Third Trimester Bleeding, Postpartum Hemorrhage, & Shock Management
Upload
aboubakr-elnasharCategory
view
1.978download
1
FIRST
TRIMESTER
BLEEDING
Aboubakr
Elnashar Benha university Hospital
Egypt
Aboubakr Elnashar
CONTENTS
1. INCIDENCE
2. CAUSES
3. DIAGNOSIS
Aboubakr Elnashar
1. INCIDENCE
Vaginal bleeding is common in 1st T
20-40% of pregnant women.
Source is virtually always maternal, rather than fetal. disruption of blood vessels in the decidua discrete cervical or vaginal lesions.
Aboubakr Elnashar

2. CAUSES
Related to pregnancy:
Miscarriage (95%)
Ectopic pregnancy
Hydatidiform mole
Vanishing twin
Implantation bleeding.
Associated with
pregnancy: unrelated to pregnancy
pre-existing or aggravated
during pregnancy.
Cervico-vaginitis
Vascular erosion
Polyp, fibroid
Ruptured varicose veins
Malignancy.
Trauma
Aboubakr Elnashar
1. Miscarriage:
most common
15 to 20% of pregnancies
±heavy:1%
Aboubakr Elnashar

2. Ectopic pregnancy
much less common 2% of pregnancies most serious {rupture of the extrauterine pregnancy is a life threatening complication} must be excluded in every pregnant woman with bleeding.
Aboubakr Elnashar

3. Trophoblastic disease
Aboubakr Elnashar
4. Vanishing twin
Singleton pregnancy
{very early loss of one member of a multiple
gestation}.
often the product of ART
can be associated with vaginal bleeding
Aboubakr Elnashar

5. Physiologic or implantation bleeding
small amount of spotting or bleeding
10-14 days after fertilization (at the time of the
missed menstrual period)
{implantation of the fertilized egg in the decidua}, although this hypothesis has been questioned
Diagnosis of exclusion.
No intervention is indicated.
Aboubakr Elnashar

Vaginitis, trauma, tumor, warts, polyps, fibroids
Diagnosis
Visual inspection
Additional tests as indicated:
wet mount, pH of vaginal discharge,cytology
biopsy of mass lesions, US Ectropion: common and normal finding in pregnancy. The exposed columnar epithelium is prone to light bleeding when touched, such as during coitus, insertion of a speculum, bimanual examination, or when a cervical specimen is obtained for cytology or culture. Therapy is unnecessary
Aboubakr Elnashar

3. DIAGNOSIS
History:
gestational age
character of bleeding:
light or heavy
associated with pain or painless
intermittent or constant
Examination
Laboratory:
TVS
confirm or revise the initial diagnosis.
Aboubakr Elnashar

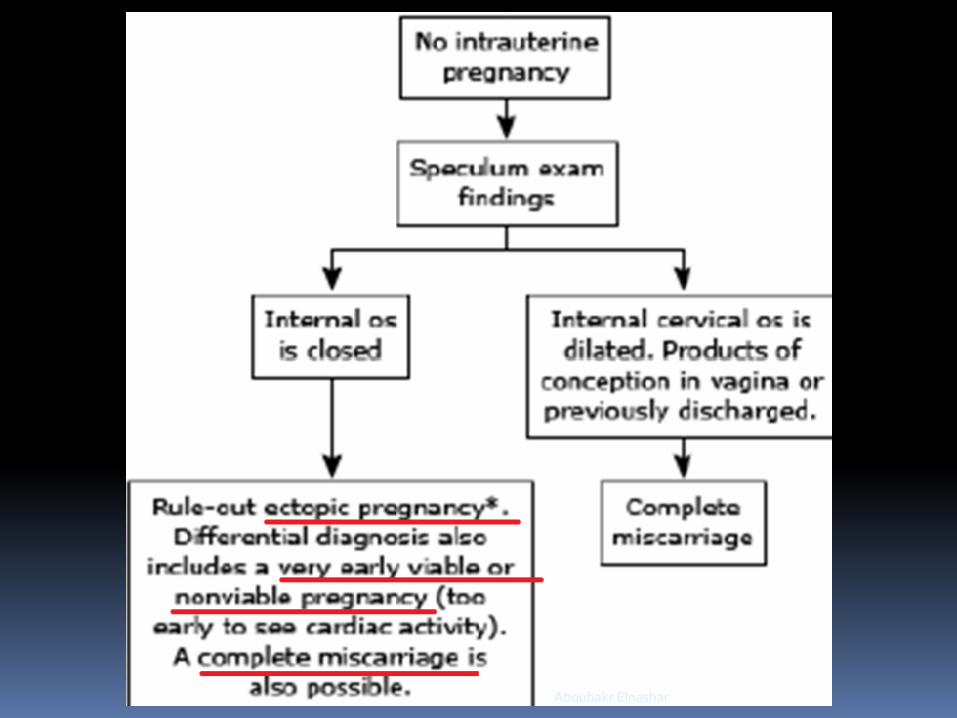
Speculum examination
:
1.3% change of management
4.2% change of diagnosis
: minority of management decisions.
The need for speculum examination
should be assessed on a case-by-case basis,
depending on whether the findings on bimanual
examination are conclusive.
Aboubakr Elnashar
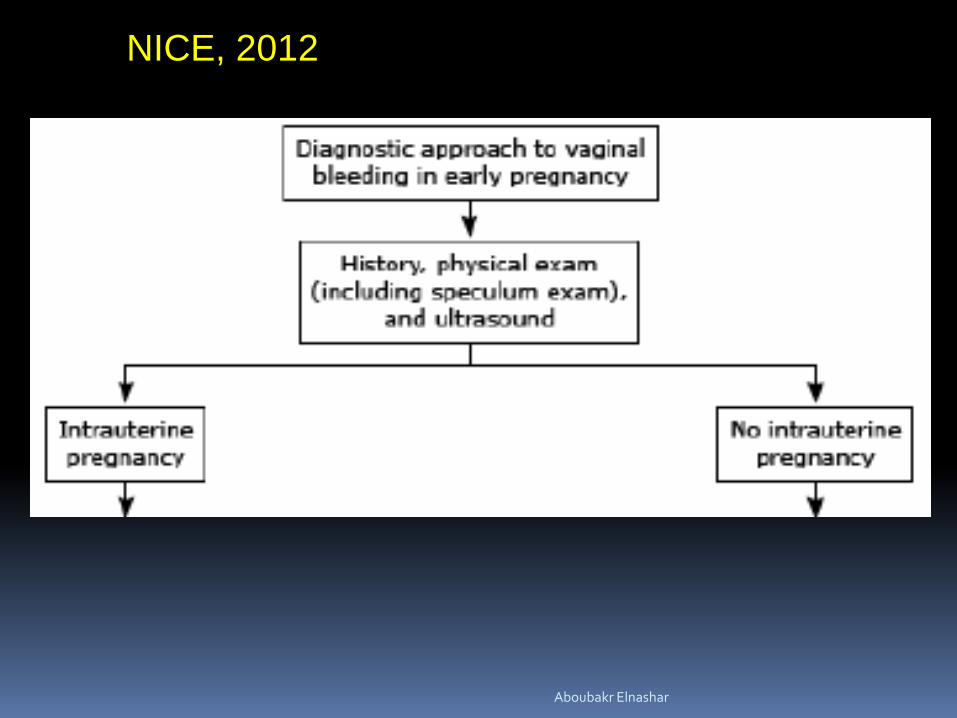
NICE, 2012
Aboubakr Elnashar
Aboubakr Elnashar
Aboubakr Elnashar

TVS
Cornerstone of the evaluation of bleeding in 1st T.
Most useful
Intrauterine or extrauterine
Viable or nonviable.
Heterotopic pregnancy
Gestational trophoblastic disease
Loss of one fetus from a multiple gestation.
Aboubakr Elnashar
It is vital to describe clinical and ultrasound
findings in early pregnancy using appropriate
terminology
Miscarriage
should replace ‘abortion’ in clinical practice.
Aboubakr Elnashar

Pregnancy of unknown location: PUL
should replace pregnancy of indeterminate
location Positive pregnancy test but no signs of intra- or
extrauterine pregnancy or retained products of conception
Pregnancy of uncertain viability: PUV
Should replace pregnancy of indeterminate
viability IUGS 20 mm mean diameter with no obvious yolk sac or
fetus, or
fetal echo 6 mm CRL with no obvious fetal heart activity.
In these circumstances a repeat scan at a
minimum interval of 1 week.
Aboubakr Elnashar
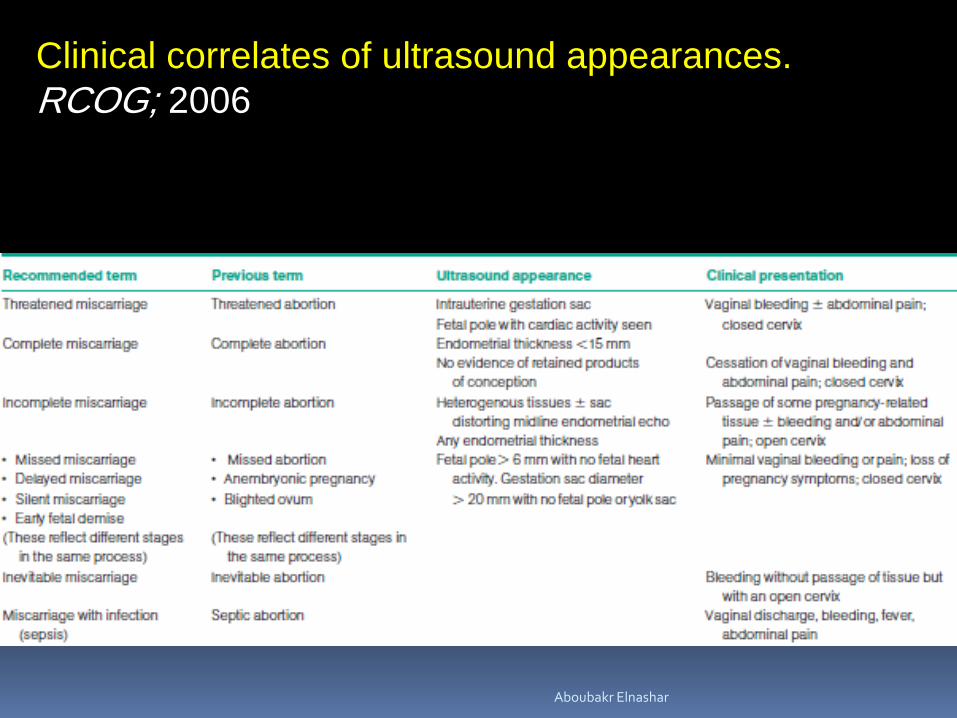
Clinical correlates of ultrasound appearances.
RCOG; 2006
Aboubakr Elnashar

TAS:
most useful for assessing
free fluid in the abdomen
abnormalities beyond the field of view of a high
frequency vaginal probe
Aboubakr Elnashar
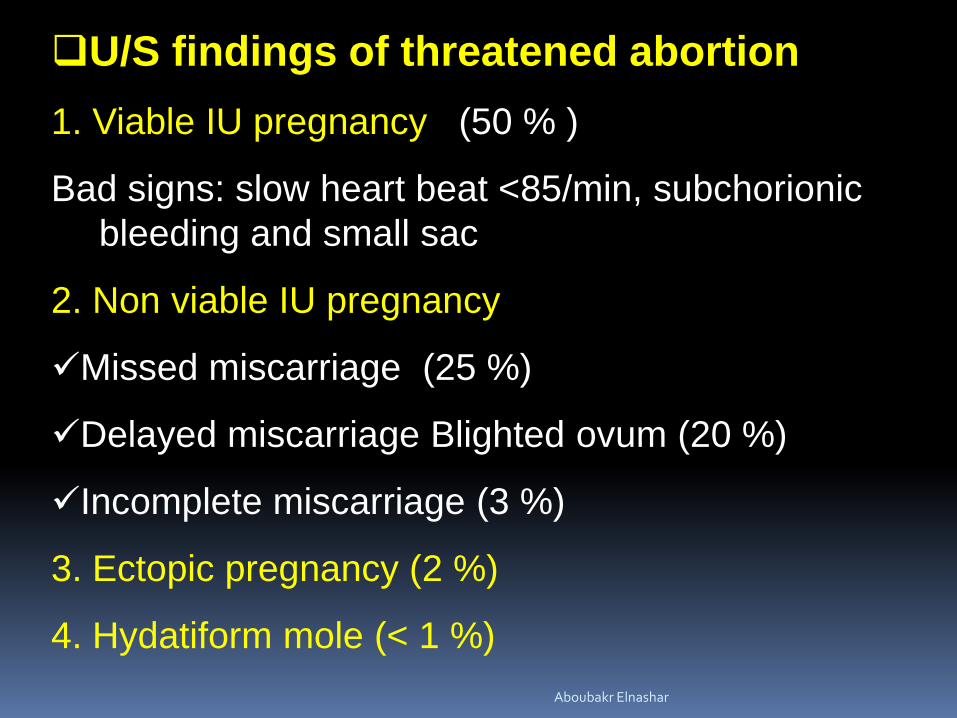
U/S findings of threatened abortion
1. Viable IU pregnancy (50 % )
Bad signs: slow heart beat <85/min, subchorionic
bleeding and small sac
2. Non viable IU pregnancy
Missed miscarriage (25 %)
Delayed miscarriage Blighted ovum (20 %)
Incomplete miscarriage (3 %)
3. Ectopic pregnancy (2 %)
4. Hydatiform mole (< 1 %)
Aboubakr Elnashar

1. PUL
Positive pregnancy test +
No IU pregnancy
No extrauterine pregnancy
No retained products of conception
NICE, 2012
Aboubakr Elnashar

Aboubakr Elnashar
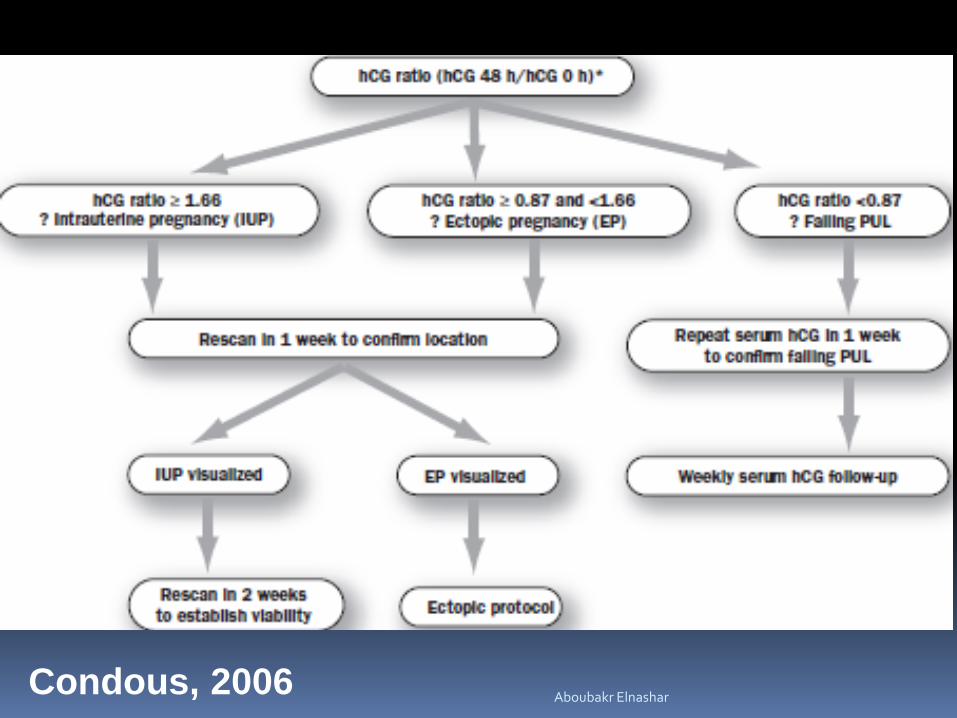
Condous, 2006 Aboubakr Elnashar
Most PULs are at low risk for an ectopic
pregnancy provided that US is sufficiently skilled
and uses US with acceptable image quality.
HCG at defined times in women with a PUL can
reliably predict immediately viability of a PUL, but
cannot predict its location.
An hCG ratio cut-off <0.87 can be used to identify
spontaneously resolving pregnancies in a PUL
population.
Aboubakr Elnashar

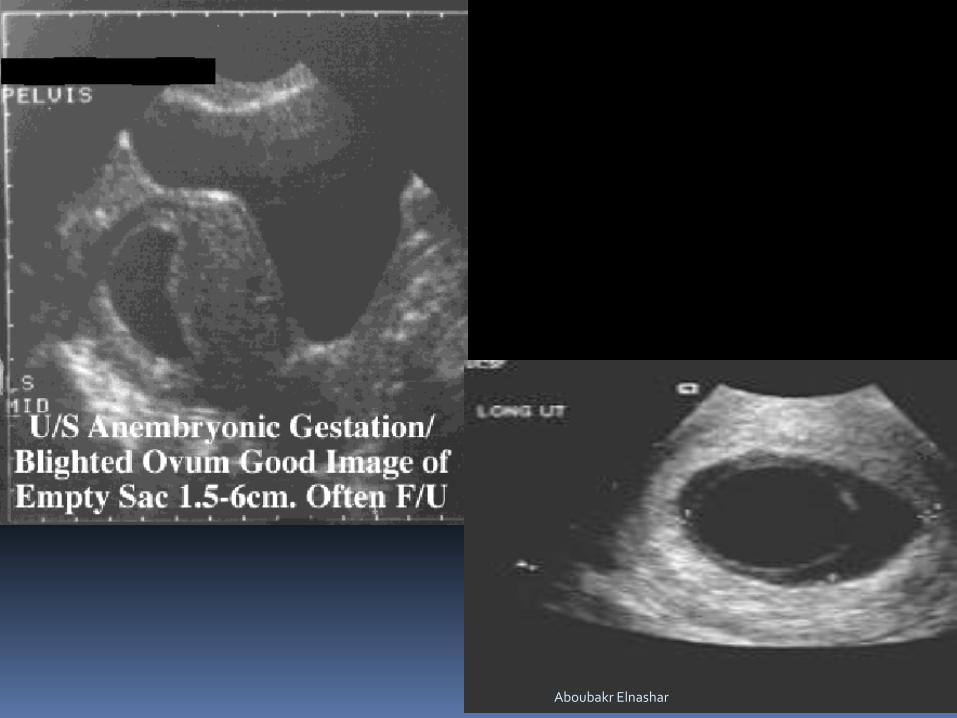
2. BLIGHTED OVUM
(Anembryonic pregnancy)
No fetal parts with sac diameters > 20 mm (TV) 30 mm (TA)
No yolk sac
Irregular sac contour
If unsure repeat in 1 week
Aboubakr Elnashar
Aboubakr Elnashar

3. MISSED ABORTION
CRL: 6 mm & no cardiac activity or
< 6 mm & no change at the time of repeat
scan 7 days later (embryonic growth rate is 1 mm/d)
Abnormal form of G S
Aboubakr Elnashar

Aboubakr Elnashar
4. INCOMPLETE ABORTION
The endometrial midline echo:
distorted
>15 mm in the anteroposterior plane
Hetrogenous & irregular tissues.
Aboubakr Elnashar

5. COMPLETE ABORTION
The endometrial thickness
<15 mm in the anteroposterior plane
No evidence of retained products of conception
Aboubakr Elnashar

Aboubakr Elnashar

6. INEVITABLE ABORTION
GS situated low in uterus or cervix
Aboubakr Elnashar

Aboubakr Elnashar

7. ECTOPIC PREGNANCY
A. Uterine
1. No IU gestational sac Normally BHCG doubles/48h Discrimination zone: BHCG increasing by >60% in 48 h if not and no considerable bleeding think of ectopic pregnancy if uterus Is empty on scan However 5% of normal pregnancies don’t behave like that
Aboubakr Elnashar

2. Pseudo gestational sac (a fluid collection or
debris in the cavity)
10-20% of ectopic P.
No double decidual sac sign
No yolk sac or embryo
Not eccentric (within the cavity)
3. No yolk sac in a G. sac > 20 mm
Aboubakr Elnashar

Aboubakr Elnashar

B. Adnexal
1. Non cystic mass:
(Blob sign) inhomogeneous small mass next to the
ovary with no sac or embryo.
By pressing the vaginal probe gently against the
ectopic it moves separately to the ovary.
The most appropriate sign. Sensitivity 84% & specificity
99%
Aboubakr Elnashar

loop
Non cystic mass
D pouch
Aboubakr Elnashar

complex mass.
The adjacent ovary is marked by the presence of
regular follicular structures in the ovarian
parenchyma.
Aboubakr Elnashar
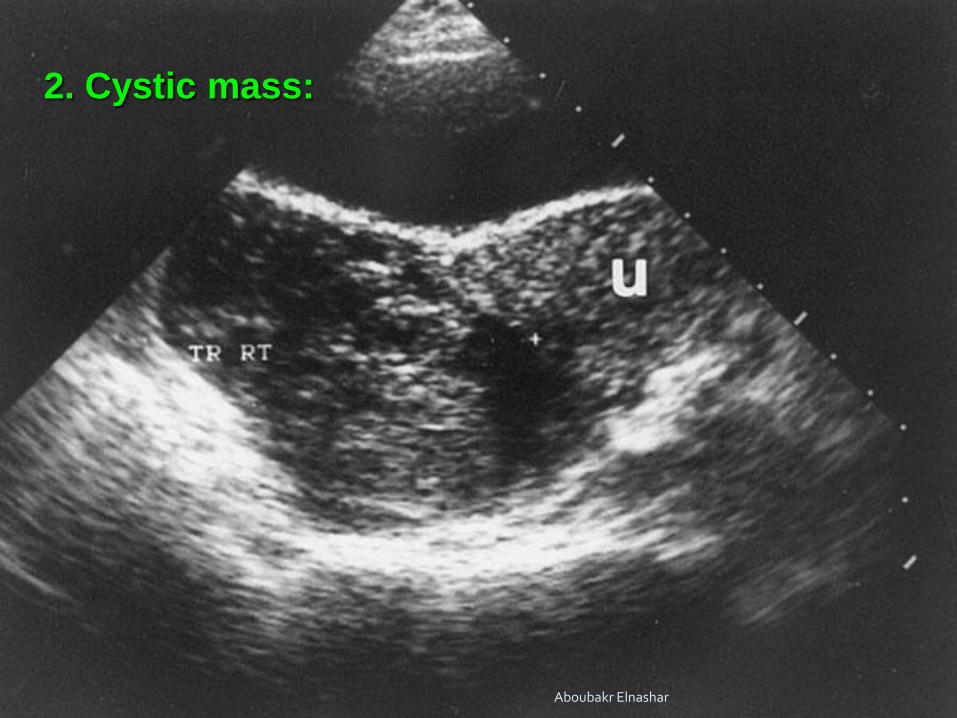
2. Cystic mass:
Aboubakr Elnashar

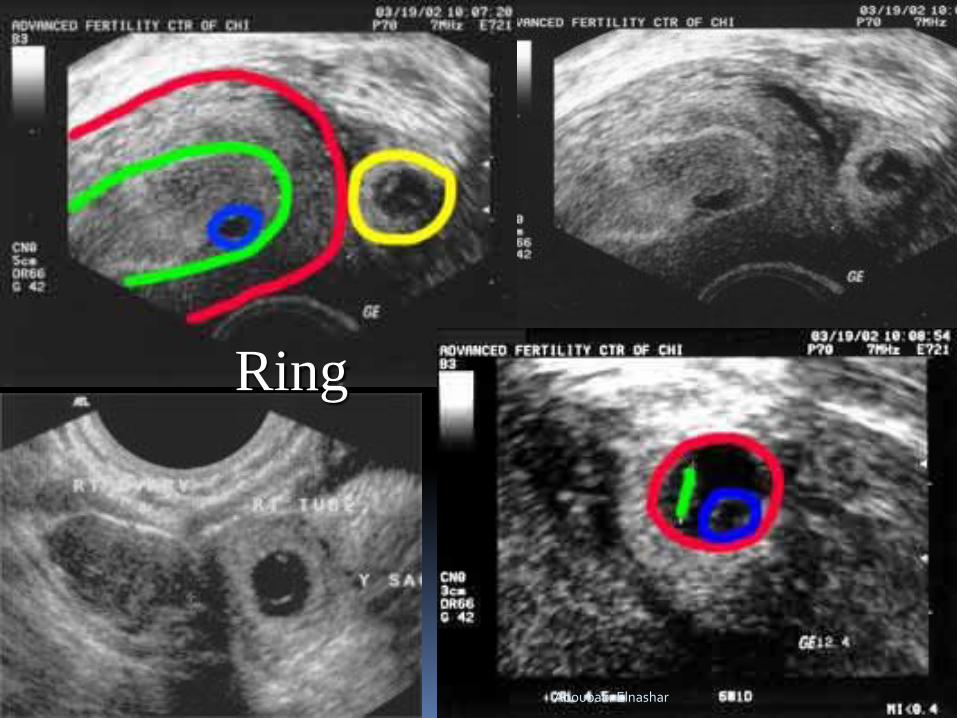
3. Ring:
(Bagel sign) hyperechoic ring around the GS
Note the circular morphology and the strongly
echogenic appearance of the trophoblast.
The content is anechoic {accumulation of fluid in GS}
Aboubakr Elnashar
Ring
Aboubakr Elnashar

4.Sac & embryo.
Only seen in 10-20% of ectopic pregncncies
Ipsilateral side: Corpus luteum: 85% of cases
Aboubakr Elnashar

C. D. pouch:
Fluid with or without blood clots
Aboubakr Elnashar

Cervical
pregnancy
Abdominal
pregnancy
Aboubakr Elnashar

Aboubakr Elnashar

8. HYDATIFORM MOLE
1. Placenta with multiple small sonolucent areas
(snowstorm)
2. Ovarian theca lutein cysts
D.D :
1.Missed abortion with hydropic degeneration
2 .Degenerating fibroid
Aboubakr Elnashar
Definitive diagnosis is made by histological
examination.
U/S: Early detection reduced from 16 W (passage of
vesicles) to 12 w
βhCG levels > 2 multiples of the median
RCOG Guideline No. 38 ; 2010 Aboubakr Elnashar

Aboubakr Elnashar

The characteristic snowstorm pattern representing the
hydropic chorionic villi
Aboubakr Elnashar

Increased flow
Complete hydatidiform mole. The classic "snowstorm"
appearance is created by the multiple placental vesicles. Aboubakr Elnashar

Complete hydatidiform mole. The classic
"snowstorm" appearance is created by the
multiple placental vesicles. Aboubakr Elnashar

Color Doppler Scan In A Patient With A Molar Gestation
Aboubakr Elnashar

In most patients
Cl and US diagnosis is usually
missed or incomplete abortion.
Thorough histopathologic evaluation of
all missed or incomplete abortions
Partial H .Mole
Disaia &Creasman Clinical Gynecological Oncologym 7th edd. 2007 Aboubakr Elnashar

Classically:
Placenta: Thickened, hydropic
Fetal or embryonic tissue
Multiple soft markers, including:
Cystic spaces in the placenta
Transverse to AP dimension a ratio of the GS of >
1.5, is required for the reliable diagnosis of a partial
molar pregnancy
RCOG Guideline No. 38 ; 2010 Aboubakr Elnashar

Partial molar pregnancy
The placenta shows multiple small cystic lesions, suggesting a
molar change.
a viable fetus
- Aboubakr Elnashar

Multicystic placenta
embryo
Aboubakr Elnashar

Multicystic placenta
Yolk sac
Dead embryo
Partial Molar Pregnancy Aboubakr Elnashar
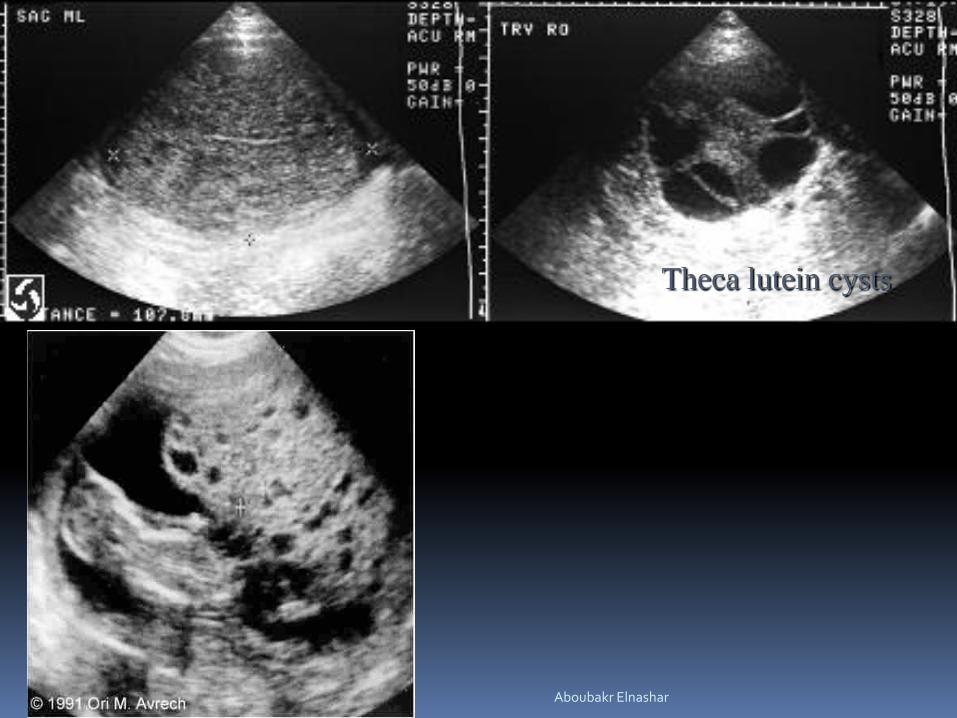
Theca lutein cysts
Aboubakr Elnashar

246 lectures
3003 members
Aboubakr Elnashar