
First WHO Model List of Essential In Vitro Diagnostics
73
WHO Technical Report Series 1017 First WHO Model List of Essential In Vitro Diagnostics 1017 First WHO Model List of Essential In Vitro Diagnostics WHO Technical Report Series
Transcript of First WHO Model List of Essential In Vitro Diagnostics

W H O T e c h n i c a l R e p o r t S e r i e s
1017
First WHO Model List of Essential In Vitro Diagnostics
1017First W
HO
Model List of Essential In Vitro D
iagnosticsW
HO
Technical Report Series
ISBN 978 92 4 121026 3
This report presents the First WHO Model List of Essential In Vitro Diagnostics (EDL) and recommendations by the Strategic Advisory Group of Experts on In Vitro Diagnostics (SAGE IVD), commissioned to act as an advisory body on matters of global policies and strategies related to in vitro diagnostics (IVDs). The report described the scope and recommended use of the List and details of the methods, the criteria for prioritizing IVDs and the procedures for establishing the List. It also includes the procedures for updating the List, its integration with other WHO initiatives and its adaption to national contexts. Finally, it contains recommendations from the SAGE IVD on EDLs.

The World Health Organization was established in 1948 as a specialized agency of the United Nations serving as the directing and coordinating authority for international health matters and public health. One of WHO’s constitutional functions is to provide objective and reliable information and advice in the field of human health, a responsibility that it fulfils in part through its extensive programme of publications
The Organization seeks through its publications to support national health strategies and address the most pressing public health concerns of populations around the world. To respond to the needs of Member States at all levels of development, WHO publishes practical manuals, handbooks and training material for specific categories of health workers; internationally applicable guidelines and standards; reviews and analyses of health policies, programmes and research; and state-of-the-art consensus reports that offer technical advice and recommendations for decision-makers. These books are closely tied to the Organization’s priority activities, encompassing disease prevention and control, the development of equitable health systems based on primary health care, and health promotion for individuals and communities. Progress towards better health for all also demands the global dissemination and exchange of information that draws on the knowledge and experience of all WHO’s Member countries and the collaboration of world leaders in public health and the biomedical sciences.
To ensure the widest possible availability of authoritative information and guidance on health matters, WHO secures the broad international distribution of its publications and encourages their translation and adaptation. By helping to promote and protect health and prevent and control disease throughout the world, WHO’s books contribute to achieving the Organization’s principal objective – the attainment by all people of the highest possible level of health.
The WHO Technical Report Series makes available the findings of various international groups of experts that provide WHO with the latest scientific and technical advice on a broad range of medical and public health subjects. Members of such expert groups serve without remuneration in their personal capacities rather than as representatives of governments or other bodies; their views do not necessarily reflect the decisions or the stated policy of WHO.
For further information, please contact: WHO Press, World Health Organization, 20 avenue Appia, 1211 Geneva 27, Switzerland (tel. +41 22 791 3264; fax: +41 22 791 4857; email: [email protected]; order on line: www.who.int/bookorders).

W H O T e c h n i c a l R e p o r t S e r i e s1 0 1 7
First WHO Model List of Essential In Vitro Diagnostics

© World Health Organization 2019
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization.
Suggested citation. First WHO Model List of Essential In Vitro Diagnostics. Geneva: World Health Organization; 2019 (WHO Technical Report Series, No. 1017). Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
Printed in Switzerland
First WHO Model List of Essential In Vitro Diagnostics(WHO Technical Report Series, No. 1017)ISBN 978-92-4-121026-3 ISSN 0512-3054

iii
Contents
Abbreviations and acronyms iv
1. Introduction 1
2. First WHO Model List of Essential In Vitro Diagnostics 32.1 Explanatory notes 3
2.1.1 Scope of the first EDL 32.1.2 Content and format 32.1.3 Recommended use of the EDL 42.1.4 Glossary 5
2.2 Model List of Essential In Vitro Diagnostics 6I. For primary health care 6I.a General IVDs for primary health care 8I.b Disease-specific IVDs for primary health care 11II. For health care facilities with clinical laboratories 18II.a General IVDs for health care facilities with clinical laboratories 19II.b Disease-specific IVDs for health care facilities with clinical laboratories 25
3. Methods used to establish the List 433.1 Strategic Advisory Group of Experts on In Vitro Diagnostics 433.2 Selection of IVDs for inclusion in the first EDL 443.3 Principles that should guide preparation of the EDL 453.4 Draft first EDL proposed by the Secretariat 46
3.4.1 Method for assessing IVDs for inclusion or deletion 473.4.2 Identification of high-priority IVDs for the EDL 48
4. Integration of the EDL with other WHO initiatives 51
5. Procedures for revising the EDL 54
6. Adaptation of the EDL for national lists 56
7. Recommendations 57
References 59
WHO sources used to select the general laboratory tests 60
Acknowledgements 61
Annex 1 Participants in the first meeting of the WHO Strategic Advisory Group of Experts on
In Vitro Diagnostics 62
Annex 2Declarations of interest of SAGE IVD members 65

iv
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9
Abbreviations and acronyms
CLIA chemiluminescence immunoassay
ECL electrochemiluminescence
EDL Model List of Essential In Vitro Diagnostics
EIA enzyme immunoassay
G6PD glucose-6-phosphate dehydrogenase
GLASS Global Antimicrobial Resistance Surveillance System
HBV hepatitis B virus
HCV hepatitis C virus
IVD in vitro diagnostic
MSF Médecins Sans Frontières
RDT rapid diagnostic test
SAGE Strategic Advisory Group of Experts
TB tuberculosis
USCDC Centers for Disease Control and Prevention (USA)
USFDA Food and Drug Administration (USA)

1
1. IntroductionThe three strategic priorities of WHO stated in its Thirteenth General Programme of Work 2019–2023 are to advance universal health coverage, address health emergencies and promote healthier populations (1). The WHO Model List of Essential Medicines contains the medications considered to be the most effective and safe to meet the most important needs in a health system, thus advancing these strategic priorities. Access to good-quality, affordable in vitro diagnostics (IVDs) that allow health providers to make timely diagnoses and offer the most appropriate treatment is also essential for reaching these goals. The WHO Model List of Essential Medicines published in 2017 (2) included a recommendation by the Expert Committee on the Selection of Essential Medicines that WHO prepare a list of essential in vitro diagnostics, which will make an important contribution to universal health coverage.
Like the Model List of Essential Medicines, the Model List of Essential In Vitro Diagnostics (“essential diagnostics list”, EDL) is intended to provide evidence-based guidance to countries for creating their own lists of essential in vitro diagnostic tests. National essential medicines lists have been successful in facilitating access to treatment, particularly in low-resourced countries, by prioritizing the most important medicines all countries should make available to their populations. It is expected that national EDLs will provide the same benefits for in vitro diagnostic tests. It should be noted that EDLs may be included in national lists of essential / priority medical devices that are used for public procurement, reimbursement or for universal health coverage (3).
The EDL comprises a group of IVDs that are recommended by WHO for use at various levels of a tiered national health care system (4). The List is not intended to be prescriptive with respect to the IVDs nor the levels at which they can or should be used. Countries should make their own decisions about which IVDs to select and where they are to be used on the basis of the national or regional burden of the disease, unmet needs, available resources and priorities.
The EDL will provide guidance and serve as a reference to ministries of health, programme managers, users such as laboratory managers, procurement officers and reimbursement systems in Member States, who are establishing or updating national lists of essential IVDs for universal health coverage. It will also inform United Nations agencies and nongovernmental organizations that support the selection, procurement, supply, donations or provision of IVDs. Finally, it will inform and guide the private sector for medical technology on IVD priorities and the IVDs needed to address global health issues.
While the EDL provides a list of tests required at various levels of the health care system, the EDL cannot be useful without an integrated, connected, tiered laboratory system, with adequate human resources, training, laboratory
2
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
infrastructure and regulatory and quality-assurance systems (5). Its impact also requires adoption and adaptation of the EDL by Member States, establishment of national and regional EDLs and the selection and supply mechanisms necessary to ensure access to the IVDs.
This report presents the first EDL and describes the process by which it was established and proposed next steps.

3
2. First WHO Model List of Essential In Vitro Diagnostics2.1 Explanatory notes2.1.1 Scope of the first EDLThis List is the definitive Model List of Essential In Vitro Diagnostics and replaces two previous versions that were published on the WHO website in May and November 2018.
The EDL consists of:
■ general laboratory tests that can be used for routine patient care as well as for the detection and diagnosis of communicable and noncommunicable diseases. These IVDs are grouped by discipline (e.g. clinical chemistry, serology, haematology, microbiology and mycology) and test type (e.g. bilirubin, complete blood count).
■ IVDs for the detection, diagnosis and monitoring of WHO priority diseases: HIV infection, tuberculosis (TB), malaria, hepatitis B, hepatitis C, human papillomavirus (HPV) infection and syphilis. These IVDs are grouped by disease area and analyte tested.
The EDL does not list specific brands but lists IVDs according to their biological targets. Links are provided to information on specific products in categories of tests listed in the EDL that have been prequalified by WHO or are recommended by a WHO disease programme; these are updated regularly.
2.1.2 Content and formatThe first EDL consists of:
■ 35 test categories of general IVDs that can be used for the assessment and diagnosis of a wide array of common and important diseases and
■ 27 test categories of IVDs for the detection, diagnosis and monitoring of HIV infection, tuberculosis, malaria, hepatitis B and C, syphilis and HPV infection,
for a total of 62 test categories and 107 test formats.For each test listed in the EDL, the following are described:
■ test purpose; ■ assay format; ■ specimen type;

4
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
■ facility level (primary level or higher level with laboratory); ■ link to WHO guidance, if available; and ■ link to a WHO prequalified or recommended test or that specific
category, if available.
2.1.3 Recommended use of the EDLFor effective use of the EDL and its adaptation for national requirements, Member States should consider factors such as local demographics, burden of disease, disease elimination priorities, availability of treatments, training and experience of personnel, local unmet testing needs and gaps, supply chain, cost of IVDs, reagents and supplies, quality assurance capacity, financial resources, information technology capability and environmental factors. For that purpose, WHO has collated and maintains an IVD-specific webpage1 linked to the EDL, with information to support selection and use of IVDs, including relevant WHO clinical guidelines, selected systematic reviews, key references, lists of prequalified IVDs and IVDs recommended by WHO disease control departments and resources on quality assurance, basic techniques, procurement and maintenance.
The EDL should not be used in isolation but within the scope of testing services that meet the clinical needs and expectations of each country through their laboratory networks. An example of a tiered health care delivery and laboratory network in a resource-limited country is shown in Fig. 1 (6). The base of the pyramid reflects primary care facilities, which serve most patients directly. Next, there is a smaller number of centralized facilities that serve fewer patients directly. National reference laboratories and some provincial laboratories may not serve patients directly or may offer broad specialist consultation and serve as referral centres for quality assurance and training or for complex testing of samples either sent by facilities lower down the system and transported or from patients referred from other facilities. Other factors that determine use of IVDs are access to electricity, reagent-grade water and specialized human resources (7).
1 https://www.who.int/in-vitro-diagnostic/en/

First WHO Model List of Essential In Vitro Diagnostics
5
Fig. 1Example of tiered health facilities for use of IVDs
Source: adapted from reference 6.
In the first EDL, to simplify its presentation and use, IVDs are listed for two tiers: primary care settings where no or minimal laboratory services are available (level I in Fig. 1) and facilities with laboratories (levels II, III and IV).
2.1.4 GlossaryEssential diagnostics. Diagnostics that satisfy the priority health care needs of the population and are selected with due regard to disease prevalence and public health relevance, evidence of efficacy and accuracy and comparative cost-effectiveness; similar to the definition of an essential medicines.
Health care facility with laboratory support. District, regional, provincial or specialized hospitals or laboratories and national reference laboratories. Trained laboratory technicians, specialist expertise and laboratory infrastructure/equipment are available at the appropriate level. All diagnostic tests available at the primary care level are assumed to be available at higher levels as appropriate.
In vitro diagnostics. A subset of medical devices, defined as devices which, whether used alone or in combination, are intended by the manufacturer for the examination in vitro of specimens derived from the human body solely or principally to provide information for diagnostic, monitoring or compatibility purposes. They include reagents, calibrators, control material and test kits (8).
Medical device. Any article, apparatus, instrument, machine, appliance, implant, reagent for in vitro use, software, material or other similar related articles,

6
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
intended to be used, alone or in combination, for human beings, for one or more of the specific medical purpose(s) of:
■ diagnosis, prevention, monitoring, treatment or alleviation of disease; ■ diagnosis, monitoring, treatment, alleviation of or compensation for
an injury; ■ investigation, replacement, modification, or support of the anatomy
or of a physiological process; ■ supporting or sustaining life; ■ control of conception; ■ disinfection of medical devices; ■ providing information by means of in vitro examination of
specimens derived from the human body; and ■ does not achieve its primary intended action by pharmacological,
immunological or metabolic means, in or on the human body, but which may be assisted in its intended function by such means (8).
Primary health care facilities. Health centres, doctors’ offices, health posts, outreach clinics. Typically, self-testing and rapid diagnostics tests are available, but there are either no laboratories or small laboratories with trained health care personnel but no trained laboratory technicians.
2.2 Model List of Essential In Vitro Diagnostics
The EDL is presented by health care facility level in two tiers:
■ I. Primary health care; with section:a. for general IVDs,2 andb. for specific diseases
■ II. Health care facilities with clinical laboratories, with section:a. for general IVDs,2 andb. for specific diseases
I. For primary health careIncludes IVDs for health posts, community health centres, doctors’ offices, outreach clinics and ambulatory care. Typically, self-testing and rapid diagnostics
2 WHO documents used to compile general laboratory tests for the first EDL are listed under “Sources used for general laboratory tests”.

First WHO Model List of Essential In Vitro Diagnostics
7
tests are available, but there are either no laboratories or only small laboratories with trained health care personnel but no trained laboratory technicians. If laboratory facilities are available in a primary health care facility, please refer to the IVDs described in the next tier. In some cases, samples may be taken where there are no laboratories and processed at the next tier.

8
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
I.a G
ener
al IV
Ds fo
r prim
ary h
ealth
care
Use
Dia
gnos
tic te
stTe
st p
urpo
seA
ssay
form
atSp
ecim
en ty
pe
Hae
mat
olog
y H
aem
oglo
bin
(Hb)
Dia
gnos
is a
nd m
onito
ring
of
anae
mia
Key
clin
ical
mar
ker f
or s
ever
e in
fect
ions
(i.e
. mal
aria
, den
gue,
vi
ral h
aem
orrh
agic
feve
rs)
Safe
ty m
onito
ring
whe
n us
ing
cert
ain
drug
s (e
.g. Z
idov
udin
e fo
r HIV
infe
ctio
n)
Hae
mog
lobi
nom
eter
Capi
llary
who
le b
lood
Veno
us w
hole
blo
od
Dip
stic
kU
rine
Whi
te b
lood
cel
l cou
ntSu
rrog
ate
mar
ker f
or c
erta
in
infe
ctio
ns, i
nflam
mat
ion
or
cert
ain
canc
ers
(e.g
. leu
kaem
ia)
Hae
mat
olog
y an
alys
erCa
pilla
ry w
hole
blo
od
Veno
us w
hole
blo
od
Com
plet
e bl
ood
coun
t (C
BC) m
anua
l (on
ly a
s ba
ck-u
p to
aut
omat
ed
met
hod)
To d
etec
t ana
emia
, inf
ectio
ns
and
leuk
aem
iaH
aem
ocyt
omet
er (t
o m
easu
re W
BC) a
nd
Wrig
ht, M
ay-G
rünw
ald
or G
iem
sa s
tain
(for
di
ffere
ntia
l det
ectio
n of
pa
rasi
tes,
mal
igna
nt c
ells
)
Capi
llary
who
le b
lood
Veno
us w
hole
blo
od
Perip
hera
l blo
od fi
lm
exam
inat
ion
Capi
llary
who
le b
lood
Veno
us w
hole
blo
od

First WHO Model List of Essential In Vitro Diagnostics
9
Tabl
e I.a continued
Use
Dia
gnos
tic te
stTe
st p
urpo
seA
ssay
form
atSp
ecim
en ty
pe
Clin
ical
ch
emis
try
and
imm
unoa
ssay
s
Alb
umin
To d
etec
t/m
onito
r kid
ney
dise
ase
Dip
stic
kU
rine
Bilir
ubin
To d
etec
t/m
onito
r liv
er
dise
ase,
live
r/pa
ncre
as a
nd b
ile
duct
dis
orde
rs, a
nd re
d ce
ll de
stru
ctio
n
Dip
stic
kU
rine
Glu
cose
To d
iagn
ose
and
scre
en fo
r di
abet
es a
nd in
term
edia
te
hype
rgly
caem
ia, t
o di
agno
se
hypo
glyc
aem
ia
Dip
stic
kCa
pilla
ry w
hole
blo
od
Urin
e
Glu
com
eter
Capi
llary
who
le b
lood
Hae
mog
lobi
n A
1c
(HbA
1c)
Dia
gnos
is a
nd m
onito
ring
of
diab
etes
mel
litus
Han
dhel
d an
d sm
all
anal
yser
Capi
llary
who
le b
lood
Who
le b
lood
lact
ate
To a
sses
s m
etab
olic
aci
dosi
s, di
abet
ic k
eto-
acid
osis
, sep
sis
and
dehy
drat
ion
Elec
tro-
anal
ytic
al m
etho
d
Han
dhel
d an
alys
er
Art
eria
l who
le b
lood
Veno
us w
hole
blo
od
Bloo
d tr
ansf
usio
nBl
ood
typi
ngTo
det
erm
ine
bloo
d co
mpa
tibili
ty fo
r blo
od
tran
sfus
ions
; Rh
typi
ng fo
r pr
egna
nt w
omen
Ant
iser
a fo
r agg
lutin
atio
nCa
pilla
ry w
hole
blo
od
Veno
us w
hole
blo
od
Sero
logy
Hum
an c
horio
nic
gona
dotr
opin
(hCG
)Pr
egna
ncy
Dip
stic
kU
rine

10
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e I.a continued
Use
Dia
gnos
tic te
stTe
st p
urpo
seA
ssay
form
atSp
ecim
en ty
pe
Mic
robi
olog
y,
myc
olog
y an
d pa
rasi
tolo
gy
Urin
e di
pstic
k an
d ur
ine
mic
rosc
opy
Det
ectio
n of
UTI
s (d
ipst
ick)
and
id
entifi
catio
n of
red
and
whi
te
bloo
d ce
lls, c
asts
, squ
amou
s ep
ithel
ial c
ells
, bac
teria
, yea
st,
Schi
stos
oma
haem
atob
ium
an
d ot
her c
ellu
lar c
ompo
nent
s (m
icro
scop
y)
Mul
ti-pa
ram
eter
str
ips
(dip
stic
k) a
nd li
ght
mic
rosc
opy
Urin
e
Mic
rosc
opy
Mic
robi
al m
orph
olog
y,
pres
ence
/abs
ence
of w
hite
bl
ood
cells
ver
sus
squa
mou
s ep
ithel
ial c
ells
for p
resu
mpt
ive
iden
tifica
tion
Mic
rosc
opic
exa
min
atio
n of
slid
es a
s w
et
prep
arat
ions
or w
hich
ha
ve b
een
trea
ted
with
a
varie
ty o
f org
anis
m-
spec
ific
chem
ical
sta
ins
(e.g
. Gra
m s
tain
)
Dis
ease
app
ropr
iate
sp
ecim
ens
(e.g
. ve
nous
who
le b
lood
, ur
ine,
sto
ol, e
tc.)

First WHO Model List of Essential In Vitro Diagnostics
11
I.b D
iseas
e-sp
ecifi
c IVD
s for
prim
ary h
ealth
care
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
Hep
atiti
s B
Hep
atiti
s B
surf
ace
antig
en
(HBs
Ag)
Scre
enin
g fo
r acu
te
and
chro
nic
hepa
titis
B
(HBV
) inf
ectio
n:
infa
nts
> 12
m
onth
s of
ag
e, c
hild
ren,
ad
oles
cent
s, ad
ults
RDT
Ora
l flui
d
Capi
llary
w
hole
blo
od
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
hbsa
g/pu
blic
_rep
ort/
en/)
Gui
delin
es o
n he
patit
is B
an
d C
test
ing
(Feb
ruar
y 20
17):
http
://ap
ps.w
ho.in
t/iri
s/
bits
trea
m/h
andl
e/10
665/
25
4621
/978
9241
5499
81-
eng.
pdf?
sequ
ence
=1
Hep
atiti
s B
e an
tigen
(H
BeAg
)
Stag
ing
to
asse
ss th
e ne
ed fo
r HBV
tr
eatm
ent i
n ch
roni
c H
BV
infe
ctio
n
RDT
Capi
llary
w
hole
blo
od
Hep
atiti
s C
Hep
atiti
s C
viru
s an
tibod
y(a
nti-H
CV A
b)
Scre
enin
g fo
r H
CV in
fect
ion:
in
fant
s >
18
mon
ths
of
age,
chi
ldre
n,
adol
esce
nts,
adul
ts
RDT
Ora
l flui
d
Capi
llary
w
hole
blo
od
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
hcv/
publ
ic_r
epor
t/en
/)
Gui
delin
es o
n he
patit
is B
an
d C
test
ing
(Feb
ruar
y 20
17):
http
://ap
ps.w
ho.in
t/iri
s/
bits
trea
m/h
andl
e/10
665/
25
4621
/978
9241
5499
81-
eng.
pdf?
sequ
ence
=1

12
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e I.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
HIV
in
fect
ion
HIV
1/2
an
tibod
y (a
nti-H
IV A
b)
HIV
sel
f-tes
ting
RDT
Ora
l flui
d
Capi
llary
w
hole
blo
od
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
self-
test
ing_
publ
ic-r
epor
t/en
/)
Gui
delin
es o
n H
IV s
elf-
test
ing
and
part
ner
notifi
catio
n (2
016)
http
://ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/han
dle/
1066
5/
2516
55/9
7892
4154
9868
-en
g.pd
f?se
quen
ce=1
Cons
olid
ated
gui
delin
es
on H
IV te
stin
g se
rvic
es
(Jul
y 20
15)
http
://w
ww
.who
.int/
hiv/
pub/
guid
elin
es/h
iv-
test
ing-
serv
ices
/en/
WH
O im
plem
enta
tion
tool
for p
re-e
xpos
ure
prop
hyla
xis
(PrE
P) o
f HIV
in
fect
ion,
mod
ule
10 fo
r te
stin
g pr
ovid
ers
(201
7)
http
://w
ww
.who
.int/
hiv/
pub/
prep
/pre
p-im
plem
enta
tion-
tool
/en/
For t
he
diag
nosi
s of
H
IV in
fect
ion:
ad
ults
, ad
oles
cent
s, ch
ildre
n an
d in
fant
s ov
er 1
8 m
onth
s of
age
RDT
Ora
l flui
d
Capi
llary
w
hole
blo
od

First WHO Model List of Essential In Vitro Diagnostics
13
Tabl
e I.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
HIV
in
fect
ion
cont
inue
d
Com
bine
d H
IV a
ntib
ody/
p24
antig
en
(ant
i-HIV
/p2
4 Ag
)
For t
he
diag
nosi
s of
H
IV in
fect
ion:
ad
ults
, ad
oles
cent
s, ch
ildre
n an
d in
fant
s ov
er 1
8 m
onth
s of
age
RDT
Ora
l flui
d
Capi
llary
w
hole
blo
od
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
hiv-
rdts
/pub
lic_r
epor
t/en
/)
Cons
olid
ated
gui
delin
es
on H
IV te
stin
g se
rvic
es
(201
5)ht
tp://
ww
w.w
ho.in
t/hi
v/pu
b/gu
idel
ines
/hiv
-te
stin
g-se
rvic
es/e
n/
Mal
aria
Plas
mod
ium
sp
p. a
ntig
ens;
sp
ecie
s sp
ecifi
c (e
.g.
HRP
2) a
nd/o
r pa
n-sp
ecie
s sp
ecifi
c (e
.g.
pan-
pLD
H)
For d
iagn
osis
of
one
or
mor
e hu
man
m
alar
ia s
peci
es
(P. f
alci
paru
m,
P. v
ivax
, P.
mal
aria
e,
P. o
vale
)
RDT
Capi
llary
w
hole
blo
odPu
blic
repo
rts
of W
HO
pr
equa
lified
IVD
s (h
ttp:
//w
ww
.who
.int/
diag
nost
ics_
labo
rato
ry/
eval
uatio
ns/p
q-lis
t/m
alar
ia/p
ublic
_rep
ort/
en/)
WH
O g
uide
lines
for t
he
trea
tmen
t of m
alar
ia, t
hird
ed
ition
(201
5)ht
tp://
apps
.who
.int/
iris/
bits
trea
m/1
0665
/162
441/
1/
9789
2415
4912
7_en
g.pd
f
Mal
aria
rapi
d di
agno
stic
te
st p
erfo
rman
ce. R
esul
ts
of W
HO
pro
duct
test
ing
of m
alar
ia R
DTs
: Rou
nd 7
(2
015–
2016
)ht
tp://
ww
w.w
ho.in
t/m
alar
ia/p
ublic
atio
ns/
atoz
/978
9241
5126
8/en
/

14
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e I.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
Mal
aria
co
ntin
ued
WH
O g
ood
prac
tices
for
sele
ctin
g an
d pr
ocur
ing
rapi
d di
agno
stic
test
s fo
r m
alar
ia (2
011)
ht
tp://
apps
.who
.int/
iris/
bi
tstr
eam
/han
dle/
1066
5/
4453
0/97
8924
1501
125_
eng.
pdf?
sequ
ence
=1
Plas
mod
ium
sp
p.Fo
r dia
gnos
is
of o
ne o
r mor
e hu
man
mal
aria
sp
ecie
s (P
. fal
cipa
rum
,P.
viv
ax, P
. m
alar
iae,
P.
oval
e an
d P.
kno
wle
si) a
nd
mon
itorin
g re
spon
se to
tr
eatm
ent
Ligh
t m
icro
scop
y (if
goo
d qu
ality
m
icro
scop
y av
aila
ble)
Capi
llary
w
hole
blo
odW
HO
gui
delin
es fo
r the
tr
eatm
ent o
f mal
aria
, thi
rd
editi
on (2
015)
http
://ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/106
65/1
6244
1/
1/97
8924
1549
127_
eng.
Basi
c m
alar
ia m
icro
scop
y Pa
rt I:
Lea
rner
’s gu
ide
(201
0)
http
://ap
ps.w
ho.in
t/iri
s/
bits
trea
m/h
andl
e/10
665/
44
208/
9789
2415
4782
6_en
g.pd
f?se
quen
ce=1

First WHO Model List of Essential In Vitro Diagnostics
15
Tabl
e I.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
*
WH
O s
uppo
rtin
g do
cum
ents
Mal
aria
co
ntin
ued
Mal
aria
mic
rosc
opy
stan
dard
ope
ratin
g pr
oced
ures
(201
5)
http
://w
ww
.wpr
o.w
ho.
int/
mvp
/lab_
qual
ity/
mm
_sop
/en/
Tube
rcul
osis
Myc
obac
teriu
m
tube
rcul
osis
For d
iagn
osis
an
d tr
eatm
ent
mon
itorin
g of
ac
tive
TB
Mic
rosc
opy
Sput
umIm
plem
entin
g tu
berc
ulos
is
diag
nost
ics:
Pol
icy
fram
ewor
k (2
015)
ht
tp://
apps
.who
.int/
iri
s/bi
tstr
eam
/106
65/
1627
12/1
/978
9241
50
8612
_eng
Com
pend
ium
of W
HO
gu
idel
ines
and
ass
ocia
ted
stan
dard
s: E
nsur
ing
optim
um d
eliv
ery
of
the
casc
ade
of c
are
for
patie
nts
with
tube
rcul
osis
(2
017)
http
://ap
ps.w
ho.in
t/iri
s/
bits
trea
m/h
andl
e/10
665/
25
9180
/978
9241
5125
72-
eng.
pdf?
sequ
ence
=1Im
plem
entin
g tu
berc
ulos
is d
iagn
ostic
s:
Polic
y fr
amew
ork
(201
5)
http
://ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/106
65/1
6271
2/
1/97
8924
1508
612_
eng.
* All
TB te
sts a
re e
valu
ated
and
gui
delin
es d
evel
oped
thro
ugh
the
WHO
Glo
bal T
B Pr
ogra
mm
e.

16
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e I.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
*
WH
O s
uppo
rtin
g do
cum
ents
Tube
rcul
osis
co
ntin
ued
For d
iagn
osis
of
act
ive
TBLo
op
med
iate
d is
othe
rmal
am
plifi
catio
n (L
AM
P)
Sput
umTh
e us
e of
loop
-m
edia
ted
isot
herm
al
ampl
ifica
tion
(TB-
LAM
P)
for t
he d
iagn
osis
of
pulm
onar
y tu
berc
ulos
is:
Polic
y gu
idan
ce (2
016)
http
://ap
ps.w
ho.in
t/iri
s/
bits
trea
m/1
0665
/ 24
9154
/1/9
7892
4151
1 18
6-en
g.pd
f?ua
=1
Imm
une
resp
onse
For d
iagn
osis
of
late
nt T
B in
fect
ion
Intr
ader
mal
tu
berc
ulin
sk
in te
st
(TST
)
N/A
Late
nt T
B in
fect
ion:
U
pdat
ed a
nd
cons
olid
ated
gui
delin
es
for p
rogr
amm
atic
m
anag
emen
t (20
18)
http
://ap
ps.w
ho.in
t/iri
s/
bits
trea
m/h
andl
e/10
665/
26
0233
/978
9241
5502
39-
eng.
pdf;j
sess
ioni
d=
6D1B
B246
312B
378A
CF
EBF9
BFFA
FEB0
ED?
sequ
ence
=1
* All
TB te
sts a
re e
valu
ated
and
gui
delin
es d
evel
oped
thro
ugh
the
WHO
Glo
bal T
B Pr
ogra
mm
e.

First WHO Model List of Essential In Vitro Diagnostics
17
Tabl
e I.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
Syph
ilis
Ant
ibod
ies
to
Trep
onem
a pa
llidu
m
For d
iagn
osis
or
as
an a
id in
th
e di
agno
sis
of T
. pal
lidum
RDT
Capi
llary
w
hole
blo
odW
HO
list
of p
requ
alifi
ed
in v
itro
diag
nost
ic
prod
ucts
(htt
p://
ww
w.
who
.int/
diag
nost
ics_
labo
rato
ry/e
valu
atio
ns/
PQ_l
ist/
en/)
WH
O la
bora
tory
di
agno
sis
of s
exua
lly
tran
smitt
ed in
fect
ions
, in
clud
ing
hum
an
imm
unod
efici
ency
viru
s (2
013)
ht
tp://
apps
.who
.int/
iris/
bi
tstr
eam
/han
dle/
1066
5/
8534
3/97
8924
1505
840_
en
g.pd
f?se
quen
ce=1
Com
bine
d an
tibod
ies
to
T. p
allid
um
and
to
HIV
-1/2
For d
iagn
osis
or
as
an a
id in
th
e di
agno
sis
of H
IV-1
/2 a
nd/
or T
. pal
lidum
RDT
Capi
llary
w
hole
blo
odPu
blic
repo
rts
of W
HO
pr
equa
lified
IVD
s (h
ttp:
//w
ww
.who
.int/
diag
nost
ics_
labo
rato
ry/
eval
uatio
ns/p
q-lis
t/hi
v-rd
ts/p
ublic
_rep
ort/
en/)
WH
O In
form
atio
n no
te
on th
e us
e of
dua
l HIV
/sy
phili
s ra
pid
diag
nost
ic
test
s (R
DT)
(201
7)ht
tp://
apps
.who
.int/
iris/
bi
tstr
eam
/han
dle/
1066
5/
2528
49/W
HO
-RH
R-17
.01-
en
g.pd
f?se
quen
ce=1

18
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
II. For health care facilities with clinical laboratoriesThis list is for district, regional, provincial or specialized hospitals or laboratories and national reference laboratories. Trained laboratory technicians, specialist expertise and laboratory infrastructure and equipment are available at the appropriate level. All diagnostic tests available at the primary care level are assumed to be available at higher levels, as appropriate. The list comprises: section a for general laboratory equipment and section b for tests for specific diseases.

First WHO Model List of Essential In Vitro Diagnostics
19
II.a
Gene
ral I
VDs f
or h
ealth
care
facil
ities
with
clin
ical l
abor
ator
ies
Use
Dia
gnos
tic te
stTe
st p
urpo
seA
ssay
form
atSp
ecim
en ty
pe
Clin
ical
ch
emis
try
and
imm
unoa
ssay
s
Ala
nine
am
ino-
tran
sfer
ase
(ALT
)To
ass
ess
liver
func
tion
(oft
en d
one
with
asp
arta
te
amin
otra
nsam
inas
e A
ST))
Opt
ical
and
ele
ctro
-an
alyt
ical
met
hods
Seru
m
Plas
ma
Alb
umin
To d
etec
t or m
onito
r mal
nutr
ition
, liv
er
or k
idne
y di
seas
ePh
otom
etric
, tur
bidi
met
ric
and
neph
elom
etric
test
ing
Urin
e
Seru
m
Plas
ma
Alk
alin
e ph
osph
atas
eTo
det
ect o
r mon
itor m
alnu
triti
on,
Page
t’s d
isea
se o
r cer
tain
mal
igna
ncie
s, in
clud
ing
liver
can
cer
Colo
rimet
ric te
stin
gSe
rum
Plas
ma
Asp
arta
te a
min
o-
tran
sfer
ase
(A
ST)
To a
sses
s of
live
r fun
ctio
n (o
ften
don
e w
ith a
lani
ne
amin
otra
nsfe
rase
(ALT
))
Opt
ical
and
ele
ctro
-an
alyt
ical
met
hods
Seru
m
Plas
ma
Bilir
ubin
To d
etec
t/m
onito
r liv
er d
isea
se, l
iver
/pa
ncre
as a
nd b
ile d
uct d
isor
ders
, and
re
d ce
ll de
stru
ctio
n
Opt
ical
and
ele
ctro
-an
alyt
ical
met
hods
Seru
m
Plas
ma
Bloo
d pH
and
ga
ses
To a
sses
s lu
ng fu
nctio
n, m
etab
olic
or
kidn
ey d
isor
ders
, and
mon
itor o
xyge
n th
erap
y
Mea
sure
men
t of b
lood
pH
, oxy
gen
and
carb
on d
ioxi
de
Elec
tro-
anal
ytic
al m
etho
ds,
incl
udin
g po
rtab
le a
naly
sers
Art
eria
l who
le b
lood
Veno
us w
hole
blo
od
Bloo
d ur
ea
nitr
ogen
(BU
N)
To a
sses
s ki
dney
func
tion
and
dise
ase
Opt
ical
and
ele
ctro
-an
alyt
ical
met
hods
Seru
m
Plas
ma

20
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e II.a
continued
Use
Dia
gnos
tic te
stTe
st p
urpo
seA
ssay
form
atSp
ecim
en ty
pe
Clin
ical
ch
emis
try
and
imm
unoa
ssay
s co
ntin
ued
Crea
tinin
eTo
est
imat
e gl
omer
ular
filtr
atio
n ra
te
(eG
FR) a
nd u
rine
albu
min
/cre
atin
ine
ratio
Key
clin
ical
mar
ker f
or m
anag
emen
t of
sev
ere
infe
ctio
ns (i
.e. s
epsi
s, La
ssa
feve
r), a
nd a
ntim
icro
bial
regi
men
ad
just
men
t
Opt
ical
and
ele
ctro
-an
alyt
ical
met
hods
Seru
m
Urin
e
Elec
trol
ytes
To m
onito
r org
an d
amag
e an
d el
ectr
olyt
e al
tera
tions
Opt
ical
and
ele
ctro
-an
alyt
ical
met
hods
Seru
m
Plas
ma
Glu
cose
To d
iagn
ose
and
scre
en fo
r dia
bete
s an
d in
term
edia
te h
yper
glyc
aem
ia, t
o di
agno
se h
ypog
lyca
emia
Auto
mat
ed a
naly
ser
Plas
ma
Seru
m
Hae
mog
lobi
n A
1c
(HbA
1c)
Dia
gnos
is a
nd m
onito
ring
of d
iabe
tes
mel
litus
ELIS
A
Auto
mat
ed a
naly
ser
Capi
llary
who
le
bloo
d
Veno
us w
hole
blo
od
C-re
activ
e pr
otei
n (C
RP)
To d
etec
t infl
amm
atio
n as
an
indi
cato
r of v
ario
us c
ondi
tions
(e.g
. ca
rdio
vasc
ular
dis
ease
[CVD
] – h
igh
sens
itivi
ty C
RP re
quire
d -
seps
is)
RDT
EIA
Veno
us w
hole
blo
od
Seru
m
Plas
ma
Lipi
d pr
ofile
To a
sses
s ris
k of
dev
elop
ing
CVD
an
d ty
pe 2
dia
bete
s by
mea
surin
g ch
oles
tero
l, tr
igly
cerid
es a
nd
lipop
rote
ins
Colo
urim
etry
Spec
trop
hoto
met
ryPl
asm
a
Seru
m

First WHO Model List of Essential In Vitro Diagnostics
21
Tabl
e II.a
continued
Use
Dia
gnos
tic te
stTe
st p
urpo
seA
ssay
form
atSp
ecim
en ty
pe
Clin
ical
ch
emis
try
and
imm
unoa
ssay
s co
ntin
ued
Basi
c m
etab
olic
pa
nel (
BMP)
Incl
udes
glu
cose
, sod
ium
chl
orid
e,
carb
on d
ioxi
de, b
lood
ure
a ni
trog
en
(BU
N),
BUN
/cre
atin
ine
ratio
, glo
mer
ular
fil
trat
ion
rate
(eG
FR) a
nd m
ay in
clud
e ca
lciu
m
Phot
omet
ric a
nd
colo
rimet
ric te
stin
g, io
n-se
lect
ive
pote
ntio
met
ry
(8-p
aram
eter
aut
omat
ed
clin
ical
che
mis
try
anal
yser
)
Veno
us w
hole
blo
od
Seru
m
Plas
ma
Com
preh
ensi
ve
met
abol
ic p
anel
BMP
plus
mag
nesi
um, p
rote
in,
albu
min
, glo
bulin
, alb
umin
/glo
bulin
ra
tio, b
iliru
bin
(dire
ct o
r tot
al),
alka
line
phos
phat
ase,
ala
nine
and
asp
arta
te
amin
otra
nsfe
rase
s (A
LT a
nd A
ST)
As
with
BM
P (1
4 or
mor
e pa
ram
eter
au
tom
ated
clin
ical
che
mis
try
anal
yser
)
Veno
us w
hole
blo
od
Seru
m
Plas
ma
Am
ylas
e an
d lip
ase
To a
sses
s ac
ute
panc
reat
itis
Colo
urim
etric
and
ph
otom
etric
ana
lyse
rsSe
rum
Perit
onea
l flui
d (A
myl
ase)
Trop
onin
T/I
For d
iagn
osis
of m
yoca
rdia
l inf
arct
ion
EIA
(han
dhel
d or
larg
e au
tom
ated
inst
rum
ent)
Veno
us w
hole
blo
od
Plas
ma
Urin
alys
isD
etec
tion
of s
ubst
ance
s in
the
urin
e as
soci
ated
with
met
abol
ic d
isor
ders
, re
nal d
ysfu
nctio
n or
urin
ary
trac
t in
fect
ions
Auto
mat
ed c
hem
ical
an
alys
erU
rine

22
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e II.a
continued
Use
Dia
gnos
tic te
stTe
st p
urpo
seA
ssay
form
atSp
ecim
en ty
pe
Bloo
d tr
ansf
usio
nBl
ood
cros
s-m
atch
ing
To d
eter
min
e bl
ood
com
patib
ility
fo
r blo
od tr
ansf
usio
ns; R
h ty
ping
for
preg
nant
wom
en
Ant
iser
a fo
r agg
lutin
atio
nVe
nous
who
le b
lood
Tran
sfus
ion
tran
smitt
ed
infe
ctio
ns
To s
cree
n fo
r e.g
. Cha
gas,
hum
an
T-ly
mph
otro
pic
viru
s (H
TLV
) in
the
bloo
d su
pply
etc
. (se
e al
so E
DL
sect
ions
on
HIV
& s
yphi
lis)
EIA
(mic
ropl
ate)
Man
ual m
etho
dSe
rum
Plas
ma
CLIA
/ECL
(aut
omat
ed
inst
rum
ent)
Seru
m
Plas
ma
Sero
logy
Hum
an c
horio
nic
gona
dotr
opin
(h
CG)
Preg
nanc
yO
ptic
al m
etho
dSe
rum
Mic
robi
olog
y,
myc
olog
y an
d pa
rasi
tolo
gy
Urin
e di
pstic
k an
d ur
ine
mic
rosc
opy
Det
ectio
n of
UTI
s (d
ipst
ick)
and
id
entifi
catio
n of
red
and
whi
te b
lood
ce
lls, c
asts
, squ
amou
s ep
ithel
ial
cells
, bac
teria
, yea
st, S
chis
toso
ma
haem
atob
ium
and
oth
er c
ellu
lar
com
pone
nts
(mic
rosc
opy)
Mul
ti-pa
ram
eter
str
ips
(dip
stic
k) a
nd li
ght
mic
rosc
opy
Urin
e
Mic
rosc
opy
Mic
robi
al m
orph
olog
y, p
rese
nce
or a
bsen
ce o
f whi
te b
lood
cel
ls
vers
us s
quam
ous
epith
elia
l cel
ls fo
r pr
esum
ptiv
e id
entifi
catio
n
Mic
rosc
opic
exa
min
atio
n of
sl
ides
as
wet
pre
para
tions
or
whi
ch h
ave
been
trea
ted
with
org
anis
m-s
peci
fic
chem
ical
sta
ins
(e.g
. Gra
m
stai
n)
Dis
ease
app
ropr
iate
sp
ecim
ens
(e.g
. ve
nous
who
le
bloo
d, u
rine,
sto
ol,
cere
bros
pina
l flui
d,
etc.
)

First WHO Model List of Essential In Vitro Diagnostics
23
Tabl
e II.a
continued
Use
Dia
gnos
tic te
stTe
st p
urpo
seA
ssay
form
atSp
ecim
en ty
pe
Mic
robi
olog
y,
myc
olog
y an
d pa
rasi
tolo
gy
cont
inue
d
Cultu
reIn
itial
ste
p in
det
ectio
n an
d id
entifi
catio
n of
bac
teria
l spe
cies
for
sele
ctio
n of
app
ropr
iate
ant
ibio
tic
regi
men
s
Cultu
re o
n gr
owth
med
ia
plat
es in
an
incu
bato
r fo
llow
ed b
y re
cove
ry
of is
olat
es a
nd s
peci
es
iden
tifica
tion
(tra
ditio
nal
man
ual t
echn
ique
s or
au
tom
ated
equ
ipm
ent)
Dis
ease
app
ropr
iate
sp
ecim
ens
(e.g
. ve
nous
who
le
bloo
d, u
rine,
sto
ol,
cere
bros
pina
l flui
d et
c.)
Bloo
d cu
lture
Fo
r the
dia
gnos
is o
f bac
teria
l and
fu
ngal
blo
odst
ream
infe
ctio
ns (s
epsi
s)Bl
ood
cultu
re b
ottle
in
an in
cuba
tor f
ollo
wed
by
reco
very
of i
sola
tes
and
spec
ies
iden
tifica
tion
(tra
ditio
nal m
anua
l te
chni
ques
or a
utom
ated
eq
uipm
ent)
Veno
us w
hole
blo
od
Ant
imic
robi
al
susc
eptib
ility
te
stin
g
Fina
l ste
p in
sel
ectio
n of
app
ropr
iate
an
tibio
tic re
gim
ens
afte
r spe
cies
id
entifi
catio
n
Ant
imic
robi
al s
usce
ptib
ility
te
stin
g of
isol
ates
– m
ay
be d
one
man
ually
by
disc
di
ffusi
on te
chni
que
or
auto
mat
ed p
latf
orm
s
Mic
robi
al is
olat
es
Hae
mat
olog
yH
aem
atoc
rit (H
t)D
iagn
osis
and
mon
itorin
g of
ana
emia
Volu
me
of re
d bl
ood
cells
as
a pe
rcen
tage
of t
otal
blo
od v
olum
e
Mic
ro-h
aem
atoc
rit
cent
rifug
eCa
pilla
ry o
r ven
ous
who
le b
lood

24
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e II.a
continued
Use
Dia
gnos
tic te
stTe
st p
urpo
seA
ssay
form
atSp
ecim
en ty
pe
Hae
mat
olog
y co
ntin
ued
Prot
hrom
bin
time
test
and
in
tern
atio
nal
norm
aliz
ed ra
tio
(PT/
INR)
To d
etec
t or d
iagn
ose
a bl
eedi
ng
diso
rder
or e
xces
sive
clo
ttin
g di
sord
er
(pro
thro
mbi
n tim
e (P
T));
mon
itor
perf
orm
ance
of a
ntic
oagu
lant
m
edic
atio
ns (I
nter
natio
nal n
orm
alis
ed
ratio
(IN
R))
Han
d-he
ld o
r aut
omat
ed
coag
ulat
ion
anal
yser
Citr
ate
plas
ma
Plat
elet
cou
ntD
iagn
osis
of t
hrom
bocy
tope
nia
Mar
ker t
o m
anag
e se
vere
infe
ctio
ns
asso
ciat
ed w
ith b
leed
ing
and
seps
is (i
.e. v
iral h
aem
orrh
agic
feve
r, m
enin
goco
ccae
mia
) and
cer
tain
ha
emat
olog
ical
dis
orde
rs
Hae
moc
ytom
eter
Capi
llary
who
le
bloo
d
Hae
mat
olog
y an
alys
erVe
nous
who
le b
lood
Com
plet
e bl
ood
coun
t (CB
C)Au
tom
ated
, di
ffere
ntia
l
Eval
uatio
n of
pat
ient
’s ov
eral
l hea
lth
and
to d
etec
t a w
ide
rang
e of
di
sord
ers,
incl
udin
g an
aem
ia, i
nfec
tion
and
leuk
aem
ia
Auto
mat
ed h
emat
olog
y an
alys
er (w
hite
blo
od c
ell
coun
t (W
BC),
red
bloo
d ce
ll co
unt (
RBC)
, pla
tele
ts,
haem
oglo
bin
(Hb)
and
ha
emat
ocrit
(Ht)
incl
udes
ly
mph
ocyt
es, m
onoc
ytes
an
d gr
anul
ocyt
es (f
or th
ree-
part
diff
eren
tial)
Veno
us w
hole
blo
od

First WHO Model List of Essential In Vitro Diagnostics
25
II.b
Dise
ase-
spec
ific I
VDs f
or h
ealth
care
facil
ities
with
clin
ical l
abor
ator
ies
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
Hep
atiti
s B
Hep
atiti
s B
surf
ace
antig
en
(HBs
Ag)
Scre
enin
g fo
r acu
te
and
chro
nic
hepa
titis
B v
irus
(HBV
) inf
ectio
n:
infa
nts
> 12
m
onth
s of
ag
e, c
hild
ren,
ad
oles
cent
s, ad
ults
RDT
Veno
us
who
le b
lood
Plas
ma
Seru
m
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
hbsa
g/pu
blic
_rep
ort/
en/)
Gui
delin
es o
n he
patit
is B
an
d C
test
ing
(Feb
ruar
y 20
17)
http
://ap
ps.w
ho.in
t/iri
s/
bits
trea
m/h
andl
e/10
665/
25
4621
/978
9241
5499
81-
eng.
pdf?
sequ
ence
=1
EIA
Plas
ma
Seru
m
CLIA
Plas
ma
Seru
m
Viro
logi
cal
(HBV
DN
A –
qu
antit
ativ
e)
Stag
ing
to
asse
ss th
e ne
ed
for t
reat
men
t in
chr
onic
HBV
in
fect
ion
and
mon
itorin
g of
re
spon
se to
tr
eatm
ent
Nuc
leic
ac
id te
stSe
rum
Plas
ma

26
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
Hep
atiti
s B
cont
inue
dH
epat
itis
B e
antig
en
(HBe
Ag)
Stag
ing
to
asse
ss th
e ne
ed fo
r HBV
tr
eatm
ent i
n ch
roni
c H
BV
infe
ctio
n
EIA
Seru
m
Plas
ma
CLIA
Seru
m
Plas
ma
IgM
-spe
cific
an
tibod
ies
to h
epat
itis
B co
re a
ntig
en
(IgM
ant
i-HBc
)
For t
he
diag
nosi
s of
ac
ute
HBV
in
fect
ion
– us
ed fo
r ou
tbre
ak
inve
stig
atio
n
EIA
(m
icro
plat
e)
Man
ual
met
hod
Seru
m
Plas
ma
CLIA
/ECL
(a
utom
ated
in
stru
men
t)
Seru
m
Plas
ma
Ant
ibod
ies
to h
epat
itis
B su
rfac
e an
tigen
(ant
i-H
Bs)
To d
eter
min
e eff
ectiv
enes
s of
H
BV v
acci
natio
n at
pat
ient
and
at
a p
opul
atio
n le
vel
Als
o us
ed a
s a
mar
ker f
or
reco
very
from
H
BV in
fect
ion
EIA
(m
icro
plat
e)
Man
ual
met
hod
Seru
m
Plas
ma
CLIA
/ECL
(a
utom
ated
in
stru
men
t)
Seru
m
Plas
ma
First WHO Model List of Essential In Vitro Diagnostics
27
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
Hep
atiti
s C
Ant
ibod
ies
to
HCV
(ant
i-HCV
)
Scre
enin
g fo
r H
CV in
fect
ion:
in
fant
s >
18
mon
ths
of
age,
chi
ldre
n,
adol
esce
nts,
adul
ts
RDT
Veno
us
who
le b
lood
Plas
ma
Seru
m
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
hcv/
publ
ic_r
epor
t/en
/)
Gui
delin
es o
n he
patit
is B
an
d C
test
ing
(Feb
ruar
y 20
17)
http
://ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/han
dle/
1066
5/
2546
21/9
7892
4154
9981
- en
g.pd
f?se
quen
ce=1
EI
A
(mic
ropl
ate)
M
anua
l m
etho
d
Seru
m
Plas
ma
CLIA
/ECL
(a
utom
ated
in
stru
men
t)
Seru
m
Plas
ma
Ant
ibod
ies
to
HCV
(ant
i-H
CV) a
nd H
CV
core
ant
igen
(H
CV c
Ag)
Scre
enin
g fo
r pa
st o
r pre
sent
H
CV in
fect
ion:
in
fant
s >
18
mon
ths
of
age,
chi
ldre
n,
adol
esce
nts,
adul
ts
EIA
(m
icro
plat
e)
Man
ual
met
hod
Seru
m
Plas
ma
CLIA
/ECL
(a
utom
ated
in
stru
men
t)
Seru
m
Plas
ma
HCV
cor
e an
tigen
(H
CV c
Ag)
For d
iagn
osis
of
vira
emic
HCV
CL
IA/E
CL
(aut
omat
ed
inst
rum
ent)
Seru
m
Plas
ma

28
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
Hep
atiti
s C
cont
inue
dH
CV R
NA
(q
ualit
ativ
e or
qu
antit
ativ
e)
For d
iagn
osis
of
vira
emic
HCV
an
d m
onito
ring
of re
spon
se to
tr
eatm
ent a
s a
test
of c
ure
Nuc
leic
ac
id te
stSe
rum
Plas
ma
HIV
in
fect
ion
Ant
ibod
ies
to
HIV
-1/2
(ant
i-H
IV) t
est
For t
he
diag
nosi
s of
H
IV in
fect
ion:
ad
ults
, ad
oles
cent
s, ch
ildre
n an
d in
fant
s >
18
mon
ths
of a
ge
RDT
Veno
us
who
le b
lood
Plas
ma
Seru
m
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
self-
test
ing_
publ
ic-r
epor
t/en
/)
Gui
delin
es o
n H
IV s
elf-
test
ing
and
part
ner
notifi
catio
n (2
016)
ht
tp://
apps
.who
.int/
iris/
bi
tstr
eam
/han
dle/
1066
5/
2516
55/9
7892
4154
9868
-en
g.pd
f?se
quen
ce=1
EIA
(m
icro
plat
e)
Man
ual
met
hod
Seru
mPl
asm
aCo
nsol
idat
ed g
uide
lines
on
HIV
test
ing
serv
ices
(J
uly
2015
) ht
tp://
ww
w.w
ho.in
t/hi
v/pu
b/gu
idel
ines
/hiv
-te
stin
g-se
rvic
es/e
n/CL
IA/E
CL
(aut
omat
ed
inst
rum
ent)
Seru
mPl
asm
a

First WHO Model List of Essential In Vitro Diagnostics
29
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
HIV
in
fect
ion
cont
inue
d
WH
O im
plem
enta
tion
tool
for p
re-e
xpos
ure
prop
hyla
xis
(PrE
P) o
f HIV
in
fect
ion,
mod
ule
10 fo
r te
stin
g pr
ovid
ers
(201
7)
http
://w
ww
.who
.int/
hiv/
pub/
prep
/pre
p-im
plem
enta
tion-
tool
/en/
For s
cree
ning
fo
r HIV
in th
e bl
ood
supp
ly
and
in b
lood
pr
oduc
ts.
EIA
(m
icro
plat
e)
Man
ual
met
hod
Seru
m
Plas
ma
Scre
enin
g do
nate
d bl
ood
for t
rans
fusi
on
tran
smis
sibl
e in
fect
ions
: Re
com
men
datio
ns (2
009)
http
://ap
ps.w
ho.in
t/iri
s/
bits
trea
m/h
andl
e/10
665/
44
202/
9789
2415
4788
8_
eng.
pdf?
sequ
ence
= 1&
isA
llow
ed=y
CLIA
/ECL
(a
utom
ated
in
stru
men
t)
Seru
m
Plas
ma
Com
bine
d H
IV a
ntib
ody/
p24
antig
en
(ant
i-HIV
/p24
Ag
) tes
t
For t
he
diag
nosi
s of
HIV
in
fect
ion:
adu
lts,
adol
esce
nts,
child
ren
and
infa
nts
> 18
m
onth
s of
age
RDT
Veno
us
who
le b
lood
Plas
ma
Seru
m
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
hiv-
rdts
/pub
lic_r
epor
t/en
/)
Cons
olid
ated
gui
delin
es
on H
IV te
stin
g se
rvic
es
(201
5)
http
://ap
ps.w
ho.in
t/iri
s/
bits
trea
m/h
andl
e/10
665/
17
9870
/978
9241
5089
26_
eng.
pdf?
sequ
ence
=1

30
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
HIV
in
fect
ion
cont
inue
d
EIA
(m
icro
plat
e)
Man
ual
met
hod
Seru
mPl
asm
a
CLIA
/ECL
(a
utom
ated
in
stru
men
t)
Seru
mPl
asm
a
For s
cree
ning
fo
r HIV
in th
e bl
ood
supp
ly
and
in b
lood
pr
oduc
ts
EIA
(m
icro
plat
e)
Man
ual
met
hod
Seru
mPl
asm
aSc
reen
ing
dona
ted
bloo
d fo
r tra
nsfu
sion
tr
ansm
issi
ble
infe
ctio
ns:
Reco
mm
enda
tions
(200
9)ht
tp://
apps
.who
.int/
iris/
bits
trea
m/h
andl
e/10
665/
44
202/
9789
2415
4788
8_
eng.
pdf?
sequ
ence
= 1&
isA
llow
ed=y
CLIA
/ECL
(a
utom
ated
in
stru
men
t)
Seru
mPl
asm
a
Qua
litat
ive
or
quan
titat
ive
viro
logi
cal t
est
For d
iagn
osis
of
HIV
infe
ctio
n in
infa
nts
< 18
m
onth
s of
age
Nuc
leic
ac
id te
stCa
pilla
ry
who
le b
lood
Veno
us
who
le b
lood
Drie
d bl
ood
spot
Seru
mPl
asm
a
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
hiv-
vrl/p
ublic
_rep
ort/
en/)
Cons
olid
ated
gu
idel
ines
on
the
use
of
antir
etro
vira
l dru
gs fo
r tr
eatin
g an
d pr
even
ting
HIV
infe
ctio
n (2
016)
http
://w
ww
.who
.int/
hiv/
pub/
arv/
arv-
2016
/en/

First WHO Model List of Essential In Vitro Diagnostics
31
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
HIV
in
fect
ion
cont
inue
d
Qua
ntita
tive
viro
logi
cal t
est
Mon
itorin
g re
spon
se
to a
ntiv
iral
trea
tmen
t
Nuc
leic
ac
id te
stD
ried
bloo
d sp
ot
Seru
m
Plas
ma
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
hiv-
vrl/p
ublic
_rep
ort/
en/)
CD4
cell
enum
erat
ion
(qua
ntita
tive)
For s
tagi
ng
adva
nced
HIV
di
seas
e
Flow
cy
tom
etry
Capi
llary
w
hole
blo
od
Veno
us
who
le b
lood
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
hiv-
vrl/p
ublic
_rep
ort/
en/)
Cryp
toco
ccal
an
tigen
test
Fo
r scr
eeni
ng
and
diag
nosi
s of
cry
ptoc
occa
l m
enin
gitis
in
peop
le li
ving
w
ith a
dvan
ced
HIV
dis
ease
RDT
Cere
bros
pina
l flu
id
Veno
us w
hole
bl
ood
Seru
m
Plas
ma
Gui
delin
es fo
r the
di
agno
sis,
prev
entio
n,
and
man
agem
ent o
f cr
ypto
cocc
al d
isea
se
in H
IV-in
fect
ed a
dults
, ad
oles
cent
s an
d ch
ildre
n (2
018)
ht
tp://
apps
.who
.int/
iris/
bi
tstr
eam
/han
dle/
1066
5/
2603
99/9
7892
4155
0277
- en
g.pd
f?se
quen
ce=1
EIA
Cere
bros
pina
l flu
id
Seru
m
Plas
ma
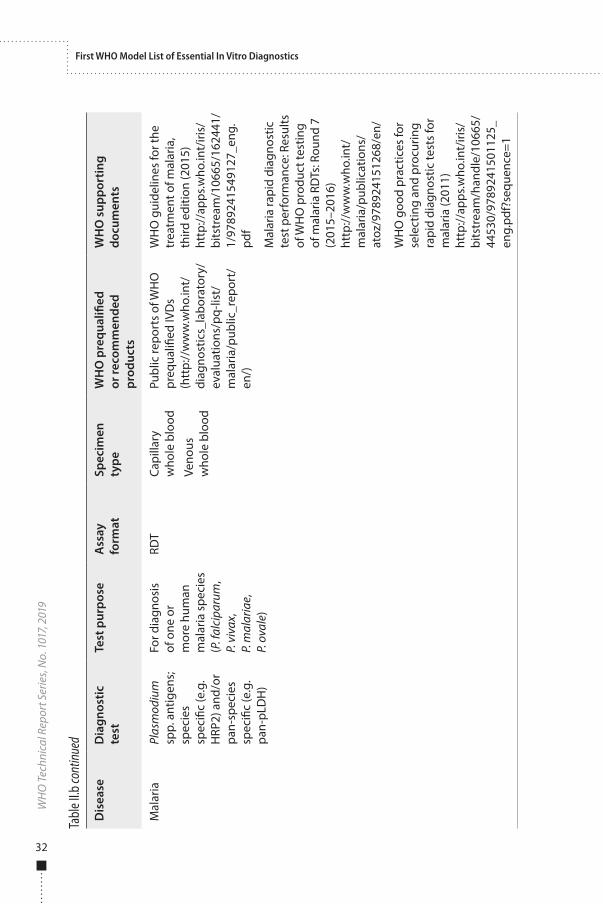
32
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
Mal
aria
Plas
mod
ium
sp
p. a
ntig
ens;
sp
ecie
s sp
ecifi
c (e
.g.
HRP
2) a
nd/o
r pa
n-sp
ecie
s sp
ecifi
c (e
.g.
pan-
pLD
H)
For d
iagn
osis
of
one
or
mor
e hu
man
m
alar
ia s
peci
es
(P. f
alci
paru
m,
P. v
ivax
, P.
mal
aria
e,
P. o
vale
)
RDT
Capi
llary
w
hole
blo
od
Veno
us
who
le b
lood
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
mal
aria
/pub
lic_r
epor
t/en
/)
WH
O g
uide
lines
for t
he
trea
tmen
t of m
alar
ia,
third
edi
tion
(201
5)ht
tp://
apps
.who
.int/
iris/
bits
trea
m/1
0665
/162
441/
1/
9789
2415
4912
7_en
g.
Mal
aria
rapi
d di
agno
stic
te
st p
erfo
rman
ce: R
esul
ts
of W
HO
pro
duct
test
ing
of m
alar
ia R
DTs
: Rou
nd 7
(2
015–
2016
)ht
tp://
ww
w.w
ho.in
t/
mal
aria
/pub
licat
ions
/ at
oz/9
7892
4151
268/
en/
WH
O g
ood
prac
tices
for
sele
ctin
g an
d pr
ocur
ing
rapi
d di
agno
stic
test
s fo
r m
alar
ia (2
011)
ht
tp://
apps
.who
.int/
iris/
bi
tstr
eam
/han
dle/
1066
5/
4453
0/97
8924
1501
125_
en
g.pd
f?se
quen
ce=1

First WHO Model List of Essential In Vitro Diagnostics
33
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
Mal
aria
cont
inue
dPl
asm
odiu
m
spp.
For d
iagn
osis
of
one
or
mor
e hu
man
m
alar
ia s
peci
es
(P. f
alci
paru
m,
P. v
ivax
, P.
mal
aria
e,
P. o
vale
and
P.
kno
wle
si) a
nd
mon
itorin
g re
spon
se to
tr
eatm
ent
Ligh
t m
icro
scop
yCa
pilla
ry
who
le b
lood
Veno
us
who
le b
lood
WH
O g
uide
lines
for t
he
trea
tmen
t of m
alar
ia,
third
edi
tion
(201
5)ht
tp://
apps
.who
.int/
iris/
bi
tstr
eam
/106
65/1
6244
1/
1/97
8924
1549
127_
eng.
pd
f
Basi
c m
alar
ia m
icro
scop
y Pa
rt I:
Lea
rner
’s gu
ide
(201
0)
http
://ap
ps.w
ho.in
t/iri
s/
bits
trea
m/h
andl
e/10
665/
44
208/
9789
2415
4782
6_
eng.
pdf?
sequ
ence
=1
Mal
aria
mic
rosc
opy
stan
dard
ope
ratin
g pr
oced
ures
(201
5)ht
tp://
ww
w.w
pro.
who
. in
t/m
vp/la
b_qu
ality
/ m
m_s
op/e
n/

34
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
Mal
aria
cont
inue
dG
luco
se-6
-ph
osph
ate
dehy
drog
enas
e ac
tivity
(G6P
D)
To d
eter
min
e G
6PD
act
ivity
(n
orm
al,
inte
rmed
iate
, de
ficie
nt) a
nd
spec
ifica
lly to
in
form
dec
isio
n to
adm
inis
ter 8
- am
inoq
uino
line
grou
p dr
ugs
for
radi
cal c
ure
of
P. v
ivax
For s
cree
ning
ne
wbo
rns
for
G6P
D d
efici
ency
Sem
i qu
antit
ativ
e flu
ores
cent
sp
ot te
st
Veno
us
who
le b
lood
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
mal
aria
/pub
lic_r
epor
t/en
/)
Beut
ler E
, Blu
me
KG,
Kapl
an JC
, Loh
r GW
, Ra
mot
B, V
alen
tine
WN
. In
tern
atio
nal C
omm
ittee
fo
r Sta
ndar
diza
tion
in H
aem
atol
ogy:
Re
com
men
ded
scre
enin
g te
st fo
r gl
ucos
e-6-
phos
phat
e de
hydr
ogen
ase
defic
ienc
y. B
r J H
aem
atol
19
79;4
3:46
9–47
7W
HO
gui
delin
es fo
r the
tr
eatm
ent o
f mal
aria
, th
ird e
ditio
n (2
015)
http
://ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/106
65/1
6244
1/
1/97
8924
1549
127_
eng.
pd
f

First WHO Model List of Essential In Vitro Diagnostics
35
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
*
WH
O s
uppo
rtin
g do
cum
ents
Tube
rcul
osis
Myc
obac
teriu
m
tube
rcul
osis
ba
cter
ia
For d
iagn
osis
an
d tr
eatm
ent
mon
itorin
g of
ac
tive
TB
Mic
rosc
opy
Oth
er
spec
imen
ty
pes
Impl
emen
ting
tube
rcul
osis
dia
gnos
tics:
Po
licy
fram
ewor
k (2
015)
ht
tp://
apps
.who
.int/
iris/
bits
trea
m/1
0665
/ 16
2712
/1/9
7892
4150
8 61
2_en
g.pd
f
Com
pend
ium
of W
HO
gu
idel
ines
and
ass
ocia
ted
stan
dard
s: E
nsur
ing
optim
um d
eliv
ery
of
the
casc
ade
of c
are
for
patie
nts
with
tube
rcul
osis
(2
017)
http
://ap
ps.w
ho.in
t/iri
s/
bits
trea
m/h
andl
e/10
665/
25
9180
/978
9241
5125
72-
eng.
pdf?
sequ
ence
=1
Impl
emen
ting
tube
rcul
osis
dia
gnos
tics:
Po
licy
fram
ewor
k (2
015)
ht
tp://
apps
.who
.int/
iris/
bits
trea
m/1
0665
/162
712/
1/
9789
2415
0861
2_en
g.
For d
iagn
osis
an
d tr
eatm
ent
mon
itorin
g of
act
ive
TB
incl
udin
g dr
ug-
resi
stan
t TB
Bact
eria
l cu
lture
Sput
um
or o
ther
sp
ecim
en
type
s
* All
TB te
sts a
re e
valu
ated
and
gui
delin
es d
evel
oped
thro
ugh
the
WHO
Glo
bal T
B Pr
ogra
mm
e.

36
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
*
WH
O s
uppo
rtin
g do
cum
ents
Tube
rcul
osis
co
ntin
ued
M. t
uber
culo
sis
DN
AFo
r dia
gnos
is
of a
ctiv
e TB
and
si
mul
tane
ous
dete
ctio
n of
rif
ampi
cin
resi
stan
ce
Cart
ridge
-ba
sed
nucl
eic
acid
te
st
Sput
um
or e
xtra
-pu
lmon
ary
tube
rcul
osis
sp
ecim
en
type
s
WH
O M
eetin
g re
port
of
a te
chni
cal e
xper
t co
nsul
tatio
n: N
on-
infe
riorit
y an
alys
is o
f Xp
ert M
TB/R
IF U
ltra
com
pare
d to
Xpe
rt M
TB/
RIF
(201
7)ht
tp://
apps
.who
.in
t/iri
s/bi
tstr
eam
/ha
ndle
/106
65/2
5479
2/W
HO
-HTM
-TB-
2017
.04-
eng.
pdf;j
sess
ioni
d=E0
2D09
9493
0ED
BD9A
4BC5
BB3D
3A28
568?
sequ
ence
=1
Auto
mat
ed re
al-t
ime
nucl
eic
acid
am
plifi
catio
n te
chno
logy
for r
apid
and
si
mul
tane
ous
dete
ctio
n of
tube
rcul
osis
and
rif
ampi
cin
resi
stan
ce:
Polic
y up
date
(201
3)ht
tp://
apps
.who
.int/
iris/
bits
trea
m/1
0665
/112
472/
1/
9789
2415
0633
5_en
g.
* All
TB te
sts a
re e
valu
ated
and
gui
delin
es d
evel
oped
thro
ugh
the
WHO
Glo
bal T
B Pr
ogra
mm
e.

First WHO Model List of Essential In Vitro Diagnostics
37
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
*
WH
O s
uppo
rtin
g do
cum
ents
Tube
rcul
osis
co
ntin
ued
M. t
uber
culo
sis
DN
A
mut
atio
ns
asso
ciat
ed
with
re
sist
ance
For d
etec
tion
of re
sist
ance
for
first
-line
ant
i-TB
med
icin
es
Mol
ecul
ar
line
prob
e as
say
(LPA
)
Sput
umTh
e us
e of
mol
ecul
ar
line
prob
e as
says
for t
he
dete
ctio
n of
resi
stan
ce to
is
onia
zid
and
rifam
pici
n:
Polic
y up
date
(201
6)
http
://ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/106
65/
2505
86/1
/978
9241
511
261-
eng.
pdf?
ua=1
M. t
uber
culo
sis
DN
A
mut
atio
ns
asso
ciat
ed
with
re
sist
ance
For d
etec
tion
of re
sist
ance
fo
r sec
ond-
line
anti-
TB
med
icin
es
Mol
ecul
ar
line
prob
e as
say
(LPA
)
Sput
umTh
e us
e of
mol
ecul
ar
line
prob
e as
says
for t
he
dete
ctio
n of
resi
stan
ce
to s
econ
d-lin
e an
ti-tu
berc
ulos
is d
rugs
: Po
licy
upda
te (2
016)
http
://ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/han
dle/
1066
5/
2461
31/9
7892
4151
0561
-en
g.pd
f?se
quen
ce=1
* All
TB te
sts a
re e
valu
ated
and
gui
delin
es d
evel
oped
thro
ugh
the
WHO
Glo
bal T
B Pr
ogra
mm
e.

38
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
*
WH
O s
uppo
rtin
g do
cum
ents
Tube
rcul
osis
co
ntin
ued
Dru
g su
scep
tibili
ty
test
ing
in
M. t
uber
culo
sis
cultu
re
To d
etec
t re
sist
ance
to
first
-line
and
/or
sec
ond-
line
anti-
TB
med
icin
es
Dru
g su
scep
tibili
ty
test
ing
(DST
)
Bact
eria
l cu
lture
of
M. t
uber
culo
sis
Tech
nica
l rep
ort o
n cr
itica
l con
cent
ratio
ns
for d
rug
susc
eptib
ility
te
stin
g of
med
icin
es
used
in th
e tr
eatm
ent
of d
rug-
resi
stan
t tu
berc
ulos
is (2
018)
http
://w
ww
.who
.int/
tb/p
ublic
atio
ns/2
018/
WH
O_t
echn
ical
_re
port
_con
cent
ratio
ns_
TB_d
rug_
susc
eptib
ility
/en
/
* All
TB te
sts a
re e
valu
ated
and
gui
delin
es d
evel
oped
thro
ugh
the
WHO
Glo
bal T
B Pr
ogra
mm
e.

First WHO Model List of Essential In Vitro Diagnostics
39
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
*
WH
O s
uppo
rtin
g do
cum
ents
Tube
rcul
osis
co
ntin
ued
Lipo
arab
ino-
m
anna
n (L
AM
) ant
igen
To a
id in
the
diag
nosi
s of
TB
in s
erio
usly
ill
HIV
-pos
itive
in
patie
nts
RDT
Urin
eTh
e us
e of
la
tera
l flow
urin
e lip
oara
bino
man
nan
assa
y (L
F-LA
M) f
or th
e di
agno
sis
and
scre
enin
g of
act
ive
tube
rcul
osis
in
peop
le li
ving
with
HIV
: Po
licy
upda
te (2
015)
http
://ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/han
dle/
1066
5/19
3633
/978
9241
5096
33_
eng.
pdf;j
sess
ioni
d=9A
9EB8
86D
C176
58BF
7 FD
F867
58D
7A9F
9?se
quen
ce=1
* All
TB te
sts a
re e
valu
ated
and
gui
delin
es d
evel
oped
thro
ugh
the
WHO
Glo
bal T
B Pr
ogra
mm
e.

40
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
*
WH
O s
uppo
rtin
g do
cum
ents
Tube
rcul
osis
co
ntin
ued
Imm
une
resp
onse
Fo
r dia
gnos
is
of la
tent
TB
infe
ctio
n
Inte
rfer
on
gam
ma
rele
ase
assa
y (IG
RA)
Veno
us
who
le b
lood
Late
nt T
B In
fect
ion:
U
pdat
ed a
nd
cons
olid
ated
gui
delin
es
for p
rogr
amm
atic
m
anag
emen
t (20
18)
http
://ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/han
dle/
1066
5/26
0233
/978
9241
5502
39-
eng.
pdf;j
sess
ioni
d=6D
1BB2
4631
2B37
8ACF
E BF
9BFF
AFE
B0ED
?se
quen
ce=1
* All
TB te
sts a
re e
valu
ated
and
gui
delin
es d
evel
oped
thro
ugh
the
WHO
Glo
bal T
B Pr
ogra
mm
e.

First WHO Model List of Essential In Vitro Diagnostics
41
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
HPV
in
fect
ion
Hum
an
papi
llom
aviru
s (H
PV) n
ucle
ic
acid
For c
ervi
cal
canc
er
scre
enin
g
Nuc
leic
ac
id te
stCe
rvic
al c
ells
co
llect
ed in
te
st s
peci
fic
tran
spor
t flu
id
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/pq-
list/
publ
ic_r
epor
t_hp
v/en
/)
WH
O h
uman
pa
pillo
mav
irus
labo
rato
ry m
anua
l, fir
st
editi
on (2
009)
http
://ap
ps.w
ho.
int/
iris/
bits
trea
m/
hand
le/1
0665
/705
05/
WH
O_I
VB_1
0.12
_eng
.pd
f?se
quen
ce=1
Syph
ilis
Ant
ibod
ies
to
Trep
onem
a pa
llidu
m
For d
iagn
osis
or
as
an a
id in
th
e di
agno
sis
of T
. pal
lidum
RDT
Veno
us
who
le b
lood
Plas
ma
Seru
m
Publ
ic re
port
s of
WH
O
preq
ualifi
ed IV
Ds
(htt
p://
ww
w.w
ho.in
t/di
agno
stic
s_la
bora
tory
/ev
alua
tions
/PQ
_lis
t/en
/)
WH
O la
bora
tory
di
agno
sis
of s
exua
lly
tran
smitt
ed in
fect
ions
, in
clud
ing
hum
an
imm
unod
efici
ency
viru
s (2
013)
ht
tp://
apps
.who
.int/
iris/
bits
trea
m/h
andl
e/10
665/
8534
3/97
8924
1505
840_
eng.
pdf?
sequ
ence
=1
EIA
(M
icro
plat
e)
Man
ual
met
hod
Seru
m
Plas
ma
CLIA
/ECL
(a
utom
ated
in
stru
men
t)
Seru
m
Plas
ma

42
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Tabl
e II.b
continued
Dis
ease
Dia
gnos
tic
test
Test
pur
pose
Ass
ay
form
atSp
ecim
en
type
WH
O p
requ
alifi
ed
or re
com
men
ded
prod
ucts
WH
O s
uppo
rtin
g do
cum
ents
Syph
ilis
cont
inue
dFo
r scr
eeni
ng
bloo
d an
d bl
ood
prod
ucts
EIA
(M
icro
plat
e)
Man
ual
met
hod
Seru
m
Plas
ma
Scre
enin
g do
nate
d bl
ood
for t
rans
fusi
on
tran
smis
sibl
e in
fect
ions
(2
009)
http
://ap
ps.w
ho.in
t/iri
s/
bits
trea
m/h
andl
e/10
665/
44
202/
9789
2415
4788
8_
eng.
pdf?
sequ
ence
= 1&
isA
llow
ed=y
Com
bine
d an
tibod
ies
to T
. pal
lidum
an
d to
HIV
-1/
2 (a
nti-H
IV)
For t
he
diag
nosi
s or
as
an a
id in
the
diag
nosi
s of
H
IV-1
/2 a
nd/o
r T.
pal
lidum
RDT
Veno
us
who
le b
lood
Plas
ma
Seru
m
http
://w
ww
.who
.int/
diag
nost
ics_
labo
rato
ry/
eval
uatio
ns/p
q-lis
t/hi
v-rd
ts/p
ublic
_rep
ort/
en/
WH
O In
form
atio
n no
te
on th
e us
e of
dua
l HIV
/sy
phili
s ra
pid
diag
nost
ic
test
s (R
DT)
(201
7)ht
tp://
apps
.who
.in
t/iri
s/bi
tstr
eam
/ha
ndle
/106
65/2
5284
9/W
HO
-RH
R-17
.01-
eng.
pdf?
sequ
ence
=1

43
3. Methods used to establish the List3.1 Strategic Advisory Group of Experts on In Vitro DiagnosticsIn March 2017, the WHO Expert Committee on Selection and Use of Essential Medicines recommended that an EDL be developed. In support of that recommendation, WHO created an EDL Secretariat, which drafted the first edition of the EDL in consultation with WHO disease programmes. A strategic technical advisory group of experts (SAGE IVD)3 was then established to advise WHO on the in vitro diagnostics to be included. The terms of reference of the group were as follows:
1. Serve as a principal advisory group to the WHO Director-General on all aspects of IVDs.4
2. For priority, essential and neglected IVDs, where no established advisory mechanisms exist, the SAGE IVD will:a. provide technical advice on global policies and strategies,
ranging from development, assessment, use of IVDs and their linkages with other health interventions;
b. advise on the adequacy of progress towards the achievement of IVDs-related goals set in the World Health Assembly resolutions;
c. recommend policies for long-term and integrated diagnostic capabilities as indispensable element for universal health coverage and global public health security;
d. suggest guiding principles for how, when and where to use particular IVDs in national, regional and global settings;
e. review the pipeline of existing and innovative IVDs for noncommunicable diseases, rare diseases and infectious diseases, including for emerging pathogens and existing public health conditions of international concern, and identify major gaps;
3 All introductory and background material, including the terms of reference of the SAGE IVD, are available on the WHO website (http://www.who.int/medical_devices/diagnostics/back-doc_WHO-model-list-essential-diagnostics-updt.pdf ).
4 Except where policy and technical recommendations on IVD are provided through WHO established advisory mechanisms, such as for HIV, tuberculosis and malaria. For these, SAGE IVD would accept such recommendations without further review and incorporate such advice in its consideration of organization-wide policies.

44
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
f. provide high level advice on development and maintenance of appropriate standards for IVDs, including methodologies for evidence review;
g. provide advice to WHO Secretariat for the development of the List of Essential Diagnostics (EDL) and in line with the work of the Expert Committee on Selection and Use of Essential Medicines.
h. provide advice on WHO activities in the area of IVDs, including engagement of WHO in partnerships in the development, access and use of needed IVDs.
The terms of reference were approved by the Director-General of WHO and posted on the WHO website with a call for candidates. The applications were reviewed by the EDL Secretariat and sent for approval to the Director-General. The 19 members of the SAGE IVD were selected with due attention to regional, professional and gender balance. SAGE IVD operated with its current membership until September 2018, and the Group agreed to hold monthly teleconferences until that time to discuss matters related to the EDL. A new SAGE IVD will be convened for each review of the EDL, some members being replaced each time.
3.2 Selection of IVDs for inclusion in the first EDLThe EDL Secretariat prepared a draft list of IVDs in collaboration with WHO departments that had assessed in vitro diagnostic tests for HIV, malaria, tuberculosis and syphilis, defined as categories of tests for identifying specific biological markers. The EDL Secretariat also reviewed WHO guidance, disease-specific clinical and diagnostic guidelines, technical manuals, and the WHO priority medical devices list.5 They also considered the tests listed by WHO Prequalification of In Vitro Diagnostics and in other WHO IVD assessments.
The draft list was posted for public consultation in March 2018. The comments received from the consultation were analysed by the EDL Secretariat and integrated into a list presented to the SAGE IVD at its first meeting, on 16–20 April 2018 at WHO headquarters in Geneva, Switzerland. The work of the SAGE IVD takes place in the context of WHO’s commitment to transparent, evidence-based decision-making. Annex 1 lists the participants at the first meeting of the SAGE IVD, and Annex 2 lists their declarations of interest.
The first SAGE IVD was asked to make recommendations to the EDL Secretariat on:
■ principles that should guide preparation of the EDL;
5 WHO documents reviewed to compile and propose the general laboratory tests for the first EDL are listed under “Sources used for general laboratory test”.

Methods used to establish the List
45
■ integration of the EDL with existing WHO work on IVDs; ■ the draft first EDL proposed by the Secretariat; ■ procedures for revising the EDL, including methods for assessing
candidate IVDs for inclusion, priorities for inclusion of IVDs in subsequent Lists and procedures for addressing applications for inclusion or deletion; and
■ integrating user feedback and adapting the EDL for national lists.
SAGE IVD designated IVDs that should be available in primary health care settings where laboratories are not available and those that should be available in laboratories, hospitals and reference laboratories.
3.3 Principles that should guide preparation of the EDLThe EDL comprises IVDs, a subset of medical devices intended for examination in vitro of specimens taken from the human body. For the purposes of the EDL, “IVD” refers to categories of tests for identifying specific biological markers and not to individual tests. For example, as several tests are available for measuring HIV load, the IVD for “HIV load” refers to a category of tests for measuring this end-point. The word “test” is used interchangeably with “assay” to refer to laboratory assays and rapid diagnostic tests. Further, the word “sample” is used interchangeably with “specimen”.
The proposed procedure for preparing the EDL was based on experience in preparing the WHO Model List of Essential Medicines, which suggested that the best approach would be to include tests associated with WHO priority diseases, for which there is robust evidence and which are well covered by WHO guidelines for use; these would be complemented by a set of general laboratory tests described in WHO publications.6 The list will be reviewed annually, with the addition or deletion of items as appropriate. On principle, it was proposed that IVDs be added or deleted according to an evidence-based, public health approach, as little evidence may be available for certain types of tests and in certain countries, especially in low- and middle-income countries.
The first SAGE IVD endorsed the aim of the EDL, to offer wide-ranging benefits to health care systems by:
■ prioritizing laboratory testing and infrastructure; ■ bulk and advance purchasing of IVDs to increase affordability; ■ improving laboratory capacity, organization, sample processing and
other aspects to improve responses to public health emergencies;
6 WHO documents reviewed to compile and propose the general lab tests for the first draft EDL are listed in the reference section under WHO sources for general laboratories

46
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
■ helping IVD designers and manufacturers to develop new or improved IVDs, including through target product profiles; and
■ supporting the rational use of medicines in the WHO Model List of Essential Medicines.
The SAGE IVD agreed on the core principle of prioritizing IVDs required for progress towards universal health coverage. The Group also agreed that the EDL should, in principle, include IVDs recommended by or necessary for implementation of WHO guidelines. It noted, however, that some publications are out of date and recommended revision of the WHO technical documents that constitute resources for EDL as a priority.
The SAGE IVD identified four main themes in preparation of the EDL.
1. The scope must be clearly defined.2. The EDL should indicate the tests and laboratory infrastructure
that are appropriate for different levels of health care delivery.3. The results of clinical studies indicate treatment decisions and
not the direct result of test performance and cannot be used as evidence to support the use of IVDs.
4. The EDL should not be read in isolation, because diagnostic tests are part of an entire system of diagnostics delivery, which includes training, laboratory infrastructure, quality assurance and supply chain management.
An executive summary, which included the initial version of the List, was published on the WHO website in May 2018. After identification of several minor errors by SAGE IVD members and the EDL secretariat, a corrected version was posted in November 2018. The List included in this publication, which has further minor corrections, is the definitive first WHO Model List of Essential In Vitro Diagnostics and replaces the two previous versions.
3.4 Draft first EDL proposed by the SecretariatThe SAGE IVD considered the subjects summarized above and a first draft of the EDL.
The SAGE IVD endorsed the procedure that was used to draft the first EDL and concluded that the EDL should have three components.
■ A preface describing the scope and objectives and instructions for users, including the appropriate level of the health care system in which tests should be used, how tests were selected for inclusion on the EDL, the relation between EDL and prequalification and any necessary disclaimers.

Methods used to establish the List
47
■ A chart of the laboratory tests chosen for inclusion, consisting of IVD tests for physiological evaluation of patients and detection and diagnosis of diseases and IVD tests for the detection, diagnosis and monitoring of WHO priority diseases: HIV infection, TB, malaria, hepatitis B, hepatitis C, syphilis and HPV infection. The list will include links to WHO technical information.
■ Procedures for revising the EDL, including methods for assessing candidate IVDs for inclusion, priorities for inclusion of IVDs in subsequent EDLs and procedures for addressing applications for inclusion or deletion
The SAGE IVD discussed how the EDL should be structured, the process to be used in considering applications for addition or deletion of tests, the collection and assessment of evidence about IVDs and assessment of the utility of the EDL for its target audience.
3.4.1 Method for assessing IVDs for inclusion or deletion The SAGE IVD considered the methods used to assess IVDs in WHO disease programmes and suggestions for optimizing methods for future editions of the EDL. The Group also considered the importance of avoiding methodological requirements that render assessment of applications technically demanding or create inequitable obstacles to submissions from stakeholders with limited resources.
The SAGE IVD agreed that in all cases there should be:
■ a systematic summary of evidence, with systematic reviews of test accuracy performed with accepted methods;
■ assessment of the strength and limitations of the evidence, including significant aspects for which evidence is lacking; and
■ consideration of the generalizability of evidence, particularly to low-resource settings.
The SAGE IVD also agreed that:
■ assessment of the clinical accuracy of a test in the setting in which it would be used will generally be required;
■ the required accuracy of a tests will be difficult to decide, given that clinical accuracy depends on reference standards, patient populations and testing protocols;
■ randomized controlled clinical trials are not necessarily applicable for assessing the performance of IVDs; and

48
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
■ evidence of impact on disease detection and management may be easier to obtain and more useful than evidence of impact on patient outcomes.
3.4.2 Identification of high-priority IVDs for the EDLThe SAGE IVD considered a proposal for identifying high-priority candidate IVDs by reference to WHO disease priorities. Relevant WHO staff and the SAGE IVD discussed areas of high clinical priority that might guide prioritization of candidate IVDs for inclusion in future editions of the EDL. The areas were:
■ antimicrobial resistance ■ fungal disease ■ influenza ■ reproductive health ■ neglected tropical diseases ■ public health emergencies ■ noncommunicable diseases.
Antimicrobial resistanceThe Global Antimicrobial Resistance Surveillance System (GLASS) was launched in 2015 for collaboration in surveillance of antimicrobial resistance by standardized collection of data on patients and populations from national surveillance sites. GLASS has drawn up a list of essential IVDs for the identification and testing of eight priority pathogens for antimicrobial susceptibility: Escherichia coli, Klebsiella pneumoniae, Acinetobacter baumannii, Staphylococcus aureus, Streptococcus pneumoniae, Salmonella spp., Shigella spp. and Neisseria gonorrhoeae.
Fungal diseasesFungi that cause opportunistic infections in patients with HIV/AIDS were discussed, particularly cryptococcal meningitis, Pneumocystis pneumonia, disseminated histoplasmosis and aspergillosis complicating pulmonary TB.
InfluenzaThe gold standard in testing is polymerase chain reaction, for which there are a number of commercial kits. The Centers for Disease Control and Prevention in the USA (USCDC) has an in-house test that is updated regularly; primers and probes are made available only to national reference laboratories and public health laboratories.

Methods used to establish the List
49
Reproductive healthThe priority IVDs for reproductive health are point-of-care tests for syphilis, HPV infection and N. gonorrhoeae. WHO recommends that all pregnant women be screened for syphilis as part of the universal health coverage package. HPV testing and treatment of pre-cancerous cervical lesions are also part of the package for women, and WHO will launch a campaign on HPV testing in 2018. Point-of-care testing for N. gonorrhoeae is considered important to ensure appropriate selection of antibiotic.
Neglected tropical diseasesWHO focuses on three neglected tropical diseases: dengue, visceral leishmaniasis and schistosomiasis and soil-transmitted helminths. These infections present a range of challenges for health care: outbreak management for dengue, elimination and case management for leishmaniasis and mass drug administration for schistosomiasis and soil-transmitted helminths. For each disease, there is either a test for which performance has been assessed or a recent “diagnostic landscape” document.
Public health emergenciesThe emergencies addressed by WHO are cholera, Ebola virus disease, Lassa virus disease, Marburg virus disease, meningitis, Middle East respiratory syndrome coronavirus disease, plague, severe acute respiratory syndrome and yellow fever. The responsible technical group did not propose inclusion of IVDs for these diseases in the first EDL. It plans comprehensive mapping of IVDs for 35 diseases of concern and consultation with the United Nations Children’s Fund, Médecins Sans Frontières (MSF), USCDC, the International Federation of Red Cross and Red Crescent Societies, the United States Agency for International Development and the Department for International Development in the United Kingdom with a view to submitting candidate tests for the 2019 and 2020 editions of the EDL.
Noncommunicable diseasesThe priority is IVDs for cancer that can be widely used in low- and middle-income countries. At present, diagnosis of cancer requires anatomical pathology services, which are often weak or lacking in resource-poor settings. Screening tests for several cancers allow effective, affordable treatment of early-stage disease. These are cancers of the breast, cervix (HPV testing) and colo-rectum (faecal immunochemical tests in stool).
SAGE IVD agreed that the above list of priority conditions, with the addition of sepsis, could usefully guide prioritization of IVDs for inclusion in

50
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
the next editions of EDL. With regard to antimicrobial resistance, SAGE IVD agreed that the GLASS list of priority pathogens for surveillance should guide assessment of candidate IVDs for the EDL.

51
4. Integration of the EDL with other WHO initiativesThe SAGE IVD identified groups within WHO that are conducting work relevant to that of the SAGE IVD and agreed on the importance of coordinating the work.
WHO Expert Committee on Biological StandardizationThe WHO Constitution requires the Organization “to develop, establish and promote international standards with respect to biological and pharmaceutical products”. For this purpose, WHO has established expert committees, including the Expert Committee on Biological Standardization. The Committee has published a number of written standards on IVDs, invited discussion with the SAGE IVD and noted that it looked forward to discussing the report of the first SAGE IVD meeting at the meeting of the Committee in October 2018.
The SAGE IVD agreed that it should establish regular, formal communication with the Expert Committee on Biological Standardization on matters of common concern.
WHO priority status of HIV, tuberculosis, malaria, viral hepatitis, syphilis and human papillomavirusIt was proposed that the first EDL include tests relevant to WHO priority diseases – HIV infection, tuberculosis, malaria, viral hepatitis B and C, syphilis and HPV infection – for which there are WHO guidelines and technical reports, including recommendations for the IVDs to be used. The SAGE IVD considered:
■ the IVDs recommended for each of these diseases and the reasons for the recommendations;
■ the evaluation process used to recommend the tests; ■ how guidelines for testing and treatment in each disease were
developed, including evidence retrieval, assessment and synthesis; ■ how the recommendations are formulated; and ■ whether “grading of recommendations assessment, development
and evaluation” (GRADE) was used, when applicable, to assess the quality of evidence from studies for formulating recommendations.
The SAGE IVD agreed that:
■ existing recommendations for IVD use in the proposed WHO priority disease areas would form the basis for inclusion of IVDs in the first edition of the EDL;

52
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
■ testing for cryptococcal antigen in blood and cerebrospinal fluid would be included in the HIV section; and
■ tests included in the EDL should be commercially available.
General laboratory testsA second area proposed for inclusion in the first EDL was general core and routine laboratory tests for clinical chemistry, haematology, blood transfusion, microbiology (virology, bacteriology, parasitology and mycology) and histopathology. For the first EDL, the tests proposed to the SAGE IVD were selected on the basis of the scientific validity of an analyte, i.e. the association between an analyte and a clinical condition or physiological state; and clinical utility. Many of these tests are required for effective management of patients with the high-priority diseases listed above and have already been described in WHO publications.7
The SAGE IVD agreed to include the proposed list of general laboratory tests in the first EDL.
WHO Prequalification of In Vitro Diagnostics The EDL and the list of the WHO Prequalification of In Vitro Diagnostics are complementary and distinct. The Prequalification lists include high-priority IVDs that have been assessed by WHO and are identified by brand (in contrast to the EDL, which lists categories of IVDs). Currently, the Prequalification lists has a narrower scope than the EDL. The inclusion of a category of tests on the Prequalification list is not a requirement for it to be considered for inclusion on the EDL. In the context of the EDL, the Prequalification lists should be considered a resource, as they list prequalified brands of products that correspond to certain categories of tests in the EDL. Relevant links are provided in the EDL.
The SAGE IVD noted that WHO prequalification plays an important role in increasing access to IVDs of assured quality, safety and performance. The Group affirmed that the EDL and the WHO programme for prequalification are complementary in improving access of Member States to IVDs.
The Prequalification of In Vitro Diagnostics requested guidance from the SAGE IVD with respect to its proposed process for selecting IVDs for review, which comprised the:
■ burden of disease associated with the target condition;
7 WHO documents reviewed to compile and propose the general lab tests for the first draft EDL are listed in the reference section under WHO sources for general laboratories

Integration of the EDL with other WHO initiatives
53
■ health interventions associated with the IVD; ■ existence of WHO recommendations for the IVD; ■ EDL listing of the IVD; ■ current demand for similar tests; and ■ expectation of donor funding for supplying the IVD.
The SAGE IVD discussed the criteria and agreed that they were appropriate, with the addition of a public health impact on disease burden and deletion of the availability of donor funding. The Group agreed that prequalification of tests by WHO was neither necessary nor sufficient for their inclusion on the EDL.
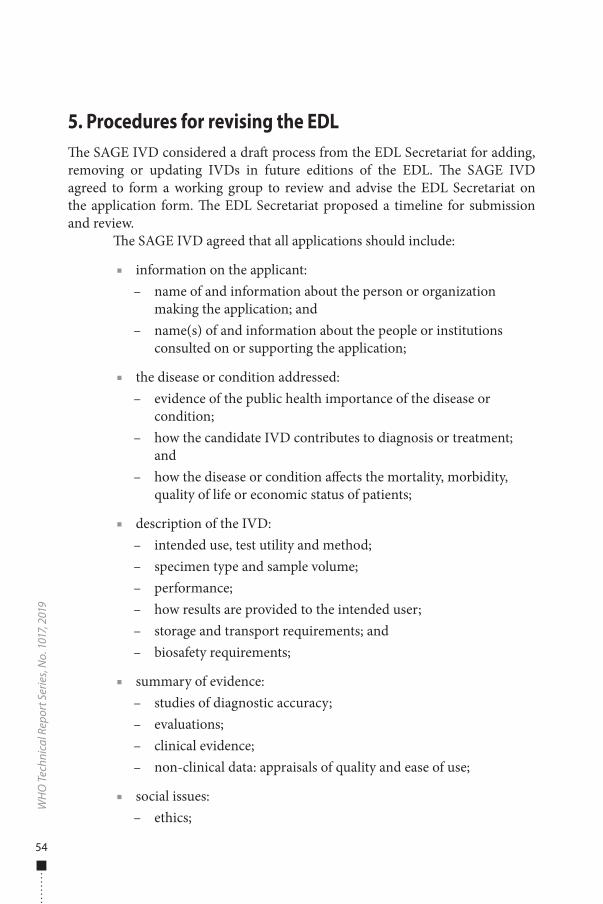
54
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9
5. Procedures for revising the EDLThe SAGE IVD considered a draft process from the EDL Secretariat for adding, removing or updating IVDs in future editions of the EDL. The SAGE IVD agreed to form a working group to review and advise the EDL Secretariat on the application form. The EDL Secretariat proposed a timeline for submission and review.
The SAGE IVD agreed that all applications should include:
■ information on the applicant: – name of and information about the person or organization
making the application; and – name(s) of and information about the people or institutions
consulted on or supporting the application;
■ the disease or condition addressed: – evidence of the public health importance of the disease or
condition; – how the candidate IVD contributes to diagnosis or treatment;
and – how the disease or condition affects the mortality, morbidity,
quality of life or economic status of patients;
■ description of the IVD: – intended use, test utility and method; – specimen type and sample volume; – performance; – how results are provided to the intended user; – storage and transport requirements; and – biosafety requirements;
■ summary of evidence: – studies of diagnostic accuracy; – evaluations; – clinical evidence; – non-clinical data: appraisals of quality and ease of use;
■ social issues: – ethics;

Procedures for revising the EDL
55
– human rights; and – equity;
■ impact on health care system: – comparative cost and cost–effectiveness; – resource and budget impact on health care systems, including
human resources and supplies of consumables; and – sustainability;
■ proposed text for the EDL.
The proposed process for review of applications for inclusion in the EDL is illustrated in Fig. 2.
The EDL will be updated annually. WHO will issue a call each year for applications to add IVD test categories to the next edition of the EDL, and additions will be made to the List to promote progress towards the goal of universal health coverage.

56
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9
6. Adaptation of the EDL for national listsThe SAGE IVD considered adaptation of the model EDL for national and institutional EDLs, including factors such as local patterns of prevalent diseases, the availability of diagnostics and treatments, including medicines, health care facilities and personnel, sustainability and affordability. The SAGE IVD asked that feedback from countries be solicited as a priority. It noted that there would be a process of trial, feedback and revision and suggested that WHO work with “pathfinder” countries to make the process more efficient.
It will be important that Member States adopt and adapt the EDL to establish national EDLs. Implementation of the lists will require investment in integrated, connected, tiered laboratory systems, with adequate human resources, training, laboratory infrastructure, and regulatory and quality assurance systems. The local costs of IVDs, supplies and reagents should also be considered.

57
7. Recommendations The SAGE IVD made the following recommendations to the WHO Secretariat.
■ Recognizing the importance of tests for a wide variety of diseases, the EDL should include a broad list of general laboratory tests, as well as tests for the following initial set of diseases, pursuant to WHO policy and for which there is high-quality guidance: HIV infection, TB, malaria, hepatitis B, hepatitis C, HPV infection and syphilis.
■ The EDL Secretariat should consider including tests for the following priority diseases or conditions in future editions of the EDL: antimicrobial resistance, neglected tropical diseases, noncommunicable diseases, outbreaks and emergencies and sepsis.
■ The EDL Secretariat should include a detailed preface to the EDL to explain its objectives, limitations and guidance for use. The preface should include: the scope of the EDL, definitions of health service levels, the rationale for the contents and the importance of adapting the list to local or regional settings and conditions.
■ The EDL Secretariat should emphasize that, while the EDL provides a list of important tests for use at various levels of the health system, the list will not be useful without an integrated, connected, tiered laboratory system, with adequate human resources, training, laboratory infrastructure and regulatory and quality assurance systems.
■ Member States can adapt the EDL and prepare national or regional EDLs; they should also ensure the necessary mechanisms for impact.
■ Revise and update the WHO technical documents that constitute resources for the EDL to ensure that they are relevant and current. This task should be a priority, if necessary supported by WHO collaborating centres, other institutions and SAGE IVD.
■ Support EDL with a dedicated page on the WHO website containing information on IVDs and laboratories.
■ The EDL Secretariat should review the WHO prequalification process, and acknowledge that it plays an important role in increasing access to IVDs of assured quality, safety and performance. SAGE IVD appreciates that EDL and prequalification are complementary in improving access of Member States to IVDs.
On 20 April 2018, an open session was held with SAGE IVD members and representatives of nongovernmental organizations, trade associations and

58
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
WHO Member States to discuss the outcomes of the first SAGE IVD meeting. It was agreed that, for future EDLs, an open session will be held before the SAGE IVD meeting to discuss issues raised during the open consultation.

59
References1. Thirteenth General Programme of Work 2019–2023. Geneva: World Health Organization; 2018
(http://www.who.int/about/what-we-do/gpw-thirteen-consultation/en/).
2. The selection and use of essential medicines. Report of the WHO Expert Committee, 2017 (including the 20th WHO Model List of Essential Medicines and the 6th Model List of Essential Medicines for Children). Geneva: World Health Organization; 2017 (WHO Technical Report Series, No. 1006; https://apps.who.int/iris/handle/10665/259481, accessed 21 February 2019).
3. Global Health Observatory data on national lists of medical devices. Geneva: World Health Organization; 2017 (https://www.who.int/gho/health_technologies/medical_devices/lists/en/).
4. Consultation on technical and operational recommendations for clinical laboratory testing harmonization and standardization, 22–24 January 2008, Maputo, Mozambique. Geneva: World Health Organization; 2008 (http://www.who.int/healthsystems/round9_9.pdf).
5. Guidance for development of national laboratory strategic plans. Brazzaville: WHO Regional Office for Africa; Atlanta (GA): Centers for Disease Control and Prevention; 2009 (http://www.who.int/hiv/amds/amds_guide_dev_nat_lab_strat.pdf).
6. Guidance for procurement of in vitro diagnostics and related laboratory items and equipment. Geneva: World Health Organization; 2017 (https://apps.who.int/iris/handle/10665/255577).
7. Guide for national public health laboratory networking to strengthen integrated disease surveillance and response (IDSR). Brazzaville: WHO Regional Office for Africa; 2008 (http://www.afro.who.int/publications/guide-national-public-health-laboratory-networking-strengthen-integrated-disease).
8. Global Harmonization Task Force. Definition of the terms medical and in vitro diagnostic (IVD) medical device. Geneva: World Health Organization; 2012 (http://www.imdrf.org/docs/ghtf/find/891/technical-docs/ghtf-sg1-n071-2012-definition-of-terms-120516.pdf#search, accessed 3 May 2018).

60
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9
WHO sources used to select the general laboratory testsAsia Pacific strategy for strengthening health laboratory services (2010–2015). New Delhi: WHO Regional Office for South-East Asia and Manila: WHO Regional Office for the Western Pacific; 2010 (http://www.wpro.who.int/health_technology/documents/asia_pacific_laboratory_strategy2010-2015.pdf?ua=1).
Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach, second edition. Geneva: World Health Organization; 2016 (http://apps.who.int/iris/handle/10665/208825).
Guidelines on hepatitis B and C testing. Geneva: World Health Organization; 2017 (http://apps.who.int/iris/ /handle/10665/254621).
HEARTS Technical package for cardiovascular disease management in primary health care: access to essential medicines and technology. Geneva: World Health Organization; 2018 (WHO/NMH/NVI/18.3; http://apps.who.int/iris/handle/10665/260420).
Interagency list of priority medical devices for essential interventions for reproductive, maternal, newborn and child health. Geneva: World Health Organization; 2015 (http://www.who.int/medical_devices/publications/interagency_med_dev_list/en/).
Laboratory quality standards and their implementation. Manila: WHO Regional Office for the Western Pacific; and New Delhi: WHO Regional Office for South-East Asia; 2011 (https://apps.who.int/iris/handle/10665/205405).
WHO expert meeting report on short, medium and longer term product development priorities in HIV-related diagnostics, 6–7 June 2012, Geneva, Switzerland. Geneva: World Health Organization; 2012 (https://apps.who.int/iris/handle/10665/75971).
WHO Global Model Regulatory Framework for Medical Devices including in vitro diagnostic medical devices. WHO Medical device technical series. Geneva: World Health Organization; 2017 (https://apps.who.int/iris/handle/10665/255177).
WHO guide for the stepwise laboratory improvement process towards accreditation in the African Region (SLIPTA). Brazzaville: WHO Regional Office for Africa; 2015 (http://www.afro.who.int/publications/who-guide-stepwise-laboratory-improvement-process-towards-accreditation-slipta-african).
WHO list of priority medical devices for cancer management. WHO Medical device technical series. Geneva: World Health Organization; 2017 (https://apps.who.int/iris/handle/10665/255262).
Manual of basic techniques for a health laboratory, 2nd edition. Geneva: World Health Organization; 2003 (https://apps.who.int/iris/handle/10665/42295).
Screening donated blood for transfusion-transmissible infections: recommendations. Geneva: World Health Organization; 2009 (http://apps.who.int/iris/handle/10665/44202).
Use of glycated haemoglobin (HbA1c) in the diagnosis of diabetes mellitus: abbreviated report of a WHO consultation. Geneva: World Health Organization; 2011 (WHO/NMH/CHP/CPM/11.1; https://apps.who.int/iris/handle/10665/70523).
The sources also includedWHO publications on medical devices (http://www.who.int/medical_devices/publications/en/).

61
Acknowledgements WHO acknowledges the technical input of all SAGE IVD members and WHO programmes and comments from various nongovernmental organizations, industry, academics and other stakeholders and from the EDL Secretariat.
WHO thanks the Department for International Development, United Kingdom, for providing a funding grant to support the EDL.

62
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9
Annex 1
Participants in the first meeting of the WHO Strategic Advisory Group of Experts on In Vitro DiagnosticsGeneva, Switzerland, 16–20 April 2018
Members8
Professor G. Araj, Director of Clinical Microbiology, Department of Pathology and Laboratory Medicine, American University of Beirut Medical Center, Lebanon
Dr S. Best, former Director, National Serology Reference Laboratory, Fitzroy, Victoria, Australia
Dr R. Bhatia, former Director, Communicable Diseases, WHO Regional Office for South-East Asia, New Delhi, India
Dr J.Y. Carter, Technical Director, Clinical and Diagnostics, Amref Health Africa, Nairobi, Kenya
Professor F. Chappuis, Head, Division of Tropical and Humanitarian Medicine, and Associate Professor, University Hospitals of Geneva; Medical Advisor (human African trypanosomiasis), Médecins Sans Frontières, Switzerland
Professor J. Deeks, Biostatistics, Evidence Synthesis and Test Evaluation Research Group, Institute of Applied Health Research, University of Birmingham, Birmingham, England
Professor A.O. Emeribe, Laboratory of Haematology and Blood Transfusion Science, University of Calabar, Etagbor; Registrar and Chief Executive Officer, Medical Laboratory Science Council of Nigeria, Abuja, Nigeria
Professor H.Y. Faye-Kette, Microbiology, Bacteriology and Virology, Medical Sciences School, University Felix Houphouet-Boigny, Abidjan, Côte d’Ivoire
Dr S.A. Hojvat, consultant, Rockville (MD), USA
Professor H. Huang, Director, National Tuberculosis Clinical Laboratory, Centres for Disease Control, Beijing, China
Professor J. Jacobs, Tropical Laboratory Medicine, Institute of Tropical Medicine, University of Antwerp, Antwerp, Belgium
Dr N. Janejai, Deputy Director, National Institute of Health, Department of Medical Sciences, Nonthaburi, Thailand
8 Unable to attend: Professor P.E. Castle, Department of Epidemiology and Population Health, Albert Einstein College of Medicine, New York City (NY), United States of America (USA); Dr W. Sikhondze, Technical Advisor and Research Coordinator, Swaziland National Tuberculosis Control Programme, Mbabane, Eswatini.

Annex 1
63
Professor A. Newland, Haematology, The Royal London Hospital, Barts Health NHS Trust, London, England
Professor M. Pai, Canada Research Chair in Epidemiology and Global Health; Director, McGill Global Health Programmes; Associate Director, McGill International TB Centre; McGill University, Montreal, Canada
Professor R. Peeling, Chair of Diagnostics Research, London School of Hygiene and Tropical Medicine; Director, International Diagnostics Centre, London, England
Professor O. Perovic, Principal Pathologist, Antimicrobial Resistance Laboratory and Culture Collection Centre for Healthcare-Associated Infections, Antimicrobial Resistance and Mycoses; Associate Professor, University of Witwatersrand, Johannesburg, South Africa
Dr K. Walia, Lead, Antimicrobial Surveillance Network, Senior Scientist, Division of Epidemiology and Communicable Diseases, Indian Council of Medical Research, New Delhi, India
ObserversProfessor K. Cichutek, Paul-Ehrlich Institute, Langen, Germany
Dr C. Morris, National Institute for Biological Standards and Control, Ridge, Hertfordshire, England
Secretariat (World Health Organization, Geneva, Switzerland)Ms A. Alic, Ethics Officer, Compliance and Risk Management and Ethics
Dr T. Besselaar, Technical Officer, High Threat Pathogens
Ms B. Cappello, Technical Officer, Innovation, Access and Use, Department of Essential Medicines and Health Products
Ms E. Cooke, Head, Regulation of Medicines and Other Health Technologies, Department of Essential Medicines and Health Products
Dr J. Cunningham, Technical Officer, Prevention Diagnostics and Treatment, Global Malaria Programme
Dr S. Garner, Coordinator, Innovation Access and Use, Department of Essential Medicines and Health Products
Dr C. Gilpin, Scientist, Laboratories, Diagnostics and Drug Resistance, Global TB Programme
Ms L. Hattingh, Berkeley (CA), United States of America (USA) (WHO Consultant)
Dr S. Hill, Director, Department of Essential Medicines and Health Products
Dr A. Ilbawi, Technical Officer, Management of Noncommunicable Diseases
Dr I. Knezevic, Team Leader, Technologies, Standards and Norms, Department of Essential Medicines and Health Products

64
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
Dr A.C. Kuesel, Scientist (Intervention Research), UNICEF/UNDP/World Bank/UN Special Programme for Research and Training in Tropical Diseases
Dr F.X. Lery, Coordinator, Technologies, Standards and Norms, Department of Essential Medicines and Health Products
Dr L. Moja, Technical Officer, Innovation, Access and Use, Department of Essential Medicines and Health Products
Dr F.G. Moussy, Scientist, Innovation, Access and Use, Department of Essential Medicines and Health Products
Mr D. Mubangizi, Coordinator, Prequalification Team, Department of Essential Medicines and Health Products
Murtagh, Evanston, IL, USA (WHO Consultant)
Dr W.A. Perea Caro, High Threat Pathogens, WHO Health Emergencies Programme
Ms M.M. Perez Gonzalez, Technical Officer, Prequalification Team, Department of Essential Medicines and Health Products
Dr C.L. Pessoa da Silva, Medical Officer, Surveillance Team, Antimicrobial Resistance
Mrs I. Prat, Technical Officer, Prequalification Team, Department of Essential Medicines and Health Products
Mr J. Quirin, Legal Officer, Office of the Legal Counsel
Ms M. Rabini, Technical Officer, Innovation, Access and Use, Department of Essential Medicines and Health Products
Ms A. Sands, Safety and Vigilance Team, Department of Essential Medicines and Health Products
Professor L. Schroeder, Chemical Pathology, Director of Point of Care Testing; Associate Director, Chemical Pathology, Clinical Pathology, Department of Pathology, University of Michigan, Ann Arbor (MI), USA (WHO Consultant)
Dr M. Simão, Assistant Director-General, Access to Medicines, Vaccines and Pharmaceuticals
Dr S. Swaminathan, Deputy Director-General for Programmes
Dr M. Taylor, Medical Officer, Human Reproduction
Dr W.S.K. Urassa, Scientist, Prequalification Team, Department of Essential Medicines and Health Products
Mrs A. Velazquez Berumen, Senior Adviser, Innovation, Access and Use, Department of Essential Medicines and Health Products
Dr L. Vojnov, Technical Officer (Diagnostics Adviser), Treatment and Care, HIV/AIDS

65
Annex 2
Declarations of interest of SAGE IVD members
Professor Madhukar Pai advised the Group that he had been a consultant with the Bill & Melinda Gates Foundation and provided technical assistance to their TB India Program. The consultancy ended on 31 March 2018. He is a member of the Scientific Advisory Committee of the Foundation for Innovative New Diagnostics (FIND) and serves on the Access Advisory Committee of the Global Alliance for TB Drug Development. Since 2015, he has also been part of WHO’s Strategic and Technical Advisory Group for TB.
Dr Susan Best advised the Group that she was given support by DiaSorin to attend a European Society of Clinical Virology conference in Italy in September 2017, where she presented a poster that reported on the performance of the DiaSorin Liaison hepatitis B immunoassay in blood specimens collected from cadavers. DiaSorin did not financially support the work that led to the presentation.
Dr Jonathan Deeks advised the Group that he reviewed WHO guidelines related to diagnostics for TB, malaria, HIV and hepatitis with a view to harmonizing processes. Dr Deeks also developed background materials for the HIV department to support their guideline development.
Dr Sally Hojvat advised the Group that, in 2016–2017, she reviewed dossiers on two HPV diagnostic devices and subsequent responses on deficiencies from diagnostics companies for the WHO prequalification team. She also reviewed several documents on product technical specifications for the WHO prequalification team in 2016–2017. Additionally, she provides advice to a regulatory contractor for non-profit institutions and commercial diagnostic companies on matters related to the US Food and Drug Administration pre- and post-commercialization regulatory policy, which involves infectious disease diagnostics (except for HIV laboratory tests of moderate complexity). She provides advice to the same contractor on matters related to the protection of human subjects in clinical trials for diagnostic devices. Further, Dr Hojvat was the Director of the Division of Microbiology at the US Food and Drug Administration, which was responsible for reviewing and evaluating the safety and effectiveness of all IVD microbiology devices (reagents, software and instruments) submitted to the US Food and Drug Administration for pre-market device clearance, approval, waiver of the Clinical Laboratory Improvement Amendments and Emergency Use Authorization and was responsible for ensuring pre-market and post-market compliance associated with IVD microbiology devices. She also represented the US Food and Drug Administration on human subject protection

66
WH
O T
echn
ical
Rep
ort S
erie
s, N
o. 1
017,
201
9First WHO Model List of Essential In Vitro Diagnostics
and was responsible for outreach on IVDs for infectious diseases, including the response to emerging pathogens such as influenza H1N1, Middle East respiratory syndrome, and Ebola virus, and potential biological threats such as anthrax and plague, working with US health and human services agencies (Biomedical Advanced Research and Development Authority, National Institutes of Health, Public Health Emergency Medical Countermeasures Enterprise), the Department of Defense research laboratories and WHO prequalification regulatory teams.
The EDL Secretariat reviewed the disclosures listed above and concluded that these experts had no conflict of interest in respect of the meeting and could fully participate.

W H O T e c h n i c a l R e p o r t S e r i e s
1017
First WHO Model List of Essential In Vitro Diagnostics
1017First W
HO
Model List of Essential In Vitro D
iagnosticsW
HO
Technical Report Series
ISBN 978 92 4 121026 3
This report presents the First WHO Model List of Essential In Vitro Diagnostics (EDL) and recommendations by the Strategic Advisory Group of Experts on In Vitro Diagnostics (SAGE IVD), commissioned to act as an advisory body on matters of global policies and strategies related to in vitro diagnostics (IVDs). The report described the scope and recommended use of the List and details of the methods, the criteria for prioritizing IVDs and the procedures for establishing the List. It also includes the procedures for updating the List, its integration with other WHO initiatives and its adaption to national contexts. Finally, it contains recommendations from the SAGE IVD on EDLs.


















