Five years’ experience at a single centre of craniocerebral injury from winnowing fan blades
4
Clinical Study Five years’ experience at a single centre of craniocerebral injury from winnowing fan blades Apoorva Kumar * , Ravi Shankar, Rajendra P. Pandey, Virendra Keshri, Kulwant Singh, Vivek Sharma Department of Neurosurgery, Institute of Medical Sciences, Banaras Hindu University, Lanka, Varanasi 221005, India article info Article history: Received 29 March 2009 Accepted 17 May 2009 Keywords: Agricultural injuries Head injury Pediatric Winnowing Fan blade abstract India, an agriculture-based country, relies heavily on indigenous farm machinery. In our study we present 31 patients with winnowing fan blade head injury, operated on at our centre between 2004 and 2008. The mechanism and nature of the injuries, operative methods, outcome and methods of prevention are dis- cussed with special reference to the occurrence of this type of injury in the pediatric population. Ó 2009 Elsevier Ltd. All rights reserved. 1. Introduction India, a developing country, depends heavily on agriculture re- lated occupations. About two-thirds of the population lives in vil- lages and, directly or indirectly, takes up farming as an occupation. The farms are small and the methods are primitive, re- lated to poverty and illiteracy. During the harvesting season the crops are winnowed to separate the grain from the chaff. The win- nowing machines (Fig. 1) are made by the blacksmith and have large exposed blades. As both parents work in the fields, children are left to play nearby, and because of their curious nature, will venture near the machines. Some are hit by the blades. Winnowing fan blade injury is rare and the data worldwide are scant. We conducted a retrospective study of all patients who underwent surgery for fan blade injury at our Institute from Janu- ary 2004 to December 2008 and discuss the nature, mechanism, management and possible preventive measures for this type of injury. 2. Patients and methods We conducted a retrospective analysis of all patients who had fan blade injuries from January 2004 to December 2008. Patients brain CT scans, clinical notes and operative records were analyzed. 3. Results A total of 31 patients who underwent surgery in our depart- ment for fan blade injury were included. Twenty-six patients were male (83.87%) and five were female (16.13%). The mean age of the patients was 8.2 years (range 1.5–50 years). All patients had lacer- ated wounds in various parts of the scalp ranging from 3 cm to 7 cm in length (Figs. 2 and 3). There was a bimodal incidence peak: (i) patients 6 years to 8 years of age (14 patients, 45.16%); and (ii) patients 11–13 years of age (12 patients, 38.71%). All pediatric patients had a similar his- tory of either playing near the machinery or trying to crawl under- neath the machinery to reach their parents. The most common site of injury was frontal alone (15 patients, 48.39%), followed by the frontoparietal region (nine patients, 29.03%) (Table 1). The least common site was the occipital region (two patients, 6.45%) (Fig. 4). A basal dural tear with fracture was seen in two patients along with a frontal and craniofacial bone fracture. Repair was achieved with fibrin glue and a pericranial graft. Most patients arrived at our centre with good Glasgow Coma Scale (GCS) scores, the mean GCS score being 13 (range 7–15). Twenty-six patients (83.87%) had a compound depressed fracture with underlying contusion (Figs. 5 and 6). All patients had a dural tear (Table 2). Three patients (9.68%) had an extradural fracture hematoma, which was evacuated (Table 2). The operative interven- tion comprised elevation of the fractured segment, dural repair by either primary closure or duroplasty using pericranial, temporalis fascia or tensor fascia lata grafts. During surgery, foreign bodies 0967-5868/$ - see front matter Ó 2009 Elsevier Ltd. All rights reserved. doi:10.1016/j.jocn.2009.05.011 * Corresponding author. Tel.: +91 542 2307534; fax: +91 542 2367568. E-mail address: [email protected] (A. Kumar). Journal of Clinical Neuroscience 17 (2010) 178–181 Contents lists available at ScienceDirect Journal of Clinical Neuroscience journal homepage: www.elsevier.com/locate/jocn
-
Upload
apoorva-kumar -
Category
Documents
-
view
212 -
download
0
Transcript of Five years’ experience at a single centre of craniocerebral injury from winnowing fan blades

Journal of Clinical Neuroscience 17 (2010) 178–181
Contents lists available at ScienceDirect
Journal of Clinical Neuroscience
journal homepage: www.elsevier .com/ locate/ jocn
Clinical Study
Five years’ experience at a single centre of craniocerebral injury fromwinnowing fan blades
Apoorva Kumar *, Ravi Shankar, Rajendra P. Pandey, Virendra Keshri, Kulwant Singh, Vivek SharmaDepartment of Neurosurgery, Institute of Medical Sciences, Banaras Hindu University, Lanka, Varanasi 221005, India
a r t i c l e i n f o a b s t r a c t
Article history:Received 29 March 2009Accepted 17 May 2009
Keywords:Agricultural injuriesHead injuryPediatricWinnowingFan blade
0967-5868/$ - see front matter � 2009 Elsevier Ltd. Adoi:10.1016/j.jocn.2009.05.011
* Corresponding author. Tel.: +91 542 2307534; faxE-mail address: [email protected] (A. K
India, an agriculture-based country, relies heavily on indigenous farm machinery. In our study we present31 patients with winnowing fan blade head injury, operated on at our centre between 2004 and 2008. Themechanism and nature of the injuries, operative methods, outcome and methods of prevention are dis-cussed with special reference to the occurrence of this type of injury in the pediatric population.
� 2009 Elsevier Ltd. All rights reserved.
1. Introduction
India, a developing country, depends heavily on agriculture re-lated occupations. About two-thirds of the population lives in vil-lages and, directly or indirectly, takes up farming as anoccupation. The farms are small and the methods are primitive, re-lated to poverty and illiteracy. During the harvesting season thecrops are winnowed to separate the grain from the chaff. The win-nowing machines (Fig. 1) are made by the blacksmith and havelarge exposed blades. As both parents work in the fields, childrenare left to play nearby, and because of their curious nature, willventure near the machines. Some are hit by the blades.
Winnowing fan blade injury is rare and the data worldwide arescant. We conducted a retrospective study of all patients whounderwent surgery for fan blade injury at our Institute from Janu-ary 2004 to December 2008 and discuss the nature, mechanism,management and possible preventive measures for this type ofinjury.
2. Patients and methods
We conducted a retrospective analysis of all patients who hadfan blade injuries from January 2004 to December 2008. Patientsbrain CT scans, clinical notes and operative records were analyzed.
ll rights reserved.
: +91 542 2367568.umar).
3. Results
A total of 31 patients who underwent surgery in our depart-ment for fan blade injury were included. Twenty-six patients weremale (83.87%) and five were female (16.13%). The mean age of thepatients was 8.2 years (range 1.5–50 years). All patients had lacer-ated wounds in various parts of the scalp ranging from 3 cm to7 cm in length (Figs. 2 and 3).
There was a bimodal incidence peak: (i) patients 6 years to 8years of age (14 patients, 45.16%); and (ii) patients 11–13 yearsof age (12 patients, 38.71%). All pediatric patients had a similar his-tory of either playing near the machinery or trying to crawl under-neath the machinery to reach their parents.
The most common site of injury was frontal alone (15 patients,48.39%), followed by the frontoparietal region (nine patients,29.03%) (Table 1). The least common site was the occipital region(two patients, 6.45%) (Fig. 4). A basal dural tear with fracture wasseen in two patients along with a frontal and craniofacial bonefracture. Repair was achieved with fibrin glue and a pericranialgraft.
Most patients arrived at our centre with good Glasgow ComaScale (GCS) scores, the mean GCS score being 13 (range 7–15).Twenty-six patients (83.87%) had a compound depressed fracturewith underlying contusion (Figs. 5 and 6). All patients had a duraltear (Table 2). Three patients (9.68%) had an extradural fracturehematoma, which was evacuated (Table 2). The operative interven-tion comprised elevation of the fractured segment, dural repair byeither primary closure or duroplasty using pericranial, temporalisfascia or tensor fascia lata grafts. During surgery, foreign bodies

Fig. 2. (a) Anterior and (b) superior views of a patient following fan blade injuryshowing extensive craniofacial laceration.
Fig. 1. A winnowing fan showing (a) blades and (b) a fan with thresher.
A. Kumar et al. / Journal of Clinical Neuroscience 17 (2010) 178–181 179
were found impregnated in brain matter such as grass, small peb-bles or even metal pieces.
Post-operative complications (Table 3) included wound infec-tions in four patients (12.9%), and cerebrospinal fluid (CSF) leaksin three patients (9.7%), which was managed by repeated lumbarpuncture in two patients and continuous lumbar drainage in onepatient. Pseudomeningocele developed in two patients (6.45%)and was managed conservatively. Two patients (6.45%) developeddelayed onset post-traumatic epilepsy and were managed on anti-epileptic drugs.
All patients recovered and there was no mortality in the group.Three patients (9.7%) developed limb weakness and were sent forphysiotherapy and rehabilitation. Every year there was a regulartrend of admissions of patients with similar injuries: 24 patients(77.42%) were admitted from November to January and seven
patients (22.58%) were admitted between March and April, whichcorresponds to the harvesting season in Indian agriculture.
The mean hospital stay was 7 days (range 5–15 days). The dura-tion of follow-up ranged from 3 months to 4 years (mean 9months).
4. Discussion
A young child needs parental supervision, care and monitoringfor proper development. Playing in the fields, running with peersand hiding in small places are common to children worldwide,but on farms this may prove gravely dangerous and can cause seri-ous morbidity and mortality when children are left unsupervised.Children in rural areas in India lack the facilities for proper hospitalcare, as well as having poor schooling infrastructure and almost no‘‘playgrounds”. Poor parents work in the fields, which become the

Fig. 3. A patient following fan blade injury showing facial laceration.
Table 1Sites of craniocerebral injury from winnowing fan blades
Site No. patients
Frontal with craniofacial structures 15Frontoparietal region 9Multiple 5Occipital 2
Fig. 4. Axial CT scan showing a depressed fracture over the occipital region.
ig. 5. (a) Superior and (b) anterior three-dimensional reconstruction CT scan ofmpound depressed fractures showing the pattern of injury.
180 A. Kumar et al. / Journal of Clinical Neuroscience 17 (2010) 178–181
Fco
childrens’ playground. Parental illiteracy also adds to the problemas the parents are unaware of the serious consequences of proxim-ity to agricultural machinery.
A winnowing fan blade is a blunt blade fan used to dry grain andremove chaff. It moves at high speed and gains enough momentumto cause injury for some time after the machine has been switchedoff. The tangential injuries caused by the blades are high-velocitypenetrating injuries.
The high risk of injury to children playing on working farms hasbeen established.1–3 Studies have documented the types of injuriessuffered by preschool children on farms.4 However, case reportsand series of any kind of fan blade injury are scarce.5–7 Some char-acteristics of farm children have previously been associated withfarm injury and mortality in the United States, including malesex,1,8,9 age (with increased injury frequency at ages 3–4 years10
and 15–19 years1), and lack of supervision11 Factors related tosupervision could have a role in agricultural machinery death. In-creased frequency of injury and mortality has also been relatedto the intensity of farming activity and seasonal variation.4,8,12
Boys also outnumber girls in fan blade injury.
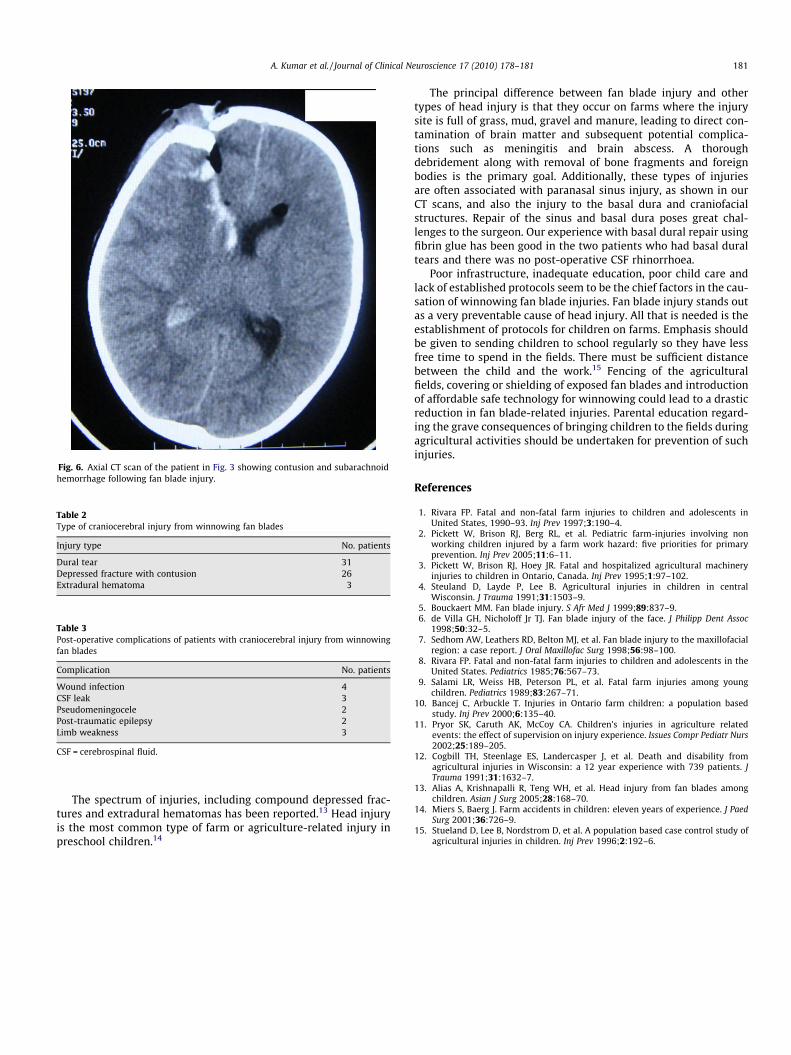
Table 2Type of craniocerebral injury from winnowing fan blades
Injury type No. patients
Dural tear 31Depressed fracture with contusion 26Extradural hematoma 3
Table 3Post-operative complications of patients with craniocerebral injury from winnowingfan blades
Complication No. patients
Wound infection 4CSF leak 3Pseudomeningocele 2Post-traumatic epilepsy 2Limb weakness 3
CSF = cerebrospinal fluid.
Fig. 6. Axial CT scan of the patient in Fig. 3 showing contusion and subarachnoidhemorrhage following fan blade injury.
A. Kumar et al. / Journal of Clinical Neuroscience 17 (2010) 178–181 181
The spectrum of injuries, including compound depressed frac-tures and extradural hematomas has been reported.13 Head injuryis the most common type of farm or agriculture-related injury inpreschool children.14
The principal difference between fan blade injury and othertypes of head injury is that they occur on farms where the injurysite is full of grass, mud, gravel and manure, leading to direct con-tamination of brain matter and subsequent potential complica-tions such as meningitis and brain abscess. A thoroughdebridement along with removal of bone fragments and foreignbodies is the primary goal. Additionally, these types of injuriesare often associated with paranasal sinus injury, as shown in ourCT scans, and also the injury to the basal dura and craniofacialstructures. Repair of the sinus and basal dura poses great chal-lenges to the surgeon. Our experience with basal dural repair usingfibrin glue has been good in the two patients who had basal duraltears and there was no post-operative CSF rhinorrhoea.
Poor infrastructure, inadequate education, poor child care andlack of established protocols seem to be the chief factors in the cau-sation of winnowing fan blade injuries. Fan blade injury stands outas a very preventable cause of head injury. All that is needed is theestablishment of protocols for children on farms. Emphasis shouldbe given to sending children to school regularly so they have lessfree time to spend in the fields. There must be sufficient distancebetween the child and the work.15 Fencing of the agriculturalfields, covering or shielding of exposed fan blades and introductionof affordable safe technology for winnowing could lead to a drasticreduction in fan blade-related injuries. Parental education regard-ing the grave consequences of bringing children to the fields duringagricultural activities should be undertaken for prevention of suchinjuries.
References
1. Rivara FP. Fatal and non-fatal farm injuries to children and adolescents inUnited States, 1990–93. Inj Prev 1997;3:190–4.
2. Pickett W, Brison RJ, Berg RL, et al. Pediatric farm-injuries involving nonworking children injured by a farm work hazard: five priorities for primaryprevention. Inj Prev 2005;11:6–11.
3. Pickett W, Brison RJ, Hoey JR. Fatal and hospitalized agricultural machineryinjuries to children in Ontario, Canada. Inj Prev 1995;1:97–102.
4. Steuland D, Layde P, Lee B. Agricultural injuries in children in centralWisconsin. J Trauma 1991;31:1503–9.
5. Bouckaert MM. Fan blade injury. S Afr Med J 1999;89:837–9.6. de Villa GH, Nicholoff Jr TJ. Fan blade injury of the face. J Philipp Dent Assoc
1998;50:32–5.7. Sedhom AW, Leathers RD, Belton MJ, et al. Fan blade injury to the maxillofacial
region: a case report. J Oral Maxillofac Surg 1998;56:98–100.8. Rivara FP. Fatal and non-fatal farm injuries to children and adolescents in the
United States. Pediatrics 1985;76:567–73.9. Salami LR, Weiss HB, Peterson PL, et al. Fatal farm injuries among young
children. Pediatrics 1989;83:267–71.10. Bancej C, Arbuckle T. Injuries in Ontario farm children: a population based
study. Inj Prev 2000;6:135–40.11. Pryor SK, Caruth AK, McCoy CA. Children’s injuries in agriculture related
events: the effect of supervision on injury experience. Issues Compr Pediatr Nurs2002;25:189–205.
12. Cogbill TH, Steenlage ES, Landercasper J, et al. Death and disability fromagricultural injuries in Wisconsin: a 12 year experience with 739 patients. JTrauma 1991;31:1632–7.
13. Alias A, Krishnapalli R, Teng WH, et al. Head injury from fan blades amongchildren. Asian J Surg 2005;28:168–70.
14. Miers S, Baerg J. Farm accidents in children: eleven years of experience. J PaedSurg 2001;36:726–9.
15. Stueland D, Lee B, Nordstrom D, et al. A population based case control study ofagricultural injuries in children. Inj Prev 1996;2:192–6.