
FINAL REPORT Speech & Language Therapy Service Model ... · FINAL REPORT Speech & Language Therapy...
154
FINAL REPORT Speech & Language Therapy Service Model & Effectiveness Review: Stages II and III (5-18 year olds) Prepared for The Department of Education and Children’s Services and the Department of Health, South Australia Prepared by Deborah G H James, Leah Jeffries & Anthea Worley Centre for Allied Health Evidence University of South Australia North Terrace Adelaide SA 5000 Email: [email protected] Telephone: 08 8302 2769 Submission date of final report 12 th December 2008 This report should be referenced as follows: James, D.G.H., Jeffries, L. & Worley. A. (2008) Speech & Language Therapy Service Model & Effectiveness Review: Stages II and III (5-18 year olds).Centre for Allied Health Evidence, University of South Australia
Transcript of FINAL REPORT Speech & Language Therapy Service Model ... · FINAL REPORT Speech & Language Therapy...
FINAL REPORT
Speech & Language Therapy Service Model &
Effectiveness Review:
Stages II and III (5-18 year olds)
Prepared for
The Department of Education and Children’s Services and the
Department of Health, South Australia
Prepared by
Deborah G H James, Leah Jeffries & Anthea Worley
Centre for Allied Health Evidence
University of South Australia
North Terrace
Adelaide SA 5000
Email: [email protected]
Telephone: 08 8302 2769
Submission date of final report
12th December 2008
This report should be referenced as follows:
James, D.G.H., Jeffries, L. & Worley. A. (2008) Speech & Language Therapy Service Model &
Effectiveness Review: Stages II and III (5-18 year olds).Centre for Allied Health Evidence,
University of South Australia
2
TABLE OF CONTENTS
Table of Contents ................................................................................................................................... 2 Glossary of Outcome Measures ............................................................................................................. 3 Chapter 1: Introduction ...................................................................................................................... 4
Background ........................................................................................................................................ 4 Primary speech and language impairment in school children ....................................................... 4 Incidence and prevalence of primary speech and language difficulties ........................................ 5
Speech Pathology Services ................................................................................................................ 6 Research Questions ............................................................................................................................ 7
Chapter 2: Method ............................................................................................................................... 8 PECOT (Population, Exposure, Comparator, Outcomes, Time) ....................................................... 8
Search strategy ................................................................................................................................... 8 Search terms Stage II & III combined ........................................................................................... 8 Search limits ................................................................................................................................... 9 Search validation ............................................................................................................................ 9
Data extraction ................................................................................................................................... 9 Chapter 3: Results .............................................................................................................................. 10
Description of the studies ................................................................................................................. 10 Country of origin .......................................................................................................................... 10 Level of Evidence and quality of research ................................................................................... 10 The nature of the service delivery ................................................................................................ 11 Sample sizes ................................................................................................................................. 11 The age of participants ................................................................................................................. 11
The nature of the impairments ..................................................................................................... 12 Types of outcome measures ......................................................................................................... 12
Key Results ...................................................................................................................................... 12 Service delivery ........................................................................................................................... 13 Efficacy of the interventions ........................................................................................................ 17
Chapter 4: Discussion ........................................................................................................................ 22 Efficacy of Interventions .................................................................................................................. 22
Effectiveness and effects .............................................................................................................. 22 Efficiency of the interventions ..................................................................................................... 22
Service Delivery Constructs ............................................................................................................ 24 Efficacy of Direct models of service delivery ............................................................................. 24 Efficacy of Indirect models of service delivery ........................................................................... 24
Efficacy Of The Collaborative Models Of Service Delivery ....................................................... 25 Limitations of the review ................................................................................................................. 26
Chapter 5: Core learnings ................................................................................................................. 27 Efficacy of Interventions .................................................................................................................. 27
Effectiveness ................................................................................................................................ 27
Efficiency ..................................................................................................................................... 27 Models of Service delivery .............................................................................................................. 28
Effectiveness ................................................................................................................................ 28
Efficiency ..................................................................................................................................... 28 References ........................................................................................................................................... 29 Acknowledgements ............................................................................................................................ 35
Appendices .......................................................................................................................................... 36 Appendix 1. Summary of all the studies against extraction criteria. .............................................. 36 Appendix 2 Complete summary of each of article .......................................................................... 51
Appendix 3 Summary of the Articles in the review by Cirrin & Gillam (2008) ........................... 137
3
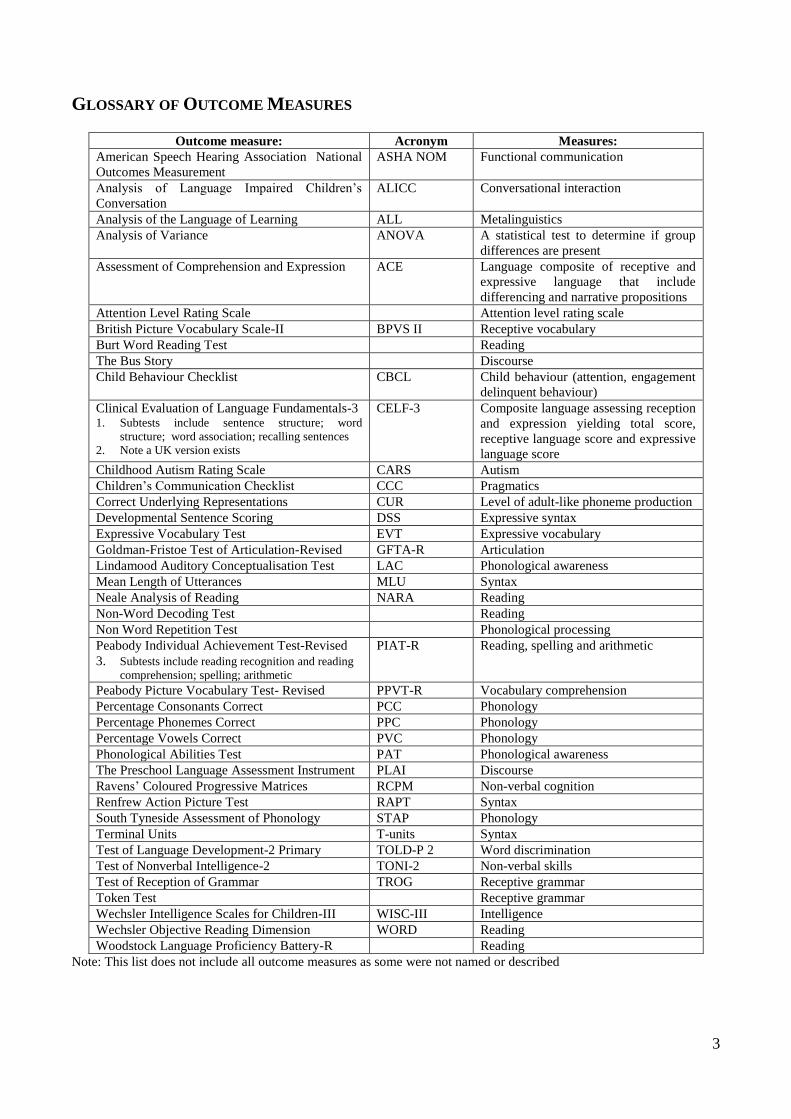
GLOSSARY OF OUTCOME MEASURES
Outcome measure: Acronym Measures:
American Speech Hearing Association National
Outcomes Measurement
ASHA NOM Functional communication
Analysis of Language Impaired Children‟s
Conversation
ALICC Conversational interaction
Analysis of the Language of Learning ALL Metalinguistics
Analysis of Variance ANOVA A statistical test to determine if group
differences are present
Assessment of Comprehension and Expression ACE Language composite of receptive and
expressive language that include
differencing and narrative propositions
Attention Level Rating Scale Attention level rating scale
British Picture Vocabulary Scale-II BPVS II Receptive vocabulary
Burt Word Reading Test Reading
The Bus Story Discourse
Child Behaviour Checklist CBCL Child behaviour (attention, engagement
delinquent behaviour)
Clinical Evaluation of Language Fundamentals-3 1. Subtests include sentence structure; word
structure; word association; recalling sentences
2. Note a UK version exists
CELF-3 Composite language assessing reception
and expression yielding total score,
receptive language score and expressive
language score
Childhood Autism Rating Scale CARS Autism
Children‟s Communication Checklist CCC Pragmatics
Correct Underlying Representations CUR Level of adult-like phoneme production
Developmental Sentence Scoring DSS Expressive syntax
Expressive Vocabulary Test EVT Expressive vocabulary
Goldman-Fristoe Test of Articulation-Revised GFTA-R Articulation
Lindamood Auditory Conceptualisation Test LAC Phonological awareness
Mean Length of Utterances MLU Syntax
Neale Analysis of Reading NARA Reading
Non-Word Decoding Test Reading
Non Word Repetition Test Phonological processing
Peabody Individual Achievement Test-Revised
3. Subtests include reading recognition and reading
comprehension; spelling; arithmetic
PIAT-R Reading, spelling and arithmetic
Peabody Picture Vocabulary Test- Revised PPVT-R Vocabulary comprehension
Percentage Consonants Correct PCC Phonology
Percentage Phonemes Correct PPC Phonology
Percentage Vowels Correct PVC Phonology
Phonological Abilities Test PAT Phonological awareness
The Preschool Language Assessment Instrument PLAI Discourse
Ravens‟ Coloured Progressive Matrices RCPM Non-verbal cognition
Renfrew Action Picture Test RAPT Syntax
South Tyneside Assessment of Phonology STAP Phonology
Terminal Units T-units Syntax
Test of Language Development-2 Primary TOLD-P 2 Word discrimination
Test of Nonverbal Intelligence-2 TONI-2 Non-verbal skills
Test of Reception of Grammar TROG Receptive grammar
Token Test Receptive grammar
Wechsler Intelligence Scales for Children-III WISC-III Intelligence
Wechsler Objective Reading Dimension WORD Reading
Woodstock Language Proficiency Battery-R Reading
Note: This list does not include all outcome measures as some were not named or described
4
CHAPTER 1: INTRODUCTION
BACKGROUND
The State Government of South Australia recognises the importance of optimal speech and language
outcomes, as measured by literacy and numeracy rates, for all children in South Australia and this
has been demonstrated in “South Australia’s Strategic Plan 2007”. In 2006, it instituted a review of
the state paediatric speech pathology services. The South Australian State-wide Interagency Speech
Pathology Group, representing the departments of Health, Education and Children‟s Services and
Disability has the delegated responsibility for conducting this project. As a part of this process, they
commissioned the Centre of Allied Health Evidence (CAHE) within the University of South
Australia, to conduct a systematic review of the literature to examine the evidence for speech and
language therapy services for children aged 0-18 years with speech, language and communication
needs and the service delivery constructs underpinning that intervention. They divided the review
into four stages. Stage I addressed children with primary speech and language impairment from birth
to less than five years and this review was concluded in December 2007. Stages II and III are the
focus of this report, addressing children with primary speech and language impairment, aged five to
eight years and nine to eighteen years. The final stage will address children, aged 0-18 years with
speech, language and communication needs secondary to disabilities such as cerebral palsy, autism,
intellectual disability, hearing impairment, behavioural or emotional difficulties or neurological
impairment.
PRIMARY SPEECH AND LANGUAGE IMPAIRMENT IN SCHOOL CHILDREN
For the approximate 10% of children who begin school with a primary speech and/or language
impairment (PSLI), their difficulties begin manifesting in reading and writing in addition to speaking
and listening difficulties. The cause of PSLI is unknown and they are not the consequence of hearing
loss, intellectual disability, frank neurological problems or syndromes (Law et al. 2003). Rather,
these problems exist despite normal functioning in these other areas.
Speech impairment affects the phonological system, that is the production (pronunciation) and
processing of sounds. School-age speech production or phonological output difficulties may be overt
and obvious such as a young school-child who says I tan tee a do ditting in na buet meaning I can
see a dog sitting in the bucket. However, school-age speech production difficulties are typically
covert and insidious, possibly only manifesting as literacy problems (Gillon & Dodd 1993). The
typical pathway of speech impairment that persists into the school years is to manifest overtly first as
pronunciation difficulties in the years before school and in the early school years, then manifest
covertly as literacy problems without obvious pronunciation difficulties and then as academic, social
and vocational difficulties (Felsenfeld, Broen & McGuel 1992, 1994; Gillon & Dodd 1993;
Snowling, Adams, Bishop & Stothard 2001; Stothard, Snowling, Bishop, Chipchase & Kaplan
1998).
Phonological processing is different to and broader than phonological awareness (Gillon 2004).
Phonological processing difficulties mean that children may have problems with making sense of the
acoustic information in speech for both spoken and written language and manifests in a variety of
ways. Phonological awareness problems are one such way and may mean difficulty segmenting
words into sounds (sounding out words), a skill critical to literacy success (Gillon 2004). Other
phonological processing problems may be short-term memory problems or retrieving information
from long-term memory, manifesting in word finding problems. Difficulties with phonological
processing are thought to be causal component of primary speech and/or language impairment,
including specific language impairment and dyslexia (Gillon 2004; Stackhouse & Wells, 1997;
5
2001). What is important to note is that children can have poor phonological processing skills with
apparently normal speech.
Language impairment manifests in a variety of ways. It may affect one or many domains of
language, affecting the reception (comprehension) or expression of words (semantics/vocabulary),
sentences (syntax/grammar), discourse and pragmatics in oral and/or written form. Language
difficulties may be overt and obvious such as a young school-age child with syntax problems who
says “Me go toilet” for “Could I go to the toilet please?” More typically, however, school-age
language difficulties are covert, buried within discourse and pragmatics. Discourse problems result in
poor linkages between sentences resulting in conversations and written work (essays and
composition) that are disorganised and hard for listeners and readers to follow. Pragmatic problems
often mean that the children cannot match the language to the social context and this in turn, may
make them appear uncooperative, insolent or inattentive. The typical pathway of language
impairment that persists into the school years is to overtly manifest as grammar problems in the years
before school and in the early school years and then the pathway is similar to that for speech
difficulties, as language impairment manifests as literacy, academic, social and vocational difficulties
(Gillon & Dodd 1993; Nation, Clarke, Marshall & Durand 2004; Stothard et al. 1998). For both
groups the social difficulties may include the previously stated manifestations of uncooperativeness,
insolence and inattentiveness as well as social isolation and withdrawal, depression and offending
(Bercow 2008; Bryan 2004; Damico & Oller 1980; Snow & Powell 2004).
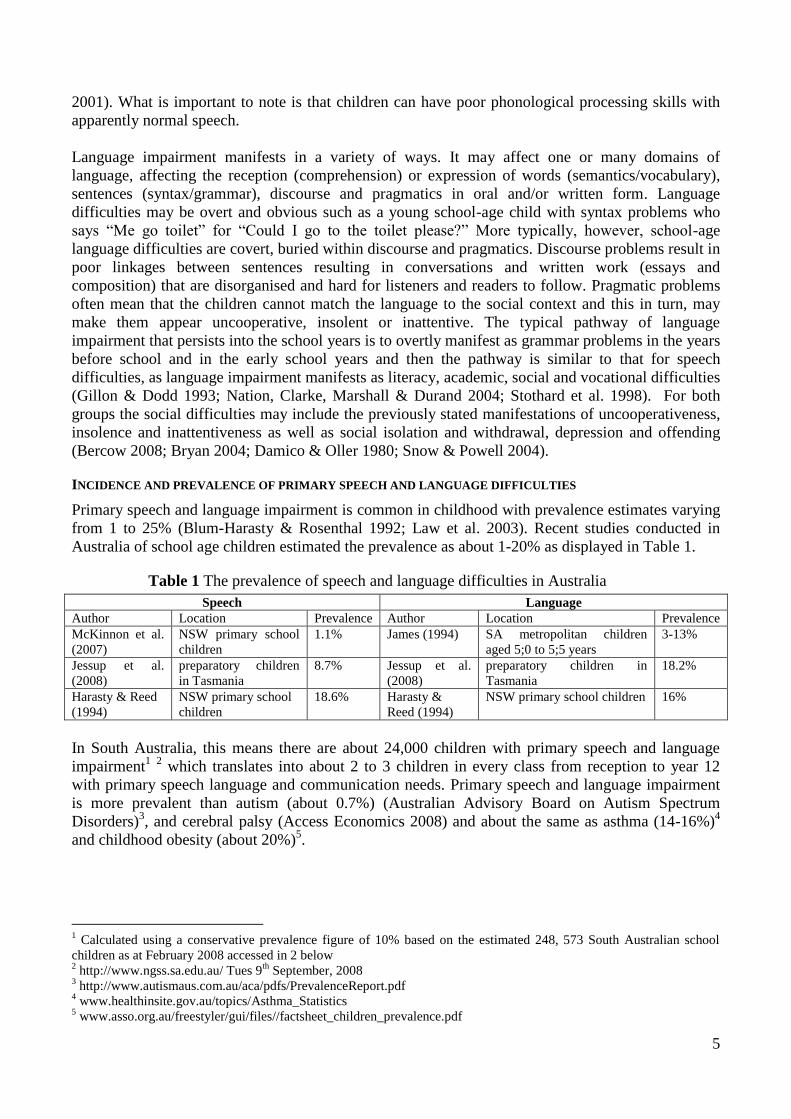
INCIDENCE AND PREVALENCE OF PRIMARY SPEECH AND LANGUAGE DIFFICULTIES
Primary speech and language impairment is common in childhood with prevalence estimates varying
from 1 to 25% (Blum-Harasty & Rosenthal 1992; Law et al. 2003). Recent studies conducted in
Australia of school age children estimated the prevalence as about 1-20% as displayed in Table 1.
Table 1 The prevalence of speech and language difficulties in Australia
Speech Language
Author Location Prevalence Author Location Prevalence
McKinnon et al.
(2007)
NSW primary school
children
1.1% James (1994) SA metropolitan children
aged 5;0 to 5;5 years
3-13%
Jessup et al.
(2008)
preparatory children
in Tasmania
8.7% Jessup et al.
(2008)
preparatory children in
Tasmania
18.2%
Harasty & Reed
(1994)
NSW primary school
children
18.6% Harasty &
Reed (1994)
NSW primary school children 16%
In South Australia, this means there are about 24,000 children with primary speech and language
impairment1
2 which translates into about 2 to 3 children in every class from reception to year 12
with primary speech language and communication needs. Primary speech and language impairment
is more prevalent than autism (about 0.7%) (Australian Advisory Board on Autism Spectrum
Disorders)3, and cerebral palsy (Access Economics 2008) and about the same as asthma (14-16%)
4
and childhood obesity (about 20%)5.
1 Calculated using a conservative prevalence figure of 10% based on the estimated 248, 573 South Australian school
children as at February 2008 accessed in 2 below 2 http://www.ngss.sa.edu.au/ Tues 9
th September, 2008
3 http://www.autismaus.com.au/aca/pdfs/PrevalenceReport.pdf
4 www.healthinsite.gov.au/topics/Asthma_Statistics
5 www.asso.org.au/freestyler/gui/files//factsheet_children_prevalence.pdf
6
SPEECH PATHOLOGY SERVICES
An array of models of service delivery and interventions exist for school-age children with primary
speech and language impairment. Models of service delivery are the ways agencies deliver their
speech pathology services from an organisational perspective and typically encompass the
organisational values, strategies and goals as well as inputs and intended outcomes (Greenhalgh,
Harvey & Walshe 2005). Models of service delivery include clinical (direct), consultancy (indirect),
collaborative and language based classroom models (Paul 2007). The clinical model involves a
speech pathologist working directly with a child or a group of children having determined the goals
and strategies of the management plan based on an assessment of the children. Within the
consultancy model, the speech pathologist works indirectly with children through another agent such
as teachers, parents and teacher assistants but often is still responsible for determining the
management plan. In the language based classroom model, the speech pathologist is also the teacher,
and again develops the management plan. The collaborative model may combine aspects from all
three models, but is differentiated from these approaches in that the development of the management
plan is usually a collaborative effort with all stakeholders, rather than it being only the speech
pathologist‟s responsibility. However, in practice, the divisions between these delivery models are
not this distinct, that is, different permutations of these models occur.
By contrast, interventions occur within models of service delivery and involve the techniques to
strengthen linguistic skills. An array of interventions techniques exist for all speech and language
domains (Paul 2007).
Speech pathology models of service delivery and interventions are ever evolving. Some of the
drivers of change are:
the gathering momentum within the profession about the application of the World Health
Organization‟s International Classification of Functioning, Disability and Health (ICF) (WHO
2001) to care (e.g. Issues 1 & 2 of the International Journal of Speech-Language Pathology6
2008 were devoted to this topic; Campbell & Skarakis-Doyle 2007). The ICF describes human
functioning at three levels. One level is body function and structures referring to physiological
systems and body parts. So in the context of this review that encompasses speech and language.
The second level is activity and refers to the ability to execute tasks and the third level,
participation, is the ability to participate, to be involved in life activities. So these two levels
encompass the ability to use speech and language to discharge daily activities of communicating.
the gathering momentum to add public health frameworks to models of service delivery (Bercow
2008; Snow 2008a,b,c)
the increasing press for evidence based practice and (Bernstein Ratner 2006; Dodd 2007; Fey
2006; Gillam & Gillam 2006; Kent 2006)
the extensive and growing database indicating children‟s oral language skills are both risk and
protective factors for later literacy, academic, social and vocational success (e.g. Bercow,
Felsenfeld et al. 1992, 1994; Law et al. 2003; Lewis & Freebairn 1992; Snowling et al. 2001;
Stothard et al. 1998).
Given the increasing recognition of the benefits of speech pathology services for children with
primary speech and/or language impairment, it is important to evaluate service delivery models and
interventions for school children (i.e. 5-18 years) in order to ensure access to optimal services in a
timely manner. It is also anticipated that both innovative and varying means of identification and
6 Speech Pathology Australia, the Australian professional body of speech pathologists, publishes this journal. All
members of this association receive this journal.

7
intervention in this age group need consideration because of the possibility that these children may
be undetected.
Although a previous systematic review (Law et al 2003) concluded that speech and language therapy
interventions for children with expressive phonological and expressive vocabulary difficulties had a
positive effect, the review only considered randomised controlled trials and not other experimental
studies. The majority of the studies located for this review were about children aged five years and
under so it was not clear from this review what the intervention outcomes were for school children.
Also, this review did not examine the constructs underpinning service delivery models. Since it is
widely recognised that in addition to knowing “what” works best, it is also important to know “how”
to go about performing what is considered to be best practice; this review aims to investigate the
efficacy of speech pathology services for school children and some of the constructs underpinning
service delivery models.
RESEARCH QUESTIONS
Stage II: What is the evidence underpinning speech and language therapy services for children aged
5-8 years with primary speech and/or language impairment/delay/disorder for improved speech and
communication outcomes?
Stage III: What is the evidence underpinning speech and language therapy services for children aged
9-18 years with primary speech and/or language impairment/delay/disorder for improved speech and
communication outcomes?
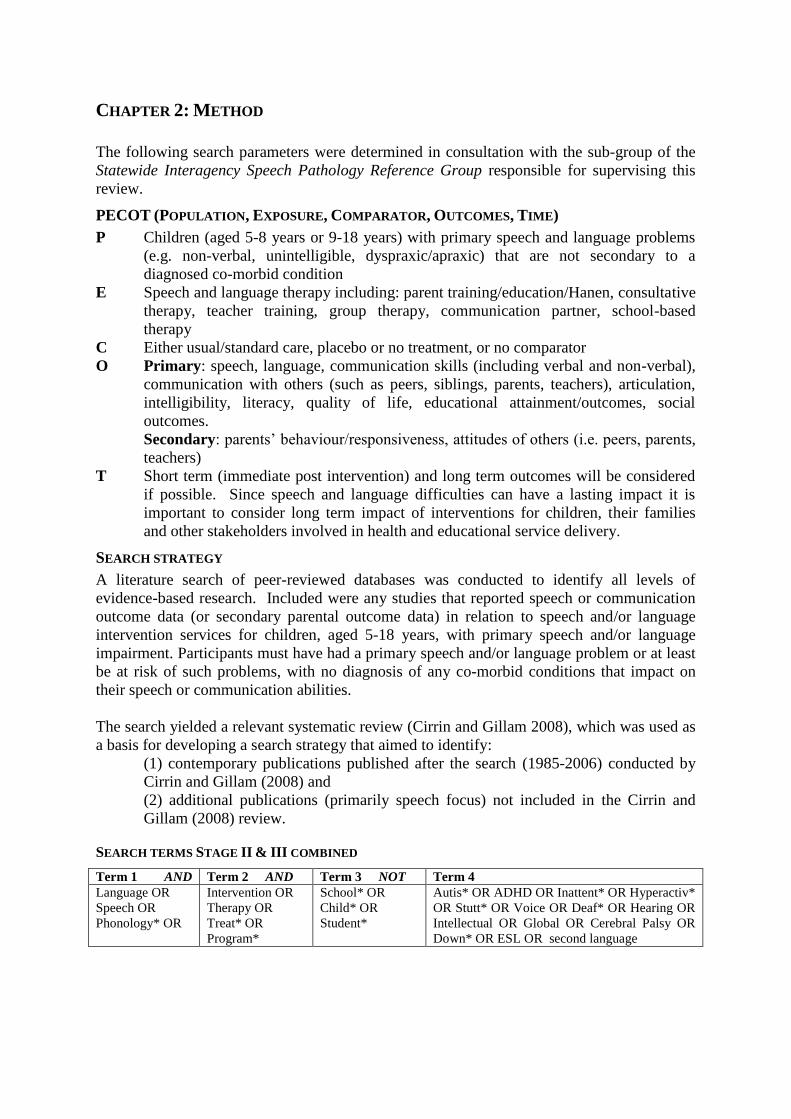
CHAPTER 2: METHOD
The following search parameters were determined in consultation with the sub-group of the
Statewide Interagency Speech Pathology Reference Group responsible for supervising this
review.
PECOT (POPULATION, EXPOSURE, COMPARATOR, OUTCOMES, TIME)
P Children (aged 5-8 years or 9-18 years) with primary speech and language problems
(e.g. non-verbal, unintelligible, dyspraxic/apraxic) that are not secondary to a
diagnosed co-morbid condition
E Speech and language therapy including: parent training/education/Hanen, consultative
therapy, teacher training, group therapy, communication partner, school-based
therapy
C Either usual/standard care, placebo or no treatment, or no comparator
O Primary: speech, language, communication skills (including verbal and non-verbal),
communication with others (such as peers, siblings, parents, teachers), articulation,
intelligibility, literacy, quality of life, educational attainment/outcomes, social
outcomes.
Secondary: parents‟ behaviour/responsiveness, attitudes of others (i.e. peers, parents,
teachers)
T Short term (immediate post intervention) and long term outcomes will be considered
if possible. Since speech and language difficulties can have a lasting impact it is
important to consider long term impact of interventions for children, their families
and other stakeholders involved in health and educational service delivery.
SEARCH STRATEGY
A literature search of peer-reviewed databases was conducted to identify all levels of
evidence-based research. Included were any studies that reported speech or communication
outcome data (or secondary parental outcome data) in relation to speech and/or language
intervention services for children, aged 5-18 years, with primary speech and/or language
impairment. Participants must have had a primary speech and/or language problem or at least
be at risk of such problems, with no diagnosis of any co-morbid conditions that impact on
their speech or communication abilities.
The search yielded a relevant systematic review (Cirrin and Gillam 2008), which was used as
a basis for developing a search strategy that aimed to identify:
(1) contemporary publications published after the search (1985-2006) conducted by
Cirrin and Gillam (2008) and
(2) additional publications (primarily speech focus) not included in the Cirrin and
Gillam (2008) review.
SEARCH TERMS STAGE II & III COMBINED
Term 1 AND Term 2 AND Term 3 NOT Term 4
Language OR
Speech OR
Phonology* OR
Intervention OR
Therapy OR
Treat* OR
Program*
School* OR
Child* OR
Student*
Autis* OR ADHD OR Inattent* OR Hyperactiv*
OR Stutt* OR Voice OR Deaf* OR Hearing OR
Intellectual OR Global OR Cerebral Palsy OR
Down* OR ESL OR second language
9
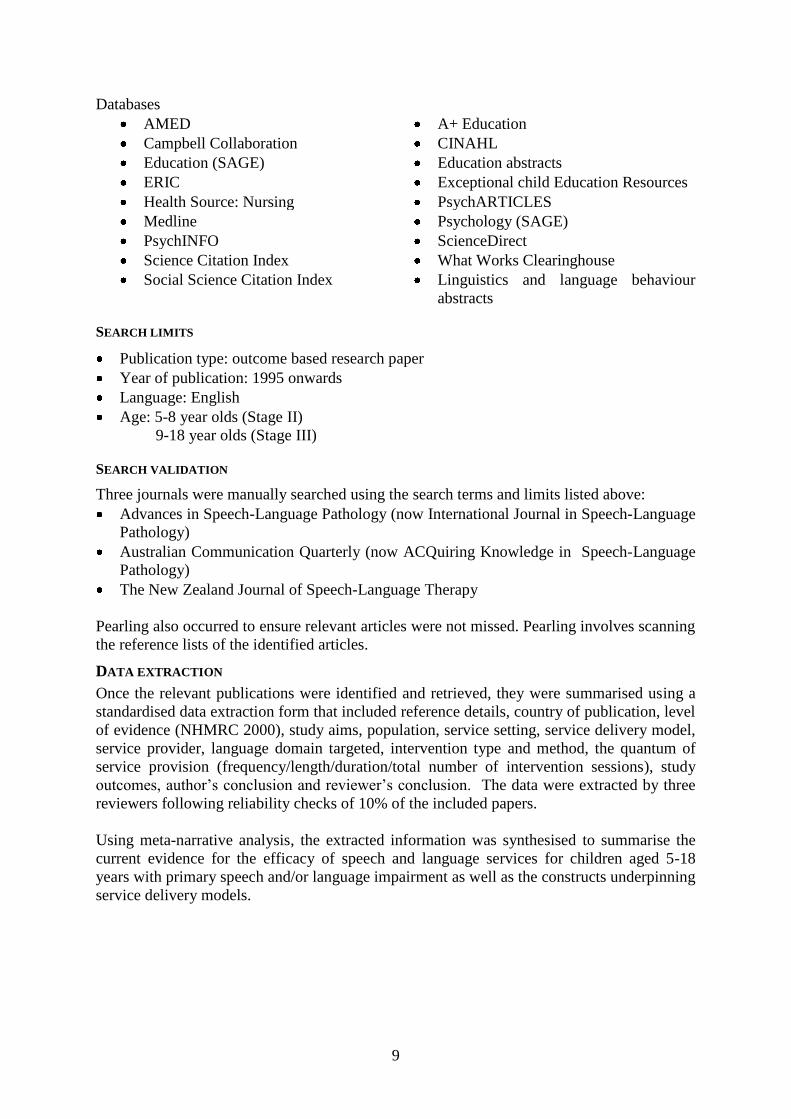
Databases
AMED A+ Education
Campbell Collaboration CINAHL
Education (SAGE) Education abstracts
ERIC Exceptional child Education Resources
Health Source: Nursing PsychARTICLES
Medline Psychology (SAGE)
PsychINFO ScienceDirect
Science Citation Index What Works Clearinghouse
Social Science Citation Index Linguistics and language behaviour
abstracts
SEARCH LIMITS
Publication type: outcome based research paper
Year of publication: 1995 onwards
Language: English
Age: 5-8 year olds (Stage II)
9-18 year olds (Stage III)
SEARCH VALIDATION
Three journals were manually searched using the search terms and limits listed above:
Advances in Speech-Language Pathology (now International Journal in Speech-Language
Pathology)
Australian Communication Quarterly (now ACQuiring Knowledge in Speech-Language
Pathology)
The New Zealand Journal of Speech-Language Therapy
Pearling also occurred to ensure relevant articles were not missed. Pearling involves scanning
the reference lists of the identified articles.
DATA EXTRACTION
Once the relevant publications were identified and retrieved, they were summarised using a
standardised data extraction form that included reference details, country of publication, level
of evidence (NHMRC 2000), study aims, population, service setting, service delivery model,
service provider, language domain targeted, intervention type and method, the quantum of
service provision (frequency/length/duration/total number of intervention sessions), study
outcomes, author‟s conclusion and reviewer‟s conclusion. The data were extracted by three
reviewers following reliability checks of 10% of the included papers.
Using meta-narrative analysis, the extracted information was synthesised to summarise the
current evidence for the efficacy of speech and language services for children aged 5-18
years with primary speech and/or language impairment as well as the constructs underpinning
service delivery models.
10
CHAPTER 3: RESULTS
The search located 97 potential articles; 82 from the peer-reviewed databases, 10 from the
manual search and five from pearling. Stage I articles were included if the number of children
five years and over could be ascertained from all participants in the study and there was more
than one participant. Two articles from Stage 1 met these requirements and were included.
The sub-group of the Statewide Interagency Speech Pathology Reference Group and the first
two authors scrutinised the 82 articles from the peer-reviewed databases and rejected those
that Cirrin and Gillam (2008) reviewed and those they judged outside the search parameters
based on the information in the title and abstract. The full texts of the remaining 45 articles
were retrieved along with nine of the ten articles located manually and all five from pearling.
Eleven more articles were rejected leaving a final pool of 50 articles, including the two from
Stage I.
DESCRIPTION OF THE STUDIES
The 50 papers comprised 48 studies of primary research and two systematic reviews. The
search for this review, coupled with the searches from the two systematic reviews means that
the literature from 1872 to 2008 was searched. This report captures the findings of 105
studies because the systematic reviews included 57 articles.
COUNTRY OF ORIGIN
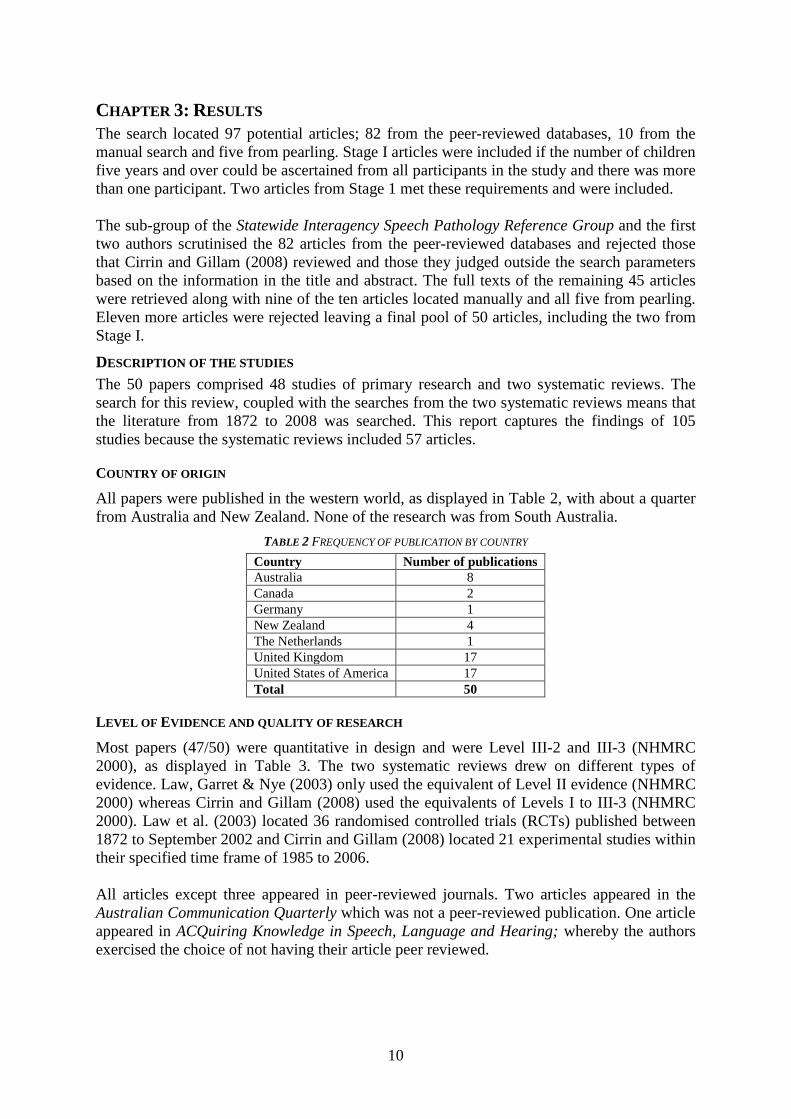
All papers were published in the western world, as displayed in Table 2, with about a quarter
from Australia and New Zealand. None of the research was from South Australia.
TABLE 2 FREQUENCY OF PUBLICATION BY COUNTRY
Country Number of publications
Australia 8
Canada 2
Germany 1
New Zealand 4
The Netherlands 1
United Kingdom 17
United States of America 17
Total 50
LEVEL OF EVIDENCE AND QUALITY OF RESEARCH
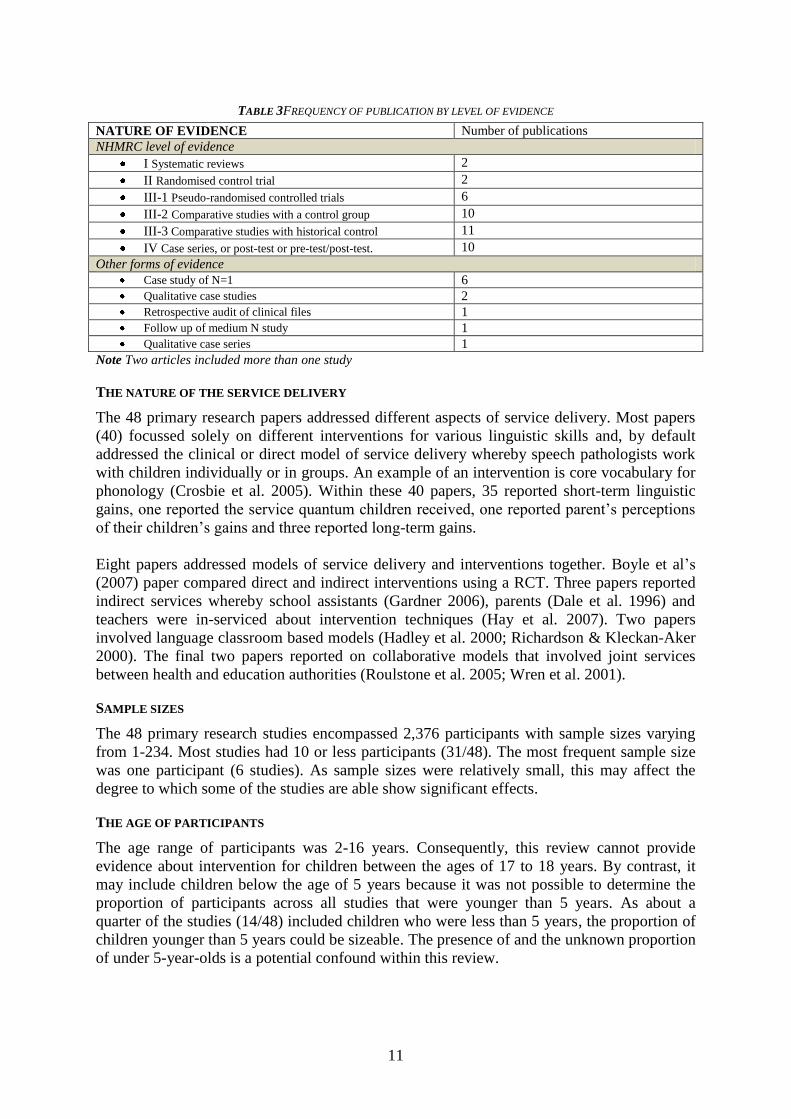
Most papers (47/50) were quantitative in design and were Level III-2 and III-3 (NHMRC
2000), as displayed in Table 3. The two systematic reviews drew on different types of
evidence. Law, Garret & Nye (2003) only used the equivalent of Level II evidence (NHMRC
2000) whereas Cirrin and Gillam (2008) used the equivalents of Levels I to III-3 (NHMRC
2000). Law et al. (2003) located 36 randomised controlled trials (RCTs) published between
1872 to September 2002 and Cirrin and Gillam (2008) located 21 experimental studies within
their specified time frame of 1985 to 2006.
All articles except three appeared in peer-reviewed journals. Two articles appeared in the
Australian Communication Quarterly which was not a peer-reviewed publication. One article
appeared in ACQuiring Knowledge in Speech, Language and Hearing; whereby the authors
exercised the choice of not having their article peer reviewed.
11
TABLE 3FREQUENCY OF PUBLICATION BY LEVEL OF EVIDENCE
NATURE OF EVIDENCE Number of publications
NHMRC level of evidence
I Systematic reviews 2
II Randomised control trial 2
III-1 Pseudo-randomised controlled trials 6
III-2 Comparative studies with a control group 10
III-3 Comparative studies with historical control 11
IV Case series, or post-test or pre-test/post-test. 10
Other forms of evidence
Case study of N=1 6
Qualitative case studies 2
Retrospective audit of clinical files 1
Follow up of medium N study 1
Qualitative case series 1
Note Two articles included more than one study
THE NATURE OF THE SERVICE DELIVERY
The 48 primary research papers addressed different aspects of service delivery. Most papers
(40) focussed solely on different interventions for various linguistic skills and, by default
addressed the clinical or direct model of service delivery whereby speech pathologists work
with children individually or in groups. An example of an intervention is core vocabulary for
phonology (Crosbie et al. 2005). Within these 40 papers, 35 reported short-term linguistic
gains, one reported the service quantum children received, one reported parent‟s perceptions
of their children‟s gains and three reported long-term gains.
Eight papers addressed models of service delivery and interventions together. Boyle et al‟s
(2007) paper compared direct and indirect interventions using a RCT. Three papers reported
indirect services whereby school assistants (Gardner 2006), parents (Dale et al. 1996) and
teachers were in-serviced about intervention techniques (Hay et al. 2007). Two papers
involved language classroom based models (Hadley et al. 2000; Richardson & Kleckan-Aker
2000). The final two papers reported on collaborative models that involved joint services
between health and education authorities (Roulstone et al. 2005; Wren et al. 2001).
SAMPLE SIZES
The 48 primary research studies encompassed 2,376 participants with sample sizes varying
from 1-234. Most studies had 10 or less participants (31/48). The most frequent sample size
was one participant (6 studies). As sample sizes were relatively small, this may affect the
degree to which some of the studies are able show significant effects.
THE AGE OF PARTICIPANTS
The age range of participants was 2-16 years. Consequently, this review cannot provide
evidence about intervention for children between the ages of 17 to 18 years. By contrast, it
may include children below the age of 5 years because it was not possible to determine the
proportion of participants across all studies that were younger than 5 years. As about a
quarter of the studies (14/48) included children who were less than 5 years, the proportion of
children younger than 5 years could be sizeable. The presence of and the unknown proportion
of under 5-year-olds is a potential confound within this review.
12
This same pattern was apparent in the 25 studies that Law et al. (2003) reviewed as 13 studies
addressed children younger than 5 years and six studies included children with a lower age
range of less than 5 years and an upper age range of 5 or 6 years. Only the remaining studies
exclusively included school age children. While Cirrin and Gillam reviewed (2008) studies
about schoolchildren, 19 of the 21 studies they reviewed were about children younger than 10
years.
Thus, the greatest number of participants were at the lower end of the range set for this
review. This bias towards children younger than the age of 10 years is another potential
confound within this review.
THE NATURE OF THE IMPAIRMENTS
All 48 primary research studies contained children with primary speech and language
impairments. Some studies included children with impairments outside this range (e.g.
Hadley et al. 2000) and such studies were only included if the participants with primary
speech and language impairments were isolated from the other participants. The two
systematic reviews only included participants with primary speech and language
impairments. Law et al. (2003) addressed children with primary speech and language
impairments whereas Cirrin and Gillam (2008) only included school-aged participants with
primary language difficulties.
TYPES OF OUTCOME MEASURES
Studies reporting the outcomes of interventions measured children‟s linguistic outcomes with
formal, standardised tests, criterion referenced tests, developmental scores and behavioural
observations. The measuring tools provided information about aspects of expressive,
metalinguistic7 and receptive language functioning in pragmatics, discourse, semantics,
syntax, and phonology, either separately or as composite scores. Generally, each study used
different outcome measures, limiting comparisons across studies. Interviews and surveys of
parents, teachers and assistants were used to measure children‟s linguistic functioning
indirectly. Secondary measures such as self esteem were taken.
Studies reporting the outcomes of service delivery models reported outcomes about the
identified stakeholders and organisational features. Stakeholders included children, parents,
teachers, assistants, speech pathologists and authorities (e.g. health and education).
Organisational features included referral processes, redeployment of staff time, meetings and
classroom practices. Measuring tools included interviews, questionnaires and surveys.
KEY RESULTS
The key results about service delivery are presented first, with the results about intervention
efficacy following. The results are summarised in Appendix 1. Appendix 2 contains a full
summary of each of the articles, while Appendix 3 is a summary of the articles that Cirrin
and Gillam reviewed. The articles Law et al. (2003) reviewed are freely available on the
internet. Chapter 4 discusses the efficacy of service delivery models.
7 Metalinguistics is the language of language (i.e. linguistics). Metalinguistic ability is the skills to reflect on
language and describe it. It encompasses skills such as phonological awareness (sounding out words, playing
with rhyme), defining words, parsing sentences into nouns and verbs etc and editing. Metalinguistic ability is a
critical skill for literacy acquisition (Paul 2007)
13
SERVICE DELIVERY
The following points about service delivery relate to the 48 primary research articles. The
two systematic reviews are not included.
PROVIDER/INTERVENTION AGENTS
Speech pathologists8 were the agent in 41 of the papers. This was clear in 33 papers and
assumed in another eight as the authors provided the intervention without detailing their
qualifications. Other agents included teachers, nurses and speech pathology assistants either
alone or in combination with a speech pathologist. In six studies, whilst the speech
pathologist was the provider, the service they provided was negotiated as a part of a team
within the school context. One study (Boyle et al. 2007) compared the service provided by
speech pathologists and speech pathology assistants trained by speech pathologists. There
were no studies of speech pathologists providing services in collaboration with other allied
health professionals such as physiotherapists or occupational therapists.
SERVICE SETTING
Schools were the main service setting (26/48) followed by clinics (community/medical/not
specified) (16) and then university clinics (6). In one study, the families had the choice of
intervention occurring at home, school or a clinic (Swanson et al. 2005). A school summer
camp was the setting in another study (Pokorni et al. 2004).
THERAPY GOALS
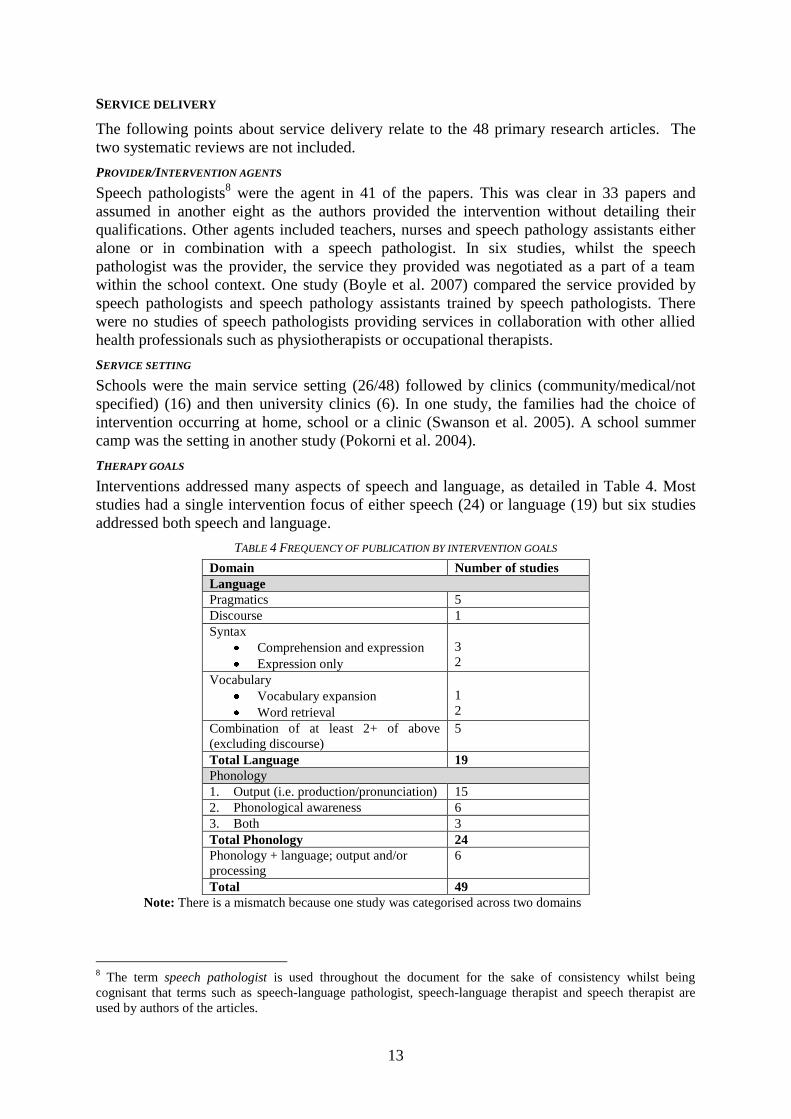
Interventions addressed many aspects of speech and language, as detailed in Table 4. Most
studies had a single intervention focus of either speech (24) or language (19) but six studies
addressed both speech and language.
TABLE 4 FREQUENCY OF PUBLICATION BY INTERVENTION GOALS
Domain Number of studies
Language
Pragmatics 5
Discourse 1
Syntax
Comprehension and expression
Expression only
3
2
Vocabulary
Vocabulary expansion
Word retrieval
1
2
Combination of at least 2+ of above
(excluding discourse)
5
Total Language 19
Phonology
1. Output (i.e. production/pronunciation) 15
2. Phonological awareness 6
3. Both 3
Total Phonology 24
Phonology + language; output and/or
processing
6
Total 49
Note: There is a mismatch because one study was categorised across two domains
8 The term speech pathologist is used throughout the document for the sake of consistency whilst being
cognisant that terms such as speech-language pathologist, speech-language therapist and speech therapist are
used by authors of the articles.
14
Language goals were relatively even across receptive and expressive pragmatics, syntax and
semantics but not discourse. Pragmatic goals included adapting language to the context.
Syntax goals included morphology, passives, relative clauses and complex sentences.
Semantic goals included improving word retrieval.
Phonology output goals occurred more frequently than phonological processing goals. Output
goals included error patterns (phonological processes), or individual sounds such as fricatives
(e.g. /v/). Phonological processing goals included phonological awareness (e.g. rhyming,
phoneme deletion) and enhancing processing speed.
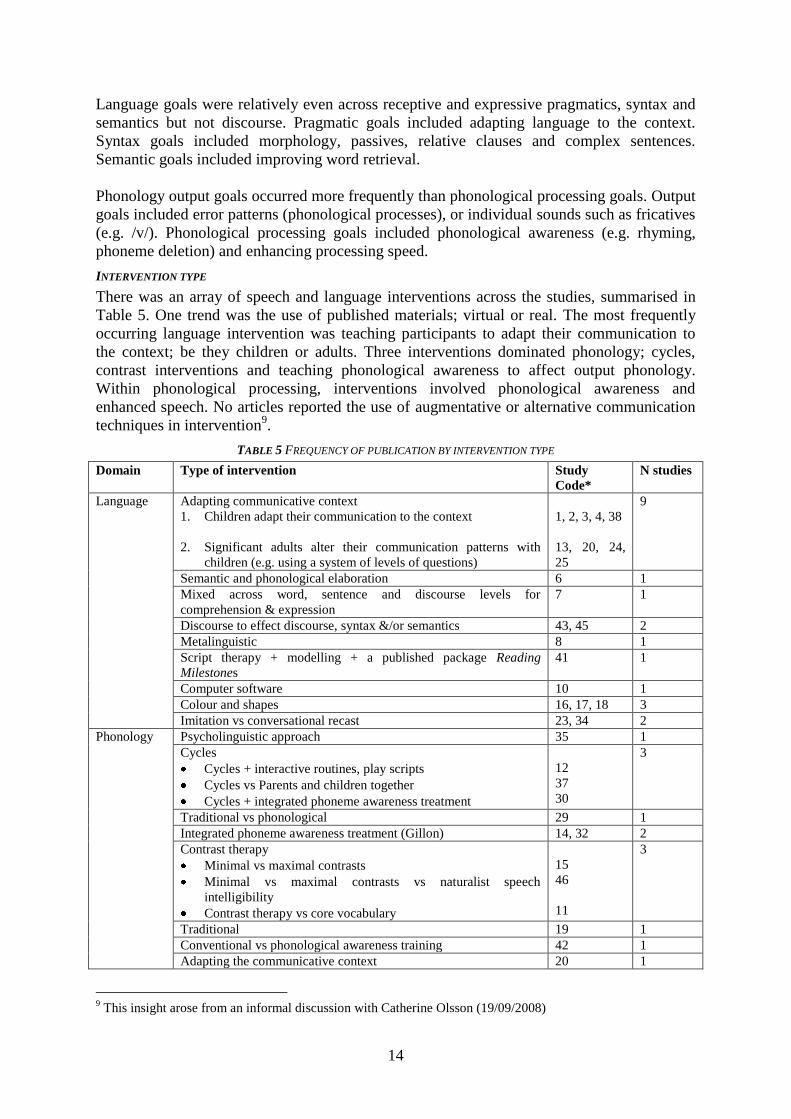
INTERVENTION TYPE
There was an array of speech and language interventions across the studies, summarised in
Table 5. One trend was the use of published materials; virtual or real. The most frequently
occurring language intervention was teaching participants to adapt their communication to
the context; be they children or adults. Three interventions dominated phonology; cycles,
contrast interventions and teaching phonological awareness to affect output phonology.
Within phonological processing, interventions involved phonological awareness and
enhanced speech. No articles reported the use of augmentative or alternative communication
techniques in intervention9.
TABLE 5 FREQUENCY OF PUBLICATION BY INTERVENTION TYPE
Domain Type of intervention Study
Code*
N studies
Language Adapting communicative context
1. Children adapt their communication to the context
2. Significant adults alter their communication patterns with
children (e.g. using a system of levels of questions)
1, 2, 3, 4, 38
13, 20, 24,
25
9
Semantic and phonological elaboration 6 1
Mixed across word, sentence and discourse levels for
comprehension & expression
7 1
Discourse to effect discourse, syntax &/or semantics 43, 45 2
Metalinguistic 8 1
Script therapy + modelling + a published package Reading
Milestones
41 1
Computer software 10 1
Colour and shapes 16, 17, 18 3
Imitation vs conversational recast 23, 34 2
Phonology Psycholinguistic approach 35 1
Cycles
Cycles + interactive routines, play scripts
Cycles vs Parents and children together
Cycles + integrated phoneme awareness treatment
12
37
30
3
Traditional vs phonological 29 1
Integrated phoneme awareness treatment (Gillon) 14, 32 2
Contrast therapy
Minimal vs maximal contrasts
Minimal vs maximal contrasts vs naturalist speech
intelligibility
Contrast therapy vs core vocabulary
15
46
11
3
Traditional 19 1
Conventional vs phonological awareness training 42 1
Adapting the communicative context 20 1
9 This insight arose from an informal discussion with Catherine Olsson (19/09/2008)
15
Integral stimulation dynamic temporal cueing 44
Phonological
processing
Tabletop vs computer activities vs no Rx 48 1
Phonological awareness general 33 1
Enhanced speech
Enhanced speech vs not enhanced
Fast ForWord
Fast ForWord vs enhanced speech vs LiPs
40
31
36
3
Language &
phonology
LiPs + published syntax and semantic resources 21, 22 2
Not described (focus on service delivery model) 39, 47 2
Others Follow up/audit 6, 9, 27, 28,
25
5
Total studies 48
Key: *See Appendix 1 for code
NUMBER OF CHILDREN IN INTERVENTION SESSIONS
Intervention occurred on an individual basis in 36/48 (75%) studies, in groups 9/48 (20%)
studies and in combination in 3/48 (5%) studies.
DOSAGE
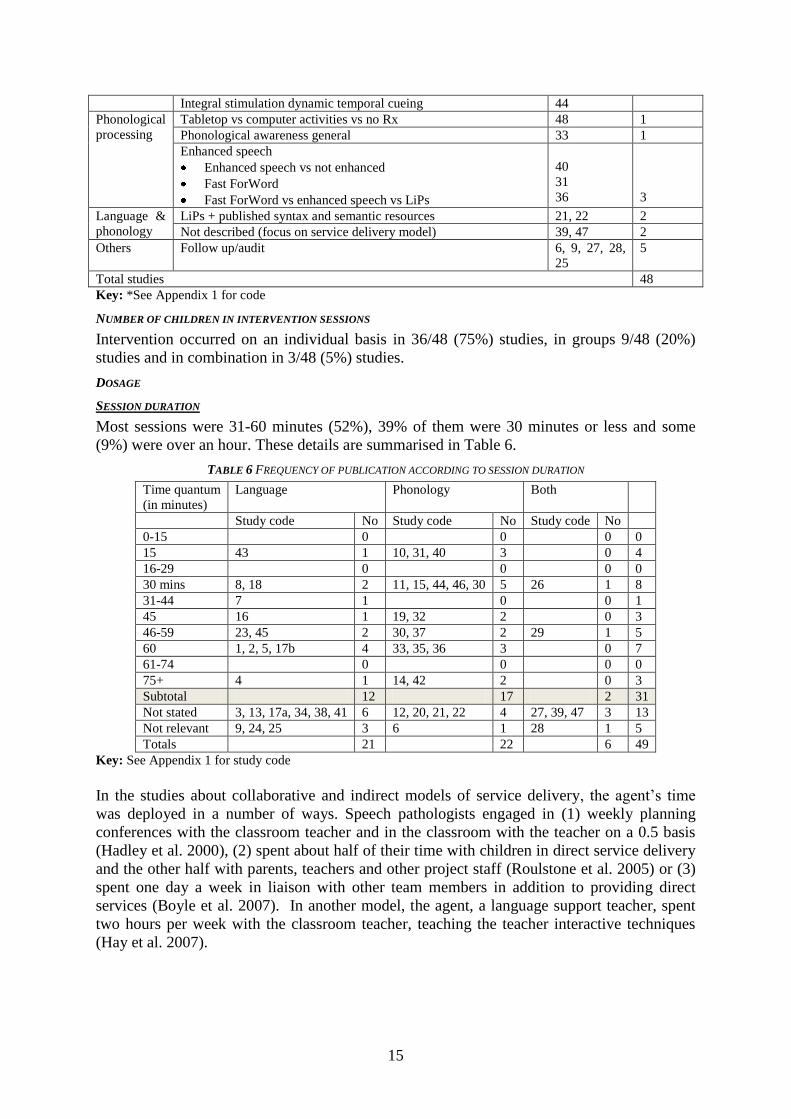
SESSION DURATION
Most sessions were 31-60 minutes (52%), 39% of them were 30 minutes or less and some
(9%) were over an hour. These details are summarised in Table 6.
TABLE 6 FREQUENCY OF PUBLICATION ACCORDING TO SESSION DURATION
Time quantum
(in minutes)
Language Phonology Both
Study code No Study code No Study code No
0-15 0 0 0 0
15 43 1 10, 31, 40 3 0 4
16-29 0 0 0 0
30 mins 8, 18 2 11, 15, 44, 46, 30 5 26 1 8
31-44 7 1 0 0 1
45 16 1 19, 32 2 0 3
46-59 23, 45 2 30, 37 2 29 1 5
60 1, 2, 5, 17b 4 33, 35, 36 3 0 7
61-74 0 0 0 0
75+ 4 1 14, 42 2 0 3
Subtotal 12 17 2 31
Not stated 3, 13, 17a, 34, 38, 41 6 12, 20, 21, 22 4 27, 39, 47 3 13
Not relevant 9, 24, 25 3 6 1 28 1 5
Totals 21 22 6 49
Key: See Appendix 1 for study code
In the studies about collaborative and indirect models of service delivery, the agent‟s time
was deployed in a number of ways. Speech pathologists engaged in (1) weekly planning
conferences with the classroom teacher and in the classroom with the teacher on a 0.5 basis
(Hadley et al. 2000), (2) spent about half of their time with children in direct service delivery
and the other half with parents, teachers and other project staff (Roulstone et al. 2005) or (3)
spent one day a week in liaison with other team members in addition to providing direct
services (Boyle et al. 2007). In another model, the agent, a language support teacher, spent
two hours per week with the classroom teacher, teaching the teacher interactive techniques
(Hay et al. 2007).
16
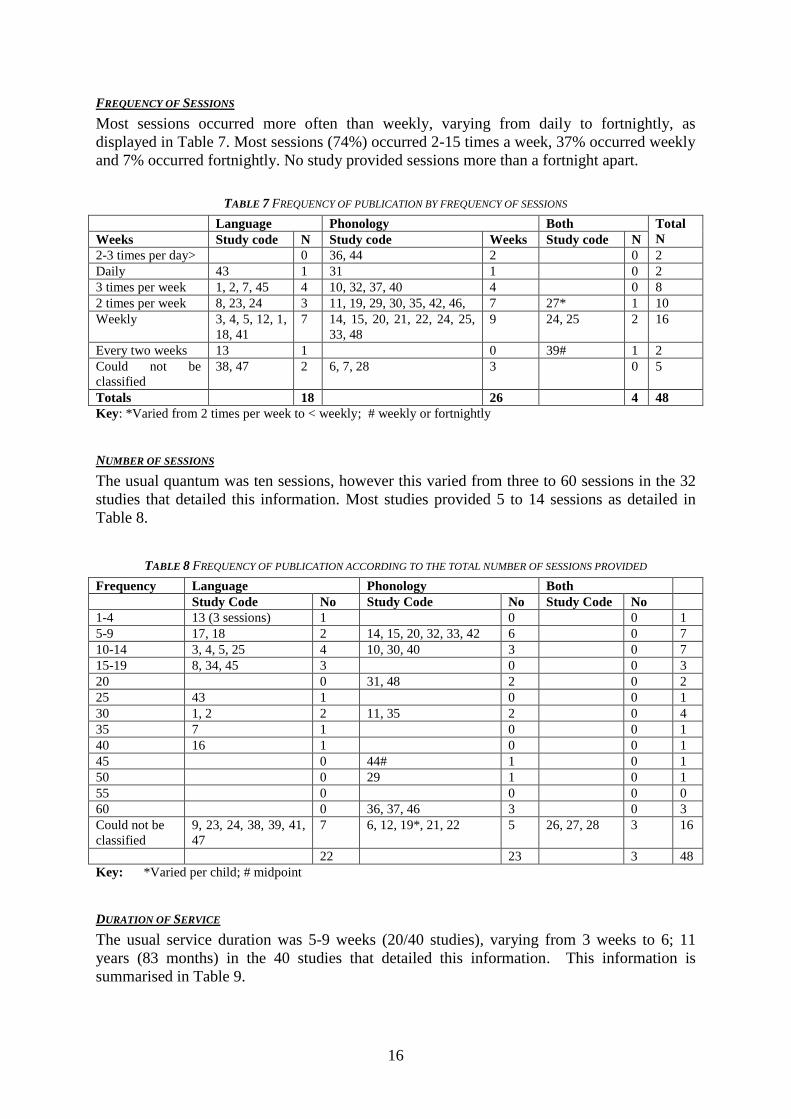
FREQUENCY OF SESSIONS
Most sessions occurred more often than weekly, varying from daily to fortnightly, as
displayed in Table 7. Most sessions (74%) occurred 2-15 times a week, 37% occurred weekly
and 7% occurred fortnightly. No study provided sessions more than a fortnight apart.
TABLE 7 FREQUENCY OF PUBLICATION BY FREQUENCY OF SESSIONS
Language Phonology Both Total
N Weeks Study code N Study code Weeks Study code N
2-3 times per day> 0 36, 44 2 0 2
Daily 43 1 31 1 0 2
3 times per week 1, 2, 7, 45 4 10, 32, 37, 40 4 0 8
2 times per week 8, 23, 24 3 11, 19, 29, 30, 35, 42, 46, 7 27* 1 10
Weekly 3, 4, 5, 12, 1,
18, 41
7 14, 15, 20, 21, 22, 24, 25,
33, 48
9 24, 25 2 16
Every two weeks 13 1 0 39# 1 2
Could not be
classified
38, 47 2 6, 7, 28 3 0 5
Totals 18 26 4 48
Key: *Varied from 2 times per week to < weekly; # weekly or fortnightly
NUMBER OF SESSIONS
The usual quantum was ten sessions, however this varied from three to 60 sessions in the 32
studies that detailed this information. Most studies provided 5 to 14 sessions as detailed in
Table 8.
TABLE 8 FREQUENCY OF PUBLICATION ACCORDING TO THE TOTAL NUMBER OF SESSIONS PROVIDED
Frequency Language Phonology Both
Study Code No Study Code No Study Code No
1-4 13 (3 sessions) 1 0 0 1
5-9 17, 18 2 14, 15, 20, 32, 33, 42 6 0 7
10-14 3, 4, 5, 25 4 10, 30, 40 3 0 7
15-19 8, 34, 45 3 0 0 3
20 0 31, 48 2 0 2
25 43 1 0 0 1
30 1, 2 2 11, 35 2 0 4
35 7 1 0 0 1
40 16 1 0 0 1
45 0 44# 1 0 1
50 0 29 1 0 1
55 0 0 0 0
60 0 36, 37, 46 3 0 3
Could not be
classified
9, 23, 24, 38, 39, 41,
47
7 6, 12, 19*, 21, 22 5 26, 27, 28 3 16
22 23 3 48
Key: *Varied per child; # midpoint
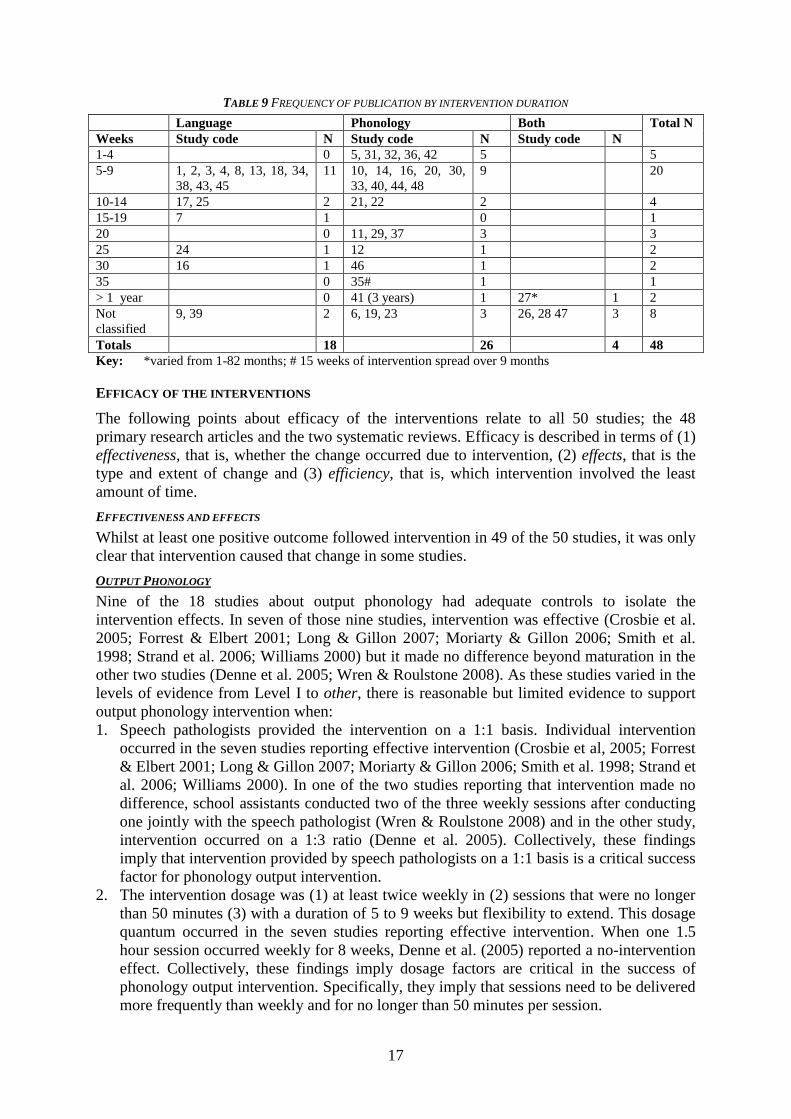
DURATION OF SERVICE
The usual service duration was 5-9 weeks (20/40 studies), varying from 3 weeks to 6; 11
years (83 months) in the 40 studies that detailed this information. This information is
summarised in Table 9.
17
TABLE 9 FREQUENCY OF PUBLICATION BY INTERVENTION DURATION
Language Phonology Both Total N
Weeks Study code N Study code N Study code N
1-4 0 5, 31, 32, 36, 42 5 5
5-9 1, 2, 3, 4, 8, 13, 18, 34,
38, 43, 45
11 10, 14, 16, 20, 30,
33, 40, 44, 48
9 20
10-14 17, 25 2 21, 22 2 4
15-19 7 1 0 1
20 0 11, 29, 37 3 3
25 24 1 12 1 2
30 16 1 46 1 2
35 0 35# 1 1
> 1 year 0 41 (3 years) 1 27* 1 2
Not
classified
9, 39 2 6, 19, 23 3 26, 28 47 3 8
Totals 18 26 4 48
Key: *varied from 1-82 months; # 15 weeks of intervention spread over 9 months
EFFICACY OF THE INTERVENTIONS
The following points about efficacy of the interventions relate to all 50 studies; the 48
primary research articles and the two systematic reviews. Efficacy is described in terms of (1)
effectiveness, that is, whether the change occurred due to intervention, (2) effects, that is the
type and extent of change and (3) efficiency, that is, which intervention involved the least
amount of time.
EFFECTIVENESS AND EFFECTS
Whilst at least one positive outcome followed intervention in 49 of the 50 studies, it was only
clear that intervention caused that change in some studies.
OUTPUT PHONOLOGY
Nine of the 18 studies about output phonology had adequate controls to isolate the
intervention effects. In seven of those nine studies, intervention was effective (Crosbie et al.
2005; Forrest & Elbert 2001; Long & Gillon 2007; Moriarty & Gillon 2006; Smith et al.
1998; Strand et al. 2006; Williams 2000) but it made no difference beyond maturation in the
other two studies (Denne et al. 2005; Wren & Roulstone 2008). As these studies varied in the
levels of evidence from Level I to other, there is reasonable but limited evidence to support
output phonology intervention when:
1. Speech pathologists provided the intervention on a 1:1 basis. Individual intervention
occurred in the seven studies reporting effective intervention (Crosbie et al, 2005; Forrest
& Elbert 2001; Long & Gillon 2007; Moriarty & Gillon 2006; Smith et al. 1998; Strand et
al. 2006; Williams 2000). In one of the two studies reporting that intervention made no
difference, school assistants conducted two of the three weekly sessions after conducting
one jointly with the speech pathologist (Wren & Roulstone 2008) and in the other study,
intervention occurred on a 1:3 ratio (Denne et al. 2005). Collectively, these findings
imply that intervention provided by speech pathologists on a 1:1 basis is a critical success
factor for phonology output intervention.
2. The intervention dosage was (1) at least twice weekly in (2) sessions that were no longer
than 50 minutes (3) with a duration of 5 to 9 weeks but flexibility to extend. This dosage
quantum occurred in the seven studies reporting effective intervention. When one 1.5
hour session occurred weekly for 8 weeks, Denne et al. (2005) reported a no-intervention
effect. Collectively, these findings imply dosage factors are critical in the success of
phonology output intervention. Specifically, they imply that sessions need to be delivered
more frequently than weekly and for no longer than 50 minutes per session.
18
3. Intervention that integrates phonological awareness and word production work. This
occurred in five of the nine studies (Crosbie et al 2005; Forrest & Elbert 2001; Long &
Gillon 2007; Moriarty & Gillon 2006; Williams 2000). In particular, word production
work focuses on reducing homophony rather than on the correction of individual sounds.
Homophony is a common occurrence in speech impairment whereby children say many
different words identically, compromising listeners‟ comprehension of what it said.
Phonology gains may be sustained beyond the conclusion of intervention but the evidence is
mixed. Bernhardt and Major (2005) followed up twelve 7-year-olds who had received
intervention for output phonology when they were 3-4 years of age and found that all
children were intelligible and had normal language scores as measured by the PPVT and the
CELF. Ten of them had normal reading skills and seven had normal spelling scores. Dodd et
al. (2008) reported that 14 of their 19 participants had maintained the gains from contrast
intervention measured 14 weeks after the intervention had ceased. Long and Gillon (2007)
reported that a boy, aged 5 years maintained the changes in speech (and phonological
awareness) five months later. However, although Wren & Roulstone (2008) reported
phonology increased over the study period, they found no intervention effect as there were no
differences between the control and experimental groups at the conclusion of the intervention
period or three months later.
The effects of intervention were measured in a variety of ways and included consistency of
word production (Crosbie et al. 2005), percentage of phonemes correct (Crosbie et al. 2005;
Long & Gillon 2007; Moriarty & Gillon 2006), correct underlying representations (the level
of adult like production of phonemes) (Williams 2000), individual phoneme accuracy
(Forrest & Elbert 2001) and whole words (Strand et al. 2006). Whilst Smith et al. (1998) used
the South Tyneside Test of Phonology to measure phonology output, they did not describe the
outcome measure.
PHONOLOGICAL PROCESSING
Seven of the 11 studies on phonological processing had adequate controls to isolate the
intervention effects. In four of those seven studies, intervention was effective but it made no
difference for three studies. As these studies varied in the levels of evidence from Level I to
other, there is reasonable but limited evidence to support phonological processing
intervention it its focus is phonological awareness. All four studies which aimed to develop
phonological awareness reported effectiveness (Cirrin & Gillam 2008; Hadley et al. 2000;
Munro & Atkinson 2003; Long & Gillon 2007). Further, phonological awareness intervention
was effective when provided individually (Long & Gillon 2007), in a group (Munro &
Atkinson 2003) or in a classroom (Hadley et al. 2000), either weekly or more frequently.
If the focus of intervention is to improve phonological processing through intense exposure to
slowed speech (acoustic properties manipulated), then intervention seems to make no
difference because the four studies investigating this impact reported no effectiveness (Cirrin
& Gillam 2008; Marler et al. 2001; Pokorni et al. 2004; Segers & Verhoeven 2004).
The evidence that phonological processing skills are sustained after intervention ceases is
mixed. The one study reporting on phonological awareness indicated gains five months post
intervention (Long & Gillon 2007), whereas the one study about phonological processing did
not show any gains four months post intervention (Segers & Verhoeven 2004).
19
PRAGMATICS
Three of the seven studies addressing pragmatics had adequate controls indicating that the
changes were attributable to intervention (Adams et al. 2006; Adams & Lloyd 2007; Cirrin &
Gillam 2008). As these studies varied in the levels of evidence from Level I to IV, there is
some limited evidence to support pragmatic intervention in the short term when intervention
is conducted by a speech pathologist on an individual basis. However, there was no evidence
to indicate if these gains were sustained over time.
The effects of the intervention measured, included whether children responded in a socially
appropriate way within conversations (Adams et al. 2006; Adams & Lloyd 2007).
Specifically, Adams and colleagues determined whether children were over- or under-
dominant in conversation and whether they could “read between the lines”.
DISCOURSE
One of the three studies addressing discourse had adequate controls indicating that the
changes were attributable to intervention (Cirrin & Gillam 2008). This systematic review
(Level I) study provides strong but limited evidence to support discourse intervention. There
was no evidence about whether gains in discourse were sustained over time.
SYNTAX
Seven of the 13 studies described in 11 articles had adequate controls to determine the
influence of syntax intervention (Cirrin & Gillam 2008; Ebbels & van der Lely 2001; Ebbels
2007 (Studies 1 & 2); Ebbels et al. 2007; Law et al. 2003; Nelson et al. 1996). In all of those
studies, intervention was reported as effective. The following results are highlighted when
considering the collective evidence.
1. The conclusions of the two systematic reviews were that there was only evidence to
support expressive syntax intervention not receptive syntax.
2. Ebbels and colleagues (Ebbels & van der Lely 2001; Ebbels 2007; Ebbels et al. 2007)
reported effective intervention for receptive and expressive syntax for children aged 11 to
16 years. In all studies, a speech pathologist provided the intervention. Reported increases
in children‟s comprehension and use of syntactic construction included questions (wh-
and comparative), passives, dative case (the cow is giving the pig the sheep) and past
tense markers.
As these studies varied in the levels of evidence from Level I to IV, there is reasonable but
limited evidence to support syntax receptive and expressive intervention when intervention is
conducted by a speech pathologist on an individual basis. Further, the studies by Ebbels and
colleagues imply that the intervention is predicated on in-depth language analysis to yield a
highly individualised care package indicate and that it needs to occur in a specialised school
for children with specific language impairment.
There was no evidence about whether syntax gains were sustained.
SEMANTICS
Six of the 10 semantics studies had adequate controls to determine the influence of
intervention. In five of these six studies, intervention was effective (Bayne & Moran 2005;
Cirrin & Gillam 2008; Hadley et al 2000; Law et al. 2003; Steigler & Hoffman 2001). The
following results are highlighted for considering the collective evidence.
1. Expansion of expressive semantics intervention was supported in all three studies
examining this (Cirrin & Gillam 2008; Hadley et al. 2000; Law et al. 2003)
2. Word retrieval was enhanced in the two studies examining this skill (Bayne & Moran
2005; Steigler & Hoffman 2001)
20
3. Support for receptive vocabulary intervention was mixed with support in a no-
intervention control group study (Hadley et al. 2000) but not in an RCT (Boyle et al.
2007).
As these studies varied in the levels of evidence from Level I to IV, there is reasonable but
limited evidence to support semantic intervention when delivered by a speech pathologist
directly or in a collaborative situation (Hadley et al. 2000). As Boyle et al. (2007) reported no
changes to receptive vocabulary on the PPVT, this finding suggests that the program they
developed may not have been effective for enhancing receptive vocabulary (see pg 26 for the
conditions).
There was no evidence that semantics gains were sustained.
COMPOSITE LANGUAGE OUTCOMES
One of the five studies expressing outcomes in composite scores (combined score of more
than one language domain) had adequate controls to determine the influence of intervention
(Boyle et al. 2007). This level II study reported effectiveness for expressive language but not
receptive language with changes sustained over 12 months.
EFFICIENCY
OUTPUT PHONOLOGY
Five of the 19 studies about output phonology compared interventions. Core vocabulary
intervention resulted in more speech changes for 10 4- to 6-year-olds with inconsistent
speech impairment than consistent speech impairment. However, contrast therapy resulted in
more speech changes for eight 4- to 6-year-olds with consistent speech impairment than
inconsistent speech impairment (Crosbie et al. 2005). Minimal and maximal contrast
interventions were equally effective for all 19 3- to 6-year-olds with phonological disorder
(Dodd et al. 2008). Phonological therapy was more efficient than traditional therapy for 36
children with multiple articulation errors, aged 3;0 to 5;10 years (Klein 1996). Conventional
therapy combined with phonological awareness training altered output for nine of the 18 5- to
8-year-olds with persistent specific phonological disorder (Smith et al. 1998).
The final study has significant implication for schoolchildren. Kirk and Gillon (2007)
concluded that children with speech impairment who received intervention that integrated
phonological awareness with production work as 4-year-olds had better long-term literacy
outcomes as 8-year-olds than their peers whose intervention only focussed on sound
production and excluded phonological awareness work.
PHONOLOGICAL PROCESSING
Three of the 12 studies about phonological processing compared interventions. They showed
that children did not receive a phonological processing advantage from working with
proprietary software using enhanced (slowed) speech over normal speech, vocabulary work
or phonological awareness work (Marler et al. 2001; Pokorni et al. 2004; Segers &
Verhoeven 2004). More specifically, the proprietary software Fast ForWord did not deliver
an advantage.
However, with respect to phonological awareness, Pokorni et al. (2004) reported that the
LiPS and Earobics programmes improved phonological awareness whereas Fast ForWord
did not. Also, Earobics, seemed most effective for enhancing phoneme segmentation whereas
LiPs, seemed most effective for enhancing phoneme blending and segmentation.
21
SYNTAX
Three of the 10 primary syntax research studies compared interventions. Conversational
recasts10
resulted in quicker gains in syntax than imitation across 14 children with language
impairment, aged 4-6 years and seven typically developing control children, aged 2-4 years
(Gillum et al. 2003; Nelson et al. 1996). By contrast, syntactic-semantic therapy and semantic
therapy11
appear equally effective in fostering receptive and expressive syntax for children
with specific language impairment, aged 11 to 16 years but superior to the usual package of
care with respect to syntax (Ebbels et al. 2007).
PRAGMATICS, DISCOURSE, SEMANTICS AND COMPOSITE LANGUAGE
None of the studies about pragmatics, discourse, semantics and composite language
compared different interventions so there is no evidence about efficiency from this review.
10
Conversational recasts occur when an agent repeats children‟s immature or erroneous sentences in a more
correct way to model to the child accurate production. Usually there is not expectation for the child to respond
however extensive studies of typically developing children indicate they do this spontaneously whilst acquiring
language. 11
See the descriptions of these interventions in the full description of the articles authored by Ebbels and
colleagues in Appendix 2
CHAPTER 4: DISCUSSION
The studies located for this review were heterogeneous with regards to many of the variables
under consideration such as service delivery model, the intervention and intervention goals.
This limits the generalities that can be distilled from them. For example, whilst output
phonology was the focus of many articles, it was rare that the same intervention was used and
if the same intervention was used, the goals were not, limiting comparisons. So whilst some
generalities are determined, practitioners will need to consider this heterogeneity when
applying the findings of this review to their local situation.
EFFICACY OF INTERVENTIONS
Overall, intervention was efficacious for children aged 5 to 16 years with primary speech and
or language impairment indicated by higher and lower levels of evidence.
EFFECTIVENESS AND EFFECTS
The higher level evidence (systematic reviews and RCTS) (Boyle et al. 2007; Ebbels et al.
2007; Cirrin & Gillam 2008; Law et al. 2003) indicates that speech and language intervention
was responsible for the intended changes in children‟s speech and language.
The lower level evidence (non-randomised control studies through to single subject case
series studies) implied that intervention was associated with improvements in children‟s
outcomes ranging from increased sound accuracy, phonological awareness, discourse,
receptive and expressive semantics, word retrieval and receptive and expressive syntax.
On balance, the evidence seems to support output phonology and expressive vocabulary
intervention but is mixed for phonological processing, receptive vocabulary and receptive
and expressive syntax intervention. The evidence for discourse and pragmatics intervention is
small in amount but positive.
EFFICIENCY OF THE INTERVENTIONS
Given some phonology and syntax interventions seemed more efficient than others, aspects
of the relevant studies are further considered.
Whilst Pokorni et al. (2004) reported that the proprietary packages of Earobics and LiPs
resulted in differential effects for phonological awareness the opportunity costs of their
program are noteworthy. The children appeared to achieve small gains for considerable
expenditure of time, as each child received 60 hours of intervention over 20 days. Whilst this
study is not directly comparable with other studies about phonological awareness, these
findings of minimal gains for 60 hours of intervention contrast with Gillon and colleagues‟
findings (Gillon & Dodd 1995; 1998; Kirk & Gillon 2007; Long & Gillon 2007; Gillon &
Moriarty 2006) who achieved significant effects in phonological awareness with packages of
6 to 27 hours.
The theme common to the studies that Gillon and colleagues (Gillon & Dodd 1995; 1998;
Kirk & Gillon 2007; Long & Gillon 2007; Gillon & Moriarty 2006) conducted is that
production and phonological awareness work were integrated and this may have been the key
to success in phonological awareness and production. This notion that children need a
multidimensional input that includes information about the motoric (movement) and
phonological information is well supported in the theoretical phonology literature (e.g.
Stackhouse & Wells 1997; 2001) and other intervention literature (e.g. Baker 2000 and see
23
Stage 1 of this review). However, it is noteworthy that Denne et al. (2005) did not achieve the
same outcomes as Gillon and colleagues did when using the program that Gillon and
colleagues developed. However, Denne et al. (2005) implemented this intervention with at
least three variations that may account for these outcome differences. They conducted all
sessions with in groups of three children rather than in individual and group sessions.
Sessions were weekly rather than 2 to 3 times per week. And finally, sessions ran for 1.5
hours rather than no longer than 50 minutes. These three differences in service delivery may
be the critical features for successful phonological intervention.
Dodd et al. (2008) found no differences when using minimal or maximal pairs in
phonological intervention. This may have significant implications for planning time for
children‟s intervention. Minimal pairs require much greater planning time than maximal pairs
because minimal pairs demand a greater level of customising the intervention words than
maximal pairs. For example, if a child substitutes „t‟ for „s‟ in words (sat, sack, seal, said as
tat, tack and teal respectively), the minimal pair approach dictates that the only rhyming
words that can be used are those staring with „t‟, requiring the speech pathologist to select a
custom group of words for that child. This also means that this package of words could not be
used again with another child who erred on the same words but substituted „s‟ with „ch‟ and
said chat chack and cheal instead. By contrast, the maximal pair approach requires a broader
group of rhyming words to be used. So for the child who substitutes „t‟ for „s‟, the
intervention words could include chat, mat bat and cat in addition to tat (and so on for all the
other intervention words).This means that this same group of words can be used for the child
in the second example, thereby saving considerable planning time.
The evidence that Ebbels and colleagues (Ebbels 2007; Ebbels & van der Lely 2001; Ebbels
et al. 2007) presented about positive outcomes for receptive syntax is at variance with the
conclusions of the two systematic reviews that receptive language was resistant to
intervention (Law et al. 2003; Cirrin & Gillam 2008). Whilst the studies within the reviews
are not comparable with those of Ebbels and colleagues, the fact that Ebbels and colleagues
achieved positive outcomes may indicate that their technique was effective in promoting
receptive syntax. The three steps in their technique involved; segmenting sentences into
grammatical components (such as subject and verbs), linking each component with a specific
shape of a particular colour then manipulating the coloured shapes, and therefore the
grammar components to develop their comprehension of grammar. Whilst their findings need
replication to increase confidence in them, their findings may suggest that the use of coloured
shapes as codes in syntax intervention is a key success factor.
Given this success in receptive syntax intervention, it is interesting to note that Gillon and
colleagues (Gillon & Dodd 1995, 1998; Kirk & Gillon 2007; Long & Gillon 2007; Gillon &
Moriarty 2006) and Denne et al. (2005) used a similar technique and steps to advance
children‟s phonology. Specifically, the children were engaged in tasks to segment words into
sounds, link each sound to different coloured blocks (shapes) and then manipulate the
coloured blocks and therefore the sounds of the words to enhance phonology. Gillon and
colleagues reported associated changes in phonological awareness and output phonology in
the short term (Gillon & Dodd 1995, 1998; Long & Gillon 2007; Gillon & Moriarty 2006)
and literacy in the long term (Kirk & Gillon 2007). Denne et al. (2005) using similar
techniques and steps reported improved outcomes for children‟s phonological awareness but
not for output phonology. Thus taking the findings of the Gillon and colleagues and Ebbels
and colleagues together may indicate that representing components of linguistic structures
24
with coloured shapes and then manipulating those shapes may be a critical feature of
successful intervention in phonology and language.
SERVICE DELIVERY CONSTRUCTS
Given the studies that focus on interventions has now been considered, taken together,
generalities can be distilled from these studies about interventions that relate to the efficacy
of models of service delivery.
EFFICACY OF DIRECT MODELS OF SERVICE DELIVERY
Direct, clinical services for speech and language appear to be effective. They were the most
frequent type of service occurring in 39 of the 48 studies. The repeated findings of
improvements over a broad range of outcomes in phonology and language imply that direct
services are effective, especially from the 33 studies that had sufficient controls to determine
the influence of intervention.
Direct clinical services provided on an individual or group basis appear effective. This seems
clearer for individual services than group services, merely because individual services
occurred more frequently (29 studies) than group services (seven studies) with another three
studies combining the two. However, the RCT that Boyle et al. (2007) conducted is
particularly noteworthy for this point about the effectiveness of direct group or individual
intervention because they compared it for language intervention. They found that the children
in both groups made significantly more gains than the control children who received usual
care, but there were no differences between the two experimental groups. This suggests that
both types of intervention are equally successful, when the conditions they developed are met
(these are detailed on the next page).
Group intervention may be equally as effective as individual intervention for phonology
(Law et al. 2003). Law et al. (2003) concluded this within their Level I study for school age
children receiving phonology intervention. However, this one study was published in the
1960s using an intervention that is rarely used now, precluding comparisons to contemporary
publications.
There were 33 direct service delivery model studies that included adequate controls to
determine the effect of the direct intervention. Common features from the successful
interventions are:
provided by a speech pathologist
usually on an individual basis
time-limited and intense with a dosage of two to three 30-minute sessions per week
for about 5 to 9 weeks but with the flexibility to extend if needed
usually addressing either speech or language rather than both
integrating production and phonological awareness work to achieve positive outcomes
for phonology.
EFFICACY OF INDIRECT MODELS OF SERVICE DELIVERY
Indirect services occurred in four of the studies. Only one study had adequate controls to
determine the intervention effect. This study also compared indirect services with direct
services. Boyle et al. (2007) suggested that direct and indirect language services were equally
effective because all the experimental groups made significant gains over the children in the
control group who received usual care, and there were no significant differences in the gains
made between the experimental groups, as measured by the CELFUK
. Whilst this is only one
25
study, it was a well-constructed RCT and it may be worth noting the program features and
some of the secondary outcomes. Boyle et al. (2007) noted that their findings about the
children‟s outcomes and the outcomes about cost can only be generalised to other
educational/health systems where the resources would equate to those described in this study
which included:
a programme explicitly negotiated with and supported by senior management and
with management providing dedicated resources in addition to staff
a well planned program whose implementation was preceded by a long lead time for
planning and developing the service, including predicting and marshalling all
resources
allocated liaison time of one day per week for each speech pathologist
a caseload of 9 children for each speech pathologist or speech pathology assistant
intensive therapy provision (3 times per week for 30-40 minutes for 15 weeks)
a detailed intervention manual, developed from an extensive literature review
clearly articulated policy and procedures
assistants that were provided with extensive training and support. Prior to the
commencement of the programme, the assistants were trained using a credentialed
training package and were supported throughout the project.
transporting children from their home school to the programme schools to receive
their intervention..
In addition to measuring language outcomes about impairment status, activity and
participation information was procured through parent and teacher questionnaires and focus
groups. Teachers reported that children‟s self-esteem increased (Boyle et al. 2007, p56)
indicated by statements such as, „The child was much happier and began to participate in the
class discussion‟; „It helped the child with conversation and this gave her more confidence
with reading and writing‟. Parents also reported improvements in self-confidence, social
interaction, behaviour and literacy (Boyle et al. 2007, p. 61). This implies that this type of
package may also address the impairment, activity and participation levels of the ICF (WHO
2001).
EFFICACY OF THE COLLABORATIVE MODELS OF SERVICE DELIVERY
Four of the studies were described as collaborative services (Gardner 2006; Hadley et al.
2000; Roulstone et al. 2005; Wren et al. 2001). Whilst all papers reported improved outcomes
for children and other stakeholders, only one study had adequate controls to determine the
influence of interventions (Hadley et al. 2000).
However, given one of the aims of this review was to determine service delivery constructs
these four studies are discussed further because they were judged as providing useful
information.
These four studies involved schools and shared many of the following service delivery
characteristic constructs with two of them receiving explicit support for these projects by
senior levels of management or the relevant authority(ies) (Roulstone et al. 2005; Wren et al.
2001). In these later two studies, local service agreements were developed collaboratively
and grounded in philosophies, policies and procedures relevant to the local stakeholders but
with the imprimatur of senior management. These philosophies typically had children and
their communication difficulties at their core but recognised that to maximise children‟s
speech, language and communication outcomes the focus of intervention had to be broader
26
than the child (Roulstone et al. 2005; Wren et al. 2001). Resources (human and other) were
predicted from a system perspective, negotiated, planned, and procured prior to
implementation. Thus, the service delivery procedures were not centrally prescribed but
developed locally to suit the local context within guidelines. Implementation was supported
by dedicated, inclusive joint management structures that enabled team members to be
accountable to their project and professional managers. Management practices supported
collaboration rather than leaving it to chance, by allocating times for collaboration between
teachers and speech pathologists. Staff development was an integral part of all four projects
to ensure that team members developed a shared language as well as enhanced understanding
of the roles of other team professionals to facilitate collaboration. These practices meant that
accessibility of speech pathologists in schools was increased and their time was deployed in
varying ways. One way was being in the classroom for half a week working with the teacher
and children (Hadley et al. 2000). Another way was to spend about half the allocated time
working with children individually and the other half with parents and teachers (Roulstone et
al. 2005).
In addition to measuring the children‟s outcomes, Roulstone et al. (2005) and Wren et al
(2001) reported on the outcomes from the perspectives of other stakeholders including
parents, teachers and speech pathologists. Parents reported that they were pleased with the
outcomes for their children. Teachers and speech pathologist‟s self- reported an increased
knowledge about other professionals and that speech pathologist‟s were considered as part of
the school team. For organisations that provide peripatetic speech pathology services,
projects such as these may provide guidelines for team building and may have staffing
implications.
LIMITATIONS OF THE REVIEW
One limitation of this review is that the studies within it may not reflect community clinical
practice with respect to the time expended on planning and evaluating them. These studies
were probably developed by academics in academic environments that may well be different
to community services in a number of ways including access to resources such as journals
and time for project development and evaluation. Whilst it is impossible to quantify this time,
it is reasonable to assume it is considerable. This is so because all the studies are published
and, this in turn, presupposes a number of planning and evaluations processes. Aside from the
preparation time to write grant and ethics applications, considerable time was probably
expended developing the intervention using processes which may include literature reviews,
peer review, negotiations with stakeholders, trials and developing instruction manuals. These
steps were explicitly acknowledged by Boyle et al. (2007) and Roulstone and colleagues
(2001; 2005) in developing their service delivery models and are implied in most of the
studies. Some or all of these processes may be critical to the success of the interventions and
therefore may be constructs for consideration in developing services.
27
CHAPTER 5: CORE LEARNINGS
EFFICACY OF INTERVENTIONS
EFFECTIVENESS
1 Speech pathology seems effective for children, aged 5 years and above with primary
speech and/or language impairment to advance their linguistic skills. There is some
evidence for secondary gains in literacy and self-esteem.
2 Output phonology, phonological awareness and expressive vocabulary intervention is
supported.
3 Phonology interventions that combine phonological awareness with production work
appear to positively affect speech and literacy.
4 Phonological awareness interventions that codes sounds with coloured blocks that can be
manipulated seem effective.
5 Gains in phonology from intervention appear to be sustained in the short and long term.
There appear to be secondary gains for literacy.
6 Intervention that aims to enhance phonological processing intervention with the use of
enhanced (slowed) speech is not supported. More particularly, there was no support for
using the proprietary software programme, Fast ForWord.
7 The evidence is mixed for receptive vocabulary and receptive and expressive syntax
intervention. However, recent positive evidence about intervention for receptive and
expressive syntax is at variance with the earlier consensus that it seemed not to be
beneficial.
8 Syntax interventions that code grammatical constituents with coloured shapes that can be
manipulated seem effective.
9 The evidence for discourse and pragmatics intervention is small in amount but positive.
10 The applicability of many of the findings is limited because within each of the domains
of language the numbers of studies were too small to adequately cover all the relevant
variables.
EFFICIENCY
1 Phonology output intervention that combines speech production work and phonological
awareness seems more efficient than speech production work alone.
2 Children with different forms of speech (phonological) impairment appear to respond
differentially to different interventions.
3 The phonological interventions of minimal and maximal contrast therapy may be equally
efficient (1 study).
4 Customised intervention for phonological awareness intervention seems more efficient
than the commercial packages of LiPS™ and Earobics.
5 Within expressive syntax, conversational recasts seem a more efficient intervention than
imitation.
6 Syntactic-semantic therapy and semantic therapy for receptive and expressive syntax
may be equally effective.
7 There was no efficiency data about pragmatics, discourse, semantics or composite
language interventions.
8 Representing linguistic components (sounds and syntax components) with coloured
shapes such as blocks that can be manipulated may be a key feature of successful
phonology and syntax interventions.
28
MODELS OF SERVICE DELIVERY
EFFECTIVENESS
1. Direct intervention seems effective. More particularly, time-limited intensive direct
intervention with a dosage of two to three 30-minute sessions per week, for about 5 to 9
weeks, results in significant changes to speech and language.
2. Direct therapy should ideally be administered by a qualified speech pathologist,
particularly for phonology.
3. Direct and indirect group or individual intervention for children with language
impairment seems effective when meeting a prescribed set of conditions (see page 26).
4. The constructs of indirect and collaborative models on service delivery appear to be:
a programme explicitly negotiated with and supported by senior management and
with management providing dedicated resources in addition to staff that is
underpinned by a negotiated philosophy
This philosophy appears to subsume many principles of the International
Classification of Functioning
Deployment of resources such that
a. Speech pathologists provide time-limited intensive therapy provision (e.g. 3
times per week for 30-40 minutes for 3 to 15 weeks). In one study, this co-
occurred with a case load of 9 children (at any one block of time)
b. There is allocated liaison time for teachers and speech pathologists and other
staff involved in service delivery
c. Staff are educated to meet the agency requirements and are supported with
work manuals
d. Speech pathologists are recognised as a key team member when planning
speech pathology services and they are involved in service level planning,
irrespective of rank within the service.
EFFICIENCY
1 For language
Group or individual direct therapy may be equally effective when a range of
conditions are met (see page 26). Clinical decision making can take into account
clinician judgement and experience, and client preference when making a decision
about using group or individual direct therapy.
2 For phonology
There appears to be clear evidence to support individual direct intervention. As there
is little information about other models of service delivery for phonology,
comparisons between direct and other service delivery models cannot be made.
29
REFERENCES
Access Economics Pty. Ltd. (2008). The economic impact of cerebral palsy in Australia in
2007. Australia: Access Economics Pty. Ltd.
Adams, C., Baxendale, J., Lloyd, J., & Aldred, C. (2005). Pragmatic Language Impairment:
Case Studies of Social and Pragmatic Language Therapy. Child Language Teaching
and Therapy, 21(3), 227-250.
Adams, C., & Lloyd, J. (2007). The effects of speech and language therapy intervention on
children with pragmatic language impairments in mainstream school. British Journal
of Special Education, 34(4), 226-233.
Adams, C., Lloyd, J., Aldred, C., & Baxendale, J. (2006). Exploring the effects of
communication intervention for developmental pragmatic language impairments: A
signal-generation study. International Journal of Language & Communication
Disorders, 41(1), 41-65.
Anger, N., & Sullivan, L. (1995). Problem solving with parents and children. Australian
Communication Quarterly Summer, 28-31.
Baker, E. (2000). Changing nail to snail: A treatment efficacy study of phonological
impairment in children. Unpublished PhD, Sydney: University of Sydney.
Bayne, G., & Moran, C. (2005). The effect of single word semantic-phonological
intervention on developmental word finding difficulties at single words and discourse
levels. New Zealand Journal of Speech-Language Therapy, 60, 31-44.
Bercow, J. (2008). The Bercow report: A review of services for children and young people
(0-19) with speech, language and communication needs. Nottingham: DCSF.
www.dcsf.gov.uk/bercowreview.
Bernhardt, B., & Major, E. (2005). Speech, language and literacy skills 3 years later: A
follow-up study of early phonological and metaphonological intervention.
International Journal of Language and Communication Disorders, 40(1), 1-27.
Bernstein Ratner, N. (2006). Evidence-based practice: An examination of its ramifications for
the practice of speech-language pathology Language, Speech & Hearing Services in
Schools, 37(4), 257-267.
Boyle, J., McCartney, E., Forbes, J., & O'Hare, A. (2007). A randomised controlled trial and
economic evaluation of direct versus indirect and individual versus group modes of
speech and language therapy for children with primary language impairment. Health
Technology Assessment, 11(25:iii-iv, xi-xii), 1-139.
Blum-Harasty, J. A., & Rosenthal, J. B. M. (1992). The prevalence of communication
disorders in children: A summary and critical review. Australian Journal of Human
Communication Disorders, 20, 63-80.
Bryan, K. (2004). Preliminary study of the prevalence of speech and language difficulties in
young offenders International Journal of Language & Communication Disorders,
39(3), 391-400.
Campbell, W. N., & Skarakis-Doyle, E. (2007). School-aged children with SLI: The ICF as a
framework for collaborative service delivery Journal of Communication Disorders,
40, 513-535.
Cirrin, F. M., & Gillam, R. B. (2008). Language intervention practices for school-age
children with spoken language disorders: A systematic review. Languag , Speech, and
Hearing Services in Schools, 39(Supplement), S110-S137.
Conti-Ramsden, G., Botting, N., Knox, E., & Simkin, Z. (2002). Different school placements
following language unit attendance: which factors affect language outcome?
International Journal of Language & Communication Disorders, 37(2), 185-195.
30
Cox, S. (2003). Using computer technology to teach phonological awareness skills
ACQuiring Knowledge in Speech, Language and Hearing, 5(3), 111-113.
Crosbie, S., Holm, A., & Dodd, B. (2005). Intervention for children with severe speech
disorder: A comparison of two approaches. International Journal of Language &
Communication Disorders 40(4), 467 - 491.
Culatta, B., Setzer, L. A., & Horn, D. (2005). Meaning-based intervention for a child with
speech and language disorders. Topics in Language Disorders, 25(4), 388-401.
Dale, P. S., & Crain-Thoreson, C. (1996). Parent-child book reading as an intervention
technique for young children with language delays. Topics in Early Childhood
Special Education, 16(2), 213-235.
Damico, J. S., & Oller, J. W. J. (1980). Pragmatics versus morphological/syntactic criteria for
language referrals. Languag , Speech, and Hearing Services in Schools, 11, 85-94.
Denne, M., Langdown, N., Pring, T., & Roy, P. (2005). Treating children with expressive
phonological disorders: does phonological awareness therapy work in the clinic?
International Journal of Language & Communication Disorders, 40(4), 493-504
Dodd, B. (2007). Evidence-based practice and speech-language pathology: Strengths,
weaknesses, opportunities and threats. Folia Phoniatrica et Logopaedica, 59, 118-
129.
Dodd, B., Crosbie, S., McIntosh, B., Holm, A., Harvey, C. Liddy, M., Fontyne, K., Pinchin,
B., & Rigby, H. (2008). The impact of selecting different contrasts in phonological
therapy. International Journal of Speech-Language Pathology, 10(5) 334-345.
Ebbels, S. (2007). Teaching grammar to school age children with specific language
impairment using Shape Coding SLI: A randomized control trial. Child Language
Teaching & Therapy, 23(1), 56-93.
Ebbels, S., & van der Lely, H.K.J. (2001). Meta-syntactic therapy using visual coding for
children with severe persistent SLI. International Journal of Language &
Communication Disorders, 36 Suppl:345-50.
Ebbels, S., van der Lely, H. K. J., & Dockrell, J. E. (2007). Intervention for verb argument
structure in children with persistent SLI: A randomized control trial. Journal of
Speech, Language and Hearing Research, 50(5), 1330-1349.
Felsenfeld, S., Broen, P.A., & McGue, M. (1992). A 28-year follow-up of adults with a
history of moderate phonological disorder: Linguistic and personality results. Journal
of Speech and Hearing Research, 35, 1114-1125.
Felsenfeld, S., Broen, P. A., & McGue, M. (1994). A 28-year follow-up of adults with a
history of moderate phonological disorder: Educational and occupational results.
Journal of Speech and Hearing Research, 37, 1341-1353.
Fey, M. E. (2006). Commentary on "Making Evidence-Based Decisions About Child
Language Intervention in Schools" by Gillam and Gillam. Language, Speech &
Hearing Services in Schools, 37(4), 316-319.
Forrest, K., & Elbert, M. (2001). Treatment for phonologically disordered children with
variable substitution patterns. Clinical Linguistics & Phonetics, 15(1), 41-45.
Gardner, H. (2006). Training others in the art of therapy for speech sound disorders: An
interactional approach Child Language Teaching and Therapy, 22 (1), 27-46.
Gillam, S. L., & Gillam, R. B. (2006). Making evidence-based decisions about child language
intervention in schools. Language, Speech & Hearing Services in Schools, 37(4), 304-
315.
Gillon, G., & Dodd, B. (1993). The phonological, syntactic and semantic skills of children
with specific reading disability. Australian Journal of Human Communication
Disorders, 21 (1), 86-102.
31
Gillon, G., & Dodd, B. (1995). The effects of training phonological, semantic and syntactic
processing skills in spoken language on reading ability. Language, Speech, and
Hearing Services in Schools, 26, 58-68.
Gillon, G., & Dodd, B. (1998). A developmental case study of a child with severe reading
disability: Response to specific intervention programmes. New Zealand Journal of
Speech-Language Therapy, 52, 9-21.
Gillon, G. T. (2004). Phonological awareness: From research to practice. New York:
Guilford Press.
Gillum, H., Camarata, S., Nelson, K. E., & Camarata, M. N. (2003). A comparison of
naturalistic and analog treatment effects in children with expressive language disorder
and poor preintervention imitation skills. Journal of Positive Behavior Interventions,
5(3), 171-178.
Hadley, P. A., Simmerman, A., Long, M., & Luna, M. (2000). Facilitating language
development for inner-city children: Experimental evaluation of a collaborative,
classroom-based intervention. Language, Speech, and Hearing Services in Schools,
31(2).
Harasty, J., & Reed, V. A. (1994). The prevalence of speech and language impairment in two
Sydney metropolitan schools: A summary and critical review. Australian Journal of
Human Communication Disorders, 22(1-23), 63-80.
Hay. I., Elias, G., F ielding-Barnsley, R., Homel, R., & Freiberg, K. (2007). Language delays,
reading delays, and learning difficulties: Interactive elements requiring
multidimensional programming. Journal of Learning Disabilities, 40(5), 400-409.
Jacoby, G. P., Lee, L., Kummer, A. W., Levin, L., & Creaghead, N. A. (2002). The number
of individual treatment units necessary to facilitate functional communication
improvements in the speech and language of young children. American Journal of
Speech-Language Pathology, 11(4), 370-380.
James, D. G. H. (1994). The efficacy of a language screening battery for Australian five-year-
old children. Australian Journal of Human Communication Disorders, 22(2), 31-46.
Jessup, B., Ward, E., Cahill, L., & Keating, D. (2008). Prevalence of speech and/or language
impairment in preparatory students in northern Tasmania. International Journal of
Speech-Language Pathology.10 (5) 364-377
Keilmann, A., Braun, L., & Napiontek, U. (2004). Emotional satisfaction of parents and
speech-language therapists with outcome of training intervention in children with
speech and language disorders. Folia Phoniatrica et Logopaedica, 56(1), 51-61.
Kent, R. D. (2006). Evidence-based practice in communication disorders: Progress not
perfection. Language, Speech & Hearing Services in Schools, 37(4), 268-270.
Kirk, C., & Gillon, G. T. (2007). Longitudinal effects of phonological awareness intervention
on morphological awareness in children with speech impairment. Language Speech
and Hearing Services in Schools, 38, 342-352.
Klein, E. S. (1996). Phonological/traditional approaches to articulation therapy: a
retrospective group comparison. Language, Speech, and Hearing Services in Schools,
27(4), 3140323.
Law, J., Garrett, Z., & Nye, C. (2003). Speech and language therapy interventions for
children with primary speech and language delay or disorder. Cochrane Database of
Systematic Reviews, Issue 3 Art. No.: CD004110. DOI: 004110.001002/14651858.
CD14004110.
Lewis, B. A. & Freebairn, L. (1992). Residual effects of preschool phonology disorders in
grade-school, adolescence and adulthood. Journal of Speech and Hearing Research,
35, 819-831.
32
Long, K., & Gillon, G. T. (2007). Enhancing early literacy acquisition in a child with speech
and language impairment: A case study. New Zealand Journal of Speech-Language
Therapy, 62(4-19).
Marler, J. A., Champlin, C. A., & Gillam, R. B. (2001). Backward and simultaneous masking
measured in children with language-learning impairments who received intervention
with Fast ForWord or Laureate Learning Systems software. American Journal of
Speech-Language Pathology, 10(3), 258-268
McKinnon, D., McLeod, S., & Reilly, S. (2007). The prevalence of stuttering, voice and
speech-sound disorders in primary school students in Australia. Language, Speech &
Hearing Services in Schools, 38(1), 5-15.
Moriarty, B. C., & Gillon, G. T. (2006). Phonological awareness intervention for children
with childhood apraxia of speech. International Journal of Language and
Communication Disorders, 41, 713-734.
Munro, N., & Atkinson, K. (2003). School-aged group therapy within community health
services. ACQuiring Knowledge in Speech, Language and Hearing, 5(2), 72-75.
Nation, K., Clarke, P., Marshall, C. M., & Durand, M. (2004). Hidden language impairment
in children: Parallels between poor reading comprehension and specific language
impairment. Journal of Speech, Language, and Hearing Research, 47, 199-211.
National Health and Medical Research Council. (2000). How to use the evidence: Assessment
and application of scientific evidence. Canberra: Commonwealth of Australia.
Nelson, K. E., Camarata, S. M., Welsh, J., Butkovsky, L., & Camarata, M. (1996). Effects of
imitative and conversational recasting treatment on the acquisition of grammar in
children with specific language impairment and younger language-normal children.
Journal of Speech & Hearing Research, 39(4), 850-859.
Pascoe, M., Stackhouse, J., & Wells, B. (2005). Phonological therapy within a
psycholinguistic framework: Promoting change in a child with persisting speech
difficulties. International Journal of Language & Communication Disorders, 40(2),
189-220.
Paul, R. (2007). Language disorders from infancy through adolescence. (3rd
ed.). St Louis,
Missouri: Mosby Elsevier.
Pawson, R., Greenhalgh, T., Harvey, G., & Walshe, K. (2005). Realist review-A new method
of systematic review designed for complex policy interventions. The Journal of
Health Service Research Policy, 10 (Supp 13), S1:21- 34.
Pokorni, J. L., Worthington, C. K., & Jamison, P. J. (2004). Phonological awareness
intervention: Comparison of Fast ForWord, Earobics, and LiPS. The Journal of
Educational Research, 97(3), 147-157.
Ray, J. (2002). Treating phonological disorders in a multilingual child: A case study.
American Journal of Speech-Language Pathology, 11(3), 305-315.
Richardson, K., & Klecan-Aker, J. S. (2000). Teaching pragmatics to language-learning
disabled children: a treatment outcome study. Child Language Teaching & Therapy,
16(1), 23-42.
Roulstone, S., Owen, R., & French, L. (2005). Speech and language therapy and the Knowles
Edge standards fund project: An evaluation of the service provided to a cluster of
primary schools. British Journal of Special Education, 32(2), 78-85.
Scientific Learning Corporation. (1998). Fast ForWord. Berkeley, CA: Scientific Learning
Corporation.
Segers, E., & Verhoeven, L. (2004). Computer-supported phonological awareness
intervention for kindergarten children with specific language impairment Language,
Speech & Hearing Services in the Schools, 35(3), 229-239.
33
Skarakis-Doyle, E. (2005). Reconceptualizing treatment goals from language impairment to
functional limitations: A case study. Topics in Language Disorders, 25(4), 353-363.
Smith, J., Downs, M., & Mogford-Bevan, K. (1998). Can phonological awareness training
facilitate minimal pair therapy? International Journal of Language & Communication
Disorders, 33(supplement), 463-468.
Snow, P. (2008a, May). Child abuse and neglect: Is speech-language pathology missing in
action? Paper presented at the Joint conference between New Zealand Speech-
Language Therapists Association and Speech Pathology Australia, Auckland, New
Zealand.
Snow, P. (2008b, May). Oral language competence in childhood and adolescence: The
missing link in mental health promotion? Paper presented at the Joint conference
between New Zealand Speech-Language Therapists Association and Speech
Pathology Australia, Auckland, New Zealand.
Snow, P. (2008c, May). Strengthening schools as mental health promotion settings: The role
of speech-language pathologist as language and literacy advocates. Paper presented
at the Joint conference between New Zealand Speech-Language Therapists
Association and Speech Pathology Australia, Auckland, New Zealand.
Snow, P. C., & Powell, M. B. (2004). Developmental language disorders and adolescent risk:
A public health advocacy role for speech pathologists? Advances in Speech-Language
Pathology, 6(4), 221-229.
Snowling, M. J., Adams, J. W., Bishop, D. V. M., & Stothard, S. E. (2001). Educational
attainment of school leavers with a preschool history of speech-language
impairments. International Journal of Language and Communication Disorders, 36,
173-183.
Stackhouse, J., & Wells, B. (1997). Children's speech and literacy difficulties. London:
Whurr.
Stackhouse, J., & Wells, B. (Eds.). (2001). Children's speech and literacy difficulties 2:
Identification and intervention. London: Whurr.
Stiegler, L. N., & Hoffman, P. R. (2001). Discourse-based intervention for word finding in
children. Journal of Communication Disorders, 34, 277-303.
Stothard, S. E., Snowling, M. J., Bishop, D. V. M., Chipchase, B. B., & Kaplan, C. A. (1998).
Language impaired preschoolers: A follow-up into adolescence. Journal of Speech,
Language and Hearing Research, 41, 407-418.
Strand, E. A., Stoeckel, R., & Baas, B. (2006). Treatment of severe childhood apraxia of
speech: a treatment efficacy study. Journal of Medical Speech-Language Pathology,
14(4), 297-307.
Swanson, L. A., Fey, M. E., Mills, C. E., & Hood, L. S. (2005). Use of narrative-based
language intervention with children who have specific language impairment.
American Journal of Speech - Language Pathology, 14(2), 131-143.
Ward, S. (1999). An Investigation into the Effectiveness of an Early Intervention Method for
Delayed Language Development in Young Children. International Journal of
Language & Communication Disorders, 34(3), 243-264.
Williams, A. L. (2000). Multiple oppositions: Case studies of variables in phonological
intervention. American Journal of Speech-Language Pathology, 9(4), 289-299.
World Health Organization. (2001). International classification of functioning, disability and
health. Geneva: WHO.
Wren, Y., & Roulstone, S. (2008). A comparison between computer and tabletop delivery of
phonology therapy. International Journal of Speech-Language Pathology,10(5) 346-
363.

34
Wren, Y., Roulstone, S., Parkhouse, J., & Hall, B. (2001). A model for a mainstream school-
based speech and language therapy service. Child Language Teaching & Therapy,
17(2), 107-126.
35
ACKNOWLEDGEMENTS
The Department of Education and Children‟s Services and Department of Health, SA for
funding this project.
Cathy Olsson, Jenny Moody, Ellie Chronis, Linda Nimmo, Craig Mattiske and other
members of the Statewide Interagency Speech Pathology Reference Group, SA for their
guidance.
Stephanie Grant, Libby McMahon and Lynn Williams for their preparedness to answer
questions about their organisations and work.
Saravana Kumar, Cathy Olsson and the Reference Groupd for their helpful comments on
earlier drafts.
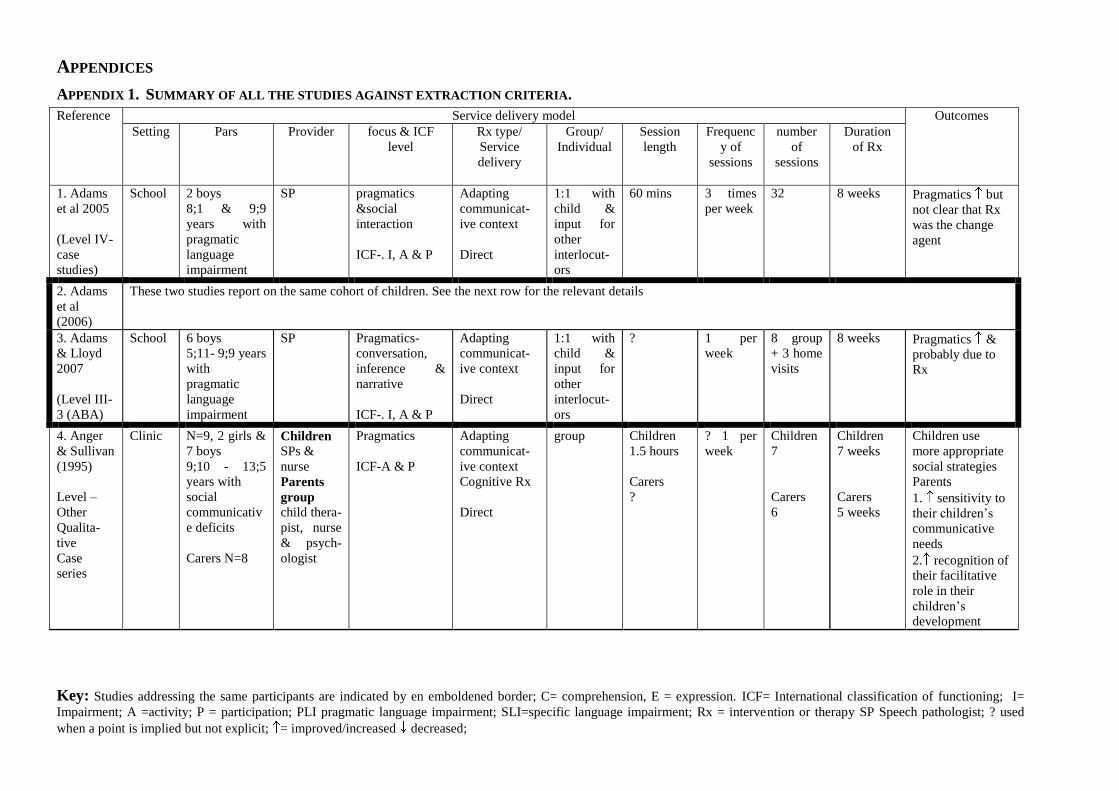
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
APPENDICES
APPENDIX 1. SUMMARY OF ALL THE STUDIES AGAINST EXTRACTION CRITERIA.
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
1. Adams
et al 2005
(Level IV-
case
studies)
School 2 boys
8;1 & 9;9
years with
pragmatic
language
impairment
SP pragmatics
&social
interaction
ICF-. I, A & P
Adapting
communicat-
ive context
Direct
1:1 with
child &
input for
other
interlocut-
ors
60 mins 3 times
per week
32 8 weeks Pragmatics but
not clear that Rx
was the change
agent
2. Adams
et al
(2006)
These two studies report on the same cohort of children. See the next row for the relevant details
3. Adams
& Lloyd
2007
(Level III-
3 (ABA)
School 6 boys
5;11- 9;9 years
with
pragmatic
language
impairment
SP Pragmatics-
conversation,
inference &
narrative
ICF-. I, A & P
Adapting
communicat-
ive context
Direct
1:1 with
child &
input for
other
interlocut-
ors
? 1 per
week
8 group
+ 3 home
visits
8 weeks Pragmatics &
probably due to
Rx
4. Anger
& Sullivan
(1995)
Level –
Other
Qualita-
tive
Case
series
Clinic N=9, 2 girls &
7 boys
9;10 - 13;5
years with
social
communicativ
e deficits
Carers N=8
Children
SPs &
nurse
Parents
group
child thera-
pist, nurse
& psych-
ologist
Pragmatics
ICF-A & P
Adapting
communicat-
ive context
Cognitive Rx
Direct
group Children
1.5 hours
Carers
?
? 1 per
week
Children
7
Carers
6
Children
7 weeks
Carers
5 weeks
Children use
more appropriate
social strategies
Parents
1. sensitivity to
their children‟s
communicative
needs
2. recognition of
their facilitative
role in their
children‟s
development
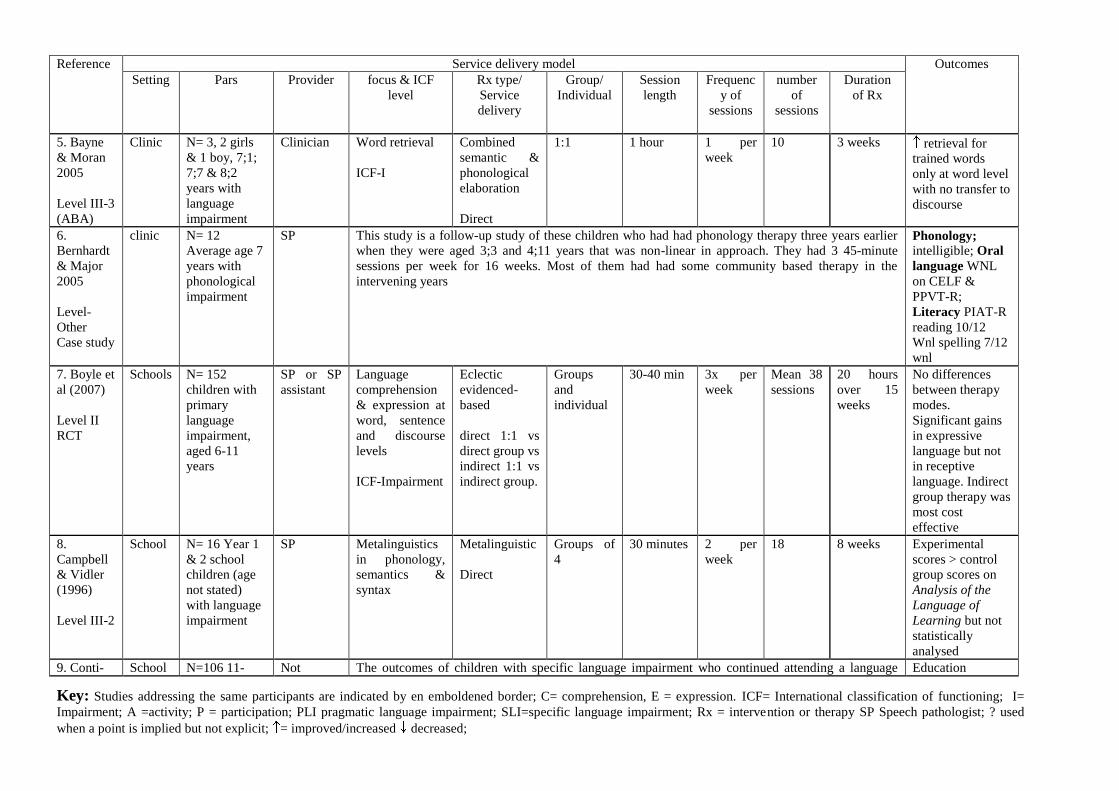
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
5. Bayne
& Moran
2005
Level III-3
(ABA)
Clinic N= 3, 2 girls
& 1 boy, 7;1;
7;7 & 8;2
years with
language
impairment
Clinician Word retrieval
ICF-I
Combined
semantic &
phonological
elaboration
Direct
1:1 1 hour 1 per
week
10 3 weeks retrieval for
trained words
only at word level
with no transfer to
discourse
6.
Bernhardt
& Major
2005
Level-
Other
Case study
clinic N= 12
Average age 7
years with
phonological
impairment
SP This study is a follow-up study of these children who had had phonology therapy three years earlier
when they were aged 3;3 and 4;11 years that was non-linear in approach. They had 3 45-minute
sessions per week for 16 weeks. Most of them had had some community based therapy in the
intervening years
Phonology; intelligible; Oral
language WNL
on CELF &
PPVT-R;
Literacy PIAT-R
reading 10/12
Wnl spelling 7/12
wnl
7. Boyle et
al (2007)
Level II
RCT
Schools N= 152
children with
primary
language
impairment,
aged 6-11
years
SP or SP
assistant
Language
comprehension
& expression at
word, sentence
and discourse
levels
ICF-Impairment
Eclectic
evidenced-
based
direct 1:1 vs
direct group vs
indirect 1:1 vs
indirect group.
Groups
and
individual
30-40 min 3x per
week
Mean 38
sessions
20 hours
over 15
weeks
No differences
between therapy
modes.
Significant gains
in expressive
language but not
in receptive
language. Indirect
group therapy was
most cost
effective
8.
Campbell
& Vidler
(1996)
Level III-2
School N= 16 Year 1
& 2 school
children (age
not stated)
with language
impairment
SP Metalinguistics
in phonology,
semantics &
syntax
Metalinguistic
Direct
Groups of
4
30 minutes 2 per
week
18 8 weeks Experimental
scores > control
group scores on
Analysis of the
Language of
Learning but not
statistically
analysed
9. Conti- School N=106 11- Not The outcomes of children with specific language impairment who continued attending a language Education
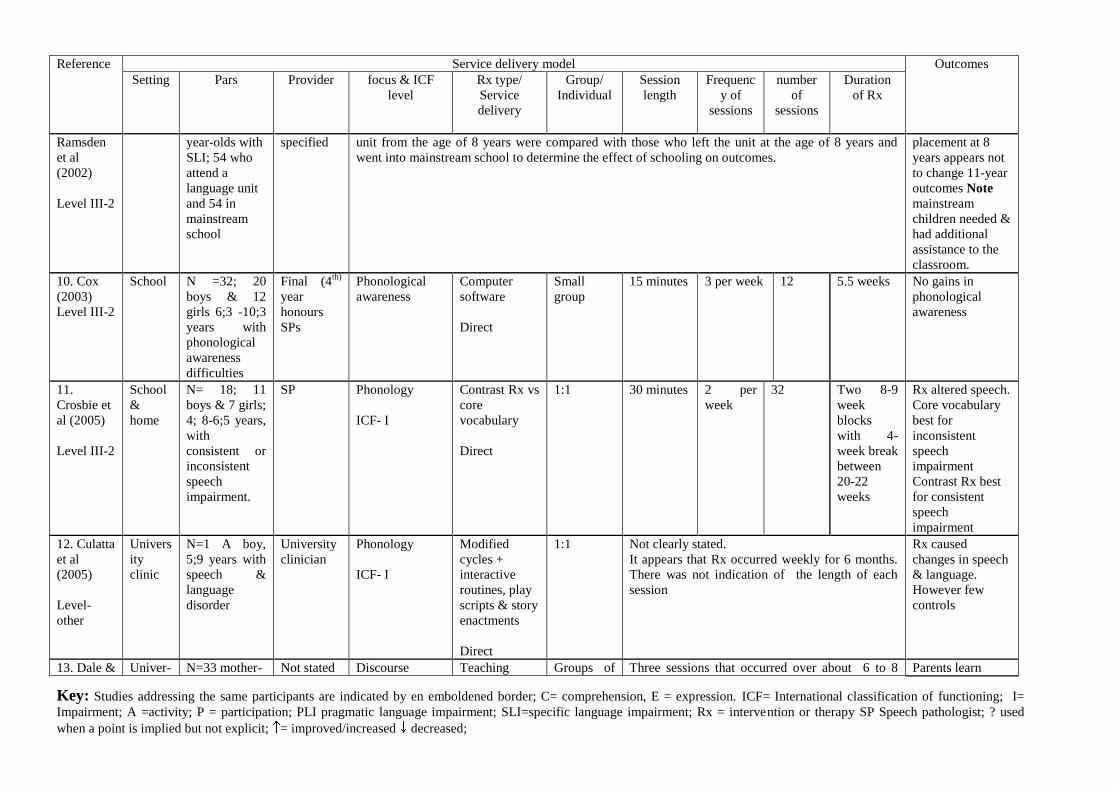
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
Ramsden
et al
(2002)
Level III-2
year-olds with
SLI; 54 who
attend a
language unit
and 54 in
mainstream
school
specified unit from the age of 8 years were compared with those who left the unit at the age of 8 years and
went into mainstream school to determine the effect of schooling on outcomes.
placement at 8
years appears not
to change 11-year
outcomes Note
mainstream
children needed &
had additional
assistance to the
classroom.
10. Cox
(2003)
Level III-2
School N =32; 20
boys & 12
girls 6;3 -10;3
years with
phonological
awareness
difficulties
Final (4th)
year
honours
SPs
Phonological
awareness
Computer
software
Direct
Small
group
15 minutes 3 per week 12 5.5 weeks No gains in
phonological
awareness
11.
Crosbie et
al (2005)
Level III-2
School
&
home
N= 18; 11
boys & 7 girls;
4; 8-6;5 years,
with
consistent or
inconsistent
speech
impairment.
SP Phonology
ICF- I
Contrast Rx vs
core
vocabulary
Direct
1:1 30 minutes 2 per
week
32 Two 8-9
week
blocks
with 4-
week break
between
20-22
weeks
Rx altered speech.
Core vocabulary
best for
inconsistent
speech
impairment
Contrast Rx best
for consistent
speech
impairment
12. Culatta
et al
(2005)
Level-
other
Univers
ity
clinic
N=1 A boy,
5;9 years with
speech &
language
disorder
University
clinician
Phonology
ICF- I
Modified
cycles +
interactive
routines, play
scripts & story
enactments
Direct
1:1 Not clearly stated.
It appears that Rx occurred weekly for 6 months.
There was not indication of the length of each
session
Rx caused
changes in speech
& language.
However few
controls
13. Dale & Univer- N=33 mother- Not stated Discourse Teaching Groups of Three sessions that occurred over about 6 to 8 Parents learn
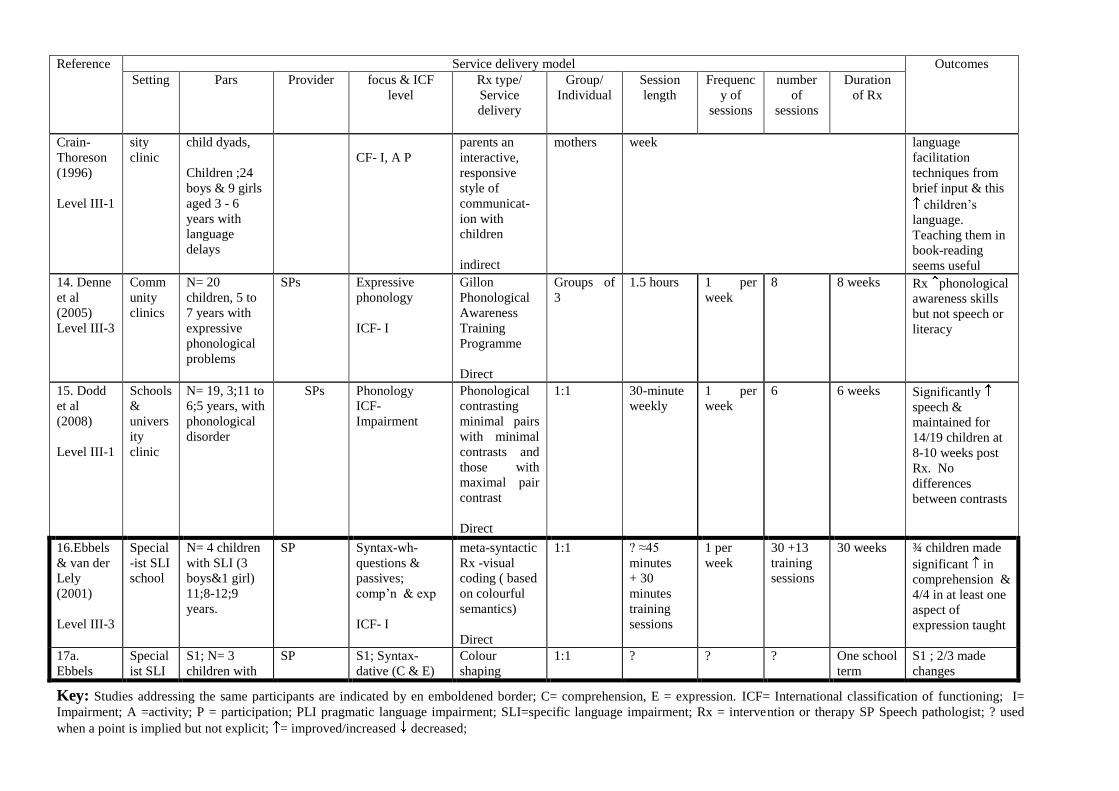
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
Crain-
Thoreson
(1996)
Level III-1
sity
clinic
child dyads,
Children ;24
boys & 9 girls
aged 3 - 6
years with
language
delays
CF- I, A P
parents an
interactive,
responsive
style of
communicat-
ion with
children
indirect
mothers week language
facilitation
techniques from
brief input & this
children‟s
language.
Teaching them in
book-reading
seems useful
14. Denne
et al
(2005)
Level III-3
Comm
unity
clinics
N= 20
children, 5 to
7 years with
expressive
phonological
problems
SPs Expressive
phonology
ICF- I
Gillon
Phonological
Awareness
Training
Programme
Direct
Groups of
3
1.5 hours 1 per
week
8 8 weeks Rx phonological
awareness skills
but not speech or
literacy
15. Dodd
et al
(2008)
Level III-1
Schools
&
univers
ity
clinic
N= 19, 3;11 to
6;5 years, with
phonological
disorder
SPs Phonology
ICF-
Impairment
Phonological
contrasting
minimal pairs
with minimal
contrasts and
those with
maximal pair
contrast
Direct
1:1 30-minute
weekly
1 per
week
6 6 weeks Significantly
speech &
maintained for
14/19 children at
8-10 weeks post
Rx. No
differences
between contrasts
16.Ebbels
& van der
Lely
(2001)
Level III-3
Special
-ist SLI
school
N= 4 children
with SLI (3
boys&1 girl)
11;8-12;9
years.
SP Syntax-wh-
questions &
passives;
comp‟n & exp
ICF- I
meta-syntactic
Rx -visual
coding ( based
on colourful
semantics)
Direct
1:1 ? ≈45
minutes
+ 30
minutes
training
sessions
1 per
week
30 +13
training
sessions
30 weeks ¾ children made
significant in
comprehension &
4/4 in at least one
aspect of
expression taught
17a.
Ebbels
Special
ist SLI
S1; N= 3
children with
SP S1; Syntax-
dative (C & E)
Colour
shaping
1:1 ? ? ? One school
term
S1 ; 2/3 made
changes
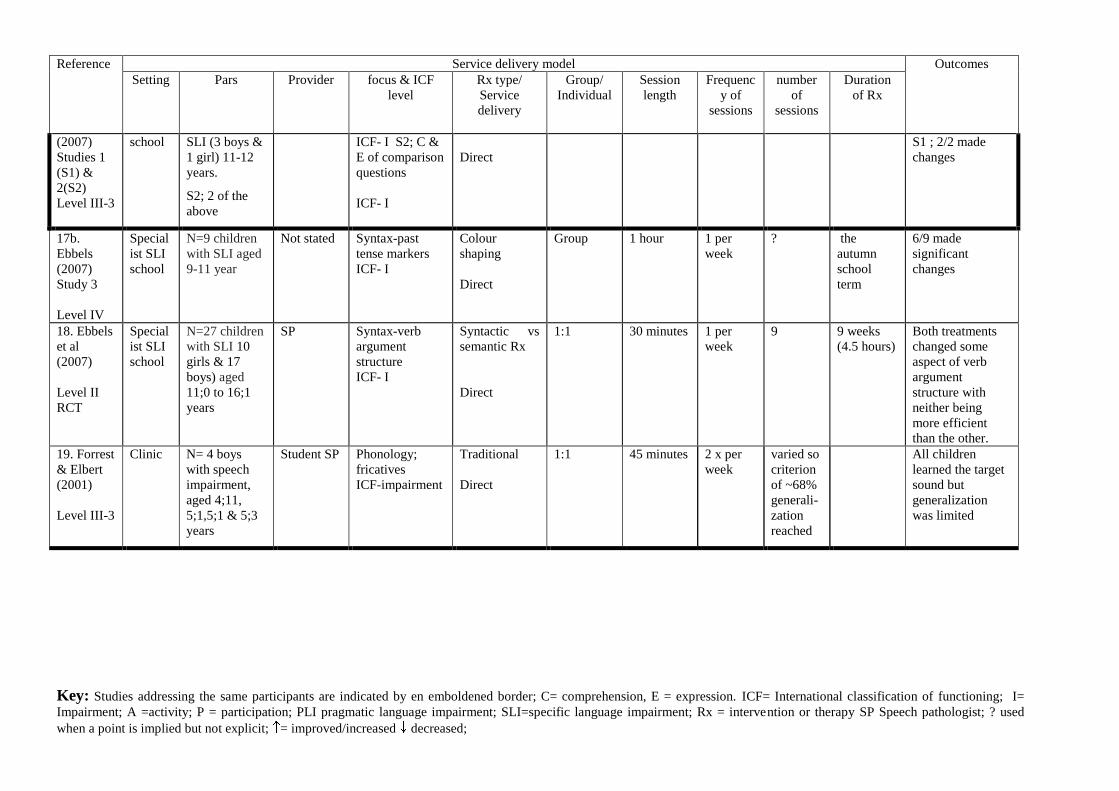
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
(2007)
Studies 1
(S1) &
2(S2)
Level III-3
school SLI (3 boys &
1 girl) 11-12
years.
S2; 2 of the
above
ICF- I S2; C &
E of comparison
questions
ICF- I
Direct
S1 ; 2/2 made
changes
17b.
Ebbels
(2007)
Study 3
Level IV
Special
ist SLI
school
N=9 children
with SLI aged
9-11 year
Not stated Syntax-past
tense markers
ICF- I
Colour
shaping
Direct
Group 1 hour 1 per
week
? the
autumn
school
term
6/9 made
significant
changes
18. Ebbels
et al
(2007)
Level II
RCT
Special
ist SLI
school
N=27 children
with SLI 10
girls & 17
boys) aged
11;0 to 16;1
years
SP Syntax-verb
argument
structure
ICF- I
Syntactic vs
semantic Rx
Direct
1:1 30 minutes 1 per
week
9 9 weeks
(4.5 hours)
Both treatments
changed some
aspect of verb
argument
structure with
neither being
more efficient
than the other.
19. Forrest
& Elbert
(2001)
Level III-3
Clinic N= 4 boys
with speech
impairment,
aged 4;11,
5;1,5;1 & 5;3
years
Student SP Phonology;
fricatives
ICF-impairment
Traditional
Direct
1:1 45 minutes 2 x per
week
varied so
criterion
of ~68%
generali-
zation
reached
All children
learned the target
sound but
generalization
was limited
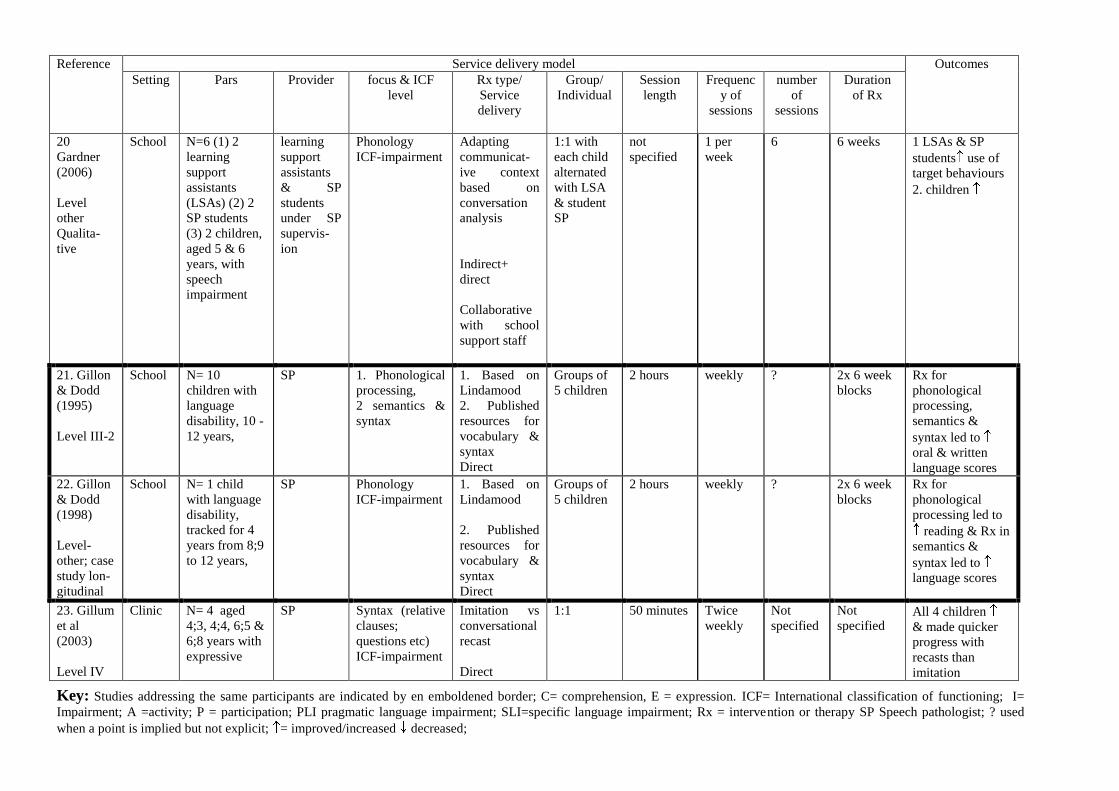
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
20
Gardner
(2006)
Level
other
Qualita-
tive
School N=6 (1) 2
learning
support
assistants
(LSAs) (2) 2
SP students
(3) 2 children,
aged 5 & 6
years, with
speech
impairment
learning
support
assistants
& SP
students
under SP
supervis-
ion
Phonology
ICF-impairment
Adapting
communicat-
ive context
based on
conversation
analysis
Indirect+
direct
Collaborative
with school
support staff
1:1 with
each child
alternated
with LSA
& student
SP
not
specified
1 per
week
6 6 weeks 1 LSAs & SP
students use of
target behaviours
2. children
21. Gillon
& Dodd
(1995)
Level III-2
School N= 10
children with
language
disability, 10 -
12 years,
SP 1. Phonological
processing,
2 semantics &
syntax
1. Based on
Lindamood
2. Published
resources for
vocabulary &
syntax
Direct
Groups of
5 children
2 hours weekly ? 2x 6 week
blocks
Rx for
phonological
processing,
semantics &
syntax led to
oral & written
language scores
22. Gillon
& Dodd
(1998)
Level-
other; case
study lon-
gitudinal
School N= 1 child
with language
disability,
tracked for 4
years from 8;9
to 12 years,
SP Phonology
ICF-impairment
1. Based on
Lindamood
2. Published
resources for
vocabulary &
syntax
Direct
Groups of
5 children
2 hours weekly ? 2x 6 week
blocks
Rx for
phonological
processing led to
reading & Rx in
semantics &
syntax led to
language scores
23. Gillum
et al
(2003)
Level IV
Clinic N= 4 aged
4;3, 4;4, 6;5 &
6;8 years with
expressive
SP Syntax (relative
clauses;
questions etc)
ICF-impairment
Imitation vs
conversational
recast
Direct
1:1 50 minutes Twice
weekly
Not
specified
Not
specified All 4 children
& made quicker
progress with
recasts than
imitation
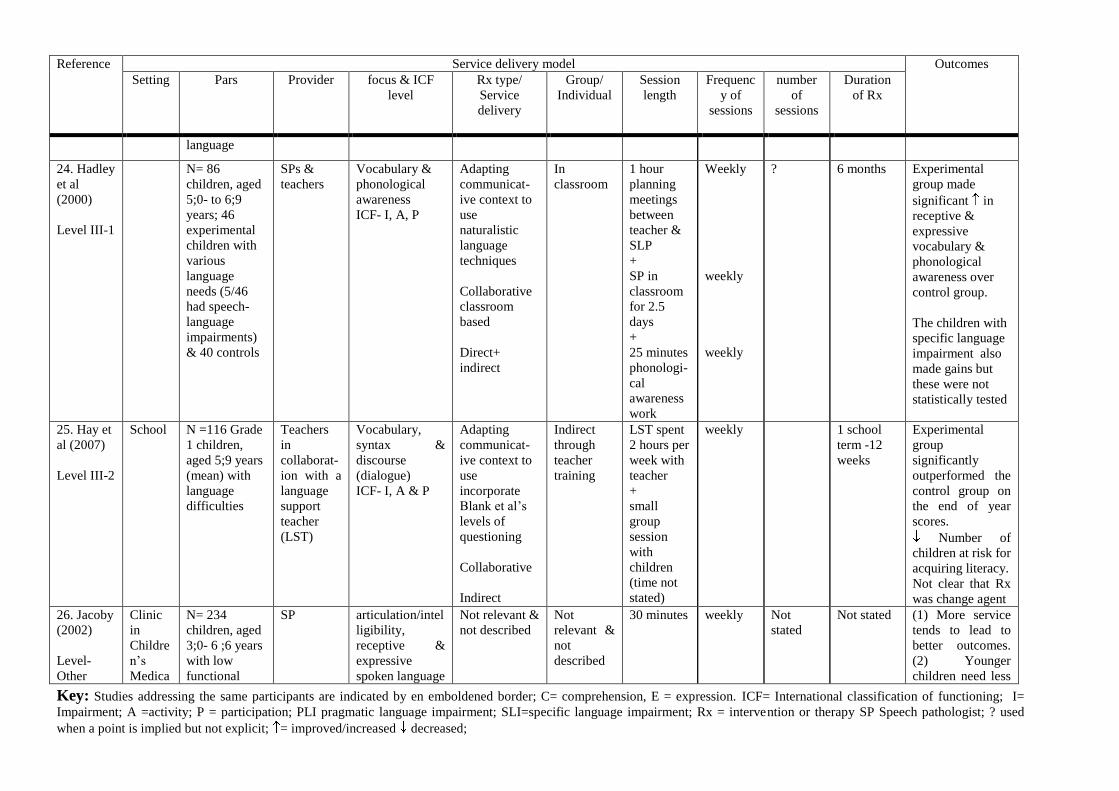
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
language
24. Hadley
et al
(2000)
Level III-1
N= 86
children, aged
5;0- to 6;9
years; 46
experimental
children with
various
language
needs (5/46
had speech-
language
impairments)
& 40 controls
SPs &
teachers
Vocabulary &
phonological
awareness
ICF- I, A, P
Adapting
communicat-
ive context to
use
naturalistic
language
techniques
Collaborative
classroom
based
Direct+
indirect
In
classroom
1 hour
planning
meetings
between
teacher &
SLP
+
SP in
classroom
for 2.5
days
+
25 minutes
phonologi-
cal
awareness
work
Weekly
weekly
weekly
? 6 months Experimental
group made
significant in
receptive &
expressive
vocabulary &
phonological
awareness over
control group.
The children with
specific language
impairment also
made gains but
these were not
statistically tested
25. Hay et
al (2007)
Level III-2
School N =116 Grade
1 children,
aged 5;9 years
(mean) with
language
difficulties
Teachers
in
collaborat-
ion with a
language
support
teacher
(LST)
Vocabulary,
syntax &
discourse
(dialogue)
ICF- I, A & P
Adapting
communicat-
ive context to
use
incorporate
Blank et al‟s
levels of
questioning
Collaborative
Indirect
Indirect
through
teacher
training
LST spent
2 hours per
week with
teacher
+
small
group
session
with
children
(time not
stated)
weekly 1 school
term -12
weeks
Experimental
group
significantly
outperformed the
control group on
the end of year
scores.
Number of
children at risk for
acquiring literacy.
Not clear that Rx
was change agent
26. Jacoby
(2002)
Level-
Other
Clinic
in
Childre
n‟s
Medica
N= 234
children, aged
3;0- 6 ;6 years
with low
functional
SP articulation/intel
ligibility,
receptive &
expressive
spoken language
Not relevant &
not described
Not
relevant &
not
described
30 minutes weekly Not
stated
Not stated (1) More service
tends to lead to
better outcomes.
(2) Younger
children need less
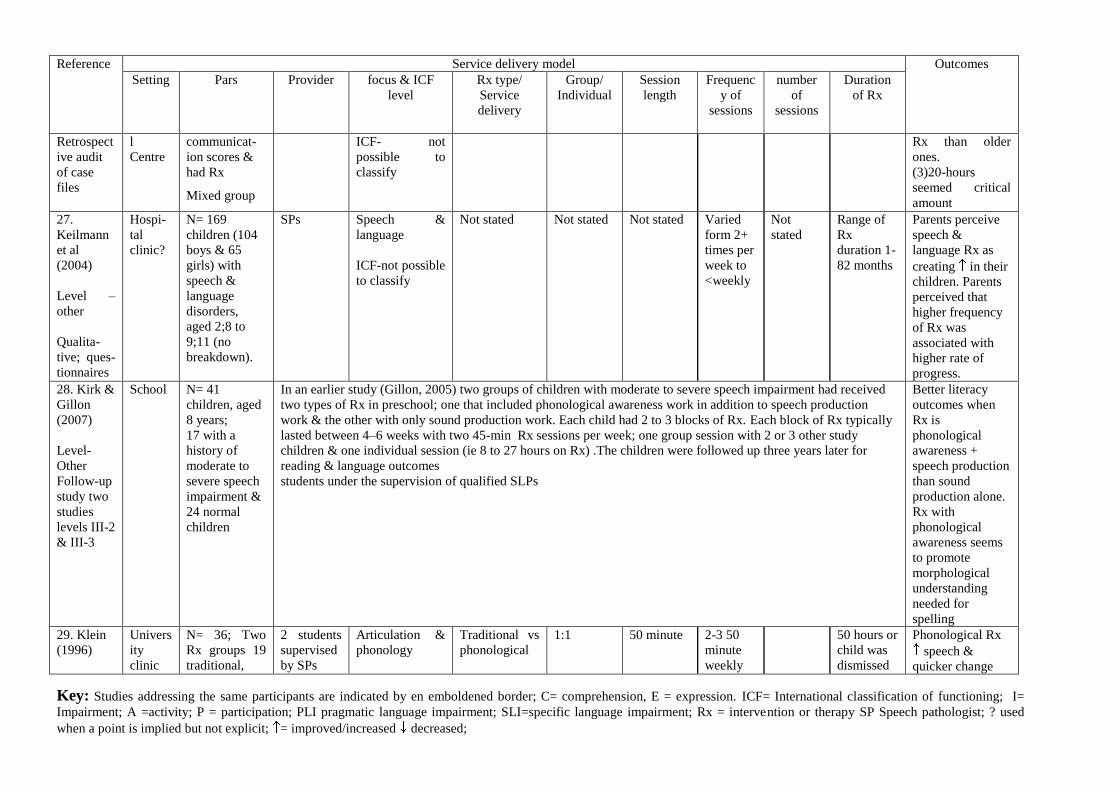
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
Retrospect
ive audit
of case
files
l
Centre
communicat-
ion scores &
had Rx
Mixed group
ICF- not
possible to
classify
Rx than older
ones.
(3)20-hours
seemed critical
amount
27.
Keilmann
et al
(2004)
Level –
other
Qualita-
tive; ques-
tionnaires
Hospi-
tal
clinic?
N= 169
children (104
boys & 65
girls) with
speech &
language
disorders,
aged 2;8 to
9;11 (no
breakdown).
SPs Speech &
language
ICF-not possible
to classify
Not stated Not stated Not stated Varied
form 2+
times per
week to
<weekly
Not
stated
Range of
Rx
duration 1-
82 months
Parents perceive
speech &
language Rx as
creating in their
children. Parents
perceived that
higher frequency
of Rx was
associated with
higher rate of
progress.
28. Kirk &
Gillon
(2007)
Level-
Other
Follow-up
study two
studies
levels III-2
& III-3
School N= 41
children, aged
8 years;
17 with a
history of
moderate to
severe speech
impairment &
24 normal
children
In an earlier study (Gillon, 2005) two groups of children with moderate to severe speech impairment had received
two types of Rx in preschool; one that included phonological awareness work in addition to speech production
work & the other with only sound production work. Each child had 2 to 3 blocks of Rx. Each block of Rx typically
lasted between 4–6 weeks with two 45-min Rx sessions per week; one group session with 2 or 3 other study
children & one individual session (ie 8 to 27 hours on Rx) .The children were followed up three years later for
reading & language outcomes
students under the supervision of qualified SLPs
Better literacy
outcomes when
Rx is
phonological
awareness +
speech production
than sound
production alone.
Rx with
phonological
awareness seems
to promote
morphological
understanding
needed for
spelling
29. Klein
(1996)
Univers
ity
clinic
N= 36; Two
Rx groups 19
traditional,
2 students
supervised
by SPs
Articulation &
phonology
Traditional vs
phonological
1:1 50 minute 2-3 50
minute
weekly
50 hours or
child was
dismissed
Phonological Rx
speech &
quicker change
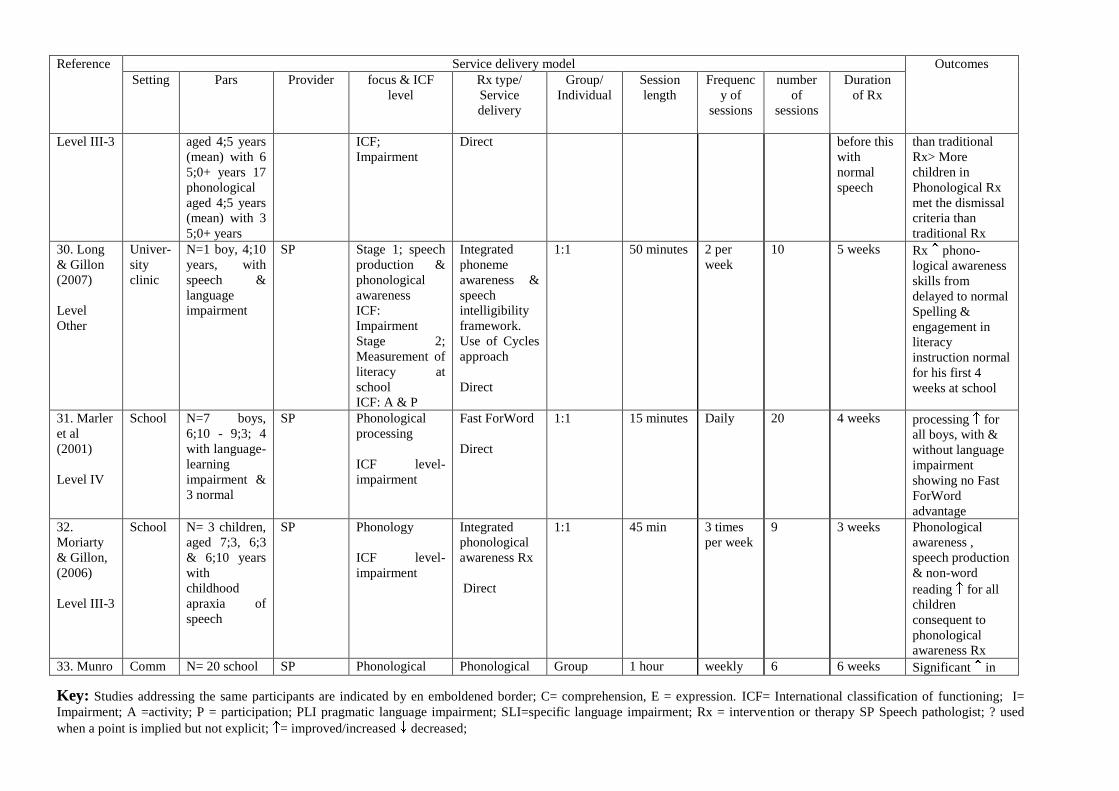
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
Level III-3 aged 4;5 years
(mean) with 6
5;0+ years 17
phonological
aged 4;5 years
(mean) with 3
5;0+ years
ICF;
Impairment
Direct before this
with
normal
speech
than traditional
Rx> More
children in
Phonological Rx
met the dismissal
criteria than
traditional Rx
30. Long
& Gillon
(2007)
Level
Other
Univer-
sity
clinic
N=1 boy, 4;10
years, with
speech &
language
impairment
SP Stage 1; speech
production &
phonological
awareness
ICF:
Impairment
Stage 2;
Measurement of
literacy at
school
ICF: A & P
Integrated
phoneme
awareness &
speech
intelligibility
framework.
Use of Cycles
approach
Direct
1:1 50 minutes 2 per
week
10 5 weeks Rx phono-
logical awareness
skills from
delayed to normal
Spelling &
engagement in
literacy
instruction normal
for his first 4
weeks at school
31. Marler
et al
(2001)
Level IV
School N=7 boys,
6;10 - 9;3; 4
with language-
learning
impairment &
3 normal
SP Phonological
processing
ICF level-
impairment
Fast ForWord
Direct
1:1 15 minutes Daily 20 4 weeks processing for
all boys, with &
without language
impairment
showing no Fast
ForWord
advantage
32.
Moriarty
& Gillon,
(2006)
Level III-3
School N= 3 children,
aged 7;3, 6;3
& 6;10 years
with
childhood
apraxia of
speech
SP Phonology
ICF level-
impairment
Integrated
phonological
awareness Rx
Direct
1:1 45 min 3 times
per week
9 3 weeks Phonological
awareness ,
speech production
& non-word
reading for all
children
consequent to
phonological
awareness Rx
33. Munro Comm N= 20 school SP Phonological Phonological Group 1 hour weekly 6 6 weeks Significant in
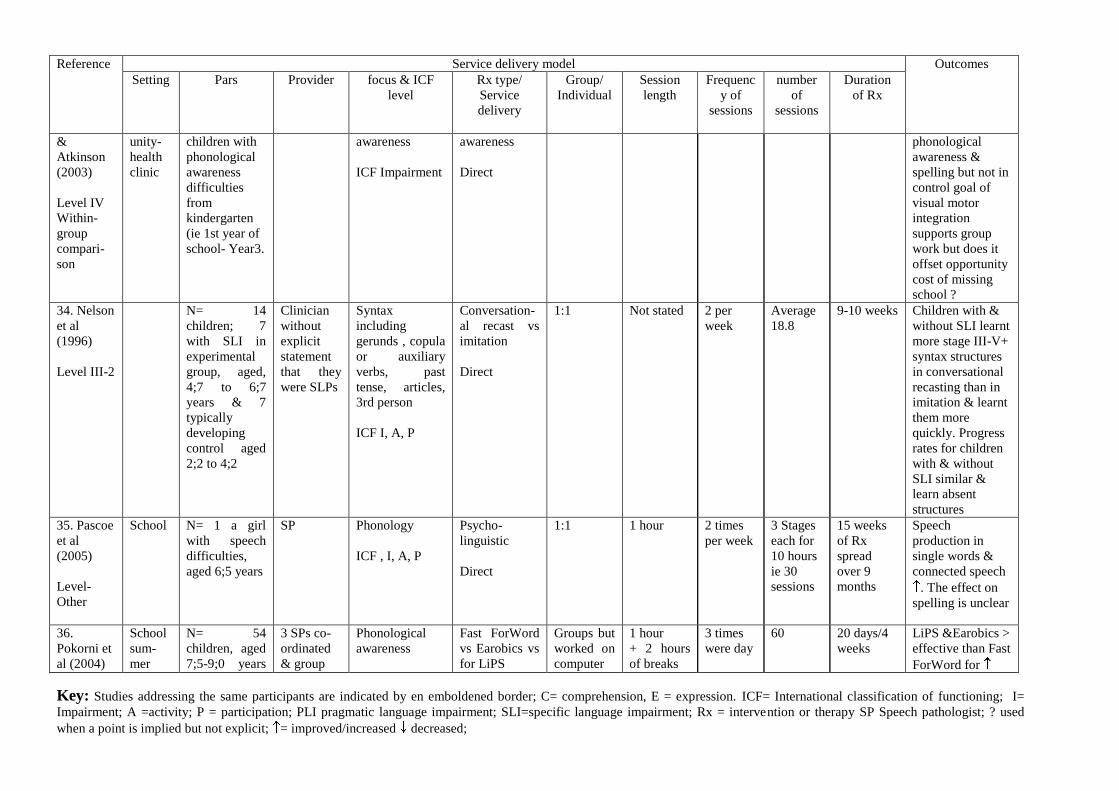
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
&
Atkinson
(2003)
Level IV
Within-
group
compari-
son
unity-
health
clinic
children with
phonological
awareness
difficulties
from
kindergarten
(ie 1st year of
school- Year3.
awareness
ICF Impairment
awareness
Direct
phonological
awareness &
spelling but not in
control goal of
visual motor
integration
supports group
work but does it
offset opportunity
cost of missing
school ?
34. Nelson
et al
(1996)
Level III-2
N= 14
children; 7
with SLI in
experimental
group, aged,
4;7 to 6;7
years & 7
typically
developing
control aged
2;2 to 4;2
Clinician
without
explicit
statement
that they
were SLPs
Syntax
including
gerunds , copula
or auxiliary
verbs, past
tense, articles,
3rd person
ICF I, A, P
Conversation-
al recast vs
imitation
Direct
1:1 Not stated 2 per
week
Average
18.8
9-10 weeks Children with &
without SLI learnt
more stage III-V+
syntax structures
in conversational
recasting than in
imitation & learnt
them more
quickly. Progress
rates for children
with & without
SLI similar &
learn absent
structures
35. Pascoe
et al
(2005)
Level-
Other
School N= 1 a girl
with speech
difficulties,
aged 6;5 years
SP Phonology
ICF , I, A, P
Psycho-
linguistic
Direct
1:1 1 hour 2 times
per week
3 Stages
each for
10 hours
ie 30
sessions
15 weeks
of Rx
spread
over 9
months
Speech
production in
single words &
connected speech
. The effect on
spelling is unclear
36.
Pokorni et
al (2004)
School
sum-
mer
N= 54
children, aged
7;5-9;0 years
3 SPs co-
ordinated
& group
Phonological
awareness
Fast ForWord
vs Earobics vs
for LiPS
Groups but
worked on
computer
1 hour
+ 2 hours
of breaks
3 times
were day
60 20 days/4
weeks
LiPS &Earobics >
effective than Fast
ForWord for
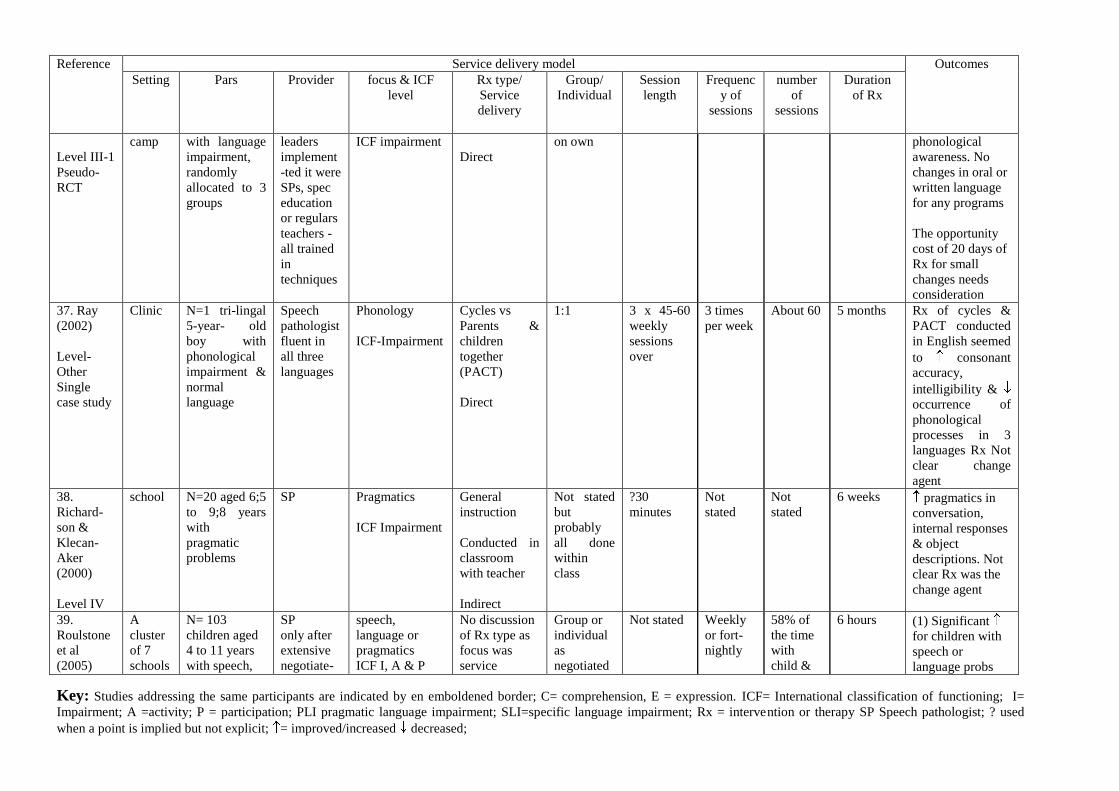
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
Level III-1
Pseudo-
RCT
camp with language
impairment,
randomly
allocated to 3
groups
leaders
implement
-ted it were
SPs, spec
education
or regulars
teachers -
all trained
in
techniques
ICF impairment
Direct
on own phonological
awareness. No
changes in oral or
written language
for any programs
The opportunity
cost of 20 days of
Rx for small
changes needs
consideration
37. Ray
(2002)
Level-
Other
Single
case study
Clinic N=1 tri-lingal
5-year- old
boy with
phonological
impairment &
normal
language
Speech
pathologist
fluent in
all three
languages
Phonology
ICF-Impairment
Cycles vs
Parents &
children
together
(PACT)
Direct
1:1 3 x 45-60
weekly
sessions
over
3 times
per week
About 60 5 months Rx of cycles &
PACT conducted
in English seemed
to consonant
accuracy,
intelligibility &
occurrence of
phonological
processes in 3
languages Rx Not
clear change
agent
38.
Richard-
son &
Klecan-
Aker
(2000)
Level IV
school N=20 aged 6;5
to 9;8 years
with
pragmatic
problems
SP Pragmatics
ICF Impairment
General
instruction
Conducted in
classroom
with teacher
Indirect
Not stated
but
probably
all done
within
class
?30
minutes
Not
stated
Not
stated
6 weeks pragmatics in
conversation,
internal responses
& object
descriptions. Not
clear Rx was the
change agent
39.
Roulstone
et al
(2005)
A
cluster
of 7
schools
N= 103
children aged
4 to 11 years
with speech,
SP
only after
extensive
negotiate-
speech,
language or
pragmatics
ICF I, A & P
No discussion
of Rx type as
focus was
service
Group or
individual
as
negotiated
Not stated Weekly
or fort-
nightly
58% of
the time
with
child &
6 hours (1) Significant
for children with
speech or
language probs
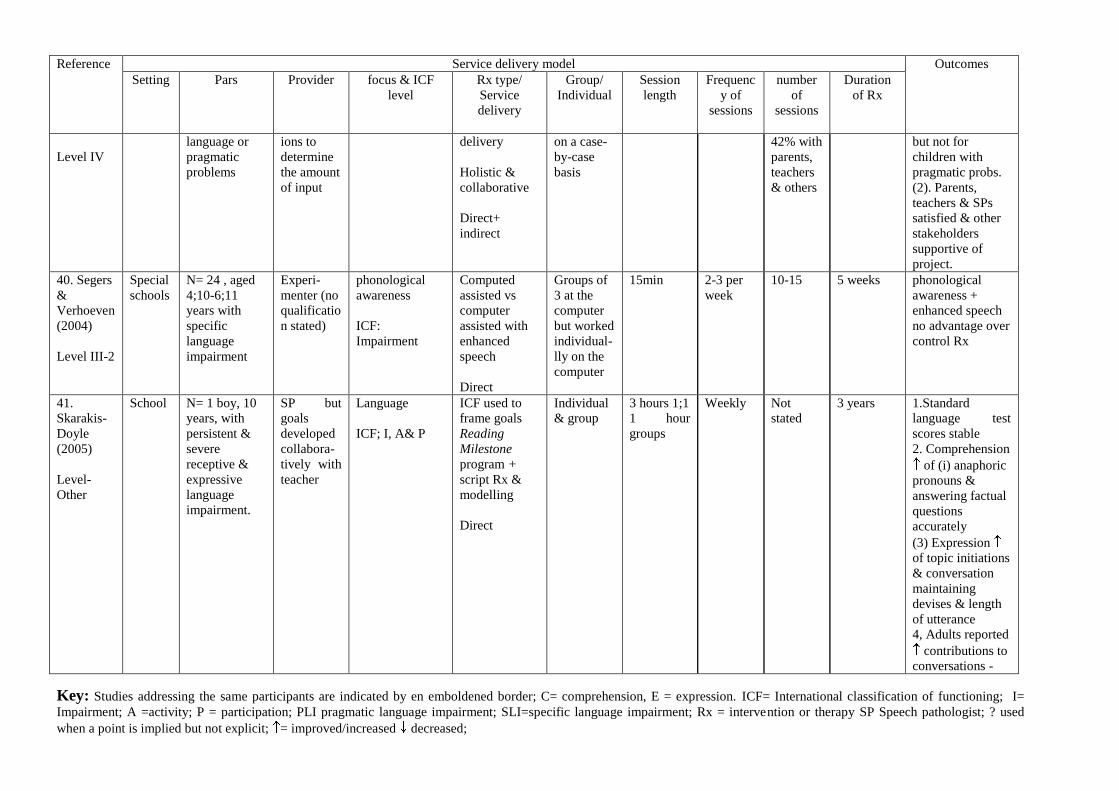
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
Level IV
language or
pragmatic
problems
ions to
determine
the amount
of input
delivery
Holistic &
collaborative
Direct+
indirect
on a case-
by-case
basis
42% with
parents,
teachers
& others
but not for
children with
pragmatic probs.
(2). Parents,
teachers & SPs
satisfied & other
stakeholders
supportive of
project.
40. Segers
&
Verhoeven
(2004)
Level III-2
Special
schools
N= 24 , aged
4;10-6;11
years with
specific
language
impairment
Experi-
menter (no
qualificatio
n stated)
phonological
awareness
ICF:
Impairment
Computed
assisted vs
computer
assisted with
enhanced
speech
Direct
Groups of
3 at the
computer
but worked
individual-
lly on the
computer
15min 2-3 per
week
10-15 5 weeks phonological
awareness +
enhanced speech
no advantage over
control Rx
41.
Skarakis-
Doyle
(2005)
Level-
Other
School N= 1 boy, 10
years, with
persistent &
severe
receptive &
expressive
language
impairment.
SP but
goals
developed
collabora-
tively with
teacher
Language
ICF; I, A& P
ICF used to
frame goals
Reading
Milestone
program +
script Rx &
modelling
Direct
Individual
& group
3 hours 1;1
1 hour
groups
Weekly Not
stated
3 years 1.Standard
language test
scores stable
2. Comprehension
of (i) anaphoric
pronouns &
answering factual
questions
accurately
(3) Expression
of topic initiations
& conversation
maintaining
devises & length
of utterance
4, Adults reported
contributions to
conversations -
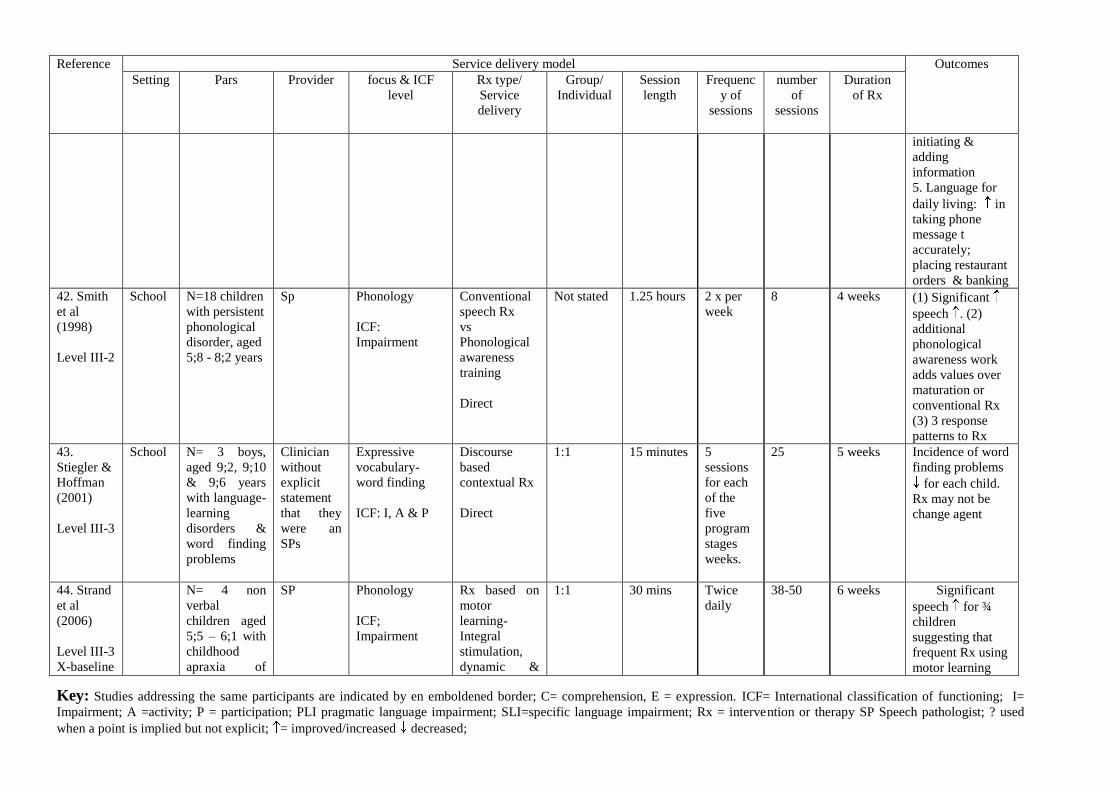
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
initiating &
adding
information
5. Language for
daily living: in
taking phone
message t
accurately;
placing restaurant
orders & banking
42. Smith
et al
(1998)
Level III-2
School N=18 children
with persistent
phonological
disorder, aged
5;8 - 8;2 years
Sp Phonology
ICF:
Impairment
Conventional
speech Rx
vs
Phonological
awareness
training
Direct
Not stated 1.25 hours 2 x per
week
8 4 weeks (1) Significant
speech . (2)
additional
phonological
awareness work
adds values over
maturation or
conventional Rx
(3) 3 response
patterns to Rx
43.
Stiegler &
Hoffman
(2001)
Level III-3
School N= 3 boys,
aged 9;2, 9;10
& 9;6 years
with language-
learning
disorders &
word finding
problems
Clinician
without
explicit
statement
that they
were an
SPs
Expressive
vocabulary-
word finding
ICF: I, A & P
Discourse
based
contextual Rx
Direct
1:1 15 minutes 5
sessions
for each
of the
five
program
stages
weeks.
25 5 weeks Incidence of word
finding problems
for each child.
Rx may not be
change agent
44. Strand
et al
(2006)
Level III-3
X-baseline
N= 4 non
verbal
children aged
5;5 – 6;1 with
childhood
apraxia of
SP Phonology
ICF;
Impairment
Rx based on
motor
learning-
Integral
stimulation,
dynamic &
1:1 30 mins Twice
daily
38-50 6 weeks 1. Significant
speech for ¾
children
suggesting that
frequent Rx using
motor learning
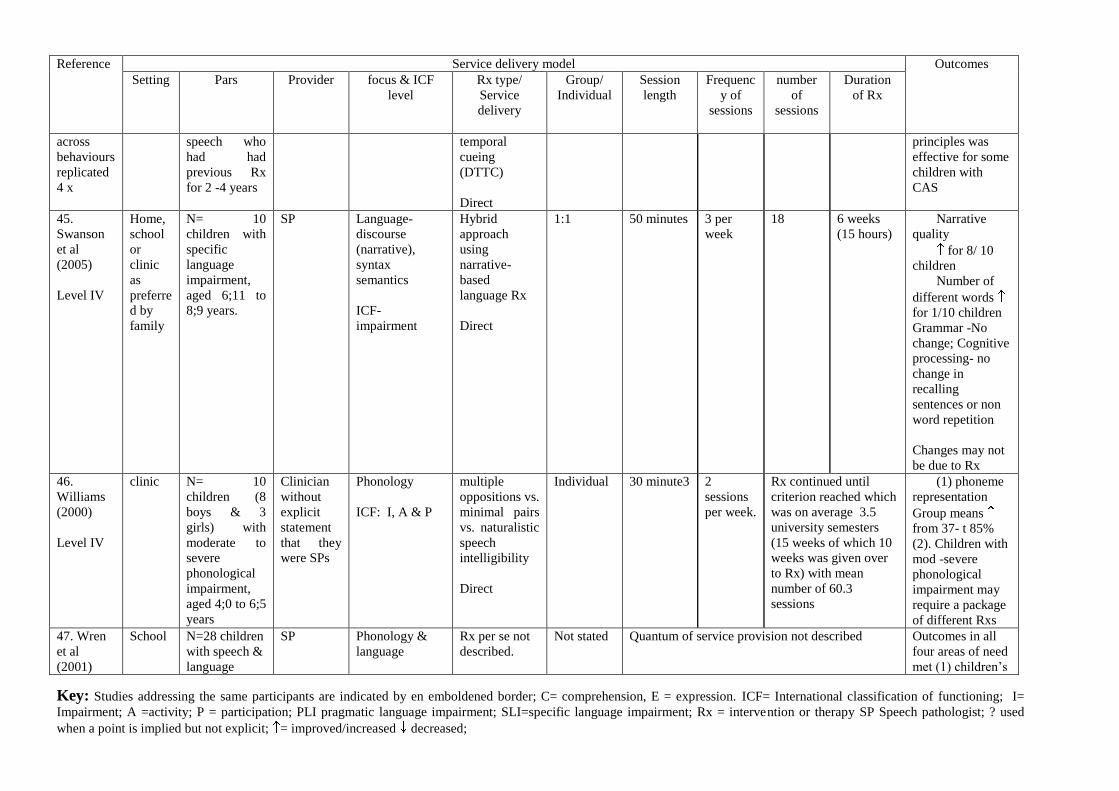
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
across
behaviours
replicated
4 x
speech who
had had
previous Rx
for 2 -4 years
temporal
cueing
(DTTC)
Direct
principles was
effective for some
children with
CAS
45.
Swanson
et al
(2005)
Level IV
Home,
school
or
clinic
as
preferre
d by
family
N= 10
children with
specific
language
impairment,
aged 6;11 to
8;9 years.
SP Language-
discourse
(narrative),
syntax
semantics
ICF-
impairment
Hybrid
approach
using
narrative-
based
language Rx
Direct
1:1 50 minutes 3 per
week
18 6 weeks
(15 hours)
2. Narrative
quality
3. for 8/ 10
children
4. Number of
different words
for 1/10 children
Grammar -No
change; Cognitive
processing- no
change in
recalling
sentences or non
word repetition
Changes may not
be due to Rx
46.
Williams
(2000)
Level IV
clinic N= 10
children (8
boys & 3
girls) with
moderate to
severe
phonological
impairment,
aged 4;0 to 6;5
years
Clinician
without
explicit
statement
that they
were SPs
Phonology
ICF: I, A & P
multiple
oppositions vs.
minimal pairs
vs. naturalistic
speech
intelligibility
Direct
Individual 30 minute3 2
sessions
per week.
Rx continued until
criterion reached which
was on average 3.5
university semesters
(15 weeks of which 10
weeks was given over
to Rx) with mean
number of 60.3
sessions
5. (1) phoneme
representation
Group means
from 37- t 85%
(2). Children with
mod -severe
phonological
impairment may
require a package
of different Rxs
47. Wren
et al
(2001)
School N=28 children
with speech &
language
SP Phonology &
language
Rx per se not
described.
Not stated Quantum of service provision not described Outcomes in all
four areas of need
met (1) children‟s
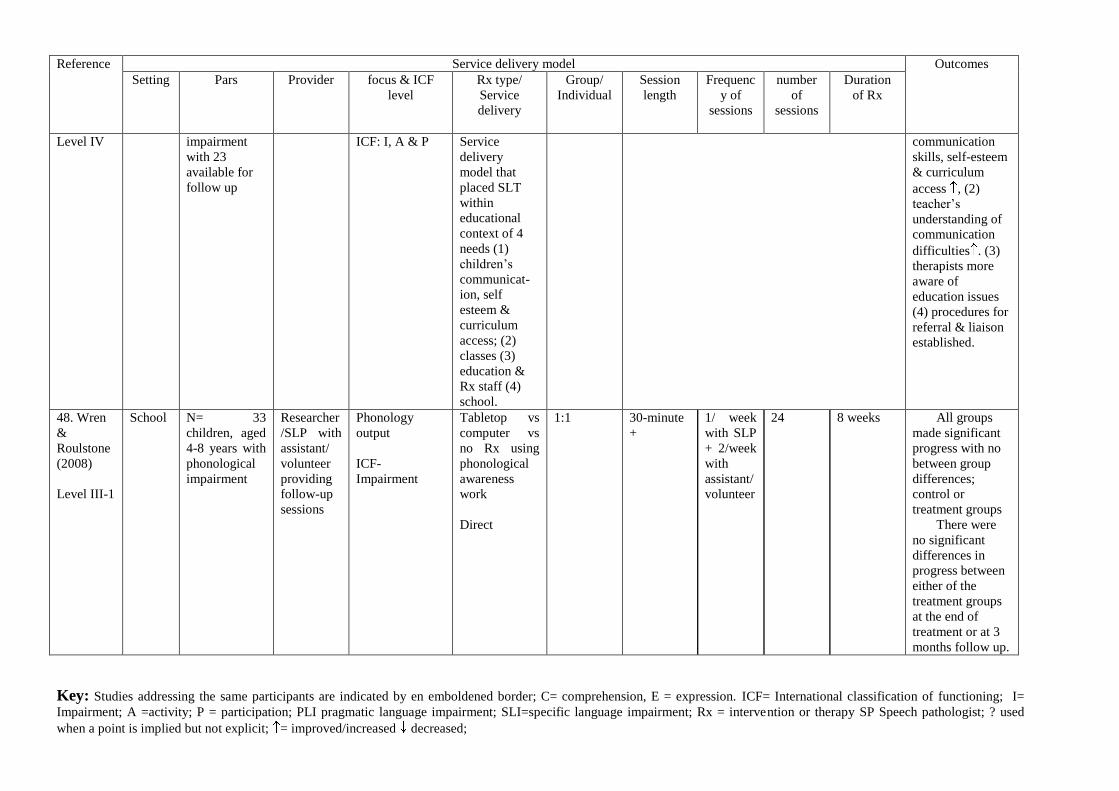
Key: Studies addressing the same participants are indicated by en emboldened border; C= comprehension, E = expression. ICF= International classification of functioning; I=
Impairment; A =activity; P = participation; PLI pragmatic language impairment; SLI=specific language impairment; Rx = intervention or therapy SP Speech pathologist; ? used
when a point is implied but not explicit; = improved/increased decreased;
Reference Service delivery model Outcomes
Setting Pars Provider focus & ICF
level
Rx type/
Service
delivery
Group/
Individual
Session
length
Frequenc
y of
sessions
number
of
sessions
Duration
of Rx
Level IV impairment
with 23
available for
follow up
ICF: I, A & P Service
delivery
model that
placed SLT
within
educational
context of 4
needs (1)
children‟s
communicat-
ion, self
esteem &
curriculum
access; (2)
classes (3)
education &
Rx staff (4)
school.
communication
skills, self-esteem
& curriculum
access , (2)
teacher‟s
understanding of
communication
difficulties . (3)
therapists more
aware of
education issues
(4) procedures for
referral & liaison
established.
48. Wren
&
Roulstone
(2008)
Level III-1
School N= 33
children, aged
4-8 years with
phonological
impairment
Researcher
/SLP with
assistant/
volunteer
providing
follow-up
sessions
Phonology
output
ICF-
Impairment
Tabletop vs
computer vs
no Rx using
phonological
awareness
work
Direct
1:1 30-minute
+
1/ week
with SLP
+ 2/week
with
assistant/
volunteer
24 8 weeks 6. All groups
made significant
progress with no
between group
differences;
control or
treatment groups
7. There were
no significant
differences in
progress between
either of the
treatment groups
at the end of
treatment or at 3
months follow up.
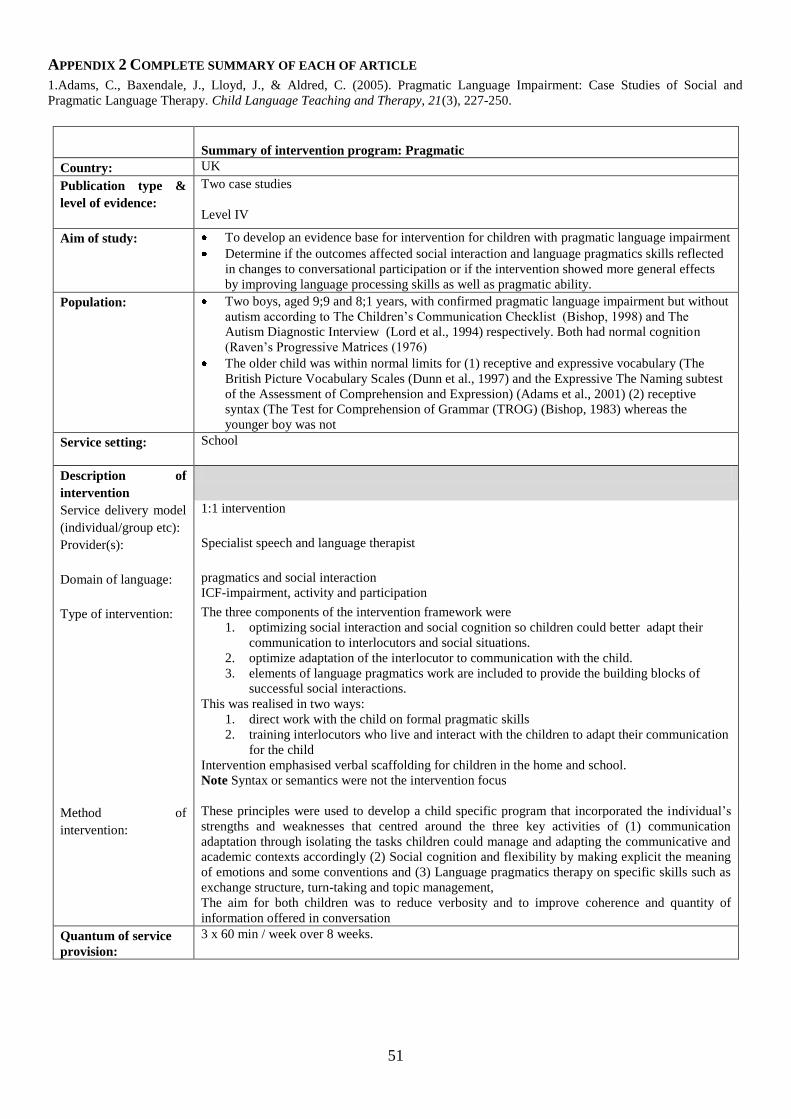
51
APPENDIX 2 COMPLETE SUMMARY OF EACH OF ARTICLE
1.Adams, C., Baxendale, J., Lloyd, J., & Aldred, C. (2005). Pragmatic Language Impairment: Case Studies of Social and
Pragmatic Language Therapy. Child Language Teaching and Therapy, 21(3), 227-250.
Summary of intervention program: Pragmatic
Country: UK
Publication type &
level of evidence:
Two case studies
Level IV
Aim of study:
To develop an evidence base for intervention for children with pragmatic language impairment
Determine if the outcomes affected social interaction and language pragmatics skills reflected
in changes to conversational participation or if the intervention showed more general effects
by improving language processing skills as well as pragmatic ability.
Population:
Two boys, aged 9;9 and 8;1 years, with confirmed pragmatic language impairment but without
autism according to The Children‟s Communication Checklist (Bishop, 1998) and The
Autism Diagnostic Interview (Lord et al., 1994) respectively. Both had normal cognition
(Raven‟s Progressive Matrices (1976)
The older child was within normal limits for (1) receptive and expressive vocabulary (The
British Picture Vocabulary Scales (Dunn et al., 1997) and the Expressive The Naming subtest
of the Assessment of Comprehension and Expression) (Adams et al., 2001) (2) receptive
syntax (The Test for Comprehension of Grammar (TROG) (Bishop, 1983) whereas the
younger boy was not
Service setting:
School
Description of
intervention
Service delivery model
(individual/group etc):
1:1 intervention
Provider(s):
Specialist speech and language therapist
Domain of language:
pragmatics and social interaction
ICF-impairment, activity and participation
Type of intervention:
The three components of the intervention framework were
1. optimizing social interaction and social cognition so children could better adapt their
communication to interlocutors and social situations.
2. optimize adaptation of the interlocutor to communication with the child.
3. elements of language pragmatics work are included to provide the building blocks of
successful social interactions.
This was realised in two ways:
1. direct work with the child on formal pragmatic skills
2. training interlocutors who live and interact with the children to adapt their communication
for the child
Intervention emphasised verbal scaffolding for children in the home and school.
Note Syntax or semantics were not the intervention focus
Method of
intervention:
These principles were used to develop a child specific program that incorporated the individual‟s
strengths and weaknesses that centred around the three key activities of (1) communication
adaptation through isolating the tasks children could manage and adapting the communicative and
academic contexts accordingly (2) Social cognition and flexibility by making explicit the meaning
of emotions and some conventions and (3) Language pragmatics therapy on specific skills such as
exchange structure, turn-taking and topic management,
The aim for both children was to reduce verbosity and to improve coherence and quantity of
information offered in conversation
Quantum of service
provision:
3 x 60 min / week over 8 weeks.
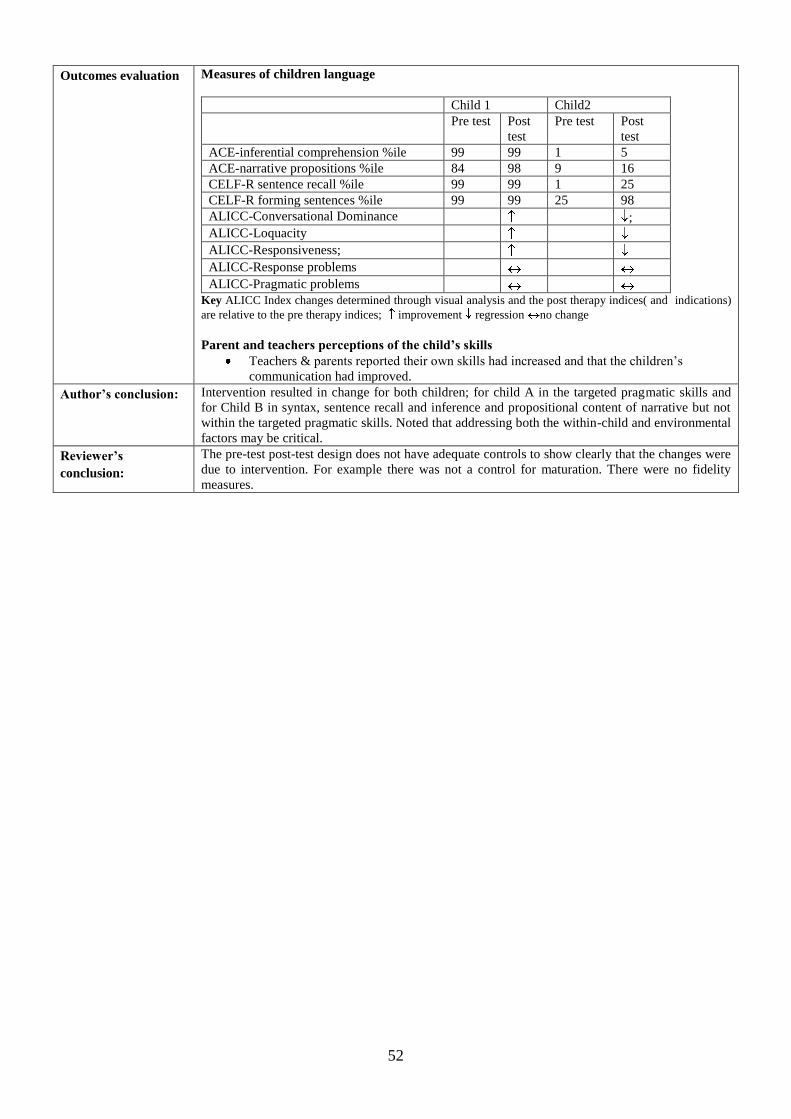
52
Outcomes evaluation
Measures of children language
Child 1 Child2
Pre test Post
test
Pre test Post
test
ACE-inferential comprehension %ile 99 99 1 5
ACE-narrative propositions %ile 84 98 9 16
CELF-R sentence recall %ile 99 99 1 25
CELF-R forming sentences %ile 99 99 25 98
ALICC-Conversational Dominance ;
ALICC-Loquacity
ALICC-Responsiveness;
ALICC-Response problems
ALICC-Pragmatic problems Key ALICC Index changes determined through visual analysis and the post therapy indices( and indications)
are relative to the pre therapy indices; improvement regression no change
Parent and teachers perceptions of the child’s skills
Teachers & parents reported their own skills had increased and that the children‟s
communication had improved.
Author’s conclusion: Intervention resulted in change for both children; for child A in the targeted pragmatic skills and
for Child B in syntax, sentence recall and inference and propositional content of narrative but not
within the targeted pragmatic skills. Noted that addressing both the within-child and environmental
factors may be critical.
Reviewer’s
conclusion:
The pre-test post-test design does not have adequate controls to show clearly that the changes were
due to intervention. For example there was not a control for maturation. There were no fidelity
measures.
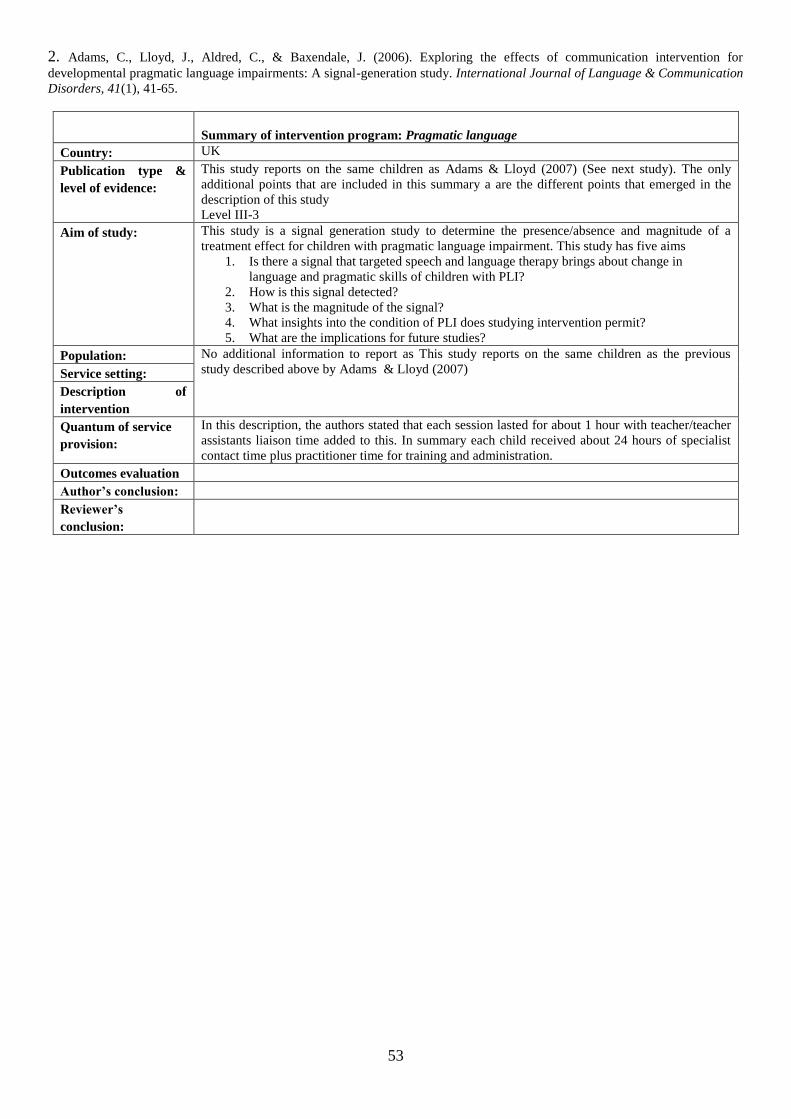
53
2. Adams, C., Lloyd, J., Aldred, C., & Baxendale, J. (2006). Exploring the effects of communication intervention for
developmental pragmatic language impairments: A signal-generation study. International Journal of Language & Communication
Disorders, 41(1), 41-65.
Summary of intervention program: Pragmatic language
Country: UK
Publication type &
level of evidence:
This study reports on the same children as Adams & Lloyd (2007) (See next study). The only
additional points that are included in this summary a are the different points that emerged in the
description of this study
Level III-3
Aim of study:
This study is a signal generation study to determine the presence/absence and magnitude of a
treatment effect for children with pragmatic language impairment. This study has five aims
1. Is there a signal that targeted speech and language therapy brings about change in
language and pragmatic skills of children with PLI?
2. How is this signal detected?
3. What is the magnitude of the signal?
4. What insights into the condition of PLI does studying intervention permit?
5. What are the implications for future studies?
Population: No additional information to report as This study reports on the same children as the previous
study described above by Adams & Lloyd (2007) Service setting:
Description of
intervention
Quantum of service
provision:
In this description, the authors stated that each session lasted for about 1 hour with teacher/teacher
assistants liaison time added to this. In summary each child received about 24 hours of specialist
contact time plus practitioner time for training and administration.
Outcomes evaluation
Author’s conclusion:
Reviewer’s
conclusion:
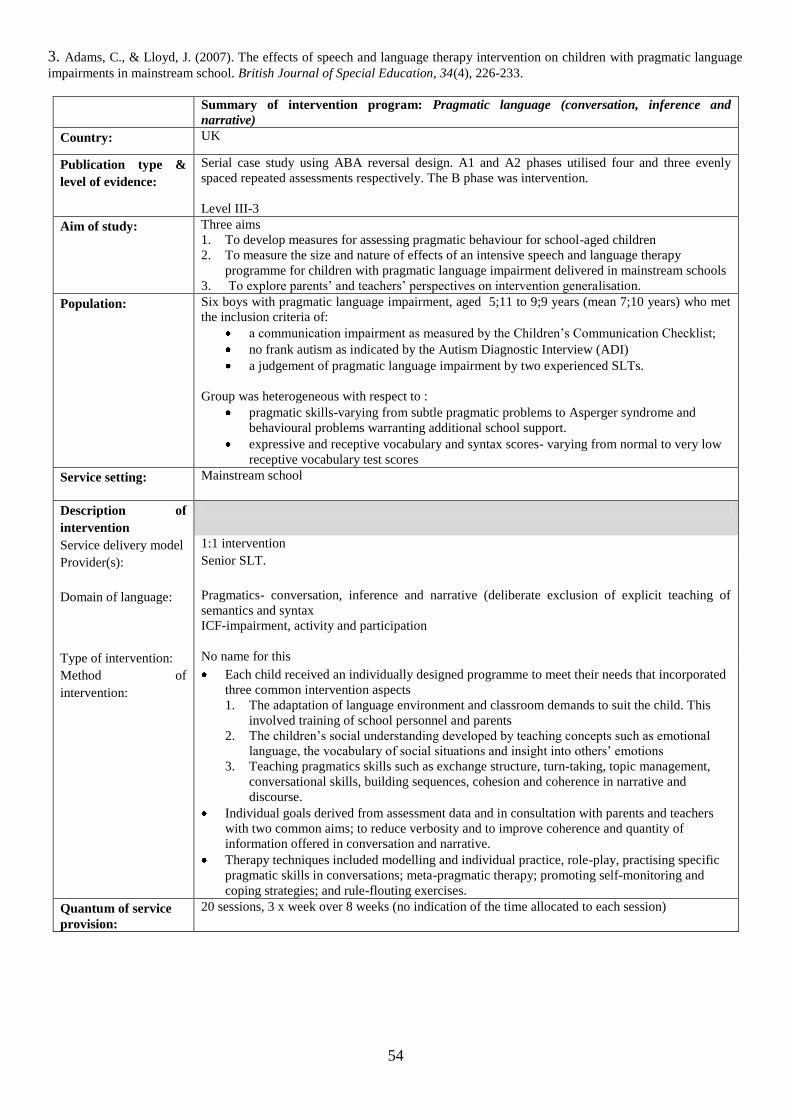
54
3. Adams, C., & Lloyd, J. (2007). The effects of speech and language therapy intervention on children with pragmatic language
impairments in mainstream school. British Journal of Special Education, 34(4), 226-233.
Summary of intervention program: Pragmatic language (conversation, inference and
narrative)
Country: UK
Publication type &
level of evidence:
Serial case study using ABA reversal design. A1 and A2 phases utilised four and three evenly
spaced repeated assessments respectively. The B phase was intervention.
Level III-3
Aim of study:
Three aims
1. To develop measures for assessing pragmatic behaviour for school-aged children
2. To measure the size and nature of effects of an intensive speech and language therapy
programme for children with pragmatic language impairment delivered in mainstream schools
3. To explore parents‟ and teachers‟ perspectives on intervention generalisation.
Population:
Six boys with pragmatic language impairment, aged 5;11 to 9;9 years (mean 7;10 years) who met
the inclusion criteria of:
a communication impairment as measured by the Children‟s Communication Checklist;
no frank autism as indicated by the Autism Diagnostic Interview (ADI)
a judgement of pragmatic language impairment by two experienced SLTs.
Group was heterogeneous with respect to :
pragmatic skills-varying from subtle pragmatic problems to Asperger syndrome and
behavioural problems warranting additional school support.
expressive and receptive vocabulary and syntax scores- varying from normal to very low
receptive vocabulary test scores
Service setting:
Mainstream school
Description of
intervention
Service delivery model 1:1 intervention
Provider(s):
Senior SLT.
Domain of language:
Pragmatics- conversation, inference and narrative (deliberate exclusion of explicit teaching of
semantics and syntax
ICF-impairment, activity and participation
Type of intervention: No name for this
Method of
intervention:
Each child received an individually designed programme to meet their needs that incorporated
three common intervention aspects
1. The adaptation of language environment and classroom demands to suit the child. This
involved training of school personnel and parents
2. The children‟s social understanding developed by teaching concepts such as emotional
language, the vocabulary of social situations and insight into others‟ emotions
3. Teaching pragmatics skills such as exchange structure, turn-taking, topic management,
conversational skills, building sequences, cohesion and coherence in narrative and
discourse.
Individual goals derived from assessment data and in consultation with parents and teachers
with two common aims; to reduce verbosity and to improve coherence and quantity of
information offered in conversation and narrative.
Therapy techniques included modelling and individual practice, role-play, practising specific
pragmatic skills in conversations; meta-pragmatic therapy; promoting self-monitoring and
coping strategies; and rule-flouting exercises.
Quantum of service
provision:
20 sessions, 3 x week over 8 weeks (no indication of the time allocated to each session)
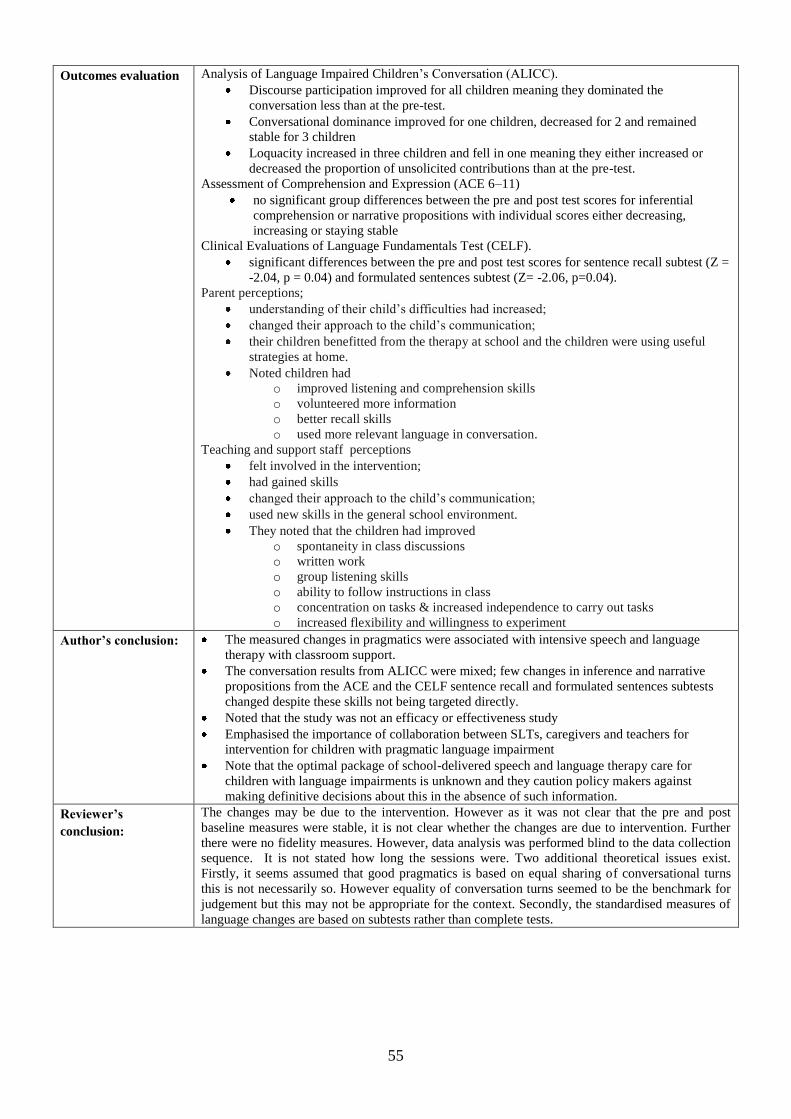
55
Outcomes evaluation Analysis of Language Impaired Children‟s Conversation (ALICC).
Discourse participation improved for all children meaning they dominated the
conversation less than at the pre-test.
Conversational dominance improved for one children, decreased for 2 and remained
stable for 3 children
Loquacity increased in three children and fell in one meaning they either increased or
decreased the proportion of unsolicited contributions than at the pre-test.
Assessment of Comprehension and Expression (ACE 6–11)
no significant group differences between the pre and post test scores for inferential
comprehension or narrative propositions with individual scores either decreasing,
increasing or staying stable
Clinical Evaluations of Language Fundamentals Test (CELF).
significant differences between the pre and post test scores for sentence recall subtest (Z =
-2.04, p = 0.04) and formulated sentences subtest (Z= -2.06, p=0.04).
Parent perceptions;
understanding of their child‟s difficulties had increased;
changed their approach to the child‟s communication;
their children benefitted from the therapy at school and the children were using useful
strategies at home.
Noted children had
o improved listening and comprehension skills
o volunteered more information
o better recall skills
o used more relevant language in conversation.
Teaching and support staff perceptions
felt involved in the intervention;
had gained skills
changed their approach to the child‟s communication;
used new skills in the general school environment.
They noted that the children had improved
o spontaneity in class discussions
o written work
o group listening skills
o ability to follow instructions in class
o concentration on tasks & increased independence to carry out tasks
o increased flexibility and willingness to experiment
Author’s conclusion:
The measured changes in pragmatics were associated with intensive speech and language
therapy with classroom support.
The conversation results from ALICC were mixed; few changes in inference and narrative
propositions from the ACE and the CELF sentence recall and formulated sentences subtests
changed despite these skills not being targeted directly.
Noted that the study was not an efficacy or effectiveness study
Emphasised the importance of collaboration between SLTs, caregivers and teachers for
intervention for children with pragmatic language impairment
Note that the optimal package of school-delivered speech and language therapy care for
children with language impairments is unknown and they caution policy makers against
making definitive decisions about this in the absence of such information.
Reviewer’s
conclusion:
The changes may be due to the intervention. However as it was not clear that the pre and post
baseline measures were stable, it is not clear whether the changes are due to intervention. Further
there were no fidelity measures. However, data analysis was performed blind to the data collection
sequence. It is not stated how long the sessions were. Two additional theoretical issues exist.
Firstly, it seems assumed that good pragmatics is based on equal sharing of conversational turns
this is not necessarily so. However equality of conversation turns seemed to be the benchmark for
judgement but this may not be appropriate for the context. Secondly, the standardised measures of
language changes are based on subtests rather than complete tests.
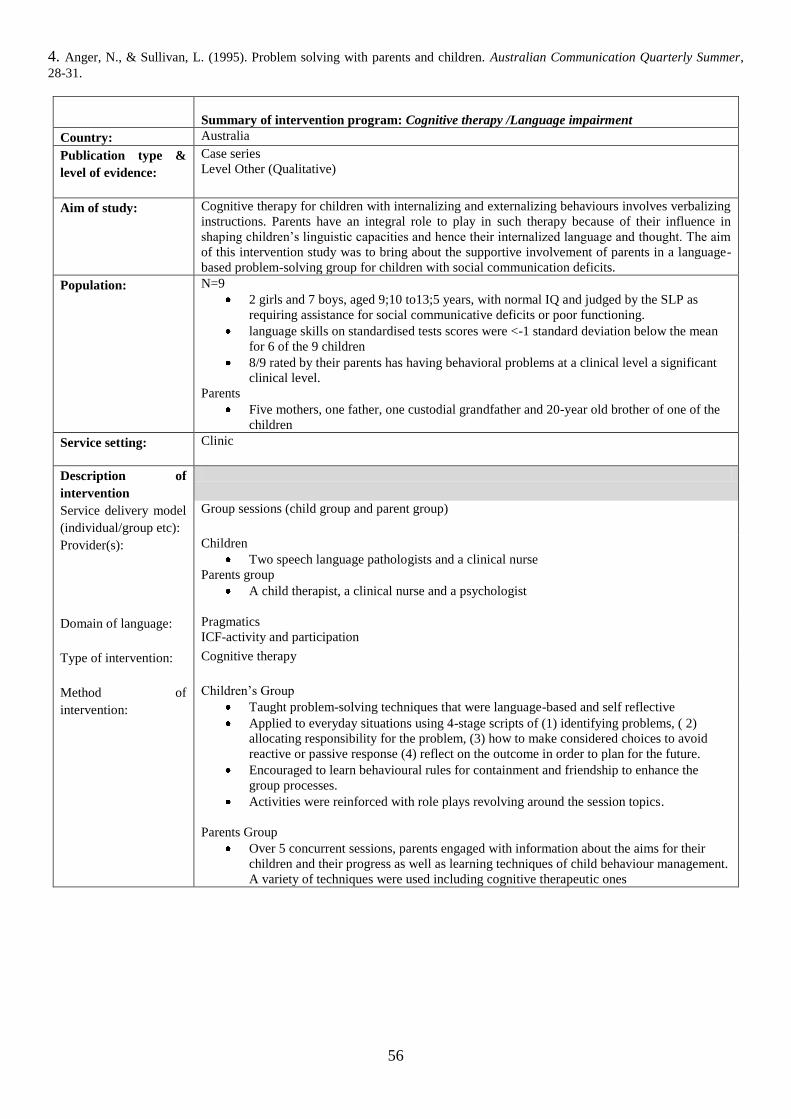
56
4. Anger, N., & Sullivan, L. (1995). Problem solving with parents and children. Australian Communication Quarterly Summer,
28-31.
Summary of intervention program: Cognitive therapy /Language impairment
Country: Australia
Publication type &
level of evidence:
Case series
Level Other (Qualitative)
Aim of study:
Cognitive therapy for children with internalizing and externalizing behaviours involves verbalizing
instructions. Parents have an integral role to play in such therapy because of their influence in
shaping children‟s linguistic capacities and hence their internalized language and thought. The aim
of this intervention study was to bring about the supportive involvement of parents in a language-
based problem-solving group for children with social communication deficits.
Population:
N=9
2 girls and 7 boys, aged 9;10 to13;5 years, with normal IQ and judged by the SLP as
requiring assistance for social communicative deficits or poor functioning.
language skills on standardised tests scores were <-1 standard deviation below the mean
for 6 of the 9 children
8/9 rated by their parents has having behavioral problems at a clinical level a significant
clinical level.
Parents
Five mothers, one father, one custodial grandfather and 20-year old brother of one of the
children
Service setting:
Clinic
Description of
intervention
Service delivery model
(individual/group etc):
Group sessions (child group and parent group)
Provider(s):
Children
Two speech language pathologists and a clinical nurse
Parents group
A child therapist, a clinical nurse and a psychologist
Domain of language:
Pragmatics
ICF-activity and participation
Type of intervention:
Cognitive therapy
Method of
intervention:
Children‟s Group
Taught problem-solving techniques that were language-based and self reflective
Applied to everyday situations using 4-stage scripts of (1) identifying problems, ( 2)
allocating responsibility for the problem, (3) how to make considered choices to avoid
reactive or passive response (4) reflect on the outcome in order to plan for the future.
Encouraged to learn behavioural rules for containment and friendship to enhance the
group processes.
Activities were reinforced with role plays revolving around the session topics.
Parents Group
Over 5 concurrent sessions, parents engaged with information about the aims for their
children and their progress as well as learning techniques of child behaviour management.
A variety of techniques were used including cognitive therapeutic ones
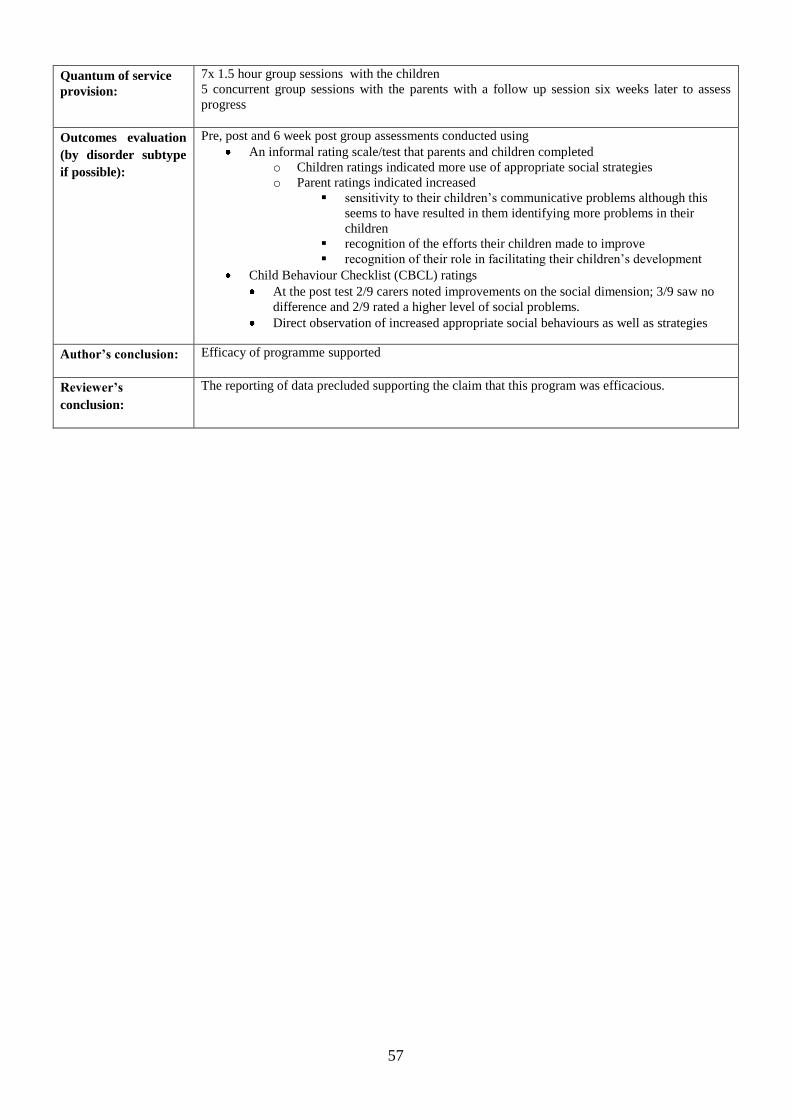
57
Quantum of service
provision:
7x 1.5 hour group sessions with the children
5 concurrent group sessions with the parents with a follow up session six weeks later to assess
progress
Outcomes evaluation
(by disorder subtype
if possible):
Pre, post and 6 week post group assessments conducted using
An informal rating scale/test that parents and children completed
o Children ratings indicated more use of appropriate social strategies
o Parent ratings indicated increased
sensitivity to their children‟s communicative problems although this
seems to have resulted in them identifying more problems in their
children
recognition of the efforts their children made to improve
recognition of their role in facilitating their children‟s development
Child Behaviour Checklist (CBCL) ratings
At the post test 2/9 carers noted improvements on the social dimension; 3/9 saw no
difference and 2/9 rated a higher level of social problems.
Direct observation of increased appropriate social behaviours as well as strategies
Author’s conclusion:
Efficacy of programme supported
Reviewer’s
conclusion:
The reporting of data precluded supporting the claim that this program was efficacious.
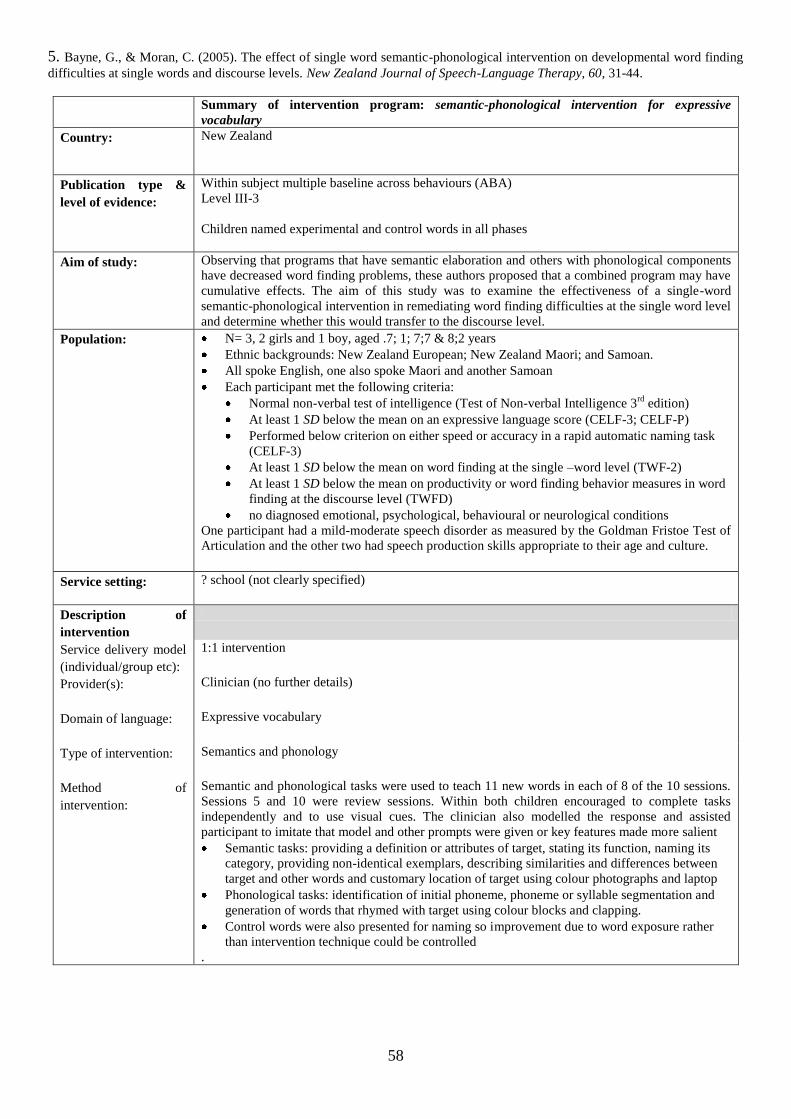
58
5. Bayne, G., & Moran, C. (2005). The effect of single word semantic-phonological intervention on developmental word finding
difficulties at single words and discourse levels. New Zealand Journal of Speech-Language Therapy, 60, 31-44.
Summary of intervention program: semantic-phonological intervention for expressive
vocabulary
Country: New Zealand
Publication type &
level of evidence:
Within subject multiple baseline across behaviours (ABA)
Level III-3
Children named experimental and control words in all phases
Aim of study:
Observing that programs that have semantic elaboration and others with phonological components
have decreased word finding problems, these authors proposed that a combined program may have
cumulative effects. The aim of this study was to examine the effectiveness of a single-word
semantic-phonological intervention in remediating word finding difficulties at the single word level
and determine whether this would transfer to the discourse level.
Population:
N= 3, 2 girls and 1 boy, aged .7; 1; 7;7 & 8;2 years
Ethnic backgrounds: New Zealand European; New Zealand Maori; and Samoan.
All spoke English, one also spoke Maori and another Samoan
Each participant met the following criteria:
Normal non-verbal test of intelligence (Test of Non-verbal Intelligence 3rd
edition)
At least 1 SD below the mean on an expressive language score (CELF-3; CELF-P)
Performed below criterion on either speed or accuracy in a rapid automatic naming task
(CELF-3)
At least 1 SD below the mean on word finding at the single –word level (TWF-2)
At least 1 SD below the mean on productivity or word finding behavior measures in word
finding at the discourse level (TWFD)
no diagnosed emotional, psychological, behavioural or neurological conditions
One participant had a mild-moderate speech disorder as measured by the Goldman Fristoe Test of
Articulation and the other two had speech production skills appropriate to their age and culture.
Service setting:
? school (not clearly specified)
Description of
intervention
Service delivery model
(individual/group etc):
1:1 intervention
Provider(s):
Clinician (no further details)
Domain of language:
Expressive vocabulary
Type of intervention:
Semantics and phonology
Method of
intervention:
Semantic and phonological tasks were used to teach 11 new words in each of 8 of the 10 sessions.
Sessions 5 and 10 were review sessions. Within both children encouraged to complete tasks
independently and to use visual cues. The clinician also modelled the response and assisted
participant to imitate that model and other prompts were given or key features made more salient
Semantic tasks: providing a definition or attributes of target, stating its function, naming its
category, providing non-identical exemplars, describing similarities and differences between
target and other words and customary location of target using colour photographs and laptop
Phonological tasks: identification of initial phoneme, phoneme or syllable segmentation and
generation of words that rhymed with target using colour blocks and clapping.
Control words were also presented for naming so improvement due to word exposure rather
than intervention technique could be controlled
.
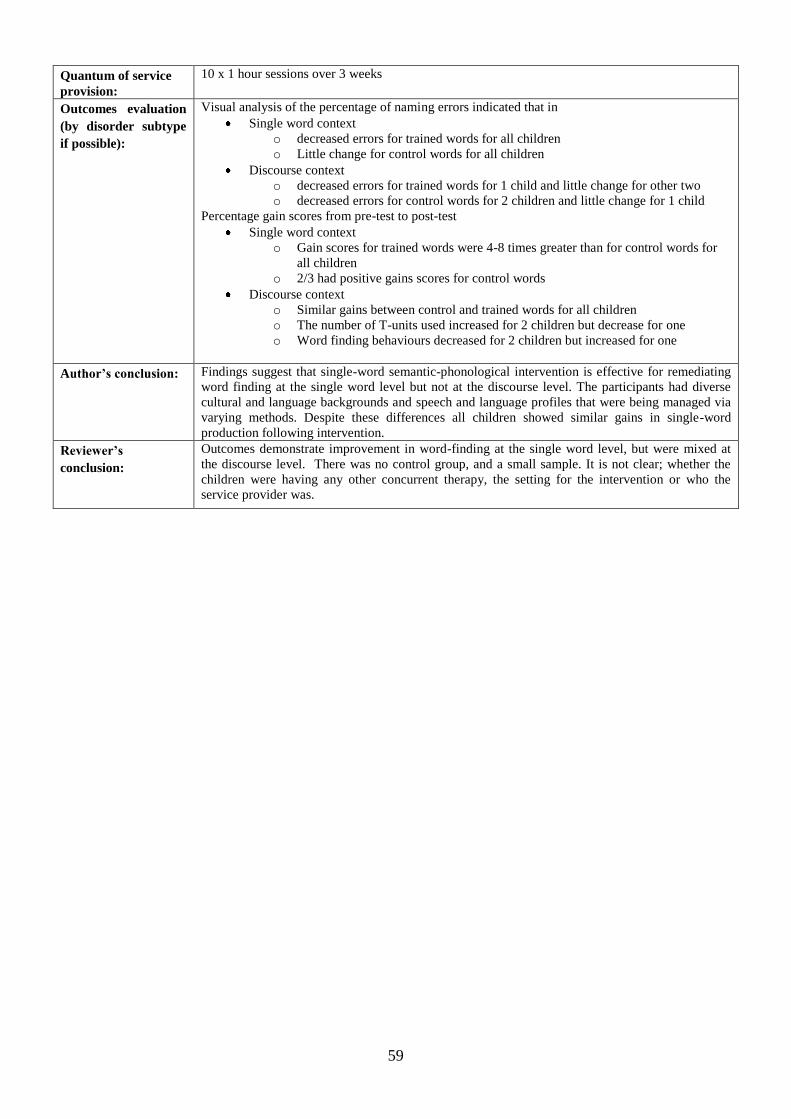
59
Quantum of service
provision:
10 x 1 hour sessions over 3 weeks
Outcomes evaluation
(by disorder subtype
if possible):
Visual analysis of the percentage of naming errors indicated that in
Single word context
o decreased errors for trained words for all children
o Little change for control words for all children
Discourse context
o decreased errors for trained words for 1 child and little change for other two
o decreased errors for control words for 2 children and little change for 1 child
Percentage gain scores from pre-test to post-test
Single word context
o Gain scores for trained words were 4-8 times greater than for control words for
all children
o 2/3 had positive gains scores for control words
Discourse context
o Similar gains between control and trained words for all children
o The number of T-units used increased for 2 children but decrease for one
o Word finding behaviours decreased for 2 children but increased for one
Author’s conclusion:
Findings suggest that single-word semantic-phonological intervention is effective for remediating
word finding at the single word level but not at the discourse level. The participants had diverse
cultural and language backgrounds and speech and language profiles that were being managed via
varying methods. Despite these differences all children showed similar gains in single-word
production following intervention.
Reviewer’s
conclusion:
Outcomes demonstrate improvement in word-finding at the single word level, but were mixed at
the discourse level. There was no control group, and a small sample. It is not clear; whether the
children were having any other concurrent therapy, the setting for the intervention or who the
service provider was.
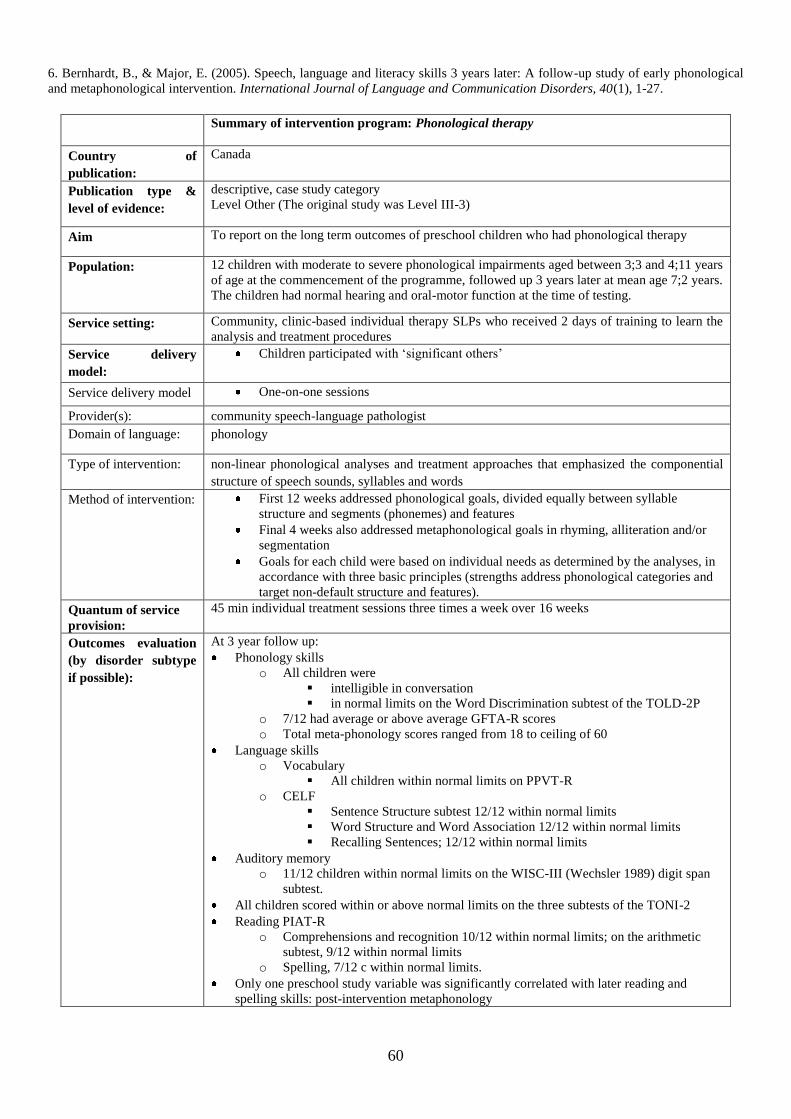
60
6. Bernhardt, B., & Major, E. (2005). Speech, language and literacy skills 3 years later: A follow-up study of early phonological
and metaphonological intervention. International Journal of Language and Communication Disorders, 40(1), 1-27.
Summary of intervention program: Phonological therapy
Country of
publication:
Canada
Publication type &
level of evidence:
descriptive, case study category
Level Other (The original study was Level III-3)
Aim To report on the long term outcomes of preschool children who had phonological therapy
Population:
12 children with moderate to severe phonological impairments aged between 3;3 and 4;11 years
of age at the commencement of the programme, followed up 3 years later at mean age 7;2 years.
The children had normal hearing and oral-motor function at the time of testing.
Service setting: Community, clinic-based individual therapy SLPs who received 2 days of training to learn the
analysis and treatment procedures
Service delivery
model:
Children participated with „significant others‟
Service delivery model One-on-one sessions
Provider(s): community speech-language pathologist
Domain of language: phonology
Type of intervention: non-linear phonological analyses and treatment approaches that emphasized the componential
structure of speech sounds, syllables and words
Method of intervention:
First 12 weeks addressed phonological goals, divided equally between syllable
structure and segments (phonemes) and features
Final 4 weeks also addressed metaphonological goals in rhyming, alliteration and/or
segmentation
Goals for each child were based on individual needs as determined by the analyses, in
accordance with three basic principles (strengths address phonological categories and
target non-default structure and features).
Quantum of service
provision:
45 min individual treatment sessions three times a week over 16 weeks
Outcomes evaluation
(by disorder subtype
if possible):
At 3 year follow up:
Phonology skills
o All children were
intelligible in conversation
in normal limits on the Word Discrimination subtest of the TOLD-2P
o 7/12 had average or above average GFTA-R scores
o Total meta-phonology scores ranged from 18 to ceiling of 60
Language skills
o Vocabulary
All children within normal limits on PPVT-R
o CELF
Sentence Structure subtest 12/12 within normal limits
Word Structure and Word Association 12/12 within normal limits
Recalling Sentences; 12/12 within normal limits
Auditory memory
o 11/12 children within normal limits on the WISC-III (Wechsler 1989) digit span
subtest.
All children scored within or above normal limits on the three subtests of the TONI-2
Reading PIAT-R
o Comprehensions and recognition 10/12 within normal limits; on the arithmetic
subtest, 9/12 within normal limits
o Spelling, 7/12 c within normal limits.
Only one preschool study variable was significantly correlated with later reading and
spelling skills: post-intervention metaphonology

61
Author’s conclusion:
Most children performed within normal limits on a number of speech, language and literacy
tasks, in spite of their early history of severe phonological impairments and delays in language
production and metaphonology. Early phonological and metaphonological intervention can
promote normalization of speech development, and normal acquisition of literacy skills for
children with severe phonological impairments. Not all children will demonstrate short-term
normalization, but the level and prevalence of risk can be reduced.
Reviewer’s
conclusion:
The phonological intervention appeared to lead to improved outcomes for children with
phonological impairments, both in the short term, and at 3 years follow-up. Although only a
small case series, it may give some indication that ongoing intensive therapy may not be
required for this population.
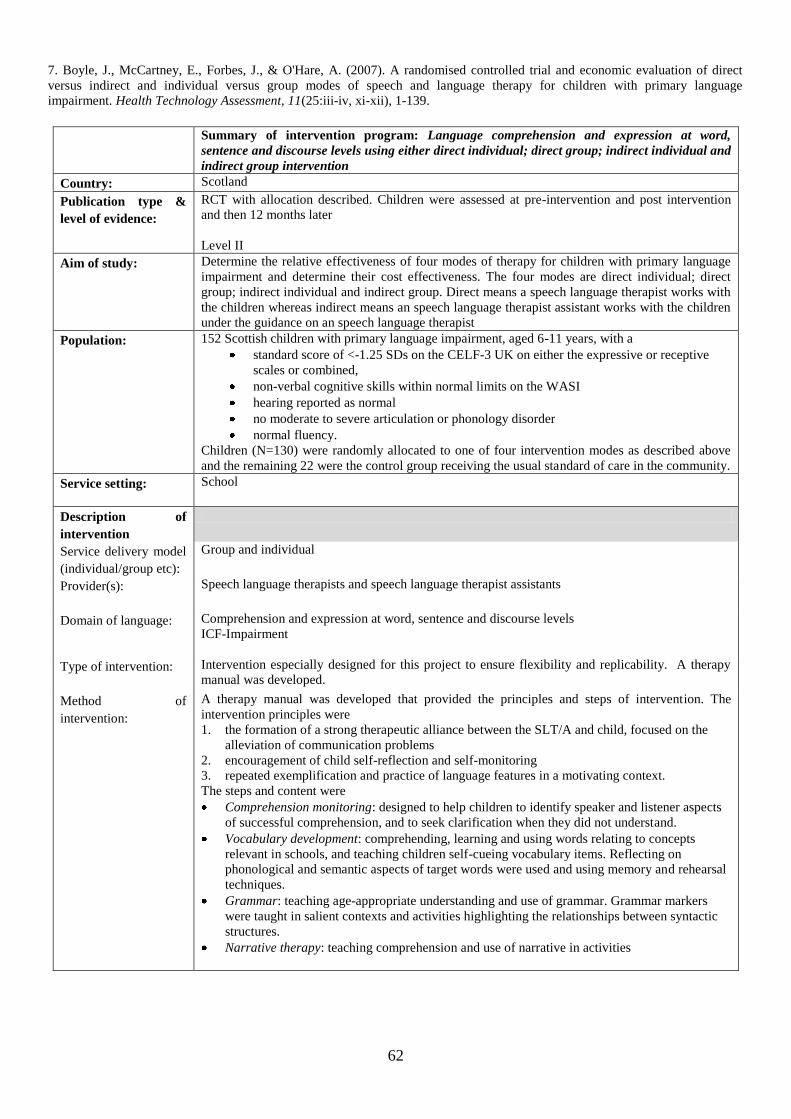
62
7. Boyle, J., McCartney, E., Forbes, J., & O'Hare, A. (2007). A randomised controlled trial and economic evaluation of direct
versus indirect and individual versus group modes of speech and language therapy for children with primary language
impairment. Health Technology Assessment, 11(25:iii-iv, xi-xii), 1-139.
Summary of intervention program: Language comprehension and expression at word,
sentence and discourse levels using either direct individual; direct group; indirect individual and
indirect group intervention
Country: Scotland
Publication type &
level of evidence:
RCT with allocation described. Children were assessed at pre-intervention and post intervention
and then 12 months later
Level II
Aim of study:
Determine the relative effectiveness of four modes of therapy for children with primary language
impairment and determine their cost effectiveness. The four modes are direct individual; direct
group; indirect individual and indirect group. Direct means a speech language therapist works with
the children whereas indirect means an speech language therapist assistant works with the children
under the guidance on an speech language therapist
Population:
152 Scottish children with primary language impairment, aged 6-11 years, with a
standard score of <-1.25 SDs on the CELF-3 UK on either the expressive or receptive
scales or combined,
non-verbal cognitive skills within normal limits on the WASI
hearing reported as normal
no moderate to severe articulation or phonology disorder
normal fluency.
Children (N=130) were randomly allocated to one of four intervention modes as described above
and the remaining 22 were the control group receiving the usual standard of care in the community.
Service setting:
School
Description of
intervention
Service delivery model
(individual/group etc):
Group and individual
Provider(s):
Speech language therapists and speech language therapist assistants
Domain of language:
Comprehension and expression at word, sentence and discourse levels
ICF-Impairment
Type of intervention:
Intervention especially designed for this project to ensure flexibility and replicability. A therapy
manual was developed.
Method of
intervention:
A therapy manual was developed that provided the principles and steps of intervention. The
intervention principles were
1. the formation of a strong therapeutic alliance between the SLT/A and child, focused on the
alleviation of communication problems
2. encouragement of child self-reflection and self-monitoring
3. repeated exemplification and practice of language features in a motivating context.
The steps and content were
Comprehension monitoring: designed to help children to identify speaker and listener aspects
of successful comprehension, and to seek clarification when they did not understand.
Vocabulary development: comprehending, learning and using words relating to concepts
relevant in schools, and teaching children self-cueing vocabulary items. Reflecting on
phonological and semantic aspects of target words were used and using memory and rehearsal
techniques.
Grammar: teaching age-appropriate understanding and use of grammar. Grammar markers
were taught in salient contexts and activities highlighting the relationships between syntactic
structures.
Narrative therapy: teaching comprehension and use of narrative in activities
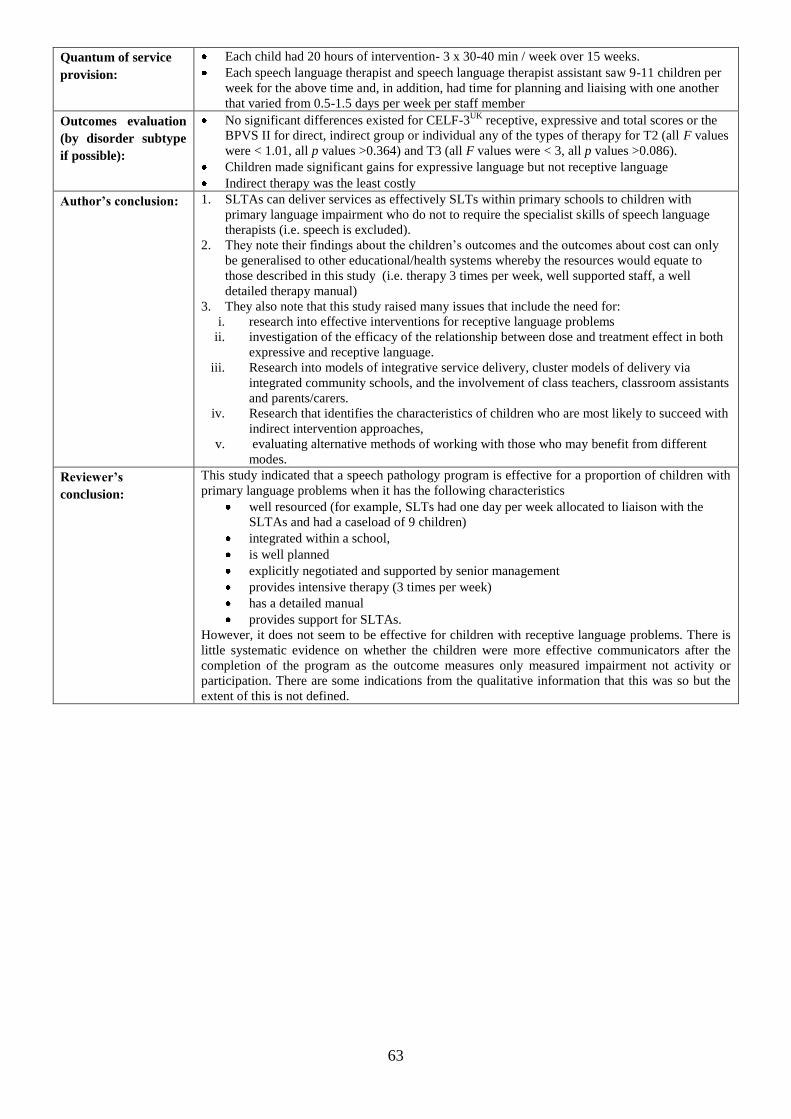
63
Quantum of service
provision:
Each child had 20 hours of intervention- 3 x 30-40 min / week over 15 weeks.
Each speech language therapist and speech language therapist assistant saw 9-11 children per
week for the above time and, in addition, had time for planning and liaising with one another
that varied from 0.5-1.5 days per week per staff member
Outcomes evaluation
(by disorder subtype
if possible):
No significant differences existed for CELF-3UK
receptive, expressive and total scores or the
BPVS II for direct, indirect group or individual any of the types of therapy for T2 (all F values
were < 1.01, all p values >0.364) and T3 (all F values were < 3, all p values >0.086).
Children made significant gains for expressive language but not receptive language
Indirect therapy was the least costly
Author’s conclusion: 1. SLTAs can deliver services as effectively SLTs within primary schools to children with
primary language impairment who do not to require the specialist skills of speech language
therapists (i.e. speech is excluded).
2. They note their findings about the children‟s outcomes and the outcomes about cost can only
be generalised to other educational/health systems whereby the resources would equate to
those described in this study (i.e. therapy 3 times per week, well supported staff, a well
detailed therapy manual)
3. They also note that this study raised many issues that include the need for:
i. research into effective interventions for receptive language problems
ii. investigation of the efficacy of the relationship between dose and treatment effect in both
expressive and receptive language.
iii. Research into models of integrative service delivery, cluster models of delivery via
integrated community schools, and the involvement of class teachers, classroom assistants
and parents/carers.
iv. Research that identifies the characteristics of children who are most likely to succeed with
indirect intervention approaches,
v. evaluating alternative methods of working with those who may benefit from different
modes.
Reviewer’s
conclusion:
This study indicated that a speech pathology program is effective for a proportion of children with
primary language problems when it has the following characteristics
well resourced (for example, SLTs had one day per week allocated to liaison with the
SLTAs and had a caseload of 9 children)
integrated within a school,
is well planned
explicitly negotiated and supported by senior management
provides intensive therapy (3 times per week)
has a detailed manual
provides support for SLTAs.
However, it does not seem to be effective for children with receptive language problems. There is
little systematic evidence on whether the children were more effective communicators after the
completion of the program as the outcome measures only measured impairment not activity or
participation. There are some indications from the qualitative information that this was so but the
extent of this is not defined.
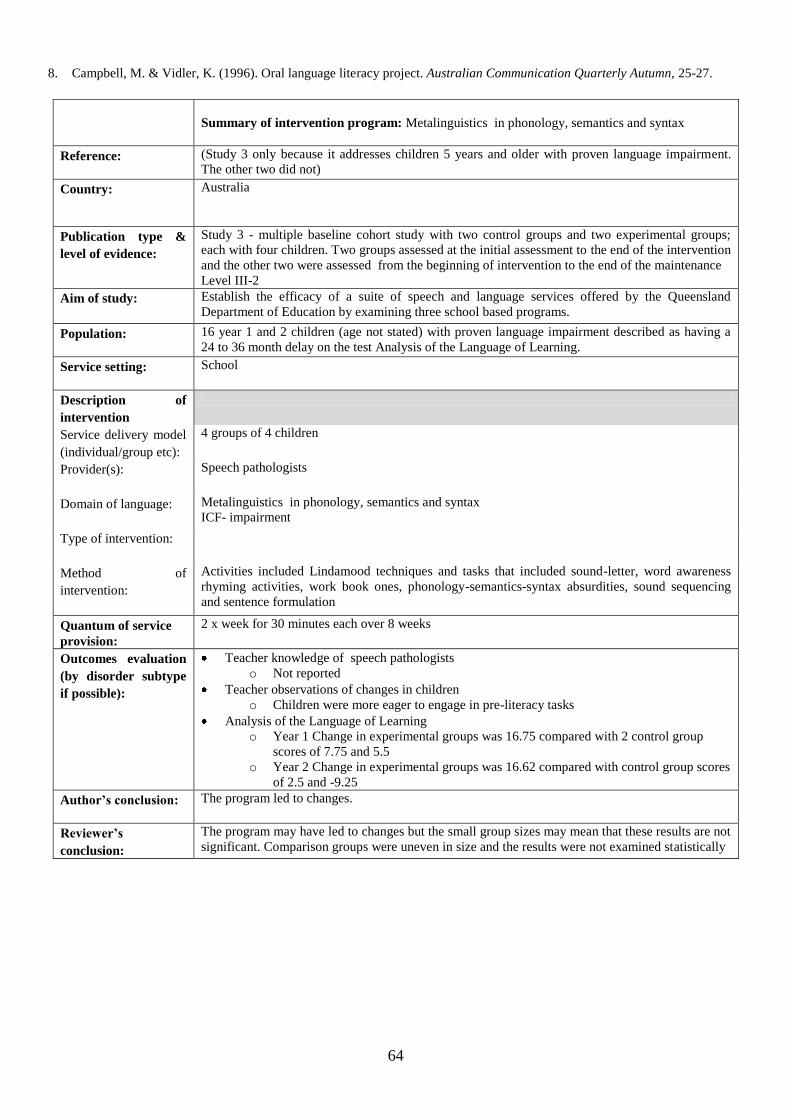
64
8. Campbell, M. & Vidler, K. (1996). Oral language literacy project. Australian Communication Quarterly Autumn, 25-27.
Summary of intervention program: Metalinguistics in phonology, semantics and syntax
Reference:
(Study 3 only because it addresses children 5 years and older with proven language impairment.
The other two did not)
Country: Australia
Publication type &
level of evidence:
Study 3 - multiple baseline cohort study with two control groups and two experimental groups;
each with four children. Two groups assessed at the initial assessment to the end of the intervention
and the other two were assessed from the beginning of intervention to the end of the maintenance
Level III-2
Aim of study:
Establish the efficacy of a suite of speech and language services offered by the Queensland
Department of Education by examining three school based programs.
Population:
16 year 1 and 2 children (age not stated) with proven language impairment described as having a
24 to 36 month delay on the test Analysis of the Language of Learning.
Service setting:
School
Description of
intervention
Service delivery model
(individual/group etc):
4 groups of 4 children
Provider(s):
Speech pathologists
Domain of language:
Metalinguistics in phonology, semantics and syntax
ICF- impairment
Type of intervention:
Method of
intervention:
Activities included Lindamood techniques and tasks that included sound-letter, word awareness
rhyming activities, work book ones, phonology-semantics-syntax absurdities, sound sequencing
and sentence formulation
Quantum of service
provision:
2 x week for 30 minutes each over 8 weeks
Outcomes evaluation
(by disorder subtype
if possible):
Teacher knowledge of speech pathologists
o Not reported
Teacher observations of changes in children
o Children were more eager to engage in pre-literacy tasks
Analysis of the Language of Learning
o Year 1 Change in experimental groups was 16.75 compared with 2 control group
scores of 7.75 and 5.5
o Year 2 Change in experimental groups was 16.62 compared with control group scores
of 2.5 and -9.25
Author’s conclusion:
The program led to changes.
Reviewer’s
conclusion:
The program may have led to changes but the small group sizes may mean that these results are not
significant. Comparison groups were uneven in size and the results were not examined statistically
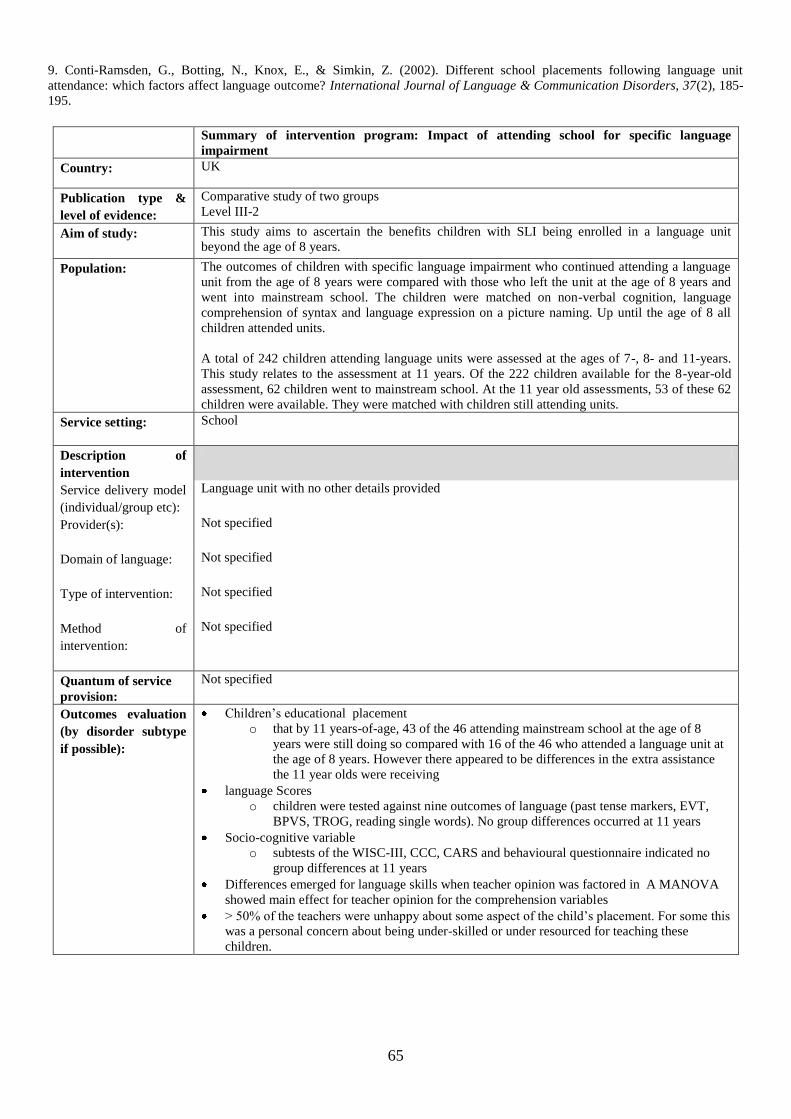
65
9. Conti-Ramsden, G., Botting, N., Knox, E., & Simkin, Z. (2002). Different school placements following language unit
attendance: which factors affect language outcome? International Journal of Language & Communication Disorders, 37(2), 185-
195.
Summary of intervention program: Impact of attending school for specific language
impairment
Country: UK
Publication type &
level of evidence:
Comparative study of two groups
Level III-2
Aim of study:
This study aims to ascertain the benefits children with SLI being enrolled in a language unit
beyond the age of 8 years.
Population:
The outcomes of children with specific language impairment who continued attending a language
unit from the age of 8 years were compared with those who left the unit at the age of 8 years and
went into mainstream school. The children were matched on non-verbal cognition, language
comprehension of syntax and language expression on a picture naming. Up until the age of 8 all
children attended units.
A total of 242 children attending language units were assessed at the ages of 7-, 8- and 11-years.
This study relates to the assessment at 11 years. Of the 222 children available for the 8-year-old
assessment, 62 children went to mainstream school. At the 11 year old assessments, 53 of these 62
children were available. They were matched with children still attending units.
Service setting:
School
Description of
intervention
Service delivery model
(individual/group etc):
Language unit with no other details provided
Provider(s):
Not specified
Domain of language:
Not specified
Type of intervention:
Not specified
Method of
intervention:
Not specified
Quantum of service
provision:
Not specified
Outcomes evaluation
(by disorder subtype
if possible):
Children‟s educational placement
o that by 11 years-of-age, 43 of the 46 attending mainstream school at the age of 8
years were still doing so compared with 16 of the 46 who attended a language unit at
the age of 8 years. However there appeared to be differences in the extra assistance
the 11 year olds were receiving
language Scores
o children were tested against nine outcomes of language (past tense markers, EVT,
BPVS, TROG, reading single words). No group differences occurred at 11 years
Socio-cognitive variable
o subtests of the WISC-III, CCC, CARS and behavioural questionnaire indicated no
group differences at 11 years
Differences emerged for language skills when teacher opinion was factored in A MANOVA
showed main effect for teacher opinion for the comprehension variables
> 50% of the teachers were unhappy about some aspect of the child‟s placement. For some this
was a personal concern about being under-skilled or under resourced for teaching these
children.
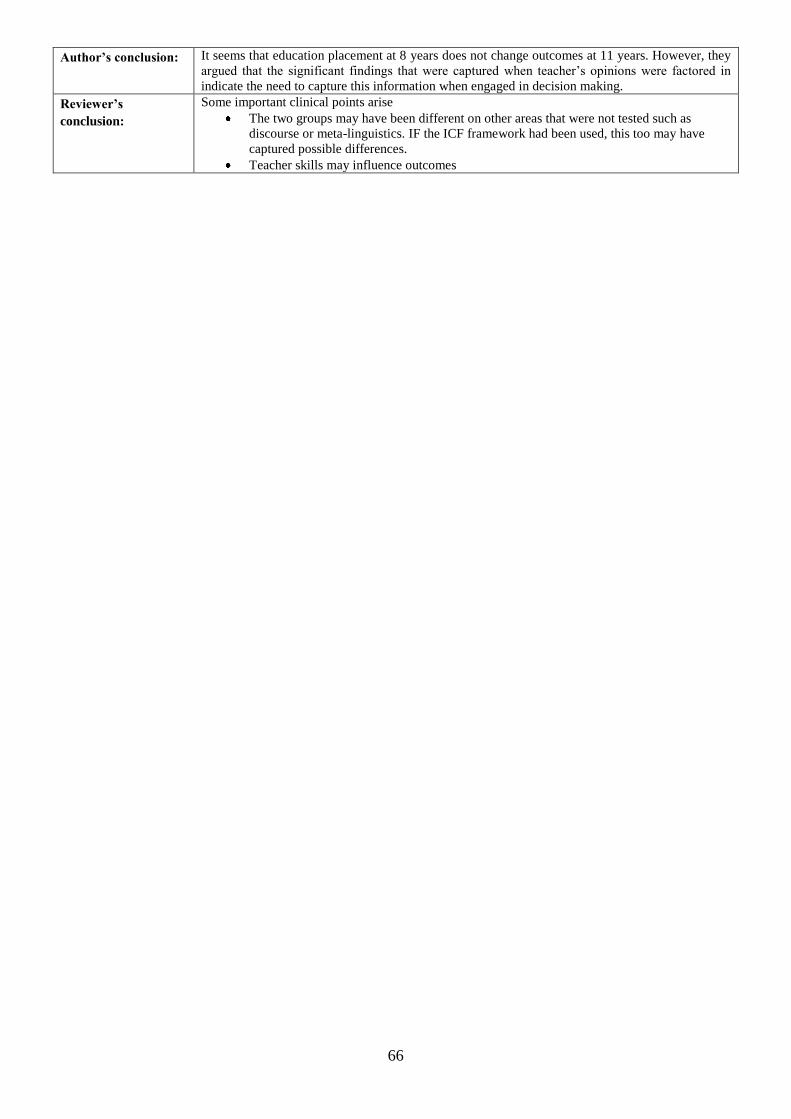
66
Author’s conclusion:
It seems that education placement at 8 years does not change outcomes at 11 years. However, they
argued that the significant findings that were captured when teacher‟s opinions were factored in
indicate the need to capture this information when engaged in decision making.
Reviewer’s
conclusion:
Some important clinical points arise
The two groups may have been different on other areas that were not tested such as
discourse or meta-linguistics. IF the ICF framework had been used, this too may have
captured possible differences.
Teacher skills may influence outcomes
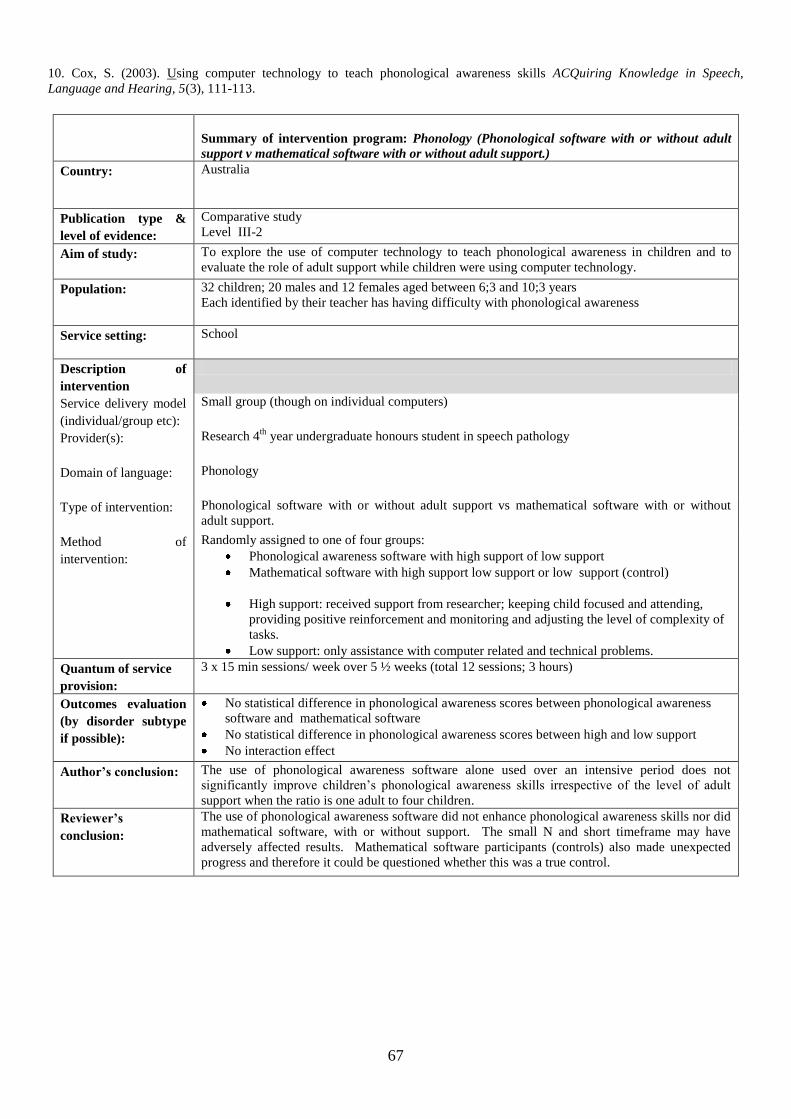
67
10. Cox, S. (2003). Using computer technology to teach phonological awareness skills ACQuiring Knowledge in Speech,
Language and Hearing, 5(3), 111-113.
Summary of intervention program: Phonology (Phonological software with or without adult
support v mathematical software with or without adult support.)
Country: Australia
Publication type &
level of evidence:
Comparative study
Level III-2
Aim of study:
To explore the use of computer technology to teach phonological awareness in children and to
evaluate the role of adult support while children were using computer technology.
Population:
32 children; 20 males and 12 females aged between 6;3 and 10;3 years
Each identified by their teacher has having difficulty with phonological awareness
Service setting:
School
Description of
intervention
Service delivery model
(individual/group etc):
Small group (though on individual computers)
Provider(s):
Research 4th
year undergraduate honours student in speech pathology
Domain of language:
Phonology
Type of intervention:
Phonological software with or without adult support vs mathematical software with or without
adult support.
Method of
intervention:
Randomly assigned to one of four groups:
Phonological awareness software with high support of low support
Mathematical software with high support low support or low support (control)
High support: received support from researcher; keeping child focused and attending,
providing positive reinforcement and monitoring and adjusting the level of complexity of
tasks.
Low support: only assistance with computer related and technical problems.
Quantum of service
provision:
3 x 15 min sessions/ week over 5 ½ weeks (total 12 sessions; 3 hours)
Outcomes evaluation
(by disorder subtype
if possible):
No statistical difference in phonological awareness scores between phonological awareness
software and mathematical software
No statistical difference in phonological awareness scores between high and low support
No interaction effect
Author’s conclusion:
The use of phonological awareness software alone used over an intensive period does not
significantly improve children‟s phonological awareness skills irrespective of the level of adult
support when the ratio is one adult to four children.
Reviewer’s
conclusion:
The use of phonological awareness software did not enhance phonological awareness skills nor did
mathematical software, with or without support. The small N and short timeframe may have
adversely affected results. Mathematical software participants (controls) also made unexpected
progress and therefore it could be questioned whether this was a true control.
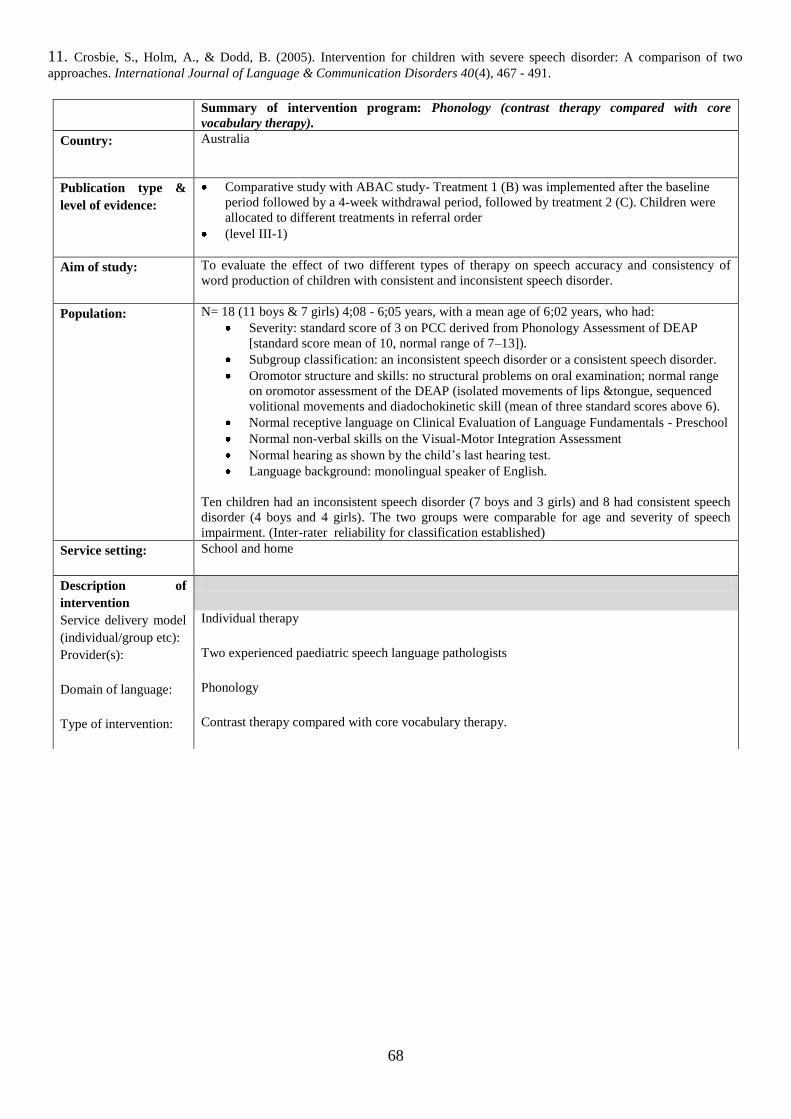
68
11. Crosbie, S., Holm, A., & Dodd, B. (2005). Intervention for children with severe speech disorder: A comparison of two
approaches. International Journal of Language & Communication Disorders 40(4), 467 - 491.
Summary of intervention program: Phonology (contrast therapy compared with core
vocabulary therapy).
Country: Australia
Publication type &
level of evidence:
Comparative study with ABAC study- Treatment 1 (B) was implemented after the baseline
period followed by a 4-week withdrawal period, followed by treatment 2 (C). Children were
allocated to different treatments in referral order
(level III-1)
Aim of study:
To evaluate the effect of two different types of therapy on speech accuracy and consistency of
word production of children with consistent and inconsistent speech disorder.
Population:
N= 18 (11 boys & 7 girls) 4;08 - 6;05 years, with a mean age of 6;02 years, who had:
Severity: standard score of 3 on PCC derived from Phonology Assessment of DEAP
[standard score mean of 10, normal range of 7–13]).
Subgroup classification: an inconsistent speech disorder or a consistent speech disorder.
Oromotor structure and skills: no structural problems on oral examination; normal range
on oromotor assessment of the DEAP (isolated movements of lips &tongue, sequenced
volitional movements and diadochokinetic skill (mean of three standard scores above 6).
Normal receptive language on Clinical Evaluation of Language Fundamentals - Preschool
Normal non-verbal skills on the Visual-Motor Integration Assessment
Normal hearing as shown by the child‟s last hearing test.
Language background: monolingual speaker of English.
Ten children had an inconsistent speech disorder (7 boys and 3 girls) and 8 had consistent speech
disorder (4 boys and 4 girls). The two groups were comparable for age and severity of speech
impairment. (Inter-rater reliability for classification established)
Service setting:
School and home
Description of
intervention
Service delivery model
(individual/group etc):
Individual therapy
Provider(s):
Two experienced paediatric speech language pathologists
Domain of language:
Phonology
Type of intervention:
Contrast therapy compared with core vocabulary therapy.
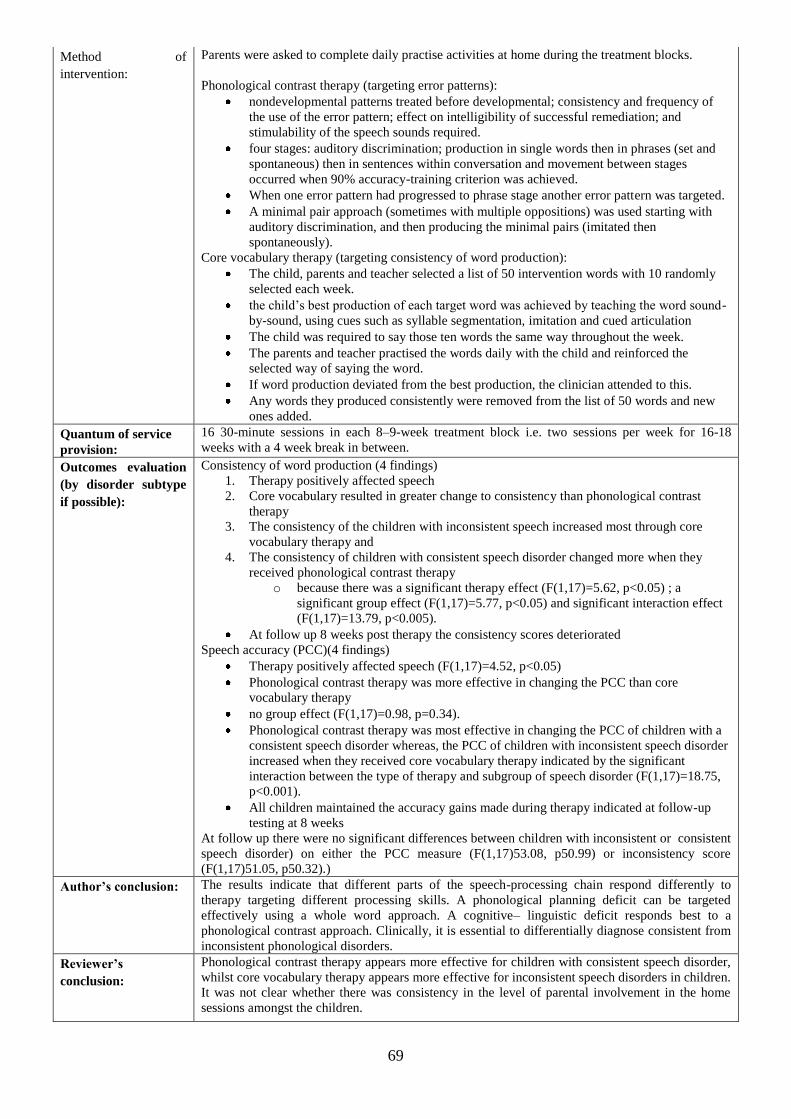
69
Method of
intervention:
Parents were asked to complete daily practise activities at home during the treatment blocks.
Phonological contrast therapy (targeting error patterns):
nondevelopmental patterns treated before developmental; consistency and frequency of
the use of the error pattern; effect on intelligibility of successful remediation; and
stimulability of the speech sounds required.
four stages: auditory discrimination; production in single words then in phrases (set and
spontaneous) then in sentences within conversation and movement between stages
occurred when 90% accuracy-training criterion was achieved.
When one error pattern had progressed to phrase stage another error pattern was targeted.
A minimal pair approach (sometimes with multiple oppositions) was used starting with
auditory discrimination, and then producing the minimal pairs (imitated then
spontaneously).
Core vocabulary therapy (targeting consistency of word production):
The child, parents and teacher selected a list of 50 intervention words with 10 randomly
selected each week.
the child‟s best production of each target word was achieved by teaching the word sound-
by-sound, using cues such as syllable segmentation, imitation and cued articulation
The child was required to say those ten words the same way throughout the week.
The parents and teacher practised the words daily with the child and reinforced the
selected way of saying the word.
If word production deviated from the best production, the clinician attended to this.
Any words they produced consistently were removed from the list of 50 words and new
ones added.
Quantum of service
provision:
16 30-minute sessions in each 8–9-week treatment block i.e. two sessions per week for 16-18
weeks with a 4 week break in between.
Outcomes evaluation
(by disorder subtype
if possible):
Consistency of word production (4 findings)
1. Therapy positively affected speech
2. Core vocabulary resulted in greater change to consistency than phonological contrast
therapy
3. The consistency of the children with inconsistent speech increased most through core
vocabulary therapy and
4. The consistency of children with consistent speech disorder changed more when they
received phonological contrast therapy
o because there was a significant therapy effect (F(1,17)=5.62, p<0.05) ; a
significant group effect (F(1,17)=5.77, p<0.05) and significant interaction effect
(F(1,17)=13.79, p<0.005).
At follow up 8 weeks post therapy the consistency scores deteriorated
Speech accuracy (PCC)(4 findings)
Therapy positively affected speech (F(1,17)=4.52, p<0.05)
Phonological contrast therapy was more effective in changing the PCC than core
vocabulary therapy
no group effect (F(1,17)=0.98, p=0.34).
Phonological contrast therapy was most effective in changing the PCC of children with a
consistent speech disorder whereas, the PCC of children with inconsistent speech disorder
increased when they received core vocabulary therapy indicated by the significant
interaction between the type of therapy and subgroup of speech disorder (F(1,17)=18.75,
p<0.001).
All children maintained the accuracy gains made during therapy indicated at follow-up
testing at 8 weeks
At follow up there were no significant differences between children with inconsistent or consistent
speech disorder) on either the PCC measure (F(1,17)53.08, p50.99) or inconsistency score
(F(1,17)51.05, p50.32).)
Author’s conclusion:
The results indicate that different parts of the speech-processing chain respond differently to
therapy targeting different processing skills. A phonological planning deficit can be targeted
effectively using a whole word approach. A cognitive– linguistic deficit responds best to a
phonological contrast approach. Clinically, it is essential to differentially diagnose consistent from
inconsistent phonological disorders.
Reviewer’s
conclusion:
Phonological contrast therapy appears more effective for children with consistent speech disorder,
whilst core vocabulary therapy appears more effective for inconsistent speech disorders in children.
It was not clear whether there was consistency in the level of parental involvement in the home
sessions amongst the children.
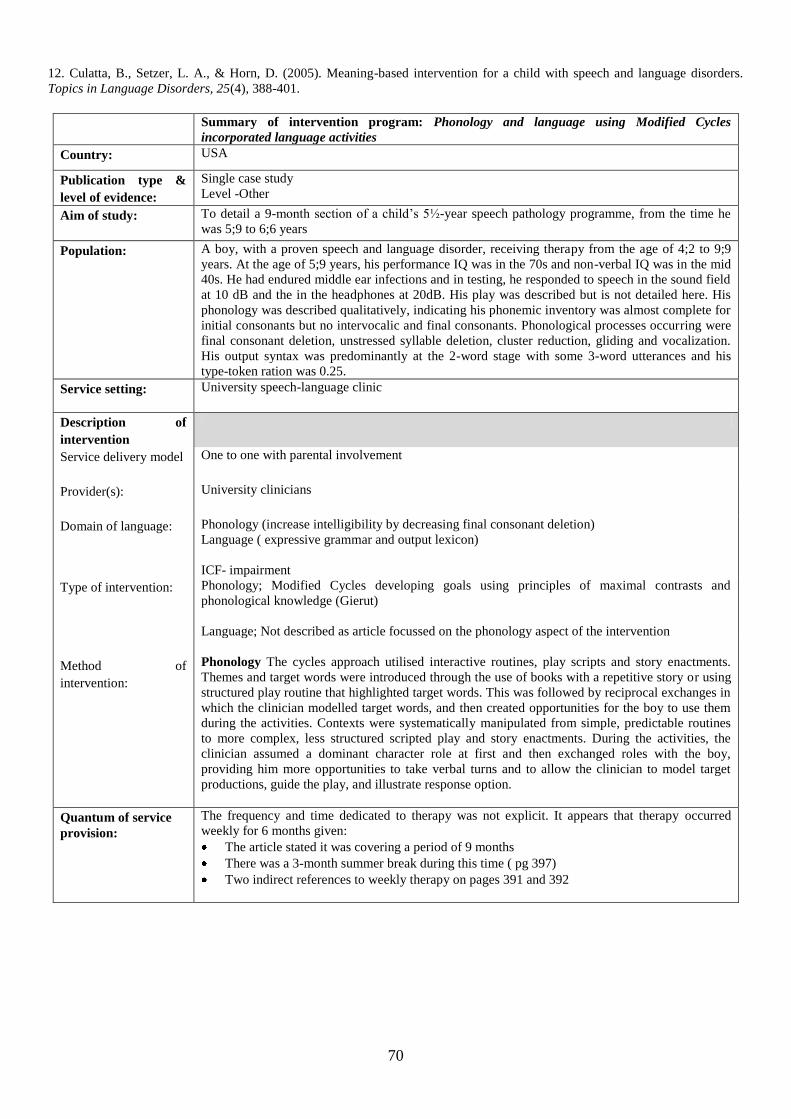
70
12. Culatta, B., Setzer, L. A., & Horn, D. (2005). Meaning-based intervention for a child with speech and language disorders.
Topics in Language Disorders, 25(4), 388-401.
Summary of intervention program: Phonology and language using Modified Cycles
incorporated language activities
Country: USA
Publication type &
level of evidence:
Single case study
Level -Other
Aim of study:
To detail a 9-month section of a child‟s 5½-year speech pathology programme, from the time he
was 5;9 to 6;6 years
Population:
A boy, with a proven speech and language disorder, receiving therapy from the age of 4;2 to 9;9
years. At the age of 5;9 years, his performance IQ was in the 70s and non-verbal IQ was in the mid
40s. He had endured middle ear infections and in testing, he responded to speech in the sound field
at 10 dB and the in the headphones at 20dB. His play was described but is not detailed here. His
phonology was described qualitatively, indicating his phonemic inventory was almost complete for
initial consonants but no intervocalic and final consonants. Phonological processes occurring were
final consonant deletion, unstressed syllable deletion, cluster reduction, gliding and vocalization.
His output syntax was predominantly at the 2-word stage with some 3-word utterances and his
type-token ration was 0.25.
Service setting:
University speech-language clinic
Description of
intervention
Service delivery model
One to one with parental involvement
Provider(s):
University clinicians
Domain of language:
Phonology (increase intelligibility by decreasing final consonant deletion)
Language ( expressive grammar and output lexicon)
ICF- impairment
Type of intervention:
Phonology; Modified Cycles developing goals using principles of maximal contrasts and
phonological knowledge (Gierut)
Language; Not described as article focussed on the phonology aspect of the intervention
Method of
intervention:
Phonology The cycles approach utilised interactive routines, play scripts and story enactments.
Themes and target words were introduced through the use of books with a repetitive story or using
structured play routine that highlighted target words. This was followed by reciprocal exchanges in
which the clinician modelled target words, and then created opportunities for the boy to use them
during the activities. Contexts were systematically manipulated from simple, predictable routines
to more complex, less structured scripted play and story enactments. During the activities, the
clinician assumed a dominant character role at first and then exchanged roles with the boy,
providing him more opportunities to take verbal turns and to allow the clinician to model target
productions, guide the play, and illustrate response option.
Quantum of service
provision:
The frequency and time dedicated to therapy was not explicit. It appears that therapy occurred
weekly for 6 months given:
The article stated it was covering a period of 9 months
There was a 3-month summer break during this time ( pg 397)
Two indirect references to weekly therapy on pages 391 and 392
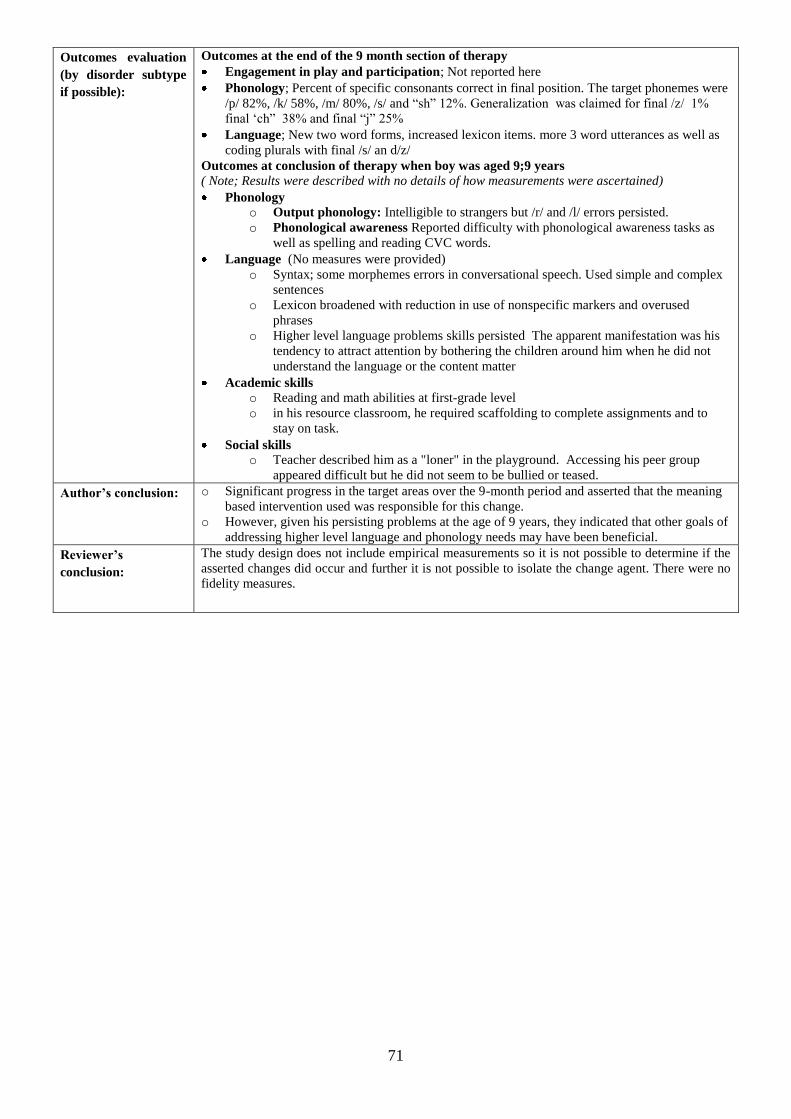
71
Outcomes evaluation
(by disorder subtype
if possible):
Outcomes at the end of the 9 month section of therapy
Engagement in play and participation; Not reported here
Phonology; Percent of specific consonants correct in final position. The target phonemes were
/p/ 82%, /k/ 58%, /m/ 80%, /s/ and “sh” 12%. Generalization was claimed for final /z/ 1%
final „ch” 38% and final “j” 25%
Language; New two word forms, increased lexicon items. more 3 word utterances as well as
coding plurals with final /s/ an d/z/
Outcomes at conclusion of therapy when boy was aged 9;9 years
( Note; Results were described with no details of how measurements were ascertained)
Phonology o Output phonology: Intelligible to strangers but /r/ and /l/ errors persisted.
o Phonological awareness Reported difficulty with phonological awareness tasks as
well as spelling and reading CVC words.
Language (No measures were provided)
o Syntax; some morphemes errors in conversational speech. Used simple and complex
sentences
o Lexicon broadened with reduction in use of nonspecific markers and overused
phrases
o Higher level language problems skills persisted The apparent manifestation was his
tendency to attract attention by bothering the children around him when he did not
understand the language or the content matter
Academic skills o Reading and math abilities at first-grade level
o in his resource classroom, he required scaffolding to complete assignments and to
stay on task.
Social skills o Teacher described him as a "loner" in the playground. Accessing his peer group
appeared difficult but he did not seem to be bullied or teased.
Author’s conclusion:
o Significant progress in the target areas over the 9-month period and asserted that the meaning
based intervention used was responsible for this change.
o However, given his persisting problems at the age of 9 years, they indicated that other goals of
addressing higher level language and phonology needs may have been beneficial.
Reviewer’s
conclusion:
The study design does not include empirical measurements so it is not possible to determine if the
asserted changes did occur and further it is not possible to isolate the change agent. There were no
fidelity measures.
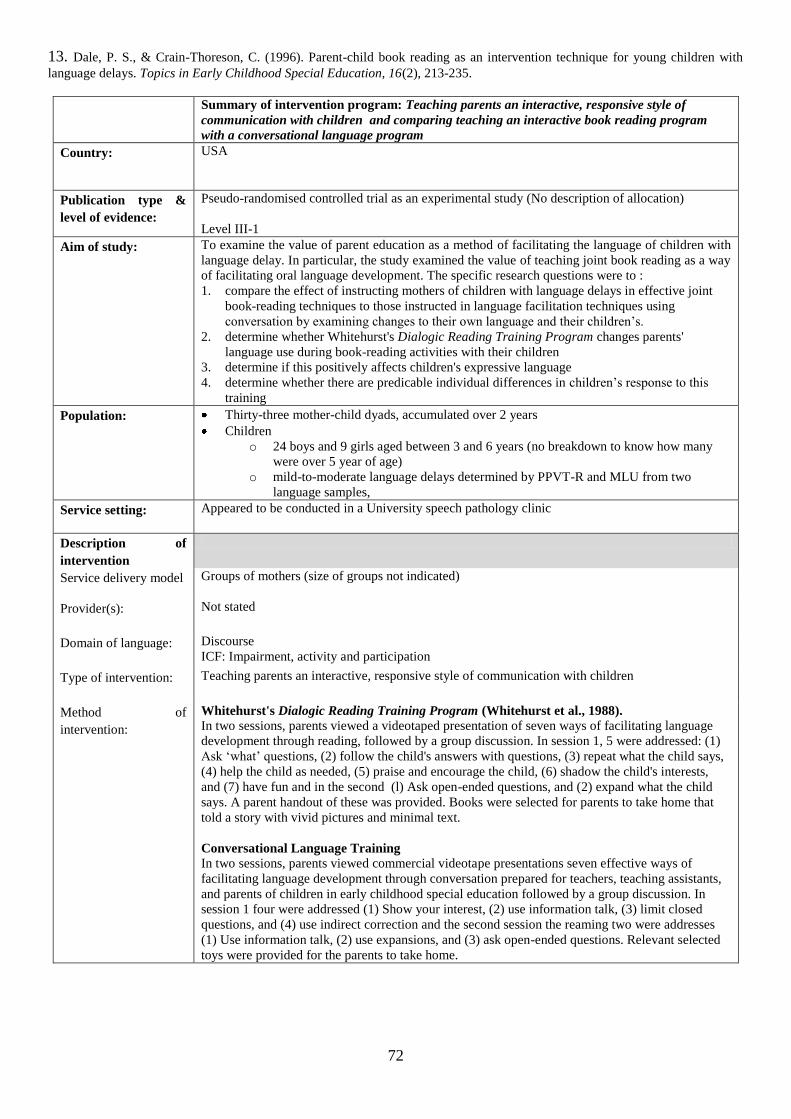
72
13. Dale, P. S., & Crain-Thoreson, C. (1996). Parent-child book reading as an intervention technique for young children with
language delays. Topics in Early Childhood Special Education, 16(2), 213-235.
Summary of intervention program: Teaching parents an interactive, responsive style of
communication with children and comparing teaching an interactive book reading program
with a conversational language program
Country: USA
Publication type &
level of evidence:
Pseudo-randomised controlled trial as an experimental study (No description of allocation)
Level III-1
Aim of study:
To examine the value of parent education as a method of facilitating the language of children with
language delay. In particular, the study examined the value of teaching joint book reading as a way
of facilitating oral language development. The specific research questions were to :
1. compare the effect of instructing mothers of children with language delays in effective joint
book-reading techniques to those instructed in language facilitation techniques using
conversation by examining changes to their own language and their children‟s.
2. determine whether Whitehurst's Dialogic Reading Training Program changes parents'
language use during book-reading activities with their children
3. determine if this positively affects children's expressive language
4. determine whether there are predicable individual differences in children‟s response to this
training
Population:
Thirty-three mother-child dyads, accumulated over 2 years
Children
o 24 boys and 9 girls aged between 3 and 6 years (no breakdown to know how many
were over 5 year of age)
o mild-to-moderate language delays determined by PPVT-R and MLU from two
language samples,
Service setting:
Appeared to be conducted in a University speech pathology clinic
Description of
intervention
Service delivery model Groups of mothers (size of groups not indicated)
Provider(s):
Not stated
Domain of language:
Discourse
ICF: Impairment, activity and participation
Type of intervention:
Teaching parents an interactive, responsive style of communication with children
Method of
intervention:
Whitehurst's Dialogic Reading Training Program (Whitehurst et al., 1988).
In two sessions, parents viewed a videotaped presentation of seven ways of facilitating language
development through reading, followed by a group discussion. In session 1, 5 were addressed: (1)
Ask „what‟ questions, (2) follow the child's answers with questions, (3) repeat what the child says,
(4) help the child as needed, (5) praise and encourage the child, (6) shadow the child's interests,
and (7) have fun and in the second (l) Ask open-ended questions, and (2) expand what the child
says. A parent handout of these was provided. Books were selected for parents to take home that
told a story with vivid pictures and minimal text.
Conversational Language Training
In two sessions, parents viewed commercial videotape presentations seven effective ways of
facilitating language development through conversation prepared for teachers, teaching assistants,
and parents of children in early childhood special education followed by a group discussion. In
session 1 four were addressed (1) Show your interest, (2) use information talk, (3) limit closed
questions, and (4) use indirect correction and the second session the reaming two were addresses
(1) Use information talk, (2) use expansions, and (3) ask open-ended questions. Relevant selected
toys were provided for the parents to take home.
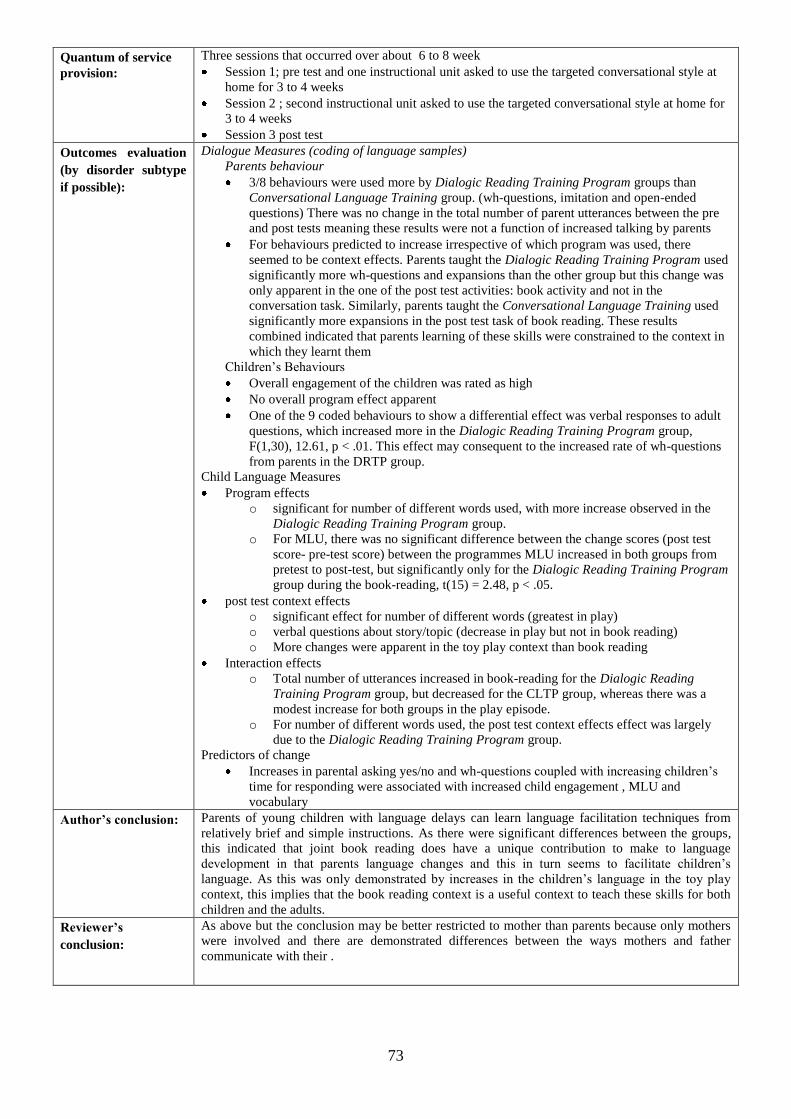
73
Quantum of service
provision:
Three sessions that occurred over about 6 to 8 week
Session 1; pre test and one instructional unit asked to use the targeted conversational style at
home for 3 to 4 weeks
Session 2 ; second instructional unit asked to use the targeted conversational style at home for
3 to 4 weeks
Session 3 post test
Outcomes evaluation
(by disorder subtype
if possible):
Dialogue Measures (coding of language samples)
Parents behaviour
3/8 behaviours were used more by Dialogic Reading Training Program groups than
Conversational Language Training group. (wh-questions, imitation and open-ended
questions) There was no change in the total number of parent utterances between the pre
and post tests meaning these results were not a function of increased talking by parents
For behaviours predicted to increase irrespective of which program was used, there
seemed to be context effects. Parents taught the Dialogic Reading Training Program used
significantly more wh-questions and expansions than the other group but this change was
only apparent in the one of the post test activities: book activity and not in the
conversation task. Similarly, parents taught the Conversational Language Training used
significantly more expansions in the post test task of book reading. These results
combined indicated that parents learning of these skills were constrained to the context in
which they learnt them
Children‟s Behaviours
Overall engagement of the children was rated as high
No overall program effect apparent
One of the 9 coded behaviours to show a differential effect was verbal responses to adult
questions, which increased more in the Dialogic Reading Training Program group,
F(1,30), 12.61, p < .01. This effect may consequent to the increased rate of wh-questions
from parents in the DRTP group.
Child Language Measures
Program effects
o significant for number of different words used, with more increase observed in the
Dialogic Reading Training Program group.
o For MLU, there was no significant difference between the change scores (post test
score- pre-test score) between the programmes MLU increased in both groups from
pretest to post-test, but significantly only for the Dialogic Reading Training Program
group during the book-reading, t(15) = 2.48, p < .05.
post test context effects
o significant effect for number of different words (greatest in play)
o verbal questions about story/topic (decrease in play but not in book reading)
o More changes were apparent in the toy play context than book reading
Interaction effects
o Total number of utterances increased in book-reading for the Dialogic Reading
Training Program group, but decreased for the CLTP group, whereas there was a
modest increase for both groups in the play episode.
o For number of different words used, the post test context effects effect was largely
due to the Dialogic Reading Training Program group.
Predictors of change
Increases in parental asking yes/no and wh-questions coupled with increasing children‟s
time for responding were associated with increased child engagement , MLU and
vocabulary
Author’s conclusion:
Parents of young children with language delays can learn language facilitation techniques from
relatively brief and simple instructions. As there were significant differences between the groups,
this indicated that joint book reading does have a unique contribution to make to language
development in that parents language changes and this in turn seems to facilitate children‟s
language. As this was only demonstrated by increases in the children‟s language in the toy play
context, this implies that the book reading context is a useful context to teach these skills for both
children and the adults.
Reviewer’s
conclusion:
As above but the conclusion may be better restricted to mother than parents because only mothers
were involved and there are demonstrated differences between the ways mothers and father
communicate with their .
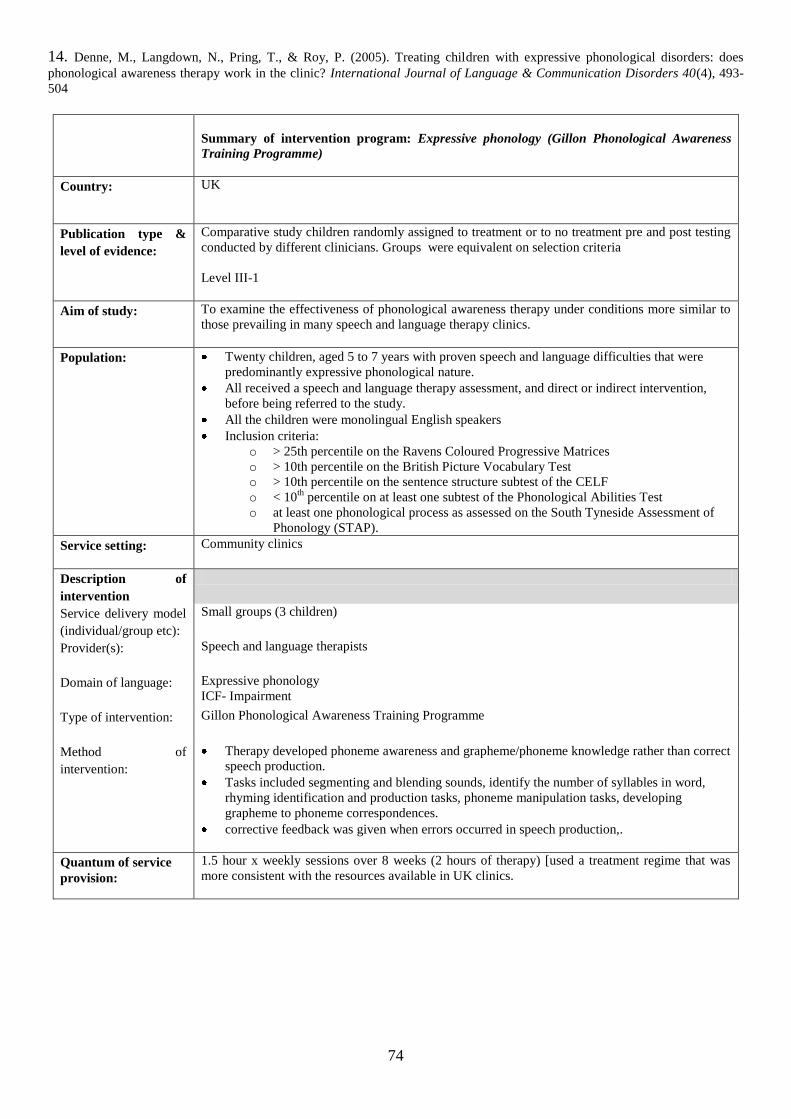
74
14. Denne, M., Langdown, N., Pring, T., & Roy, P. (2005). Treating children with expressive phonological disorders: does
phonological awareness therapy work in the clinic? International Journal of Language & Communication Disorders 40(4), 493-
504
Summary of intervention program: Expressive phonology (Gillon Phonological Awareness
Training Programme)
Country: UK
Publication type &
level of evidence:
Comparative study children randomly assigned to treatment or to no treatment pre and post testing
conducted by different clinicians. Groups were equivalent on selection criteria
Level III-1
Aim of study:
To examine the effectiveness of phonological awareness therapy under conditions more similar to
those prevailing in many speech and language therapy clinics.
Population:
Twenty children, aged 5 to 7 years with proven speech and language difficulties that were
predominantly expressive phonological nature.
All received a speech and language therapy assessment, and direct or indirect intervention,
before being referred to the study.
All the children were monolingual English speakers
Inclusion criteria:
o > 25th percentile on the Ravens Coloured Progressive Matrices
o > 10th percentile on the British Picture Vocabulary Test
o > 10th percentile on the sentence structure subtest of the CELF
o < 10th
percentile on at least one subtest of the Phonological Abilities Test
o at least one phonological process as assessed on the South Tyneside Assessment of
Phonology (STAP).
Service setting:
Community clinics
Description of
intervention
Service delivery model
(individual/group etc):
Small groups (3 children)
Provider(s):
Speech and language therapists
Domain of language:
Expressive phonology
ICF- Impairment
Type of intervention:
Gillon Phonological Awareness Training Programme
Method of
intervention:
Therapy developed phoneme awareness and grapheme/phoneme knowledge rather than correct
speech production.
Tasks included segmenting and blending sounds, identify the number of syllables in word,
rhyming identification and production tasks, phoneme manipulation tasks, developing
grapheme to phoneme correspondences.
corrective feedback was given when errors occurred in speech production,.
Quantum of service
provision:
1.5 hour x weekly sessions over 8 weeks (2 hours of therapy) [used a treatment regime that was
more consistent with the resources available in UK clinics.
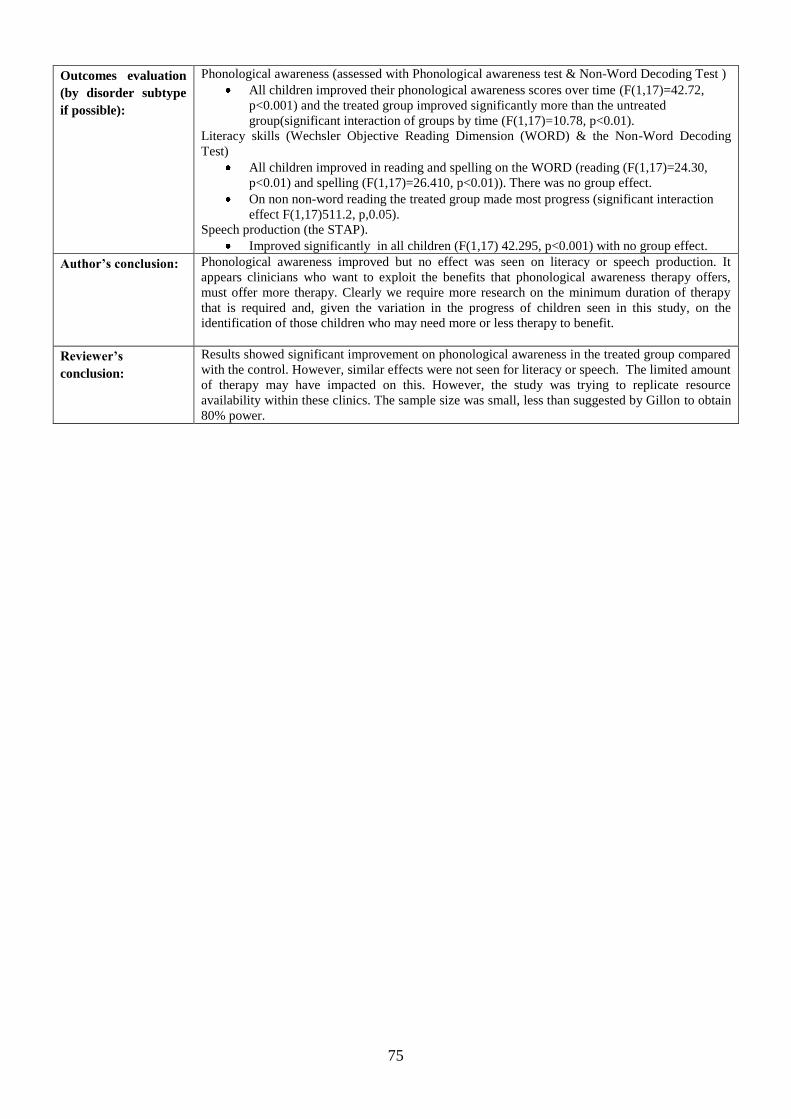
75
Outcomes evaluation
(by disorder subtype
if possible):
Phonological awareness (assessed with Phonological awareness test & Non-Word Decoding Test )
All children improved their phonological awareness scores over time (F(1,17)=42.72,
p<0.001) and the treated group improved significantly more than the untreated
group(significant interaction of groups by time (F(1,17)=10.78, p<0.01).
Literacy skills (Wechsler Objective Reading Dimension (WORD) & the Non-Word Decoding
Test)
All children improved in reading and spelling on the WORD (reading (F(1,17)=24.30,
p<0.01) and spelling (F(1,17)=26.410, p<0.01)). There was no group effect.
On non non-word reading the treated group made most progress (significant interaction
effect F(1,17)511.2, p,0.05).
Speech production (the STAP).
Improved significantly in all children (F(1,17) 42.295, p<0.001) with no group effect.
Author’s conclusion:
Phonological awareness improved but no effect was seen on literacy or speech production. It
appears clinicians who want to exploit the benefits that phonological awareness therapy offers,
must offer more therapy. Clearly we require more research on the minimum duration of therapy
that is required and, given the variation in the progress of children seen in this study, on the
identification of those children who may need more or less therapy to benefit.
Reviewer’s
conclusion:
Results showed significant improvement on phonological awareness in the treated group compared
with the control. However, similar effects were not seen for literacy or speech. The limited amount
of therapy may have impacted on this. However, the study was trying to replicate resource
availability within these clinics. The sample size was small, less than suggested by Gillon to obtain
80% power.
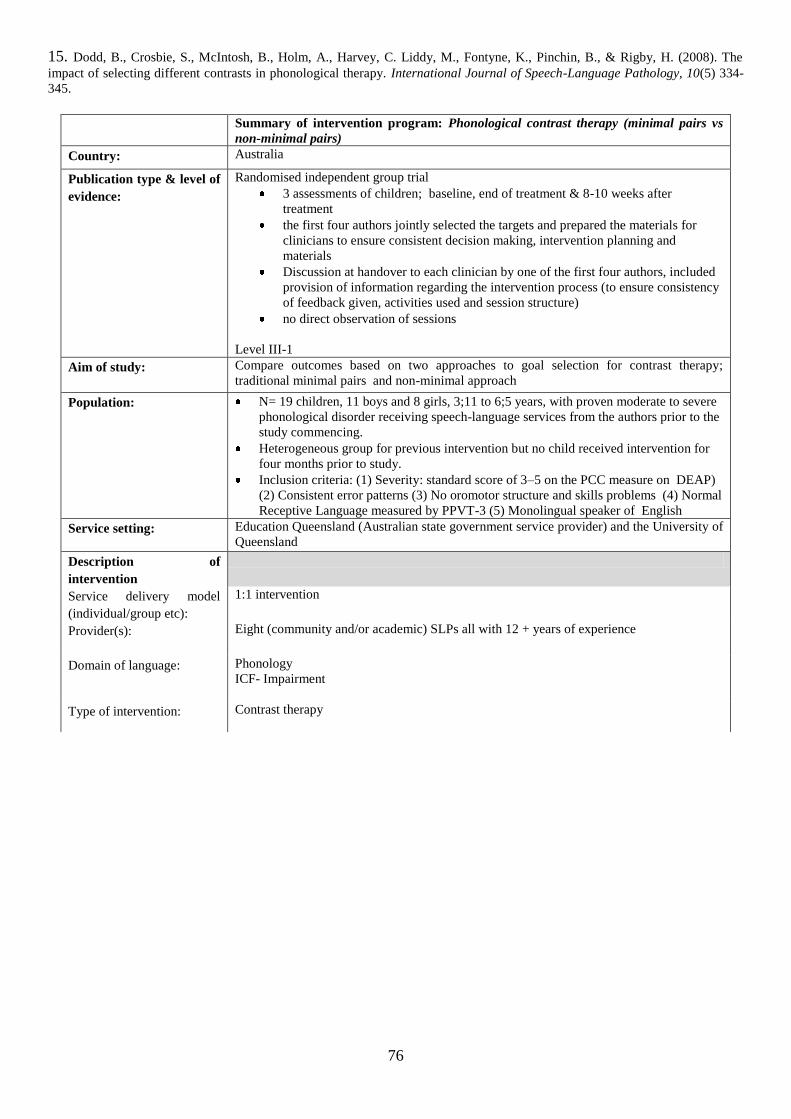
76
15. Dodd, B., Crosbie, S., McIntosh, B., Holm, A., Harvey, C. Liddy, M., Fontyne, K., Pinchin, B., & Rigby, H. (2008). The
impact of selecting different contrasts in phonological therapy. International Journal of Speech-Language Pathology, 10(5) 334-
345.
Summary of intervention program: Phonological contrast therapy (minimal pairs vs
non-minimal pairs)
Country: Australia
Publication type & level of
evidence:
Randomised independent group trial
3 assessments of children; baseline, end of treatment & 8-10 weeks after
treatment
the first four authors jointly selected the targets and prepared the materials for
clinicians to ensure consistent decision making, intervention planning and
materials
Discussion at handover to each clinician by one of the first four authors, included
provision of information regarding the intervention process (to ensure consistency
of feedback given, activities used and session structure)
no direct observation of sessions
Level III-1
Aim of study:
Compare outcomes based on two approaches to goal selection for contrast therapy;
traditional minimal pairs and non-minimal approach
Population:
N= 19 children, 11 boys and 8 girls, 3;11 to 6;5 years, with proven moderate to severe
phonological disorder receiving speech-language services from the authors prior to the
study commencing.
Heterogeneous group for previous intervention but no child received intervention for
four months prior to study.
Inclusion criteria: (1) Severity: standard score of 3–5 on the PCC measure on DEAP)
(2) Consistent error patterns (3) No oromotor structure and skills problems (4) Normal
Receptive Language measured by PPVT-3 (5) Monolingual speaker of English
Service setting:
Education Queensland (Australian state government service provider) and the University of
Queensland
Description of
intervention
Service delivery model
(individual/group etc):
1:1 intervention
Provider(s):
Eight (community and/or academic) SLPs all with 12 + years of experience
Domain of language: Phonology
ICF- Impairment
Type of intervention: Contrast therapy
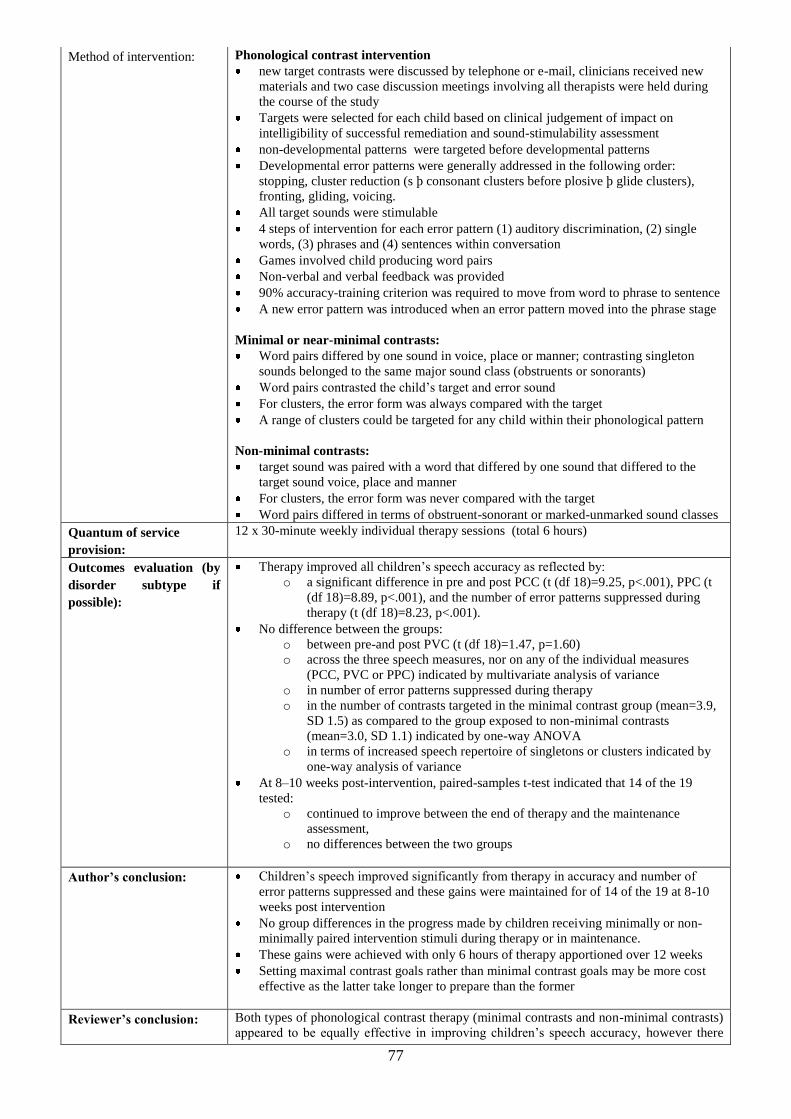
77
Method of intervention:
Phonological contrast intervention
new target contrasts were discussed by telephone or e-mail, clinicians received new
materials and two case discussion meetings involving all therapists were held during
the course of the study
Targets were selected for each child based on clinical judgement of impact on
intelligibility of successful remediation and sound-stimulability assessment
non-developmental patterns were targeted before developmental patterns
Developmental error patterns were generally addressed in the following order:
stopping, cluster reduction (s þ consonant clusters before plosive þ glide clusters),
fronting, gliding, voicing.
All target sounds were stimulable
4 steps of intervention for each error pattern (1) auditory discrimination, (2) single
words, (3) phrases and (4) sentences within conversation
Games involved child producing word pairs
Non-verbal and verbal feedback was provided
90% accuracy-training criterion was required to move from word to phrase to sentence
A new error pattern was introduced when an error pattern moved into the phrase stage
Minimal or near-minimal contrasts:
Word pairs differed by one sound in voice, place or manner; contrasting singleton
sounds belonged to the same major sound class (obstruents or sonorants)
Word pairs contrasted the child‟s target and error sound
For clusters, the error form was always compared with the target
A range of clusters could be targeted for any child within their phonological pattern
Non-minimal contrasts:
target sound was paired with a word that differed by one sound that differed to the
target sound voice, place and manner
For clusters, the error form was never compared with the target
Word pairs differed in terms of obstruent-sonorant or marked-unmarked sound classes
Quantum of service
provision:
12 x 30-minute weekly individual therapy sessions (total 6 hours)
Outcomes evaluation (by
disorder subtype if
possible):
Therapy improved all children‟s speech accuracy as reflected by:
o a significant difference in pre and post PCC (t (df 18)=9.25, p<.001), PPC (t
(df 18)=8.89, p<.001), and the number of error patterns suppressed during
therapy (t (df 18)=8.23, p<.001).
No difference between the groups:
o between pre-and post PVC (t (df 18)=1.47, p=1.60)
o across the three speech measures, nor on any of the individual measures
(PCC, PVC or PPC) indicated by multivariate analysis of variance
o in number of error patterns suppressed during therapy
o in the number of contrasts targeted in the minimal contrast group (mean=3.9,
SD 1.5) as compared to the group exposed to non-minimal contrasts
(mean=3.0, SD 1.1) indicated by one-way ANOVA
o in terms of increased speech repertoire of singletons or clusters indicated by
one-way analysis of variance
At 8–10 weeks post-intervention, paired-samples t-test indicated that 14 of the 19
tested:
o continued to improve between the end of therapy and the maintenance
assessment,
o no differences between the two groups
Author’s conclusion:
Children‟s speech improved significantly from therapy in accuracy and number of
error patterns suppressed and these gains were maintained for of 14 of the 19 at 8-10
weeks post intervention
No group differences in the progress made by children receiving minimally or non-
minimally paired intervention stimuli during therapy or in maintenance.
These gains were achieved with only 6 hours of therapy apportioned over 12 weeks
Setting maximal contrast goals rather than minimal contrast goals may be more cost
effective as the latter take longer to prepare than the former
Reviewer’s conclusion:
Both types of phonological contrast therapy (minimal contrasts and non-minimal contrasts)
appeared to be equally effective in improving children‟s speech accuracy, however there
78
was no control group with which to compare this outcome
Questions arising:
Assumption that previous therapy does not influence later gains so this may have had
an impact
No information on attendance rate and what parents may have done at home
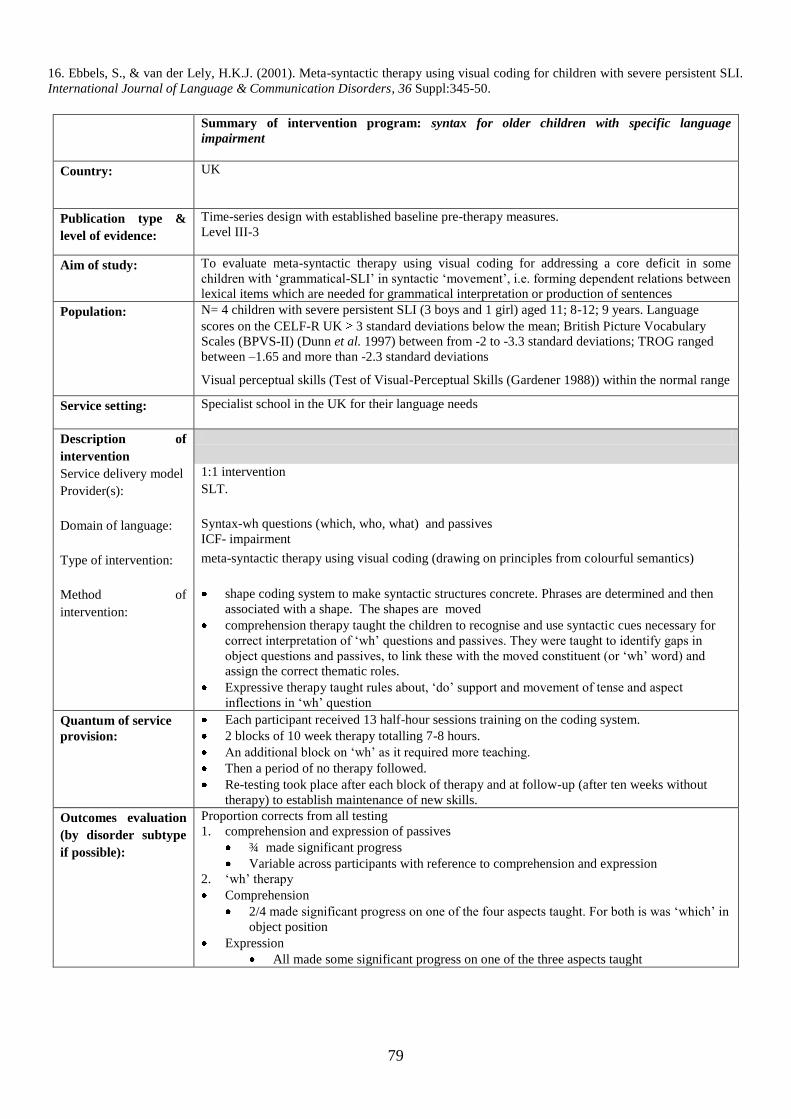
79
16. Ebbels, S., & van der Lely, H.K.J. (2001). Meta-syntactic therapy using visual coding for children with severe persistent SLI.
International Journal of Language & Communication Disorders, 36 Suppl:345-50.
Summary of intervention program: syntax for older children with specific language
impairment
Country: UK
Publication type &
level of evidence:
Time-series design with established baseline pre-therapy measures.
Level III-3
Aim of study:
To evaluate meta-syntactic therapy using visual coding for addressing a core deficit in some
children with „grammatical-SLI‟ in syntactic „movement‟, i.e. forming dependent relations between
lexical items which are needed for grammatical interpretation or production of sentences
Population:
N= 4 children with severe persistent SLI (3 boys and 1 girl) aged 11; 8-12; 9 years. Language
scores on the CELF-R UK 3 standard deviations below the mean; British Picture Vocabulary
Scales (BPVS-II) (Dunn et al. 1997) between from -2 to -3.3 standard deviations; TROG ranged
between –1.65 and more than -2.3 standard deviations
Visual perceptual skills (Test of Visual-Perceptual Skills (Gardener 1988)) within the normal range
Service setting:
Specialist school in the UK for their language needs
Description of
intervention
Service delivery model 1:1 intervention
Provider(s):
SLT.
Domain of language:
Syntax-wh questions (which, who, what) and passives
ICF- impairment
Type of intervention:
meta-syntactic therapy using visual coding (drawing on principles from colourful semantics)
Method of
intervention:
shape coding system to make syntactic structures concrete. Phrases are determined and then
associated with a shape. The shapes are moved
comprehension therapy taught the children to recognise and use syntactic cues necessary for
correct interpretation of „wh‟ questions and passives. They were taught to identify gaps in
object questions and passives, to link these with the moved constituent (or „wh‟ word) and
assign the correct thematic roles.
Expressive therapy taught rules about, „do‟ support and movement of tense and aspect
inflections in „wh‟ question
Quantum of service
provision:
Each participant received 13 half-hour sessions training on the coding system.
2 blocks of 10 week therapy totalling 7-8 hours.
An additional block on „wh‟ as it required more teaching.
Then a period of no therapy followed.
Re-testing took place after each block of therapy and at follow-up (after ten weeks without
therapy) to establish maintenance of new skills.
Outcomes evaluation
(by disorder subtype
if possible):
Proportion corrects from all testing
1. comprehension and expression of passives
¾ made significant progress
Variable across participants with reference to comprehension and expression
2. „wh‟ therapy
Comprehension
2/4 made significant progress on one of the four aspects taught. For both is was „which‟ in
object position
Expression
All made some significant progress on one of the three aspects taught

80
Author’s conclusion:
Meta-syntactic therapy using visual coding was effective in improving the performance of at least
three out of four participants. The aspect of grammar that it seemed to assist was comprehension of
grammatical structures which involve „movement‟ involving dependent structural knowledge
between sentence constituents.
Reviewer’s
conclusion:
Meta-syntactic therapy using visual coding was effective in bringing about some change in
comprehension. This is significant given the resistance to change that has been reported. The
observation that change seemed selective to just some of the aspects implies that different aspects
of grammar may need different interventions and adds to the consensus of the need for
individualised planning that targets the deficit. This is an important study is that it is one of the few
that focus on children, older than 8 years.
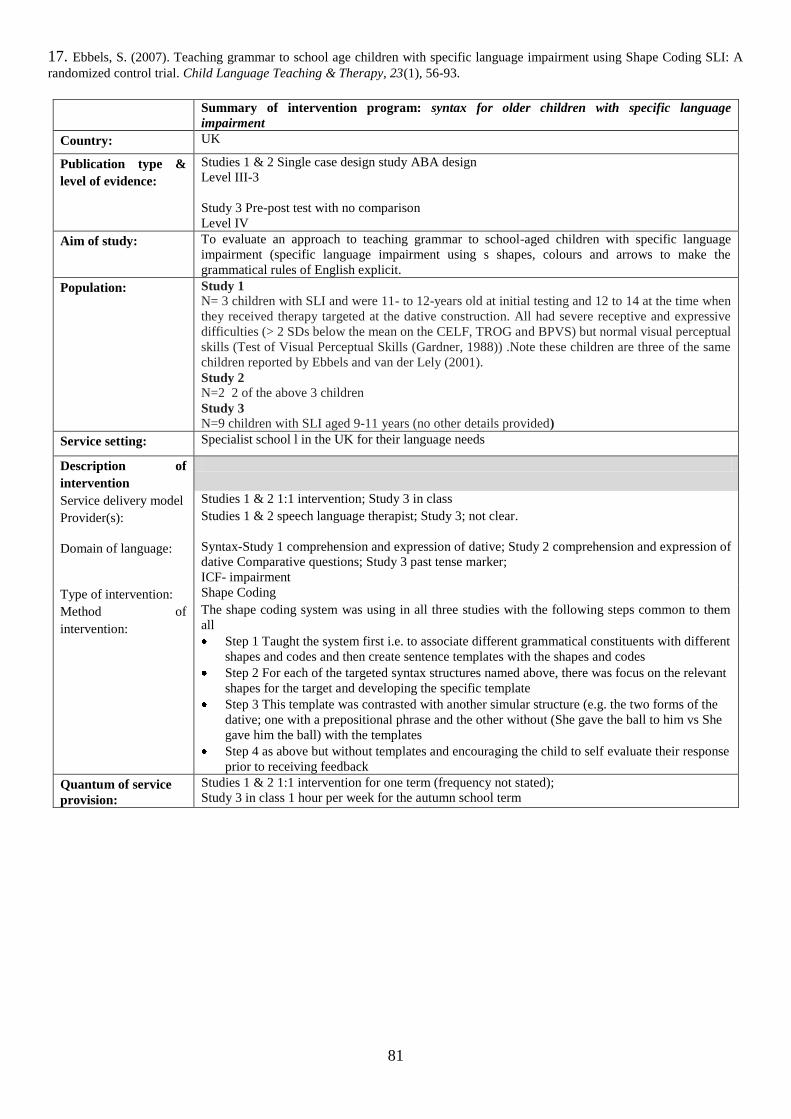
81
17. Ebbels, S. (2007). Teaching grammar to school age children with specific language impairment using Shape Coding SLI: A
randomized control trial. Child Language Teaching & Therapy, 23(1), 56-93.
Summary of intervention program: syntax for older children with specific language
impairment
Country: UK
Publication type &
level of evidence:
Studies 1 & 2 Single case design study ABA design
Level III-3
Study 3 Pre-post test with no comparison
Level IV
Aim of study:
To evaluate an approach to teaching grammar to school-aged children with specific language
impairment (specific language impairment using s shapes, colours and arrows to make the
grammatical rules of English explicit.
Population:
Study 1
N= 3 children with SLI and were 11- to 12-years old at initial testing and 12 to 14 at the time when
they received therapy targeted at the dative construction. All had severe receptive and expressive
difficulties (> 2 SDs below the mean on the CELF, TROG and BPVS) but normal visual perceptual
skills (Test of Visual Perceptual Skills (Gardner, 1988)) .Note these children are three of the same
children reported by Ebbels and van der Lely (2001).
Study 2
N=2 2 of the above 3 children
Study 3
N=9 children with SLI aged 9-11 years (no other details provided)
Service setting: Specialist school l in the UK for their language needs
Description of
intervention
Service delivery model Studies 1 & 2 1:1 intervention; Study 3 in class
Provider(s): Studies 1 & 2 speech language therapist; Study 3; not clear.
Domain of language:
Syntax-Study 1 comprehension and expression of dative; Study 2 comprehension and expression of
dative Comparative questions; Study 3 past tense marker;
ICF- impairment
Type of intervention: Shape Coding
Method of
intervention:
The shape coding system was using in all three studies with the following steps common to them
all
Step 1 Taught the system first i.e. to associate different grammatical constituents with different
shapes and codes and then create sentence templates with the shapes and codes
Step 2 For each of the targeted syntax structures named above, there was focus on the relevant
shapes for the target and developing the specific template
Step 3 This template was contrasted with another simular structure (e.g. the two forms of the
dative; one with a prepositional phrase and the other without (She gave the ball to him vs She
gave him the ball) with the templates
Step 4 as above but without templates and encouraging the child to self evaluate their response
prior to receiving feedback
Quantum of service
provision:
Studies 1 & 2 1:1 intervention for one term (frequency not stated);
Study 3 in class 1 hour per week for the autumn school term
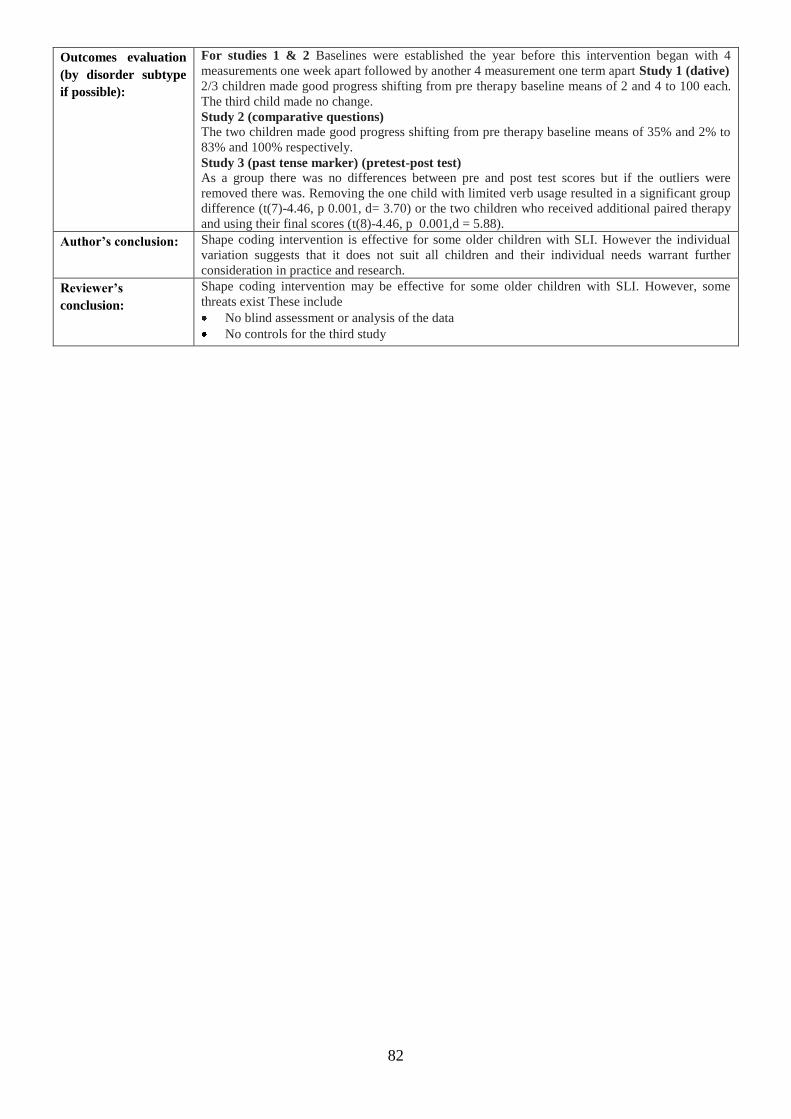
82
Outcomes evaluation
(by disorder subtype
if possible):
For studies 1 & 2 Baselines were established the year before this intervention began with 4
measurements one week apart followed by another 4 measurement one term apart Study 1 (dative)
2/3 children made good progress shifting from pre therapy baseline means of 2 and 4 to 100 each.
The third child made no change.
Study 2 (comparative questions)
The two children made good progress shifting from pre therapy baseline means of 35% and 2% to
83% and 100% respectively.
Study 3 (past tense marker) (pretest-post test)
As a group there was no differences between pre and post test scores but if the outliers were
removed there was. Removing the one child with limited verb usage resulted in a significant group
difference (t(7)-4.46, p 0.001, d= 3.70) or the two children who received additional paired therapy
and using their final scores (t(8)-4.46, p 0.001,d = 5.88).
Author’s conclusion:
Shape coding intervention is effective for some older children with SLI. However the individual
variation suggests that it does not suit all children and their individual needs warrant further
consideration in practice and research.
Reviewer’s
conclusion:
Shape coding intervention may be effective for some older children with SLI. However, some
threats exist These include
No blind assessment or analysis of the data
No controls for the third study
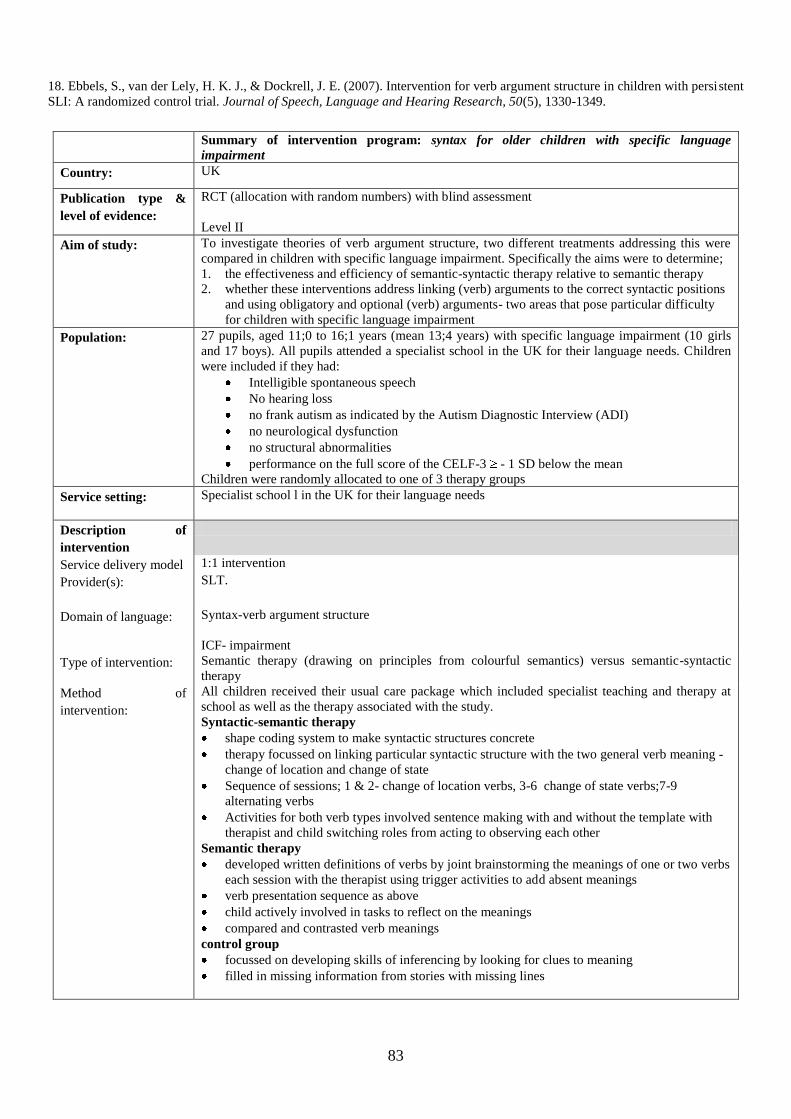
83
18. Ebbels, S., van der Lely, H. K. J., & Dockrell, J. E. (2007). Intervention for verb argument structure in children with persistent
SLI: A randomized control trial. Journal of Speech, Language and Hearing Research, 50(5), 1330-1349.
Summary of intervention program: syntax for older children with specific language
impairment
Country: UK
Publication type &
level of evidence:
RCT (allocation with random numbers) with blind assessment
Level II
Aim of study:
To investigate theories of verb argument structure, two different treatments addressing this were
compared in children with specific language impairment. Specifically the aims were to determine;
1. the effectiveness and efficiency of semantic-syntactic therapy relative to semantic therapy
2. whether these interventions address linking (verb) arguments to the correct syntactic positions
and using obligatory and optional (verb) arguments- two areas that pose particular difficulty
for children with specific language impairment
Population:
27 pupils, aged 11;0 to 16;1 years (mean 13;4 years) with specific language impairment (10 girls
and 17 boys). All pupils attended a specialist school in the UK for their language needs. Children
were included if they had:
Intelligible spontaneous speech
No hearing loss
no frank autism as indicated by the Autism Diagnostic Interview (ADI)
no neurological dysfunction
no structural abnormalities
performance on the full score of the CELF-3 - 1 SD below the mean
Children were randomly allocated to one of 3 therapy groups
Service setting:
Specialist school l in the UK for their language needs
Description of
intervention
Service delivery model 1:1 intervention
Provider(s):
SLT.
Domain of language:
Syntax-verb argument structure
ICF- impairment
Type of intervention: Semantic therapy (drawing on principles from colourful semantics) versus semantic-syntactic
therapy
Method of
intervention:
All children received their usual care package which included specialist teaching and therapy at
school as well as the therapy associated with the study.
Syntactic-semantic therapy
shape coding system to make syntactic structures concrete
therapy focussed on linking particular syntactic structure with the two general verb meaning -
change of location and change of state
Sequence of sessions; 1 & 2- change of location verbs, 3-6 change of state verbs;7-9
alternating verbs
Activities for both verb types involved sentence making with and without the template with
therapist and child switching roles from acting to observing each other
Semantic therapy
developed written definitions of verbs by joint brainstorming the meanings of one or two verbs
each session with the therapist using trigger activities to add absent meanings
verb presentation sequence as above
child actively involved in tasks to reflect on the meanings
compared and contrasted verb meanings
control group
focussed on developing skills of inferencing by looking for clues to meaning
filled in missing information from stories with missing lines
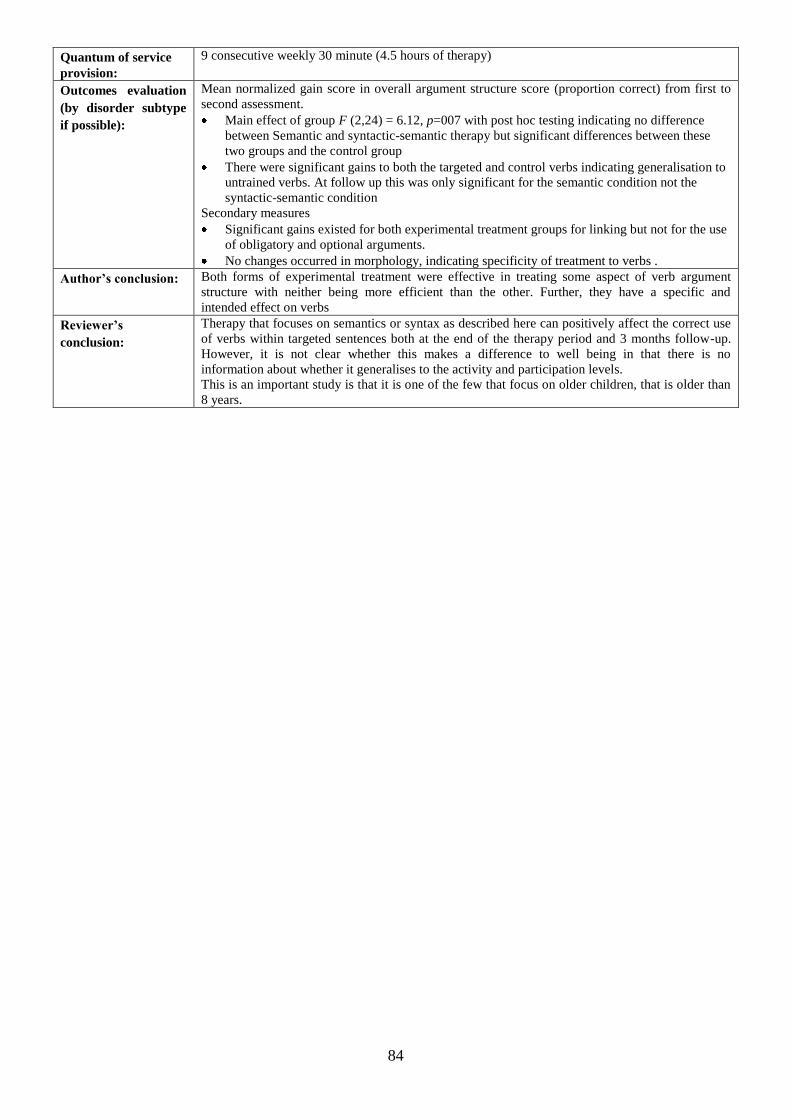
84
Quantum of service
provision:
9 consecutive weekly 30 minute (4.5 hours of therapy)
Outcomes evaluation
(by disorder subtype
if possible):
Mean normalized gain score in overall argument structure score (proportion correct) from first to
second assessment.
Main effect of group F (2,24) = 6.12, p=007 with post hoc testing indicating no difference
between Semantic and syntactic-semantic therapy but significant differences between these
two groups and the control group
There were significant gains to both the targeted and control verbs indicating generalisation to
untrained verbs. At follow up this was only significant for the semantic condition not the
syntactic-semantic condition
Secondary measures
Significant gains existed for both experimental treatment groups for linking but not for the use
of obligatory and optional arguments.
No changes occurred in morphology, indicating specificity of treatment to verbs .
Author’s conclusion:
Both forms of experimental treatment were effective in treating some aspect of verb argument
structure with neither being more efficient than the other. Further, they have a specific and
intended effect on verbs
Reviewer’s
conclusion:
Therapy that focuses on semantics or syntax as described here can positively affect the correct use
of verbs within targeted sentences both at the end of the therapy period and 3 months follow-up.
However, it is not clear whether this makes a difference to well being in that there is no
information about whether it generalises to the activity and participation levels.
This is an important study is that it is one of the few that focus on older children, that is older than
8 years.
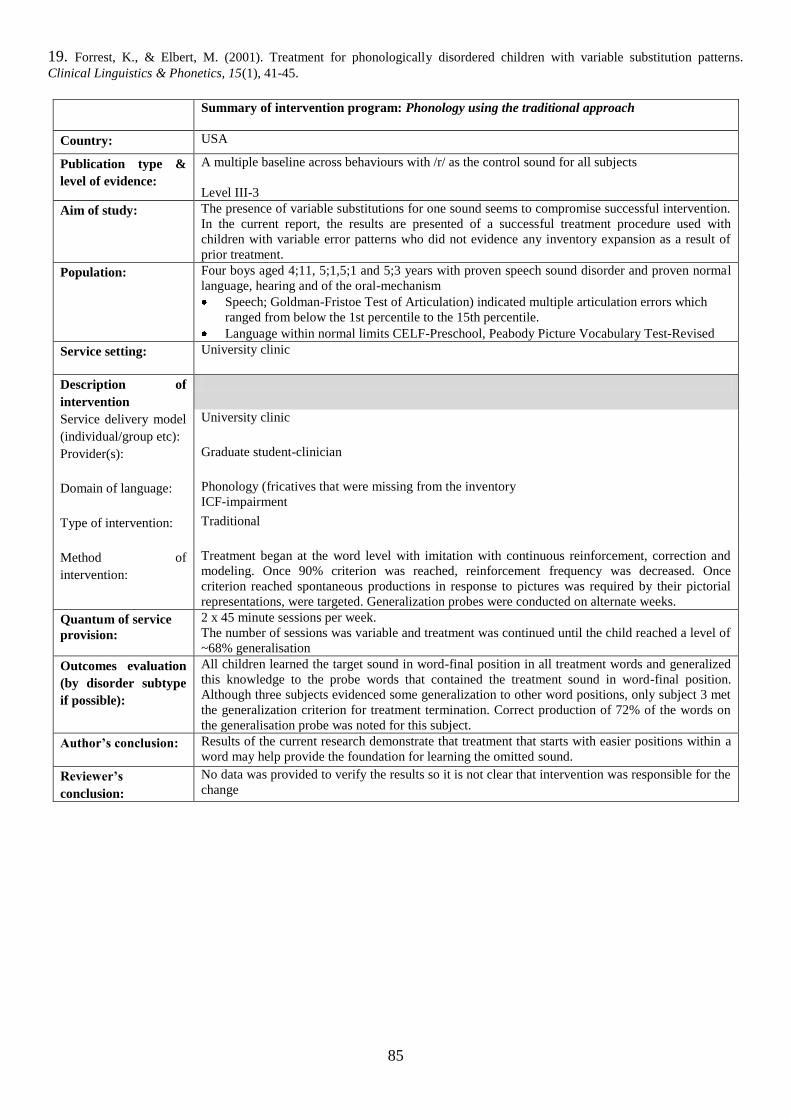
85
19. Forrest, K., & Elbert, M. (2001). Treatment for phonologically disordered children with variable substitution patterns.
Clinical Linguistics & Phonetics, 15(1), 41-45.
Summary of intervention program: Phonology using the traditional approach
Country: USA
Publication type &
level of evidence:
A multiple baseline across behaviours with /r/ as the control sound for all subjects
Level III-3
Aim of study:
The presence of variable substitutions for one sound seems to compromise successful intervention.
In the current report, the results are presented of a successful treatment procedure used with
children with variable error patterns who did not evidence any inventory expansion as a result of
prior treatment.
Population:
Four boys aged 4;11, 5;1,5;1 and 5;3 years with proven speech sound disorder and proven normal
language, hearing and of the oral-mechanism
Speech; Goldman-Fristoe Test of Articulation) indicated multiple articulation errors which
ranged from below the 1st percentile to the 15th percentile.
Language within normal limits CELF-Preschool, Peabody Picture Vocabulary Test-Revised
Service setting:
University clinic
Description of
intervention
Service delivery model
(individual/group etc):
University clinic
Provider(s):
Graduate student-clinician
Domain of language:
Phonology (fricatives that were missing from the inventory
ICF-impairment
Type of intervention:
Traditional
Method of
intervention:
Treatment began at the word level with imitation with continuous reinforcement, correction and
modeling. Once 90% criterion was reached, reinforcement frequency was decreased. Once
criterion reached spontaneous productions in response to pictures was required by their pictorial
representations, were targeted. Generalization probes were conducted on alternate weeks.
Quantum of service
provision:
2 x 45 minute sessions per week.
The number of sessions was variable and treatment was continued until the child reached a level of
~68% generalisation
Outcomes evaluation
(by disorder subtype
if possible):
All children learned the target sound in word-final position in all treatment words and generalized
this knowledge to the probe words that contained the treatment sound in word-final position.
Although three subjects evidenced some generalization to other word positions, only subject 3 met
the generalization criterion for treatment termination. Correct production of 72% of the words on
the generalisation probe was noted for this subject.
Author’s conclusion:
Results of the current research demonstrate that treatment that starts with easier positions within a
word may help provide the foundation for learning the omitted sound.
Reviewer’s
conclusion:
No data was provided to verify the results so it is not clear that intervention was responsible for the
change
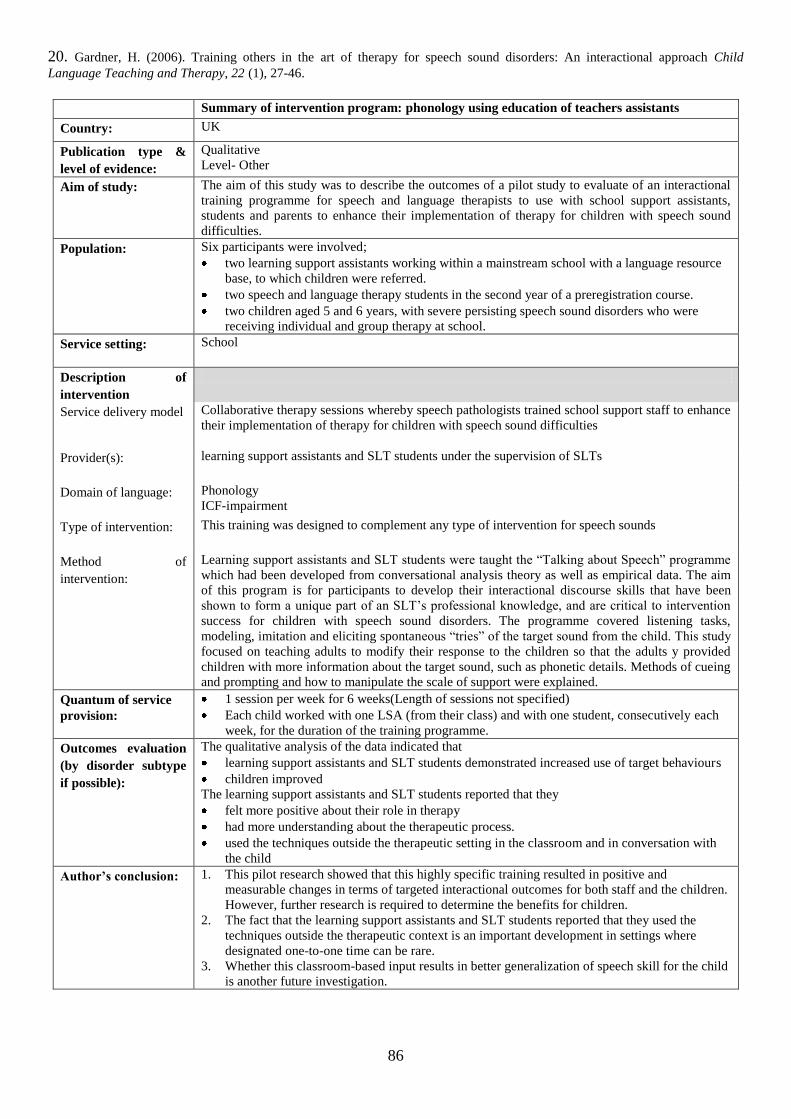
86
20. Gardner, H. (2006). Training others in the art of therapy for speech sound disorders: An interactional approach Child
Language Teaching and Therapy, 22 (1), 27-46.
Summary of intervention program: phonology using education of teachers assistants
Country: UK
Publication type &
level of evidence:
Qualitative
Level- Other
Aim of study:
The aim of this study was to describe the outcomes of a pilot study to evaluate of an interactional
training programme for speech and language therapists to use with school support assistants,
students and parents to enhance their implementation of therapy for children with speech sound
difficulties.
Population:
Six participants were involved;
two learning support assistants working within a mainstream school with a language resource
base, to which children were referred.
two speech and language therapy students in the second year of a preregistration course.
two children aged 5 and 6 years, with severe persisting speech sound disorders who were
receiving individual and group therapy at school.
Service setting:
School
Description of
intervention
Service delivery model Collaborative therapy sessions whereby speech pathologists trained school support staff to enhance
their implementation of therapy for children with speech sound difficulties
Provider(s):
learning support assistants and SLT students under the supervision of SLTs
Domain of language:
Phonology
ICF-impairment
Type of intervention:
This training was designed to complement any type of intervention for speech sounds
Method of
intervention:
Learning support assistants and SLT students were taught the “Talking about Speech” programme
which had been developed from conversational analysis theory as well as empirical data. The aim
of this program is for participants to develop their interactional discourse skills that have been
shown to form a unique part of an SLT‟s professional knowledge, and are critical to intervention
success for children with speech sound disorders. The programme covered listening tasks,
modeling, imitation and eliciting spontaneous “tries” of the target sound from the child. This study
focused on teaching adults to modify their response to the children so that the adults y provided
children with more information about the target sound, such as phonetic details. Methods of cueing
and prompting and how to manipulate the scale of support were explained.
Quantum of service
provision:
1 session per week for 6 weeks(Length of sessions not specified)
Each child worked with one LSA (from their class) and with one student, consecutively each
week, for the duration of the training programme.
Outcomes evaluation
(by disorder subtype
if possible):
The qualitative analysis of the data indicated that
learning support assistants and SLT students demonstrated increased use of target behaviours
children improved
The learning support assistants and SLT students reported that they
felt more positive about their role in therapy
had more understanding about the therapeutic process.
used the techniques outside the therapeutic setting in the classroom and in conversation with
the child
Author’s conclusion:
1. This pilot research showed that this highly specific training resulted in positive and
measurable changes in terms of targeted interactional outcomes for both staff and the children.
However, further research is required to determine the benefits for children.
2. The fact that the learning support assistants and SLT students reported that they used the
techniques outside the therapeutic context is an important development in settings where
designated one-to-one time can be rare.
3. Whether this classroom-based input results in better generalization of speech skill for the child
is another future investigation.
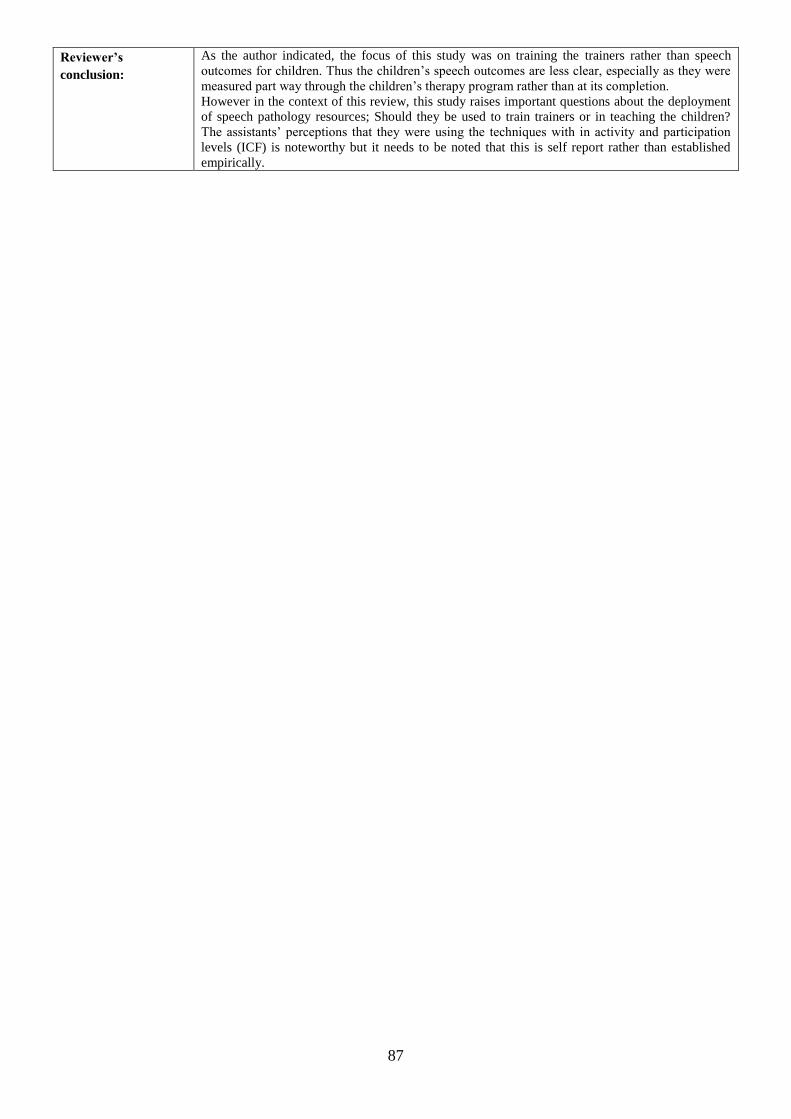
87
Reviewer’s
conclusion:
As the author indicated, the focus of this study was on training the trainers rather than speech
outcomes for children. Thus the children‟s speech outcomes are less clear, especially as they were
measured part way through the children‟s therapy program rather than at its completion.
However in the context of this review, this study raises important questions about the deployment
of speech pathology resources; Should they be used to train trainers or in teaching the children?
The assistants‟ perceptions that they were using the techniques with in activity and participation
levels (ICF) is noteworthy but it needs to be noted that this is self report rather than established
empirically.
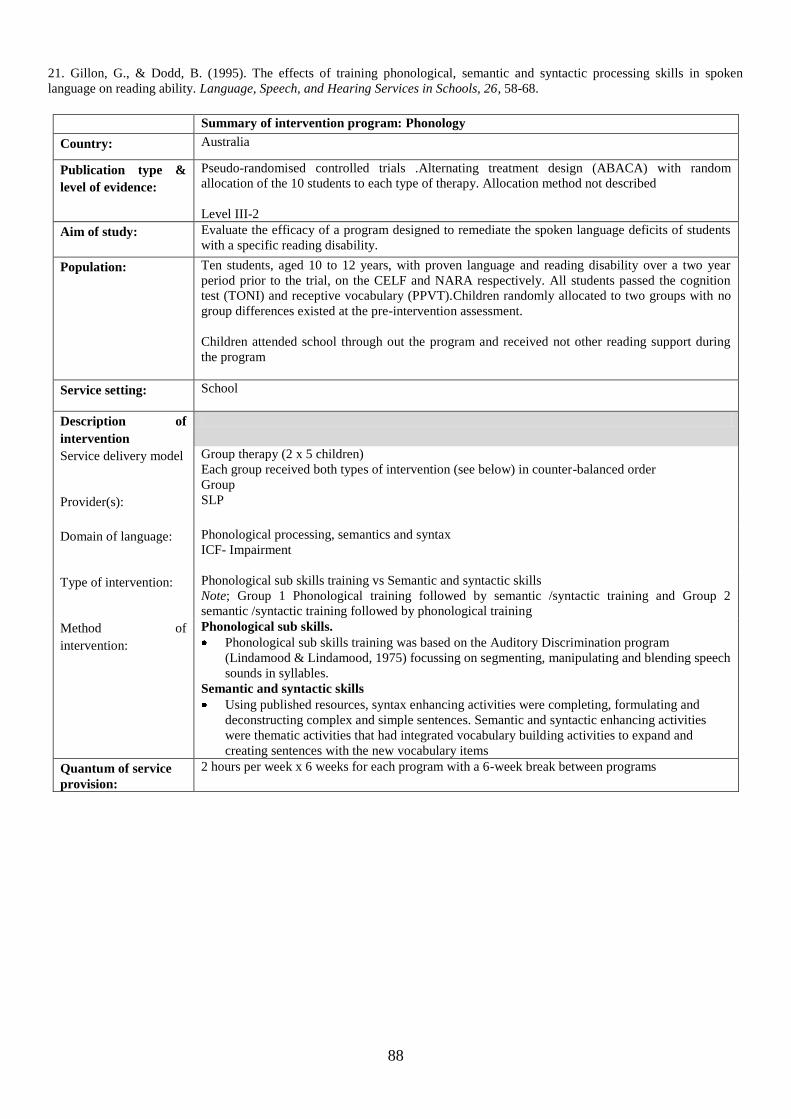
88
21. Gillon, G., & Dodd, B. (1995). The effects of training phonological, semantic and syntactic processing skills in spoken
language on reading ability. Language, Speech, and Hearing Services in Schools, 26, 58-68.
Summary of intervention program: Phonology
Country: Australia
Publication type &
level of evidence:
Pseudo-randomised controlled trials .Alternating treatment design (ABACA) with random
allocation of the 10 students to each type of therapy. Allocation method not described
Level III-2
Aim of study:
Evaluate the efficacy of a program designed to remediate the spoken language deficits of students
with a specific reading disability.
Population:
Ten students, aged 10 to 12 years, with proven language and reading disability over a two year
period prior to the trial, on the CELF and NARA respectively. All students passed the cognition
test (TONI) and receptive vocabulary (PPVT).Children randomly allocated to two groups with no
group differences existed at the pre-intervention assessment.
Children attended school through out the program and received not other reading support during
the program
Service setting: School
Description of
intervention
Service delivery model
Group therapy (2 x 5 children)
Each group received both types of intervention (see below) in counter-balanced order
Group
Provider(s):
SLP
Domain of language:
Phonological processing, semantics and syntax
ICF- Impairment
Type of intervention:
Phonological sub skills training vs Semantic and syntactic skills
Note; Group 1 Phonological training followed by semantic /syntactic training and Group 2
semantic /syntactic training followed by phonological training
Method of
intervention:
Phonological sub skills.
Phonological sub skills training was based on the Auditory Discrimination program
(Lindamood & Lindamood, 1975) focussing on segmenting, manipulating and blending speech
sounds in syllables.
Semantic and syntactic skills
Using published resources, syntax enhancing activities were completing, formulating and
deconstructing complex and simple sentences. Semantic and syntactic enhancing activities
were thematic activities that had integrated vocabulary building activities to expand and
creating sentences with the new vocabulary items
Quantum of service
provision:
2 hours per week x 6 weeks for each program with a 6-week break between programs
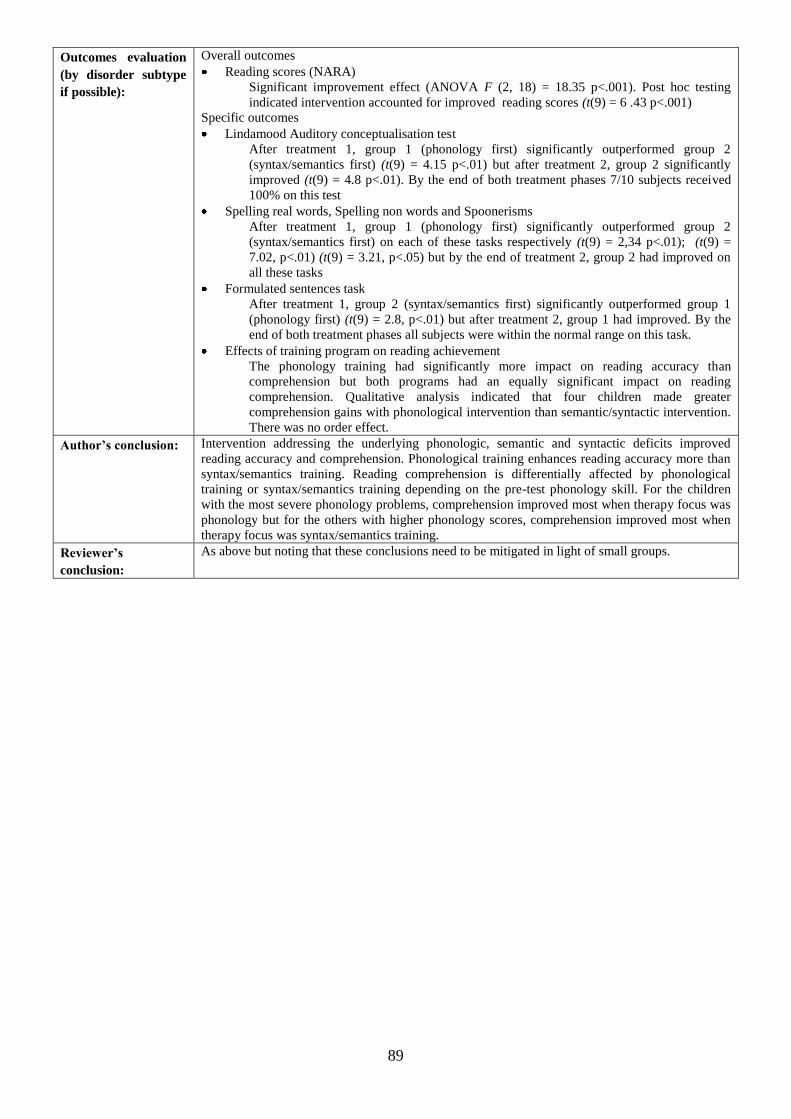
89
Outcomes evaluation
(by disorder subtype
if possible):
Overall outcomes
Reading scores (NARA)
Significant improvement effect (ANOVA F (2, 18) = 18.35 p<.001). Post hoc testing
indicated intervention accounted for improved reading scores (t(9) = 6 .43 p<.001)
Specific outcomes
Lindamood Auditory conceptualisation test
After treatment 1, group 1 (phonology first) significantly outperformed group 2
(syntax/semantics first) (t(9) = 4.15 p<.01) but after treatment 2, group 2 significantly
improved (t(9) = 4.8 p<.01). By the end of both treatment phases 7/10 subjects received
100% on this test
Spelling real words, Spelling non words and Spoonerisms
After treatment 1, group 1 (phonology first) significantly outperformed group 2
(syntax/semantics first) on each of these tasks respectively (t(9) = 2,34 p<.01); (t(9) =
7.02, p<.01) (t(9) = 3.21, p<.05) but by the end of treatment 2, group 2 had improved on
all these tasks
Formulated sentences task
After treatment 1, group 2 (syntax/semantics first) significantly outperformed group 1
(phonology first) (t(9) = 2.8, p<.01) but after treatment 2, group 1 had improved. By the
end of both treatment phases all subjects were within the normal range on this task.
Effects of training program on reading achievement
The phonology training had significantly more impact on reading accuracy than
comprehension but both programs had an equally significant impact on reading
comprehension. Qualitative analysis indicated that four children made greater
comprehension gains with phonological intervention than semantic/syntactic intervention.
There was no order effect.
Author’s conclusion:
Intervention addressing the underlying phonologic, semantic and syntactic deficits improved
reading accuracy and comprehension. Phonological training enhances reading accuracy more than
syntax/semantics training. Reading comprehension is differentially affected by phonological
training or syntax/semantics training depending on the pre-test phonology skill. For the children
with the most severe phonology problems, comprehension improved most when therapy focus was
phonology but for the others with higher phonology scores, comprehension improved most when
therapy focus was syntax/semantics training.
Reviewer’s
conclusion:
As above but noting that these conclusions need to be mitigated in light of small groups.
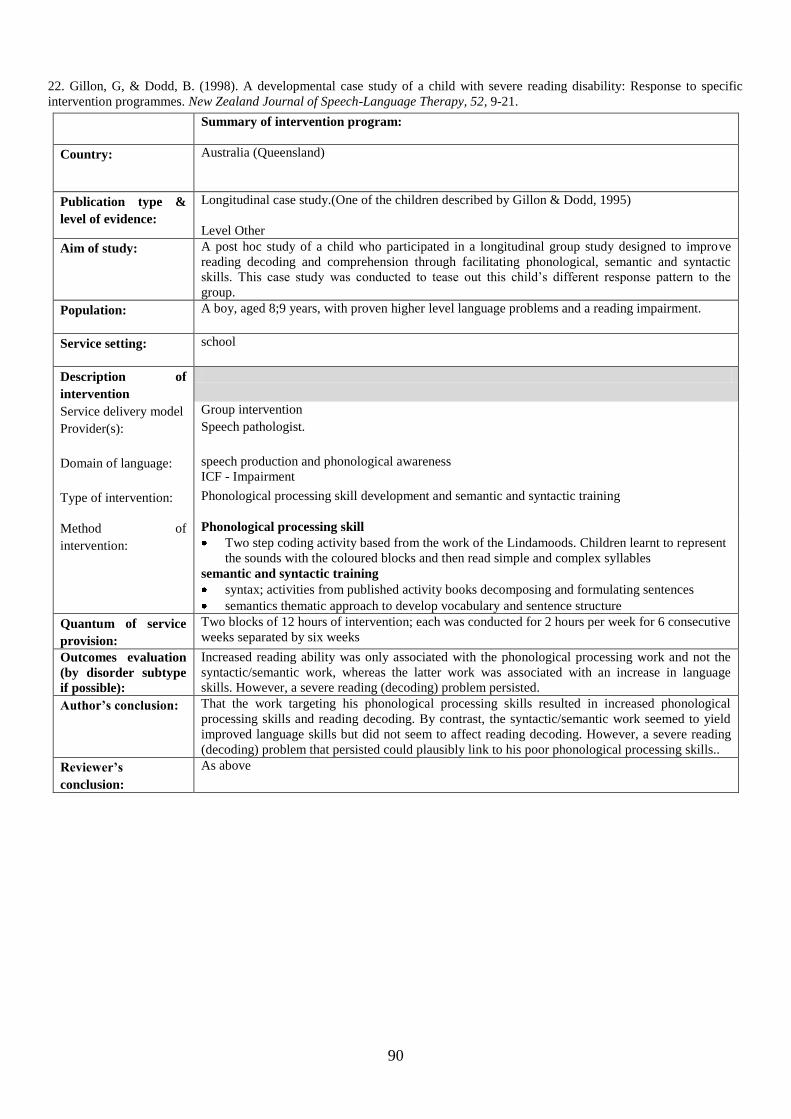
90
22. Gillon, G, & Dodd, B. (1998). A developmental case study of a child with severe reading disability: Response to specific
intervention programmes. New Zealand Journal of Speech-Language Therapy, 52, 9-21.
Summary of intervention program:
Country: Australia (Queensland)
Publication type &
level of evidence:
Longitudinal case study.(One of the children described by Gillon & Dodd, 1995)
Level Other
Aim of study:
A post hoc study of a child who participated in a longitudinal group study designed to improve
reading decoding and comprehension through facilitating phonological, semantic and syntactic
skills. This case study was conducted to tease out this child‟s different response pattern to the
group.
Population:
A boy, aged 8;9 years, with proven higher level language problems and a reading impairment.
Service setting:
school
Description of
intervention
Service delivery model Group intervention
Provider(s):
Speech pathologist.
Domain of language:
speech production and phonological awareness
ICF - Impairment
Type of intervention: Phonological processing skill development and semantic and syntactic training
Method of
intervention:
Phonological processing skill
Two step coding activity based from the work of the Lindamoods. Children learnt to represent
the sounds with the coloured blocks and then read simple and complex syllables
semantic and syntactic training
syntax; activities from published activity books decomposing and formulating sentences
semantics thematic approach to develop vocabulary and sentence structure
Quantum of service
provision:
Two blocks of 12 hours of intervention; each was conducted for 2 hours per week for 6 consecutive
weeks separated by six weeks
Outcomes evaluation
(by disorder subtype
if possible):
Increased reading ability was only associated with the phonological processing work and not the
syntactic/semantic work, whereas the latter work was associated with an increase in language
skills. However, a severe reading (decoding) problem persisted.
Author’s conclusion:
That the work targeting his phonological processing skills resulted in increased phonological
processing skills and reading decoding. By contrast, the syntactic/semantic work seemed to yield
improved language skills but did not seem to affect reading decoding. However, a severe reading
(decoding) problem that persisted could plausibly link to his poor phonological processing skills..
Reviewer’s
conclusion:
As above
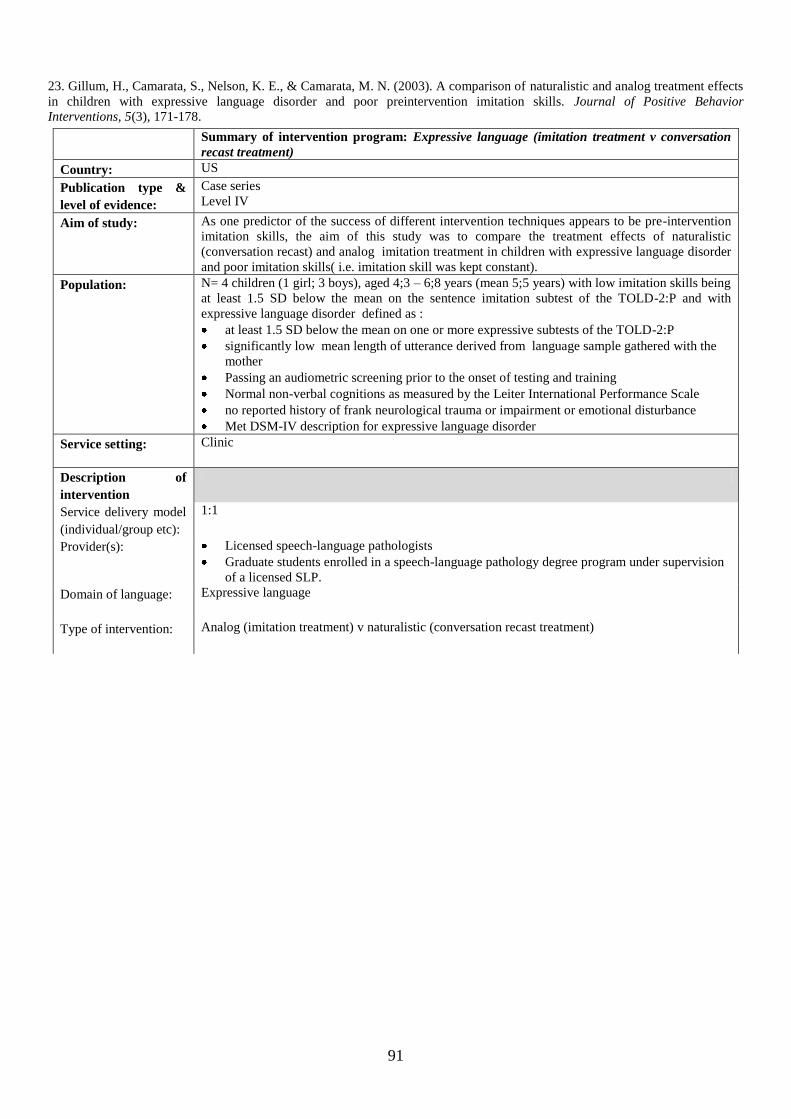
91
23. Gillum, H., Camarata, S., Nelson, K. E., & Camarata, M. N. (2003). A comparison of naturalistic and analog treatment effects
in children with expressive language disorder and poor preintervention imitation skills. Journal of Positive Behavior
Interventions, 5(3), 171-178.
Summary of intervention program: Expressive language (imitation treatment v conversation
recast treatment)
Country: US
Publication type &
level of evidence:
Case series
Level IV
Aim of study:
As one predictor of the success of different intervention techniques appears to be pre-intervention
imitation skills, the aim of this study was to compare the treatment effects of naturalistic
(conversation recast) and analog imitation treatment in children with expressive language disorder
and poor imitation skills( i.e. imitation skill was kept constant).
Population:
N= 4 children (1 girl; 3 boys), aged 4;3 – 6;8 years (mean 5;5 years) with low imitation skills being
at least 1.5 SD below the mean on the sentence imitation subtest of the TOLD-2:P and with
expressive language disorder defined as :
at least 1.5 SD below the mean on one or more expressive subtests of the TOLD-2:P
significantly low mean length of utterance derived from language sample gathered with the
mother
Passing an audiometric screening prior to the onset of testing and training
Normal non-verbal cognitions as measured by the Leiter International Performance Scale
no reported history of frank neurological trauma or impairment or emotional disturbance
Met DSM-IV description for expressive language disorder
Service setting:
Clinic
Description of
intervention
Service delivery model
(individual/group etc):
1:1
Provider(s):
Licensed speech-language pathologists
Graduate students enrolled in a speech-language pathology degree program under supervision
of a licensed SLP.
Domain of language:
Expressive language
Type of intervention:
Analog (imitation treatment) v naturalistic (conversation recast treatment)
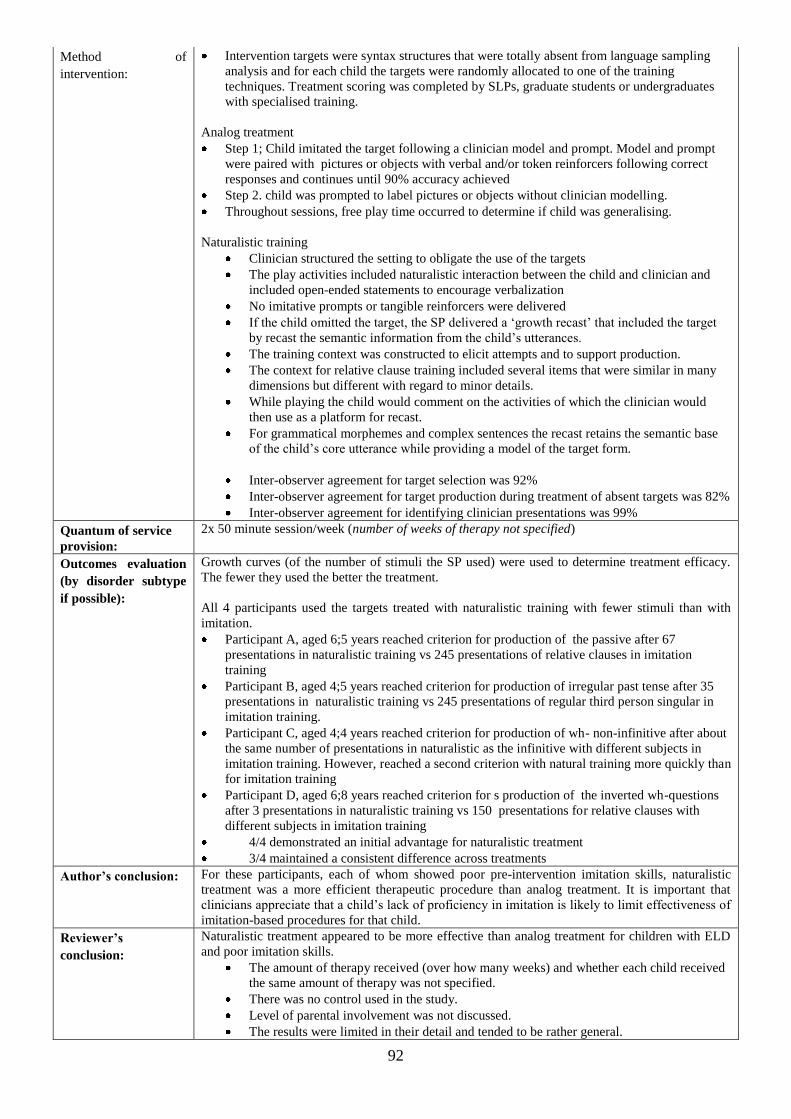
92
Method of
intervention:
Intervention targets were syntax structures that were totally absent from language sampling
analysis and for each child the targets were randomly allocated to one of the training
techniques. Treatment scoring was completed by SLPs, graduate students or undergraduates
with specialised training.
Analog treatment
Step 1; Child imitated the target following a clinician model and prompt. Model and prompt
were paired with pictures or objects with verbal and/or token reinforcers following correct
responses and continues until 90% accuracy achieved
Step 2. child was prompted to label pictures or objects without clinician modelling.
Throughout sessions, free play time occurred to determine if child was generalising.
Naturalistic training
Clinician structured the setting to obligate the use of the targets
The play activities included naturalistic interaction between the child and clinician and
included open-ended statements to encourage verbalization
No imitative prompts or tangible reinforcers were delivered
If the child omitted the target, the SP delivered a „growth recast‟ that included the target
by recast the semantic information from the child‟s utterances.
The training context was constructed to elicit attempts and to support production.
The context for relative clause training included several items that were similar in many
dimensions but different with regard to minor details.
While playing the child would comment on the activities of which the clinician would
then use as a platform for recast.
For grammatical morphemes and complex sentences the recast retains the semantic base
of the child‟s core utterance while providing a model of the target form.
Inter-observer agreement for target selection was 92%
Inter-observer agreement for target production during treatment of absent targets was 82%
Inter-observer agreement for identifying clinician presentations was 99%
Quantum of service
provision:
2x 50 minute session/week (number of weeks of therapy not specified)
Outcomes evaluation
(by disorder subtype
if possible):
Growth curves (of the number of stimuli the SP used) were used to determine treatment efficacy.
The fewer they used the better the treatment.
All 4 participants used the targets treated with naturalistic training with fewer stimuli than with
imitation.
Participant A, aged 6;5 years reached criterion for production of the passive after 67
presentations in naturalistic training vs 245 presentations of relative clauses in imitation
training
Participant B, aged 4;5 years reached criterion for production of irregular past tense after 35
presentations in naturalistic training vs 245 presentations of regular third person singular in
imitation training.
Participant C, aged 4;4 years reached criterion for production of wh- non-infinitive after about
the same number of presentations in naturalistic as the infinitive with different subjects in
imitation training. However, reached a second criterion with natural training more quickly than
for imitation training
Participant D, aged 6;8 years reached criterion for s production of the inverted wh-questions
after 3 presentations in naturalistic training vs 150 presentations for relative clauses with
different subjects in imitation training
4/4 demonstrated an initial advantage for naturalistic treatment
3/4 maintained a consistent difference across treatments
Author’s conclusion:
For these participants, each of whom showed poor pre-intervention imitation skills, naturalistic
treatment was a more efficient therapeutic procedure than analog treatment. It is important that
clinicians appreciate that a child‟s lack of proficiency in imitation is likely to limit effectiveness of
imitation-based procedures for that child.
Reviewer’s
conclusion:
Naturalistic treatment appeared to be more effective than analog treatment for children with ELD
and poor imitation skills.
The amount of therapy received (over how many weeks) and whether each child received
the same amount of therapy was not specified.
There was no control used in the study.
Level of parental involvement was not discussed.
The results were limited in their detail and tended to be rather general.
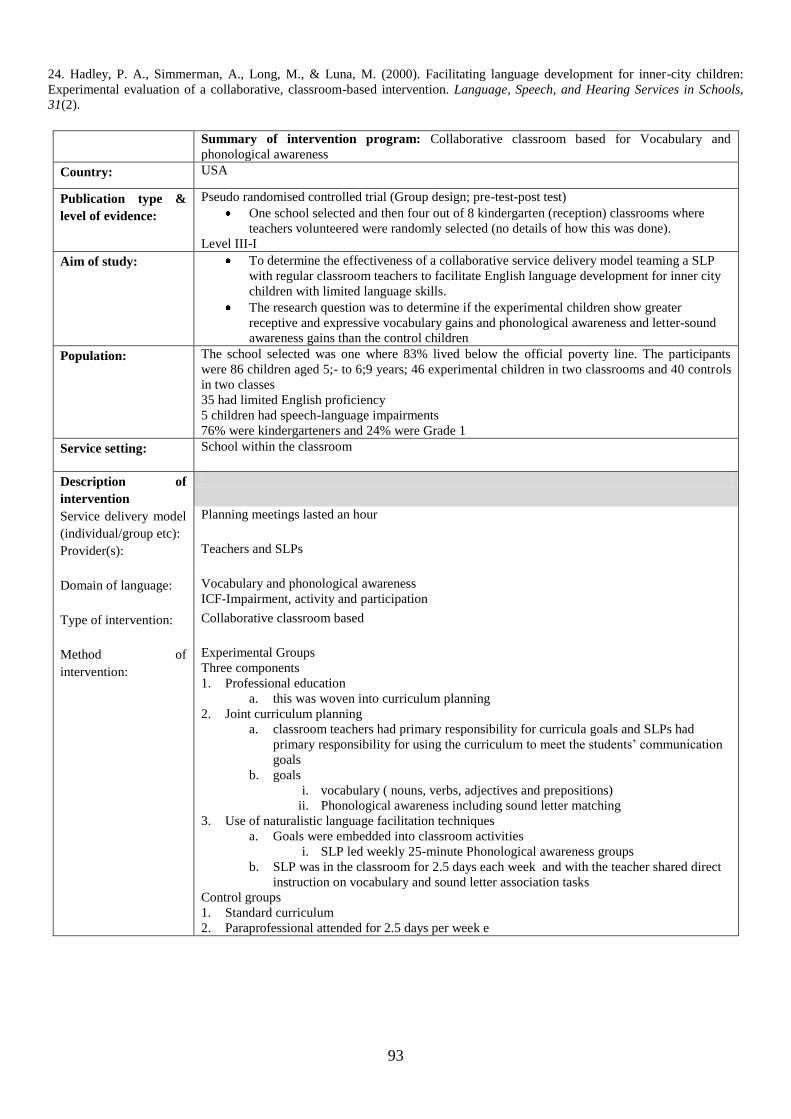
93
24. Hadley, P. A., Simmerman, A., Long, M., & Luna, M. (2000). Facilitating language development for inner-city children:
Experimental evaluation of a collaborative, classroom-based intervention. Language, Speech, and Hearing Services in Schools,
31(2).
Summary of intervention program: Collaborative classroom based for Vocabulary and
phonological awareness
Country: USA
Publication type &
level of evidence:
Pseudo randomised controlled trial (Group design; pre-test-post test)
One school selected and then four out of 8 kindergarten (reception) classrooms where
teachers volunteered were randomly selected (no details of how this was done).
Level III-I
Aim of study:
To determine the effectiveness of a collaborative service delivery model teaming a SLP
with regular classroom teachers to facilitate English language development for inner city
children with limited language skills.
The research question was to determine if the experimental children show greater
receptive and expressive vocabulary gains and phonological awareness and letter-sound
awareness gains than the control children
Population:
The school selected was one where 83% lived below the official poverty line. The participants
were 86 children aged 5;- to 6;9 years; 46 experimental children in two classrooms and 40 controls
in two classes
35 had limited English proficiency
5 children had speech-language impairments
76% were kindergarteners and 24% were Grade 1
Service setting:
School within the classroom
Description of
intervention
Service delivery model
(individual/group etc):
Planning meetings lasted an hour
Provider(s):
Teachers and SLPs
Domain of language:
Vocabulary and phonological awareness
ICF-Impairment, activity and participation
Type of intervention:
Collaborative classroom based
Method of
intervention:
Experimental Groups
Three components
1. Professional education
a. this was woven into curriculum planning
2. Joint curriculum planning
a. classroom teachers had primary responsibility for curricula goals and SLPs had
primary responsibility for using the curriculum to meet the students‟ communication
goals
b. goals
i. vocabulary ( nouns, verbs, adjectives and prepositions)
ii. Phonological awareness including sound letter matching
3. Use of naturalistic language facilitation techniques
a. Goals were embedded into classroom activities
i. SLP led weekly 25-minute Phonological awareness groups
b. SLP was in the classroom for 2.5 days each week and with the teacher shared direct
instruction on vocabulary and sound letter association tasks
Control groups
1. Standard curriculum
2. Paraprofessional attended for 2.5 days per week e
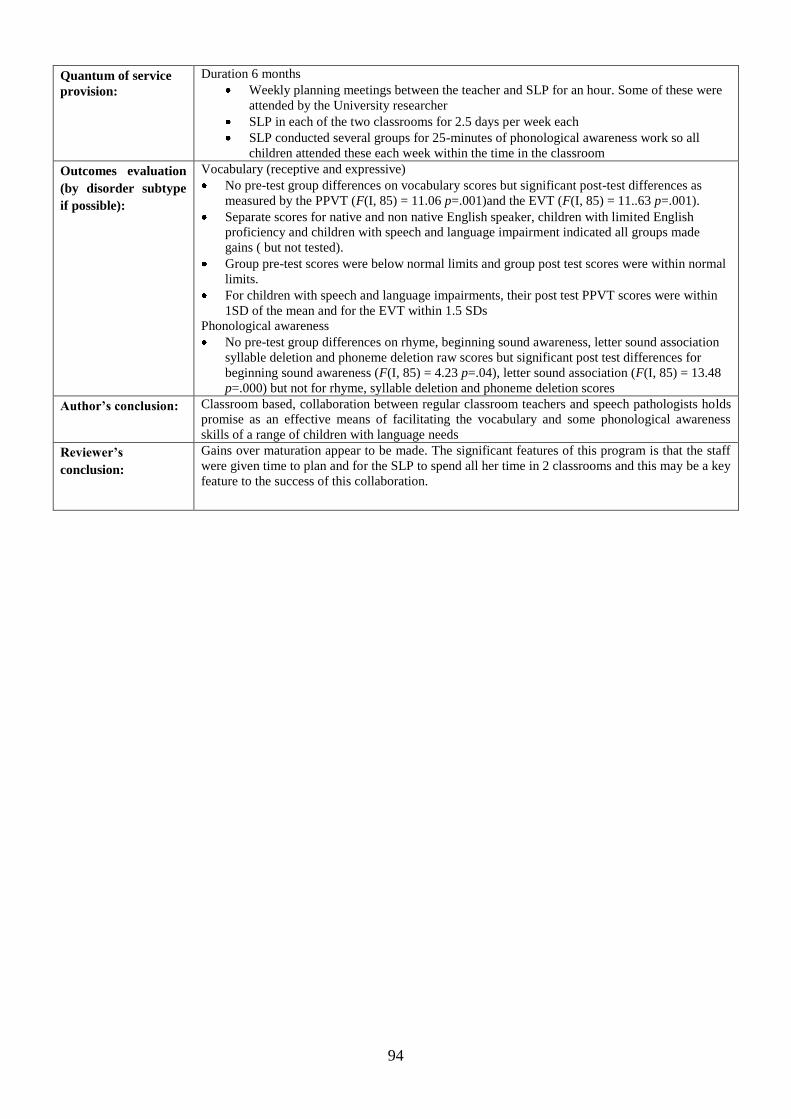
94
Quantum of service
provision:
Duration 6 months
Weekly planning meetings between the teacher and SLP for an hour. Some of these were
attended by the University researcher
SLP in each of the two classrooms for 2.5 days per week each
SLP conducted several groups for 25-minutes of phonological awareness work so all
children attended these each week within the time in the classroom
Outcomes evaluation
(by disorder subtype
if possible):
Vocabulary (receptive and expressive)
No pre-test group differences on vocabulary scores but significant post-test differences as
measured by the PPVT (F(I, 85) = 11.06 p=.001)and the EVT (F(I, 85) = 11..63 p=.001).
Separate scores for native and non native English speaker, children with limited English
proficiency and children with speech and language impairment indicated all groups made
gains ( but not tested).
Group pre-test scores were below normal limits and group post test scores were within normal
limits.
For children with speech and language impairments, their post test PPVT scores were within
1SD of the mean and for the EVT within 1.5 SDs
Phonological awareness
No pre-test group differences on rhyme, beginning sound awareness, letter sound association
syllable deletion and phoneme deletion raw scores but significant post test differences for
beginning sound awareness (F(I, 85) = 4.23 p=.04), letter sound association (F(I, 85) = 13.48
p=.000) but not for rhyme, syllable deletion and phoneme deletion scores
Author’s conclusion:
Classroom based, collaboration between regular classroom teachers and speech pathologists holds
promise as an effective means of facilitating the vocabulary and some phonological awareness
skills of a range of children with language needs
Reviewer’s
conclusion:
Gains over maturation appear to be made. The significant features of this program is that the staff
were given time to plan and for the SLP to spend all her time in 2 classrooms and this may be a key
feature to the success of this collaboration.
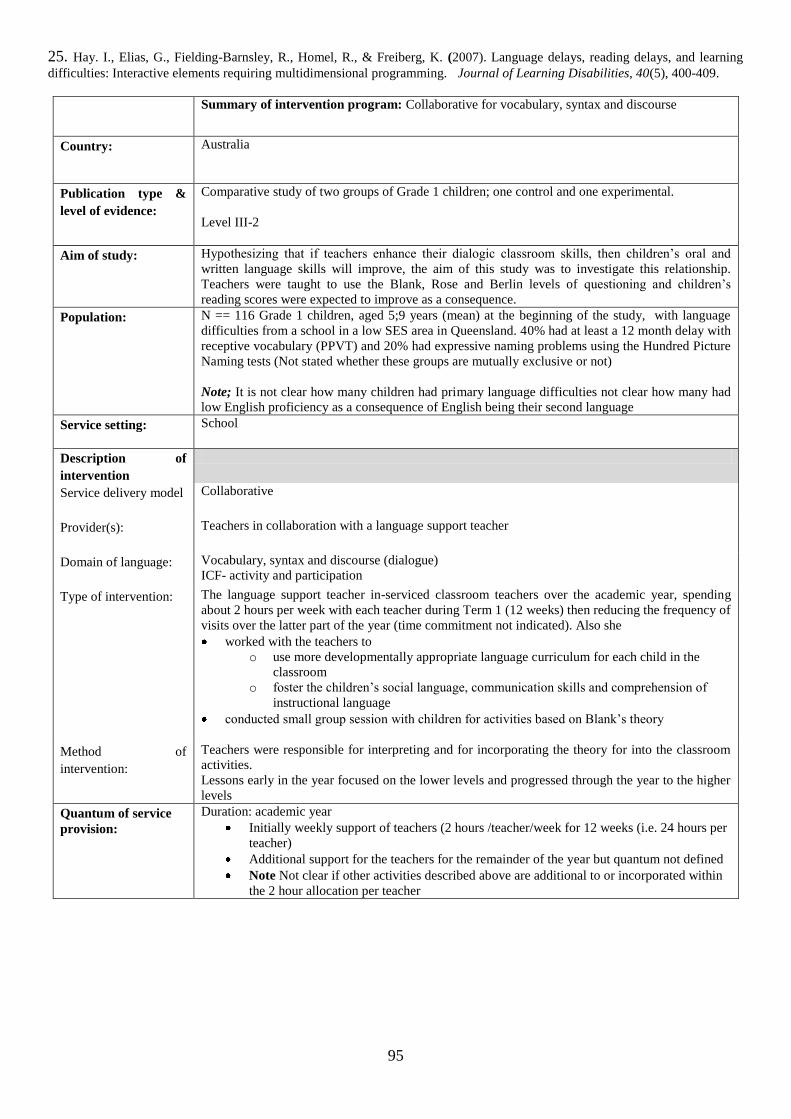
95
25. Hay. I., Elias, G., Fielding-Barnsley, R., Homel, R., & Freiberg, K. (2007). Language delays, reading delays, and learning
difficulties: Interactive elements requiring multidimensional programming. Journal of Learning Disabilities, 40(5), 400-409.
Summary of intervention program: Collaborative for vocabulary, syntax and discourse
Country: Australia
Publication type &
level of evidence:
Comparative study of two groups of Grade 1 children; one control and one experimental.
Level III-2
Aim of study:
Hypothesizing that if teachers enhance their dialogic classroom skills, then children‟s oral and
written language skills will improve, the aim of this study was to investigate this relationship.
Teachers were taught to use the Blank, Rose and Berlin levels of questioning and children‟s
reading scores were expected to improve as a consequence.
Population:
N == 116 Grade 1 children, aged 5;9 years (mean) at the beginning of the study, with language
difficulties from a school in a low SES area in Queensland. 40% had at least a 12 month delay with
receptive vocabulary (PPVT) and 20% had expressive naming problems using the Hundred Picture
Naming tests (Not stated whether these groups are mutually exclusive or not)
Note; It is not clear how many children had primary language difficulties not clear how many had
low English proficiency as a consequence of English being their second language
Service setting:
School
Description of
intervention
Service delivery model
Collaborative
Provider(s):
Teachers in collaboration with a language support teacher
Domain of language:
Vocabulary, syntax and discourse (dialogue)
ICF- activity and participation
Type of intervention:
The language support teacher in-serviced classroom teachers over the academic year, spending
about 2 hours per week with each teacher during Term 1 (12 weeks) then reducing the frequency of
visits over the latter part of the year (time commitment not indicated). Also she
worked with the teachers to
o use more developmentally appropriate language curriculum for each child in the
classroom
o foster the children‟s social language, communication skills and comprehension of
instructional language
conducted small group session with children for activities based on Blank‟s theory
Method of
intervention:
Teachers were responsible for interpreting and for incorporating the theory for into the classroom
activities.
Lessons early in the year focused on the lower levels and progressed through the year to the higher
levels
Quantum of service
provision:
Duration: academic year
Initially weekly support of teachers (2 hours /teacher/week for 12 weeks (i.e. 24 hours per
teacher)
Additional support for the teachers for the remainder of the year but quantum not defined
Note Not clear if other activities described above are additional to or incorporated within
the 2 hour allocation per teacher

96
Outcomes evaluation
(by disorder subtype
if possible):
Experimental group significantly outperformed the control group on the end of year scores
Reading scores (Burt Word Reading test) F(1,114)=5.59 p = 016
The number of children reading below their age level as measured on Neale Analysis of
reading decreased in the experimental group 2 (1, N=116)=11.45 p<.001 (
The number of children judged as at risk for language skills according to the PLAI decreased
significantly in the experimental group 2 (1, N=57) =15.96, p<.001 (Note the number in the
control group was not given)
Author’s conclusion:
Concluded that
the addition of Blank et al‟s. language development strategies facilitated reading development
and that this was consequent to multi-dimensional intervention rather than uni-dimensional
intervention that focused on phonological and word decoding.
o Reading instruction requires attention on the specifics of literacy AND oral language
Noted limitations including the lack of controls for all variables in this program
Reviewer’s
conclusion:
It is not clear what contributed to the experimental groups increased end-of -year reading
performance because of the
lack of experimental controls,
no fidelity checks
the comparability of the two groups prior to intervention was not established
What is clear is that groups differences existed at the end of the year
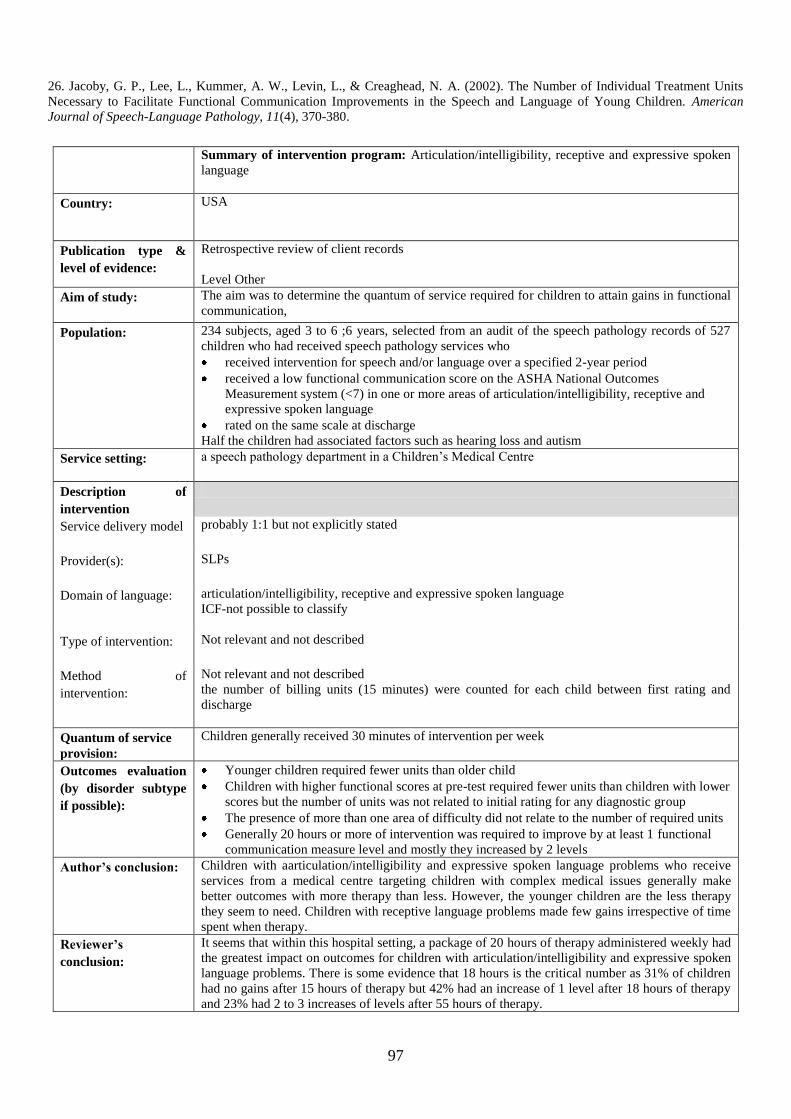
97
26. Jacoby, G. P., Lee, L., Kummer, A. W., Levin, L., & Creaghead, N. A. (2002). The Number of Individual Treatment Units
Necessary to Facilitate Functional Communication Improvements in the Speech and Language of Young Children. American
Journal of Speech-Language Pathology, 11(4), 370-380.
Summary of intervention program: Articulation/intelligibility, receptive and expressive spoken
language
Country: USA
Publication type &
level of evidence:
Retrospective review of client records
Level Other
Aim of study:
The aim was to determine the quantum of service required for children to attain gains in functional
communication,
Population:
234 subjects, aged 3 to 6 ;6 years, selected from an audit of the speech pathology records of 527
children who had received speech pathology services who
received intervention for speech and/or language over a specified 2-year period
received a low functional communication score on the ASHA National Outcomes
Measurement system (<7) in one or more areas of articulation/intelligibility, receptive and
expressive spoken language
rated on the same scale at discharge
Half the children had associated factors such as hearing loss and autism
Service setting:
a speech pathology department in a Children‟s Medical Centre
Description of
intervention
Service delivery model
probably 1:1 but not explicitly stated
Provider(s):
SLPs
Domain of language:
articulation/intelligibility, receptive and expressive spoken language
ICF-not possible to classify
Type of intervention:
Not relevant and not described
Method of
intervention:
Not relevant and not described
the number of billing units (15 minutes) were counted for each child between first rating and
discharge
Quantum of service
provision:
Children generally received 30 minutes of intervention per week
Outcomes evaluation
(by disorder subtype
if possible):
Younger children required fewer units than older child
Children with higher functional scores at pre-test required fewer units than children with lower
scores but the number of units was not related to initial rating for any diagnostic group
The presence of more than one area of difficulty did not relate to the number of required units
Generally 20 hours or more of intervention was required to improve by at least 1 functional
communication measure level and mostly they increased by 2 levels
Author’s conclusion:
Children with aarticulation/intelligibility and expressive spoken language problems who receive
services from a medical centre targeting children with complex medical issues generally make
better outcomes with more therapy than less. However, the younger children are the less therapy
they seem to need. Children with receptive language problems made few gains irrespective of time
spent when therapy.
Reviewer’s
conclusion:
It seems that within this hospital setting, a package of 20 hours of therapy administered weekly had
the greatest impact on outcomes for children with articulation/intelligibility and expressive spoken
language problems. There is some evidence that 18 hours is the critical number as 31% of children
had no gains after 15 hours of therapy but 42% had an increase of 1 level after 18 hours of therapy
and 23% had 2 to 3 increases of levels after 55 hours of therapy.
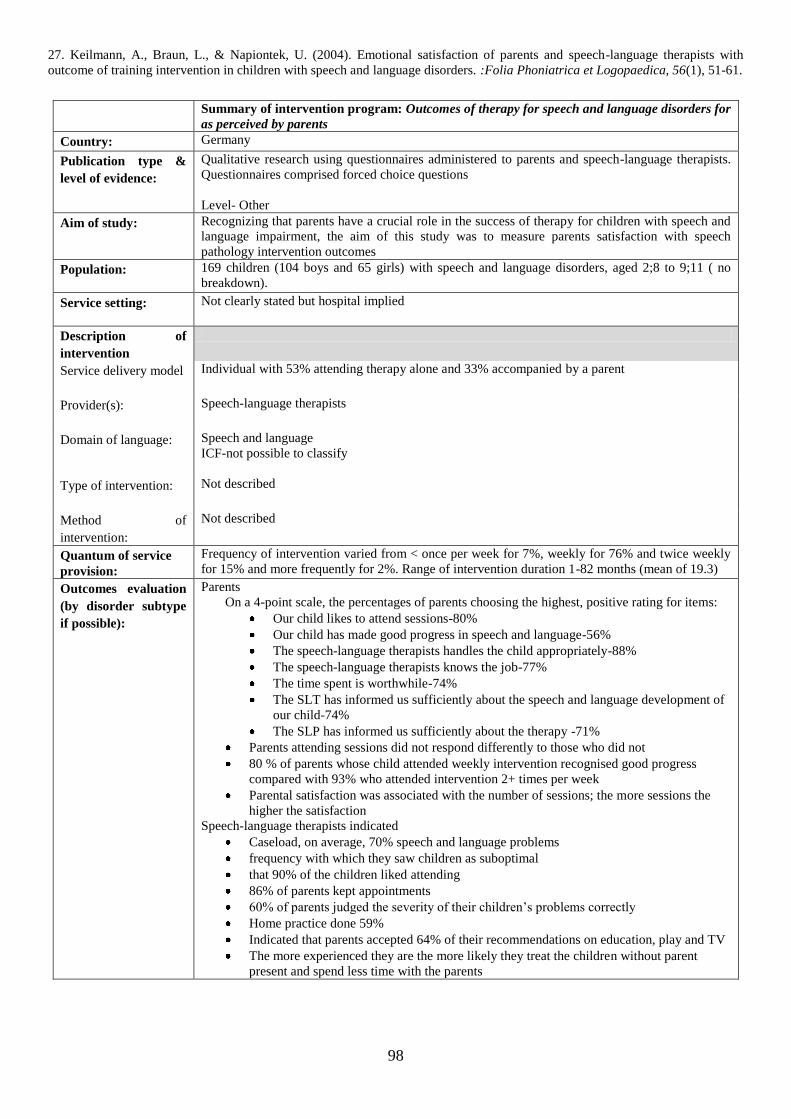
98
27. Keilmann, A., Braun, L., & Napiontek, U. (2004). Emotional satisfaction of parents and speech-language therapists with
outcome of training intervention in children with speech and language disorders. :Folia Phoniatrica et Logopaedica, 56(1), 51-61.
Summary of intervention program: Outcomes of therapy for speech and language disorders for
as perceived by parents
Country: Germany
Publication type &
level of evidence:
Qualitative research using questionnaires administered to parents and speech-language therapists.
Questionnaires comprised forced choice questions
Level- Other
Aim of study:
Recognizing that parents have a crucial role in the success of therapy for children with speech and
language impairment, the aim of this study was to measure parents satisfaction with speech
pathology intervention outcomes
Population:
169 children (104 boys and 65 girls) with speech and language disorders, aged 2;8 to 9;11 ( no
breakdown).
Service setting:
Not clearly stated but hospital implied
Description of
intervention
Service delivery model
Individual with 53% attending therapy alone and 33% accompanied by a parent
Provider(s):
Speech-language therapists
Domain of language:
Speech and language
ICF-not possible to classify
Type of intervention:
Not described
Method of
intervention:
Not described
Quantum of service
provision:
Frequency of intervention varied from < once per week for 7%, weekly for 76% and twice weekly
for 15% and more frequently for 2%. Range of intervention duration 1-82 months (mean of 19.3)
Outcomes evaluation
(by disorder subtype
if possible):
Parents
On a 4-point scale, the percentages of parents choosing the highest, positive rating for items:
Our child likes to attend sessions-80%
Our child has made good progress in speech and language-56%
The speech-language therapists handles the child appropriately-88%
The speech-language therapists knows the job-77%
The time spent is worthwhile-74%
The SLT has informed us sufficiently about the speech and language development of
our child-74%
The SLP has informed us sufficiently about the therapy -71%
Parents attending sessions did not respond differently to those who did not
80 % of parents whose child attended weekly intervention recognised good progress
compared with 93% who attended intervention 2+ times per week
Parental satisfaction was associated with the number of sessions; the more sessions the
higher the satisfaction
Speech-language therapists indicated
Caseload, on average, 70% speech and language problems
frequency with which they saw children as suboptimal
that 90% of the children liked attending
86% of parents kept appointments
60% of parents judged the severity of their children‟s problems correctly
Home practice done 59%
Indicated that parents accepted 64% of their recommendations on education, play and TV
The more experienced they are the more likely they treat the children without parent
present and spend less time with the parents

99
Author’s conclusion:
Parents do not perceive speech and language therapy as harming children, rather most expressed
happiness with it and attributed improvement in children to the therapy. Parents perceived that
higher frequency of therapy was associated with higher rate of progress.
Reviewer’s
conclusion:
As above. However for this review it is not clear how these results relate to the children five years
and older
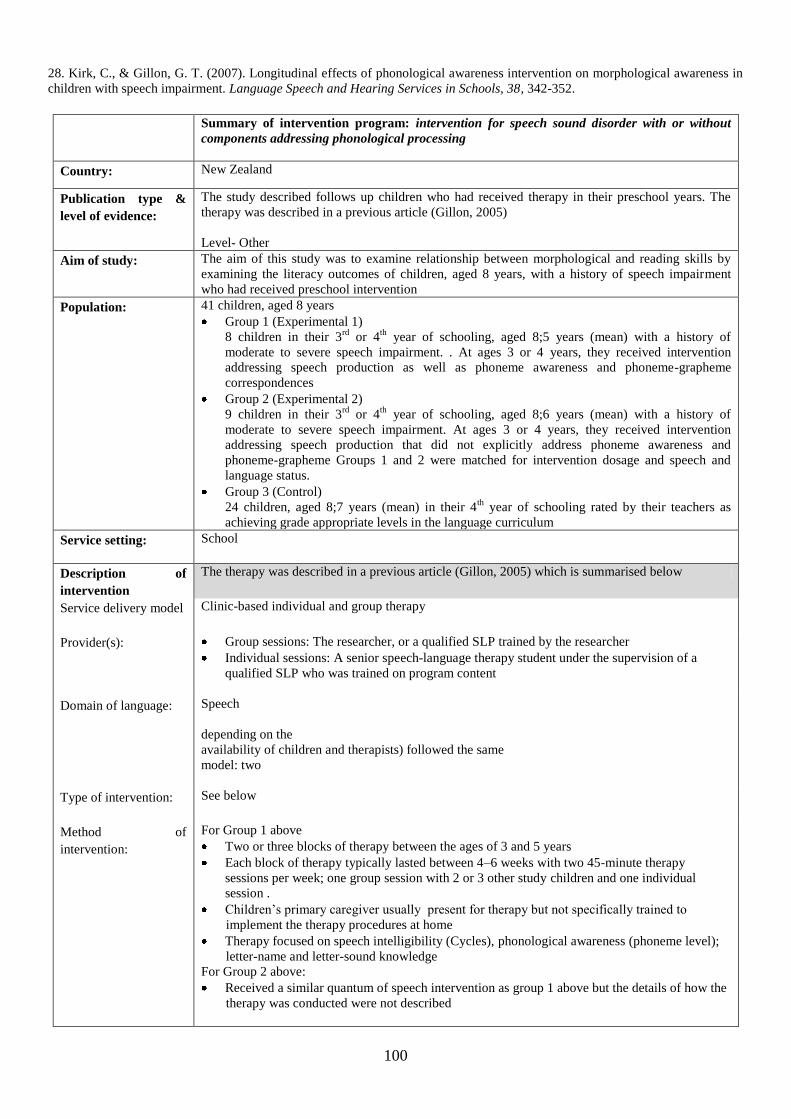
100
28. Kirk, C., & Gillon, G. T. (2007). Longitudinal effects of phonological awareness intervention on morphological awareness in
children with speech impairment. Language Speech and Hearing Services in Schools, 38, 342-352.
Summary of intervention program: intervention for speech sound disorder with or without
components addressing phonological processing
Country: New Zealand
Publication type &
level of evidence:
The study described follows up children who had received therapy in their preschool years. The
therapy was described in a previous article (Gillon, 2005)
Level- Other
Aim of study:
The aim of this study was to examine relationship between morphological and reading skills by
examining the literacy outcomes of children, aged 8 years, with a history of speech impairment
who had received preschool intervention
Population:
41 children, aged 8 years
Group 1 (Experimental 1)
8 children in their 3rd
or 4th
year of schooling, aged 8;5 years (mean) with a history of
moderate to severe speech impairment. . At ages 3 or 4 years, they received intervention
addressing speech production as well as phoneme awareness and phoneme-grapheme
correspondences
Group 2 (Experimental 2)
9 children in their 3rd
or 4th
year of schooling, aged 8;6 years (mean) with a history of
moderate to severe speech impairment. At ages 3 or 4 years, they received intervention
addressing speech production that did not explicitly address phoneme awareness and
phoneme-grapheme Groups 1 and 2 were matched for intervention dosage and speech and
language status.
Group 3 (Control)
24 children, aged 8;7 years (mean) in their 4th
year of schooling rated by their teachers as
achieving grade appropriate levels in the language curriculum
Service setting:
School
Description of
intervention
The therapy was described in a previous article (Gillon, 2005) which is summarised below
Service delivery model
Clinic-based individual and group therapy
Provider(s):
Group sessions: The researcher, or a qualified SLP trained by the researcher
Individual sessions: A senior speech-language therapy student under the supervision of a
qualified SLP who was trained on program content
Domain of language:
Speech
depending on the
availability of children and therapists) followed the same
model: two
Type of intervention:
See below
Method of
intervention:
For Group 1 above
Two or three blocks of therapy between the ages of 3 and 5 years
Each block of therapy typically lasted between 4–6 weeks with two 45-minute therapy
sessions per week; one group session with 2 or 3 other study children and one individual
session .
Children‟s primary caregiver usually present for therapy but not specifically trained to
implement the therapy procedures at home
Therapy focused on speech intelligibility (Cycles), phonological awareness (phoneme level);
letter-name and letter-sound knowledge
For Group 2 above:
Received a similar quantum of speech intervention as group 1 above but the details of how the
therapy was conducted were not described
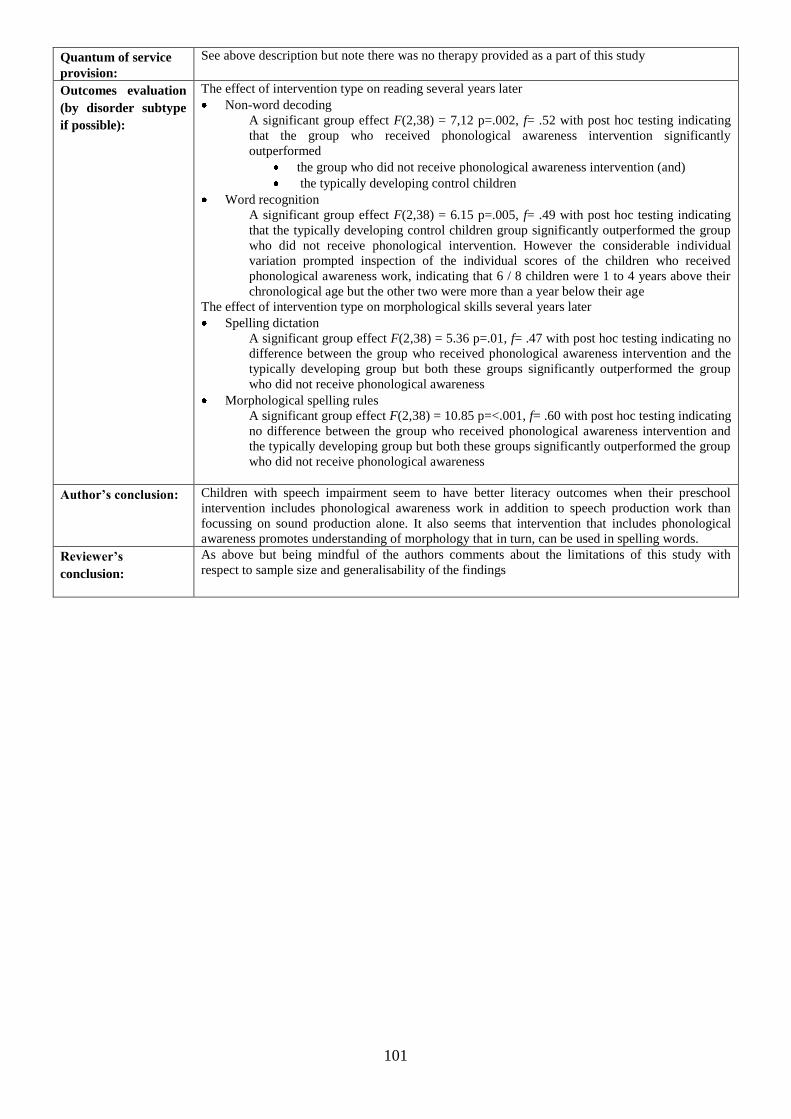
101
Quantum of service
provision:
See above description but note there was no therapy provided as a part of this study
Outcomes evaluation
(by disorder subtype
if possible):
The effect of intervention type on reading several years later
Non-word decoding
A significant group effect F(2,38) = 7,12 p=.002, f= .52 with post hoc testing indicating
that the group who received phonological awareness intervention significantly
outperformed
the group who did not receive phonological awareness intervention (and)
the typically developing control children
Word recognition
A significant group effect F(2,38) = 6.15 p=.005, f= .49 with post hoc testing indicating
that the typically developing control children group significantly outperformed the group
who did not receive phonological intervention. However the considerable individual
variation prompted inspection of the individual scores of the children who received
phonological awareness work, indicating that 6 / 8 children were 1 to 4 years above their
chronological age but the other two were more than a year below their age
The effect of intervention type on morphological skills several years later
Spelling dictation
A significant group effect F(2,38) = 5.36 p=.01, f= .47 with post hoc testing indicating no
difference between the group who received phonological awareness intervention and the
typically developing group but both these groups significantly outperformed the group
who did not receive phonological awareness
Morphological spelling rules
A significant group effect F(2,38) = 10.85 p=<.001, f= .60 with post hoc testing indicating
no difference between the group who received phonological awareness intervention and
the typically developing group but both these groups significantly outperformed the group
who did not receive phonological awareness
Author’s conclusion:
Children with speech impairment seem to have better literacy outcomes when their preschool
intervention includes phonological awareness work in addition to speech production work than
focussing on sound production alone. It also seems that intervention that includes phonological
awareness promotes understanding of morphology that in turn, can be used in spelling words.
Reviewer’s
conclusion:
As above but being mindful of the authors comments about the limitations of this study with
respect to sample size and generalisability of the findings
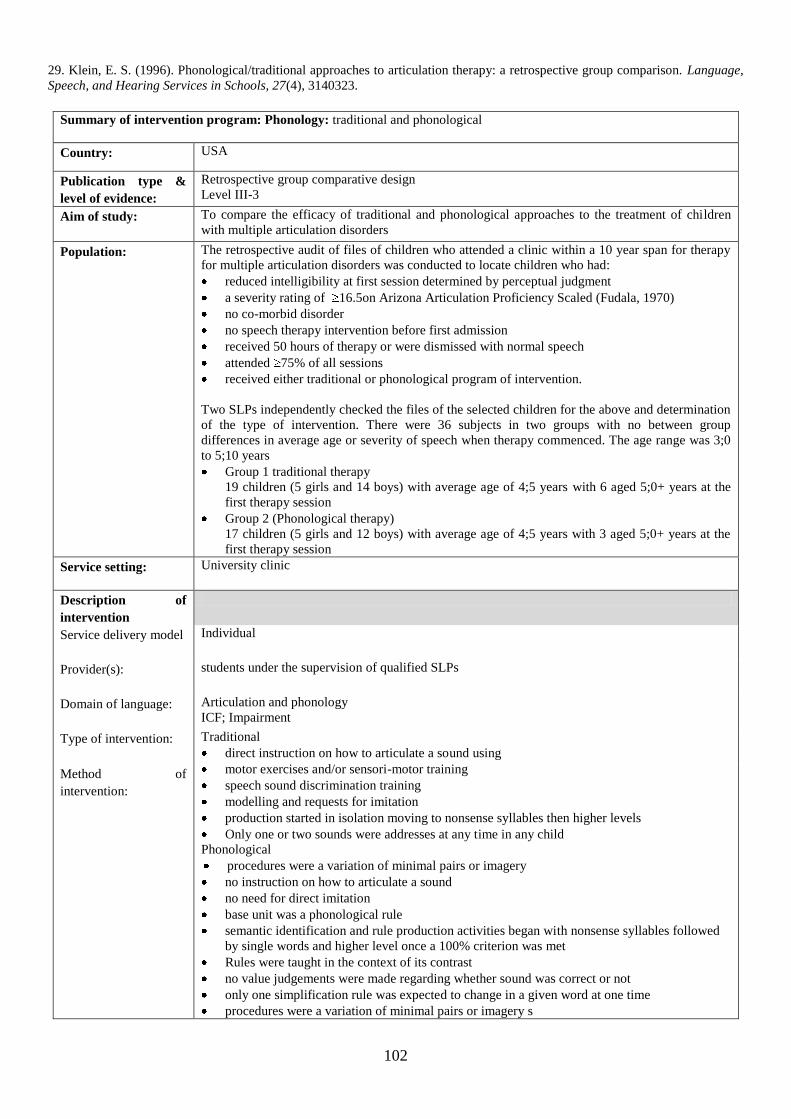
102
29. Klein, E. S. (1996). Phonological/traditional approaches to articulation therapy: a retrospective group comparison. Language,
Speech, and Hearing Services in Schools, 27(4), 3140323.
Summary of intervention program: Phonology: traditional and phonological
Country: USA
Publication type &
level of evidence:
Retrospective group comparative design
Level III-3
Aim of study:
To compare the efficacy of traditional and phonological approaches to the treatment of children
with multiple articulation disorders
Population:
The retrospective audit of files of children who attended a clinic within a 10 year span for therapy
for multiple articulation disorders was conducted to locate children who had:
reduced intelligibility at first session determined by perceptual judgment
a severity rating of 16.5on Arizona Articulation Proficiency Scaled (Fudala, 1970)
no co-morbid disorder
no speech therapy intervention before first admission
received 50 hours of therapy or were dismissed with normal speech
attended 75% of all sessions
received either traditional or phonological program of intervention.
Two SLPs independently checked the files of the selected children for the above and determination
of the type of intervention. There were 36 subjects in two groups with no between group
differences in average age or severity of speech when therapy commenced. The age range was 3;0
to 5;10 years
Group 1 traditional therapy
19 children (5 girls and 14 boys) with average age of 4;5 years with 6 aged 5;0+ years at the
first therapy session
Group 2 (Phonological therapy)
17 children (5 girls and 12 boys) with average age of 4;5 years with 3 aged 5;0+ years at the
first therapy session
Service setting:
University clinic
Description of
intervention
Service delivery model
Individual
Provider(s):
students under the supervision of qualified SLPs
Domain of language:
Articulation and phonology
ICF; Impairment
Type of intervention:
Traditional
direct instruction on how to articulate a sound using
motor exercises and/or sensori-motor training
speech sound discrimination training
modelling and requests for imitation
production started in isolation moving to nonsense syllables then higher levels
Only one or two sounds were addresses at any time in any child
Phonological
procedures were a variation of minimal pairs or imagery
no instruction on how to articulate a sound
no need for direct imitation
base unit was a phonological rule
semantic identification and rule production activities began with nonsense syllables followed
by single words and higher level once a 100% criterion was met
Rules were taught in the context of its contrast
no value judgements were made regarding whether sound was correct or not
only one simplification rule was expected to change in a given word at one time
procedures were a variation of minimal pairs or imagery s
Method of
intervention:
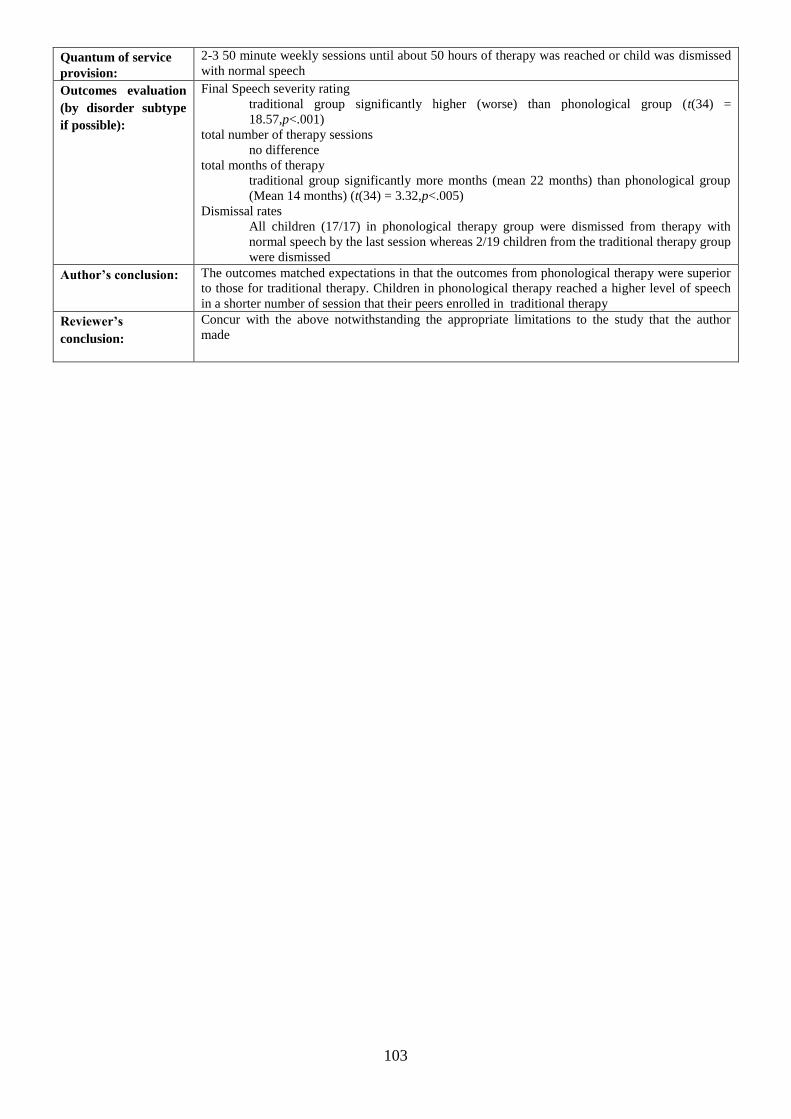
103
Quantum of service
provision:
2-3 50 minute weekly sessions until about 50 hours of therapy was reached or child was dismissed
with normal speech
Outcomes evaluation
(by disorder subtype
if possible):
Final Speech severity rating
traditional group significantly higher (worse) than phonological group (t(34) =
18.57,p<.001)
total number of therapy sessions
no difference
total months of therapy
traditional group significantly more months (mean 22 months) than phonological group
(Mean 14 months) (t(34) = 3.32,p<.005)
Dismissal rates
All children (17/17) in phonological therapy group were dismissed from therapy with
normal speech by the last session whereas 2/19 children from the traditional therapy group
were dismissed
Author’s conclusion:
The outcomes matched expectations in that the outcomes from phonological therapy were superior
to those for traditional therapy. Children in phonological therapy reached a higher level of speech
in a shorter number of session that their peers enrolled in traditional therapy
Reviewer’s
conclusion:
Concur with the above notwithstanding the appropriate limitations to the study that the author
made
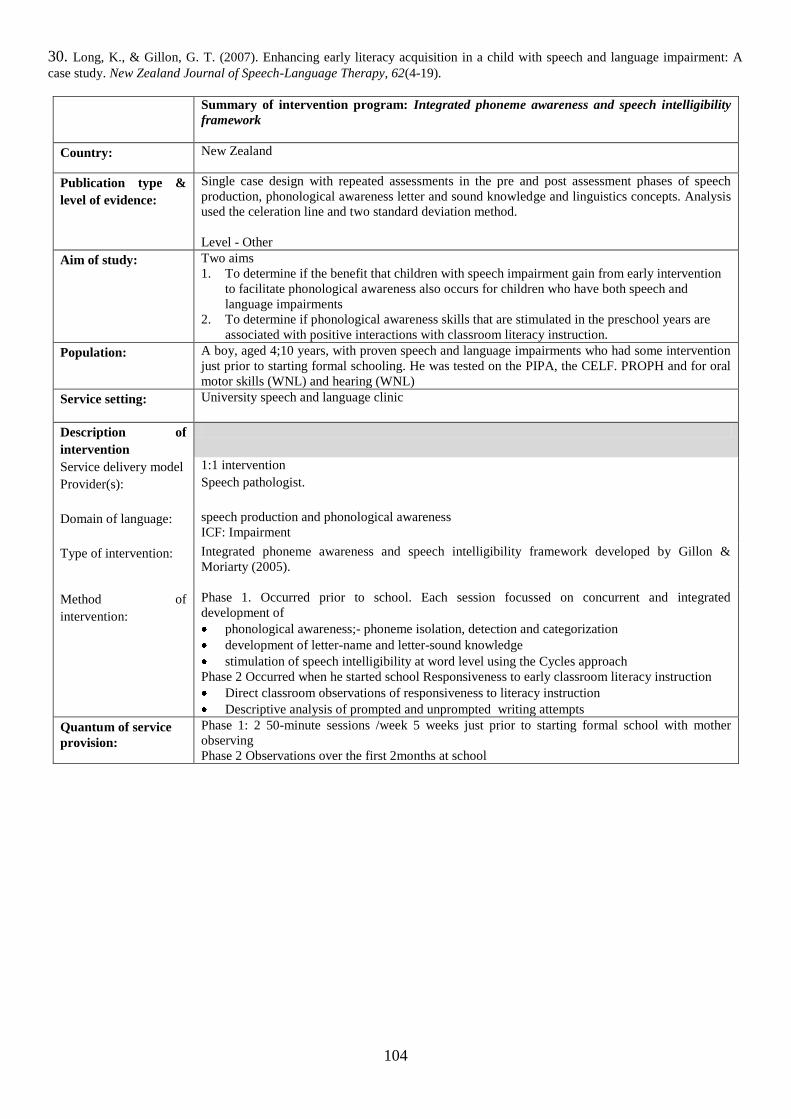
104
30. Long, K., & Gillon, G. T. (2007). Enhancing early literacy acquisition in a child with speech and language impairment: A
case study. New Zealand Journal of Speech-Language Therapy, 62(4-19).
Summary of intervention program: Integrated phoneme awareness and speech intelligibility
framework
Country: New Zealand
Publication type &
level of evidence:
Single case design with repeated assessments in the pre and post assessment phases of speech
production, phonological awareness letter and sound knowledge and linguistics concepts. Analysis
used the celeration line and two standard deviation method.
Level - Other
Aim of study:
Two aims
1. To determine if the benefit that children with speech impairment gain from early intervention
to facilitate phonological awareness also occurs for children who have both speech and
language impairments
2. To determine if phonological awareness skills that are stimulated in the preschool years are
associated with positive interactions with classroom literacy instruction.
Population:
A boy, aged 4;10 years, with proven speech and language impairments who had some intervention
just prior to starting formal schooling. He was tested on the PIPA, the CELF. PROPH and for oral
motor skills (WNL) and hearing (WNL)
Service setting:
University speech and language clinic
Description of
intervention
Service delivery model 1:1 intervention
Provider(s):
Speech pathologist.
Domain of language:
speech production and phonological awareness
ICF: Impairment
Type of intervention: Integrated phoneme awareness and speech intelligibility framework developed by Gillon &
Moriarty (2005).
Method of
intervention:
Phase 1. Occurred prior to school. Each session focussed on concurrent and integrated
development of
phonological awareness;- phoneme isolation, detection and categorization
development of letter-name and letter-sound knowledge
stimulation of speech intelligibility at word level using the Cycles approach
Phase 2 Occurred when he started school Responsiveness to early classroom literacy instruction
Direct classroom observations of responsiveness to literacy instruction
Descriptive analysis of prompted and unprompted writing attempts
Quantum of service
provision:
Phase 1: 2 50-minute sessions /week 5 weeks just prior to starting formal school with mother
observing
Phase 2 Observations over the first 2months at school
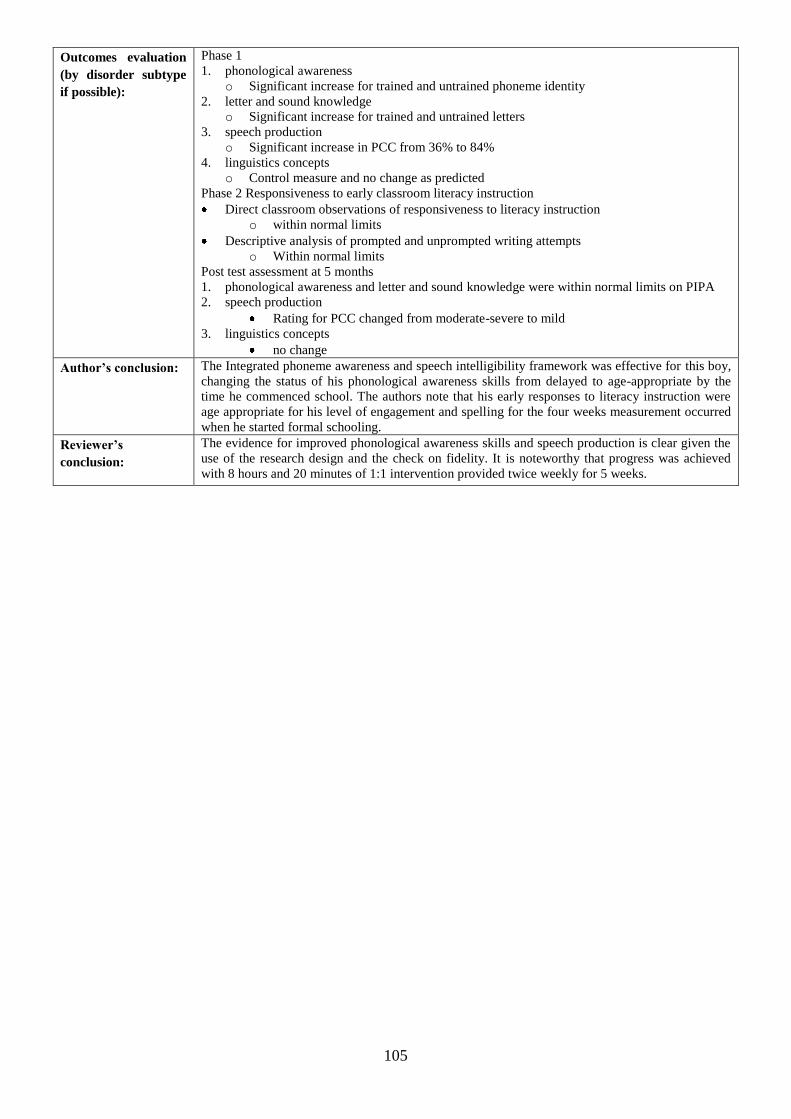
105
Outcomes evaluation
(by disorder subtype
if possible):
Phase 1
1. phonological awareness
o Significant increase for trained and untrained phoneme identity
2. letter and sound knowledge
o Significant increase for trained and untrained letters
3. speech production
o Significant increase in PCC from 36% to 84%
4. linguistics concepts
o Control measure and no change as predicted
Phase 2 Responsiveness to early classroom literacy instruction
Direct classroom observations of responsiveness to literacy instruction
o within normal limits
Descriptive analysis of prompted and unprompted writing attempts
o Within normal limits
Post test assessment at 5 months
1. phonological awareness and letter and sound knowledge were within normal limits on PIPA
2. speech production
Rating for PCC changed from moderate-severe to mild
3. linguistics concepts
no change
Author’s conclusion:
The Integrated phoneme awareness and speech intelligibility framework was effective for this boy,
changing the status of his phonological awareness skills from delayed to age-appropriate by the
time he commenced school. The authors note that his early responses to literacy instruction were
age appropriate for his level of engagement and spelling for the four weeks measurement occurred
when he started formal schooling.
Reviewer’s
conclusion:
The evidence for improved phonological awareness skills and speech production is clear given the
use of the research design and the check on fidelity. It is noteworthy that progress was achieved
with 8 hours and 20 minutes of 1:1 intervention provided twice weekly for 5 weeks.
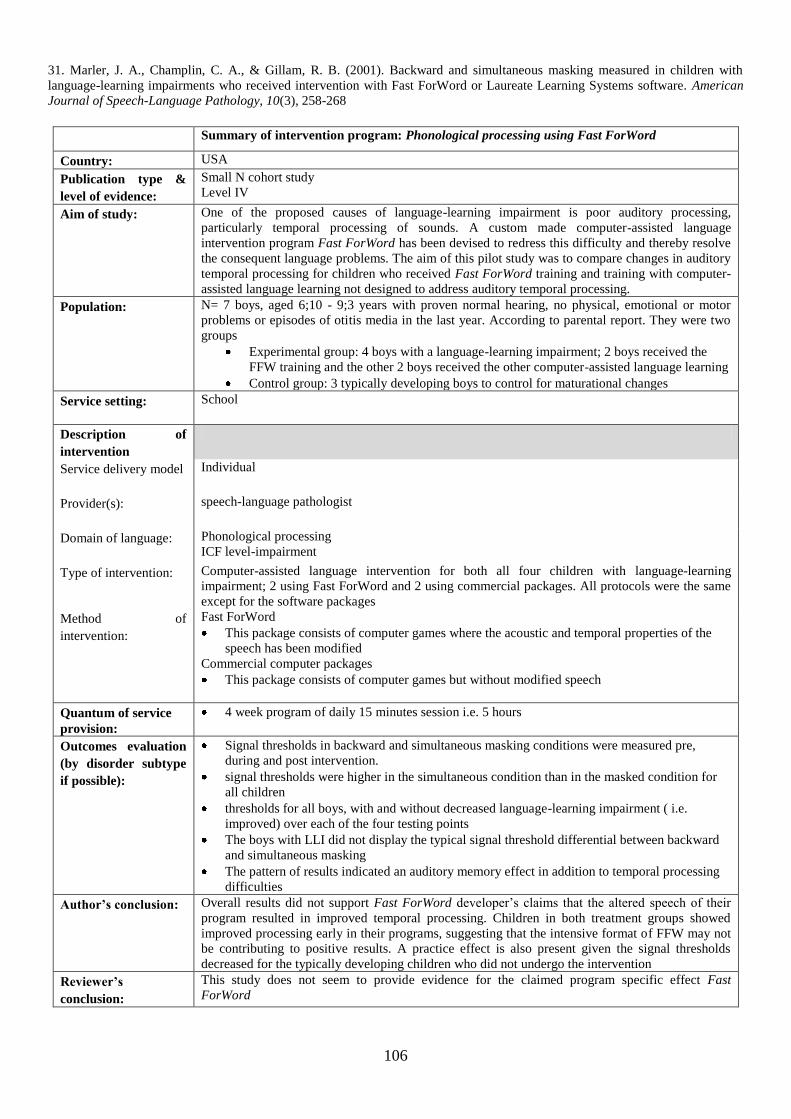
106
31. Marler, J. A., Champlin, C. A., & Gillam, R. B. (2001). Backward and simultaneous masking measured in children with
language-learning impairments who received intervention with Fast ForWord or Laureate Learning Systems software. American
Journal of Speech-Language Pathology, 10(3), 258-268
Summary of intervention program: Phonological processing using Fast ForWord
Country: USA
Publication type &
level of evidence:
Small N cohort study
Level IV
Aim of study:
One of the proposed causes of language-learning impairment is poor auditory processing,
particularly temporal processing of sounds. A custom made computer-assisted language
intervention program Fast ForWord has been devised to redress this difficulty and thereby resolve
the consequent language problems. The aim of this pilot study was to compare changes in auditory
temporal processing for children who received Fast ForWord training and training with computer-
assisted language learning not designed to address auditory temporal processing.
Population:
N= 7 boys, aged 6;10 - 9;3 years with proven normal hearing, no physical, emotional or motor
problems or episodes of otitis media in the last year. According to parental report. They were two
groups
Experimental group: 4 boys with a language-learning impairment; 2 boys received the
FFW training and the other 2 boys received the other computer-assisted language learning
Control group: 3 typically developing boys to control for maturational changes
Service setting:
School
Description of
intervention
Service delivery model
Individual
Provider(s):
speech-language pathologist
Domain of language:
Phonological processing
ICF level-impairment
Type of intervention:
Computer-assisted language intervention for both all four children with language-learning
impairment; 2 using Fast ForWord and 2 using commercial packages. All protocols were the same
except for the software packages
Method of
intervention:
Fast ForWord
This package consists of computer games where the acoustic and temporal properties of the
speech has been modified
Commercial computer packages
This package consists of computer games but without modified speech
Quantum of service
provision:
4 week program of daily 15 minutes session i.e. 5 hours
Outcomes evaluation
(by disorder subtype
if possible):
Signal thresholds in backward and simultaneous masking conditions were measured pre,
during and post intervention.
signal thresholds were higher in the simultaneous condition than in the masked condition for
all children
thresholds for all boys, with and without decreased language-learning impairment ( i.e.
improved) over each of the four testing points
The boys with LLI did not display the typical signal threshold differential between backward
and simultaneous masking
The pattern of results indicated an auditory memory effect in addition to temporal processing
difficulties
Author’s conclusion:
Overall results did not support Fast ForWord developer‟s claims that the altered speech of their
program resulted in improved temporal processing. Children in both treatment groups showed
improved processing early in their programs, suggesting that the intensive format of FFW may not
be contributing to positive results. A practice effect is also present given the signal thresholds
decreased for the typically developing children who did not undergo the intervention
Reviewer’s
conclusion:
This study does not seem to provide evidence for the claimed program specific effect Fast
ForWord
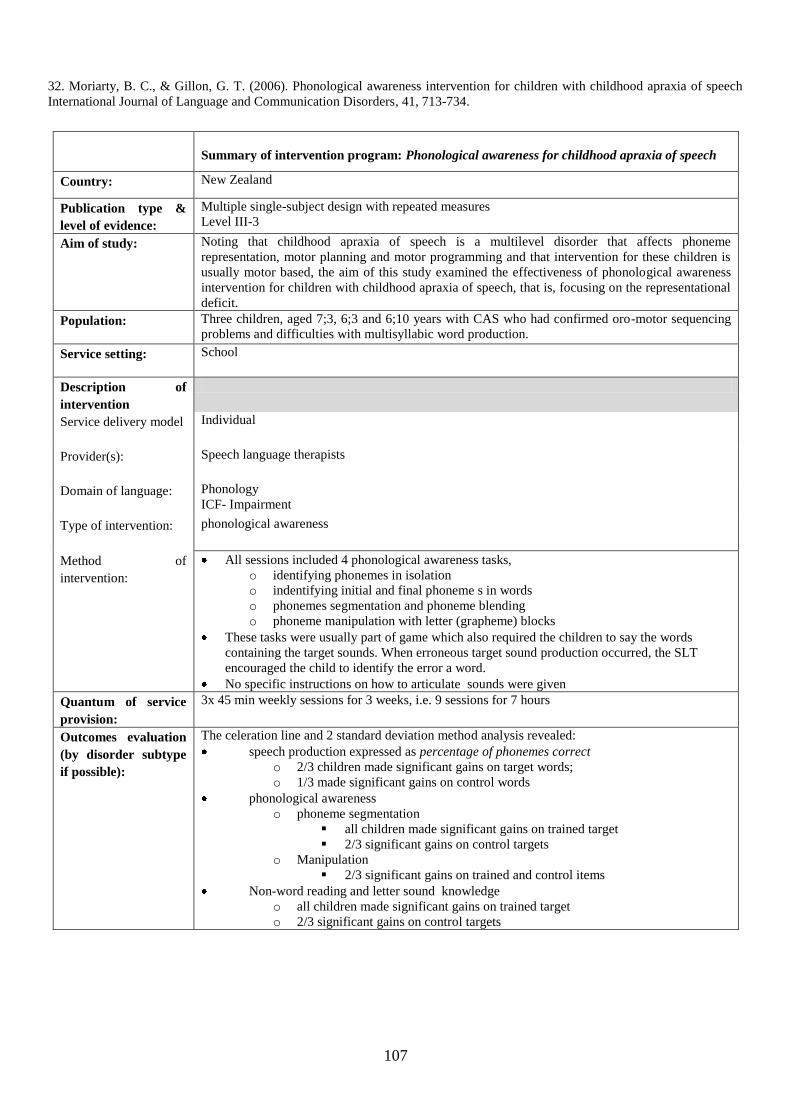
107
32. Moriarty, B. C., & Gillon, G. T. (2006). Phonological awareness intervention for children with childhood apraxia of speech
International Journal of Language and Communication Disorders, 41, 713-734.
Summary of intervention program: Phonological awareness for childhood apraxia of speech
Country: New Zealand
Publication type &
level of evidence:
Multiple single-subject design with repeated measures
Level III-3
Aim of study:
Noting that childhood apraxia of speech is a multilevel disorder that affects phoneme
representation, motor planning and motor programming and that intervention for these children is
usually motor based, the aim of this study examined the effectiveness of phonological awareness
intervention for children with childhood apraxia of speech, that is, focusing on the representational
deficit.
Population:
Three children, aged 7;3, 6;3 and 6;10 years with CAS who had confirmed oro-motor sequencing
problems and difficulties with multisyllabic word production.
Service setting:
School
Description of
intervention
Service delivery model
Individual
Provider(s):
Speech language therapists
Domain of language:
Phonology
ICF- Impairment
Type of intervention:
phonological awareness
Method of
intervention:
All sessions included 4 phonological awareness tasks,
o identifying phonemes in isolation
o indentifying initial and final phoneme s in words
o phonemes segmentation and phoneme blending
o phoneme manipulation with letter (grapheme) blocks
These tasks were usually part of game which also required the children to say the words
containing the target sounds. When erroneous target sound production occurred, the SLT
encouraged the child to identify the error a word.
No specific instructions on how to articulate sounds were given
Quantum of service
provision:
3x 45 min weekly sessions for 3 weeks, i.e. 9 sessions for 7 hours
Outcomes evaluation
(by disorder subtype
if possible):
The celeration line and 2 standard deviation method analysis revealed:
speech production expressed as percentage of phonemes correct
o 2/3 children made significant gains on target words;
o 1/3 made significant gains on control words
phonological awareness
o phoneme segmentation
all children made significant gains on trained target
2/3 significant gains on control targets
o Manipulation
2/3 significant gains on trained and control items
Non-word reading and letter sound knowledge
o all children made significant gains on trained target
o 2/3 significant gains on control targets

108
Author’s conclusion:
This investigation revealed that an integrated phonological awareness intervention can
facilitate speech production, phonological awareness, linking letters and sounds and decoding
for some children with CAS as 2/3 children made significant progress on target and control
targets across these areas.
The study supports notion that CAS is a multilevel impairment
Supports that short periods on intense therapy over a 3-week time frame achieves significant
change for some children.
Reviewer’s
conclusion:
This study seems robust in design and method (e.g. fidelity check) that allow one to agree with the
cautious conclusions that the authors make given the acknowledged limitations. These include no
follow up and that intervention was not limited to representational work. However, it does provide
evidence that an intervention that has as its primary focus phonological awareness work has the
capacity to bring about change in children‟s production. The child who did not make progress does
not fit the usual criteria for CAS as his non-verbal skills were below normal limits.
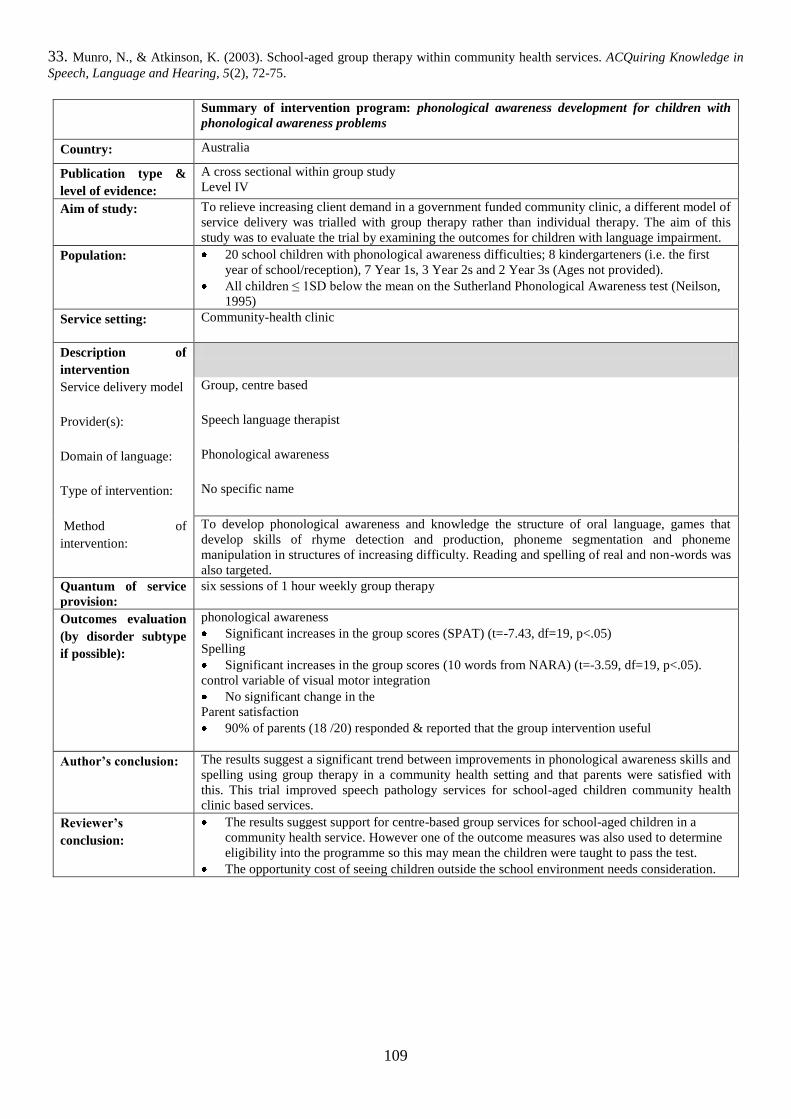
109
33. Munro, N., & Atkinson, K. (2003). School-aged group therapy within community health services. ACQuiring Knowledge in
Speech, Language and Hearing, 5(2), 72-75.
Summary of intervention program: phonological awareness development for children with
phonological awareness problems
Country: Australia
Publication type &
level of evidence:
A cross sectional within group study
Level IV
Aim of study:
To relieve increasing client demand in a government funded community clinic, a different model of
service delivery was trialled with group therapy rather than individual therapy. The aim of this
study was to evaluate the trial by examining the outcomes for children with language impairment.
Population:
20 school children with phonological awareness difficulties; 8 kindergarteners (i.e. the first
year of school/reception), 7 Year 1s, 3 Year 2s and 2 Year 3s (Ages not provided).
All children ≤ 1SD below the mean on the Sutherland Phonological Awareness test (Neilson,
1995)
Service setting:
Community-health clinic
Description of
intervention
Service delivery model
Group, centre based
Provider(s):
Speech language therapist
Domain of language:
Phonological awareness
Type of intervention:
No specific name
Method of
intervention:
To develop phonological awareness and knowledge the structure of oral language, games that
develop skills of rhyme detection and production, phoneme segmentation and phoneme
manipulation in structures of increasing difficulty. Reading and spelling of real and non-words was
also targeted.
Quantum of service
provision:
six sessions of 1 hour weekly group therapy
Outcomes evaluation
(by disorder subtype
if possible):
phonological awareness
Significant increases in the group scores (SPAT) (t=-7.43, df=19, p<.05)
Spelling
Significant increases in the group scores (10 words from NARA) (t=-3.59, df=19, p<.05).
control variable of visual motor integration
No significant change in the
Parent satisfaction
90% of parents (18 /20) responded & reported that the group intervention useful
Author’s conclusion:
The results suggest a significant trend between improvements in phonological awareness skills and
spelling using group therapy in a community health setting and that parents were satisfied with
this. This trial improved speech pathology services for school-aged children community health
clinic based services.
Reviewer’s
conclusion:
The results suggest support for centre-based group services for school-aged children in a
community health service. However one of the outcome measures was also used to determine
eligibility into the programme so this may mean the children were taught to pass the test.
The opportunity cost of seeing children outside the school environment needs consideration.
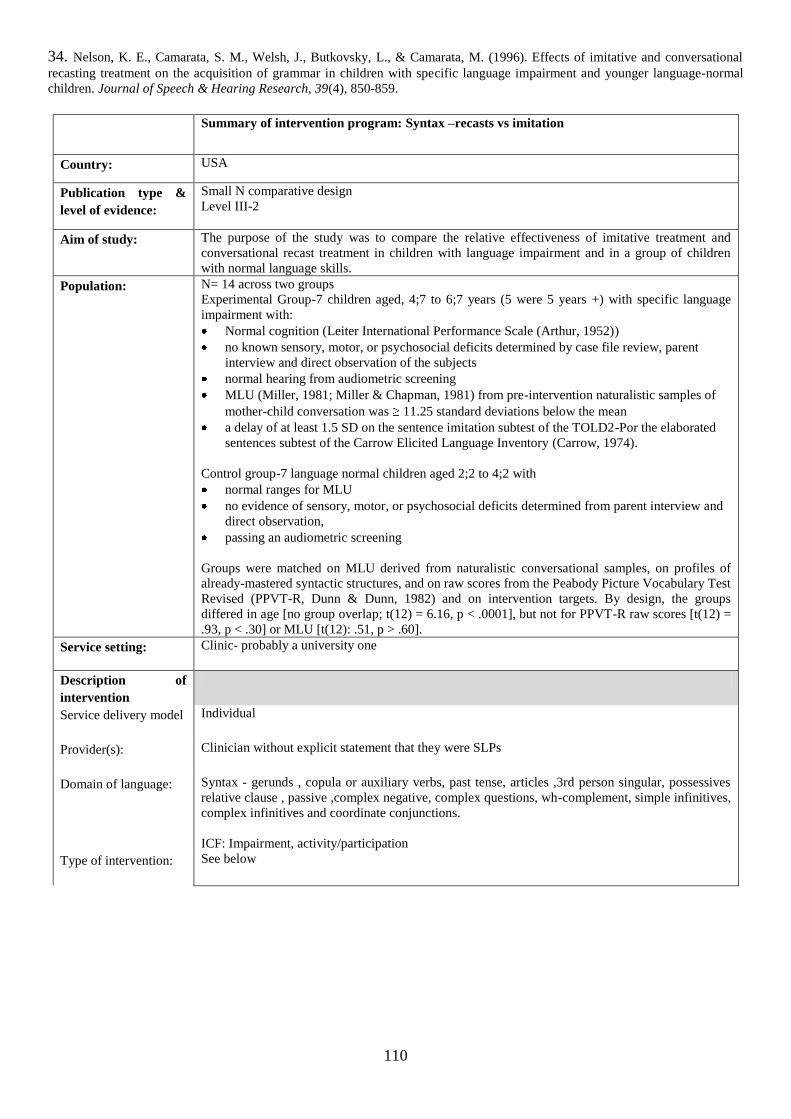
110
34. Nelson, K. E., Camarata, S. M., Welsh, J., Butkovsky, L., & Camarata, M. (1996). Effects of imitative and conversational
recasting treatment on the acquisition of grammar in children with specific language impairment and younger language-normal
children. Journal of Speech & Hearing Research, 39(4), 850-859.
Summary of intervention program: Syntax –recasts vs imitation
Country: USA
Publication type &
level of evidence:
Small N comparative design
Level III-2
Aim of study:
The purpose of the study was to compare the relative effectiveness of imitative treatment and
conversational recast treatment in children with language impairment and in a group of children
with normal language skills.
Population:
N= 14 across two groups
Experimental Group-7 children aged, 4;7 to 6;7 years (5 were 5 years +) with specific language
impairment with:
Normal cognition (Leiter International Performance Scale (Arthur, 1952))
no known sensory, motor, or psychosocial deficits determined by case file review, parent
interview and direct observation of the subjects
normal hearing from audiometric screening
MLU (Miller, 1981; Miller & Chapman, 1981) from pre-intervention naturalistic samples of
mother-child conversation was 11.25 standard deviations below the mean
a delay of at least 1.5 SD on the sentence imitation subtest of the TOLD2-Por the elaborated
sentences subtest of the Carrow Elicited Language Inventory (Carrow, 1974).
Control group-7 language normal children aged 2;2 to 4;2 with
normal ranges for MLU
no evidence of sensory, motor, or psychosocial deficits determined from parent interview and
direct observation,
passing an audiometric screening
Groups were matched on MLU derived from naturalistic conversational samples, on profiles of
already-mastered syntactic structures, and on raw scores from the Peabody Picture Vocabulary Test
Revised (PPVT-R, Dunn & Dunn, 1982) and on intervention targets. By design, the groups
differed in age [no group overlap; t(12) = 6.16, p < .0001], but not for PPVT-R raw scores [t(12) =
.93, p < .30] or MLU [t(12): .51, p > .60].
Service setting:
Clinic- probably a university one
Description of
intervention
Service delivery model
Individual
Provider(s):
Clinician without explicit statement that they were SLPs
Domain of language:
Syntax - gerunds , copula or auxiliary verbs, past tense, articles ,3rd person singular, possessives
relative clause , passive ,complex negative, complex questions, wh-complement, simple infinitives,
complex infinitives and coordinate conjunctions.
ICF: Impairment, activity/participation
Type of intervention:
See below
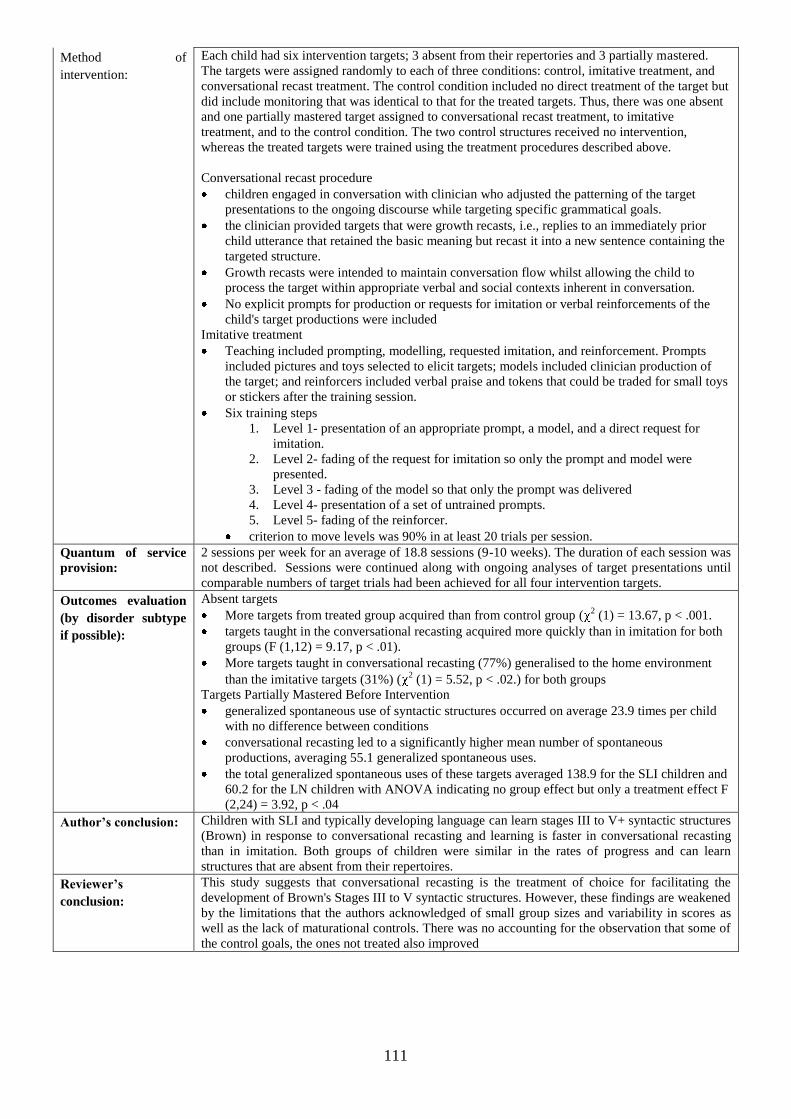
111
Method of
intervention:
Each child had six intervention targets; 3 absent from their repertories and 3 partially mastered.
The targets were assigned randomly to each of three conditions: control, imitative treatment, and
conversational recast treatment. The control condition included no direct treatment of the target but
did include monitoring that was identical to that for the treated targets. Thus, there was one absent
and one partially mastered target assigned to conversational recast treatment, to imitative
treatment, and to the control condition. The two control structures received no intervention,
whereas the treated targets were trained using the treatment procedures described above.
Conversational recast procedure
children engaged in conversation with clinician who adjusted the patterning of the target
presentations to the ongoing discourse while targeting specific grammatical goals.
the clinician provided targets that were growth recasts, i.e., replies to an immediately prior
child utterance that retained the basic meaning but recast it into a new sentence containing the
targeted structure.
Growth recasts were intended to maintain conversation flow whilst allowing the child to
process the target within appropriate verbal and social contexts inherent in conversation.
No explicit prompts for production or requests for imitation or verbal reinforcements of the
child's target productions were included
Imitative treatment
Teaching included prompting, modelling, requested imitation, and reinforcement. Prompts
included pictures and toys selected to elicit targets; models included clinician production of
the target; and reinforcers included verbal praise and tokens that could be traded for small toys
or stickers after the training session.
Six training steps
1. Level 1- presentation of an appropriate prompt, a model, and a direct request for
imitation.
2. Level 2- fading of the request for imitation so only the prompt and model were
presented.
3. Level 3 - fading of the model so that only the prompt was delivered
4. Level 4- presentation of a set of untrained prompts.
5. Level 5- fading of the reinforcer.
criterion to move levels was 90% in at least 20 trials per session.
Quantum of service
provision:
2 sessions per week for an average of 18.8 sessions (9-10 weeks). The duration of each session was
not described. Sessions were continued along with ongoing analyses of target presentations until
comparable numbers of target trials had been achieved for all four intervention targets.
Outcomes evaluation
(by disorder subtype
if possible):
Absent targets
More targets from treated group acquired than from control group (2 (1) = 13.67, p < .001.
targets taught in the conversational recasting acquired more quickly than in imitation for both
groups (F (1,12) = 9.17, p < .01).
More targets taught in conversational recasting (77%) generalised to the home environment
than the imitative targets (31%) (2 (1) = 5.52, p < .02.) for both groups
Targets Partially Mastered Before Intervention
generalized spontaneous use of syntactic structures occurred on average 23.9 times per child
with no difference between conditions
conversational recasting led to a significantly higher mean number of spontaneous
productions, averaging 55.1 generalized spontaneous uses.
the total generalized spontaneous uses of these targets averaged 138.9 for the SLI children and
60.2 for the LN children with ANOVA indicating no group effect but only a treatment effect F
(2,24) = 3.92, p < .04
Author’s conclusion:
Children with SLI and typically developing language can learn stages III to V+ syntactic structures
(Brown) in response to conversational recasting and learning is faster in conversational recasting
than in imitation. Both groups of children were similar in the rates of progress and can learn
structures that are absent from their repertoires.
Reviewer’s
conclusion:
This study suggests that conversational recasting is the treatment of choice for facilitating the
development of Brown's Stages III to V syntactic structures. However, these findings are weakened
by the limitations that the authors acknowledged of small group sizes and variability in scores as
well as the lack of maturational controls. There was no accounting for the observation that some of
the control goals, the ones not treated also improved
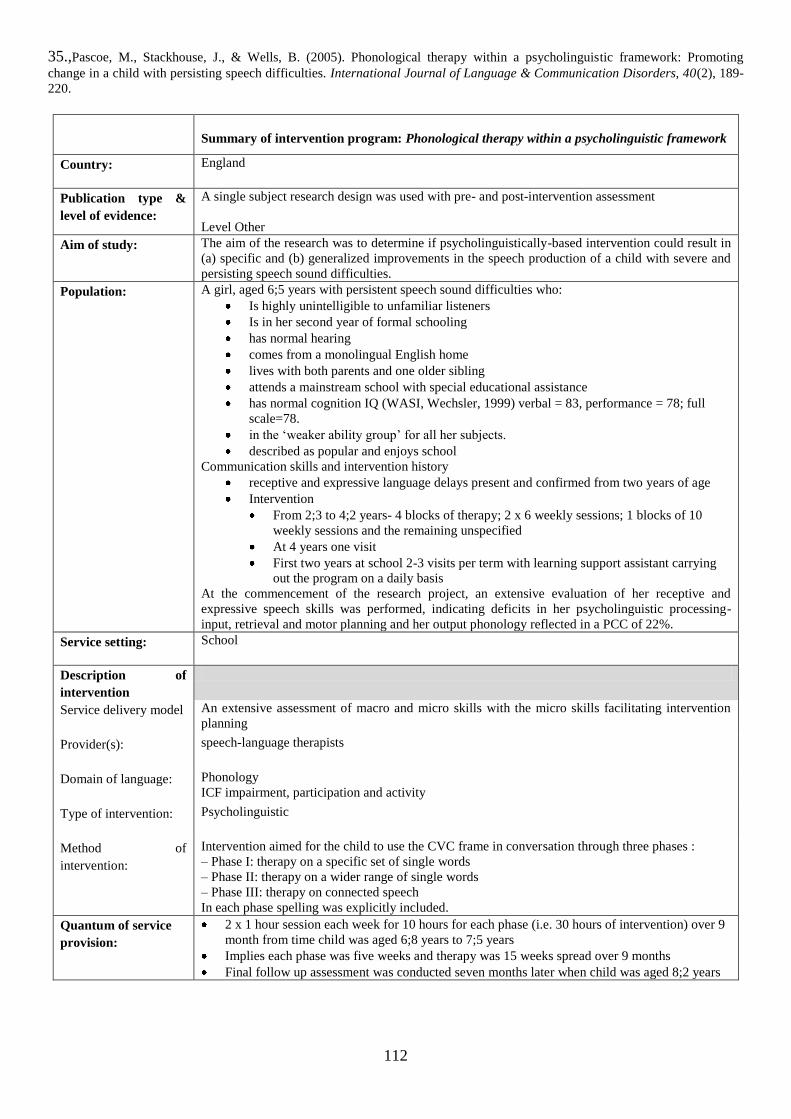
112
35.,Pascoe, M., Stackhouse, J., & Wells, B. (2005). Phonological therapy within a psycholinguistic framework: Promoting
change in a child with persisting speech difficulties. International Journal of Language & Communication Disorders, 40(2), 189-
220.
Summary of intervention program: Phonological therapy within a psycholinguistic framework
Country: England
Publication type &
level of evidence:
A single subject research design was used with pre- and post-intervention assessment
Level Other
Aim of study:
The aim of the research was to determine if psycholinguistically-based intervention could result in
(a) specific and (b) generalized improvements in the speech production of a child with severe and
persisting speech sound difficulties.
Population:
A girl, aged 6;5 years with persistent speech sound difficulties who:
Is highly unintelligible to unfamiliar listeners
Is in her second year of formal schooling
has normal hearing
comes from a monolingual English home
lives with both parents and one older sibling
attends a mainstream school with special educational assistance
has normal cognition IQ (WASI, Wechsler, 1999) verbal = 83, performance = 78; full
scale=78.
in the „weaker ability group‟ for all her subjects.
described as popular and enjoys school
Communication skills and intervention history
receptive and expressive language delays present and confirmed from two years of age
Intervention
From 2;3 to 4;2 years- 4 blocks of therapy; 2 x 6 weekly sessions; 1 blocks of 10
weekly sessions and the remaining unspecified
At 4 years one visit
First two years at school 2-3 visits per term with learning support assistant carrying
out the program on a daily basis
At the commencement of the research project, an extensive evaluation of her receptive and
expressive speech skills was performed, indicating deficits in her psycholinguistic processing-
input, retrieval and motor planning and her output phonology reflected in a PCC of 22%.
Service setting:
School
Description of
intervention
Service delivery model
An extensive assessment of macro and micro skills with the micro skills facilitating intervention
planning
Provider(s):
speech-language therapists
Domain of language:
Phonology
ICF impairment, participation and activity
Type of intervention:
Psycholinguistic
Method of
intervention:
Intervention aimed for the child to use the CVC frame in conversation through three phases :
– Phase I: therapy on a specific set of single words
– Phase II: therapy on a wider range of single words
– Phase III: therapy on connected speech
In each phase spelling was explicitly included.
Quantum of service
provision:
2 x 1 hour session each week for 10 hours for each phase (i.e. 30 hours of intervention) over 9
month from time child was aged 6;8 years to 7;5 years
Implies each phase was five weeks and therapy was 15 weeks spread over 9 months
Final follow up assessment was conducted seven months later when child was aged 8;2 years
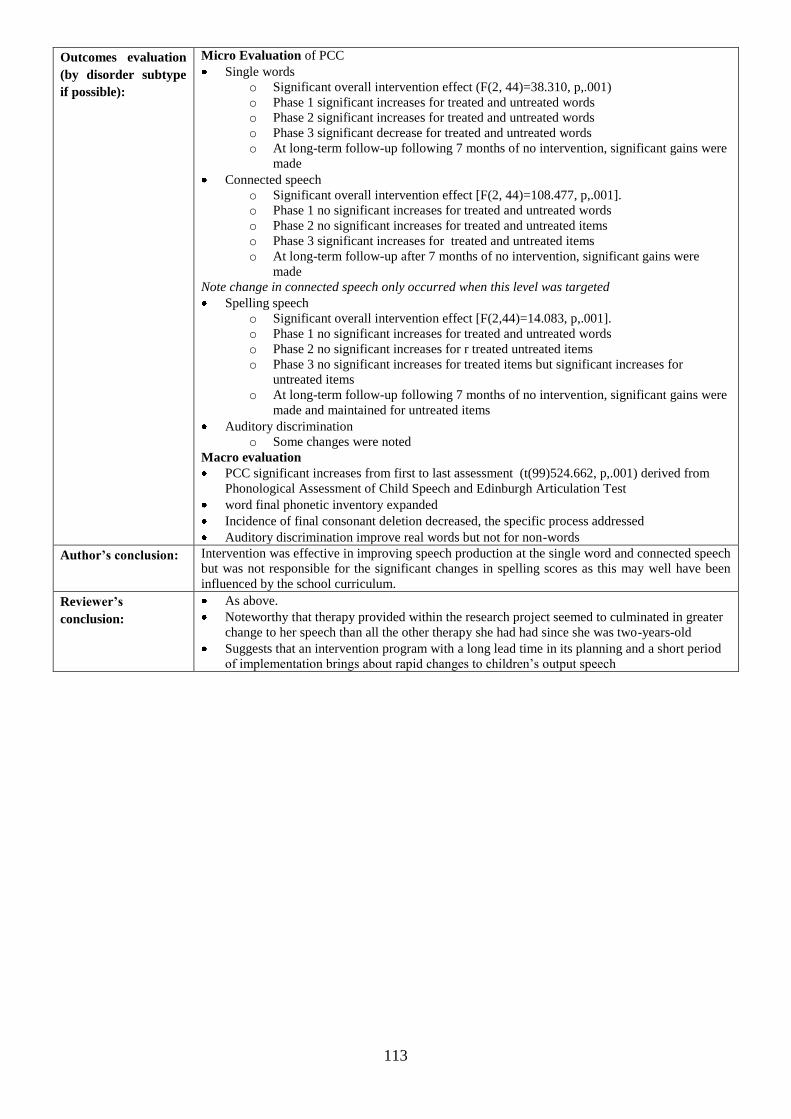
113
Outcomes evaluation
(by disorder subtype
if possible):
Micro Evaluation of PCC
Single words
o Significant overall intervention effect (F(2, 44)=38.310, p,.001)
o Phase 1 significant increases for treated and untreated words
o Phase 2 significant increases for treated and untreated words
o Phase 3 significant decrease for treated and untreated words
o At long-term follow-up following 7 months of no intervention, significant gains were
made
Connected speech
o Significant overall intervention effect [F(2, 44)=108.477, p,.001].
o Phase 1 no significant increases for treated and untreated words
o Phase 2 no significant increases for treated and untreated items
o Phase 3 significant increases for treated and untreated items
o At long-term follow-up after 7 months of no intervention, significant gains were
made
Note change in connected speech only occurred when this level was targeted
Spelling speech
o Significant overall intervention effect [F(2,44)=14.083, p,.001].
o Phase 1 no significant increases for treated and untreated words
o Phase 2 no significant increases for r treated untreated items
o Phase 3 no significant increases for treated items but significant increases for
untreated items
o At long-term follow-up following 7 months of no intervention, significant gains were
made and maintained for untreated items
Auditory discrimination
o Some changes were noted
Macro evaluation
PCC significant increases from first to last assessment (t(99)524.662, p,.001) derived from
Phonological Assessment of Child Speech and Edinburgh Articulation Test
word final phonetic inventory expanded
Incidence of final consonant deletion decreased, the specific process addressed
Auditory discrimination improve real words but not for non-words
Author’s conclusion:
Intervention was effective in improving speech production at the single word and connected speech
but was not responsible for the significant changes in spelling scores as this may well have been
influenced by the school curriculum.
Reviewer’s
conclusion:
As above.
Noteworthy that therapy provided within the research project seemed to culminated in greater
change to her speech than all the other therapy she had had since she was two-years-old
Suggests that an intervention program with a long lead time in its planning and a short period
of implementation brings about rapid changes to children‟s output speech
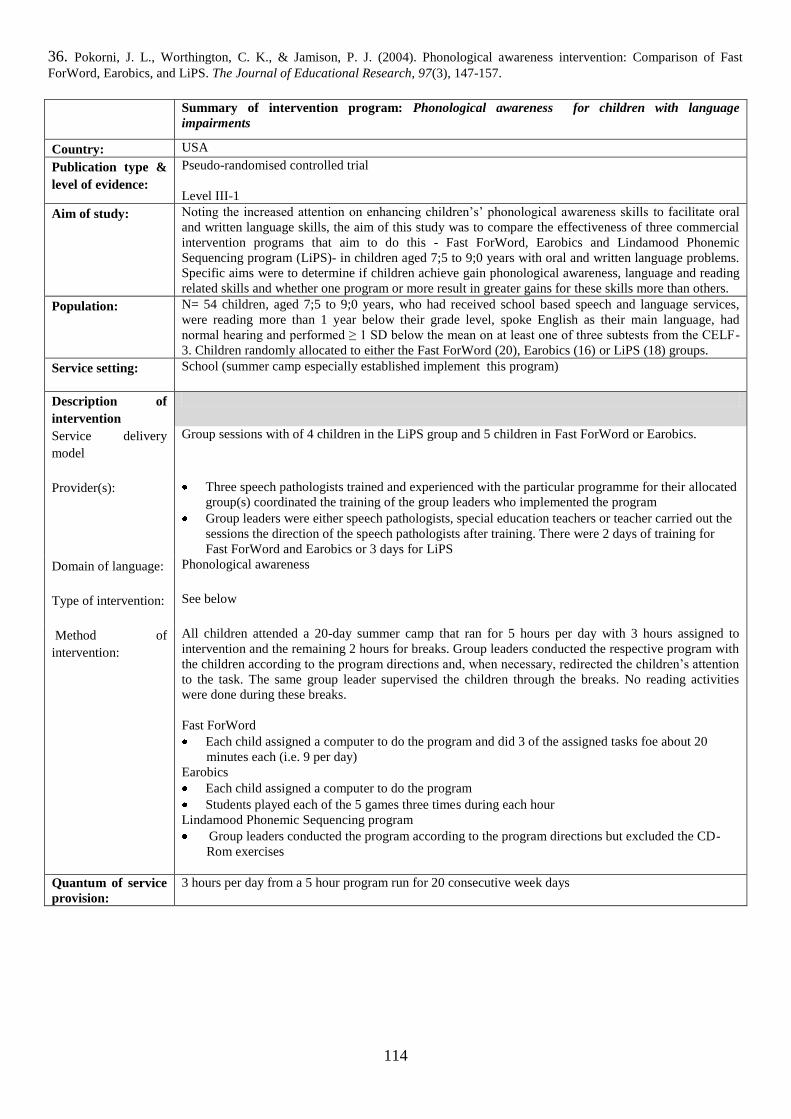
114
36. Pokorni, J. L., Worthington, C. K., & Jamison, P. J. (2004). Phonological awareness intervention: Comparison of Fast
ForWord, Earobics, and LiPS. The Journal of Educational Research, 97(3), 147-157.
Summary of intervention program: Phonological awareness for children with language
impairments
Country: USA
Publication type &
level of evidence:
Pseudo-randomised controlled trial
Level III-1
Aim of study:
Noting the increased attention on enhancing children‟s‟ phonological awareness skills to facilitate oral
and written language skills, the aim of this study was to compare the effectiveness of three commercial
intervention programs that aim to do this - Fast ForWord, Earobics and Lindamood Phonemic
Sequencing program (LiPS)- in children aged 7;5 to 9;0 years with oral and written language problems.
Specific aims were to determine if children achieve gain phonological awareness, language and reading
related skills and whether one program or more result in greater gains for these skills more than others.
Population:
N= 54 children, aged 7;5 to 9;0 years, who had received school based speech and language services,
were reading more than 1 year below their grade level, spoke English as their main language, had
normal hearing and performed ≥ 1 SD below the mean on at least one of three subtests from the CELF-
3. Children randomly allocated to either the Fast ForWord (20), Earobics (16) or LiPS (18) groups.
Service setting:
School (summer camp especially established implement this program)
Description of
intervention
Service delivery
model
Group sessions with of 4 children in the LiPS group and 5 children in Fast ForWord or Earobics.
Provider(s):
Three speech pathologists trained and experienced with the particular programme for their allocated
group(s) coordinated the training of the group leaders who implemented the program
Group leaders were either speech pathologists, special education teachers or teacher carried out the
sessions the direction of the speech pathologists after training. There were 2 days of training for
Fast ForWord and Earobics or 3 days for LiPS
Domain of language:
Phonological awareness
Type of intervention:
See below
Method of
intervention:
All children attended a 20-day summer camp that ran for 5 hours per day with 3 hours assigned to
intervention and the remaining 2 hours for breaks. Group leaders conducted the respective program with
the children according to the program directions and, when necessary, redirected the children‟s attention
to the task. The same group leader supervised the children through the breaks. No reading activities
were done during these breaks.
Fast ForWord
Each child assigned a computer to do the program and did 3 of the assigned tasks foe about 20
minutes each (i.e. 9 per day)
Earobics
Each child assigned a computer to do the program
Students played each of the 5 games three times during each hour
Lindamood Phonemic Sequencing program
Group leaders conducted the program according to the program directions but excluded the CD-
Rom exercises
Quantum of service
provision:
3 hours per day from a 5 hour program run for 20 consecutive week days
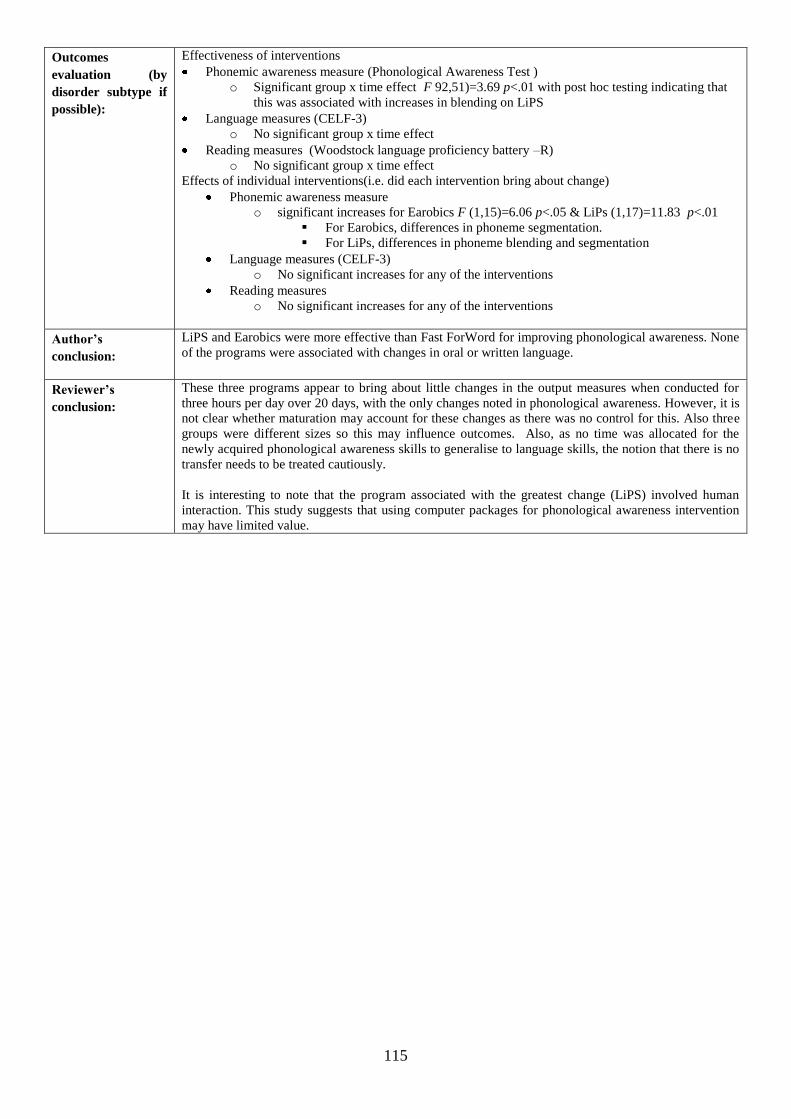
115
Outcomes
evaluation (by
disorder subtype if
possible):
Effectiveness of interventions
Phonemic awareness measure (Phonological Awareness Test )
o Significant group x time effect F 92,51)=3.69 p<.01 with post hoc testing indicating that
this was associated with increases in blending on LiPS
Language measures (CELF-3)
o No significant group x time effect
Reading measures (Woodstock language proficiency battery –R)
o No significant group x time effect
Effects of individual interventions(i.e. did each intervention bring about change)
Phonemic awareness measure
o significant increases for Earobics F (1,15)=6.06 p<.05 & LiPs (1,17)=11.83 p<.01
For Earobics, differences in phoneme segmentation.
For LiPs, differences in phoneme blending and segmentation
Language measures (CELF-3)
o No significant increases for any of the interventions
Reading measures
o No significant increases for any of the interventions
Author’s
conclusion:
LiPS and Earobics were more effective than Fast ForWord for improving phonological awareness. None
of the programs were associated with changes in oral or written language.
Reviewer’s
conclusion:
These three programs appear to bring about little changes in the output measures when conducted for
three hours per day over 20 days, with the only changes noted in phonological awareness. However, it is
not clear whether maturation may account for these changes as there was no control for this. Also three
groups were different sizes so this may influence outcomes. Also, as no time was allocated for the
newly acquired phonological awareness skills to generalise to language skills, the notion that there is no
transfer needs to be treated cautiously.
It is interesting to note that the program associated with the greatest change (LiPS) involved human
interaction. This study suggests that using computer packages for phonological awareness intervention
may have limited value.
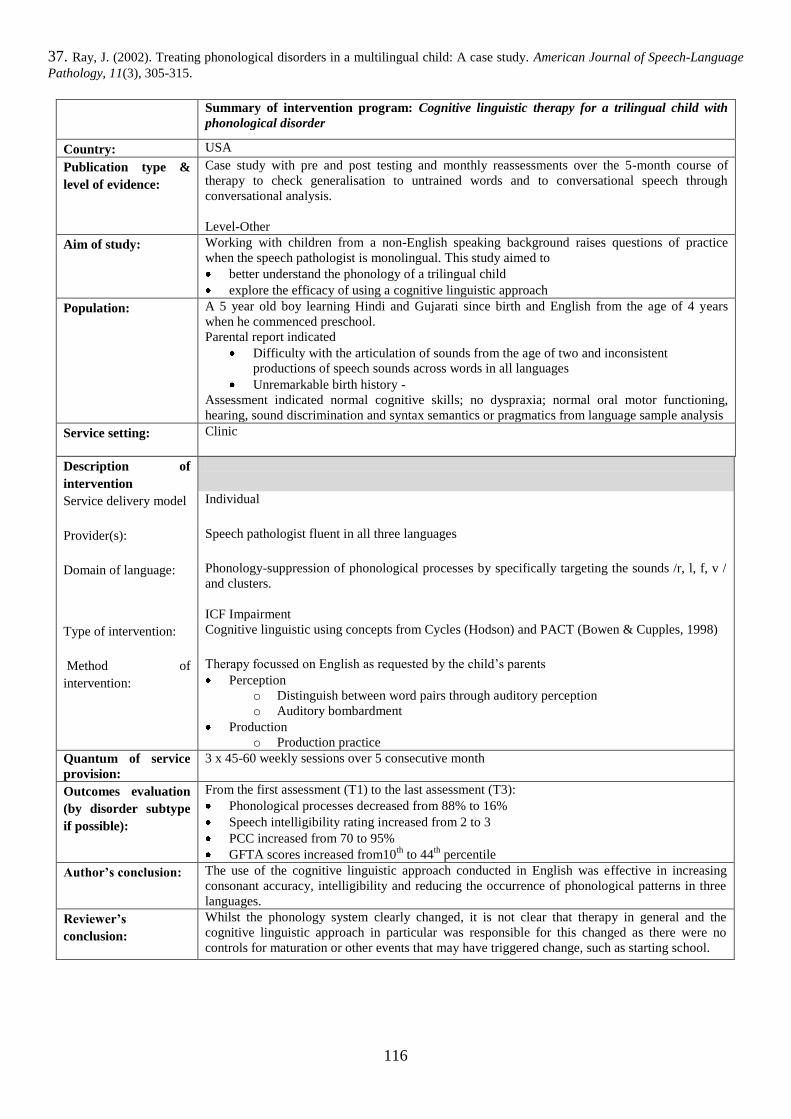
116
37. Ray, J. (2002). Treating phonological disorders in a multilingual child: A case study. American Journal of Speech-Language
Pathology, 11(3), 305-315.
Summary of intervention program: Cognitive linguistic therapy for a trilingual child with
phonological disorder
Country: USA
Publication type &
level of evidence:
Case study with pre and post testing and monthly reassessments over the 5-month course of
therapy to check generalisation to untrained words and to conversational speech through
conversational analysis.
Level-Other
Aim of study:
Working with children from a non-English speaking background raises questions of practice
when the speech pathologist is monolingual. This study aimed to
better understand the phonology of a trilingual child
explore the efficacy of using a cognitive linguistic approach
Population:
A 5 year old boy learning Hindi and Gujarati since birth and English from the age of 4 years
when he commenced preschool.
Parental report indicated
Difficulty with the articulation of sounds from the age of two and inconsistent
productions of speech sounds across words in all languages
Unremarkable birth history -
Assessment indicated normal cognitive skills; no dyspraxia; normal oral motor functioning,
hearing, sound discrimination and syntax semantics or pragmatics from language sample analysis
Service setting:
Clinic
Description of
intervention
Service delivery model
Individual
Provider(s):
Speech pathologist fluent in all three languages
Domain of language:
Phonology-suppression of phonological processes by specifically targeting the sounds /r, l, f, v /
and clusters.
ICF Impairment
Type of intervention:
Cognitive linguistic using concepts from Cycles (Hodson) and PACT (Bowen & Cupples, 1998)
Method of
intervention:
Therapy focussed on English as requested by the child‟s parents
Perception
o Distinguish between word pairs through auditory perception
o Auditory bombardment
Production
o Production practice
Quantum of service
provision:
3 x 45-60 weekly sessions over 5 consecutive month
Outcomes evaluation
(by disorder subtype
if possible):
From the first assessment (T1) to the last assessment (T3):
Phonological processes decreased from 88% to 16%
Speech intelligibility rating increased from 2 to 3
PCC increased from 70 to 95%
GFTA scores increased from10th
to 44th
percentile
Author’s conclusion:
The use of the cognitive linguistic approach conducted in English was effective in increasing
consonant accuracy, intelligibility and reducing the occurrence of phonological patterns in three
languages.
Reviewer’s
conclusion:
Whilst the phonology system clearly changed, it is not clear that therapy in general and the
cognitive linguistic approach in particular was responsible for this changed as there were no
controls for maturation or other events that may have triggered change, such as starting school.
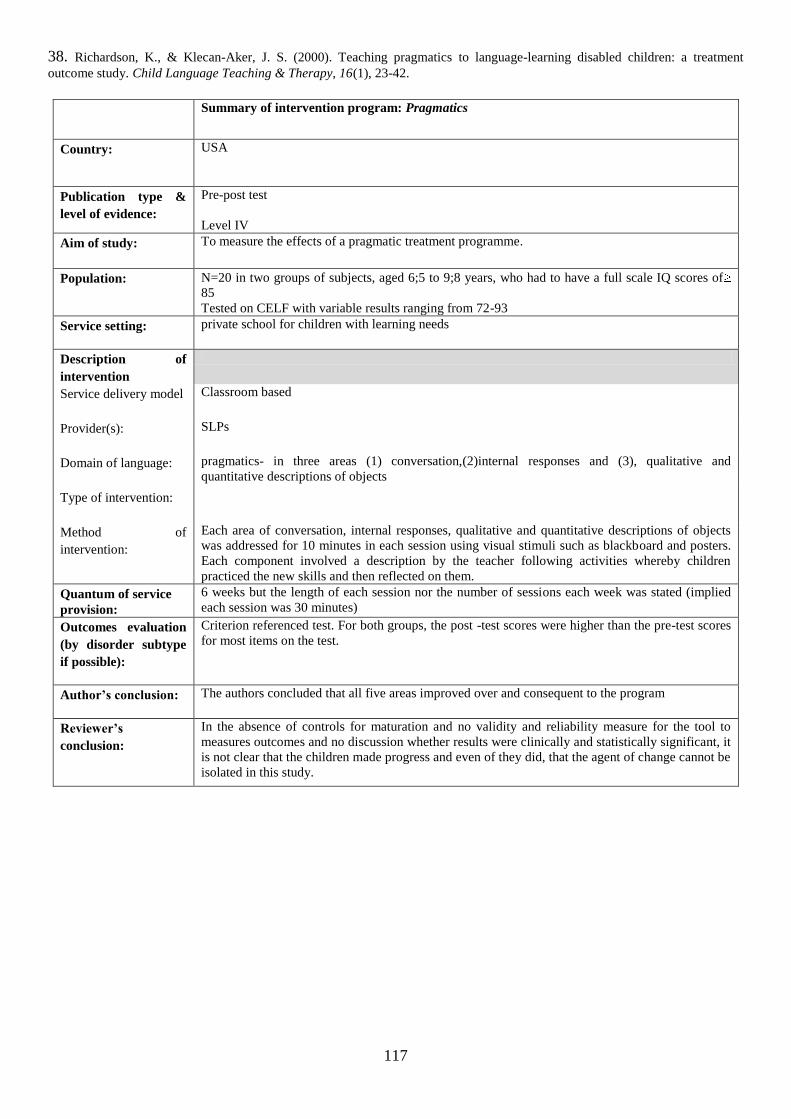
117
38. Richardson, K., & Klecan-Aker, J. S. (2000). Teaching pragmatics to language-learning disabled children: a treatment
outcome study. Child Language Teaching & Therapy, 16(1), 23-42.
Summary of intervention program: Pragmatics
Country: USA
Publication type &
level of evidence:
Pre-post test
Level IV
Aim of study:
To measure the effects of a pragmatic treatment programme.
Population:
N=20 in two groups of subjects, aged 6;5 to 9;8 years, who had to have a full scale IQ scores of
85
Tested on CELF with variable results ranging from 72-93
Service setting:
private school for children with learning needs
Description of
intervention
Service delivery model
Classroom based
Provider(s):
SLPs
Domain of language:
pragmatics- in three areas (1) conversation,(2)internal responses and (3), qualitative and
quantitative descriptions of objects
Type of intervention:
Method of
intervention:
Each area of conversation, internal responses, qualitative and quantitative descriptions of objects
was addressed for 10 minutes in each session using visual stimuli such as blackboard and posters.
Each component involved a description by the teacher following activities whereby children
practiced the new skills and then reflected on them.
Quantum of service
provision:
6 weeks but the length of each session nor the number of sessions each week was stated (implied
each session was 30 minutes)
Outcomes evaluation
(by disorder subtype
if possible):
Criterion referenced test. For both groups, the post -test scores were higher than the pre-test scores
for most items on the test.
Author’s conclusion:
The authors concluded that all five areas improved over and consequent to the program
Reviewer’s
conclusion:
In the absence of controls for maturation and no validity and reliability measure for the tool to
measures outcomes and no discussion whether results were clinically and statistically significant, it
is not clear that the children made progress and even of they did, that the agent of change cannot be
isolated in this study.
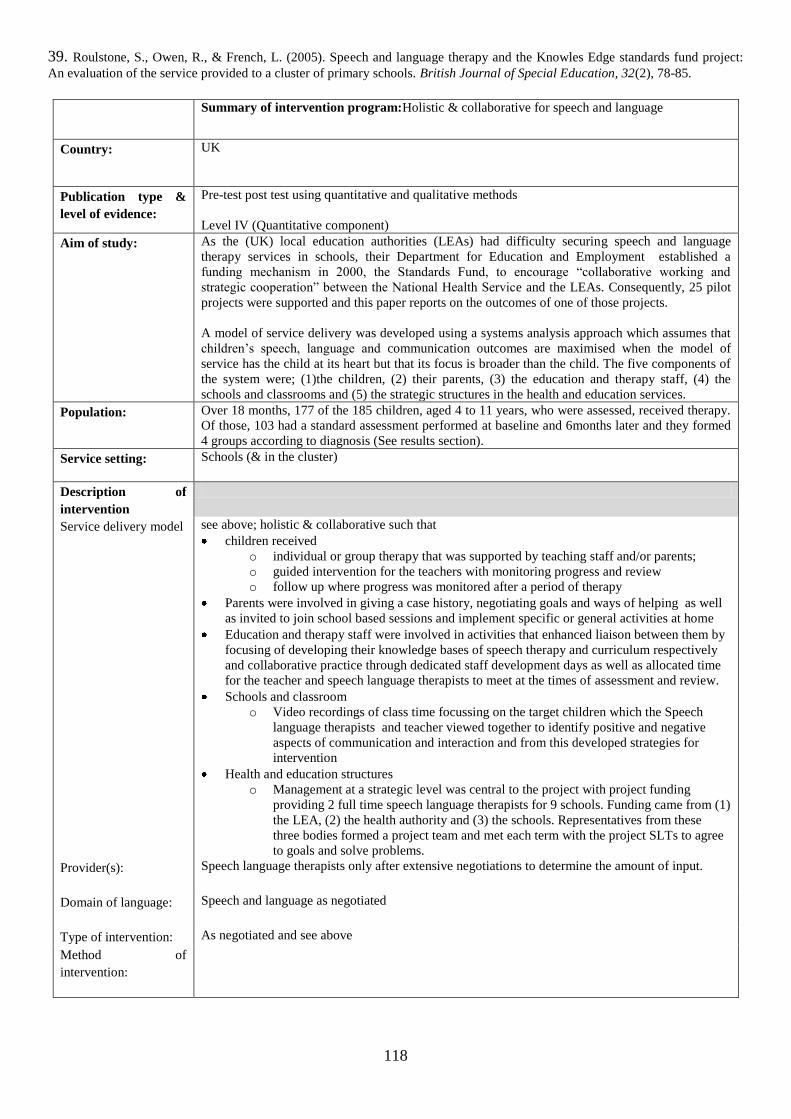
118
39. Roulstone, S., Owen, R., & French, L. (2005). Speech and language therapy and the Knowles Edge standards fund project:
An evaluation of the service provided to a cluster of primary schools. British Journal of Special Education, 32(2), 78-85.
Summary of intervention program:Holistic & collaborative for speech and language
Country: UK
Publication type &
level of evidence:
Pre-test post test using quantitative and qualitative methods
Level IV (Quantitative component)
Aim of study:
As the (UK) local education authorities (LEAs) had difficulty securing speech and language
therapy services in schools, their Department for Education and Employment established a
funding mechanism in 2000, the Standards Fund, to encourage “collaborative working and
strategic cooperation” between the National Health Service and the LEAs. Consequently, 25 pilot
projects were supported and this paper reports on the outcomes of one of those projects.
A model of service delivery was developed using a systems analysis approach which assumes that
children‟s speech, language and communication outcomes are maximised when the model of
service has the child at its heart but that its focus is broader than the child. The five components of
the system were; (1)the children, (2) their parents, (3) the education and therapy staff, (4) the
schools and classrooms and (5) the strategic structures in the health and education services.
Population:
Over 18 months, 177 of the 185 children, aged 4 to 11 years, who were assessed, received therapy.
Of those, 103 had a standard assessment performed at baseline and 6months later and they formed
4 groups according to diagnosis (See results section).
Service setting:
Schools (& in the cluster)
Description of
intervention
Service delivery model see above; holistic & collaborative such that
children received
o individual or group therapy that was supported by teaching staff and/or parents;
o guided intervention for the teachers with monitoring progress and review
o follow up where progress was monitored after a period of therapy
Parents were involved in giving a case history, negotiating goals and ways of helping as well
as invited to join school based sessions and implement specific or general activities at home
Education and therapy staff were involved in activities that enhanced liaison between them by
focusing of developing their knowledge bases of speech therapy and curriculum respectively
and collaborative practice through dedicated staff development days as well as allocated time
for the teacher and speech language therapists to meet at the times of assessment and review.
Schools and classroom
o Video recordings of class time focussing on the target children which the Speech
language therapists and teacher viewed together to identify positive and negative
aspects of communication and interaction and from this developed strategies for
intervention
Health and education structures
o Management at a strategic level was central to the project with project funding
providing 2 full time speech language therapists for 9 schools. Funding came from (1)
the LEA, (2) the health authority and (3) the schools. Representatives from these
three bodies formed a project team and met each term with the project SLTs to agree
to goals and solve problems.
Provider(s):
Speech language therapists only after extensive negotiations to determine the amount of input.
Domain of language:
Speech and language as negotiated
Type of intervention: As negotiated and see above
Method of
intervention:
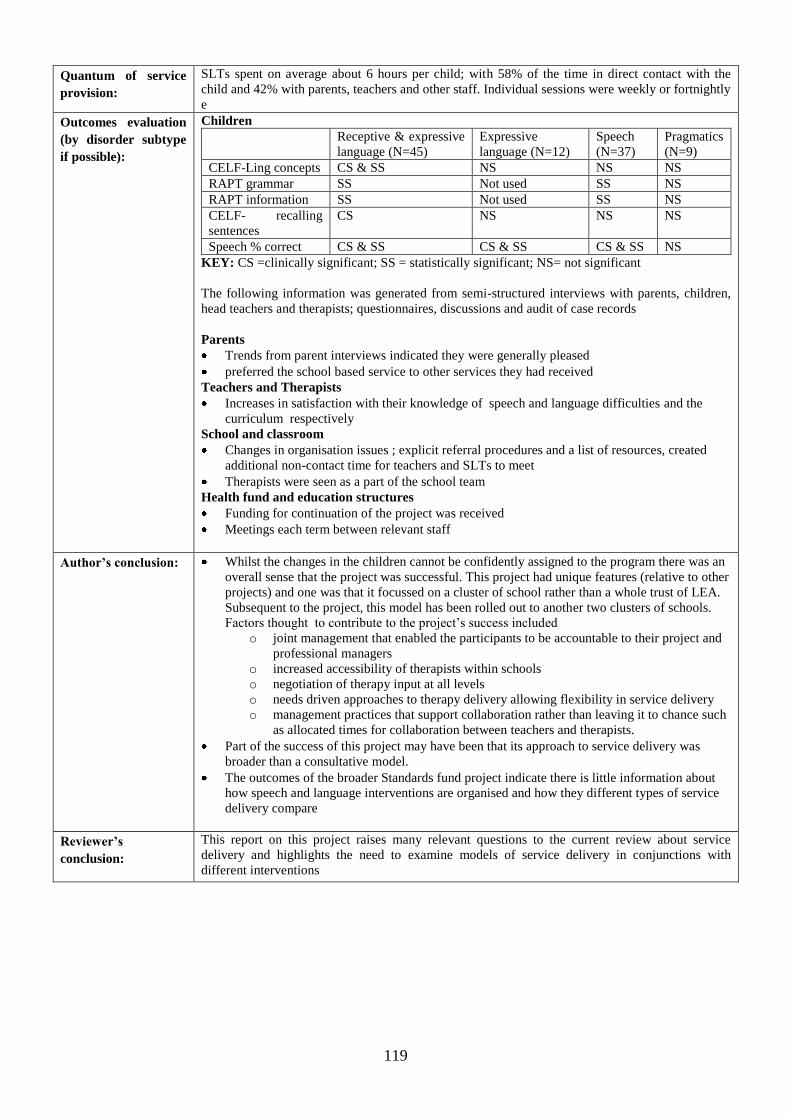
119
Quantum of service
provision:
SLTs spent on average about 6 hours per child; with 58% of the time in direct contact with the
child and 42% with parents, teachers and other staff. Individual sessions were weekly or fortnightly
e
Outcomes evaluation
(by disorder subtype
if possible):
Children
Receptive & expressive
language (N=45)
Expressive
language (N=12)
Speech
(N=37)
Pragmatics
(N=9)
CELF-Ling concepts CS & SS NS NS NS
RAPT grammar SS Not used SS NS
RAPT information SS Not used SS NS
CELF- recalling
sentences
CS NS NS NS
Speech % correct CS & SS CS & SS CS & SS NS
KEY: CS =clinically significant; SS = statistically significant; NS= not significant
The following information was generated from semi-structured interviews with parents, children,
head teachers and therapists; questionnaires, discussions and audit of case records
Parents
Trends from parent interviews indicated they were generally pleased
preferred the school based service to other services they had received
Teachers and Therapists
Increases in satisfaction with their knowledge of speech and language difficulties and the
curriculum respectively
School and classroom
Changes in organisation issues ; explicit referral procedures and a list of resources, created
additional non-contact time for teachers and SLTs to meet
Therapists were seen as a part of the school team
Health fund and education structures
Funding for continuation of the project was received
Meetings each term between relevant staff
Author’s conclusion:
Whilst the changes in the children cannot be confidently assigned to the program there was an
overall sense that the project was successful. This project had unique features (relative to other
projects) and one was that it focussed on a cluster of school rather than a whole trust of LEA.
Subsequent to the project, this model has been rolled out to another two clusters of schools.
Factors thought to contribute to the project‟s success included
o joint management that enabled the participants to be accountable to their project and
professional managers
o increased accessibility of therapists within schools
o negotiation of therapy input at all levels
o needs driven approaches to therapy delivery allowing flexibility in service delivery
o management practices that support collaboration rather than leaving it to chance such
as allocated times for collaboration between teachers and therapists.
Part of the success of this project may have been that its approach to service delivery was
broader than a consultative model.
The outcomes of the broader Standards fund project indicate there is little information about
how speech and language interventions are organised and how they different types of service
delivery compare
Reviewer’s
conclusion:
This report on this project raises many relevant questions to the current review about service
delivery and highlights the need to examine models of service delivery in conjunctions with
different interventions
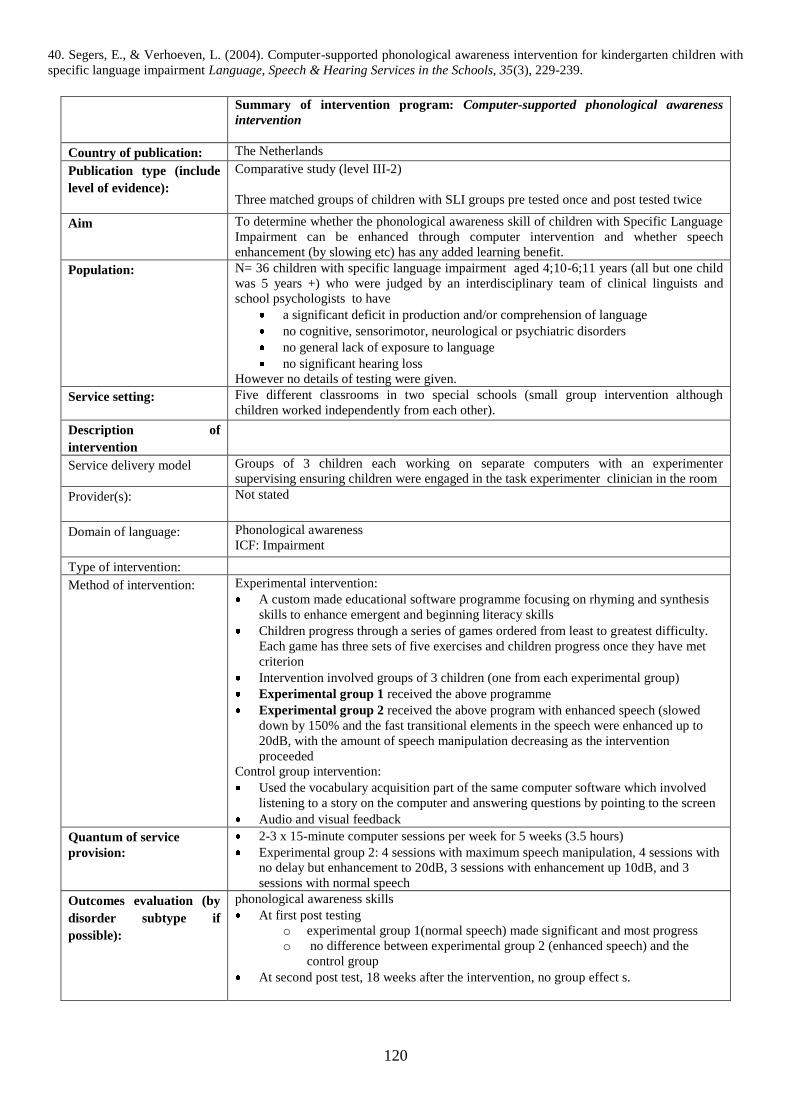
120
40. Segers, E., & Verhoeven, L. (2004). Computer-supported phonological awareness intervention for kindergarten children with
specific language impairment Language, Speech & Hearing Services in the Schools, 35(3), 229-239.
Summary of intervention program: Computer-supported phonological awareness
intervention
Country of publication: The Netherlands
Publication type (include
level of evidence):
Comparative study (level III-2)
Three matched groups of children with SLI groups pre tested once and post tested twice
Aim To determine whether the phonological awareness skill of children with Specific Language
Impairment can be enhanced through computer intervention and whether speech
enhancement (by slowing etc) has any added learning benefit.
Population:
N= 36 children with specific language impairment aged 4;10-6;11 years (all but one child
was 5 years +) who were judged by an interdisciplinary team of clinical linguists and
school psychologists to have
a significant deficit in production and/or comprehension of language
no cognitive, sensorimotor, neurological or psychiatric disorders
no general lack of exposure to language
no significant hearing loss
However no details of testing were given.
Service setting:
Five different classrooms in two special schools (small group intervention although
children worked independently from each other).
Description of
intervention
Service delivery model Groups of 3 children each working on separate computers with an experimenter
supervising ensuring children were engaged in the task experimenter clinician in the room
Provider(s):
Not stated
Domain of language:
Phonological awareness
ICF: Impairment
Type of intervention:
Method of intervention:
Experimental intervention:
A custom made educational software programme focusing on rhyming and synthesis
skills to enhance emergent and beginning literacy skills
Children progress through a series of games ordered from least to greatest difficulty.
Each game has three sets of five exercises and children progress once they have met
criterion
Intervention involved groups of 3 children (one from each experimental group)
Experimental group 1 received the above programme
Experimental group 2 received the above program with enhanced speech (slowed
down by 150% and the fast transitional elements in the speech were enhanced up to
20dB, with the amount of speech manipulation decreasing as the intervention
proceeded
Control group intervention:
Used the vocabulary acquisition part of the same computer software which involved
listening to a story on the computer and answering questions by pointing to the screen
Audio and visual feedback
Quantum of service
provision:
2-3 x 15-minute computer sessions per week for 5 weeks (3.5 hours)
Experimental group 2: 4 sessions with maximum speech manipulation, 4 sessions with
no delay but enhancement to 20dB, 3 sessions with enhancement up 10dB, and 3
sessions with normal speech
Outcomes evaluation (by
disorder subtype if
possible):
phonological awareness skills
At first post testing
o experimental group 1(normal speech) made significant and most progress
o no difference between experimental group 2 (enhanced speech) and the
control group
At second post test, 18 weeks after the intervention, no group effect s.

121
Author’s conclusion:
Children with SLI who had not begun formal literacy education benefited from a short,
intensive computer assisted phonological awareness intervention with speech that was not
manipulated. Computer assisted phonological awareness intervention that incorporated
manipulated speech did not produce any additional effect over vocabulary work or
phonological awareness work
Reviewer’s conclusion:
A short computer assisted phonological awareness programme appeared to be beneficial
for children with SLI, however the addition of speech manipulation may have actually
decreased its effectiveness as these children were no different to the control group. It is
also possible that the control treatment may have improved children‟s phonological skills.
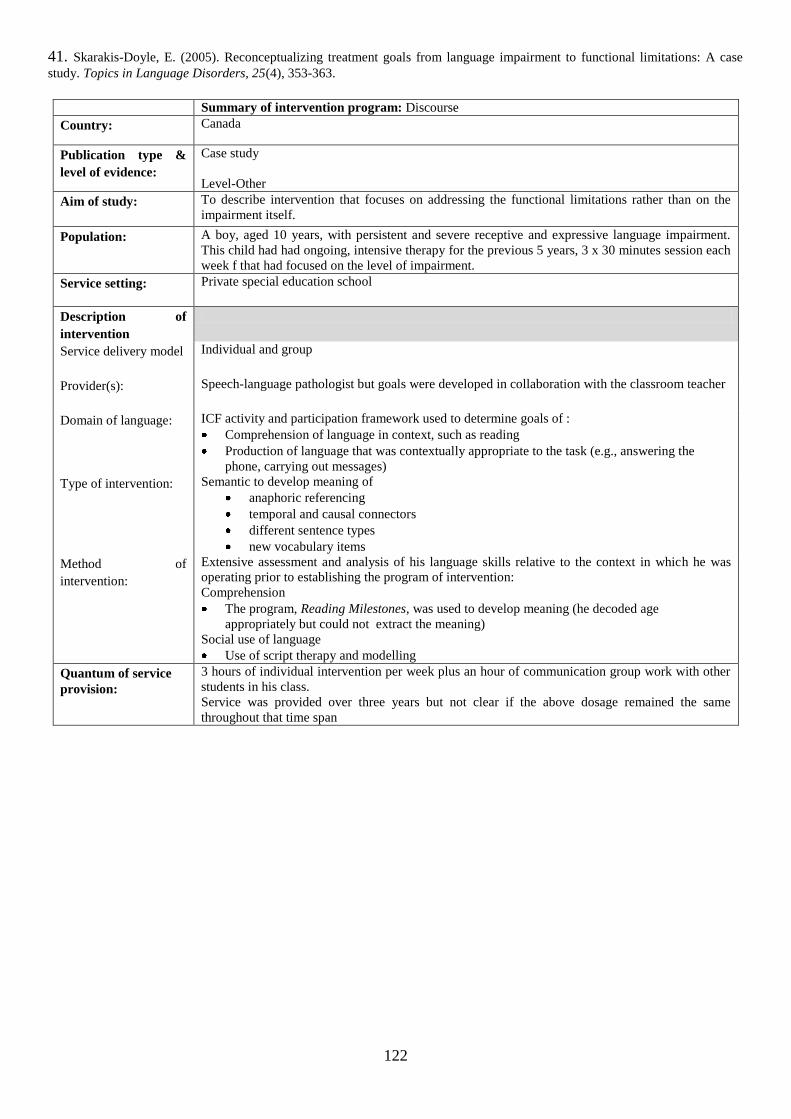
122
41. Skarakis-Doyle, E. (2005). Reconceptualizing treatment goals from language impairment to functional limitations: A case
study. Topics in Language Disorders, 25(4), 353-363.
Summary of intervention program: Discourse
Country: Canada
Publication type &
level of evidence:
Case study
Level-Other
Aim of study:
To describe intervention that focuses on addressing the functional limitations rather than on the
impairment itself.
Population:
A boy, aged 10 years, with persistent and severe receptive and expressive language impairment.
This child had had ongoing, intensive therapy for the previous 5 years, 3 x 30 minutes session each
week f that had focused on the level of impairment.
Service setting:
Private special education school
Description of
intervention
Service delivery model
Individual and group
Provider(s):
Speech-language pathologist but goals were developed in collaboration with the classroom teacher
Domain of language:
ICF activity and participation framework used to determine goals of :
Comprehension of language in context, such as reading
Production of language that was contextually appropriate to the task (e.g., answering the
phone, carrying out messages)
Type of intervention:
Semantic to develop meaning of
anaphoric referencing
temporal and causal connectors
different sentence types
new vocabulary items
Method of
intervention:
Extensive assessment and analysis of his language skills relative to the context in which he was
operating prior to establishing the program of intervention:
Comprehension
The program, Reading Milestones, was used to develop meaning (he decoded age
appropriately but could not extract the meaning)
Social use of language
Use of script therapy and modelling
Quantum of service
provision:
3 hours of individual intervention per week plus an hour of communication group work with other
students in his class.
Service was provided over three years but not clear if the above dosage remained the same
throughout that time span
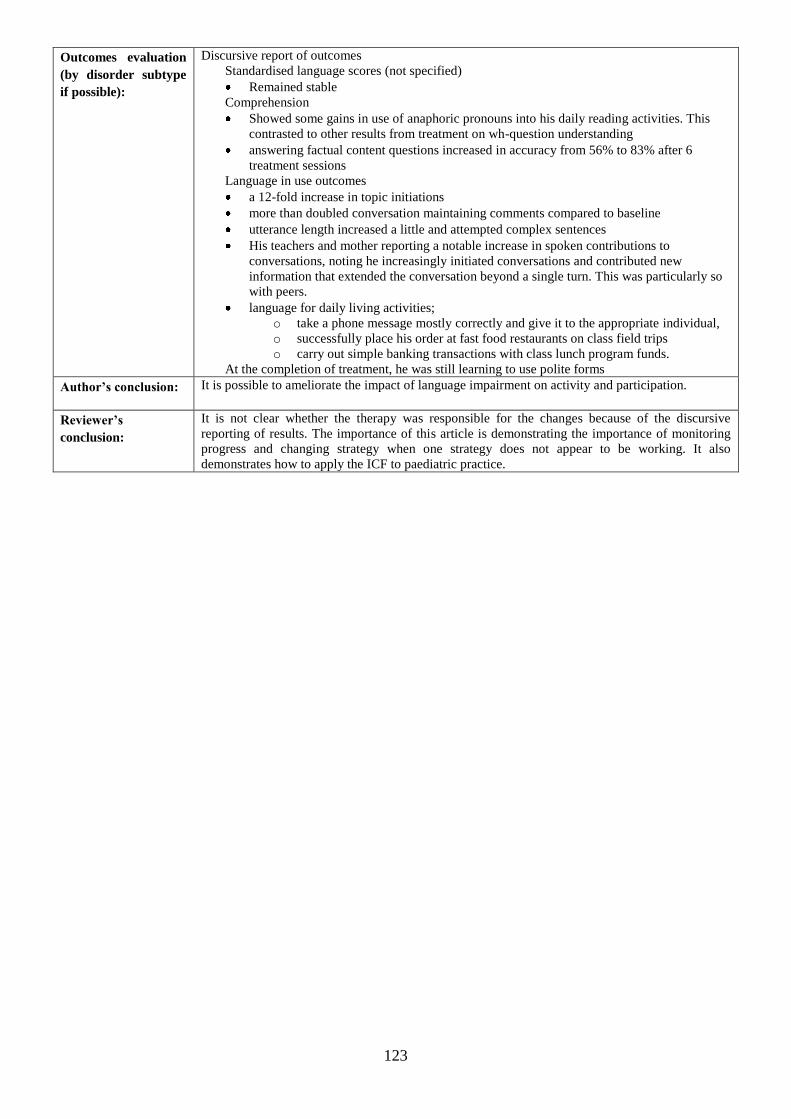
123
Outcomes evaluation
(by disorder subtype
if possible):
Discursive report of outcomes
Standardised language scores (not specified)
Remained stable
Comprehension
Showed some gains in use of anaphoric pronouns into his daily reading activities. This
contrasted to other results from treatment on wh-question understanding
answering factual content questions increased in accuracy from 56% to 83% after 6
treatment sessions
Language in use outcomes
a 12-fold increase in topic initiations
more than doubled conversation maintaining comments compared to baseline
utterance length increased a little and attempted complex sentences
His teachers and mother reporting a notable increase in spoken contributions to
conversations, noting he increasingly initiated conversations and contributed new
information that extended the conversation beyond a single turn. This was particularly so
with peers.
language for daily living activities;
o take a phone message mostly correctly and give it to the appropriate individual,
o successfully place his order at fast food restaurants on class field trips
o carry out simple banking transactions with class lunch program funds.
At the completion of treatment, he was still learning to use polite forms
Author’s conclusion:
It is possible to ameliorate the impact of language impairment on activity and participation.
Reviewer’s
conclusion:
It is not clear whether the therapy was responsible for the changes because of the discursive
reporting of results. The importance of this article is demonstrating the importance of monitoring
progress and changing strategy when one strategy does not appear to be working. It also
demonstrates how to apply the ICF to paediatric practice.
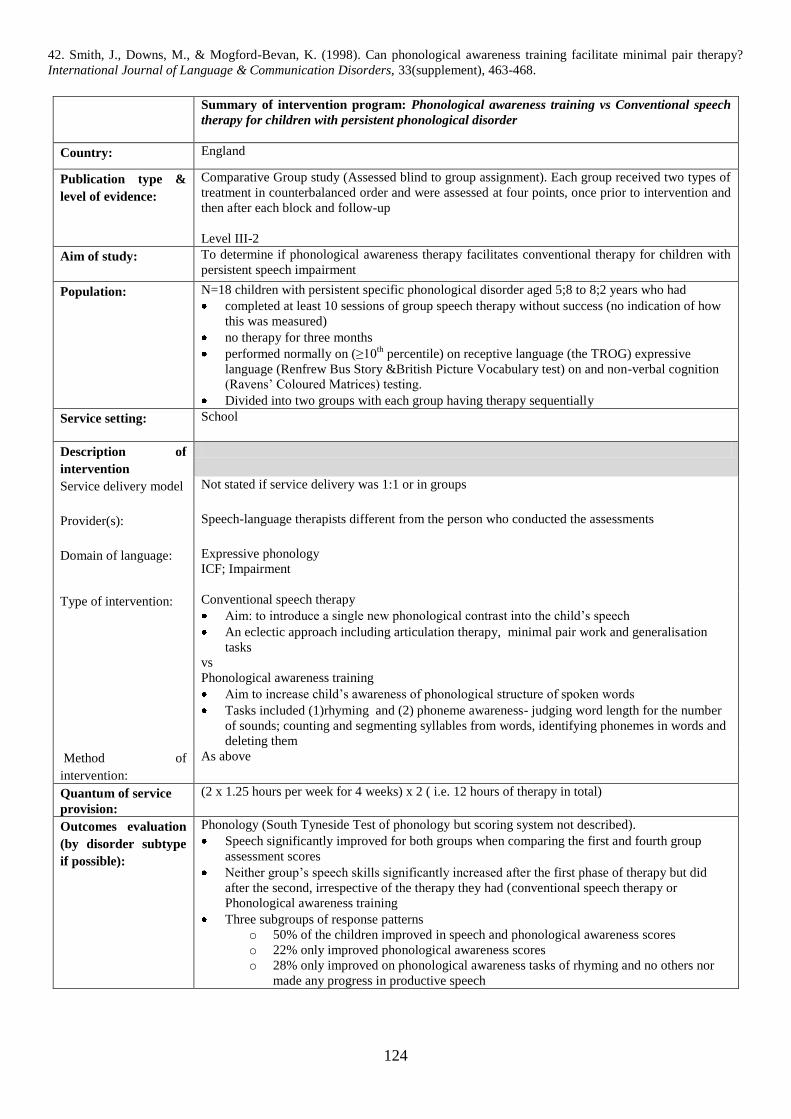
124
42. Smith, J., Downs, M., & Mogford-Bevan, K. (1998). Can phonological awareness training facilitate minimal pair therapy?
International Journal of Language & Communication Disorders, 33(supplement), 463-468.
Summary of intervention program: Phonological awareness training vs Conventional speech
therapy for children with persistent phonological disorder
Country: England
Publication type &
level of evidence:
Comparative Group study (Assessed blind to group assignment). Each group received two types of
treatment in counterbalanced order and were assessed at four points, once prior to intervention and
then after each block and follow-up
Level III-2
Aim of study:
To determine if phonological awareness therapy facilitates conventional therapy for children with
persistent speech impairment
Population:
N=18 children with persistent specific phonological disorder aged 5;8 to 8;2 years who had
completed at least 10 sessions of group speech therapy without success (no indication of how
this was measured)
no therapy for three months
performed normally on (≥10th
percentile) on receptive language (the TROG) expressive
language (Renfrew Bus Story &British Picture Vocabulary test) on and non-verbal cognition
(Ravens‟ Coloured Matrices) testing.
Divided into two groups with each group having therapy sequentially
Service setting:
School
Description of
intervention
Service delivery model
Not stated if service delivery was 1:1 or in groups
Provider(s):
Speech-language therapists different from the person who conducted the assessments
Domain of language:
Expressive phonology
ICF; Impairment
Type of intervention:
Conventional speech therapy
Aim: to introduce a single new phonological contrast into the child‟s speech
An eclectic approach including articulation therapy, minimal pair work and generalisation
tasks
vs
Phonological awareness training
Aim to increase child‟s awareness of phonological structure of spoken words
Tasks included (1)rhyming and (2) phoneme awareness- judging word length for the number
of sounds; counting and segmenting syllables from words, identifying phonemes in words and
deleting them
Method of
intervention:
As above
Quantum of service
provision:
(2 x 1.25 hours per week for 4 weeks) x 2 ( i.e. 12 hours of therapy in total)
Outcomes evaluation
(by disorder subtype
if possible):
Phonology (South Tyneside Test of phonology but scoring system not described).
Speech significantly improved for both groups when comparing the first and fourth group
assessment scores
Neither group‟s speech skills significantly increased after the first phase of therapy but did
after the second, irrespective of the therapy they had (conventional speech therapy or
Phonological awareness training
Three subgroups of response patterns
o 50% of the children improved in speech and phonological awareness scores
o 22% only improved phonological awareness scores
o 28% only improved on phonological awareness tasks of rhyming and no others nor
made any progress in productive speech
125
Author’s conclusion:
The addition of phonological awareness training added significant value over and above that
attributable to maturation or conventional therapy.
Reviewer’s
conclusion:
It appears that the about half of the children need a therapy package that incorporates conventional
components as well as phonological awareness training. However, others need a more specialised
package and this may only become apparent once therapy has commenced hence underscoring the
need to closely monitor children‟s progress in therapy.
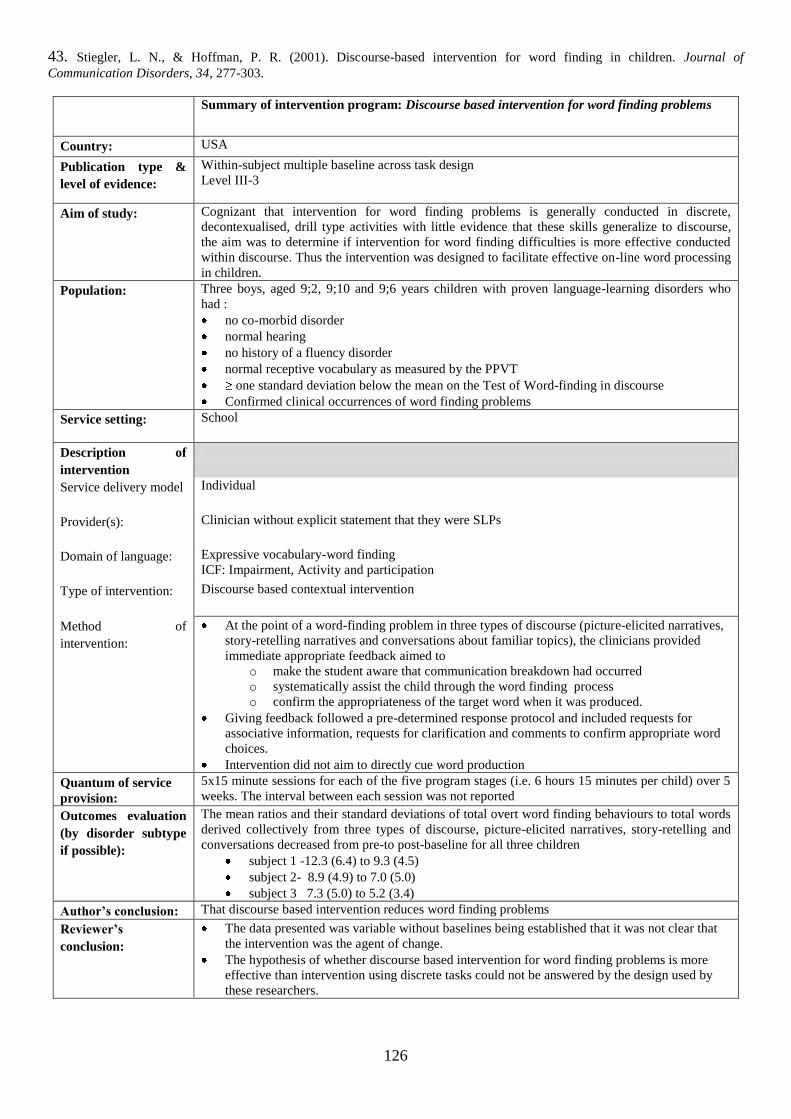
126
43. Stiegler, L. N., & Hoffman, P. R. (2001). Discourse-based intervention for word finding in children. Journal of
Communication Disorders, 34, 277-303.
Summary of intervention program: Discourse based intervention for word finding problems
Country: USA
Publication type &
level of evidence:
Within-subject multiple baseline across task design
Level III-3
Aim of study:
Cognizant that intervention for word finding problems is generally conducted in discrete,
decontexualised, drill type activities with little evidence that these skills generalize to discourse,
the aim was to determine if intervention for word finding difficulties is more effective conducted
within discourse. Thus the intervention was designed to facilitate effective on-line word processing
in children.
Population:
Three boys, aged 9;2, 9;10 and 9;6 years children with proven language-learning disorders who
had :
no co-morbid disorder
normal hearing
no history of a fluency disorder
normal receptive vocabulary as measured by the PPVT
one standard deviation below the mean on the Test of Word-finding in discourse
Confirmed clinical occurrences of word finding problems
Service setting:
School
Description of
intervention
Service delivery model
Individual
Provider(s):
Clinician without explicit statement that they were SLPs
Domain of language:
Expressive vocabulary-word finding
ICF: Impairment, Activity and participation
Type of intervention:
Discourse based contextual intervention
Method of
intervention:
At the point of a word-finding problem in three types of discourse (picture-elicited narratives,
story-retelling narratives and conversations about familiar topics), the clinicians provided
immediate appropriate feedback aimed to
o make the student aware that communication breakdown had occurred
o systematically assist the child through the word finding process
o confirm the appropriateness of the target word when it was produced.
Giving feedback followed a pre-determined response protocol and included requests for
associative information, requests for clarification and comments to confirm appropriate word
choices.
Intervention did not aim to directly cue word production
Quantum of service
provision:
5x15 minute sessions for each of the five program stages (i.e. 6 hours 15 minutes per child) over 5
weeks. The interval between each session was not reported
Outcomes evaluation
(by disorder subtype
if possible):
The mean ratios and their standard deviations of total overt word finding behaviours to total words
derived collectively from three types of discourse, picture-elicited narratives, story-retelling and
conversations decreased from pre-to post-baseline for all three children
subject 1 -12.3 (6.4) to 9.3 (4.5)
subject 2- 8.9 (4.9) to 7.0 (5.0)
subject 3 7.3 (5.0) to 5.2 (3.4)
Author’s conclusion: That discourse based intervention reduces word finding problems
Reviewer’s
conclusion:
The data presented was variable without baselines being established that it was not clear that
the intervention was the agent of change.
The hypothesis of whether discourse based intervention for word finding problems is more
effective than intervention using discrete tasks could not be answered by the design used by
these researchers.
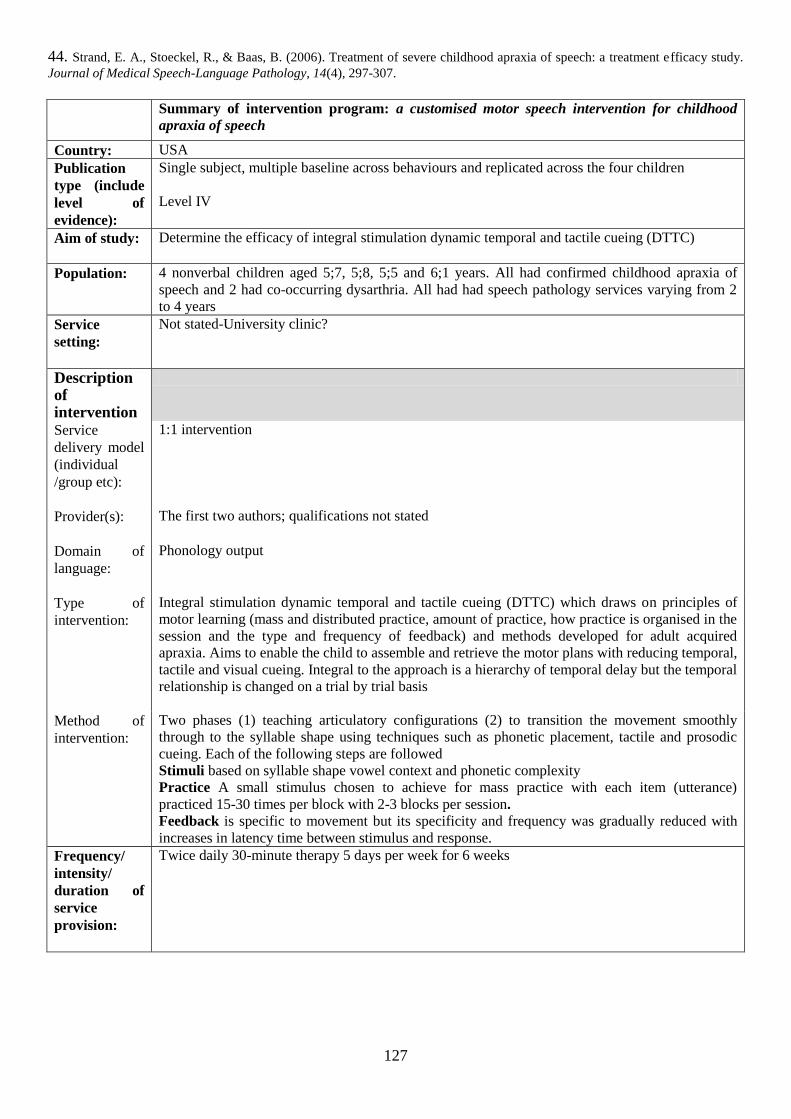
127
44. Strand, E. A., Stoeckel, R., & Baas, B. (2006). Treatment of severe childhood apraxia of speech: a treatment efficacy study.
Journal of Medical Speech-Language Pathology, 14(4), 297-307.
Summary of intervention program: a customised motor speech intervention for childhood
apraxia of speech
Country: USA
Publication
type (include
level of
evidence):
Single subject, multiple baseline across behaviours and replicated across the four children
Level IV
Aim of study:
Determine the efficacy of integral stimulation dynamic temporal and tactile cueing (DTTC)
Population:
4 nonverbal children aged 5;7, 5;8, 5;5 and 6;1 years. All had confirmed childhood apraxia of
speech and 2 had co-occurring dysarthria. All had had speech pathology services varying from 2
to 4 years
Service
setting:
Not stated-University clinic?
Description of intervention
Service
delivery model
(individual
/group etc):
1:1 intervention
Provider(s):
The first two authors; qualifications not stated
Domain of
language:
Phonology output
Type of
intervention:
Integral stimulation dynamic temporal and tactile cueing (DTTC) which draws on principles of
motor learning (mass and distributed practice, amount of practice, how practice is organised in the
session and the type and frequency of feedback) and methods developed for adult acquired
apraxia. Aims to enable the child to assemble and retrieve the motor plans with reducing temporal,
tactile and visual cueing. Integral to the approach is a hierarchy of temporal delay but the temporal
relationship is changed on a trial by trial basis
Method of
intervention:
Two phases (1) teaching articulatory configurations (2) to transition the movement smoothly
through to the syllable shape using techniques such as phonetic placement, tactile and prosodic
cueing. Each of the following steps are followed
Stimuli based on syllable shape vowel context and phonetic complexity
Practice A small stimulus chosen to achieve for mass practice with each item (utterance)
practiced 15-30 times per block with 2-3 blocks per session.
Feedback is specific to movement but its specificity and frequency was gradually reduced with
increases in latency time between stimulus and response.
Frequency/
intensity/
duration of
service
provision:
Twice daily 30-minute therapy 5 days per week for 6 weeks
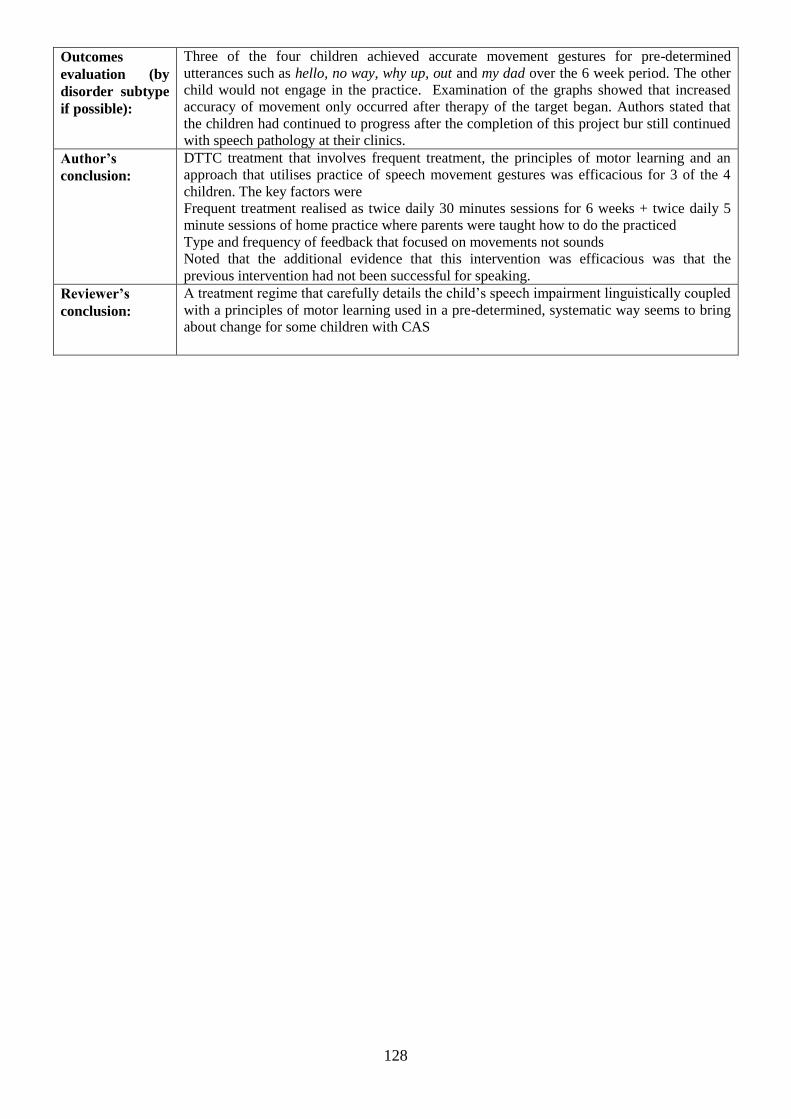
128
Outcomes
evaluation (by
disorder subtype
if possible):
Three of the four children achieved accurate movement gestures for pre-determined
utterances such as hello, no way, why up, out and my dad over the 6 week period. The other
child would not engage in the practice. Examination of the graphs showed that increased
accuracy of movement only occurred after therapy of the target began. Authors stated that
the children had continued to progress after the completion of this project bur still continued
with speech pathology at their clinics.
Author’s
conclusion:
DTTC treatment that involves frequent treatment, the principles of motor learning and an
approach that utilises practice of speech movement gestures was efficacious for 3 of the 4
children. The key factors were
Frequent treatment realised as twice daily 30 minutes sessions for 6 weeks + twice daily 5
minute sessions of home practice where parents were taught how to do the practiced
Type and frequency of feedback that focused on movements not sounds
Noted that the additional evidence that this intervention was efficacious was that the
previous intervention had not been successful for speaking.
Reviewer’s
conclusion:
A treatment regime that carefully details the child‟s speech impairment linguistically coupled
with a principles of motor learning used in a pre-determined, systematic way seems to bring
about change for some children with CAS
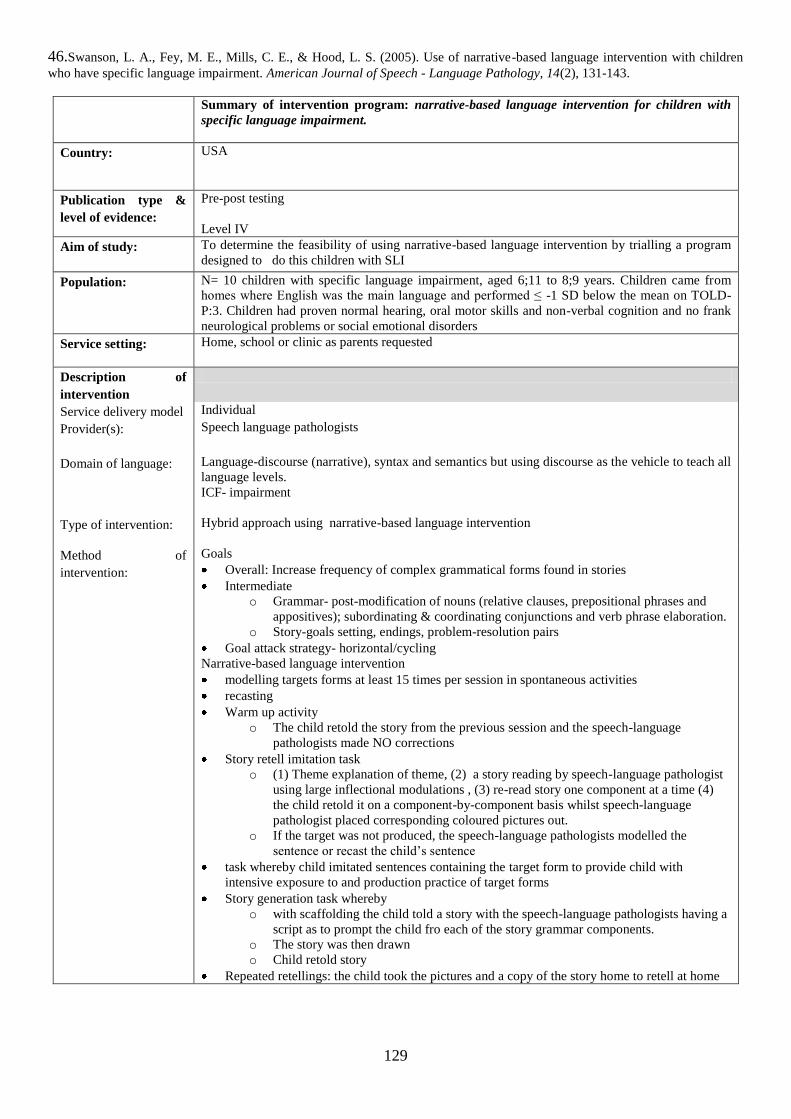
129
46.Swanson, L. A., Fey, M. E., Mills, C. E., & Hood, L. S. (2005). Use of narrative-based language intervention with children
who have specific language impairment. American Journal of Speech - Language Pathology, 14(2), 131-143.
Summary of intervention program: narrative-based language intervention for children with
specific language impairment.
Country: USA
Publication type &
level of evidence:
Pre-post testing
Level IV
Aim of study:
To determine the feasibility of using narrative-based language intervention by trialling a program
designed to do this children with SLI
Population:
N= 10 children with specific language impairment, aged 6;11 to 8;9 years. Children came from
homes where English was the main language and performed ≤ -1 SD below the mean on TOLD-
P:3. Children had proven normal hearing, oral motor skills and non-verbal cognition and no frank
neurological problems or social emotional disorders
Service setting:
Home, school or clinic as parents requested
Description of
intervention
Service delivery model Individual
Provider(s):
Speech language pathologists
Domain of language:
Language-discourse (narrative), syntax and semantics but using discourse as the vehicle to teach all
language levels.
ICF- impairment
Type of intervention: Hybrid approach using narrative-based language intervention
Method of
intervention:
Goals
Overall: Increase frequency of complex grammatical forms found in stories
Intermediate
o Grammar- post-modification of nouns (relative clauses, prepositional phrases and
appositives); subordinating & coordinating conjunctions and verb phrase elaboration.
o Story-goals setting, endings, problem-resolution pairs
Goal attack strategy- horizontal/cycling
Narrative-based language intervention
modelling targets forms at least 15 times per session in spontaneous activities
recasting
Warm up activity
o The child retold the story from the previous session and the speech-language
pathologists made NO corrections
Story retell imitation task
o (1) Theme explanation of theme, (2) a story reading by speech-language pathologist
using large inflectional modulations , (3) re-read story one component at a time (4)
the child retold it on a component-by-component basis whilst speech-language
pathologist placed corresponding coloured pictures out.
o If the target was not produced, the speech-language pathologists modelled the
sentence or recast the child‟s sentence
task whereby child imitated sentences containing the target form to provide child with
intensive exposure to and production practice of target forms
Story generation task whereby
o with scaffolding the child told a story with the speech-language pathologists having a
script as to prompt the child fro each of the story grammar components.
o The story was then drawn
o Child retold story
Repeated retellings: the child took the pictures and a copy of the story home to retell at home
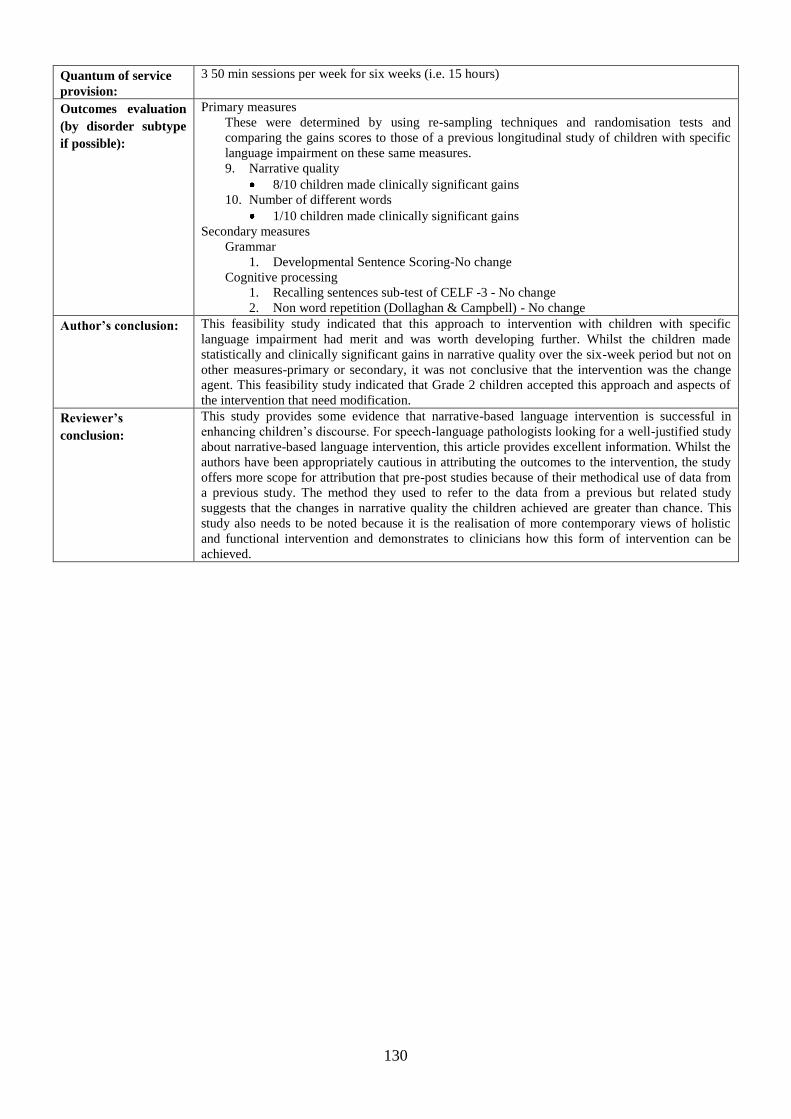
130
Quantum of service
provision:
3 50 min sessions per week for six weeks (i.e. 15 hours)
Outcomes evaluation
(by disorder subtype
if possible):
Primary measures
These were determined by using re-sampling techniques and randomisation tests and
comparing the gains scores to those of a previous longitudinal study of children with specific
language impairment on these same measures.
9. Narrative quality
8/10 children made clinically significant gains
10. Number of different words
1/10 children made clinically significant gains
Secondary measures
Grammar
1. Developmental Sentence Scoring-No change
Cognitive processing
1. Recalling sentences sub-test of CELF -3 - No change
2. Non word repetition (Dollaghan & Campbell) - No change
Author’s conclusion:
This feasibility study indicated that this approach to intervention with children with specific
language impairment had merit and was worth developing further. Whilst the children made
statistically and clinically significant gains in narrative quality over the six-week period but not on
other measures-primary or secondary, it was not conclusive that the intervention was the change
agent. This feasibility study indicated that Grade 2 children accepted this approach and aspects of
the intervention that need modification.
Reviewer’s
conclusion:
This study provides some evidence that narrative-based language intervention is successful in
enhancing children‟s discourse. For speech-language pathologists looking for a well-justified study
about narrative-based language intervention, this article provides excellent information. Whilst the
authors have been appropriately cautious in attributing the outcomes to the intervention, the study
offers more scope for attribution that pre-post studies because of their methodical use of data from
a previous study. The method they used to refer to the data from a previous but related study
suggests that the changes in narrative quality the children achieved are greater than chance. This
study also needs to be noted because it is the realisation of more contemporary views of holistic
and functional intervention and demonstrates to clinicians how this form of intervention can be
achieved.
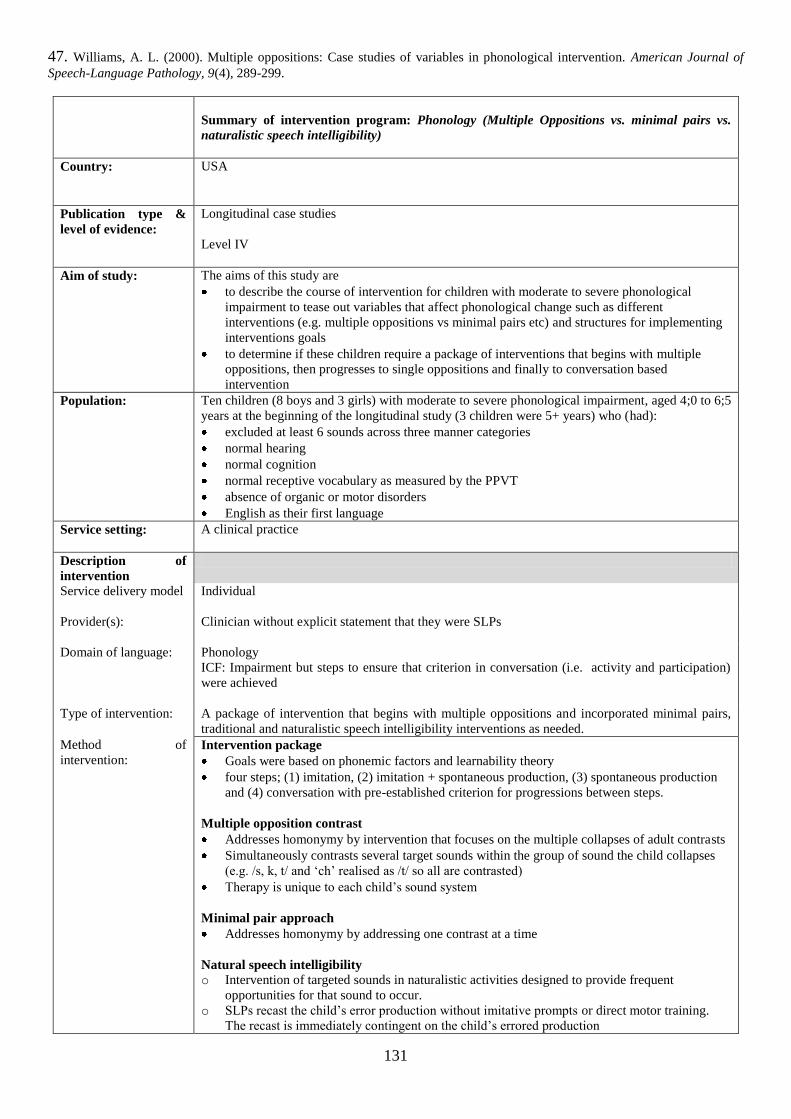
131
47. Williams, A. L. (2000). Multiple oppositions: Case studies of variables in phonological intervention. American Journal of
Speech-Language Pathology, 9(4), 289-299.
Summary of intervention program: Phonology (Multiple Oppositions vs. minimal pairs vs.
naturalistic speech intelligibility)
Country: USA
Publication type &
level of evidence:
Longitudinal case studies
Level IV
Aim of study:
The aims of this study are
to describe the course of intervention for children with moderate to severe phonological
impairment to tease out variables that affect phonological change such as different
interventions (e.g. multiple oppositions vs minimal pairs etc) and structures for implementing
interventions goals
to determine if these children require a package of interventions that begins with multiple
oppositions, then progresses to single oppositions and finally to conversation based
intervention
Population:
Ten children (8 boys and 3 girls) with moderate to severe phonological impairment, aged 4;0 to 6;5
years at the beginning of the longitudinal study (3 children were 5+ years) who (had):
excluded at least 6 sounds across three manner categories
normal hearing
normal cognition
normal receptive vocabulary as measured by the PPVT
absence of organic or motor disorders
English as their first language
Service setting:
A clinical practice
Description of
intervention
Service delivery model
Individual
Provider(s):
Clinician without explicit statement that they were SLPs
Domain of language:
Phonology
ICF: Impairment but steps to ensure that criterion in conversation (i.e. activity and participation)
were achieved
Type of intervention:
A package of intervention that begins with multiple oppositions and incorporated minimal pairs,
traditional and naturalistic speech intelligibility interventions as needed.
Method of
intervention:
Intervention package
Goals were based on phonemic factors and learnability theory
four steps; (1) imitation, (2) imitation + spontaneous production, (3) spontaneous production
and (4) conversation with pre-established criterion for progressions between steps.
Multiple opposition contrast
Addresses homonymy by intervention that focuses on the multiple collapses of adult contrasts
Simultaneously contrasts several target sounds within the group of sound the child collapses
(e.g. /s, k, t/ and „ch‟ realised as /t/ so all are contrasted)
Therapy is unique to each child‟s sound system
Minimal pair approach
Addresses homonymy by addressing one contrast at a time
Natural speech intelligibility
o Intervention of targeted sounds in naturalistic activities designed to provide frequent
opportunities for that sound to occur.
o SLPs recast the child‟s error production without imitative prompts or direct motor training.
The recast is immediately contingent on the child‟s errored production
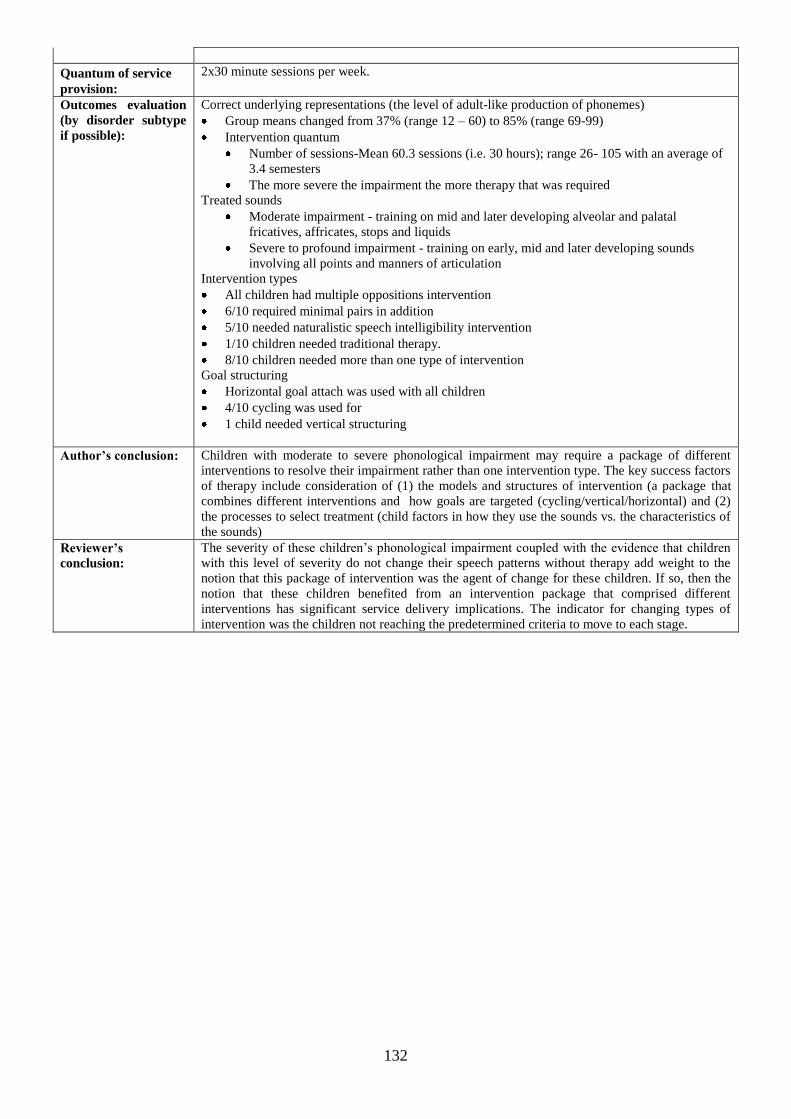
132
Quantum of service
provision:
2x30 minute sessions per week.
Outcomes evaluation
(by disorder subtype
if possible):
Correct underlying representations (the level of adult-like production of phonemes)
Group means changed from 37% (range 12 – 60) to 85% (range 69-99)
Intervention quantum
Number of sessions-Mean 60.3 sessions (i.e. 30 hours); range 26- 105 with an average of
3.4 semesters
The more severe the impairment the more therapy that was required
Treated sounds
Moderate impairment - training on mid and later developing alveolar and palatal
fricatives, affricates, stops and liquids
Severe to profound impairment - training on early, mid and later developing sounds
involving all points and manners of articulation
Intervention types
All children had multiple oppositions intervention
6/10 required minimal pairs in addition
5/10 needed naturalistic speech intelligibility intervention
1/10 children needed traditional therapy.
8/10 children needed more than one type of intervention
Goal structuring
Horizontal goal attach was used with all children
4/10 cycling was used for
1 child needed vertical structuring
Author’s conclusion:
Children with moderate to severe phonological impairment may require a package of different
interventions to resolve their impairment rather than one intervention type. The key success factors
of therapy include consideration of (1) the models and structures of intervention (a package that
combines different interventions and how goals are targeted (cycling/vertical/horizontal) and (2)
the processes to select treatment (child factors in how they use the sounds vs. the characteristics of
the sounds)
Reviewer’s
conclusion:
The severity of these children‟s phonological impairment coupled with the evidence that children
with this level of severity do not change their speech patterns without therapy add weight to the
notion that this package of intervention was the agent of change for these children. If so, then the
notion that these children benefited from an intervention package that comprised different
interventions has significant service delivery implications. The indicator for changing types of
intervention was the children not reaching the predetermined criteria to move to each stage.
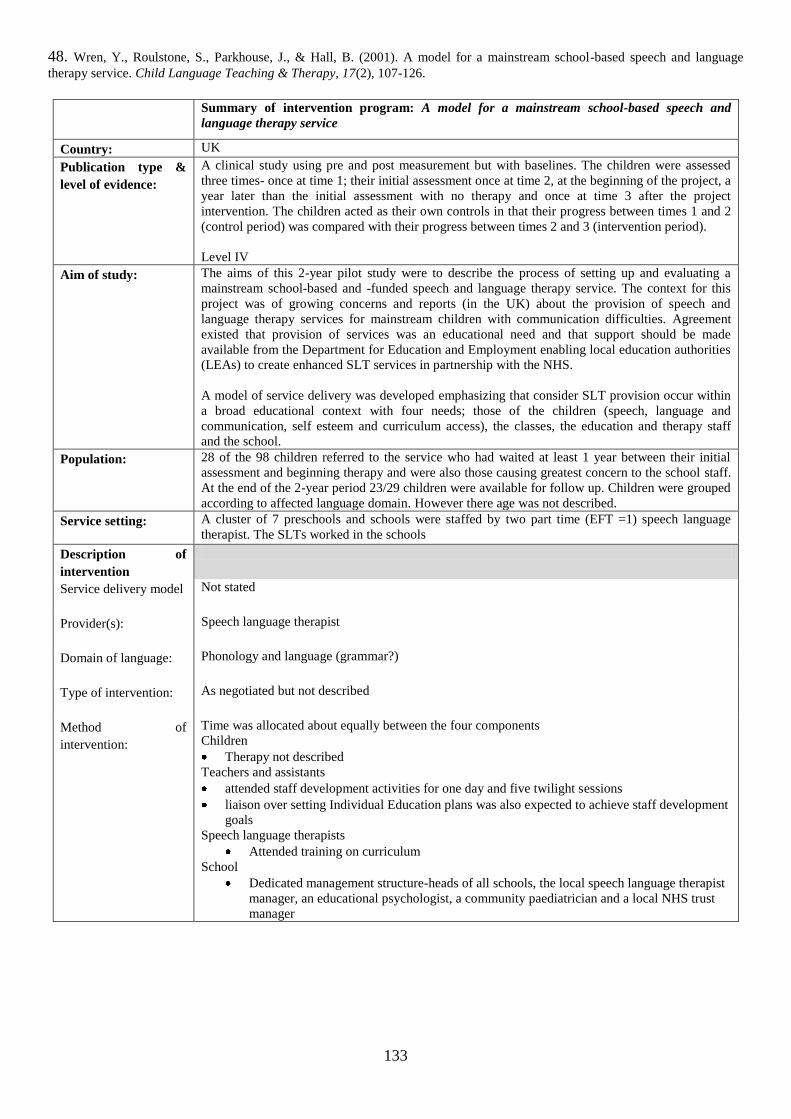
133
48. Wren, Y., Roulstone, S., Parkhouse, J., & Hall, B. (2001). A model for a mainstream school-based speech and language
therapy service. Child Language Teaching & Therapy, 17(2), 107-126.
Summary of intervention program: A model for a mainstream school-based speech and
language therapy service
Country: UK
Publication type &
level of evidence:
A clinical study using pre and post measurement but with baselines. The children were assessed
three times- once at time 1; their initial assessment once at time 2, at the beginning of the project, a
year later than the initial assessment with no therapy and once at time 3 after the project
intervention. The children acted as their own controls in that their progress between times 1 and 2
(control period) was compared with their progress between times 2 and 3 (intervention period).
Level IV
Aim of study:
The aims of this 2-year pilot study were to describe the process of setting up and evaluating a
mainstream school-based and -funded speech and language therapy service. The context for this
project was of growing concerns and reports (in the UK) about the provision of speech and
language therapy services for mainstream children with communication difficulties. Agreement
existed that provision of services was an educational need and that support should be made
available from the Department for Education and Employment enabling local education authorities
(LEAs) to create enhanced SLT services in partnership with the NHS.
A model of service delivery was developed emphasizing that consider SLT provision occur within
a broad educational context with four needs; those of the children (speech, language and
communication, self esteem and curriculum access), the classes, the education and therapy staff
and the school.
Population:
28 of the 98 children referred to the service who had waited at least 1 year between their initial
assessment and beginning therapy and were also those causing greatest concern to the school staff.
At the end of the 2-year period 23/29 children were available for follow up. Children were grouped
according to affected language domain. However there age was not described.
Service setting:
A cluster of 7 preschools and schools were staffed by two part time (EFT =1) speech language
therapist. The SLTs worked in the schools
Description of
intervention
Service delivery model
Not stated
Provider(s):
Speech language therapist
Domain of language:
Phonology and language (grammar?)
Type of intervention:
As negotiated but not described
Method of
intervention:
Time was allocated about equally between the four components
Children
Therapy not described
Teachers and assistants
attended staff development activities for one day and five twilight sessions
liaison over setting Individual Education plans was also expected to achieve staff development
goals
Speech language therapists
Attended training on curriculum
School
Dedicated management structure-heads of all schools, the local speech language therapist
manager, an educational psychologist, a community paediatrician and a local NHS trust
manager
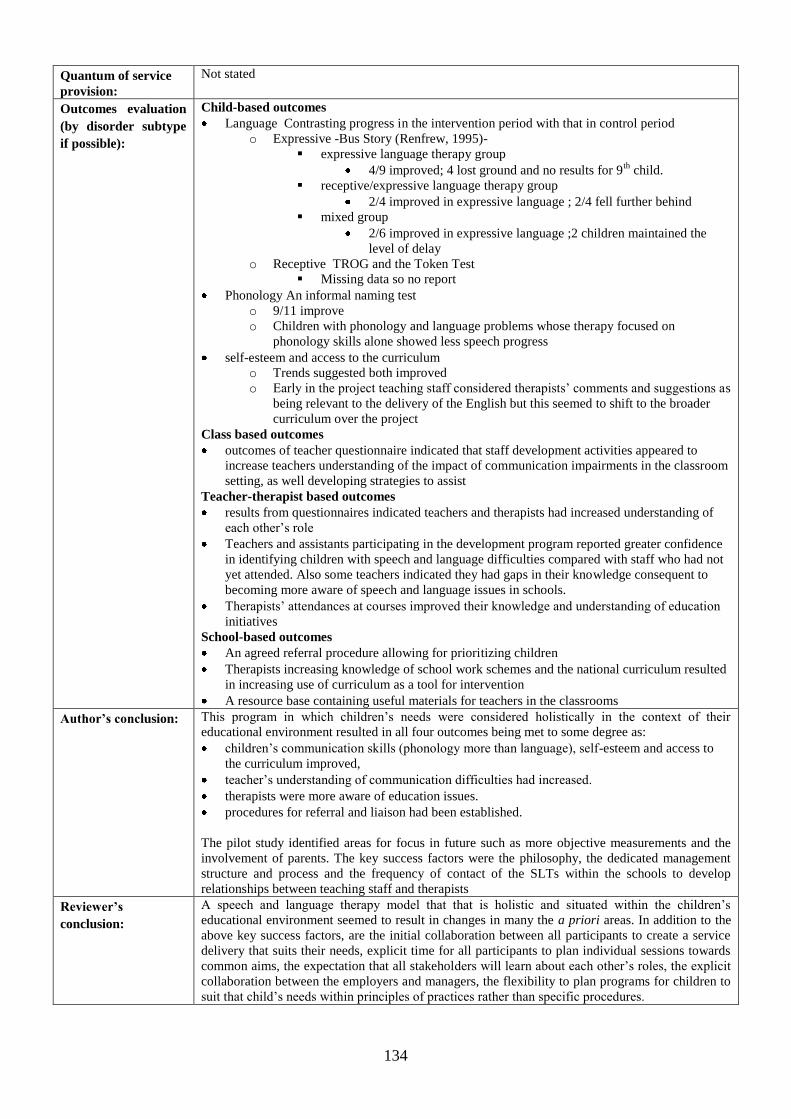
134
Quantum of service
provision:
Not stated
Outcomes evaluation
(by disorder subtype
if possible):
Child-based outcomes
Language Contrasting progress in the intervention period with that in control period
o Expressive -Bus Story (Renfrew, 1995)-
expressive language therapy group
4/9 improved; 4 lost ground and no results for 9th
child.
receptive/expressive language therapy group
2/4 improved in expressive language ; 2/4 fell further behind
mixed group
2/6 improved in expressive language ;2 children maintained the
level of delay
o Receptive TROG and the Token Test
Missing data so no report
Phonology An informal naming test
o 9/11 improve
o Children with phonology and language problems whose therapy focused on
phonology skills alone showed less speech progress
self-esteem and access to the curriculum
o Trends suggested both improved
o Early in the project teaching staff considered therapists‟ comments and suggestions as
being relevant to the delivery of the English but this seemed to shift to the broader
curriculum over the project
Class based outcomes
outcomes of teacher questionnaire indicated that staff development activities appeared to
increase teachers understanding of the impact of communication impairments in the classroom
setting, as well developing strategies to assist
Teacher-therapist based outcomes
results from questionnaires indicated teachers and therapists had increased understanding of
each other‟s role
Teachers and assistants participating in the development program reported greater confidence
in identifying children with speech and language difficulties compared with staff who had not
yet attended. Also some teachers indicated they had gaps in their knowledge consequent to
becoming more aware of speech and language issues in schools.
Therapists‟ attendances at courses improved their knowledge and understanding of education
initiatives
School-based outcomes
An agreed referral procedure allowing for prioritizing children
Therapists increasing knowledge of school work schemes and the national curriculum resulted
in increasing use of curriculum as a tool for intervention
A resource base containing useful materials for teachers in the classrooms
Author’s conclusion:
This program in which children‟s needs were considered holistically in the context of their
educational environment resulted in all four outcomes being met to some degree as:
children‟s communication skills (phonology more than language), self-esteem and access to
the curriculum improved,
teacher‟s understanding of communication difficulties had increased.
therapists were more aware of education issues.
procedures for referral and liaison had been established.
The pilot study identified areas for focus in future such as more objective measurements and the
involvement of parents. The key success factors were the philosophy, the dedicated management
structure and process and the frequency of contact of the SLTs within the schools to develop
relationships between teaching staff and therapists
Reviewer’s
conclusion:
A speech and language therapy model that that is holistic and situated within the children‟s
educational environment seemed to result in changes in many the a priori areas. In addition to the
above key success factors, are the initial collaboration between all participants to create a service
delivery that suits their needs, explicit time for all participants to plan individual sessions towards
common aims, the expectation that all stakeholders will learn about each other‟s roles, the explicit
collaboration between the employers and managers, the flexibility to plan programs for children to
suit that child‟s needs within principles of practices rather than specific procedures.
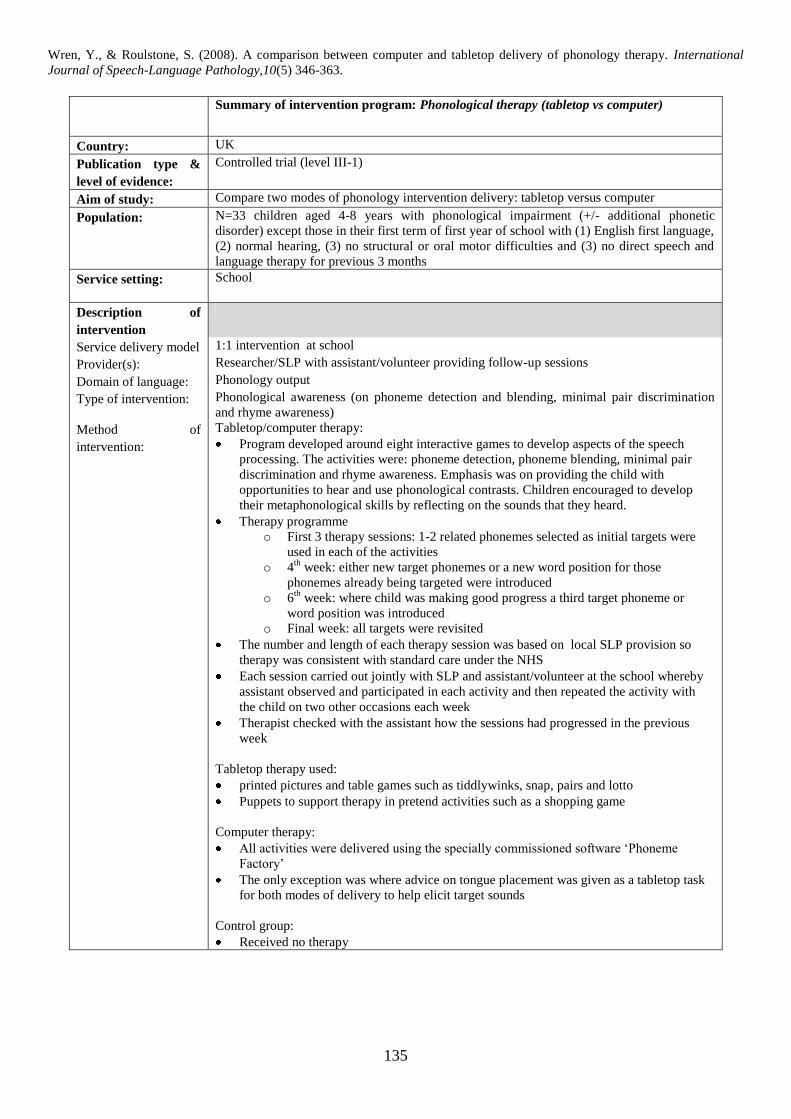
135
Wren, Y., & Roulstone, S. (2008). A comparison between computer and tabletop delivery of phonology therapy. International
Journal of Speech-Language Pathology,10(5) 346-363.
Summary of intervention program: Phonological therapy (tabletop vs computer)
Country: UK
Publication type &
level of evidence:
Controlled trial (level III-1)
Aim of study: Compare two modes of phonology intervention delivery: tabletop versus computer
Population:
N=33 children aged 4-8 years with phonological impairment (+/- additional phonetic
disorder) except those in their first term of first year of school with (1) English first language,
(2) normal hearing, (3) no structural or oral motor difficulties and (3) no direct speech and
language therapy for previous 3 months
Service setting:
School
Description of
intervention
Service delivery model 1:1 intervention at school
Provider(s): Researcher/SLP with assistant/volunteer providing follow-up sessions
Domain of language: Phonology output
Type of intervention: Phonological awareness (on phoneme detection and blending, minimal pair discrimination
and rhyme awareness)
Method of
intervention:
Tabletop/computer therapy:
Program developed around eight interactive games to develop aspects of the speech
processing. The activities were: phoneme detection, phoneme blending, minimal pair
discrimination and rhyme awareness. Emphasis was on providing the child with
opportunities to hear and use phonological contrasts. Children encouraged to develop
their metaphonological skills by reflecting on the sounds that they heard.
Therapy programme
o First 3 therapy sessions: 1-2 related phonemes selected as initial targets were
used in each of the activities
o 4th
week: either new target phonemes or a new word position for those
phonemes already being targeted were introduced
o 6th
week: where child was making good progress a third target phoneme or
word position was introduced
o Final week: all targets were revisited
The number and length of each therapy session was based on local SLP provision so
therapy was consistent with standard care under the NHS
Each session carried out jointly with SLP and assistant/volunteer at the school whereby
assistant observed and participated in each activity and then repeated the activity with
the child on two other occasions each week
Therapist checked with the assistant how the sessions had progressed in the previous
week
Tabletop therapy used:
printed pictures and table games such as tiddlywinks, snap, pairs and lotto
Puppets to support therapy in pretend activities such as a shopping game
Computer therapy:
All activities were delivered using the specially commissioned software „Phoneme
Factory‟
The only exception was where advice on tongue placement was given as a tabletop task
for both modes of delivery to help elicit target sounds
Control group:
Received no therapy
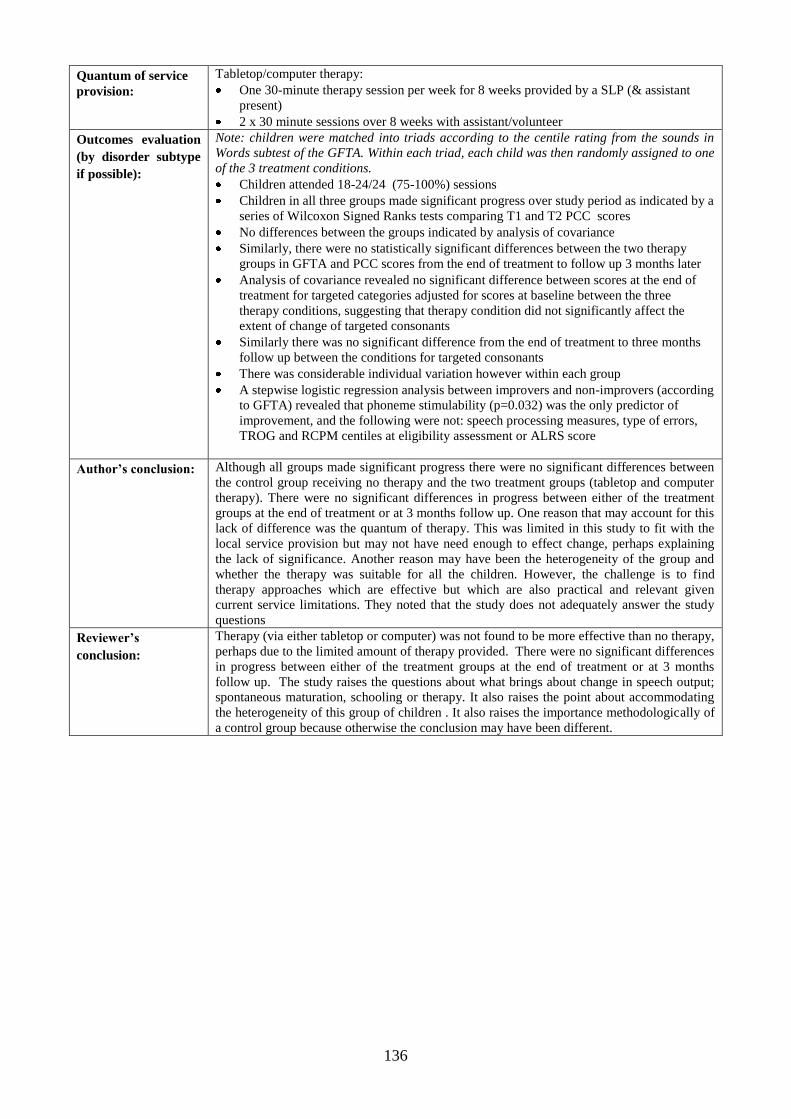
136
Quantum of service
provision:
Tabletop/computer therapy:
One 30-minute therapy session per week for 8 weeks provided by a SLP (& assistant
present)
2 x 30 minute sessions over 8 weeks with assistant/volunteer
Outcomes evaluation
(by disorder subtype
if possible):
Note: children were matched into triads according to the centile rating from the sounds in
Words subtest of the GFTA. Within each triad, each child was then randomly assigned to one
of the 3 treatment conditions.
Children attended 18-24/24 (75-100%) sessions
Children in all three groups made significant progress over study period as indicated by a
series of Wilcoxon Signed Ranks tests comparing T1 and T2 PCC scores
No differences between the groups indicated by analysis of covariance
Similarly, there were no statistically significant differences between the two therapy
groups in GFTA and PCC scores from the end of treatment to follow up 3 months later
Analysis of covariance revealed no significant difference between scores at the end of
treatment for targeted categories adjusted for scores at baseline between the three
therapy conditions, suggesting that therapy condition did not significantly affect the
extent of change of targeted consonants
Similarly there was no significant difference from the end of treatment to three months
follow up between the conditions for targeted consonants
There was considerable individual variation however within each group
A stepwise logistic regression analysis between improvers and non-improvers (according
to GFTA) revealed that phoneme stimulability (p=0.032) was the only predictor of
improvement, and the following were not: speech processing measures, type of errors,
TROG and RCPM centiles at eligibility assessment or ALRS score
Author’s conclusion:
Although all groups made significant progress there were no significant differences between
the control group receiving no therapy and the two treatment groups (tabletop and computer
therapy). There were no significant differences in progress between either of the treatment
groups at the end of treatment or at 3 months follow up. One reason that may account for this
lack of difference was the quantum of therapy. This was limited in this study to fit with the
local service provision but may not have need enough to effect change, perhaps explaining
the lack of significance. Another reason may have been the heterogeneity of the group and
whether the therapy was suitable for all the children. However, the challenge is to find
therapy approaches which are effective but which are also practical and relevant given
current service limitations. They noted that the study does not adequately answer the study
questions
Reviewer’s
conclusion:
Therapy (via either tabletop or computer) was not found to be more effective than no therapy,
perhaps due to the limited amount of therapy provided. There were no significant differences
in progress between either of the treatment groups at the end of treatment or at 3 months
follow up. The study raises the questions about what brings about change in speech output;
spontaneous maturation, schooling or therapy. It also raises the point about accommodating
the heterogeneity of this group of children . It also raises the importance methodologically of
a control group because otherwise the conclusion may have been different.
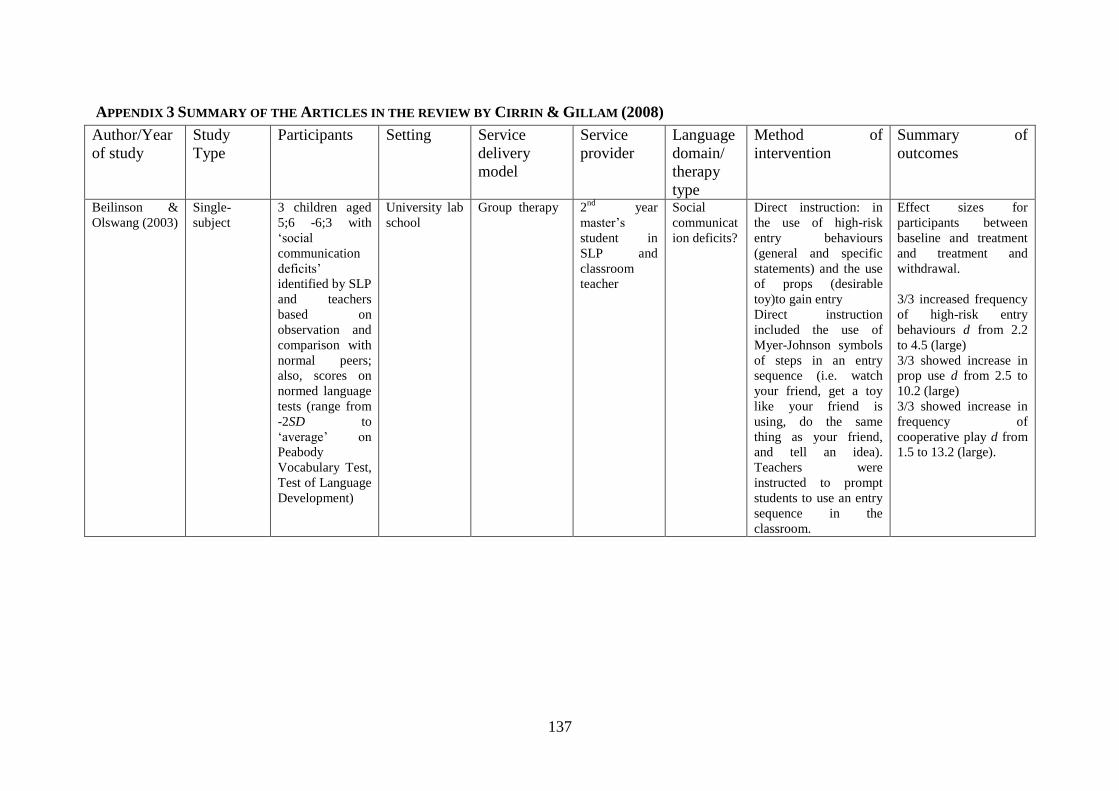
137
APPENDIX 3 SUMMARY OF THE ARTICLES IN THE REVIEW BY CIRRIN & GILLAM (2008)
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Beilinson &
Olswang (2003)
Single-
subject
3 children aged
5;6 -6;3 with
„social
communication
deficits‟
identified by SLP
and teachers
based on
observation and
comparison with
normal peers;
also, scores on
normed language
tests (range from
-2SD to
„average‟ on
Peabody
Vocabulary Test,
Test of Language
Development)
University lab
school
Group therapy 2nd
year
master‟s
student in
SLP and
classroom
teacher
Social
communicat
ion deficits?
Direct instruction: in
the use of high-risk
entry behaviours
(general and specific
statements) and the use
of props (desirable
toy)to gain entry
Direct instruction
included the use of
Myer-Johnson symbols
of steps in an entry
sequence (i.e. watch
your friend, get a toy
like your friend is
using, do the same
thing as your friend,
and tell an idea).
Teachers were
instructed to prompt
students to use an entry
sequence in the
classroom.
Effect sizes for
participants between
baseline and treatment
and treatment and
withdrawal.
3/3 increased frequency
of high-risk entry
behaviours d from 2.2
to 4.5 (large)
3/3 showed increase in
prop use d from 2.5 to
10.2 (large)
3/3 showed increase in
frequency of
cooperative play d from
1.5 to 13.2 (large).
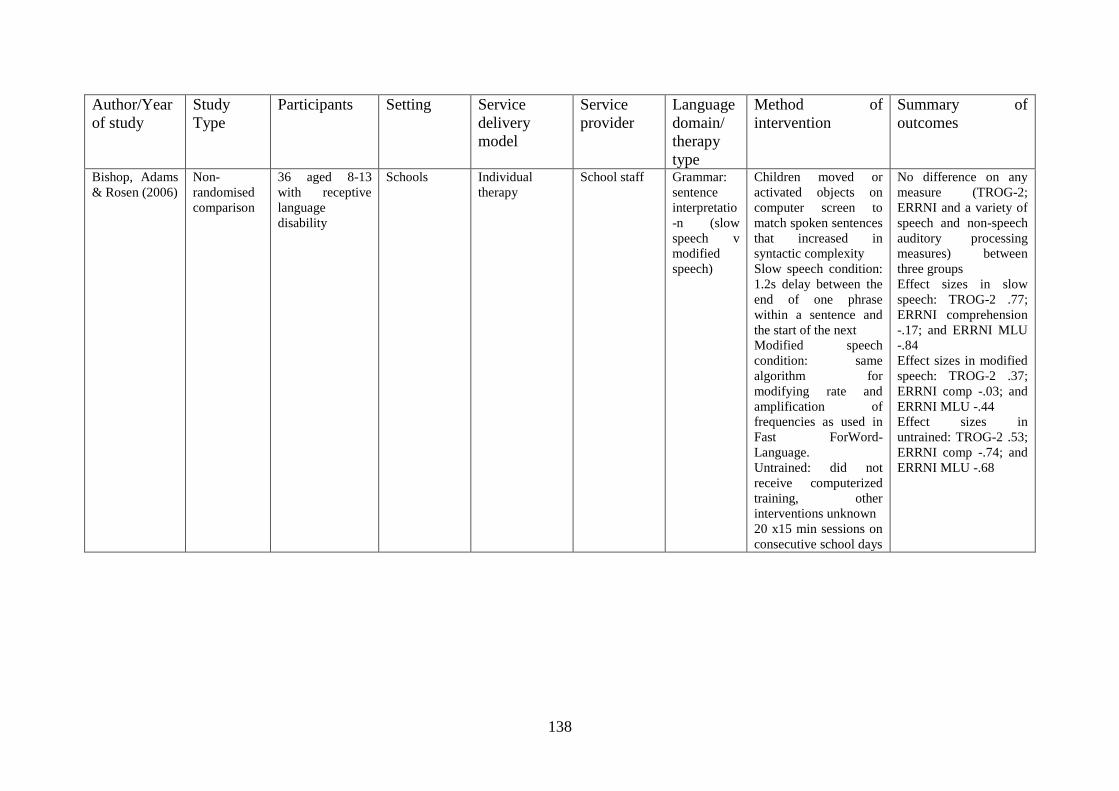
138
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Bishop, Adams
& Rosen (2006)
Non-
randomised
comparison
36 aged 8-13
with receptive
language
disability
Schools Individual
therapy
School staff Grammar:
sentence
interpretatio
-n (slow
speech v
modified
speech)
Children moved or
activated objects on
computer screen to
match spoken sentences
that increased in
syntactic complexity
Slow speech condition:
1.2s delay between the
end of one phrase
within a sentence and
the start of the next
Modified speech
condition: same
algorithm for
modifying rate and
amplification of
frequencies as used in
Fast ForWord-
Language.
Untrained: did not
receive computerized
training, other
interventions unknown
20 x15 min sessions on
consecutive school days
No difference on any
measure (TROG-2;
ERRNI and a variety of
speech and non-speech
auditory processing
measures) between
three groups
Effect sizes in slow
speech: TROG-2 .77;
ERRNI comprehension
-.17; and ERRNI MLU
-.84
Effect sizes in modified
speech: TROG-2 .37;
ERRNI comp -.03; and
ERRNI MLU -.44
Effect sizes in
untrained: TROG-2 .53;
ERRNI comp -.74; and
ERRNI MLU -.68
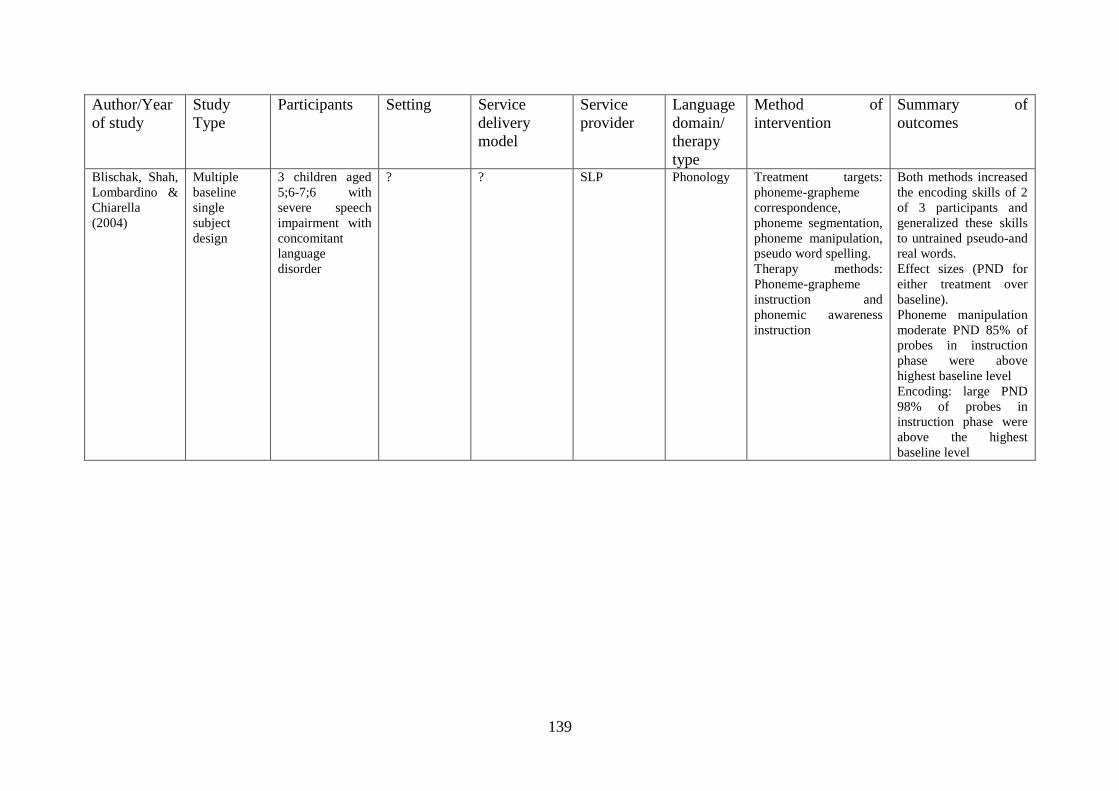
139
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Blischak, Shah,
Lombardino &
Chiarella
(2004)
Multiple
baseline
single
subject
design
3 children aged
5;6-7;6 with
severe speech
impairment with
concomitant
language
disorder
? ? SLP Phonology Treatment targets:
phoneme-grapheme
correspondence,
phoneme segmentation,
phoneme manipulation,
pseudo word spelling.
Therapy methods:
Phoneme-grapheme
instruction and
phonemic awareness
instruction
Both methods increased
the encoding skills of 2
of 3 participants and
generalized these skills
to untrained pseudo-and
real words.
Effect sizes (PND for
either treatment over
baseline).
Phoneme manipulation
moderate PND 85% of
probes in instruction
phase were above
highest baseline level
Encoding: large PND
98% of probes in
instruction phase were
above the highest
baseline level
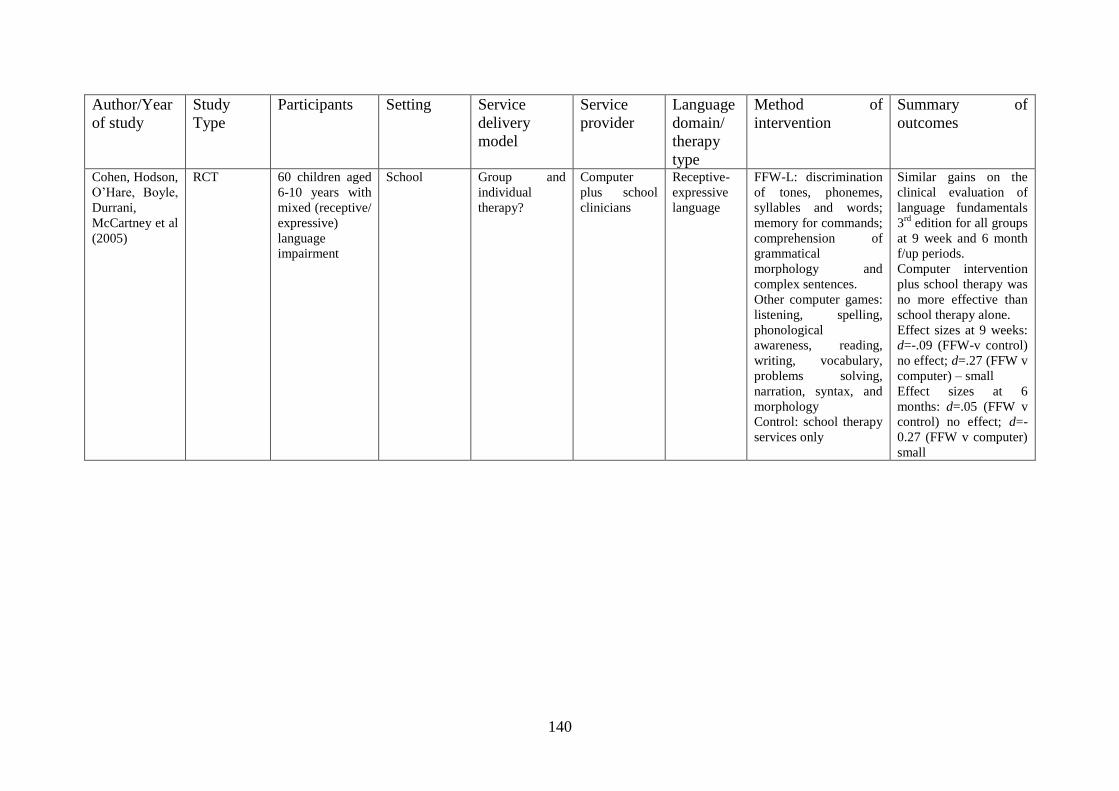
140
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Cohen, Hodson,
O‟Hare, Boyle,
Durrani,
McCartney et al
(2005)
RCT 60 children aged
6-10 years with
mixed (receptive/
expressive)
language
impairment
School Group and
individual
therapy?
Computer
plus school
clinicians
Receptive-
expressive
language
FFW-L: discrimination
of tones, phonemes,
syllables and words;
memory for commands;
comprehension of
grammatical
morphology and
complex sentences.
Other computer games:
listening, spelling,
phonological
awareness, reading,
writing, vocabulary,
problems solving,
narration, syntax, and
morphology
Control: school therapy
services only
Similar gains on the
clinical evaluation of
language fundamentals
3rd
edition for all groups
at 9 week and 6 month
f/up periods.
Computer intervention
plus school therapy was
no more effective than
school therapy alone.
Effect sizes at 9 weeks:
d=-.09 (FFW-v control)
no effect; d=.27 (FFW v
computer) – small
Effect sizes at 6
months: d=.05 (FFW v
control) no effect; d=-
0.27 (FFW v computer)
small
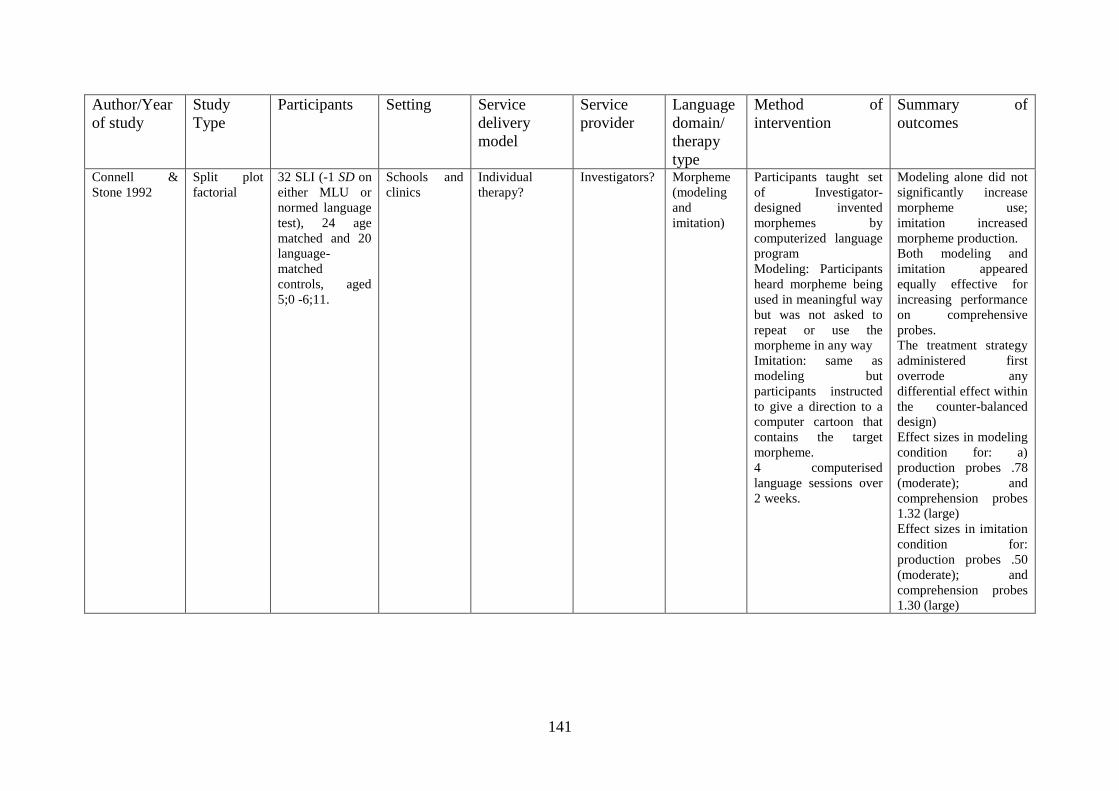
141
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Connell &
Stone 1992
Split plot
factorial
32 SLI (-1 SD on
either MLU or
normed language
test), 24 age
matched and 20
language-
matched
controls, aged
5;0 -6;11.
Schools and
clinics
Individual
therapy?
Investigators? Morpheme
(modeling
and
imitation)
Participants taught set
of Investigator-
designed invented
morphemes by
computerized language
program
Modeling: Participants
heard morpheme being
used in meaningful way
but was not asked to
repeat or use the
morpheme in any way
Imitation: same as
modeling but
participants instructed
to give a direction to a
computer cartoon that
contains the target
morpheme.
4 computerised
language sessions over
2 weeks.
Modeling alone did not
significantly increase
morpheme use;
imitation increased
morpheme production.
Both modeling and
imitation appeared
equally effective for
increasing performance
on comprehensive
probes.
The treatment strategy
administered first
overrode any
differential effect within
the counter-balanced
design)
Effect sizes in modeling
condition for: a)
production probes .78
(moderate); and
comprehension probes
1.32 (large)
Effect sizes in imitation
condition for:
production probes .50
(moderate); and
comprehension probes
1.30 (large)
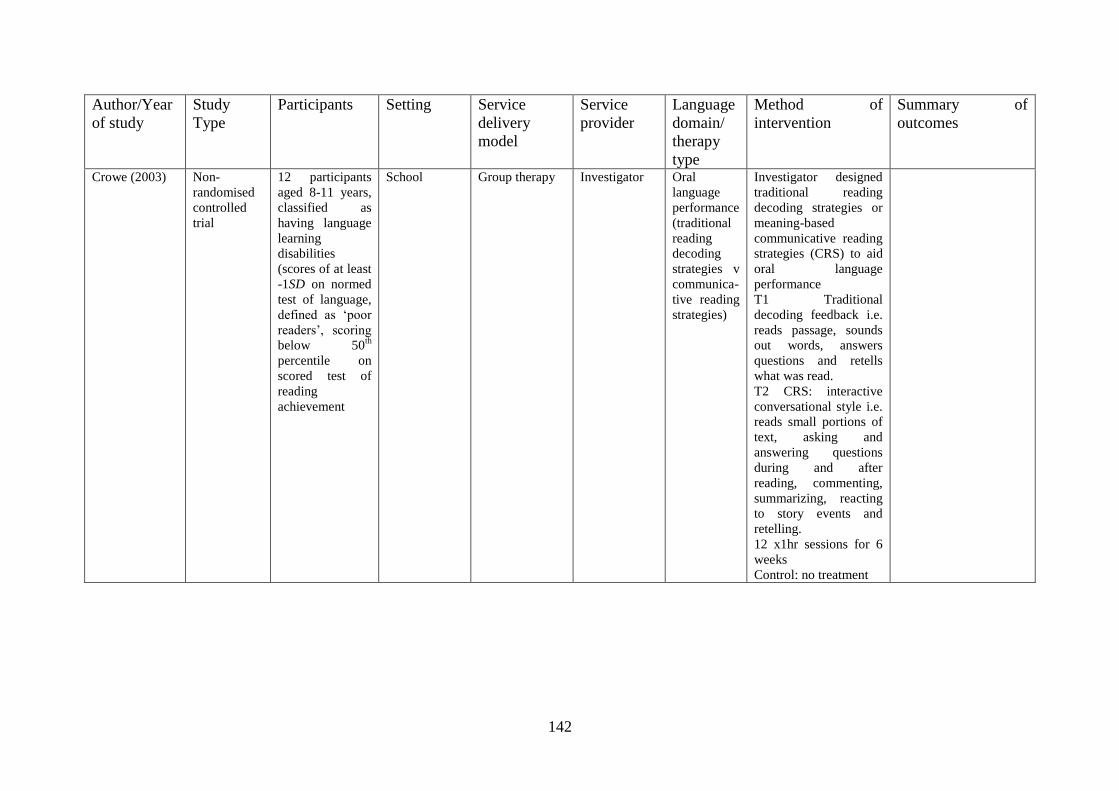
142
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Crowe (2003) Non-
randomised
controlled
trial
12 participants
aged 8-11 years,
classified as
having language
learning
disabilities
(scores of at least
-1SD on normed
test of language,
defined as „poor
readers‟, scoring
below 50th
percentile on
scored test of
reading
achievement
School Group therapy Investigator Oral
language
performance
(traditional
reading
decoding
strategies v
communica-
tive reading
strategies)
Investigator designed
traditional reading
decoding strategies or
meaning-based
communicative reading
strategies (CRS) to aid
oral language
performance
T1 Traditional
decoding feedback i.e.
reads passage, sounds
out words, answers
questions and retells
what was read.
T2 CRS: interactive
conversational style i.e.
reads small portions of
text, asking and
answering questions
during and after
reading, commenting,
summarizing, reacting
to story events and
retelling.
12 x1hr sessions for 6
weeks
Control: no treatment
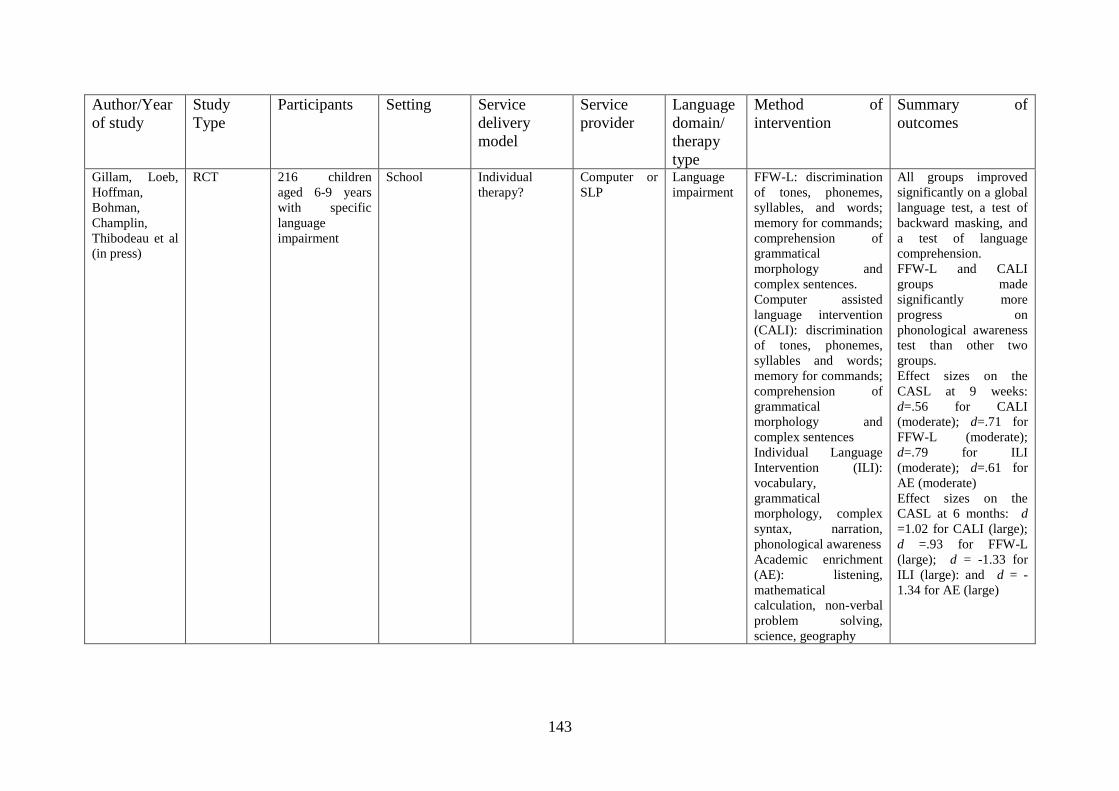
143
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Gillam, Loeb,
Hoffman,
Bohman,
Champlin,
Thibodeau et al
(in press)
RCT 216 children
aged 6-9 years
with specific
language
impairment
School Individual
therapy?
Computer or
SLP
Language
impairment
FFW-L: discrimination
of tones, phonemes,
syllables, and words;
memory for commands;
comprehension of
grammatical
morphology and
complex sentences.
Computer assisted
language intervention
(CALI): discrimination
of tones, phonemes,
syllables and words;
memory for commands;
comprehension of
grammatical
morphology and
complex sentences
Individual Language
Intervention (ILI):
vocabulary,
grammatical
morphology, complex
syntax, narration,
phonological awareness
Academic enrichment
(AE): listening,
mathematical
calculation, non-verbal
problem solving,
science, geography
All groups improved
significantly on a global
language test, a test of
backward masking, and
a test of language
comprehension.
FFW-L and CALI
groups made
significantly more
progress on
phonological awareness
test than other two
groups.
Effect sizes on the
CASL at 9 weeks:
d=.56 for CALI
(moderate); d=.71 for
FFW-L (moderate);
d=.79 for ILI
(moderate); d=.61 for
AE (moderate)
Effect sizes on the
CASL at 6 months: d
=1.02 for CALI (large);
d =.93 for FFW-L
(large); d = -1.33 for
ILI (large): and d = -
1.34 for AE (large)
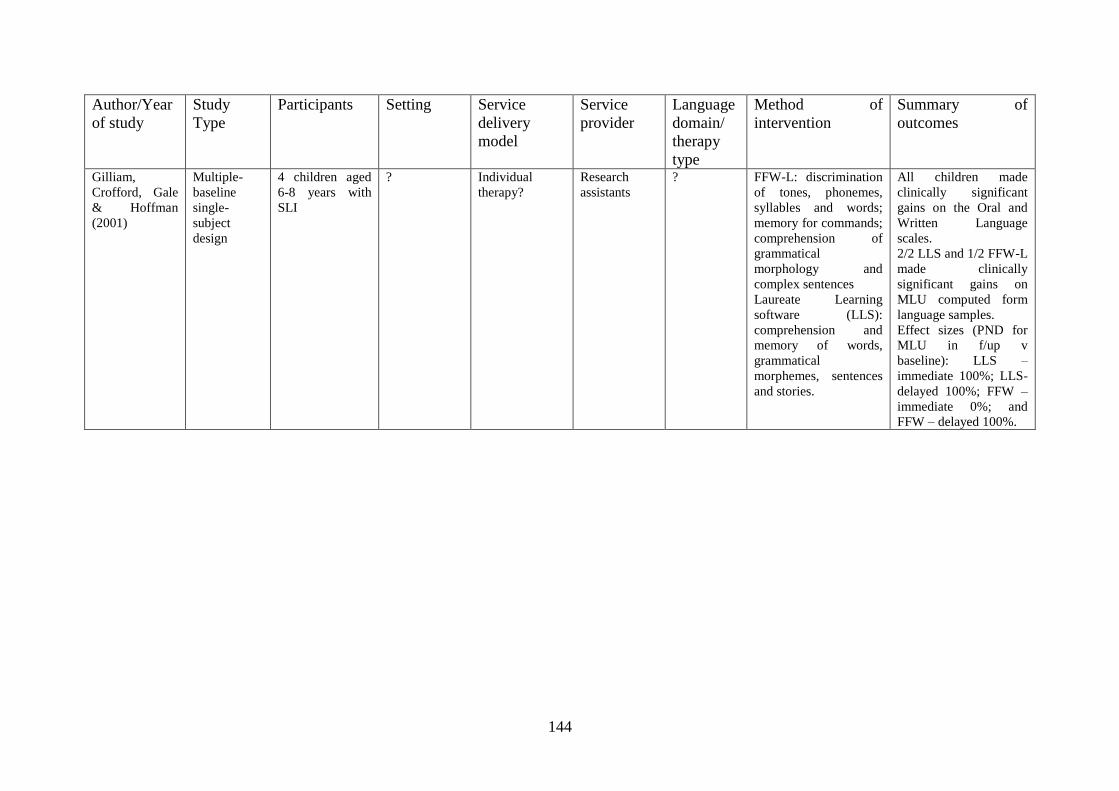
144
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Gilliam,
Crofford, Gale
& Hoffman
(2001)
Multiple-
baseline
single-
subject
design
4 children aged
6-8 years with
SLI
? Individual
therapy?
Research
assistants
? FFW-L: discrimination
of tones, phonemes,
syllables and words;
memory for commands;
comprehension of
grammatical
morphology and
complex sentences
Laureate Learning
software (LLS):
comprehension and
memory of words,
grammatical
morphemes, sentences
and stories.
All children made
clinically significant
gains on the Oral and
Written Language
scales.
2/2 LLS and 1/2 FFW-L
made clinically
significant gains on
MLU computed form
language samples.
Effect sizes (PND for
MLU in f/up v
baseline): LLS –
immediate 100%; LLS-
delayed 100%; FFW –
immediate 0%; and
FFW – delayed 100%.
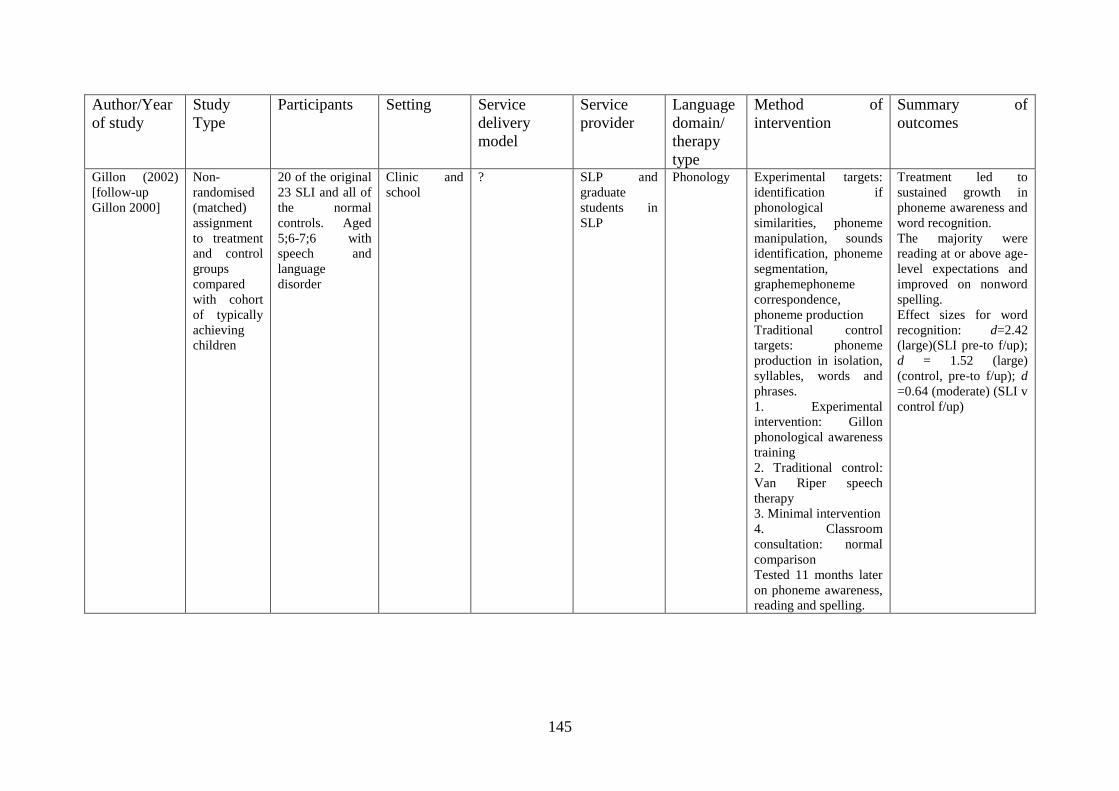
145
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Gillon (2002)
[follow-up
Gillon 2000]
Non-
randomised
(matched)
assignment
to treatment
and control
groups
compared
with cohort
of typically
achieving
children
20 of the original
23 SLI and all of
the normal
controls. Aged
5;6-7;6 with
speech and
language
disorder
Clinic and
school
? SLP and
graduate
students in
SLP
Phonology Experimental targets:
identification if
phonological
similarities, phoneme
manipulation, sounds
identification, phoneme
segmentation,
graphemephoneme
correspondence,
phoneme production
Traditional control
targets: phoneme
production in isolation,
syllables, words and
phrases.
1. Experimental
intervention: Gillon
phonological awareness
training
2. Traditional control:
Van Riper speech
therapy
3. Minimal intervention
4. Classroom
consultation: normal
comparison
Tested 11 months later
on phoneme awareness,
reading and spelling.
Treatment led to
sustained growth in
phoneme awareness and
word recognition.
The majority were
reading at or above age-
level expectations and
improved on nonword
spelling.
Effect sizes for word
recognition: d=2.42
(large)(SLI pre-to f/up);
d = 1.52 (large)
(control, pre-to f/up); d
=0.64 (moderate) (SLI v
control f/up)
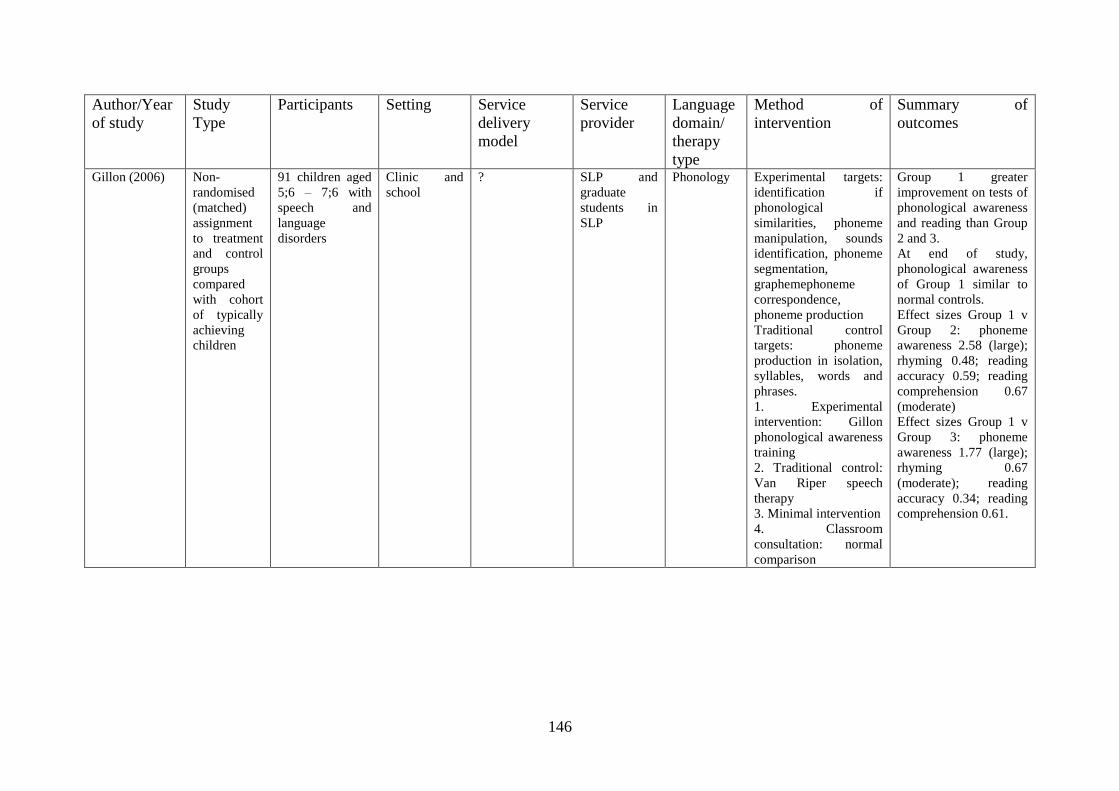
146
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Gillon (2006) Non-
randomised
(matched)
assignment
to treatment
and control
groups
compared
with cohort
of typically
achieving
children
91 children aged
5;6 – 7;6 with
speech and
language
disorders
Clinic and
school
? SLP and
graduate
students in
SLP
Phonology Experimental targets:
identification if
phonological
similarities, phoneme
manipulation, sounds
identification, phoneme
segmentation,
graphemephoneme
correspondence,
phoneme production
Traditional control
targets: phoneme
production in isolation,
syllables, words and
phrases.
1. Experimental
intervention: Gillon
phonological awareness
training
2. Traditional control:
Van Riper speech
therapy
3. Minimal intervention
4. Classroom
consultation: normal
comparison
Group 1 greater
improvement on tests of
phonological awareness
and reading than Group
2 and 3.
At end of study,
phonological awareness
of Group 1 similar to
normal controls.
Effect sizes Group 1 v
Group 2: phoneme
awareness 2.58 (large);
rhyming 0.48; reading
accuracy 0.59; reading
comprehension 0.67
(moderate)
Effect sizes Group 1 v
Group 3: phoneme
awareness 1.77 (large);
rhyming 0.67
(moderate); reading
accuracy 0.34; reading
comprehension 0.61.
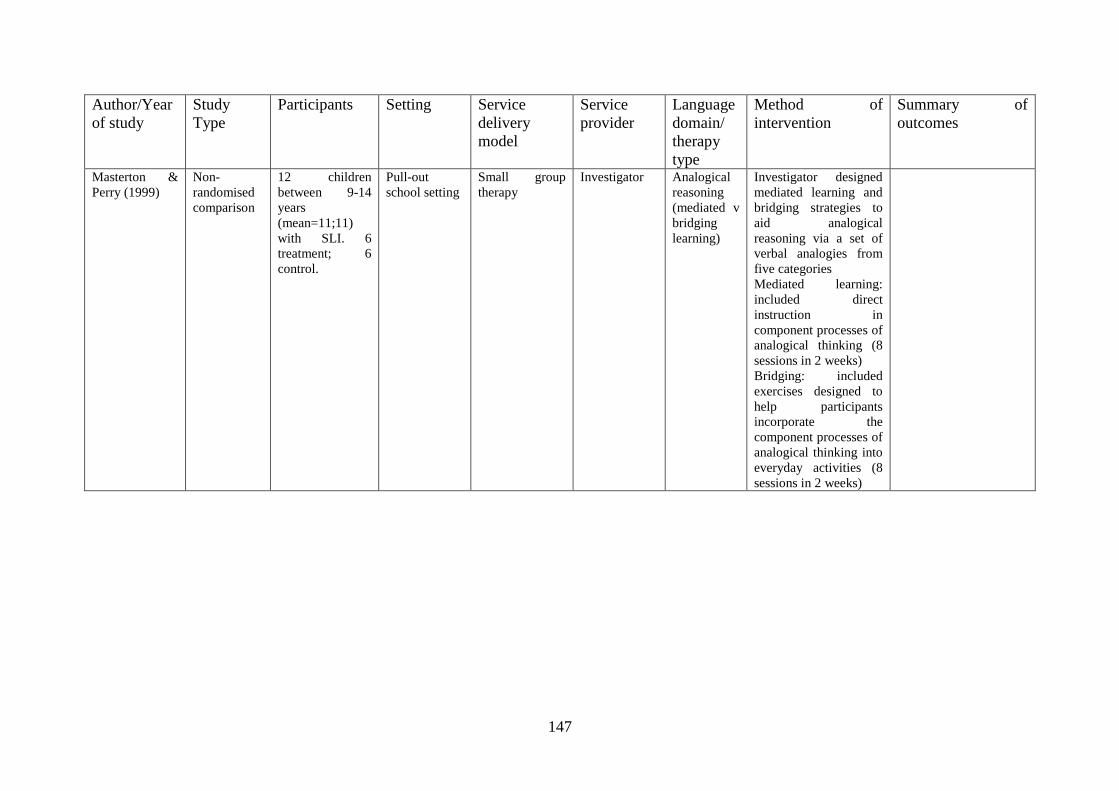
147
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Masterton &
Perry (1999)
Non-
randomised
comparison
12 children
between 9-14
years
(mean=11;11)
with SLI. 6
treatment; 6
control.
Pull-out
school setting
Small group
therapy
Investigator Analogical
reasoning
(mediated v
bridging
learning)
Investigator designed
mediated learning and
bridging strategies to
aid analogical
reasoning via a set of
verbal analogies from
five categories
Mediated learning:
included direct
instruction in
component processes of
analogical thinking (8
sessions in 2 weeks)
Bridging: included
exercises designed to
help participants
incorporate the
component processes of
analogical thinking into
everyday activities (8
sessions in 2 weeks)
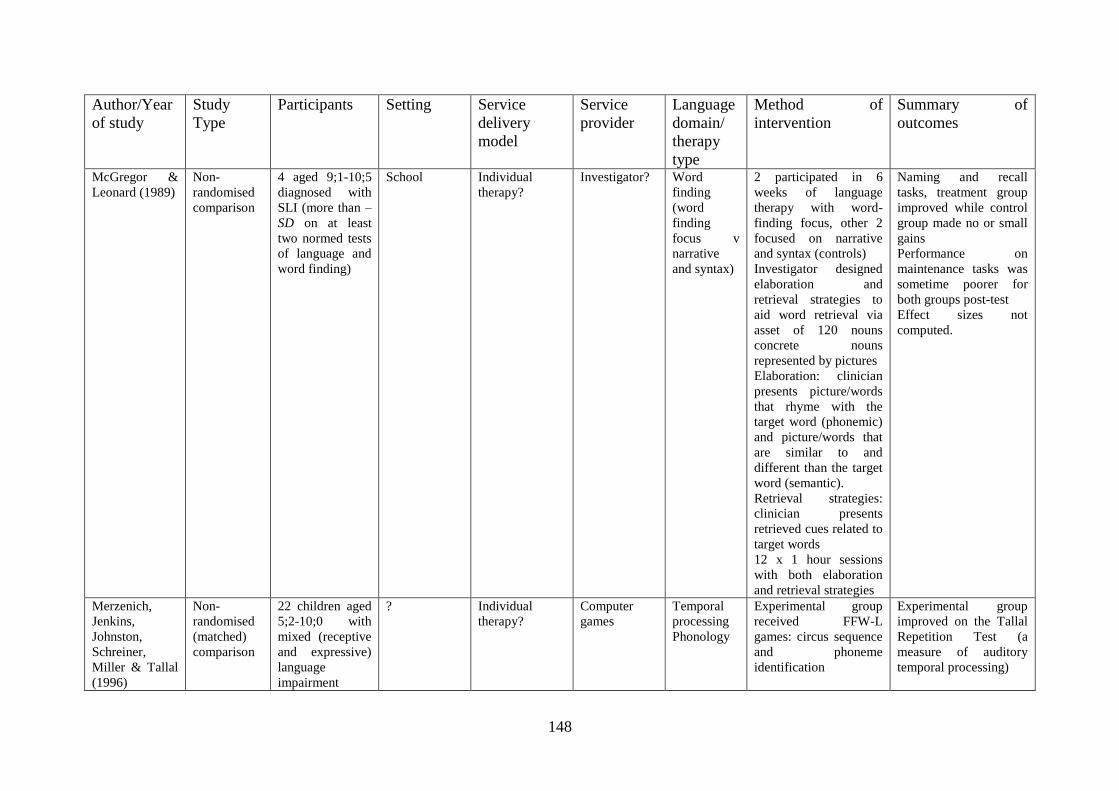
148
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
McGregor &
Leonard (1989)
Non-
randomised
comparison
4 aged 9;1-10;5
diagnosed with
SLI (more than –
SD on at least
two normed tests
of language and
word finding)
School Individual
therapy?
Investigator? Word
finding
(word
finding
focus v
narrative
and syntax)
2 participated in 6
weeks of language
therapy with word-
finding focus, other 2
focused on narrative
and syntax (controls)
Investigator designed
elaboration and
retrieval strategies to
aid word retrieval via
asset of 120 nouns
concrete nouns
represented by pictures
Elaboration: clinician
presents picture/words
that rhyme with the
target word (phonemic)
and picture/words that
are similar to and
different than the target
word (semantic).
Retrieval strategies:
clinician presents
retrieved cues related to
target words
12 x 1 hour sessions
with both elaboration
and retrieval strategies
Naming and recall
tasks, treatment group
improved while control
group made no or small
gains
Performance on
maintenance tasks was
sometime poorer for
both groups post-test
Effect sizes not
computed.
Merzenich,
Jenkins,
Johnston,
Schreiner,
Miller & Tallal
(1996)
Non-
randomised
(matched)
comparison
22 children aged
5;2-10;0 with
mixed (receptive
and expressive)
language
impairment
? Individual
therapy?
Computer
games
Temporal
processing
Phonology
Experimental group
received FFW-L
games: circus sequence
and phoneme
identification
Experimental group
improved on the Tallal
Repetition Test (a
measure of auditory
temporal processing)
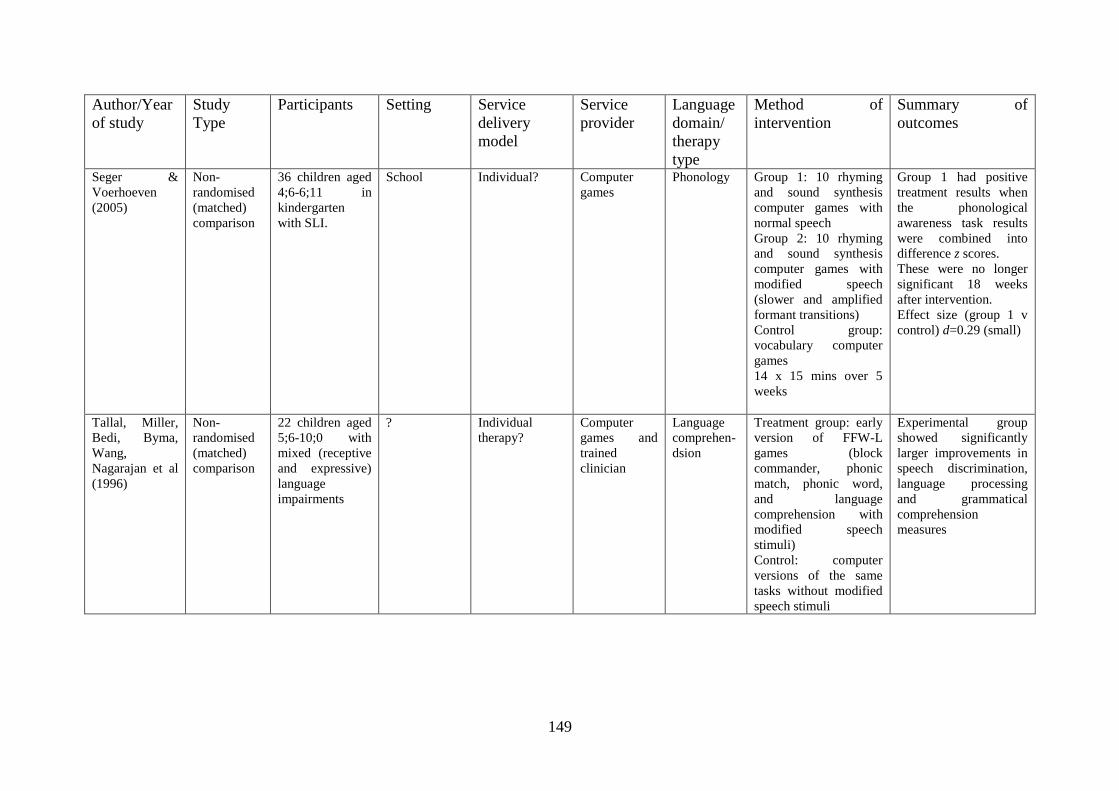
149
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Seger &
Voerhoeven
(2005)
Non-
randomised
(matched)
comparison
36 children aged
4;6-6;11 in
kindergarten
with SLI.
School Individual? Computer
games
Phonology Group 1: 10 rhyming
and sound synthesis
computer games with
normal speech
Group 2: 10 rhyming
and sound synthesis
computer games with
modified speech
(slower and amplified
formant transitions)
Control group:
vocabulary computer
games
14 x 15 mins over 5
weeks
Group 1 had positive
treatment results when
the phonological
awareness task results
were combined into
difference z scores.
These were no longer
significant 18 weeks
after intervention.
Effect size (group 1 v
control) d=0.29 (small)
Tallal, Miller,
Bedi, Byma,
Wang,
Nagarajan et al
(1996)
Non-
randomised
(matched)
comparison
22 children aged
5;6-10;0 with
mixed (receptive
and expressive)
language
impairments
? Individual
therapy?
Computer
games and
trained
clinician
Language
comprehen-
dsion
Treatment group: early
version of FFW-L
games (block
commander, phonic
match, phonic word,
and language
comprehension with
modified speech
stimuli)
Control: computer
versions of the same
tasks without modified
speech stimuli
Experimental group
showed significantly
larger improvements in
speech discrimination,
language processing
and grammatical
comprehension
measures
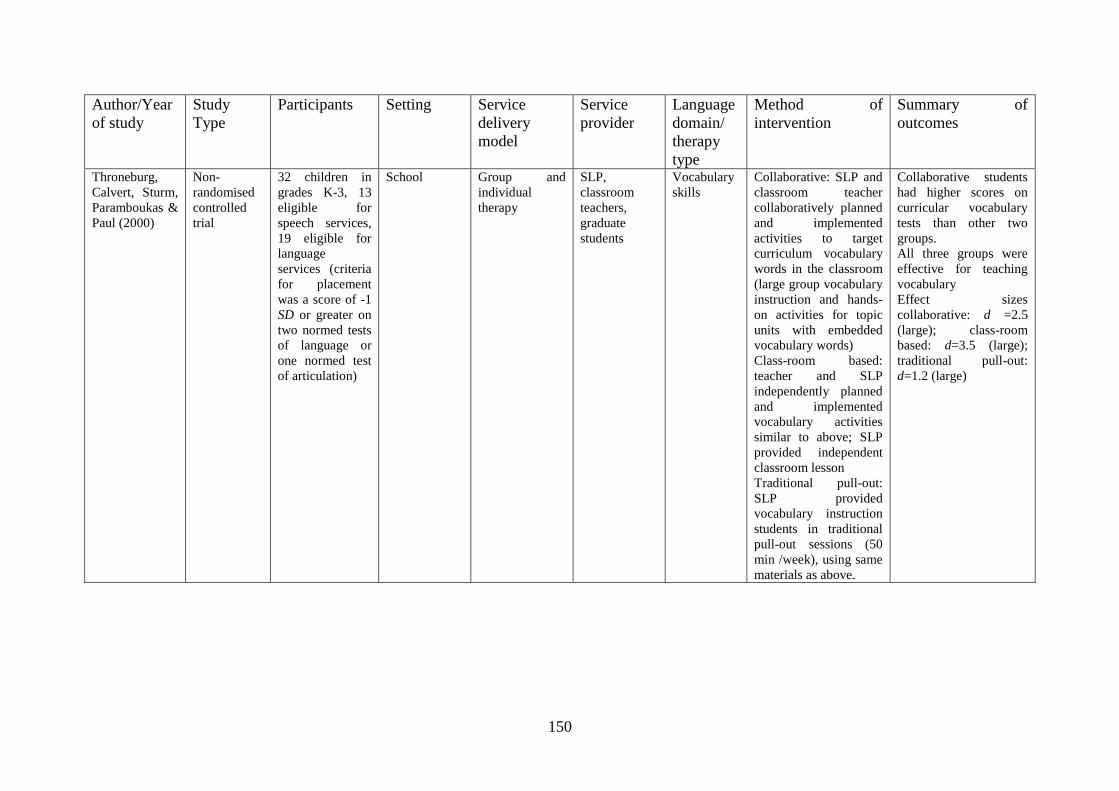
150
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Throneburg,
Calvert, Sturm,
Paramboukas &
Paul (2000)
Non-
randomised
controlled
trial
32 children in
grades K-3, 13
eligible for
speech services,
19 eligible for
language
services (criteria
for placement
was a score of -1
SD or greater on
two normed tests
of language or
one normed test
of articulation)
School Group and
individual
therapy
SLP,
classroom
teachers,
graduate
students
Vocabulary
skills
Collaborative: SLP and
classroom teacher
collaboratively planned
and implemented
activities to target
curriculum vocabulary
words in the classroom
(large group vocabulary
instruction and hands-
on activities for topic
units with embedded
vocabulary words)
Class-room based:
teacher and SLP
independently planned
and implemented
vocabulary activities
similar to above; SLP
provided independent
classroom lesson
Traditional pull-out:
SLP provided
vocabulary instruction
students in traditional
pull-out sessions (50
min /week), using same
materials as above.
Collaborative students
had higher scores on
curricular vocabulary
tests than other two
groups.
All three groups were
effective for teaching
vocabulary
Effect sizes
collaborative: d =2.5
(large); class-room
based: d=3.5 (large);
traditional pull-out:
d=1.2 (large)
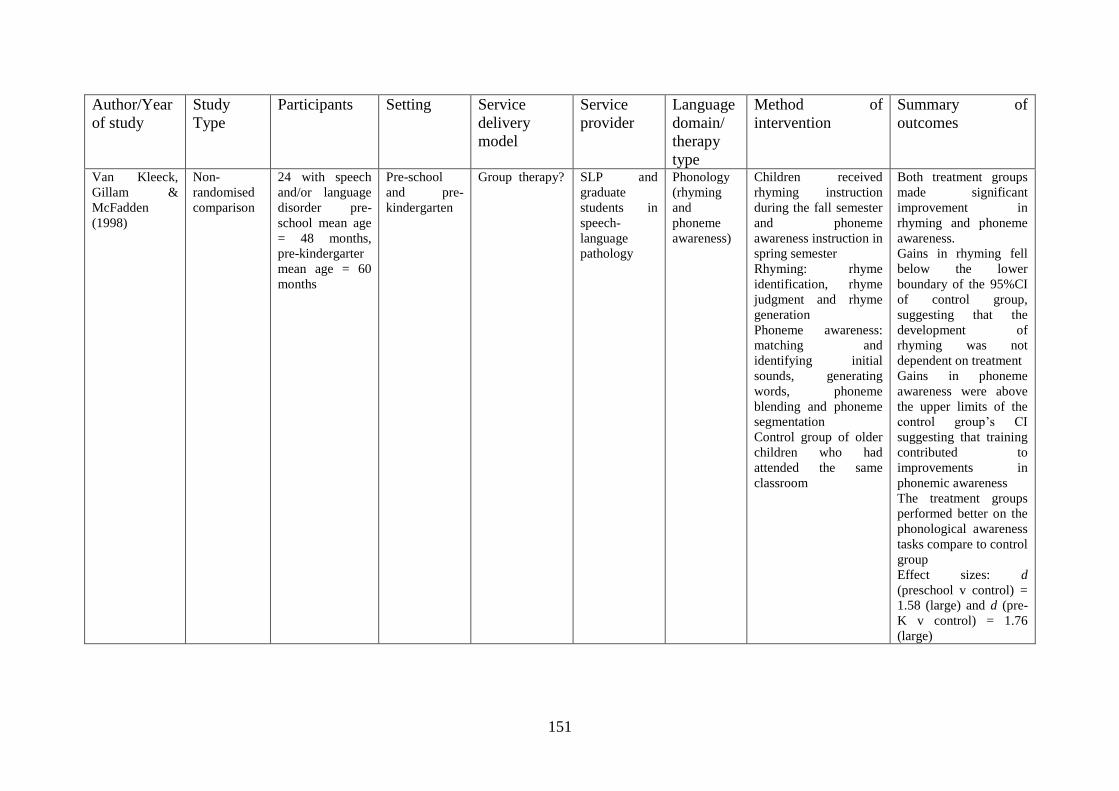
151
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Van Kleeck,
Gillam &
McFadden
(1998)
Non-
randomised
comparison
24 with speech
and/or language
disorder pre-
school mean age
= 48 months,
pre-kindergarter
mean age = 60
months
Pre-school
and pre-
kindergarten
Group therapy? SLP and
graduate
students in
speech-
language
pathology
Phonology
(rhyming
and
phoneme
awareness)
Children received
rhyming instruction
during the fall semester
and phoneme
awareness instruction in
spring semester
Rhyming: rhyme
identification, rhyme
judgment and rhyme
generation
Phoneme awareness:
matching and
identifying initial
sounds, generating
words, phoneme
blending and phoneme
segmentation
Control group of older
children who had
attended the same
classroom
Both treatment groups
made significant
improvement in
rhyming and phoneme
awareness.
Gains in rhyming fell
below the lower
boundary of the 95%CI
of control group,
suggesting that the
development of
rhyming was not
dependent on treatment
Gains in phoneme
awareness were above
the upper limits of the
control group‟s CI
suggesting that training
contributed to
improvements in
phonemic awareness
The treatment groups
performed better on the
phonological awareness
tasks compare to control
group
Effect sizes: d
(preschool v control) =
1.58 (large) and d (pre-
K v control) = 1.76
(large)
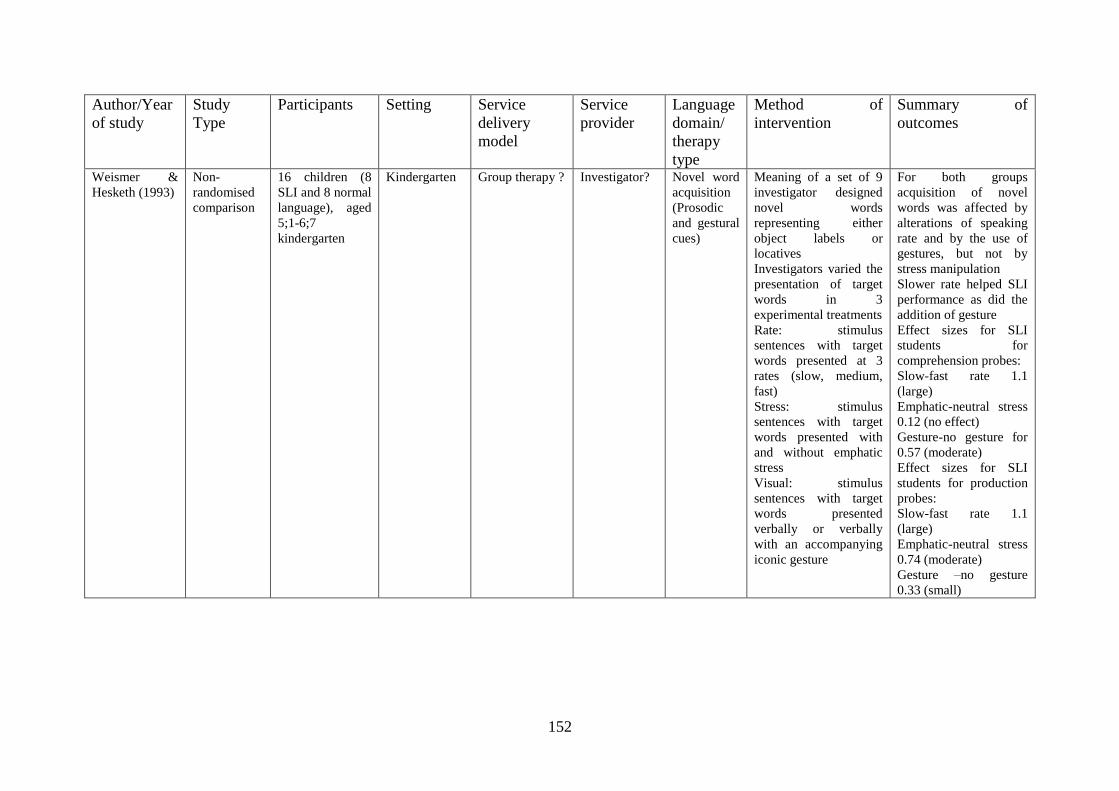
152
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Weismer &
Hesketh (1993)
Non-
randomised
comparison
16 children (8
SLI and 8 normal
language), aged
5;1-6;7
kindergarten
Kindergarten Group therapy ? Investigator? Novel word
acquisition
(Prosodic
and gestural
cues)
Meaning of a set of 9
investigator designed
novel words
representing either
object labels or
locatives
Investigators varied the
presentation of target
words in 3
experimental treatments
Rate: stimulus
sentences with target
words presented at 3
rates (slow, medium,
fast)
Stress: stimulus
sentences with target
words presented with
and without emphatic
stress
Visual: stimulus
sentences with target
words presented
verbally or verbally
with an accompanying
iconic gesture
For both groups
acquisition of novel
words was affected by
alterations of speaking
rate and by the use of
gestures, but not by
stress manipulation
Slower rate helped SLI
performance as did the
addition of gesture
Effect sizes for SLI
students for
comprehension probes:
Slow-fast rate 1.1
(large)
Emphatic-neutral stress
0.12 (no effect)
Gesture-no gesture for
0.57 (moderate)
Effect sizes for SLI
students for production
probes:
Slow-fast rate 1.1
(large)
Emphatic-neutral stress
0.74 (moderate)
Gesture –no gesture
0.33 (small)
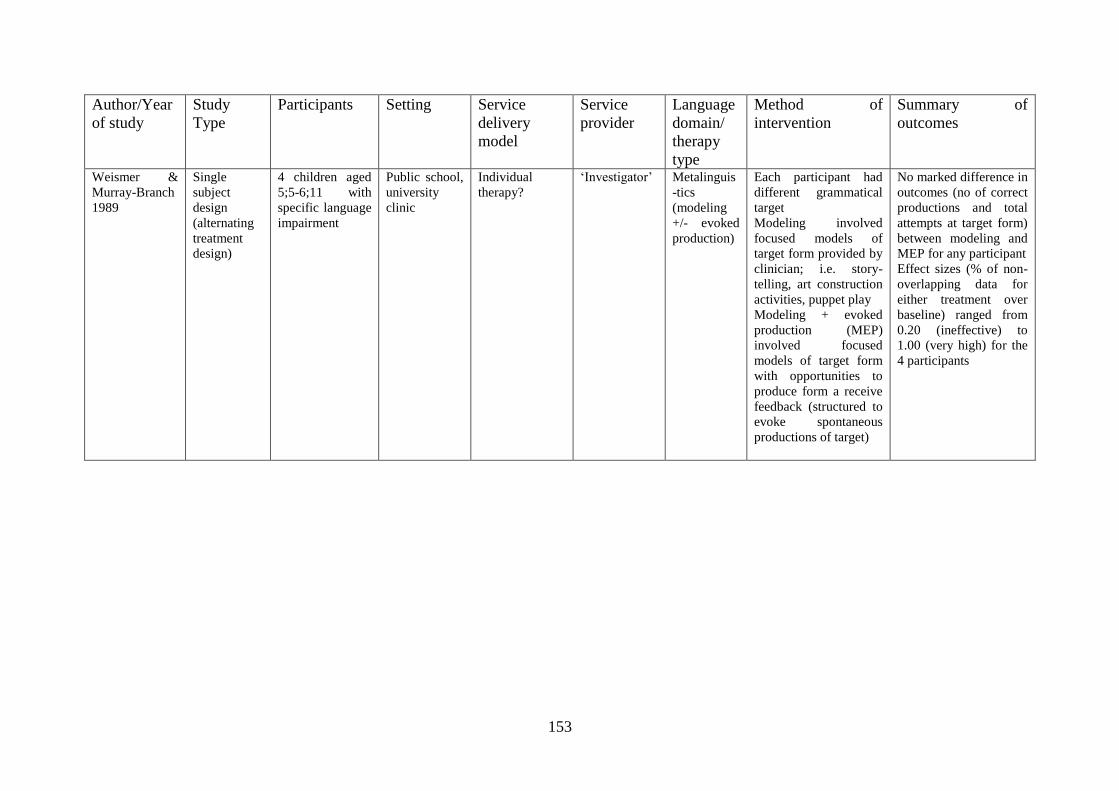
153
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Weismer &
Murray-Branch
1989
Single
subject
design
(alternating
treatment
design)
4 children aged
5;5-6;11 with
specific language
impairment
Public school,
university
clinic
Individual
therapy?
„Investigator‟ Metalinguis
-tics
(modeling
+/- evoked
production)
Each participant had
different grammatical
target
Modeling involved
focused models of
target form provided by
clinician; i.e. story-
telling, art construction
activities, puppet play
Modeling + evoked
production (MEP)
involved focused
models of target form
with opportunities to
produce form a receive
feedback (structured to
evoke spontaneous
productions of target)
No marked difference in
outcomes (no of correct
productions and total
attempts at target form)
between modeling and
MEP for any participant
Effect sizes (% of non-
overlapping data for
either treatment over
baseline) ranged from
0.20 (ineffective) to
1.00 (very high) for the
4 participants
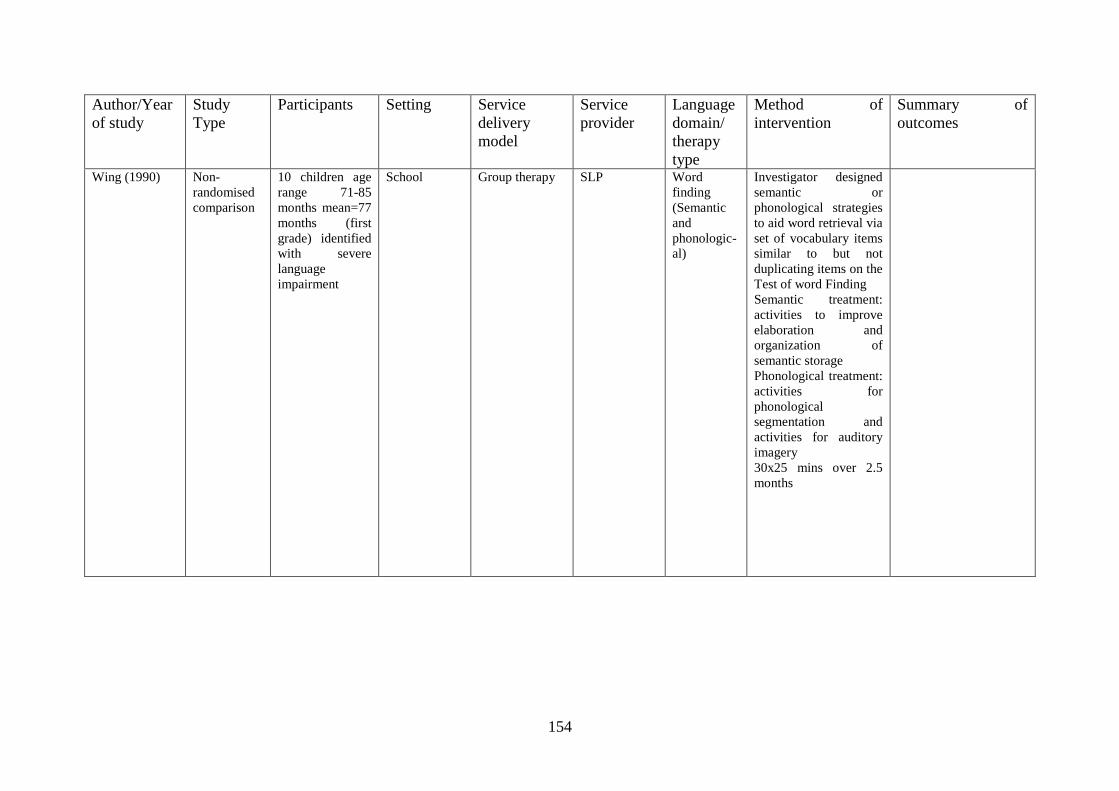
154
Author/Year
of study
Study
Type
Participants Setting Service
delivery
model
Service
provider
Language
domain/
therapy
type
Method of
intervention
Summary of
outcomes
Wing (1990) Non-
randomised
comparison
10 children age
range 71-85
months mean=77
months (first
grade) identified
with severe
language
impairment
School Group therapy SLP Word
finding
(Semantic
and
phonologic-
al)
Investigator designed
semantic or
phonological strategies
to aid word retrieval via
set of vocabulary items
similar to but not
duplicating items on the
Test of word Finding
Semantic treatment:
activities to improve
elaboration and
organization of
semantic storage
Phonological treatment:
activities for
phonological
segmentation and
activities for auditory
imagery
30x25 mins over 2.5
months












![Comparison of speech and language therapy techniques for ...€¦ · [Intervention Review] Comparison of speech and language therapy techniques for speech problems in Parkinson’s](https://static.fdocuments.in/doc/165x107/5f3cd008f32a407b616e050d/comparison-of-speech-and-language-therapy-techniques-for-intervention-review.jpg)





