First high quality alternative to phaco
42
Manual small incision cataract surgery (MSICS): opening the door to a new strategy for addressing blindness Glenn Strauss MD Mercy Ships with thanks for contributions by James MacAllister, M.D.
description
Manual small incision cataract surgery (MSICS): opening the door to a new strategy for addressing blindness Glenn Strauss MD Mercy Ships with thanks for contributions by James MacAllister, M.D. First high quality alternative to phaco. An elegant sutureless ECCE procedure - PowerPoint PPT Presentation
Transcript of First high quality alternative to phaco

Manual small incision cataract surgery (MSICS): opening the door to a new strategy for addressing blindness
Glenn Strauss MD Mercy Ships
with thanks for contributions by James MacAllister, M.D.
Manual small incision cataract surgery (MSICS): opening the door to a new strategy for addressing blindness
Glenn Strauss MD Mercy Ships
with thanks for contributions by James MacAllister, M.D.

First high quality alternative to phacoFirst high quality alternative to phaco
An elegant sutureless ECCE procedure
It is ideal for situations where high quality, high volume output is desirable without high-tech instrumentation or equipment
Provides an alternative to standard ECCE when phaco is high risk.
An elegant sutureless ECCE procedure
It is ideal for situations where high quality, high volume output is desirable without high-tech instrumentation or equipment
Provides an alternative to standard ECCE when phaco is high risk.

Opens the door to new strategies in patient care Opens the door to new strategies in patient care
Ideally utilized as part of a team system to maximize efficiency as a single procedure approach to cataract surgery
Increasingly being utilized as an alternative tool for high risk cataracts
Integral part of a “funnel” strategy: screening, diagnostics, perioperative care, and surgical care
Has provided a new paradigm to address the problem of global cataract blindness
Ideally utilized as part of a team system to maximize efficiency as a single procedure approach to cataract surgery
Increasingly being utilized as an alternative tool for high risk cataracts
Integral part of a “funnel” strategy: screening, diagnostics, perioperative care, and surgical care
Has provided a new paradigm to address the problem of global cataract blindness

The funnel strategyThe funnel strategy
Utilizes key skills at each level of care Maximizes use of individual strengths Surgical yield in areas of low access is
approximately 15% of those being screened Criteria based: Decreased vision, nl pupils,
clear cornea If surgical goal is 3,000 cases, 20,000 will
need to be screened, 8,000 examined.
Utilizes key skills at each level of care Maximizes use of individual strengths Surgical yield in areas of low access is
approximately 15% of those being screened Criteria based: Decreased vision, nl pupils,
clear cornea If surgical goal is 3,000 cases, 20,000 will
need to be screened, 8,000 examined.

Flexible enough to be used with a variety of cataract pathologies
Quick, efficient surgery once mastered Rapid recovery
Minimal postoperative corneal edema• Minimal induced astigmatism (studies show
comparable to phaco) No sutures to be removed late Low cost per case
Flexible enough to be used with a variety of cataract pathologies
Quick, efficient surgery once mastered Rapid recovery
Minimal postoperative corneal edema• Minimal induced astigmatism (studies show
comparable to phaco) No sutures to be removed late Low cost per case
MSICS features:MSICS features:

A brief review of the technique as practiced on
Mercy Ships
A brief review of the technique as practiced on
Mercy Ships

Anesthesia Anesthesia
Routine peribulbar or anterior conal block- topical possible but less desirable
Lidocaine 2% 5cc alone usually sufficient because of short case time
Orbital compression helpful but does not require soft eye like ECCE
Routine prep and drapeTopical 5% betadine conj. drops and skin scrub,
isolate lashes
Routine peribulbar or anterior conal block- topical possible but less desirable
Lidocaine 2% 5cc alone usually sufficient because of short case time
Orbital compression helpful but does not require soft eye like ECCE
Routine prep and drapeTopical 5% betadine conj. drops and skin scrub,
isolate lashes

Adequate conjunctival/tenons dissection and wet field cautery
May use flame cautery if only option but avoid over cauterization

Dry carefully before scleral dissectionDry carefully before scleral dissection

Scleral incisionScleral incision
With fine toothed forceps hold limbal tissue and create 7.5 mm “frown’’ incision 1.5 mm from limbus at apex of the frown. 1/2 to 2/3 depth.
Initially it may be easier to make a simple linear incision
With fine toothed forceps hold limbal tissue and create 7.5 mm “frown’’ incision 1.5 mm from limbus at apex of the frown. 1/2 to 2/3 depth.
Initially it may be easier to make a simple linear incision

Sclero-corneal tunnel dissectionSclero-corneal tunnel dissection
Carefully follow the curve of the globe, slicing anteriorly approx 2 mm into clear cornea centrally
Take care to “straighten” the limbal junction angle A 3 to 3.5 mm tunnel length (half the length of the
crescent blade)
Carefully follow the curve of the globe, slicing anteriorly approx 2 mm into clear cornea centrally
Take care to “straighten” the limbal junction angle A 3 to 3.5 mm tunnel length (half the length of the
crescent blade)

Premature entry results in iris prolapse
Premature entry results in iris prolapse

Tunnel button hole is easily fixed with new tunnel plane
Tunnel button hole is easily fixed with new tunnel plane

Sweep to each side to create an 8 to 8.5 mm internal opening
Sweep to each side to create an 8 to 8.5 mm internal opening

Tunnel size can be titrated to the anticipated size of the
nucleus
Tunnel size can be titrated to the anticipated size of the
nucleus

Paracentesis at 9 o’clock with 15 deg blade- no anterior chamber
maintainer necessary
Paracentesis at 9 o’clock with 15 deg blade- no anterior chamber
maintainer necessary
Useful for reforming chamber

Keratome entry at anterior most extent of scleral tunnel
Keratome entry at anterior most extent of scleral tunnel

Sweep keratome left and right “floating” in the tunnel to fully open. If done well, chamber is maintained.
Sweep keratome left and right “floating” in the tunnel to fully open. If done well, chamber is maintained.
Consider supporting AC with viscoelastic

A B
C D
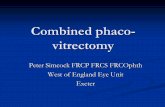
Careful 8 to 8.5mm “can opener” capsulotomy after filling AC with viscoelastic. CCC may be done for softer nucleus.
Careful 8 to 8.5mm “can opener” capsulotomy after filling AC with viscoelastic. CCC may be done for softer nucleus.

A B
C D
With capsulotomy needle inserted into nucleus, “rock and roll”, rotating and lifting the nucleus from the capsular bag
With capsulotomy needle inserted into nucleus, “rock and roll”, rotating and lifting the nucleus from the capsular bag

With lens loop, depress posterior lip of scleral tunnel and allow nucleus to glide out through the incision. (must be large enough)
With lens loop, depress posterior lip of scleral tunnel and allow nucleus to glide out through the incision. (must be large enough)

Tunnel acts hydro dynamically like a funnelTunnel acts hydro dynamically like a funnel Nuclear material never contacts
endothelium Facilitates increased efficiency of
nucleus removal Improves safety in high risk cases
(trauma, zonular instability, partially dislocated cataracts, hypermature cataracts, previous surgery)
Nuclear material never contacts endothelium
Facilitates increased efficiency of nucleus removal
Improves safety in high risk cases (trauma, zonular instability, partially dislocated cataracts, hypermature cataracts, previous surgery)

Gently depress post. lip of tunnel to milk out remaining lens material while tilting the globe by holding the limbus at 6 o’clock
Gently depress post. lip of tunnel to milk out remaining lens material while tilting the globe by holding the limbus at 6 o’clock

Remove remaining cortex using suck and wash approach (dragging cortex to center of pupil and releasing).
Standard Simcoe is not ideal instrument- designed for limbal incision. Chamber maintenance is dependant on making inner opening the pivot point. The eye is now ready for lens implantation.
Fill anterior chamber with methylcellulose or air.
Remove remaining cortex using suck and wash approach (dragging cortex to center of pupil and releasing).
Standard Simcoe is not ideal instrument- designed for limbal incision. Chamber maintenance is dependant on making inner opening the pivot point. The eye is now ready for lens implantation.
Fill anterior chamber with methylcellulose or air.

Insert IOL and remove methylcellulose. Inject BSS to moderate pressure. AC should remain formed. No conj closure needed.
Insert IOL and remove methylcellulose. Inject BSS to moderate pressure. AC should remain formed. No conj closure needed.

Complete the operation with routine antibiotics +/- steroid. Remove the speculum by lifting out inferior blade first
Complete the operation with routine antibiotics +/- steroid. Remove the speculum by lifting out inferior blade first

Other techniques for MSICSOther techniques for MSICS ACM Fish hook Plastic glide for nucleus
ACM Fish hook Plastic glide for nucleus

Phaco nightmare

ResultsResults
0
50
100
150
200
250
P LHM
C F - 20/200
20/160 - 20/100
20/80-20/30
P re Op V is ion
P os t OpV is ion
0
50
100
150
200
250
P LHM
C F - 20/200
20/160 - 20/100
20/80-20/30
P re Op V is ion
P os t OpV is ion

ResultsResults
0102030405060708090
100
Nu
mb
er o
f P
atien
ts
< -2 0+ /-2
3-6 7-11 12-16
17-21
22-27
27+
C hang e in vis ion / L og MAR lines
C hang e in vis ion
0102030405060708090
100
Nu
mb
er o
f P
atien
ts
< -2 0+ /-2
3-6 7-11 12-16
17-21
22-27
27+
C hang e in vis ion / L og MAR lines
C hang e in vis ion

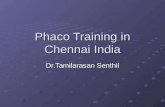
Pre and post op visual functionN
o o
f p
atie
nts

Improvement of vision by age: 30 to 40 y/o success are primarily traumatic cataracts.
Ave
rage
num
ber
of li
nes
impr
oved
Age of patient * p<0.05

% o
f pa
tient
sReported success rates from developing countries

Barriers to implementationBarriers to implementation
Cost: low cost does not mean NO cost Local regulatory issues Lack of clear, positive motivations for the
team and surgeon Medical community resistance: MSICS is
gaining credibility Ophthalmic corporate resistance: less
dependence on high tech equipment Surgeon skills
Cost: low cost does not mean NO cost Local regulatory issues Lack of clear, positive motivations for the
team and surgeon Medical community resistance: MSICS is
gaining credibility Ophthalmic corporate resistance: less
dependence on high tech equipment Surgeon skills

For discussion: how to take advantage of this approach for the benefit of South Africa
Brief review of recent RAAB study Eastern Cape
For discussion: how to take advantage of this approach for the benefit of South Africa
Brief review of recent RAAB study Eastern Cape

Rapid Assessment of Avoidable Blindness in Eastern Cape Province
of South Africa
Rapid Assessment of Avoidable Blindness in Eastern Cape Province
of South AfricaS.Saravanan of
PRASHASA ConsultantsOn behalf of FHFSA
S.Saravanan ofPRASHASA Consultants
On behalf of FHFSA

SummarySummary The all-age prevalence of blindness for Eastern
Cape Province of South Africa is estimated to be 0.58%;
The all-age magnitude of blindness for EC Province is estimated to be 38,354 people out of a population of 6.57 million;
Avoidable causes of blindness accounted for 73.2% of blindness, 86.1% of severe visual impairment and 85.7% of visual impairment.
The all-age prevalence of blindness for Eastern Cape Province of South Africa is estimated to be 0.58%;
The all-age magnitude of blindness for EC Province is estimated to be 38,354 people out of a population of 6.57 million;
Avoidable causes of blindness accounted for 73.2% of blindness, 86.1% of severe visual impairment and 85.7% of visual impairment.

SummarySummary Cataract (62.2%) and sequel related to
cataract extraction (1.2%) accounted for 63.4% of all causes of bilateral blindness;
Posterior segment disease is responsible for 31% of bilateral blindness;
36.1% of people with bilateral cataract VA<3/60 had surgery and 18.9% at VA<6/18.
Cataract (62.2%) and sequel related to cataract extraction (1.2%) accounted for 63.4% of all causes of bilateral blindness;
Posterior segment disease is responsible for 31% of bilateral blindness;
36.1% of people with bilateral cataract VA<3/60 had surgery and 18.9% at VA<6/18.

Results – Cataract Surgery CoverageResults – Cataract Surgery Coverage
Cataract surgical coverage: 36.1 % of people with bilateral cataract blind (VA<3/60) had surgery and 18.9 % at VA<6/18;
Cataract surgical coverage: 36.1 % of people with bilateral cataract blind (VA<3/60) had surgery and 18.9 % at VA<6/18;

Results – Cataract Surgery OutcomeResults – Cataract Surgery Outcome
22 % of the 109 eyes that had undergone cataract surgery had a poor outcome (i.e VA<6/60) with best correction;
Best corrected, good visual outcome (>6/18) was estimated as 64.2%;
109 eyes had cataract surgery with 79% having an IOL implant.
22 % of the 109 eyes that had undergone cataract surgery had a poor outcome (i.e VA<6/60) with best correction;
Best corrected, good visual outcome (>6/18) was estimated as 64.2%;
109 eyes had cataract surgery with 79% having an IOL implant.

Results – Cataract SurgeryResults – Cataract Surgery 99% of all surgeries performed were at
public health facilities; 19.3% were using spectacles after cataract
surgery.
99% of all surgeries performed were at public health facilities;
19.3% were using spectacles after cataract surgery.

KEY FINDINGS - ProductivityKEY FINDINGS - Productivity Demand and Supply mismatch. Number
of surgeries not enough to match “incidence”.
Low surgical Productivity CSR in Eastern Cape province = 1022 Required CSR = 4,000
“Unaware of treatment”(63.7%, SVI-57.8%)
Demand and Supply mismatch. Number of surgeries not enough to match “incidence”.
Low surgical Productivity CSR in Eastern Cape province = 1022 Required CSR = 4,000
“Unaware of treatment”(63.7%, SVI-57.8%)