Fitness Instructing (Gym)• Understand the structure and function of the skeleton. • Understand...
320
Fitness Instructing (Gym) Level 2 Version AIQ003323
Transcript of Fitness Instructing (Gym)• Understand the structure and function of the skeleton. • Understand...

Fitness Instructing (Gym)
Level 2
Version AIQ003323

Copyright © 2014, Active IQ Ltd
Active IQ wishes to emphasise that whilst every effort is made to ensure accuracy, the material contained within this document is subject to alteration or amendment in terms of overall policy, financial or other constraints. Reproduction of this publication is prohibited unless authorised by Active IQ Ltd. No part of this document should be published elsewhere or reproduced in any form without prior written permission.
Anatomy and physiology for exerciseIntroduction .......................................................4Section 1: The structure and function of the skeleton ............................................................5Section 2: Joints in the skeleton .......................... 14Section 3: The muscular system .......................... 21Section 4: The nervous system ............................ 30Section 5: The respiratory system ........................ 35Section 6: The circulatory system ........................ 40Section 7: The energy systems............................. 50Section 8: The life course of the musculoskeletal system and implications for special populations ..... 56
Supporting clients who take part in exercise and physical activitySection 1: Forming effective working relationships with clients .......................................................62Section 2: Addressing barriers to exercise and physical activity .................................................73Section 3: Supporting clients in their adherence to exercise and physical activity ............................... 77Section 4: Providing ongoing customer service to clients ..............................................................89
Health, safety and welfare in a fitness environmentSection 1: Emergency procedures in a fitness environment ......................................................96Section 2: Health and safety requirements in a fitness environment ............................................107Section 3: How to control risks in a fitness environment ......................................................117Section 4: Safeguarding children and vulnerable adults ...............................................................128
Principles of exercise fitness and healthSection 1: The components of fitness ................... 138Section 2: The effects of exercise on the body ....... 155Section 3: The principles and variables of fitness in an exercise programme ................................... 165Section 4: Health benefits of physical activity ........ 181Section 5: Monitoring exercise intensity ................ 185Section 6: Contraindications to exercise and key safety guidelines for special populations ................ 189Section 7: The importance of healthy eating .......... 201
Planning gym-based exerciseSection 1: Understanding how to collect and use client information ...............................................210Section 2: Physical assessments .......................... 224Section 3: Understanding how to plan gym-based exercise ............................................................236
Instructing gym-based exerciseSection 1: Preparing for gym-based exercise ........ 267Section 2: Instructing and supervising gym-based exercise and supporting clients ............................ 271Section 3: Ending a gym-based session and reflective practice ..............................................285Appendix 1: Exercise archive ............................... 290
References ........................................................317
Contents

AimA basic understanding of anatomy and physiology in relation to exercise is essential foundation knowledge for all fitness instructing disciplines.
Exercise affects all body systems. An understanding of the benefits of exercise and the demands it places on the body will help with the programming of safe and effective exercise.
Learning outcomesAt the end of this unit you will:
• Understand the structure and function of the skeleton.
• Understand joints in the skeleton.
• Understand the muscular system.
• Understand the nervous system and its relation to exercise.
• Understand the structure and function of the respiratory system.
• Understand the structure and function of the circulatory system.
• Understand energy systems and their relation to exercise.
• Understand the life course of the musculoskeletal system and its implications for special populations exercise.
ANATOMY AND PHYSIOLOGY FOR EXERCISE

Introduction
The body is a living structure comprised of many finely integrated and interconnected systems. Each system can be described independently and separately, but it is important to remember that they are actually interdependent. Every system depends on other systems for optimal functioning.
Here is a very basic example of the interconnection: The skeletal system of bones and joints provides the framework. The muscles create movement of the skeletal framework. The heart and circulatory system pump oxygen and nutrients to fuel the muscles. The respiratory system takes in oxygen and removes waste products. The nervous system is the control centre responsible for overseeing and responding to all demands and actions. The digestive system breaks down and stores the nutrients required for energy production.
At level 2 the aim is to provide a basic introduction to some of these systems. At higher levels of study these systems and others are explored in more detail and other systems are introduced.
Anatomical terminologyThere are a number of common terms used in anatomy text books to describe the position of different body structures in relation to the anatomical position.
The anatomical position is defined as the body in an upright position with legs parallel, arms by the sides of the body and the palms facing forward.
Anterior – in front, at the front of the body.
Lateral – away from the midline.
Superior – the upper aspect of a structure.
Sub – underneath.
Deep – further from the body surface.
Proximal – closer to the trunk.
Posterior – behind, at the rear of the body.
Medial – towards the midline.
Inferior – the lower aspect of a structure.
Superficial – closer to the body surface.
Distal – further from the trunk.
Posterior
Inferior
Dorsum of hand
Palmar surface of hand
Proximal
Distal
Plantar surface of foot
Dorsum of foot
Medial
Lateral
Anterior
Superior
4 | Copyright © 2014 Active IQ Ltd. Not for resale
Introduction

Section 1: The structure and function of the skeleton
The skeletal system consists of two main types of connective tissue: bones and different types of cartilage.
Bone is the calcified connective tissue that forms most of the adult skeleton. There are around 206 bones in the body and they are connected via a series of different types of joint. Joints are discussed in Section 2.
Cartilage is a dense, durable, tough fibrous connective tissue that is able to withstand compression forces. There are three types of cartilage found in the body, each fulfilling a separate function:
• Hyaline cartilage is the cartilage tissue that forms the temporary skeleton of the foetus, which is eventually replaced by bone when calcium is deposited. It is found at the end of the long bones that meet to form the synovial joints.
• Elastic cartilage is similar to hyaline cartilage, but has more fibres and most of these are made up of elastin as opposed to collagen. Elastic cartilage has the ability to regain and return to its original shape. It is found in the ear, the walls of the Eustachian tube and the epiglottis, which are all places that require a specific shape to be maintained.
• Fibrocartilage is thicker and stronger and has limited distribution within the body. It forms various shapes according to its role. It acts like a shock absorber in cartilaginous joints.
Functions of the skeletonThe skeletal system performs a range of functions. The complete skeletal framework gives the body its shape and the large bones offer protection to the vital organs. The bones meet at various junctions to form the joints, which enable the body to move in different ways. The muscles attach to the bones and create the force needed to make movement happen. Inside the bones, red and white blood cells are produced in the bone marrow. Vital minerals, including calcium, are stored in the bone.
FUNCTION DESCRIPTION
Shape The skeletal bones provide the framework that gives the body its basic shape. Basic body types include:• Ectomorph – a tall, lean body frame with long levers.• Endomorph – a short, more rounded frame with shorter levers. • Mesomorph – an athletic frame, with broad shoulders and narrow hips.NB: Muscle and body fat are also distributed differently.
Protection Different bones protect different organs:• The skull protects the brain. The ribcage and sternum protect the lungs and heart. • The vertebral column protects the spinal cord. The pelvic girdle protects the internal reproductive
organs. Locomotion The long bones act as levers that muscles pull on to create movement at a joint.
NB: Initiation of movement is the role of the nervous system.Attachment Various tissues attach to the skeleton:
• Ligaments attach bone to bone to keep the joints stable. • Tendons attach some muscles to the bones. • Some muscles attach directly to the surface of the bones.
Storage The bones store several minerals, such as calcium and phosphorus; these are essential for many functions including bone growth and development. Triglycerides (fats) are also stored in the adipocytes (cells for fat storage) of yellow bone marrow.
Production Some bones produce red and white blood cells and platelets from their bone marrow.• Red blood cells carry oxygen. White blood cells fight bacteria and infection.
Table 1.1 Functions of the skeleton
Copyright © 2014 Active IQ Ltd. Not for resale | 5
Section 1: The structure and function of the skeletonAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

The axial and appendicular skeleton
Figures 1.1 and 1.2 show the location of the main bones
THE AXIAL SKELETON
GENERAL AREA
BONES NO. OF BONES
NOTES
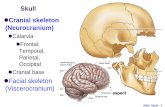
Skull Cranial 8 The head.
Spine Cervical vertebrae 7 The neck region; includes the atlas and axis bones which form the pivot joint.
Thoracic vertebrae 12 The trunk region; join with the ribs.
Lumbar vertebrae 5 The lower back.
Sacral vertebrae 5 Fused bones. At the back of pelvis, joining with the iliac bones.
Coccygeal vertebrae 4 Fused bones. Used to be the tail (tail bone).
Chest/thorax
Ribs (costals) 12 pairs
The ribs originate from the thoracic vertebrae and the right and left pairs extend to form the chest wall. The first seven pairs attach onto the sternum. The next three pairs have common cartilaginous attachment to the sternum. The last two pairs are free (floating).
Sternum 1 Forms an immovable joint with the clavicle and upper ten pairs of ribs.
Table 1.2 The axial skeleton
The skeletal system consists of around 206 bones.
• The axial skeleton consists of the bones that form the main frame or axis: the spine, ribs and skull (see table 1.2).
• The appendicular skeleton consists of the bones that attach to the main frame (the appendages): the upper and lower limbs, the pelvic and shoulder girdles (see table 1.3).
cranium
cervical vertebrae
scapula
humerus
thoracic vertebrae
ilium
coccyx
phalangesfemur
fibula
tibia
sacrum
cranium
clavicle
sternum
lumbar vertebrae
rib humerus
metatarsals
tibia
patella
femur ischium
metacarpals carpals pubis radius ulna
phalanges
tarsals
6 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The structure and function of the skeleton

THE APPENDICULAR SKELETON
GENERAL AREA
BONES NO. OF BONES
NOTES
Shoulders Scapulae (shoulder blade)
2 Muscular attachment to the ribcage (at the back) and the clavicle (at the front) maintain the position of the scapulae.
Clavicle (collar bone) 2 Maintains the scapula at a correct distance from the chest wall.
Arms Humerus 2 Bones of the upper arm. Forms part of the elbow joint and shoulder joint.
Radius 2 Outer bone of the forearm. Forms part of the elbow joint.
Ulna 2 Forms the elbow joint (with the radius and humerus) and the wrist joint with the carpals.
Hands Carpals 16 Two rows of four short bones that form the wrist.
Metacarpals 10 First metacarpal is the thumb and the rest are in the palm.
Phalanges 28 Each finger has three phalangeal bones. Each thumb has two phalangeal bones.
Pelvis Ilium 2 The large flat iliac bones join with the sacrum to form the upper part of the pelvis. The ilium is fused with the ischium and pubis and together they form an articulation for the lower limbs (the hip joint).
Ischium 2 The sitting bones at the bottom of the pelvis.
Pubis 2 The front of the pelvis.
Legs Femur 2 The thigh bone is the longest bone in the body and forms the knee joint with the tibia.
Tibia 2 The thicker, weight-bearing long bone of the lower leg.
Fibula 2 The finer bone of the lower leg. Lies outside the tibia and forms part of the ankle joint.
Patella (kneecap) 2 Lies within the tendons of the quadriceps muscles that cross over the knee joint.
Feet Tarsals 14 Form the ankle joint (7 bones in each ankle).
Metatarsals 10 First metatarsal is the big toe.
Phalanges 28 Each toe has three phalangeal bones. Each big toe has two phalangeal bones.
Table 1.3 The appendicular skeleton
Classification of bonesBones can be classified according to their formation and shape (see table 1.4).
CLASSIFICATION DESCRIPTION EXAMPLES
Long bones • Have a greater length than width.• Consist of a main shaft (diaphysis) with normally two extremities (epiphysis). • Principally act as levers.• Contain mostly compact bone in their diaphysis.• Contain more cancellous bone in their epiphysis.
Humerus, femur, fibula, tibia, ulna, radius, metacarpals, metatarsals and phalanges.
Short bones • Normally about as long as they are wide (cube-shaped).• Usually highly cancellous, which gives them strength with
reduced weight.
Carpals and tarsals.
Flat bones • Thin layer of cancellous bone sandwiched between two plate-like layers of compact bone (visualise an Oreo cookie).
• Provide protection and large areas for muscle attachment.
Scapula, cranial bones, costals (ribs), sternum and ilium.
Irregular bones • Form very complex shapes and cannot be classified within the previous groups.
Vertebrae and calcaneus (heel bone).
Sesamoid (‘seed-like’)
• Develop within particular tendons at a site of considerable friction or tension.
• Serve to improve leverage and protect the joint from damage.
Patella (kneecap).
Table 1.4 Bone classifications
Copyright © 2014 Active IQ Ltd. Not for resale | 7
Section 1: The structure and function of the skeletonAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Structure of long bone
Bone development In a fully developed skeleton, bone contains both living tissue and non-living tissue.
The living tissues are the blood vessels, nerves, collagen and bone cells including:
• Osteoblasts (cells that help form bone).• Osteoclasts (cells that help eat away old bone).• Osteocytes (mature osteoblasts that have ended their bone-forming role).
The non-living, but equally important, substances in bone are the minerals (like calcium) and salts.
Ossification
Ossification is the process by which bone is formed in the body from the activity of osteoblasts and osteoclasts with the addition of minerals and salts. Calcium compounds must be present for ossification to take place. Osteoblasts take calcium compounds from the blood and deposit them in the bone.
All long bones, like the femur and radius, contain many different components (see figure 1.3). These include:
• Epiphysis – the expanded portions at each end of the bone. Contains the cancellous bone tissue.
• Diaphysis – the shaft of the bone. Contains a thick layer of compact bone with a hollow centre (the medullary cavity).
• Epiphyseal plates – the growth plates located between the diaphysis and epiphysis that allow the diaphysis to increase in length until adulthood.
• Hyaline cartilage – this covers the end of the bone (the epiphysis), where the bones meet to form joints.
• Periosteum – a tough, fibrous sheath covering the whole bone.
• Compact bone – this is solid and strong to help the long bone withstand weight-bearing stress.
• Cancellous bone – spongy bone tissue that contains red marrow. Flat, short and irregular bones are formed mainly from cancellous bone.
• Medullary cavity – the hollow tube down the centre of the diaphysis (the marrow cavity).
• Yellow marrow – functions for the storage of fat. Found in the medullary cavity.
• Red marrow – functions in the production of various types of blood cell. Found in cancellous bone tissue.
EpiphysisDiaphysisEpiphysis
Epiphyseal growth plate
Compact bone
Cancellous (spongy) bone
Articular (hyaline) cartilage
Medullary cavity
PeriosteumArticular (hyaline) cartilage
Figure 1.3 Long bone structure
8 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The structure and function of the skeleton

Stages of bone growthFoetal stage
In the foetus most of the skeleton is made up of cartilage; a tough, flexible connective tissue containing no minerals or salts. As the foetus grows, osteoblasts and osteoclasts slowly replace cartilage cells and ossification begins. Many of the bones have been at least partly formed (ossified) by the time we are born.
Birth to adulthood
In long bones the growth and elongation (lengthening) continue from birth through adolescence.
Bone lengthening is achieved by the activity of two cartilage plates (called epiphyseal plates) located between the shaft (the diaphysis) and the heads (epiphyses) of the bones. The epiphyseal plates expand, forming new cells and enabling the diaphysis to lengthen. The length of the diaphysis increases at both ends and the heads of the bone move progressively apart.
As growth continues, the thickness of the epiphyseal plates gradually decreases and the bone lengthening process ends. Different bones stop lengthening at different ages, but ossification is fully complete between the ages of 18 and 30. During this lengthening period the stresses of physical activity result in the strengthening of bone tissue.
The thickness and strength of bone must be continually maintained. Old bone must be replaced by new bone to maintain bone strength and bone mass.
Osteoblasts are responsible for depositing calcium to form new bone and, at the same time, osteoclasts reabsorb and break down any old bone.
Adulthood to later life
Calcium is progressively lost from the bones as the skeleton ages. This happens earlier in women. Loss of calcium and bone mass can lead to osteoporosis. Osteoporosis increases the risk of fractures. It is also responsible for loss of height and changes in posture (hunched back) in senior years.
Factors affecting bone formationBone development and bone health are influenced by a number of factors, including:
• Nutrition.• Exposure to sunlight.• Hormonal secretions.• Physical activity and exercise.
Nutrition
A healthy diet is essential for bone health. The mineral calcium is especially essential. Calcium-rich foods include dairy products (milk and cheese), oily fish (sardines) and green vegetables (spinach, kale).
Bone health can be compromised by excessive intake of caffeine, alcohol and carbonated drinks, as these reduce the absorption of calcium.
Sunlight
Exposing the skin to the ultraviolet portion of sunlight is favourable to bone development because the skin can produce vitamin D when exposed to such radiation.
KEY POINTExercise and activity during formative years (up to age 30) is essential for building bone strength.
KEY POINT Regular activity and a healthy diet are essential for maintaining bone health and strength.
Copyright © 2014 Active IQ Ltd. Not for resale | 9
Section 1: The structure and function of the skeletonAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Vitamin D is necessary for the proper absorption of calcium in the small intestine. If calcium is poorly absorbed the bone matrix will be deficient in calcium and the bones are likely to be deformed or very weak.
Hormonal secretions
Hormones produced by the endocrine system have a significant role to play in bone development and growth.
The growth hormone secreted by the pituitary gland is responsible for general development.
The sex hormones oestrogen and testosterone are also important because they help with osteoblast activity.
Physical activity and exercise
Weight-bearing exercise (such as walking, running and lifting weights) helps to keep the bones strong. During exercise and activity the muscles pull against the bone to create movement and there is an increased circulation of blood and nutrients to the bones.
Posture and the spineThe spine is formed from 33 irregular bones. Each region of the spine has a different number of bones and the bones are shaped differently (see figure 1.4).
Figure 1.4 The regions of the spine
7 Cervical (secondary curve)
12 Thoracic (primary curve)
5 Lumbar (secondary curve)
5 Sacral (fused)
4 Coccygeal (fused)
Cervical vertebrae.
Thoracic vertebrae.
Lumbar vertebrae.
Sacral vertebrae (fused).
Coccygeal vertebrae (fused).4
5
7
12
5
SOMETHING EXTRA Late onset of menstruation and early menopause (when significant hormonal changes occur) increase the risk of osteoporosis for women.
10 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The structure and function of the skeleton

Curves of the spine
In the foetus the spine is shaped in a single curve. As the spine matures it develops into four natural curves; two convex (thoracic and sacral) and two concave (lumbar and cervical). See figure 1.5.
Potential ranges of motion of the spine
The bone shape and structure and the number of bones in each region of the spine give them different movement potential.
The cervical spine is capable of flexion, extension, lateral flexion and rotation. It has the greatest amount of lateral flexion and rotation of any region of the spine.
The skull sits on top of the atlas bone enabling flexion, extension and lateral flexion. The atlas and the axis bones of the cervical vertebrae form a pivot joint, allowing rotation.
The thoracic spine is more stable and less mobile than the cervical. It also allows flexion, extension, lateral flexion and rotation.
The upper thoracic vertebrae are limited in their flexion and extension. The lower thoracic vertebrae allow a much greater range. The combined thoracic vertebrae are capable of significant amounts of rotation.
The lumbar spine allows some flexion with a greater capacity for extension. Rotation and lateral flexion are more limited than the other regions of the spine.
The sacral spine does not move. The bones of the sacrum and coccyx are fused. See Section 2 for descriptions of ranges of motion.
Neutral spine
The term ‘neutral spine’ describes the position of the spine when the natural s-shaped curves are all present and aligned (see figure 1.7a).
When the spine is in this position the stress on the passive structures of the spine (vertebrae and ligaments) is minimal and the risk of strain or injury to the lower back is minimised. It is therefore the ideal and essential position to maintain during daily activities and also during exercise.
7 Cervical(secondary curve)
Development of spinal curves
12 Thoracic(primary curve)
5 Lumbar(secondary curve)
5 Sacral(fused)
4 Coccygeal(fused)
Figure 1.5 Spinal curves in the foetus and in the
adult spine
TRAINER TIP Lifting and moving the body using a neutral spine will help spare the stress on the ligaments and vertebrae. Also, the correct engagement and use of abdominal and hip musculature will hold the body in this optimal position.
THROUGH EAR LOBE
THROUGH THE GREATER TROCHANTER
SLIGHTLY ANTERIOR TO THE AXIS OF THE KNEE
SLIGHTLY ANTERIOR TO THE LATERAL MALLEOLUS
THROUGH THE AXIS OF THE SHOULDER
Figure 1.6 Optimal posture
Copyright © 2014 Active IQ Ltd. Not for resale | 11
Section 1: The structure and function of the skeletonAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Common postural abnormalitiesFigure 1.7 shows the difference between optimal posture and some common postural abnormalities.
a) Neutral spine (optimal with s-shaped curves present and aligned).
b) Lordosis (excessive lower back curvature).
c) Kyphosis (excessive mid-back curvature).
d) Scoliosis (lateral deviation of the spine).
These abnormalities increase stress on the spine and surrounding soft tissue structures, as well as decreasing the efficiency with which the body moves. It is thought that the normal thoracic and lumbar curves should be approximately 20-45 degrees when in a static neutral position. A minor lateral deviation of the spine is considered fairly normal, but a curve of more than 10 degrees would be considered a scoliosis.
Postural deviations can be caused by sustained poor postures (e.g. driving, excess sitting and desk-based work) that result in changes in opposing muscle length and strength.
Hyperkyphosis (Kyphosis): The muscles at the front of the chest (pectorals) and upper back (upper trapezius) are short and tight and the muscles of the middle back (rhomboids and lower trapezius) are lengthened and weakened. This gives a hunched back appearance.
Hyperlordosis (Lordosis): The abdominal muscles (rectus abdominis) and trunk stabilising muscles (transversus abdominis) are weaker and the back extensor muscles (erector spinae) are short and tight. This gives a hollow back appearance.
The spine and pregnancyIt is not uncommon for posture to alter during pregnancy. The growing baby causes the abdominal muscles to lengthen and weaken and the extra weight can cause alterations to the position of the pelvis leading to a hyperlordotic posture.
Other postural deviations may also present. Scoliosis can develop following childbirth as a result of the mother carrying the child on their hip to one side, which may cause a lateral deviation to the spine. Kyphosis can develop from holding and cradling the baby.
Figure 1.7 (a) Neutral (b) Hyperlordosis (c) Hyperkyphosis (d) Scoliosis
TRAINER TIP To improve kyphosis lengthen the pectoral muscles and strengthen the lower trapezius and rhomboids.
To improve lordosis strengthen the abdominal core muscles and lengthen the hamstrings and spine extensors.
12 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The structure and function of the skeleton

Effects of exercise on the bones and skeleton
• Muscles pull on the bones. • Increased blood and
nutrients circulated to the bones.
SHORT-TERM EFFECTS
• Stronger bones.• Increased bone density. • Reduced risk of
osteoporosis. • Improved posture.
LONG-TERM EFFECTS
End of section: Learning check Answer the following questions and make notes to revise this section.
• What minerals are stored in the bones?
• What is produced in the red bone marrow?
• What is the name of the main bone shaft?
• Name a soft tissue that attaches to bone.
• What vital organ is protected by the cranium?
• What vital organs are protected by the ribs and sternum?
• Which bones form the axial skeleton?
• Which bones form the appendicular skeleton?
• Which bones are more distal – the carpals or the phalanges?
• Which bone is more proximal – the ischium or the tibia?
• Name the bones that form the pelvis.
• Name the bones that form the leg or lower limb.
• Give an example of a long bone.
• Give an example of a short bone.
• Give an example of a flat bone.
• Give an example of an irregular bone.
• Give an example of a sesamoid bone.
• What is hyaline cartilage?
• What is ossification?
• What is osteoporosis?
• How can diet and exercise affect the health of bones?
• How many natural curves are there in the developed spine?
• What is a neutral spine alignment?
• What is the name of an excess curvature of the lumbar spine?
• What is the name of an excess curvature of the thoracic spine?
• What ranges of motion are possible at the cervical spine?
• What ranges of motion are possible at the thoracic spine?
• What ranges of motion are possible at the lumbar spine?
Copyright © 2014 Active IQ Ltd. Not for resale | 13
Section 1: The structure and function of the skeletonAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Section 2: Joints in the skeleton
A joint is the junction where two or more bones in the body meet.
Classification of jointsThere are three types of joint. They are classified according to their degree of movement.
Structure of synovial jointsAll freely movable joints share the following characteristics:
TRAINER TIP Exercises that move the joints through their full range of motion (mobility exercises) promote the release of synovial fluid into the joint, nourishing the cartilage and enabling smoother movement.
• The ends of the bone are covered with hyaline cartilage. This reduces friction during movement. It is nourished by the release of synovial fluid.
• They are surrounded by a fibrous capsule, which protects and stabilises the joint. Areas of the fibrous capsule thicken to form ligaments.
• Ligaments connect bones to one another across joints to increase stability and alignment.
• The capsule is lined by a synovial membrane that secretes synovial fluid, which gives lubrication to the joint. When the joints move, the temperature of the synovial fluid increases and it flows more readily to lubricate the joint.
• Muscles cross over the joints and attach to the bones via tendons. Muscle contraction creates joint movement.
Figure 2.1 illustrates a simple synovial joint.
Fibrous joints are immovable with interlocking bones, e.g. the plates in the skull.
Cartilaginous joints are slightly movable joints connected by cartilage, e.g. the vertebrae.
Synovial joints are freely movable. They are the most common type of joint found in the body, e.g. hip, knee, shoulder, wrist and elbow.
Figure 2.1 The structure of a synovial joint
.
Synovial cavity
Bursa
Joint capsule and synovial lining
Tendon
Articular cartilage
Ligament
14 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Joints in the skeleton

CartilageCartilage is a dense, durable, tough fibrous connective tissue that is able to withstand compression forces (e.g. when jumping and running). Cartilage does not have a blood supply, so it has limited ability to repair itself.
Two key considerations are:
• Cartilage is dependent on regular activity for health, e.g. release of synovial fluid.
• Cartilage can be worn or torn, e.g. excess use, overuse, repetitive movement (high-impact) and ageing.
LigamentsLigaments are made of tough, white, non-elastic, fibrous tissue which is strung together in a cord or strap-like formation. They can withstand a lot of tension, but prolonged tension (e.g. repetitive incorrect movement patterns) will permanently damage the fibres.
Ligaments have four main functions within the body:
• Attaching and connecting bone to bone in all joints.
• Enhancing joint stability.
• Guiding joint motion and alignment.
• Preventing excessive or unwanted motion in the joint.
TendonsTendons attach muscle to bone across the joint and transmit the force produced by the muscle. They are formed from all the muscle fibres and connective tissue of the muscle. The Achilles tendon attaches the calf muscles to the heel bone and the quadriceps tendon crosses the knee joint and attaches to the tibia.
Injury and healing
Blood supply is one of the major factors in the healing process of any injury. Bone and muscle tissue often heal fairly easily and quickly because they have a healthy blood supply.
Ligaments, tendons and cartilage have a poor blood supply and this limits their healing potential and the speed of recovery.
Healing is particularly doubtful for cartilage, which has a lower nutrient supply. Fibrocartilage may need surgical removal when torn (e.g. the menisci in the knee).
KEY POINTHyaline cartilage is lubricated and becomes slippery when synovial fluid is released. This reduces friction and allows for optimal joint movement.
TRAINER TIPCorrect alignment and posture are essential to prevent damage to the ligaments.
DID YOU KNOWMuscles and bones have a good blood supply; they heal more effectively than ligaments, tendons or cartilage.
Hyaline cartilage is found covering the bone ends that form freely movable joints. It is also found in cartilaginous joints.
Fibrocartilage is thicker and stronger. It acts like a shock absorber in cartilaginous joints.
Copyright © 2014 Active IQ Ltd. Not for resale | 15
Section 2: Joints in the skeletonAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Types of synovial joints and their ranges of motionSynovial joints can be broken down into six sub-groups:
• Gliding joints, e.g. the mid-carpal and mid-tarsal bones of the wrist and ankle. • Pivot joints, e.g. between the atlas and axis of the cervical vertebrae. • Saddle joints, e.g. the thumb.• Ball and socket joints, e.g. the hip and shoulder. • Ellipsoid joints, e.g. the knuckles between the phalangeal bones of the fingers and toes. • Hinge joints, e.g. the knee and elbow.
The range of motion and movement potential at different joints is influenced by their structure. Table 2.1 illustrates the different types of joint and explains their ranges of motion.
JOINT TYPE DIAGRAM EXAMPLE PICTURE RANGES OF MOTION
Ball and socket
Allows for movement in almost any direction.
Examples: The shoulder and hip joint.
Actions: Flexion, extension, rotation, circumduction, adduction and abduction.
Hinge Allows flexion and extension of an appendage.
Example: The knee and elbow joint.
Actions: Flexion and extension.
Pivot Allows rotation around an axis.
Examples: In the neck, the atlas (the uppermost cervical vertebra – C1) rotates around the axis (second cervical vertebra – C2). In the forearms the radius and ulna twist around each other.
Action: Rotation.
Saddle Allows movement back and forth and side to side.
Example: The carpometacarpal joint (thumb).
Action: Adduction and abduction, flexion and extension
Gliding(plane)
Allows two bones to slide past each other.
Examples: The acromio-clavicular joint.The mid-carpal and mid-tarsal joints of the wrist and ankle.
Action: Elevation and depression of the shoulder girdle.
Ellipsoid Similar to a ball and socket joint – allows the same type of movement but to a lesser magnitude.
Example: The metacarpo-phalangeal joints (knuckles).
Action: Flexion, extension, adduction, abduction and circumduction but no rotation.
Table 2.1 Different types of synovial joint and their ranges of motion 16 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Joints in the skeleton

Joint movement potential and joint actionsSpecific terms are used to describe the different actions of the joints (see table 2.2). These movements are illustrated in figure 2.2.
This terminology is important for understanding the actions of muscles. Muscles pull on bones to create these joint movements, e.g. elbow flexion and knee extension. The muscles responsible for specific joint actions are explored in Section 3.
MOVEMENT TERMINOLOGY
NORMAL TERMS (GENERAL) DESCRIPTION
Flexion The angle of the joint decreases, or the return from extension (e.g. bending the knee or elbow).
Extension The angle of the joint increases, or the return from flexion (e.g. straightening the elbow or knee).
Rotation A bone rotating on its own long axis – may be internal or external (e.g. twisting the neck or trunk to the right or left).
Abduction Away from the midline of the body (e.g. taking the leg or arm out to the side of the body).
Adduction Towards the midline of the body (e.g. drawing the leg or arm in towards and across the front of the body).
SPECIFIC TERMS (REGIONAL) DESCRIPTION
Horizontal flexion Arm towards the midline of the body in the horizontal plane (e.g. bringing the arms in front of the body – a hugging action).
Horizontal extension Arm away from the midline of the body in the horizontal plane (e.g. drawing the arms backward in a horizontal position).
Lateral flexion Bending to the side (e.g. bending the spine or neck to the right or left).
Circumduction A circular or cone-shaped movement that occurs at ball and socket joints (e.g. moving the arm in a full circle, like a cricket bowling action).
Elevation Upward movement of the shoulder girdle (e.g. lifting the shoulder girdle towards the ears).
Depression Downward movement of the shoulder girdle (e.g. lowering the shoulder girdle down and further away from the ears).
Protraction Forward movement of the shoulder girdle (e.g. rounding the shoulder girdle forward).
Retraction Backward movement of the shoulder girdle (e.g. squeezing the shoulder blades together).
Pronation Palm of the hand facing downward. The action occurs between the radius and ulna (e.g. turning the palm down).
Supination Palm of the hand facing upward. The action occurs between the radius and ulna (e.g. turning the palm up to hold something in the hand).
Dorsiflexion Foot moves toward the shin. Only occurs at the ankle (e.g. lifting the toes towards the knees).
Plantarflexion Foot moves away from the shin (tip-toe action). Only occurs at the ankle (e.g. pointing the toes away from the knees, or rising onto the balls of the feet).
Inversion Sole of the foot faces the midline (e.g. turning the foot inwards).
Eversion Sole of the foot faces away from the midline (e.g. turning the foot outwards).
Table 2.2 Joint movement terminology
Copyright © 2014 Active IQ Ltd. Not for resale | 17
Section 2: Joints in the skeletonAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Flexion Internal rotation External rotationExtension
Adduction Horizontal extension Horizontal flexionAbduction
Flexion Lateral flexion RotationExtension
Elevation Protraction RetractionDepression
Shoulder movements
Shoulder girdle movements
Spinal movements
18 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Joints in the skeleton

Elbow movements
Flexion Pronation SupinationExtension
Hip movements
Extension Abduction AdductionFlexion
External rotation Circumduction FlexionInternal rotation
Knee movements
Flexion Eversion PlantarflexionExtension
Ankle movements
Inversion Dorsiflexion
Figure 2.2 Joint actions
Copyright © 2014 Active IQ Ltd. Not for resale | 19
Section 2: Joints in the skeletonAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

End of section: Learning check Answer the following questions and make notes to revise this section.
• What is a joint?
• Name the three classifications of joints and describe their movement potential.
• Give an example of each joint classification.
• Give an example of a ball and socket joint.
• Give an example of a hinge joint.
• Give an example of a pivot joint.
• What is the role of tendons?
• What is the role of cartilage?
• What is the role of ligaments?
• State two characteristics of ligaments.
• What is synovial fluid?
• Name the joints that can perform each of the following movements:
• Flexion.
• Extension.
• Abduction.
• Adduction.
• Circumduction.
• Rotation.
• Plantarflexion.
• Dorsiflexion.
• Elevation.
• Depression.
Effects of exercise on the joints
Short-term• Synovial fluid is released into the joint, providing lubrication and reducing the risk of wear and tear.
• Warmer joints move more freely.
Long-term• Stronger ligaments.
• Stronger tendons.
• Healthier cartilage (nourished by synovial fluid).
• Improved joint mobility and reduced stiffness.
20 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Joints in the skeleton

Section 3: The muscular system
There are over 600 muscles in the body, making up around 40% of the body’s total weight. Without these muscles there would be no motion or movement.
The bones and joints create the framework of levers (bones) and pivots (joints) which give the body the potential to move, but this framework cannot move on its own.
It is the action, contraction and relaxation of muscles, controlled by the nervous system, that bring about movement.
Types of muscle tissue There are three types of muscle tissue and each one has a different function. The three types are:
• Smooth muscle, e.g. the digestive system.
• Cardiac muscle (myocardium), e.g. the heart.
• Skeletal muscle (striated), e.g. the hamstrings or triceps.
Functions of different muscle tissue
Smooth muscle
Smooth muscle is described as involuntary. It is controlled by the autonomic nervous system and is not under conscious control. Smooth muscle is found in the digestive system, the blood vessels and urinary and reproductive systems. It is used in all processes that maintain the body’s internal environment. For example, the blood vessels constrict and dilate (narrow and widen) to alter the flow of blood. The muscles of the digestive tract contract to move food through the body.
Cardiac muscle
Cardiac muscle is found in the heart (the chamber walls). The function of the cardiac muscle is to pump blood (and oxygen) around the body. The heart works continuously. It is not under conscious control. Contraction of the heart is controlled by the sinoatrial node (SAN). The set rhythm of the heart (on average 72bpm at rest) is called autorhythmicity.
Skeletal muscle
Skeletal muscle is striated. The skeletal muscles cross over the joints and attach to the bones via tendons. They are controlled by the somatic nervous system and work under conscious or voluntary control. When stimulated to work they contract, pull on the bones and create different body movements. For example, the skeletal muscles contract and resist the force of gravity to hold the body upright; they contract and pull on bones to create different types of body movement.
Copyright © 2014 Active IQ Ltd. Not for resale | 21
Section 3: The muscular systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Characteristics of muscle tissueMuscle tissue has four key characteristics:
• Contractility (contract).
• Extensibility (stretch and lengthen).
• Elasticity (return to original shape).
• Excitability (respond to stimuli from the nervous system).
The heart contracts to pump blood and relaxes to fill with blood. The skeletal muscles work in pairs and contract and relax to create movement of the skeleton.
Contraction of the muscles occurs in response to different stimuli, such as neurotransmitters and hormones. Skeletal muscle is controlled by the somatic nervous system. Smooth muscle is controlled by the autonomic nervous system. Contraction of the heart is controlled by the sinoatrial node.
Muscle is elastic; it can stretch and then recoil to its original shape. Skeletal muscle is like an elastic band; if the muscle is pulled too far it can tear.
The anterior and posterior skeletal musclesThe main skeletal muscles are shown in figure 3.1 (anterior) and 3.2 (posterior).
Figure 3.1 Anterior muscles Figure 3.2 Posterior muscles
Upper Trapezius Deltoids
PectoralisMajor
Rectus Abdominis
External and Internal Obliques
Quadriceps
Tibialis Anterior
Hip Adductors
Iliopsoas - Hip Flexors
Biceps Brachii
MiddleTrapezius
UpperTrapezius
LatissimusDorsi
Hamstrings
GluteusMaximus
Soleus
Gastrocnemius
TricepsBrachii
Erector Spinae
LowerTrapezius
Hip Abductors
22 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: The muscular system

The structure of skeletal muscleThe main constituents of skeletal muscle are:
• 70% water.
• 23% protein, e.g. actin and myosin (elastin) and connective tissue (collagen).
• 7% minerals (e.g. calcium, potassium and phosphorus) and substrates (e.g. glycogen, glucose and fatty acids).
Skeletal muscle is constructed from many bundles of muscle fibres bound together by connective tissue (epimysium). The epimysium, or
fascia, covers the entire muscle.
Each bundle of individual muscle fibres (fasciculi) is also wrapped in connective tissue (perimysium) and each single fibre within the bundle is wrapped in connective tissue (endomysium).
Inside the individual fibres, there are smaller myofibrils and within each myofibril are strands of myofilaments (actin and myosin). It is the action of myosin and actin that brings about movement.
The numerous fibres and connective tissues are continuous throughout the length of the muscle. Layers of connective tissue converge to form tendons, which are strong, inelastic and strap-like. The tendon attaches to the periosteum, which is the sheath that surrounds the bone.
Figure 3.3 shows the structure of muscle.
Figure 3.3 Structure of muscle
Muscle structure summary
• Whole muscle wrapped in epimysium.
• Bundles of fibres or fasciculi, wrapped in perimysium.
• Single muscle fibres wrapped in endomysium.
• Myofibrils (inside single fibres).
• Myofilaments – myosin and actin (in the sarcomere).
Myosin
Actin
Myofibril
Sarcomere
Figure 3.4 Sliding filament action
Bone
Myofibril
Tendon
Muscle belly
Fasciculi
Endomysium
Perimysium
Muscle fibre
Epimysium
Copyright © 2014 Active IQ Ltd. Not for resale | 23
Section 3: The muscular systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Sliding filament theoryThe sliding filament theory was proposed by Huxley in 1954 to explain the contraction of skeletal muscle. The theory states that the myofilaments actin (a thin protein strand) and myosin (a thick protein strand) slide over each other, creating a shortening of the sarcomere (the contractile units in the muscle where myosin and actin are found), which causes the shortening or lengthening of the entire muscle. The myofilaments do not decrease in length themselves (see figure 3.5).
This proposed action is accomplished by the unique structure of the protein
myosin. The myosin myofilaments are shaped like golf clubs and form cross bridges with actin. Each myosin molecule (there are many) has two projecting heads. These heads attach to the actin filaments which surround each myosin filament and pull the actin closer.
Stimulus from the nervous system and the release of adenosine triphosphate (ATP) – the high-energy molecule stored on the myosin head – provides the impetus for this head to ‘nod’ in what is termed the ‘power stroke’. It is this nodding action which ‘slides’ the thin actin myofilaments over the thick myosin myofilaments. The myosin head then binds with another ATP molecule, causing it to detach from the actin-binding site, which is known as the ‘recovery stroke’. It is then able to attach to the next binding site and perform the same routine. ATP and energy systems are explored further in Section 7.
Skeletal muscle fibre types and their characteristicsSkeletal muscle fibres differ in both structure and function. Two distinct fibre types have been identified and classified by their contractile and metabolic characteristics.
• Slow twitch (or type I) fibres are slower to contract and slower to tire. • Fast twitch (or type II) fibres are faster to contract and quicker to tire.
Table 3.1 highlights the structural and functional features of both muscle fibres, as well as examples of activities to which they are best suited.
FIBRE TYPE STRUCTURAL FEATURES FUNCTIONAL FEATURES ACTIVITIES
Slow twitch or type I
Smaller diameter.Large myoglobin content.Many mitochondria (cells where aerobic energy is produced).Many capillaries to deliver blood and oxygen. Red in colour.
Increased oxygen delivery.Produce less force.Long-term contractions. Resistant to fatigue.Aerobic.
Maintaining posture, i.e. stabilisation.Endurance-based activities.Lower-intensity, aerobic activities.
Fast twitch or type II
Larger diameter.Smaller myoglobin content.Fewer mitochondria.Fewer capillaries.White (pale) in colour.
Decreased oxygen delivery.Produce more force.Short-term contractions.Less resistant to fatigue.Anaerobic.
Rapid, intense movements.Strength training. Sprinting. Anaerobic training.
Adapted from Tortora and Grabowski (1996)
Table 3.1 Muscle fibre types
SLIDING FILAMENT THEORY Myosin and actin filaments slide over each other, creating a shortening of the sarcomeres and the whole muscle.
Figure 3.5 The sliding filament theory
Myofibril
Muscle fibre
SARCOMERE IS CONTRACTED
SARCOMERE IS RELAXED
Actin filamentMyosin filament
24 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: The muscular system

Muscle fibre considerations
Most people have a mixture of muscle fibres in their skeletal muscles. The actual percentage of fibre types for each individual is determined by genetics and heredity. This means that different people may have relatively more of one variety in a specific area. These genetic differences significantly contribute to athletic abilities.
For example, the muscles of marathon runners have a higher percentage of slow twitch fibres (about 80%), while those of sprinters contain a higher percentage of fast twitch fibres (about 60%).
The proportion of slow and fast twitch fibres is also determined by the role of the muscle.
The muscles of the neck and back, for example, have a key role to play in the maintenance of correct posture and so have a high proportion of slow twitch fibres. In contrast, the muscles of the shoulders and arms are often called upon to generate considerable force and are not continually active in posture; consequently these muscles have a higher proportion of fast twitch fibres. Leg muscles often have large numbers of both fast and slow twitch muscles, since they must both continually support the body and play a role in locomotion.
Exercise and the type of training undertaken also affect muscle fibre proportions. Specific types of training will increase the size and capacity of specific types of muscle fibres.
• Fast twitch: intense exercise producing anaerobic metabolism increases muscular strength and mass. It results in an increase in the size of fast twitch fibres.
• Slow twitch: moderate-intensity aerobic endurance exercise increases the vascularity of muscle. More blood and oxygen can be delivered and will develop the aerobic capacity of slow twitch fibres.
• Intermediate fibres: fast twitch and slow twitch muscle fibres cannot be converted into each other. However, there is one type of fast twitch fibre (intermediate fibres) that can adapt in different ways depending on the type of training performed. In response to endurance training they will adapt and respond like slow twitch fibres. In response to strength training they will adapt and respond like other fast twitch fibres.
Different types of muscle actionWhen standing upright and erect, the skeletal muscles are in a constant state of tone or tension (muscle tone). Muscles are contracting, resisting the force of gravity and preventing the body from falling to the floor.
To create specific movement of the joints (when moving the body) muscles exert a force and pull on the bones. As one muscle contracts to bring about a specific action, the opposing muscle relaxes.
Key principles relating to muscle work and contraction
Skeletal muscles:
• Have a start and end point; an origin and insertion. • Cross joints and attach to bones (levers).• Contract in different ways and pull on bones to bring about specific joint actions that align and
position the body.• Work together in pairs; as one muscle contracts the opposing muscle relaxes and other muscles
play supporting roles.
SOMETHING OF INTEREST Muscle is meat. Cows graze all day; their muscle meat is red in colour (aerobic endurance fibres).Chickens can only use their wings for short bursts of flight; their breast muscle meat is white (anaerobic fibres).Chicken leg meat is redder in colour because they use their legs to walk around.
Copyright © 2014 Active IQ Ltd. Not for resale | 25
Section 3: The muscular systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Concentric contraction Eccentric
contraction
Origins and insertionsEach muscle has a recognisable start and end point.
Origin: the end of the muscle is attached to a fixed bone or bones; it doesn’t move during body movement. It is called the origin (the origin of a muscle). The origin is described as the proximal attachment, i.e. the one nearest to the centre midline of the body (usually the anchor). Muscles may have more than one origin, e.g. quadriceps (four), triceps (three), biceps (two).
Insertion: the end of the muscle attached to the bone that usually moves during contraction is called the insertion (the muscle insertion). The insertion is described as the distal attachment, i.e. the one furthest away from the centre midline. Usually muscles have a single insertion.
Types of muscle actionMuscles work in different ways. They can contract and shorten, contract and lengthen or contract and stay the same length, with no movement occurring. They can also relax and lengthen or stretch. To lift a weight, for example, the muscles shorten. To lower a weight the muscles lengthen. To hold a position, e.g. pausing an activity, the muscles stay the same length.
A number of terms are used to help distinguish between these different types of muscular activity:
During the lifting action of a bicep curl, for example, the bicep brachii would be working concentrically. If at any point the weight were held still this would represent an isometric action. Finally, as the weight is lowered (in a controlled manner) the biceps would be lengthening and working eccentrically.
MUSCLE WORKConcentric – contracting and shortening to lift a resistance.
Eccentric – contracting and lengthening to lower a resistance.
The muscle generates force and stays the same length.ISOMETRIC
The muscle actions involve movement at a constant speed.ISOKINETIC (SAME SPEED)
(Same tone) describes muscle actions involving movement, i.e. concentric and eccentric.
• Concentric: the muscle generates force and shortens. The origin and insertion move closer together; this is usually the lifting phase of body movement, e.g. the upward phase of a curl-up, press-up or squat.
• Eccentric: the muscle generates force and lengthens. The origin and insertion move apart, usually the lowering phase of a body movement, e.g. the downward phase of a curl-up, press-up or squat.
ISOTONIC
The muscle lengthens and relaxes; the origin and insertion move further apart.STRETCHING
26 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: The muscular system

Roles of musclesEfficient human movement is dependent on the coordinated activity of whole groups of muscles and will involve varying combinations of different muscle actions happening simultaneously. During any movement different muscles can be working in the following ways:
• Agonist/prime mover – the muscle(s) that contracts and causes a desired action, e.g. the bicep brachii contracts during a bicep curl or the quadriceps contract during a leg extension.
• Antagonist – the opposing muscle(s) to the agonist that relaxes, e.g. the triceps brachii during a bicep curl or the hamstrings during a leg extension.
• Synergist – the muscle(s) that contracts to assist or modify the movement of the prime mover, e.g. during hip extension the hamstrings act as synergists for the gluteus maximus.
• Fixators – the muscles that contract to stabilise the part of the body that remains fixed, e.g. shoulder girdle muscles stabilise the scapula to allow for efficient movement at the shoulder joint when the arm moves.
Joint actions brought about by specific muscle group contractionsWhen specific muscles contract and shorten (concentric muscle work) they pull on bones to create an action or movement at the joints they cross. Table 3.2 identifies the different joint actions/movements that are brought about when specific muscles contract and shorten (concentric muscle work) while working in the role of a prime mover.
MUSCLE LOCATION ORIGINSTART POINT
INSERTIONEND POINT
PRIMARY CONCENTRIC ACTIONS
Deltoids Shoulder Clavicle and upper scapula
Upper humerus Abduction, flexion and extension, horizontal flexion and extension, internal and external rotation of the shoulder joint.
Biceps brachii Front of the upper arm
Anterior surface of the scapula
Upper radius Flexion of the elbow, supination of the forearm and flexion of the shoulder.
Triceps brachii Back of the upper arm
Posterior upper humerus and the scapula
Upper ulna Extension of the elbow, extension and abduction of the shoulder joint.
Latissimus dorsi
Sides of the back Lower seven thoracic vertebrae, inferior angle of the scapula, thoracolumbar fascia and the iliac crest
Anterior upper humerus
Adduction, extension and internal rotation of the shoulder joint.
Trapezius Upper back Base of skull, spinous processes of C7-T12
Lateral clavicle and upper surface of the scapula
Elevation, retraction and depression of the shoulder girdle, extension, lateral flexion and rotation of the neck.
Rhomboids Mid back Spinous processes of C7-T5
Medial border of the scapula
Retraction and elevation of the scapula.
Pectoralis major
Chest Medial clavicle and sternum
Upper humerus Flexion, horizontal flexion, adduction and internal rotation of the shoulder joint.
Erector spinae Either side of spine
Sacrum, ilium, ribs and vertebrae
Ribs, vertebrae and base of the skull
Extension and lateral flexion of the spine.
Rectus abdominis
Along the centre of the abdomen
Pubis Cartilage of 5th-7th
rib and base of the sternum
Flexion and lateral flexion of spine and tilting the pelvis posteriorly.
Internal obliques
Sides of the abdomenDeeper to external obliques
Iliac crest and thoracolumbar fascia
Lower three ribs and the fascial connection to the linea alba
Rotation and lateral flexion of the spine.
Copyright © 2014 Active IQ Ltd. Not for resale | 27
Section 3: The muscular systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

MUSCLE LOCATION ORIGINSTART POINT
INSERTIONEND POINT
PRIMARY CONCENTRIC ACTIONS
External obliques
Sides of the abdomenCloser to the surface – superficial
Outer surface of the6th-12th ribs
Iliac crest, the pubis and the fascial connection to the linea alba
Rotation and lateral flexion of spine.
Transversus abdominis
Abdomen Iliac crest, thoracolumbar fascia and lower six ribs
Pubis and fascial connection to the linea alba
Compressing and supporting the abdominal contents.
Deep stabiliser of the spine. Diaphragm Beneath ribcage Base of the sternum,
inner surface of the lower six ribs and the upper three lumbar vertebrae
Central tendon of the diaphragm
Drawing the central diaphragmatic tendon downwards, increasing volume of the thorax.
Intercostals Between ribs Inferior border of the ribs and costal cartilages
Superior border of the rib below
Elevate ribs to aid inspiration and draw ribs down to aid expiration.
Hip flexors Through the pelvis and onto the femur
Iliac fossa and lumbar vertebrae
Lesser trochanter of the femur
Flexion and external rotation of hip.
Gluteus maximus
BottomButtocks
Coccyx, sacrum andiliac crest
Upper femur and iliotibial band
Extension, external rotation and abduction of the hip.
Abductor groupGluteus medius and minimus
Outside of upper thigh/hip
Outer surface of the ilium
Upper femur and upper tibia (via ITB)
Abduction of the hip.
Adductor group Inner thigh The pubis and ischium
Upper, mid and lower femur
Adduction and internal rotation of the hip.
Quadriceps group
Front of the thigh Anterior inferior iliac spine (AIIS) and the femur
Anterior, upper tibia via the patella
Flexion of the hip and extension of the knee.
Hamstrings group
Back of the thigh Ischium and posterior surface of the femur
Head of the fibula and upper, medial surface of the tibia
Extension of the hip, flexion of the knee and tilting the pelvis posteriorly.
Gastrocnemius Calf Posterior, lower femur
Calcaneus Plantarflexion of the ankle and flexion of the knee.
Soleus Calf Upper, posterior tibia Calcaneus Plantarflexion of ankle.Tibialis anterior Front of lower leg Lateral, upper tibia 1st metatarsal and
medial tarsalDorsiflexion and inversion of the ankle.
Table 3.2 Muscle actions
Pelvic floor muscles
Structure
The pelvic floor or pelvic diaphragm is composed of a small group of muscles and associated connective tissue which span the area underneath the pelvis. These muscles form a muscular sling-like structure under the pelvis, running back from the pubis toward the coccyx, uniting behind the anorectal junction with some fibres inserting into the prostate, urethra and vagina.
Figure 3.6 The pelvic floor
Pubis
Bulbocavernosus muscle
Deep transverseperineal muscle
Iliococcygeus
External sphincter
Ischiocavernosus muscle
Superficialtransverse perineal muscle
Pubococcygeusmuscle
Gluteus maximus
Coccyx
28 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: The muscular system

Function
The pelvic floor muscles provide support for pelvic organs, such as the bladder and the intestines, in the maintenance of continence and facilitating the birthing process. In women these muscles can become damaged during pregnancy and birth.
Damage to the pelvic floor can contribute to urinary incontinence and lead to pelvic organ prolapse. Pelvic floor exercises can be given to help improve the tone and function of the pelvic floor muscles.
FUNCTIONS OF THE PELVIC FLOOR• Prevent stress
incontinence. • Facilitate birth. • Support the pelvic
organs. • Prevent prolapse. • Assist excretion and
urination. • Assist childbirth.
End of section: Learning check Answer the following questions and make notes to revise this section.
• Name and describe the three types of muscle tissue. • Give an example of each type of muscle tissue. • Name the muscles of the leg. • Name the muscles of the arm. • Name the muscles of the trunk. • Summarise the sliding filament theory.• Describe the difference between fast and slow twitch muscle fibres. • Describe the following types of muscle work:
• Isotonic. • Concentric. • Eccentric. • Isometric.
• What are the origin and insertion of the muscle? • Which muscle flexes the knee?• Which muscle extends the hip?• Which muscle rotates the thoracic region of the spine? • Which muscle extends the elbow?• Which muscle plantar flexes the ankle?• Which muscle laterally flexes the spine? • Which muscle abducts the hip?• Which muscle adducts the shoulder? • Which muscle will contract – and how will it contract – during the lowering phase of a curl-up?• Name the antagonist to the following prime movers:
• Biceps. • Hip flexors. • Adductors. • Quadriceps. • Tibialis anterior. • Deltoids. • Rectus abdominis.
• What is the function of the pelvic floor muscles?
Copyright © 2014 Active IQ Ltd. Not for resale | 29
Section 3: The muscular systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Section 4: The nervous system
The nervous system is the main control and communication centre of the body.
It is responsible for maintaining homeostasis (balance) of all internal body processes, e.g. digestion of food and dilation of blood vessels.
It is also responsible for providing the electrical stimulus that triggers skeletal muscle to contract, e.g. to move the body, sit, stand, walk or run.
Role of the nervous systemThe main function of the nervous system is to gather information (sensation), interpret the information gathered (integration) and then initiate the appropriate response or action (response). See figure 4.1.
Sensation
The nervous system gathers information about the internal and external environment. A vast array of sensors throughout the body (including the eyes, ears and internal proprioceptors) gather information about the internal environment (e.g. blood CO2 levels) and the external environment (e.g. air temperature and space available).
Integration
The nervous system interprets and analyses the information gathered from the sensors and decides on the most appropriate action. Many of these ‘decisions’ are automatic (involuntary) without conscious control, e.g. digestion. Others are consciously controlled, e.g. voluntary muscle action.
Response
The nervous system responds to the information analysed by initiating an appropriate response. Responses may include muscle contraction to perform a movement or lift a weight, or glandular secretion. The nervous system works closely with the endocrine system, which is responsible for releasing hormones (chemicals) to maintain homeostasis.
Figure 4.1 Role of the nervous system
RESPONSEINTEGRATIONSENSATION(INTERPRETATION
AND ANALYSIS)
30 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: The nervous system

Structure of the nervous system The nervous system consists of two primary divisions:
• The central nervous system (CNS).
• The peripheral nervous system (PNS).
Central nervous system
The central nervous system is the control base for the whole nervous system. It consists of the brain (see figure 4.2) and the spinal cord.
All nerve impulses that stimulate muscles to contract and create movement of the body originate from the CNS.
The brain is made up of four main parts:
The spinal cord consists of cervical, thoracic, lumbar and sacral segments, named according to the portions of the vertebral column through which they pass.
The spinal cord is the communication link between the brain and the PNS. It integrates incoming information and produces responses via reflex mechanisms (reflex arc). See figure 4.3.
CEREBRUM The largest and most superior aspect. This takes up most of the space in the
skull.
CEREBELLUMThe smaller part; it is inferior to the cerebrum and posterior to the brain
stem. The cerebellum acts as a memory bank for all learnt skills. The cerebellum
is mainly responsible for controlling the group action of muscles. It
communicates and works harmoniously with the cerebrum.
DIENCELPHALON (Thalamus and hypothalamus).
BRAIN STEM(Medulla oblongata, midbrain and
pons) – the stalk-like component at the inferior aspect of the brain. The lower portion is a continuation of the spinal
cord.
Figure 4.2 The brain
Cerebellum
Cerebrum
Spinal cord
Brain stem
Thalamus
Hypothalamus
Copyright © 2014 Active IQ Ltd. Not for resale | 31
Section 4: The nervous systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Peripheral nervous system
The PNS consists of all the branches of nerves that lie outside the spinal cord.
The peripheral nervous system subdivides into the:
• Somatic system: the system that controls voluntary (conscious) movement of the skeletal muscles, e.g. standing, walking, lifting a weight.
• Autonomic system: the system that controls involuntary functions, e.g. digestion.
Neurons
Nerve cells or neurons are responsible for transmitting electrical messages. Spinal nerves are divided into motor and sensory neurons.
Principles of muscle contractionThe nervous system controls the actions of the muscular system. There would be no movement without activity from the nervous system.
To lift a weight, for example, the eyes gather information (how heavy the weight is and where and how it is positioned). This information is sent to the CNS to be processed. The brain sends information on how to position the body, which muscles to contract and the number of motor units to recruit to perform the
lift. Once they are stimulated to contract, the muscles pull on the bones and create appropriate movement of the joints, through the sliding action of the myofilaments (myosin and actin).
SENSORY NEURONS
MOTOR NEURONS
Due to the symbiotic nature of the nervous and muscular
systems, they are often referred to collectively as the
neuromuscular system.
Carry messages to the CNS from the sensory organs.
Sensory nerves arrive on the posterior side of the spinal cord from a variety of sensory receptors spread throughout the body. Sensory receptors in the muscles, tendons and joints relay information concerning muscle dynamics and limb movements to the CNS, giving important feedback on the position of those limbs at any time.
Carry messages from the CNS to the muscles or glands.
Motor neurons exit on the anterior side of the spinal cord. These neurons transmit impulses from the CNS to muscles and glands. These impulses cause muscles to contract and glands to secrete.
AN INDIVIDUAL NERVE CELL CONSISTS OF:• The cell body which directs the activities of
the neuron.
• Dendrites which pick up impulses and transmit these to the cell body.
• The axon which transmits messages away from the cell body.
Figure 4.3 The peripheral nervous system
CNS
PNS
Cell body
Nucleus
Dendrites
Axon
Figure 4.4 A nerve cell
32 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: The nervous system

Motor unit recruitment and ‘all or none law’
A motor unit consists of a single motor neuron and all the muscle fibres it innervates (activates). One single motor neuron may be responsible for innervating between five and 1000 muscle fibres, depending on its location and function.
When an impulse is sent down a neuron, all the muscle fibres within that motor unit are innervated. The motor unit activates all of its fibres or none at all. This is known as the ‘all or none law’.
The ‘all or none law’ applies to individual motor units – not the entire muscle. Only the muscle fibres stimulated by the motor unit/s recruited
will contract. Number of motor units The number and size of motor units in specific areas of the body depends on their role and function. Muscles controlling posture have fewer motor units supplying more fibres; muscles involved in more intricate movements have more motor units supplying fewer fibres.
The hands, for example, have a lot of small motor units and these supply fewer fibres to enable more intricate and finer movement, e.g. playing a musical instrument or using a computer.
The legs and muscles involved in maintaining posture have fewer motor neurons, but these are larger and supply more muscle fibres. Maintaining posture and movement of the legs to walk, kick, run and jump is less intricate than the movement of the hands.
Exercise, neuromuscular connections and motor fitness
Exercise can enhance neuromuscular (nerve and muscle) connections, which in turn help to improve motor fitness – the skill-related component of fitness.
One long-term adaptation to resistance exercise is the recruitment of more motor units. This adaptation will generate increased force and strength of contraction.
A beginner to exercise will only be able to recruit a certain number of motor units. This offers protection because the muscle cannot develop too much force that could damage the muscle or connective tissue. As neuromuscular connections develop the individual will gradually be able to recruit more motor units and produce more force. The risk of injury is reduced in a trained individual because their muscles and connective tissues strengthen in response to training.
MUSC
LE FI
BRES
, FOR
CE AN
D MO
TOR
UNITS
A motor unit is typically made up of one type of muscle fibre (slow or fast twitch) spread throughout the muscle.
For tasks requiring less effort, smaller neurons controlling slow twitch fibres are recruited.
For tasks requiring more effort, larger neurons controlling fast twitch fibres are recruited.
TRAINER TIP Early improvements in strength are often due to increased recruitment of motor units and improvement in neuromuscular connections.
Copyright © 2014 Active IQ Ltd. Not for resale | 33
Section 4: The nervous systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Muscle sense organsThere are different muscle sense organs that form part of the autonomic nervous system:
• Joint receptors are found in the ligaments and joint capsule. They inform the brain about the position of the joint.
• Muscle spindles are found in the muscle and inform the brain about how stretched or lengthened the muscle is and how many motor units to activate or fire.
• Golgi tendon organs are found in the tendons and tell the brain how much force has been generated in the muscle. If the force is too great they cause the muscle to relax.
These organs have a significant role to play in flexibility training, e.g. ballistic stretching (bouncing at the end of the range of motion) can create excess tension because the muscle spindles are active to prevent over-stretching or damage to the muscle and joint. Action of the Golgi tendon organ, causing the muscle to relax, is one theory proposed for improving flexibility, e.g. if the muscle can relax the stretch can be taken further. It is manipulated during a stretching method called proprioceptive neuromuscular facilitation (PNF).
They also have a role in resistance training. If an individual tries to lift a resistance that is too heavy the tension generated in the muscle will be too great and this will cause the Golgi tendon organ to relax the muscle, for example when an Olympic weight lifter strains to create part of the lift and then has to drop the bar.
Improvements in motor fitnessRegular performance of specific types of activity will improve different components of motor fitness or skill-related fitness. These include:
Activities that improve coordination are different from activities that improve balance or power. Neuromuscular connections and nerve pathways required to perform specific movements develop through regular practice of the specific activity. To perform a choreographed routine, for example, you must practise the movements that are part of that routine. To develop balance in a yoga posture, for example, you need to practise that specific posture.
• Coordination. • Balance. • Power.
• Speed. • Reaction time. • Agility.
TRAINER TIP When lifting heavy weights it is good practice to use a spotter. If the Golgi tendon organ causes the muscle to relax and the lifter drops the weight, the spotters can take the weight and keep the lifter safe.
TRAINER TIP It is important to warm up before exercise.Warming up alerts the nervous system to prepare the body!
End of section: Learning check Answer the following questions and make notes to revise this section.
• What is the role of the nervous system?• Name the main structures of the central nervous system. • Name the main structures of the peripheral nervous system.• What is the difference between a sensory neuron and a motor neuron?• What is a motor unit?• Describe the ‘all or none law’.• How can exercise enhance neuromuscular connections and improve motor fitness?
34 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: The nervous system

Section 5: The respiratory system
The respiratory system is responsible for the intake of oxygen from the air into the body and the removal of carbon dioxide from the body into the air. It consists of the lungs and respiratory muscles (the diaphragm and intercostal muscles).
The respiratory system works interdependently with the circulatory system, which is responsible for transporting the oxygen supplied by the respiratory system.
Oxygen keeps the body alive and performing its daily functions. It is essential for aerobic energy production and muscle work.
The location of the lungsThe right and left lungs are located in the thorax. They are positioned on either side of the ribcage, which gives them protection. A large sheet of muscle at the bottom of the ribcage (the diaphragm) separates the thorax from the abdomen.
The heart is positioned between the lungs (slightly left of centre). The heart and the lungs are connected by the pulmonary blood vessels (see figure 5.1).
The function of the lungsThe function of the lungs is to take in oxygen from the air we breathe and remove carbon dioxide (a by-product of aerobic energy production) from the body into the air (see table 5.1).
All body functions require oxygen, so respiration and the exchange of gases (taking in oxygen and removing carbon dioxide) happens continuously without conscious thought or control (involuntarily). However, remember that we can bring our breath under conscious control; disciplines such as Pilates and yoga control and use breathing techniques as part of their practice.
The lungs take in oxygen and the body uses it to produce energy for daily functions. The waste
product is carbon dioxide, which is transported back to the lungs for
removal.
SOMETHING EXTRABreathing is controlled by the respiratory centre in the brain. Breathing would stop without commands from the brain!
Figure 5.1 The respiratory tract
Copyright © 2014 Active IQ Ltd. Not for resale | 35
Section 5: The respiratory systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

GAS INHALED AIR EXHALED AIR DIFFERENCE KEY POINT
Nitrogen N2 79% 79% No change Not used by the body
Oxygen O2 21% 17% 4% decrease Used by the body for energy production
Carbon dioxide CO2
< 1% 4% 4% increase Produced by the body (a waste product)
Trace gases < 0.001% < 0.001% No change Not used by the body
Table 5.1 Composition of air
Breathing stimulusThe two different mechanisms that trigger the human body to breathe are:
• Rising levels of CO2 in the blood.
• Stretch receptors in the respiratory muscles (intercostal muscles) becoming stretched.
The passage of air through the respiratory tractAir enters the body through the following structures during inhalation:
• Nose and mouth.
• Pharynx (throat).
• Larynx (voice box).
• Trachea (wind pipe) – a tube-like structure kept open by cartilage rings.
• Primary bronchi (right and left).
• Bronchioles.
• Alveoli (air sacs).
Carbon dioxide and oxygen leave the body in the reverse direction during exhalation (see figures 5.2 and 5.3).
Figure 5.2 The respiratory tract
Nose
Larynx
Trachea
Lungs
Bronchi
Diaphragm
36 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 5: The respiratory system

Structure of the lungsFigure 5.3 illustrates the key structures of the lungs.
Mechanics of breathing
The main muscles involved in the action of breathing are the diaphragm and the internal and external intercostal muscles.
The main phases of the breathing cycle are:
• Inspiration/inhalation – drawing air into the lungs.
• Expiration/exhalation – expelling air out of the lungs.
• There is also a short pause before both inspiration and expiration.
These four stages of the breath are a focus during yoga and some practices will manipulate the ratios of breathing during each stage.
During inspiration the diaphragm muscle contracts causing the normal ‘dome shape’ to flatten. The external intercostal muscles also contract, raising the ribcage (see figure 5.4). These actions increase the chest cavity volume. This increase in volume creates a negative pressure between the air in the lungs and air in the atmosphere. This is very much like a vacuum effect in which the negative pressure sucks air into the lungs until the two pressures are balanced.
During expiration the diaphragm muscle relaxes and rises returning upwards to its dome shape. The intercostal muscles also relax, decreasing the chest cavity volume. This creates a positive pressure, which ‘pushes’ some of the air out of the lungs.
During exercise, when breathing becomes more vigorous, the internal intercostal muscles become active. During expiration they contract, forcing the ribs down and removing the air in the lungs.
Breathing patternCostal breathing is a shallow pattern of breathing through the chest and involves the contraction of the external intercostal muscles. Individuals with a sedentary lifestyle may develop a pattern of shallow breathing because the diaphragm has reduced space to move. Shallow breathing is also experienced during times of stress.
Diaphragmatic breathing is a deeper method of breathing. The abdomen is encouraged to rise and fall; it involves the contraction and lowering of the diaphragm. Diaphragmatic breathing is promoted in activities like yoga to assist relaxation.
Figure 5.3 Structure of the lungs
MUSCLES INVOLVED IN BREATHING The main muscles involved in breathing are the diaphragm, which is at the bottom of the ribcage, and the intercostal muscles between the ribs.
Figure 5.4 Movement of the diaphragm
Left lung
Left bronchus
Bronchiole
Terminalbronchiole
Alveoli
Right bronchus
Right lung
Trachea
Copyright © 2014 Active IQ Ltd. Not for resale | 37
Section 5: The respiratory systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Lateral and thoracic breathing encourage the sides and back of the ribcage to expand during inhalation to maximise the expansion of the ribcage and use of the lower lungs. Breathing in this way allows engagement of the abdominals to be maintained while exercising. It is a very efficient way of breathing (used in Pilates); it also promotes flexibility in the thoracic spine.
Gaseous exchange Gaseous exchange occurs in the lungs and the cells of the body.
The lungs and the circulatory system
Oxygen (O2) in the alveoli (lungs) diffuses into the bloodstream (capillaries surrounding the alveoli) and travels to the heart where it is circulated around the body.
Carbon dioxide (CO2) is transported from the body via the blood. It diffuses into the alveoli (lungs) where it is removed during expiration.
The body cells and the circulatory system
Oxygen in the blood (travelling from the heart) diffuses into the cells (mitochondria) for aerobic energy production.
Carbon dioxide from the cells diffuses into the blood where it is circulated back to the heart and then onto the lungs for removal during expiration.
Diffusion
Gaseous exchange occurs through a process called diffusion, which is the movement of a gas from an area of high concentration to an area of low concentration. The concentration of oxygen decreases between the mouth and the lungs, therefore the gas flows in this direction. Carbon dioxide flows in the opposite direction.
Once the oxygen gets into the alveoli (the air sacs) it continues to follow this concentration gradient and diffuse into the bloodstream. The alveoli have minute capillaries running over and around them. The alveolar walls and the capillary walls are so thin that they allow gases to pass through them; oxygen passes into the blood and at the same time carbon dioxide passes back into the lungs to be exhaled.
Links between the respiratory and circulatory system
Haemoglobin (Hb) is the protein in red blood cells that carries oxygen, carbon dioxide and carbon monoxide (CO) in the blood. The oxygen (O2) binds to the haemoglobin in the red blood cells and, at the same time, carbon dioxide (CO2) dissociates from the haemoglobin and diffuses from the blood into the alveoli in the lungs to be removed from the body.
The red blood cells are transported via the circulatory system.
SOMETHING EXTRAThe surface area of the alveoli in both lungs is equivalent to the size of a half a tennis court.
DIFFUSION During inspiration high levels of oxygen are present in the alveoli. This diffuses into the capillaries that surround the alveoli, where there is a low concentration of oxygen. Oxygen is then transported to the heart via the pulmonary vein.
Figure 5.5 Gaseous exchange between the alveoli and capillaries in the lungs
CapillariesAlveoli
• Oxygen from the lungs is carried by the red blood cells to the heart where it is pumped from the heart to the body.
• Carbon dioxide from the cells is carried by the red blood cells back to the heart and into the lungs.
38 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 5: The respiratory system

Lung volumes and definitionsThe study of lung function is called spirometry and there are a number of different measurements, all of which can be affected by age, gender, size and physique:
• Tidal volume (TV) – the amount of air inhaled/exhaled in one breath.
• Minute ventilation (MV) – the amount of air inhaled/exhaled in one minute.
• Breathing rate (BR) – the number of breaths taken in one minute.
Exercise and the respiratory system
End of section: Learning check Answer the following questions and make notes to revise this section.
• Where are the lungs located?• What is the function of the lungs?• Where does oxygen enter the body during inhalation?• How does air pass through the respiratory tract?• What are the main muscles involved in breathing? • What is inspiration?• What is expiration? • What are the alveoli?• What is gaseous exchange?• Where does gaseous exchange take place?• Explain the process of gaseous exchange.• What is diffusion? • How does exercise affect the respiratory system?• What is costal breathing?• What is diaphragmatic breathing?• What is lateral thoracic breathing?• Which exercise discipline uses lateral thoracic breathing?
MV (ml/min) = BR (per min) x TV (ml) = 12 x 500 (ml) = 6000ml/min x or (6 l/min)
SHORT-TERM
LONG-TERM
During exercise tidal volume increases; more air is inhaled and exhaled and breathing rate increases.
Capillary beds surrounding the alveoli increase allowing greater potential for gaseous exchange. The respiratory muscles also become stronger, assisting inspiration and expiration during exercise. There are no changes to the lungs.
DID YOU KNOWTHE AVERAGE BREATHING RATE FOR ADULTS AT REST IS 12-18 BREATHS PER MINUTE.
Copyright © 2014 Active IQ Ltd. Not for resale | 39
Section 5: The respiratory systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Section 6: The circulatory system
The circulatory system is the main transport system of the body. It is responsible for the delivery of oxygen, nutrients, hormones and medication (when taken) to different parts of the body. It is also responsible for transporting waste products, such as carbon dioxide and lactic acid, for removal.
The circulatory system consists of the:
• Heart.
• Blood.
• Blood vessels.
The function and location of the heartThe heart is essentially a muscular pump which pushes oxygen and nutrients around the body to the body tissues. It is about the size of a man’s clenched fist and lies behind the sternum, just left of centre. It is positioned between the right and left lungs (see figure 6.1).
Heart rateThe heart is stimulated to contract by a complex series of integrated systems. The heart’s pacemaker – the sinoatrial (SA) node – initiates the cardiac muscle contraction. The SA node is located in the wall of the right atrium. The myocardium (heart muscle) is stimulated to contract about 72 times per minute by the SA node as part of the autonomic nervous system.
The structure of the heartThe heart is a cardiac muscle. It is made up of thick muscular walls (myocardium) and is divided into separate left and right halves.
• The right half receives blood from the body and pumps blood to the lungs.
• The left half receives blood from the lungs and pumps blood to the body.
Each side of the heart is hollow and is further broken down into two smaller connected chambers.
There are four chambers in total:
• The two upper chambers (atria) are the chambers that receive blood from the veins.
• The two lower chambers (ventricles) are the chambers that pump blood into the arteries.
Atrium is the Latin word for ‘hall’ or ‘entranceway’ and this is the chamber that blood flows into first when entering either side of the heart. The atria receive blood via the veins from different parts of the body and pump the blood down into the ventricles. The atria are smaller than the ventricles and do not really have to contract particularly hard. Even if the atria fail to contract properly, most of the blood in the atria still flows into the ventricles passively.
HEART RATEThe average adult heart rate is around 72 beats per minute.
Figure 6.1 Location of the heart
40 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 6: The circulatory system

The ventricles supply the force to push the blood to its various destinations. In a cardiogram it would be easy to see that the left ventricle has larger muscular walls than the right ventricle. This is because the left side pumps its contents to the furthest parts of the body, whereas the right side only has to pump its contents to the adjacent lungs.
Heart valvesThere are a number of different valves around the heart, which all perform slightly different tasks.
The atrioventricular (AV) valves separate the atria and ventricles and prevent the flow of blood back into the atria during ventricular contraction.
The semilunar valves prevent the flow of blood back into the right (pulmonary valve) and left ventricles (aortic valve) during ventricular relaxation.
Ventricular contraction is called systole and ventricular relaxation is called diastole. Systole and diastole are measurements of blood pressure.
Open and closed valvesHeart valves Figure 6.3 (b) closed and open valvesFigure 6.3 (a) heart valves
REMEMBER Systole and diastole are measurements of blood pressure.
Systole = the pumping and contracting phase of the cardiac cycle.
Diastole = the relaxing, resting phase of the cardiac cycle.
Pulmonary Vein - Oxygen rich blood from the lungs
Pulmonary Artery - Oxygen poor blood to the lungs
Aorta - Oxygen rich blood to the body
Vena Cavae - Oxygen poor blood from the body
Left Atrium
Left Ventricle
Right Ventricle
Right Atrium
The heart circulationFigure 6.2 Structure of the heart
Copyright © 2014 Active IQ Ltd. Not for resale | 41
Section 6: The circulatory systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Movement of blood through the four chambers of the heartOxygenated blood (blood rich in oxygen) travels from the lungs via the pulmonary vein and enters the left atrium. It passes into the left ventricle and is then pumped to the body via the aorta (the largest artery of the body).
When the oxygenated blood reaches the tissues it diffuses into the cells (gaseous exchange). Oxygen is delivered to the cells and carbon dioxide is collected. Deoxygenated blood (blood with high levels of carbon dioxide) then travels from the body to the heart via the veins.
Deoxygenated blood enters the right atrium via the vena cava (the largest vein in the body), it passes to the right ventricle and is pumped to the lungs. At the lungs gaseous exchange occurs; carbon dioxide is removed and oxygen is taken in, and the cycle repeats.
Systemic and pulmonary circulationPulmonary circulation is the circulation between the heart and lungs.
• The pulmonary heart chambers are the left atrium and right ventricle.• The pulmonary blood vessels are the pulmonary artery and the pulmonary vein.
Systemic circulation is the circulation between the heart and the body.
• The systemic heart chambers are the left ventricle and right atrium. • The systemic blood vessels are the aorta and the inferior and superior vena cava. The inferior vena
cava carries blood from the lower body. The superior vena cava carries blood from the upper body.
Deoxygenated blood is dark red in colour, but may appear bluish when viewed through blood vessel walls. It is normally coloured blue when shown in diagrams of the heart.
Oxygenated blood is bright red in colour. It is normally coloured red when shown in diagrams of the heart.
Figure 6.4 Circulatory system
Pulmonaryvein
Leftatrium
Aorta
Left ventricle
LUNGS
Pulmonaryartery
Venacava
Rightatrium
Rightventricle
BODY
Pulmonary circulation
Systemic circulation
Oxygenatedblood
Deoxygenatedblood
Gaseous exchange between alveoli and capillaries
Gaseous exchange between muscles and capillaries
42 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 6: The circulatory system

Function of blood vesselsBlood vessels are the transport system for the blood. They carry blood from the heart to the rest of the body and back again.
Blood is the medium that carries nutrients and oxygen to all structures of the body and removes waste products and carbon dioxide. Blood is composed of a number of cells suspended in a liquid called plasma (see table 6.1). Blood consists of the following four components:
COMPONENT DESCRIPTION
Red blood cells (erythrocytes)Carry oxygen
Red blood cells are produced in the soft red bone marrow. They contain the protein haemoglobin (Hb), which binds to oxygen allowing them to carry oxygen (O2). Haemoglobin is the iron-rich pigment that gives red blood cells (and therefore blood) a red colour.The body contains approximately 240-270 million red blood cells in every drop of blood. Blood volume usually consists of about 40% red blood cells.
White blood cells (leukocytes)Destroy bacteria
White blood cells are produced in the red bone marrow. They are transparent and do not contain haemoglobin. They are part of the immune system that fights infection. White blood cells destroy bacteria and other harmful living organisms, protecting the body by removing diseased or injured tissue.
There are fewer white blood cells than red blood cells (approximately 700 times fewer).
Platelets (thrombocytes)Help blood clotting
Platelets are cell fragments rather than whole cells. They assist in preventing blood loss from a damaged blood vessel by forming a platelet plug. They also release chemicals that help to promote blood clotting. This is the initial stage of repair to damaged tissues.
Plasma Plasma is the straw-coloured liquid portion of the blood. It consists predominantly of water (91.5%) and solutes (8.5%), such as proteins, electrolytes, nutrients, gases, hormones, enzymes, vitamins and waste products.
Table 6.1 Components of blood
Structure of blood vesselsThere are different types of blood vessel and these are categorised according to their shape and function. However, all blood vessels are linked to form a continuous circulatory loop; one type of blood vessel is gradually split or linked to form another type of vessel.
There are three main types of vessel that differ in construction and size, according to their function and position in the body. These are the arteries, capillaries and veins. There are two additional sub-types called arterioles (a subdivision of arteries) and venules (a subdivision of veins). These blood vessels are responsible for transporting the blood to and from the heart and delivering nutrients to and from the tissues.
Red blood cells.
White blood cells.
Platelets.
Plasma.
Copyright © 2014 Active IQ Ltd. Not for resale | 43
Section 6: The circulatory systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Arteries
Arteries are muscular tubes with thick walls, which can contract (like all muscle) to squeeze blood along the passageways and away from the heart. The large artery that leaves the left ventricle of the heart is called the aorta. This divides and subdivides to gradually become arterioles.
The smooth muscle tissue that surrounds the artery and arteriole walls is thicker and more powerful than that surrounding the walls of veins. As blood is ejected powerfully from the heart, the arterial walls are required to stretch passively to receive the blood under high pressure. They then contract immediately in a recoil action, to help propel the blood further down the line to the body. This action is called peristalsis.
There are no valves in the arteries other than those at the exit points of the ventricles that prevent backflow. Arteries and arterioles predominantly carry oxygenated blood around the body. The exception to this rule is the pulmonary arteries and arterioles, which carry deoxygenated blood to the lungs to be re-oxygenated.
The arteries branch off into smaller arterioles which lead to smaller and thinner capillaries.
Capillaries
Capillaries have extremely thin walls (approximately one cell thick) and spread to all parts of the body – even the smallest area of tissue.
The walls of these blood vessels are so thin that they allow the diffusion of nutrients and gases into the tissue cells. Food and oxygen pass through the walls from the blood and into individual tissue cells to be used. The waste products (such as CO2 and lactic acid) pass back into the blood to be carried away and excreted. Blood flows through the capillary beds slowly to allow for this exchange. There are a greater number of capillaries than any other type of blood vessel.
After the capillaries have passed the tissue (muscle or alveoli) they gradually link together to form progressively larger blood vessels called venules. These venules then become larger veins.
KEY POINTArteries carry blood AWAY from the heart.All arteries carry oxygenated blood EXCEPT for the pulmonary artery, which carries deoxygenated blood from the heart TO the lungs.
AORTA ARTERIES ARTERIOLES CAPILLARIES
DID YOU KNOWAerobic exercise causes the capillary beds to expand. More capillaries develop in the muscle to enable a greater delivery of oxygen.
CAPILLARIES VENULES VEINS VENA CAVA
Figure 6.5 Structure of blood vessels
44 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 6: The circulatory system

Veins
Veins carry blood from the tissues and back towards the heart. They have thinner walls than arteries with little muscular contractility.
The smooth muscle in the walls contracts automatically in a peristaltic (or wave-like) action to assist the returning blood flow. Veins and venules predominantly carry deoxygenated blood, which is high in carbon dioxide (CO2) as a result. The exception to this rule is the pulmonary veins and venules, which carry oxygenated blood to the heart.
The flow of blood back to the heart is called venous return. Unlike arteries, veins carry blood under low pressure, which makes its return back up the body to the heart more difficult. All veins have a series of one-way valves that work against gravity to prevent the backflow of blood as it passes back towards the heart. This helps to prevent reversed blood flow or pooling of blood.
Control of circulatory blood flowThe blood vessels are able to narrow (vasoconstrict) or widen (vasodilate) because of the smooth muscle found in their walls. More or less blood will flow through them as a result.
This enables the body to direct the flow of blood to different tissues, depending on what state the body is in and where the oxygen and nutrients are required. This also plays a part in the regulation of blood pressure.
After a meal the blood vessels that feed the digestive system are vasodilated and blood flow is increased to assist digestion, while blood vessels feeding the muscles are vasoconstricted, reducing the blood flow.
During exercise the opposite happens; more blood is routed to the muscles and less is available to the organs and digestive tracts.
Eating a large meal too close to a training session or match will not allow enough time for the food to be digested in the stomach, causing cramp and sometimes vomiting.
KEY POINTVasoconstriction = blood vessels narrow.
Vasodilation = blood vessels widen.
Capillary / alveoli interaction
Pulmonary artery
Vena cavae
Capillary / tissue interaction
Aorta
Pulmonary vein
Pulmonary Circulation
Systemic Circulation
Circulation to the head
TRAINER TIP Avoid eating a large meal before exercise (1-2 hours). Blood will be needed for digestion and any redistribution of blood to the working muscles may cause stomach cramps or vomiting.
KEY POINTVeins carry blood TOWARDS the heart.All veins carry deoxygenated blood EXCEPT for the pulmonary vein which carries oxygenated blood FROM the lungs to the heart.
Figure 6.6 Overview of circulation
Copyright © 2014 Active IQ Ltd. Not for resale | 45
Section 6: The circulatory systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Venous return and blood pooling Blood pooling occurs when blood in the veins pools in the extremities. Stopping suddenly during intense exercise can contribute to blood pooling. The heart is pumping out larger volumes of blood and when the leg muscles stop working there is reduced assistance for helping the veins return blood back to the heart.
Venous return is an important mechanism for helping the return flow of blood to the heart and preventing blood pooling. Long periods of inactivity can slow the blood flow from the lower legs, which can result in blood pooling. A blood clot or deep vein thrombosis (DVT) may then form, blocking the blood vessel. Pressure (e.g. caused by an airline seat pressing on the veins in the back of the knee) can contribute to reduced blood flow.
Blood pressureBlood pressure is a measure of the force that the blood applies to the walls of the arteries as it flows through them.
Blood pressure is measured in millimetres of mercury (mmHg) and is expressed using two numerical readings. The optimal blood pressure reading is written as 120/80 mmHg (one hundred and twenty over eighty). These two numbers represent the systolic and diastolic blood pressures respectively.
THE CONTRIBUTING FACTORS THAT ASSIST VENOUS RETURN ARE:
GRAVITY
SKELETAL MUSCLE CONTRACTION
NON-RETURN VALVES IN THE VEINS
THE DIAPHRAGM
THE RIGHT ATRIUM
Assists in the return of blood from anywhere above the heart, such as the head and shoulders.
The squeezing action of the skeletal muscles against the veins assists blood flow and venous return (especially contraction of the muscles in the lower extremities).
Prevent the back flow of blood and are one of the biggest factors for assisting venous return.
The large dome-shaped muscle of respiration in the chest cavity produces a suction effect on the veins below the heart.
Helps to ‘suck’ the blood back. As the blood in this chamber empties into the ventricle below, the empty chamber creates a small vacuum helping to draw in blood from the vena cava.
SMOOTH MUSCLE CONTRACTION (PERISTALSIS)
A pumping action of the smooth muscle tissue that takes place continually (veins contain smooth muscle tissue).
KEY POINTThe contraction of the calf muscles during exercise assists venous return and helps to prevent blood pooling.
TRAINER TIP A pulse-lowering activity as part of a cool-down is thought to reduce blood pooling in the lower extremities at the end of an exercise session.
46 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 6: The circulatory system

Systolic blood pressure (SBP) is the pressure exerted on the artery walls when the cardiac muscle is contracting and pumping blood. This is the higher of the two numbers and is usually noted first. It is caused by the increased volume of blood flowing through the arteries with each beat, which increases the pressure within the arteries.
Diastolic blood pressure (DBP) is the pressure exerted on the artery walls when the heart is in a relaxed state. The heart goes through this period of relaxation (or diastole) to allow the chambers of the heart to fill with blood prior to contraction. The diastolic blood pressure is always the lower of the two readings.
Blood pressure is an expression of the arterial blood flow and the peripheral resistance the blood encounters as it flows around the body. It can therefore be expressed in the following equation.
Blood pressure = Cardiac output x Total peripheral resistance
Cardiac output is the volume of blood pumped out by the heart in one minute (ml/min). The greater the cardiac output, the higher the blood pressure.
Total peripheral resistance is the resistance the blood vessels offer to blood flow. The greater the resistance, the higher the blood pressure. Peripheral resistance is increased by constriction or decreased by dilation of the blood vessels (arterioles).
Blood pressure classifications
The blood circulation is a closed system in which the pressure varies constantly. It rises to a peak at the height of the contraction of each heartbeat as the heart pumps blood out. It then falls to a lower level, which it reaches just before each heartbeat.
This variance of pressure is necessary for a healthy circulatory system, but if the pressure is consistently higher than normal at rest it is described as high blood pressure or hypertension.
Optimal blood pressure
Optimal blood pressure, to reduce cardiovascular risk, is below 120 mmHg for systolic and 80 mmHg for diastolic pressure (ACSM, 2014). Readings much lower than this may have some clinical significance, but are not associated with increased cardiovascular risk. Readings higher than optimal pose an increased cardiovascular risk. Readings above 180 systolic and 110 diastolic are a contraindication for exercise.
CATEGORY SYSTOLIC (MMHG) DIASTOLIC (MMHG)
Low < 100 < 60
Optimal < 120 < 80
Normal < 130 < 85
High normal – Pre-hypertension 130-139 85-89
Stage 1 Hypertension 140-159 90-99
Stage 2 Hypertension 160-179 100-109
Stage 3 Hypertension > 180 > 110
Table 6.2 Blood pressure classifications
Copyright © 2014 Active IQ Ltd. Not for resale | 47
Section 6: The circulatory systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Short-term effects of exercise on blood pressure
The short-term effects of exercise are a linear increase in systolic blood pressure (SBP) with increasing levels of exertion. In contrast, diastolic blood pressure (DBP) might decrease slightly during exertion due to vasodilation or remain unchanged, except in individuals with hypertension, where it may rise as a result of an impaired vasodilatory response.
Heavy weight training and isometric exercise increase both systolic and diastolic blood pressure significantly. It is also important to avoid holding one’s breath when performing such exercises. An expiratory effort against a closed glottis, which increases pressure within the thoracic cavity and thereby impedes venous return of blood to the heart, is known as the Valsalva manoeuvre.
Long-term effects of exercise on blood pressure
Aerobic exercise using large muscle groups in rhythmical activity is very appropriate for reducing blood pressure over time. Durstine and Moore (2003) state that endurance training can elicit an average decrease of 10 mmHg in both systolic and diastolic blood pressure in mild and moderate hypertensives.
With the exception of circuit weight training, chronic strength or resistive training has not consistently been shown to lower resting blood pressure (Durstine and Moore, 2003). Resistance training can have many benefits for such groups, but it is not recommended as a means of decreasing blood pressure on its own.
Effects of exercise on the cardiovascular and circulatory systemShort-term effects include:
• Increases in heart rate.
• Increases in stroke volume (amount of blood pumped per heart beat).
• Increases in cardiac output (amount of blood pumped per minute).
• Increases in systolic blood pressure.
• Dilating capillaries.
Long-term effects include:
• Stronger heart muscle.
• Lower resting heart rate (taken after a long sleep).
• An increase in blood pumped in one contraction (stroke volume).
• An increase in blood pumped in one minute (cardiac output).
• Lower working heart rate for the same effort.
• An increase in size and number of mitochondria (cells in the muscle that use oxygen for energy production).
• An increase in the number of capillaries in the muscles leading to increased oxygen delivery to the muscle fibres.
• Sustained optimal blood pressure.
48 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 6: The circulatory system

End of section: Learning check Answer the following questions and make notes to revise this section.
• Where is the heart located?
• What is the function of the heart?
• Where does the heart receive oxygenated blood from?
• Where does the heart pump deoxygenated blood to?
• How many chambers does the heart have?
• Which chambers of the heart receive blood?
• Which chambers of the heart pump blood?
• What is the name of the largest artery leaving the heart?
• What is the name of the largest vein entering the heart?
• What is oxygenated blood?
• What is deoxygenated blood?
• What type of blood is found in the aorta?
• What type of blood is found in the pulmonary vein?
• What type of blood is found in the pulmonary artery?
• Describe some of the differences between arteries and veins.
• Describe capillaries.
• What is blood pooling?
• What is venous return?
• What is blood pressure?
• What is vasoconstriction?
• What is vasodilation?
• Describe systolic and diastolic blood pressure.
• What is optimal blood pressure?
• What blood pressure reading is stage 1 hypertension?
• List some of the effects of exercise on the circulatory system.
• What is pulmonary circulation?
• What is systemic circulation?
• Which side of the heart deals with oxygenated blood?
• Which blood vessel leaves the left atrium?
• Which blood vessel enters the right atrium?
Copyright © 2014 Active IQ Ltd. Not for resale | 49
Section 6: The circulatory systemAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Section 7: The energy systems
All functions of the body require energy; including muscle contraction to move the skeleton, digestion of food, respiration, and repair and growth of the body tissues.
This energy comes from the breakdown of a chemical substance known as adenosine triphosphate (ATP). ATP is the energy currency of the body; it is the only fuel the human body recognises and uses. The body would cease to function and survive without ATP.
Adenosine triphosphate (ATP) can be likened to the fuel that runs a car. A car that is fuelled by unleaded petrol cannot run on leaded petrol or diesel. Similarly, the body can only be fuelled by ATP.
Adenosine triphosphate – the energy currency ATP is composed of one adenosine molecule bond with three phosphate molecules. ATP releases its energy when one of its high energy phosphate bonds is broken and it is converted to adenosine diphosphate (ADP). When this high energy bond is broken down, energy is released (see figure 7.1).
There is a very limited store of ATP within the muscles; it only lasts for approximately one to two seconds. Once the limited store of ATP has been used up, it has to be remade. Re-synthesis of ATP comes from either the breakdown of phosphocreatine (another chemical in the body) or from the breakdown of certain nutrients in the diet (such as carbohydrate, fat and protein), which can be used to rebuild stores of ATP.
Production of energy and adenosine triphosphate The three energy systems use different fuels to convert the ADP back into ATP for use by the cells. These energy systems are:
• Creatine phosphate (or phosphocreatine) system (anaerobic).
• Lactate (or anaerobic glycolysis) system (anaerobic).
• Aerobic (or oxygen) system (aerobic).
KEY POINTAdenosine triphosphate (ATP) is the energy currency of the body; it is the only fuel the human body recognises and uses. Without ATP, the body would cease to function and survive.
Figure 7.1 Breakdown of ATP to produce energy; ATP is converted to ADP when energy is released
APPAP
PP
P PAP
PP
energy
50 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 7: The energy systems

Creatine phosphate (CP) or phosphocreatine system
The CP system uses chemical energy to remake ATP. It does not require oxygen, fat or carbohydrate.
ATP can almost immediately be regenerated by using creatine phosphate – another chemical that is stored in the body. The phosphate from the creatine phosphate is used to remake ATP.
Creatine phosphate, like ATP, has a high energy bond which, when broken down by the enzyme creatine kinase, releases enough energy to yield an ATP molecule. This chemical reaction is very quick, but only lasts for a very short period of time because of limited creatine phosphate stores. The CP system is exhausted after a maximum of ten seconds.
This system is utilised during activities requiring near maximal exertion and, when a muscle needs to generate a lot of force very quickly, e.g. 100-metre sprint, javelin throw, golf swing, high jump or a maximal resistance lift.
CP and ATP stores are 50% restored after 30 seconds and fully restored after about five minutes of rest.
Lactate system
The lactate system uses glycogen (carbohydrate) stored in the muscle fibres to remake ATP. Glycogen is broken down into glucose without oxygen and ATP is produced along with lactic acid (a waste product).
The lactate system provides a lot of the required energy in one of two instances:
• When near maximal exercise lasts longer than CP sources can provide (beyond ten seconds).
• When the intensity during aerobic activity starts to demand more energy than the aerobic system can provide.
The conversion of glucose to lactic acid occurs constantly within the body and only becomes a problem when lactic acid starts to accumulate. If the rates of lactic acid production and removal are equal then there is no problem, but if the production of lactic acid exceeds the muscles’ and cardiovascular system’s ability to disperse it, there will be a build-up of lactic acid, which will eventually cause the cessation of activity.
PP
P
energy for muscle
contraction
CP from muscle lends
a phosphate (P) to ADP ATP
is resynthesized into
ATPloses phosphate to
release energy
ADP
ADP+P
KEY POINTATP is remade using creatine phosphate. It lasts up to 10 seconds. It is used during high-intensity activities, e.g. 100-metre sprint.
KEY POINTThe lactate system uses stored glycogen to remake ATP without oxygen. The by-product is lactic acid. When lactic acid levels increase at a higher rate than they can be removed, a burning sensation is experienced in the muscles.
THE LACTATE SYSTEM High-intensity activities that last for up to three minutes will use this system, e.g. a 400-metre sprint.
Figure 7.3 ATP derived from the creatine phosphate system
ADP creatinephosphate ATP creatine
(waste product)
Figure 7.2 Re-synthesis of ATP using creatine phosphate
Copyright © 2014 Active IQ Ltd. Not for resale | 51
Section 7: The energy systemsAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

This is known as the onset of blood lactate accumulation (OBLA), which is associated with certain sensations, such as laboured breathing (or breathlessness), ‘heavy’ limbs and pain (‘the burn’), usually causing a necessity to slow down or stop.
Targeted interval training improves the body’s ability to withstand the build-up of lactic acid (lactate tolerance) and/or the ability to remove it quickly, which delays or prevents accumulation.
Anaerobic training uses up the glycogen stored in the muscles quickly and requires short periods (one to three minutes) of strenuous activity followed by periods of recovery. Ideally this recovery should be active (e.g. walking between running intervals) to aid the return of blood to the liver. Insufficient recovery, or static rest, might not allow the lactic acid to be dispersed before the commencement of the next interval.
Aerobic (oxygen) system
Aerobic simply means ‘with oxygen’ and refers to the energy system that produces ATP from the complete breakdown of carbohydrate, fat and protein in the presence of oxygen.
The aerobic energy system is dominant when there is sufficient oxygen in the cells to meet the energy production requirements, e.g. when the body is at rest and the intensity of the activity is low to moderate (when adequate oxygen can be delivered by the circulatory system).
Fat (fatty acids) and carbohydrate (glucose) are the two main macronutrients that supply the body with ATP during aerobic metabolism. Whether the body is at rest or exercising aerobically, both carbohydrate and fat are required in varying proportions.
The aerobic system produces ATP, carbon dioxide, water (H2O) and heat from the breakdown of fat and carbohydrate. These waste products are easily removed from the body. Carbon dioxide is transported to the lungs via the circulatory system and water is removed via sweat. The complete breakdown of one glucose molecule regenerates 36 moles of ATP, or 263 kcal. One molecule of fat (one glycerol and three fatty acids) yields 460 moles of ATP, making it a far greater energy supply. Carbohydrate is a preferred energy source because it releases it a lot faster (although it releases less energy per molecule).
KEY POINTCarbohydrate is a preferred energy source because it will release energy a lot faster (although it will release less energy per molecule).
AEROBIC SYSTEM It uses oxygen, glycogen and fats as fuel. The by-products carbon dioxide and water are easy to remove.
It lasts as long as oxygen can be supplied, so it is dependent only on the strength and efficiency of the heart and circulatory system.
cellular respiration in mitochondria
fatty acids
oxygen
CO2 H20
glucose
ATPFigure 7.5 Aerobic energy system
Figure 7.4 Glycogen/glucose to resynthesize ATP
52 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 7: The energy systems

Oxygen uptake and fitnessThe use of oxygen by the cells of the body is known as oxygen uptake or consumption. When the body is at rest the volume of this oxygen uptake (VO2) is approximately 3.5 millilitres of oxygen per kilogram of bodyweight per minute (ml/kg/min).
This value of oxygen uptake is also known as one metabolic equivalent (or MET). Activities can therefore be categorised as light, moderate or strenuous intensity, depending on the amount of oxygen uptake required or the METs.
The maximal amount of oxygen a person can take in (respiratory), transport (cardiovascular) and utilise (muscular) provides an indication of their fitness.
The more oxygen taken in and used by the muscles, the higher the intensity they could work at and the fitter they would be. This maximal oxygen uptake (or VO2 max) is generally accepted as the best way to measure someone’s fitness levels and can be directly measured or estimated using various aerobic fitness tests.
Where aerobic and anaerobic energy production take place
All three energy systems produce energy at the cellular level, but in different places within the actual cell.
Aerobic energy production occurs in small cell structures called mitochondria.
The larger the mitochondria (or the more mitochondria within the cell) the greater the potential for ATP production of that cell. This indicates that an athlete could run, swim or cycle at a higher intensity for a sustained period of time without fatigue.
Anaerobic energy production (CP and lactate system) occurs in the muscle cells, but outside the mitochondria.
The use of the three energy systems during aerobic and anaerobic exercise
It is very important to realise that all three systems are working together at any one time to provide the body with energy, but activities of different intensity and duration tend to use one system more predominantly than the others:
• A golf swing or shot put would predominantly use the CP system.• A 400-metre sprint or a squash or tennis rally would predominantly use the lactate system.• A long-distance marathon run would predominantly use the aerobic system.
It is the intensity and duration of the activity or sport that determines which system predominates.
KEY POINTAerobic energy production takes place in the mitochondria.
Anaerobic energy production takes place in the muscle cell, but outside the mitochondria.
Figure 7.6 The aerobic energy system
Figure 7.7 The use of energy systems
Creatine phosphate Lactate Aerobic
100
75
50
25
0
Time 0 seconds 60 seconds 120 seconds
% of
Tota
l Ene
rgy
Copyright © 2014 Active IQ Ltd. Not for resale | 53
Section 7: The energy systemsAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

During a 5000-metre race, for example, the first ten seconds will use the ATP/CP system. During the next 20-30 seconds there will be a transition from the CP to lactate system. After 30 seconds and up to two minutes the lactate system will be used. Between two and five minutes there will be a transition from the lactate to aerobic system and beyond five minutes the aerobic system will be used. A final sprint will combine both aerobic and lactate systems (Davis, Kimmet & Auty, 1986).
A similar process of movement through the energy systems would apply during an exercise or training session. The immediate system to engage to supply energy and resynthesise ATP is the creatine phosphate system. When CP stores deplete, the transition will be to the lactate system, which doesn’t use oxygen. Gradually, the circulatory system will respond to the demands and deliver oxygen and the
aerobic energy system will be used. However, the intensity of the activity and the efficiency of the individual’s circulatory system, will also be determining factors that influence the energy system used predominantly.
Summary of energy systems
ENERGY SYSTEMS
CP SYSTEM LACTATE SYSTEM AEROBIC SYSTEM
Oxygen dependency Anaerobic Anaerobic Aerobic
Speed of energy production Very rapid Rapid Slow
Substrate needed(energy source)
Stored chemical energy(phosphocreatine)
Glycogen Glycogen and fat
Amount of energy produced Very limited ATP Limited ATP Unlimited ATP
By-products of energy production
No fatiguing waste products
Lactic acid No fatiguing waste products (only carbon dioxide and water)
Duration of energy production
Short duration (0-10 seconds)
1-3 minutes of intense activity
Long duration
Intensity of activity Very high intensity(95-100% max effort)
High intensity(60-95% max effort)
Low to moderate intensity(up to 60% max effort)
Recovery required Quick recovery(30 seconds-5 minutes)
20 minutes-2 hours(breakdown lactic acid)
Time to eat and drink(to replenish fuel stores)
Predominant fibre types Type IIb Type IIa Type I
Table 7.1 Summary of the energy systems
The energy continuum
At no point in time do we solely use either aerobic or anaerobic energy sources. The intensity of the activity determines which system is most active. Figure 7.8 shows how the energy systems are used by different activities.
TRAINER TIP It is important to warm up before exercise to give the heart and circulatory system time to respond and deliver oxygen. Untrained individuals will need a longer and more gradual warm-up.
Figure 7.8 The energy continuum
aerobic anaerobicWeight lifting
Gymnastics200m sprintIce hockey
100m swimTennis
Hockey
800m runBoxing
2000m row1mile run
400m swim
2mile run3mile run
Skating 10kmMarathon
100m sprint; golf & tennis swings;American football
Basketball; baseball; 400m sprint
Lacrosse
200m swim; skating
1500m run
800m swim
0%102030405060708090
100%
100%9080706050403020100%
54 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 7: The energy systems

Effects of exercise on the energy systems
Exercise results in the following aerobic adaptations:
• Increased number of red blood cells.
• Increased efficiency of the heart and lungs.
• Stronger heart muscle.
• Increased stroke volume.
• Lower resting and working heart rate for a given intensity.
• Increased capillarisation at the muscles.
• Increased size and number of mitochondria.
• Increased efficiency of gaseous exchange in the lungs and at a muscular level.
• Increased oxygen uptake.
• Improved removal of metabolic waste products.
• Improved efficiency of oxygen use at a muscular level.
Exercise results in the following anaerobic adaptations:
• Increased creatine phosphate stores in the muscles.
• Increased muscle glycogen storage capacity.
• Increased thickness or diameter of muscle fibres.
• Increased force production capacity of muscle fibres.
• Improved resistance to fatigue under high-stress, anaerobic conditions.
• Increased efficiency of lactic acid removal from muscles.
• Improved recovery after high-intensity exercise.
End of section: Learning check Answer the following questions and make notes to revise this section.
• What is the energy currency for the body? • What does aerobic mean?• What does anaerobic mean? • What is creatine phosphate? • Which energy system can produce energy for long durations?• Which energy system would be used maximally during a 100-metre sprint?• Which energy system would be used predominantly during a 400-metre sprint?• What are the by-products of the aerobic energy system? • What would be experienced when lactic acid levels rise in the muscle? • How is carbon dioxide removed from the body?• Which energy system uses glycogen and fats to produce ATP?• Which energy system uses glycogen without oxygen to produce ATP? • What is H2O?• What is the chemical symbol for oxygen?• What is the chemical symbol for carbon dioxide? • Describe how carbohydrates, fats and proteins are used in the production of energy/adenosine
triphosphate.• Explain the use of the three energy systems during aerobic and anaerobic exercise.
Copyright © 2014 Active IQ Ltd. Not for resale | 55
Section 7: The energy systemsAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Section 8: The life course of the musculoskeletal system and implications for special populationsAll body systems change and develop throughout the lifespan and in response to life events, such as pregnancy. A basic awareness of these changes allows for a comprehensive understanding of the implications of exercise when dealing with specific populations.
Young people (14-16) The musculoskeletal system undergoes some significant developmental changes during adolescence.
Muscle mass
Muscle mass steadily increases as children grow. At birth approximately 25% of body weight is muscle mass. During puberty an increase in hormone production results in an increase in muscle mass. Hormonal differences between boys and
girls mean that increases in muscle mass are greater for boys throughout adolescence. However, at age 11 (pre-adolescence) girls can be stronger because their lean body mass may be higher at this point. By adulthood about 40% of a person’s total body mass is muscle.
Body fat
Girls generally carry more body fat than boys during and after the growth spurt. Increasing levels of obesity in children and young people also require specific consideration, i.e. reducing impact and intensity to minimise stress on joints for young people who are overweight or obese. Young people who are obese may find it challenging to achieve the recommended 60 minutes of moderate to vigorous activity per day; therefore both intensity and duration need to be progressed gradually to reach the recommended targets (ACSM, 2014).
The skeletal system and the growth spurt
There are various stages of maturation at which bones suddenly develop at a more rapid rate. These growth spurts happen at different rates and ages for boys and girls.
• For girls, it is usually between the ages of 10 and 12, growing fastest at 12 to 13, and normally ending at the age of 18.
• For boys, it is usually between the ages of 12 and 14, growing fastest at 14 to 15, and normally ending at the age of 20.
KEY POINTMuscle mass steadily increases with age. At birth approximately 25% of body weight is muscle mass and by adulthood about 40% of total body mass is muscle.
Adolescence
Cartilage growth plate
Compact bone containing osteocytes
Cartilage growth plate
Childhood
Cavity
Foetus: At 2-3 months
Blood vessel
Foetus: First 2 months
Cartilage model forms
Compact bone develops starting at primary ossification site
Spongy bone develops at secondary ossification sites
The growth plates promote longitudinal growth until young adulthood
Figure 8.1 Development of bone throughout childhood56 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 8: The life course of the musculoskeletal system and implications for special populations

During the growth spurt, growth cartilage is vulnerable to trauma and overuse. An injury that would cause a ligament sprain in an adult could be a potentially serious growth plate injury for children and adolescents.
Growth plate fractures are more common in boys than girls, with the greatest incidence occurring among 14-16-year-old boys and 11-13-year-old girls.
Approximately half of all growth plate fractures occur in the lower end of the outer bone of the forearm (radius) at the wrist. These injuries also occur frequently in the bones of the leg, e.g. femur, ankle, foot or hip bones. The actual fracture occurs between the shaft and the head of the bone around the growth area (epiphyseal plates). Growth plate injuries at the knee present the greatest risk of complications. Nerve and blood vessel damage occurs most frequently at this joint and therefore injuries to the knee have a much higher incidence of premature growth arrest and crooked growth.
About 85% of growth plate fractures heal without any lasting effects. An arrest in growth depends on the following factors:
• Severity of the injury.• Age of the child.• Area of the body affected.
Flexibility
During the growth spurt there is an increased injury risk because the soft tissue around the joints is already stretched, as muscle growth does not keep up with bone growth.
Caution should be taken when teaching any stretch exercise. The aim should be to stretch only to the point of mild tension and to avoid overstretching.
Limb length
During the growth spurt young people have disproportionately long legs, meaning that they are biomechanically out of balance and potentially less coordinated.
The vulnerability of the musculoskeletal system requires specific considerations. Some general guidelines include:
• Avoid heavy, repetitive lifting. • Avoid excessive high-impact movements, e.g. jumping.• Promote optimal technique.• Warm up and cool down for longer.
Older adults (50+)The ageing process brings many changes to the musculoskeletal system (see table 8.1); these include:
• Progressive loss of bone mass (osteopenia and risk of osteoporosis).• Reduction in joint range of movement. Thickening of ligaments.Loss of elasticity of connective tissue and muscle.• Wear and tear to cartilage found on bone ends leading to degenerative changes in joint structures (osteoarthritis).• Postural changes (kyphosis).• Decrease in number of functioning fast twitch muscle fibres and an increase in functioning slow twitch
muscle fibres. Loss of muscle mass (sarcopenia).• Higher body fat and lower fat-free body mass.
Staying active slows down the rate of these changes. However, after the age of 35-40 there is a steady and gradual decline.
SOMETHING EXTRA Although many growth plate injuries are caused by accidents that occur during play or athletic activity, growth plates are also susceptible to other types of injury, infection and disease.
Copyright © 2014 Active IQ Ltd. Not for resale | 57
Section 8: The life course of the musculoskeletal system and implications for special populationsAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

Bone mass
Loss of bone mass is a significant effect of ageing (see figures 8.2a and 8.2b).
Osteopenia is a condition where bone mineral density is lower than normal. It is considered to be a precursor to osteoporosis.
Osteoporosis is a disease characterised by low bone mass and deterioration of bone tissue (the bones become more porous) leading to enhanced bone fragility and the increased risk of fracture (see figure 8.2b).
Osteoporosis affects both genders, but is more common in females. Bone development is dependent upon the presence of hormones. In women this is the female hormone oestrogen and in men it is the male hormone testosterone. These hormones influence the formation of bone by promoting the activity of bone building cells called osteoblasts. The body replaces around 10% of its bone a year as long as osteoblasts are active. However, bone mass will start to decrease if osteoclast cells, which destroy or break down old bone, are more active than osteoblasts.
Regular weight-bearing exercise has been shown to help maintain and build up bone mass. Low-impact exercise is generally favoured to avoid unnecessary trauma to the skeletal and muscular systems. Resistance training is also recommended to reduce the effects of ageing. A large percentage of the elderly (over 65s) find it difficult to stand from a seated position (without using the arms to assist lifting) due to an age-related decline in muscle functioning. Exercise promotes stronger muscles, better balance and agility and can also help to prevent falls. People with osteoporosis must take special care when exercising to reduce the risk of fracture due to impact or falls.
EFFECTS OF AGEING FITNESS POTENTIAL CONSIDERATIONS
Fewer fast twitch muscle fibres. Weaker and smaller muscle fibres.Reduced motor neurons. Reduced neuromuscular transmission (fewer nerves sending messages).Fewer capillaries in the muscle.Increased connective tissue. Sensory decline (loss of vision and hearing). Cognitive decline.
Reduced muscular strength. Reduced muscle power. Reduced movement speed.Reduced muscular endurance.Reduced flexibility and range of motion. Reduced balance and coordination. Reduced postural stability. Reduced short-term memory.
Loss of bone mass and reduced bone density.Increased risk of osteoporosis. Reduced availability of synovial fluid. Calcification of the joints (calcium laid down in the cartilage).
Bones less resilient to stress and more susceptible to fracture. Stiffer, less mobile joints. Reduced shock absorption in the joints.
Reduced stroke volume and cardiac output. Less efficient heart and circulatory system.Increased blood pressure. Fewer capillaries. Less elastic vessels.Reduced intake, uptake and utilisation of oxygen.
Lower maximal heart rate. Lower training heart rate. Slower recovery rate. Decreased tolerance to fatigue. Faster rate of tiring. Lower anaerobic threshold. Lower tolerance of high-intensity exercise.
Lawrence (2008)
Table 8.1 Effects of ageing and fitness potential considerations
Figure 8.2a Healthy bone
Figure 8.2b Osteoporotic bone
58 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 8: The life course of the musculoskeletal system and implications for special populations

Adaptations to exercise depend on the age and fitness of the individual. Some general guidelines include:
• Lengthen the warm-up and cool-down. • Lower impact.• Strengthen around fracture sites (wrist, hip and spine).• Promote weight-bearing activity. • Include activities that improve balance. • Lower resistance to accommodate reduced strength.• Use a smaller range of motion in stretches to accommodate reduced flexibility. • Include functional daily activities, e.g. sit to stand.
Pre- and post-natal womenThere are many changes to the musculoskeletal system during pregnancy and the post-natal period (see table 8.2). These include:
• Reduced joint stability (effects of relaxin).• Weaker pelvic floor muscles.• Lengthened and weakened abdominal muscles (growing foetus).• Postural changes, e.g. hyperlordosis or lordosis (hollow back posture).
Relaxin
During pregnancy relaxin (a hormone released from the first trimester) softens ligaments, cartilage and the cervix, allowing greater potential movement at joints. This is especially important for the pelvic girdle and particularly the pubis symphysis and the sacroiliac joint which need to separate to some degree to facilitate delivery of the baby. However, the effects of relaxin mean that joints throughout the body are potentially vulnerable and therefore should not be overly stressed, for example through excessive and vigorous stretching.
Exactly how long relaxin stays in the body after birth is debatable and will vary between mothers. Five months is often quoted, but estimates vary from three months up to a year. In reality, the hormone can be present for as long as the mother is breastfeeding, which may be for up to two years. The mother is the best judge and will know when she no longer ‘feels loose’.
Pelvic floor
Throughout the pre-natal period exercises should be given to strengthen the pelvic floor muscles. As the uterus grows, these muscles become overly stressed and start to sag. This can cause several potential problems; not least of which is stress incontinence, i.e. the leaking of urine.
Abdominal muscles
The abdominal muscles lengthen to accommodate the growing baby and therefore vigorous abdominal exercises should be avoided, with a focus given to maintaining posture.
The American College of Obstetricians and Gynaecologists (ACOG, 1994) recommends that women should avoid all physical stress for two weeks (i.e. ‘not carrying anything heavier than the baby’) and avoid full daily activities for a minimum of six weeks after delivery. It is also advised that those who delivered by caesarean section should not exercise for 12 weeks after delivery to allow proper healing time.
TRAINER TIPPelvic floor exercises should be continued for as long as possible during the post-natal period.
Copyright © 2014 Active IQ Ltd. Not for resale | 59
Section 8: The life course of the musculoskeletal system and implications for special populationsAn
AToM
y An
d P
HySIo
Log
y FoR
ExERC
ISE

End of section: Learning check Answer the following questions and make notes to revise this section.
• At what age does the growth spurt start for girls?
• At what age does the growth spurt start for boys?
• What is osteoporosis?
• What effect does relaxin have during pregnancy?
• What changes to the musculoskeletal system would affect exercise for young people (14-16)?
• What changes to the musculoskeletal system would affect exercise for older adults (50+)?
• What changes to the musculoskeletal system would affect exercise for pregnant or post-natal women?
TRIMESTER 1
(0-3 MONTHS)
TRIMESTER 2
(3-6 MONTHS)
TRIMESTER 3
(6-9 MONTHS)
POST-BIRTH
Increase in weight + 1-3kg. Breasts and uterus start to enlarge. Hormonal changes commence, e.g. increased relaxin, affecting ligaments and joint stability.Morning sickness.
Increase in weight + 6-8kg.Postural changes (shoulder girdle protraction, thoracic kyphosis, long upper back extensors and short tight pectoral muscles). Possible low back pain, neck or shoulder pain. Abdominal muscles start to lengthen and stretch as the baby grows.Change in centre of gravity.
Increase in weight + 3-4 kg. Tired more easily. Venous return may be reduced.Weight of the baby presses on pelvic floor. Pelvic girdle becomes less stable (effects of relaxin).Weight of the baby places stress on the lower spine (increased lordotic curve).Centre of gravity changes affecting balance.
Avoid physical stress for two weeks (ACOG). Return to activity six weeks after normal birth or 12 weeks after a caesarean birth. Hormone levels still high (up to one year).Weaker pelvic floor.Pelvic girdle becomes less stable. Check for diastasis rectii (abdominal separation).Rectus abdominis is mechanically weaker for at least 12 months.
The physiological and postural changes of pregnancy persist after birth for several months, making women vulnerable to injury and long-term physical health problems, such as pelvic floor dysfunction. This has particular significance for exercise involving impact, twisting and rapid, ballistic movements, which should be avoided for at least six months and introduced progressively, when relevant for specific training purposes (e.g. sports performance).
Table 8.2 Effects of pregnancy and post-birth
Key general guidelines are to:
• Include pelvic floor strengthening.
• Focus on correct technique and posture.
• Avoid supine lying after 16 weeks.
• Avoid heavy abdominal exercises.
• Avoid high-impact exercises.
• Avoid excessive stretching (due to relaxin and joint instability).
60 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 8: The life course of the musculoskeletal system and implications for special populations

AimKnowing how to support clients is essential for promoting their long-term commitment to exercise and physical activity. Building an effective working relationship, communicating effectively, understanding client barriers and exploring strategies to overcome them are integral to providing the ongoing support and customer care needed to ensure commitment to any exercise or physical activity programme.
Learning outcomesAt the end of this unit you will:
• Understand how to form effective working relationships with clients.
• Understand how to address barriers to exercise or physical activity that clients experience.
• Understand how to support clients to adhere to exercise or physical activity.
• Understand how to provide ongoing customer service to clients.
SUPPORTING CLIENTS WHO TAKE PART IN EXERCISE AND PHYSICAL ACTIVITY
NB: The terms ‘exercise professional’ and ‘fitness instructor’ are used synonymously to refer to the person who works with clients and delivers exercise and activity sessions. The terms ‘client’ and ‘customer’ are used synonymously to refer to the person who uses the services provided.

The importance of forming effective working relationships with clientsIt is important to develop and maintain effective relationships with clients for many reasons. These are:
• To make the client feel supported and welcome.
• To engage them in active, healthy living.
• To offer relevant advice, information and support, e.g. correct exercise technique.
• To help and support them in any changes they wish to make to their activity levels and lifestyle.
• To promote exercise adherence and generate repeat business, so that they continue to use the service.
• To provide the best possible customer experience – to meet their needs and expectations.
• To gain their trust and make them feel valued.
• To establish and maintain appropriate, professional working boundaries.
• To clarify roles, responsibilities and expectations.
• To uphold the reputation of the organisation as an excellent service provider.
All professional working relationships depend on certain qualities:
• Mutual respect.
• Trust.
• Effective communication.
• Rapport.
• Empathy and positive regard.
• Feelings of safety and security.
• Professional and ethical standards of practice and conduct, with respect to diversity and equality.
• Respect of boundaries.
Section 1: Forming effective working relationships with clients
Working relationships exist in all professions and are developed for a variety of purposes. These include relationships among:
• Clients and customers.
• Work colleagues and team members.
• Managers.
• Other professionals, e.g. GPs and physiotherapists.
Effective working relationships are important for ensuring the efficient and professional delivery of all services and for enhancing the reputation of the industry.
DID YOU KNOWA ‘relationship’ exists when the actions of one person have an effect on another person or group of people.
62 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Forming effective working relationships with clients

Establishing and respecting boundaries All relationships need boundaries in order to function effectively; they are the foundations for the development of trust and mutual respect. Boundaries are especially important in working relationships for ensuring that both parties are clear on their specific roles and responsibilities, and on the expectations of the other person.
Clear boundaries and agreements for working can minimise the potential for conflict, which might arise if boundaries are ambiguous or expectations are not met. It is helpful to clarify all roles and boundaries once you start working with a client, rather than operate on assumptions. In some professions (e.g. counselling), written contracts are discussed, signed and agreed before any work can commence.
Most professions have a code of conduct or professional practice to ensure that clear boundaries are established. For fitness instructors, this code of practice is live on the website of the Register of Exercise Professionals.
Instructors can periodically find themselves in situations that have the potential for boundary violation, e.g. accepting a gift from a client, giving a client a hug when they are successful or unhappy or accepting an invitation to a social event with the client. While these violations may not seem serious, it is important to consider the messages that these actions might send to the other person and the impact they can have on the relationship.
Imagine you were to attend a social event with a client. It might be construed as a ‘date’ or the development of a friendship, in which case the ethics and consequences of changing the relationship in this way must be considered professionally, with appropriate actions taken to ensure that there is no abuse of power.
The instructor should consider how a change in the relationship would affect their employment and the work they do for their organisation. They should also consider the industry codes of practice. In many instances, if a personal relationship (friendship) develops with a client, then it is appropriate to remove any potential conflicts of interest. For example, referring a client to work with another instructor might be preferable to balancing a personal and professional relationship.
EXAMPLES OF AREAS IN WHICH WORKING RELATIONSHIPS MIGHT NEED BOUNDARIES INCLUDE:
• Punctuality and time-keeping.
• Payment for services, e.g. method and time of payment.
• Appointment cancellation and any sundry charges.
• Information sharing and confidentiality.
• Appropriate areas for imparting information, e.g. fitness instructors should not give advice on diets or attempt to diagnose medical conditions.
• Equality, diversity and treating people fairly.
• Advertising professional services honestly; this entails delivering sessions for which qualifications are held.
• Personal relationships with clients.
• Accepting gifts.
• Attending social events with clients.
KEY POINTSetting clear boundaries and respecting these boundaries is important for personal wellbeing (e.g. stress) and to maintain healthy relationships.
Copyright © 2014 Active IQ Ltd. Not for resale | 63
Section 1: Forming effective working relationships with clientsSU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

ACTI
VIT
Y Think about your professional boundaries.
Use your notebook to complete these statements:
• A fitness instructor should always…..
• A fitness instructor should never…..
• The limits of the professional fitness instructor role are determined by…..
• When working with the client, it is the fitness instructor’s responsibility to…..
• When working with the client, it is not the fitness instructor’s responsibility to…..
You might like to compare and discuss your notes with your peers or other instructors.
(Gavin, 2005)
The importance of presenting oneself and the organisation positively to clientsIt is important to present yourself and your organisation in a positive light at all times. This is considered standard practice in all professions.
PRES
ENTIN
G ON
ESEL
F POS
ITIVE
LY TO
CL
IENT
S IS I
MPOR
TANT
FOR:
REPR
ESEN
TING
THE O
RGAN
ISATIO
N PO
SITIV
ELY I
S IMP
ORTA
NT FO
R:
Gaining respect as a professional.
Reflecting high standards of practice.
Building trust and respect.
Reflecting professional integrity.
Building a positive working relationship with the client.
Showing a united working front.
Reflecting high standards of professional practice.
Fulfilling professional duties.
Ensuring the client feels secure and part of a reputable, professional organisation.
Maintaining a positive relationship with the organisation.
64 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Forming effective working relationships with clients

Ann
Presenting a professional image
The way someone thinks and feels about themselves, others and their work (their attitude and beliefs) is often reflected in their appearance, actions, behaviours and communication.
A positive attitude and demeanour (e.g. smiling and being polite) is attractive; a negative attitude (e.g. grumbling and being miserable) can be repellent.
Nobody is happy, positive and upbeat all the time. Personal circumstances can affect thoughts and feelings on a daily basis. Events in the workplace can also trigger feelings of discontent (e.g. work rotas and shifts).
It is poor professional practice to bring any personal or work-related issues to the workplace. It is important to put aside any issues and show a professional approach. Personal problems should be managed in your spare time and any work-related issues should be handled assertively by following organisational procedures.
It would be unprofessional, for example, to speak negatively about an organisation (e.g. complaining to customers or being rude to them); this is passive-aggressive behaviour and often leads to further discontent and conflict. Assertive actions are constructive and enable resolution of problems.
Professional appearance
Clothing and personal grooming should be consistent with the ‘image’ of the organisation and meet the expectations of the clientele. Examples of these include:
HAVING LONG HAIR TIED BACK.
WEARING A CLEAN, IRONED COMPANY UNIFORM AND A NAME BADGE.
WEARING MINIMAL JEWELLERY.
KEEPING TATTOOS AND BODY ART COVERED.
MAINTAINING PERSONAL HYGIENE.
Copyright © 2014 Active IQ Ltd. Not for resale | 65
Section 1: Forming effective working relationships with clientsSU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

Punctuality and reliability
Punctuality and reliability are essential professional ethics. Lack of punctuality suggests a lack of care and effort; it infers poor organisation and time management skills.
It is important to arrive early for client appointments and training sessions; to prepare the necessary resources; to be available to meet and greet the client or clients and to be able to answer (or ask) any questions (e.g. pre-exercise screening checks).
Being late for client appointments or training sessions is unacceptable and reflects badly on both the instructor and the organisation. Repeated lateness will alienate clients (which could cause them to go elsewhere) and may lead to dismissal from a working role.
Professionalism and integrity
Professionalism and integrity are essential. It is important to be honest and to live and work to a high moral code; this means setting the highest possible standards of conduct and includes keeping promises, fulfilling duties and doing what is required to fulfil all working contracts with clients and the organisation. It also means ‘walking the talk’ and practising what is being preached. For a fitness professional or exercise instructor, this would include maintaining your own training and activity levels.
Integrity is also important for dealing with personal client information. Personal information is confidential and should never be discussed with a third party without the client’s consent.
KEY POINTHigh professional standards inspire confidence among clients and help to establish a professional reputation for the instructor and the organisation.
ACTI
VIT
Y Think about the different instructors you have experienced.
Use your notebook to list some of the qualities and behaviours they exhibit, which present them and their organisation positively.
66 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Forming effective working relationships with clients

BE APPROACHABLE
Clients need to feel comfortable if they ask for help.
BE CONFIDENT Self-confidence grows from experience and is a quality that attracts people. It should not be confused with overconfidence, which is often a ‘turn off’ and can push people away rather than attract them.
BE MOTIVATIONAL Providing positive encouragement and constructive, helpful feedback is essential for supporting clients.
BE ORGANISED Keep a day-to-day diary to plan appointments and sessions.
BE A ROLE MODEL
Practise what you preach. Clients are often drawn to instructors because they are inspired by a quality or attribute the instructor possesses. Aim to demonstrate positive attitudes, behaviours and actions.
BE ADAPTABLE Sometimes even the best-laid plans can go wrong. Be flexible and ready to adapt. This includes having alternative activities available to meet different client needs or being ready to use a different piece of equipment if the one you intended to work with is in use or being maintained. Develop an action plan and prepare for the unexpected.
BE EMPOWERING Educate and give clients the chance to make informed decisions for themselves. Use effective communication skills to listen to clients and draw the solutions to overcome the barriers that face them – facilitate rather than dictate.
Personal qualities
Some personal qualities improve the client experience as a whole and reflect positively on the instructor and the organisation.
BE PATIENT, COMPASSIONATE AND SENSITIVE
These reflect empathy and help you gain an understanding of the client’s needs, wants and expectations. For example, if a client is new to exercise, they might need extra time to learn concepts (e.g. how to operate equipment or perform an exercise). Patience and compassion can go a long way towards helping the client develop their skills and knowledge; it could also inspire an instructor to evaluate their approach and search for creative ways of enhancing the client’s learning experience.
BE ENTHUSIASTIC AND MAINTAIN
A SENSE OF HUMOUR
Enthusiasm reflects passion and it is ‘contagious.’ It is pleasant to be in the company of enthusiastic people and their energy can lift spirits in the workplace, as well as the training session.
Copyright © 2014 Active IQ Ltd. Not for resale | 67
Section 1: Forming effective working relationships with clientsSU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

Communication skills to help clients with motivationEffective communication skills are essential in all professional working roles. As an exercise professional and fitness instructor, communication skills are needed to:
• Build rapport and motivate clients to engage with exercise and activity: to become more active.
• Support and encourage clients to maintain their long-term commitment: to continue being active.
Communication skills are used during consultations with clients. They are also needed for delivering sessions to clients.
ACTIVE LISTENING SKILLS NON-VERBAL COMMUNICATION SKILLS
VERBAL COMMUNICATION SKILLS
• Nodding as the client speaks.• Leaning forward.• Positive facial expressions.• Eye contact.• Paraphrasing.• Reflecting and summarising.
• Being aware of personal space.• Using hand gestures.• Smiling.• Maintaining eye contact.• Body language and posture, e.g.
avoiding crossing arms when interacting, as it can appear hostile.
• Avoiding aggressive acts, such as pointing or standing over the client.
• Appropriate tone, rhythm and pitch of voice.
• Appropriate richness, warmth and volume of voice.
• Matching the customer’s words.• Appropriate language.
Table 1.1 Communication skills
Listening
One of the most important skills to develop when working with clients is active listening. When one person listens fully to what another person is saying, it encourages and motivates the person to carry on speaking and sharing information. Active listening is essential for gathering information from clients. Fitness instructors and exercise professionals need to understand their clients to be able to support and motivate them fully. This entails knowing:
THE MOTIVATION TO START BEING MORE ACTIVE
THE MOTIVATION TO MAINTAIN ACTIVE BEHAVIOUR
CLIENT MOTIVATION
The barriers they face.
What they enjoy and dislike.
What motivates and inspires them.
Active listening means more than just listening to the spoken word; it means looking for the meaning behind the words in order to fully understand the person and their wants and needs. Active listening should be supported by effective observation skills, as non-verbal communication (the client’s facial expression, tone of voice, body posture, eye contact and gestures) brings extra meaning to what is being said. Valuable information can be gathered about a client’s emotions, beliefs and motivation by observing these non-verbal cues.
68 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Forming effective working relationships with clients

To listen effectively you should:
Show attention and interest – both verbal and non-verbal communication can be used to communicate attention and interest.
• Verbal statements include acknowledging statements, e.g. “Okay,” “Yes” and “I hear what you say,” and specific skills, e.g. using reflective statements or paraphrasing your client to show attention.
• Non-verbal gestures include maintaining regular eye contact, using nods of the head, gestures (e.g. a smile) and body movements (e.g. leaning forwards) that show attention and interest.
Showing interest and giving attention to a client are supportive, motivational behaviours that help to build the working relationship.
Show empathy and non-judgement. Empathy is the ability to see from another person’s perspective. It doesn’t mean agreeing or disagreeing; it means appreciating and accepting the validity of the other person’s view as their own perspective.
Showing empathy means suspending any need to pass judgement (to agree or disagree) with something the other person says or does (actions, behaviour and words). Empathy is about understanding the other person and getting to know why they behave as they do, rather than judging them for their actions.
Empathy can be developed by reflecting the client’s words back to them, e.g. if the client says they feel tired, a simple reflective statement would be: “you are feeling tired today” or “you don’t feel you have the energy for exercise today.”
Empathy builds rapport and supports the development of a working relationship. Lack of empathy would stop the client from feeling understood or heard and compromise the quality of the relationship.
Any non-empathetic, flippant, dismissive, judgemental or patronising statements in response to something a client says are likely to discourage them from sharing information and might trigger defensiveness, e.g. if the client says they feel tired, responding ineffectively with statements such as “don’t we all,” “never mind, you’ll feel better after this” or “how can you feel tired, you haven’t done anything yet?” would be non-empathetic.
KEY POINTEmpathy builds rapport and will support the development of the working relationship. Lack of empathy will block the client from feeling understood or heard and negatively affect the quality of the relationship.
Copyright © 2014 Active IQ Ltd. Not for resale | 69
Section 1: Forming effective working relationships with clientsSU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

Paraphrasing and summarising are other effective methods of showing attention and interest. The instructor can use their own words to restate or summarise their understanding of the conversation. Paraphrasing and summarising allow the client to expand (say more), disagree (e.g. “no, that wasn’t what I meant, I meant…..”) or confirm that the understanding is accurate.
Client: “I would really like to exercise regularly, but I just don’t have the time.”
Instructor: “You want to exercise more, but can’t find the time.”
Clarifying statements or questions allow you to check your understanding with a client. They can also help the client to elaborate and give more information.
Client: “I need to take it easy at the moment.”
Instructor: “Take it easy?” (a reflective statement asked with a questioning tone) or “What do you mean by ‘take it easy at the moment’?” (an open question).
NB: Care should be taken when asking questions. The aim should be to enquire and gather information, not to confront or challenge.
Use of silence can be powerful. During a consultation, periods of silence can be used to give clients time to think, reflect and find the right words to express their objectives and barriers.
Managing silence requires you to refrain from jumping in and filling the gap with another question or piece of advice; this can hamper the client’s thinking and reflective process.
TRAINER TIPTreat other people the way you would like them to treat you.
COMMUNICATION MOTIVATING DEMOTIVATING
Jargon-free Use simple, accessible language. Overly technical or medical terminology can confuse and frighten clients.
Positive feedback Use constructive, descriptive and positive feedback, e.g. “Great alignment and control.”
Critical or negative comments are not helpful; they can trigger feelings of shame and humiliation that demotivate clients.
Listen rather than giving premature advice
Listen and use active listening skills. Jumping in with ‘expert opinions’ or advice before you have seen the bigger picture shows a lack of interest and respect.
Open body language
Keep an open posture, smile, maintain eye contact and be friendly and approachable.
Closed posture, avoiding eye contact, scowling and raising eyebrows are negative body language; they are likely to put clients off.
Words and language
Use positive, inspiring words, e.g. “well done,” “good to see you,” “great work,” “fabulous” and “do this.”
Avoid negative language and an aggressive tone of voice, e.g. “not like that,” “just don’t,” “poor technique” and “that’s bad.”
Interest and attention
Pay attention to people and show a genuine interest in them.
Being dismissive and disinterested doesn’t motivate clients. Feigning interest is usually recognised at some level of consciousness.
Empathy and non-judgement
Aim to understand clients. Avoid passing judgement; this is a way of telling people that they are ‘not okay.’
Table 1.2 Motivation and communication
70 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Forming effective working relationships with clients

The importance of valuing equality and diversity when working with clientsIt is important to value equality and diversity and to give people the respect and care that they deserve and have a right to expect. It is also important to ensure all work is conducted in accordance with legal, professional and ethical codes of practice.
Equality, diversity and difference
There are various characteristics that people share and have in common (similarities) and some that make them different to others (differences).
These characteristics include age, gender, race, ethnic origin, religion and beliefs, disability (physical or mental), sexual orientation, socio-economic status, ability, levels of confidence, employment status, language spoken, education background, body shape and type, activity levels, fitness and many others.
People have the right to be valued and treated with equal respect and importance regardless of differences.
Some characteristics are protected by legislation, to ensure that people do not experience prejudice, discrimination, harassment or bullying when using services.
Current equality legislation includes The Equality Act 2010, which incorporates the Sex Discrimination Act 1975, Race Relations Act 1976 as amended by the Race Relations Amendment Act 2000, the Disability Discrimination Act 1995, the Sexual Orientation Regulations 2003 and the Religion or Belief Regulations 2003.
All professionals (including exercise professionals and fitness instructors) and organisations are required to operate within the legal framework of equality when providing services, to ensure that all clients and prospective customers are treated equally, fairly and with the highest standards of customer care, irrespective of differences.
Codes of conduct and ethical practice
Most professions have codes of conduct and ethical practice to which professionals within the industry sector have to adhere. These values of the profession are translated into standards of conduct and are applicable to roles across the industry.
Codes of conduct and ethical practice are different to law. Ethical codes guide professionals in their work and help them to make ethical decisions. These codes regulate the behaviour of professionals and breaking them can carry punitive measures. A professional can be charged with breaking the code of conduct without breaking the law.
DEFINITIONSEquality: “Enjoying equal rights and being of the same importance.”
Diversity: “Valuing the individual difference of a person.”
(Gravells and Simpson, 2009)
ETHICAL RESPONSIBILITY “(to) do nothing that will harm the client or society.”
(Ivey, Ivey and Simek-Morgan, 1997)
Copyright © 2014 Active IQ Ltd. Not for resale | 71
Section 1: Forming effective working relationships with clientsSU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

Ethical practice
The responsibility for ethical behaviour and practice lies entirely with the exercise professional. The client could be vulnerable and susceptible to the influence of those who offer help. All actions and behaviours should aim to empower clients.
Koocher and Keith-Spiegel (1998) use the following principles to guide ethics in psychology; these apply equally to other professions:
1. Professional action must bring no harm to clients.
2. Clients have the right to choose their own direction.
3. Be faithful to clients, the profession, the employing organisations and ultimately to yourself.
4. Be just and fair to all clients, thereby ensuring non-discriminatory professional actions.
5. Be of benefit to clients by promoting their welfare.
6. Treat all clients with dignity and respect.
7. Be fully accountable to clients.
8. Maintain clear and unwavering professional boundaries.
ACTI
VIT
Y Use your notebook to list the ways in which you could apply the principles in your work (give examples).
Visit the REPs website and look at the code of conduct. Make a note of the ways in which you can apply these guidelines to your work.
Examples of how fitness instructors can comply with legislation and industry codes of conduct include:
• Respecting individual difference and diversity.
• Challenging discrimination and unfairness.
• Dealing with client information confidentially.
• Promoting inclusion, rather than exclusion (unless exclusion is required on medical grounds, e.g. exercise contraindications).
• Adapting communication to accommodate clients’ specific needs.
• Tailoring programmes to accommodate different clients’ needs and abilities (e.g. alternative exercises).
End of section: Learning check Answer the questions and make notes to revise this section.
• Why is it important to form effective working relationships with clients?
• How would you form effective working relationships with your clients?
• Why is it important to present yourself in a positive light to clients?
• Why is it important to present the organisation in a positive light?
• How would you use these communication skills to help and motivate clients to become more active?
• Active listening.• Observation.
• Empathy. • Verbal encouragement.
• Non-verbal encouragement.
• What do the terms ‘equality’ and ‘diversity’ mean?
• Why is it important to value equality and diversity when working with clients?
• Where would you source information on professional codes of conduct for the fitness industry?
• How would you ensure your methods of practice respect equality and diversity?
72 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Forming effective working relationships with clients

Section 2: Addressing barriers to exercise and physical activity
Increasing activity levels is a process of acquiring new behaviours and giving up old habits of inactivity.
To ensure a degree of reasonably regular participation, experiences of activity and exercise need to be rewarding and positive; they must provide a sense of satisfaction and success.
There will always be issues that can prevent people from being active. The role of the instructor is to help people to identify and work through these barriers, so that they can make positive changes.
Typical barriers to exercise and physical activityBarriers to physical activity can manifest themselves in a number of forms.
Barriers can be:
Intrinsic - something the person perceives as a barrier, e.g. a belief or attitude.
Extrinsic - something that constitutes an actual barrier, e.g. an exercise contraindication.
1 PHYSICAL e.g. an injury or illness.
PSYCHOLOGICAL e.g. an attitude, belief or state of mind.
SOCIAL e.g. something in the environment, such as transport or availability of services.
2
3
Finding ways to remove or overcome the barrier can often incite the motivation needed to make changes.
All barriers – real or perceived – tend to fall within one of three categories:
Copyright © 2014 Active IQ Ltd. Not for resale | 73
Section 2: Addressing barriers to exercise and physical activitySU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

TYPE OF BARRIER
BARRIER STRATEGY
Physical Lack of fitness. Plan a programme that is appropriate for their starting level of fitness and progress steadily.Build activity into their daily lifestyle (e.g. walking and moving more) before they embark on the programme.
Injury, illness or medical condition.
Ensure the client has medical clearance prior to exercise. Signpost them to a specialist instructor if necessary (exercise referral).
Psychological Self-conscious or embarrassed to use a gym or studio.
Provide a home activity programme that is appropriate to their level of fitness.Discuss times when the studio or gym is less busy. Suggest attending with a friend or family member.Offer newcomer and induction sessions for groups of clients who have similar fears.
Previous failure (e.g. dropping out).
Explore their reasons for dropping out. Explore their activity preferences; look for things they like and enjoy.
Struggling to motivate themselves.
Work with an instructor or personal trainer. Attend with their family or friends. Establish a training partner and buddy system.
Dislike exercise. Explore activities they like and find ways of making them more active, e.g. gardening, walking or playing a sport.
Social Lack of time. Build activity into everyday life, e.g. take the stairs instead of the lift, do exercises at home and take short journeys on foot or by bicycle.
No transport or local services available.
Go for a walk in the park; gym and studio activities are not the only ways of improving fitness.
Can’t afford gym membership.
Plan activities for daily living. Offer off-peak membership or reduced rates at quiet times.
Table 2.1 Barriers to activity with example strategies
“I’M TOO OLD.”
“I’M TOO UNFIT.”
“I’M NOT ‘SPORTY.’”“I DON’T LIKE
EXERCISE.”
“I DON’T HAVE THE ENERGY.”
“I DON’T HAVE TIME.”
“I MIGHT EMBARRASS MYSELF.”
“I MIGHT INJURE MYSELF.”
74 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Addressing barriers to exercise and physical activity

Helping clients overcome typical barriers The first steps to help clients overcome their barriers for engaging in physical activity are to help them:
• Identify their barriers - the things that stop them being active and the reasons they give for not being active.
• Explore their motivations - their reasons for wanting to make changes and be more active.
This is where the client is the expert; they know all the reasons that stop them from doing something. The role of the instructor is to facilitate a conversation and explore these reasons. This is the essence of the helping method: motivational interviewing.
The next step, which should not be hurried until the client is ready (ONCE they have fully explored the why and why not for making changes) is to explore how they could make the changes. This is when the instructor has the expertise, they will know different ways of improving fitness and being active and should be able to discuss lots of possibilities with the client, rather than prescribing one type of programme.
The decision balance sheetThe decision balance sheet (figure 2.1) can be used with individuals when they are considering making changes. It requires the individual to sit down and consider all the gains they will receive from starting a programme of exercise and also any losses they may experience. Hopefully, the gains will vastly outweigh the losses and provide the impetus to start exercise and continue the programme. The decision balance sheet could be displayed in a prominent place in the home and serve as a continual motivating factor, especially in times of weakness or uncertainty.
TRAINER TIPBARRIERS are the reasons people give as to why they can’t do something.
MOTIVATION describes the reasons people give for doing or wanting to do something.
Clients use both types of language when they speak.
The key is to facilitate the conversation so that they focus on motivational language and talk themselves into making a change. This is the essence of motivational interviewing.
DISADVANTAGES OF MAKING THE
CHANGE
DISADVANTAGES OF NOT MAKING
THE CHANGE
BENEFITS OF NOT MAKING THE CHANGE
BENEFITS OF MAKING THE CHANGE
Figure 2.1 Decision balance sheet
ACTI
VIT
Y Think about something you may like to change and complete the decisional balance sheet to explore the advantages and disadvantages for this change.
Copyright © 2014 Active IQ Ltd. Not for resale | 75
Section 2: Addressing barriers to exercise and physical activitySU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

The importance of incorporating clients’ exercise and physical activity preferences into their programme Incorporating clients’ exercise and physical activity preferences into their programme can strengthen their motivation and commitment.
It is important to select and plan activities that clients enjoy; that they find fun and pleasurable and that help them to relieve stress. This promotes commitment and motivation by allowing for positive associations with exercise.
It is best to avoid asking a client to do something they don’t like because this reinforces negative associations.
Too many negative thoughts and feelings in an exercise programme ultimately lower motivation levels; this can hamper participation and commitment. It can also lead to relapse and a return to old habits.
End of section: Learning check Answer the questions and make notes to revise this section.
• List some of the barriers to activity and exercise that clients can experience.
• Physical. • Psychological. • Social.
• Think of a strategy to overcome each barrier.
• Give examples of incentives and rewards that could be used to strengthen a client’s motivation.
• Why might it be useful to incorporate activities the client enjoys into their programme?
• Why might it be counterproductive to programme activities the client doesn’t enjoy?
Incentives and rewards that can strengthen clients’ motivation and adherenceIncentives and rewards can be a valuable way of strengthening a client’s motivation and commitment.
Incentives can include:• A free t-shirt or water bottle with membership.• A free training session for every ten sessions booked. • Special deals for introducing friends, e.g. a complimentary training
session.
Rewards can include:• Praise and encouragement, reinforcing what the client has achieved. • A free gift after a specific period of attendance or achievement of a
target or goal.• Displaying the top ten attendances on an organisation’s noticeboard
or newsletter.
This system of positive reinforcement is valuable because it shows people that their efforts have been recognised and rewarded.
NB: Any system of rewards or incentives should be applied with discretion, as some could introduce competition, which may lead to counterproductive overtraining.
VARIETY Giving clients the opportunity to experience new activities or try different training methods can be a powerful incentive. For example: “you managed this really well today, how about we try some stability exercises with equipment next week?”Varying the activities and types of exercise make a programme more interesting and allow the client to try activities that they might enjoy; these are all helpful for motivation and adherence. Changing variables (such as intensity, duration andfrequency) enables progressionand this, in itself, can be amotivator. Examples include walking for longer or at a faster pace; increasing the number of repetitions of an exercise and attempting to hold a balancing posture (e.g. a yoga position) for longer.
76 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Addressing barriers to exercise and physical activity

Section 3: Supporting clients in their adherence to exercise and physical activity
Getting people to start exercising is often easier than motivating them to continue. It is widely known that exercise is good for our health. Many New Year’s resolutions involve health and fitness-related targets, such as losing weight, getting fit, running long distances or joining the gym. Similarly, the arrival of spring and summer and events, such as summer holidays, weddings and parties, can also help to initiate momentum for making changes. When joining a health club, the attractive environment, coupled with the opportunity to enjoy the facilities and mix with people, can spur a client’s initial motivation.
Other factors that can trigger a desire for change include:
• Persuasion and advice from a trusted source, e.g. a doctor.
• Observation of changes in others, e.g. fat loss or increased energy levels.
• Physiological feedback, e.g. clothes feeling tight.
• Feedback from others (direct or indirect), e.g. overheard remarks or directed statements.
However, the initial enthusiasm and enjoyment tend to wear off, leaving the person to face the simple facts that exercise can be uncomfortable, and requires effort and commitment.
A key aspect of the exercise professional’s role is to find ways of helping people to maintain their motivation and stick to their exercise programme.
The importance of clients taking personal responsibility for their fitness and motivationTo sustain any long-term commitment and adherence to exercise, it is important for the client to take personal responsibility for their own fitness and motivation. Taking responsibility increases the likelihood of independence and commitment to the strategies implemented for reaching fitness goals. Relying solely on other people, such as instructors or doctors, can encourage the client to blame other people for a lack of results. They might also become overly reliant on other people to do the work for them; this can leave them unable to do anything about their health and fitness without the presence of the person on whom they have become dependent.
Taking personal responsibility requires you to be actively involved in goal-setting, exercise choices, commitment to attend, monitoring of progress and changes and overcoming the desire to revert to old behaviours. It also means making some sacrifices. For example, in order to be more active, the desire to be inactive has to be minimised. These responsibilities require a high level of self-determination and a shift in attitude towards wanting to do or achieve something for its own sake, and for personal intrinsic fulfilment, rather than external reward.
AIDE MEMOIRE The term ‘adherence’ can be explained by comparing it with the term ‘adhesive.’ An adhesive is used to ‘stick’ something together.
Adherence means sticking to an exercise programme.
Copyright © 2014 Active IQ Ltd. Not for resale | 77
Section 3: Supporting clients in their adherence to exercise and physical activitySU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

Reasons for exercisingKnowing why a person wants to be more active and exercise more often can help to identify their level of self-determination (how much they want something). It can also help to develop strategies that promote motivation and adherence.
ENJOYMENT One of the main motivators for regular, sustained participation in any sport or exercise is enjoyment. If the person is used to an inactive or sedentary lifestyle, this enjoyment might be compromised. However, as their level of fitness improves – especially if they get to try different types of activity – exercise can become increasingly enjoyable and rewarding.
HEALTH People are becoming much more aware of the benefits of health-related exercise as a way of preventing illnesses, such as heart disease, hypertension and stress-related diseases. They might decide to embark on an active exercise programme to improve their health, especially if it has been recommended by their doctor or specialist, following medical examination or illness.
APPEARANCE AND WEIGHT CONTROL
The largest proportion of people joining health clubs or attending exercise sessions is probably made up by those aiming to enhance their appearance by improving their body composition, general muscle tone and posture.
SOCIAL AND FASHION STATUS
A significant number of people take up exercise because others are doing so. Membership of a particular health club can be a status symbol; alternatively, people might simply enjoy the social aspect of group exercise. People who participate for these reasons should ideally continue exercising because they enjoy the activities.
REHABILITATION A programme may be started following illness or injury, when the need for rehabilitation requires exercise participation.
GENERAL FITNESS Some people take up exercise for general fitness goals; they might want to improve their cardiovascular fitness, muscular tone, endurance or strength, or lose body fat.
GENERAL WELLBEING
Sometimes, people feel lethargic, moody and mentally drained before the day has even begun. They might try to improve their general sense of wellbeing by joining a fitness facility to increase their activity levels.
SPORT-SPECIFIC FITNESS
Anyone taking up a new sport or returning to a sport after a long absence might wish to start a fitness programme before competing. It needs to be specific in its objectives, in order to prepare them physically for the demands of the sporting activity and improve their levels of performance.
78 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Supporting clients in their adherence to exercise and physical activity

Helping clients develop their own strategies for motivation and commitmentThere is no single approach for helping clients to develop their own strategies for motivation and commitment. Different clients have different needs; these include their stages of readiness to make changes.
Strategies for building motivation
There is a range of strategies that can be used to assist clients in their motivation and adherence:
INFORMATION LEAFLETS
Can be useful for clients who are not considering change, but could benefit from making an informed choice about their behaviour. Leaflets can be provided to explain the health benefits of activity and exercise.
With the aim of understanding the client, is essential for working with those who are considering change. Active listening can help to explore their motivations and barriers and where they are in the process of making changes. Most people, at some level of consciousness, know the solutions to their barriers or problems. The aim is to:
• Give them space to explore their barriers and motivations openly and without judgement.
• Build and facilitate their personal desire to make the changes – incite them to genuinely want to be more active.
Is a useful tool for clients who are considering becoming more active. It can help them to explore and weigh up the benefits and disadvantages of making changes.
Can be used with a client to assess how ready they feel to make a proposed change (their motivation). The person can explore the grading they give to themselves to identify any additional barriers.
1 = Not ready 10 = Very ready
Figure 3.1 Psychological readiness scale
Can be used or discussed with clients who have made the decision to increase their activity levels. SMART goals can be negotiated and agreed as targets to work towards or achieve. Attaining goals can generate a feeling of success, which can help to build and maintain motivation.
Keeping a training log can be a useful activity for clients who are making changes to their activity and exercise behaviour. Maintaining a record shows them how they are improving and how their efforts and commitment have paid off. It can be very satisfying for them to review the sessions they have completed and the progress they have made.
Are ways of treating clients. Rewards can be offered or bought by the client to reward themselves after achieving a target. Rewards can also include verbal praise and encouragement; telling clients what they do well and highlighting their achievements.
ACTIVE LISTENING
A DECISION BALANCE SHEET
PSYCHOLOGICAL READINESS SCALE
10987654321
GOAL-SETTING
TRAINING DIARIES OR JOURNALS
REWARDS AND INCENTIVES
Copyright © 2014 Active IQ Ltd. Not for resale | 79
Section 3: Supporting clients in their adherence to exercise and physical activitySU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

Affirmations are the beliefs a person holds about themselves. A positive attitude and self-perception brings more benefits and builds far more motivation than a negative attitude.
Examples of positive affirmations are:
“I have the power to make positive changes.”
“I enjoy exercise.”
“I deserve to have good health.”
“I take good care of my body.”
“I feel positive and energetic.”
“My actions are making a difference.”
The aim is for clients to become mindful of any negative thinking patterns and attitudes and when they arise, so that they can challenge their thinking and rebalance their thoughts with positive, self-enhancing thought patterns.
Such as family, friends or training buddies can help to boost motivation and offer encouragement. A common reason for giving up on exercise programmes is a feeling that no one will notice or care; the aim of a social support network is to give the client the necessary support. A broad support network is vital for people who are not receiving positive encouragement at home.
Group training (small personal training groups or larger group exercise sessions) is a very effective method for encouraging commitment. The social aspect of training promotes enjoyment and increases the level of commitment among clients who do not want to let down their peers.
It is useful for clients to have some strategies in place for the times when they don’t feel like attending or need to miss a session – especially if they then find it hard to get back into their routine. It is also useful to have strategies for times when a client relapses to their previous inactive behaviour or gives up. Commonly cited reasons for giving up on programmes include:
• Boredom.
• Lack of fitness gains or improvements.
• Poor instruction or lack of support.
• Lack of time.
• Expense.
• Lack of motivation.
Positive affirmations can help to ensure that the client doesn’t become too self-critical.
Active listening can help the client to explore the reasons for their relapse.
Establishing a goal (e.g. attend on Tuesday) can help them to take steps to return to action. Incentives can also help them to resume physical activity.
POSITIVE AFFIRMATIONS
SOCIAL SUPPORT NETWORKS
LAPSE OR RELAPSE PREVENTION STRATEGIES
80 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Supporting clients in their adherence to exercise and physical activity

Behaviour change approaches and strategies that can encourage adherence to exercise and physical activities
The trans-theoretical model (TTM)
The trans-theoretical model (TTM) evolved from the work of Prochaska and Diclemente (1983). The model suggests that people go through different stages of readiness and processes before partaking in exercise.
Figure 3.2 The trans-theoretical model of change
Stages of change
It is important to be aware of the different stages and to develop strategies that facilitate the client’s progress throughout each step.
The role of the instructor is to:
• Identify where the client falls within the change cycle (their psychological readiness).
• Provide support for their processes by using appropriate cognitive (thinking) or behavioural (action) strategies.
Risk of relapse or lapse
Risk of relapse or lapse
PRE-CONTEMPLATION (Not considering making
a change)
TERMINATION (Permanent change made)
Risk of relapse or lapse MAINTENANCE
(Change has been continued for longer than six months)
ACTION(Change has started and been sustained for up to six months)
CONTEMPLATION (Considering change within the next six months)
PREPARATION (Getting ready to make some changes)
Copyright © 2014 Active IQ Ltd. Not for resale | 81
Section 3: Supporting clients in their adherence to exercise and physical activitySU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

Pre-contemplationAt this stage clients are inactive and have no serious intention of starting an exercise programme. It requires the instructor to develop an interest by ensuring information is readily available. This information should use clear, simple messages and easily comprehensible language. The instructor should also educate the client, offer incentives and banish any myths and preconceptions. It is their responsibility to be a suitable role model and offer instructions on the next move.
ContemplationAt this stage the client is still inactive but intent on starting an exercise programme within six months. At this point, the instructor provides realistic goals, a choice of enjoyable activities, flexible activity packages and short-term ideas for stimulating interest and uptake.
PreparationDuring this stage clients are planning to make specific changes or experimenting with small changes. It is the point at which they’re ready for change.
ActionThis stage is the most important in terms of offering feedback and support, as it tends to be the most difficult time. Clients start to see and feel changes in their body and health but may reach a plateau and need motivation to carry on.
Maintenance and relapseThis stage requires motivation, support, goal reinforcement and monitoring; it is the most unstable stage, as motivation can be difficult to maintain at the required levels. The instructor might wish to encourage the use of fitness diaries to ensure adherence.
RelapseAt this point the instructor would need to redefine goals and offer more support than before to prevent relapse or to redirect clients who have relapsed back to the ‘action’ stage.
KEY POINTThe trans-theoretical model is a cyclical process; clients may move forwards or backwards (lapse) through the cycle, or even leave it (relapse). A person might need to travel through the stages of the cycle a number of times before permanent behavioural changes are achieved.
82 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Supporting clients in their adherence to exercise and physical activity

Strategies for supporting change
The strategies that can be used to help the client make changes involve:
In the early and contemplative stages the focus is on cognitive strategies and reframing clients’ thinking – increasing their motivation to exercise and be more active.
This process can incite the client to explore the reasons why they think they should exercise and be more active (their ‘motivation to change’ talk).
Once the client has decided to make a change and become more active, the focus shifts to behavioural and action strategies, such as goal-setting and how they can achieve them. This process includes cognitive strategies for supporting the change, such as discussing possible ways in which they could achieve their goal and how they can make it happen (their change and action talk).
STAGE ATTITUDE INTERVENTION
Pre-contemplation
Denial of need to change. Resistant. “I don’t like exercise.” “I don’t need to exercise.”
• Facilitate conversation.• Use active listening skills. • Provide information hand-outs on the benefits of exercise
and ways of increasing activity levels.
Contemplation Considering making changes.Managing internal conflicts of barriers against motivations. “I know I need to start exercising.”
• Facilitate conversation. • Use active listening skills. • Explore the client’s motivations and barriers to get a
decision balance.
Preparation Small changes have been made. “I have joined the gym.”
• Use active listening skills. • Offer praise and encouragement for small changes. • Implement goal-setting. • Explore additional support systems. • Explore rewards and incentives. • Explore relapse prevention strategies.
Action Changes have been made (one day to six months).“I attended my first session.”
• Use active listening skills. • Offer praise and encouragement for changes. • Review goals. • Explore other possible rewards and incentives. • Explore relapse prevention strategies.
Maintenance Changes sustained for more than six months.Some coping strategies are in place. “I’m active on most days now.”
• Use active listening skills. • Offer praise and encouragement for changes. • Review goals. • Build the client’s confidence. • Highlight successes.• Discuss triggers for relapse. • Increase strategies to prevent relapse.
Relapse Return to previous behaviour.“I haven’t been able to get back into my programme since I got back from holiday.’’
• Facilitate conversation. • Use active listening skills. • Explore causes and triggers. • Be empathetic and non-judgemental.• Reframe the situation as an opportunity to learn rather
than a failure.• Discuss re-planning. • Offer support to manage the upset; use empathetic
listening and reflect any positive changes made.• Provide a review and action plan.
(Lawrence & Bolitho, 2011)
Table 3.1 Stages of change and interventions
Reframing their thinking (cognitive strategies).
Taking action (behavioural strategies).
Copyright © 2014 Active IQ Ltd. Not for resale | 83
Section 3: Supporting clients in their adherence to exercise and physical activitySU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

It is important to set goals in the interests of:
• Persistence; goals can help the client to continue a task over time and keep their objectives in mind.
• Attention; goals help to keep a client directed to the important aspects of their programme.
• Effort; goals help to mobilise and direct the intensity of effort towards a specific task or outcome.
• Strategies; goals can help clients to develop new approaches for achieving their desired outcomes.
The reasons why people might not set goals could be that:
• They don’t understand the importance or value of goal-setting.
• They don’t know how to set goals effectively.
• They fear failure to achieve goals.
• They don’t know what they want to achieve.
How to set, review and revise short-, medium- and long-term SMART goals
The purpose of goal-setting
Goal-setting can be used as a strategy to enhance motivation and commitment.
KEY POINTA goal is what an individual is trying to achieve. It is the object or aim of an action.
Goals can be short-, medium- or long-term.
Types of goal
Goal-setting can be used in different areas of life, as well as aspects of health, wellbeing and personal growth. The main categories of goals are:
• Personal goals, which relate to personal life, such as family, social commitments, relationships, sporting aims, health and fitness objectives and pursuits we enjoy.
• Business, career and economic goals, which relate to the development of a career or working role and the necessary financial rewards.
• Self-improvement goals, which relate to aspects of personal growth and development.
• Outcome goals, which focus on the outcome of an event or situation, such as winning a race or beating an opponent. Achieving an outcome goal depends on individual effort and the opponent’s ability and performance.
• Performance goals, which focus on making comparisons with one’s own performance; they differ from outcome goals because they are within the athlete’s control.
• Process goals, which focus on the process or actions that a person must take in order to perform well; this could be emphasising a particular technique or the components within it.
Short-, medium- and long-term goals
Goals must be set for short-, medium- and long-term timeframes. It is important to set short-, medium- and long-term goals because the fulfilment of short-term goals ultimately contributes to the achievement of longer-term objectives.
GOAL CATEGORIES
Short-term goals
These goals are set over a period of one day to one month. A short-term goal can relate to something the client aims to achieve in one session, or within a one-month timeframe.
Medium-term goals
These are goals set over a period of one to six months; one-month and three-month goals are the most common.
Long-term goals
These goals relate to timeframes that range from six months to several years. People might set ‘lifetime goals’ which cannot be assessed until retirement. Most long-term goals in sport are set for achievement over the course of a year or competitive season.
Table 3.2 Goal categories84 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Supporting clients in their adherence to exercise and physical activity

SAY WHAT YOU WANT, NOT WHAT YOU WANT TO AVOID.This means using positive language to state the goal, which helps to put the client in the right emotional state to achieve it. As an example, “I will avoid gaining body fat” should be replaced by: “I will improve my body fat percentage.”
1
MAKE GOALS CHALLENGING BUT REALISTIC.This means setting achievable goals; setting a goal too high can cause stress, due to fear of failure or overtraining in an attempt to improve performance. In turn, goals that are too easy hamper motivation.
2
INFLUENCE THE RESULT DIRECTLY.This means that the goal must be under the person’s control and not reliant on the actions of other people. The goal should always start with “I” and be in the present tense; a goal such as “I will win this race” is not always appropriate because it relies on the performance of the other competitors – aiming for a specific race time would be better.
3
MEASURE PROGRESS.Goals should always have a deadline with a specific date or timeframe, e.g. a number of weeks or months. Goals should be a combination of short-, medium- and long-term objectives.It is important to be able to measure goals in numerical terms, e.g. “I want to get stronger” is not as good as “I want to improve my bench press by 25%” ; this makes it clear whether the goal has been reached or not.
4
Principles of goal-setting
There are seven principles that must be considered to make goals realistic, achievable and motivating (O’Connor, 2001):
CHECK RESOURCES.Identify what types of help are available for achieving the goal. This could involve people who have an interest in the achievement of the goal, such as a coach, team mate, friend, family member or partner. Resources can include facilities, books and equipment.
5
COUNT THE COST.What will be the cost of working towards the goal? This doesn’t just involve money, but expenditure of time and loss of social opportunities.
6
PROVIDE REWARDS.Goal achievement should be congratulated and recognised with an appropriate reward. Do not give rewards that involve indulging in previous bad habits!
7 Copyright © 2014 Active IQ Ltd. Not for resale | 85
Section 3: Supporting clients in their adherence to exercise and physical activitySU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

Specific means that goals must relate to particular actions: something the client is going to do, e.g. walk to the park, go to the gym or attend a class.
It can also relate to specific aspects of fitness. It is not enough to want to get fitter; the goal must be specific and state whether the aim involves aerobic fitness, flexibility, core stability, balance, fat loss, muscle development or another aspect of fitness.
Measurable means that goals must be quantifiable: they should be stated in measurable figures. As an example, “I want to walk more” is not measurable, whereas an aim to walk for 30 minutes, on two days next week is measurable. “I want to lose weight” is not measurable, but statements such as “I want to reduce body fat by 3%” or “I want to fit into 32-inch waist jeans” are measurable.
Achievable means that the targets need to be humanly possible for the person. It is important to take into account both the intrinsic and external factors that may affect success (e.g. barriers and motivation).
Goals should be moderately difficult but realistically achievable. If goal-setting is not done carefully it could be demotivating; if goals are too hard to achieve or the timescale is too long, motivation will be lost because the client might be put off and not make the necessary changes.
Over-ambitious goals can place a lot of stress on a person as they seek to achieve them; goals that are too easy won’t achieve the desired effect because they can cause the client to resume previous behaviours after they have been achieved.
T
S SPECIFIC
MEASURABLE
ACHIEVABLE
REALISTIC AND RELEVANT
TIME-BOUND
M
A
R
SMART formula
When setting goals, it is useful to use the acronym, SMART, to ensure that they’re:
86 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Supporting clients in their adherence to exercise and physical activity

Realistic and relevant mean that the goal should fit with the client’s values, wants and needs. Goals must be devised and agreed by the instructor and client, not dictated or enforced.
Allow for client input in the development of goals. Lots of psychological theories state that people do not respond well to imposed restrictions or bombardment with commands or instructions. Clients are more likely to feel committed to their goals if they have contributed towards making them; this approach helps them to develop their own strategies for motivation and adherence.
Time-bound means that there must be a timescale to accompany the goal, so that the client can measure their success with a clear deadline or target. An example would be improving their aerobic capacity by 10% in three months.
An effective goal would take all of the SMART criteria into account. For example, an outcome goal to reduce body fat by 3% in three months is specific to one aspect of fitness, measurable, time-bound and can be achieved if it is something the client wants – it is relevant to their values and needs.
Additional strategies for goal-setting
WRITE GOALS DOWN
All goals must be committed to paper with both the client and the instructor keeping copies for their records. The client should be encouraged to display the goals in a clearly visible place.
The client should be encouraged to visualise how they might look and feel when they have achieved their goal. Linking mental images and emotions to goal achievement makes the process more real and intense.
Goals will only be achieved if there is the determination, persistence and resolve not to give up; these qualities need to be instilled in the client.
All clients experience times of weakness and doubt in their ability to achieve their goals. At these times, they need a support network; this could include the instructor, a friend or a family member.
Bear in mind that changes in behaviour might not always be supported, as they can affect the client’s relationships. For example, if the client decides to stop drinking alcohol this could hamper their social life and cause them to lose contact with friends. Friends might also try to prevent behavioural changes which are not in their interests.
It is useful for the client to record any activities they have undertaken to achieve their goal, with full details of training sessions or food they have eaten. Writing a diary can help clients to be honest with themselves and use visible progression to aid motivation.
Anything that can be done to help the achievement of goals is useful. Putting up pictures of an ideal body image, writing notes to oneself or publishing motivational phrases can all help to keep a person motivated. For example, the client might have a note on the fridge saying ‘think before you eat’ or a note on the bathroom door saying ‘go to the gym today.’ These can only work for a short time because clients can train themselves to ignore them.
USE IMAGERY
HAVE A SUPPORT SYSTEM
KEEP A DIARY
USE REMINDERS
Copyright © 2014 Active IQ Ltd. Not for resale | 87
Section 3: Supporting clients in their adherence to exercise and physical activitySU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

Reviewing goals
Setting and defining goals is of limited value without a follow-up procedure, which evaluates progress and helps the development of future goals.
Reviewing goals on a regular basis serves two very important purposes:
• Accountability: taking time to stop and check progress and achievements can spur on motivation and self-accountability.
• Feedback: a review of goals allows for easy evaluation of how realistic, effective and motivational they were. It helps to clarify which actions worked and which ones did not, and to identify where a change of strategy might be needed.
Figure 3.3 Review timeframes
It is important to set specific dates at the outset for goal review and progress evaluation. Breaking long-term goals down into smaller, manageable time periods helps to motivate the client and allows for regular minor adjustments, which in turn makes achieving the outcome much more likely.
Revising goals
Unless there are major problems with the original goals, it would be expected that the periodic goal reviews would only bring about minor modifications to make them as effective as possible.
Ten years
Five years
One year
Six months
Three months
One month
Two weeks
One week
One day
End of section: Learning checkAnswer the questions and make notes to revise this section.
• Why is it important for a client to take personal responsibility for their own fitness and motivation?
• How can you help clients to develop their own strategies for motivation and commitment?
• What are the different stages of change in the trans-theoretical model (TTM)?
• What approaches or strategies would you use to encourage commitment to exercise or physical activity at each stage of the TTM?
• What is a short-term goal?
• What is a medium-term goal?
• What is a long-term goal?
• What are the components of the SMART formula?
• What are the benefits of setting goals?
• Why might people not set goals?
• How would you review and revise short-, medium- and long-term goals?
88 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Supporting clients in their adherence to exercise and physical activity

Section 4: Providing ongoing customer service to clients
Any person you attend to while working in a professional role can be considered a customer.
• Are people who work for or with an organisation; they include people who rely on the instructor and people on whom the instructor relies for support, information and products. Internal customers include managers, cleaners, receptionists, maintenance staff and healthcare providers.
INTERNAL CUSTOMERS
• Are the people who pay to use services and facilities, e.g. health club members, visitors and guests of members.
EXTERNAL CUSTOMERS
The terms ‘client care’ and ‘customer service’ describe the ability to consistently meet (and, ideally, exceed) customers’ needs, wants and expectations.
The importance of good client careCustomers are vital for every organisation or service in the health and fitness industry. The industry would not survive without customers.
Upholding standards of customer care is essential. It is important for the client, as it allows for an enjoyable experience in the health and fitness environment and encourages long-term involvement in physical activity. It also benefits the organisation by helping to secure repeat business and recommendations.
ADVANTAGES FOR THE CLIENT ADVANTAGES FOR THE ORGANISATION
Provides a positive customer experience. Builds a positive reputation.
Increases their enjoyment and satisfaction. Shows high standards of professional practice.
Ensures that their needs, wants and expectations are met.
Increases the chance of repeat business and returning customers.
Increases the likelihood of them adhering to their programme.
Helps to acquire new customers through recommendation.
Makes them likely to share their experience with friends. Helps the business to flourish and grow.
Makes them likely to continue using the services. Promotes industry sector growth.
Provides a positive, upbeat environment for external customers.
Provides a positive working environment for internal customers.
Table 4.1 The advantages of good client care
KEY POINTClient care is the ability to consistently meet (and, ideally, exceed) customers’ needs, wants and expectations.
Copyright © 2014 Active IQ Ltd. Not for resale | 89
Section 4: Providing ongoing customer service to clientsSU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

Meeting and exceeding customers’ needsCustomers have a wide variety of needs; they might ask questions, need guidance or want information. They expect competent staff and instructors; safe, up-to-date equipment and fast, efficient service.
Meeting clients’ needs is a minimum requirement; it provides a satisfactory experience. Providing an exceptional service requires you to exceed clients’ expectations.
MEETING CLIENT NEEDS
Doing what the client wants or giving them what they
expect.
EXCEEDING CLIENT NEEDS
Giving clients more than they want, doing more than they expect and ‘going the extra
mile.’
Positive relationships and a customer-friendly attitudeThe key to good customer service is forging positive relationships with customers and developing a customer-friendly attitude.
Positive relationships lead to positive experiences and happy customers. Happy customers are more likely to return and spread the word than unhappy ones! Rapport and relationships can be established with customers through the use of effective communication skills – especially active listening and empathy.
First impressions count; simply smiling and addressing someone by name instantly forms a positive connection with lasting impact.
Customers do not care how knowledgeable the instructor is unless the instructor shows them how much they CARE. The acronym CARE (Consideration, Active listening, Responsiveness and Empathy) captures the essence of a customer-friendly attitude.
• Consideration: Always offer to help, don’t make promises unless they can be kept, always be honest about the service provided and consider the customer’s circumstances and feelings.
• Active listening: Listen to the customer and demonstrate an understanding by responding appropriately.
• Responsiveness: Deal with complaints promptly. If a customer asks a question, don’t pass them onto someone else – make the effort to respond in person and introduce compensatory measures for complaints, e.g. a free fitness session or discount. Gestures of goodwill help to maintain positive relationships.
• Empathy: Be non-judgemental and understanding of customers’ needs; view the situation from their perspective.
KEY POINTDeveloping a friendly attitude towards customers comes from an appreciation of how important they are to a business; customers are the reason why businesses exist.
90 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: Providing ongoing customer service to clients

An exercise professional who ‘goes the extra mile’ can make all the difference to the customer experience. Examples include:
• Contacting the client to check on progress with their exercise regime.
• Asking them how they feel the day after a session.
• Asking them about their programme and whether they would like anything reviewed.
• Asking them about their goals and whether they would like some help.
• Finding out information on behalf of the client (where relevant).
• Letting them know about new services or products and offering free trial sessions.
• Getting to know the client and meeting additional needs, e.g. gathering information on stress management, relaxation techniques or mindfulness for a client with stress issues.
• Remembering clients’ birthdays and wishing them happy birthday if they attend on or near the day (some clubs register birthdays for this purpose).
• Asking clients for feedback after a period of membership or use of a service to see how their experience can be improved. This could be in conversation or via a survey.
EXCEEDING CLIENT EXPECTATIONS Under promise and over deliver.
Copyright © 2014 Active IQ Ltd. Not for resale | 91
Section 4: Providing ongoing customer service to clientsSU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

Sources of relevant and appropriate information for meeting clients’ needsMeeting customers’ needs requires you to access certain information. Different clients have different needs and most fitness establishments have documents that answer frequently asked questions and outline the procedures for dealing with complaints.
Resources that detail the procedures, standards and customer service levels expected of an organisation include:
• Normal operating procedures.
• Membership types and packages.
• Health club or gym rules and regulations.
• Health club or gym customer service standards.
• Health and safety regulations.
• REPs code of conduct.
• Studio timetables and class descriptions.
• Booking information, e.g. for swimming lessons, tennis courts, facilities and activities.
• Hair and beauty services, e.g. sunbeds and massages.
• Exercise referral operating standards and procedures.
Other team members can also be relied upon to provide information. Studio instructors, personal trainers, yoga and Pilates teachers and sports massage therapists can all share information about the services they deliver.
Clients who require information outside employees’ areas of expertise should be signposted to relevant information sources.
INFORMATION REQUESTED SOURCE OF INFORMATION
Medical information GP
Diet and weight loss Dietitian
Mental health concerns, e.g. stress, depression or eating disorders
Counsellor or mental health charity
Pregnancy GP or clinic
Alcohol or drugs Alcohol charity, e.g. Drinkaware
Giving up smoking Smoking cessation service
Table 4.2 Sources of information
EXCEEDING CUSTOMER EXPECTATIONS If a customer asks whether a massage service is available, and it isn’t, the instructor could recommend or offer to enquire about availability elsewhere, on the customer’s behalf, instead of merely saying ‘no.’
92 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: Providing ongoing customer service to clients

The importance of handling client complaints positively and following an organisation’s proceduresWhen dealing with customer complaints you must not take them personally or become defensive. Instead, look at a complaint as valuable customer feedback.
How the problem is dealt with can strongly influence how the instructor is perceived and leave a lasting impression on the customer. The client might not just be displeased; they may be upset, confused, disillusioned or angry.
IN THE EVENT OF A COMPLAINT YOU SHOULD:• Listen without interrupting.
• Thank the client for their feedback and for bringing the issue to your attention.
• Take ownership of the complaint.
• Be polite.
• Remain calm and never enter into an argument.
• Follow organisational procedures: record the complaint (fill in a complaint form), acknowledge receipt of it and reassure the customer that it will be resolved.
• Offer a point of contact: advise the client of possible solutions or alternatives; allow them to decide on an appropriate solution and ensure that they are appeased before they leave.
• Inform relevant staff of the problem.
• Communicate with the client and update them on progress.
Dealing with clients’ needs and delays in meeting needs satisfactorily All customer needs and complaints should be dealt with immediately, or as soon as possible. Keeping clients waiting or delaying responses looks lazy and unprofessional.
It is essential to keep the customer up to date on progress when dealing with their needs or complaints.
Maintaining communication links is important, as customers tend to become frustrated if they don’t know what is happening. Keeping them informed shows that the instructor and organisation are dealing with their requirements and not ignoring them.
TRAINER TIP Always check with the client that any need or complaint has been dealt with to their satisfaction. This shows attention and interest and allows for any unresolved issues to be sorted. This attention may exceed their expectations.
Copyright © 2014 Active IQ Ltd. Not for resale | 93
Section 4: Providing ongoing customer service to clientsSU
PP
oR
TIng
CLIEn
TS wH
o TA
kE PA
RT In
ExERC
ISE An
d P
HySIC
AL A
CTIVITy

Dealing with angry customers
Dealing with an angry customer requires practice. The key is to listen; sometimes being heard is all that is needed. Most people can only rant for a short period of time. Active listening allows them to hear themselves and tends to have a calming effect. When listening to angry clients, try to imagine yourself in their position and to see things from their perspective (empathy). Always avoid being confrontational, dismissive or aggressive, although it is important to be assertive. Be mindful of your tone of voice, words and body language.
Compare these examples of aggressive and assertive communication.
AGGRESSIVE LANGUAGE ASSERTIVE LANGUAGE
“Don’t you dare speak to me like that!” “I’d prefer it if you didn’t speak to me in that way.”
“With that attitude, how do you expect to resolve this?” “I can understand your frustration; let’s see what we can do about this.”
“Shut up, or I won’t continue this conversation!” “I won’t be able to continue this conversation if you keep using bad language.”
AGGRESSIVE BODY LANGUAGE ASSERTIVE BODY LANGUAGE
Scowling Open facial expression
Closed posture with the arms folded Open posture
Invading personal space Standing at a respectful distance
Table 4.3 Aggressive and assertive communication
Organisational procedures
All organisations have procedures for dealing with complaints. These need to be followed in order to ensure all complaints are dealt with fairly, consistently and effectively. They must also be dealt with positively, or it could reflect badly on the organisation. Remember that every complaint is an opportunity for services to be improved.
End of section: Learning check Answer the questions and make notes to revise this section.
• Why is customer care important for the client?
• Why is customer care important for the organisation?
• Why is it important to meet clients’ needs?
• Where would you source relevant and appropriate information to meet these client needs?
• Finding information about a medical condition, e.g. high blood pressure or osteoporosis.
• Devising a diet plan to help them lose weight.
• Helping them to stop smoking.
• Addressing concerns about their alcohol intake.
• Helping a client who has just found out that they are pregnant.
• Helping a client who is feeling depressed.
• Why is it important to deal with delays in meeting client needs effectively and in good time?
• Give some examples of how you could exceed customer expectations, where appropriate.
• Why is it important to handle client complaints positively?
• Why is it important to follow the organisation’s procedures for dealing with client complaints?
• What are the procedures for dealing with complaints in the organisation where you work?
94 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: Providing ongoing customer service to clients

AimHealth and safety is of prime importance in every industry. In a fitness environment all staff need to know the organisation’s health and safety policies, risk management strategies and emergency procedures. They should also understand their responsibilities and limitations with regard to duty of care and the welfare interests of themselves, their colleagues and clients, which can include children and vulnerable adults.
Learning outcomesAt the end of this unit you will:
• Understand emergency procedures in a fitness environment.
• Understand health and safety requirements in a fitness environment.
• Understand how to control risks in a fitness environment.
• Understand how to safeguard children and vulnerable adults.
HEALTH, SAFETY AND WELFARE IN A FITNESS ENVIRONMENT

Section 1: Emergency procedures in a fitness environment
KEY POINTRisk assessment and management procedures in the workplace will ensure all hazards are identified and steps are taken to minimise them.
ACTI
VIT
Y 1. Make a list of all the potential hazards in a gym environment and the surrounding area.
2. Make a note of anyone who could be harmed by the hazard.
3. Make a note of the harm that could be caused by the hazard.
4. Assess the likelihood of somebody being harmed by each hazard (low, medium, high or very high).
5. Assess the severity of harm caused by the hazard, i.e. minor injury (low) or potential to kill or maim (very high).
Prevention is the priority for managing emergencies in a fitness environment. Organisations and staff need to be aware of all potential hazards, evaluate the level of risk or harm and aim to eliminate or control them.
There are many potential hazards in a fitness environment. If they are not identified and managed they will increase the risk of accidents and emergencies.
• A hazard is anything that can cause harm, e.g. heavy weights, hot temperatures, chemicals, trailing wires and even electricity.
• A risk is the likelihood of somebody being harmed by the hazard, and the severity of the harm it could cause, e.g. sprains, strains, fainting, burns, falls and electrocution.
Risk assessment and management procedures ensure that all hazards in the workplace are identified and steps are taken to prevent them from causing harm.
96 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Emergency procedures in a fitness environment

MAJO
R INJURY, DISABILITY OR DEATH
INJURY THAT WOULD LAST 3 DAYS O
R MO
RE
MINOR INJURY
CERTAIN TO OCCUR
LIKELY TO OCCUR
POSSIBLE
RISKLIKELIHOOD
SEVERITYOF RISK
HIGH RATING
MEDIUM RATING
LOW RATING
Emergencies in a fitness environmentEmergency situations that can happen in a fitness environment include:
• Accidental injuries caused by unsafe exercise or lifting technique, dropping weights, unsafe spotting practices or falls (possibly on slippery floors), e.g. strains and sprains, cuts and bruises.
• Sudden illness or medical emergencies brought on by existing medical conditions, e.g. fainting, hyperglycaemia, hypoglycaemia and asthma attacks.
• Other large- or small-scale emergencies, e.g. fire, chemical spillage or a bomb alert.
ACCIDENTAL INJURIES SUDDEN ILLNESS OR MEDICAL EMERGENCIES
OTHER EMERGENCIES
Strains and sprains Asthma attack Fire
Cuts, bleeding and bruising Dizziness and fainting Bomb alert
Back injuries Dehydration Chemical spillage
Collisions (contact sports) Loss of consciousness Missing child
Falls (especially older adults) Heart attack or angina Theft
Fractures Hyperglycaemia or hypoglycaemia
Burns
Table 1.1 Types of emergency that can happen in a fitness environment
Some of these emergencies are unlikely to happen and others are highly likely. Some pose a low risk to the person if they occur, while others can be life threatening.
Table 1.2 Rating risk and severity
Copyright © 2014 Active IQ Ltd. Not for resale | 97
Section 1: Emergency procedures in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

The roles of employees and external services in an emergencyAll staff members need to concentrate their efforts towards preventing accidents and emergencies. It is a legal requirement to protect everyone from harm and ensure that everything ‘reasonably practicable’ has been done to keep people safe.
All workplaces should have procedures in place for assessing and managing risks in different environments, e.g. the gym, the swimming pool, the studio, the reception area, and the canteen and kitchen.
All staff play a role in assessing and managing risks and in preventing accidents and emergencies.
The best strategy for risk assessment and management is to have procedures in place for staff to follow in accidents and emergencies.
The actions and requirements of staff should be made clear and appropriate, with training provided according to specific responsibilities, especially for first aiders, fire wardens and health and safety officers.
All staff may be required to help in emergency situations. They might need to:
• Help with evacuations.
• Administer first aid.
• Call the emergency services.
• Log and record all incidents.
During an incident the focus should be on providing the requisite help, while looking after one’s own safety.
KEY POINTEliminate the risk if possible.
Control the risk if it is unavoidable.
98 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Emergency procedures in a fitness environment

INTERNAL SERVICES ROLE
Managers and directors Overall responsibility for health and safety in the workplace:• Ensures all aspects of health and safety are considered.• Implements policies and procedures to protect staff and customers. • Appoints appropriate staff for key roles and duties.
Duty first aider The number of first aiders required depends on the size, needs and assessment findings of the organisation.First aiders:• Provide emergency first aid. • Call the emergency services. • Log accidents in an incident book.
Appointed person All organisations are required to have at least one appointed person who:• Looks after first aid equipment and facilities. • Calls the emergency services. • Provides emergency first aid (if they are sufficiently qualified) in the absence of
first aiders.
Health and safety officer There should be a named person responsible for health and safety in the workplace. Their role is to:• Develop appropriate procedures for managing emergencies and for assessing
and managing risks. • Oversee all health and safety in the workplace. • Provide staff training. • Provide reporting and recording mechanisms. • Plan rehearsals for emergency practice, e.g. fire drills.
Fire warden Manages evacuation of the affected area. Their role is to:• Guide staff and customers to a designated meeting point. • Take registers.• Inform the relevant emergency service of missing people.
All staff • Follow organisation procedures.• Report hazards and risks.• Help with risk management in their work area. • Offer help in emergency situations (within their level of competence).• Contact the emergency services. • Log and record accidents and emergencies. • Ensure their safety at all times.
Table 1.3 Internal staff roles
Emergency services
Emergency services are organisations that ensure public safety by responding to crises and urgent situations. Some agencies only deal with certain types of emergency while others are qualified for a variety of situations. The three main agencies are the police, fire and rescue and ambulance services.
EXTERNAL SERVICES ROLE
Police The police manage incidents relating to theft or anti-social behaviour. They would also need to be contacted for a bomb alert.
Fire and rescue The fire and rescue service manage fires and chemical spillages.
Ambulance Paramedics deal with medical incidents and accidents.
Table 1.4 External staff roles
Copyright © 2014 Active IQ Ltd. Not for resale | 99
Section 1: Emergency procedures in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

Following emergency procedures calmly and correctlyWhen dealing with an emergency it is important to stay calm and follow the organisation’s procedure for managing the situation.
The priorities are:
• To ensure all actions are in line with relevant legislation (e.g. health and safety at work) and the best possible working practices.
• To ensure the situation is managed correctly.
• To maintain the safety of everyone involved, including yourself.
• To prevent any further danger or harm to the casualty, or to anyone else who could be affected.
• To minimise the potential for panic and confusion.
• To promote the recovery of any casualties (in medical emergencies).
• To resolve the situation as quickly as possible.
Maintaining the safety of people involved in emergencies In addition to having emergency procedures in place, organisations are expected to train the relevant staff to manage certain situations. The purpose of this is to ensure staff acquire the requisite knowledge and skills for managing people’s safety in different emergencies.
Training can include:
• First aid at work (appointed person).
• Health and safety at work.
• CPR and defibrillation.
• Evacuation.
• Control of Substances Hazardous to Health (COSHH).
• Manual handling.
• Fire marshalling.
• Reporting of Injuries, Diseases and Dangerous Occurrences Regulations, 1995 (RIDDOR).
100 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Emergency procedures in a fitness environment

C
A
L
M
Managing accidents and sudden illness emergencies
The effects of an accident (e.g. fall and fracture) or sudden illness (e.g. asthma attack) can cause the body’s functioning and structure to change. It is important to remain calm, recognise signs and symptoms, call the emergency services (if required), care for the casualty (with first aid) and yourself and deal with the aftermath. Some emergency situations can be traumatic and compel you to seek therapeutic help (e.g. a counsellor).
The ‘CALM’ acronym summarises the steps to follow in accidents and medical emergencies:
Non-emergency injuries (such as minor strains, sprains, cuts and bruises) can usually be dealt with by a qualified first aider.
Calm yourself.
Assess the situation (what happened and how).
Locate assistance, if available (first aider or emergency services).
Make the area safe (e.g. remove bystanders).
Copyright © 2014 Active IQ Ltd. Not for resale | 101
Section 1: Emergency procedures in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

KEY POINTTo contact the emergency services dial 999 or 112.
First aid box
The contents of a first aid box need to be assessed according to the needs of the specific environment. The minimum contents suggested by the Health and Safety Executive (HSE) for low-hazard environments are:
• One guidance leaflet, e.g. HSE basic first aid advice.
• 20 individually wrapped sterile adhesive dressings of various sizes.
• Two sterile eye pads.
• Four individually wrapped triangular bandages (sterile).
• Six safety pins.
• Six medium-sized and two large individually wrapped, sterile wound dressings.
• Three pairs of disposable gloves.
For further information on the content of workplace first aid kits, refer to British Standard BS 8599 (a link is available on the HSE website).
When to contact emergency services
Some situations require the emergency services to be contacted, for example:
• An unconscious casualty.
• Suspected head, neck or spine injury.
• Suspected fractures or severe dislocations.
• Severe external bleeding.
• Suspected internal injuries.
• Serious medical problems, such as heart attacks, asthma and diabetic emergencies.
• Any worsening condition or situation you feel unable to handle.
When contacting the emergency services you need to provide certain information.
CONTACTING THE EMERGENCY SERVICES
Location Telephone number, district and guiding landmarks.Incident Description of the accident.Other services required Police or fire brigade, for example.Number of casualties Number of people, sexes and ages.Extent of injuries Description and seriousness of injury or condition.Location Repeat of location description.
Table 1.5 Information provided to emergency services102 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Emergency procedures in a fitness environment

RECORDING ACCIDENTSIt is usually the first aider or appointed person who records all accidents.
• If you discover a fire operate the nearest fire alarm or, if no alarm is provided, shout ‘fire!’
• If you hear a fire alarm, leave the building via the nearest available escape route and go to your assembly area. Lifts must not be used.
• If you are an appointed fire warden, follow organisational procedures. • Contact the emergency services as soon as possible.• If there are any casualties, send for the nearest available first aider and contact
the relevant emergency services if necessary.
AC
TIO
NS
TO T
AK
EIN
TH
E E
VEN
T O
FA
FIR
E
Recording accidents
When an accident has been managed it is important to record the information accurately. Records need to include:
• The date, time and place of the incident.
• The name and job of the casualty.
• Details of the injury or illness and the first aid provided.
• Details of the aftermath (e.g. the person went back to work, was sent home or was taken to hospital).
• The name and signature of the person (first aider) dealing with the incident.
Managing other emergency situationsIt is crucial that you follow the procedures set by the organisation because employees can be held responsible for harm caused in the work environment if certain actions are not taken. Procedures provide focus and clarity for dealing with emergencies; they are put together by qualified professionals to provide the ideal course of action.
Fires
Organisational procedures for fire management should cover:
• Appointment of appropriately trained fire wardens.
• Location plans of fire hoses, extinguishers and water sources.
• Access for emergency services.
• Provision of firewater lagoons.
• Area evacuations.
• Assembly points.
• Appointment of responsible people for evacuating designated areas, taking registers to identify missing people and notifying the central emergency services of any absentees. This is usually the role of the health and safety officer or fire wardens.
Copyright © 2014 Active IQ Ltd. Not for resale | 103
Section 1: Emergency procedures in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

Chemical or toxic spillage
The emergency spill control procedure should include:
• Identification of all hazardous substances.
• Identification of alternative substances for risk reduction.
• Other measures taken to control risk (e.g. reduce exposure and use protective clothing).
In the event of a spillage:
• Prevent the spread of any hazardous material; this could require the use of sand bags, dry sand, earth, proprietary booms or absorbent pads.
• If possible the material should be rendered safe by being treated with appropriate chemicals.
• Fine, dusty materials should be cleared by vacuum cleaners rather than dry brushing.
• Any treated material should be absorbed onto inert carrier material so it can be cleared up, removed to a safe place and completely disposed of or neutralised.
• Waste should not be allowed to accumulate; regular and frequent waste removal procedures should be in place.
• Evacuation areas, assembly points and toxic gas shelters should be provided (where appropriate).
Ensuring the safety of children, disabled people and older adultsAll organisations have specific plans and procedures in place to maintain the safety of vulnerable groups, such as children, disabled people and older adults, in emergency situations.
Maintaining the safety of children
In emergency situations, changes and even regressions in children’s behaviour are commonplace. Preparation for emergencies can manage and minimise these, e.g. rehearsing emergency procedures and using age-appropriate tasks to explain what to do in an emergency.
It is also important to remain calm and positive, as this will influence the children’s behaviour. Encourage them to be dependent on an adult, explain what is happening and provide direct, short and truthful answers to any questions they ask.
Listen to children’s feelings; these can be expressed in different ways and should not be trivialised or met with an anxious response. To ensure safe evacuation, it is essential that appropriate staff-to-child ratios are considered.
AGE OF CHILDREN RATIO OF CHILDREN TO ADULTS
4 to 8 years 6:19 to 12 years 8:113 to 18 years 10:1
Table 1.6 Child-to-adult ratios for different age groups
104 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Emergency procedures in a fitness environment

Maintaining the safety of disabled people and older adults
Safety procedures for disabled people and older adults depend on the needs of the individual and the extent of their vulnerability. These needs could be:
• Blindness or partial sight.
• Deafness or partial hearing.
• Physical disability or mobility issues, e.g. needing a wheelchair or walking aid.
• Medical condition, e.g. chronic obstructive pulmonary disease or panic attacks.
• Learning disability, e.g. Down’s syndrome.
Evacuation plans
When planning for emergency evacuations it is important to consider:
• Preparing evacuation procedures without reliance on emergency services.
• The characteristics of the building and evacuation routes from different locations.
• The equipment required to assist disabled people and how it should be checked and maintained.
• The rules to follow in an evacuation (these need to be clear for disabled people and all staff involved in the evacuation process).
• The number of disabled people and their location in the premises.
• How to raise the alarm for specific needs, e.g. flashing light warnings for people with impaired hearing.
• Appointing staff members to help disabled people or older adults with evacuation; some people might require one-to-one assistance.
Lots of disabled people are able to use a stairway, but some might need assistance. People with visual impairments can be guided on level surfaces by offering an arm for them to hold. On stairways the guide should descend first so that the person following can place their hand on the guide’s shoulder.
There is equipment available for safely transporting people with mobility impairments down stairways; it needs to be given serious consideration, especially in high-rise buildings. Lifts are normally prohibited from use in an evacuation. Some buildings have special types of lift, known as evacuation or fire-fighting lifts, for evacuating disabled people. These lifts must only be operated in accordance with the evacuation procedure by a member of staff. Wheelchairs, guide dogs and other equipment should also be evacuated if safe to do so.
KEY POINTUse ramps to evacuate wheelchairs.
Copyright © 2014 Active IQ Ltd. Not for resale | 105
Section 1: Emergency procedures in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

End of section: Learning check Answer the questions and make notes to revise this section.
• What is the difference between a hazard and a risk?
• Name six different types of emergency situation that can happen in a fitness environment.
• Describe the roles of these employees in an emergency:
• First aider.
• Health and safety officer.
• Fire warden.
• Organisation staff.
• Police officer.
• Paramedic.
• Fire fighter.
• Why is it important to follow emergency procedures calmly and correctly?
• How would you contact the emergency services?
• What information would you provide for the emergency services?
• What information would you record in an accident report book?
• How should you deal with sufferers of these incidents?
• A minor sprain of the ankle.
• Fainting.
• Angina – chest pain.
• Fire.
• How would you maintain the safety of these groups in an emergency?
• Children.
• Older adults and disabled people.
106 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Emergency procedures in a fitness environment

KEY POINTHealth and safety in the workplace is a legal requirement.
Section 2: Health and safety requirements in a fitness environment
The purpose of health and safety in a fitness environment is to ensure the welfare of all people in the workplace, as far as is reasonably practicable. This includes the welfare of employees, customers and any person using services or visiting the facility.
Legal and regulatory requirementsThe main piece of health and safety legislation for any workplace in the UK (including a fitness environment) is the Health and Safety at Work Act, 1974. The Act comprises a variety of health and safety laws and regulations that stipulate the duties of employers and employees. As of 5th April 2014 a Health and Safety Law poster must be clearly displayed in the workplace or an equivalent pocket card/ leaflet given to all employees.
Employers
Employers must:
• Carry out a risk assessment.
• Implement safety measures in response to issues identified by the risk assessment.
• Appoint competent people to manage the welfare of others and implement safety measures.
• Devise emergency procedures.
• Provide clear guidance and training for employees.
• Consult with employees on all health and safety issues.
• Report injuries in the workplace.
• Provide insurance for injuries.
• Provide facilities and equipment for dealing with health and safety issues.
• Work with other employers (where relevant) who share the workplace.
• Displaying a health and safety policy statement when employing five or more people.
Arrangements can include:
• Providing and maintaining appropriate equipment for work.
• Providing toilets and washing areas.
• Providing drinking water.
• Appointing and training staff to manage potential areas of risk (e.g. first aid and chemical spillage procedures).
Copyright © 2014 Active IQ Ltd. Not for resale | 107
Section 2: Health and safety requirements in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

Employees
Employees’ responsibilities include:
• Following procedures and training programmes correctly.
• Taking care of their health and safety at work.
• Taking care of the health and safety of those around them.
• Cooperating with their employer and reporting any concerns immediately.
LEGISLATION REQUIREMENTS
Reporting of Injuries, Diseases and Dangerous Occurrences Regulations, 1995 (RIDDOR)
Employers must report occupational injuries, diseases and dangerous events that happen in the workplace.
Manual Handling Operations Regulations, 1992
Employers must have procedures in place for the lifting or moving of objects by hand or bodily force. Hazardous lifting should be eliminated where possible; if it is unavoidable, mechanical aids must be provided.
Management of Health and Safety at Work Regulations, 1999
Employers must carry out risk assessments and implement appropriate measures to manage risks, e.g. appointing and training staff to deal with safety issues.
Employers’ Liability (Compulsory Insurance) Act, 1969
Employers must have insurance for covering accidents and ill health.
Health and Safety (First Aid) Regulations, 1981
Employers must have at least one qualified first aider or appointed person (depending on risk assessment). First aid kits and facilities must be available.
Personal Protective Equipment at Work Regulations, 1992
Employers must provide adequate, suitable protective clothing and equipment for their employees (as appropriate). Equipment must fit properly, carry the CE kite mark and be kept clean and stored correctly.
Control of Substances Hazardous to Health Regulations, 2002 (COSHH)
Employers must assess and take precautions against the risks of hazardous substances (e.g. chemicals, dust, gases and fumes) and train their staff to use them safely.
Health and Safety Information for Employees Regulations, 1989
Employers must display a poster that provides employees with information on health and safety.
Provision and Use of Work Equipment Regulations, 1998
Employers must ensure that all equipment and machinery is safe to use and adequately checked and maintained.
Noise at Work Regulations,1989 Employers must take action to ensure employees are protected from hearing damage in the workplace, e.g. caused by drilling or music.
Workplace (Health, Safety and Welfare) Regulations, 1992
Outlines numerous welfare issues for employers to consider, including workstations, seating, heating, lighting and ventilation.
Table 2.1 Health and safety legislation and regulations (HSE, 2014)
108 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Health and safety requirements in a fitness environment

Duty of care and professional role boundaries Everyone in the workplace has a duty of care to protect themselves and others, as far as is reasonably practicable. Personal responsibilities are specified in each employee’s job description.
The aspects of health and safety that fall within the role of a fitness instructor are personal safety, client safety and environment safety.
ROLE ASPECT RESPONSIBILITIES
Personal safety • Holding appropriate qualifications for any session delivered. • Only working with people or groups for which they are qualified. • Holding public liability insurance and employer liability insurance.• Maintaining continuing professional development (CPD).• Being a member of appropriate regulatory bodies (e.g. Register of Exercise Professionals).• Adhering to industry codes of conduct. • Following organisational procedures. • Holding a first aid or CPR qualification if working with certain groups (e.g. exercise referral). • Awareness of health and safety policy and responsible behaviour, e.g. reporting hazards. • Knowing the duty first aider, location of the nearest contact phone and first aid kit, and the
procedure for reporting accidents.
Client safety • Screening clients before exercise, using appropriate methods, e.g. PAR-Q and verbal screening checks.
• Referring clients to the GP when necessary (e.g. medical conditions).• Ensuring clients dress appropriately (e.g. acceptable footwear and no jewellery).• Ensuring clients are not chewing gum. • Ensuring that clients’ technique and use of equipment is safe by observing and correcting
them wherever necessary.
Environment safety
• Ensuring there is enough space for participants (no overcrowding or risk of collision).• Ensuring there are no trailing wires (risk of slips and trips).• Ensuring floors are dry or signs are positioned to identify wet floors.• Ensuring the environment is prepared for exercise (e.g. checking that equipment is set up
properly and nothing is causing an obstruction).• Ensuring the environment is left clear and tidy after exercise, with everything put away in
the correct place.• Keeping floors clean and swept.
Equipment safety • Ensuring equipment is stored appropriately, e.g. steps stacked at an appropriate height, weights stored on racks and pool equipment in baskets.
• Ensuring equipment is clean, e.g. wiping down CV equipment or mats.• Placing ‘out of order’ signs on any broken equipment. • Reporting broken equipment to maintenance personnel.
Table 2.2 Health and safety responsibilities for fitness instructors
Copyright © 2014 Active IQ Ltd. Not for resale | 109
Section 2: Health and safety requirements in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

KEY POINTIf instructors do not have the requisite qualification and training in the adaptation of exercise they should inform clients. Clients should be given the choice to stay in the session and follow basic recommended guidelines or seek further guidance from an appropriately qualified instructor.
TRAINER TIPAlways check that the employer’s insurance policy (and any personal policy) covers work with special populations.
Duty of care and professional role boundaries in relation to vulnerable groupsThere are certain groups to whom you have a particular duty of care, such as:
One essential priority is screening clients; all clients must be screened using appropriate forms before they can exercise. Clients who answer ‘no’ to PAR-Q questions can engage in exercise, as long as activities are suitably and personally modified by the instructor.
If planning to work with a vulnerable client group on a long-term basis, additional specialist training and qualifications are required.
Level 2 fitness instructors are not qualified to do the following, as these would constitute acts of negligence and breaches of duty of care:
Duty of care is the obligation to exercise a reasonable level of care towards an individual, to avoid injury or damage to property. Negligence is failing to follow responsibilities. A negligent act may be unintentional, but it is careless, and can result in loss.
Children and young people (aged 14-16 years).
Older adults.
Pre- and post-natal women.
Disabled clients.
Clients with medical conditions.
Vulnerable adults.
Act as a specialist instructor.
Advertise as a specialist instructor.
Instruct clients from specialist groups (one-to-one or in groups) on a regular basis.
Plan progressive, long-term programmes for clients from specialist groups.
110 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Health and safety requirements in a fitness environment

Roles of staff members responsible for health and safety in a fitness organisationThe management team and organisation’s directors assume overall responsibility for health and safety in the workplace. However, they often appoint and train people for specific duties.
Health and safety officer
There is usually a designated advocate for health and safety in a fitness workplace; it is often the duty manager because of their multi-faceted role and responsibilities.
Department health and safety lead
Each department typically has a designated health and safety lead; it is usually the manager or head of department. They are responsible for ensuring the welfare of others and making sure that any incidents are reported and acted upon appropriately.
First aiders
A number of employees in a fitness environment are delegated and trained to provide first aid.
Fitness instructors
Fitness instructors will be required to conduct a number of health and safety checks during their hours of work. All checks should follow the employer’s health and safety policies and procedures. All associated documentation must be filled in correctly to demonstrate evidence of health and safety compliance.
Any person who fails to follow current health and safety legislation may be made liable for incidents or accidents that occur (negligence). If their duty of care/service is questioned, this may be taken to a court of law and challenged as negligence. Any relevant documentation would be used as evidence. A court will consider the current standard working practices within the industry and the chain of responsibility to highlight areas of failure (negligence).
Key health and safety documents relevant in a fitness environmentKey health and safety documents include various screening forms used to provide clearance for clients. Other important documentation relates to health and safety and emergency procedures in the facility.
PAR-Q forms
The PAR-Q and other screening forms are written questionnaires that ask clients a series of questions to check whether exercise needs to be delayed or GP clearance is required before participation. Clients who answer ‘yes’ to one or more questions on the forms must be signposted to their GP to obtain clearance.
The questionnaires are provided by the Canadian Society for Exercise Physiology (CSEP). Permission is not required to photocopy the forms for personal or clinical use, but it is required to reproduce the forms. The forms can be downloaded from the CSEP website.
Copyright © 2014 Active IQ Ltd. Not for resale | 111
Section 2: Health and safety requirements in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

PAR-Q:This is a one-page questionnaire for clients aged 15 to 69. It asks clients to answer seven questions. Most gyms ask members and guests to complete this form when they join.
The questions are:
1. Has your doctor ever said that you have a heart condition and that you should only do physical activity recommended by a doctor?
2. Do you feel pain in your chest when you do physical activity?
3. In the past month, have you had chest pain when you were not doing physical activity?
4. Do you lose your balance because of dizziness or do you ever lose consciousness?
5. Do you have a bone or joint problem (for example, back, knee or hip) that could be made worse by a change in your physical activity?
6. Is your doctor currently prescribing drugs (for example, water pills) for your blood pressure or heart condition?
7. Do you know of any other reason why you should not do physical activity?
Source: CSEP, 2014
PAR-Q+:This form is used in exercise referral. It is a four-page questionnaire and asks seven main questions (similar to the PAR-Q) with additional questions on chronic health conditions.
Physician Physical Activity Readiness Clearance (PPARC):This is used by GPs to give further information to instructors about clients for whom they have provided clearance.
PARmedX for pregnancy:This is a four-page questionnaire for screening women who are pregnant and want to exercise.
Challenges of administering the written PAR-Q formIf the PAR-Q is completed at the front desk before the participant enters the facility it can sometimes be a challenge to get the information to instructors. Considerations include:
1
2
3
How is information collected at the front desk passed to instructors? If information is not collected at the front desk, how and when is it collected?
How is information collected for group exercise sessions if participants arrive late?
How and when is information checked to ensure it is up to date and who will check this?
KEY POINTWritten screening must be completed by all clients before participating in physical activity.
112 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Health and safety requirements in a fitness environment

Informed consent recordInformed consent must be obtained from the client before participation in any fitness testing or exercise session. Informed consent can only be given when the purpose, risks and benefits of participation have been fully explained and understood and all the client’s questions answered and recorded.
Informed consent documents are legal records and should be checked by legal professionals. An informed consent record should contain:
• An explanation of the purpose of the assessment and/or programme.
• A description of the components of the assessment and/or programme.
• An explanation of the possible risks, discomforts and benefits.
• Clarification of the responsibilities of the client.
• A reference to confidentiality and privacy.
• An emphasis on the client’s voluntary participation and right to change their mind.
• The opportunity for the client to ask questions (with space to record questions and answers).
• The signature of client and witness (instructor) and date.
Health Commitment StatementThe Health Commitment Statement (HCS) is the evolution of the PAR-Q. It reflects government policy and legal trends, which aim to shift responsibility for personal health from the operator to the user. The HCS recognises that individuals are able to make informed decisions about their own health and wellbeing when given appropriate information about the risks involved in getting active.
More information on the HCS is available from ukactive (previously the Fitness Industry Association), which has taken the lead in allowing operators to be more accessible.
The HCS has been developed by fitness industry operators, medico-legal professionals and health providers to support the evolving requirements of users and operators.
Information for providers who wish to purchase the HCS for use is available from ukactive.
The purpose of the HCS is to:
• Develop the PAR-Q to simplify user access to activity facilities.
• Assist the health, medical and fitness industries to work in harmony while supporting initiatives to encourage the nation to become more active.
• Bring health and fitness clubs in line with virtually all other sports and active leisure in relation to health matters.
• Demonstrate respect for members by placing responsibility with the individual member.
• Be consistent with government policies that encourage every individual to take responsibility for their own health.
• Offer the opportunity for clubs to maximise their membership.
• Be consistent with current trends in legislation and case law.
• Be consistent with a more modern approach to individual responsibility in medicine and the law.
• Provide the opportunity for a uniform approach across the health and fitness industry, producing greater clarity and reducing costs.
• Offer a simple solution in plain English, which is accessible to fitness instructors, staff and members.
• Remove stress and anxiety from staff in relation to the health of members.
ukactive, 2014
Copyright © 2014 Active IQ Ltd. Not for resale | 113
Section 2: Health and safety requirements in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

EXPERT TIPThere are very few conditions which cannot be improved by taking regular exercise and the HCS seeks to make it as easy as possible for people to get active.
UKACTIVE, 2014
Client emergency contact records
It is important that clients’ emergency contact numbers (e.g. next of kin) and doctor’s contact details are available. In the event of an accident or emergency these details are vital. This information should be available in gym membership records and can be incorporated into a PAR-Q form. All staff must know where these details are stored and who to contact to access the information.
Emergency action plans and procedures (EAPs)
Emergency action plans set out the procedures to follow in the event of an accident or incident, e.g. bomb threat, evacuation, gas leak or fire. EAPs are generally specific to an environment, for example the requirements for a poolside incident will be different to a gym-based incident. Staff training will be given to all employees and this is often followed by a competence test.
EAPs cover the following requirements:
1
2
3
What to do in the event of the accident/incident.
What to do during the accident/incident.
What to do after the accident/incident.
Accident and incident report bookAll organisations must have an accident and incident report book. This is a legal requirement (RIDDOR - see table 2.1).
Information recorded may include:
• Full information about the organisation and reporting person.
• What happened.
• When it happened.
• Where it happened.
• How it happened.
• Who it happened to and how they were affected (type of injury).
• Any witnesses, including statements and signatures.
• What actions were taken.
• Date and signatures of the person reporting the incident.
• Follow-up notes.
Information on reporting different types of accident and incident is available from the Health and Safety Executive (HSE).
114 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Health and safety requirements in a fitness environment

INTRUDER ALARMS
PANIC ALARMS
PERSONAL ALARMS
MINIMISING LONE WORKING
Intruder alarms are fitted in buildings to protect against unlawful entry particularly after hours. It is possible to appoint a company to monitor and attend alarm callouts that may occur. Trained personnel will attend with backup and dogs if necessary.
Panic alarms are used in areas such as reception and consultation rooms and located where they can be covertly operated by a threatened staff member.
Personal alarms or warning devices (whistles) can be carried by employees to attract attention (e.g. pool lifeguard) or temporarily distract an attacker.
Minimising lone working helps protect staff at the facility. Lone working is any work activity intended to be carried out in isolation from other workers. This may include opening and closing a building.
Types of security procedure in a fitness environment There are a number of security procedures in place within a fitness environment to help protect staff and participants.
External gym security
A fitness facility’s responsibility for maintaining participant safety is not limited to the inside of the building. Customers may have to drive, park and walk to and from the building safely. This requires varying levels of security depending on the location of the facility. Ideally there should be a complete security system in place.
Video monitoring systems (CCTV), lights and alarmsFacility owners adjust their level of security to match their environment; deterring crime is worth the effort and expense. A video monitoring system is recommended for security outside the facility. At least one system with a camera should monitor the front entrance and other cameras should monitor the parking area. The monitor should be placed in the security office or at the front desk.
Every exit door should have outdoor cameras and a monitor just inside the door for maximum security, so the area can be viewed before leaving the building.
Sufficient security lighting should be available. Outdoor car park lighting is often operated with motion detectors. They are also often run with timers that turn on and off according to the facility hours.
Security and alarm stickers should be placed on every door and window as a deterrent, even if there is no alarm system.
Indoor gym security
There are many ways to control access to protect people and property, e.g. staffed receptions, barriers and swipe cards and simple coded locks. The layout, size and design of the building will largely influence what methods are chosen.
Further information on health, safety and security can be sourced from the HSE.
Copyright © 2014 Active IQ Ltd. Not for resale | 115
Section 2: Health and safety requirements in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

Preventing violence
Procedures should be devised to minimise the risk of violence from the public, e.g. elimination of cash handling, changes of route when transporting valuables, adequate building security for out-of-hours working. Consideration should be given to the fact that women working alone are particularly at risk.
Radios, pagers or mobile phones
Pagers or radios are often provided to duty managers and staff with specific responsibilities (e.g. duty first aider), so they can be contacted easily while moving around a facility. These provide effective means of communication and keep colleagues informed of people’s movements and problems. Mobile phones are often provided for area managers who travel between sites. They can report travel delays between sites or when moving to another site for a meeting.
Training for staff
Staff training should be encouraged to keep abreast of industry standards and changes to legislation and to stay aware of dangers that may be presented and how to handle them. Induction training is also essential for new employees.
Confidentiality
All confidential information and personal information files (employees and clients) should be locked away in an office filing cabinet that is only accessible by those who need to use it.
End of section: Learning check Answer the following questions and make notes to revise this section.
• Why is health and safety important in a fitness environment?
• Name five legal and regulatory requirements for health and safety relevant to working in a fitness environment.
• What is duty of care?
• What things would be considered part of a fitness instructor’s duty of care?
• What are a fitness professional’s duty of care and professional role boundaries in relation to special population groups?
• Who would have overall responsibility for health and safety in a fitness environment?
• What is the role of a health and safety officer?
• Name three types of security procedure that may apply in a fitness environment.
• Describe the following health and safety documents:
• PAR-Q.
• Informed consent.
• Health Commitment Statement.
• Emergency action plan.
116 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Health and safety requirements in a fitness environment

Section 3: How to control risks in a fitness environment
A risk assessment is a careful examination of what could potentially cause harm to people in the workplace, so that responsible people can decide whether appropriate precautions are in place or more needs to be done to prevent harm. The aim is to minimise the potential for accidents or incidents to make sure that nobody gets hurt or becomes ill.
Assessing risks in the workplaceThe Health and Safety Executive (HSE) provides five simple steps for assessing and managing risk.
Table 3.1 Five steps to risk assessment
1
2
3
4
5
IDENTIFY THE HAZARDS
DECIDE WHO MIGHT BE HARMED
EVALUATE THE RISKS & DECIDE ON PRECAUTIONS
RECORD THE FINDINGS AND IMPLEMENT THEM
REVIEW THE ASSESSMENT & UPDATE (AS REQUIRED)
CONSIDERATIONSFIVE STEPS TO RISK ASSESSMENT
What are the hazards? Slips, trips, falls, chemicals, machinery, electricity, manual handling, noise, exercise risks, poor lighting and temperature.
Who might be harmed and how could they be harmed? Office staff, cleaners, visitors, contractors, gym members, gym staff (pay particular attention to people with disabilities). Is it a minor injury or are there more severe consequences?
Evaluate the risks and decide whether the existing precautions are adequate or whether more should be done. Provide instruction or training where necessary, reduce risk as far as reasonably practicable. What is the likelihood of an accident occurring? What level of risk is attached? What control measures can be used to control the risk?
Use a risk assessment tool to report and manage all identified risks. An example risk assessment report is available from the HSE website.
Review and update all risks and procedures at agreed intervals.
EXPERT TIPRisk assessment is:a careful examination of what, in your work or workplace, could potentially cause harm to people. HSE, 2014
Copyright © 2014 Active IQ Ltd. Not for resale | 117
Section 3: How to control risks in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

Possible hazards in a fitness environmentA hazard is anything that may potentially cause harm. There are many potential hazards in a fitness environment, which may relate to the facilities, the equipment, working practices, manual handling and lifting, security, client behaviour and hygiene.
AREA FOR CONSIDERATION
POSSIBLE HAZARDS
Facilities Loose or trailing electrical wires.Power cut.Flooring or carpet damage.Ceiling tiles damaged or loose.Lack of ventilation.High pool chlorine levels.
Heating failure.Gas leak.Broken window.Damaged fixtures.Temperature too hot or cold. Fire exits blocked.
Equipment Faulty wiring.Fraying cables on weight machines.Belt slipping on treadmill.
Foot straps broken on spinning bike.Loose dumbbell weights.Damaged seat on rower.Poor positioning of equipment.
Working practices Insufficient maintenance checks.Cleaning rota poorly adhered to.Gym floor insufficiently monitored.Poor manual handling and lifting.
Poor performance on evacuation drills.Pool plant room chemicals in close proximity.Poorly filed PAR-Q and member medical records.
Clients Medical conditions. Older adults. Disability. Pregnant or post-natal. Inactive.
Cardiovascular disease risk factors.Injuries. Body type. Skill and fitness level. Incorrect clothing or footwear.
Client behaviour Aggression.Drunkenness.Diving into a shallow pool.Lifting heavy weights without spotter. Not cleaning machines after use. Failure to disclose essential information (e.g. medical conditions).
Unsafe exercise technique.Incorrect back alignment when handling heavy weights.Stepping on and off moving treadmill belt.Chewing gum. Ignoring instructions or guidelines.Not replacing equipment after use.
Security Broken security camera.Faulty emergency exit door.Emergency doors left open in hot weather.
Late night lone worker left to secure building.Unmanned reception. Busy reception (security monitors not observed).
Hygiene Insufficient cleaning rota.Bins not emptied regularly.Drinking fountains with lime scale build-up.Stretching mats not disinfected.Toilets dirty. CV machines dirty.
Obvious scum line in pool.Excessive foam in the spa.Mould build-up in shower sealant.Shower room floors dirty. No toilet roll.
Table 3.2 Potential hazards in a fitness environment
118 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: How to control risks in a fitness environment

Manual handling and liftingManual handling is any activity in the workplace that involves lifting. It also usually includes climbing, pushing, pulling and pivoting objects. Manual handling and lifting can put safety at risk, so precautions are needed.
Potentially injurious tasks involve bending and twisting, repetitive motions, carrying or lifting heavy loads and maintaining fixed positions for a long time. These circumstances can lead to damaged muscles, tendons, ligaments, nerves and blood vessels. Potential musculoskeletal injuries, such as strains and sprains, often affect the lower back, shoulders and upper limbs. Any job that involves heavy labour or manual handling might include a high risk of injury, i.e. lifting objects can place strain on the lower back musculature when performed incorrectly.
Ergonomic intervention in manual handling can decrease injuries and increase worker productivity. The first consideration is whether the object needs to be moved, i.e. don’t move it unless you have to.
If the risk cannot be eliminated then the following ergonomic lifting techniques can provide controls to improve safety:
• Keep loads close to the body and near your centre of gravity.
• Use diagonal foot positions.
• Move loads at waist height rather than directly from the floor.
• Use a second person or mechanical device to assist lifting (as appropriate).
Table 3.3 Other considerations when lifting
CLIMBING
PUSHING & PULLING
PIVOTING
If climbing with a load (e.g. using stairs or a ladder) safe manual handling includes maintaining contact with the ladder or stairs at three points (two hands and a foot or both feet and a hand). Bulky loads require a second person or a mechanical device to assist.
Pushing is generally easier on the back than pulling. It is important to use arms and legs to provide leverage to start the push.
When moving containers it is safer to pivot shoulders, hips and feet (keeping the load in front at all times rather than twisting the back). The lower back is not designed to torque or twist repeatedly.
Copyright © 2014 Active IQ Ltd. Not for resale | 119
Section 3: How to control risks in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

Client risk assessment Evaluating the risk of exercise is complex because it is dependent on a range of variables. All variables must be considered when conducting a risk assessment and the potential risks must be weighed up against the potential benefits of the activity/exercise.
The starting point for the risk assessment must be a written screening to check whether medical clearance is required (e.g. PAR-Q).
Verbal screening checks will also be needed to gather additional information to help gauge the suitability of specific exercises for the individual client, e.g. exercise experience, skill and fitness level, any injuries, illnesses or disabilities which may affect the safety of some exercises.
This information must be evaluated by the exercise professional to assess the level of risk and take appropriate precautions to reduce the risk (e.g. exclude a specific exercise from a person’s programme or modify the exercise).
The exercise professional must respect their own role boundaries when gathering information from the client, e.g. they are not qualified to diagnose injuries. However, if a participant presents with an unspecified medical condition or injury, or if the client or exercise professional has concerns about the safety of participation, then clearance should be sought from a suitably qualified health/medical professional.
Some individual factors that may influence the safety of participation and the safety of specific recommended exercises are listed in table 3.4.
TRAINER TIPPre-screening is the first step of risk assessment to identify clients who need medical clearance before starting to exercise.
120 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: How to control risks in a fitness environment

RISK FACTORS FOR CONSIDERATION
EXERCISE CONSIDERATIONS
Medical status Client answers ‘yes’ to PAR-Q.GP clearance will be required. The client will need to be referred to a specialist instructor by GP (exercise referral).Some exercises may be inappropriate and many will need modification. For example, intense overhead exercises (e.g. shoulder press, lots of high arm punches) may be unsafe if someone presented with hypertension (high blood pressure).
Risk category Multiple risk factors for CVD, e.g. inactive, overweight, smoker, over age 55.GP clearance will be required for clients who are at low to moderate risk.Clients may need to work with a specialist instructor.Intensity and type of exercise would need to be reduced to enable safe participation. For example, low impact, lower intensity, shorter duration, accumulated approaches, less weight bearing will offer less risk.
Past surgery Past surgery may result in a weakness that would make certain exercises higher risk. A client who has had surgery to fuse vertebrae in the lumbar spine would be at high risk from exercises like plyometric hopping or lifting (explosive, high-impact), due to the increased pressure in the spine during these activities.
Exercise experience
Clients who are new to exercise and have low fitness and skill level will be at increased risk. Clients who are new to exercise will need to start at a lower level and progress gradually.For example, low complexity, low impact, lower intensity, shorter duration, accumulated approaches, less weight bearing will offer less stress/risk.
Injuries Any former injuries that have had little or no rehabilitative treatment.Clients may have altered their pattern of movement to compensate for pain. For example, a client with an ankle injury might have shifted their bodyweight away from the injured side while walking, creating muscle imbalances and postural changes.
Body type Body type may affect exercise potential and injury risk.Endomorphs may not be well suited to high-impact cardiovascular training. There may be greater stress on the joints. Ectomorphs may struggle to lift heavy resistances due to low muscularity and longer levers.Mesomorphs may struggle to float in water-based activities due to increased muscle mass and low levels of body fat.
Occupation The physical requirements of a person’s job can make certain exercises higher-risk.Fatigue levels need to be considered when training clients with physically demanding work. For example, at the end of a working day they may have a high fatigue level. Alternatively, if they are trained in the early morning hours they may arrive at work in a fatigued state. Both situations might leave them susceptible to injury.Occupation may also influence posture and muscle imbalances, e.g. a sedentary occupation (lots of desk work) may contribute to a flat back and hyperkyphotic posture.
Nutrition Poor eating behaviours and incorrect pre-exercise nutrition or post-exercise nutrition can have implications.If a client is trained after missing breakfast any high calorie burning and intense exercise will be higher risk.Low calorie diets affect energy levels and performance.
Stress Stress hormones (including adrenaline) may have significant side effects, which affect the client’s concentration and ability to sleep. Stress level and mood can affect posture, motivation and performance. After a stressful day it may not be advisable to take part in any highly challenging proprioceptive exercises, e.g. an explosive lift.There is a risk that clients will drop out of activity programmes if their mood is low.
Table 3.4 Individual factors that affect safety
Copyright © 2014 Active IQ Ltd. Not for resale | 121
Section 3: How to control risks in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

Exercise risk assessment Different types of exercise and activity and specific exercise variables also offer risks that may affect some clients more than others. Many of these variables have a significant impact on the selection of appropriate exercises.
VARIABLE CONSIDERATION
Weight and resistance
Increasing the weight or resistance of the load can increase risk. The risk will be further increased if the exercise also requires a high level of proprioception, as this will affect technique. For example, a squat is an effective exercise if performed correctly, but performing with excessive weight will place greater stress on the structures of the body.High-impact exercises (running and jumping) are effective for improving cardiovascular fitness, but for a person who is overweight, these would be higher-risk due to increased stress on the weight-bearing joints. Low-impact exercises would be safer and water-based exercise would support body weight.
Proprioception Exercises that require greater levels of proprioception increase risk because exercise technique is affected. Free weights and any gravity-dependent external load (medicine balls, kettlebells) are effective training tools, but offer an increased challenge that may offer greater risk for some participants.For example, a dumbbell press is preferable to a machine press in terms of the proprioceptive challenge, but requires greater body awareness and technique. It would offer a higher risk for newcomers.
Movement speed
Speed of movement affects safety, as it can affect the control and alignment of the movement. Some faster movements may need to be included in training because they are essential in activities of daily life and sport, but control and alignment shouldn’t be sacrificed. For example, a skilled marathon runner is well coordinated, which allows them to run faster with little risk. A beginner won’t have the same level of coordination, so their movement will need to be slower to maintain control and keep the risk minimal.A group of muscles will initially contract to generate movement; the faster the movement the greater the level of contraction needed. The opposing muscles will also have to contract in order to decelerate the movement or act as a brake. If the decelerating muscles cannot generate at least the same level of force as the accelerating muscles then injury is likely to occur.For example, when forcefully contracting the hip flexors and knee extensors (quadriceps) to kick a ball a great distance the hip extensors and knee flexors (hamstrings) will have to contract eccentrically to decelerate the leg (and control the kick). If the opposing muscles (hamstrings) have not got the strength needed to perform this deceleration they may become injured.
Fixed resistance machines
Fixed resistance machines are based on fixed path range of motion and often a fixed body position. If the machine does not allow the posture of the person performing the exercise to remain optimal and the load to be distributed correctly then the exercise can become high-risk.For example, most bicep curl machines require the exerciser to lean over a pad, which compromises the integrity of the shoulder by putting it into a protracted position. This increases the degree of risk associated with the exercise.
Stability Some exercise positions offer greater stability. The use of stability equipment should be included only when clients have sufficient stability and balance to perform an exercise safely and effectively without equipment. Stretches may need to be performed in stable and supportive positions for clients who lack flexibility and balance. For example, correct technique for exercises like abdominal curls and back raises should be mastered before performing them using stability equipment. Exercises that challenge balance (e.g. yoga postures) should be progressed according to the needs of the individual. Stretch positions may need to be floor based or use balance aids (wall or chair) to assist stability and balance initially.
Table 3.5 Exercise risk considerations
122 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: How to control risks in a fitness environment

The exercise risk continuum
Figure 3.1 shows a continuum of risks that will assist risk assessment of specific exercises for clients.
LOWER RISK HIGHER RISK
Apparently healthy client. Client with medical conditions or injury or special populations.
Lower training effect. Higher training effect.
Lower intensity.Lower % of maximal heart rate. Lower % of repetition maximum. Lower:• Resistance (up to 60% effort).• Range of motion.• Repetitions.• Sets.
Higher intensity.Higher % of maximal heart rate.Higher % of repetition maximum.Higher:• Resistance (70% + effort).• Range of motion.• Repetitions.• Sets.
Lower impact. Higher impact.
Lower weight-bearing. Higher weight-bearing.
Shorter duration or accumulated approaches. Longer duration.
More stable and supportive positions. Less stable positions.
Low proprioception required. High proprioception required.
Slower speed, controlled movements. Fast, higher-speed movements.
No equipment used. Use of equipment, e.g. medicine balls, stability balls.
Figure 3.1 Exercise risk continuum
One key consideration is that there are no right and wrong or good and bad exercises. However, there are exercises that will offer increased risk for some clients. Relevant individual factors, such as fitness level, skill level, training goals and other factors, such as equipment and environment should all be considered when deciding whether or not an exercise is appropriate.
All potential risks should be evaluated and if the risks outweigh the benefits an alternative or modification should be found. Alternatively, if the benefits outweigh the risks, then it may be safe to proceed without modification.
NB: Appropriateness of specific exercises will be considered in the planning and programming manuals for the specific exercise disciplines.
High risk
High stimulation
Low risk
Low stimulation
Copyright © 2014 Active IQ Ltd. Not for resale | 123
Section 3: How to control risks in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

Assessing the possible hazards in a fitness environmentThe HSE ‘five steps’ model should be used when assessing risks. The important things to decide are whether a hazard offers a significant risk and whether satisfactory precautions are in place to reduce the level of risk.
For example, electricity can kill but the risk of this in an office environment is remote, provided that the ‘live’ components are insulated and metal casings properly earthed.
Evaluating risk
Risk assessments are rated using a numbered system from 1 to 5 according to:
• Likelihood of risk occurring.
• Risk severity.
The two numbers are then multiplied together to give a risk rating. The result will determine what action needs to be taken.
SCORE 1 2 3 4 5
LIKELIHOOD 2% Unlikely 5% 10% 25% 50% Likely
SEVERITY Minor injury – near miss
First aid – back to work
Off work for over three days
Major injury/disease
Death
RISK RATING • 1-2 acceptable LOW (no further action).• 3-10 tolerable MEDIUM (maintain controls).• 11-25 danger HIGH (stop – immediate action required).
Table 3.6 Risk rating
For example, the likelihood of an apparently healthy young adult, who exercises regularly, experiencing a cardiac emergency is unlikely (1-2), but the consequences would be severe if it were to happen (4-5). The likelihood of a client with an existing cardiac condition experiencing a cardiac emergency is much more likely (5) and the severity of risk would be high (5).
POSSIBLE RISK LIKELIHOOD SEVERITY SCORE RISK AND ACTION
ACTIONS
An apparently healthy young adult, who exercises regularly, experiencing a cardiac emergency when exercising.
1 4-5 4 to 5 Medium – maintain controls.
Pre-screen.Monitor intensity. Warm up and cool down appropriately. Programme training to meet specific needs.
A client with an existing cardiac condition, who is inactive, experiencing a cardiac emergency when exercising.
5 5 25 High –Stop!Immediate action required.
Signpost to GP.Specialist and clinically supervised exercise.
Table 3.7 Risk rating example
124 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: How to control risks in a fitness environment

ACTI
VIT
Y The purpose of this activity is to encourage you to think about the many factors that might affect levels of risk. You can use your notebook to make some additional notes. You can also discuss your notes with your peers or a tutor.
Evaluate the following risks. Multiply the likelihood and severity scores to find the total.
HAZARD/RISK
LIKELIHOOD
SCORE: 1 TO 5
SEVERITY
SCORE: 1 TO 5
TOTAL SCORE
RISK RATING
LOW, MEDIUM, HIGH
SAFETY CONTROLS
Client drowning in a swimming pool.Client experiencing an increase in blood pressure during exercise.Client tripping over a dumbbell in the gym.Client straining their back lifting a heavy weight.Client dropping a weight on their foot.
Controlling risks associated with hazards in a fitness environmentThe first consideration for controlling any hazard and potential risk is to eliminate the risk altogether if possible. For example:
• Requesting GP clearance for some clients and not working with these clients unless qualified (exercise referral).
• Not attempting to lift a weight that has been left on the floor and is too heavy to stack when tidying the gym area.
• Using professional services to move or maintain cardiovascular equipment.
• Asking clients to collect and return pins to a central point (reception or gym desk) before and after use to eliminate risk of clients leaving weight pins in resistance weight stacks.
Copyright © 2014 Active IQ Ltd. Not for resale | 125
Section 3: How to control risks in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

1
2
3
4
5
IS THERE A LESS RISKY OPTION?
CAN ACCESS TO THE HAZARD BE LIMITED?
CAN EXPOSURE TO THE HAZARD BE REDUCED?
WOULD PERSONAL PROTECTIVE EQUIPMENT BE USEFUL?
ARE THERE WELFARE FACILITIES IN THE EVENT OF AN ACCIDENT?
For example, using a spotter or helper to lift a heavy weight, or performing a modification of an exercise for a client with a specific need (e.g. walking instead of running), or using a less hazardous chemical.
For example, using a sign to identify a wet floor, or using a rope to identify changes in swimming pool depth, or securing any trailing wires to reduce the likelihood of trips.
For example, restricting access to a pool plant area with chemicals, or planning work schedules to limit exposure (e.g. shorter life-guarding rotas), or allowing access only to clients who have been inducted.
For example, wearing correct clothing and footwear in the gym.
For example, first aiders, first aid kits.
ELIMINATE THE RISK REDUCE THE RISK ISOLATE THE RISK CONTROL THE RISK WEAR PROTECTIVE CLOTHING
If the hazard or risk cannot be eliminated the next consideration should be how can it be controlled or managed. For example:
ACTI
VIT
Y Use your notebook to think about how you would control the following hazards.
• A broken treadmill or spin bike.
• Heavy weights left on the floor.
• A client with hypertension and other cardiovascular risk factors.
• A client exercising while unwell.
• A client wearing incorrect or no footwear in the gym.
• A client chewing gum.
• A client wearing lots of jewellery.
• A non-swimmer entering the deep end of a swimming pool.
126 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: How to control risks in a fitness environment

Who to contact when hazards and risks cannot be controlled personally
When hazards or risks cannot be controlled personally the person responsible for health and safety should be contacted. This may be:
• A duty manager.
• An appointed health and safety officer.
• A line manager who leads on health and safety for a specific department.
A risk assessment report will need to be completed. An example risk assessment report is available from the HSE website.
End of section: Learning check Answer the following questions and make notes to revise this section.
• Identify two possible hazards in a fitness environment relating to each of the following:
• Facilities.
• Equipment.
• Working practices, including lifting and handling of equipment.
• Client behaviour.
• Security.
• Hygiene.
• How would you risk assess the hazards in a fitness environment?
• How would you control risks associated with hazards in a fitness environment?
• Who would you contact in an organisation when hazards and risks cannot be controlled personally?
• Prepare a risk assessment for your work environment. Use the table below or download a risk assessment report from the HSE website.
HAZARD WHO MAY BE AFFECTED?
LEVEL OF RISK (USE SCORING TABLE)
WHAT CONTROLS CAN BE PUT IN PLACE?
WHAT ADDITIONAL ACTIONS MAY BE REQUIRED?
Copyright © 2014 Active IQ Ltd. Not for resale | 127
Section 3: How to control risks in a fitness environmentH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

Section 4: Safeguarding children and vulnerable adults
Safeguarding the welfare of children and vulnerable adults means ensuring their safety, protecting them against maltreatment and removing any risk of harm, neglect or abuse.
Children: In the UK most protection agencies refer to children as any person under the age of 18 (NSPCC, 2014).
Vulnerable adults: A vulnerable adult is any person ‘aged 18 years or over, who is in receipt, or in need, of community care services by reason of mental or other disability, age or illness and who is or may be unable to take care of him or herself, or unable to protect him or herself against significant harm or exploitation’ (Department of Health, 2000).
Vulnerable people may include people with a learning disability, physical disability, sensory impairment or mental health needs including dementia, or a person who misuses substances or alcohol, or who is physically or mentally frail.
Working with children and vulnerable adultsPeople who work with children and vulnerable adults on a regular basis provide a link to the identification of a child/vulnerable adult who has been (or is) at risk of harm. All those directly or indirectly involved with children’s leisure activities have a responsibility to:
• Review their own practice in situations to ensure they are complying with recognised codes of conduct.
• Identify their own values and feelings in relation to abuse and recognise how they might potentially affect how they respond.
• Recognise the signs and symptoms and indicators of abuse and their impact.
• Respond in an appropriate way to a child or vulnerable adult who discloses information to them.
• Take appropriate action if concerns are raised.
Safeguarding responsibilities and limitations
All people have responsibilities in relation to safeguarding. Specific duties form part of a job description.
Responsibilities of organisations include:
• Develop a safeguarding policy and procedures.
• Develop appropriate codes of behaviour.
• Ensure effective recruitment and management of staff and volunteers working with children and vulnerable adults.
• Provide training for staff to ensure they know how to recognise and report concerns and identify and manage risks.
• Deal with complaints and feedback.
• Appoint a named person responsible for managing safeguarding and related issues.
• Manage records, including confidentiality and sharing information.
128 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: Safeguarding children and vulnerable adults

Responsibilities of instructors include:
• Adhere to all policies and procedures in relation to safeguarding.
• Attend training provided by organisations as requested.
• Follow appropriate codes of behaviour related to safeguarding, including wearing a uniform and name badge (when provided) and preventing circumstances which may lead to allegations of abuse.
• Act as a role model and build a culture of honesty and integrity.
• Know how to identify and manage risks in relation to safeguarding.
• Know how to recognise and report concerns, including appropriate people and statutory agencies to contact.
• Know how to share information confidentially.
Types of abuse and possible signs The term ‘abuse’ is used to describe the ways in which children or vulnerable people can be harmed. It affects the physical and mental development and wellbeing of the person and may occur at home, at school or in a community setting, such as a leisure centre. It may be a single incident or it may be repeated occurrences.
Abuse may occur by an adult abusing a child or vulnerable adult. It can also involve a child abusing another child.
Abuse can take many forms at various levels of severity, but it can be broadly separated into five main categories (see table 4.1). Some types of abuse are criminal offences.
Physical abuse
This occurs when someone causes physical harm or injury. For example, hitting or shaking, scalding or burning, punching, kicking, restraining, giving inappropriate drugs or alcohol and otherwise inflicting deliberate physical harm.
Emotional abuse
This is any form of ill-treatment that makes someone feel worthless, unloved, unvalued, frightened or in danger. It has severe and persistent adverse effects on wellbeing. Any person who has suffered neglect, physical or sexual abuse will also have suffered a degree of emotional abuse. However, this mistreatment can also occur on its own. Emotional abuse may include name calling, hurtful criticism, putting them down, lying to others about the person, ignoring them, shouting at them, threatening or taunting.
Sexual abuse
This occurs when adults use a child or vulnerable person to meet their own sexual needs. It also occurs when young people use children to meet their own sexual needs. This could include rape or sexual assault, involving children in producing or showing pornographic material, refusing to accept ‘no’ in response to an advance, making the person feel scared, touching or fondling in a sexual manner.
SOMETHING EXTRASome forms of abuse can lead to prosecution.
KEY POINT‘Abuse is a violation of an individual’s human and civil rights by any other person or persons’.
Department of Health, 2000
Copyright © 2014 Active IQ Ltd. Not for resale | 129
Section 4: Safeguarding children and vulnerable adultsH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

Neglect
This occurs when the child or vulnerable person’s basic needs (physical and/or mental) are ignored and not met. Examples of neglect include failing to provide adequate shelter, food or clothing; regularly leaving children or vulnerable adults alone or unsupervised; failing to give access to appropriate medical care; refusing to give a child or vulnerable person attention.
Bullying and harassment
This is deliberately hurtful behaviour, usually repeated over a period of time, where it is difficult for those bullied to defend themselves. It can be verbal, written or physical abuse, such as threats and gestures, name calling, discrimination, racist taunts, being ignored, physical assaults, shouting or swearing at the person.
TYPE OF ABUSE
POSSIBLE SIGNS
Physical abuse • Fear of parent, guardian or carer being contacted.
• Aggressive or angry outbursts.• Running away.• Fear of going home.• Flinching.• Depression.• Keeping arms and legs covered.
• Cigarette burns.• Bite marks.• Broken bones.• Scalds.• Withdrawn behaviour.• Unexplained bruising or injuries.• Bruises which reflect hand marks.
Common sites of non-accidental injury: Eyes, ears, nose, cheeks, mouth (inside and out), neck, shoulders, upper arms, inner arms, chest, back, abdomen, genitals, buttocks, thighs.
Common sites of accidental injury: Crown of head, forehead, nose, bony spinal protuberances, elbows, hips, hands, knees, shins.
Emotional abuse • Neurotic behaviour.• Inability to take part.• Fear of making mistakes.• Sudden speech disorders.
• Self-harm.• Fear of parents, guardian or carer being
contacted.• Delayed development (children).
Sexual abuse • Sudden changes in behaviour.• Becoming aggressive/withdrawn.• Apparent fear of one person.• Running away.• Sexual drawings/language.• Bedwetting.• Advanced sexual knowledge or behaving
beyond their age.
• Sexually explicit behaviour.• Pain/itching/bruising in the genital area.• Sexually transmitted diseases.• Stomach pains.• Discomfort when walking/sitting.• Pregnancy.• Self-harm or suicidal thoughts.
Neglect • Regular lack of supervision and loneliness.• Constant hunger.• Unkempt state.
• Weight loss.• Inappropriate dress.• Truancy and lateness (children).
Bullying and harassment
• Shyness.• Insecurity.• Hypersensitivity.
• Depression. • Withdrawn behaviour.• Fear of a particular person.
Table 4.1 Types of abuse and possible signs
Another type of abuse of vulnerable adults is financial abuse. This includes stealing from them, fraud, financial exploitation and abusing their vulnerability to extort money.
130 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: Safeguarding children and vulnerable adults

Policies and procedures in relation to safeguardingA safeguarding policy explicitly states an organisation’s views in relation to keeping children and vulnerable adults safe and sets out what it will do to keep them safe, including reporting procedures.
All organisations including fitness centres, leisure facilities and sports clubs/governing bodies will have a safeguarding policy that outlines:
• The organisation’s purpose and function.
• The organisation’s views about keeping children and vulnerable people safe.
• The steps the organisation is taking.
• The main legislation and guidance that supports the policy.
• How the organisation is going to meet this responsibility and put it into action (procedures).
• Who the policy applies and relates to (e.g. staff, volunteers, children up to 18 years old, vulnerable adults).
• Links to other relevant policies and procedures, e.g. recruitment, codes of conduct and behaviour, taking photographs and videos.
• Running safe activities and events for children and vulnerable people.
• Potential risks and how to manage them.
• Reporting procedures to follow in the event of any concerns.
• Protection against allegations.
• Named contacts for dealing with concerns (e.g. safeguarding or child protection officer).
• Recording and sharing information.
Key principles
The specific content of a policy for safeguarding and protecting children and vulnerable adults will depend on the working environment, but most policies would require staff to:
• Follow appropriate procedures.
• Demonstrate appropriate personal behaviour and conduct at all times.
• Maintain a high level of competence (qualifications and ongoing training) to ensure safe and correct practice.
• Develop a relationship with children, vulnerable adults and staff based on openness, honesty, mutual trust and respect.
• Respect and champion the rights of every individual to participate in leisure activities.
Copyright © 2014 Active IQ Ltd. Not for resale | 131
Section 4: Safeguarding children and vulnerable adultsH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

Staff recruitment
Organisations have policies and procedures for the recruitment, employment and deployment of staff and volunteers. This identifies the level of experience or qualification required by each member of staff according to their employed role (e.g. sports coaches, lifeguards, gym instructors, duty managers) and reflects relevant guidelines of the local authority and governing bodies where relevant and applicable.
The policy will outline:
• All recruitment and selection procedures.
• How references will be obtained.
• Disclosure and Barring Service (criminal record checks).
• Interview protocol.
• Training requirements.
• Appraisal and monitoring procedures.
• Formal complaints or grievance procedures.
• Responding to breaches of the codes of conduct; managing concerns about an individual.
• Dismissal.
Disclosure and Barring Service (DBS)
The Disclosure and Barring Service (previously known as Criminal Records Bureau or CRB and Disclosure Scotland and the Wales Council for Voluntary Action Criminal Records Unit or CRU) was set up by government to improve access to criminal record checks for organisations making decisions about the employment of staff and volunteers whose roles involve the responsibility for, or contact with, children, young people, and/or vulnerable adults.
If a centre knowingly appoints a person who is banned from working with children they will be committing a criminal offence, as will the individual concerned.
An employer may request a criminal record check processed through the DBS as part of its recruitment process. For certain roles the check will also include information held on the DBS’ children and adults barred lists, together with information held locally by police that is reasonably considered relevant to the post.
These checks assist employers in making safer recruitment and licensing decisions. However, a check is just one part of robust recruitment practice. When a check has been processed by the DBS and completed, the employer and individual will receive a DBS certificate.
KEY POINTIf an organisation knowingly appoints a person who is banned from working with children they will be committing a criminal offence, as will the individual applying for a role that involves working with children.
132 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: Safeguarding children and vulnerable adults

KEY POINTIt is not a fitness instructor’s responsibility to decide if abuse is taking place.
It is their responsibility to report any concerns to the appropriate agencies.
It is essential to take action in all instances!
Procedures to follow to protect oneself from accusations of abuseIt is important to follow the organisation’s procedures when working with children or vulnerable adults to promote the safety of the child or vulnerable adult and protect oneself from possible allegations of abuse.
The key is to avoid being placed in a vulnerable position where you may be susceptible to allegations.
• Always tell another person what you are doing and why.
• Always use appropriate language and behaviour (no hurtful or disrespectful comments, and no rough physical games).
• Never spend excessive amounts of time alone with one child or a vulnerable adult away from other people.
• Always remain in sight of other people (e.g. if taking the child or vulnerable adult to the toilet).
• Never offer to give a child or vulnerable person a lift home, if this would mean being alone with them.
• Never take a child or vulnerable adult to your home or office.
• Never reduce a child or vulnerable adult to tears as a way of control.
• Never let any allegations made by a child or vulnerable adult go unreported. All allegations should be investigated, recorded and acted upon.
• Record all incidents or allegations and ensure this is witnessed by another adult.
• Never take photographs (or allow photographs to be taken) of children and young people without gaining written permission from parents, carers and facility operators. For example, if considering taking photos of a group activity, all parents would have to give their written permission. Photography would be forbidden if even one parent refused to give consent. Most organisations have a policy for taking photographs of children and the staff are responsible for ensuring this is advertised and upheld.
Responding to and reporting suspected abuseIt is not always easy to recognise situations where abuse has taken place or is potentially likely to occur. Fitness instructors are not expected to be experts, but they have a responsibility to act if they have concerns about the safety of a child or vulnerable adult.
Concerns are likely to be raised if:
Abuse is observed, i.e. you witness bullying, harassment or physical abuse taking place.
Signs of abuse are observed.
Another person reports their concerns.
A child or vulnerable adult discloses abuse directly.
Copyright © 2014 Active IQ Ltd. Not for resale | 133
Section 4: Safeguarding children and vulnerable adultsH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

Responding to abuse
In all instances it is essential to take action. All concerns should first be reported to the organisation’s responsible person, e.g. the safeguarding officer or senior manager. Written records should support all concerns. If the type of abuse reported is a criminal offence, it must also be reported to the relevant statutory agencies, e.g. the police.
Recording information
When recording information you should:
Dealing with direct disclosure
A child or vulnerable person who is being abused will only tell people they trust and with whom they feel safe. Follow the organisation’s safeguarding guidelines and be aware of where to refer information; this would normally be the child protection officer or a senior manager.
Guidelines for responding to direct disclosure
• Listen and let the child or vulnerable adult speak.
• Stay calm, accept what is being said, avoid the need to judge (i.e. display shock or disbelief).
• Reassure them that they have done the right thing by telling you.
• Tell them that you take what they are saying seriously.
• Don’t promise to keep secrets.
• Be honest and explain that you will have to tell someone else to protect them.
• Don’t make them repeat the story, interrogate them or ask leading questions.
• Don’t tell people who do not need to know.
• Don’t approach the alleged abuser or the parents, guardian or carer.
• Record in writing the details of the individual, what has been said, heard or seen; include dates, times and a description of any visual bruising or injury and details of who has been informed and what action was taken in an incident report book.
• Maintain contact with the child or vulnerable adult if possible.
KEY POINTIt is not the role of the trusted person to investigate the disclosure, but they should gather enough information to pass on to the organisation’s responsible person, e.g. the safeguarding officer or senior manager and subsequently to the social services, if necessary.
1
2
3
Report the facts – what you have seen, heard or what has been reported or disclosed.
Not give your personal opinions; be clear when reporting your own or others’ interpretation of events and the reasons.
Clearly distinguish between what is your personal knowledge and what you have been told by others.
134 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: Safeguarding children and vulnerable adults

Statutory agencies responsible for safeguarding The statutory agencies responsible for safeguarding children and vulnerable adults are:
• Responsible persons in the workplace, i.e. safeguarding officer, child protection officers, appointed persons or senior management.
• Local safeguarding children boards (LSCBs).
• Independent safeguarding authority (ISA).
• Adult social care services (ASCs).
• Police.
• Social services.
• Child welfare agencies.
• Child welfare officers.
• Childline.
• NSPCC.
• Samaritans.
When it may be necessary to contact statutory agencies
Physical and sexual abuse are illegal. Allegations and concerns should be reported to the police who will investigate and decide whether to take criminal action. Other types of abuse, such as discrimination and financial exploitation, may also be considered to be criminal and these should be reported.
Maintaining confidentiality of information An instructor needs to maintain confidentiality, but does not need to take full responsibility for the process. This will be the responsibility of the responsible person, such as the safeguarding officer or senior manager. Key considerations are:
• Organisational procedures should be followed when reporting.
• Guidance from relevant legislation (data protection, information governance and sharing) should be adhered to.
• Information should only be shared on a ‘need-to-know basis’ with relevant people.
• The child or vulnerable adult’s confidence, safety and security must be assured; remember they will be the centre of the whole process.
• All written reports relating to the incident must be locked away securely; this includes the incident report form.
KEY POINTAll alleged criminal offences must be reported to the police.
Copyright © 2014 Active IQ Ltd. Not for resale | 135
Section 4: Safeguarding children and vulnerable adultsH
EALTH
, SAFETy A
nd
wELFA
RE In
A FITn
ESS EnVIR
on
MEn
T

End of section: Learning check Answer the following questions and make notes to revise this section.
• What is meant by safeguarding the welfare of children and vulnerable adults?
• At what age is a person considered to be a child in the UK?
• Which groups may be considered ‘vulnerable adults’?
• State two responsibilities and two limitations of a fitness instructor in regard to safeguarding.
• Give an example of each of the following types of abuse:
• Physical.
• Emotional.
• Neglect.
• Bullying.
• Sexual.
• What are signs of the following types of abuse?
• Physical.
• Emotional.
• Neglect.
• Bullying.
• Sexual.
• What procedures would you follow to protect yourself from accusations of abuse?
• What action would you take if a child directly disclosed physical abuse?
• Name three statutory agencies responsible for safeguarding children and vulnerable adults.
136 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: Safeguarding children and vulnerable adults

AimAn understanding of the principles of exercise, fitness and health is essential foundation knowledge for all fitness instructing disciplines.
Knowledge of the components of fitness, the effects that exercise has on the body, the training variables for programme design and methods for monitoring intensity will enable the fitness instructor to design safe and effective exercises for a range of clients.
Learning outcomesAt the end of this unit you will:
• Understand the components of fitness.
• Understand the effects of exercise on the body.
• Understand how to apply the principles and variables of fitness to an exercise programme.
• Understand the health benefits of physical activity.
• Understand how to safely monitor exercise intensity.
• Understand the exercise contraindications and key safety guidelines for special populations.
• Understand the importance of healthy eating.
PRINCIPLES OF EXERCISE, FITNESS AND HEALTH

Section 1: The components of fitness
The terms exercise, fitness, health and activity often mean different things to different people. To design a safe and effective exercise or activity programme to improve a client’s fitness or health, it is important to understand what each of these terms mean.
This understanding, as well as knowledge of the different components of fitness and factors affecting fitness, will help the fitness instructor to select and plan appropriate activities to achieve specific client objectives.
HEALTH-RELATED FITNESS
SKILL-RELATED FITNESS
Cardiorespiratory or cardiovascular endurance, muscular strength, muscular endurance, flexibility.
Speed, reaction time, agility, balance, coordination, power.
‘A state of wellbeing thatprovides optimal performance.’
Robergs and Roberts (1997)
‘Attributes related to how well one performs physical activity.’
McArdle et al (2001)
Figure 1.1 Definitions of physical fitness
KEY MESSAGE Encourage clients to move more often and sit down less.
KEY POINT Exercise can be differentiated from physical activity because it is planned, structured and targeted to improve specific components of physical fitness.
Inactivity and leading a sedentary lifestyle is a contributory risk factor for many chronic health conditions, including coronary heart disease, stroke, obesity, diabetes, depression and osteoporosis.
To maintain health it is recommended that all adults (aged 18 to 65) achieve the following activity guidelines as a minimum.
• 150 minutes of moderate-intensity aerobic activity every week (e.g. 30 minutes on five days a week. This can be accumulated in bouts of ten minutes).
• Or 75 minutes of vigorous-intensity activities (at least 20 minutes on three days a week).
• Or an equivalent combination of both moderate- and vigorous-intensity activities. • Plus at least two days a week of muscular strength and endurance training
(ACSM, 2014; Department of Health, 2011).
Exercise Exercise is a form of physical activity; it can be differentiated from ‘being active’ because it is planned, structured and performed regularly with the specific intention of maintaining or improving one or more of the components of physical fitness.
Structured exercise includes a wide variety of gym, studio, pool and outdoor activities. The volume of exercise needed to achieve specific fitness goals and improve or maintain specific components of fitness (health- or skill-related) is described in terms of frequency, intensity, time and type.
Physical fitnessPhysical fitness is a potential outcome from taking part in regular physical activity and exercise. Being physically fit defines an individual’s ability to perform activities or exercises that train different components of fitness, which may be:
Physical activity
Physical activity can be defined as any body movement that increases energy expenditure above resting levels. This would include:
• Everyday activities, e.g. climbing stairs or vigorous housework. • Active leisure and recreation, such as going to an exercise class. • Playing sport, such as badminton or football.
138 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The components of fitness

Being physically fit enables a person to carry out their daily activities and tasks with more vigour and energy and without excess stress or fatigue. An individual who is physically fit will have more energy and reserves to cope with the challenges of daily life.
Some clients will be seeking fitness related goals based on physical performance, e.g. to get stronger, run for longer, lose weight and gain muscle. Others may be looking to improve their general health and wellbeing, e.g. to reduce stress or tension, to reduce the risk of developing a chronic health condition, e.g. high blood pressure (hypertension), or to manage a health condition, e.g. low back pain.
Knowledge of the components of fitness and health helps the design and planning of an appropriate programme to support clients’ achievement of their unique goals.
MAKE A NOTEWhat is health? How would you define health?
PHYSICAL FITNESS
MENTAL AND EMOTIONAL FITNESS
MEDICAL FITNESS
NUTRITIONAL FITNESS
SOCIAL FITNESS
Total fitness, health and wellbeingHealth or total fitness is more than just being physically fit or medically healthy. It is a holistic concept that embraces a number of components that influence overall wellbeing:
• The wellbeing of the body systems, the heart, lungs, muscles, bones and joints. Health-related and skill-related components.
• The wellbeing of the mind; a positive mental state and harmony between the mind and emotions. Being able to manage stress.
• Being free from injury, chronic disease and illness.
• Having access to healthy food, eating a healthy diet, with a balanced nutritional intake for fuel, growth and repair.
• Having healthy interactions and relationships with others.
In 1948 the World Health Organisation defined ‘health’ as:
‘A state of complete physical, mental and social wellbeing and not merely the absence of disease or infirmity’.
This definition remains unchanged.
Copyright © 2014 Active IQ Ltd. Not for resale | 139
Section 1: The components of fitnessPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Figure 1.2 Total fitness
TOTA
L FI
TNESS
PHYSICAL FITNESS
MENTAL AND EMOTIONAL FITNESS
MEDICAL FITNESS
NUTRITIONAL FITNESS
SOCIAL FITNESS
HEA
LTH
-RELA
TED
FIT
NESS CARDIOVASCULAR FITNESS
MUSCULAR STRENGTH
MUSCULAR ENDURANCE
FLEXIBILITY
BODY COMPOSITION
Figure 1.3 Health-related fitness
Health-related physical fitnessThe main components of health-related physical fitness are cardiovascular or cardiorespiratory fitness, muscular strength and muscular endurance (sometimes referred to collectively as muscular fitness), flexibility and body composition.
AN INDIVIDUAL WHO IS PHYSICALLY ACTIVE MAY:
• Cope with stress more effectively (mental and emotional fitness).
• Meet new friends at their exercise sessions (social fitness).
• Reduce their cholesterol levels (medical fitness).
• Start eating more healthily (nutritional fitness).
REMEMBERThe cardiovascular system’s efficiency will be improved through regular aerobic training.
AEROBIC means ‘with oxygen’.
ANAEROBIC means ‘without oxygen’.
Cardiovascular fitness
Cardiovascular fitness is the ability of the heart, lungs and muscles to take in, transport and utilise oxygen during exercise. It is also referred to as cardiorespiratory fitness, stamina and aerobic fitness.
Cardiovascular activities increase the heart rate and breathing rate with the aim of increasing the blood flow and delivering more oxygen to the body to produce energy aerobically. When the pulse quickens and breathing gets deeper the cardiovascular system is working.
Activities that will improve the efficiency of the heart, lungs and circulatory system and improve cardiovascular fitness are those which use the large muscles of the body in a continuous and rhythmic way and which elevate the heart rate to an appropriate intensity (see Section 5). This includes walking, swimming, running, cycling, rowing and dancing.
Working with clients to improve physical fitness will be the main focus for a fitness instructor. However, many components are interrelated, so developments in one area may also have an impact on other components.
140 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The components of fitness

To improve cardiovascular fitness these activities need to be performed regularly (frequency), for an appropriate duration (time) and at an appropriate intensity. Table 1.1 provides the recommended training guidelines to develop cardiovascular fitness.
Frequency Three to five days a week.
Intensity Moderate to vigorous intensity. Heart rate reserve (HRR)• Moderate: 40-60% HRR.• Vigorous: 60-90% HRR.Maximal heart rate (MHR) • Moderate: 50-65% of MHR.• Vigorous: 65-90% of MHR. Rating of perceived exertion (RPE)• Moderate: 12-14 RPE. • Vigorous: 15-18 RPE.
Time 20-30 minutes or up 60 minutes of continuous or intermittent activity.• Moderate intensity: 30 minutes, which can be accumulated in bouts of 10 minutes or
more. • Vigorous intensity: 20 minutes sustained.
Considerations Untrained or deconditioned individuals will need to work towards these recommendations, they may require:• Lower intensities. • Shorter durations (accumulated approaches).
To minimise injury risk or repetitive strain:• Warm up before exercise and cool down after exercise. • Reduce the frequency if working at higher, more vigorous intensity. • Vary the type of activity.• Alter the impact.
• High-impact activity involves jumping or running actions, where the body weight is lifted away from the floor.
• Low-impact activity always maintains contact with the floor, e.g. squats or walking.
Table 1.1 Recommendations for cardiovascular exercise
THE LONG-TERM BENEFITS OF CARDIOVASCULAR TRAINING INCLUDE:
• The heart becomes stronger (cardiac muscle).
• More blood is circulated in one contraction or heart beat (increased stroke volume).
• More capillaries develop in the muscles.
• More oxygen can enter the muscles.
• Waste products can be removed more efficiently (carbon dioxide and lactic acid).
• More mitochondria (cells which use oxygen to create energy) develop in the muscles; they also grow larger.
• Weight management is assisted.
• Risk of cardiovascular disease (CVD) is reduced, e.g. coronary heart disease, stroke.
Copyright © 2014 Active IQ Ltd. Not for resale | 141
Section 1: The components of fitnessPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Muscular strength
Muscular strength can be defined as the maximal amount of force a muscle or group of muscles can generate during one contraction. It is the maximum weight a person could lift for one repetition maximum (1RM).
Strength-focussed activities require the lifting of heavier resistances or weights for a lower number of repetitions; usually fewer than ten repetitions. Examples of activities requiring maximal strength include heavy weight lifting and lifting or moving heavy objects.
Muscular strength is useful for two key reasons. First, the individual is able to produce a greater maximal force when required, e.g. lifting something heavy, such as moving a piece of furniture. Second, with enhanced levels of strength, everyday sub-maximal tasks require a smaller percentage of the individual’s maximal effort, which makes the task easier.
MUSCULAR STRENGTH High resistance. Low repetitions.
Muscular endurance
Muscular endurance can be defined as the ability of a muscle or group of muscles to contract repeatedly for extended periods of time without fatigue. The vast majority of everyday situations that require an individual to exert muscular effort and force also require muscular endurance.
MUSCULAR ENDURANCELower resistance. Higher repetitions.
Daily activities that require muscular endurance include carrying shopping, climbing stairs, maintaining optimal posture, gardening and exercise sessions involving high-repetition resistance training.
TYPES OF MUSCULAR STRENGTH AND ENDURANCE TRAININGResistance for muscular strength and endurance training may come from a range of different types of exercise. The resistance may include:• Body weight exercises, e.g. curl-ups, squats, back extensions, press-ups and various yoga postures and Pilates exercises.• Dumbbell exercises or exercises with resistance bands, e.g. bicep curls, shoulder press and lunges.• Fixed-resistance machine exercises, e.g. chest press, leg press and leg extension machines. • Free-weight exercises, e.g. bench press, squats and also group resistance training programmes, such as body pump.• Water-based resistance exercises, e.g. using water bells and floatation devices to provide resistance against the water.• Manual resistance (applied by a partner or an opposing limb).• Cable machines.
142 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The components of fitness

The strength and endurance continuum
Some exercises can be classified as strength-biased or endurance-biased, but it is often individual factors that determine whether a specific activity involves more strength or endurance.
A person who is only able to perform one press-up, for example, would be developing strength whereas a person who is able to perform lots of press-ups would be developing endurance. So strength or endurance bias will be determined by the individual and how hard the exercise is for them, which will influence the resistance they can lift and the number of repetitions they can perform (see figure 1.4).
Figure 1.4 Muscular strength and endurance continuum
STRENGTH
LOW REPETITIONS
HIGH RESISTANCE1-10 repetition maximum
LOWER RESISTANCE40-70% of repetition maximum (RM)
HIGHER REPETITIONS
ENDURANCE
Copyright © 2014 Active IQ Ltd. Not for resale | 143
Section 1: The components of fitnessPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

The recommended training guidelines (frequency, intensity, time) to improve muscular strength and endurance are provided in table 1.2.
Frequency Two-three days a week for each major muscle group on non-consecutive days. A rest of 48 hours between training sessions for any specific muscle group.
Intensity Percentage of one repetition maximum (1RM):• 40-50% of 1RM for older adults or sedentary adults. • 60-70% of 1RM for beginners. • > 80% of 1RM for experienced.
Time Session duration • No specific time recommended.Repetitions• 8-12 repetitions. • 10-15 repetitions for beginners. • 15-20 repetitions for endurance. Sets• Single sets effective for beginners or older adults. • 2-4 sets for adults. • < 2 sets is effective for endurance.Rest• Intervals or 2-3 minutes between sets.
Considerations Assessment of repetition maximum will need to be estimated for deconditioned clients and beginners.
Use correct posture and technique.
Use controlled movements through a full range of motion: • Isotonic muscle work (concentric-eccentric) works the muscle through full range of motion. • Isometric muscle work (static muscle contractions) strengthens the muscle in the position
held.
Aim for balance between muscle groups (muscles work in pairs):• Compound exercises work more than one muscle at one time, e.g. press-ups or squats. • Isolation exercises target single muscles, e.g. bicep curls.
Progress gradually to minimise delayed onset muscle soreness (DOMS).
Table 1.2 Recommendations for resistance
THE LONG-TERM BENEFITS OF MUSCULAR STRENGTH AND ENDURANCE TRAINING INCLUDE:
• Stronger muscles, tendons and ligaments.
• Stronger bones (increased bone density).
• Improved joint stability.
• Improved muscle tone, shape and physical appearance.
• Increased hypertrophy (muscle size) of type II fibres (strength-biased training).
• Improved body composition (muscle to fat ratios).
• Improved neuromuscular connections and motor unit recruitment.
• More capillaries in the muscles to deliver blood and oxygen (endurance training).
• Improved posture.
MUSCULAR FITNESS FOR ADULTS 2-4 sets of 8-12 reps per set.
Rest 2-3 mins between sets.
60-70% of 1RM for beginners.
MUSCULAR FITNESS FOR OLDER ADULTS OR DECONDITIONED1 set of 15 reps.
Moderate intensity (40-50% of 1RM).
144 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The components of fitness

Flexibility
Flexibility can be defined as the range of movement about a joint or series of joints. It is determined by the shape of the bones and cartilage and by the length of the muscles and connective tissues (ligaments and tendons) that cross over the joint. The amount of muscle tension is also affected by the nervous system, which determines muscle tone (tension).
ImmobilityA significant lack of flexibility can dramatically affect posture and force production at a joint and can impair performance and daily functioning. Inactivity can lead to muscle shortening and a loss of flexibility (e.g. sedentary living or when a body part has been immobilised in a plaster cast). Certain sports may reduce flexibility. For example, jogging, football, boxing and hockey all involve movements where muscles are not worked through their full range. This can lead to muscle tightness and adaptive shortening. Imbalanced exercise programmes that overdevelop one muscle group (prime movers) while neglecting the opposing muscle group (antagonists) can also cause muscle imbalances that restrict flexibility.
HypermobilityA high degree of flexibility or ‘hypermobility’ (sometimes erroneously referred to as being ‘double-jointed’) may lead to reduced joint stability and an increased incidence of injury. Some sports, such as gymnastics and martial arts, demand higher levels of flexibility.
Examples of activities that require flexibility include dance, yoga and daily activities that require the body to bend, twist and move through extended ranges of motion.
Flexibility can vary enormously from one person to another and is specific within individuals (see figure 1.5). It is important that individuals develop and maintain appropriate levels of flexibility to ensure an appropriate range of motion and freedom of movement at all joints.
Figure 1.5 The flexibility continuum
IMMOBILE STIFF JOINTS BALANCED FLEXIBILITY HYPERMOBILE
LESS STABLE JOINTS
Copyright © 2014 Active IQ Ltd. Not for resale | 145
Section 1: The components of fitnessPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Different methods and types of stretching
A muscle is lengthening and stretching when the two ends of the muscle (the origin and insertion) move further apart and away from each other. There are different ways of achieving this lengthening.
Active static stretchingActive stretching involves actively contracting one muscle or muscle group (agonist) to bring about a stretch of its opposing muscle group (antagonist).
Actively contracting the tibialis anterior, for example, will stretch the gastrocnemius and actively contracting the hamstrings will lengthen the quadriceps.
Passive static stretching Passive stretching is where another body part or external force (a yoga strap, wall or partner) is used to facilitate the stretch, enabling both the agonist and antagonist to relax. Passive stretching is used to increase joint range and muscle length.
Taking hold of the toe, for example, with the hand (or using a strap around the foot) will relax the tibilalis anterior and bring about a greater stretch of the gastrocnemius. Taking hold of the lower leg will enable the hamstrings to relax and bring about a greater stretch of the quadriceps.
Static stretching applications Active or passive static stretching is where the muscle is taken to the end of its normal range and held still for a specified duration. Static stretches can be used to lengthen muscles prior to exercise (consideration should be given to muscle temperature), maintain the existing range of motion and return the muscles to their normal length after they have finished working (at the end of a session) or to develop and improve flexibility.
TRAINER TIP A muscle is lengthening and stretching when the two ends of the muscle (the origin and insertion) move further apart and away from each other.
PARTNER STRETCHING A training partner can assist passive stretching by gently easing parts of their partner’s body into a stretch position. However, great care and effective communication are required to ensure the muscle does not overstretch.
Partner stretching is not recommended for beginners.
MAInTEnAnCE These are short stretches most appropriate for use in the warm-up or during the cool-down to maintain flexibility in muscles that are not particularly tight. The muscle is taken to the point of mild tension and held for 10-15 seconds.
dEVELoPMEnTAL These stretches are held for a longer period of time, typically 30-60 seconds. These can be used in the cool-down to improve the range of motion in areas of tightness and are not recommended during the warm-up phase. When the tension eases (stretch reflex relaxes) the stretch is taken further to increase the range of motion. This process can be repeated, moving a little further into the stretch when the muscle relaxes.
EXPERT TIP A total of 60 seconds stretching per muscle group is recommended. Stretches can be repeated two-four times to achieve this total, e.g. four 15-second stretches or two 30-second stretches.
Stretch to a point of mild tension or discomfort.
ACSM, 2014
The recommended training guidelines (frequency, intensity, time) to improve flexibility are provided in table 1.3.
146 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The components of fitness

Dynamic stretching techniques
Dynamic stretching Dynamic stretching, sometimes called range of movement stretching, moves the limbs to lengthen muscles to the end of their range of motion under control. There is no bouncing or jerking, which differentiates this method from ballistic stretching. Alternative dynamic stretching techniques may involve mimicking the movements to be performed in the activity or sport and may act as a kind of rehearsal during the warm-up. Around eight to ten repetitions of each movement are performed under control, gradually taking the stretch further to increase the range of motion.
FOR EXAMPLE: leg curls raising the heel to the buttocks to stretch the quadriceps, or pressing the arms back and opening the chest to stretch the pectorals and anterior deltoid.
Ballistic stretchingBallistic stretching involves quick, repetitive bouncing or bobbing actions at the end of the muscle’s normal range of motion. The momentum, speed and body weight involved in this type of stretching (bouncing at the end of the range), activate the stretch reflex (a safety mechanism to prevent overstretching) in the short term (causing the muscle to tense and contract to stop it exceeding the range of motion). This is counterproductive, as it shortens rather than lengthens the muscle.
In the long term, ballistic stretching may increase firing threshold of the stretch reflex to enable a greater range of motion. However, generally it is not advised for anyone, especially beginners or people with health-related goals, as the risk of injury is high and benefit is low compared to other stretching techniques.
FOR EXAMPLE: flexing from the hip to reach the toes and bouncing the body weight down.
This type of stretching can produce muscle soreness and even losses in resilience and elasticity. It is generally considered inappropriate for the average exerciser, due to the muscle and connective tissue damage that can occur as a result of forcing the joint beyond its current range of motion. Ballistic type stretches are sometimes used in physiotherapy and rehabilitation as a more radical method of breaking down adhesions and stubborn fibrous (scar) tissue.
Frequency > 2-3 days a week.Ideally every day.
Intensity To the point of mild tension and mild discomfort.
Time Static stretches 10-30 seconds.Older adults may benefit from longer durations. 2-4 repetitions of specific muscle stretches. PNF – static contraction for 3-6 seconds followed by 10-30 second static stretch. NB: A total of 60 seconds per muscle group is recommended. Stretches can be repeated 2-4 times to achieve this total, e.g. 4 x 15 seconds.
Considerations Ensure the body is warm before stretching. Lengthen all muscles before exercise (dynamic or static).Stretch all major muscle groups after work (static stretching – developmental or maintenance).Different methods of stretching may be appropriate for different groups. • Static – holding a stretch position.• Dynamic – controlled movement into a stretch position.• Proprioceptive neuromuscular facilitation (PNF) involves static (isometric) contraction and
then static stretch of a muscle group.• Ballistic – using momentum to stretch (must be performed safely, and for the appropriate
groups only, e.g. some sports).Avoid overstretching or exceeding the range of motion where mild tension is experienced as this may create DOMs.
Table 1.3 Recommendations for flexibility
Copyright © 2014 Active IQ Ltd. Not for resale | 147
Section 1: The components of fitnessPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

THE LONG-TERM BENEFITS OF FLEXIBILITY TRAINING INCLUDE:• Improved mobility for the joints and muscles. • Reduced muscle tension and tightness.• Improved physical and mental relaxation. • Improved range of motion. • More effective and efficient movements (ability to bend, stretch, lift, reach etc).• Improved posture. • Reduced risk of joint or muscle strains.• Reduced risk of low back pain. • Decreased delayed onset muscular soreness (DOMS) associated with other exercise activities.• Decreased muscle viscosity, enabling contractions to be easier and smoother.• Improved coordination by allowing for greater ease of movement.• Improvement and development of body awareness.
EXPERT TIPExcess body fat contributes to around 58% of cases of type 2 diabetes, 21% of heart disease and between 8% and 42% of certain cancers.
The point at which the level of body fat becomes a risk for health varies between ethnic groups.
NICE, 2013
Body composition
Body composition describes the percentages of fat, bone and muscle in human bodies. The body fat percentage is of most interest because it is used as a measure of health.
Two individuals may be of equal weight and height, but their body composition and appearance may be totally different. Muscular tissue takes up less space in the body than fat tissue and this influences how lean people appear.
WEIGHT 150 KG HIGHER % OF BODY FAT NON-EXERCISER
WEIGHT 150 KG HIGHER % OF MUSCLE ATHLETE OR BODY BUILDER
Body fat percentages viewed as satisfactory for optimal health are:
MEN
WOMEN
10-22% of total body weight.
20-32% of total body weight.
(ACSM, 2014)
The point at which body fat becomes a risk for health varies between ethnic groups and age groups (NICE, 2013). Generally speaking, levels significantly above the percentages stated may indicate excess body fat. Many athletes and sports people have a body fat percentage lower than the levels stated (depending on the sport). Performance in many sports will be enhanced when body fat percentages reach 7%-19% for men and 10%-25% for women.
148 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The components of fitness

The components of skill-related fitness
There are six components of skill-related fitness.
SpeedSpeed defines how quickly a movement can be performed in a short space of time. Speed is required for many sporting events, including sprinting and throwing.
PowerPower is the ability to exert maximum muscular contraction instantly in an explosive burst of movement (in a short timeframe). The two components of power are strength and speed. Sporting activities requiring power include jumping (high jump or long jump), throwing (shot put or javelin), and sprinting out of the starting blocks (a sprint start).
Reaction timeReaction time is the ability to respond quickly to a stimulus. It is important in many sports and day-to-day activities. ‘Simple reaction time’ is the time taken between a stimulus and movement, e.g. a sprint start.
1
2
3CoordinationCoordination is the ability to smoothly move two or more body parts under control, accurately and efficiently. It involves use of the senses (eyes and ears). Most activities require coordination, albeit different types of coordination, these include performing choreography and dance or gymnastic routines, throwing, catching (eye to ball coordination), kicking and hitting (e.g. golf swings, kicking a football).
BalanceBalance is the ability to control the body’s position when stationary (e.g. a handstand or a yoga posture) or while moving (e.g. a spring board diver during take-off).
AgilityAgility is the ability to change the position of the body quickly and move in different directions quickly, e.g. zigzag running and moving through and around a field of players in team sports.
4
5
6Training to improve motor fitness or neuromuscular fitness depends on which component an individual wants to improve and for what purpose, e.g. to play a particular sport or improve function of daily activities, such as reducing the risk of falls in older adults. Activities that improve different components are very specific; improving balance will require different activities to those required to develop power.
Copyright © 2014 Active IQ Ltd. Not for resale | 149
Section 1: The components of fitnessPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Table 1.4 outlines the recommendations for improving motor fitness.
Frequency Two-three days a week.
Intensity Not specified.
Time 20-30 minutes.
Type Balance, agility, speed, power, coordination, gait.
Tai chi and yoga are recommended for older adults (to reduce risk of falling in those at risk).
Considerations Which component or components? What is the purpose (e.g. functional or sport related)? What is the current ability of the individual, e.g. deconditioned or sports person?
Other components of fitness may be involved at the same time (e.g. power requires muscular strength) and there may be physiological considerations (48 hours’ rest between work of same muscle group).
Table 1.4 Recommendations for neuromuscular training
Factors that affect health and skill-related fitnessThere are many factors that influence an individual’s health, fitness and training potential. These include factors specific to the individual (e.g. age, gender) and also more general factors, such as the environment, weather and temperature.
AGE
The body changes throughout a lifetime. During formative years, when the body is growing, consideration will need to be given to the effects of exercise on the developing bones, muscles and other body systems.
A person’s fitness is generally greatest during their twenties and declines with age. For older adults the changes to the body systems, which progressively result in weaker muscles, lighter bones, stiffer joints, slower reflexes and an increase in body fat, will reduce training potential. Benefits can still be achieved, but the rate at which developments occur will be slightly slower. Age-related changes generally begin to occur at the age of 50 and make their mark at around 65. The onset of the ageing process and the rate of decline are influenced (and can be offset) by regular physical activity and exercise.
Age and flexibility: people are usually more flexible when they are younger. Babies and infants are very flexible and start to lose this natural flexibility as soon as they start to walk (when the joints become weight-bearing and need more stability). As people get older, muscle contractility remains, but elasticity is lost; resulting in tighter, stiffer muscles. This may also be influenced by activity levels, which tend to decrease as people get older.
Activity levels and age: activity levels also reduce progressively with age in both men and women. An estimated 40% of older men and 58% of older women (over 50) are classed as being inactive. At the age of 75 it is estimated that only 8% of men and 3% of women meet the recommended activity guidelines (Department of Health, 2011). Reduced activity levels can lead to a loss of mobility, loss of independence and increased isolation.
There are a number of anatomical and physiological differences between men and women that influence their training potential. Throughout childhood and up to adolescence males and females tend to have equal levels of general fitness. Specific gender-related changes occur at puberty.
150 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The components of fitness

GENDER
Hormones: increased levels of testosterone during puberty mean that active males grow stronger due to their greater muscle mass.
Cardiovascular potential: males are generally larger than women. They have longer bones, larger muscles, larger hearts and larger lungs which gives them greater potential for transporting oxygen and developing their cardiovascular fitness.
Body composition: males generally have a lower percentage of body fat and higher levels of muscle than females. Females need higher levels of body fat to equip them for pregnancy and childbirth. Reducing body fat below recommended levels would reduce levels of the female hormone (oestrogen) and may cause the cessation of the menstrual cycle. This in turn would contribute to lower levels of calcium in the bones and may increase the risk of osteoporosis in later life.
Skeletal frame: the female pelvis is wider and deeper in order to support pregnancy and childbirth. The Q angle (quadriceps angle) of the female pelvis is also greater, which gives women a biomechanical disadvantage when running or squatting. It also leads to an inward rotation of the knees. These differences may also influence running speed; females have to move their legs through a wider angle, which potentially reduces speed.
Gender and flexibility: females of all ages tend to be more flexible than males. This may be due to specificity of training they take part in, but may also be attributed to structural and anatomical differences.
HEREDITY
An individual’s health, physical appearance and training potential are all influenced largely by genetic characteristics inherited from their parents.
Physically inherited characteristics may include eye colour, skin colour and hair texture. They may also include things like body type and muscle fibre type, which will have a greater influence on training potential. An individual who inherits an ectomorphic body type and a larger percentage of slow twitch muscle fibres will be more suited to long-distance endurance activities than an individual who inherits a mesomorphic body type and a greater percentage of fast twitch muscle fibres. Training potential and goals need to be considerate of inherited characteristics.
Various health conditions are believed to have a genetic (family) risk component (e.g. cardiovascular disease).
Heredity and flexibility
Some people are born with a naturally greater (sometimes excessive) range of motion (ROM) known as hypermobility (sometimes called being ‘double-jointed’, which is inaccurate). Hypermobility can create a greater potential for injury (i.e. joint dislocation) and it may be necessary to concentrate on strengthening the muscles acting over the joint to increase stability.
Heredity and progression
Each individual has a genetic potential that defines how far their fitness could progress if training, nutrition and recovery were optimised.
The deconditioned novice has a large potential because they are starting from a point far below their genetic limits. As a result of this and their unfamiliarity with the exercise stimulus, almost any programme will work for an untrained individual (Fleck and Kraemer, 1997). This adaptation potential enables beginners to initially make rapid progress in the early stages of their training. Over time, and as they get closer to their genetic potential, the rate of progress will slow down.
Copyright © 2014 Active IQ Ltd. Not for resale | 151
Section 1: The components of fitnessPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

PHYSIQUE/BODY TYPE
An individual’s body type has a significant impact on their ability to perform various physical tasks successfully, e.g. a tall, thin person may be more suited to basketball than rugby.
A simple system for visually assessing body type is the system of somatotyping. The somatotyping system suggests that there are three distinct body types: ectomorph, endomorph and mesomorph.
EctomorphsEctomorphs are naturally thin with little body fat or muscle mass. They find it difficult to gain weight (either muscle or fat). They have long levers and light body frames, which make them more suited to weight-bearing aerobic activities, such as long-distance running. Their light body frame means there will be comparatively less body weight being borne by the joints.
MesomorphsMesomorphs tend to be naturally lean and muscular with broad shoulders and narrow waist and hips. Mesomorphs are naturally athletic and tend to be suited to a wide variety of sporting activities, especially those requiring a good power-to-weight ratio, e.g. sprinting, hurdling and jumping. High levels of muscle mass may reduce their potential to float in water.
EndomorphsEndomorphs are naturally predisposed to fat storage. They tend to be apple or pear shaped and carry larger amounts of body fat. Endomorphs also tend to possess a reasonable degree of muscle mass, but this is often overlooked due to the predisposition for fat storage. Higher levels of body fat increase their potential to float in water, but also place additional stress on the weight-bearing joints during high-impact and weight-bearing activities. Endomorphs may be suited to activities such as the shot put or hammer throwing.
Awareness of body types may be useful when discussing client objectives. An endomorph with a goal of becoming a competitive marathon runner, for example, may need to re-evaluate this objective as they are not structurally suited to this type of activity. Similarly, ectomorphs are unlikely to succeed in competitive bodybuilding, as they have difficulty gaining muscular size. Any discussions about the suitability of certain activities should always be conducted with sensitivity.
ACTIVITY LEVEL
Inactivity and sedentary living offer an increased risk of poor health. Regular non-structured physical activities, such as walking the dog, cycling and gardening can make significant improvements in maintaining health if performed on a daily basis. The key message from the Department of Health (2011) is to sit down less and move more often.
Active people and people who exercise regularly generally have greater mobility and flexibility than sedentary individuals. This may depend on the type of exercise and activity they perform, e.g. performing lots of resistance training exercises with a limited range of motion and higher loads may actually decrease range of motion.
BODY TYPEMost individuals are not exclusively one body type, but rather a combination, usually with a bias toward two types, e.g. ectomorph/mesomorph (taller, lean and muscular) or endomorph/mesomorph (shorter, rounder and muscular).
Figure 1.6 Ectomorph, mesomorph, endomorph
152 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The components of fitness

DIET
The body needs specific nutrients for energy, growth and repair. These nutrients are provided by the food eaten in the diet. A healthy, balanced diet will help to ensure that the body is functioning optimally. An unhealthy or imbalanced diet may negatively affect health and increase the risk of cardiovascular disease, diabetes, obesity and other chronic health conditions (see Section 7).
PHYSICAL DISABILITIESPeople with disabilities are able to exercise and do not have to be inactive. A physical impairment may prevent a specific part of the body functioning or moving in a certain way, but exercise can be adapted and modified to enable participation, promote inclusion and improve health and fitness. Many disabled people are first-class athletes.
ILLNESS AND FATIGUEDuring temporary illness (colds or flu) the recommendation is to rest the body rather than exercise. Exercising with a fever (febrile illness) is contraindicated and places stress on the body systems. All clinical symptoms should have passed before returning to exercise and it may be necessary to start at a lower level before building up.
When the body is tired (through working too hard or insufficient rest between sessions) performance diminishes and this may hinder potential training gains. It may be necessary to review training plans and also eating behaviour to balance energy requirements.
Chronic health conditions also affect exercise potential and require exercises to be modified prior to participation. A client who is obese, for example, may need to perform low-impact or non-weight-bearing activities, e.g. swimming or cycling. A client with high blood pressure may need to exercise at a lower intensity.
NB: Clients with chronic health conditions should be supervised by an appropriately qualified (Level 3 Exercise Referral) instructor.
DRUGSPrescribed and recreational drugs (alcohol, nicotine, caffeine and illegal substances) will affect exercise and fitness potential.
Prescribed medications used to treat chronic health conditions often have side effects that influence the exercise response. Clients using prescribed medication should be supervised by an appropriately qualified instructor.
Recreational drugs (alcohol, nicotine and caffeine) all have negative effects on health and have an impact on exercise performance.
Cigarettes contain carbon monoxide, which reduces the potential to take in and use oxygen. Alcohol affects the nervous system, disrupting balance and coordination, which reduces the safety of exercise; especially if using equipment. Caffeine is a stimulant and may offer a short-term boost to performance. However, in the long term, excess caffeine can contribute to health conditions including increased blood pressure, anxiety, depression and osteoporosis.
STRESSHigh levels of prolonged stress can lead to many other chronic health conditions including high blood pressure, coronary heart disease and depression. It will have negative impact on the person’s overall wellbeing and enjoyment of life.
Exercise and activity can assist with stress management. It provides an outlet for managing the physical tension caused by stress and a distraction for the mind, which can reduce mental strain. Exercise in the outdoors and in natural environments can have further positive benefits on mood and wellbeing.
Copyright © 2014 Active IQ Ltd. Not for resale | 153
Section 1: The components of fitnessPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

End of section: Learning check Answer the following questions and make notes to revise this section.
• Explain what is meant by the following terms: • Physical activity.• Exercise.• Health. • Fitness.
• Name the different components of health or total fitness.• How may physical fitness influence the other components of total fitness or health?• Name the five components of physical or health-related fitness. • Define the terms aerobic and anaerobic. • Give an example of one low-impact cardiovascular activity. • Give an example of one high-impact cardiovascular activity. • What are the recommended guidelines to improve cardiovascular fitness? • What does FITT stand for? • What is the difference between muscular strength and muscular endurance?• What are the recommended guidelines to improve muscular strength and muscular endurance? • What does RM stand for in relation to muscular fitness training? • What does DOMS stand for? • What is flexibility? • What are the recommended guidelines to improve flexibility? • What is body composition? • Name the six components of skill-related fitness. • Describe two factors that will affect a person’s training potential.• Name the three main body types.• How could heredity affect fitness and health?• How might age affect fitness and health? • How might body type affect fitness and health?
ENVIRONMENT AND WEATHERExercise safety can be affected by the environment. The quality of the air taken in will determine the amount of oxygen that can be utilised. Aerobic fitness can be significantly influenced by the following environmental factors:
• Fumes from traffic and factories.• Altitude, i.e. air is thinner at high altitudes and individuals need to breathe harder to get enough
oxygen.• Weather, i.e. temperature and humidity.
The weather and temperature may also affect exercise patterns. Some people may use poor weather conditions (e.g. snow, rain, heat) as a reason not to exercise. In most weather conditions and temperatures exercise may need to be modified; in hot temperatures intensity may need to be reduced. In cold environments it may be necessary to lengthen the warm-up and wear additional clothing to prevent heat loss or wind chill.
PREGNANCYDuring both the pre- and post-natal periods there are significant changes to the female body that affect exercise potential.
During pregnancy women produce excess amounts of a hormone called relaxin to assist the birth process. Relaxin affects the ligaments of the pelvis and will also affect other ligaments allowing greater flexibility than normal and potentially reducing joint stability.
154 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: The components of fitness

Section 2: The effects of exercise on the body
Exercise provides a stimulus to the body and the body responds to this stimulus. In the short term different body systems (heart, lungs, muscles, etc.) respond to help the body cope with the immediate demands of exercise. In the longer term the body will gradually respond to repeated demands by adapting physiologically, so it is better able to cope the next time the stimulus is provided. Different types of exercise for the different components of fitness provide specific stimuli and the body will adapt to these demands.
Cardiovascular and respiratory adaptations to endurance/aerobic training
Immediate effects of cardiovascular exercise
In a healthy and trained individual the immediate response to exercise will be efficient and effective because many of their body systems will be developed. They are better equipped to deliver oxygen to the working muscles.
In an untrained individual the body systems will be less efficient and the short-term responses may be more acute; they are not so well equipped to deliver oxygen and as a result may produce energy anaerobically (unless the activity is of an appropriate and much lower intensity).
This will have a significant impact on how individual training sessions are designed – the intensity, type and duration of activities. It will also affect how the programme progresses over time – the volume of exercise and rate of progression.
FOR A TRAINED PERSONThe heart will start to beat at a faster rate and more blood will be pumped to the working muscles. The breathing rate will also become faster and deeper, and more oxygen will enter the body. At a muscular level, the capillaries will dilate (widen) to allow more blood to enter the muscle. Oxygen will be delivered and used to create energy and waste products (lactic acid) will be removed from the muscle.
FOR AN UNTRAINED PERSONThe heart will need to beat much faster to supply the same volume of blood, placing the heart under greater stress; the breathing rate will be higher, in an attempt to get more oxygen into the body. At a muscular level, there will be fewer capillaries, so less oxygen can get into the muscle, contributing to futher increases in heart rate and breathing rate and eventually, uncomfortable waste products, like lactic acid or carbon dioxide will build up, so that person has to stop or slow down.
Copyright © 2014 Active IQ Ltd. Not for resale | 155
Section 2: The effects of exercise on the bodyPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

The long-term adaptation of the cardiovascular system to aerobic exercise
In the long term the cardiovascular system will adapt to ensure that it is able to cope with aerobic endurance exercise. Some of the adaptations which help the cardiovascular system cope and work more efficiently are listed in table 2.1.
HEART AND LUNGS BLOOD VESSELS AND MUSCLES
Heart • Increased size of heart muscle (left
ventricular hypertrophy).• Increased strength of contraction (stronger
heart).• Increased stroke volume (more blood
ejected in one contraction/heart beat).• Increased cardiac output (more blood
ejected in a minute).• Decreased working heart rate at a given
intensity. • Higher working threshold before
accumulation of lactate (anaerobic work).• Reduced resting heart rate.• Decreased risk of cardiovascular disease. Lungs• Increased functional capacity during
exercise.• Improved gaseous exchange (diffusion of
respiratory gases).• Increased vital capacity.• Increased maximal O² uptake (VO² max).
Blood vessels• Increased blood vessel size.• Reduced resting systolic and diastolic blood pressure (SBP
and DBP).• Favourable change in blood lipids (increased high density
lipoprotein and reduced low density lipoprotein and triglycerides).
• Increased haemoglobin.• Increased blood volume.Muscles • Increased capillaries in the muscles enabling transport of
oxygen and removal of waste products. • Increased enzymatic function within muscle cells.• Increased size and number of mitochondria (for aerobic
energy production).
Wilmore and Costill, 1999; ACSM, 2014.
Table 2.1 Long-term cardiovascular and respiratory adaptations to endurance/aerobic training
• Improved self-mastery.• Increased social interaction.• Distraction from the daily
routine.• Decreased depression and
anxiety.• Improved cognitive function. • Enhanced sense of wellbeing.
PSYCHOLOGICAL BENEFITS INCLUDE:
• Reduced insulin needs and improved glucose tolerance.
• Decreased insulin resistance.
• Reduced total body fat. • Reduced intra-abdominal
fat.
METABOLIC BENEFITS INCLUDE:
Other advantages of aerobic endurance training include metabolic and psychological benefits.
156 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: The effects of exercise on the body

Effects of aerobic exercise on blood pressure
OPTIMAL BLOOD PRESSURESystolic < 120mmHgDiastolic < 80mmHg
BLOOD PRESSURE
SYSTOLIC The contracting and pumping phase of the cardiac cycle.
DIASTOLIC The resting phase of the cardiac cycle, when the heart is filling with blood.
TRAINER TIPTo minimise the effects of blood pooling: 1. Cool down
thoroughly. 2. Keep the legs
moving during higher-intensity activities, e.g. pedal the feet.
Blood pooling
During cardiovascular exercise the heart rate increases and there is an increased flow of blood to muscles. Venous return (the return of blood to the heart and brain) is maintained mainly by the increased pumping action of the muscles (the muscles contract and squeeze the blood vessels, assisting the return of blood).
If the activity stops suddenly the heart will continue pumping blood around the body at the exercising rate, but without the muscular pumping action to assist venous return. Veins do not have the same level of muscularity as arteries, so without assistance from the muscles the extra blood will begin to build up or ‘pool’ in the extremities (particularly the legs). This effect is known as ‘blood pooling’.Common symptoms of blood pooling are nausea, dizziness and even fainting if insufficient blood flow reaches the brain.
Long-term effects
Aerobic exercise can reduce resting systolic and diastolic blood pressure (ACSM, 2014). It can elicit an average decrease of 10 mmHg in both systolic and diastolic blood pressure in individuals with mild and moderate hypertension (Durstine and Moore, 2003).
Heavy strength or resistance training (with the exception of circuit weight training) has not consistently been shown to lower resting blood pressure (Durstine and Moore, 2003). Resistance training can have many benefits, but it is not recommended on its own as a means of decreasing blood pressure.
Aerobic exercise also has an effect on blood pressure. The immediate effect is an increase in blood pressure. Individuals who already have high blood pressure (hypertension) will need a longer and more gradual warm-up to prepare them for exercise and will need to exercise at a lower intensity to ensure any increase does not place the body under too much stress. In the longer term exercise may have a positive and normalising effect on blood pressure (ACSM, 2014).
Short-term effects
There is a linear increase in systolic blood pressure (SBP) with increasing levels of exertion. Higher exercise intensity results in a greater increase of SBP.
Diastolic blood pressure (DBP) will usually remain unchanged or may decrease slightly during exertion due to vasodilation. In individuals with hypertension DBP may also rise as a result of an impaired vasodilatory response (Gordon, 1997).
Some types of exercise, e.g. heavy weight training and isometric exercise, will significantly increase both systolic and diastolic blood pressure. It may be better to avoid these activities with individuals who have hypertension, as the risks would potentially outweigh any benefits.
To reduce the effects of blood pooling it is essential to cool down thoroughly. The heart rate should be gradually reduced, so that the volume of blood circulated is reduced before exercise is stopped. This will also reduce any stress on the heart muscle.
During higher-intensity exercise it is important to keep the legs moving. Pedalling the feet and marching will maintain the muscle pumping action and assist the return of blood in the veins.
Copyright © 2014 Active IQ Ltd. Not for resale | 157
Section 2: The effects of exercise on the bodyPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Effects of exercise on the muscular and skeletal systemsRegular exercise also has a positive effect on the muscular and skeletal systems. Muscular strength and endurance training and flexibility training will offer specific beneficial effects.
Short-term effects – bones and joints
When the freely movable joints of the body start to move synovial fluid is released into the joint capsule. This acts as a lubricant enabling the joint to move more easily, which can help to protect the joint from excess wear and tear.
The temperature of the muscles around the joints will increase, making them more pliable and elastic. These effects improve the mobility of the joints, enabling them to move through a greater range of motion and with greater ease.
Long-term adaptations – bones and joints
In the long term the release of synovial fluid into the joints may become more efficient. Trained individuals may require less focus on specific mobility exercises than a deconditioned individual because their joints move more easily (and are less stiff) and they may have a greater starting range of motion.
Joint stability will also improve in the long term. The ligaments and tendons will become stronger, giving greater protection to the joints against risk of injury.
TRAINER TIPMobility exercises form part of the warm-up.
Individuals with mobility conditions (e.g. arthritis) will benefit from additional mobility exercises that move the joints through their full potential range of motion.
TRAINER TIPWeight-bearing exercises, such as walking, can help to reduce the loss of bone mass associated with ageing. They can help to reduce the risk of osteoporosis.
Adaptations to weight-bearing activities
Weight-bearing activities are those in which the body weight is borne by the muscles and joints, e.g. standing, walking, climbing stairs, resistance training, squatting, press-ups, running, jumping and hopping.
Weight-bearing exercises demand greater effort from the muscles to resist the forces of gravity. In the long term they will help to reduce the loss of bone mass associated with ageing (reducing the risk of osteoporosis) and can increase bone density, keeping the bones strong and healthy.
Non-weight-bearing activities are those in which all or most of the body weight is supported, e.g. swimming or aqua aerobics, chair-based exercise and (to some extent) seated cardiovascular exercises like cycling which require less weight bearing. Non-weight-bearing exercise provides additional support for the body weight and reduces the stress on the joints, which can be particularly beneficial for individuals who are overweight or have injuries or mobility related conditions, such as osteoarthritis or rheumatoid arthritis.
158 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: The effects of exercise on the body

The short- and long-term effects of exercise on the muscular system
Delayed onset of muscular soreness (DOMS)
DOMS The pain, soreness or stiffness in muscles typically experienced between 12-72 hours after exercise (one-two days after a training session).
Delayed onset of muscular soreness (DOMS) is the name given to the pain, soreness or stiffness in muscles typically experienced 12-72 hours after exercise.
It is particularly common following the beginning of a new exercise programme, e.g. when someone who has been inactive for a long time starts exercising. It is also likely to be experienced if the activity involves lots of eccentric muscle work and loading, e.g. going down stairs, running downhill, downward motion of squats or lunges (like in a game of squash); especially if the action is unfamiliar.
DOMS may also occur when there is an increase in exercise intensity, e.g. if an exercise is progressed and made harder.
Long-term effects and benefits of resistance training on the muscles
Resistance training exercises specifically improve muscular strength and endurance and offer numerous benefits to the muscles as well as the bones. Some of the many benefits, depending on the type of training (strength or endurance), include:
• Increased strength, power or muscular endurance (depending on the type of training).• Increased muscle size and strength; hypertrophy of type II muscles fibres (hypertrophy or strength
training).• Increases in contractile proteins (actin and myosin).• Stronger connective tissues (tendons and ligaments).• Increased number and size of mitochondria in the muscle fibres (aerobic endurance training).• Increased number of capillaries surrounding the muscle fibres (aerobic endurance training).• Increased number of aerobic enzymes, stored glycogen and triglycerides in the muscle fibres (aerobic
endurance training).• Increased glycolytic activity of the muscle allowing more work to be performed under anaerobic
conditions or high-stress conditions (hypertrophy or strength training).• Improved neuromuscular connections. • Increased motor unit activation and recruitment.• Increased discharge (nerve impulses) frequency of motor neurons (nerve cell).• Decreased neural inhibition (muscles’ protective braking mechanisms).• Slightly increased stores of adenosine triphosphate (ATP) and creatine phosphate (CP).• Increased testosterone and growth hormone. • Improved body composition; potential increase in fat-free mass/muscle mass and decrease in fat mass
and relative body fat percentage.• Increased metabolic rate.• Increased range of motion if exercises are performed through a full range of movement.• Improved posture; balanced strength between opposing muscles.
The exact mechanisms that cause DOMS are not fully understood, but it is thought to be triggered by exercise-induced muscle damage (micro tears in the muscle) followed by an inflammatory response (a small bleed in the muscles that aggravates the nerves and causes pain).
Copyright © 2014 Active IQ Ltd. Not for resale | 159
Section 2: The effects of exercise on the bodyPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Table 2.2 outlines specific effects of different types of resistance training.
TRAINING METHOD ADAPTATION OF MUSCLE AFTER EXERCISE
Aerobic endurance training(Long duration repeated contractions using bodyweight load or lower resistance.)
Increased mitochondria size and number, greater stores of glycogen, increased aerobic enzymes, hypertrophy of type I fibres only, possible atrophy of some type II fibres.
Muscular endurance training(Resistance training, 13+ reps, 2-3 sets, 30-60 seconds’ rest.)
As above plus increased anaerobic enzymes and improved lactic acid tolerance and removal.
Hypertrophy training(Resistance training, 6-12 reps, 3-6 sets, 60-120 seconds’ rest.)
Increased cross-sectional diameter of fibres (type I and II) and intracellular volume. Increased glycogen storage. Increased anaerobic lactic acid system enzymes. Improvement in lactic acid tolerance and clearance.
Strength training(Resistance training, 1-5 reps, 2-6 sets, 3-5 minutes’ rest.)
Increased muscle size, but to a lesser extent than hypertrophy training. Great improvement in neuromuscular firing through reduced firing threshold. Increased creatine phosphate and free creatine stores and enzymes for the phosphocreatine system.
Power training(Plyometric drills or explosive heavy lifting guidelines, as per strength training, but performed at maximal speed.)
As above. Neuromuscular coordination is even more significant than intramuscular adaptations.
Table 2.2 Effects of different types of resistance training
Long-term effects and benefits of flexibility training on muscles
The long-term effects of flexibility and stretching exercises include:
• Reduced muscle tension and tightness.
• Improved muscle length.
• Improved range of motion.
• Improved posture if muscle tightness and restrictions are reduced.
• Reduced risk of joint or muscle strains; flexible muscles can move to greater range of motion with reduced risk of injury.
• Reduced risk of back problems.
• Decreased muscular soreness (DOMS) associated with other exercise activities.
• Decreased muscle viscosity causing contractions to be easier and smoother.
• Improved coordination by allowing for greater ease of movement.
• Improvement and development of body awareness.
160 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: The effects of exercise on the body

Improving postureA balance of muscular strength and flexibility is required to improve posture. Muscles work in pairs and an imbalance of strength and length between the pair will be reflected in a change of posture and alignment.
Modern lifestyles often involve sitting for long periods of time, e.g. using a computer or driving. This can lead to weakness and lengthening of some muscles and shortening and loss of flexibility in others, which can result in postural changes that may lead to decreased function and increased risk of injury, pain and discomfort.
Other factors that may contribute to changes in posture include age, fashion, sport and confidence.
Carrying a bag on one shoulder can cause adaptive shortening of the muscles on one side of the body (scoliosis or a lateral spine curvature). Wearing high-heeled shoes will change the centre of gravity and balance and cause shortening of the gastrocnemius muscle.
FASHION
Sports can develop some muscle groups more than others, creating imbalances that lead to postural changes, e.g. racket sports (single arm strengthening) and cycling (flexed posture).
SPORT
People who lack confidence tend to have a more hunched and closed posture.
SELF-ESTEEM AND CONFIDENCE
Loss of bone mass can lead to osteoporosis, degeneration of vertebral discs can lead to arthritis and, if the spine is affected, this can contribute to a loss of mobility and kyphotic posture. This posture type can increase the risk of falls in frailer older adults.
AGE
Optimal posture
Correct posture and alignment, both static and dynamic, are essential for safe and effective exercise.
Optimal posture can be observed by viewing a client standing side-on and visualising an imaginary plumb line falling vertically from the top of the head to the feet (see figure 2.1). In optimal posture the plumb line would align through the following points:
• Crown of the head.
• Ear lobe.
• Bodies of the cervical vertebrae.
• Middle of the tip of the shoulder (acromion process).
• Divide the thorax (ribcage) in half (equally, back to front).
• Bodies of the lumbar vertebrae.
• Slightly posterior to the hip joint (greater trochanter – projection on the lateral femur).
• Slightly anterior to the axis (mid-point) of the knee joint.
Copyright © 2014 Active IQ Ltd. Not for resale | 161
Section 2: The effects of exercise on the bodyPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Figure 2.1 Optimal posture
oPTIMAL PoSTURE InSTRUCTIonS
• Head aligned equally between shoulders, without poking forward.
• Chest open and shoulders not rolling forward.
• Shoulder blades, scapulae neutral and slide down towards buttocks, not lifted.
• Neutral spine, maintaining natural S curves.
• Pelvis neutral, without anterior or posterior tilt.
• Knees straight but unlocked.
• Feet neutral, under knees and hips, without rolling inwards or outwards.
Exercising to improve posture
Exercise to improve posture will be dependent on the postural deviation. A balanced approach to muscular strengthening and stretching is required. It is also important to encourage correct posture whenever standing and seated. Table 2.3 outlines some of the muscles that may need to be strengthened or lengthened for specific posture types.
POSTURE TYPE STRENGTHENING STRETCHING AND MOBILITY
Kyphosis or hyperkyphosis
• Strengthen lower and middle trapezius.
• Strengthen rhomboids.
• Lengthen pectorals, anterior deltoid and upper trapezius.
• Mobilise thoracic spine.
Lordosis or hyperlordosis
• Strengthen abdominal muscles (rectus abdominis, external obliques).
• Strengthen deep core stabilisers (transversus abdominis).
• Lengthen hip flexor and spine extensors (erector spinae).
• Mobilise spine, especially flexion.
Flat back • Strengthen deep core stabilisers (transversus abdominis).
• Mobilise spine, especially extension. • Stretch hamstrings and rectus abdominis.
Table 2.3 Muscles to strengthen and stretch to improve specific posture types
162 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: The effects of exercise on the body
oPTIMAL PoSTURE
THROUGH EAR LOBE
THROUGH THE GREATER TROCHANTER
SLIGHTLY ANTERIOR TO THE AXIS OF THE KNEE
SLIGHTLY ANTERIOR TO THE LATERAL MALLEOLUS
THROUGH THE AXIS OF THE SHOULDER

These include:
HYPERKYPHOSIS OR KYPHOTIC POSTURE – an exaggerated curve of the thoracic spine.
HYPERLORDOSIS OR LORDOTIC POSTURE – an exaggerated curve of the lumbar spine.
FLAT BACK – flat lumbar spine without curve.
POSTURAL DEVIATIONS
Figure 2.2 Deviations from optimal posture
Copyright © 2014 Active IQ Ltd. Not for resale | 163
Section 2: The effects of exercise on the bodyPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH
FLAT BACk
• Flattened lumbar curve. • Stiffness in lumbar spine. • Posterior tilt of pelvis. • Hip flexors lengthened. • Hamstrings tight. • Rectus abdominis tight.
• Anterior tilt of pelvis.• Lengthened rectus abdominis. • Gluteus maximus usually weaker
and inactive.• Hamstrings tight (but not
necessarily shortened).• Hip flexor shortened.• Increased lumbar curve.• Short erector spinae.
• Head pokes forward. • Short and over-active upper
trapezius. • Short and tight pectorals.• Lengthened and inactive lower
trapezius, middle trapezius and rhomboids.
• Posterior deltoid lengthened. • Hip flexor shortened.• Increased lumbar curve.• Short erector spinane.
HyPERLoRdoSIS
HyPERkyPHoSIS

End of section: Learning checkAnswer the following questions and make notes to revise this section.
• State three effects of aerobic exercise on the cardiovascular and respiratory systems.
• What is an optimal blood pressure?
• What is hypertension?
• Give one short-term effect of exercise on blood pressure.
• State one long-term effect of exercise on blood pressure.
• What is blood pooling?
• How can the risk of blood pooling be reduced during exercise?
• What is weight-bearing exercise?
• What is non-weight-bearing exercise?
• What are the benefits of weight-bearing exercise?
• What are the benefits of non-weight-bearing exercise?
• What is DOMS?
• Name two types of exercise that may contribute to DOMS.
• State the short-term effects of exercise on the joints, bones and muscles.
• State the long-term effects of exercise on the joints, bones and muscles.
• What is hypertrophy?
• What is optimal posture?
• What is hyperlordosis?
• What is hyperkyphosis?
• How can exercise improve kyphotic posture?
164 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: The effects of exercise on the body

Section 3: The principles and variables of fitness in an exercise programme
There are various principles and variables that need to be understood and applied when designing an exercise programme. Manipulation of these can make an exercise programme harder (progression) or easier (regression) and can be applied to modify specific exercises to meet a client’s specific needs.
THE SAID PRINCIPLE• Specific Adaptation to Imposed Demand. • The body specifically adapts to the training demands placed on it.
Fundamental principles and physiological implicationsThere are several fundamental principles, which include:
• Specificity.
• Progressive overload.
• Reversibility.
• Adaptability.
• Individuality.
• Recovery time.
• Frequency.
• Intensity.
• Time.
• Type.
Specificity
Any change or adaptation in the body’s muscles, organs and systems will be very specific to the type of training (stress or stimulus) undertaken.
Exercises that develop and improve each component of fitness bring about specific adaptations. Stretching exercises improve flexibility; they won’t develop cardiovascular fitness. Aerobic endurance exercises improve cardiovascular fitness; they won’t develop muscular strength. Strength training improves muscular strength, but it won’t improve cardiovascular fitness or flexibility.
Different types of exercise that improve the same component of fitness also have specific effects. Strength training for the legs makes them stronger, but won’t make the upper body stronger. Stretching the hamstrings makes them more flexible, but won’t improve flexibility of other muscle groups. Swimming won’t improve running ability or speed; there would be generalised improvements in the cardiorespiratory system, which might contribute to improvements, but for specific and more effective results the individual will need to practise the specific activity they want to develop.
The training goals of an individual are essential when considering the appropriateness of specific types of exercise, e.g. are they aiming to improve general fitness or improve performance for a specific sport or athletic event? If fitness goals are specific it will be important to consider:
• The predominant energy system and muscle fibre type used for the sport.• The main prime movers recruited and joint actions required. • The joint angle and range of movement used. • The type of muscle contraction (concentric/eccentric) and speed of movement.
1
Copyright © 2014 Active IQ Ltd. Not for resale | 165
Section 3: The principles and variables of fitness in an exercise programmePR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH
Adaptation
Imposed
Demand
Specific
AID
S

Progressive overload
To bring about any adaptation the body will have to work a little bit harder than it is used to. Progressive overload can be achieved by increasing the volume of work (frequency, intensity, time) and balancing rest and recovery time.
The stimulus provided must be large enough to challenge and evoke the required adaptation. Improvements in range of movement can be achieved by working at or beyond the current range of motion, i.e. stretching a little bit further (to a point of mild tension). Improvements in muscle strength will require the weight lifted to progressively increase and improvements in endurance will require more repetitions. The number of sets and rest between sets will also offer methods of progressive overload.
The level of overload applied will be determined by the current fitness of the individual and their goals. An untrained, sedentary person may need comparatively small changes to bring about a training effect, whereas a trained individual may need a greater challenge.
2
3 ReversibilityImprovements in fitness can only be maintained by regular exercise and activity. If training (the exercise stimulus) stops the benefits gained will gradually decline.
The rate of decline is determined by the fitness of the individual, the level of stimulus reduction (e.g. total cessation or reduced volume) and the length of time the stimulus is reduced. Total inactivity or bed rest will produce a greater decline than maintaining some activity. Athletes, for example, often plan timed rest periods as part of their training programme (post season) to give the body time to rest and recover.
Total inactivity or lack of movement for extended time periods contributes to increased risk of many chronic health conditions. To maintain optimal function all body systems need to be trained regularly at an appropriate volume.
AdaptabilityThe body reacts and adapts in accordance with the type of challenge and overload to which it is subjected. High-resistance and low-repetition exercise, for example, can lead to an increase in strength. Intense exercise (lasting under ten seconds), e.g. sprints or maximal strength training, can cause adaptations in the adenosine triphosphate/creatine phosphate systems, making them more efficient. Lower-intensity, longer-duration activities help to improve aerobic endurance by improving the efficiency of the aerobic energy system (cardiovascular endurance).
Recovery and restPhysiological adaptations occur in the time following the activity rather than during the activity. Scheduled rest periods are a vital part of any exercise programme; this will include rest periods between exercises/sets within individual sessions and also rest between training sessions.
Rest and recovery time is essential to prevent overtraining. Factors that influence the amount of required rest and recovery time include the volume of exercise and also the fitness level of the individual. The quality of the recovery will largely be determined by the quality of sleep and dietary intake.
To bring about any adaptation, the body will have to work a little bit harder than it is used to. The exercise stimulus must increase.OVERLOAD
PROGRESSION= The need to increase the demand over time to cause adaptation.
4
5RECOVERY AND RESTPhysiological adaptations occur in the time following the activity rather than during it.
166 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: The principles and variables of fitness in an exercise programme

Individuality
There are many factors that will affect an individual’s training potential; these include their age, body type, gender, heredity and other physiological differences, such as their range of motion, current strength and cardiovascular fitness.
Clients may have similar general goals (e.g. to lose weight, get fitter), but individual differences will significantly influence the type of exercise that is recommended to ensure the programme is safe and effective.
6 INDIVIDUAL DIFFERENCES• Age.• Gender. • Body type. • Heredity. • Muscle fibre type. • Range of motion (ROM).• Strength. • Cardiovascular fitness.
If a client is overweight and deconditioned, for example, then low-impact, non-weight-bearing exercise may be a safer alternative to high-impact activities. If a client has restricted range of motion at their hips, additional stretching exercises in this region may be appropriate.
A client’s skill level and coordination may also influence exercise choice. A newcomer to gym training, for example, with low skill levels may find they are better able to maintain correct alignment using fixed resistance machines than free weights. A Pilates beginner will require modifications to many of the exercises to enable them to perform safely.
The FITT principles When planning a programme of activity it is essential to consider the:
Frequency of training (how often the activity will be performed).
Intensity of training (how hard the activities will be).
Time or duration (how long the activities will be performed).
Type of training (the specific activities that will be performed, e.g. strength, endurance, walking, running, Pilates).
F
I
T
Frequency
Frequency refers to the number of training sessions carried out per week. The number of exercise sessions should reflect the individual’s goals (e.g. increase physical activity or improve a specific component of fitness) and take into account their current fitness level and the time they have available, including commitments like family and work.
An untrained inactive individual can start by gradually increasing their daily activity levels, so that they are eventually active at a moderate intensity on five or more days of the week. Scheduled exercise sessions for a beginner may be planned on two to three non-consecutive days a week (with a rest in between each session).
T
Copyright © 2014 Active IQ Ltd. Not for resale | 167
Section 3: The principles and variables of fitness in an exercise programmePR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Competitive athletes may train up to twelve times a week, with morning and evening sessions on many days; different muscles and fitness components will be the focus in different sessions.
Frequency of training also depends on the component of fitness being trained. It is safe to stretch every day if the muscles are warm, but for muscular strength and endurance training, 48 hours’ rest is required prior to working the same muscle groups. Training specific muscles should therefore be planned on non-consecutive days. If different muscle groups are worked on different days (e.g. a split routine) then muscular training can be more frequent.
Table 3.1 Provides a basic illustration of how frequency can be manipulated to correspond with increased fitness.
TRAINING STATUS FREQUENCY GUIDELINES (SESSIONS / WEEK)Beginner 2-3Intermediate 3-4Advanced 4-7
Table 3.1 Frequency and fitness level (Earle and Baechle, 2000)
Another key factor that affects frequency is the intensity of the exercise. Moderate-intensity aerobic exercise can be performed more often (every day), with less risk of injury. Vigorous-intensity aerobic exercise will increase the risk of injury and therefore may need to be performed less frequently (e.g. three days a week).
Intensity
The intensity of exercise will be determined by individual factors (existing fitness and skills level, etc.) and specific goals, e.g. the components of fitness trained (strength, flexibility, cardiovascular).
The intensity of cardiovascular exercise is traditionally monitored by measuring heart rate or rating of perceived exertion. The intensity of flexibility exercise is traditionally monitored by measuring the range of motion. The intensity of muscle strength and endurance training is traditionally monitored by measuring the resistance lifted and the number of repetitions.
The variables that will change the intensity for specific fitness components include:
• Resistance, including lever length, gravity and body weight.
• Repetitions.
• Range of motion.
• Rest.
• Sets.
• Rate/speed.
ResistanceThe resistance lifted is an important aspect to be considered when designing a muscular fitness programme. The resistance or weight lifted will alter the intensity and the training benefits.
STREngTH – HIGH RESISTANCE, LOW REPETITIONS.
EndURAnCE – LOW RESISTANCE, HIGH REPETITIONS.
168 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: The principles and variables of fitness in an exercise programme

Different types of resistance for improving muscular strength and endurance may include:
• Body weight exercises, e.g. curl-ups, squats, back extensions, press-ups and various yoga postures and Pilates exercises.
• Dumbbell exercises or exercises with resistance bands, e.g. bicep curls, shoulder press and lunges.
• Fixed-resistance machine exercises, e.g. chest press, leg press and leg extension machines.
• Free-weight exercises, e.g. bench press, squatting and also group resistance training programmes, like body pump.
• Water-based resistance exercises, e.g. using water bells and floatation devices to provide resistance.
• Manual resistance (applied by a partner or an opposing limb).
• Cable machines.
Lever lengthThe length of the levers being moved (arms, legs or trunk) will affect the intensity and resistance being moved.
A LongER LEVER wILL InCREASE RESISTAnCE.
A SHoRTER LEVER wILL REdUCE RESISTAnCE.
A box press-up, for example, offers less leverage and moves less body weight than a full press-up, making it a more appropriate exercise for a beginner.
BOX PRESS-UP FULL PRESS-UP
The pivot point for the box press-up is the hip and the leverage moved is the trunk of the body.
The pivot point for the full press-up is the foot and the leverage moved includes the weight of the legs as well as the trunk of the body.
Some individuals have naturally longer levers, which increases the resistance they are moving and the range of motion, e.g. someone with longer forearms would have an increased lever arm during a bicep curl. This will affect the amount of weight they are able to lift, e.g. an individual with shorter levers only has to move the weight through a small range of motion and may be able to lift a heavier weight than someone who has longer levers and needs to lift the weight through a naturally larger range of motion.
Levers can be deliberately manipulated to add (or reduce) intensity.
Copyright © 2014 Active IQ Ltd. Not for resale | 169
Section 3: The principles and variables of fitness in an exercise programmePR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH
LONGER INCREASE
SHORTER REDUCE

Adding weight to the end of the lever or lengthening the lever will add resistance.
SpeedChanging the speed of an exercise can also increase the intensity, e.g. sprinting is more intense than running at a steady pace. Olympic power lifts, such as the clean and jerk, are more intense than performing a bench press at a moderate tempo.
Increasing the speed of a movement may be detrimental for some individuals because it makes it more difficult to maintain correct posture and alignment. Performing exercises at a moderate controlled speed enables the conscious mind to process information and respond to feedback more easily, making it easier to maintain safe technique. Fast and rapid movements make it harder to keep focussed on all body parts, which means alignment and posture may be lost.
Sometimes slowing down an exercise can also make an exercise more intense because the muscle has to maintain the contraction for a longer period of time.
Some studio-based group resistance programmes deliberately manipulate this variable. There may be, for example, a number of repetitions at a moderate tempo followed by a number of repetitions at a slower tempo (e.g. taking four-eight counts to lower the weight and four-eight counts to lift the weight). Speed variations are sometimes also planned for different phases of the movement, e.g. taking one count to lift the weight (concentric phase) and three counts to lower the weight (eccentric phase) and vice versa.
GravityWhenever the body is upright and moving it is resisting the gravitational force of the Earth. Gravity adds resistance to movement.
Weight-bearing exercises, e.g. walking or kneeling on all fours, fully utilise the resistance of gravity as a resistance.
Non-weight-bearing activities reduce the effects of gravity, e.g. in a water-based session the gravitational forces are reduced and replaced by the force of buoyancy as a resistance.
High-impact activities, e.g. running and jumping, add intensity to cardiovascular training because the body weight must overcome the force of gravity to lift away from the floor. They also add weight-bearing stress to the joints as the body lands. Lower-impact exercises, e.g. walking, reduce the impact stress on the body.
Exercise position and gravity Some muscular exercises can be performed in different positions to manipulate the force of gravity and change the intensity (progress or regress).
Performing a press-up against a wall, for example, is working across the force of gravity, whereas a press-up from a prone position (on the floor, facing downwards) will be working maximally to resist the force of gravity.
TRAINER TIPEnsure the speed of exercise allows the individual to maintain correct posture and alignment.
170 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: The principles and variables of fitness in an exercise programme

Across gravity = less resistance. Against gravity = more resistance.
Gravity can also be used to assist the performance of some stretch positions, e.g. in a lying hamstring stretch gravity draws the leg closer to the body; the restriction to movement will be the length of the muscles and any tightness.
Range of movementRange of movement can be used to progress and add intensity to all components of fitness.
• Stretching exercises performed through a larger range of motion will improve flexibility.
• Bending more deeply or jumping higher will move the body weight through a larger range of movement, increasing the intensity of some cardiovascular exercises, e.g. knee bends and star jumps.
• Working through a full range of motion during resistance training maximises strength gains through the full movement range.
In a gym it is common to see people lifting weights that may be too heavy. This makes it more difficult to lift through a full range of movement. Decreasing the load makes the exercise less intense, allowing the lifter to move through a fuller range.
Time
The total time dedicated to a training session is largely dependent upon the type of exercise, component of fitness, fitness level of the individual and amount of time they have available or are willing to dedicate.
The minimum duration of training to improve cardiovascular fitness is around 20-30 minutes, excluding the warm-up and cool-down.
Sufficient time will need to be allowed in muscular fitness training to train all major groups and perform the planned sets and repetitions for each specific exercise.
The time allocated for stretching should be sufficient to stretch all major muscle groups for the appropriate number of seconds.
Group exercise sessions (exercise in water, outdoor boot camps, Pilates and yoga) tend to be planned for a set duration, usually a minimum of 45 minutes and a maximum of 90 minutes, which includes warm-up and preparatory exercises and cool-down and closing phase exercises.
TRAINER TIPIndividuals with a high body mass (overweight or obese) will naturally be moving more body weight against gravity, so reducing these effects (use of non-weight-bearing or water-based activities) will reduce some of this natural resistance, making movement more comfortable and less stressful.
This may be beneficial for those who are untrained or deconditioned.
SAFETYCONSIDERATION Moving through a full range of movement during exercise is important, although there are potential risks to the connective tissues and joints when approaching end ranges, particularly where momentum is involved (ballistic stretching).
Copyright © 2014 Active IQ Ltd. Not for resale | 171
Section 3: The principles and variables of fitness in an exercise programmePR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Gym-based sessions are planned with similar timeframes (between 45 and 120 minutes) including a warm-up and cool-down. The time allocated to the main workout will depend on the components of fitness trained (cardiovascular training only or muscular fitness training only or both) and the time required for each component. For example, a circuit weight training session integrating cardio and muscular exercises may require less time than a strength-biased resistance programme using more sets and longer rests between sets.
Type
There are many different types of exercise and activity and specific activities will train specific components of fitness.
gyM-BASEd TRAInIngGym-based training programmes use a combination of cardiovascular machines, fixed resistance machines, free weights, cable machines and body weight exercises to train specific components of fitness.
Changing the type of equipment will change the forces that the body has to cope with and can be used as a method of progression or regression according to client need. For example, a movement such as a chest press can be performed sitting down with the back resting against a seat pad on a machine with a single pivot point. This will load the prime movers (pectorals and triceps) but requires minimal contribution from other synergist and fixator muscles. Using the same movement lying on a bench and lifting a barbell (bench press) will use the same prime movers, but involve additional stabilisation from muscles of the shoulder, shoulder girdle, torso and even the legs in order to prevent the bar from toppling to one side. Progressing even further to using dumbbells for the movement (a chest press) greatly increases the demand for stabilisation of the shoulder joint and shoulder girdle as well as requiring more coordination, which increases nervous system involvement. Further progressions such as a single arm dumbbell press or a standing cable chest press will increase the rotational force through the body and the demand on the obliques, hip stabilisers and leg muscles. The choice of equipment must be carefully considered to meet both the client’s stated goals and their current ability level.
gRoUP ExERCISEGroup exercise programmes (studio or water-based) mainly use body weight exercises to train specific components of fitness (cardiovascular, muscular fitness and flexibility). One key consideration is that group activity sessions are unlikely to elicit maximal strength improvements; they are more likely to improve muscular endurance and/or cardiovascular fitness. Some classes will use small equipment to add resistance and challenge strength and stability, e.g. dumbbells and bands (exercise to music) and foam rollers (Pilates), but the intensity tends not to be maximal.
Varying the type of exercise can add interest and improve adherence and motivation for general populations. Cross training (swimming, cycling, walking and running) improves cardiovascular fitness and aerobic endurance and meets general fitness goals, but individuals with specific goals will need to focus on specific activities (e.g. focus on running in order to run a marathon).
172 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: The principles and variables of fitness in an exercise programme

Principles of a progressive training programmeThe purpose of a progressive training programme is to:
• Build up gradually and allow the body adapt progressively.
• Minimise risk of injury or overwork (including DOMS).
• Provide adequate rest and recovery time.
• Encourage adherence.
• Avoid a plateau or decrease in performance.
Progression means that when an overload is applied it should be gradual and sufficient to elicit an adaptation, but it should not be excessive. An excessive stimulus is counterproductive because it leads to overwork and possibly overtraining. A prime example of applying excessive stimulus is excessive post-training muscular soreness lasting seven-eleven days after resistance training.
A progressive training programme should take all the principles and variables previously described into consideration.
For an individual who is new to exercise the programme will need to start at an appropriate level and consider all individual factors, such as age, body type, current fitness and activity levels, and specific goals. It will then need to progress at an appropriate rate over a number of weeks to enable adaptations to take place.
The programme will need to start at a lower level and build up gradually to ensure progressive overload is applied. Different variables (resistance, repetitions, rest, sets) may need to be increased at different times to allow progression to be gradual (e.g. not changing all variables at the same time).
Some general guidelines for progression of different components of an exercise session are provided in table 3.2.
WARM-UP CARDIOVASCULAR MUSCULAR COOL-DOWN
Beginners Longer duration. Lower intensity. Less complex exercise.Slower pace.
Shorter duration. Lower intensity (RPE, heart rate).Less complex exercises. Slower pace. Less impact.
Fewer repetitions. Fewer sets. Lower resistance. Less complex exercises.
Longer duration. Simpler stretch positions (e.g. isolate rather than combine stretches).Shorter hold initially. More supported positions. Smaller range of motion.
Intermediate to advanced
Duration can decrease. Intensity can increase more quickly. Slightly faster pace. Exercises can be more complex, e.g. combining mobility and pulse raising activities (walking and mobilising shoulders at same time).
Increased duration. Higher intensity (RPE, heart rate).Inclusion of more complex exercises or CV machines. Faster pace. Inclusion of higher impact.
Resistance can increase. Repetitions can increase (depending on resistance).Number of sets can increase. Can progress to more complex exercises.
Shorter duration. Use of more challenging stretch positions. Longer hold. Larger range of motion.
Table 3.2 General guidelines for progression of different components of an exercise session
STARTER CONSIDERATIONS INCLUDE:
• The type of exercise and activity should be something the client enjoys and likes and should be an activity to achieve their specific goals.
• The frequency should reflect the commitment the client can give and their current activity levels.
• The duration and intensity should reflect the client’s current fitness and other individual factors.
Copyright © 2014 Active IQ Ltd. Not for resale | 173
Section 3: The principles and variables of fitness in an exercise programmePR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

When to regress a programme Regression is the opposite of progression; it means making the exercise easier to reduce the challenge. Reasons for regression may include:
• A holiday, vacation or a break from training.
• A period of illness.
• Progression or worsening of a chronic health condition.
• The individual is unable to cope.
Overtraining Any exercise programme requires a balance between overload and recovery. If the overload stimulus exceeds the body’s ability to adapt, it may result in injury or overtraining.
If overtraining is suspected the programme should be regressed (made easier) to enable the person to recover fully.
It is not necessary to regress every aspect of a training programme if overtraining is suspected. It may be sufficient to reduce just a few of the variables, such as selecting one or two of the following:
• Increase the rest time between sets.
• Reduce from four to three exercise sessions per week (frequency of training).
• Reduce the weight lifted on certain exercises (decrease resistance).
• Reduce the length of the total session.
• Reduce high-impact activities to low-impact activities.
• Change exercise complexity by choosing simpler exercises (less complex equipment).
HOW TO REGRESSReduce the:
• Frequency of training.
• Intensity.
• Resistance, repetitions.
• Working heart rate level.
• Total workout time.
• Impact.
SIGNS AND SYMPTOMS OF OVERTRAINING MAY INCLUDE:
• Reduction in performance.
• Sudden loss of coordination.
• Lack of ability to concentrate.
• Irritability and over sensitivity to criticism.
• Reported disrupted sleep patterns.
• General lethargy.
• Susceptibility to colds, illness.
174 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: The principles and variables of fitness in an exercise programme

Programming exercise for physical fitness and health benefits Programming exercise to improve physical fitness requires a different approach to programming for health benefits.
Programming for health
Health benefits can be gained by being physically active throughout the day on most days of the week (a minimum of 150 minutes, moderate intensity every week) and spending less time sedentary. Activity levels to improve health can be accumulated throughout the day in bouts of ten minutes or more.
Moderate intensity activities include active travel (walking or cycling to work), walking the dog, climbing stairs, active and physical work and vigorous housework. It may also include structured exercise.
Stretching exercises can be integrated into a daily activity routine, but the body must be warm prior to lengthening the muscles.
Programming for physical fitness
To improve one or more of the components of physical fitness, exercise needs to be structured and planned more specifically using the FITT principles.
Types of exercise include gym training (cardiovascular and resistance machines), group exercise to music or exercise in water, outdoor exercise (running, walking, circuits) and many other variations, which may focus on more specific components of fitness like yoga or Pilates.
ACTIVITY FOR HEALTH Activities to maintain and improve health include:
• Active travel (walking or cycling to work).
• Walking the dog.
• Climbing stairs.
• Active and physical work.
• Vigorous housework.
• Gardening.
• Structured exercise.
Copyright © 2014 Active IQ Ltd. Not for resale | 175
Section 3: The principles and variables of fitness in an exercise programmePR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Session structure Any exercise session designed to improve physical fitness should contain each of the following class components:
• Warm-up or preparatory phase to prepare the body for activity.
• Main session to train the specific components of fitness (cardiovascular and/or muscular strength and endurance).
• Cool-down or closing phase to return the body to a non-exercising state and improve flexibility.
The warm-upThe warm-up is the preparatory component at the start of the exercise session. The aim of the warm-up is to prepare the body for the type of exercise to follow.
Exercise sessions aimed at training all components of fitness should include exercises to prepare all body systems, including the heart and lungs (cardiovascular and respiratory systems), the muscles and nerve pathways (neuromuscular systems) and the joints (skeletal system).
WARM-UP OR PREPARATORY PHASE MAIN SESSION COOL-DOWN OR
CLOSING PHASE
EXPERT TIPRunners who ‘never’ warm up compared to those who ‘always’, ‘usually’ and ‘sometimes’ warm up have a significantly increased risk of sustaining injury.
WALTER ET AL (1989)
A slow, gradual approach to warming up will allow all body systems to adjust effectively, e.g. steadily raise the pulse rate to increase the body temperature, mobilising the major joints gradually through a larger range of motion and stretching the muscles. Using a graduated approach will reduce lactic acid build-up in the early stages of exercising.
The immediate effects of specific warm-up activities are different for mobility exercises and pulse-raising and body-warming exercises.
Mobility exercises• Synovial fluid is secreted to lubricate joints, which should reduce the risk of injury to soft tissue
structures.
• Mobility exercises reduce the viscosity (thickness) of synovial fluid enabling the joints to move with greater ease, giving reduced stiffness and improved range of motion.
TRAINER TIPThe warm-up should include exercises to: • Mobilise the joints. • Warm the muscles. • Increase the heart
rate gradually. • Lengthen and
stretch the muscles.
• Rehearse activities in the main session.
Pulse-raising and body-warming exercises• Blood vessels widen (vasodilation) to increase blood flow and delivery of
oxygen to the muscles, which in turn increases core temperature and makes the muscles warmer.
• Increased muscle temperature improves the elasticity of intramuscular connective tissue, making the muscles more pliable and less viscous, allowing smoother and more efficient muscle contractions.
• Neuromuscular pathways are stimulated, increasing the speed at which nerve impulses travel, enabling more efficient movement.
• Metabolic activity in the muscle tissue is stimulated (energy production).
• The heart is better prepared to respond to more strenuous exercise (raising the heart rate gradually promotes use of the aerobic energy system).
176 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: The principles and variables of fitness in an exercise programme

Stretching exercises
Lengthening the muscles provides a more effective range of motion and reduces the potential risk of injury.
Dynamic stretches help to maintain the body temperature. They can mimic and rehearse the general movement of the following session.
Static stretches may reduce body temperature, so should be integrated between warming exercises if they are used.
DYNAMIC STRETCHES
STATIC STRETCHES
Other types of warm-upThere are three types of warm-up: passive, active general and active specific.
PASSIVE WARM-UP A passive warm-up uses some form of external heating, for example taking a warm shower or hot bath, using heat lamps, warm clothing or even pre-exercise massage. Heart rate can increase together with blood pressure and increased circulation around the body, but skeletal muscle will be relatively unaffected. Blood will be diverted towards the skin rather than the muscles.
ACTIVE GENERAL WARM-UP The active general warm-up method increases body temperature as the individual engages in activities that involve large muscle groups, e.g. marching, walking, knee bends/squats, jogging. This type of warm-up increases muscle temperature more effectively than the passive method.
An active specific warm-up involves going through basic movement patterns using muscle groups that will be used in the activity, but at a reduced intensity. This is an effective physiological and mental rehearsal of a performance skill.
Some individuals combine all the warm-up methods. For example, they start with a general warm-up (joint mobilising activities and low-intensity warming movements) wearing more layers of clothing. As they become warmer they remove outer clothing layers and the activity progresses to a more skill-specific warm-up.
ACTIVE SPECIFIC WARM-UP
ACTIVE WARM-UPWhen the body starts moving, the heart rate and circulation of blood increase. The capillaries in the muscles dilate allowing more oxygen to reach the muscles, which in turn increases the temperature of the muscles, making them warmer and more pliable and ready to lengthen, e.g. walking on a treadmill or gentle cycling.
Copyright © 2014 Active IQ Ltd. Not for resale | 177
Section 3: The principles and variables of fitness in an exercise programmePR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Planning considerations for the warm-up
The intensity and duration of a warm-up will vary depending on the individual’s fitness level and the type of session. As a general guideline around 10-20 minutes is ideal. Warming up should not be too intense because it may impair physical performance.
The warm-up (time and intensity) should be adjusted according to the environment, temperature, humidity, space, etc. In a cold environment it may take longer to warm up and clothing may need to be worn, in a hot environment the intensity of warm-up activities may need to be lower to prevent overheating.
The main session – training different components of fitness The structure and content of the main session will vary significantly depending on the type of session and the specific component/s of fitness that are the focus for that session. Individuals may choose different types of exercise programme to achieve specific goals. Different exercise disciplines often focus on different components of fitness.
GYM-BASED TRAINING GROUP EXERCISE TO MUSIC
PILATES YOGA
A cardiovascular training session, e.g. treadmill.
and/or
A muscular strength and endurance session using fixed resistance machines and/or free weights.
A choreographed aerobic component for cardiovascular fitness.
and/or
A body weight muscular fitness component.
Mind and body focus.
Exercises focussing on posture and core stability in different movement planes.
Mobility, strengthening, stability and flexibility focus.
Mind and body focus.
A range of postures to increase flexibility, strength and balance.
Postures:• Standing and
balancing. • Strengthening. • Backbends and
forward bends. • Lateral extensions and
rotations.• Inversions.• Relaxation and
meditation.
NB: This is an outline of content type; each exercise discipline has many variations.
Variations:
CV: Interval, continuous, circuit resistance training.
MS&E: Single-set and multiple-set, e.g. super-sets, pre-exhaust, pyramids.
Variations:
CV: Aerobics and themed classes.
MS&E: Body conditioning, sculpt, body training systems.
Variations:
• Modern. • Contemporary. • Clinical. • Fitness Pilates.
Variations:
• Iyengar. • Asthtanga. • Vini yoga. • Fitness yoga.
Table 3.3 Main session content for different disciplines
178 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: The principles and variables of fitness in an exercise programme

The cool-downThe cool-down is the closing component at the end of an exercise session. The aim of the cool-down is to return the body and mind back to a non-exercising or pre-exercise state. Exercises should gradually taper down and become less intense; decreasing the heart rate, decreasing the body temperature and stretching the muscles to leave the body and mind in a relaxed and refreshed state.
Cooling down after cardiovascular activities
Following intense activity blood has been diverted to the working muscles. If exercise stops suddenly there is a risk that the blood may ‘pool’ in the extremities; especially in the legs. Cool-down exercises after cardiovascular exercise should focus on gradually lowering the heart rate by reducing the intensity of the movements, e.g. progressively slowing down the speed of movements and the range of movement and reducing any high-impact activities until the heart rate has slowed down. Slowing down gradually will assist venous return to the heart and prevent dizziness and nausea.
TRAINER TIPThe cool-down and closing phase will be specific to the type of training.
Cooling down after a run, when the heart rate is elevated, will be different to cooling down at the end of a Pilates class, when the heart rate has not been elevated in the same way.
Cooling down after resistance training
Following resistance training there will be a benefit from performing light, rhythmical low-intensity exercises, as these will help to disperse any lactic acid. Cool-down exercises after resistance training can be steady, e.g. walking or gentle cycling, rather than decreasing from a higher to a lower intensity.
Stretching in the cool-down
Stretching is an essential part of the cool-down and closing phase for every type of training session, cardiovascular training, resistance training, group exercise to music, Pilates, etc. Stretching the muscles after they have worked helps to prevent muscle soreness after exercise. Maintenance and developmental static stretches can be used.
MAINTENANCE STRETCHES:
DEVELOPMENTAL STRETCHES:
The muscle is taken to an extended range of motion and the point of mild tension. When the muscle relaxes the position is held for 10-15 seconds.
The muscle is taken to an extended range and the point of mild tension. When the tension subsides the stretch is taken further to an increased range of motion. This process can be repeated, moving a little further into the stretch when the muscle relaxes. The extended stretch position can be held for longer periods of time, from 15-60 seconds.
Stretch positions should allow the muscles to relax. Floor-based, seated and lying positions may enable greater muscle relaxation for some individuals, depending on their existing range of movement.
Gradually bringing the body back to normal also helps clients to wind down and promotes mental relaxation, some types of session (e.g. yoga and Pilates) integrate specific relaxation and meditation exercises into the closing phase to emphasise these positive effects.
Copyright © 2014 Active IQ Ltd. Not for resale | 179
Section 3: The principles and variables of fitness in an exercise programmePR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

End of section: Learning checkAnswer the following questions and make notes to revise this section.
• What is meant by each of the following terms?
• Specificity.
• Progressive overload.
• Reversibility.
• Adaptability.
• Individuality.
• Recovery time.
• Frequency.
• Intensity.
• Time.
• Type.
• How would you modify the FITT principles to progress the following components of fitness?
• Flexibility.
• Muscular strength and endurance.
• Cardiovascular fitness.
• When and how would you regress a training programme?
• How would you adapt an exercise programme using the FITT principles?
• What effect will speed of exercise have on posture, alignment and intensity?
• Give an example of how changing the length of levers will affect exercise.
• Give an example of how gravity will affect exercise.
• Give an example of how changing the resistance will affect exercise.
• What are the differences between programming exercise for physical fitness and health?
Planning considerations for the cool-down
The intensity and duration of the cool-down will vary depending on the individual’s fitness level and the intensity of the specific training session. More time will be required to cool down after cardiovascular training because the heart rate needs to be gradually lowered. If the training session has not focussed on training cardiovascular fitness then less time may be needed, but the inclusion of additional relaxation exercises may extend the time required. As a general guideline, around 10-20 minutes is effective to achieve the aims of the cool-down.
The cool-down (time and intensity) should be adjusted according to the environment, temperature, humidity, space, etc. In a cold environment the body may cool down quickly and layers of clothing may need to be added for stretching.
180 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: The principles and variables of fitness in an exercise programme

Section 4: Health benefits of physical activity
Health benefitsRegular moderate-intensity physical activity offers many benefits for health, these include:
• Reducing the risk of premature death by 20-30%.
• Reducing the risk of developing coronary heart disease (CHD), stroke, diabetes and certain cancers by 50%.
• Improving functional capacity.
• Reducing the risk of back pain.
• Increasing independence in older people.
• Increasing bone density and reducing the risk of osteoporosis.
• Improving psychological wellbeing.
• Reducing the risk of stress, anxiety and clinical depression.
• Reducing the symptoms of depression and anxiety.
• Reducing the risk of falls in older adults.
• Improving weight loss and weight management, reducing the risk of obesity.
• Improving quality of life and general wellbeing. (Department of Health, 2011)
Diseases of inactivity (hypokinetic) are the main causes of death in the UK and many developed nations (World Health Organisation, 2003).
In each of the UK home countries less than half of all adults meet the recommended activity levels (150 minutes a week).
HOME COUNTRY SCOTLAND ENGLAND WALES NORTHERN IRELANDMen 43% 40% 36% 33%Women 32% 28% 23% 28%
Table 4.1 Percentage of adults meeting physical activity recommendations
Populations with the lowest levels of physical activity include:
• South Asian and Chinese women and men. • Bangladeshi men and women (reported to be the least physically active).• Individuals from low income households, lower social classes and with lower levels of educational
attainment.• Individuals working in non-professional and non-managerial occupations.• Women and girls (all age groups are less active than men).• Older populations (activity levels decline with age).
(Department of Health, 2009)
Copyright © 2014 Active IQ Ltd. Not for resale | 181
Section 4: Health benefits of physical activityPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

The effect of physical activity on the causes of chronic health conditions Physical activity and exercise have a specific impact on many of the modifiable risk factors that contribute to cardiovascular disease.
• It assists with weight management (achievement and maintenance of weight loss) and reduces the risk of obesity.
• It maintains optimal blood pressure. • It improves cholesterol levels. • It prevents or delays the development of type 2 diabetes.• It assists stress management and reduces stress levels.• It assists with smoking cessation (activity can be a replacement and
more positive activity for some).
Table 4.2 outlines the effects of physical activity on the causes of various chronic health conditions.
CHRONIC HEALTH CONDITION EFFECTS OF EXERCISE ON CAUSES
Hypertension
High blood pressure increases the risk of cardiovascular disease and stroke.
• Helps to reduce and normalise mild hypertension. • Prevents age-related increases in blood pressure (longevity of exposure
risk).• Assists with stress management and weight management (risk factors
for developing hypertension).
Hypercholesterolemia
High levels of blood cholesterol, specifically high levels of low density lipoproteins (LDLs) are attributed as one of the major risks for death from coronary heart disease.
• Offers a preventative effect. • Increases high density lipoproteins (HDL) cholesterol which reduces
risk of coronary heart disease. • Decreases LDL levels.• Decreases overall cholesterol levels. • Reduces other modifiable cardiovascular disease risk factors.
Diabetes
Diabetes is linked with coronary heart disease (CHD), obesity, hypertension and hypercholesterolemia. 50% of people with diabetes will die from CHD.
• Offers a preventative effect. • Reduces the risk of developing type 2 diabetes. • Assists with the management of blood sugar levels and glycaemic
management. • Improves insulin sensitivity. • Assists weight management, which may contribute to the onset of
type 2 diabetes.
Obesity
Obesity is linked with increased risk of cardiovascular disease (CVD) and loss of independence.
• Offers a preventative measure. • Assists weight management.• Increases calorific expenditure. • Increases resting metabolic rate. • Assists with reducing body fat. • Reduces other CVD risk factors.
Osteoarthritis
Osteoarthritis is the most common joint disease and nearly every person over the age of 60 has affected joints (Department of Health, 2004).
• Offers a preventative effect. • Improves range of movement.• Improves joint and muscle strength.• Nourishes cartilage (synovial fluid).• Reduces stiffness and pain. • Improves functioning and reduces disabling effects.
Osteoporosis
Osteoporosis increases the risk of fracture (from falls) in frail older adults. The two primary risks for osteoporosis are peak bone mass and bone loss.
• Helps to develop peak bone mass (being active in formative years, up to age 30, will help to develop bone strength and reduce bone loss in later years).
• Maintains bone mass in pre-menopausal women. • Reduces the rate of bone loss post menopause. • Improves strength, coordination and balance and will help to
reduce the risk of falls and bone fractures in people diagnosed with osteoporosis.
CVD RISK FACTORS Modifiable
• Smoking. • Hypertension. • High cholesterol. • Inactivity. • Diet. • Diabetes. • Stress.
Non-modifiable
• Age. • Heredity. • Gender.
182 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: Health benefits of physical activity

Low back pain
80% of the population experience low back pain at some point in their lives and 150 million working days are lost each year because of LBP (Department of Health, 2004).
• Prevents occurrence and recurrence of LBP. • Assists rehabilitation. • Promotes a return to work.• Reduces stress and anxiety, which may contribute to LBP.
Anxiety and depression
It is estimated that around one in six people experience a mental health condition at any one time (Department of Health, 2004).
• Reduces the risk of clinical depression. • Assists with stress management. • Provides a distraction from negative thinking patterns and worries. • Offers an opportunity for socialisation, which can reduce isolation. • Helps to manage physical co-morbidities and reduces other CVD risk
factors.• Can be as successful as psychotherapy and medication in the longer
term (Department of Health, 2004).• Improves mood, reduces anxiety, improves self-esteem and
confidence, improves body image.
Cancer
In England, over 220,000 people are diagnosed with cancer, with more than 120,000 dying each year from the disease (Department of Health, 2004).
• Reduces the overall risk. • Has a protective effect against colon cancer. • Reduces risk of breast cancer in post-menopausal women. • By reducing the risk of obesity, it offers a secondary preventative effect
against cancer (Department of Health, 2004).
Table 4.2 The effects of physical activity on the causes of various chronic health conditions
Planning exercise for health To maintain health and reduce the risk of chronic health conditions, it is recommended that all adults (aged 18 to 65 years) achieve the following physical activity guidelines as a minimum!
• Adults should aim to be active daily. Over one week activity should add up to at least 150 minutes of moderate-intensity activity in bouts of ten minutes or more. One way to approach this is to do 30 minutes of activity on at least five days a week.
• Alternatively, comparable benefits can be achieved through 75 minutes of vigorous-intensity activity spread across the week or a combination of moderate- and vigorous-intensity activity.
• Adults should also undertake physical activity to improve muscle strength on at least two days a week.
• All adults should minimise the amount of time spent being sedentary (sitting) for extended periods.
• Higher volumes of activity are associated with even greater health benefits.
Department of Health (2011); ACSM (2014)
MODERATE VIGOROUS
• Fly fishing.• Gardening.• Cricket.• Golf.• Cycling for
pleasure.• Walking briskly.• Mowing the
lawn.• Recreational
badminton.
• Rowing.• Swimming.• Hard cycling.• Circuit training.• Running at 7
mph.• Hockey, squash
and tennis.• Hill walking.• Skipping.• Stair climbing.• Cross country
skiing.• Rock climbing.
Table 4.3 Examples of activities considered moderate or vigorous
InTEnSITy dESCRIPTIonSLight activity is defined as little or no exertion that does not normally cause a noticeable change in breathing.
Moderate activity requires sustained, rhythmic muscular movements (at least the equivalent of brisk walking) and leaves a person feeling warm and slightly out of breath.
Vigorous activity requires sustained, large muscle movements at 60%-70% or more of maximum heart rate; a level that makes a person sweaty and out of breath.
Copyright © 2014 Active IQ Ltd. Not for resale | 183
Section 4: Health benefits of physical activityPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Types of activity
Physical activity to improve health can include a range of activities, including activities of daily living, structured exercise and playing sport.
ACTIVITIES OF DAILY LIVING (ADLS)
ACTIVE LEISURE AND RECREATION (INCLUDING STRUCTURED EXERCISE)
SPORT (SOCIAL OR COMPETITIVE)
• Vigorous housework.• Gardening.• Cleaning the car.• DIY.• Active travelling.• Active work (not desk-
based).• Active play.• Using stairs more often.
• Gym training. • Group exercise to music.• Aqua aerobics. • Circuit training.• Health walks. • Cycling. • Swimming. • Dance and movement. • Yoga.• Pilates. • Outdoor activities, e.g. hill walking
and climbing.
• Games, e.g. basketball, football, cricket, netball, rugby, hockey.
• Athletics, e.g. various track and field.
• Water sports, e.g. swimming, sailing, rowing.
• Individual sports, e.g. judo, boxing, weight-lifting, swimming.
Table 4.4 Types of physical activity
End of section: Learning checkAnswer the following questions and make notes to revise this section.
• What are the health benefits of physical activity?
• State two population groups that are reported as being less active.
• Name the modifiable and non-modifiable risk factors of cardiovascular disease.
• State some of the positive effects of activity on the following health conditions:
• Hypertension.
• Obesity.
• Diabetes.
• Asthma.
• Depression and anxiety.
• Osteoporosis.
• Osteoarthritis.
• What are the current physical activity recommendations to improve health?
• Describe the difference between moderate and vigorous intensity.
• What does ADL stand for?
• Give some examples of ADLs.
184 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 4: Health benefits of physical activity

Section 5: Monitoring exercise intensity
Monitoring exercise intensity is essential for ensuring an exercise programme is safe and effective and checking that clients are working at an appropriate level.
It can provide useful information to determine the success of the session in the short term and provide a benchmark against which future sessions can be progressed and reviewed.
Key methods for monitoring intensity include:
• The talk test.
• Rating of perceived exertion.
• Heart rate monitoring.
Benefits and limitations of different methods of monitoring exercise intensity
The talk test
When working aerobically and at a moderate intensity an individual should be able to hold a conversation with a mild level of breathlessness at the end of a sentence. If they are able to speak with little effect on their breathing the activities would be low intensity. If they can only speak a couple of words and are highly breathless they are working at a much higher intensity.
The talk test is an easy and simple method to use and doesn’t require any specialist equipment or specific learning from the client. The instructor can ask the client questions and gauge their response. Its limitations are that it is less accurate than other methods and interpretation is subjective. As a guideline:
Light activity is measured by talking easily and breathing lightly, but heart rate has increased.
Moderate activity is measured by talking comfortably, but breathing is deeper and quicker, and the body is warming up.
Vigorous activity is measured by talking with more difficulty, breathing more deeply and harder (heavy increasing to very heavy). Breathing becomes increasingly difficult as intensity increases to a point when there is a shortness of breath and an inability to carry on a conversation.
TALKING EASILY AND LIGHT BREATHLESSNESS
TALKING EASILY BUT MORE BREATHLESS
TALKING BECOMES MORE DIFFICULT AND BREATHING IS HEAVIER
LIGHT ACTIVITY
MODERATE ACTIVITY
VIGOROUS ACTIVITY
UNABLE TO TALK AND BREATHING VERY HEAVY
Copyright © 2014 Active IQ Ltd. Not for resale | 185
Section 5: Monitoring exercise intensityPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Rating of perceived exertion (RPE)
The RPE method was developed by the Scandinavian physiologist Gunnar Borg. There are two main variations of the Rating of Perceived Exertion (RPE) scale.
• The original RPE scale runs from 6 to 20 and is supposed to reflect heart rates ranging from 60-200 bpm (see table 5.1).
• The modified CR10 scale runs from 0 to 10 and offers a more user-friendly approach (see table 5.2).
It is recommended that intensity for aerobic work should remain somewhere between 12 and 13 on the original scale and between 4 and 7 on the CR10 scale.
A key limitation is that it takes time and practice for individuals to become proficient at using the scales. Effort is also very subjective and individuals have different perceptions of difficulty. The methods work most effectively with individuals who are more experienced at training and rating the sensations they experience.
HEART RATE RPE CLASSIFICATION
60-80 bpm 6-8 Nothing
< 90 bpm < 9 Very light
~ 100 – 110 bpm 10 - 11 Light
~ 120 – 130 bpm 12 - 13 Moderate
~ 140 – 160 bpm 14 - 16 Heavy
> 160 bpm >16 Very heavy
Table 5.1 The classic 6-20 Borg RPE scale
MODIFIED RPE/CR10 TRAINING ZONE
Nothing at all 0 Warm-up/cool-down zone
Very, very weak 0.5
Very weak 1
Weak 2
Moderate 3
Somewhat strong 4 Aerobic zone
5
Strong 6
Very strong 7
8 High-intensity intervals – anaerobic zone
Very, very strong 9
10
Table 5.2 Rating of perceived exertion (RPE) modified CR10 scale
RATING OF PERCEIVED EXERTION RPE provides a scale of how hard an individual feels they are working when they exercise. The response of the client should take into account all the symptoms of exertion, such as breathing, muscular fatigue and the subjective feeling of effort.
186 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 5: Monitoring exercise intensity

Heart rate monitoring and the use of different heart rate zones Heart rate is traditionally the most common method of monitoring exercise intensity. The main methods for determining heart rate are to manually measure the pulse in the wrist or neck, or to use a heart rate monitor. The latter method is more accurate.
The guidance for improving cardiovascular fitness is that individuals should work at a target heart rate (THR) range between around 50-90% of their maximum heart rate (MHR or HR max), depending on their fitness level. Beginners should exercise at the lower end of their range (50%) and increase intensity progressively over a number of weeks, as the body becomes more conditioned to exercise.
Maximal heart rate (MHR or HR max)
To calculate maximum heart rate use the equation:
220 BEATS PER MInUTE (BPM) – AgE
The main limitation of this calculation is it can only be used as an estimate of MHR due to a potential error range of plus or minus around 11 bpm. The only way to truly determine an individual’s actual HR max is to exercise them to exhaustion and measure their heart rate at this intensity. However, this level of assessment is not appropriate for most clients.
Target heart rate or training heart rate (THR)
Target heart rate (THR) is 50-90% of MHR. THR can be calculated by multiplying the individual’s MHR x 0.5 (50% THR), 0.6 (60% THR), 0.7 (70% THR), 0.8 (80% THR) or 0.9 (90% THR) to get the lower and upper limits of the target heart rate zone.
Heart rate zones
The intensity levels recommended by the ACSM (2014) are:
MAXIMAL HEART RATE 220 – AGE = MHRFor a 26-year-old this would be:
220 – 26 = 194 bpm
TARGET HEART RATE MHR X 0.6 = 60% THRMHR X 0.9 = 90% THRFor a 26-year-old this would be:
194 x 0.6 = 116 bpm
194 x 0.9 = 175 bpm
MODERATE INTENSITY VIGOROUS INTENSITY
50-65% OF MHR 65-90% OF MHR
Copyright © 2014 Active IQ Ltd. Not for resale | 187
Section 5: Monitoring exercise intensityPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

As intensity and heart rate increase, energy production will shift from aerobic towards anaerobic; the latter of which cannot be sustained for a long duration due to the accumulation of lactate.
100% (MHR) Maximal intensity Anaerobic
90% Vigorous intensity Anaerobic threshold
Lactate accumulation in the blood increases 80% Vigorous intensity
70% Vigorous intensity
60% Moderate intensity Aerobic
50% Light intensity
One myth associated with aerobic training zones and heart rates is that lower training heart rates represent a ‘fat burning zone’. There is no direct relationship between an individual’s heart rate and their metabolism of fat while exercising. Some individuals have been recorded as metabolising fat at up to 97% of their HR max, while others stopped metabolising fat at 54% of their HR max. Individuals respond very differently to exercise and any attempt to provide standard calculations or zones cannot be accurate for all people.
Observation
Observation is another subjective method for monitoring intensity. Observations may include:
• Posture and alignment.
• Levels of coordination.
• Exercise technique.
• Facial expressions.
• Skin colouring (pallor around the lips may represent reduced oxygen).
• Sweating.
While each of these may provide some general indication of fatigue, particularly if the client’s response is well known, there is no direct research-based evidence on their validity.
In practice a combination of methods may be useful for monitoring the response of a single client or a group of participants.
End of section: Learning checkAnswer the following questions and make notes to revise this section.
• What are the benefits and limitations of the talk test?
• What does RPE stand for?
• What are the benefits and limitations of RPE?
• What are the benefits and limitations of heart rate monitoring?
• What does MHR stand for?
• What does THR stand for?
• How would you calculate an individual’s maximum heart rate?
• How would you calculate 80% of an individual’s target heart rate zone?
188 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 5: Monitoring exercise intensity

Section 6: Contraindications to exercise and key safety guidelines for special populations
Working with any special population group on a regular basis requires a full understanding of their specific needs. Further training and qualifications will ensure that any specific needs are fully understood and can be accommodated when developing exercise programmes.
However, if a comprehensive screening is conducted it may identify that a client is apparently healthy and has no contraindications for exercise. In these circumstances the person may participate on a non-regular basis provided any required adaptations are made.
Populations that are considered specialist include:
• Older adults (50+).
• Pre- and post-natal women.
• Young people (14-16).
• Disabled people.
PRE-EXERCISE SCREENINGA comprehensive pre-screening process needs to be completed prior to participation to check for any medical considerations that need to be signposted to and cleared by a GP.
Any client responding ‘yes’ to the PAR-Q questions, should be signposted to a GP prior to participation.
Older adults (50+)The ageing process is characterised by progressive loss and decline in the functioning of the skeletal/cardiovascular and neuromuscular systems (see table 6.1).
These changes affect fitness potential and safety during exercise. They require adaptation of exercise to be considered to meet specific needs.
EXPERT TIPOlder adults are:• Aged 65 and over. • Aged 50-64 with
chronic health conditions or physical limitations.
ACSM, 2014
GP REFERRAL All medical conditions should be signposted to a GP prior to participation.
Ageing is a natural and highly individual process. It often begins to take effect around the age of 50; with the effects becoming more noticeable and apparent around the age of 65. The progressive decline in functioning may lead to reduced mobility, loss of independence, increased frailty and increased risk of falls for some older adults.
However, people of the same age may not have the same loss of functioning. Those who maintain an active and healthy lifestyle may delay some of the effects of ageing to a much later age. Alternatively, those who are inactive and who follow an unhealthy lifestyle, may show more marked signs of ageing at a much younger age (40 or earlier).
Contraindications to exercise may include:
• Unstable or controlled medical conditions (diabetes, asthma, angina).• Resting blood pressure greater than 180/90. • Resting heart rate over 100 bpm. • Joint condition made worse by exercise. • Unexplained dizziness. • The effects of the ageing process.
Copyright © 2014 Active IQ Ltd. Not for resale | 189
Section 6: Contraindications to exercise and key safety guidelines for special populationsPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Ageing affects all body systems and once the process is underway there is a corresponding 1-2% decline in physical capacity each year. Functional declines (such as loss of flexibility, agility and mobility) make everyday activities harder to perform, e.g. getting up and down from the floor/chairs safely. These changes may partly contribute to the reduction of activity levels associated with ageing.
There will also be longevity of exposure to risk factors for some chronic health conditions: increased joint wear and tear (osteoarthritis); loss of bone mass (osteoporosis); atherosclerosis (hypertension, coronary heart disease).
EFFECTS OF AGEING FITNESS POTENTIAL CONSIDERATIONS
• Fewer fast twitch muscle fibres. • Weaker and smaller muscle fibres. • Reduced motor neurons. • Reduced neuromuscular transmission (fewer nerves
sending messages).• Reduced capillaries in the muscle. • Increased connective tissue. • Sensory decline (loss of hearing and vision). • Cognitive decline.
• Reduced muscular strength. • Reduced muscle power. • Reduced coordination. • Reduced movement speed.• Reduced muscular endurance. • Reduced flexibility and range of motion. • Reduced balance and coordination. • Reduced postural stability. • Reduced short-term memory.
• Loss of bone mass and reduced bone density.• Increased risk of osteoporosis. • Reduced availability of synovial fluid. • Calcification of the joints (calcium laid down in the
cartilage).
• Bones less resilient to stress and more susceptible to fracture.
• Stiffer, less mobile joints. • Reduced shock absorption in the joints.
• Reduced stroke volume and cardiac output. • Less efficient heart and circulatory system. • Increased blood pressure. • Fewer capillaries. • Less elastic vessels.• Reduced intake, uptake and utilisation of oxygen.
• Lower maximal heart rate. • Lower training heart rate. • Slower recovery rate. • Decreased tolerance to fatigue. • Tire quicker.• Lower anaerobic threshold. • Less tolerant of high-intensity exercise.
Lawrence (2008)
Table 6.1 Effects of ageing and considerations
190 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 6: Contraindications to exercise and key safety guidelines for special populations

Safety considerations and guidelines
Prior to participation all clients should be pre-screened. A healthy older adult between the ages of 50 and 65 can be reasonably accommodated in a regular exercise session, with appropriate adaptations to meet any specific age-related needs (see table 6.2).
Older adults aged over 65 or between 50 and 64 with health conditions would need to be signposted to a GP for advice, as they may require referral to a specialist exercise referral instructor.
The following general guidelines are recommended for all adults over 50 to minimise the risk of any adverse effects.
COMPONENT ADAPTATION
Warm-up and preparation
• Use a longer, more gradual warm-up (around 15 minutes).• Use more mobility exercises.• Build range of motion of mobility exercises gradually. Begin with moderate range
mobility exercise (e.g. small shoulder circles) before increasing the shoulder ROM and progressing to arm circles.
• Use slower controlled movements.• Focus on posture, alignment and correct technique.
Cardiovascular training
• Build intensity more gradually. • Lower working intensity. • Use less impact. • Use less choreography (group exercise to music).• Use a longer, more gradual cool-down.• Emphasise correct technique.• Layer information (in stages rather than all at once).
Muscular training • Use less resistance and shorter leverage for some exercises. • Use fewer repetitions and sets, and more rest. • Use more stable and balanced positions. • Allow transition time to get down and up from the floor. • Use slower pace. • Use more time to change exercises/positions. • Emphasise correct technique. • Supine lying may be contraindicated (osteoporosis); extreme spinal flexion (i.e. full or
half curl-ups from supine) may be contraindicated (consider other alternatives). • Strengthen postural muscles, pelvic floor muscles and around potential fracture sites
for osteoporosis (wrist, hip and spine).
Cool-down and closing
• Use longer duration. • Perhaps use more stretches for specific muscles. • Use more stable positions. • Use smaller range of motion.
Table 6.2 Adaptions for older adults
Copyright © 2014 Active IQ Ltd. Not for resale | 191
Section 6: Contraindications to exercise and key safety guidelines for special populationsPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Pre- and post-natal women Maintaining activity levels and exercise for healthy pregnant women is generally recommended. In most cases activity and exercise at the appropriate intensity are safe for both mother and baby and not associated with any adverse effects.
However, the PARmedX for pregnancy screening tool should always be completed prior to participation to identify any contraindications and reasons for exclusion or referral to a specialist instructor.
Note: The guidance offered in this section relates only to normal, healthy, adult women experiencing a normal, healthy, singleton pregnancy or women who have had a normal, healthy birth and who have had previous normal, healthy pregnancies and births.
The effects of pregnancy
The needs of pre- and post-natal clients vary depending on the stage of pregnancy and the different physiological effects. Some general effects include:
• Increased heart rate.
• Increased stroke volume.
• Increased cardiac output.
• Increased oxygen uptake.
Other specific effects at each trimester are listed in table 6.3.
EXPERT TIPRelative contraindications: • Very sedentary
lifestyle. • Severe anaemia. • Morbid obesity. • Extreme
underweight.• Heavy smoker.
Absolute contraindications: • Heart or lung
disease.• Persistent second
or third trimester bleeding.
• Preeclampsia/pregnancy induced hypertension.
• Premature labour.
ACSM, 2014
TRIMESTER 1
(0-3 MONTHS)
TRIMESTER 2
(3-6 MONTHS)
TRIMESTER 3
(6-9 MONTHS)
POST BIRTH
Increase in weight + 1-3kg. Breasts and uterus start to enlarge. Hormonal changes commence, e.g. increased relaxin affects ligaments and joint stability.Morning sickness.
Increase in weight + 6-8kg.Postural changes (shoulder girdle protraction, thoracic kyphosis, long upper back extensors and short, tight pectoral muscles). Possible low back pain, neck or shoulder pain. Abdominal muscles start to lengthen and stretch as baby grows.Change in centre of gravity.
Increase in weight + 3-4 kg. Tired more easily. Venous return may be reduced. Weight of baby presses on pelvic floor. Pelvic girdle less stable (effects of relaxin).Weight of baby places stress on lower spine (increased lordotic curve).Centre of gravity changes affect balance.
Avoid physical stress for two weeks. Return to activity normal birth (six weeks) caesarean birth (12 weeks).Hormone levels still high (up to one year).Weaker pelvic floor.Pelvic girdle less stable. Check for diastasis rectii (abdominal separation).Rectus abdominis is mechanically weaker for at least 12 months.
The physiological and postural changes of pregnancy persist for several months after birth, making women vulnerable to injury and long-term physical health problems, such as pelvic floor dysfunction. This has particular significance for exercise involving impact, twisting and rapid, ballistic or aggressive movements, which should be avoided for at least six months and introduced progressively.
Table 6.3 Physiological changes at different stages of pregnancy
192 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 6: Contraindications to exercise and key safety guidelines for special populations

Pre-natal adaptations to session structure and content
Pregnant women should always exercise according to how they are feeling. Hormonal and postural changes make them more vulnerable to injury, joint misalignment, muscle imbalance and motor skills decline, especially if they are genetically hypermobile. These changes may start from very early in pregnancy and gradually become more significant as pregnancy progresses. Pregnant women are vulnerable to nausea, dizziness and fainting.
Pregnant women should avoid:
• Exercising in the supine position after 16 weeks.
• Exercising to the point of exhaustion (the goal is to maintain activity, rather than improve fitness).
• Prone lying exercise.
• Prolonged motionless standing.
• Heavy, uncontrolled, isometric or prolonged resistance work above the head.
• Leg adduction and abduction against a resistance.
• Isometric exercises.
• Loaded forward flexion.
• Rapid changes of direction or position.
• Uncontrolled twisting.
• Exercise with a risk of falling or abdominal trauma.
• Excessive and uncontrolled de-stabilisation (balance) techniques.
• Abdominal exercises (focus instead on posture, mobility and pelvic floor).
Post-natal adaptations to session structure and content
Women should not begin exercising post birth until they have received the permission of their healthcare professional, usually at the post-partum six-to-eight-week check.
After birth (prior to progressing to more vigorous exercise) the focus should be to re-educate posture and joint alignment, address muscle imbalances, improve stability and motor skills, and encourage transversus abdominis (TA) recruitment and pelvic floor function.
A woman should be referred to a health professional if she is experiencing any of the following symptoms post birth:
• Stress incontinence or pelvic floor muscle weakness.
• ‘Dragging’ pain or a feeling of heaviness in the lower abdominal or pelvic floor area.
• Groin, low back pain or difficulty walking; even if mild and intermittent.
• Abdominal muscle weakness, excessive abdominal doming, abdominal muscle separation or softness/sinking at the umbilical mid-line, umbilical hernia.
Exercise should stop and a doctor or midwife should be consulted by the participant if any abnormal symptoms occur, for example:
• Dizziness, faintness or nausea.
• Bleeding or leakage of amniotic fluid.
• Abdominal or contraction type pain.
• Unexplained pain in the back, pelvis, groin, buttocks or legs.
• Excessive shortness of breath, chest pain or palpitations.
Copyright © 2014 Active IQ Ltd. Not for resale | 193
Section 6: Contraindications to exercise and key safety guidelines for special populationsPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

CLASS COMPONENT ADAPTATIONS
Warm-up and preparatory phase
• Emphasise correct posture at the start and throughout the session.• Make movements slower and more controlled.• Increase the number of mobility exercises.• Use full range of motion mobility exercises to warm the muscles.• Build up intensity of movements much more gradually to avoid sudden increases in
blood pressure.• Support stretch positions and take care not to exceed a comfortable range of motion.
Cardiovascular • Use low to moderate intensity. • Use low impact.• Use more gradual build up and lowering of intensity. • Use less choreography (group exercise to music).• Use slower tempo.• Women who are unused to exercise should start with shorter durations (begin with
15 minutes and increase gradually to 30 minutes).• Maintain adequate hydration. • Avoid exercising in very hot or humid conditions.• Avoid heart rate monitoring – use the talk test.
Muscular fitness • Include exercises for the pelvic floor muscles.• Avoid supine and prone lying (pre-natal).• Select comfortable starting positions.• Avoid exercises which may place too much pressure on the pelvic girdle.• Use movements related to everyday life.• Perform fewer repetitions.• Use lower and less intense exercises.• Do not use heavy abdominal exercises; sit-up, crunch or oblique cross-over type
exercises are not an appropriate choice for abdominal muscle re-education post birth.
Cool-down and closing • Include specific relaxation work. • Avoid positions which may over stretch the ligaments.• Select balanced and comfortable positions for passive stretching.• Use shorter-hold stretches to maintain rather than develop flexibility.
Table 6.4 General adaptations
194 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 6: Contraindications to exercise and key safety guidelines for special populations

Disabled peoplePeople often automatically think of disabled people as wheelchair users; in fact they make up only 6% of the disabled population. The majority of registered disabled people (around 8-10 million in the UK) have other health and physical conditions, which include:
• Blindness or partial sightedness.
• Deafness or partial hearing.
• Down’s syndrome.
• Stroke.
• Obesity.
• Arthritic conditions.
• Mental health conditions (e.g. severe depression).
• Cancer.
• HIV.
• Limb amputation.
• Fibromylagia.
• Cerebral palsy.
Benefits and barriers to activity
Regular physical activity in a safe and supportive environment offers many health benefits for disabled people. It will reduce the risk of developing chronic health conditions and can help to maintain and improve independence.
Disabled people are one of the populations identified as not meeting the recommended levels of physical activity. Many disabled people find they experience various barriers to accessing sufficient physical exercise. Promoting physical activity and enabling participation are therefore priorities.
The Equality Act (2010)
The Equality Act 2010 brings all previous legislation regarding diversity and discrimination into one document. A requirement of the Act is that service providers must make ‘reasonable adjustments’ to their facilities and services so that they are accessible to disabled people. Adjustments to buildings and services must be made in expectation of attendance by disabled people to enable inclusion rather than exclusion.
The Inclusive Fitness Initiative (IFI)
The IFI provides guidance and support to operators interested in welcoming disabled people into their facilities and to disabled people interested in getting active. This guidance is provided in line with their policies.
Disability
‘An umbrella term covering impairments, activity limitationsand participation restrictions.’
(World Health Organisation)
• Impairment: a problem in body function or structure.
• Activity limitation: a difficulty encountered by an individual in executing a task or action.
• Participation restriction: a problem experienced by an individual in involvement in life situations.
LEGISLATIONService providers must anticipate the needs of disabled clients and make reasonable changes to accommodate these.
Equality Act (2010)
Copyright © 2014 Active IQ Ltd. Not for resale | 195
Section 6: Contraindications to exercise and key safety guidelines for special populationsPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Contraindications and safety considerations
Prior to participation it is essential to pre-screen (PAR-Q) and check for any contraindications (e.g. stage 3 hypertension, heart conditions) and seek clearance and guidance from a GP or health professional. Specific medical conditions will require activity interventions led by a specialist instructor.
To enable participation the following must be considered for adaptation in relation to the needs of the individual.
These conditions worsen over time, e.g. multiple sclerosis. Careful monitoring is required to ensure that the exercise programme does not cause the condition to worsen (exacerbation).
These conditions result in a difference in strength between the left and right sides of the body, e.g. stroke and cerebral palsy. The aim should be to improve the affected side as much as possible without neglecting the unaffected side. If the nerves controlling the affected side have been partially or completely damaged the ability to improve in the affected muscles is greatly reduced.
EXERCISE SELECTION:This will be determined by specific needs and may include:
Simplifying some exercises.
Reducing intensity (fewer repetitions, lower resistance, appropriate range of motion, controlled rate).
Modifying exercise positions and modalities, e.g. using wheelchair-based activities for wheelchair users or chair-based activities for individuals with physical or functional limitations or issues with balance.
TEACHING STYLE: Teaching style and methods will need to accommodate specific needs and may include:
Clarity of verbal instructions for the blind or visually impaired.
Clarity of demonstrations; facing the person and speaking clearly when instructing the deaf or those with partial hearing (e.g. to enable lip reading).
Finding appropriate ways to engage and encourage people with learning disabilities, e.g. Down’s syndrome.
HEALTH AND SAFETY: This will include consideration of entry and access to all facilities; safe evacuation procedures in emergencies and respect to other legislation e.g. safeguarding vulnerable adults.
PROGRESSIVE DISORDERS:
ASYMMETRICAL WEAKNESS:
196 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 6: Contraindications to exercise and key safety guidelines for special populations

Many physical disabilities present with spastic muscles that are very tight or rigid. Flexibility training is important. Seek advice from a suitably trained medical authority on how to stretch a spastic muscle without causing injury before incorporating any flexibility into a programme.
These affect the central nervous system (CNS), e.g. muscular dystrophy. Muscles can become progressively weaker as a result of the decline in CNS functioning; this can be offset in the programme by working on general fitness levels. Any rapid decline in function should immediately be referred to their GP for guidance.
Damage to sensory nerves occurs with many types of physical disability. An inability to detect pressure against the skin can result in a pressure sore. Using a wheelchair increases the risk of developing pressure sores and clients will usually be aware of the importance of frequent checks. The use of gym equipment may also bring similar risks and so additional checks should be advised.
This is a disabling condition in its own right. It can sometimes be a secondary condition resulting from the physical and psychological challenges of living with a disability. Depression reduces motivation and energy levels and can contribute to drop-out from the programme. Medications used to treat depression have many negative side effects, including weight gain and suicide risk.
SPASTICITY:
NEUROLOGICAL CONDITIONS:
SENSORY NERVE DAMAGE:
DEPRESSION: TRAINER TIP Always refer to a medical authority if there are any doubts regarding the ability to work safely and effectively with a disabled client.
Young people (14-16)Most healthy 14-16 year olds can be accommodated within a regular exercise session with basic modifications. However, it is advisable to seek further training on working with adolescents to gain understanding of the physiological and psychological changes that affect this age group. As with all populations a comprehensive pre-screening process is essential and any medical conditions must be signposted to a GP prior to participation.
Growth plate fractures
The growth plate is the weakest area of the growing skeleton. Growth plate fractures account for up to 15% of all childhood fractures with the greatest incidence among 14-16-year-old boys and 11-13-year-old girls. A serious injury to a joint is more likely to damage the growth plate than the ligaments around it.
Preventative measures to avoid growth-related injuries include:
• Avoid excessive training; this includes playing too much of one sport, playing the wrong sport for the young person’s body type or using a resistance that is too heavy.
• Consider gender differences and the differing stages of development.
• Avoid inappropriate size matching in pairs activities.
• Avoid too much static, high-impact activity, e.g. jogging on the spot.
• Warm up and cool down thoroughly.
• Use appropriate equipment for the activity, e.g. correct size and weight.
Copyright © 2014 Active IQ Ltd. Not for resale | 197
Section 6: Contraindications to exercise and key safety guidelines for special populationsPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Flexibility
During the growth spurt there is an increased injury risk because the soft tissue around the joints is already stretched, as muscle growth does not keep up with bone growth.
Caution should be taken when teaching any stretch exercise. The aim should be to stretch only to the point of mild tension and to avoid overstretching.
TRAINER TIPProgression should only be applied when correct technique is mastered.
TRAINER TIPThe main cardiovascular and respiratory differences between adolescents and adults include: • Lower cardiac output. • Lower stroke volume.• Higher heart rate. • Lower blood pressure. • Higher respiratory rate.
ACSM, 2014
Limb length
During the growth spurt young people have disproportionately long legs, meaning that they are biomechanically out of balance and are potentially less coordinated.
Technique
Young adults have not generally developed their ‘body awareness’ and coordination. They require closer supervision to ensure correct alignment. To reduce the risk of injury, begin with simple non-complex, low resistance exercises and, where possible, use movement patterns that replicate everyday activities. Progression should only be applied when technique is correct.
Gymnasium equipment
The resistance machines in most gyms are designed for adult users and the weight increments are generally too great for young people. Free weights can be a better choice because they allow smaller weight increases and their safe and effective use is not dependent on the size of the exerciser. Care should be taken to ensure correct technique.
Cardiovascular and cardiorespiratory considerations
Young adults have smaller heart chambers and lower heart volumes. This results in a lower stroke volume at rest and during exercise. Chamber size and blood volume gradually increase with body growth. The lower stroke volume is compensated by having higher maximal heart rates. However, higher heart rates cannot fully compensate for the lower stroke volume and so cardiac output (volume of blood pumped from the left ventricle in one minute) is lower.
Young adults generally have lower blood pressure than adults, mainly because they have not been exposed to the risk factors affecting blood pressure for so long (longevity effects).
Lung volume and peak flow rates steadily increase until full growth. For example, maximum ventilation increases from 40L/min at five years of age to more than 110L/min as an adult. This means that children and young people have higher respiratory rates than adults; 60 breaths per minute compared to 40 breaths per minute for the equivalent level of exercise.
The measure of the amount of ventilation (passage of air in and out of the lungs) required for each litre of oxygen consumed (VE/VO2) is also higher in young people, which means that children have inferior pulmonary functions.
Children and young people’s arterial/venous oxygen difference is greater and this suggests that a greater percentage of the cardiac output goes to the working muscles than for an adult and is another way that children/young adults compensate for their lower stroke volume.
198 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 6: Contraindications to exercise and key safety guidelines for special populations

Aerobic capacity in young people is higher in absolute terms; VO2 max (measured in L/min) increases from age 6-18 for boys and age 6-14 for girls. However, little change is observed with age when VO2 max is normalised by bodyweight. There is a slight decline after puberty in girls because of the increase in body fat rather than muscle mass, with VO2 max slightly increasing at puberty for boys as a result of the increase in muscle mass. Any absolute difference in VO2 max does not limit endurance performance. Young people more often lack technique and coordination and end up with poor economy of movement in activities such as running.
Anaerobic exercise
The anaerobic capacity for both boys and girls increases with age, but is not fully developed until around the age of 20. Young people have less glycogen stored per gram of muscle and have fewer stores of creatine phosphates. They have a lower anaerobic work level and should work at lower-to-moderate intensity rather than higher intensities. Activities to avoid until they reach physical and skeletal maturity include: power lifting, body building and maximal resistance lifts.
Body temperature and dehydration
Young people have an inferior cooling mechanism due to low blood volume and high skin temperature. They are sensitive to heat stress because they expend more energy per kilogram of bodyweight than an adult during exercise.
Adolescents are at risk of dehydration when exercising due to overheating. In the cold they lose heat more quickly due to their relatively large surface area compared to their mass.
Summary of the key safety considerations
GROWTH RELATED ISSUES AND INJURIES: Lower impact and lower intensity (fewer repetitions, less resistance) and avoid overtraining.
FLEXIBILITY: Modify stretch positions, stretch to the point of mild tension (without overstretching), modify range of motion and focus on correct technique, avoid ballistic stretching.
TEMPERATURE: Maintain hydration, lower intensity and avoid exercise in humid conditions.
SELF-ESTEEM AND CONFIDENCE: Be mindful of any lack of confidence and low self-esteem and how this may affect behaviour and motivation. Body image issues may be apparent (eating disorders would present a contraindication for exercise).
MEDICAL CONDITIONS: The presence of any medical conditions need to be signposted to a GP prior to participation.
OBESITY: This may present with other CVD risk factors (inactivity, hypertension, high cholesterol, diabetes) that negatively affect health. These need to be signposted to a GP prior to participation.
IMMATURITY: This may affect behaviour and regard for safety.
REDUCED COORDINATION AND MOTOR SKILLS: Simpler and non-complex activities with less technical demand. Focus on exercise technique and adapt teaching style to match needs.
TRAINER TIP • Maintain hydration; give
regular water breaks.• Avoid exercise in hot
humid conditions. • Use a less intense warm-
up component. • Use active rests between
bouts of vigorous activity.
Copyright © 2014 Active IQ Ltd. Not for resale | 199
Section 6: Contraindications to exercise and key safety guidelines for special populationsPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Frequency Aerobic – every day.Strength – three days a week.Bone strengthening – three days a week.
Intensity Moderate-to-vigorous-intensity aerobic exercise.
Time 60 minutes.
Type Cardio – swimming, dancing, cycling, running, walking.Strength – climbing trees, games (tug of war) as well as resistance exercises. Bone strengthening – jumping, running, skipping, hop scotch and games (basketball, tennis, etc.).
Table 6.5 Recommended guidelines for children and adolescents
End of section: Learning checkAnswer the following questions and make notes to revise this section.
• What is an essential first action prior to working with any specialist population?
• List some of the contraindications (when not to exercise) for the following groups:
• Older adults.
• Pre-natal women.
• Post-natal women.
• Young people.
• Disabled people.
• List some of the safety considerations for working with each of the following groups:
• Older adults.
• Pre-natal women.
• Post-natal women.
• Young people.
• Disabled people.
• What action would you take if you had any specific concerns about being able to work with a specialist population?
• What action would be appropriate if an older adult presented with a number of cardiovascular risk factors?
• What is the Equality Act 2010?
200 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 6: Contraindications to exercise and key safety guidelines for special populations

Section 7: The importance of healthy eating
Nutritional fitness is a key component of health and total fitness. The foods eaten as part of the daily diet influence energy levels during exercise and affect overall health and wellbeing. Fitness professionals are often asked for advice and support in helping clients to achieve goals that require them to change their eating habits. It is important to respect professional boundaries when providing information or advice relating to nutrition. Only state-registered dietitians are qualified and insured to provide detailed, specific nutrition advice and diagnose nutrient deficiencies. When providing nutrition information to clients ensure that only evidence-based guidelines are referred to and focus on using a coaching approach to help clients adopt and maintain the healthy eating approaches they suggest for themselves. Advising a client to follow a specific diet or take a specific supplement could lead to illness and constitute negligence.
Health risks of poor nutritionIn the short term an unhealthy diet can cause fatigue and lethargy, poor concentration and memory, headaches and various vitamin and mineral deficiencies.
The foods eaten as part of the diet contribute to an individual’s overall health and wellbeing. A healthy diet with a balanced intake of the main nutrients can help to prevent and manage many health conditions. An imbalanced and unhealthy diet and poor nutrition offers a significant risk to health and wellbeing.
Professional role boundaries in offering nutritional adviceSpecific dietary advice and guidance should only be given by an appropriately qualified and registered dietitian. Their role is to analyse eating behaviours and determine specific nutrient deficiencies from which they can prescribe food and supplementation to meet the individual’s needs and promote optimal health.
Fitness instructors should only provide general healthy eating guidance to healthy individuals. Any guidance offered should reflect the current UK guidelines.
It would be outside of scope of practice to plan or give advice on specific diets or food supplements or to give advice to clients who have specific health conditions (e.g. diabetes or obesity).
Poor nutrition is a contributory factor for a number of physical and mental health conditions including:
• Obesity.
• Type 2 diabetes.
• Coronary heart disease.
• Hypertension.
• High cholesterol.
• Stroke.
• Some cancers.
• Depression and stress.
• Dementia.
• Asthma.
• Some types of arthritis.
• Menstrual irregularities.
• Osteoporosis.
• Infertility.
• Eczema.
Copyright © 2014 Active IQ Ltd. Not for resale | 201
Section 7: The importance of healthy eatingPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Figure 7.1 The Eatwell plate
The national food model The national food model in the UK is the ‘Eatwell plate’. The model provides guidance on healthy eating for the general public and aims to ease some of the confusion that often arises when trying to plan a menu.
Healthy eating advice that underpins a healthy diet
The eight main guidelines for healthy eating provided by Public Health England in conjunction with the Welsh Government, Scottish Government and the Food Standards Agency of Northern Ireland (2013) are:
Base all meals around starchy foods (rice, pasta, etc.).
Eat lots of fruit and vegetables (at least five portions per day).
Eat more fish (two portions a week, one portion of which should be oily fish).
Cut down on saturated fat and sugar (including processed and fast food).
Eat less salt, no more than six grams per day.
Get active and maintain a healthy weight.
Drink plenty of water (six-eight glasses per day).
Don’t skip breakfast.
ADDITIONAL ADVICE:Use the Eatwell plate when planning and cooking all meals. Check food labels (use the traffic light system).Eat only as much food (energy) as you need.
12345678202 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 7: The importance of healthy eating

Calorie and energy requirements
Energy intake and output is measured using kilocalories (kcals). The number of calories needed depends on many things, including activity levels.
Foods contain different macronutrients and have different calorie content:
• Carbohydrates – 4 calories per gram.
• Proteins – 4 calories per gram.
• Fats – 9 calories per gram.
• Alcohol (not a nutrient) – 7 calories per gram (calories from alcohol can easily increase energy input but have no nutritional value. They are nutritionally empty calories).
The recommendation is to eat and drink less of the food types that are high in calories (high sugar and fat content) and more of the foods that are lower in calories.
Table 7.1 provides some guidelines on the recommendations for specific foods.
FOOD GROUPS AND RECOMMENDATIONS GUIDELINES
Fruit and vegetables
(at least five a day)
One portion is 80g or any of these:• 1 apple, banana, pear, orange or similar-size fruit.• 3 heaped tablespoons of vegetables.• 1 dessert bowl of salad.• 1 glass (150ml) of unsweetened fruit juice.
Bread, rice, pasta and potatoes
(at least one starchy food with each meal)
• A bowl of wholegrain cereal (low in sugar and salt) for breakfast.
• A wholemeal sandwich for lunch.• An evening meal with potatoes, wholemeal pasta or
wholemeal rice as a base.
Meat, fish, eggs and beans
(eat some but cut down on fat)
To cut down on fat:• Choose lean cuts of meat. • Cut the fat off meat and the skin off chicken.• Grill instead of frying.• Eat fewer pies and sausages (high fat).• Eat a poached or boiled egg rather than a fried egg.
Pulses like beans, peas and lentils are low-fat, high-protein alternatives to meat. They are also high in vitamins and minerals.
Milk and dairy
(eat some, but ideally choose lower-fat options or eat smaller amounts of high-fat options)
Cheese, yoghurt, milk and fromage frais.
NB: Butter and cream are excluded because they are high in fat.
Food and drinks high in fat or sugar
(use minimally to help weight management)
• Cakes, biscuits, jam, honey, sweets, chocolate, ice cream.• Sugary drinks, puddings and pastries, crisps.• Butter, oils, margarine and spreads.• Cream and mayonnaise.
Public Health England, 2013
Table 7.1 Food consumption recommendations and guidelines
Copyright © 2014 Active IQ Ltd. Not for resale | 203
Section 7: The importance of healthy eatingPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Additional guidance for populations that have more specific and specialist needs, including babies and young children, older adults, pregnant women, and people with medical conditions are offered by Public Health England. Any specific and specialist dietary guidance should be provided by a registered dietitian.
Key nutrients and their dietary roleA healthy diet contains a balance of the main nutrient groups. Nutrients are the substances found in food, which the body is able to use for building material and fuel. There are five nutrient groups.
Carbohydrate
The primary role of carbohydrate is to provide the body with fuel for energy. The brain is dependent on glucose as a source of fuel and the working muscles use glycogen, particularly during more intensive exercise. For this reason, the body is able to store small amounts of carbohydrate as glycogen within the liver and the muscles. Sources of this nutrient are divided into three categories: sugar, starches and fibre.
CATEGORY DIETARY SOURCE
SugarsThese are simple structures, the most common of which is glucose.
• Fruit.• Fruit juice.• Dried fruit.• Table sugar.
• Honey.• Jams.• Confectionery.
StarchesThese are complex structures made mostly from long chains of saccharides.
• Bread.• Pasta.• Rice.• Cereals, grains
and beans.
• Potatoes.• Sweet
potatoes.• Vegetables.
Fibre These are indigestible forms of starch which help to keep the digestive system healthy.
• Fruit.• Vegetables.• Whole grains
and cereals.
• Beans and lentils.
• Sweetcorn. • Bran.• Nuts and
seeds.
Table 7.3 Dietary sources of carbohydrate
Fibre
Dietary fibre is a tough substance, which is found in unrefined starchy foods and cannot be broken down by the body to provide fuel. This indigestible material stays within the digestive system where it helps to provide bulk, which in turn enables the smooth passage of food and waste products along the digestive tract. Insoluble fibre helps to prevent constipation and bowel disease. Soluble fibre can also help to reduce cholesterol.
THE MICRONUTRIENTS
(NUTRIENTS NEEDED IN SMALL AMOUNTS)
THE MACRONUTRIENTS
(NUTRIENTS NEEDED IN LARGE AMOUNTS)
Table 7.2 The five main nutrient groups
1
2
3
4
5
CARBoHydRATE (CHo)
PRoTEIn
FAT
VITAMInS
MInERALS
204 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 7: The importance of healthy eating

Protein
Protein fulfils many functions, ranging from helping to transport important substances in the blood to allowing growth and repair of human tissue. Protein is particularly important to aid recovery from heavy and intensive physical training.
Proteins are made from building blocks called amino acids. There are 20 amino acids which the body uses to make the many proteins that it requires. The body is able to make some of these amino acids for itself, whereas others have to be gained from dietary sources.
There are two categories of foods which can provide these important building blocks: animal sources and plant sources.
CATEGORY FOOD EXAMPLES
Animal sourcesThese are an excellent source of protein; each source contains plenty of amino acids and in favourable amounts.
• Meat.• Poultry.• Fish.• Dairy
produce.• Eggs.
Plant sources These are a poorer source of protein, containing fewer amino acids and in smaller amounts. A vegetarian diet would need to contain a variety of plant sources to obtain all the essential amino acids.
• Grains.• Cereals.• Nuts.• Beans.• Pulses.
Table 7.4 Dietary sources of protein
Fat
Fat fulfils many vital functions in the body and is an important component of a balanced diet. Fat has the following functions:
• Forms an important component of cell membranes or walls.
• Helps the body to absorb and use the fat soluble vitamins – A, D, E and K.
• Provides insulation under the skin.
• Provides protection for the internal organs.
• Provides energy and a means of energy storage.
• Makes up the greater percentage of the brain and the spinal cord.
There are three basic categories of fat: saturated, monounsaturated and polyunsaturated. Each category is important for maintaining health and performance.
CATEGORY FOOD EXAMPLES
Saturated fat Mostly found in animal sources but also present in select plant sources, important for the body’s cells and the nervous system.
• Meat.• Eggs.• Dairy produce.
• Poultry skin.• Coconut oil.• Palm oil.
Monounsaturated fat Found in animal and plant sources, helps to protect from heart disease.
• Meat.• Olive oil.
• Peanut oil.• Avocados.
Polyunsaturated fat Found in fish and plant sources, important for cells and proper brain function.
• Oily fish.• Sunflower seeds.• Sunflower oil.
• Flax seed.• Dietary fats.
Table 7.5 Dietary sources of fat
KEY POINTSaturated fat recommendations:• Men – no more than 30g
of saturated fat a day.• Women – no more than
20g of saturated fat a day.
Public Health England, 2013
Copyright © 2014 Active IQ Ltd. Not for resale | 205
Section 7: The importance of healthy eatingPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

Vitamins and minerals
Vitamins and minerals are vital for normal growth, repair and daily functioning of the body. A diet rich in fruit and vegetables will be rich in vitamins and minerals. The simple rule when selecting fruit and vegetables to eat is variety and colour. A brighter and deeper colour signifies a greater overall nutrient content.
Minerals occur naturally within the soil and are drawn into plants via their root systems.
Vitamins are formed by plants and can be obtained in the diet by eating the appropriate plants or by eating products from the animals that have eaten those plants.
DIETARY SOURCES VITAMINS AND MINERALS
Plant sources• Fruit and vegetables.• Nuts.• Whole grains and cereals.
Variety and colour will ensure that a range of vitamins and minerals are supplied, e.g. green vegetables, citrus fruits, berries, beans, root vegetables will all supply different vitamins and minerals.
Animal sources• Meat.• Eggs.• Dairy produce.
These provide:• Fat soluble vitamins A, D, E and K.• Vitamin B6, B12 and folic acid.• Zinc.• Iron.• Calcium.
Table 7.6 Dietary sources of vitamins and minerals
The importance of adequate hydration An adequate intake of water is essential for life, health and performance. Water is found both inside and outside the body’s cells and there must be sufficient quantities present in order to maintain the many chemical reactions that support life and functioning. Water accounts for around two thirds of the weight of a healthy body. The amount of water required will depend on varying factors, for example:
• Environmental temperature.
• Body temperature.
• Humidity.
• Physical activity.
• Respiration rate.
Hydration
To stay adequately hydrated and prevent dehydration it is essential to replace the water that is lost through various bodily processes including breathing, sweating and urination.
The first sign of dehydration is feeling thirsty, but by the time thirst is sensed the body is already slightly dehydrated. Other signs of dehydration include headaches, feeling lightheaded, lack of energy and dark-coloured urine. Fluid levels should ideally be maintained to prevent thirst. The recommended daily intake of fluid to prevent dehydration is at least 1.2 litres per day, although 2 litres per day is frequently cited.
Water assists the body with a number of important functions, these include:• Formation and maintenance
of blood plasma, tissue fluid and lymph.
• Effective passage of substances in and out of cells (including circulation of nutrients via the blood and removal of waste).
• Enabling life-sustaining reactions to occur within the body.
• Transport and filtration of waste products for excretion.
206 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 7: The importance of healthy eating

The body actually loses much more fluid than this but some is replaced through aerobic energy production (called metabolic water) and some is ingested within foods, particularly fruit and vegetables.
All drinks are fluid and can be included as part of daily intake. The healthiest option is water (still or sparkling) and a slice of lime or lemon can be added to add flavour for individuals who do not like plain water. Fruit juices or milk (ideally skimmed or semi-skimmed) are also healthy choices in small amounts and contain vitamins and minerals in addition to providing energy from natural sugars and fats.
Tea and coffee may be less healthy choices, as they contain caffeine (a stimulant) which can have a dehydrating effect. It is recommended not to consume in excess of 300mg of caffeine per day; this is equivalent to around six cups of tea or instant coffee, or just two espresso coffees. Tea and coffee contain various plant compounds that can have a positive effect on health, although adding milk to tea may block the absorption of some of these. Fizzy drinks and sodas often contain lots of sugar, caffeine and other artificial additives and can contribute to increasing calorie intake leading to weight gain, as well contributing to tooth decay, which has been linked to increased cardiovascular disease risk (NHS choices, 2012a).
The energy balance equationThe energy balance equation is an essential component in weight management.
Energy intake refers to sources for taking energy into the body, such as food and drink. It includes the type and amount of food eaten and all drinks consumed that contain energy, including alcohol.
Energy output refers to sources for using energy. This includes resting metabolic rate (RMR) – the amount of energy used while at rest – and the amount of energy used through activity and exercise.
ENERGY INTAKE
ENERGY OUTPUT
The term weight management refers to the actions taken by an individual to achieve or maintain an acceptably healthy level of body fat.
Energy input and energy output can be adjusted to meet individual goals.
• When energy intake exceeds energy output there will be weight gain. Body fat and body weight increase.
• When energy output exceeds energy intake there will be weight loss.
• When energy intake and energy output are balanced, weight will be managed.
Figure 7.2 Energy balance
BODY IN ENERGY BALANCE
BODY FAT INCREASES
ENERGY INPUT
ENERGY INPUT
ENERGY OUTPUT
ENERGY OUTPUT
Copyright © 2014 Active IQ Ltd. Not for resale | 207
Section 7: The importance of healthy eatingPR
InC
IPLES o
F ExERC
ISE, FITnESS A
nd
HEA
LTH

End of section: Learning checkAnswer the following questions and make notes to revise this section.
• What are the health risks of poor nutrition?
• What is healthy eating?
• State three key guidelines from the national food model ‘the Eatwell plate’.
• Why is adequate hydration important?
• What are the professional boundaries of a fitness instructor in relation to giving nutritional advice?
• What is the dietary role of the following nutrients?
• Carbohydrates.
• Fats.
• Proteins.
• Minerals and vitamins.
• Fibre.
• Give examples of food from each of the following food groups:
• Carbohydrates.
• Fats.
• Proteins.
• Minerals and vitamins.
• Fibre.
• What is the energy balance equation?
• What would need to happen to the energy balance equation to maintain weight?
208 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 7: The importance of healthy eating

AimExercise sessions need to be planned before they can be delivered. All fitness instructors should understand how to gather information from their clients and how to use it to plan a safe, effective programme.
Planning helps fitness instructors to assess clients’ readiness for exercise, identify their goals and develop a programme at an appropriate starting level for their fitness and skill.
Learning outcomesAt the end of this unit you will:
• Understand how to collect client information to plan gym-based exercise.
• Understand how to use client information to plan gym-based exercise.
• Understand how to plan gym-based exercise with clients.
• Be able to collect and use client information to plan a gym-based exercise programme.
• Be able to plan a safe and effective gym-based exercise programme with clients.
PLANNING GYM-BASED EXERCISE

Section 1: Understanding how to collect and use client information
Exercising and increasing activity levels are commonly-held aspirations. Exercising regularly and avoiding a sedentary lifestyle enhance wellbeing, assist stress management and reduce the risk of developing chronic health conditions, such as coronary heart disease, osteoporosis, obesity and diabetes.
Increasing activity levels carries far fewer health risks than potential benefits for ‘apparently healthy’ people with no known health conditions. Physical activity at an appropriate level is both safe and desirable.
By contrast, people with injuries or health conditions, such as hypertension, may be at a significant risk of further injury (e.g. strains and sprains) or medical emergencies (e.g. angina or heart attacks) when they participate in exercise. These risks need to be removed or managed before the clients can exercise.
It is important to understand how to gather and use information from clients, identify any risks that exercise could pose and act appropriately.
All fitness instructors should be able to:
• Plan a gym-based programme using appropriate methods of data collection.
• Check that the information is accurate and up to date.
• Identify the client’s needs, potential and any possible risks a gym-based programme could pose.
• Maintain client confidentiality.
Principles of screeningAll clients should be screened before they start an exercise programme to assess their readiness to exercise, their health status and current activity and fitness levels. They should also give their informed consent to participate.
Screening clients and acquiring informed consent are compulsory legal and ethical duties of care for exercise and fitness instructors.
Information gathered from the various screening procedures:
• Governs the advice and guidance offered to clients.
• Influences the design of any exercise and activity programme, including the frequency, intensity and type of activity recommended.
EXPERT TIP ‘Physically active adults have a 20-30% reduced risk of premature death and up to a 50% reduced risk of developing major chronic diseases, such as coronary heart disease, stroke, diabetes and cancers.’
(Department of Health, 2004)
KEY POINTAll clients should be screened before taking part in exercise; it is a legal and ethical requirement.
210 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Understanding how to collect and use client information

The purpose of screening
The purpose of pre-exercise screening is to:
• Assess the client’s readiness for exercise.
• Identify high-risk clients, who need clearance from their GP in order to participate.
• Inform the design and planning of the programme.
• Maximise the benefits of exercise participation for the client.
• Minimise the risks of exercise participation for the client.
• Protect the instructor and organisation from litigation.
• Fulfil professional, legal and ethical requirements.
Factors that compromise the safety of exerciseIn some instances, clients need to delay exercise or be referred to a qualified health professional before participation.
Reasons for temporary deferral of exercise
Reasons for delaying exercise include:
• Illness, such as a cold or flu. Sufferers are advised to delay exercise until they are feeling better.
• Pregnancy, which can require GP clearance before exercise can commence. It is covered in the PARmedX.
• Health changes; these should be reported and could require referral to a GP.
• Inappropriate clothing or footwear, e.g. no trainers for a gym session.
• Inebriation; gym equipment should not be used under the influence of alcohol.
Reasons for medical referral and clearanceGP consent and clearance for exercise are recommended in these cases:
PAR-Q RESPONSE If the client answers ‘Yes’ to one or more of the questions on the PAR-Q form; if they have any diagnosed metabolic, pulmonary or cardiovascular disease; or if they are experiencing signs or symptoms of a pulmonary or cardiovascular disease they are at a heightened risk of medical emergency.
COMBINED RISK FACTORS
Exercise can be dangerous for clients who have several risk factors for cardiovascular disease (CVD); they should check for these with their GP. CVD risk factors include inactivity, high blood pressure, smoking, age, obesity, stress, diabetes, high cholesterol and a family history of CVD (genetics).
INJURIES THAT CAN BE
AGGRAVATED BY EXERCISE
Clients with minor injuries such as sprains and strains might need clearance from their GP, as these can be exacerbated by exercise.
Copyright © 2014 Active IQ Ltd. Not for resale | 211
Section 1: Understanding how to collect and use client informationPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

INSTRUCTOR DOUBT OR
UNCERTAINTY
If the instructor has any doubts about the client’s health, they should advise them to check with their GP for clearance.
CLIENT PREFERENCE OR
DOUBT
If the client wants to have a medical check before starting an exercise programme, they should be encouraged to pursue it with their GP.
AGE Clients aged over 69, who are unused to exercise, should be assessed by their GP.
If a client is considered unfit for exercise they can be referred to an appropriate healthcare professional, e.g. a GP. They must then obtain medical clearance before they can start the programme.
NB: The Canadian Society of Exercise Physiology (CSEP) provides an example of a clearance form that can be used by GPs for referred clients.
The client should be given an explanation for their referral and an opportunity for a follow-up after they have spoken with their GP. This can be via telephone or face-to-face appointment.
Fitness instructors are not qualified to work with clients with medical conditions, or to rehabilitate them from injury; these fall beyond an instructor’s scope of practice. Clients with medical conditions need supervised exercise sessions with a level 3 exercise referral instructor or a level 4 specialist instructor.
Collecting client informationThere are different types of client information required for planning a gym-based exercise programme.
This information includes:
• Informed consent to participate.
• Personal information and details.
• Medical history.
• Physical assessments (fitness and health).
• Lifestyle information.
• Lifestyle habits.
• Motivation and preferences.
• Goals and reasons for exercise.
The information gathered will affect:
• The selection of exercises; this includes the type of activities planned.
• The frequency and duration of training; this includes the number and length of sessions.
• The exercise intensity, e.g. number of reps and sets, working heart rate, speed or range of motion.
212 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Understanding how to collect and use client information

The process of getting informed consentInformed consent must be obtained from the client before:
• Any fitness testing.
• Any exercise sessions, including gym-based exercise.
Informed consent can only be given when certain information has been explained by the instructor and fully understood by the client:
• What is being proposed (e.g. fitness test or exercise programme).
• The reasons for the proposed exercise programme or fitness test.
• The benefits of the proposed exercise programme or fitness test.
• The risks attached and how they are managed.
• The responsibilities of everyone involved (the client and the instructor).
The client must also understand that their participation is entirely voluntary (not compulsory) and be given the opportunity to ask questions, which must be answered (all questions and answers must also be recorded on the informed consent document).
The informed consent document needs to be dated and signed by the client and the instructor, kept as a permanent record and stored securely with other client details.
The informed consent document is not a waiver of any rights or responsibilities; it is one of many records that can be produced in a court of law in the event of a lawsuit.
It is mandatory that you obtain informed consent and appropriate information from a client before you make any recommendations. This ensures that you are both adequately protected.
KEY POINTAs a legal record, an informed consent document should be checked by legal professionals. Most gyms have their own records for instructors to use with clients.
SUMMARY OF AN INFORMED CONSENT RECORDThe information presented on an informed consent record should be clearly typed and worded and provide:
• An explanation of the purpose of the assessment or programme.
• A description of the components of the assessment or programme.
• An explanation of the potential risks, discomforts and benefits.
• Clarification of the client’s responsibilities.
• A reference to confidentiality and privacy.
• An emphasis on the client’s voluntary participation and right to change their mind.
• The opportunity for the client to ask questions (with space for recording questions and answers).
• Signatures of the client and witness (instructor) and date.
Copyright © 2014 Active IQ Ltd. Not for resale | 213
Section 1: Understanding how to collect and use client informationPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

INFO
RM
ATIO
N
METH
OD
OF
CO
LLEC
TIO
NC
HEC
KS
TO M
AK
E
FAC
TOR
S TH
AT C
AN
AFF
EC
T SA
FE P
AR
TIC
IPAT
ION
AN
D R
EQ
UIR
E C
ON
SID
ER
ATIO
N
WH
EN
PLA
NN
ING
Pers
onal
in
form
atio
n an
d de
tails
Que
stio
nnai
re
Inte
rvie
w•
Nam
e.•
Addr
ess.
• Em
erge
ncy
cont
act d
etai
ls.
• Ag
e.•
Gen
der.
• Et
hnic
ity.
• D
isab
ilitie
s.•
Lang
uage
spo
ken.
• Se
lect
ion
of a
ctiv
ities
app
ropr
iate
for
age-
rela
ted
phys
iolo
gica
l cha
nges
, e.g
. los
s of
bon
e m
ass
or jo
int d
eter
iora
tion.
• Se
lect
ion
of c
ultu
rally
app
ropr
iate
act
iviti
es fo
r so
me
ethn
ic g
roup
s, e
.g. w
omen
-onl
y se
ssio
ns.
• Ac
tivity
mod
ifica
tions
for
clie
nts
with
dis
abili
ties.
•
Avai
labi
lity
of w
ritte
n re
sour
ces
(e.g
. scr
eeni
ng fo
rms)
in o
ther
lang
uage
s.
Med
ical
his
tory
PAR
-Q s
uppo
rted
by
inte
rvie
w•
Curr
ent m
edic
al c
ondi
tions
and
m
edic
atio
ns ta
ken.
• R
elev
ant m
edic
al h
isto
ry.
• Cl
ient
s m
ight
nee
d to
def
er e
xerc
ise
and
be r
efer
red
to a
GP
befo
re e
mba
rkin
g on
a
prog
ram
me.
•
A cl
ient
mig
ht n
eed
to w
ork
with
a s
peci
alis
t ins
truct
or, e
.g. e
xerc
ise
refe
rral
. •
A cl
ient
mig
ht n
eed
to b
e ex
clud
ed fr
om e
xerc
ise,
e.g
. in
case
of m
edic
al c
ontra
indi
catio
ns
(sta
ge 3
hyp
erte
nsio
n or
tach
ycar
dia)
.
Hea
lth a
nd fi
tnes
s le
vel
Phys
ical
as
sess
men
ts•
Blo
od p
ress
ure.
• H
eart
rat
e.•
Post
ure.
• Fl
exib
ility
.
• Ch
eck
curr
ent h
ealth
sta
tus
and
iden
tify
reas
ons
for
defe
rral
(e.
g. il
lnes
s) o
r re
ferr
al (
e.g.
hig
h bl
ood
pres
sure
or
hear
t rat
e).
• Pr
ovid
e ba
selin
e m
easu
res
that
gau
ge th
e st
artin
g po
int f
or a
ny a
ctiv
ity; t
hese
can
be
used
to
mon
itor
prog
ress
.
Life
styl
e in
form
atio
nIn
terv
iew
Que
stio
nnai
re•
Occ
upat
ion.
• W
orki
ng h
ours
.•
Man
ual o
r se
dent
ary
wor
k de
man
ds a
nd p
ostu
res
adop
ted.
• Le
isur
e ac
tiviti
es a
nd p
ostu
res
adop
ted.
• Ac
tivity
leve
ls –
sed
enta
ry,
limite
d, m
oder
atel
y or
hig
hly
activ
e –
and
frequ
ency
.
• It
can
influ
ence
the
time
the
clie
nt h
as a
vaila
ble
and
whe
n th
ey c
an a
ttend
.•
It in
fluen
ces
the
clie
nt’s
fitn
ess
leve
ls a
nd p
ostu
re; i
f the
y’re
inac
tive,
the
prog
ram
me
mus
t st
art a
t a lo
wer
leve
l. •
Life
styl
e ac
tiviti
es, e
.g. w
alki
ng a
nd u
sing
sta
irs m
ore
ofte
n ca
n be
rec
omm
ende
d to
incr
ease
ac
tivity
leve
ls.
• Ex
erci
ses
can
be p
rogr
amm
ed to
impr
ove
post
ure.
214 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Understanding how to collect and use client information

INFO
RM
ATIO
N
METH
OD
OF
CO
LLEC
TIO
NC
HEC
KS
TO M
AK
E
FAC
TOR
S TH
AT C
AN
AFF
EC
T SA
FE P
AR
TIC
IPAT
ION
AN
D R
EQ
UIR
E C
ON
SID
ER
ATIO
N
WH
EN
PLA
NN
ING
Life
styl
e ha
bits
Que
stio
nnai
re
Inte
rvie
w•
Nut
ritio
nal h
abits
– ty
pes
of
food
and
drin
k an
d fre
quen
cy o
f co
nsum
ptio
n.•
Alco
hol c
onsu
mpt
ion
– es
timat
ed a
mou
nts
and
frequ
ency
.•
Smok
ing
habi
ts –
sm
oker
or
non
-sm
oker
, am
ount
s,
frequ
ency
and
leng
th o
f hab
it.
• D
iet a
nd e
atin
g be
havi
ours
can
affe
ct e
nerg
y le
vels
, moo
d, b
ody
fat l
evel
s (o
verw
eigh
t and
ob
esity
) an
d m
anag
emen
t of h
ealth
con
ditio
ns (
e.g.
dia
bete
s).
• Sm
okin
g is
a m
ajor
ris
k fa
ctor
for
coro
nary
hea
rt d
isea
se a
nd c
hron
ic o
bstru
ctiv
e pu
lmon
ary
dise
ase.
It a
lso
ham
pers
car
dior
espi
rato
ry fi
tnes
s, w
hich
can
com
prom
ise
exer
cise
inte
nsity
. •
Mul
tiple
CVD
ris
k fa
ctor
s (t
wo
or m
ore)
– e
.g. s
mok
er, a
ged
59, m
ale
and
over
wei
ght –
may
w
arra
nt c
once
rn a
nd s
ubse
quen
t ref
erra
l to
a G
P be
fore
the
clie
nt c
an p
arta
ke in
exe
rcis
e (e
ven
with
out e
xper
ienc
e of
sym
ptom
s).
Mot
ivat
ion
and
pref
eren
ces
Inte
rvie
wQ
uest
ionn
aire
•
Activ
ity p
refe
renc
es a
nd
prev
ious
exe
rcis
e ex
perie
nces
. •
Pers
onal
goa
ls a
nd o
bjec
tives
.•
Leve
l of m
otiv
atio
n an
d re
adin
ess
to s
tart
mak
ing
chan
ges.
•
Supp
ort s
yste
ms
avai
labl
e, e
.g.
frien
ds a
nd fa
mily
.
• Cl
ient
act
ivity
pre
fere
nces
and
per
sona
l goa
ls s
houl
d in
fluen
ce th
e ch
oice
of a
ctiv
ities
. •
Leve
ls o
f mot
ivat
ion
and
read
ines
s in
fluen
ce a
clie
nt’s
com
mitm
ent,
dete
rmin
atio
n an
d po
tent
ial f
or lo
ng-t
erm
adh
eren
ce; t
hey
mig
ht n
eed
addi
tiona
l sup
port
.•
Supp
ort s
yste
ms
can
influ
ence
clie
nt m
otiv
atio
n an
d de
term
ine
the
leve
l of s
uppo
rt r
equi
red.
Rea
sons
for
exer
cise
an
d go
als
Inte
rvie
w
Que
stio
nnai
re
• W
hat t
he c
lient
wan
ts to
ac
hiev
e an
d w
heth
er it
is
real
istic
or
feas
ible
.
• Cl
ient
goa
ls in
fluen
ce th
e ch
oice
of a
ctiv
ities
and
leve
l of c
omm
itmen
t the
y ne
ed to
rea
lise
the
obje
ctiv
e.•
Goa
ls c
an a
lso
high
light
whe
re a
dditi
onal
sup
port
is n
eede
d.
Tabl
e 1
.1 C
lient
info
rmat
ion
Copyright © 2014 Active IQ Ltd. Not for resale | 215
Section 1: Understanding how to collect and use client informationPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Methods of gathering information Different methods can be used for gathering information from clients, these include:
• Questionnaires, e.g. PAR-Q.
• Interviews or one-to-one consultations.
• Observation.
• Fitness and health assessments, e.g. heart rate and blood pressure.
Questionnaires
Questionnaires are useful for gathering specific information, especially when time is limited. By contrast interviews allow clients to elaborate on objective responses. For example, if a client indicates that they are taking medication, it would be useful to know what they are taking and for what condition; it could mean that they need to work with a specialist instructor.
Written questionnaires, e.g. PAR-Q, can be used to gather health and medical information. They can also be used to highlight lifestyle behaviours (e.g. smoking, diet or alcohol use).
There are a number of recognised questionnaires, including:
• PAR-Q forms for checking medical and health status.
• Questionnaires for gathering information on general wellbeing (e.g. EQ5D) and physical activity levels (IPAQ). These are standard forms used in exercise referral.
• Specialist questionnaires used to gauge the level of pain, discomfort or distress caused by specific medical conditions, e.g. low back pain (Roland-Morris), mental health (hospital anxiety depression scale or HADS) or falls risk assessment tool (FRAT) for older adults at risk of falls.
NB: Level 2 fitness instructors only use the PAR-Q form. The EQ5D, IPAQ, Roland-Morris, HADS and FRAT are used by level 3 exercise referral instructors and level 4 specialist instructors.
Table 1.2 Advantages and disadvantages of questionnaires
ADVANTAGES• Closed questions enable ‘yes’ or ‘no’
answers and are easy to complete (e.g. PAR-Q).
• Relatively quick to complete, depending on the number of questions.
• Can be completed in one’s own time.• Lots of people can complete them
simultaneously.• Questions need to be well phrased with
enough space given for responses. • Provide a written record which can be
stored securely. • Information is immediate and accurate at
the point of asking. • Questionnaires such as the PAR-Q are
recognised as valid and reliable.
DISADVANTAGES• Need to be able to read and write in the language used for
the questionnaire (language and literacy barriers can hinder accuracy).
• Can appear impersonal, unless discussed with the client. • Does not allow for clarification or explanation.• Instructor needs time to read and act on the responses. • Clients might require an explanation, otherwise they cannot
fully understand the questions; they may not always answer truthfully or keep to relevant information.
• Information may become out of date. • As a record of client information, they need to be updated
regularly and stored securely in accordance with data protection and confidentiality legislation.
• Some questionnaires require permission for use. • Instructor-designed questionnaires may lack the required
validity and reliability.
216 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Understanding how to collect and use client information

PAR-Q formsOne of the most essential tools for gathering information from clients is the physical activity readiness questionnaire (PAR-Q).
The PAR-Q and other recognised screening forms are provided by the Canadian Society for Exercise Physiology (CSEP). They include a series of questions that clarify whether exercise needs to be delayed until GP clearance is obtained.
The PAR-Q is a one-page questionnaire for clients aged 15-69. It has seven questions and advises clients to check with their GP if they answer ‘yes’ to any of the questions, which are:
1. Has your doctor ever said that you have a heart condition and that you should only do physical activity recommended by a doctor?
2. Do you feel pain in your chest when you do physical activity?
3. In the past month, have you had chest pain when you were not doing physical activity?
4. Do you lose your balance because of dizziness or do you ever lose consciousness?
5. Do you have a bone or joint problem (for example, back, knee or hip) that could be made worse by a change in your physical activity?
6. Is your doctor currently prescribing drugs (for example, water pills) for your blood pressure or heart condition?
7. Do you know of any other reason why you should not do physical activity?
Source: CSEP, 2014
PAR-Q+: The PAR-Q+ is a four-page questionnaire which incorporates seven main questions (similar to the PAR-Q) and some additional questions on chronic health conditions. It is used by specialist instructors. Clients who answer ‘yes’ to one or more questions on the PAR-Q+ must obtain GP clearance before they can partake in exercise. The CSEP has also developed the Physician Physical Activity Readiness Clearance (PPARC) for GPs to use to inform instructors about the clients for whom they provide clearance.
PARmedX for pregnancy: The PARmedX for pregnancy is a four-page questionnaire for screening pregnant women who want to exercise.
Please note: Permission is not required to photocopy the forms for personal or clinical use, but is required to reproduce the forms.
Copyright © 2014 Active IQ Ltd. Not for resale | 217
Section 1: Understanding how to collect and use client informationPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Interview
One-to-one consultations are time-consuming but they can be a richer source of information than objective questionnaires. Information can be verified and elaborated and behavioural cues, such as body language, can be observed.
Interviewing is more personal than questionnaires and offers an opportunity for building rapport with the client. However, face-to-face meetings can sometimes be daunting for less confident clients and the instructor must be able to adapt their communication style to suit different client needs. Instructors need to be able to ask appropriate open questions to gather information and actively listen to check that they understand the client correctly. Additional training and practice is often required to develop these skills effectively.
Table 1.3 Advantages and disadvantages of interviews
Observation
Observation is a quick, easy method of gathering information on subjects that do not require questions (e.g. gender) or verbal description (e.g. posture).
Observation can also be used to gather information on subjects that clients might find uncomfortable (e.g. body fat) without using invasive or inappropriate fitness assessments (e.g. calipers or tape measures) which can cause embarrassment.
Some observations require a degree of experience and additional training to make an informed assessment that can be used to inform planning and exercise selection (e.g. posture assessments).
Table 1.4 Advantages and disadvantages of observation
ADVANTAGES• Open questions can provide lots of
information. • A personal approach helps to establish
rapport and trust. • Questions can be clarified and client
responses acknowledged (e.g. nodding), which can encourage elaboration.
DISADVANTAGES• Time-consuming. • Remembering and recording information accurately requires
skill.• Information needs to be recorded and stored securely. • Requires empathy and effective active listening and
questioning skills. • Risk of disclosure of information outside role boundaries,
especially sensitive information, e.g. medical conditions.• Need to be conducted in a private area.
ADVANTAGES• Quick and immediate. • Effective for gathering information, such as
gender, age, posture, body composition, walking gait, facial expressions, skin colour changes during activity, clothing, footwear and whether the client is a healthy weight.
DISADVANTAGES• Some information must be checked for accuracy
(e.g. age range) and recorded appropriately. • Ineffective for gathering certain information, e.g.
lifestyle behaviours and medical conditions that cannot be seen (depression, osteoarthritis).
218 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Understanding how to collect and use client information

Physical assessments (health and fitness)
Physical assessments can be used to obtain detailed information about the client’s current fitness and health status.
Health assessments include:
• Blood pressure.
• Heart rate.
• Height and weight.
• Body mass index.
Fitness assessments include:
• Flexibility assessments.
• Muscular assessments.
• Cardiovascular assessments.
Table 1.5 Advantages and disadvantages of health and fitness assessments
ADVANTAGES• Provide baseline information that can
inform programme design and exercise selection.
• Assessments gather specific information, e.g. blood pressure, heart rate, body mass index (BMI), flexibility (sit and reach) and muscular fitness (curl-up or press-up).
• Heart rate and blood pressure can identify medical contraindications for exercise, e.g. severe hypertension or tachycardia.
• Assessments provide valid, reliable measurements.
• Comprehensive information can be gathered and can be retested to check developments and changes.
DISADVANTAGES• Informed consent is required.• Some assessments can pose risks for clients (e.g. use of a
cardiovascular step test for a client with a knee injury).• Some assessments can be invasive or insensitive, e.g.
using calipers on an obese client. • Equipment needs to be calibrated to ensure valid, reliable
readings.• Equipment should be of good quality, regularly inspected
and well maintained.• Instructors need to be qualified and competent to conduct
assessments.• Test guidelines need to be followed to ensure results are
accurate. • Clients must be in a ‘neutral state’ (variables reduced) for
test accuracy. • Time is required to instruct clients properly and to
complete.
Copyright © 2014 Active IQ Ltd. Not for resale | 219
Section 1: Understanding how to collect and use client informationPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Client instructions – pre-test information Clients should be fully informed of the guidelines or pre-test procedures before any physical testing begins. Pre-test procedures can be listed on the back of an appointment card and given to the client on the initial booking. It is important to check that the guidelines have been followed before testing.
PRE-TEST GUIDELINES FOR CLIENTS
Consumption • Avoid eating heavy meals less than three hours before the test.• Avoid excessive alcohol consumption on the day before the test and avoid any alcohol on
the day of the test.• Avoid caffeinated drinks, e.g. coffee, two hours before the test.• Avoid smoking for at least two hours before the test.
Action • Avoid exercise or strenuous physical activity on the day of the test.• Have a good night’s sleep on the night before the test.• Avoid using a Jacuzzi, sauna or sunbed less than two hours before the test.
Medical • Cancel the assessment if you have a temperature or feel unwell.• Bring any medication you take (e.g. inhalers) with you on the test day.
Clothing • Wear appropriate exercise clothing and footwear, e.g. trainers.
Table 1.6 Pre-test procedures
How to choose the correct methods of gathering informationYou should generally use a combination of methods to gather client information. Obtaining a PAR-Q and informed consent are minimum requirements; they are compulsory for legal and ethical reasons. Interviews are useful for planning individually tailored programmes. They can guide exercise selection to meet specific client needs. Physical assessments (health and fitness) are optional. They are useful for gathering baseline information that can determine the starting level of the programme, but some tests would not be appropriate for certain clients.
Other considerations for choosing research methods include:
• The time the client and instructor have available.
• The client’s level of experience – some fitness assessments are inappropriate for certain clients.
• Language spoken by the client, e.g. clients who speak English as a second language may need written materials in their first language.
• Client disabilities that can get in the way of assessments, e.g. visually impaired or blind clients would require the PAR-Q to be read out, while deaf or partial hearing clients might need a signer. Injured and disabled clients would also need to be excluded from certain physical assessments.
Client goals and objectivesClient objectives are a major determinant of exercise programme content. Different types of goal suit different types of programme.
Client goals need to be checked to ensure that they are realistically achievable. For example, a client who is inactive and unused to running would be ill-advised to name completing a marathon as a short-term goal, although it could become a longer-term goal once they have established their baseline fitness.
220 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Understanding how to collect and use client information

A novice client who aspires to become stronger might not fully appreciate the type of training required to develop maximal strength. They may also fail to realise that advanced muscular goals of hypertrophy, strength and power require a significant background in resistance training in order to be performed safely and effectively.
Another consideration is that clients may have limited knowledge of the components of fitness. They will therefore need help and support from the instructor to interpret and translate their goals. Clients might make broad statements about wanting to ‘tone up’ or ‘get fit,’ so the instructor must gather all the necessary information to identify what they mean by these statements. They might simply want to be able to play with their grandchildren without getting exhausted or breathless, rather than increase their fitness to a significant level.
Client goals or objectives can often translate into one of the following:
• Posture.
• Aerobic conditioning.
• Muscular strength.
• Muscular endurance.
• Flexibility.
• Fat loss.
• Health.
• Hypertrophy.
Each one of these objectives would require a different type of programme.
Available timeThe duration and frequency of the workouts are determined by the time the client has available and their current activity and fitness levels.
All exercise and activity should fit well with the client’s lifestyle or their exercise adherence could be compromised, especially if they are novice clients who are not accustomed to ‘regular exercise’ or patterns of active behaviour.
Clients who are inactive and have a low level of fitness may be best advised to start incorporating activities into their daily life, e.g. walking short distances and using stairs where possible; this means they can steadily increase their fitness by accumulating more regular physical activity.
KEY POINTActivity and exercise should fit in with the client’s lifestyle to encourage adherence.
KEY POINTDifferent goals require different types of training programme.
Training status and fitness levelA beginner to resistance exercise would respond differently to a client with several years of training experience. It is important for the instructor to know:
• The length of any regular participation in training programmes (past and present) and reasons for discontinuation where relevant.
• The type of training undertaken, e.g. resistance or cardiovascular, the equipment used and the exercises practised.
• The level of intensity involved in current or previous training, e.g. resistance lifted, number of repetitions, frequency and duration of sessions and type of system used.
• The degree of exercise technique, the client’s skill level, posture and alignment and the extent to which they can perform exercises correctly.
• The ‘training age’ of the client - how long they have been training combined with their experience with different exercise modalities. This determines the type of programme the gym instructor can produce. Training a complete novice (training age of zero) would be completely different to training a client with a five-year history of structured and progressive resistance and aerobic training.
Copyright © 2014 Active IQ Ltd. Not for resale | 221
Section 1: Understanding how to collect and use client informationPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

All of this information would directly influence the programme content, including the starting level of the programme, the type and number of exercises, the level of exercise intensity and complexity and ultimately the rate of progression.
SOMETHING TO CONSIDER Years of exercise participation does not automatically qualify a person to be an advanced exerciser. Some people who have been training for years have not progressed beyond the low-intermediate stage in terms of their fitness and technical competence. This is not necessarily due to lack of application. It may be that they are satisfied with their current level or lack the knowledge required to progress further.
Likes and dislikesKnowledge of the client’s exercise preferences should be used to influence the programme content. Incorporating exercises that the client enjoys will encourage adherence.
It can be useful to explore the reasons why clients dislike certain activities and whether this affects the balance of the programme. For example, a client who doesn’t like stretching would still need to incorporate flexibility activities to maintain their current range of motion and posture. A client who doesn’t want to use heavy weights on their upper body because they don’t want ‘big muscles’ would still need to include upper body activities to ensure muscle balance.
When exploring a client’s likes and dislikes it is useful for the instructor to ask:
Does the client dislike certain exercises because they are not good at them (they have an area of weakness or muscle imbalance) or they find them uncomfortable?
Would the client only adhere to the exercise programme if they were to stick to the activities they liked and avoid those that they don’t?
It is human nature for people to want to avoid the things they struggle with and concentrate their efforts in areas that play to their strengths. Performing well at a select group of exercises might boost a client’s confidence, which is positive, but it could potentially exacerbate existing physical imbalances.
Likes and dislikes should certainly be taken into account, but not implemented in a way that compromises muscle balance or potential training outcomes. For example, a client who dislikes using the step machine could simply try an alternative option without it affecting the outcomes of the programme. A client who wants to exclude exercises for a specific body part could be at risk of imbalance and should be made aware of the merits of muscle balance and the inclusion of relevant exercises.
The client might be more inclined to follow a programme if they are educated on the benefits and reasons for including specific exercises.
12
222 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Understanding how to collect and use client information

Data protection and confidentiality Client records need to be checked regularly to ensure the information is current and up to date.
Clients should be encouraged to advise the instructor of any changes to their health at each visit; it is important to make the client aware of this responsibility.
All client records should be stored securely and in accordance with data protection legislation.
This entails:
• Keeping paper records in locked files.
• Storing electronic records using secure systems with passwords.
• Not disclosing client information to other people or third parties.
• Ensuring information is transferred securely.
• Only using information for its intended purpose.
• Only keeping records for as long as they are required.
• Disposing of records securely.
NOTE: The Data Protection Act 1998 is under review. To check updates visit the Government’s main web portal at https://www.gov.uk/data-protection/the-data-protection-act (this address may be subject to change over time, in which case use an internet search engine, using the criteria ‘Data Protection Act’).
KEY POINTFailure to comply with this legislation is a criminal offence and as such can be prosecuted in a court of law.
End of section: Learning checkAnswer the questions and make notes to revise this section.
• Why is it important to screen clients before exercise participation?
• Why is it important to obtain a client’s informed consent?
• What information needs to be included on an informed consent document?
• What sort of client information can you gather from:
• Questionnaire?
• PAR-Q?
• Interview?
• Physical measurements?
• Observation?
• What factors would influence your choice of data collection method?
• How would you check that the information is accurate and up to date?
• Give examples of three client needs that could pose safety risks if those affected partake in a gym-based programme.
• How should you maintain client confidentiality?
• Why is it important to use a PAR-Q form with clients?
• On what grounds would you need to refer a client to their GP before they can participate in exercise?
• What sort of client information would highlight issues that could affect their safety when partaking in exercise?
• Give an example of how each of these facts would influence the way you would advise the client and plan their programme:
• Aged over 50.
• Dislikes running.
• Chronic medical condition, e.g. diabetes, asthma or hypertension.
• Minor joint injury, e.g. sprained wrist.
• Pregnant.
• Poor flexibility.
• Inactive, sedentary lifestyle.
• Smoker.
• Overweight or obese.
• Limited time available.
• Low confidence.
• When would you advise a client to temporarily defer exercise?
Copyright © 2014 Active IQ Ltd. Not for resale | 223
Section 1: Understanding how to collect and use client informationPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Section 2: Physical assessments
Taking physical measurements can be helpful when identifying a client’s starting fitness level. This in turn helps decisions on how to tailor the training programme.
Test appropriatenessTests should be chosen to match the needs, goals and capabilities of the client. Bear in mind that different tests suit different clients; do not take a one-size-fits-all approach!
As an example, some people might feel uncomfortable about having physical measurements taken, or embarrassed by certain tests. You need to be sensitive to these requests. For example, it might be unwise to take skinfold or girth measurements on a notably overweight client.
Some tests might be inappropriate or unsafe for certain clients. A client with a joint injury should not perform assessments that put stress on the injured area. For example, a timed press-up test would be unsuitable for a client with a wrist, elbow or shoulder injury; a timed sit-up test could be harmful for a client with low back pain or neck problems; and a step test could exacerbate a knee injury.
Sub-maximal or maximal assessments (cardiovascular or resistance) or high-intensity assessment (e.g. VO2 max or repetition maximum tests) might be unnecessary and too stressful for untrained clients. An inactive client would need to develop cardiorespiratory fitness gradually; starting them with a test that measures muscular power through a vertical jump could carry a high risk of injury.
TRAINER TIPRemember that different tests suit different clients.
224 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Physical assessments

Test conditionsThe environment where tests are conducted can influence the accuracy (validity and reliability) of the results. Other factors to take into account when conducting tests are:
TIME OF DAY Tests and retests should be scheduled at consistent times, in the interest of accuracy. If this is not possible it needs to be noted and taken into account.
Time of day can influence the results, as clients’ body temperatures, hydration levels and activity levels change throughout the day. A female client’s phase of the menstrual cycle can also influence the accuracy of results due to fluctuation in body temperature and fluid levels.
These should be kept constant at each assessment. Temperature (and humidity) affects the heart rate response to exercise, so any differences in environmental temperature between tests should be recorded and taken into account.
You might need to postpone tests that affect heart rate if the temperature is especially hot and postpone flexibility tests if it is very cold.
A private area should be used for physical tests relating to body composition and girth measurements; the client needs to feel comfortable.
Test procedures should be explained and informed consent obtained, before the programme can begin.
ENVIRONMENTAL FACTORS
PRIVACY
ALL PROCEDURES
Grounds for stopping tests
Part of an instructor’s duty of care is to tell the client what to expect and how they may feel in each test. They must also ensure that the client is comfortable at all times; this entails keeping an eye out for any signs of discontent.
Tests should be stopped immediately and/or clients referred to their GP in case of:
• Chest pain and the onset of angina-like symptoms (NB: This can also require emergency response).
• Significant drop (10mmHg) in systolic blood pressure with increased work rate.
• Excessive rise in blood pressure: systolic pressure >250 mmHg or diastolic pressure >115 mmHg.
• Signs of poor perfusion: light-headedness, confusion, ataxia, pallor, cyanosis, nausea or cold, clammy skin.
• Noticeable change in heart rhythm.
• Client requests to stop.
• Physical or verbal signs of severe fatigue.
• Failure of testing equipment.
(ACSM, 2014)
Copyright © 2014 Active IQ Ltd. Not for resale | 225
Section 2: Physical assessmentsPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Weight and heightHeight and weight tables provide guidelines for a healthy body weight. They are also a valid method of gauging body mass index.
These tables are not a measure of body composition – they do not assess the proportion of body fat – but are a reliable gauging method for the majority of the population. They can be compared with a waist measurement or body composition analysis if the participant is active or muscular.
Total weight indications are a useful starting point for assessing health status, but body composition must ultimately be taken into account. There is a difference between weight loss and fat loss.
Test guidelines
KEY POINTHeight and weight tables do not assess body composition (the proportion of total weight that is fat or fat-free).
Body mass index (BMI)BMI is the standard measure used for clinical diagnosis of obesity. It predicts health risks for most people accurately. It is not a reliable indicator for strength athletes and body builders (around 2% of the population) because it only takes height and weight into account – not body composition. Bodybuilders with very low levels of fat are often classified as ‘obese’ by this method.
BMI is a quick and easy gauging method. A BMI reading of 30 or more is classified as clinically obese.
EXAMPLEBody mass index (BMI) is calculated using this equation:
BMI (kg/m2) = Weight (kg) ÷ Height (m)2
Example BMI calculationIf a 70 kg man (2.2lbs = 1 kg) is 1.72m tall (2.54 cm = 1 inch) then:
BMI = 70 ÷ (1.72 x 1.72)
= 70 ÷ 2.96
= 23.6 kg/m2
WEIGHT ASSESSMENT
Use calibrated scales, make sure the client removes shoes and heavy clothing and ensure all re-tests are scheduled for the same time of day.
Body composition can be differentiated as:
Fat mass (FM): the proportion of total weight that is fat. This includes internal and external fat (adipose tissue).
Fat-free mass (FFM or lean mass): the proportion of total weight that is not fat. This includes muscle, bone and internal organs.
The percentage of body fat is important information for assessing health.
HEIGHT ASSESSMENT
Make sure the client removes shoes and stands tall. Take the highest part of the head as the measurement (be aware that height decreases as the day goes on).
BMI (KG/M2) DESCRIPTION
<18.5 Underweight
18.5-25 Normal
25-30 Overweight
>30 Obese
>40 Morbidly obese
Source: WHO, 2000, 2006. NICE, 2007.
Table 2.1 BMI classifications
226 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Physical assessments

Circumference measurementsThe pattern of body fat distribution is recognised as a key indicator of health risk. Fat stored in the abdominal region (as opposed to the legs, hips and arms) is considered a particular risk factor for CHD, as it is more easily mobilised and transported directly to the coronary arteries.
Waist circumference
Central adiposity is often measured in adults by waist circumference. For this reason there are different risk classifications for waist circumference measurements.
CLASSIFICATION MALE FEMALE
Low risk <94cm <80cm
High risk >102cm >88cm
(NICE, 2006)
Table 2.2 Waist circumference
BMI and waist circumference
Current guidance suggests that the assessment of the health risks associated with overweight and obesity should be based on both BMI and waist circumference (NOO, 2009).
BMI WAIST CIRCUMFERENCE AND HEALTH RISK
Men 94-102cm
Men >102cm
Women 80-88cm
Women>88cm
18.5-24.9Ideal
No increased risk Increased risk No increased risk Increased risk
25-29.9 Increased risk High health risk Increased risk High health risk
30-39.9 High health risk Very high health risk High health risk Very high health risk
>40 Very high health risk Very high health risk Very high health risk Very high health risk
(NOO, 2009)
Table 2.3 Combined assessment of health risk using BMI and waist circumference
Waist-to-hip ratioWaist-to-hip ratio is another measurement for assessing central obesity. Health risk increases with waist-to-hip ratio to varying degrees, depending on age and gender.
Waist-to-hip ratio measurements take longer to perform and are less accurate for predicting health risk than a waist circumference alone. Use a waist circumference when measuring to stratify risk. Many clients are interested in changing their body shape and waist-to-hip ratio may be of value to these clients, as it would indicate where they are losing fat from – not just how much.
CLASSIFICATION MALE FEMALE
High risk >1.0 >0.85
Moderate risk 0.90–1.0 0.80–0.85
Low risk <0.90 <0.80
Table 2.4 Waist-to-hip ratios
Copyright © 2014 Active IQ Ltd. Not for resale | 227
Section 2: Physical assessmentsPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Taking circumference measurementsCircumference measurements are quick, easy and straightforward to take. Measurement sites include the waist, abdomen, hips, arm and chest.
TRAINER TIP When taking circumference measurements:
• Take the measurement at an exact location.
• Keep the tape in one plane.
• If possible, take measurements under clothing (if not, record details of clothing).
• Calculate the average out of three readings.
KEY POINTHigh levels of body fat around the waist indicate a heightened risk of cardiovascular disease.
AbdomenA horizontal measurement is taken (with the subject’s abdomen relaxed) at the level of the umbilicus (the navel). The measure is taken after a normal expiration.
HipsA horizontal measurement is taken at the maximum circumference with the person standing straight with feet together.
WaistA horizontal measurement is taken (with the subject’s abdomen relaxed) at the level of the narrowest part of the torso, above the iliac crest and below the 12th rib. The level of the umbilicus is also commonly used, but this is inaccurate for people with excess fat whose umbilicus has dropped, so above the bony marker of the iliac crest is the most consistent one to use. The measurement is taken after a normal expiration.
ArmA horizontal measurement is taken (with the subject’s arm relaxed) at the mid-point between the acromion process (shoulder) and the olecranon process (elbow).
228 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Physical assessments

Cardiovascular fitness testingOxygen is breathed in and transported to working muscles to be used for energy production. During exercise there is an increase in the work performed, meaning that more energy is needed and consequently more oxygen. Eventually a point is reached at which the cardiorespiratory system cannot supply enough oxygen to meet the increased energy needs.
When a point of ‘maximum oxygen uptake’ has been reached it is universally expressed as VO2 max. Functionally, VO2 max reflects the ability of the lungs, heart, blood and vascular system to transport oxygen and the ability of the tissues to extract and use oxygen (Laukkanen et al, 2002).
There are lots of tests that can be used to assess cardiovascular fitness. The Rockport Walking Test is easy to implement and appropriate for beginners with a low level of fitness.
TRAINER TIP A person’s VO2 max is a good indicator of how aerobically fit they are. In other words, an aerobically fit client is better able to take in, transport and utilise oxygen than an unfit person.
ChestWith the subject standing erect, a measurement is taken at the maximum circumference.
NB: When taking this measurement on women, it might be appropriate to ask the client to place the tape in the correct position at the front of her body, with the instructor taking the measurement from the side or back.
Copyright © 2014 Active IQ Ltd. Not for resale | 229
Section 2: Physical assessmentsPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Rockport Walking TestIn this test the client walks as fast as possible for one mile. Their pulse rate is taken immediately after they have completed the mile. If the instructor does not have a heart rate monitor, this can be done manually by counting the number of beats for a period of 30 seconds and then multiplying that by two to get the client’s heart rate. The time it takes to complete the mile should be recorded. The instructor also needs to know the client’s age and body weight (taken before the test) in order to calculate the client’s estimated VO2 max.
The calculation for estimating a client’s VO2 max (Kilne et al, 1987):
VO2 max = 132.853 – (0.0769 x weight) – (0.3877 x age) + (6.315 x gender) – (3.2649 x time) – (0.1565 x heart rate)
Key• Weight is in pounds (lbs).• Gender: male = 1 and female = 0.• Time is expressed in minutes and 100ths of minutes.• Heart rate is in beats per minute.• Age is in years.
The score obtained can be measured against the norms for different fitness levels. Improvements are expected to be noted, with appropriate training given between tests.
FITNESS CATEGORIES FOR MALES, BASED ON VO2 MAX (mL . kg-1 . min-1)
Age (years) Low Fair Average Good High
20–29 ≤24 25–33 34–42 43–52 ≥53
30–39 ≤22 23–30 31–38 39–48 ≥49
40–49 ≤19 20–26 27–35 36–44 ≥45
50–59 ≤17 18–24 25–33 34–42 ≥43
60–69 ≤15 16–22 23–30 31–40 ≥41
(American Heart Association, 1972)
Table 2.5a Rockport test norms - males
FITNESS CATEGORIES FOR FEMALES, BASED ON VO2 MAX (mL . kg-1 . min-1)
Age (years) Low Fair Average Good High
20–29 ≤23 24–30 31–37 38–48 ≥49
30–39 ≤19 20–27 28–33 34–44 ≥45
40–49 ≤16 17–23 24–30 31–41 ≥42
50–59 ≤14 15–20 21–27 28–37 ≥38
60–69 ≤12 13–17 18–23 24–34 ≥35
(American Heart Association, 1972)
Table 2.5b Rockport test norms - females
230 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Physical assessments

Measuring resting heart rateResting heart rate (RHR) is the amount of times the heart beats every minute at rest (after a long sleep). Resting heart rate averages 60-80 beats per minute (bpm). It can also be a valid indicator of health.
In middle-aged, sedentary people the resting heart rate can exceed 100 bpm, while highly trained endurance athletes can have resting rates between 28-40 bpm (Wilmore and Costill, 1999). Lower readings generally indicate higher levels of aerobic fitness, although hereditary factors also play a significant part; RHR is not always a reliable indicator.
RESTING HEART RATE (BPM) REFERENCES
Men Women
Normal 60-80 bpm 60-80 bpm
Average 70 bpm 75 bpm
Special attention 90 bpm 90 bpm
Medical referral (tachycardia) 100 bpm 100 bpm
Table 2.6 Resting heart rate (RHR) categories
KEY POINTA resting heart rate of 100 bpm is a contraindication for exercise; sufferers must be referred to their GP before they can partake in an exercise programme.
BRADYCARDIAAn RHR of less than 60 bpm.
Causes include:• High levels of fitness.
• Low body temperature (hypothermia).
• Low thyroid function (hypothyroidism).
• Higher than normal level of potassium in the bloodstream (hyperkalaemia).
• Myocardial infarction (damage or death of heart tissue).
• Genetics.
• Prescription drugs (beta blockers).
TACHYCARDIAAn RHR of more than 100 bpm (increased CVD risk).
Causes include:• Exposure to alcohol, caffeine or nicotine.
• Stress, anxiety or arousal.
• Heart failure.
• Pulmonary embolism.
• Abnormal decrease in blood volume or blood plasma (hypovolaemia).
• Hypermetabolic states (such as fever or a raised body temperature).
• Certain drugs (adrenaline, ephedrine and atropine).
• Poor cardiovascular fitness levels.
Copyright © 2014 Active IQ Ltd. Not for resale | 231
Section 2: Physical assessmentsPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

INSTRUCTIONS FOR ASSESSING RESTING HEART RATEThe ideal time to take RHR is first thing in the morning, before getting out of bed. Clients can be instructed to take their own RHR and to monitor any changes.
Pre-exercise testing:
1. Ensure the client has rested for 5-10 minutes in a seated or supine position.
2. Locate the correct site of the carotid or radial artery; these are the most commonly used sites.
3. Use the tips of the middle and index fingers. Do not use your thumb; it has a pulse of its own and could skew your reading.
4. When palpating the carotid site, apply light pressure. Baroreceptors in the carotid arteries detect pressure and if this is too heavy it can cause a reflex slowing of the heart rate.
5. Allow 30-60 seconds for your client to adjust to the assessment. Many clients feel apprehensive at the beginning of this check, which can affect results if taken immediately.
6. If you start a stopwatch simultaneously with the pulse beat, count the first beat as zero. If the stopwatch is already running, count the first beat as one.
7. Count pulse for 60 seconds, record the result and repeat.
8. If the results are significantly different, repeat for a third reading.
9. Ensure all pre-test procedures are followed and ascertain whether there is any identifiable cause of tachycardia or bradycardia.
Location of the carotid and radial pulse
Carotid pulseThe common carotid artery sites are located on both sides of the front of the neck. Both are in the groove formed by the larynx (Adam’s apple) and the sternocleidomastoid muscles (muscles on the side of the neck) just below the mandible (lower jawbone).
Radial pulse The radial artery runs deeply on the anterolateral (thumb side) aspect of the forearm and becomes superficial near the distal head of the radius (directly in line with the base of the thumb).
Carotid pulseRadial pulse
232 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Physical assessments

Muscular endurance fitness testingThere are a variety of tests for measuring endurance and strength. A person’s fitness level and experience are key determinants for the tests you should choose.
It would not be advisable to test a beginner or newcomer to resistance training to the point of exhaustion at any number of reps. Muscular endurance tests are often preferable to strength tests because:
• An all-out (maximal) test is hard work, painful and can put some clients off further resistance training.
• An all-out (maximal) test can result in delayed onset muscle soreness (DOMS), which is also likely to put clients off.
• If the client focusses on working to the maximum, good form will almost certainly be lost. Good technique is much more important than maximal exertion in the early days of resistance training.
• A beginner is at particular risk of injury if they are exercising to maximum exertion – especially in their ligaments and tendons, which take longer to gain strength than muscles (this develops through training). Using heavy free weights before coordination is developed is potentially dangerous.
Two simple muscular endurance tests are:
The press-up test.
The abdominal curl test.
Press-up testInstructions
• The client assumes the normal press-up position with the body rigid and straight and the arms shoulder-width apart.
• The client must lower himself or herself to 90° of elbow flexion.
• The test is the total number of completed press-ups to exhaustion.
• An alternative press-up method, where the client raises from a position with the knees in contact with the ground, is available for those who cannot complete the normal version.
Table 2.7 highlights fitness categories for the press-up test.
PRESS-UPS COMPLETED BY AGE AND SEX
Age 20-29 30-39 40-49 50-59 60-69
Sex M F M F M F M F M F
Excellent 36 30 30 27 25 24 21 21 18 17
Very good 35 29 29 26 24 23 20 20 17 16
29 21 22 20 17 15 13 11 11 12
Good 28 20 21 19 16 14 12 10 10 11
22 15 17 13 13 11 10 7 8 5
Fair 21 14 16 12 12 10 9 6 7 4
17 10 12 8 10 5 7 2 5 2
Needs improvement
16 9 11 7 9 4 6 1 4 1
Table 2.7 Fitness categories for the press-up test (Source: CSEP in ACSM, 2014)
Copyright © 2014 Active IQ Ltd. Not for resale | 233
Section 2: Physical assessmentsPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Abdominal curl testInstructions
• Use a matted area to cushion the lumbar spine.
• The client lies on their back with their knees bent to 90° with arms straight and palms down.
• The test is scored on the number of times the client can raise their shoulder blades off the mat (trunk at 30° of spinal flexion), so that the fingers touch a line three inches away from the resting position.
Table 2.8 highlights fitness categories for the abdominal curl test.
ABDOMINAL CURLS COMPLETED BY AGE AND SEX
Age 20-29 30-39 40-49 50-59 60-69
Sex M F M F M F M F M F
Well above average
75 70 75 55 75 55 74 48 53 50
Above average 56 45 69 43 75 42 60 30 33 30
41 37 46 34 67 33 45 23 26 24
Average 31 32 36 28 51 28 35 16 19 19
27 27 31 21 39 25 27 9 16 13
Below average 24 21 26 15 31 20 23 2 9 9
20 17 19 12 26 14 19 0 6 3
Well below average
13 12 13 0 21 5 13 0 0 0
4 5 0 0 13 0 0 0 0 0
Table 2.8 Fitness categories for the abdominal curl test (Source: CSEP in ACSM)
Flexibility testingFlexibility is the potential for movement at a joint and the ability to lengthen a muscle without causing structural damage. Flexibility is affected by many factors, including muscle mass, bone structure, adipose tissue and skin.
There are a number of tests used to measure flexibility. Where possible it is advisable to gauge flexibility through observation of a client’s range of movement, although this can be difficult to ascertain without actual measurement.
Sit and reach test
The sit and reach test assesses the flexibility of the hamstrings and lower back. The test is relatively safe to perform, provided the client is warm and has no low back injury (e.g. a prolapsed disc). Clients with back injuries should be referred to their GP for further evaluation before exercise and might need to follow a specialist programme.
234 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Physical assessments

Instructions• This test should only be performed after a thorough warm-up.
• The client should remove shoes and items of clothing that restrict movement.
• Position the client with their feet flat against the board – their legs and back should be straight.
• Ask the client to reach forward slowly and smoothly, maintaining a straight back for as long as possible.
• Record the distance reached at the point where the client starts to bend their back; this is a measure of hamstring flexibility.
• Ask the client to continue to reach forwards as far as possible (bending their back) and record the furthest point. This is a measure of hamstring and lower back flexibility.
End of section: Learning check Answer the questions and make notes to revise this section.
• What is the purpose of physical assessments?
• What would be an appropriate environment for carrying out physical assessments?
• What information can be gathered from a BMI measurement?
• What information can be gathered by checking a client’s resting heart rate?
• What would be the benefit of using a press-up or curl-up test?
• What component of fitness is assessed by the Rockport test?
• Why is it important to gain informed consent before carrying out assessments?
• What information might you need to give to a client before any physical assessments?
• How could you promote the validity and reliability of physical assessments?
• Why might some tests be inappropriate for certain clients?
PLEASE NOTE:The information on physical assessment is provided for interest and future reference. You will not be required to conduct these assessments or gather this information for the level 2 fitness instruction qualification.
Copyright © 2014 Active IQ Ltd. Not for resale | 235
Section 2: Physical assessmentsPLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Section 3: Understanding how to plan gym-based exercise
All programmes should be planned with consideration for the client’s needs and wants. When planning a gym-based programme the fitness instructor should take into account the client’s:
Fitness instructors’ duties also include:
• Agreeing objectives with clients that are appropriate for:
• Their needs and potential.
• Accepted good practice in the industry.
• Their own level of competence.
• Choosing gym-based exercises that help clients to develop their:
• Cardiovascular fitness.
• Muscular fitness.
• Flexibility.
• Motor skills.
• Ensuring risks are minimised throughout the programme.
• Planning realistic timings and sequences for exercise.
• Recording programme plans in an appropriate format.
Agreeing goals and objectives with clientsAgreeing objectives and setting goals with clients are examples of ‘good industry practice.’ They are ethical requirements, stated within the code of conduct for exercise and fitness professionals. Agreeing on goals and objectives ensures that the programme design fulfils the client’s expectations, wants and needs.
All objectives should be fully discussed, clarified and checked with the client to identify:
• Which goals are most important and can be focussed on immediately?
• Which goals might need to be set as longer-term goals?
All planned goals must be realistic for the client and their training experience. The aim of goal-setting is to encourage achievement and not set the client up for disappointment or failure. For example, if an inactive client were to say that they would like to run a marathon, it would be impracticable as a short-term goal (for most inactive people). Initial goals could be to raise their activity levels and establish a regular pattern of active behaviour. Medium- and longer-term goals could be set to develop cardiovascular fitness (walking and running), with a targeted objective to run short distances (6km).
Age and any age-related physiological changes.
Current activity levels.
Time available.
Goals, i.e. what they want to achieve.
Fitness and skill level.
Health status.
Activity preferences.
236 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

TSSPECIFIC MEASURABLE ACHIEVABLE REALISTIC
AND RELEVANT
TIME-BOUND
M A R
The programme can be planned to work progressively towards SMART goals once they have been agreed and set.
The goals will need to be reviewed regularly with the client to:
• Check their progress and reward achievement (praise and encouragement).
• Discuss any changes in goals. For example, a client may ‘change their mind’ and want to set a different target, or they might experience obstacles, such as unexpected time commitments.
The SMART goal-setting formula should be used to set short-, medium- and long-term goals. All goals should be:
Planning gym-based exercise to meet the needs of clients with different objectivesAll programmes should be planned to meet the client’s objectives. There is a broad range of objectives, or reasons, for wanting to exercise:
• Improving posture.
• Improving flexibility.
• Improving strength or endurance.
• Improving cardiovascular fitness.
• Losing weight or body fat.
• Increasing muscle hypertrophy.
• Improving muscle tone.
• Improving health or wellbeing; this can include managing stress and lowering blood pressure.
Different objectives require different programme designs and content. When designing programmes, in order to meet specific objectives, the ACSM recommendations (frequency, intensity, time and type) for each component of fitness should be considered.
The nature of the objective governs the components of fitness that should be trained. Personal client information can also determine whether these goals are achievable and realistic for their needs.
KEY POINTThe ACSM recommendations for different components of fitness should be considered when designing programmes for clients.
Copyright © 2014 Active IQ Ltd. Not for resale | 237
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

OBJECTIVE COMPONENT OF FITNESS AND INITIAL CONSIDERATIONS
Posture To improve posture the exercises planned would need to:• Strengthen weakened or overly-lengthened muscles (muscular fitness exercises).• Lengthen muscles that are tightened or shortened (flexibility or stretching exercises).
Flexibility To improve flexibility, exercises will need to be planned to develop flexibility of shortened or tight muscles (developmental stretching on most days of the week).
Health For general health-related fitness goals, exercises need to be programmed to train all components of fitness:• Cardiovascular fitness: five times per week, moderate intensity, 30 minutes.• Muscular fitness: twice per week.• Flexibility: two-three times per week (ideally daily).
Cardiovascular fitness To improve cardiovascular fitness, exercises would need to be planned to work towards the ACSM recommendations: vigorous intensity, 20 minutes, three times per week.
Suitable exercises include walking, swimming, cardiovascular machines and cycling.
NB: Clients’ health status and fitness levels affect the prescription. Some clients would need to start at a low frequency, intensity and timescale.
Fat loss and weight management programmes
Exercises would need to be planned to increase energy expenditure on a regular basis. Clients may be deconditioned and untrained, therefore initial frequency, intensity and duration would need to be low and progress steadily (emphasis should be on cardiovascular exercise but all components of fitness should be covered).
Muscular fitness goals (e.g. strength or hypertrophy)
To develop muscular fitness and work towards specific training goals (hypertrophy or strength), specific variables (repetitions, resistance and sets) would need to be manipulated in a certain way.
The ACSM muscular strength and endurance guidelines are the starting point to work towards before developing specialised or advanced objectives.
Table 3.1 Objectives and components of fitness
Resistance and muscular fitness objectivesBefore working towards specific muscular fitness training goals, it is important to develop a baseline level of muscular fitness by working towards the ACSM recommendations. Once a baseline level has been established, goals can become specific and focussed. Some training variables (reps, sets and recovery between sets) can be manipulated to work towards some of the common resistance training objectives and goals.
TRAINING GOAL STRENGTH HYPERTROPHY ENDURANCE
Intensity High Moderate Low
Load as % of 1 RM >85% of 1 repetition maximum
(RM)
67-85% of 1 repetition maximum
(RM)
<67% of 1 repetition maximum
(RM)
Repetitions 1-5 repetitions per set
6-12 repetitions per set
12+ repetitions per set
Recovery time between sets
3-5 minutes’ rest between sets
1-2 minutes’ rest between sets
30-60 seconds’ rest between sets
Sets per exercise 2-6 sets per exercise
3-6 sets per exercise
2-3 sets per exercise
Frequency per muscle group
1-2 times per week per muscle group
1-2 times per week per muscle group
2-3 times per week per muscle group
Adapted from Baechle and Earle, 2000
Table 3.2 Resistance training objectives and variables
238 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

Training experience and ageIt is important to consider the training experience (training age) of the client before setting any goals or planning the programme. The client’s training experience (current fitness) would determine the frequency (how often), duration and intensity of training required. Training variables can be progressed for resistance training, as the client’s training experience increases.
TRAINING STATUS
FREQUENCY GUIDELINES (SESSIONS PER WEEK)
EXAMPLE SYSTEM AND TRAINING APPROACH
Beginner 2-3 • Single-set or circuit weight training. • Whole-body approach. • Fewer repetitions (8-12).
Intermediate 3-4 • Multiple-set. • Repetitions and resistance varied to achieve specific fitness goals.
Advanced 4-7 • Split routine (different muscles trained on different days of the week), with advanced training systems.
• Repetitions and resistance varied to achieve specific fitness goals.
Baechle and Earle, 2000.
Table 3.3 Resistance training and training experience
Goals will become more specific and training systems more advanced as the frequency of resistance training increases. For example, a beginner might work with a single-set system which has a whole-body approach and train two-three times per week, whereas an advanced client may train more frequently, using a split routine (different muscles on different days of the week). Exceeding the maximum recommended frequency on a regular basis would be inadvisable, as the client’s ability to recover from the load would be compromised.
Exercises that develop different components of fitness Different components of fitness require different types of exercises and activities. Activities that can be planned to improve specific components of fitness are included in table 3.4.
COMPONENT OF FITNESS
EXERCISES
Cardiovascular fitness
• Body weight exercises, e.g. squats, lunges, jumping jacks, marching, jogging and shuttle runs (any exercise that uses large muscle groups continuously and rhythmically).
• Cardiovascular machines, e.g. treadmill, stepper and rower. • Group exercise, e.g. circuit training, exercise to music, exercises in water and indoor cycling.
Muscular fitness
• Body weight exercises, e.g. curl-ups, squats, back extensions, press-ups and various yoga and Pilates postures.
• Exercises with dumbbells or resistance bands, e.g. bicep curls, shoulder press and lunges.• Fixed-resistance machine exercises, e.g. chest press, leg press and leg extension machines. • Free weight exercises, such as bench press, squatting and group resistance training
programmes, e.g. body pump.• Manual resistance (applied by a partner or an opposing limb).• Cable machines. • Water-based resistance exercises, e.g. using water bells and floatation devices to provide
resistance against the water.
Flexibility • Developmental stretching.• Group exercise, e.g. yoga, Pilates, Tai chi and stretch classes.
Motor skills • Specific exercises for each skill-related component, e.g. balance, coordination, power, reaction time and speed.
• Free weight exercises would require more balance and coordination than using resistance machines.
Table 3.4 Exercises and activities that improve specific components of fitness
Copyright © 2014 Active IQ Ltd. Not for resale | 239
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

These machines can be used for:
• Warming up and preparing for exercise.
• Cardiovascular training goals.
• Cooling down (lowering the heart rate) or rewarming the muscles before stretching at the end of a session.
An instructor might use a single machine or a combination when training clients, depending on the programme.
Other considerations for planning activities on cardiovascular machines include:
• The level of weight-bearing or body support provided.
• Impact (low or high).
• Technical or skill demands of the equipment (e.g. balance).
• Similarity of the activity and joint actions to daily activities (e.g. walking would be more familiar for most people than rowing or stepping), which can influence perceived difficulty.
• Client preferences.
Rowing machine.
Elliptical trainer.
Cross trainer.
Upright cycle.
Recumbent cycle.
Treadmill.
Stepper.
Cardiovascular and resistance training machinesThere are various cardiovascular and resistance machines, free weight and body weight exercises that can be used to meet clients’ cardiovascular and resistance training objectives.
Cardiovascular machines
Examples of cardiovascular machines that can be used with clients include:
240 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

MA
CH
INE
VA
RIA
BLE
SU
SES
AN
D C
ON
SID
ER
ATIO
NS
PR
IOR
TO
SELE
CTI
ON
Upr
ight
cyc
le•
Spee
d •
Leve
l or
resi
stan
ce
Card
iova
scul
ar w
ith lo
wer
bod
y (le
g) e
ndur
ance
bia
s. It
is n
ot w
eigh
t-be
arin
g so
no
impa
ct s
tress
is e
xert
ed o
n jo
ints
, eve
n th
ough
the
cycl
ing
actio
n is
rep
etiti
ve. T
runk
sta
bilit
y is
req
uire
d to
mai
ntai
n up
right
pos
ture
(so
me
clie
nts
mig
ht fi
nd th
is c
halle
ngin
g).
Rec
umbe
nt c
ycle
• Sp
eed
• Le
vel o
r re
sist
ance
Card
iova
scul
ar w
ith lo
wer
bod
y (le
g) e
ndur
ance
bia
s. It
is n
ot w
eigh
t-be
arin
g so
no
impa
ct s
tress
is e
xert
ed o
n jo
ints
. The
rec
umbe
nt
cycl
ing
actio
n is
not
a ty
pica
l dai
ly li
fe a
ctiv
ity, s
o so
me
may
find
it m
ore
chal
leng
ing
than
upr
ight
cyc
ling
(mos
t peo
ple’
s pr
evio
us
cycl
ing
expe
rienc
e is
upr
ight
, rat
her
than
rec
umbe
nt).
The
mac
hine
offe
rs s
uppo
rt fo
r th
e ba
ck, w
hich
may
be
bene
ficia
l for
clie
nts
who
ne
ed b
ody
wei
ght o
r ba
ck s
uppo
rt.
Trea
dmill
• W
alki
ng o
r ru
nnin
g•
Spee
d an
d di
stan
ce
• In
clin
e
Card
iova
scul
ar w
ith lo
wer
bod
y (le
g) e
ndur
ance
bia
s. It
can
be
used
for
wal
king
or
runn
ing.
Wei
ght-
bear
ing
exer
tion
is o
n th
e lo
wer
bo
dy. W
alki
ng is
a lo
w-im
pact
dai
ly a
ctiv
ity fo
r m
any
peop
le. I
t is
effe
ctiv
e fo
r w
arm
-ups
and
CV
train
ing
amon
g cl
ient
s w
ith lo
w le
vels
of
fitn
ess.
Incl
ine
can
be v
arie
d to
add
inte
nsity
. Run
ning
is a
hig
h-im
pact
act
ivity
that
req
uire
s pa
rtic
ular
alig
nmen
t ski
ll an
d ex
erts
m
ajor
stre
ss o
n jo
ints
. Som
e cl
ient
s fin
d in
itial
bal
ance
a c
halle
nge.
Step
per
• Sp
eed
• St
airs
clim
bed
• Le
vel o
r re
sist
ance
Card
iova
scul
ar w
ith lo
wer
bod
y (le
g) e
ndur
ance
bia
s. W
eigh
t-be
arin
g ex
ertio
n is
on
the
low
er b
ody.
It is
low
-impa
ct. T
he r
epet
itive
, w
eigh
t-be
arin
g st
eppi
ng a
ctio
n ca
n be
cha
lleng
ing
for
som
e pe
ople
.
Row
ing
mac
hine
• Sp
eed
• Le
vel o
r re
sist
ance
Card
iova
scul
ar w
ith m
uscu
lar
endu
ranc
e bi
as fo
r th
e le
gs, b
ack
and
arm
s. It
is n
ot w
eigh
t-be
arin
g, s
o no
impa
ct s
tress
is e
xert
ed o
n jo
ints
. The
use
of m
ultip
le g
roup
s an
d co
ordi
natio
n of
row
ing
actio
n m
ay b
e ch
alle
ngin
g fo
r so
me
peop
le. I
t req
uire
s so
me
flexi
bilit
y to
use
with
cor
rect
alig
nmen
t and
tech
niqu
e. A
bdom
inal
bod
y fa
t can
get
in th
e w
ay o
f effe
ctiv
e ro
win
g ac
tion
(e.g
. hip
s ro
tatin
g ou
twar
ds).
Tru
nk s
tabi
lity
is r
equi
red
to m
aint
ain
an u
prig
ht p
ostu
re (
som
e m
ight
find
this
cha
lleng
ing)
.
Elli
ptic
al t
rain
er•
Spee
d •
Leve
l or
resi
stan
ce
Card
iova
scul
ar w
ith lo
wer
bod
y (le
g) e
ndur
ance
bia
s. W
eigh
t-be
arin
g fo
r lo
wer
bod
y . It
is a
low
-impa
ct a
ctiv
ity. S
ome
clie
nts
find
initi
al
bala
nce
and
initi
atin
g ac
tion
a ch
alle
nge.
Cro
ss t
rain
er
• Sp
eed
• Le
vel o
r re
sist
ance
Card
iova
scul
ar w
ith m
uscu
lar
endu
ranc
e bi
as fo
r th
e le
gs, b
ack
and
arm
s. W
eigh
t-be
arin
g ex
ertio
n is
on
the
low
er b
ody .
It is
a lo
w-
impa
ct a
ctiv
ity. S
ome
clie
nts
find
initi
al b
alan
ce a
nd a
ctio
n in
itiat
ion
a ch
alle
nge.
Tabl
e 3
.5 C
ardi
ovas
cula
r m
achi
ne u
ses
and
plan
ning
con
side
ratio
ns
Copyright © 2014 Active IQ Ltd. Not for resale | 241
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Resistance exercises
Resistance exercises are useful for working towards muscular fitness goals. Examples include:
• Body weight exercises.
• Free weights (barbells or dumbbells).
• Fixed resistance machines.
When working with clients it is important to consider their training goals, level of experience, personal needs and current fitness levels. All of these factors should influence the choice of exercises. Major considerations include:
EXERCISES AND EQUIPMENT
Some exercises require more technical skill and stability (e.g. certain free weight exercises) than others, meaning that they are more appropriate for clients with an established level of fitness and experience than beginners. Clients with low fitness levels may need to focus on body weight exercises before adding extra resistance or honing balance skills.
THE NUMBER OF EXERCISES
This would depend on the client’s training experience, skill level and fitness level. For general muscular fitness, the aim would be to take a whole-body approach with muscle balance, although newcomers may struggle to remember or perform copious exercises (overwork). Compound exercises that work multiple muscle groups might be more time- and memory-efficient than lots of isolation exercises. Similarly, an advanced exerciser might work with a split routine (different muscles on different days) and with a large volume of exercises (compound and isolation) for the same muscle groups.
THE TRAINING APPROACH
For general fitness and newcomers, single-set training approaches and circuit weight training might be most appropriate. Experienced exercisers tend to have particularly focussed goals and might use multiple-set approaches.
SUMMARY OF CONSIDERATIONS
• The number of exercises planned.
• The muscles worked (muscle balance).
• The exercise or equipment complexity and the stability or balance required.
• Isolated or compound exercises.
• The training approach (single- or multiple-set).
242 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

JOINT MOTION AND PRIME MOVER
RESISTANCE MACHINE FREE WEIGHT EXERCISE BODY WEIGHT EXERCISE
Shoulder flexionAnterior deltoid
Seated chest press(neutral grip)
Front raise (DB)
Shoulder extensionPosterior deltoidLatissimus dorsi
Seated row (low pulley) Seated row (neutral grip)
Single-arm rowBent-arm pull over (DB)Bent-over row
Shoulder abductionMedial deltoid
Shoulder press Shoulder press (DB)Lateral raise (DB)Upright row (BB)
Shoulder adductionLatissimus dorsi Pectoralis
Lat pull-down (front of chest)Assisted pull-up
Chins
Shoulder horizontal flexionPectoralis
Bench press Seated chest press (BB grip)Pec dec
Bench pressFlyes (DB)
Press-up
Shoulder horizontal extensionTrapeziusRhomboids
Seated row (BB grip) Prone flye (DB)
Elbow extensionTriceps
Triceps push-down (high pulley)Triceps press
Supine triceps press (BB)Single-arm triceps press (DB)
Press-upTricep dips
Elbow flexionBiceps
Bicep curl (low pulley) Seated bicep curl
Bicep curl (BB) (DB)Preacher curlConcentration curl
Hip extensionGluteus maximus
Leg pressTotal hip
Lunge (BB, DB)Dead lift (BB) (DB)
LungeRear leg raises
Hip adductionAdductors
Seated adductorTotal hip
Side leg raises
Hip abductionGluteus medius and minimus
Seated abductorTotal hip
Inner thigh raises
Knee extensionQuadriceps
Seated knee extensionLeg press
LungeDead lift (BB) (DB) Squat (DB) (BB)
LungeSquat
Knee flexionHamstrings
Lying thigh curlSeated thigh curl
Trunk flexion, rotation Rectus abdominus Obliques
Ab machine flexion Abdominal curlOblique twists
Spinal extensionErector spinae
Lower back machine Dead lift (BB) (DB) Back raise
Table 3.6 Resistance exercises (machines, free weight, body weight)
Copyright © 2014 Active IQ Ltd. Not for resale | 243
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

How to plan gym-based exercise Gym-based exercise needs to be structured and planned using the FITT principles (frequency, intensity, time and type).
Session structure
A gym-based session should contain:
• A warm-up to prepare the body for activity.
• A main session to train specific components of fitness: cardiovascular fitness (cardiovascular machines) and muscular fitness (resistance exercises).
• A cool-down to return the body to a non-exercising state and improve flexibility.
WARM-UP
MAIN WORKOUT
COOL-DOWN
> MOBILISE JOINTS
> INCREASE BODY TEMPERATURE
> LENGTHEN MUSCLES
> CARDIOVASCULAR FITNESS
> MUSCULAR FITNESS
> MAINTAIN FLEXIBILITY
> INCREASE FLEXIBILITY
244 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

Warm-up exercises
MOBILITY EXERCISES
Upper body mobility (body weight)Shoulder lifts and circles Arm circles and raises Shoulder pressing actionChest pressing action
NB: These can be performed while cycling or walking if the client can balance.
Trunk mobility (body weight)Rotations Side bends
Lower body (body weight)Knee raisesLeg curls Foot pedalling Calf raises
CV machines Cycling, treadmill and stepper mobilise the lower body (knees, hips and ankles).Rowing and cross trainer mobilise the lower (knees, hips and ankles) and upper body (elbows, shoulders) in specific movement ranges.
WARMING EXERCISES (PULSE-RAISING)
Using a CV machine warms the muscles and raises heart rate. Intensity should be progressed gradually and in accordance with the client’s level of fitness.
STRETCHING EXERCISES
Static or range-of-motion stretches Whole-body approach
NB: Static and range-of-motion upper body stretches can be performed while using some CV machines, provided the client has sufficient balance, e.g. chest pressing action while walking or cycling.
SPECIFIC WARM-UP (RESISTANCE TRAINING)
Light sets A light set of resistance exercises is sometimes used by advanced exercisers to prepare specifically for the main resistance workout.
SPECIFIC WARM-UP (CARDIOVASCULAR TRAINING)
Using a CV machine warms the muscles and raises heart rate.
Certain machines can also mobilise joints and lengthen muscles to the range of motion they will extend to during the main workout:• Cycling, treadmill and stepper mobilise the lower body (knees, hips and ankles).• Rowing and cross trainer mobilise the lower (knees, hips and ankles) and upper body (elbows, shoulders) in
specific movement ranges.
Table 3.7 Examples of gym-specific warm-up activities
Copyright © 2014 Active IQ Ltd. Not for resale | 245
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

150 minutes of moderate-intensity aerobic activity per week.
75 minutes of vigorous aerobic activity per week.
An equivalent mix of moderate- and vigorous-intensity aerobic activity each week.
Main workout: Exercise methodology and programme design
Cardiovascular (aerobic) fitness
Aerobic fitness is defined as the ability to take in, transport and utilise oxygen.
The understanding and application of training principles (frequency, intensity, time and type) is central to any physical adaptation, especially the principles of overload and specificity. These state that a minimum intensity of effort is necessary and the stimulus must be specific to the objectives if a physiological adaptation is to occur. In other words, the oxygen system must be stressed in a manner that accelerates breathing and heart rate.
Prescribing aerobic exercise
Current guidelines (Department of Health, 2011; ACSM, 2014) stipulate that in order for adults aged 19-64 to remain healthy they should exercise daily and aim for at least:
KEY POINTOnly an estimated 40% of men and 28% of women in England meet the activity guidelines.
(Department of Health, 2011)
REVISION POINT Aerobic fitness is defined as the ability to take in, transport and utilise oxygen.
MODERATE-INTENSITY
Exercise is defined as an intensity that causes a person to become slightly out of breath without undue fatigue. For the majority of unfit clients this would be equivalent to a brisk walk or gentle cycle and is associated with the lower end of 60-90% MHR. Using the RPE scale, moderate-intensity exercise is perceived as ‘light’ or an RPE of 11.
VIGOROUS EXERCISE
Causes people to become out of breath and start to sweat. It would correlate with the higher end of the 60-90% MHR or, if using RPE, would be cited between ‘somewhat hard’ and ‘hard’ – a rating of 13-14. Vigorous activity causes significant improvements in fitness levels and, when performed for short durations, can contribute to general health (Department of Health, 2011).
Intensity
Aerobic training has proven to be beneficial when performed at an intensity of 60-90% of maximum heart rate (MHR).
Or
Or
246 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

1 LONG SLOW DURATION (LSD) TRAINING.
INTERVAL TRAINING.
FARTLEK TRAINING.
2
3
Approaches to cardiovascular training In general, cardiovascular and aerobic training can be grouped into three main categories:
Long slow duration (LSD) training
LSD training was traditionally considered to be aerobic training. It involves working for extended periods of time (usually ten minutes or more) at fairly low intensities (50-70% MHR). The intensity of LSD training can vary throughout the session and best suits deconditioned clients and beginners (McArdle et al, 2001).
The benefits of LSD training include all of the physiological adaptations that improve specific aspects of the cardiovascular systems (heart, lungs and blood vessels) and oxygen transportation.
For intermediate and advanced exercisers, LSD training has traditionally formed the majority of training for endurance-based sports, such as the marathon. However, training exclusively at LSD levels eventually causes fitness to plateau.
KEY CONSIDERATIONLSD training lacks specificity in relation to many sporting activities. A football player has to perform at various levels of intensity and move in many different directions for 90 minutes. Therefore, it doesn’t make sense to continually perform LSD training in a straight line, as adaptations are specific to the type of stimulus applied.
Copyright © 2014 Active IQ Ltd. Not for resale | 247
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Interval training
Interval training involves structured periods of work and recovery; it is an effective way of developing the aerobic energy system fully. Intervals can vary from a few seconds to several minutes (McArdle et al, 2001). Exercising at higher intensities (which is done in most sports and activities) can only be maintained for a couple of minutes, due to the shortfall in oxygen supply against oxygen demand. As a result the lactic acid energy system is needed to make up the energy anaerobically so that intensity levels can be maintained.
One important benefit of interval training for many athletes and sports people is that it develops a person’s ability to tolerate high levels of lactic acid and the rate at which it is removed from the muscles.
The following should be considered when planning an interval programme:
• Interval intensity.
• Interval duration.
• Interval recovery period.
• Number of intervals including recovery periods.
Work and recovery intervals can both be tailored to clients’ ability levels, for example:
• An intermediate exerciser could be prescribed an aerobic interval training session with a three-minute work interval, followed by three minutes’ recovery, performed two-five times. The total time equivalent would be between 12 and 30 minutes.
• An advanced exerciser might have a three-minute work interval followed by 90-second rest interval, performed four-six times. The total time equivalent would be between 18 and 27 minutes.
Fartlek training
Fartlek is a Swedish term meaning ‘speed play.’ It involves the random interplay of different speeds. Fartlek training can be considered an unstructured form of interval training where the total amount of work is performed (around 30-40 minutes) at a sporadically changing variety of intensities.
Fartlek approaches can be tailored to different levels of fitness, for example:
• A client who is new to exercise could walk at randomly changing paces on a treadmill or use an incline for a short duration to add a small challenge.
• An experienced exerciser could run on a treadmill with random sprints or changes in incline for short time periods.
Fartlek approaches are useful for adding variety and can be tailored to a client’s RPE. It can be a lot of fun and lends itself to indoor programmes (circuit and group training approaches) and outdoor programmes (e.g. circuits, boot camps, group walking or running programmes).
248 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

Progression of cardiovascular exerciseCardiovascular activities need to start at an appropriate level for the client (frequency, intensity, time and type) and progress steadily over time.
Training beginners
Beginners should perform moderate-intensity activities that do not cause undue fatigue, discomfort or muscle soreness. Beginners should initially train three to four times per week working towards a guideline of five weekly sessions. The sessions should aim for 30 minutes of continuous exercise, or as long as the client can manage. Unfit clients may struggle to work continuously, so working towards 30 minutes with a low-level interval type is recommended.
It is important to note that beginners can demonstrate improvements in fitness relatively quickly and may plateau in as little as three weeks (Hickson and Rosenkoetter, 1981). For this reason, the exercise stimulus must be increased accordingly.
PROGRAMME CARD (EXCERPT)
Cardiovascular training
CV machine Time and frequency
Intensity Variables Speed Notes
Treadmill 30 minutes on 3-5 days a week
RPE 11 1% incline 7.5 KPH Long slow distance approach Aerobic focus
Table 3.8 Programme card excerpt
Training intermediate to advanced exercisers
Once an exerciser can complete 30 minutes of moderate-intensity activity five times per week, it is time to progress their training by manipulating the training principles. The most obvious change would be to increase the intensity of exercise within each session (i.e. from moderate to vigorous). For example, if the person had been working for 30 minutes at 60% MHR it would be sensible to increase the intensity to 70% MHR. Alternatively, the exercise duration could be increased to an hour, with shorter (random or Fartlek) intervals of higher-intensity work.
You must never progress a client too quickly; this can demotivate them and possibly cause an overuse injury from the increase in training volume.
An excellent way of introducing clients to higher intensities is to use interval training. The client should be encouraged to work at a moderate intensity with high-intensity periods. The long-term goal is to work towards managing a full session at a high intensity.
Any programme of physical activity will eventually plateau, so consideration should be given to the long-term plan if results are to be consistent. If training entails repeating an activity continuously, it will become very boring and the physiological adaptations would diminish. Once a baseline level of fitness is established, it is beneficial to vary training approaches (LSD, interval and Fartlek training) and try different types of cardiovascular machines (e.g. rower or stepper) to broaden the range of training stimuli.
Copyright © 2014 Active IQ Ltd. Not for resale | 249
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

TRAIN SYNERGISTS AND FIXATORS LAST.4
ACTI
VIT
Y Think about how you would plan a cardiovascular programme for:
• A sedentary beginner who wants to improve their health.
• An intermediate or advanced client who wants to improve their aerobic fitness.
Consider:
• What cardiovascular machine(s) you would use.
• What frequency, intensity and duration you would recommend.
• What approach to training you would use.
• What additional information about the client you might need.
• How you would progress the programmes over six to ten weeks.
1 PROMOTE MUSCULAR BALANCE (WITH CONSIDERATION FOR THE NUMBER OF EXERCISES).
TRAIN LARGE MUSCLES FIRST.
PERFORM COMPLEX AND HIGHLY SKILLED EXERCISES FIRST.
2
3
Muscular fitnessThe safety and effectiveness of a resistance training programme is profoundly influenced by the choice and order of the exercises. Useful strategies for programme design and exercise selection are to:
Muscular balance
Muscle balance describes the action of working all the major muscle groups. Focussing on one or two body areas can hinder overall balance and cause postural imbalances.
A concerted effort should be made to include exercises that promote postural improvement, coordination, proprioception and core strength.
ACTI
VIT
Y Draw the table below in your notebook and complete the information.
• The muscles of the different body areas.
• An exercise that uses the muscles in each area.
Body area Back Arms Legs Abdominals Chest Shoulders
Muscles
Exercise
250 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

The number of exercises selected to achieve a balanced approach depends on the objective of the workout, the client’s experience level and the time available.
Beginners might need fewer exercises (due to low skill and fitness levels) than advanced or intermediate exercisers.
Advanced exercisers might need to split their training routine to manage the demanding exercise volume.
A rough guideline for the number of resistance exercises to be selected per workout is four to ten.
ACTI
VIT
Y In your notebook:
Make a list of ten exercises that would provide a whole-body approach and work all areas.
Select four exercises that could achieve a whole-body approach and be used for a beginner.
Training large muscles
The large muscle groups should be trained first if multiple groups are to be used during a workout. Large muscle groups require the most energy to train effectively and by performing appropriate exercises early in the workout the client can obtain the greatest training effect for the large muscles (Fleck and Kraemer, 1997). Effectively loading the large muscle groups (i.e. muscles of the hips, thighs, upper back and chest) can accelerate the client’s overall progress (e.g. fat-burning potential or functional muscular fitness).
Performing complex and high-skill movements
Complex and multi-joint exercises require more energy and greater neuromuscular coordination to be performed safely and effectively than isolation exercises.
Compound exercises are best performed early in the workout when the client is free from both neural and metabolic fatigue. This is especially true for beginners who are comparatively more susceptible to fatigue and often have a low skill level.
Copyright © 2014 Active IQ Ltd. Not for resale | 251
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Training synergists and fixators
Appropriate exercise order is one of the fundamental prerequisites of successful programme design. If synergists are trained before the agonists (prime movers) in a workout then the fatigue accumulated will render them ineffective for performing their synergistic role when the agonist is trained. Inappropriate examples of this include:
• Training the triceps brachii (e.g. cable push-down or lying barbell extensions) before upper body pressing exercises (e.g. bench press or shoulder press).
• Training the biceps brachii (e.g. barbell or dumbbell curls) before any upper body pulling or rowing exercise (e.g. lateral pull-downs, bent-over rows or chins).
These inappropriate exercise orders would result in an ineffective workout for the larger muscles of the torso (e.g. pectoralis major, latissimus dorsi and deltoids); this would limit the client’s potential to make progress or gains in these areas.
Fixators contract in a predominantly isometric manner to fixate or stabilise part of the body and give the agonist a solid platform from which to work. The musculature of the core takes on a fixation role in the majority of free-standing, free weight exercises; especially those that are compound or multi-joint in nature (e.g. squats, deadlifts, overhead presses or bent-over rows).
Training the core before the rest of the body can be inappropriate for a resistance training session, as fixator fatigue would decrease the ability of the body to keep the spine in a safe alignment during exercise. Note that this can sometimes be suitable for advanced exercisers, or as part of a warm-up, to ‘wake up’ the stabilising muscles, provided intensity and volumes are low.
TRAINER TIP Training the core before the rest of the body in a resistance training session can be unwise, as fixator fatigue would decrease the ability of the body to keep the spine in a safe alignment during exercise.
ACTI
VIT
Y List these exercises in the correct order, according to the basic programme design principles. Discuss with a peer.
• Barbell bicep curl.
• Wide grip bent-over row.
• Barbell squat.
• Dumbbell shoulder press.
• Lateral pull-down.
• Lying barbell triceps extension.
• Plank.
• Stiff-leg deadlift.
• Barbell bench press.
• Dorsal raise (back raise).
252 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

Progression of resistance trainingResistance programmes need to start at an appropriate level for each client (in terms of frequency, intensity, time and type) and progress steadily over time. The recommended frequency for muscular fitness training is twice a week, on non-consecutive days, for the same muscle groups. The repetitions and resistance required would depend on the training goals.
Resistance training for beginners
Novice clients require a logical, structured introduction for resistance training. This allows them to develop a solid foundation that can be built upon as they progress. Common issues experienced by deconditioned beginners include:
Inefficient exercise technique and proprioception.
Lack of muscular strength and endurance.
Low aerobic conditioning.
Weak connective tissue.
Posture misalignment and muscle imbalance.
Low core strength.
You must consider these issues when planning exercise, so that the client can improve and progress safely.
Technique and proprioception
Newcomers to resistance training tend to have limited proprioception and poor exercise technique. This is generally down to a sedentary lifestyle and a lack of previous exposure to the exercise stimulus.
Efficient exercise technique (safe and effective) can be viewed as a person’s ability to perform the desired movement or exercise pattern consistently without external feedback (e.g. verbal, visual or physical correction).
Proprioception is a skill-related component of fitness. It describes a person’s sense of the positioning of their musculoskeletal structures, in relation to one another. Proprioception can be viewed as a sense of positional awareness without external guidance. For example, a client with good proprioception is able to know they have adopted a neutral spine position during a bent-over row without having to check in a mirror. In this instance the proprioceptive elements of the neuromuscular system provide continuous feedback, informing the central nervous system (and therefore the client) of the position of their spine and other joints involved in the exercise.
Designing resistance training programmes for beginners requires you to take their issues into account but, at the same time, address them. A lack of proprioception can compromise the client’s safety and compromise the overall effectiveness of the workout.
TRAINER TIP Safe, effective alignment or good exercise technique should be established before the progression of intensity.
Copyright © 2014 Active IQ Ltd. Not for resale | 253
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

ACT
IVIT
Y Use your notebook to design the main session of a resistance training programme for a 31-year-old female client. She is new to the gym and has no injuries or illnesses that would prevent her from performing any exercises.
Include ten resistance exercises and plan sets with appropriate repetitions and recovery periods in between. Consider the weekly workout frequency. The main session should last for 35-40 minutes; you can assume your client has performed a thorough warm-up beforehand.
You can discuss your programme with a peer or tutor using these criteria:
• How does the programme provide muscle balance?
• To what extent is the order of exercises effective?
• How would the exercises improve proprioception (which exercises)?
• How would the exercises improve posture (which exercises)?
• How would the exercises improve core strength (which exercises)?
• How would the exercises enhance function (which exercises)?
• How does the programme provide variety?
• How would the programme provide a sense of achievement?
• How would the programme fit with the client’s available time?
A general rule of resistance training is that good technique should always be established before the progression of intensity. Improper technique is commonplace among clients who attempt exercises with loads that exceed their strength capabilities.
It is advisable that the beginner initially concentrates on compound, multi-joint, free-standing exercises, such as squats, deadlifts, bent-over rows and overhead presses. This ensures that they develop functional movement patterns, which are transferable into everyday situations, as they hone their exercise technique.
It is also advisable for the beginner to start by performing resistance exercises within the muscular endurance repetition range, i.e. 12 or more repetitions per set. This allows for the performance of more repetitions while using a relatively low resistance, which is an ideal approach for learning techniques safely.
Programme goals for beginners
Designing a resistance-based programme for a deconditioned novice client requires you to ensure it meets the programme design rules and achieves certain objectives:
• Improving proprioception.
• Improving posture.
• Increasing tissue tolerance for exercise.
• Improving core strength.
• Enhancing function.
• Providing variety.
• Providing a sense of achievement.
Improvements in proprioception, posture, core strength and general functioning can be achieved by choosing appropriate resistance exercises and persevering with them over a period of time. An emphasis on performing compound free-standing exercises with good technique would fulfil this purpose. If the client is allowed to progress gradually with these exercises, their tissue tolerance for resistance-based exercise can also increase steadily; this would allow for an increase in levels of load later in the training cycle.
To add variety the beginner level training programme can also incorporate some isolation exercises and fixed path resistance machines. The inclusion of these exercises can help the client to feel a sense of achievement at the end of a workout. This is thought to help a beginner’s confidence in their performance, as these exercises require little technical competence or coordination.
TRAINER TIP When working with beginners choose:• Compound, multi-
joint, free-standing exercises.
• Muscular endurance repetition (12 or more reps).
• Low resistance levels.
254 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

Resistance training programme variablesWhen the time comes to progress a resistance training programme, there is a wide variety of variables that can be manipulated to provide a different exercise stimulus and meet different goals. These include:
• Number of exercises.
• Number of sets.
• Target repetition range (strength, hypertrophy or endurance).
• Recovery periods between sets.
• Workout frequency.
• Movement speed – slow to fast.
• Different exercises.
• Stable to unstable positions.
• Simple to complex.
• Split routines.
Changing the stimulus
The body has a tremendous ability to adapt to an exercise stimulus, so you need to plan ahead to ensure that the programme changes progressively on a relatively regular basis. The variables for generating new exercise stimuli for the client can be modified approximately every four to eight weeks. If planned correctly, this practice should encourage physical progress and minimise the risk of retention problems through boredom. Care should be taken to ensure that the progressions in volume and intensity between programmes are both progressive and manageable, e.g. conducting a strength endurance phase between endurance and hypertrophy phases.
Basic resistance progression
It is important to develop a long-term training plan if the client is to progress physically over a sustained period of time.
The basic progression pyramid is useful for coaching a novice client to advanced and intensive forms of resistance training.
NB: The basic pyramid approach to resistance training progression over time would only apply if the client’s training objectives involved strength or hypertrophy.
Many clients do not want to focus on these aspects of muscular fitness, in which case the pyramid approach may not be applicable. If this is the case then the fitness professional has various options, for example:
• As an initial option, if a client wanted to focus on muscular endurance the guideline of 12 or more repetitions per set could be subdivided into smaller repetition ranges. Successive training phases might progress from 18-20, 15-18 and 12-15 reps per set. This would provide small increments in intensity but keep within the muscular endurance repetition range.
REMEMBERThe objective of the client might not suit their current level of physical readiness.
Pre-screening is essential for assessing their suitability for performing certain types of resistance training.
Copyright © 2014 Active IQ Ltd. Not for resale | 255
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

• A second option would be to keep a constant repetition range and amend other programme variables. Increasing the movement complexity from phase to phase, while working with the endurance repetition range, is one of many possible options.
• A further option could be for the client to increase the exercise intensity (i.e. move up the pyramid from endurance to hypertrophy) without significantly increasing the volume of exercise performed.
NB: Genuine hypertrophy training requires a significant increase in training volume, so increasing the intensity without additional volume would provide a variety of stimuli without leading to significant muscle growth.
Figure 3.1 Resistance progression pyramid
STRENGTH
HYPERTROPHY
ENDURANCE
ACTI
VIT
Y Use your notebook to devise a sequence of progression in exercise complexity using these fixed path machines.
Fixed resistance machine
Complexity progression
1 2 3 4
Chest press
Seated row machine
Leg press
ACTI
VIT
Y Use your notebook to design a progressed programme for the novice client for whom you planned a starter programme.
The client has followed the planned workout for eight weeks and made good progress. Her personal technique is strong and she has expressed an interest in including more free weight exercises. Your new programme should provide the client with a new challenge but continue to meet the beginner’s programme objectives.
The workout should be significantly different so that your client feels she is getting value for money. It should also be a logical progression in terms of intensity, volume and technical difficulty. The main session should last 40-45 minutes.
256 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

Hypertrophy trainingHypertrophy training requires a long-term strategy in order to ensure progression over time. The first priority is to ensure that the client is sufficiently physically prepared. This can be achieved by assessing their training experience thoroughly, then selecting a suitable starting level and working gradually up the basic progression pyramid.
The initial increase in volume and intensity from an endurance-based programme can prove demanding to novices of hypertrophy training. Rather than going straight from endurance to pure hypertrophy training, a bridging training phase (strength and endurance) can be scheduled to acclimatise clients to the rigours of hypertrophy training using the basic principles of progression.
BRIDGING BETWEEN ENDURANCE AND HYPERTROPHY TRAINING
Variables Guideline
Intensity Moderate
Load as % of 1RM 67-85%
Rep range 6-12
Rest between sets 1-2 minutes
Sets per exercise 2-4
Frequency per muscle 1-2 times per week
NB: The overall volume per muscle should only be moderate; there should be an inversely proportional relationship between selected exercises and sets per exercise. For example, if three exercises are selected for an individual muscle group, it would be advisable to perform no more than one to two sets per exercise when training for strength endurance.
Table 3.9 Guidelines for strength endurance
Hypertrophy guidelines
As a client moves from muscular endurance to hypertrophy training, the programme changes significantly. When training for muscular endurance, the general guideline is to perform whole-body routines built around compound exercises. It is not uncommon to repeat the same workout two to three times per week.
When training for hypertrophy the number of sets performed per muscle group is far greater than that of muscular endurance training. Incorporating multiple exercises (i.e. three or more per muscle group) is the most effective approach. Training intensity (% of 1RM) is significantly higher. A key feature of hypertrophy training is high volume combined with moderate to high exercise intensities.
CHARACTERISTIC ENDURANCE HYPERTROPHY
Intensity Low Moderate
Load as % of 1RM <67% 67-85%
Suggested rep range 12+ 6-12
Rest between sets 30-60 seconds 1-2 minutes
Sets per exercise 2-3 3-6
Frequency per muscle 2-3 times per week 1-2 times per week
Workout type Whole body Split routine
Table 3.10 Comparison between endurance and hypertrophy guidelines
TRAINER TIP When training for hypertrophy the number of sets performed per muscle group is far greater than that of muscular endurance training.
Copyright © 2014 Active IQ Ltd. Not for resale | 257
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Split routines
When there is insufficient time available for the volume of work required to achieve the desired objective (e.g. progressing whole-body endurance training routines towards hypertrophy) a split routine can be used. The vast majority of clients do not have the time or the physical resilience to train for hours on end, so the split routine offers an alternative approach.
The split routine is a system used by bodybuilders, strength athletes and recreational trainers. Split routines entail moving away from the whole-body approach and focussing separately on two or more groups of muscles. These groups of muscles can then be trained on different days, in a cyclical fashion.
OPTION A – THE TWO-WAY SPLIT
Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Lower body Upper body Lower body
OPTION B – THE TWO-WAY SPLIT (INCREASED FREQUENCY)
Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Lower body Upper body Lower body Upper body
OPTION C(I) – THE THREE-WAY SPLIT
Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Back and biceps
Legs and deltoids
Chest and triceps
OPTION C(II) – THE THREE-WAY SPLIT
Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Chest and biceps
Legs and deltoids
Back and triceps
Table 3.11 Examples of hypertrophy training splits
Cool-down and flexibility exercises
PULSE-LOWERING EXERCISES – CARDIOVASCULAR MACHINES
The intensity should be reduced gradually from cardiovascular training level, to lower the heart rate. The duration of pulse-lowering would depend on the intensity of the workout and the fitness of the client.
Deconditioned clients tend to need longer to cool down than experienced athletes, even though they work at lower intensities.
CARDIO-FLUSH – RESISTANCE TRAINING
It can be useful to perform some low-intensity cardiovascular exercises between resistance training and stretching to help with the removal of waste products and aid muscle recovery by stimulating blood flow (oxygen and nutrients).
STRETCHING EXERCISES
Whole-body approach.Maintenance stretches help to maintain range of motion in all the muscles worked.Developmental stretches help to improve flexibility (as appropriate).
NB: Maintenance and upper body stretches can be performed while using some CV machines, provided the client has sufficient balance, e.g. stretching the chest or triceps while walking or cycling.
Table 3.12 Examples of gym-specific cool-down activities
258 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

Static maintenance
Static maintenance stretches take the muscle to the end of its normal range and hold it there without bouncing; they are short stretches held for 10-15 seconds and used to maintain the normal length of the muscle. The number of stretches should be enough to cover the major muscles of the body worked in the main session.
Static developmental
Static developmental stretches are used to develop flexibility and increase range of movement (ROM) at a joint.
TEACHING GUIDELINES FOR DEVELOPMENTAL STRETCHING
• Take the stretch to the point of bind (mild tension), maintaining good alignment and posture.
• Hold for 10-15 seconds until the tension within the muscle has reduced.
• Relax and passively increase the ROM of the stretch until tension is felt again.
• Hold for 10-15 seconds until the tension within the muscle has reduced.
• Increase the ROM of the stretch until tension is felt again.
• Hold until the tension reduces, then slowly return the limb to its normal position.
• Repeat the stretch if desired.
Planning gym-based exercise using circuit formatsCircuit formats can be used for both one-to-one and group training.
Exercise and equipment
The exercises used as part of the main circuit can include:
• Cardiovascular machines (e.g. treadmill or rowing machine).
• Fixed resistance machines.
• Free weight exercises (barbells and dumbbells).
• Exercises using stability equipment (bosu balls and stability balls).
• Body weight exercises (muscular and cardiovascular).
• Manual resistance exercises.
• Exercises with small equipment, e.g. resistance bands, body bars, cones, fast feet ladders, steps, benches, hurdles, skipping ropes, medicine balls and kettlebells.
Design variables
Circuit formats move from one exercise to another in a sequence. There are many ways of varying circuits according to training goals.
Copyright © 2014 Active IQ Ltd. Not for resale | 259
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Variables include:
• Number of exercise stations in each circuit.
• Exercises chosen for each station.
• Work time for each station (number of seconds or repetitions).
• Rest between stations (this could be active rest, e.g. a cardiovascular exercise between resistance exercises, such as marching, jogging or lunging).
• Rest time between circuits (this could be active rest, e.g. an allocated time for cardiovascular training between circuits, if more than one circuit is used).
• Number of circuits (which would depend on the number of exercises in one circuit).
NB: When using multiple circuits the work time on each station can be varied to change the intensity, e.g. circuit one: 30 seconds; circuit two: 45 seconds; and circuit three: 30 seconds.
• Training focus: strength, endurance, aerobic, stability or any combination.
Fitness levels
Circuits can be easily adapted to accommodate different fitness levels and specialist groups (e.g. older adults) by modifying key variables.
• Beginners can work with low volumes of exercise (fewer exercises and circuits with shorter work times).
• Advanced exercisers can work with high volumes of exercise (more exercises and circuits with longer work times).
There are different ways in which you can design a circuit with a focus on endurance and cardiovascular fitness.
EXAMPLE CIRCUIT 1: MUSCULAR ENDURANCE AND CARDIOVASCULAR FOCUS
Work station 1 2 3 4 5 6 7 8
Exercise12-15 repetitions
Leg press Chest press
Squat Lat pull-down
Lunge Abdominal curl
Shoulder press
Back raise
Complete exercises 1-8 sequentially. You can use a CV machine for a set timeframe at the end of the circuit (e.g. 5-10 minutes).You can repeat the circuit and CV machine session. NB: Repetitions, resistance and chosen exercises can be varied.
EXAMPLE CIRCUIT 2: MUSCULAR ENDURANCE AND CARDIOVASCULAR FOCUS
Work station 1 2 3 4 5 6 7 8
Exercise12-16 repetitions
Leg press Chest press
Lat pull-down
Abdominal curl
Shoulder press
Back raise Leg curl Oblique twists
Body weight CV exercise (Active rest)1 minute
March on the spot
Step-ups Jog on the spot
Squat Multi-directional
lunge
Squat and chest
press action
Lunge and bicep
curl
Jumping jacks
For individuals:Complete exercise 1 and CV exercise (active rest); move to exercise 2 and CV exercise (active rest) and then continue until all exercises are completed.For groups: • Different people can work on different exercise stations.• Body weight exercises can be performed as a group activity if there is enough space available.NB: You can also repeat the circuit and vary repetitions, rest times and exercises.
Table 3.13 Examples of circuits with a focus on endurance and cardiovascular fitness
260 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

Work-to-rest ratio The work-to-rest ratio can be adapted to achieve specific aims of the workout and accommodate different levels of fitness.
Work (time and resistance)
The work time on each station is determined by the:
• Fitness goal and resistance being lifted (strength or endurance).
• Fitness level of the individual.
Work time can vary between 20 and 60 seconds with a timed circuit approach or a specific number of repetitions according to the training goal. As resistance increases, the number of repetitions decreases, which shortens the work duration.
Rest and recovery time
The recovery period or rest time between work stations depends on the intensity of the exercise performed at the station. As a general guideline suggested recovery periods are:
• 0-10 seconds’ recovery for general and cardiovascular conditioning.
• 20-60 seconds’ recovery for older or deconditioned participants.
• 60-120 seconds’ recovery for strength and power approaches.
A higher overall intensity will involve shorter recovery periods. A lower overall intensity will involve longer recovery periods (except with strength or power approaches that require long rests to enable adequate recovery).
Recovery periods can be manipulated to achieve specific workout objectives. The use of active rests (e.g. performing a cardiovascular exercise between muscular exercises) is a way of resting a specific body area, while maintaining the intensity and flow of the circuit. This is effective for aerobic endurance training goals.
WORK-TO-REST RATIOS FOR GROUP CIRCUIT TRAINING
Work time Rest time Work-to-rest ratio Class emphasis
60 seconds No recovery but can use active rests
1:0 Aerobic endurance(advanced)
60 seconds 10-30 seconds 2:1 Aerobic endurance(beginners)
60 seconds 60-120 seconds 1:1/1:2 Muscular strength
45 seconds 15 seconds 3:1 Aerobic and muscular endurance (intermediate)
30 seconds 30 seconds 1:1 Aerobic and muscular endurance (beginners)
Table 3.14 Work-to-rest ratios for different training goals
Copyright © 2014 Active IQ Ltd. Not for resale | 261
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

Exercise sequence and orderWhen designing circuit sessions for beginners or a mixed group, the general rule is to alternate exercises to avoid overworking one area of the body or muscle group, e.g. moving from lunges to abdominal curls rather than lunges to step-ups. This prevents unnecessary muscle fatigue. The sequence of exercises between the last and the first station must also be considered.
If the group is advanced, the aim of the session may be to focus on a particular area of the body or certain muscle groups. Exercises for the same prime movers can be used consecutively to provide challenge and overload.
EXAMPLE CIRCUIT 3: MUSCULAR FITNESS (MULTIPLE EXERCISES FOR SAME MUSCLE GROUP)
Work station 1 2 3 4 5
Muscle focus Back Abdominals Legs Chest Shoulders and arms
Exercise 1 Lat pull-down Curl-ups Squats Chest press Shoulder press
Exercise 2 Seated row Reverse curls Leg press Bent-arm pull over
Bicep curl
Exercise 3 Bent-over row Oblique curls Lunges Chest flyes Tricep dips
Exercise 4 Back extensions Plank Leg curl Press-ups Dumbbell shoulder press
Complete all exercises for station 1, then station 2 and then 3-5.Repetitions, resistance and exercises can be varied.Option of using a CV machine for a set timeframe at the end of the complete circuit (e.g. 5-10 minutes).If working in groups, four people can work at each station performing a mini-circuit within a circuit.
Table 3.15 Example of a muscular fitness circuit focussed on one muscle group
Warm-up and cool-down for group circuit approachesAdequate warm-up and cool-down times must be planned for the start and end of the group circuit.
Warm-up
The warm-up should last approximately ten minutes (depending on fitness levels) and include mobility, pulse-raising and warming movements and stretching.
Exercises that prepare the body include:
• Walking with mobility and range-of-motion exercises, e.g. shoulder lifts and rolls, chest press arm action, shoulder press action, lat pull-down action or bicep curls.
• Body weight exercises, e.g. squats, knee lifts, leg curls or lunges (multi-directional with arm movement variations).
• Larger range-of-motion dynamic stretching.
• Marching or jogging on the spot or around an established exercise perimeter (with a clearly marked route and no trip hazards).
• Brisk walking and jogging combinations, e.g. wide and cross-over strides; short and long strides or heavy and light feet.
• Brisk walking or jogging with arm variations, e.g. waist-to-shoulder-height alternate arm movements (e.g. hammer curls, lateral raises and uppercuts) or shoulder-to-overhead movements (alternate punches, e.g. straight up in the air, punches out to the side and rotational uppercut).
• Brisk walking and jogging combinations of strides and arm movements, e.g. wide strides with lat raises; cross-over strides with uppercuts and short strides with overhead punches.
262 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

Cool-down
The cool-down should consist of approximately three to five minutes of continuous rhythmic movements of light to moderate intensity, similar to some of those used in the warm-up. The intensity should decrease steadily to aid the return of blood to the heart and bring the body back to a steady state. Maintenance and developmental stretches must also be included.
Ideas for cool-down exercises:
• Brisk walking with arm variations.
• Multi-directional lunges with and without arm movements and slow lunge walking.
• Body weight squats with and without arm movement variations, e.g. anterior arm reaches, overhead posterior arm reaches, overhead sideways reaches (both sides) and arms-together rotational reaches at shoulder height (both sides).
• Slow walking (with some upper body maintenance stretches, e.g. triceps and chest).
• Static stretches of all the muscle groups that have been worked during the conditioning phase.
Benefits and challenges of group training Small group circuit classes are becoming increasingly popular in gyms. Examples include:
• 10-15 minute ‘fast classes,’ abdominal classes or ‘mini’ circuits. These can take place at scheduled times or spontaneously and are generally free of charge.
• Small group training; usually delivered as courses or programmes for an additional fee.
Group sessions provide an excellent opportunity for developing rapport with clients, which can boost gym membership and client retention.
Benefits of group training
• Sociable.• Motivational with encouragement that helps exercise adherence.• Varied, which provides a sense of achievement.• Broadly accessible with exercise options that can cater for
different levels of ability.• More affordable than personal training.
FOR CLIENTS GROUP TRAINING IS:
• Relatively easy to plan and less physically demanding to teach than some other forms of group exercise (e.g. indoor cycling).
• An additional source of income.• Time-efficient when working with multiple
clients.
FOR INSTRUCTORS GROUP TRAINING IS:
Potential disadvantages of group training
Group training also has some drawbacks. These may be:
• Difficulties monitoring an entire group’s exercise intensity effectively.
• Lack of one-to-one instruction.
• Difficulties observing large groups adequately.
• Difficulties realising all clients’ session objectives.
• Possibility of competition between participants, which can result in poor technique or intimidation.
Copyright © 2014 Active IQ Ltd. Not for resale | 263
Section 3: Understanding how to plan gym-based exercisePLA
nn
Ing
gyM
-BASEd
ExERC
ISE

End of section: Learning check Answer the questions and make notes to revise this section.
• What would you need to consider when planning a gym-based programme for a beginner?
• What would you need to consider when planning a gym-based programme for an advanced exerciser?
• Why is it important to agree goals with clients?
• Which exercises could be used to develop cardiovascular fitness?
• Which exercises could be used to develop muscular fitness?
• Which exercises could be used to develop flexibility?
• Which exercises would improve specific motor skills, e.g. balance and coordination?
• Name three cardiovascular machines and explain how they can be used in a gym-based session.
• Name five resistance machine exercises and explain how they can be used in a gym-based session.
• Name five free weight exercises and explain how they can be used in a gym-based session.
• Name three body weight exercises and explain how they can be used in a gym-based session.
• How would you structure a gym-based programme?
• What would you consider when planning a gym-based programme using a circuit format?
Group planning considerations
When working with groups and delivering gym-based sessions, certain issues need to be considered:
• Client safety (pre-screening checks) and environmental risk assessment.
• Maximum possible class size for the equipment and space available.
• Choice and availability of equipment and therefore the number of people who can work on one exercise station.
• Floor space available for body weight exercises, including the warm-up and cool-down.
• Work and rest time required according to client fitness levels; choose a short work time and a long rest time for relatively unfit groups.
• Alternative exercise options at each station, for accommodating different needs among mixed-ability groups.
• Timing of the circuit, which can be controlled using a stopwatch (without clock-watching).
• Mat space available for floor-based exercises.
• Ensuring equipment and machines are kept separate from other activities during the circuit; you must be respectful of other gym users and not encroach on them.
• Required leading and teaching skills; teaching a group requires particular observational skills and changes of teaching position to check and correct clients’ technique.
264 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Understanding how to plan gym-based exercise

AimInstructional skills form the cornerstone of a gym instructor’s professional practice. Even the most knowledgeable fitness professional will struggle to provide the best service to gym members if they lack the skills to effectively instruct clients. This unit covers the skills and knowledge needed to instruct and supervise gym-based exercise.
Learning outcomesAt the end of this unit you will:
• Be able to prepare yourself and equipment for gym-based exercise.
• Be able to prepare clients for gym-based exercise.
• Understand how to provide gym-based exercise.
• Be able to provide gym-based exercise.
• Be able to instruct and supervise clients undertaking gym-based exercise.
• Be able to support clients taking part in gym-based exercise.
• Be able to bring a gym-based exercise session to an end.
• Be able to reflect on providing gym-based exercise.
INSTRUCTING GYM-BASED EXERCISE

IntroductionThe role of the gym instructor is to apply their knowledge of anatomy and physiology and the principles of exercise to plan gym-based programmes. An understanding of health, safety and welfare, and knowledge of supporting clients should then be implemented when instructing exercise.
The instructing cycle
Plan a session in accordance with identified needs and information
gathered.
Prepare self, environment and resources.
Welcome client and pre-screen.Deliver the warm up.
Instruct and supervise the session.Observe, correct and improve
technique.
End the session (cool down), gain feedback and tidy the environment.
Reflect on the session and update plans for future sessions.
266 | Copyright © 2014 Active IQ Ltd. Not for resale

Section 1: Preparing for gym-based exercise
It is essential that an instructor prepares themselves, the equipment and the environment before the client arrives for a gym-based session. The purpose of the session will guide how the instructor prepares. The purpose may be to:
• Induct the use of equipment (one-to-one or small group).
• Provide a starter programme for the client (one-to-one or small group).
• Update and review a programme (one-to-one or small group).
These activities are often combined, i.e. a first session with a client who is new to using the gym may involve both an induction and starter programme. A programme review with a client may involve inducting them to new equipment or exercises. The preparation will be similar whether working on a one-to-one basis or with a small group.
ACTI
VIT
Y Use your notebook to make a list of the things you may need to consider when preparing the environment and equipment to deliver a session to a client and how you would prepare yourself to supervise a client.
Preparing oneself, the environment and equipmentIt is essential that the instructor:
• Prepares themselves to supervise gym-based exercise.
• Selects and prepares equipment appropriate to client needs.
• Prepares the environment.
Self-preparation
Self-preparation includes ensuring any personal issues or distractions are put to one side, so that the client(s) can be given full attention during the session. It would include reviewing the client notes and information and being ready to check the information with them (e.g. changes in health or anything they would like to change from a previous programme).
It would also include having programme cards available, so they can be checked (i.e. which exercises are planned and what equipment is needed) and updated to ensure appropriate records are maintained.
Wearing appropriate dress and attire is also part of self-preparation, e.g. wearing a clean and tidy uniform, trainers and name badge, having long hair tied back and removing jewellery. This will help promote a positive image of the instructor and the organisation.
KEY POINTThe exercises and the equipment will have been planned in advance during the programme design stages. These need to be appropriate to meet the client’s objectives and their requirements and capabilities (e.g. health, current fitness and skill level, lifestyle).
Copyright © 2014 Active IQ Ltd. Not for resale | 267
Section 1: Preparing for gym-based exercise In
STRU
CTIn
g g
yM-B
ASEd
ExERC
ISE

Preparing the environment
Preparing the exercise environment includes checking the space available for all activities (including warm-up and cool-down), checking the number of other users (this may affect availability of equipment and may also influence client confidence; some clients feel more self-conscious when the gym is busy), and checking the temperature (e.g. it may be necessary to adapt activities if the environment is very hot or cold).
It would also include checking the name of the duty first aider, knowing the nearest emergency telephone and contact number, the location of the nearest first aid kit and emergency exits.
Preparing equipment
Preparing the equipment includes making sure all the equipment required to deliver the session is available. It also involves checking that the equipment is maintained and safe for use, e.g. are mats clean, are weight pins available, are cardiovascular machines switched on and operational?
Suitable alternatives need to be prepared in case another client is using the equipment at the time it is needed or if the equipment is not working.
Once all these elements are in place the instructor will be able to focus more on the client and their needs during the exercise session. Being prepared in advance prevents having to search for client programme cards at the last minute and reduces the likelihood of having to make unanticipated changes to the programme or equipment.
Preparing the client for gym-based exerciseOnce the instructor has prepared themselves, the equipment and the environment, they are ready to greet the client and prepare them for the session, this will include:
• Helping the clients to feel welcome and at ease.
• Explaining the purpose and value of the exercises, including the warm-up and cool-down.
• Describing the exercises, including their physical and technical demands.
• Confirming or revising plans with clients as appropriate.
• Advising clients of the facility’s emergency procedures.
• Using warm-up activities that are safe and effective for the clients.
Welcoming the client
On arrival the client should be welcomed and made to feel at ease. The instructor should be friendly and ask the client how they are and be interested to hear the response. Being friendly, approachable and willing to listen, helps to build a rapport and relationship with the client, which can contribute to their attendance and adherence.
Early dialogue can also help the instructor gauge the client’s state of readiness and motivation both mentally and physically. The client may express enthusiasm and excitement at the prospect of the gym session, or may indicate that work
268 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Preparing for gym-based exercise

or family life has thrown up barriers and distractions over the last week. These points must be taken into account when considering the physical demands that the planned session will put on the client and, if necessary, adjustments should be made.
During the pre-session conversation with the client, the instructor can also verbally screen to check any changes to health that may need to be considered, e.g. if the client is unwell (cold or fever) they may need to delay exercising until they feel better.
New clients will need to be informed about the facility’s emergency procedures, including the location of fire exits, the nearest first aid box, personnel trained to deliver first aid in the facility, and where the nearest phone is located. This is to ensure they know how to respond during an emergency or if they witness an accident.
Explaining the purpose and value of the exercisesAn outline of the session structure and content, including the purpose and value of the exercises, should be provided and briefly explained to the client, along with any physical and technical demands. This helps to develop the client’s understanding and can be used to confirm they are happy to continue or to revise plans as required.
If the client is feeling tired or stressed, alternatives and modifications can be suggested and discussed. If the client says they found the exercises in a previous session too easy or too difficult then these can also be revised.
Discussing the programme in a collaborative way shares the responsibility for exercise selection and design and gives the client equal and shared power, which can build their autonomy. Being informed about the purpose and value of activities and having choice or being an equal partner in the selection of activities can help to promote long-term adherence. Knowing the importance of the warm-up and cool-down will also ensure the client respects the value of each component and reduces the likelihood of them missing certain activities (e.g. missing end-of-session stretches if time is limited).
The warm-upIt is imperative that a client fully understands the importance of taking adequate time to warm up before beginning the main session. A proper warm-up will bring about many physiological benefits that not only reduce the chance of injury during a session, but more importantly lead to better performance in the main workout. This will help maximise the performance from the client and lead to improved results over time. If the client understands the necessity of these components they are more likely to include them in the future.
Safe and effective activities for a warm-up include gradual and progressive pulse raising and body warming activities (usually using a cardiovascular machine) with some range of motion activities including mobility exercises and stretches (dynamic and static, as appropriate).
The exercises planned for the warm-up will be selected in advance (after the client consultation). The activities should reflect the client’s needs and capability (skill and fitness level) and prepare them effectively for the session to follow.
During the warm-up the instructor should use appropriate instructional skills to monitor the client’s performance, e.g. observation and questions. If the client says they are finding an exercise too hard or too easy, or if the instructor notices they are struggling (e.g. in a change of posture), then it is important to regress or progress the activities to accommodate the client to match their current ability and skill level.
Copyright © 2014 Active IQ Ltd. Not for resale | 269
Section 1: Preparing for gym-based exercise In
STRU
CTIn
g g
yM-B
ASEd
ExERC
ISE

For example, if a client is unable to perform some of the more complex dynamic flexibility exercises (e.g. a lunge with a rotation) then less complex dynamic exercises (e.g. isolating different movements or changing movement) or static stretches may be more appropriate.
Table 1.1 Preparing for gym-based exercise
• Wear correct clothing and footwear (uniform and name badge).
• Review client records and information.
• Have resources available, e.g. programme card, rating of received exertion scale to monitor intensity.
• Prepare to focus on the client.
SELF ENVIRONMENT EQUIPMENT CLIENT
• Space available for warm-up and cool-down activities.
• Number of other gym users.
• Availability of water. • Location of emergency
exits and emergency telephone.
• First aider on duty. • First aid.
• Which machines are needed and when are they needed?
• Alternatives if machines are being used.
• Clean and maintained mats and machines.
• Correct weights available.
• Weight stack pins.
• Provide welcome. • Wear correct clothing
and footwear (no jewellery).
• Check timing of last meal (over two hours).
• Health changes (verbal screening check).
• Feedback from previous meeting.
• Warm up appropriately.
End of section: Learning check Answer the following questions and make notes to revise this section.
• Why is it important to prepare the environment and equipment before working with a client?
• How would you prepare yourself to supervise gym-based exercise?
• How would you check the exercise environment?
• How would you check the exercise equipment?
• Write a list of the equipment you may need to deliver a gym-based exercise session.
• Why is it important to meet and greet the client in a friendly and approachable manner?
• What type of activities (with examples) could you use for a warm-up?
• How would you decide the appropriateness of exercises to use in the warm-up for a specific client?
270 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 1: Preparing for gym-based exercise

Section 2: Instructing and supervising gym-based exercise and supporting clients
To instruct and supervise gym-based exercise safely and effectively it is important that the fitness instructor is able to:
• Identify safe and effective exercise alignment.
• Identify different methods of adapting exercises.
• Build exercises gradually to develop client coordination.
• Manage one-to-one and group inductions.
• Give technically correct explanations and demonstrations.
• Communicate appropriately to meet the client’s needs and the environment.
• Use appropriate teaching positions to observe clients.
• Monitor the safety and intensity of exercise.
• Provide clear and motivational feedback and instructing points.
• Adapt exercises to meet client needs.
• Present a positive image.
• Develop an effective working relationship with clients.
• Communicate with clients in a way that makes them feel valued.
• Use motivational styles appropriate to the client and the exercise format.
Copyright © 2014 Active IQ Ltd. Not for resale | 271
Section 2: Instructing and supervising gym-based exercise and supporting clientsIn
STRU
CTIn
g g
yM-B
ASEd
ExERC
ISE

Instructing and supervising gym-based exercise Instruction and supervision are essential for safe and effective gym-based exercise. They are needed for equipment inductions and when leading clients through a programme of exercises (e.g. early programmes and programme reviews).
• Instructing means giving direction and teaching.
• Supervising means watching and directing the performance of a task.
• Instruction and supervision may include any or all of the following:
• Showing someone how to use a piece of equipment or how to perform an exercise (giving a demonstration).
• Explaining how to use a piece of equipment or how to perform an exercise (giving instructions and teaching points).
• Watching the person use a piece of equipment or perform an exercise and guiding their performance (providing reinforcement of information, positive encouragement and feedback, and offering modifications or progressions).
Effective instructional and supervision skills allow instructors to maximise the safety and effectiveness of a training session. The success of instruction and supervision is dependent on the instructor’s ability to communicate and interact with their client, which is a two-way process.
• The instructor needs to provide clear information to the client.
• The client needs to receive the information correctly.
Effective communication is influenced by various verbal and visual skills. These include:
• The instructor’s vocabulary of verbal instructions, imagery, tone of voice, voice volume, accent, hand signals/gestures, facial expressions, posture, eye contact, and their own exercise technique and alignment.
• The client’s ability to understand and interpret what is being said by watching, listening, asking questions and integrating the information to inform their own performance.
Effective communication comes through practice and experience. An essential part of the process is to check what the client has understood and whether anything is unclear. Some guidelines for assisting communication and instruction are discussed next.
wATCHTELLSHow
272 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Instructing and supervising gym-based exercise and supporting clients

KEY INSTRUCTIONAL SKILLS
VERBAL INSTRUCTIONS VISUAL INSTRUCTIONS
Instructions – words, language and terminology that tell clients what to do.
Demonstration and alignment.
Motivation, praise and encouragement. Observation.
Teaching points – words, language and terminology that tell clients how to do something correctly.
Body language and posture.
Voice intonation, volume and accent. Teaching position – being able to see the client and be seen by the client.
Correction. Facial expression.
Cueing. Eye contact.
Questions. Gestures.
Adaptation of exercises – regressions or progressions.
Table 2.1 Instructional and communication skills
Verbal instruction
The words an instructor uses can be powerful tools that affect the client’s understanding and motivation.
Exercises should be explained and instructed using simple terminology and language that is accessible to the client. It is helpful if the instructor builds a repertoire of non-technical words to explain exercises. This will keep the instructions precise, user-friendly and easy to understand.
Table 2.2 lists common technique corrections (anatomical references) with some examples of simple terminology that may help to address incorrect alignment. Instructors need to find the words and terms that work for their clients.
ANATOMICAL CORRECTION SIMPLE VERBAL CUE
Reduce excessive kyphosis. ‘Keep your chest lifted.’ or ‘Draw the shoulder blades back and down towards the buttocks.’
Reduce excessive lordosis. ‘Brace your abdominals.’ or ‘Pull the tummy button back towards the spine.’
Prevent external/internal hip rotation and/or valgus or varus knees (knock knees or bow legs).
‘Keep your knees in line with your toes.’
Reduce forward head carriage and hyperextension of the cervical vertebrae.
‘Draw your chin back.’ or ‘Lift the crown of the head towards the ceiling.’
Prevent lateral/medial shoulder rotation during pressing or flyes.
‘Keep your elbows behind your hands.’
Prevent hyperextension of the knee or elbow. ‘Keep the knees unlocked.’ or ‘Keep the elbows unlocked.’
Table 2.2 Example teaching points
Copyright © 2014 Active IQ Ltd. Not for resale | 273
Section 2: Instructing and supervising gym-based exercise and supporting clientsIn
STRU
CTIn
g g
yM-B
ASEd
ExERC
ISE

Verbal motivation
Motivational language should be positive and constructive. It can be used to enforce correct exercise technique or to encourage the completion of an extra repetition or set. Phrases such as ‘excellent knee alignment’, ‘great control’, ‘good work – keep the elbows unlocked’ or ‘two more reps, you can do it’ can all be used to help clients succeed. These terms are far more encouraging than negative phrases, such as ‘don’t lock your knees’, ‘don’t let your chin poke forward’ or ‘poor technique’. Negative terminology and criticism should be avoided, as these are not constructive and can be demotivating and deflating to a client’s confidence.
The tone of voice used to express motivational statements should also match the terms used. Voice tone should be sincere, genuine and upbeat.
Deserved praise should never be withheld; the instructor should look for opportunities to praise and encourage. This does not mean offering praise flippantly for every completed set or exercise, regardless of performance. It means seeing and rewarding genuine effort and improvement. It is satisfying and motivating for a
client to hear how their performance is improving or that a goal has been reached.
Visual motivation
Visual motivation supports verbal motivation. It is an attitude portrayed by the fitness instructor that reflects their confidence, enthusiasm and passion. It is demonstrated through their posture, facial expressions and gestures.
Posture should be open when encouraging and motivating clients. Facial expressions should be warm and encouraging (genuine smiles) and gestures should be supportive (e.g. a thumbs-up, rather than a raise of the eyebrows).
The ability to motivate clients is essential to engage them with exercise and promote longer-term adherence. This is particularly important when dealing with new clients or clients who are outside their comfort zone.
Teaching points
Teaching points verbally reinforce a visual demonstration and explain how to perform an exercise correctly. Their application allows instructors to express, correct and fine-tune clients’ exercise techniques. To use teaching points effectively the fitness professional must be fully aware of correct technique. Teaching points can be logically broken down into two categories:
• Those that set an exercise up – the start position.
• Those that allow for proper execution.
For example, during the ‘set-up’ phase for the squat exercise, teaching points such as ‘stand with feet hip-distance apart’, ‘keep chest lifted’ and ‘look forward’ will allow a strong foundation to be established. During the ‘execution’ phase, teaching points such as ‘heels to the floor’, ‘drive the ground away’ and ‘look forward’ will reinforce what is required for successful movement.
TRAINER TIP
Use positive words and phrases to build motivation, e.g. ‘excellent’, ‘well done’, ‘great job’.
Make sure these statements are sincere!
REFLECTION – WHAT DO YOU THINK?
‘If fitness instructors are to effectively motivate their clients they need to be highly motivated themselves.’
274 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Instructing and supervising gym-based exercise and supporting clients

Teaching points should be concise, but it also pays to get creative and think of other ways of explaining alignment by using analogies. For example, ‘headlights forward’ (using a car’s headlights to refer to the pelvic bones) may help clients visualise and focus on the relevant body part and prevent twisting the pelvis, e.g. during spine rotations.
Teaching points can also be supported by visual gestures, e.g. using the example of ‘headlights forward’ the instructor can place their hands on their own pelvis, with fingers pointing forward to show the direction of the pelvis.
Some things for consideration would be to:
• Ensure teaching points are relevant (e.g. they relate to the exercise being performed and the performance of the client).
• Avoid giving too many teaching points. This may be distracting for the client and may result in confusion, e.g. they may need to focus on one or two key points at a time.
• Prioritise teaching points and give those that are most essential for safe and effective performance.
• Keep teaching points positive and tell the client what to do rather than what not to do, e.g. ‘elbows unlocked’ rather than ‘don’t lock your elbows’.
PRIoRITISEPoSITIVERELEVAnT
ACTI
VIT
Y List some of the key teaching points to promote safe and effective performance of the following exercises.
• Lat pull-down
• Leg extension
• Triceps push-down
• Rowing machine
• Treadmill walking
• Upright cycling
• Bench press
• Barbell curl
• Squat
Copyright © 2014 Active IQ Ltd. Not for resale | 275
Section 2: Instructing and supervising gym-based exercise and supporting clientsIn
STRU
CTIn
g g
yM-B
ASEd
ExERC
ISE

Voice intonation and volume
Voice tone should reflect the exercise being performed and also the client’s needs. For example, training for hypertrophy, strength or power is physically demanding and using words such as ‘explode’ or ‘let’s drive’ would be appropriate, but only if spoken with passion, commitment and at the appropriate volume. If instructing stretches as part of the cool-down, voice tone should be more relaxed.
The level of intonation (and choice of words) may need to be moderated if working with a complete beginner, an older adult or other special population (e.g. pre- and post-natal women, exercise referral clients). Voice tone may need to reflect greater empathy and at the same time offer encouragement.
Adaptations – progressions and regressions
Planned exercises will sometimes need to be modified for clients. It may be necessary to make an exercise easier or harder, or even switch it for a different exercise.
Variables that can be used to adapt and modify exercises include the load, number of repetitions, speed of motion, range of motion, type of equipment (body weight, fixed machine, free weight), and type of exercise (e.g. using a different exercise to work the same muscles).
ACTI
VIT
Y 1. Write a list of some different exercise instructions and teaching points.
2. Practise saying these instructions and teaching points using varied:
• Tone (bored, enthusiastic, tired, energised).
• Speed (slow, fast).
• Volume (whisper, quiet, loud).
3. When might you need to adapt voice intonation and volume?
ACTI
VIT
Y Name an exercise that works the same muscles and so could be given as an alternative to each exercise listed.
State how the new exercise would be a modification of the original. Is it easier or harder? What is different, e.g. range of motion or position?
• Chin-up or pull-up
• Bench press
• Seated pulley row
• Dumbbell shoulder press
• Leg press
• Dumbbell lunge
• Barbell bicep curl
• Total hip – adductor exercise
276 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Instructing and supervising gym-based exercise and supporting clients

Questions
Questions can be an effective way to check understanding. An instructor may ask:
Questions can also be used alongside other methods of monitoring intensity (i.e. the talk test, RPE and observation) to gauge how hard a client is working and their response to exercise.
Visual instruction
Demonstration and teaching position
Instructors must be competent and able to demonstrate exercises with safe and effective technique. A clear and accurate demonstration allows the client the opportunity to see and visually observe how an exercise should be performed.
When demonstrating an exercise it is essential to position the client so they are able to see all the major joints in motion. For example, during the bent-over row exercise the best viewing position would be to the side of the demonstrator. All the major joints, and more importantly the alignment of the lower back, can then be viewed successfully by the client.
Alternatively, the client could be advised to move around to observe other exercises from different angles, e.g. from the front, back and side. For example, during a demonstration of treadmill running, the instructor may request the client to observe posture from the side and then knee alignment (not rolling inwards) from either the front or the back.
When demonstrating an exercise it is advisable to perform three to six repetitions in a slow, controlled manner. You could list the main teaching points before or during the demonstration, e.g. when using resistance and cardiovascular machines the client can observe technique and maintain eye contact. The client should be allowed to ask questions to check their understanding before they try the exercise for themselves.
How does that feel?
Where can you feel this working?
What do you feel?
How hard (or easy) is this?
ACTI
VIT
Y What would be the best position for the client to observe an instructor’s demonstration of the following exercises?
• Shoulder press
• Lat pull-down
• Bench press
• Curl-up or sit-up
• Treadmill
• Rowing machines
• Stepper
• Recumbent cycle
Copyright © 2014 Active IQ Ltd. Not for resale | 277
Section 2: Instructing and supervising gym-based exercise and supporting clientsIn
STRU
CTIn
g g
yM-B
ASEd
ExERC
ISE

Observation and teaching position
When clients are performing exercises it is important for the instructor to be in a position where they can clearly see the client’s alignment. This could mean changing teaching position to observe different exercises.
For example, if a client is performing an exercise on the floor, such as a curl-up or sit-up, it makes sense to kneel down to maintain interaction. Standing up could appear dominating and also make it harder to monitor technique.
It may be necessary to change position during the performance of some exercises. For example, if the client is using the cross trainer it may be useful to check technique from a side view (to ensure correct spine alignment and check elbows and knees are not locking); it may also be useful to check alignment from a front and/or rear view to check the knees are not rolling inwards and to check the shoulders are not hunched towards the ears.
One consideration when changing teaching position is to tell the client what you are doing. To walk off suddenly while they are on the treadmill without explanation might cause them to turn their head to see what is happening and could result in them tripping or slipping.
Body language
Body language is non-verbal, visual communication. It includes posture, gestures, eye contact, facial expressions, spatial positioning and all communication that is not spoken. When communicating with clients it is important for body language to be congruent and match the spoken word; otherwise communication can be misinterpreted. Body language gives clues to the person’s current emotional and mental state. It often reflects the real message and is nearly always the message the other person receives most clearly.
For example, to say ‘well done’ with folded arms, raised eyebrows and a frown would be incongruent. The visual message will be loud and clear even if unspoken.
An instructor’s body language can affect the client’s mood and emotional state, which can influence their motivation and the outcome of a training session. It is important to be mindful and aware of body language and how it affects the relationship and rapport with the client.
Some examples of how body language may influence how communication is perceived include:
• Crossing the arms can create a barrier to effective communication. It can be perceived as reflecting boredom or lack of interest.
• Open arms and hand gestures may be perceived as reflecting openness, integration and a feeling of energy.
• Maintaining eye contact and a neutral facial expression can reflect attention and interest.
TRAINER TIP
When the client is performing an exercise move around to observe and check their technique from different angles.
278 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Instructing and supervising gym-based exercise and supporting clients

Client inductions A large percentage of a gym instructor’s time will be spent inducting gym members to ensure they know how to use gym equipment and perform new exercises.
The instructor should develop a clear process to teach new exercises to a client. The acronym NASTY can be used to help provide a logical sequence of instruction.
Teaching sequence
ACTI
VIT
Y Use your notebook to consider the effects that the following examples of body language may have on communication with a client. You can discuss your answers with a peer or tutor.
• Turning your back to a client.
• Smiling to greet a client.
• Yawning while a client is speaking.
• Sitting back in a chair with your hands behind your head during a consultation with a client.
N
A
S
T
Y
Name the exercise – give its purpose and the major muscles/areas of the body used (naming the muscles may be too much information for some clients).
Adjustments – demonstrate how to make adjustments to the equipment being used (e.g. seat height, weight, speed).
Silent demonstration – allow the client to concentrate on the technique of the exercise without distractions (three to six repetitions should be sufficient). It is advisable to use a light weight that the client can lift comfortably for your demonstration, so that they can then use the same weight for their first attempt at the exercise.
Teaching points – run through the main teaching points and provide a further demonstration of the exercise if required while discussing the main technique points.
Your turn – the client should attempt the exercise while being monitored closely by the instructor.
TRAINER TIPIt’s important to remember that the demonstration is intended to teach the client correct technique and build their confidence to perform the exercise themselves. It isn’t an opportunity to demonstrate your strength; having to drop the weight significantly for the client will undermine their self-efficacy whereas increasing the weight after their first attempt will make them feel successful.
Copyright © 2014 Active IQ Ltd. Not for resale | 279
Section 2: Instructing and supervising gym-based exercise and supporting clientsIn
STRU
CTIn
g g
yM-B
ASEd
ExERC
ISE

Layering information to build coordination
When working with beginners or newcomers to the gym it is important to develop their coordination by building up exercises and movements gradually.
The first consideration is to avoid overloading them with information and introducing too many pieces of equipment and exercises at once, as it may be too much to remember. It can be more effective to split an induction over a series of weeks for some clients. For example, at the first induction instruct them how to warm up, use one or two cardiovascular machines and explain how to cool down and stretch. Then introduce resistance exercises progressively over the following weeks.
Another consideration is the need to break down an activity into stages (more complex and coordinated activities) and combine the movements once each stage has been mastered. Attempting to complete the full exercise straight away might be too difficult for the client, leading to poor technique and risk of injury.
Managing group inductionsGroup inductions can be a time-efficient way of inducting a number of newcomers to use equipment. However, these can be quite challenging for the gym instructor to manage. The main disadvantage of group inductions is there will be less personal client attention than if working with clients on a one-to-one basis.
When inducting exercises to groups it is imperative that the instructor manages the whole group effectively and maintains their attention by manoeuvring them into appropriate viewing positions, so they are all able to view demonstrations and listen to the various teaching points.
Depending on time available and group size it may not be possible for every member to practise every exercise or machine demonstrated, but the instructor should aim to make sure that all clients have participated at some stage during the induction. One solution could be for different individuals to practise specific exercises and for the instructor to reinforce key teaching points and answer questions. At the end of the induction the instructor can offer group practice where they supervise everyone. Another option could be for the instructor to allow group practice and supervision after a set number of exercises, e.g. after CV machines and after resistance machines. The key is for the instructor to be happy that every member of the group knows how to use the equipment and perform the exercises demonstrated.
EXAMPLE 1 Beginners often find it difficult to coordinate the movements needed when using the rowing machine. One way to approach this is to instruct the client to first produce the correct movement/rhythm of the legs and omit the movement of the arms. Once the client is happy, the instructor can ask them to perform the arm movements without using their legs and finally integrate the upper and lower limbs together.
EXAMPLE 2 When teaching a client to lunge for the first time it may not be appropriate to expect them to complete the full exercise with good technique. This can be overcome by initially asking the client to take a long step forward. Once they have found their balance, a simple split squat (commonly referred to as a static lunge) may be performed. The client lowers their body to the end position of the lunge and back up again for several repetitions before returning to the start position. Once the client has developed their balance, strength and coordination during the split squat, they may be ready to precede this movement with a step forward and finish the repetition by stepping back out of the lunge to the start position. It may take several days for a client to coordinate a movement such as the lunge.
280 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Instructing and supervising gym-based exercise and supporting clients

Considerations include:
• The purpose and structure of the induction should be made clear to the group from the outset.
• Safety and the surrounding environment should also be explained. The instructor should emphasise the importance of being aware of other exercisers and the equipment they are using. Clients should also be encouraged to stay close to the group, pay attention to the instructor and refrain from performing exercises or using machines without induction or permission. The emphasis should be on safety.
• The spacing of the equipment and number of clients affects demonstrations and teaching position. It may be necessary to ask individuals to move to see an exercise from different positions.
• Maintaining the attention of all individuals in the group needs to be considered. Asking questions is one way of maintaining attention, e.g. ‘Can you remember the set up points for this exercise?’
• Observation and correction are easier if all clients are practising the same exercise at the same time (rather than different exercises), but there must be enough equipment available. A gym could have six treadmills, but there might be other users to consider. It is also unlikely that there will be six pieces of a specific resistance machine available!
• The number of clients and equipment available will affect practice time on different machines and exercises, if there are limited pieces of some equipment then consideration needs to be given to how clients can practise.
• There will be less time and potentially fewer opportunities to offer personalised activities, corrections and alternatives for all clients. A mini circuit could be planned for the end of the induction to allow practice and enable supervision and correction.
SpottingSpotting is the use of other people, such as a personal trainer or training partner, to assist the execution of an exercise and help protect the lifter from risk of injury. Correct spotting technique is vital to ensure the safety of an individual during a resistance training programme.
The three main functions of a spotter are to help the client:
Earle and Baechle, 2000
One or more spotters are recommended for the following types of free weight exercises:
• Overhead exercises (e.g. shoulder press).
• Exercises with the bar on the back (e.g. back squat, step-up, lunge).
• Exercises with the bar racked on the anterior deltoid or clavicles (e.g. front squat).
• Exercises with the bar over the face (e.g. bench press, flyes, lying triceps extension), deltoid or clavicles (e.g. front squat).
Spotters are not used during power exercises, such as the clean, the snatch and the jerk, because spotting this type of exercise is too dangerous for both lifter and spotter.
GET OUT DIFFICULTY APPLY HIGH-INTENSITY TRAINING METHODS ENSURE CORRECT TECHNIQUES
Copyright © 2014 Active IQ Ltd. Not for resale | 281
Section 2: Instructing and supervising gym-based exercise and supporting clientsIn
STRU
CTIn
g g
yM-B
ASEd
ExERC
ISE

Considerations for safe spotting
• The spotter should be strong enough to assist the client if required.
• Use more than one spotter for some exercises (heavy back squats or heavy bench lifts).
• Spotters should know the correct exercise technique for the exercise they are spotting.
• Spotters should know how many repetitions the client is attempting to lift.
• Spotters should be attentive at all times to the client and their technique.
• When spotting over-the-face barbell exercises, the spotter should hold the bar with an alternated grip, usually inside the client’s grip.
• When spotting over-the-face dumbbell exercises, spot as close to the dumbbells as possible or in a few cases (dumbbell pull-over and lying overhead dumbbell triceps extension) the dumbbell itself. Note that many individuals prefer to be spotted under the elbows during supine dumbbell exercises.
• When spotting overhead/bar on back/bar on front exercises, the spotter should be at least as tall and strong as the lifter and be performing the exercise in a power rack with the correct pin placement.
• Out-of-rack exercises, such as the lunge and step-up, are only recommended for skilled athletes and experienced spotters, as they can result in serious injury.
• Spotters should summon help if an accident or injury occurs.
Fleck and Kraemer, 1997; Earle and Baechle, 2000
Recommendations for the spotter
• Establish a solid base of support to lift and pass the weight (foot stance and position).
• Maintain a neutral spine and use correct technique when lifting and passing.
• Keep the barbell or dumbbell close to your body when lifting and passing.
• Pass the bar or dumbbell to the lifter away from their body/face and move into position together.
• Use four hands on the bar (three hands for dumbbells) to move the weight into position (see following images).
• Ensure good communication with the client; this should be practised and made clear before the exercise is executed.
• Only release the barbell or dumbbell to the lifter when they have given a clear instruction (e.g. ‘mine’, ‘my bar’).
• When passing dumbbells they should be passed one at a time by the ends to allow the client to safely grip the handle.
282 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Instructing and supervising gym-based exercise and supporting clients

Monitoring the safety and intensity of exerciseMonitoring the client’s safe performance of an exercise is a critical part of a gym instructor’s role. It is essential that optimal posture and joint alignment are maintained at all times. If a client is unable to maintain correct alignment or posture, the instructor should stop the exercise and offer a suitable alternative or regression for the exercise.
ACTI
VIT
Y Study the following exercises. Your task is to identify:
1. The aim of the exercise, i.e. muscles working.
2. The potential dangers, i.e. technique and postural misalignment.
3. The type of client the exercise would be most appropriate for, i.e. fitness and skill level.
4. The type of client the exercise would be inappropriate for, i.e. fitness and skill level.
5. Two or more alternative exercises or ways of modifying the following exercise in order to lower the risks and make them safer, while still working the same muscles.
• Biceps curl
• Press-up
• Shoulder press
• Single-arm row
• Dumbbell squat
• Triceps kickback
Monitoring exercise intensity is important to check the client is working at the appropriate level. It can be used to determine whether they need to continue to work at the same level, progress to a higher level or regress to a lower level.
There are several methods of monitoring exercise performance in a gym environment that provide valuable information for judging need or readiness for progress, these are discussed in the ‘Principles of exercise, fitness and health’ unit.
Rating of perceived exertion and heart rate
RPE scores and peak heart rate recorded during exercise allow the instructor to determine whether the desired intensities are being achieved and adjust any of the exercise variables (e.g. strokes per minute, revolutions per minute, kilometres per hour) necessary to raise or lower the intensity to the desired level for the client.
Observation
Observation of client posture, alignment, coordination and technique in conjunction with any strain or effort on the face, sweating and redness can provide reliable indicators of how hard a client is working, especially when the instructor is familiar with how an individual client usually appears at different levels of intensity.
METHODS OF MONITORING INTENSITY
• Rating of perceived exertion (RPE).
• Heart rate.• Observation.• Other performance
markers.
Copyright © 2014 Active IQ Ltd. Not for resale | 283
Section 2: Instructing and supervising gym-based exercise and supporting clientsIn
STRU
CTIn
g g
yM-B
ASEd
ExERC
ISE

End of section: Learning check Answer the following questions and make notes to revise this section.
• Name the component of fitness that could be improved by the following exercises:
• Treadmill, rowing machine and stepper.
• Chest press, leg extension and lat pull-down machine.
• Barbell squat, single-arm row and bent-arm pull over.
• How could you adapt to regress and progress the following exercises?
• Treadmill running at 7.5 kph with no incline.
• Seated pulley row – 2 sets of 15 repetitions, 20kg.
• Dumbbell lunge – 1 set of 15 repetitions, 5kg dumbbells.
• Treadmill running at 10 kph.
• Upright cycling at 55 rpm.
• Lat pull-down – 1 set of 10 repetitions, 25kg.
• Give an example of how you could build an exercise up gradually to develop client coordination.
• List some of the key things you would consider when inducting a group of five clients to use equipment, rather than an individual client.
• State the key teaching points and the teaching position you would use to demonstrate and observe the following exercises:
Rowing machine. Leg press. Bicep curl. Dumbbell lunge. Treadmill walking.
• Why is it important for an instructor to demonstrate exercises with correct technique?
• How could you adapt your communication in a noisy gym environment?
• How would you monitor the safety and intensity of exercise for individual clients?
• Why is it important to provide feedback and instructing points which are timely, clear and motivational?
• Why is it important for an instructor to present a positive image of themselves and their organisation to clients?
• How would you build an effective working relationship with your clients?
• Give an example of how you could communicate with clients to make them feel valued.
• Give an example of how you could motivate a client.
Other performance markers
Other performance markers that can be used to assess and adjust intensity include distance covered, weight or load, number of sets and repetitions or time taken to complete. For example, monitoring the total number of repetitions a client can perform in conjunction with their RPE on the final repetition can gauge whether progression (or regression) is required.
284 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 2: Instructing and supervising gym-based exercise and supporting clients

Section 3: Ending a gym-based session and reflective practice
At the end of the session it is important to allow sufficient time for the client to recover from the main workout by instructing safe and effective cool-down activities. It is also important to gather some feedback from the client to guide the reflective process and improve practice.
To end the session appropriately:
• There should be a safe and effective cool-down component appropriate to the client’s level of fitness and skill level.
• The client should be given the opportunity to reflect on the session and share their views (what they enjoyed most or least and what they found easier or harder). They should also be given the opportunity to ask questions about the session, e.g. the purpose of specific activities and enquire about activities (different machines/equipment) they might like to try in future.
• The instructor should positively summarise the client’s performance and what they have achieved in the session, and check that the client understands how to continue with the programme until their next planned appointment (e.g. a review).
• All equipment should be packed away and/or wiped down after use; this is best practice for gym etiquette (leaving the environment ready for other clients and instructors).
Cool-downThe cool-down component is the recovery component; it returns the body to an appropriate non-exercising state. It includes pulse-lowering activities after any cardiovascular work and stretches to maintain and develop flexibility.
The duration, intensity and type of activities included in the cool-down should be adapted to match the demands of the completed session and also the client’s level of fitness and skill. For example:
• If the session emphasised training the legs then more time will need to be spent stretching the lower body and comparatively less time will be needed to stretch the upper body.
• If the session emphasised training the upper body then more time would need to be devoted to stretching the upper body.
• If the cardiovascular component was the last part of the main workout then sufficient time would need to be allowed to lower the heart rate from training level (to prevent blood pooling and promote venous return), prior to stretching.
• If the session finished on some high-intensity intervals the cool-down may start at a moderate to vigorous level and diminish gradually as the body is slowed to a stop.
• If the session ended with some relatively simple core exercises it may be that the body has already started to cool down and some basic controlled mobility and stretching may suffice.
Copyright © 2014 Active IQ Ltd. Not for resale | 285
Section 3: Ending a gym-based session and reflective practice In
STRU
CTIn
g g
yM-B
ASEd
ExERC
ISE

The cool-down exercises might also be based on a client’s current health requirements. The emphasis should be to personalise the cool-down in line with specific client needs. For example:
• Beginners often need to spend longer cooling down to adequately lower their heart rate. They will also need more time to learn how to perform stretches correctly.
• A pregnant client may need to avoid developmental stretches due to ligament laxity (from the effects of the hormone relaxin). They may require static maintenance stretching applied to muscle groups likely to shorten and tighten during the pre-natal state, such as hip flexors, erector spinae and pectorals.
• An older adult with arthritic knees might find static stretching of the quadriceps too uncomfortable, but could benefit from controlled mobilisation of the knee joint and other joints.
Benefits of the cool-down
The cool-down is beneficial for a variety of reasons:
• To control the client’s return to rest.
• To address client flexibility limitations.
• To enhance mental and physical relaxation.
• To gain feedback about the session.
• To provide the client with feedback on their performance.
• To discuss other lifestyle factors.
• To reinforce teaching points and future goal achievement.
Providing feedback to the clientDuring the cool-down and closing phase it is useful to give some feedback to the client based on their performance during the session. All feedback should be positive, honest and constructive.
Praising and highlighting areas where the client clearly showed willingness, effort and good performance during the session is strongly recommended to help motivate the client and promote adherence to their programme.
Tone of voice, perspective and the words chosen can all affect how feedback is received. The following two examples are used to contrast a negative feedback statement and a positive feedback statement:
TRAINER TIP
Allow adequate time for the cool-down component to make sure it is not rushed.
This demonstrates good practice for the client.
SOMETHING EXTRA
The aim of feedback should be to motivate clients and provide encouragement.
286 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Ending a gym-based session and reflective practice

‘Great to see your effort during that set. Let’s see if you can reach those last three repetitions for the lunges in the next session. If you focus on keeping your chest lifted and your knee tracking in line with your toes, this will improve alignment.’
‘You didn’t manage to get the last three repetitions intended for the last set of the lunge exercise. You lost neutral spine and your knee was buckling inwards towards the last few repetitions.’
NEGATIVE
POSITIVE
Both statements provide feedback that is honest and accurate, but the negatively phrased feedback is more likely to reduce motivation and commitment to achieve. The positively phrased statement acknowledges the effort and sets a target to work towards in the next session. This is more encouraging and reflects the instructor’s confidence in the client’s ability to reach the objective.
Gathering feedback from the client It is also useful to gather some information from the client. This can be used to reflect on the session and make improvements.
The client can be given the opportunity to:
• Reflect on the session overall – what they enjoyed or found hard, what they felt were their strong points and weak points.
• Ask questions, e.g. they might be unsure why they are performing certain exercises or components and may want to clarify.
• Provide feedback – they may have found some of the exercises too difficult or complex and would be unlikely to perform them alone, or they may offer feedback on the type of motivation or instructions used by the instructor.
• Identify further needs – taking part in the exercise may lead the client to identify some additional objectives. They might ask for further assistance from the instructor at a later date to help them remember the programme they have just completed.
Clearing the environmentIt is important that the environment is left in a condition acceptable for future use. The instructor should educate the client on health, safety and cleanliness to ensure that:
Machines, benches and mats are wiped clean after use.
Free weights are tidied away and put in their correct place.
Mats, handles and other accessories are clean and tidied away in their correct place.
Damaged equipment has been reported to the appropriate individual.
TRAINER TIP
It is important that the client understands how to continue their programme of gym-based exercise without direct supervision. If the client is unsure then an appropriate follow-up appointment should be arranged.
Copyright © 2014 Active IQ Ltd. Not for resale | 287
Section 3: Ending a gym-based session and reflective practice In
STRU
CTIn
g g
yM-B
ASEd
ExERC
ISE

Reflective practice It is useful to reflect on the session delivered after it has ended. The instructor can review their own performance and the performance of the client and can reflect on any feedback gathered from the client regarding how they found the session, e.g. the outcomes achieved and how they experienced the session (likes, dislikes, things they found easy, things they found hard, anything they didn’t understand, etc.).
When reflecting and evaluating it is important to consider:
• How well the exercises met client needs, i.e. were they safe, effective and enjoyable, and were modifications made in relation to information provided by the client at the start of the session?
• How effective and motivational was the relationship between the instructor and client, e.g. was the rapport and energy positive and upbeat or was communication with the client challenging and why?
• How well the instructing style matched the client’s needs, e.g. did the client follow instructions correctly and perform exercises safely and effectively? Was the client clear or did they look confused at any point? Did they respond to questions?
It is important to be able to reflect objectively on the session to identify successes (things that worked and why they worked) and to identify areas for development in future sessions (what didn’t work, why it didn’t work and how it could be made better).
The value of reflective practice
The instructor that honestly evaluates their instruction will more effectively iron out inconsistencies in their teaching style and improve their ability to make future sessions more effective, in turn improving their personal practice. An instructor may not recognise their full potential unless they take the time to reflect on their practice accordingly.
TRAINER TIPReflective practice is thinking about the session that has been delivered and evaluating what worked well and what didn’t work so well, and why it worked or didn’t work.
Reflective practice is a step towards developing more effective and inclusive instructional skills and is a way for instructors to improve, develop and continue to grow in their professional role.
288 | Copyright © 2014 Active IQ Ltd. Not for resale
Section 3: Ending a gym-based session and reflective practice

Improving practice
There are many ways of improving practice and continuing professional development in the fitness instructor role, these include:
Work experience and reflecting on work experience.
Working with clients and reflecting on experience of working with clients.
Team meetings with peers to share ideas and knowledge.
Shadowing experienced practitioners (e.g. personal trainers).
Attending workshops.
Reading relevant journals and magazines.
Gaining additional qualifications, e.g. personal trainer, exercise referral.
Attending conferences.
End of section: Learning check Answer the following questions and make notes to revise this section.
• Why is it important to allow sufficient time to end a gym-based session?
• What are safe and effective cool-down activities for a gym-based session?
• Why is it important to give a client feedback at the end of the session?
• What feedback could you gather from a client at the end of a session?
• How would you check that a client understands how to continue their programme without direct supervision?
• What would you need to do to leave the environment in a condition acceptable for future use?
• Why is it important to reflect on the outcomes of working with clients and client feedback?
• Why is it useful to reflect on how well the exercises met client needs?
• Why is it useful to reflect on how effective and motivational the relationship with the client was?
• Why is it useful to reflect on how well the instructing style matched the client’s needs?
• What methods could be used to improve personal practice?
• What is the value of reflective practice?
Copyright © 2014 Active IQ Ltd. Not for resale | 289
Section 3: Ending a gym-based session and reflective practice In
STRU
CTIn
g g
yM-B
ASEd
ExERC
ISE

Appendix 1: Exercise archiveThe exercises presented in this archive are those required for the gym instructor qualification. The list is not exhaustive.
Each exercise description includes the primary muscles worked, some key teaching points (not an exhaustive list) and alternative options.
To successfully complete this qualification there must be evidence that the learner has instructed clients on the following exercises as a minimum:
• Three cardiovascular machines.
• Four resistance machine lifts.
• Four free weight lifts.
• Three body weight exercises.
CARDIOVASCULAR MACHINES
One to be observed during the course and two to be observed at the final assessment.
• Upright cycle.• Recumbent cycle.• Treadmill.• Stepper.
JOINT/MOVEMENT RESISTANCE MACHINE
(One to be observed during the course and three at the final summative assessment)
FREE WEIGHT
(One to be observed during the course and three at the final summative assessment)
BODY WEIGHT
(Two to be observed during the course and one at the final summative assessment)
Shoulder flexion Seated chest press (neutral grip) Front raise (DB)
Shoulder extension Seated row (low pulley) Seated row (neutral grip)
Single-arm rowBent-arm pull over (DB)
Shoulder abduction Shoulder press Shoulder press (DB)Lateral raise (DB)Upright row (BB)
Shoulder adduction Lat pull-down (in front of chest)Assisted pull-up
Chins
Shoulder horizontal flexion Bench pressSeated chest press (BB grip)Pec dec
Bench pressFlyes (DB)
Press-up
Shoulder horizontal extension Seated row (BB grip) Prone flye (DB)
Elbow extension Triceps push-down (high pulley)Tricep press
Supine triceps press (BB)Single-arm triceps press (DB)
Press-up
Elbow flexion Biceps curl (low pulley)Seated bicep curl
Biceps curl (BB) (DB)
Hip extension Leg pressTotal hip
Lunge (BB, DB optional)Dead lift (BB) (DB)
Lunge
Hip adduction Seated adductorTotal hip
Hip abduction Seated abductorTotal hip
Knee extension Seated knee extensionLeg press
LungeDead lift (BB) (DB)Squat (DB) (BB)
LungeSquat
Knee flexion Lying thigh curlSeated thigh curl
Trunk flexion Abdominal machine Abdominal curl
Spinal extension Lower back machine Dead lift (BB) (DB) Back raise
• Rowing machine.• Elliptical trainer.• Cross trainer.
290 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

Cardiovascular machines
TREADMILL
Teaching points
• Maintain position in the centre of the belt.
• Upright posture, abdominals engaged and look forward.
• Comfortable leg stride, using heel-to-toe action.
• Swing the arms. • Knees unlocked.
Muscles worked
• Lower body.
Options
• Treadmill walking. • Treadmill running. • Use of incline.
ROWING MACHINE
Teaching points
• Sit upright, chest lifted, abdominals engaged, knees bent, wrists in line with forearms and overhand grip of bar (pronated).
• Drive movement using the following action: legs extend, arms bend, arms extend, legs bend.
• Keep chain level with middle of body. • Align knees with feet.
Muscles worked
• Whole body.
Options
• Beginners 20-25 SPM.• Intermediate to advanced 25-35 SPM. • Adjust resistance level (1-10).
CROSS TRAINER
Muscles worked
• Whole body.
Teaching points
• Upright posture, abdominals engaged, look forward.
• Feet flat on plates. • Hips, knees and ankles aligned. • Knees and elbows unlocked.
Options
• Use with lower body or upper body movement focus.
• Forward or backward action. • Beginner 50-60 RPM.• Intermediate to advanced 60-80 RPM.• Elliptical trainer uses legs only. • Adjust resistance level to suit level of
fitness (varies on different equipment).
Copyright © 2014 Active IQ Ltd. Not for resale | 291
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

UPRIGHT CYCLE
Muscles worked
• Lower body.
Teaching points
• Stand at the side of the cycle to adjust the seat; it should be level with the hips.
• Put ball of foot on pedal. • Sit upright, abdominals engaged, look
forward. • Pedal while rocking body weight side
to side.• Hips, knees and ankles in line. • Knees unlocked. • Allow the ankle to move during
pedalling action (plantar flexion and dorsiflexion, not flat footed).
Options
• Recumbent cycling to support back (adjust seat so that leg can extend without locking at end of cycling action, back supported on rest).
• Beginners 50-70 RPM.• Intermediate to advanced 70-90 RPM.• Adjust resistance level to suit level of
fitness (varies on different equipment).
STEPPER
Muscles worked
• Lower body.
Teaching points
• Upright posture, chest lifted, abdominals engaged, look forward.
• Push through forefoot to drive step downwards around 6-8 inches on each stride.
• Knees, hips and ankles aligned. • Drive body weight through the legs.
Options
• Vary stride length. • Stair climber machine. • Use a standard aerobics step instead of
a machine. • Adjust speed for different levels of
fitness. • Adjust resistance level to suit level of
fitness (varies on different equipment).
292 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

Body weight exercises
PRESS-UP
Start Teaching points
• Prone position with arms extended and feet in contact with floor.
• Body aligned; head, shoulder, hip, knee and ankle.
• Neutral spine and abdominals engaged. • Bend the elbows to lower chest towards
floor. • Extend elbows to return to start
position. • Elbows unlocked. • Repeat for desired repetitions.
Finish
Muscles worked
• Pectoralis. • Triceps brachii. • Deltoids (anterior).
Options
• Box position with knees under hips.• Three-quarter position on thighs. • Perform against a wall (across gravity).
CHIN-UP – PRONATED GRIP, JUST WIDER THAN SHOULDER WIDTH.
PULL-UP – SUPINATED GRIP, SHOULDER WIDTH.
Start Start Teaching points
• Grip bar using relevant hand position.
• Feet crossed. • Spine neutral, abdominals
braced, arms extended but unlocked, shoulders away from ears.
• Pull body upwards towards bar.
• Lower body under control to start position.
• Repeat for desired repetitions.
Finish Finish
Muscles worked
• Latissimus dorsi and posterior deltoid (shoulder extension).• Middle trapezius and rhomboids (shoulder girdle retraction).• Lower trapezius (shoulder girdle depression).• Biceps brachii (elbow flexion).
Options
• Lat pull-down.• Assisted chin-up or pull-up
machine.
Copyright © 2014 Active IQ Ltd. Not for resale | 293
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

ABDOMINAL CURL-UP OR CRUNCH
Start Teaching points
• Supine lying on the floor, knees bent, feet on floor, fingers at side of ears, low back lightly connected with the floor.
• Engage abdominals and lift shoulders off the floor, bending the trunk, keeping head neutral.
• Lower under control. • Repeat for desired repetitions.
Finish
Muscles worked
• Rectus abdominis.
Options
• Hands on thighs. • Hands across chest.• Hands at side of ears.• Arms extended (beside ears).• Feet raised from floor. • Reverse curl. • Seated crunch machine. • Use rotation to right and left to work
obliques.
BACK EXTENSIONS
Start Teaching points
• Prone lying, with feet on the floor and hands at side of ears.
• Raise the shoulders and chest under control, keeping feet on floor and head in neutral alignment.
• Lower to start position. • Repeat for desired repetitions.
Finish
Muscles worked
• Erector spinae.
Options
• Hands at side of body. • Hands supporting body weight under
shoulders (sphinx position) without pushing off arms to lift.
• Arms extended over head, upper arm at the side of ears.
• Back extension machine.
294 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

Free weight exercises
DEADLIFT (BB)
Start Finish Teaching points
• Feet hip-width apart with toes under bar and bar lightly touching shins.
• Bend at the hips and knees, maintain neutral spine, look forward and keep chest lifted.
• Grasp the bar outside knees with an alternate grip (one hand pronated, one hand supinated).
• Drive through the thighs and buttocks to straighten hips and knees and stand upright, without locking joints.
• Lower under control to return bar.• Repeat for desired repetitions.
Muscles worked
• Quadriceps (knee extension).• Hamstrings (hip extension).• Gluteus maximus (hip extension).• Erector spinae (spine extension – isometric).• Middle trapezius and rhomboids (shoulder girdle retraction –
isometric).
Options
• Alter the hand position to grasp the bar according to the lift to be performed.
• Both hands pronated (e.g. upright row).• Both hands supinated (e.g. bicep curl).• If using dumbbells, place these outside
the feet (e.g. dumbbell lateral raise).• Perform without weights to practise
technique.
BACK SQUAT (BB)
LIFT BAR INTO POSITION FROM A RACK OR USING THE ‘CLEAN’ LIFTING ACTION (DEADLIFT, HIGH PULL, ROLL AND RECEIVE, PUSH PRESS ACTION).
Start Finish Teaching points
• Position bar on fleshy part of the upper back.
• Feet hip-width apart, abdominals braced and neutral spine.
• Initiate squat by bending from hips and knees.
• Lower under control to a comfortable range of motion.
• Knees in line with toes and heels to floor throughout.
• Drive through thighs to lift upwards and breathe out through the sticking point.
• Repeat for desired repetitions.
Muscles worked
• Quadriceps (knee extension).• Hamstrings (hip extension).• Gluteus maximus (hip extension).
Options
• Body weight only. • Dumbbell squat.
Copyright © 2014 Active IQ Ltd. Not for resale | 295
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

FORWARD LUNGE (BB)
LIFT BARBELL INTO POSITION FROM A RACK OR USING THE ‘CLEAN’ LIFTING ACTION (DEADLIFT, HIGH PULL, ROLL AND RECEIVE, PUSH PRESS ACTION).
Start Finish Teaching points
• Position bar on fleshy part of the upper back.
• Feet hip-width apart, abdominals braced and neutral spine.
• Stride one leg forward and lower body down under control into lunge position, with knee at roughly a right angle.
• Heel of back leg lifts to allow the lunge action, trailing leg stays off the floor.
• Knees in line with toes and front heel to floor throughout.
• Push through thighs and drive away from the floor to lift upwards and return to start position.
• Repeat for desired repetitions.
Muscles worked
• Quadriceps (knee extension).• Hamstrings (hip extension).• Gluteus maximus (hip extension).
Options
• Alternate leg lunges. • Same leg lunges. • Body weight only. • Dumbbell lunges.
UPRIGHT ROW (BB)
Start Finish Teaching points
• Deadlift bar to thighs. • Widen foot stance to outside hip-width. • Narrow hand position (two thumb-
widths apart).• Neutral spine and engage abdominals. • Keep bar close to the body. • Elbow lead to raise the bar. • Elbows higher than hands at the top of
the movement.• Lower under control to thighs. • Repeat for desired repetitions.
Muscles worked
• Deltoids (anterior).• Biceps brachii.• Upper trapezius.
Options
• Use dumbbells. • Use resistance bands. • Wide grip – high-pull (preparation to
roll, receive and push press bar over head in position for back squat).
296 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

FRONT RAISE (DB)
Start Finish Teaching points
• Deadlift dumbbells to front of thighs. • Feet wider than hip-width. • Neutral spine, abdominals engaged. • Raise dumbbells to shoulder height in
front of body.• Elbows slightly flexed.• Lower under control. • Repeat for desired repetitions.
Muscles worked
• Deltoids (anterior).
Options
• Alternate arm raises.
SHOULDER PRESS (DB)
POSITION DUMBBELLS USING THE ‘CLEAN’ LIFTING ACTION (DEADLIFT, HIGH PULL, ROLL AND RECEIVE).
Start Finish Teaching points
• Position dumbbells at height of ears.• Feet wider than hip-width apart.• Neutral spine, abdominals engaged. • Press dumbbells to ceiling.• Elbows extended but unlocked. • Knuckles face upwards. • Lower under control. • Repeat for desired repetitions.
Muscles worked
• Deltoids.• Triceps brachii. • Upper trapezius.
Options
• Alternate arm press.• Use a barbell. • Use a resistance band.
LATERAL RAISE (DB)
Start Finish Teaching points
• Deadlift dumbbells to side of thighs (or front).
• Feet wider than hip-width. • Neutral spine, abdominals engaged. • Raise dumbbells to shoulder-height,
rotating them slightly so they are parallel to floor.
• Elbows slightly flexed.• Lower under control. • Repeat for desired repetitions
Muscles worked
• Deltoids (medial).
Options
• Alternate raises. • An alternative exercise for the deltoids
is the shoulder press (also works the triceps).
Copyright © 2014 Active IQ Ltd. Not for resale | 297
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

BICEP CURL (BB)
Start Finish Teaching points
• Deadlift bar to thighs using a supinated grip.
• Foot stance wider than hips.• Bar grip narrowed to shoulder-width,
elbows tucked into side of body. • Neutral spine and engage abdominals. • Curl the bar towards the chest under
control, pause at the top. • Lower the bar under control to the
thighs. • Repeat for the desired repetitions.
Muscles worked
• Biceps brachii.
Options
• Use dumbbells. • Alternate arms. • Perform seated.
PRONE FLYES (DB)
Start Finish Teaching points
• Deadlift dumbbells to side of thighs. • Feet slightly wider than hips. • Maintain neutral spine and engage
abdominals.• Flex forward from the hip, dumbbells
aligned under shoulder, palms face inwards.
• Raise the dumbbells directly to the side until level with shoulders, elbows unlocked.
• Lower under control. • Repeat for desired repetitions.
Muscles worked
• Trapezius (middle).• Rhomboids. • Posterior deltoids.
Options
• Prone lying on floor without weights.
298 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

SINGLE-ARM ROW (DB)
Start Finish Teaching points
• Place the knee and same-side hand on top of a bench with hand under shoulder and knee under hip.
• Place free standing leg level with kneeling leg, forming a tripod shape.
• Bend free standing leg to lower body and pick up dumbbell from the floor using free arm and hold under shoulder.
• Neutral spine, engage abdominals. • Raise the dumbbell towards the armpit
with elbow close to body, but without twisting the body.
• Lower until arm is straight, elbow unlocked.
• Repeat for desired repetitions.
Muscles worked
• Latissimus dorsi.• Posterior deltoid.• Trapezius. • Biceps brachii.
Options
• Perform free standing using a split stance with hand supported on knee.
SINGLE-ARM TRICEP PRESS (DB)
POSITION DUMBBELL USING THE ‘CLEAN’ LIFTING ACTION (DEADLIFT, HIGH PULL, ROLL AND RECEIVE).
Start Finish Teaching points
• Stand with feet wider than hip-width apart.
• Neutral spine, abdominals engaged. • Press dumbbell overhead, elbow
extended but unlocked, and shoulder away from ear.
• Bend the elbow to lower the dumbbell under control to the rear of the head.
• Extend the elbow and press the dumbbell back to the overhead position.
• Repeat for desired repetitions.
Muscles worked
• Triceps brachii.
Options
• Both hands hold dumbbell. • Lying tricep extension. • Tricep kick back (from single-arm row,
tripod position).
Copyright © 2014 Active IQ Ltd. Not for resale | 299
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

BENCH PRESS (BB)
TO POSITION BAR, LIFT FROM A RACK AND/OR USE A SPOTTER TO PASS THE BAR.
Start Finish Teaching points
• Lie on bench with head and upper body supported and feet firmly on the floor.
• Neutral spine and engage abdominals. • Take the bar using a shoulder-width
and a half grip, wrists straight, barbell level with chest.
• Bend the elbows to lower bar under control to just above the chest, elbows slightly behind hands.
• Straighten elbows to return bar to start position, elbows unlocked.
• Repeat for desired repetitions.
Muscles worked
• Pectoralis major. • Anterior deltoids.• Triceps brachii.
Options
• Use dumbbells. • Can be performed using an inclined
bench.• Light barbells can be positioned by
lifting from a seated position and rolling bar along thighs.
BENT-ARM PULL OVER (DB)
TO POSITION THE DUMBBELL EITHER USE A SPOTTER OR, FROM A BENCH SEATED POSITION, LIFT THE DUMBBELL OFF THE FLOOR AND PLACE ON THIGHS, RECLINE THE BODY AND LIFT THE DUMBBELL INTO POSITION USING BOTH HANDS.
Start Finish Teaching points
• Lie on bench with head and upper body supported and feet firmly on the floor.
• Neutral spine and engage abdominals.
• Hold the dumbbell with both hands and position over chest, with elbows bent into side of body and fixed at a 90° angle.
• Keep elbows fixed, move from the shoulder to take the dumbbell over the head until the upper arm is in line with the torso and parallel to the floor.
• Return bringing elbows back into sides of body.
• Repeat for desired number of repetitions.
Muscles worked
• Latissimus dorsi.• Pectorals.
Options
• Use a barbell.
300 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

LYING SUPINE TRICEP EXTENSION (BB)
TO POSITION THE BARBELL EITHER USE A SPOTTER OR, FROM A BENCH SEATED POSITION, LIFT THE BARBELL OFF THE FLOOR AND PLACE ON THIGHS, RECLINE THE BODY AND LIFT BARBELL INTO POSITION USING BOTH HANDS.
Start Finish Teaching points
• Lie on bench with head and upper body supported and feet firmly on the floor.
• Neutral spine and engage abdominals. • Hold the barbell with both hands
and position over chest with elbows extended.
• Upper arm fixed, bend the elbows to lower the barbell towards the crown of the head.
• Extend the elbows without locking to raise the barbell.
• Repeat for desired number of repetitions.
Muscles worked
• Triceps brachii.
Options
• Use a dumbbell.
DUMBBELL FLYES
TO POSITION THE DUMBBELLS EITHER USE A SPOTTER OR, FROM A BENCH SEATED POSITION, LIFT THE DUMBBELLS OFF THE FLOOR AND PLACE ON THIGHS, RECLINE THE BODY AND LIFT DUMBBELLS INTO POSITION USING BOTH HANDS (LIGHT RESISTANCE ONLY).
Start Finish Teaching points
• Lie on bench with head and upper body supported and feet firmly on the floor.
• Neutral spine and engage abdominals. • Hold the dumbbells in each hand and
position over the chest with elbows extended but unlocked, and wrists firm but slightly flexed.
• Lower the dumbbells directly to the side, parallel to floor.
• Return to above the chest.• Repeat for desired repetitions.
Muscles worked
• Pectoralis. • Anterior deltoid.
Options
• Can be performed using an inclined bench.
Copyright © 2014 Active IQ Ltd. Not for resale | 301
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

Resistance machines
SEATED CHEST PRESS
Start Finish Teaching points
• Adjust seat height so that bar is level with armpit.
• Neutral spine, abdominals engaged. • Grip handles wider than shoulder-
width, keep wrists straight and aligned with elbows, knuckles forward.
• Press bar forward without locking elbows.
• Return to start position under control. • Repeat for desired repetitions.
Muscles worked
• Pectoralis.• Deltoids (anterior).• Triceps brachii.
Options
• Lying chest press machine. • Lying bench press with free weight. • Body weight press-ups.
PEC DEC
Start Finish Teaching points
• Adjust seat so that handles are level with armpits and back is supported on rest, feet on floor.
• Neutral spine, abdominals engaged and look forward.
• Grip handles with shoulder, elbow and wrist aligned, elbows unlocked.
• Drive arms forward to meet together in front of body.
• Return to start position. • Repeat for desired repetitions.
Muscles worked
• Pectoralis. • Deltoids (anterior).
Options
• Dumbbell flyes – free weights. • Cable machine flyes.
SEATED ROW
Start Finish Teaching points
• Adjust seat to support chest against pad.
• Neutral spine and abdominals engaged. • Grip bar and pull the weight towards
the abdomen, keeping elbows close to body and wrists straight.
• Return under control to start position.• Repeat for desired repetitions.
Muscles worked
• Latissimus dorsi. • Deltoid (posterior).• Biceps brachii.
Options
• Use low cable pulley row. • Single-arm row (free weight).• Bent-over row (free weight).• Seated using resistance band.
302 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

SHOULDER PRESS
Start Finish Teaching points
• Adjust seat so that handles are at shoulder height.
• Neutral spine, abdominals engaged.• Grasp handles, wrist straight and
aligned with elbow. • Press weight upwards without locking
elbows.• Lower under control. • Repeat for desired repetitions.
Muscles worked
• Deltoids. • Upper trapezius. • Triceps brachii.
Options
• Dumbbell shoulder press (free weight).• Barbell shoulder press (free weight).• Use resistance bands.
LAT PULL-DOWN
Start Finish Teaching points
• From standing, grip the bar one and a half shoulder-widths apart. Keep elbows straight and lower body to seated position with thighs secure under pad.
• Lean slightly back so that sternum is under pulley.
• Neutral spine and abdominals engaged.• Pull the bar down under control
towards the sternum, forearms vertical.• Return arms to extended position under
control and without locking elbows. • Repeat for desired repetitions.
Muscles worked
• Latissimus dorsi. • Trapezius. • Biceps brachii.
Options
• Perform with an underhand narrow grip.
• Pull-up – body weight. • Chin-up – body weight. • Seated row.
LEG PRESS
Start Finish Teaching points
• Sit with back rested on pad, feet on platform at hip-width and adjust seat so that knees are at 90° angle.
• Grasp handles at side of body.• Push platform away extending knees
and hips without locking. • Return to start position. • Repeat for desired repetitions.
Muscles worked
• Quadriceps.• Gluteals. • Hamstrings.
Options
• Squat (body weight, barbell or dumbbell).
Copyright © 2014 Active IQ Ltd. Not for resale | 303
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

ASSISTED CHIN-UPS
Start Finish Teaching points
• Hold bar with overhand position one and a half shoulder-widths apart.
• Feet on assisted pad. • Spine neutral, abdominals braced, arms
extended but unlocked, shoulders away from ears.
• Pull body upwards so that chin is level with bar.
• Lower body under control to start position.
• Repeat for desired repetitions.
Muscles worked
• Latissimus dorsi. • Biceps brachii.
Options
• Knees on assisted pad (some machines).
• Lat pull-down.• Use narrow underhand grip. • Non-assisted chin-up or pull-up.
SEATED KNEE/LEG EXTENSION
Start Finish Teaching points
• Adjust seat so that back is supported and knee is aligned with the pivot point.
• Adjust roller/shin pad and position just above shoe laces.
• Lightly grip handles at side of body, neutral spine and abdominals engaged.
• Raise the toes upwards, fully extending the knees without locking, toes to ceiling.
• Lower under control. • Repeat for desired repetitions.
Muscles worked
• Quadriceps.
Options
• One leg at a time. • Squat (body weight, barbell or
dumbbell).• Lunges (body weight, barbell or
dumbbell).
304 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

TRICEPS PRESS OR PUSH-DOWN (HIGH PULLEY USING SHORT BAR ATTACHMENT)
Start Finish Teaching points
• Stand facing cable with feet wider than hip-width apart.
• Neutral spine and abdominals engaged.• Take a narrow overhand grip of bar.• Draw bar down and fix elbows to side
of body.• Press bar down to thighs, elbows
extended without locking.• Return forearm to position parallel to
floor.• Repeat for desired repetitions.
Muscles worked
• Triceps brachii.
Options
• Tricep press machine. • Free weight variations – lying tricep
extension, overhead tricep press/extension.
• Body weight (tricep dips).• Assisted dip machine.
BICEP CURL (LOW PULLEY USING SHORT BAR ATTACHMENT)
Start Finish Teaching points
• Stand close to pulley and deadlift low pulley bar to thighs using underhand grip.
• Widen stance (feet slightly wider than hips), neutral spine and abdominals engaged.
• Elbows close to the sides of body.• Curl the bar upwards towards the chest,
forearms almost vertical. • Lower under control, extending elbows
without locking.• Repeat for desired repetitions. • Return deadlift to lower bar.
Muscles worked
• Biceps brachii.
Options
• Seated bicep curl machine. • Free weight – barbell or dumbbell curls.
Copyright © 2014 Active IQ Ltd. Not for resale | 305
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

SEATED HAMSTRING CURL
Start Finish Teaching points
• Sit on machine with back supported and set the heel pad so that when the knee is aligned with the pivot point the pad is on the Achilles tendon, toes pointing upwards.
• Lightly grip the bars at side of body, neutral spine and abdominals engaged.
• Bend the knee to 90°, pulling the weight down under control.
• Return to start position. • Repeat for desired repetitions.
Muscles worked
• Hamstrings.
Options
• Use prone lying machine.
SEATED ABDUCTOR
Start Finish Teaching points
• Sit on machine, heels on foot bars, with pads outside knees.
• Adjust lever setting so that legs are together.
• Lightly grip bars at side of body, neutral spine, abdominals engaged.
• Press pads away, opening legs as far as comfortable.
• Return under control.• Repeat for desired repetitions.
Muscles worked
• Abductors.
Options
• Use standing total hip machine with pad resting on outside of thigh and push roller up and away.
• Body weight – side lying or standing leg raises.
SEATED ADDUCTOR
Start Finish Teaching points
• Sit on machine, heels on foot bars with pad resting on inside of knees.
• Adjust lever setting so that legs are apart, as far as comfortable.
• Lightly grip bars at side of body, neutral spine, abdominals engaged.
• Squeeze legs together, adducting hip.• Return to open-leg position. • Repeat for desired repetitions.
Muscles worked
• Adductors.
Options
• Use standing total hip machine with pad resting on inside of thigh and pull roller down.
• Body weight – side lying or standing inner thigh raises.
306 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

Static stretches
STANDING GASTROCNEMIUS
Muscles stretching
• Gastrocnemius.
Teaching points
• Feet hip-width apart. • Step one foot back with large stride,
keep front knee bent and aligned with ankle.
• Back leg straight, but unlocked, back heel on floor.
• Both feet facing forward. • Neutral spine, abdominals engaged. • Align ear, shoulder, hip, knee and ankle
on stretching leg. • Pelvic bones facing forward. • Hold for desired duration.
Options
• Place hands on wall for balance. • Four-point gastrocnemius.
FOUR-POINT GASTROCNEMIUS
Teaching points
• Adopt a four-point position with both hands on floor, one leg bent and slightly forward, other leg straight, knee unlocked.
• Neutral spine, abdominals engaged, shoulders away from ears.
• Ease back heel towards the floor to feel mild tension in bulky part of muscle.
• Press hips and buttocks backwards and upwards to increase stretch.
• Hold for desired duration.
Muscles stretching
• Gastrocnemius.
Options
• Place hand on a step or bench.• Standing gastrocnemius.
STANDING SOLEUS
Muscles stretching
• Soleus.
Teaching points
• Feet hip-width apart, step one foot back, narrow stride, both knees bent, feet face forward, heels on floor.
• Neutral spine, abdominals engaged. • Pelvic bones face forward. • Drive back knee forward and sink body
weight down to stretch muscle. • Hold for desired duration.
Options
• Place hands on wall for balance. • Kneeling soleus.
Copyright © 2014 Active IQ Ltd. Not for resale | 307
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

KNEELING SOLEUS
Teaching points
• Split kneeling position – one knee and shin on floor and other foot on floor level with kneeling leg.
• Lean forward over front knee, keeping heel on floor.
• Hold for desired duration.
Muscles stretching
• Soleus.
Options
• Standing soleus.
LYING HAMSTRING STRETCH
Teaching points
• Supine lying. • Raise one leg towards the chest and
hold back of thigh, knee extended but not locked.
• Other leg on the floor either straight or bent with foot on floor.
• Feel stretch in bulky part of muscle. • Neutral spine, abdominals lightly
engaged. • Hold for an appropriate duration.
Muscles stretching
• Hamstrings.
Options
• Bend other leg.• Place strap around foot. • Kneeling hamstring stretch. • Standing hamstring stretch. • Seated hamstring stretch.
KNEELING HAMSTRING STRETCH
Muscles stretching
• Hamstrings.
Teaching points
• Kneeling position, neutral spine, abdominals engaged.
• Step one foot forward with heel on the floor, leg straight, knee unlocked.
• Bend forward from the hip, pressing the buttocks and pelvis backwards.
• Hands on hips or reaching forwards towards ankles.
• Hold for appropriate duration.
Options
• One hand supported against wall or on a step to assist balance.
• Hands on floor (if flexible to reach).
308 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

STANDING HAMSTRING STRETCH
Teaching points
• Standing with feet hip-width apart.• Step one leg forward, keep the leg
straight, knee unlocked.• Bend back leg and bend forward from
hip, sliding hands down thighs. • Press buttocks and pelvis backwards.• Neutral spine and abdominals engaged. • Hold for an appropriate duration.
Muscles stretching
• Hamstrings.
Options
• Place foot on bench to increase range of motion.
• Kneeling, lying or seated hamstring stretch variations.
LYING GLUTEAL STRETCH
Teaching points
• Supine lying, both legs straight. • Draw one knee in towards the chest
with knee bent. • Hold back of thigh and draw leg closer
and across body. • Hold for an appropriate duration.
Muscles stretching
• Gluteals. • Stretches hip flexor on straight leg.
Options
• Perform standing either balancing or using wall support.
LYING GLUTEAL (PIRIFORMIS) STRETCH
Teaching points
• Supine lying, knees bent and feet on floor.
• Cross one foot over other knee.• Draw the leg on the floor towards the
chest and hold back of thigh. • Hold for an appropriate duration.
Muscles stretching
• Gluteals. • Piriformis.
Options
• Keep the foot on the floor, rather than lifting towards chest.
• Lying gluteal stretch (see previous exercise).
• Seated gluteal.
Copyright © 2014 Active IQ Ltd. Not for resale | 309
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

LYING GLUTEAL, ABDUCTOR AND OBLIQUE
Teaching points
• Supine lying, one leg straight, other leg bent.
• Draw the knee of the bent leg across the body, creating a twisting action, use hand to ease further into stretch.
• Shoulders on floor, one arm flexed at shoulder height with elbow bent.
• Look away from stretching leg. • Hold for appropriate duration.
Muscles stretching
• Gluteals. • Abductors. • Obliques.
Options
• Both knees bent and twisting over to one side.
• Other lying or seated gluteal stretches.
SEATED GLUTEAL, ABDUCTOR AND OBLIQUES
Teaching points
• Seated position with legs straight and back lifted.
• Bend one leg and place on floor across other leg (at side of knee).
• Rotate body towards the bent knee, use hand on thigh to ease leg closer, other hand on floor behind back.
• Hold for an appropriate duration.
Muscles stretching
• Gluteals. • Abductor. • Obliques.
Options
• Seated and draw leg in without twisting.
• Other gluteal stretches (see previous exercises).
KNEELING ADDUCTORS (AND OBLIQUES)
Teaching points
• From a kneeling position, step one leg to the side and place foot on floor.
• Neutral spine, abdominals engaged, pelvic bones facing forward.
• Stretch arms over head and lean to one side (not forward or backward).
• Hold for an appropriate duration.
Muscles stretching
• Adductors. • Obliques if arms raised.
Options
• Hands on hips. • One hand on hip and single-arm
stretching towards straight leg.• Seated adductor stretches.
310 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

SEATED ADDUCTOR
Muscles stretching
• Adductors.
Teaching points
• Sit upright on floor with soles of feet together.
• Hold ankles and use elbows against knees to press knees towards the floor.
• Hold for appropriate duration.
Options
• Hands on floor behind back to assist upright sitting.
• Sit with back against wall for support. • Wide-leg straddle position adductor
stretch.
SIDE-LYING QUADRICEPS STRETCH
Teaching points
• Lie on one side, lower leg slightly bent for support.
• Bend top leg, drawing heel to buttocks, holding ankle with top hand.
• Tilt pelvis and pubic bone forward and draw knee back to increase stretch.
• Hold for an appropriate duration.
Muscles stretching
• Quadriceps.
Options
• Prone lying single-leg. • Prone lying double-leg. • Standing quadriceps stretch.
STANDING QUADRICEPS STRETCH
Muscles stretching
• Quadriceps.
Teaching points
• Stand upright. • Raise one heel towards buttocks and
hold ankle with hand of same side. • Knee of stretching leg points to the
floor. • Look forward, upright posture. • Hold for an appropriate duration.
Options
• Hold wall for balance. • Strap around ankle to assist stretch. • Prone or side lying.
Copyright © 2014 Active IQ Ltd. Not for resale | 311
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

KNEELING HIP FLEXOR STRETCH AND LATISSIMUS DORSI
Muscles stretching
• Hip flexor (iliopsoas).• Latissimus dorsi (hands over
head).
Teaching points
• Kneeling with one leg lunged forward. • Hands stretched over head. • Tilt pelvis forward to stretch hip flexor.• Reach arms back slightly.• Hold for appropriate duration.
Options
• Hands on hips. • Knee on step to reduce range of motion. • From standing half-lunge position, tilt
pelvis. • Tilt pelvis in quadriceps stretch to
stretch hip flexor.
RECTUS ABDOMINIS – SPHINX
Teaching points
• Lie prone, raise chest and support body with forearms on floor, elbows under shoulders.
• Look forward. • Hold for appropriate duration.
Muscles stretching
• Rectus abdominis.
Options
• Raise a little higher to increase range of motion.
• Supine lying with arms stretched away from feet, slightly hyperextending the spine.
ERECTOR SPINAE – CAT STRETCH
Teaching points
• Position on all fours with hands under shoulders, knees under hips.
• Round spine, pulling tummy button towards back bone, arching back.
• Shoulders away from ears. • Hold for appropriate duration.
Muscles stretching
• Erector spinae.
Options
• Standing with knees bent and hands on knees, arch spine.
• Hands on chair, feet on floor with knees bent, arch spine.
312 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

STANDING LATISSIMUS DORSI
Muscles stretching
• Latissimus dorsi.• Obliques.
Teaching points
• Stand upright. • Reach arms over head.• Bend to one side without leaning
forward or backward. • Hold for appropriate duration.
Options
• Reach up without side bend. • Smaller bend to decrease range of
motion. • One hand on hip for support. • Kneeling position. • Perform from a seated, cross-legged
position or sitting on a bench.
KNEELING LATISSIMUS DORSI
Teaching points
• Kneel on all fours. • Reach one arm forward past head
and place hand on floor in line with opposite shoulder.
• Point thumb towards ceiling.• Lower shoulder towards floor and
stretch buttocks away from shoulder to increase stretch.
• Hold for appropriate duration.
Muscles stretching
• Latissimus dorsi.
Options
• Hands above head.• Hands on top of a door frame. • Seated on a bench step.
STANDING PECTORALS
Muscles stretching
• Pectoralis.
Teaching points
• Standing with arms raised level with shoulders, elbows bent and hands facing forward, fingers towards ceiling.
• Contract the upper back and middle shoulder blade muscles to draw arms backwards.
• Keep neck long and shoulders away from ears.
• Hold for appropriate duration.
Options
• Hands on buttocks.• Hands between a doorframe. • Seated on a bench step.
Copyright © 2014 Active IQ Ltd. Not for resale | 313
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

STANDING MIDDLE TRAPEZIUS AND RHOMBOIDS
Muscles stretching
• Middle trapezius. • Rhomboids.
Teaching points
• Stand upright with hands in front of body, level with shoulders.
• Link fingers and round upper back, shoulder blades apart.
• Hold for appropriate duration.
Options
• Seated on bench or step. • Hug position with hands crossed over
chest touching opposite shoulder.
UPPER TRAPEZIUS
Muscles stretching
• Upper trapezius.
Teaching points
• Standing with hands behind back. • Grasp wrist of one arm with other hand. • Draw the arm down with the hand and
bend head away from lengthening arm. • Hold for appropriate duration.
Options
• Seated or kneeling position.
STANDING BICEPS
Muscles stretching
• Biceps.
Teaching points
• Stand upright, feet hip-width apart. • Extend hands behind the body as far as
possible, fully extending elbows without locking.
• Draw shoulder blades towards buttocks to minimise rounding of shoulders.
• Point thumbs towards the floor.• Hold for appropriate duration.
Options
• Hold a bar or rail with hands and stretch away from bar.
314 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

Dynamic stretches
SQUAT TO OVERHEAD ARM SWING
Teaching points
• Squat down by bending the ankles, knees and hips.
• Swing the arms down and back during the descent into the squat position.
• Keep chest lifted throughout.• Return to standing position with arms
stretched over head.• Repeat.
Muscles stretching
• Quadriceps.• Gluteus maximus.• Latissimus dorsi.• Soleus.• Iliopsoas.
SQUAT TO OVERHEAD ARM SWING WITH ROTATION
Teaching points
• Squat down by bending the ankles, knees and hips.
• Swing the arms down and back during the descent into the squat position.
• Keep chest lifted throughout.• Return to standing position with arms
stretched over head while rotating the upper body to one side.
• Alternate the side of rotation with each rep.
Muscles stretching
• Quadriceps.• Gluteus maximus.• Obliques.• Soleus.• Iliopsoas.
STANDING TRICEPS
Muscles stretching
• Triceps.
Teaching points
• Stand upright, feet hip-width apart.• Raise one arm over head and place
hand between shoulder blades (or as close as possible).
• Use other hand to press against upper arm and ease further into stretch position.
Options
• Perform in a seated position (cross-legged) or sitting on a bench.
• Press against arm from front rather than over head.
• Link opposite hand behind back to hold hand close to shoulder blade (will stretch anterior deltoid on other arm).
Copyright © 2014 Active IQ Ltd. Not for resale | 315
Appendix 1: Exercise archiveAPPEN
DIX 1
: EXERC
ISE AR
CH
IVE

LUNGE WITH ROTATION
Teaching points
• Stand in an upright position with feet hip-width apart.
• Lunge forward while simultaneously rotating the torso towards the lunging side leg.
• Push back strongly off the lead foot and return to the starting position.
Muscles stretching
• Quadriceps.• Gluteus maximus.• Obliques.• Iliopsoas.
POSTERIOR STEP WITH OVERHEAD REACH
Teaching points
• Stand in an upright position with feet hip-width apart.
• Take a small step back while both arms reach over head.
• Ensure the lunging side heel makes contact with the floor.
• Brace the abdominals to prevent excess lumbar extension.
• Push back strongly off the posterior foot and return to the starting position.
Muscles stretching
• Latissimus dorsi.• Rectus abdominis.• Iliopsoas.• Gastrocnemius.
STANDING DYNAMIC PECTORAL STRETCH
Teaching points
• Stand upright with feet hip-width apart.• Pull the arms back into a press-up
position.• Push the arms forward while allowing
the thoracic spine to round slightly.• Repeat the above varying the angle of
the arms or use static stretches.
Muscles stretching
• Pectoralis major.• Rhomboids.• Mid trapezius.
316 | Copyright © 2014 Active IQ Ltd. Not for resale
Appendix 1: Exercise archive

Copyright © 2014 Active IQ Ltd. Not for resale | 317
References R
EFEREn
CES
References
Unit 1 references
ACSM (2014) guidelines for Exercise Testing and Prescription. 9th Edition. USA. American College of Sports Medicine. wolters kluwer/Lippincott, williams and wilkins. American College of obstetricians and gynaecologists (1994) Exercise during Pregnancy and the Post-Partum Period. Technical Bulletin. no.189, American College of obstetricians and gynaecologists (ACog)Bursztyn, P (1990) Physiology for Sports People. A serious user’s guide to the body. USA. Manchester University Press. davis, d. kimmet, T & Auty, M (1986) Physical Education. Theory and Practice. Australia. Macmillan Education.durstine, J.L. and Moore, g.E. (2003) ACSM’s Exercise Management for Persons with Chronic diseases. 2nd Edition. USA. Human kinetics.Edward Alcamo, I. Ph.d. (2003 Anatomy Colouring Book. USA. Random House. Fleck, S.J. and kraemer, w.J. (1997) designing Resistance Training Programmes. 2nd edition. USA. Human kinetics. Lawrence, d (2008). The Complete guide to Exercise to Music. 3rd ed. A&C Black/Bloomsbury Publishing. London. Uk. McArdle, w.d. katch, F.I. and katch, V.L (1996) Exercise Physiology. Energy, nutrition and Human Performance. 3rd Edition. USA. Lea and Febinger.Mcgill, S (2002) Low Back disorders. USA. Human kinetics. Palastanga, n. Field, d. and Soames, R (1989) Anatomy and Human Movement. Uk. Butterworth Heinemann. Sharkey, B (1990) Physiology of Fitness. 3rd Edition. Champaign, Illinois. USA. Human kinetics. Stone, R. and Stone, J (1990) Atlas of Skeletal Muscles. USA. wm. C. Brown Publishers.Thompson, C (1989) Manual of Structural kinesiology. 11th Edition. USA. Times Mirror Mosby Publishing.Totora, g & Anagnostakos, n (1987) Principle of Anatomy and Physiology. 5th Edition. USA. Harper and Row.
Unit 2 references
gavin, J. (2005). Lifestyle Fitness Coaching. USA. Human kinetics.gravells, A. and Simpson, S. (2009). Equality and diversity in the Lifelong Learning Sector. Learning Matters. UkIvey, A. Ivey, M. and Simek-Morgan, L. (1997). Counselling and Psychotherapy. Allyn and Bacon. koocher, g. and keith-Spiegel, P. (1998). Ethics in Psychology. oxford University Press. Lawrence, d. and Bolitho, S (2011). The Complete guide to Physical Activity and Mental Health. Bloomsbury Publishing. Uk. o’Connor, J. (2001) nLP workbook. Element. REPs (2014). Code of Conduct. Available from: http://www.exerciseregister.org/resources/code-of-conduct. (Accessed on: 20 March 2014). Register of Exercise Professionals.
Unit 3 references
department of Health (2000) no Secrets. guidance on developing and implementingmulti-agency policies and procedures to protect vulnerable adults from abuse. Available from:https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/194272/No_secrets__guidance_on_developing_and_implementing_multi-agency_policies_and_procedures_to_protect_vulnerable_adults_from_abuse.pdf. Accessed on 4-4-2014. HSE (2014) Five Steps to Risk Assessment. Available from: http://www.hse.gov.uk/risk/fivesteps.htm. Accessed on: 3-4-2014 HSE (2014) Health and Safety Regulation. A Short guide. Available from: http://www.hse.gov.uk/pubns/hsc13.pdf. Accessed on: 4-4-201Office of the public Guardian (2013) Safeguarding Policy. Available from: https://www.justice.gov.uk/downloads/protecting-the-vulnerable/mca/safeguarding-policy.pdf. Accessed on: 7-4-2014.ukactive (2014) Health Commitment Statement. Available from: http://www.ukactive.com/membership/raising-standards/ukactive-information-notes/more/7796/page/1/health-commitment-statement-hcs. Accessed on: 4-4-2014
WebsitesnSPCC: http://www.nspcc.org.ukHSE: http://www.hse.gov.ukukactive: http://www.ukactive.comFamily action: http://www.family-action.org.uk/section.aspx?id=4470 dBS: https://www.gov.uk/dbs-check-requests-guidance-for-employersScotland (disclosure): http://www.disclosurescotland.co.uk/apply/employers Northern Ireland (Access NI Disclosure): http://www.dojni.gov.uk/accessni

318 | Copyright © 2014 Active IQ Ltd. Not for resale
References
Unit 4 references
ACSM (2014). ACSM’s guidelines for Exercise Testing and Prescription. 9th ed. American College of Sports Medicine. wolters kluwer/Lippincott williams & wilkins. Philadelphia. USAdepartment of Health (2004). At Least Five a week. Evidence on the impact of physical activity and its relationship to health. A report from the Chief Medical Officer. London. Department of Health.department of Health (2009) Be Active, Be healthy. Available from: http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_094359.pdf. Accessed on: 5-6-2011.department of Health (2011). Start Active, Stay Active: A report on physical activity for health from the four home countries’ Chief Medical Officers. London: Department of Health Physical Activity Team. Available from: http://www.bhfactive.org.uk/userfiles/Documents/startactivestayactive.pdf Accessed: 18-7-2011 Disabled world (2013) Definitions of Disability. Available from: http://www.disabled-world.com/definitions/disability-definitions.php. Accessed on: 18-10-2013Earle, R.w and Baechle, T.R (2000) Resistance Training and Spotting Techniques. In Essentials of Strength Training and Conditioning. (Baechle, T.R. and Earle, R.w. Eds). Pp.343-389. Human kinetics. USA. Government Equalities Office (2010) Equality Act 2010. What do I need to Know? Disability Quick Start Guide. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/85011/disability.pdf. Accessed on: 1-4-2014 Lawrence, d (2008). The Complete guide to Exercise to Music. 3rd ed. A&C Black/Bloomsbury Publishing. London. Uk. Lawrence, d and Hope, B (2011). The Complete guide to Circuit Training. 3rd ed. A&C Black/Bloomsbury Publishing. London. Uk. Lawrence, d and Hope, B (2008). Advanced Circuit Training. A&C Black/Bloomsbury Publishing. London. Uk. Fleck, S.J, and kraemer, w.J (1997) designing Resistance Training Programmes. 2nd ed. Human kinetics. USA.McArdle, w. katch, F and katch. V (2001). Exercise Physiology: Energy, nutrition, and Human Performance. Lippincott, williams and wilkins. USA. MHF (2007) Fundamental facts. Uk. Mental Health FoundationnHS Choices (2012a) water and drinks. Accessed on: 29-7-2012. Available from: http://www.nhs.uk/Livewell/goodfood?pages/water-drinks.aspxnICE (2013) Assessing body mass index and waist circumference thresholds for intervening to prevent ill health and premature death among adults from black, Asian and other minority ethnic groups in the Uk. Public health guidance 46. Available from: http://www.nice.org.uk/nicemedia/live/14201/64332/64332.pdf. Accessed on: 7-2-2014.Public Health England (2013) your guide to the Eatwell Plate. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/237282/Eatwell_plate_booklet.pdf. Accessed on. 1-4-2014. Robergs, R and Roberts, S (1997). Exercise Physiology: Exercise, Performance and Clinical Application. Mosby. USAWalter, S.D, et al (1989) The Ontario Cohort Study of Running-Related Injuries. Archives of Internal Medicine. 149, 2561-2564.world Health organisation (2003). world Health Report 2002, geneva: wHo.world Health organisation (2010). global Recommendations on Physical Activity for Health. Accessed on: 19-5-2013. Available from: http://www.who.int/dietphysicalactivity/publications/9789241599979/en/index.ht
Unit 5 references
American College of Sports Medicine (2014). ACSM’s guidelines for Exercise Testing and Prescription, 9th Edition. Lippincott williams and wilkins, PhiladelphiaAmerican Heart Association (1972). Exercise Testing and Training of Apparently Healthy Individuals: A handbook for Physicians. American Heart Association, dallasBaechle, T., Earle, R. and wathen, d. (2000). Essentials of strength training and conditioning, 2nd edition. Baechle, T & Earle, R. (eds). Human kineticsBlair et al. (1995). Changes in physical fitness and all-cause mortality: A prospective study of healthy and unhealthy men. Journal of the American Medical Association, 273, 1093-8Blair, S.N., Cheng, Y. and Holder, J.S. (2001). Is physical activity or physical fitness more important in defining health benefits? Med Sci Sports Exerc, 33, 379-99Canadian Society for Exercise Physiology (2014) PAR-Q forms. Available from: http://www.csep.ca/english/view.asp?x=698. Accessed on: 24-3-2014.department of Health (2004). At Least Five a week. Evidence on the impact of physical activity and its relationship to health. A report from the Chief Medical Officer. London. Department of Health.department of Health (2011). Start Active, Stay Active. A report on physical activity for health from the four home countries’ Chief Medical Officers. Department of Health, UKEarle, R.w. and Baechle, T.R. (2004). nSCA’s Essentials of Personal Training. Human kineticsFleck, S.J. and kraemer, w.J. (1997). designing Resistance Training Programs. Human kineticsHeyward, V.H. (2002). Advanced Fitness Assessment and Exercise Prescription, 4th Edition. Human kineticsHickson, R.C. and Rosenkoetter, M.A. (1981). Reduced training frequencies and maintenance of increased aerobic power. Med Sci Sports Exerc, 13, 13-6kendal, F.P. McCreary, E.k. and Provance, P.g. (1993). Muscle testing and function. Lippincott williams and wilkinskordich, J.A.C. (2004). Client Consultation and Health Appraisal. In: Essentials of Personal TrainingLaukkanen, J.A., Kurl, S. and Salonen, J.T. (2002). Cardiorespiratory fitness and physical activity as risk predictors of future atherosclerotic cardiovascular diseases. Curr Atheroscler Rep, 4, 468-76McArdle, w.d., katch, F.I. and katch, V.L. (2001). Exercise Physiology, 5th Edition. Lippincott williams & wilkins, PhiladelphiaNICE (2007) Obesity: the prevention, identification, assessment and management of overweight and obesity in adults and children [online] Available at http://www.nice.org.uk/guidance/index.jsp?action=download&o=38295, National Institute of Health and Clinical Excellence.

Copyright © 2014 Active IQ Ltd. Not for resale | 319
References
national obesity observatory (2011) Brief Interventions for weight management. Uk. nHSPaffenbarger, R.S., wing, A.L. and Hyde, R.T. (1978). Physical activity as an index of heart attack risk in college alumni. American Journal of Epidemiology, 108, 161-75Prentice, w.E. (1998). Rehabilitation Techniques in Sports Medicine. Mcgraw HillwHo (2000) ‘wHo. obesity: preventing and managing the global epidemic. Report of a wHo Consultation. wHo Technical Report Series 894’.wHo (2006) obesity: preventing and managing the global epidemic, geneva: world Health organisation.
Unit 6 references
Baechle, T., Earle, R. & wathen, d. (2000). Essentials of strength training and conditioning, 2nd edition. Baechle, T & Earle, R. (eds). Human kineticsEarle, R.w. and Baechle, T.R. (2004). nSCA’s Essentials of Personal Training. Human kineticsFleck, S.J. and kraemer, w.J. (1997). designing Resistance Training Programs. Human kinetics
REFER
EnC
ES

Active IQWestminster House, The Anderson Centre, Ermine Business ParkHuntingdon, Cambridgeshire PE29 6XY
Active IQ wishes to emphasise that whilst every effort is made to ensure accuracy, the material contained within this document is subject to alteration or amendment in terms of overall policy, financial or other constraints. Reproduction of this publication is prohibited unless authorised by Active IQ Ltd. No part of this document should be published elsewhere or reproduced in any form without prior written permission.