FINAL-My Neighbor is on Medicaid 5 · Medicaid is a partnership between federal and state...
33
FIVE-SESSION MY NEIGHBOR IS ON MEDICAID And it may not be the neighbor I think
Transcript of FINAL-My Neighbor is on Medicaid 5 · Medicaid is a partnership between federal and state...

FIVE-SESSION
MY NEIGHBOR
IS ON MEDICAID
And it may not be the neighbor I think

2
TABLE OF CONTENTS
I. MEDICAID INTRODUCTION………………………………………………………………….…3
II. PEOPLE WITH DISABILITIES………………………………………………………..…….……5
• What does the Bible say about our responsibility to care for People with Disabilities? – Professor Karoline Lewis
How does Medicaid support People with Disabilities?
III. OLDER ADULTS…………………………………………………………………………………….9 • What does the Bible say about our responsibility to care for Older
Adults – Professor Matthew Skinner
How does Medicaid support Older Adults?
IV. PEOPLE LIVING IN POVERTY…………………………………………………………………13
• What does the Bible say about our responsibility to care for People Living in Poverty? – Professor Rolf Jacobson
• How does Medicaid support Families Living in Poverty?
V. CHILDREN…………………………………………………………...…………………………..….17
• What does the Bible say about Responsibility to Care for Children – Professor Dirk Lange
• How does Medicaid Support Children?
VI. PER CAPITA CAPS & BLOCK GRANTS…………………………. .......................... 22
VII. VIDEO RESOURCES………………………………………………………………………………28
VIII. FACES OF MEDICAID……………………………………………………………………………29

3
I. MEDICAID INTRODUCTION
Anne Dutton, Esq. J.D., University of Minnesota
What is Medicaid? Medicaid is a partnership between federal and state governments to provide medical services and care to more than 70 million people in the United States. 1
In this federal‐state partnership, the federal government contributes funding and establishes minimum standards of coverage and care. The states also contribute funding and design healthcare programs that meet the federal standards. States can decide to provide additional services that go beyond the minimum standards and, in many cases, still receive federal funding for this expanded care. Because each state implements their own Medicaid program, there is significant variation in how Medicaid works in each state.
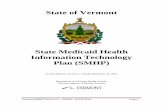
Who uses Medicaid? There are four main populations using Medicaid: children, parents, people with disabilities and older adults. Eligibility is generally limited to people that have relatively low incomes, though there are important exceptions to this requirement. The chart to the right summarizes the size

4
of each population (using 2011 enrollment numbers) compared to the cost of the services they need. 2
How do people receive care when they are “on Medicaid?” The Medicaid program does not itself provide direct services to people; rather, it distributes funding that states then use to pay for healthcare for the people who are “on Medicaid.” This means that, technically, nobody actually enrolls in the federal “Medicaid” program. Instead, they enroll in state programs that Medicaid helps fund, such as Centennial Care (in New Mexico) or the Healthy Michigan Plan—though in some states, like North Dakota, the state plan is also named “Medicaid.”
The Centers for Medicare & Medicaid Services explain that there are two main ways the state programs provide healthcare to people. 3 The majority of people receive their Medicaid‐funded healthcare through a managed care organization. These are organizations that contract with the state to provide health insurance that covers services within the organization’s network of care providers. For example, a person in New Mexico who is eligible for Medicaid will enroll in Centennial Care and choose one of the managed care organizations that contracts with the state to provide healthcare, like BlueCross BlueShield of New Mexico. Their insurance card will be issued by BlueCross and they will go to BlueCross doctors and service providers when they need care.
The second way people receive care is through “fee for service” arrangements. In these situations, people generally receive an insurance card from the state program which they then use to receive healthcare from doctors who are in the state network. After a person receives a service, the provider sends a bill directly to the state program.
Do people on Medicaid have to pay deductibles or copays? As with private insurance, most people on Medicaid‐funded programs do have to contribute to the cost of their healthcare.4 States determine the rates for premiums, deductibles, copays, or other cost‐sharing expenses. States are not allowed to impose any out‐of‐pocket costs on children or individuals living in institutions and may choose to exempt other groups or specific kinds of services from cost‐sharing.

5
II. PEOPLE WITH DISABILITIES
What Does the Bible say about our Responsibility to Care for People with Disabilities?
Professor Karoline M. Lewis
Marbury E. Anderson Chair in Biblical Preaching Luther Seminary
The Gospel of John includes a unique story about an encounter between Jesus and a man who has been unable to walk for 38 years (John 5). In our day, this is clearly a long time to be paralyzed. In the ancient world, however, this would have been a lifetime. Since the average lifespan of a Jewish male was 38‐40 years, this man has lived with his disability his entire life. For his whole existence, he has had to rely on the mercy of others. Likely blamed for his illness, as physical ailments were thought to be punishment from God for past sins committed, he had been cast aside, left alone to live a life lacking both love and relationship. And what kind of life is that?
We could easily stop reading at verse 8 and simply marvel in the fact that Jesus healed this man. We might have a similar response to Jesus’ healing of the man blind from birth (John 9). But, if we keep on reading, we find out that the healing is only the beginning.
There is a typical three‐fold pattern in the Gospel of John: a miracle is performed by Jesus, followed by a dialogue about what the miracle might mean, with then Jesus interpreting its meaning. In fact, the miracles, or signs as John calls them, are described rather briefly – it’s what the sign points to that gets the most narrative space. Reading beyond the sign in chapter 5, we come to realize that for the man ill for 38 years, this is a resurrection moment. Jesus will say, “Indeed, just as the Father raises the dead and gives them life, so also the Son gives life to whomsoever he wishes. The hour is coming, and is now here, when the dead will

6
hear the voice of the Son of God, and those who hear will live.” The paralyzed man heard the voice of Jesus, obeyed, and was healed. But not only healed, brought back from the dead, for he was basically left for dead, shamed for his illness, forced to fend for himself, abandoned, and without community. Jesus not only sees him, but heals him, and not only heals him, but gives him new life. A life he never had, never knew. A life lived in the truth that resurrection is not just an end‐of‐life promise but is now his present reality.
We are called to care for those with disabilities so that they might know life, says Jesus, even resurrected life. We may not have the power to heal those with disabilities, but we do have the power to come alongside them so that they are not alone. We may not be able to say, “stand up and walk,” but we can promise to stand with them, to show them what abundant life feels like. Jesus calls us to bring resurrection life here and now to those who have only been able to see resurrection as their future. God loves the world (John 3:16), you see, and God needs us to make that happen.

7
CHAPTER TWO: How Does Medicaid Support People with Disabilities?
Anne Dutton, Esq.
J.D., University of Minnesota
How many people with disabilities use Medicaid? More than 10 million children and adults with a disability receive health care and other supportive services funded by Medicaid, according to the Centers for Medicaid & Medicare Services. 5
Who are the people with disabilities on Medicaid? People who are living with a wide range of disabilities, including physical impairments, mental illness, and intellectual and developmental disorders, rely on Medicaid to pay for their healthcare. To qualify for Medicaid‐funded healthcare, people must generally have what the federal government calls “marked and severe functional limitations” because of their disabilities. 6
Many of the people with disabilities who use Medicaid have very low incomes. Each state determines the specific income limit and most set it somewhere
between 75 percent and 100 percent of the federal poverty level. The map above, compiled by the Kaiser Family Foundation, shows the approximate annual income

8
limit for each state in 2016. 7 However, Medicaid isn’t only for people with low incomes. In almost every state, children who have significant disabilities are eligible for Medicaid‐funded healthcare, regardless of their parents’ income or assets. Under these programs, many middle‐income families rely on Medicaid funding to care for their child in their home, rather than having to put their child into an institutional setting.
What services do people with disabilities on Medicaid receive?
People with disabilities receive the same mandatory services as other Medicaid beneficiaries (see page 15), including coverage for long‐term, institutional care. Medicaid coverage of long‐term care is particularly important for people with disabilities since it generally provides better coverage for these services than private insurers. 8
States have the option to deliver long‐term care in non‐institutional settings, an option known as home and community‐based services (HCBS). Every state has chosen to provide some form of HCBS, providing care to people living in their own homes who might otherwise have to be institutionalized. These services are tailored to the needs of people with disabilities and often include case management, personal care, and respite care.
Does Medicaid make a difference for people with disabilities? According to the Kaiser Family Foundation, it’s hard to overestimate the importance of Medicaid for people living with disabilities. 9 Though the contours of the program differ by state, Medicaid‐funded healthcare generally provides a comprehensive array of services for preventive care, primary and specialist physician visits, prescriptions, medical equipment, and long‐term care that is unmatched by private insurance companies or Medicare.
Particularly for long‐term care, Medicaid‐funded programs are virtually the only option offering the coverage that people with disabilities require. Because of Medicaid’s HCBS option, 80 percent of people with disabilities on Medicaid can afford to get the care they need without having to leave their communities to live in an institution.

9
III. OLDER ADULTS
What does the Bible say about our Responsibility to Care for Older Adults?
Matthew L. Skinner Professor of New Testament
Luther Seminary
Anyone who has ever memorized or even read the Ten Commandments already knows that the Bible emphasizes the importance of providing care for older adults. The commandment Honor your father and your mother frames the matter rather simply (Exodus 20:12; Deuteronomy 5:16).
The simplicity and force of the commandment gets lost, however, when we turn it into a tool for teaching young children and restless teens to obey what their parents tell them. For one thing, the command to honor encompasses much more than duty or obedience. It refers to generous benevolence and esteem. It implies caretaking. Furthermore, God addresses the commandment primarily to the adults among the ancient Hebrews. It summons the people of God to preserve the dignity and well‐being of the older generations in their midst. It attempts to guarantee that even the vulnerable and infirm members of society will never suffer neglect.
The motive behind the commandment exceeds simple compassion or a sense of familial obligation. As a whole, the Ten Commandments seek to promote the well‐ being of a whole community or society. Especially during times in ancient Israel’s history when an older person’s frailty, lack of mobility, or inability to work may have made them appear to be a drain on the common good, the commandment insists that the society’s overall health depends on its commitment to support those who have become more dependent on others. By contrast, when the aged are considered expendable, it signals a cynical disdain for life in general. When older adults suffer dishonor, it means that society has come to assess people’s value in terms of what they can produce. Accordingly, when the people of God

10
disregard this vital commandment, their error tends to be a symptom of even more widespread social and religious decay (see Ezekiel 22:7; Job 22:9).
Ensuring the well‐being of older adults, especially those who face financial insecurity, is a theme that appears in many parts of the Bible. Widows, many of whom lacked opportunities for significant income in ancient male‐dominated economies, frequently receive special attention. God expects them to receive care from others (see Isaiah 1:16‐17; James 1:27). Evidence indicates that the earliest Christian communities made it a priority to care for widows (see Acts 6:1‐ 4; 1 Timothy 5:3). The Gospel according to John describes Jesus, just before he dies, doing what he can to ensure that his mother will not be left alone and vulnerable (John 19:25‐27).
Obviously the cultural dynamics on display in the Bible differ significantly from how we organize ourselves in modern Western industrialized societies. Large multigenerational families dwelling together in a single household are no longer the norm. Retirement accounts, social services, and government programs allow many older people, including widows and widowers, to live securely in relative isolation from their relatives. Being older and beyond working age is not always equivalent to being at risk, as was more often the case in antiquity.
But even though the economic means by which families and a society provides care to people have changed, it does not follow that the main purpose for honoring senior generations has become outdated. The Bible consistently calls for ways of living that promote life and communal flourishing. It insists that no one can truly hope to thrive unless all members of a society are given the opportunity to do so, no matter who they are. When we treat some lives as less deserving of honor and care, we make it clear that our whole society is diseased.

11
CHAPTER THREE: How Does Medicaid Support Older Adults?
Anne Dutton, Esq.
J.D., University of Minnesota
How many older adults use Medicaid? More than 6 million older adults receive health care and other supportive services funded by Medicaid, according to the Centers for Medicare & Medicaid Services. 10
Who are the older adults using Medicaid? Medicaid‐funded programs provide healthcare to people who are older than 65 and who have a low income.
Importantly, seniors who have incomes that are generally too high to qualify for Medicaid may still be eligible if they have significant medical expenses. This includes, for example, the expense of living in a nursing home which averages more than $90,000 a year, according to the Kaiser Family Foundation. 11 Thirty‐ three states offer this option, extending coverage to seniors who have to spend so

12
much of their income on medical expenses that they are living below the poverty level. The map below shows the monthly limit to which an elderly couple must “spend down” in order to receive Medicaid‐funded services. 12 All older adults, regardless of income, are eligible for Medicare which is a separate federal program that offers health insurance to seniors and people with disabilities. Older adults who have low incomes receive both Medicare and Medicaid.
What services do older adults on Medicaid receive? Seniors on Medicaid‐funded state programs receive both the mandatory services states have to offer all recipients as well as any optional services the state provides. As for people with disabilities, the most important services for many older adults are long‐term care services. These services may be provided in an institutional setting, like a nursing home; in an assisted living facility; or in another home or community‐based setting. 13
Does Medicaid make a difference for older adults?
The importance of Medicaid for older adults is clear: according to the Kaiser Family Foundation, 63 percent of people in nursing facilities across the nation are using Medicaid‐funded programs as their primary insurer. 14 Medicaid is a critical support for our seniors, especially for those with chronic conditions that require long‐term care.
Though Medicare also plays an important role in helping our seniors stay healthy, that program focuses on acute care and can cause significant financial burden due to its coverage gaps, premiums, and co‐pays. As our population ages, Medicaid will continue to be important in helping low‐income seniors “fill in the gaps” of their Medicare coverage and provide long‐term care to all those who would otherwise be overwhelmed by the cost.

13
IV. PEOPLE LIVING IN POVERTY
What does the Bible Say about our Responsibility to Care For People Living in Poverty
Rolf A. Jacobson Professor of Old Testament and
Alvin N. Rogness Professor of Scripture, Theology, and Ministry Luther Seminary
The instructions for this Bible study were to pick one verse from Scripture about God’s care for the poor. The trouble is that picking one verse on this topic is like plucking a single petal from a dozen roses and imaging that one petal somehow captures the whole. Furthermore, picking only one verse might make it seem like God only tells us once in Scripture that God cares for the poor—and therefore we, also, are to care for the poor. Continually, throughout Scripture, God’s love for the poor is emphasized.
In the law codes of the Pentateuch, God commands that God’s people care for the poor. God commands that once every seven years, fields and orchards are to be left untouched, “so that the poor of your people may eat” (Exod 23:11). The last row of every field and a portion of ripe grapes and olives were to be left unharvested: “you shall leave them for the poor” (Lev 19:10; 23:22). Neither shall harvesters sweep up the gleanings of the grain—they were to be left for the poor. When loans were made to the poor, they were not to be charged interest (Exod 22:25). The poor were to be paid on a daily basis: “you shall pay them their wages daily before sunset, because they are poor and their livelihood depends on them” (Deut 24:14). If a poor person put up their cloak as collateral for a loan, “you shall not sleep in the garment given you as the pledge”—it might be all they have to keep them warm at night (Deut 24:12). According to one text, Israel was to devote one third of its taxes to feeding the poor and priests: “Every third year you shall bring out the full tithe of your produce for that year, and store it within your towns; the Levites . . . as well as the resident aliens, the orphans, and the widows in your towns may come and eat” (Deut 14:28‐29).

14
Examples from the Old Testament could be multiplied. Let this verse summarize God’s message: “Since there will never cease to be some in need on the earth, I therefore command you, ‘Open your hand to the poor and needy neighbor in your land’” (Deut 15:11).
God cares for the poor and commands that his people also care for the poor.
Jesus taught the same message. In his very first sermon, Jesus announced that he
had come in part “to bring good news to the poor” (Luke 4:18). He said, “Blessed are you who are poor, for yours is the Kingdom of God (6:20)”. He commanded, “When you give a banquet, invite the poor, the crippled, the lame, and the blind” (14:13). And he summed up the call to be a disciple: “sell all that you own and distribute the money to the poor.” (18:22).
Jesus cares for the poor and commands that his followers also care for the poor.
For Christians today, it is important to note that the economic and political
systems in which we live today are very different from those of either the Old Testament or the New Testament. Most of us do not have farms or orchards where we can leave the last rows and the gleanings for the poor. Most do not take or give our cloaks as collateral and most do not lend money directly to the poor.
But our God is the same God. And God still demands that we care for the poor. The challenge is to keep the spirit of the biblical laws and apply them to our new economic and political systems. The challenge is to discern together how best within our own political and economic system we can care for the poor— including the orphan, the widow, the resident alien, the crippled, the lame, the blind, and the mentally ill. In order to solve that challenge, we are going to need everybody on board.

15
CHAPTER FOUR: How does Medicaid Support Families Living in Poverty?
Anne Dutton, Esq.
J.D., University of Minnesota
How many families use Medicaid? In any given month, approximately 27 million adults receive healthcare funded by Medicaid the majority of whom are low‐income working parents, according to the Center on Budget and Policy Priorities. 15
Who are the families on Medicaid? Families on Medicaid are low‐income parents and other caretaker relatives—like grandparents, aunts, uncles, or cousins—who live with a child and have the primary responsibility for the child’s care. Each state determines the income limit for parents, detailed in the map below. 16
“FPL= federal poverty level”

16
After the Affordable Care Act, states were allowed to increase the income limit to make more parents eligible for Medicaid—the so‐called “Medicaid expansion.” According to the Kaiser Family Foundation, thirty‐two states chose to expand coverage up to 138 percent of the poverty level. 17 Nineteen states chose not to expand coverage and while the income limits in these states vary, the median limit is 44 percent of the poverty level.
Using a family of three as an example, in a state that expanded coverage a family making less than $40,840/year in 2017 will qualify for Medicaid. In the average state that did not expand coverage, the same family would only qualify for Medicaid when they made less than $8,985/year.
What services do families on Medicaid receive?
The Medicaid and Children’s Health Insurance Program (CHIP) Payment and Access Commission explains that the federal government requires states to provide certain basic services to receive Medicaid funding. 18 This includes services like physician visits, inpatient and outpatient hospital services, laboratory and x‐ray services, and nursing facility services.
However, as states design their Medicaid‐funded program they also have significant flexibility to provide additional, optional services such as prescription coverage, vision and dental care, physical therapy, or services from a clinic. As a result of this flexibility, the services funded by Medicaid vary quite a bit from state to state.
Does Medicaid make a difference for families in poverty? Medicaid‐funded healthcare plays an important role in keeping low‐income parents healthy and able to care for their children. Kaiser reports that adults who are on Medicaid are significantly more likely to access preventative/primary care and significantly less likely to have unmet healthcare needs when compared to uninsured adults.19 Without Medicaid, out‐of‐pocket spending on healthcare for these adults would be four times greater on average, causing significantly more financial strain for families already living on low incomes. 20

17
V. CHILDREN
What does the Bible Say about our Responsibility to Care For Children?
Dirk G. Lange Fredrik A. Schiotz Chair of Mission
Professor of Worship Luther Seminary
As the parents bring children to Jesus to be blessed, Jesus welcomes them all (Mark 10:13‐16). He makes me no distinction between children or value judgment on their potential: they are all welcomed and blessed. In bestowing the blessing and making them heirs of the Kingdom, he recognizes them as partners, even as equals. They are sent out with this blessing as messengers are sent out. We find the children again as Jesus enters Jerusalem, shortly before his trial and execution. They are shouting Hosanna! Jesus said to the angry adults, “Yes’; have you never read’, [Psalm 8]:‘Out of the mouths of infants and nursing babies you have prepared praise for yourself’?” (Matthew 21:16‐17).
Today, in a society that values success, which is usually defined in terms of wealth, power, and prestige, children are often over‐looked. And if not over‐ looked, they are merely considered in terms of their potential or for the signs of giftedness they might display. Music lessons, art, sports activities, even volunteer work in senior living complexes or other social agencies are all meant to encourage that potential and make for a stellar college application. Children are shaped by “grown‐up” values from a very young age on (at least those children who come from financially stable homes).
Certainly, in the United States and in other industrialized countries, forced child labor has been left behind and considerable advance has been made in proclaiming the rights of children (see the resolutions on child rights adopted by the UN Human Rights Council). As a society, we proclaim and defend those rights – for example, the right of all children to education – but seldom do we as a

18
society provide the infrastructure that makes for sustainable learning, especially for those living in poverty or those children / families dealing with illness and disabilities. Children, many children, remain superfluous in comparison to other political, social, and economic agendas. They can be easily disregarded, quickly ignored.
Aware of that danger, the Human Rights Council upholds as a fundamental right, “the right of the child to the enjoyment of the highest attainable standard of health” (A/HRC/RES/22/32). A vibrant and free society is one in which all (including children) have the right to the same opportunities (and therefore possibility of success). This right to pursue happiness, however, is dependent on the right to a healthy life. Health is a key condition for the pursuit of happiness and other goals. Yet so many children live in economic conditions that prevent them from ever having routine medical check‐ups, immunizations, prescriptions, vision, dental and other care, including emergency care if needed. They are subject to illness and even death (spiritual and physical death) because of this lack of routine medical care. Pope Francis has named this situation an economy that kills.
Prof. Skinner (in the article on care of older adults) notes that, as a whole, “the Ten Commandments seek to promote the well‐being of a whole community or society.” This well‐being of the whole community is attained when all members have access to the same opportunities that society values and offers, including health care. The Fourth Commandment also calls forth a responsibility from all members of society. The Commandment is not simply about obedience to parents (or authority) but assumes that those parents and authorities will fully live‐up to their responsibility. Martin Luther underlines the dual nature of obedience (obedience/responsibility) in his commentary on this commandment in the Large Catechism: “it would also be well to preach to parents on the nature of their responsibility, how they should treat those whom they have been appointed to rule.” The parental office, the rule of authorities (government, politicians), is not exercised for the simple fulfillment of “their own pleasure, amusement,” and ideological fancies. They are called upon to provide an environment in which all peoples, especially children, can live, learn and thrive.

19
A free and thriving society welcomes, embraces, and treats all children with the same respect and honor. It tends to the health of all children so that they may flourish, offering all of them the highest attainable standards of health care.

20
CHAPTER FIVE: How does Medicaid Support Children?
Anne Dutton, Esq.
J.D., University of Minnesota
How many kids use Medicaid?
The Center for Medicaid and Children’s Health Insurance Program (CHIP) Services reports that children are the largest group of people on Medicaid‐funded programs, representing 51 percent of all participants. In November 2016, this meant a total of 35 million kids—or 40 percent of all children in the nation— depended on Medicaid for their healthcare. 21
Who are the children on Medicaid? Medicaid requires states to provide coverage to all children whose families have incomes below 138 percent of the federal poverty line. 22
A related federal program, CHIP offers additional support to states that cover children who are above 138 percent of the poverty line. In 2017, all but two states provide coverage to children up to at least 200 percent of the federal poverty line. For a family of three, that means that children in families making less than
“FPL= federal poverty level”

21
$40,840/year will qualify for coverage funded by Medicaid/CHIP. Some states cover even more kids by setting a higher income limit, detailed in the map below. 23
Since the Affordable Care Act, foster children who were on Medicaid‐funded programs when they “aged out” of the foster care system by turning eighteen can now continue to receive coverage until their 26th birthday. 24 Children in families with higher incomes who have a disability also rely on Medicaid, discussed on page 7.
What services do kids on Medicaid receive?
Medicaid requires states to cover a comprehensive set of services for children, called Early and Periodic Screening, Diagnostic and Treatment Services (EPSDT). EPSDT includes preventative health services, vision and dental care, hospital visits, mental health care, and a wide array of other screening and treatments for physical and mental health conditions. 25
Does Medicaid make a difference for kids?
Yes! The Centers for Medicaid & Medicare Services note that the EPSDT services described above are often more robust than the services Medicaid funds for adults as they are designed to detect and treat health issues early, setting kids up for a lifetime of better health. 26 To that end, the Kaiser Family Foundation has documented how access to Medicaid‐funded healthcare in childhood is associated with declines in infant, child, and teen mortality, reduced rates of disability, and lower rates of hospitalization and ER usage as adults. 27 Beyond the health benefits, children accessing Medicaid show improved educational attainment and higher earnings in adulthood.

22
VI. PER CAPITA CAPS & BLOCK GRANTS
A nne Dutton, Esq.
J.D., University of Minnesota
How do the states and federal government currently share Medicaid costs? The cost of providing healthcare through Medicaid is split between the states and the federal government. The exact division varies by state but the federal government always covers at least half the cost while in some states it pays significantly more. For example, the Centers for Medicare & Medicaid Services report that New Jersey and the federal government are splitting the cost of New Jersey’s program evenly in 2017 while in West Virginia the federal government is paying for more than 70 percent of the total cost.28
Currently, Medicaid guarantees coverage to all who qualify. Since coverage is guaranteed there are no limits on the number of people who can enroll.
What does it mean when politicians talk about imposing per capita caps on Medicaid? The Kaiser Family Foundation explains that proposals to create per capita caps are proposals to change the way the partnerships between the federal and state governments work.29 Rather than the federal government contributing a percentage of the total cost of the healthcare needed by people in a given state, it would establish an initial level of funding for each state, essentially calculated as (1) the number of people enrolled; multiplied by (2) the current average per‐person cost of healthcare in the state—though the exact calculation depends on the proposal.
In subsequent years, the amount of funding for a state would increase or decrease as people either enroll or leave the program. The per‐person cost would continue to be based on the initial level of funding with increases to account for inflation. Since per capita caps are designed to save the federal

23
government money, this annual increase would be at a rate fixed below the anticipated growth in healthcare costs, according to Kaiser.30 Accordingly, the cuts in federal funding would start small and increase exponentially as the per capita cap fell further behind the growing cost of care.
In March 2017, a proposal was introduced in the House to repeal the Medicaid expansion and require states to switch to either per capita caps or block grant funding. An amended version of this proposal was passed by the House in May 2017. The Congressional Budget Office estimates that the initial version of this proposal would cut federal Medicaid spending by approximately $880 billion in its first ten years, a reduction of approximately 25 percent by 2026. 31
Concern over these initial cuts is compounded by the proposal’s unprecedented restructuring of Medicaid itself. Per capita caps erode Medicaid's guarantee to fund healthcare for those in need. As a result, many current participants are likely to lose coverage while those who require assistance in the future may not be able to count on Medicaid when they need it most. When considered with the revised funding structure that is based not on the actual healthcare needs of older adults or people with disabilities but on a restrictive formula that cannot respond to the cost of changing needs in the future the full impact of the proposal likely would only be knowable in the years to come.
How would a per capita cap affect people on Medicaid? With only a predetermined average amount of funding per beneficiary provided to states, there will be pressure on states to limit the amount of services provided to beneficiaries.
The amount of services people on Medicaid need varies significantly between different populations. Kaiser calculates that, on average, children on Medicaid‐ funded programs need about $2,500 of care annually compared to seniors who need $17,500 of care—to say nothing of the significant variations in cost of care within these groups.32 Accordingly, limits on services would likely have a disproportionate impact on people with higher costs of care, primarily seniors and people with disabilities.33
To give one example, in Arkansas these two populations comprise approximately a third of all people receiving Medicaid‐funded healthcare—a total of over 230,000 people, according to the AARP.34 As Medicaid is frequently the only option for the long‐term care these groups require, a per capita cap that reduces

24
services would potentially leave many without access to the care they need. Additionally, as states look for ways to reduce costs in response to limited federal funding they may pass the expense along to the people using Medicaid‐funded healthcare, requiring them to pay more for their healthcare than they already do.35
How would a per capita cap affect the states? As the amount of federal support decreases, states will face a difficult choice: they will either have to shoulder a disproportionate share of the total cost or find ways to reduce the cost by limiting their citizens’ access to coverage and care. According to the U.S. Government Accountability Office, per capita caps may force states to limit eligibility and/or reduce services.36
Per capita caps would not affect all states equally, according to the Kaiser Family Foundation.37 States that currently operate Medicaid programs, with lower per‐person spending totals, will have a lower per capita payment. This would include, for example, states like Nevada and Indiana, which have some of the lowest per‐person costs in the nation. 38
Per capita caps would also be harder on states like Arizona that are experiencing a large increase in their senior population.39 Because the per capita system permanently ties a state’s payment to its current per‐person cost, Medicaid funding will not be able to adjust down the line for a future population with more expensive healthcare needs.
What does it mean when politicians talk about “block granting” Medicaid?
A block grant is another proposal to reduce federal spending on Medicaid. Kaiser explains that, as with per capita caps, each state would get a lump sum of money from the federal government but the amount would be determined by the current level of federal Medicaid spending in the state.40 As with per capita caps, the amount of each state block grant would increase at a fixed rate set below the projected increase in healthcare costs in order to create federal savings.
How would a block grant system affect the states? The Kaiser Family Foundation predicts that cost‐saving changes in a block grant might include narrowing or eliminating eligibility categories and/or placing limits on the number of people who can enroll. States could also decide to reduce

25
services that are available.41
Kaiser notes that the impact of block granting would be felt differently by each state as the amount of each block grant would be based on the current level of federal Medicaid spending in the state.42 This means that states that spend less on Medicaid and those that currently have a more equal partnership with the federal government—like Iowa, where the cost of Medicaid is split 56/44 or North Dakota where the split is 50/50—would have a lower block grant rate in the new system.
More generally, as both the block grant and per capita cap proposals are explicitly designed to reduce federal payments, states will have to contend with significant losses in revenue.43 The AARP notes that Ohio, for example, received more than $15 billion in federal Medicaid funding in 2015, an amount that would be greatly reduced in a block grant system.44
How would a block grant system affect people on Medicaid? Depending on how a state revises its Medicaid‐funded programs in response to block grants, people who already are receiving Medicaid‐funded healthcare are likely to see their services reduced. Others who are applying for the first time may have to wait to get coverage. Some of those who currently rely on Medicaid‐ funded programs may no longer qualify for coverage.
How does this all relate to a potential repeal of the Affordable Care Act? Proposals to add a per capita cap or block grant Medicaid are generally distinct from proposals to repeal the ACA. At their core, per capita caps and block grants are changes to the federal‐state partnership that implements Medicaid while the changes to Medicaid in the ACA were primarily changes to eligibility guidelines.
However, a repeal of the ACA may exacerbate the challenges states face in a per capita or block grant system as a repeal would likely further reduce federal funding to states. The Minnesota government estimates, for example, that the combination of ACA repeal and a switch to a block grant system would create an estimated $2.2 billion shortfall in Minnesota’s budget in the first year, which would grow to an annual $8 billion shortfall within ten years of the changes.45

26
Endnote citations: 1 Medicaid & CHIP: Strengthening Coverage, Improving Health, (Centers for Medicare & Medicaid Services, Jan. 2017), https://www.medicaid.gov/medicaid/program‐information/downloads/accomplishments‐report.pdf. 2 Chart from: Julia Paradise, Medicaid Moving Forward, (The Henry J. Kaiser Family Foundation, March 9, 2015), http://kff.org/health‐reform/issue‐brief/medicaid‐moving‐forward/. 3 Financing & Reimbursement, (Centers for Medicare & Medicaid Services), https://www.medicaid.gov/medicaid/financing‐and‐reimbursement/. 4 Cost Sharing Out‐of‐Pocket Costs, (Centers for Medicare & Medicaid Services), https://www.medicaid.gov/medicaid/cost‐sharing/out‐of‐pocket‐costs/index.html. 5 Medicaid & CHIP: Strengthening Coverage, Improving Health, supra note 1. 6 Supplemental Security Income (SSI) Eligibility Requirements, (U.S. Social Security Administration, 2016), https://www.ssa.gov/ssi/text‐eligibility‐ussi.htm. 7 Map from: Kaiser Family Foundation State Health Facts. Data Source: Molly O'Malley Watts, Elizabeth Cornachione, and MaryBeth Musumeci, Medicaid Financial Eligibility for Seniors and People with Disabilities in 2015, (The Henry J. Kaiser Family Foundation, February 2016). 8 Julia Paradise, Barbara Lyons, Diane Rowland, Medicaid at 50, (The Henry J. Kaiser Family Foundation, May 6, 2015), http://kff.org/medicaid/report/medicaid‐at‐50/. 9 Medicaid at 50, supra note 8. 10 Medicaid & CHIP: Strengthening Coverage, Improving Health, supra note 1. 11 Medicaid at 50, supra note 8. 12 Map from: Kaiser Family Foundation State Health Facts, supra note 7. 13 Medicaid at 50, supra note 8. 14 Charlene Harrington, Helen Carrillo, and Rachel Garfield, Nursing Facilities, Staffing, Residents and Facility Deficiencies, 2009 Through 2014, (The Henry J. Kaiser Family Foundation, Aug. 4, 2015), http://kff.org/medicaid/report/nursing‐facilities‐staffing‐residents‐and‐facility‐deficiencies‐2009‐through‐2014/.
15 Policy Basics: Introduction to Medicaid, (Center on Budget and Policy Priorities, Aug. 16, 2016), http://www.cbpp.org/research/health/policy‐basics‐introduction‐to‐medicaid. 16 Map from: Where are States Today? Medicaid and CHIP Eligibility Levels for Children, Pregnant Women, and Adults, (The Henry J. Kaiser Family Foundation, 2017). 17 Where are States Today?, supra note 16. 18 Mandatory & Optional Benefits, (Medicaid & CHIP Access and Payment Commission, 2017), https://www.macpac.gov/subtopic/mandatory‐and‐optional‐benefits/. 19 Julia Paradise and Rachel Garfield, What is Medicaid’s Impact on Access to Care, Health Outcomes, and Quality
of Care? Setting the Record Straight on the Evidence, (The Henry J. Kaiser Family Foundation, Aug. 2, 2013), http://kff.org/report‐section/what‐is‐medicaids‐impact‐on‐access‐to‐care‐health‐outcomes‐and‐quality‐of‐care‐setting‐the‐record‐straight‐on‐the‐evidence‐issue‐brief/. 20 What is Medicaid’s Impact on Access to Care, Health Outcomes, and Quality of Care?, supra note 19. 21 November 2016 Medicaid and CHIP Enrollment Data Highlights, (Centers for Medicare & Medicaid Services, 2017), https://www.medicaid.gov/medicaid/program‐information/medicaid‐and‐chip‐enrollment‐data/report‐ highlights/child‐and‐chip‐enrollment/index.html. 22 Robin Rudowitz, Samantha Artiga, Rachel Arguello, Children’s Health Coverage: Medicaid, CHIP, and the ACA, (The Henry J. Kaiser Family Foundation, March 26, 2014), http://kff.org/health‐reform/issue‐brief/childrens‐ health‐coverage‐medicaid‐chip‐and‐the‐aca/. 23 Where are States Today?, supra note 16. 24 Tricia Brooks, Joe Touschner, Samantha Artiga, Jessica Stephens, and Alexandra Gates, Modern Era Medicaid: Findings from a 50‐State Survey of Eligibility, Enrollment, Renewal, and Cost‐Sharing Policies in Medicaid and CHIP as of January 2015, (The Henry J. Kaiser Family Foundation, Jan. 20, 2015), http://kff.org/report‐section/modern‐ era‐medicaid‐medicaid‐and‐chip‐eligibility/. 25 EPSDT – A Guide for States: Coverage in the Medicaid Benefit for Children and Adolescents (Centers for Medicare & Medicaid Services, June 2014), https://www.medicaid.gov/medicaid/benefits/epsdt/index.html.

27
26 EPSDT – A Guide for States, supra note 24. 27 Medicaid Pocket Primer, (The Henry J. Kaiser Family Foundation, Jan. 3, 2017), http://kff.org/medicaid/fact‐ sheet/medicaid‐pocket‐primer/. 28 Robin Rudowitz, 5 Key Questions: Medicaid Block Grants and Per Capita Caps (The Henry J. Kaiser Family Foundation, Jan. 31, 2017), http://kff.org/medicaid/issue‐brief/5‐key‐questions‐medicaid‐block‐grants‐per‐capita‐ caps/. 29 5 Key Questions: Medicaid Block Grants and Per Capita Caps, supra note 28. 30 Shefali Luthra, Everything You Need to Know About Block Grants–The Heart of the GOP’s Plan, (Kaiser Health News, Jan. 24, 2017), http://khn.org/news/block‐grants‐medicaid‐faq/. 31 American Health Care Act Cost Estimate, (Congressional Budget Office, March 13, 2017), https://www.cbo.gov/publication/52486. 32 Chart from: Edwin Park, House GOP Medicaid Provision Would Shift $370 Billion in Costs to States Over Decade, (Center on Budget and Policy Priorities, March 7, 2017), http://www.cbpp.org/blog/house‐gop‐medicaid‐ provisions‐would‐shift‐370‐billion‐in‐costs‐to‐states‐over‐decade. 33 Kaiser Family Foundation State Health Facts. Data Source: Kaiser Commission on Medicaid and the Uninsured and Urban Institute estimates based on data from FY 2011 MSIS and CMS‐64 reports. 34 5 Key Questions: Medicaid Block Grants and Per Capita Caps, supra note 28. 35 Brendan Flinn, Impact of Block Grants and Per Capita Caps on Medicaid Enrollees, (AARP Public Policy Institute, March 2017), http://www.aarp.org/ppi/info‐2017/impact‐of‐block‐grants‐and‐per‐capita‐caps‐on‐medicaid‐ enrollees.html. 36 Robin Rudowitz, Rachel Garfield, and Katherine Young, Overview of Medicaid Per Capita Cap Proposals, (The Henry J. Kaiser Family Foundation, June 22, 2016), http://kff.org/report‐section/overview‐of‐medicaid‐per‐capita‐ cap‐proposals‐issue‐brief/. 37 Medicaid: Key Policy and Data Considerations for Designing a Per Capita Cap on Federal Funding (U.S. Gov’t Accountability Office, Aug. 2016), http://www.gao.gov/assets/680/678968.pdf. 38 5 Key Questions: Medicaid Block Grants and Per Capita Caps, supra note 28.
39 Data Note: Variation in Per Enrollee Medicaid Spending Across States, (The Henry J. Kaiser Family Foundation, Feb. 23, 2017), http://kff.org/medicaid/issue‐brief/data‐note‐variation‐in‐per‐enrollee‐medicaid‐spending‐across‐ states/. 40 Haeyoun Park, Republicans’ Changes to Medicaid Could Have Larger Impact Than Their Changes to Obamacare, (The New York Times, March 7, 2017), https://www.nytimes.com/interactive/2017/03/07/us/politics/medicaid‐ reform‐impact‐on‐states.html. 41 5 Key Questions: Medicaid Block Grants and Per Capita Caps, supra note 28. 42 Everything You Need to Know About Block Grants, supra note 30. 43 Everything You Need to Know About Block Grants, supra note 30. 44 Edwin Park, Medicaid Block Grant Would Slash Federal Funding, Shift Costs to States, and Leave Millions More Uninsured, (Center on Budget and Policy Priorities, Nov. 30, 2016), http://www.cbpp.org/research/health/medicaid‐block‐grant‐would‐slash‐federal‐funding‐shift‐costs‐to‐states‐ and‐leave. 45 Impact of Block Grants and Per Capita Caps on Medicaid Enrollees, supra note 35. 46 Block Grants or Per Capita Caps & Minnesota’s Medicaid Program, (MN Dep’t of Human Services, Jan. 24, 2017), https://mn.gov/dhs/assets/block‐grants‐or‐per‐capita‐caps_tcm1053‐275143.pdF

VII. VIDEO RESOURCES
Brief Infographic from The Henry J. Kaiser Family Foundation on Block Grant or Per Capita Cap
Kaiser Infographic
Medicaid Pocket Primer Article from The Henry J. Kaiser Family Foundation
Medicaid Pocket Primer Article
28

https://lssmn.wistia.com/medias/w15lqmw6a2 https://lssmn.wistia.com/medias/ou0mfhdsrv
https://lssmn.wistia.com/medias/iimxjom3sg https://lssmn.wistia.com/medias/pfewjispt2
https://lssmn.wistia.com/medias/li64wulry2 https://lssmn.wistia.com/medias/fyjkscf5ml
https://lssmn.wistia.com/medias/nlymb5q0ep https://lssmn.wistia.com/medias/ht3xp2e2ey
VIII. FACES OF MEDICAID
29

30
Anne Dutton
Esquire
J.D., University of Minnesota
Anne holds a Bachelor’s Degree in Social Work from St. Olaf College and
a Juris Doctor from the University of Minnesota Law School. She is
currently working toward a Master’s Degree in Social Work at the
University of Minnesota.
She has worked for Lutheran Immigration and Refugee Service’s policy
office, as a student director in the Federal Immigration Litigation Clinic,
and she is currently working as an intern in Lutheran Social Service of
Minnesota’s Advocacy Office. Starting in the fall of 2017, Anne will join
the staff of the Center for Gender & Refugee Studies in San Francisco as
an Equal Justice Works Fellow, focusing on children’s asylum claims.
Karoline Lewis Marbury E. Anderson Chair in Biblical Preaching Luther Seminary
The Rev. Dr. Karoline M. Lewis (www.karolinelewis.com)
holds the Alvin N. Rogness Chair of Homiletics at Luther
Seminary in St. Paul, MN, and is ordained in the Evangelical
Lutheran Church in America. She is a regularly featured
preacher and presenter at the Festival of Homiletics.
Her newest book, SHE: Five Keys To Unlock the Power of Women in Ministry, is available in March 2016. She is the author of “John: Fortress Biblical Preaching Commentary Series,” the introduction and study notes for the Gospel of John in The Lutheran Study Bible, co‐author of New Proclamation: Year B, 2009, as well as articles in The Christian Century, Feasting on the Word, Lutheran Forum, Word and World, Abingdon Preaching Annual, Currents in Theology and Mission, and Odyssey Network's ON Scripture. She is a contributing writer for WorkingPreacher.org, the author of the site’s weekly column, Dear Working Preacher, and co‐host of the site’s weekly podcast Sermon Brainwave.
CONTRIBUTOR BIOGRAPHIES

31
Matthew L. Skinner Professor of New Testament Luther Seminary
Matthew L. Skinner is Professor of New Testament at Luther Seminary. He joined the seminary’s faculty in 2002, having earned degrees from Princeton Theological Seminary and Brown University. He has conducted advanced research at the Center of Theological Inquiry in Princeton, NJ, as a member‐in‐residence and a writing fellow.
Most of Skinner’s teaching and research focuses on the Gospels, the Acts of the Apostles, the cultural realities displayed in these writings, and the books’ ongoing theological relevance. His newest book, Intrusive God, Disruptive Gospel: Encountering the Divine in the Book of Acts (Brazos Press), explores how the Acts of the Apostles informs our thinking about the character of God, the challenges of faith, and the life of the church. He contributes to various print and online resources for scholars, church leaders, and laypeople interested in the Bible’s connections to faith and life. Skinner is an ordained teaching elder in the Presbyterian Church (USA).
Rolf Jacobson Professor of Old Testament and Alvin N. Rogness Professor of Scripture, Theology and Ministry Luther Seminary
Rolf Jacobson joined the Luther Seminary faculty as assistant professor of Old Testament in July 2003. Prior to joining the seminary, he taught at Augsburg College, Minneapolis, as an assistant professor of religion.
Jacobson earned his bachelor's degree from the University of St. Thomas, St. Paul, MN, in 1987. He holds a master of divinity degree from Luther Seminary (1991) and a doctor of philosophy degree from Princeton Theological Seminary, Princeton, NJ (2000).
His teaching interests include the Psalms, Old Testament prophets, biblical poetry, biblical theology, and biblical narrative. He emphasizes that the purpose of a biblical text is not just for preaching or teaching, although these are crucial functions. He says the Scriptures must also be used in pastoral care, personal spiritual growth, and for the shaping of Christian mission and theology. In addition, it can also function as a catalyst for change and growth within a congregation.

32
Ordained in 1991, Jacobson served for five years as associate pastor of Como Park Lutheran Church in St. Paul before continuing his education at Princeton Theological Seminary. At Princeton, he was the assistant editor for “Theology Today” and “The Princeton Seminary Bulletin.” He also served as a teaching fellow.
Jacobson is an in‐demand speaker and author, who produces theological and biblical scholarship for both the church and the academic guild. He recently served as editor of Crazy Talk: A Not‐So‐Stuffy Dictionary of Theological Terms, whose authors included three recent Luther Seminary graduates. His articles have appeared in Word and World, Theology Today, Interpretation, Teaching Theology and Religion, and in many collections of scholarly essays. With Kelly Fryer, he wrote the “No Experience Necessary” Bible studies. He has been a contributor to Augsburg Fortress's Handbook series (The Lutheran Handbook, The Christian Handbook, etc.), Workingpreacher.org, Lectionary Homiletics, and the like. His credits also include appearances in many video curricula, including The Lutheran Course.
Dirk G. Lange
Associate Professor of Worship
Luther Seminary
Dirk G. Lange’s ministerial experience has covered a wide
spectrum of activities, but all under one umbrella: liturgy in
the lives of people. As a brother of Taizé, he was engaged
with the prayer and songs of Taizé. His book Trauma Recalled:
Liturgy, Disruption, Theology (Fortress Press, 2009) explores
Luther’s sacramental theology and begins rewriting theology
through the lens of the liturgy. He is currently Associate
Professor of Worship and Associate Dean of Graduate
Theological Education at Luther Seminary, St. Paul, MN, and
has written extensively on topics in liturgical theology and ecumenism. He is from Winnipeg,
Canada.

33
REVIEWER
Jon Christianson, Ph.D.
University of Minnesota
Jon Christianson received his Ph.D. in economics from the
University of Wisconsin ‐ Madison. He is on the faculty of the
Division of Health Policy and Management, School of Public
Health, University of Minnesota and has held the James A.
Hamilton Chair in Health Policy and Management since 1998.
Professor Christianson has authored ten books and over 200
journal articles and book chapters. He has received the
Annual Research Award of the National Institute for Health
Care Management and chaired AcademyHealth’s annual
research meeting.
Professor Christianson’s recent research has focused on
measurement and reporting of provider performance,
physician payment arrangements, and health care purchasers. He regularly teaches graduate
courses on the health care system and on health care purchasers and health insurers.
From 1998‐2000, Professor Christianson served on the Institute of Medicine committee that
produced the report To Err Is Human. More recently, he was a member of the IOM’s
Geographic Adjustment Factors in Medicare Payment Committee and served six years on the
IOM’s Board on Health Care Services which oversees all IOM health service projects. He
currently is Vice‐Chair of the Medicare Payment Advisory Commission, which advises Congress
on Medicare, and is a member of the advisory board of the Medica Research Institute.