FINALco-infections-malignancies-hepatitisEW mini ... · 1 BHIVA ‘Best of CROI’ Feedback...
25
2/26/2009 1 BHIVA ‘Best of CROI’ Feedback Meetings Opportunistic infections Hepatitis Co-infections Malignancies February 2009, Manchester, Birmingham, London Opportunistic infection/hepatitis co- infection & malignancies Opportunistic infection: Primary prophylaxis for cryptococcal infection Prednisolone for TB-IRIS Early vs. late HAART in cryptococcal meningitis Early vs. late HAART in TB (SAPIT) Once daily NVP vs. EFV in TB
Transcript of FINALco-infections-malignancies-hepatitisEW mini ... · 1 BHIVA ‘Best of CROI’ Feedback...
2/26/2009
1
BHIVA ‘Best of CROI’ Feedback MeetingsOpportunistic infections
Hepatitis Co-infectionsMalignancies
February 2009, Manchester, Birmingham, London
Opportunistic infection/hepatitis co-infection & malignancies
�Opportunistic infection:� Primary prophylaxis for cryptococcal infection
� Prednisolone for TB-IRIS
� Early vs. late HAART in cryptococcal meningitis
� Early vs. late HAART in TB (SAPIT)
� Once daily NVP vs. EFV in TB
2/26/2009
2
Opportunistic infection/hepatitis co-infection & malignancies
�Malignancies� KS-IRIS in SSA
� Infection and non-infection related NADC
�Hepatitis co-infection� Hyaluronic acid
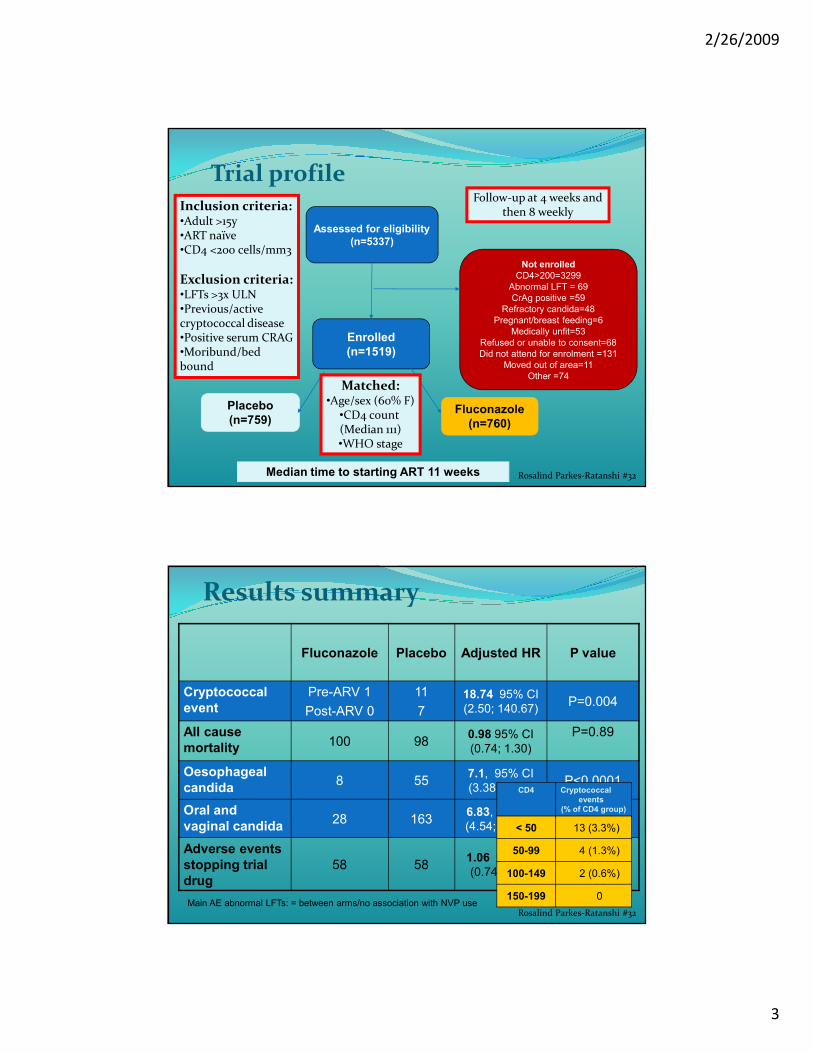
Primary prophylaxis of cryptococcal disease using fluconazole prophylaxis� Aim:
� To determine if routine fluconazole prophylaxis in HIV
infected Ugandan adults can reduce invasive cryptococcal
disease and all cause mortality
� Design:
� Double blind randomised placebo controlled trial
� Fluconazole 200mg 3x week compared with identical placebo
� Enrolment Sept 2004-Jan 2008: follow up till May 2008
� Primary outcomes:
� Incidence of invasive cryptococcal disease
� All cause mortalityRosalind Parkes-Ratanshi #32
2/26/2009
3
Trial profile
Assessed for eligibility
(n=5337)
Not enrolled
CD4>200=3299
Abnormal LFT = 69
CrAg positive =59
Refractory candida=48
Pregnant/breast feeding=6
Medically unfit=53
Refused or unable to consent=68
Did not attend for enrolment =131
Moved out of area=11
Other =74
Enrolled
(n=1519)
Fluconazole
(n=760)
Placebo
(n=759)
Inclusion criteria:•Adult >15y•ART naïve•CD4 <200 cells/mm3
Exclusion criteria:•LFTs >3x ULN•Previous/active cryptococcal disease•Positive serum CRAG•Moribund/bed bound
Matched:•Age/sex (60% F)
•CD4 count (Median 111)•WHO stage
Rosalind Parkes-Ratanshi #32Median time to starting ART 11 weeks
Follow-up at 4 weeks and then 8 weekly
Results summary
Fluconazole Placebo Adjusted HR P value
Cryptococcal
event
Pre-ARV 1
Post-ARV 0
11
7
18.74 95% CI
(2.50; 140.67)P=0.004
All cause
mortality100 98
0.98 95% CI
(0.74; 1.30)
P=0.89
Oesophageal
candida8 55
7.1, 95% CI
(3.38;14.92)P<0.0001
Oral and
vaginal candida28 163
6.83, 95% CI
(4.54; 10.27), P<0.001
Adverse events
stopping trial
drug
58 581.06 95% CI
(0.74; 1.53)P=0.74
CD4 Cryptococcal
events
(% of CD4 group)
< 50 13 (3.3%)
50-99 4 (1.3%)
100-149 2 (0.6%)
150-199 0
Rosalind Parkes-Ratanshi #32Main AE abnormal LFTs: = between arms/no association with NVP use
2/26/2009
4
Conclusions� Significant reduction in cryptococcal disease, oesophageal
candidiasis, and oral/vaginal candidiasis� Rate of cryptococcal infection was low because of:
� Exclusion of CrAg positive at screening � Early ART� Only 50% had CD4 count less than 100 cells/mm3
� No difference in all-cause mortality � Only 7 deaths attributed to cryptococcal disease
� Implications for clinical practice � In African clinical practice unlikely to have CrAg screening
and limited access to ART and effective cryptococcal treatment
� Fluconazole prophylaxis may have potentially even greater impact in this setting
Rosalind Parkes-Ratanshi #32
Prednisolone for TB-IRIS
� Background: occurs in 8-43%, anecdotal reports steroids beneficial but concerns may worsen KS/CMV
� Hypothesis: 4w prednisolone would reduce need for medical interventions, be safe and not ↑ infections
� Design:� Prednisolone or placebo, randomised double blind
� 1.5mg/kg for 2 weeks then 0.75mg/kg for 2 weeks
� Follow-up assessments: 1, 2, 4, 8, and 12 weeks
� Open-label at physicians’ discretion if clinical deterioration/relapse
� Primary endpoint:� Cumulative number of days and OPD therapeutic procedures
(arbitrarily counted as 1 additional day), ITT analysisMeintges #35
2/26/2009
5
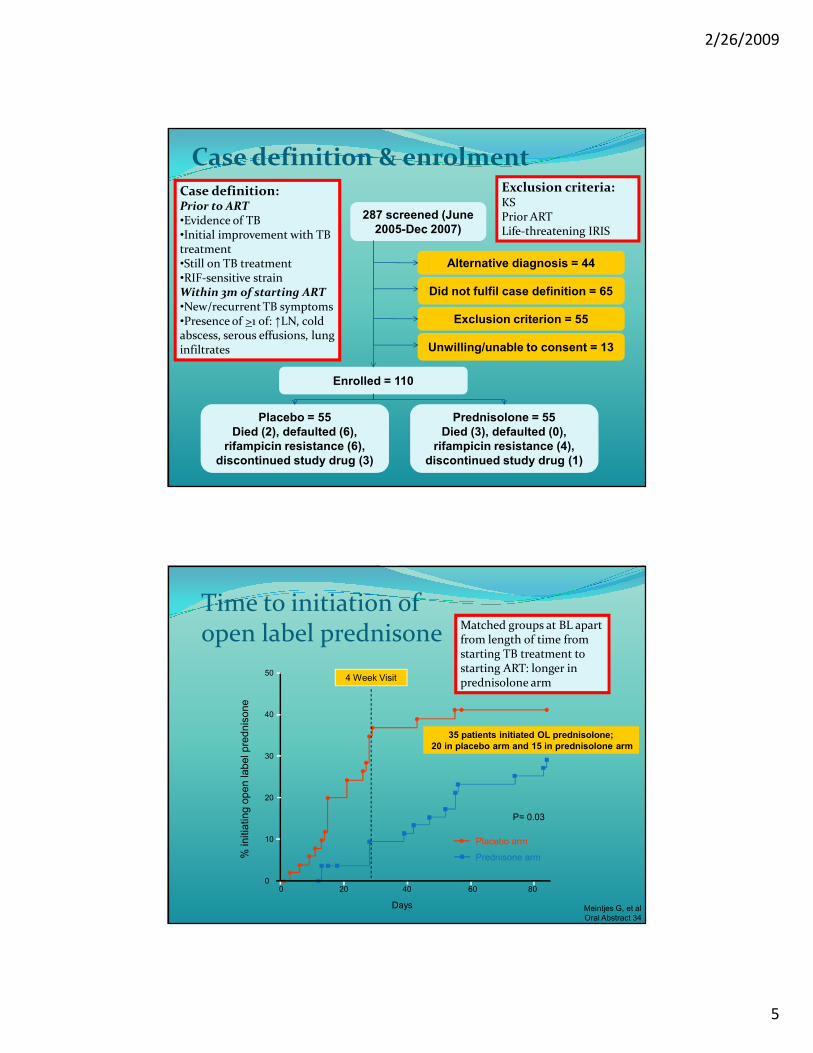
Case definition & enrolment
287 screened (June
2005-Dec 2007)
Alternative diagnosis = 44
Did not fulfil case definition = 65
Exclusion criterion = 55
Unwilling/unable to consent = 13
Enrolled = 110
Placebo = 55
Died (2), defaulted (6),
rifampicin resistance (6),
discontinued study drug (3)
Prednisolone = 55
Died (3), defaulted (0),
rifampicin resistance (4),
discontinued study drug (1)
Case definition:Prior to ART•Evidence of TB•Initial improvement with TB treatment•Still on TB treatment•RIF-sensitive strainWithin 3m of starting ART•New/recurrent TB symptoms•Presence of >1 of: ↑LN, cold abscess, serous effusions, lung infiltrates
Exclusion criteria:KSPrior ARTLife-threatening IRIS
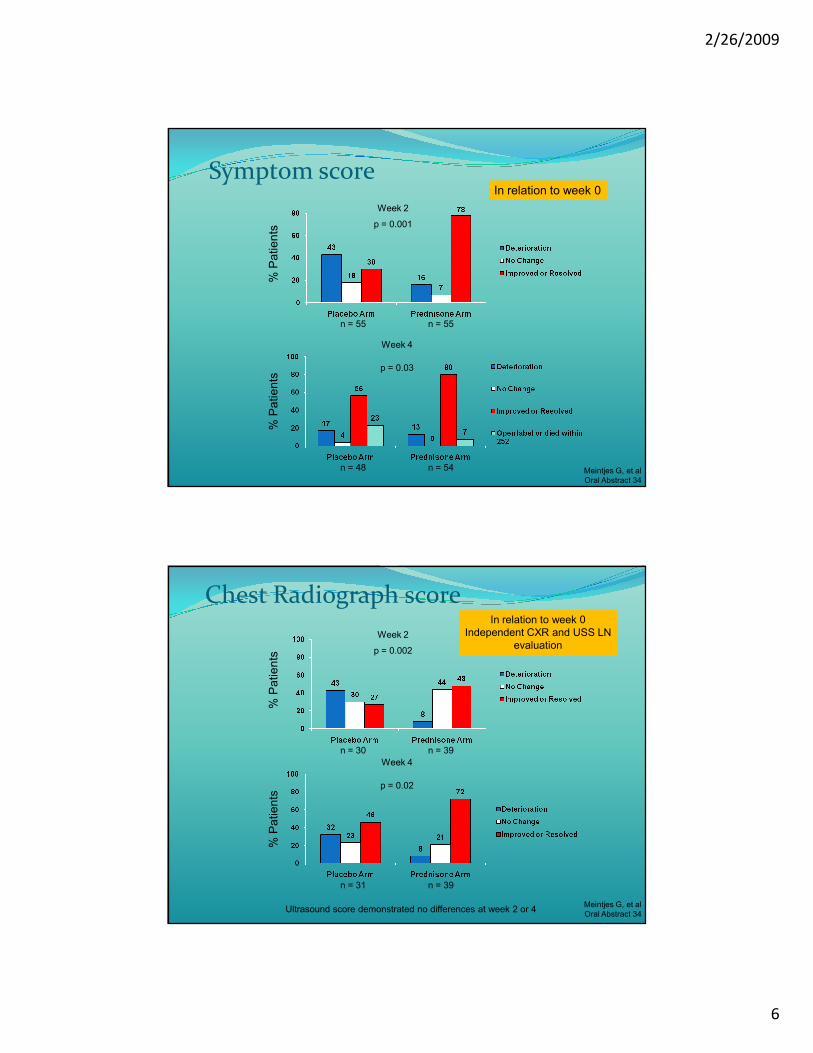
Time to initiation of open label prednisone
50
40
30
20
0
10
% initia
ting o
pen label pre
dnis
one
200 40 60 80
Placebo arm
Prednisone arm
P= 0.03
4 Week Visit
Days Meintjes G, et al
Oral Abstract 34
Matched groups at BL apart from length of time from starting TB treatment to starting ART: longer in prednisolone arm
35 patients initiated OL prednisolone;
20 in placebo arm and 15 in prednisolone arm
2/26/2009
6
Symptom score
Week 4
Week 2
p = 0.001
p = 0.03
n = 55 n = 55
n = 48 n = 54
% P
atie
nts
% P
atie
nts
Meintjes G, et al
Oral Abstract 34
In relation to week 0
Chest Radiograph score
Week 4
Week 2
p = 0.002
p = 0.02
n = 30 n = 39
n = 31 n = 39
% P
atie
nts
% P
atie
nts
Ultrasound score demonstrated no differences at week 2 or 4 Meintjes G, et al
Oral Abstract 34
In relation to week 0
Independent CXR and USS LN
evaluation
2/26/2009
7
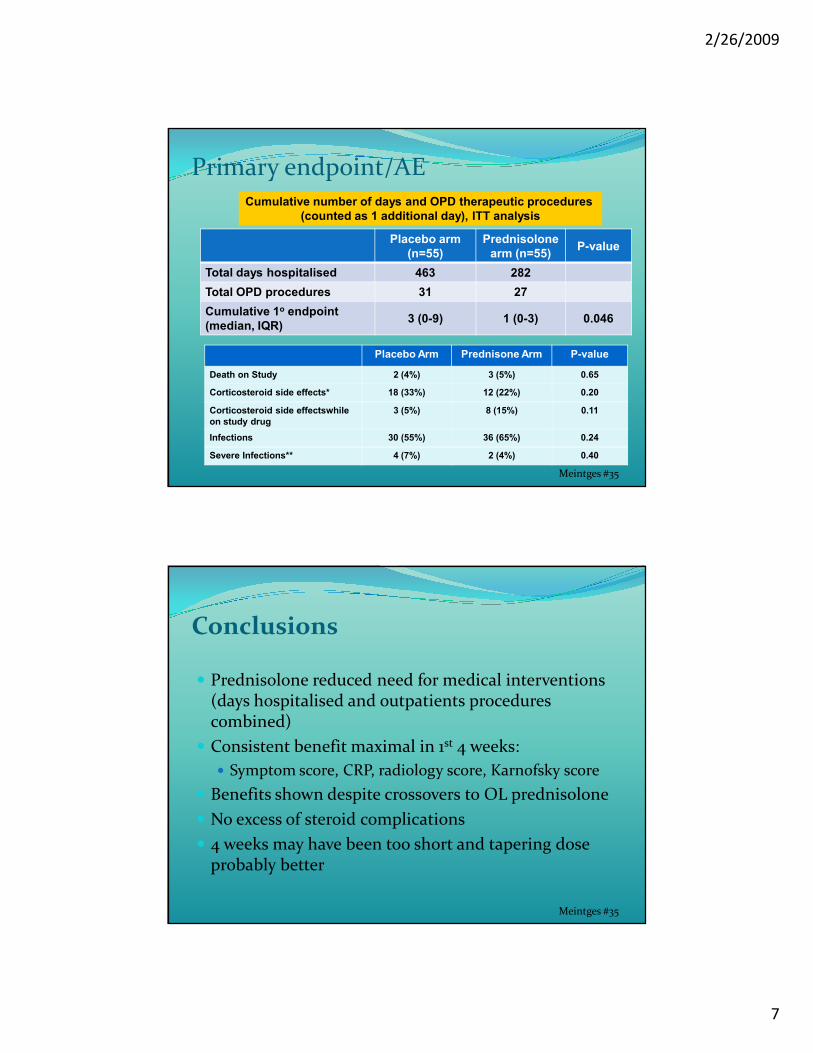
Primary endpoint/AE
Placebo arm
(n=55)
Prednisolone
arm (n=55)P-value
Total days hospitalised 463 282
Total OPD procedures 31 27
Cumulative 1o endpoint
(median, IQR)3 (0-9) 1 (0-3) 0.046
Cumulative number of days and OPD therapeutic procedures
(counted as 1 additional day), ITT analysis
Meintges #35
Placebo Arm Prednisone Arm P-value
Death on Study 2 (4%) 3 (5%) 0.65
Corticosteroid side effects* 18 (33%) 12 (22%) 0.20
Corticosteroid side effectswhile
on study drug
3 (5%) 8 (15%) 0.11
Infections 30 (55%) 36 (65%) 0.24
Severe Infections** 4 (7%) 2 (4%) 0.40
Conclusions
� Prednisolone reduced need for medical interventions (days hospitalised and outpatients procedures combined)
� Consistent benefit maximal in 1st 4 weeks:
� Symptom score, CRP, radiology score, Karnofsky score
� Benefits shown despite crossovers to OL prednisolone
� No excess of steroid complications
� 4 weeks may have been too short and tapering dose probably better
Meintges #35
2/26/2009
8
Early vs. deferred HAART in cryptococcal meningitis� Primary aim: to determine if immediate ART vs.
delayed ART improves survival and decreases risk of relapse in CM, a leading cause of death in SSA
� Study design:� 2 groups: (AMP B/5-FLU generally unavailable)
� Fluconazole 800mg od orally for 10w starting NVP/D4T/3TC <72h
� Fluconazole 800mg od orally for 10w starting NVP/D4T/3TC at end of 10w
� After 10 weeks all patients maintained on fluconazole 200mg daily and HAART
� All patients received NVP/D4T/3TC Makadzange #36cLB
Early vs. deferred HAART in cryptococcal meningitis
� Study design (cont’d)� Inclusion criteria:
� +ve CRAG or Indian Ink stain in CSF
� Exclusion criteria:� Previous diagnosis/treatment CM� Current ARV� Medications interacting with FLU (e.g., RIF-based regimens)� Major co-morbidities
� LP’s at 0, 2, 4, 10 and more frequently if required
� Patients:� N=26 early treatment group –23 completed till endpoint
reached� N=28 late treatment group – 27 completed till endpoint
reached
Makadzange #36cLB
2/26/2009
9
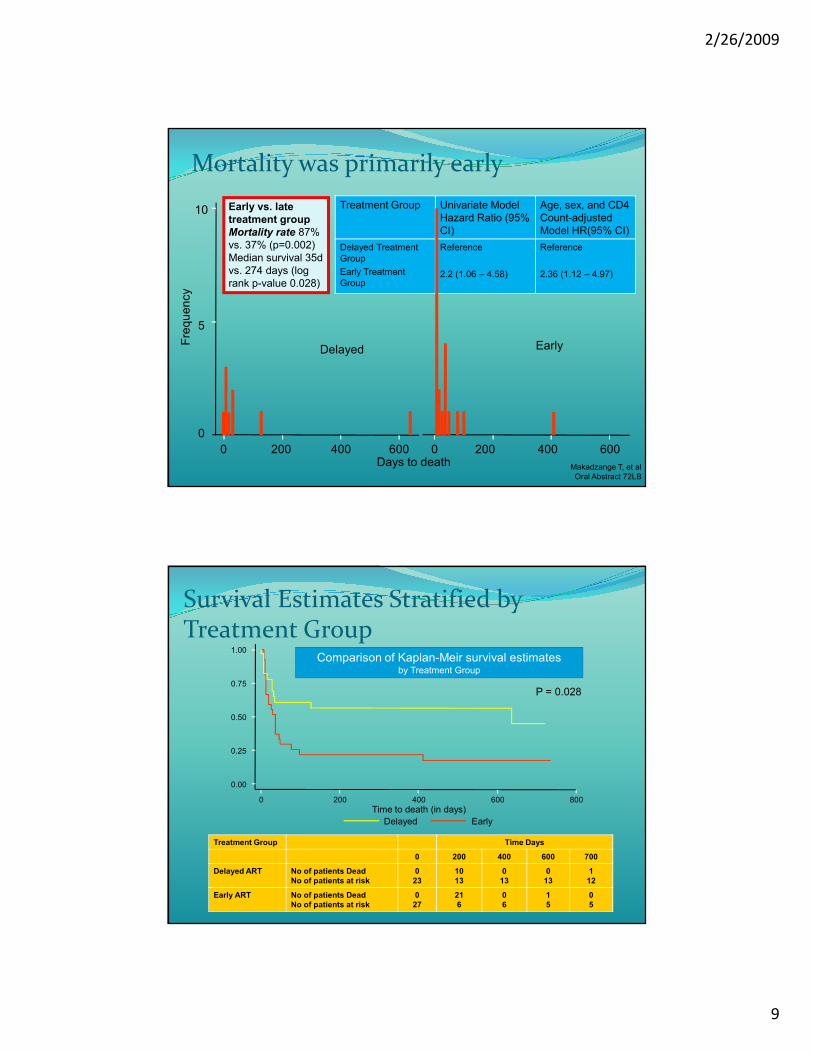
Mortality was primarily early
0 200 400 600Days to death
Delayed Early
0 200 400 600
0
5
10
Fre
qu
en
cy
Makadzange T, et al
Oral Abstract 72LB
Treatment Group Univariate Model
Hazard Ratio (95%
CI)
Age, sex, and CD4
Count-adjusted
Model HR(95% CI)
Delayed Treatment
Group
Early Treatment
Group
Reference
2.2 (1.06 – 4.58)
Reference
2.36 (1.12 – 4.97)
Early vs. late
treatment group
Mortality rate 87%
vs. 37% (p=0.002)
Median survival 35d
vs. 274 days (log
rank p-value 0.028)
Survival Estimates Stratified by Treatment Group
0.00
0.25
0.50
0.75
1.00
0 200 400 600 800
Time to death (in days)
Delayed Early
Comparison of Kaplan-Meir survival estimatesby Treatment Group
P = 0.028
Treatment Group Time Days
0 200 400 600 700
Delayed ART No of patients Dead
No of patients at risk
0
23
10
13
0
13
0
13
1
12
Early ART No of patients Dead
No of patients at risk
0
27
21
6
0
6
1
5
0
5
2/26/2009
10
Conclusions
� Cause of death presumed to be CM
� Early initiation of therapy resulted in increased mortality rates
� Most mortality occurs in the first 4 weeks
� Completely opposite to ACTG 5164
� Is excess mortality related to IRIS or progression of severe disease?
� Suboptimal therapy (higher doses of FLU or AMP B/5-FLU might be more effective)
� Is it related to interaction with NVP and FLU metabolism?
Makadzange #36cLB
SAPIT: Starting ARV therapy at three Points in TB� Primary objective:
� To determine the optimal time to initiate ARVs in TB patients (TB major entry into ARV programmes)
� Inclusion criteria:
� Smear +ve & on standard TB treatment
� HIV +ve with CD4 count <500cells/mm3
� Women using contraception (EFV being used)
� Endpoints:
� Primary – All-cause mortality
� Secondary - Tolerability, toxicity, VL, CD4, TB outcomes & IRIS rate Karim #36a
2/26/2009
11
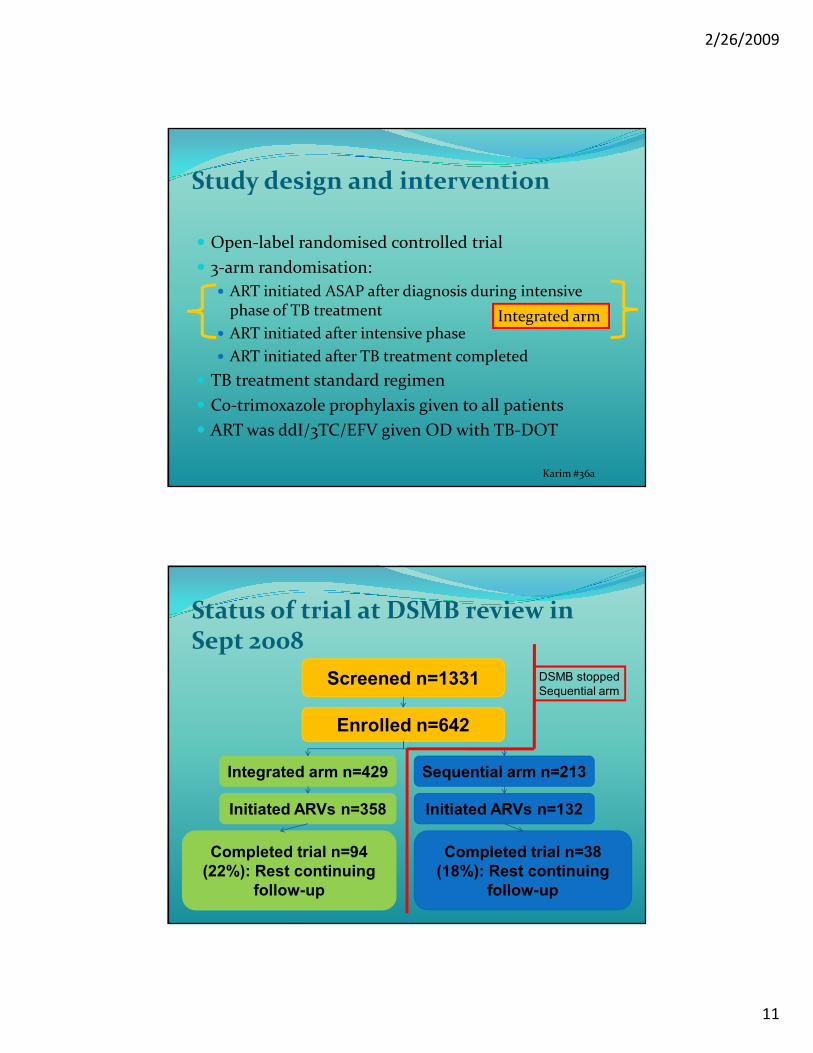
Study design and intervention
� Open-label randomised controlled trial
� 3-arm randomisation:
� ART initiated ASAP after diagnosis during intensive phase of TB treatment
� ART initiated after intensive phase
� ART initiated after TB treatment completed
� TB treatment standard regimen
� Co-trimoxazole prophylaxis given to all patients
� ART was ddI/3TC/EFV given OD with TB-DOT
Integrated arm
Karim #36a
Status of trial at DSMB review in Sept 2008
Screened n=1331
Enrolled n=642
Integrated arm n=429 Sequential arm n=213
Initiated ARVs n=358 Initiated ARVs n=132
Completed trial n=94
(22%): Rest continuing
follow-up
Completed trial n=38
(18%): Rest continuing
follow-up
DSMB stopped
Sequential arm
2/26/2009
12
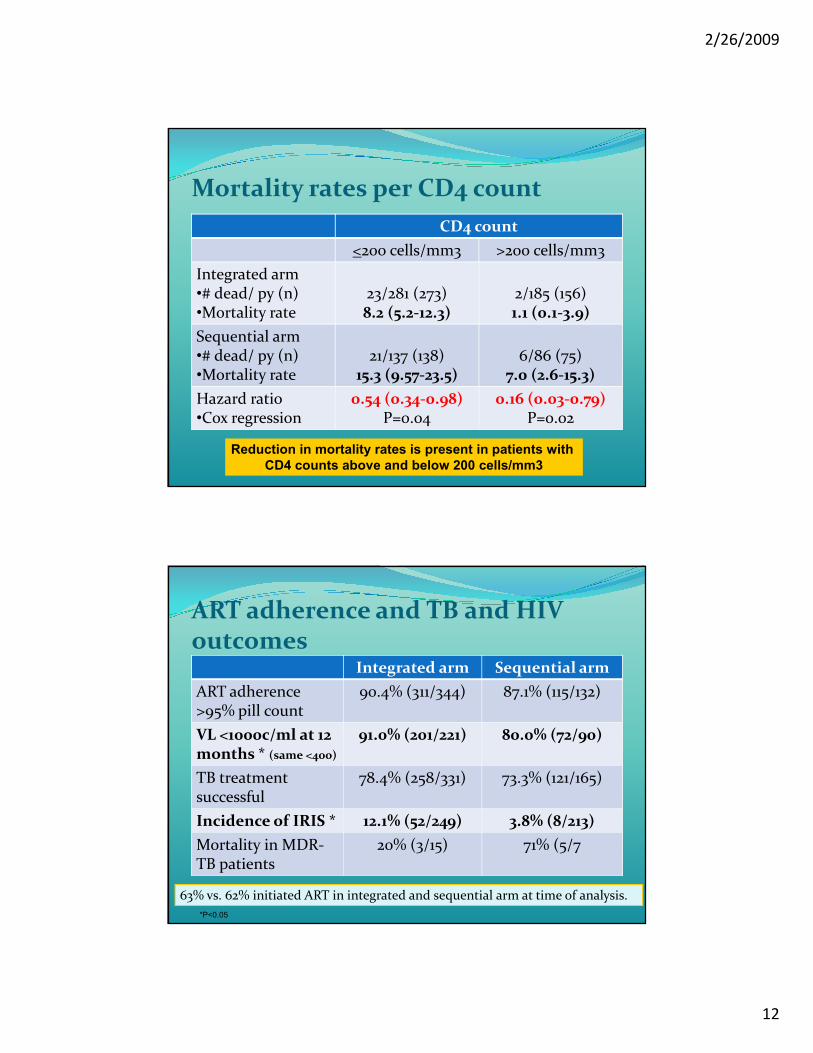
Mortality rates per CD4 count
CD4 count
<200 cells/mm3 >200 cells/mm3
Integrated arm•# dead/ py (n)•Mortality rate
23/281 (273)8.2 (5.2-12.3)
2/185 (156)1.1 (0.1-3.9)
Sequential arm•# dead/ py (n)•Mortality rate
21/137 (138)15.3 (9.57-23.5)
6/86 (75)7.0 (2.6-15.3)
Hazard ratio•Cox regression
0.54 (0.34-0.98)P=0.04
0.16 (0.03-0.79)P=0.02
Reduction in mortality rates is present in patients with
CD4 counts above and below 200 cells/mm3
ART adherence and TB and HIV outcomes
Integrated arm Sequential arm
ART adherence >95% pill count
90.4% (311/344) 87.1% (115/132)
VL <1000c/ml at 12 months * (same <400)
91.0% (201/221) 80.0% (72/90)
TB treatment successful
78.4% (258/331) 73.3% (121/165)
Incidence of IRIS * 12.1% (52/249) 3.8% (8/213)
Mortality in MDR-TB patients
20% (3/15) 71% (5/7
63% vs. 62% initiated ART in integrated and sequential arm at time of analysis.
*P<0.05
2/26/2009
13
Conclusions
� Outcome at halt of sequential arm:
� Deaths: integrated arm (25/429), sequential arm (27/213): HR 0.44 (95% CI 0.25-0.79) P=0.003
� Reduced mortality with integrated treatment (56%)
� TB outcomes similar in both arms
� IRIS rate higher in the integrated treatment arm
� VL suppression higher in the integrated treatment arm
� 2 integrated treatment arms of SAPIT continuing (ASAP vs. after initiation phase)
Karim #36a
Once daily NVP vs. EFV in the treatment of HIV/TB� Aim:
� To compare efficacy and safety of two NNRTI regimens given once daily in patients with TB receiving standard TB treatment (EFV preferred but NVP more available)
� Design:
� Randomised non-inferiority open-label CT
� Randomised to EFV or NVP OD after 8w of TB treatment with ddI/3TC
� NVP given with 2w lead in dose of 200mg
� Standard TB treatment given for 6m
� Patients received DOT for TBSwaminathan #35
2/26/2009
14
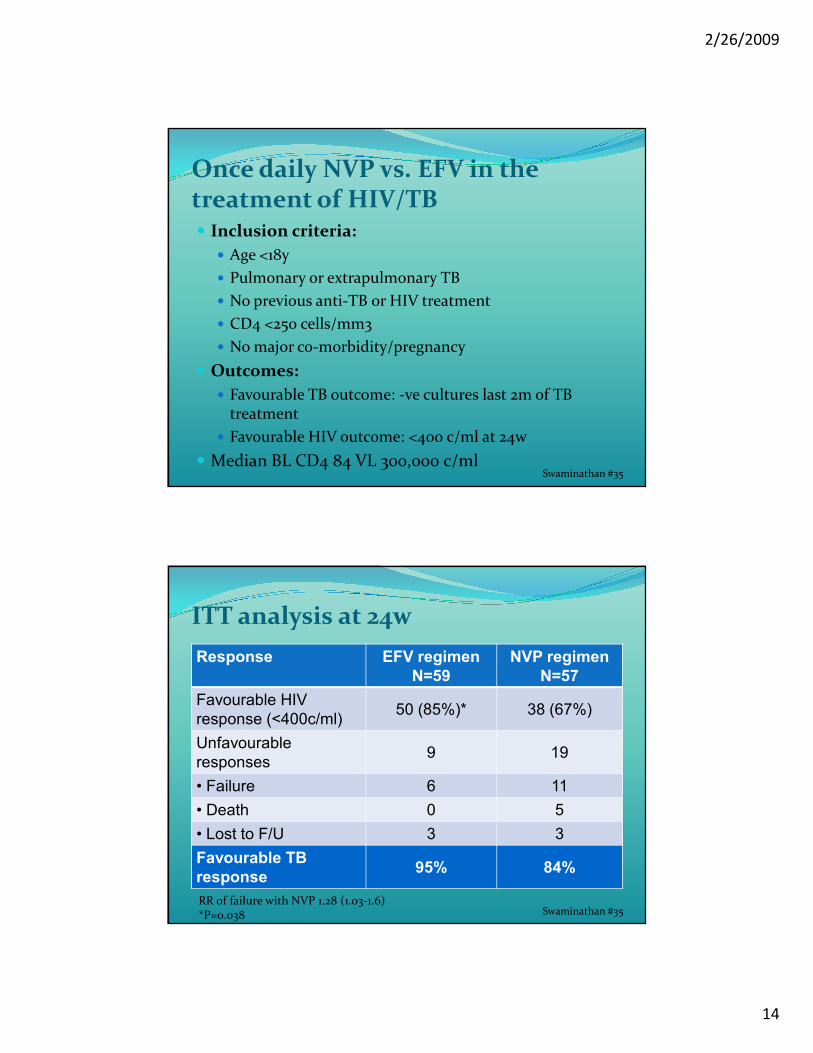
Once daily NVP vs. EFV in the treatment of HIV/TB� Inclusion criteria:
� Age <18y
� Pulmonary or extrapulmonary TB
� No previous anti-TB or HIV treatment
� CD4 <250 cells/mm3
� No major co-morbidity/pregnancy
� Outcomes:
� Favourable TB outcome: -ve cultures last 2m of TB treatment
� Favourable HIV outcome: <400 c/ml at 24w
� Median BL CD4 84 VL 300,000 c/mlSwaminathan #35
ITT analysis at 24w
Response EFV regimen
N=59
NVP regimen
N=57
Favourable HIV
response (<400c/ml)50 (85%)* 38 (67%)
Unfavourable
responses9 19
• Failure 6 11
• Death 0 5
• Lost to F/U 3 3
Favourable TB
response95% 84%
RR of failure with NVP 1.28 (1.03-1.6)*P=0.038 Swaminathan #35
2/26/2009
15
Conclusions
� 3TC/ddI/EFV good virological outcome (85%) and safety with dosing advantages of ddI over d4T:
� Caveats pregnancy and cost
� OD NVP inferior to EFV when given with RIF containing TB treatment
� 90% of patients had a favourable response to TB treatment
� PCK interactions may partly explain:
� RIF induction with NVP lead-in
� Low trough levels with once daily dosing
Swaminathan #35
Opportunistic infection/hepatitis co-infection & malignancies
�Malignancies� KS-IRS in SSA
� Infection and non-infection related NADC
�Hepatitis co-infection� Hyaluronic acid
2/26/2009
16
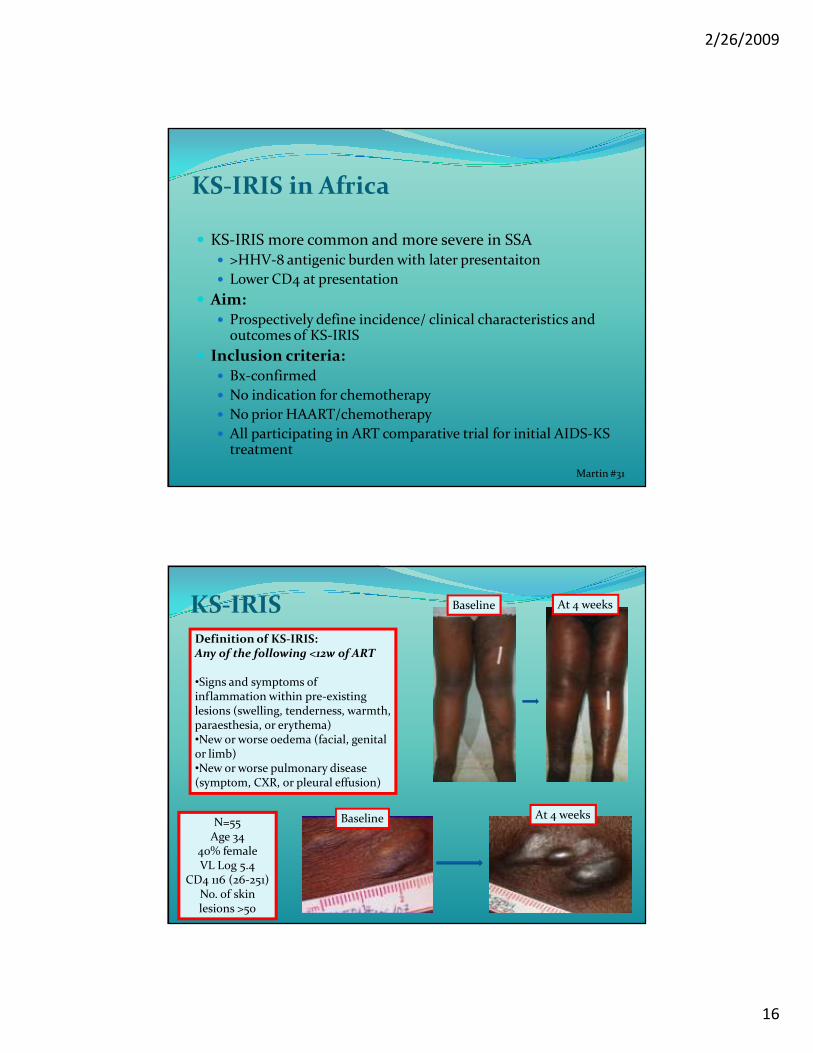
KS-IRIS in Africa
� KS-IRIS more common and more severe in SSA� >HHV-8 antigenic burden with later presentaiton
� Lower CD4 at presentation
� Aim:� Prospectively define incidence/ clinical characteristics and
outcomes of KS-IRIS
� Inclusion criteria:� Bx-confirmed
� No indication for chemotherapy
� No prior HAART/chemotherapy
� All participating in ART comparative trial for initial AIDS-KS treatment
Martin #31
KS-IRISDefinition of KS-IRIS:Any of the following <12w of ART
•Signs and symptoms of inflammation within pre-existing lesions (swelling, tenderness, warmth, paraesthesia, or erythema) •New or worse oedema (facial, genital or limb)•New or worse pulmonary disease (symptom, CXR, or pleural effusion)
N=55Age 34
40% femaleVL Log 5.4
CD4 116 (26-251)No. of skin lesions >50
Baseline At 4 weeks
At 4 weeksBaseline
2/26/2009
17
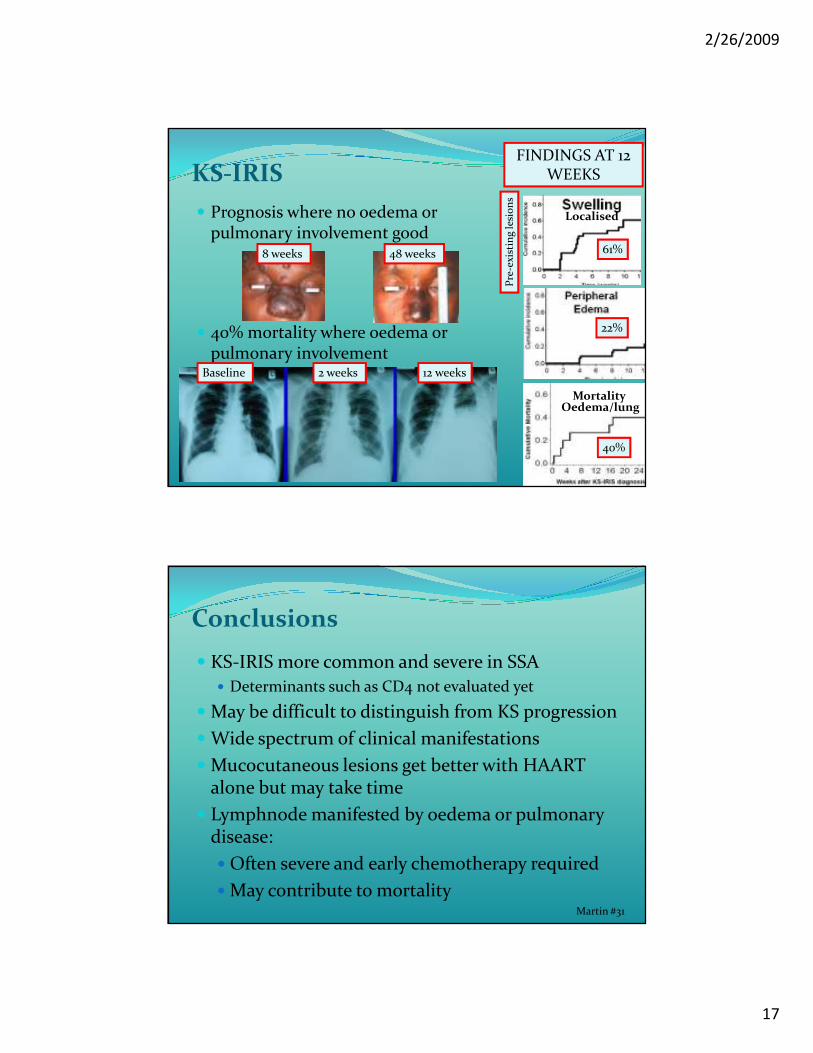
KS-IRIS
� Prognosis where no oedema or pulmonary involvement good
� 40% mortality where oedema or pulmonary involvement
Mortality
FINDINGS AT 12 WEEKS
22%
61%
Baseline 2 weeks 12 weeks
8 weeks 48 weeks
40%
Oedema/lung
Localised
Pre
-exi
stin
g le
sio
ns
Conclusions
� KS-IRIS more common and severe in SSA
� Determinants such as CD4 not evaluated yet
� May be difficult to distinguish from KS progression
� Wide spectrum of clinical manifestations
� Mucocutaneous lesions get better with HAART alone but may take time
� Lymphnode manifested by oedema or pulmonary disease:
� Often severe and early chemotherapy required
� May contribute to mortalityMartin #31
2/26/2009
18
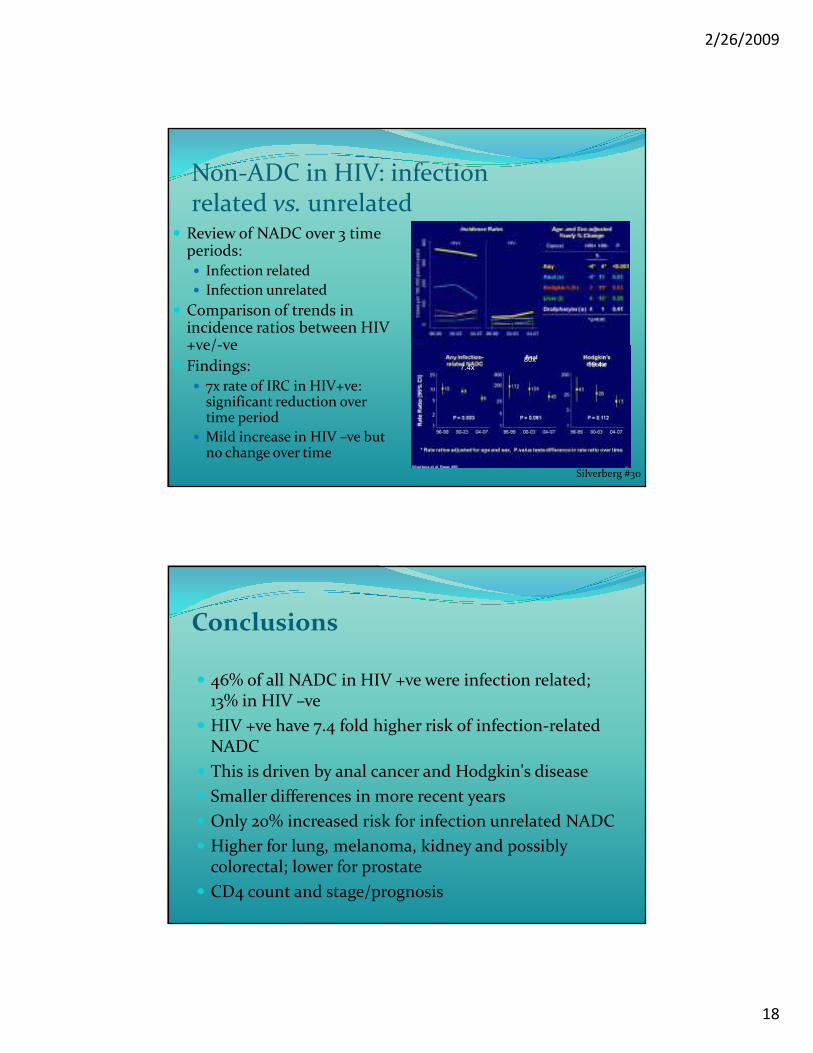
Non-ADC in HIV: infection related vs. unrelated
� Review of NADC over 3 time periods:� Infection related
� Infection unrelated
� Comparison of trends in incidence ratios between HIV +ve/-ve
� Findings:� 7x rate of IRC in HIV+ve:
significant reduction over time period
� Mild increase in HIV –ve but no change over time
Silverberg #30
80x19.4x7.4x
Conclusions
� 46% of all NADC in HIV +ve were infection related; 13% in HIV –ve
� HIV +ve have 7.4 fold higher risk of infection-related NADC
� This is driven by anal cancer and Hodgkin's disease
� Smaller differences in more recent years
� Only 20% increased risk for infection unrelated NADC
� Higher for lung, melanoma, kidney and possibly colorectal; lower for prostate
� CD4 count and stage/prognosis
2/26/2009
19
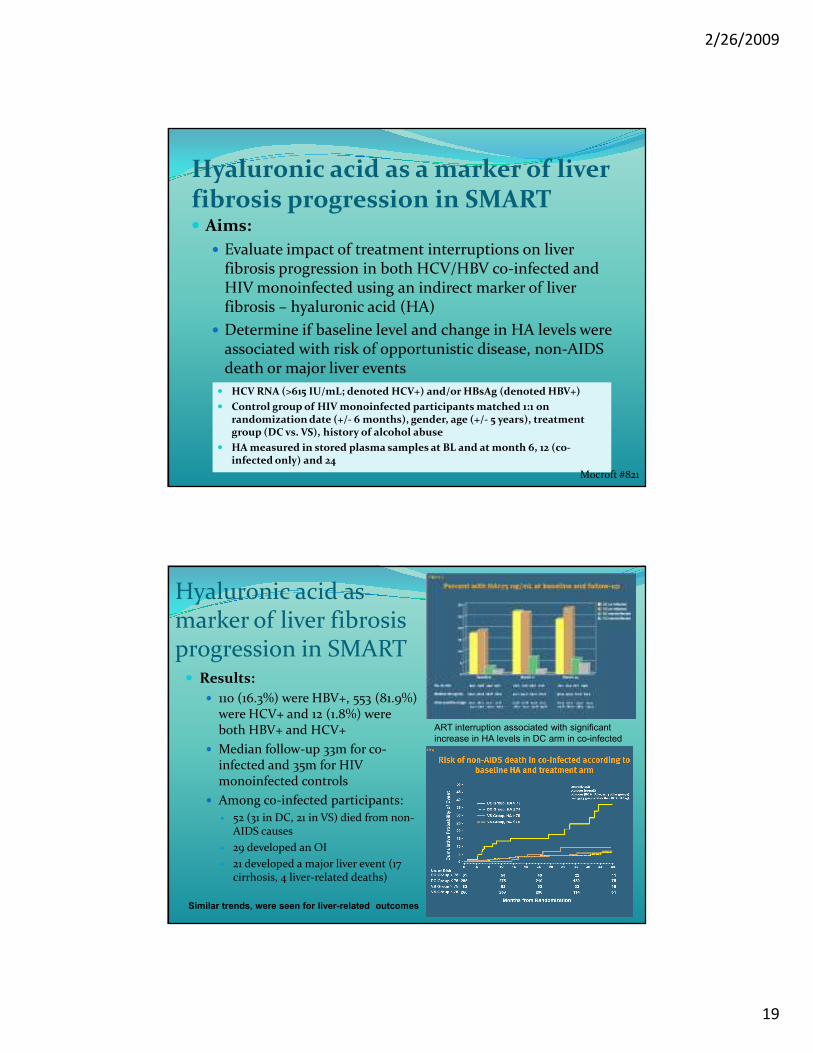
Hyaluronic acid as a marker of liver fibrosis progression in SMART� Aims:
� Evaluate impact of treatment interruptions on liver fibrosis progression in both HCV/HBV co-infected and HIV monoinfected using an indirect marker of liver fibrosis – hyaluronic acid (HA)
� Determine if baseline level and change in HA levels were associated with risk of opportunistic disease, non-AIDS death or major liver events
� HCV RNA (>615 IU/mL; denoted HCV+) and/or HBsAg (denoted HBV+)
� Control group of HIV monoinfected participants matched 1:1 on randomization date (+/- 6 months), gender, age (+/- 5 years), treatment group (DC vs. VS), history of alcohol abuse
� HA measured in stored plasma samples at BL and at month 6, 12 (co-infected only) and 24
Mocroft #821
Hyaluronic acid as marker of liver fibrosis progression in SMART� Results:
� 110 (16.3%) were HBV+, 553 (81.9%) were HCV+ and 12 (1.8%) were both HBV+ and HCV+
� Median follow-up 33m for co-infected and 35m for HIV monoinfected controls
� Among co-infected participants:
� 52 (31 in DC, 21 in VS) died from non-AIDS causes
� 29 developed an OI
� 21 developed a major liver event (17 cirrhosis, 4 liver-related deaths)
Similar trends, were seen for liver-related outcomes
ART interruption associated with significant
increase in HA levels in DC arm in co-infected
2/26/2009
20
Conclusions� Hepatitis co-infected patients had higher median
plasma levels of HA at BL and during follow-up than HIV monoinfected
� Interruption of ART was associated with a significant increase in HA levels at month 6 among co-infected patients randomized to the DC arm but not sustained at months 12 and 24
� Baseline HA was an independent predictor of time to development of non-AIDS death, but not OI disease
� Co-infected patients randomized to the DC arm with a baseline HA level > 75 ng/mL had a 37.5% risk of non-AIDS death after 48 months, whereas the risk was only 5% for those with a baseline HA ≤ 75 ng/mL
Mocroft #821
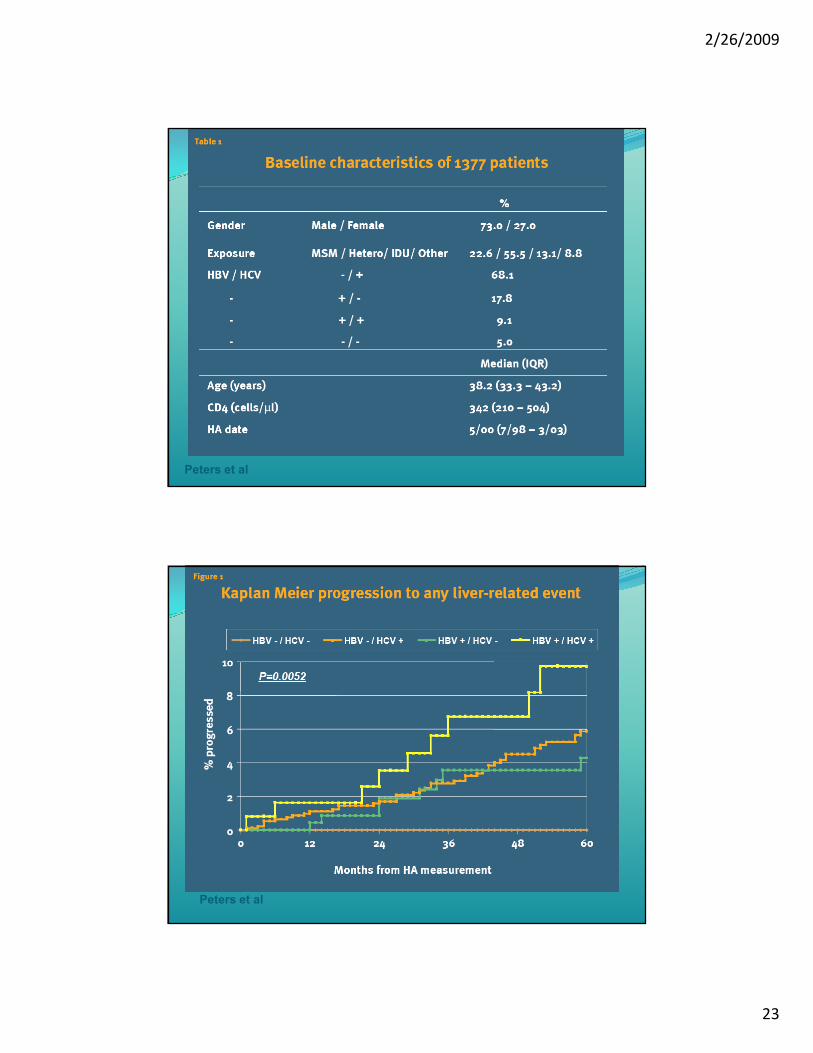
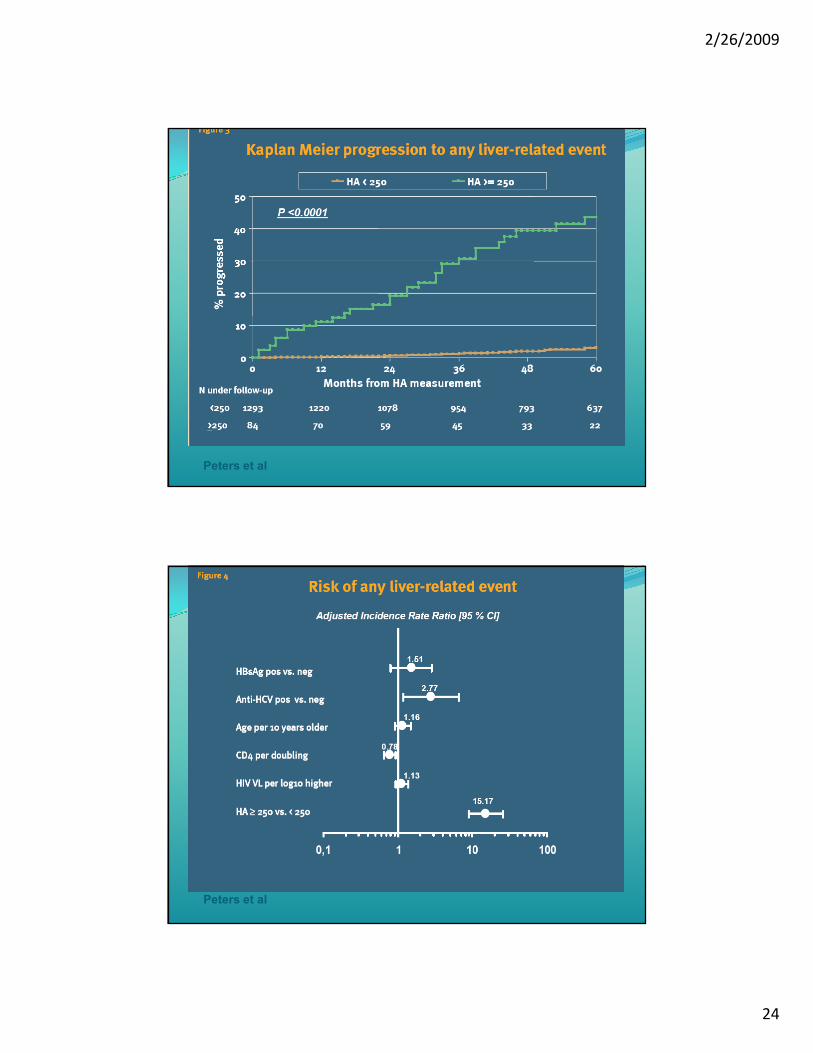
Hyaluronic Acid as a Prognostic Marker of Hepatic Encephalopathy and Liver-related Death in the EUROSIDA study
� Aim:
� To investigate plasma hyaluronic acid (HA) as a prognostic marker for LRE in HIV/viral hepatitis coinfected patients within the EuroSIDA study
� Design:
� 1377 HIV-1 infected patients were included. Of them were 1309 positive for HBsAg (denoted HBV) and/or anti-HCV (denoted HCV). Control group of 68 HIV-monoinfected patients
Peters #821
2/26/2009
21
Conclusions
� Baseline HA level was a very strong predictor of later development hepatic encephalopathy or liver-related death in HIV-1 patients coinfected with HBV +/- HCV
� Patients, who during follow-up experienced a liver-related event, had higher annual increase in HA compared to patients without an event
� High CD4 cell count reduced the risk of increasing HA
� Plasma HA may be useful, either alone or in combination with other non-invasive methods to monitor
� Progression of liver disease in patients with chronic viral hepatitis
Peters #821
Background trials� Powderley 1995 NEJM
� Fluconazole vs. clotrimoxazole alone
� 428 participants, hazard ratio placebo vs. fluconazole 8.5 � 17 cryptococcal events; 2 fluconazole group, 15 control group
� All cause mortality equivalent
� Chetchotisakd 2004 HIV Medicine� Fluconazole vs. placebo
� 90 participants
� 10 cryptococcal events; 3 fluconazole group, 7 control group
� Fluconazole increased survival (HR 4.3 95% CI: 0.9–19.8; p=0.065)
2/26/2009
22
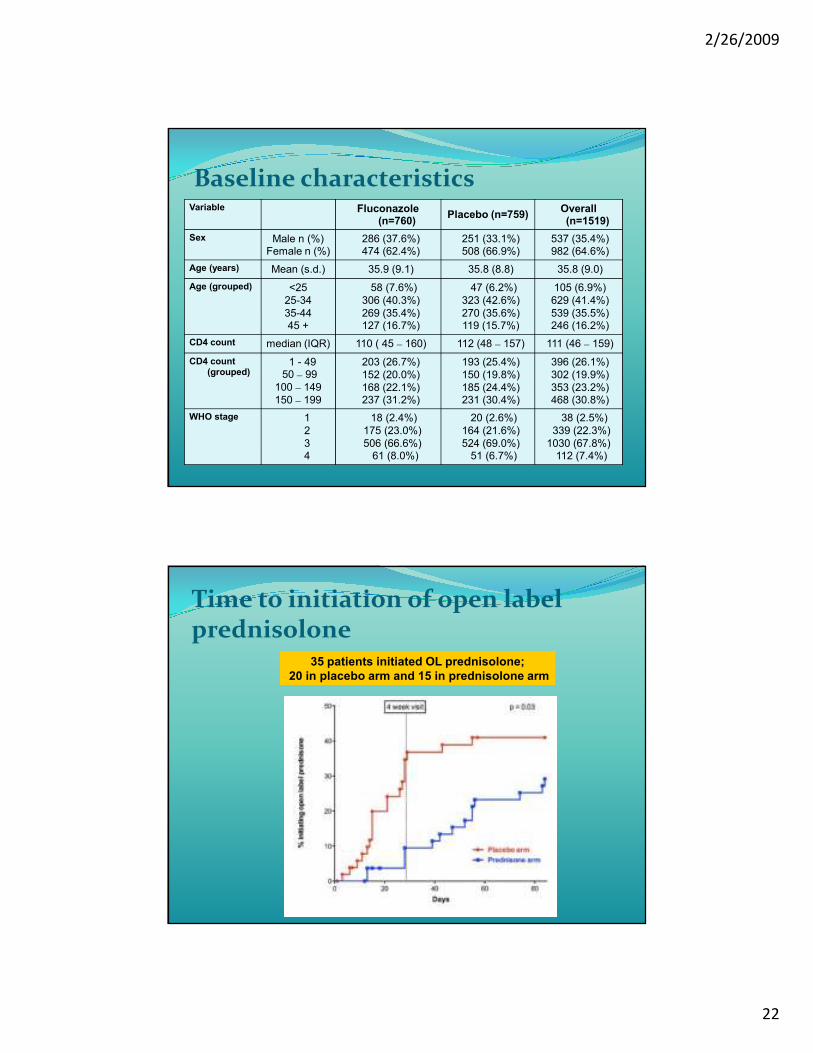
Baseline characteristicsVariable Fluconazole
(n=760)Placebo (n=759)
Overall (n=1519)
Sex Male n (%)Female n (%)
286 (37.6%)474 (62.4%)
251 (33.1%)508 (66.9%)
537 (35.4%)982 (64.6%)
Age (years) Mean (s.d.) 35.9 (9.1) 35.8 (8.8) 35.8 (9.0)
Age (grouped) <25
25-34
35-4445 +
58 (7.6%)
306 (40.3%)
269 (35.4%)127 (16.7%)
47 (6.2%)
323 (42.6%)
270 (35.6%)119 (15.7%)
105 (6.9%)
629 (41.4%)
539 (35.5%)246 (16.2%)
CD4 count median (IQR) 110 ( 45 – 160) 112 (48 – 157) 111 (46 – 159)
CD4 count (grouped)
1 - 4950 – 99
100 – 149
150 – 199
203 (26.7%)
152 (20.0%)
168 (22.1%)237 (31.2%)
193 (25.4%)
150 (19.8%)
185 (24.4%)231 (30.4%)
396 (26.1%)
302 (19.9%)
353 (23.2%)468 (30.8%)
WHO stage 1
2
34
18 (2.4%)
175 (23.0%)
506 (66.6%)61 (8.0%)
20 (2.6%)
164 (21.6%)
524 (69.0%)51 (6.7%)
38 (2.5%)
339 (22.3%)
1030 (67.8%)112 (7.4%)
Time to initiation of open label prednisolone
35 patients initiated OL prednisolone;
20 in placebo arm and 15 in prednisolone arm
2/26/2009
23
Peters et al
Peters et al
2/26/2009
24
Peters et al
Peters et al
2/26/2009
25
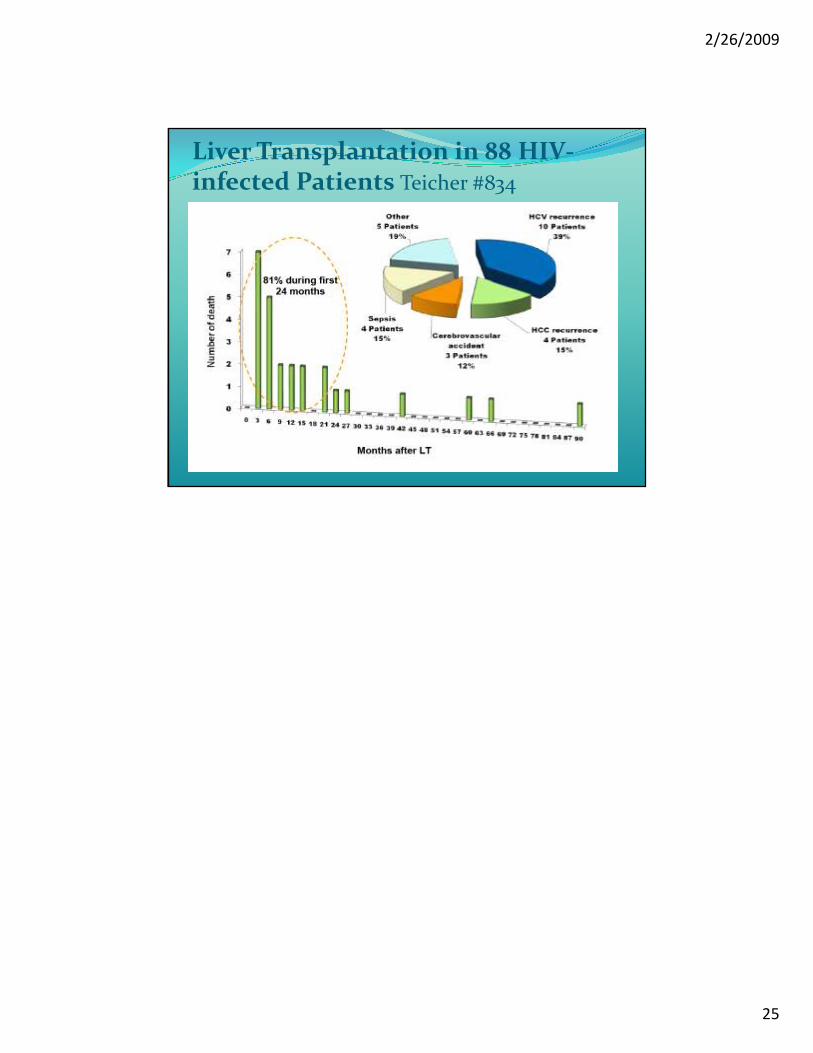
Liver Transplantation in 88 HIV-infected Patients Teicher #834