.
1963Introduction of carcinoid tumors embryologic classification (foregut, midgut o hindgut) Williams E.D. e Sandler M.
Siegfried Oberndorfer 1876-1944
1907 Introduction “karzinoide” concept (benign features)
1929 Identification of malignant and metastatizing neuroendocrine tumors

Neuroendocrine TumorsEpidemiology
Lung Appendix Stomach ColonSmall Bowel Recto Cieco Pancreas
0,6
0
1,4
1,0
0,2
Incid
en
ce e
very
10
0.0
00
su
bje
cts
1980 1990 2000
1,2
0,8
0,4
1 Oberg et al. ESMO Guidelines Working group. Ann Oncol 2009; S4: 150-1532 Newton JN et al. Br J Cancer 1994; 70: 939-42
3 Yao JC, et al. J Clin Oncol 2008; 26(18): 3063-3072.
Rare tumors: incidence 2.5-5/100,000/year in USA1
(largest group: small intestinal neuroendocrine tumors → 2.4/100000/y) 1
incidence 0.7/100000/year in Europe2
Higher incidence at autopsy: 8.4/100000/year1
Increasing incidence in the epidemiologic registry of USA3

100.000
Cases (
n)
0
1.000.000
Prevalence (database SEER)
1.200.000
NET Stomach Pancreas EsophagusColon - recto Liver
Yao JC, et al. J Clin Oncol 2008; 26(18): 3063-3072.
NET are the second most common tumors of gastrointestinal tract
Neuroendocrine TumorsEpidemiology

1.Oberg et al. ESMO Guidelines Working group. Ann Oncol 2009; S4: 150-153.2.Modified from Vierimaa et al. Eur J Endocrinol 2007; 157: 285-294
NET can appear at all age
Higher incidence from the fifth decade
Appendix carcinoid higher incidence at <30 years Patients with MEN1 or vHL: clinical onset 15 years earlier than sporadic forms
Neuroendocrine TumorsEpidemiology

Modlin IM et al. Lancet 2008.
Mortality
at the moment is nearly stable
Neuroendocrine TumorsEpidemiology

Hauso et al. Cancer 2008; 113: 2655-64Panzuto et al. Endocrine-Related Cancer
2005;12: 1083-92.
Mortality depends on:
Neuroendocrine TumorsEpidemiology
Site of NET Age at diagnosis Primary tumor dimension Tumor degree differentiation (ki67) Disease stage

Manifestation depends on:
Site of primary tumor
Functioning of the tumor
Non functioning NET: symptoms due to “mass effect” or distant metastases
Functioning NET
Paraneoplastic Syndrome: Cushing Syndrome, Acromegaly
Neuroendocrine TumorsClinical Manifestation
Tumor Syndrome Hormones Site
Carcinoid tumor Carcinoid Syndrome Serotonin, tachichinin, bradichinine, histamine Midgut Foregut
Insulinoma Hypoglycemia Insulin Pancreas
Glucagonoma Becker Syndrome (hyperglicemia, migrating necrolitic eritema) Glucagone Pancreas
Duodenum
Gastrinoma Zollinger-Ellison Syndrome Gastrin Pancreas Duodenum
VIPoma Diarrea ipokaliemia-achloridria VIP Pancreas
Lung

Neuroendocrine TumorsDiagnosis
1. Kloppel et al. ENETS Guidelines . Neuroendocrinology 2009: 90-162-169
Need of a documented hystopathological diagnosis
Biopsy
Resection Specimen
TNM classification

Oberg et al. ESMO Guidelines Working group. Ann Oncol 2009; S4: 150-153; Kloppel et al. ENETS Guidelines . Neuroendocrinology 2009: 90-162-169
.
Neuroendocrine TumorsDiagnosis
TNM classification
specific for different sites
Gastric Duodenum/ampulla/proximal jejunum
Pancreas Lower jejunum/ ileum
Grading Proposal for foregut (neuro)endocrine tumors
Grade Mitotic count (10HPF)a Ki-67 index (%)b
G1 <2 ≤ 2
G2 2-20 3-30
G3 >20 >20a 10 HPF: high power field= 2mm2, at least 40 fields (at 40x magnification) evaluated in areas of highest mitotic densityb MIBI antibody: % of 2.000 tumor cells in areas of highest nuclear labeling

11
Neuroendocrine TumorsPathology and Staging predicts Prognosis

12
Neuroendocrine TumorsGrading Predicts Prognosis
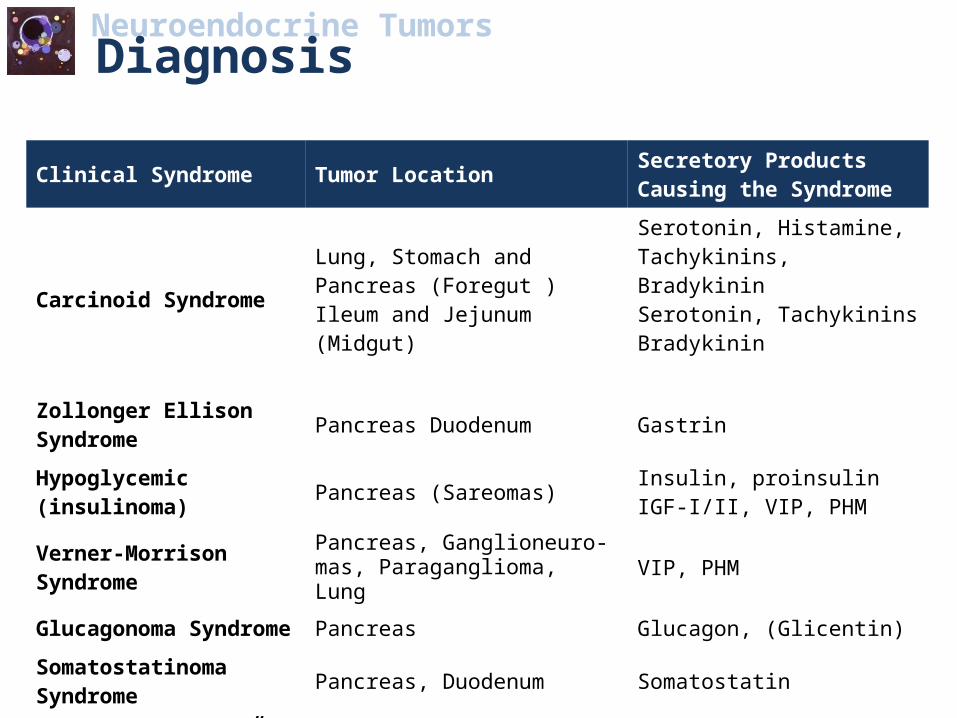
Clinical Syndrome Tumor Location Secretory Products Causing the Syndrome
Carcinoid SyndromeLung, Stomach and Pancreas (Foregut )Ileum and Jejunum(Midgut)
Serotonin, Histamine, Tachykinins, BradykininSerotonin, TachykininsBradykinin
Zollonger Ellison Syndrome Pancreas Duodenum Gastrin
Hypoglycemic (insulinoma) Pancreas (Sareomas) Insulin, proinsulin IGF-I/II, VIP, PHM
Verner-Morrison Syndrome Pancreas, Ganglioneuro-mas, Paraganglioma, Lung VIP, PHM
Glucagonoma Syndrome Pancreas Glucagon, (Glicentin)Somatostatinoma Syndrome Pancreas, Duodenum Somatostatin
“Non functioning” Tumours Pancreas, Colon CgA, HCG-α/β, PP, PYY (no endocrine related symptoms)
Neuroendocrine TumorsDiagnosis

Neuroendocrine TumorsCarcinoid Syndrome

Histopathology Argyrophil/argentaffin staining CgA, Serotonin
Tumour Markers CgA, u-5-HIAA, p-NPK, p-Subst-PP-ACTH, pCRF, PGHRH, s-calcito-nin, p-ADH, s-PP, s-HCGα/β, u-Histamine
Other Markers
Stimulatory Tests Flush provocation: Pentagastrin 0,6ug/kg bw i.v., measuring p-NKP every 5 min for 30 min
Radiology Octreoscan (111Ind-DTPA-octreotide)CT, US, MRI, (CT-angiography)
Other Investigations Endoscopy (endoscopic ultrasound)
Neuroendocrine TumorsCarcinoid Tumour Diagnosis

Tumour Location Pancreas 50-60%Duodenum 40-50%(sometimes both, MEN-I)20-25% Related to MEN-150-70% Malignant (lymphnode metastases)Gastrinoma Triangle 80%
Symptoms GastritisRecurrent ulcersDiarrhea (malabsorption)
Neuroendocrine TumorsZollinger Ellison Syndrome

Tumour Location Pancreas>90% malignant
Symptoms Necrolytic migratory erythema
Weight loss
Anemia
Trombosis
Impaired glucose tolerance
Diarrhoea
Neuroendocrine TumorsGlucagonoma Syndrome

Neuroendocrine TumorsGlucagonoma Syndrome

Tumour Location PancreasLungGanglioneuromas>80% Malignant(Pancreatic “nesidioblastosis”)
Symptoms Watery diarrhea (secretory) 3-20 litres/dayHypokalemia, Hypomagnesemia,HypercalcemiaAcidosisFlushingFlaccid distended gallbladderIleus/subileus
Neuroendocrine TumorsVerner-Morrison Syndrome (WDHA:s)

Tumour Location DuodenumPancreasColon/Rectum>80% mixed tumours
Symptoms GallstonesSteatorrheaImpaired glucose toleranceOften “non-functioning” tumours!
Neuroendocrine TumorsSomatostatinoma Syndrome

Neuroendocrine TumorsDiagnosis
O’Toole et al. ENETS Guidelines. Neuroendocrinology 2009; 90: 194-202
Biochemical Markers: Chromogranin A Recognized general serum marker →co-secreted in tumors with amines and
peptides present in neurosecretory granules Can be elevated in functional and non-functional NET More often high in midgut NET and non-functioning pancreatic NET Levels depending on: tumor cell type, differentiation, tumor volume

Neuroendocrine TumorsDiagnosis
O’Toole et al. ENETS Guidelines. Neuroendocrinology 2009; 90: 194-202
Biochemical Markers: Urinary 5-HIAA In carcinoid syndrome sensitivity 70%, specificity 90% Most frequently high in midguts carcinoid than fore- and hindgut tumors Depends on tumor volume, often normal in non metstatic carcinoids At the moment can’t be considered a reliable prognositc factor Use of HPLC has to be preferred
Falsely low: Renal impairment
Falsely high:Malabsorption (coelic disease,
intetsinal stasis, cystic fibrosis); DRUGS (FANS); FOOD (TRIPTOFAN-RICH)

Neuroendocrine TumorsDiagnosis
O’Toole et al. ENETS Guidelines. Neuroendocrinology 2009; 90: 194-202
Biochemical Markers: Gastrin Useful to diagnose Zollinger-Ellison Syndrome Elevated fasting serum gastrin Low gastric pH Secretin test: ∆ gastrin increase ≥110 pg/ml (sensitivity 93%)
∆ gastrin increase ≥200 pg/ml (sensitivity 85%) ∆ gastrin increase ≥ 120 pg/ml (sensitivity 94%;specificity 100%)

Neuroendocrine TumorsDiagnosis
O’Toole et al. ENETS Guidelines. Neuroendocrinology 2009; 90: 194-202
Biochemical Markers: Insulin Useful to diagnose Insulinomas
I. Symptoms of hypoglicemiaII. Glucose < 40-50 mg/dlIII. Relief of sympoms with glucose administration
Whipple’s Triad
72h fast→ gold standard for diagnosing insulinoma To attest: Failure of appropriate
insulin suppression Autonomus insulin secretion
Test endpoint: document hypoglycaemia blood glucose ≤ 2.2 mmol/L (≤ 40 mg/dL) [or <3 nmol/L, 50 mg/dL] concomitant insulin levels > 6 μU/L (≥ 36 pmol/L) A β-hydroxybutyrate level ≤ 2.7 mmol/L ( confirm test validity and inappropriate insulin suppression)
A glucagon test immediately after 72-hour fasting in patients without definitive results recommended
Use of a ratio insulin to glucose is not recommended to aid diagnosis Exercise test immediately after 72 hours fasting in patients without definitive results only in
supervised setting

Total BodyScreening and Staging
Octreoscan (111Ind-DTPA-octreotide) (SRI)Sensitivity <10 mm 40% >10 mm 90%Liver metastases = 90%
Disclosure of Endocrine Pancreatic Tumours
Endoscopic ultrasonography(EUS); sensitivity <10 mm ≈ 50%SRI + EUS sensitivity <10 mm ≈ 90%
Newer Techniques Positron emission tomography with
C11-5 HTP or C11-L-dopa (PET)Traditional Techniques (always a complement)
CT (+ angiography), MRIUS; sensitivity small tumours 10-30%Liver metastases 90%
Neuroendocrine TumorsRadiology of Neuroendocrine Tumours

Neuroendocrine TumorsDiagnosis - Imaging
Table 5: Ramage JK, et al. Gut 2005; 54: 1-16.
Imaging

Scan speed
multidector TC Contrastographic study with acquisition in different phases
Precocious
Arterial (20’’)
Pancreatic (35’’)
Venous (70’’)
Fenchel S et al Eur J Radiol 2003 Horton, Radiographics 2006 Rha, Eur J Radiol 2007
Neuroendocrine TumorsDiagnosis - Imaging

Multidetector TC : gastrointestinal lesions
Neuroendocrine TumorsDiagnosis -Imaging

Octreoscan
Neuroendocrine TumorsDiagnosis -Imaging

Ecography
Neuroendocrine TumorsDiagnosis -Imaging



Neuroendocrine TumorsThe Ultimate Goals for the Treatment of Neuorendocrine Tumours
•Total eradication by surgery (not possible in most cases)
•Abrogation of tumor growth and/or amelioration of clinical symptoms
•Improving and maintaining a good quality of life

Neuroendocrine TumorsTherapy of Neuroendocrine Gut and Pancreatic Tumours
Surgery
Embolisation ± Chemotherapy
Irradiation
Medical Treatment
conventional for bone metastases
experimental (local)
Somatostatin Analogues
α-Interferon
Chemotherapy
even palliative and tumors reduction
111Ind-DTPA-octreotide 45-60 Gy90 Y-DOTA-octreotide

Kaltsas et al. Endocrine Reviews 2004, 25(3): 458-511
first line therapy in localized NET
Neuroendocrine TumorsSurgical Therapy

Important role in hepatic metastatic disease
Neuroendocrine TumorsSurgical Therapy

Neuroendocrine TumorsEmbolisation of Liver Metastases
Biochemical Response Tumour Response
Embolisation(Spongostan®, Gel-Foam) 30-50%
Median duration20-30%
7-10 months
Chemoembolisation(Doxorubicin) 50-80%
Median duration40-50%
10-20 months

PROLIFERATION
DIFFERENTIATION
Biotherapy SSA IFN-α
Chemotherapy
Neuroendocrine TumorsProposed TNM classification and NET therapy
Grading Proposal for foregut (neuro)endocrine tumors
Grade Mitotic count (10HPF)a Ki-67 index (%)b
G1 <2 ≤ 2
G2 2-20 3-30
G3 >20 >20a 10 HPF: high power field= 2mm2, at least 40 fields (at 40x magnification) evaluated in areas of highest mitotic densityb MIBI antibody: % of 2.000 tumor cells in areas of highest nuclear labeling

Neuroendocrine TumorsINF-α Treatment
Subjective Response 50-70%
Biochemical Response 30-70%
Tumor Response 10-15%

Neuroendocrine TumorsSomatostatine Receptors
• Five subtypes cloned: SSTR 1-5
• SOM.14 and 28 bind to all receptor subtypes
• All receptor subtypes are 7 TM receptors and G-Protein coupled
• Effector mediators are C-AMP, CA2+ /K+ FLUX, TYROSINPHOSPHATASES
• Octreotide binds to SSTR2 and SSTR5
• SSTR2 mediates biochemical and tumour responses
• SSTR3 mediates apoptosis
• SSTR5 mediates anti-tumour response different from SSTR2 (NOT VIA PTPI-C BUT CA 2+ /K +FLUX?)

Neuroendocrine TumorsOctreotide Treatment
Subjective Response 30-75% (dose dependent)
Biochemical Response 30-60% (dose dependent)
Tumor Response 0-15% (not dose dependent)
Time (months)
Pro
po
rtio
n w
ith
ou
t p
rog
res
sio
n
0
0.25
0.5
0.75
0 6 12
18
24
30
36
42
48
54
60
66
72
78
0
0.25
0.5
0.75
1
0 6 18
24
30
36
42
48
54
60
66
72
78
84
Pro
po
rtio
n w
ith
ou
t p
rog
res
sio
n
Time (monhs
)

Tachifilaxis: Hormone secretion
Hofland, Endocrine Review 2003
Somatostatine Analogs
Neuroendocrine TumorsMedical Therapy
Tachifilaxis: antiproliferative effectWynick D, Clin Endocrinol (Oxf). 1989 Resistance of metastatic pancreatic endocrine tumours after long-term treatment with the somatostatin analogue octreotide.
Lamberts SW, Acta Endocrinol (Copenh).,1988Development of resistance to a long-acting somatostatin analogue during treatment of two patients with metastatic endocrine pancreatic tumours.
Koelz A Gastroenterology. 1987Escape of the response to a long-acting somatostatin analogue (SMS 201-995) in patients with VIPoma.

Neuroendocrine TumorsChemotherapy of Neuro-Endocrine Gut and Pancreatic Tumours
ResponseRate
Endocrine pancreatic Tumor Streptozocin + 5 FU 40-60%
Streptozocin + doxorubicin ≈ 60%
Cisplatinum + Etoposide(low differentiated tumors)
≈ 50%
Taxol + doxorubicin ≈ 40-50%
Midgut Carcinoid Tumours Streptozocin + 5 FU 10-30%
Cisplatinum + Etoposide 10-15%

Neuroendocrine Tumors PRRT:
Effects depending on: Radiosensibility:
Growth pattern of the tumor DNA repair
Concentration of radioactivity on the tumor (adsorbed dose)
Reubi JC et al. Eur J Nucl Med 2000
Receptorial affinity of radiopeptides
Receptorial density on the tumors and other organs
Mts linfonodali node mets
from paraganglioma
< liver
Mts linfonodali
da NET GHRH-sec.
> liver» kidney& spleen
VIP-secr.pancreatic NET
Pharmacokinetic: fast plasmatic clearance and renal excretion

Neuroendocrine Tumors PRRT:
Response: predictive factors
Elevated uptake Presence of liver metastasis
Progression: predictive factors
Elevated Ki-67 Higher tumor mass

New prospective will be available..
New Therapies
Neuroendocrine TumorsMedical Therapy:
At the moment drugs used only in clinical trialsModlin et al. Lancet Oncology 2008; 9: 61-72

Neuroendocrine TumorsConclusions
NET are rare neoplasms and they still remain orphan tumors with a survival that is
stable over the past three decades
Many physicians are involved in the management of NET having to cooperate daily
Therapeutic strategies must be individualized depending on tumor type, site, spread,
symptoms and general condition of the patient
We still need..• More reliable markers• Better tumor localization• Cell lines and models to define biology, behavior and genetics• More numerous and randomized trials• To develop molecularly targeted therapies• Centres of excellence and NET clinical teams to coordinate multicentre
studies, extend clinical and tissue databases

Vasily Kandinsky Several Circles 1926 oil on canvas; Solomon R. Guggenheim Museum, New York
Thanks for your attention

Acknowledgments
Enio Martino Luca Manetti Sandra Brogioni Chiara Sardella Isabella Lupi Chiara Cosci Luca Tomisti Enrica Dell’Unto Martina Lombardi Claudio Urbani Ilaria Scattina Valentina Raffaelli Francesco Raggi Dania Russo