
FINGERTIP INJURIES ARE THEY REALLY THAT SIMPLE?...FINGERTIP INJURIES ARE THEY REALLY THAT SIMPLE?...
32
FINGERTIP INJURIES ARE THEY REALLY THAT SIMPLE? SANJAY K SHARMA, MD, FACS INSTITUTE OF RECONSTRUCTIVE PLASTIC SURGERY Austin Trauma and Critical Care Conference 2018 May 31-June 1, 2018
Transcript of FINGERTIP INJURIES ARE THEY REALLY THAT SIMPLE?...FINGERTIP INJURIES ARE THEY REALLY THAT SIMPLE?...
FINGERTIP INJURIES
ARE THEY REALLY THAT SIMPLE?
SANJAY K SHARMA, MD, FACS
INSTITUTE OF RECONSTRUCTIVE PLASTIC
SURGERY
Austin Trauma and Critical Care Conference 2018
May 31-June 1, 2018
Outline
1. Scope of problem1. Stats
2. Anatomy
3. Case vignettes1. Crush
2. Nail lac
3. Burns
4. Mallet
5. Jersey finger
▪ Solutions DO nothing
Skin graft
Local flaps
Distant flaps
▪ Not going to discuss Nail infections
Abnormal nails
Infections of fingertips
Our hands/fingers
Scope of the problem

Scope of the problem

More like this
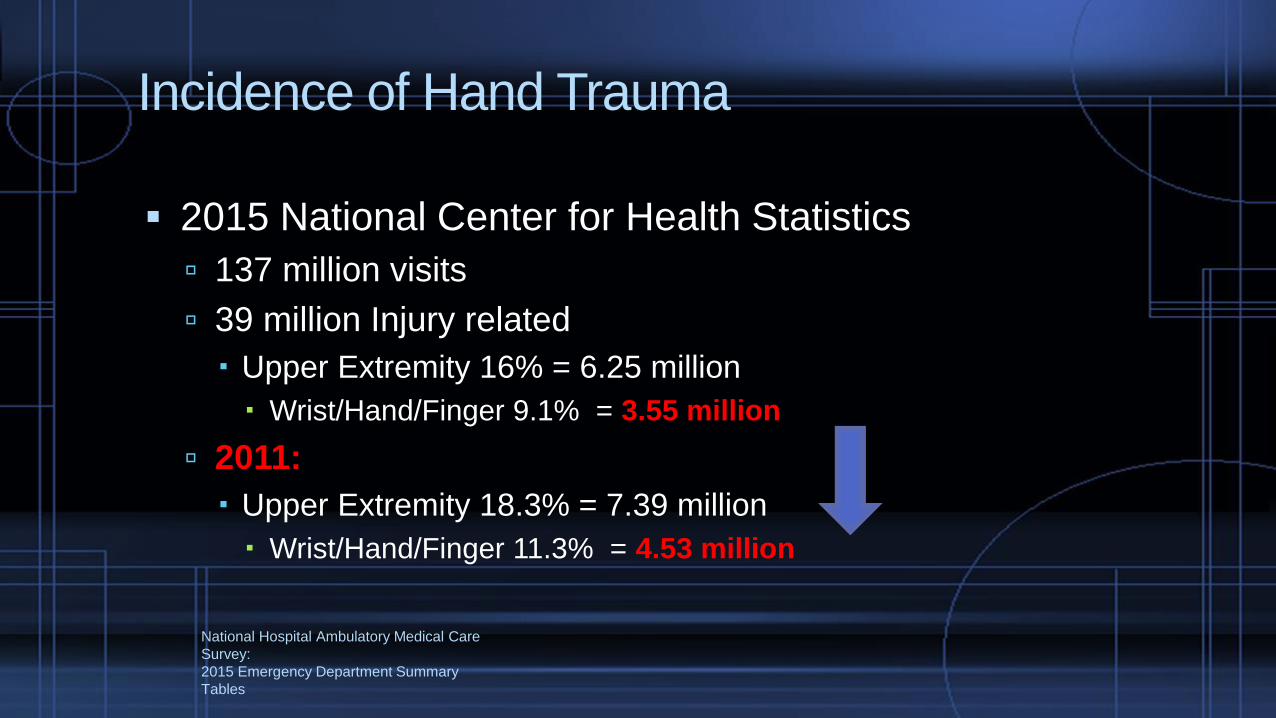
National Hospital Ambulatory Medical Care
Survey:
2015 Emergency Department Summary
Tables
Incidence of Hand Trauma
▪ 2015 National Center for Health Statistics
137 million visits
39 million Injury related
Upper Extremity 16% = 6.25 million
Wrist/Hand/Finger 9.1% = 3.55 million
2011:
Upper Extremity 18.3% = 7.39 million
Wrist/Hand/Finger 11.3% = 4.53 million
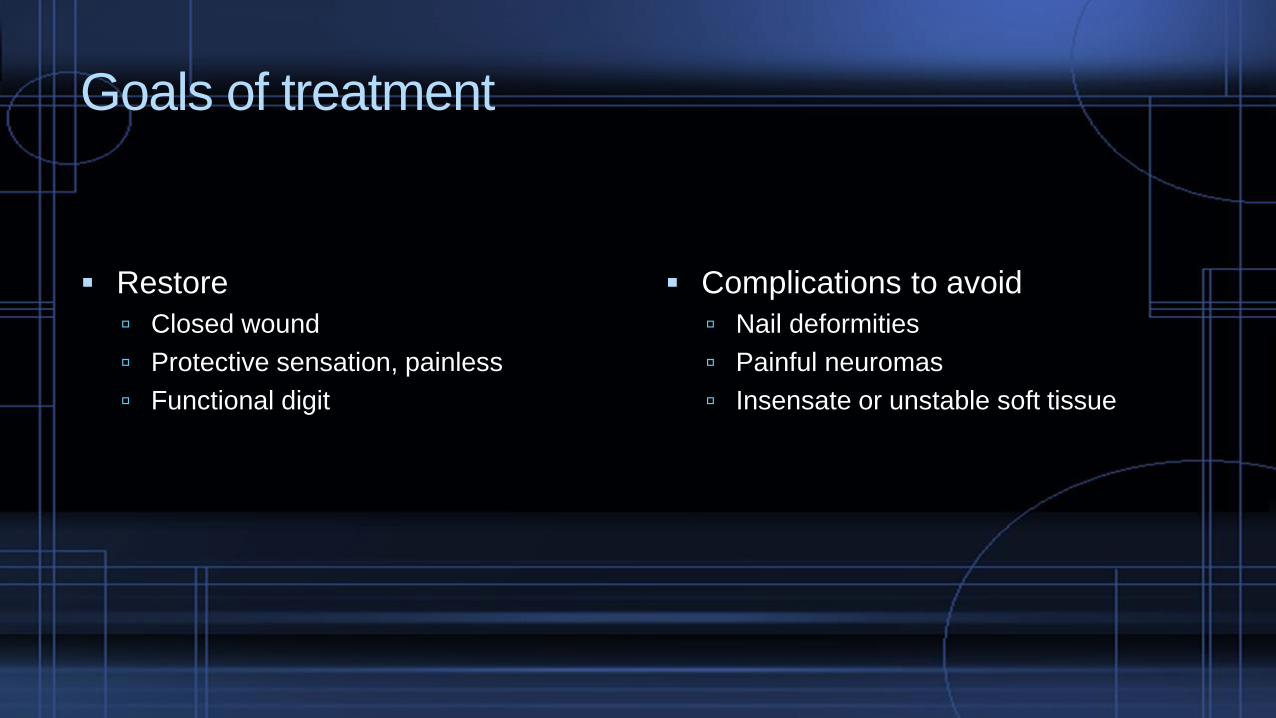
Goals of treatment
▪ Restore
Closed wound
Protective sensation, painless
Functional digit
▪ Complications to avoid
Nail deformities
Painful neuromas
Insensate or unstable soft tissue

Anatomy
▪ Germinal matrix
▪ Sterile matrix
▪ Eponychium
▪ Paronychium
▪ Lunula
▪ Pulp
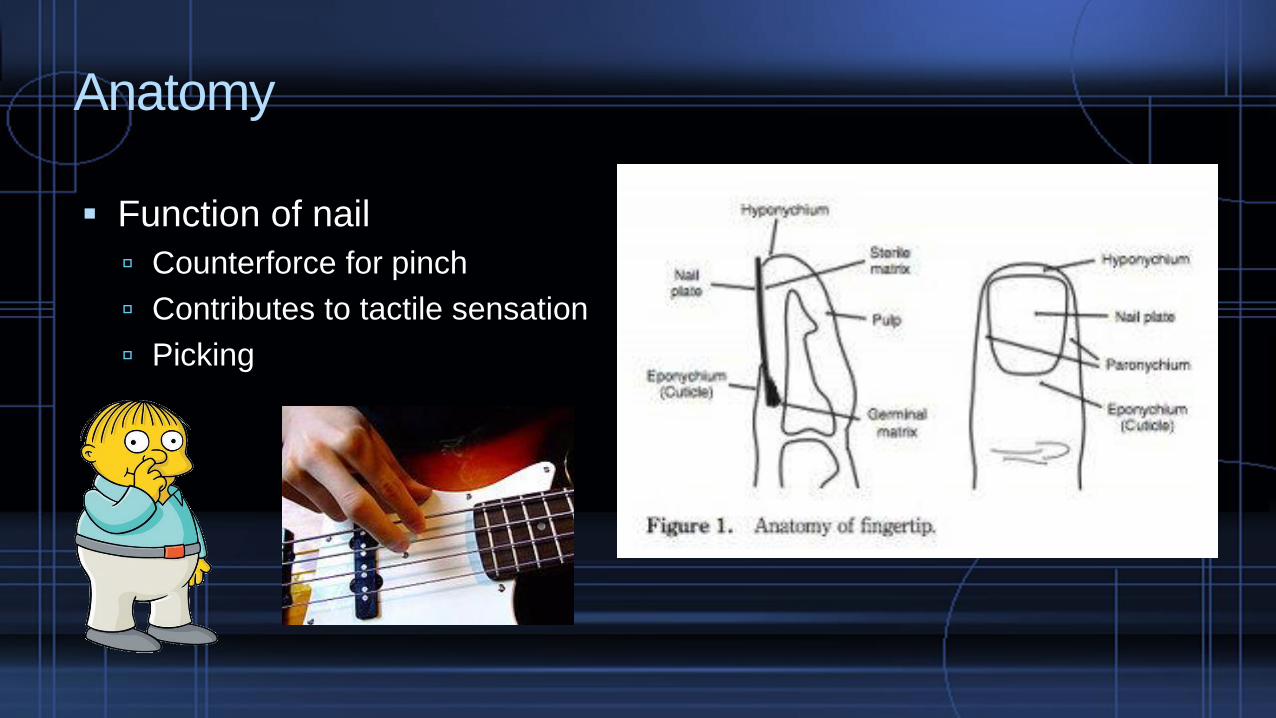
Anatomy
▪ Function of nail
Counterforce for pinch
Contributes to tactile sensation
Picking

Nailbed injury
▪ Common mechanisms
Door
Tools
Crush working
Crush working out
Drill accident
Saw
Nail gun

Injury workup
▪ Detailed History Mechanism of injury
▪ Detailed exam Noting level of finger injury
Nail involvement
▪ X-rays
▪ Comfort Local digital block: Marcaine
YES--OK TO USE EPINEPHRINE
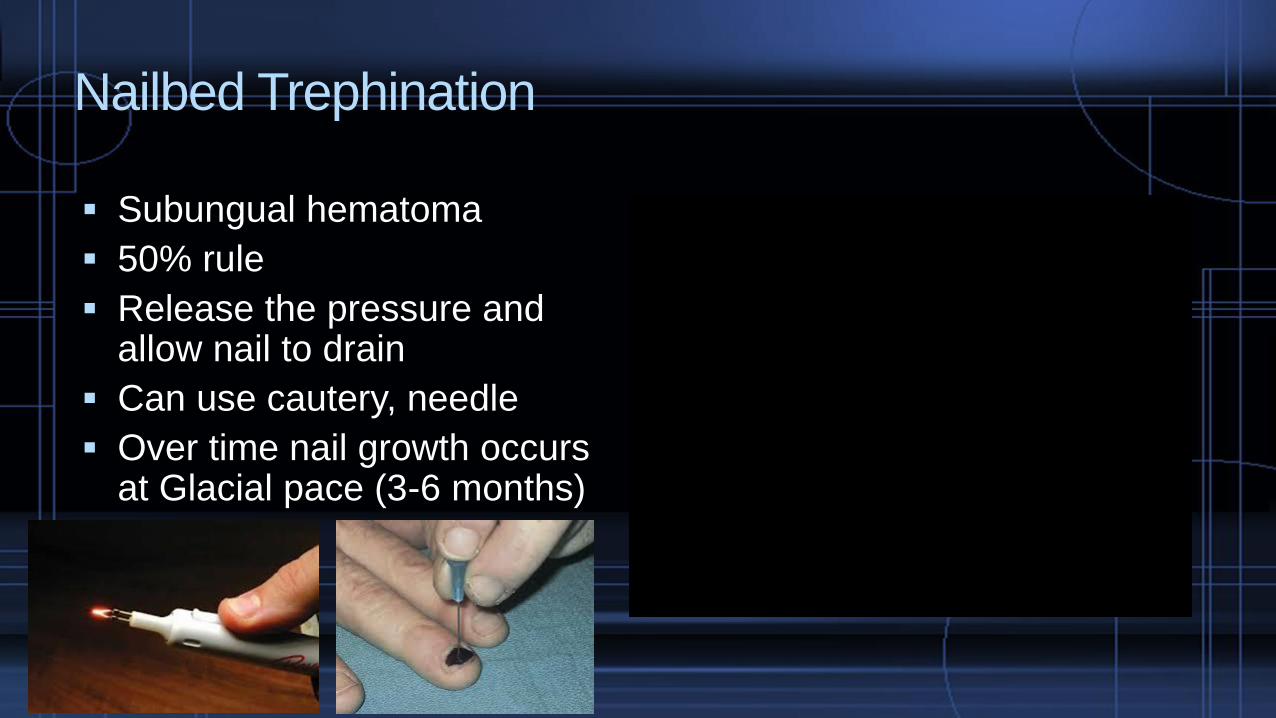
Nailbed Trephination
▪ Subungual hematoma
▪ 50% rule
▪ Release the pressure and allow nail to drain
▪ Can use cautery, needle
▪ Over time nail growth occurs at Glacial pace (3-6 months)
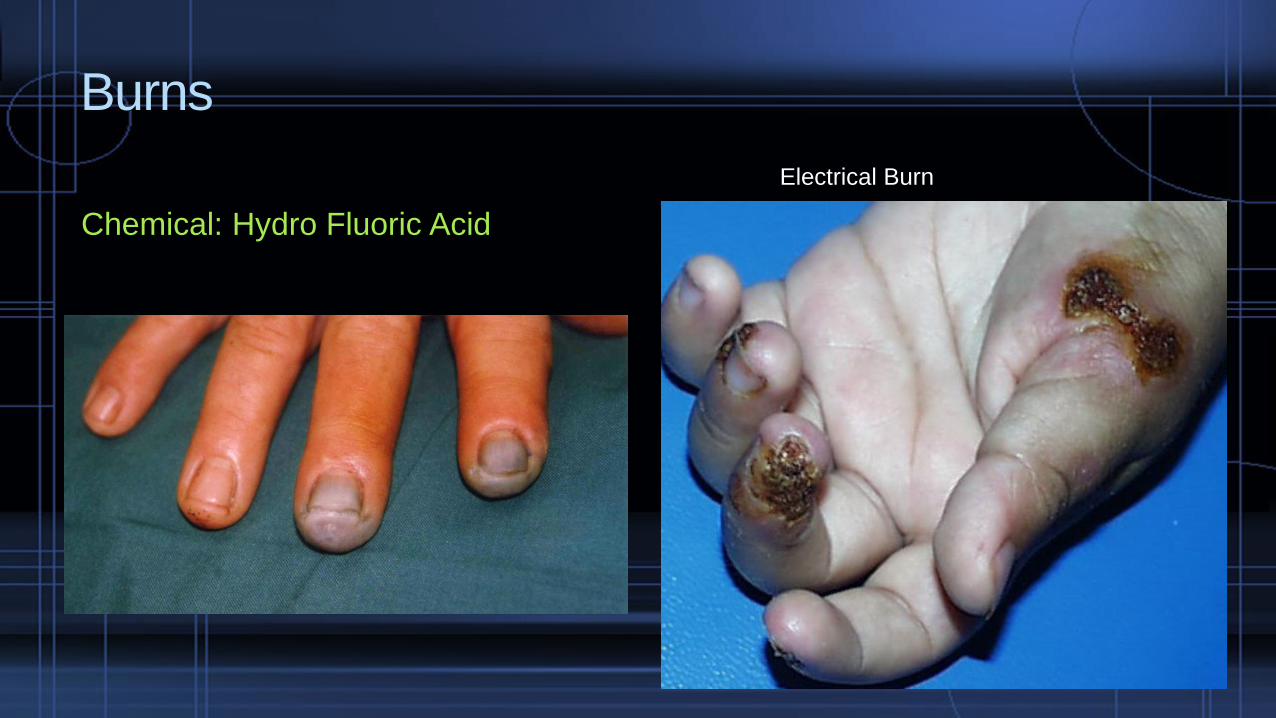
Burns
Chemical: Hydro Fluoric Acid Scalding
Electrical Burn
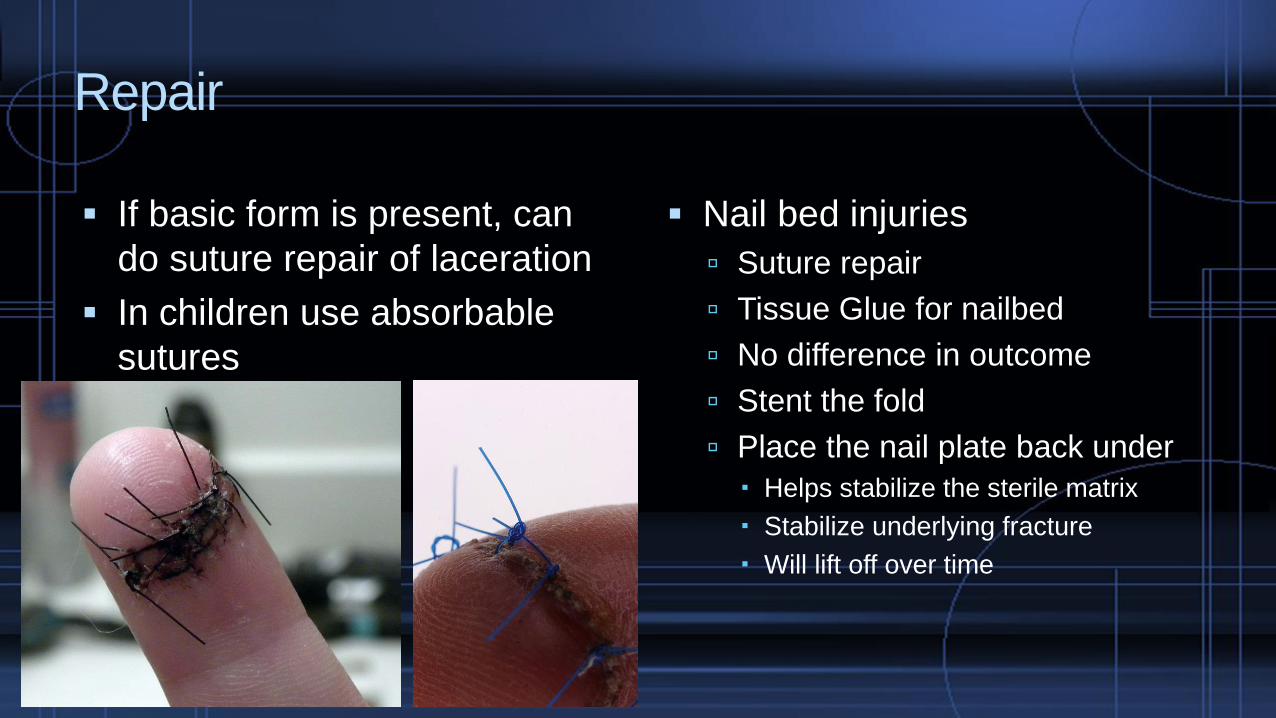
Repair
▪ If basic form is present, can
do suture repair of laceration
▪ In children use absorbable
sutures
▪ Nail bed injuries
Suture repair
Tissue Glue for nailbed
No difference in outcome
Stent the fold
Place the nail plate back under
Helps stabilize the sterile matrix
Stabilize underlying fracture
Will lift off over time
Open Fracture?
▪ Technically yes, open
▪ Rates 0.3-11%
▪ Infection Not Likely for common
mechanisms of injury
Crush, laceration, mechanical
tools
Clean, irrigated, stabilized <24 h
Antibiotics? Tendency to No, but if
going to treat should be less than
72 hours
▪ Beware of these injuries
Animal bites
Human bites
Seymour Fractures
Contaminated, comminuted and
multi-fragmented soft tissue
injury
Delay in presentation
Prophylactic antibiotics in open distal phalanx fractures: systematic review and meta-
analysis.
Metcalfe D, Aquilina AL, Hedley HM.
J Hand Surg Eur Vol. 2016 May;41(4):423-30
The High Risk of Infection With Delayed Treatment of Open Seymour
Fractures: Salter-Harris I/II or Juxta-epiphyseal Fractures of the Distal
Phalanx With Associated Nailbed Laceration.
Reyes BA, Ho CA.
J Pediatr Orthop. 2017 Jun;37(4):247-253

Repair

Need for more coverage—local Flaps
V-Y Flap

Reconstruction/Flaps
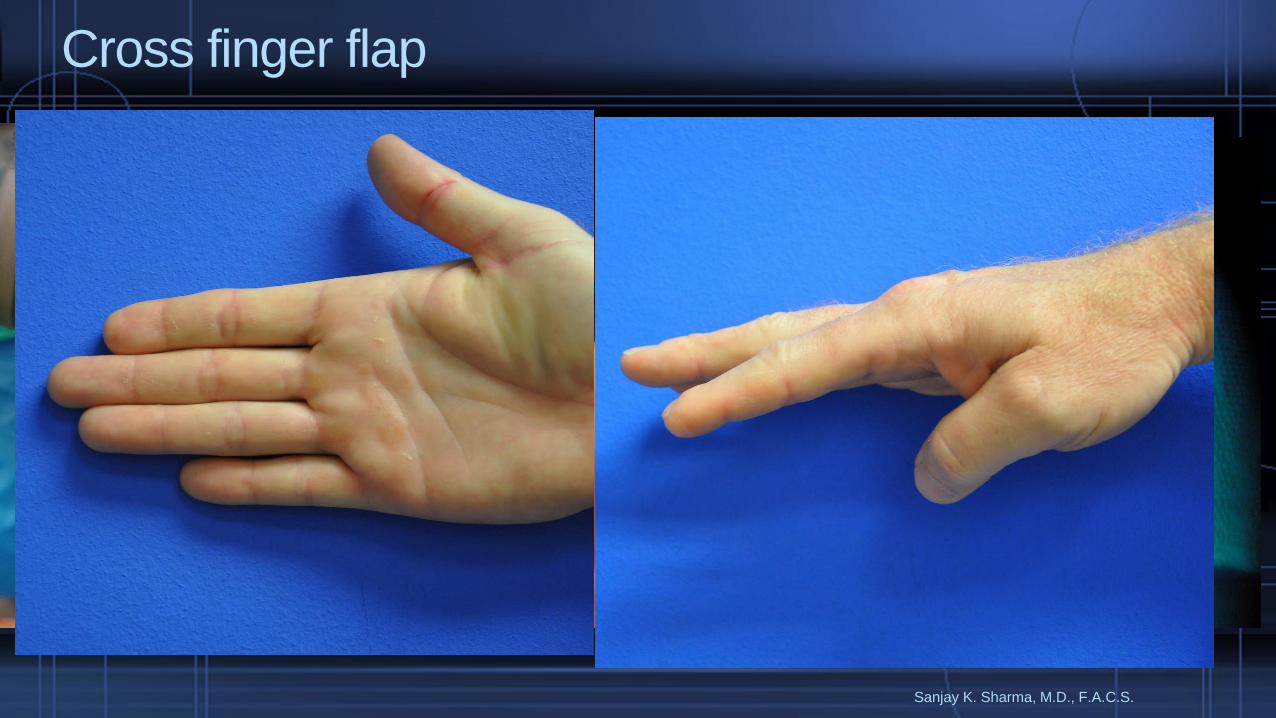
Sanjay K. Sharma, M.D., F.A.C.S.
Cross finger flap
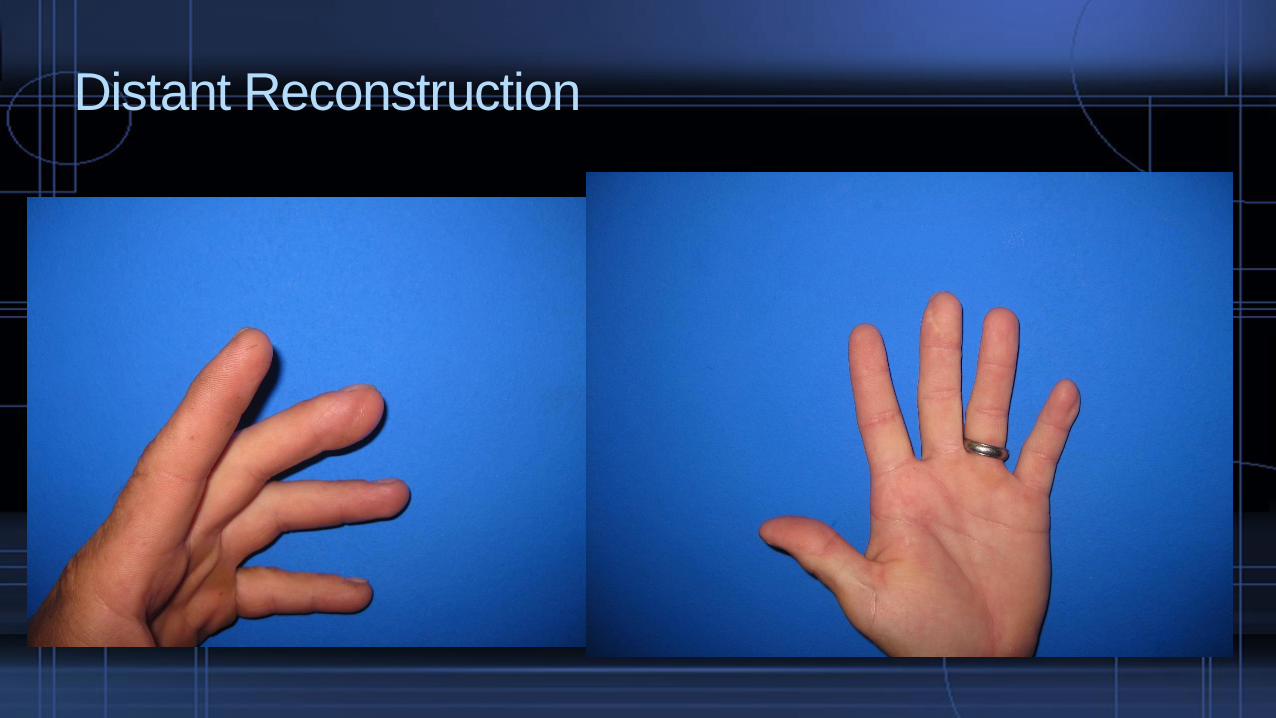
Distant Reconstruction

Then there’s this…Fingertip injuries after all
Make due with what you’re given
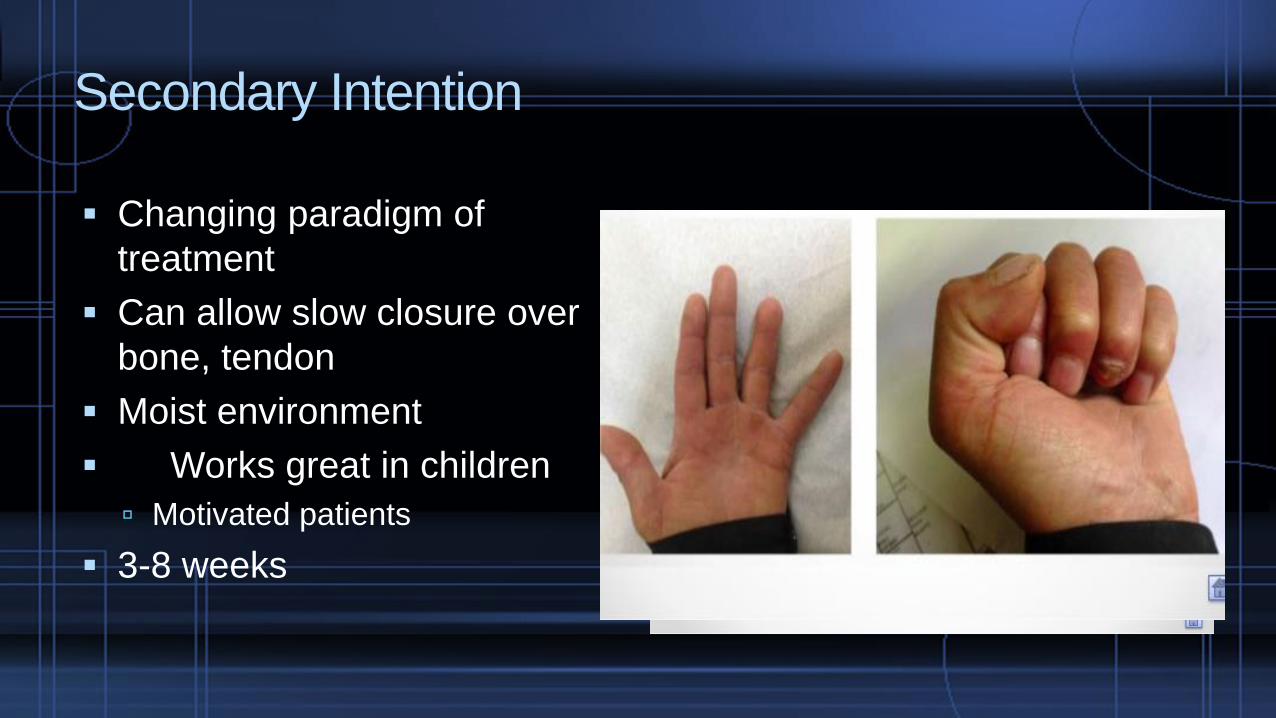
Secondary Intention
▪ Changing paradigm of
treatment
▪ Can allow slow closure over
bone, tendon
▪ Moist environment
▪ Works great in children
Motivated patients
▪ 3-8 weeks
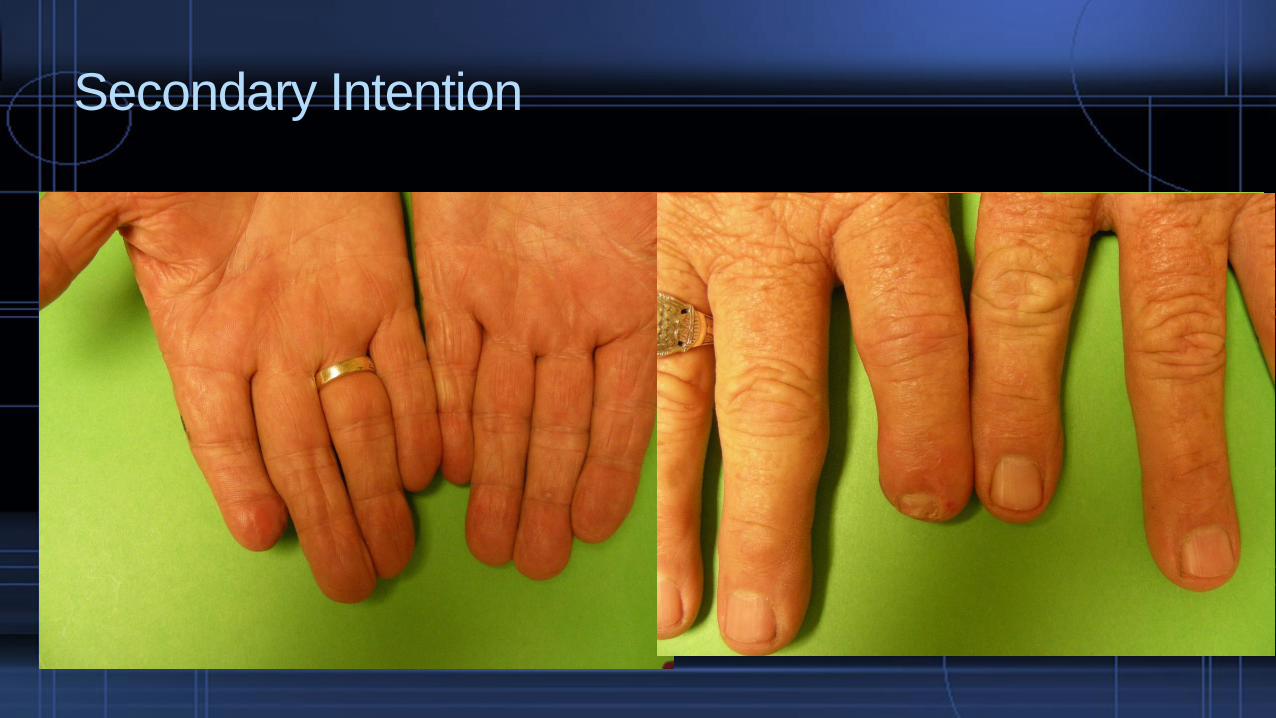
Secondary Intention

Time Lapse video

Pediatric Fingertips
Most common hand injury in child
Amputations vs soft tissue crush injuries
Supportive care: dressing changes and
splints if distal phalynx fracture
Ultimately good result

Trauma--Fingertips
▪ Seymour Fracture
Displaced physeal or juxtaphyseal distal phalanx fracture
Proximal nail avulsion with nailbed laceration
Open fracture

Unusual variation of fingertip injuries
▪ Mallet Finger
Axial injury
hyperflexion
▪ Boutonniere Deformity
Dislocations
Lacerations
Axial injury
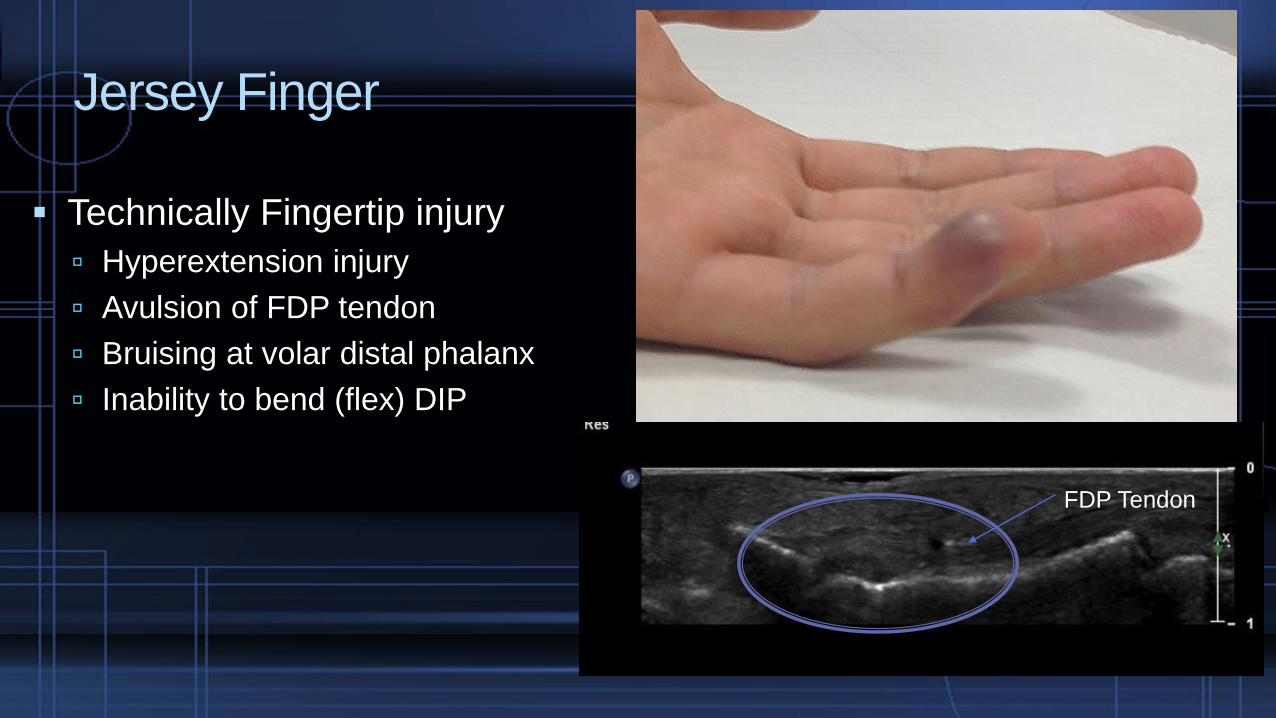
Jersey Finger
▪ Technically Fingertip injury
Hyperextension injury
Avulsion of FDP tendon
Bruising at volar distal phalanx
Inability to bend (flex) DIP
FDP Tendon

Summary
▪ Fingertip Injuries major
healthcare burden
Patient
ED Provider
Workplace/Employer
Physician
▪ Take away points:
Repair accurately
Restore sensate tip with flaps
Realize most if not all Fingertip
injuries will heal spontaneously
Consult your hand surgeon as
needed for guidance

Thank You
















