Final Perioperative Nursing
67
Prof. Joseph Bahian Abang, AHSE, BSN, RN, MAN (c) Major in Nursing Supervision and Administration
-
Upload
yucef-bahian-abang -
Category
Documents
-
view
249 -
download
4
description
lecture notes
Transcript of Final Perioperative Nursing

Prof. Joseph Bahian Abang,
AHSE, BSN, RN, MAN (c)Major in Nursing Supervision and
Administration
The Core Concepts of
Perioperative Nursing

SurgeryTerminology• -ectomy• -otomy• -oscopy• -ostomy• -oplasty• -rrhapy

Purpose of Surgery(DPACTC)
• Diagnostic• Palliative• Ablative• Constructive• Transplant• Curative

Degree of Urgency(EURE)
• Emergency• Urgent• Required • Elective

Degree of Risk(MM)
• Major• MinorAffected by factors such as:GAMeMeNu• General health condition• Age• Medications• Mental status• Nutrition

Surgical Settings(SACPHC)• Surgical suites• Ambulatory care setting• Clinics• Physician offices• Homes• Community setting

Perioperative Nursing3 Phases• Preoperative Phase
• Intraoperative Phase
• Post-operative Phase

PRE-OPERATIVE PHASE
Collaborative Management•History and data collection•Age•Drugs and substance use•Medical history, including cardiac
and pulmonary histories• Previous surgery and anesthesia•Blood donations•Discharge planning

• Physical Assessment/Clinical Manifestations• Obtain baseline vital signs.• Focus on problem areas identified by
the client’s history on all body systems affected by the surgical procedure.• Report any abnormal assessment
findings to the surgeon and to anesthesiology personnel

System Assessment• Cardiovascular system• Respiratory system• Renal/urinary system• Neurologic system• Musculoskeletal system• Nutritional status• Psychosocial assessment• Gerontological Considerations• Psychosocial considerations• Level of anxiety• Coping ability• Support systems
Gerontological ConsiderationsTake Note on the Functioning of the Following Systems• Cardiovascular• Respiratory• Nervous• Renal• Gastrointestinal•Musculoskeletal• Integumentary
Laboratory Assessment• Urinalysis• Blood type and crossmatch• Complete blood count or hemoglobin
level and hematocrit• Clotting studies (PT & PTT)• Electrolyte levels• Serum creatinine level• Pregnancy test• Chest x-ray examination• Electrocardiogram

Nursing Considerations• Consent• Implementing Dietary Measures• Administering Regularly Scheduled
Medications• Intestinal Preparation• Skin Preparation• Preparing the Client• Pre-operative Chart Review• Pre-operative Medications

Common Pre-operative Medications• Versed – Benzodiazepines • Fentanyl – Narcotic/Opiate • Tagamet – H2 receptor antagonist • Reglan – Antiemetics • Robinul – Anticholinergics • Ancef - antiinfective, antibiotic

Hazardous to Surgery• Antibiotics• Anti-depressants• Phenothiazines• Diuretics• Steriods• Anticoagulants

Pre-anesthesia Management Physical Status CategoriesASA I: Healthy patient with no diseaseASA II: Mild systemic ds without fx limitationsASA III: Severe systemic ds associated with
definite fx limitationsASA IV: Severe systemic ds that is a constant
threat to life.ASA V: Moribund pt. Who is not expected to
survive without the operation.ASA VI: A declared brain-death whose organ
are being recovered for donor.E: Emergency

INTRA-OPERATIVE PHASE

Members of the Surgical Team• Surgeon• Surgical assistant• Anesthesiologist• Certified registered nurse anesthetist• Holding area nurse• Circulating nurse• Scrub nurse• Surgical technologist • Operating room technician

Operating Room Attire• Scrub suit• Head cover (bonnet)• Shoe cover (OR Slipper)• Surgical maskPPE• Aprons• Surgical gown• Surgical gloves• Gloves• Eyewear/face shield

3 Surgical Areas of the Operating Room• Restricted area• Scrub suit, head cap, shoe cover and
mask• Semi-restricted area• Scrub suit, head cap, shoe cover
• Monitored Un-restricted area/transition area• Scrub personnel may use this area as
the transition area• Ordinary pants and shirt

Sterile vs. Asepsis Define:Sterile
-free of microorganisms including pores
Asepsis-absence of microorganisms that
cause a disease.

Surgical AsepsisPrinciples1.Only sterile items are used within the sterile
field.2.Sterile persons are gown and gloved.3.Tables are only sterile at Table Level4.Sterile Persons Touch ONLY Sterile Items while
Unsterile OR Personnel Touch Only Unsterile Items
5.Unsterile persons avoid reaching over sterile field and sterile persons avoid touching or leaning over an unsterile area.
6.Edges of anything that encloses sterile contents are considered unsterile.

7. Sterile field is set-up just before a surgical procedure.8. Sterile areas are continuously kept in view.9. Sterile persons keep well within sterile area.10. Sterile persons keep in contact with sterile areas to minimum.11. Unsterile persons avoid sterile areas12. Destruction of integrity of microbial barriers result in contamination.13. Microorganisms must be kept to irreducible minimum.

Types of Sterilization•Moist Heat • Autoclave• High speed sterilization autoclave
• Radiation • Radiation ionizing energy
• Chemical • Cidex, Sporocidin, Wexcide
• Ethylene Oxide Gas • Boiling water

Types of Sterilization•Moist Heat • Autoclave• High speed sterilization autoclave
• Radiation • Radiation ionizing energy
• Chemical • Cidex, Sporocidin, Wexcide
• Ethylene Oxide Gas • Boiling water

Types of Surgical Instruments• Graspers• Clamps and occluders • Retractors• Distractors, positioners and stereotactic
devices• Mechanical cutters (scalpels, lancets, drill bits,
rasps, trocars) Dilators and specula• Suction tips and tubes• Sealing devices• Irrigation and injection needles, tips and tubes• Tyndallers• Powered devices

Types of Surgical Instruments• Scopes and probes• Carriers and appliers • Ultrasound tissue disruptors, and
cutting laser guides• Measurement devices

Surgical Instruments
Alias - NoneUse - GraspingAdditional Info - Often used for grasping soft tissue such as breast tissue or bowel tissue

Alias - US RetractorUse - Tissue or Bone RetractionAdditional Info - Common to the both major and minor orthopedic and general surgery trays .

Alias - NoneUse - GraspingAdditional Info - For grasping soft tissue or bowel.

Alias - NoneUse - GraspingAdditional Info - Often used for grasping fascia during the closure of abdominal surgery or for closure and suturing of large orthopedic procedures such as total knee and total hip replacement surgery.
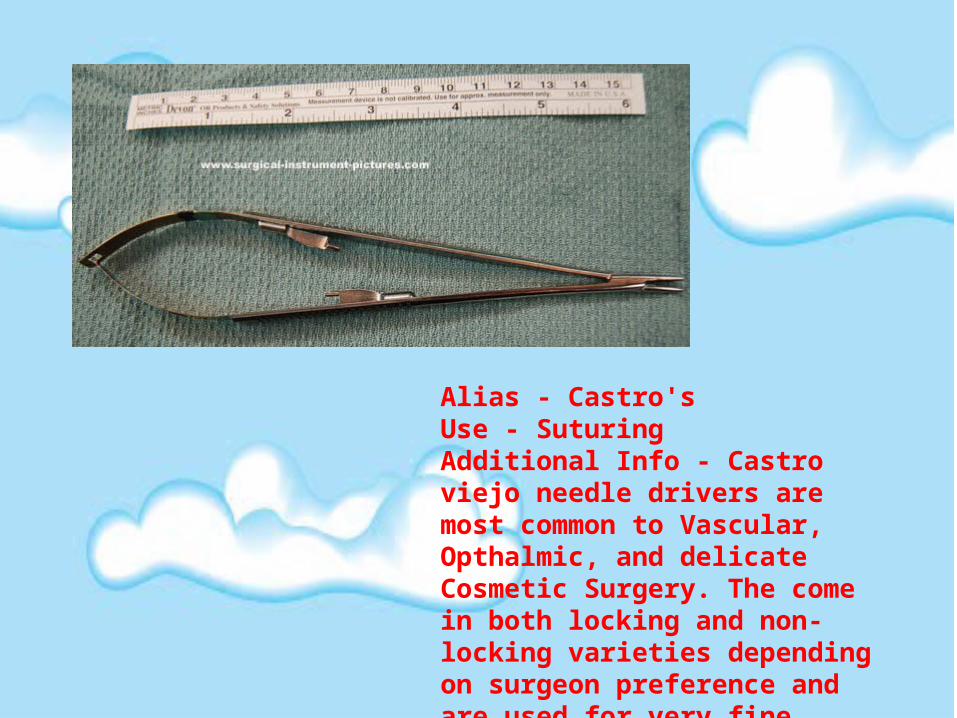
Alias - Castro'sUse - SuturingAdditional Info - Castro viejo needle drivers are most common to Vascular, Opthalmic, and delicate Cosmetic Surgery. The come in both locking and non-locking varieties depending on surgeon preference and are used for very fine suture in the 5-0 and smaller range.

Alias - NoneUse - CuttingAdditional Info - Common to most surgical trays, used for cutting dense tissue where Metz scissors are too delicate.
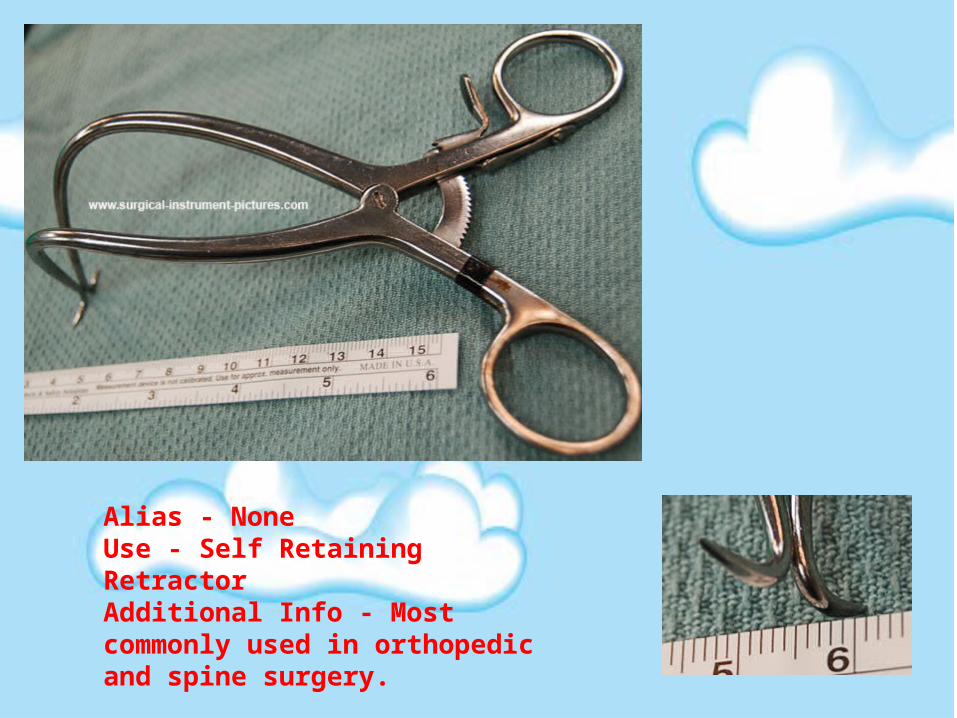
Alias - NoneUse - Self Retaining RetractorAdditional Info - Most commonly used in orthopedic and spine surgery.

Alias - NoneUse - CuttingAdditional Info - Used for cutting bone in othopedic and spine surgery.

Alias - NoneUse - ClampingAdditional Info - For both permanent and temporary ligation of vessels and marking tissue for post operative imaging.
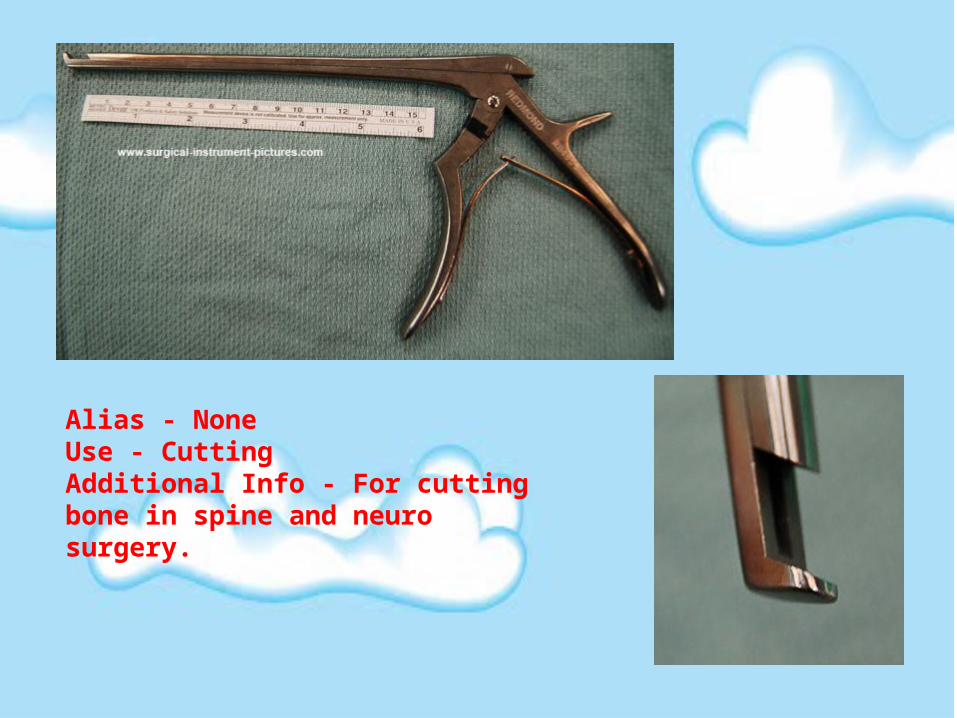
Alias - NoneUse - CuttingAdditional Info - For cutting bone in spine and neuro surgery.

Alias - NoneUse - GraspingAdditional Info - Used to grasp bone or fascia.

Alias - NoneUse - RetractionAdditional Info - For rectration in large abdominal surgeries.

Alias - MetzUse - CuttingAdditional Info - The most common scissors use for cutting tissue.

Alias - NoneUse - Blunt DisectionAdditional Info - None

Alias - NoneUse - SuctionAdditional Info - All of the holes around the poole suction allow it to suck up large amounts of fluid without getting clogged. Perfect after irrigating the abdominal cavity.

Alias - RichUse - RetractionAdditional Info - Available in multiple sizes as well as single and double ended. This is one of the most common general surgery retractors.

Alias - RussiansUse - GraspingAdditional Info - A multi purpose pick up in most instrument sets.

Alias - Suture ScissorsUse - CuttingAdditional Info - General purpose and suture cutting scissors, normally not used on tissue.

Alias - Self RetainerUse - RetractionAdditional Info - Available with both sharp and dull jaws.

Surgical Instrument Considerations
Critical Instruments• Surgical instruments
Semi-critical instruments• Catheters, endoscope materials
Non-critical Instruments • Bedpan, BP cuff

Anesthesia
Purpose• Blocks transmission of nerve
impulses• Suppress reflexes• Promotes muscle relaxation• Controlled level of unconsciousness

Types of Anesthesia
General Anesthesia
Stages of General AnesthesiaStage 1: onset/analgesiaStage 2: excitementStage 3: operative/ surgical anesthesiaStage 4: danger

General AnesthesiaAdvantages:• Because the client is unconscious rather then awake
and anxious, respiration and cardiac function are readily regulated.
• The anesthesia can be adjusted to the length of the operation and the client’s age and physical status.
Disadvantage:• It depresses the respiratory and circulatory systems.• Some clients become more anxious about a general
anesthetic that about the surgery itself. Often this is because they fear losing the capacity to control their own bodies.

Regional Anesthesia
Methods of Delivery• Topical (surface) Anesthesia• Local Anesthesia (Infiltration)• Nerve Block• Intravenous block (Bier block)• Spinal anesthesia (Subarachnoid
block)• Epidural (Eperidural) anesthesia

Surgical Positions (most common)• Dorsal recumbent• Trendelenburg• Reverse Trendelenburg• Prone• Modified Fowler• Lithotomy• Lateral recumbent• Knee-chest• Kidney position• Jack knife (Kraske)

Layers of the Abdominal Cavity• Skin• Fascia• Camper's fascia - fatty superficial layer.• Scarpa's fascia - deep fibrous layer.
• Muscle• Rectus abdominis• External oblique muscle• Internal oblique muscle• Transverse abdominal muscle
• Fascia transversalis• Peritoneum

Most Common Abdominal Incisions• Vertical•midline, paramedian, and wide
paramedian incisions• Transverse • Pfannenstiel •Maylard • Cherney

SuturesAbsorbable sutures• Surgical gut• Plain• Chromic• Fast absorbing• Polyglactin 910 (Vicryl)• Uncoated• Coated• Polyglycolic acid (Dexon)• Poliglecaprone (Monocryl)• Polydioxanone (PDS) (Quill)• Polyglyconate (Maxon)

SuturesNon-Absorbable sutures• Natural• Silk• Cotton• Stainless-steel wire (Flexon)• Nylon (Dermalon, Surgilon)• Polypropylene (Prolene, Novafil)• Braided synthetics (Dacron, Tevdek)

POST-OPERATIVE PHASE

General post-operative complications
Immediate:• Primary hemorrhage: • Basal atelectasis: • Shock: • Low urine output/Urinary Retention:• Pneumonia:• Hypoxia:• Paralytic Ileus:

Early• Acute confusion: • Nausea and vomiting:• paralytic ileus• Fever • Secondary hemorrhage: • Pneumonia• Wound or anastomosis dehiscence• Deep vein thrombosis (DVT)• Acute urinary retention• Urinary tract infection (UTI)• Post-operative wound infection• Bowel obstruction

Late• Bowel obstruction due to fibrous
adhesions• Incisional hernia• Thrombophlebitis• Embolism • Wound evisceration and dehiscence • Severe UTI• Severe Wound Infection

Post-operative feverDays 0 to 2:• Mild fever (T <38 °C) (Common)• Tissue damage and necrosis at operation site• Hematoma• Persistent fever (T >38 °C)• Atelectasis: the collapsed lung may become
secondarily infected• Specific infections related to the surgery, e.g.
biliary infection post biliary surgery, UTI post-urological surgery
• Blood transfusion or drug reaction

Days 3-5:• Bronchopneumonia• Sepsis• Wound infection• Drip site infection or phlebitis• Abscess formation• DVT

After 5 days:• Specific complications related to
surgery, e.g. bowel anastomosis breakdown, fistula formation
After the first week• Wound infection• Distant sites of infection, e.g. UTI• DVT, pulmonary embolus (PE)
Collaborative Management/ Assessment • Assess respiration.• Examine surgical area for bleeding• Monitor vital signs.• Assess for readiness to discharge once criteria
have been met.• Respiratory System• Airway assessment• Breath sounds• Cardiovascular Assessment• Vital signs• Cardiac monitoring• Peripheral vascular assessment• Neurologic System• Cerebral functioning

THANK YOU!!