Final internship report #3 - · PDF fileInternship report 5 Introduction Description of the...
33
European School of Physiotherapy Assignment #7 Clinical internship report Internship 3(Period; 06/05/2013-07/08/2013) Intern: Yagmur Hazir (500544685) Institution: Baskent University Hospital Clinical instructor: M. D. Physiatrist Mehmet Adam Clinical instructor signature: Clinical Supervisor: Pim Ranzijn Clinical supervisor signature: Intern signature: Date of submission: 02/08/2013 Date of review: Internship Report Date: 02-08-2013 Class: LP11-31 Professor: Pim Ranzijn
Transcript of Final internship report #3 - · PDF fileInternship report 5 Introduction Description of the...

European School of Physiotherapy
Assignment #7 Clinical internship report Internship 3(Period; 06/05/2013-07/08/2013) Intern: Yagmur Hazir (500544685) Institution: Baskent University Hospital Clinical instructor: M. D. Physiatrist Mehmet Adam Clinical instructor signature: Clinical Supervisor: Pim Ranzijn Clinical supervisor signature: Intern signature: Date of submission: 02/08/2013 Date of review:
Internship Report Date: 02-08-2013 Class: LP11-31 Professor: Pim Ranzijn

Internship report
2
© 2009 Hogeschool van Amsterdam. All right reserved
Last update: August 4, 2013
Internship report
3
Table of Contents
ACKNOWLEDGEMENTS 4
INTRODUCTION 5
DESCRIPTION OF THE SITE 5
PATIENT RELATED ITEMS: 5
TREATMENTS USED: 6
EXPERIENCE DURING THE CLINICAL INTERNSHIP: 7
DESCRIPTION OF THE HEALTH CARE SYSTEM 8
PERSONAL LEARNING OBJECTIVES: 9
EVALUATION OF LEARNING OBJECTIVES: 10
PATIENT CATEGORY REPORTS 12
PATIENT CATEGORY REPORT #1 (ROTATOR CUFF SYNDROME) 12
DESCRIPTION OF THE DISORDER: 12
EPIDEMIOLOGICAL DATA OF THE DISORDER: 12
INDICATION FOR PHYSIOTHERAPY: 12
PATIENT CATEGORY REPORT #2 CEREBRAL PALSY (CP) 17
DESCRIPTION OF THE DISORDER: 17
EPIDEMIOLOGICAL DATA OF THIS DISORDER: 17
INDICATION FOR PHYSIOTHERAPY: 18
EXTENSIVE PATIENT REPORT 21
SPINAL CORD INJURY (SCI) (PARAPLEGIA) 21
MOTIVATION FOR PATIENT SELECTION: 21
DESCRIPTION OF THE DISORDER, EPIDEMIOLOGY, PREVALENCE AND INCIDENCE 21
ADMINISTRATIVE DATA OF THE PATIENT: 22
HOUR JUSTIFICATION 31
GENERAL CONCLUSIONS 31
REFERENCES 32

Internship report
4
Acknowledgements
I would like to thank my CIs, Physiatrist Mehmet Adam and Physiotherapist Ozlem Sayilir
Pektas for accepting me into their department. Furthermore, I would like to thank to the M.D.
and upcoming Physiatrist Emine Ece Yilmaz for sharing with me her valuable knowledge.
Finally, a special thanks to the Physiotherapist Akin Aydemir for sharing with me his valuable
knowledge and making the last 6 weeks of my internship unforgettable.

Internship report
5
Introduction
Description of the site
My internship place is located in the city called “Adana”, where the population is over
one million. The city is highly developed and can provide lots of working opportunities in
Physical therapy. Not only there are physical therapy departments in private and public
hospitals but also there are private physical therapy and rehabilitation clinics throughout the
city.
Baskent University Hospitals branched out throughout the country. The hospital is
an outpatient clinic and has most of the medical professional fields, including Physical
therapy. The Physical Therapy department works closely with Neurology, Rheumatology,
Orthopedics, Pediatrics. There are 6 physiotherapists work, and one works as a head of
the physiotherapy department. Besides there are 4 physiatrists working with
physiotherapists. The physiatrists take patient history, do assessment and give therapy,
however the physiotherapists apply the therapy that physiatrists approved on. There is
also 1 physical modality technician. The therapy includes hot and cold modalities,
electrotherapy and therapeutic exercises. There are separate rooms depending on
the treatment type. In the physical department, there are neck and back traction
rooms with traction machines, short wave, isokinetic and balance machines which are
used for research and therapy, hydrotherapy, EMG, hand rehabilitation, splint-orthoses,
4 physiatrists, 1 physiotherapists, child and orthopedic rehabilitation rooms available.
Patient related items:
There are more than 40 patients who are treated by physiotherapists every
day. The rehabilitation are only indicated for the patients who need and willing to join the
rehabilitation. The category below, shows what type of patients I have been able to
see so far. The rehabilitation is done by me independently.
Orthopedics:
• Supraspinatus tendinitis
Internship report
6
• Meniscus
• Anterior cruciate ligament (ACL)
• Muscle strains
• Frozen shoulder
• Medial epicondylitis
• Rotator cuff syndrome
• Fractures
• Osteoarthritis
• Osteoporosis
Neurology:
• Spondylosis, spondylolesthesis, radiculopathy
• Ankylosing spondylitis
• Cerebrovascular accident (CVA)
• SCI (tetraplegia, paraplegia)
• Cerebral palsy (CP)
• Polyneuropathy, mononeuropathy
• Multiple sclerosis (MS)
• Carpal tunnel syndrome
• Scoliosis
Cardiopulmonary:
• Chronic obstructive pulmonary disorder (COPD)
Other classifications
• Rheumatoid arthritis
• Scar tissue contractures
Above the mentioned patient categories, the majority of the patients who are treated are
neurological patients. They are treated by physiotherapists after a consultation by the
physiatrists. The four physiatrists may check their patients after every 10 or 5 sessions. It
can be even more frequently than it is expected.
Treatments used:
The most used intervention is electrotherapy. To be more specific, the most used
Internship report
7
currents are TENS, Russian, Galvanic, Diadynamics and interferential. The time of
the therapy varies from 30 minutes to an hour according to the patients’ needs.
Besides Ultrasound is also applied around six minutes. There is also an application of
Infrared and laser. The electrotherapy may be applied with Hot pack around the injury
site depending on the type of current or what patient needs. Therapeutic exercises are
ADL training, ROM, muscle re-education, strengthening, releasing the muscle spasm
etc. Massage can be applied as a soft tissue release in the rehabilitation. Besides the
therapeutic exercises done by the physiotherapists in the hospital, homework
exercises are given as well.
Experience during the clinical internship:
Experience in taking Patient History:
I was able to take the patient history for diagnosis in this internship site despite the
regulations between the hospital and the health institutions. I have had two clinical instructors
who are a physiatrist and a physiotherapist. I have observed a lot of different type of patients.
While I was working with the physiotherapists I was able to take patient history by asking
permission from specific patients and from the physiotherapists. The working opportunity
under the supervision of my CI was the most beneficial time for me because I felt
independent and believed that it will be more useful for me in the future. For this time, my
strength was to include all the relevant medical data from them.
Experience in Assessment:
Just like in patient history, I was also able to perform assessment for diagnosis and
intervention. I also have seen differential diagnosis from the physiatrists. I have observed the
usage of shortened version of the assessment scales with a determined clinical reasoning.
Experience in Treatment:
The one and only intervention for a long period of time was therapy for me, either under
supervision or independent. Mostly, I was able to treat the patient category below:
• Neurology (%40)
• Orthopedics (%40)
• Pediatrics (20%)
Therapy was my strongest part from overall internship period.

Internship report
8
Working hours
Monday to Friday:
From 8.30am to 6pm.
Description of the health care system
In Turkey, healthcare is coordinated by the government, as the ministry of health.
The ministry is responsible for providing health care and organizing health care
services for patients. Furthermore, they are obliged to operate public hospitals and
supervise private hospitals and clinics. They check the usage and price of the drugs. The
quality of the private hospitals is higher than the public ones. The reason is the lack of
investments on health care in all over the country. The biomedical equipment are not
well developed in public hospitals, however in private hospitals the equipment are
supplied better in order to provide better consultation and intervention for patients.
The hospitals and the medical doctors work especially in the cities because of the
highly dense population to get profit, although in rural areas there are insufficient health
care services. There are four major organizations as social insurance for citizens. These
are social insurance institutions, pension fund for civil service, social security institution
for the self-employed and green card users. Should the patients need to get any medical
consultation, they have to claim that they are registered any of the social
organizations as mentioned above in order not to pay or pay partially. However in private
hospitals patients have to pay a certain amount as an agreement between private
hospitals and the public organizations.
The most common patients who need rehabilitation are CVA patients in my internship
site. The common reasons for this disease are traffic or any trauma related
accidents, hypertension, thrombus formation, embolism etc. These reasons cause
ischemic stroke or hemorrhages. They follow the rehabilitation for weeks with the
help of a physiotherapist under the consultation of physiatrists. The rehabilitation
period depends on the progress of the patients.
In my internship site, the physiotherapists are only in close contact with physiatrists.
They receive orders from them to apply therapy. In the ‘Order Paper’, only the diagnosis
is written in these papers, however; the physiotherapists can have access to the
patient records. Physiotherapists are charged interchangably everyday to give

Internship report
9
homework exercises to the patients who do not need rehabilitation in the hospital.
There are ready made papers, with pictures, are given as homework exercises to the
patients. The physiatrists are in close contact with orthopedists, neurologists and other
necessary specialists.
In the country itself the physiotherapists are not allowed to open any rehabilitation
clinic or physical therapy center by themselves. They work in the rehab centers or
hospitals with the physiatrists.
My CI is a physiatrist but I work with physiotherapists in every working hour. We are
eight interns now in the hospital but this number may change after certain amount of
weeks. We are allowed to directly touch the patients and give therapy
independently with or without supervision.
Personal learning objectives:
SMART goals
1.
S Rehabilitation for 2 pediatric cerebral palsy patients independently
M 2 of these patients will be checked by my CI and given to me for rehab
A Acceptance of the intake of CP patients by the hospital and my CI
R To gain experience in rehabilitation of CP patients
T In 3 months
2.
S Using Brunnstrom Fugl Meyer assessment test and Berg balance scale on
1 stroke patient
M This patient will be checked and compared with the assessment of my CI
A Acceptance of the intake of stroke patients by the hospital and my
CI. Comparison of the results after the assessments
R To gain experience in using these tests in stroke patients
T In 3 months
3.
Internship report
10
S Usage of Biodex Isokinetic machine on 1 indicated orthopedics patient
M By my CI who will assess that indicated orthopedics patient
A Acceptance of the intake of the patient by the hospital and my CI
R To gain experience using an isokinetic machine
T In 3 months
Evaluation of learning objectives:
1st Learning objective:
During my 1st and 2nd internship, I could not have so many pediatric patients. Cerebral palsy
is a growing disorder amongst children, therefore; I thought i should be able to see and treat
these patients in this category. I have treated many CP patients (more than 5) and observed
at least 10 patients. They all had different interests and intelligence in movement. I have
understood that patient specificity should be a part of an ongoing investigation.
I have accomplished this goal more than sufficient for this internship.
2nd Learning objective:
Even though I have had so many neurological patients during my 1st internship, I have never
felt confident enough to make a diagnosis in the level of impairment. I have realized that my
entire school life education for neurology was not enough, therefore; I would like to have
more experience during my internships. I was very willing to see the differentiation in the
level of impairments. To be able to achive this a very good assessment skills should have
been accomplished. In this process, I have gained practical skills in not only using Fugl-
Meyer and Berg balance test but also other neurological tests with a modified approach.
I have accomplished this goal more than sufficient for this internship.
3rd Learning objective:
I have decided to acquire this goal after I came back to the internship site. When I saw the
Biodex machine, I immediately showed an interest in using this isokinetic machine because I
knew that isokinetic exercises are known as one of the best techiques according to the
evidence. My CI told me that we could use the Biodex machine on patients together. She
gave some basic manual instructions to use and she showed me how to adjust the machine

Internship report
11
for the patients. We have only used this machine on quadriceps muscles, however; this
machine could be used for other joints as well (i.e. shoulder). I have accomplished an extra
skill to apply into practice when I have the opportunity to see this type of machine in the
future. I have accomplished this goal more than sufficient for this internship.
Expectations
During this internship, one of my expectations is to see the differences in assessment
and treatment approaches towards patients between the private and public
hospitals. The internship place where I will be going is a private hospital and I am
expecting differences in approaches towards patients. For example, in public hospitals
in Turkey, the number of patients can be quite high, therefore; the physiotherapists
may spend less time for treating each patient. Secondly, the apparatus can be different
in quality and quantity than the public hospitals. I would like to see the variations in
treating these patients. I do not have high expectations in joining the assessment
sessions with the physiatrists. Turkey is one of the countries where the physiotherapists
are not allowed to assess the patients primarily. I will request for supervision from
physiatrists yet, I might not be able to get this opportunity.

Internship report
12
Patient Category Reports Patient Category Report #1 (Rotator Cuff Syndrome)
Description of the disorder:
Figure 1: Rotator cuff tear
Muscle pain, around the shoulder joint
area is a common complaint. Rotator cuff
problems are the most common problems
in the shoulder region (Lewis 2009).
Patients mostly complain about pain for
the movements that involve overhead shoulder activities that may usually cause
impairments, limitations in the activities of
daily living and diminished muscle strength
(Lewis 2009). Rotator cuff consists of four
muscles and their tendons that are
involved in stabilizing the shoulder joint.
These four muscles are supraspinatus,
infraspinatus, teres minor and
subscapularis. These four muscles
together with the attachments cover the
humeral head. Musculotendinous injury to
these muscles causes a rotator cuff
syndrome.
Epidemiological data of the disorder:
Tempelhof et al. (1999) tried to find out the age-related prevalence of the asymptomatic
rotator cuff syndrome. It was reported that out of 411 volunteers, %23 of them had rotator
cuff disorder. The patients were divided into age related four groups. Each group had
different ranges of age. Out of these four groups, in the over 80 years old group, %51 of
them had rotator cuff disorders. According to this study, it is more likely to get a rotator cuff
syndrome with an increasing age. Another study found out the same results that rotator cuff
syndrome mostly occurs over the age of 65 with a degenerative cause (Lewis 2009). There
was no information found considering this disorder, occuring in different race, ethnicity etc.
Indication for physiotherapy:
As mentioned above, the patients can have limitations, pain and weakness in the rotator cuff
muscles. Physiotherapy plays an important part in treatment and improving the quality of life.

Internship report
13
The physiotherapeutic approach should be optimal for each specific patient. The older and
the younger generation may have this disorder due to different causes, therefore; the
treatment should also focus on the mechanism of injury. The aim in physiotherapeutic
approach should be improving strength, range of motion and decreasing pain that is specific
to that patient (Kamkar et al. 1993). Not only the physiotherapsist-supervised exercises is
given, but also home exercises are combined in this treatment process. Even though, more
research should be done, it was reported that there was no statistically significant effect in
physiotherapist-supervised exercises other than home exercises (Andersen et al. 1999). This
may be an indication of decreasing the physiotherapists visits to benefit the health care
expenses.
In my internship clinic, the protocol can be divided as postoperative and preoperative care.
These two protocols can be patient specific as well. The protocol is followed by the
physiotherapists under the supervision of physiatrists and orthopedic surgeons. The most
used intervention is electrotherapy, progressive resistant exercises and stretching exercises
for possible limited range of motion.
Patient 1: F.S.
The patient is female and 68 years old. Medication: Gabapentin 300 mg 3*1
She is diabetic. Diagnosis: Rotator Cuff syndrome
Patient history: The patient is a housewife. She only works at home, doing household chores. She did not
have any trauma or any surgery. She came to the clinic with pain in her right shoulder. She
also had complaint in her left arm. She had been having this pain for 3-4 months. During the
night, she had been experiencing pain a bit more in her right shoulder. She claimed that she
also had numbness in her right shoulder. The patient said that she also had problems with
getting up from the bed. The household activities were not easy to accomplish anymore. One
of the most complaints were overhead activities like getting a glass or a plate from the
cupboard.
She was upset about not being able to work at home and especially cooking. She said that
her daughter in law helped her to cook. She felt dependent on activities that she wanted to
do it alone. The psychologial load was more than her carriability. She wanted to get rid of
pain as soon as possible.
Assessment: Neer test: (+) Hawkins-Kennedy: (+)
ICF injury classification: d630-d649
Specific: d630,d640, d649 (preparing
meals, doing household tasks)

Internship report
14
Right shoulder ROM:
Abduction: Painful arch between 70º to 180º (active and passive)
Flexion: 180º(active and passive) experiencing pain
External Rotation: 90˚(active and passive) experiencing pain
Therapy: The 15 sessions of treatment is indicated for this patient.
Electrotherapy: 20min TENS with 20min right shoulder Hot pack application. After the
application of TENS and hotpack, 10 min of Ultrasound is applied.
Physiotherapy-supervised and home based exercises: Theraband strengthening exercises in
external and internal rotation, extension, abduction and flexion. 2 sets of 10 reps 1kg
dumbbell exercises.
Patient 2: S.K.
The patient is 42 years old female. Medication: None
Diagnosis: Rotator cuff syndrome
Patient history: The patient works voluntarily in a disabled children care. She is an active person and willing
to help these disabled kids. She did not have any trauma or a surgery.
She came to the clinic with complaints in the right shoulder and pain in her upper back and
chest. It was hard for her to lift the kids from the wheelchair to the floor. She had been having
this shoulder pain for a year and a half. Although she did not have any difficulty in breathing.
The pain had gotten worse since last week. The patient was experiencing night pain. There
was no loss in apetite and weight. The patient claimed to have complaints in burping and
bloating, therefore she had a consultation from a pulmonary specialist. The scintigraphy was
taken and according to the medical doctor there were no abnormal signs. This patient was
willing to get better. Her load was lower than her carriability.
Assessment: Neer test: (+) Speed test: (-) Hawkins-Kennedy: (+)
Painful fibrosis in trapezius and rhomboids muscles.
Right shoulder ROM:
Abduction: Painful arch between 70º to 180º (active and passive)
Flexion: 180º(active and passive) experiencing pain
External Rotation: 90˚(active and passive) experiencing pain
ICF injury classification: d430-d449
Specific: d440 (lifting,carrying)

Internship report
15
Therapy: The 15 sessions of treatment is indicated for this patient.
Electrotherapy: 20min TENS with 20min right shoulder Hot pack application. After the
application of TENS and hotpack, 10 min of Ultrasound is applied.
Physiotherapy-supervised and home based exercises: Theraband strengthening exercises in
external and internal rotation, extension, abduction and flexion. 2 sets of 10 reps with 1kg
and 2kg dumbbell exercises. Massage was applied for 10 min for the taut bands in trapezius
and rhomboids. Swiss ball exercises on the wall.
Patient 3: I.O.
The patient is a 55 years old female. Medication: Rantudil forte 60mg, Lansor 15mg
Diagnosis: Rotator cuff syndrome MRI results: Type II Acromion
Patient history: The patient works as a farmer. She picks up the farm products from the field. She works for 8
hours in a day, including 2 hours break in between, and she picks up the farm products from
the field She described her job as an intense physiological job. The patient came to the clinic
with complaint in her right shoulder, arm and upper back pain. She had been having these
pain for 3 days. It started with a sudden abnormal movement. The patient did not have any
neck pain. She had been experiencing difficulties in picking up and lifting the products
because of the pain. She was unable to use her right shoulder. This patient was depressed.
Her load was higher than her carriability.
Assessment: Neer test: (+) Hawkins-Kennedy: (+)
Right shoulder ROM:
Abduction, flexion, extension: Full ROM in active and passive, painful ROM
External Rotation: 90˚(active and passive) experiencing pain at the end range of motion
Therapy: The 15 sessions of treatment is indicated for this patient.
Electrotherapy: 20min TENS with 20min right shoulder Hot pack application. After the
application of TENS and hotpack, 10 min of Ultrasound is applied.
Physiotherapy-supervised and home based exercises: Theraband strengthening exercises in
external and internal rotation, extension, abduction and flexion. 2 sets of 10 reps with 1kg
and 2kg dumbbell exercises.
ICF injury classification: d430-d449
Specific: d440 (lifting,carrying)

Internship report
16
This protocol was proven to be successful especially in decreasing pain. The sessions were
clear for the patients after the first session. The feedback was given to educate the patients
about their disorders. The treatment sessions were patient specific and evidence based,
therefore; it was expected to get better results in the certain amount of time. TENS was
applied for pain and three of my patients felt relieved after this stimulation. The exercises
gave benefit for long term. The patients continued to do their exercises after 3 weeks of
treatment in the hospital.
My opinion about these protocol is to be more patient specific, therefore; the patients can
adjust to their work sooner. The acute injuries can have different tissue modelling and may
require different treatment strategies. The patients can have flexion synergy because of
experiencing pain in their shoulders. This flexion synergy may cause tightness in the
shoulder muscles (i.e pectoralis major or latissimus dorsi), therefore; the structures around
the shoulder joint should be examined carefully. Stretching these muscles may diminish the
limited ROM.
I have gained great experiences in seeing the rotator cuff patients. I have seen acute and
chronic rotator cuff syndrome patients try to analyze the inter-individual differences and
similarities. For example, the three patients experienced night pain. My next step is to
research the validity and the reliability of the impingement tests for rotator cuff syndrome in
acute and chronic rotator cuff patients.

Internship report
17
Patient Category Report #2 Cerebral Palsy (CP)
Description of the disorder:
Cerebral Palsy is a pediatric disorder that
occurs when there is a damage to the
cerebral motor cortex in the central
nervous system (Koman et al. 2004). The
infants in pregnancy and not older than 2
year olds may have a lesion in their part of
central nervous system (CNS). This
disorder can be classified as the location
of the lesion, the level of deformity and
distribution of the abnormality. Brainstem
lesion, spasticity and hemiplegia can be
given as an example for the classification
of this disorder (Koman et al. 2004). The
symptoms may appear bilateral or
unilateral depending on the site of the
lesion. These symptoms may present itself
as spasticity, rigidity, muscle weakness,
chorea, athetosis, ataxia, dystonia,
abnormal gait etc. (Koman et al. 2004).
The development of movements in a
cerebral palsy child is slower than a
normal child. (Koman et al. 2004). This
disorder is not a progressive fatal disorder,
although; the disabilities and impairments
are long lasting and life hardening.
Figure 2: Child with CP (Koman et. 2004)
Epidemiological data of this disorder:
Cerebral palsy is a life devastating disorder that causes an irreversible damage to the
movement development. The factors that link to this disorder may vary. Fetal infection,
labouring more than 4 hours, vaginal bleeding before giving birth, anoxic birth can be given
as examples to the linked factors (Koman et al. 2004). The children who have
hydracephalus, severe quadriparesis, refractory seizures, have shorter lifespan and a high
mortality, although; the children, who do not have a comorbid condition live a longer life with
an effective care as the general population (Koman et al. 2004).
The frequency and the appearence of this disorder in the worldwide is not very well
documented, therefore; the incidence and prevalence of this disorder is still not precise
enough to make statistics (Koman et al. 2004). On the other hand, one of the few countries,

Internship report
18
for almost two decades an increased number of cerebral palsy has been reported in the USA
due to a better documentation than other countries. (Koman et al. 2004).
Indication for physiotherapy:
The clinical assessment determine the type of treatment. As it is mentioned above, the
abnormal motor development is the most common clinical findings in this disorder. There are
multiple management strategies that are goal-oriented and patient specific in cerebral palsy.
The severity of the condition and the age of children are also important factors for an optimal
treatment. Physiotherapy is indicated for these patients to improve the quality of life.
Botulinium toxin injections and orthotics can be beneficial together with physiotherapy.
Strength training, stretching exercises, patient specific exercise therapy and gait training are
the most common physiotherapeutic treatments. Hippotherapy is proven to be effective in
improving the trunk control, balance, weight bearing, gait and gross motor functioning in
patients with bilateral spasticity (Kwon et al. 2011).
In my clinic, the protocol is patient specific. The most used intervention is gait training,
stretching, strengthening, balance exercises, home program. Electrotherapy can be applied
as well when it is indicated. The clinical assessment is done by the physiatrists and the
therapy is determined by the physiotherapists.
Patient 1: N.K.
The patient is female and 4 years old. Diagnosis: Spastic diplegia CP
Medication: none Medical history: None, close relative marriage
Patient history: The patient was the first child from a 21 years old mother. After birth, she stayed in incubator
for 12 days. She does not have hepatitis or any disease. According to her mother, when she
started walking she had inverted feet. Her communication with other children and adults is
normal. At the age of 2, she was diagnosed as CP.
The child is very cooperative and she likes playing with baby dolls and balls. Her carriability
is higher than her load, therefore; it is expected that therapy sessions will be beneficial.
Assessment: Her mental condition is fine. She is cooperative, speaks well. The patient does not have a
dysmorphic feature, organomegaly or murmur in her heart.
Tardieu scale: R & L (lower ext) : 2/-30 V1, V2 DTR lower extremity: Hyperreflexive
Patrick’s test: (-) Clonus: (+)
ICF injury classification: d450-d469
Specific: d450 (walking)

Internship report
19
Gait analysis: Achillies tendon tightness, spastic gait with bilateral inverted feet
Therapy: The therapy includes variable neurophysical exercises for both legs, sitting, getting up from a
bed, standing still, walking exercises on parallel bar and stretching exercises for tight plantar
flexors.
Patient 2: S.Y.
The patient is female and 9 years old. Diagnosis: Spastic diplegia CP
Medical history: Prenatal Hydracephalus Medication: Botulinium toxin injection
Patient History: When the patient was 2 months old, she was operated for 4 times due to hydrocephaly and
the shunt was inserted. According to her mother, she has no problems with understanding,
talking and communication, although; her success is lower than other kids at school. She has
problems with her motor development.
The child likes to play so often and she gets bored and tired so easily while doing her
exercises. She does not want to do her exercises because she thinks they are tiring and
boring. Her carriability is lower than her load.
Assessment: Her mental condition is fine. She is cooperative, speaks well.
Tardieu scale: R & L (lower ext): 1/-70 V1, V2 DTR lower extremity: Hyperreflexive
Patrick’s test: (-) Clonus: (+)
Gait analysis: Achillies tendon tightness, bilateral spastic gait on tiptoes and with flexed
knees.
Therapy: The therapy includes variable neurophysical exercises for both legs, sitting, getting up from a
bed, standing still, walking exercises on parallel bar and stretching exercises for tight plantar
flexors.
Patient 3: M.Y.S.
The patient is male and 2 years old. Diagnosis: Right hemiplegia CP
Medical history: None Medication: None
ICF injury classification: d450-d469
Specific: d450 (walking)
Internship report
20
Patient History: According to his mother, the patient does not use his hand enough. He is using an
orthopedic shoes to correct his externally rotated leg pattern. He understand his mother and
what happens in his surroundings. He likes to play with balls, although; he can not use his
right hand efficiently to grab the big things. Due to his age, his load is higher than his
carriability.
Assessment:
Right shoulder ROM: full active and passive Right elbow ROM: full active and passive except supination.
Right hand ROM: flexors of the wrist and fingers, extension
Partial spherical, lateral and pinch grip
Patrick’s test: (-) Clonus: (-)
DTR lower and upper: Hyperreflexive No spasticity
Gait analysis: Slight externally rotated leg
Therapy: The therapy includes variable neurophysical exercises, occupational therapy for his hand,
walking exercises, and postural correction and strengthening the arms and legs.
This protocol is proven to be successful depending on the patient. Children need a different
communication style for therapy. When a different approach is achieved towards each
patient, and a communication between the physiotherapist and the child is successful, this
protocol is proven to be beneficial. Each child had different coping style with his condition
and his surroundings, therefore: the therapeutic approach was patient specific.
What I have experienced for these type of patients was different than other adult patients.
They require too much attention and a different approach. Children also have different
mental and motor development and that makes the physiotherapeutic approach more
complicated than others. I have seen more than these patients and I believe that each
patient should also be consulted by the pediatrician because some of the children were not
consulted from a pediatrician. The clinical findings from a physiatrist and pediatrician may
differ, therefore; it should be integrated.
Even though I am not interested in working as a physiotherapist who is specialized in
pediatrics, I am glad that I have gained great experiences in treating these type of patients. I
have seen inter-individual differences and learned more about the classification of this
disorder.
ICF injury classification: d450-d469
Specific: d450 (walking)
Internship report
21
Extensive Patient Report
Spinal cord injury (SCI) (Paraplegia)
Motivation For patient selection:
I have chosen this pathology to work with because of subjective and objective reasons.
Objectively, I have had an acute complete tetraplegic patient in my first internship and could
not feel comfortable afterwards for treating these type of patients because of his acute
condition. When I started my internship in this clinic she was already treated by the other
physiotherapist. I talked with her about her condition and how she improved over the course
of the treatment. She was very enthusiastic and ambitious about her condition and she was
willing to get better. Naturally, this has encouraged me to work with her. I find myself very
lucky to see this kind of SCI patient.
My internship site and the physical therapy department received a lot of neurological patients
especially CVA and SCI patients. I have experienced in treating a lot of neurological patients,
however; I have never thought i have seen enough. Because I believe that these type of
patients may have a lot of symptoms that are important to see. Before I came to his
internship place, I have made an SCI patient report by myself and the more I went in detail,
the more I found interesting things in this pathology. Classifying these patients was not easy
to present and intervene. Even though there are certain symptoms the patient is expected to
experience, according to evidence the neuroplasticity may reveal otherwise. I have seen that
these patients have to improve a lot to function independently and because of this I find this
as a challange to get the patient back to his/her partial independent life. Each patient has
different approaches to his/her condition. To be able to overcome with psychological
disturbances and physical disabilities the patient need to understand the recovery process
and accept the certain consequences.
Description of the disorder, epidemiology, prevalence and incidence
Spinal cord injuries are long lasting, life hardening disorders for individuals everywhere in the
world. The injuries occur when there is a compressive, penetrating or distracted damage to
the spinal cord. The spine is a part of the central nervous system, and in case there is a
damage, the neural and neuromuscular response get affected. Not only there are trauma
involved injuries, but also non-traumatic spinal cord diseases, affecting the spinal cord (i.e.
metastatic tumors, spina bifida). Assessment has to include motor, sensory, cranial or
autonomic nervous system, gait, coordination and mental status of the patients. Therefore;
Internship report
22
the level and the extent of the injury which determines the classification of this disorder
should be precise and carefully monitored.
It has been reported that in every million, 15-40 acute SCI occurs in UK (Winter et al. 2011).
The cause for this injuries involve traffic accidents, violence, falls, sports etc. In these
population young males (20-40 years old) get more effected than females (4:1 ratio) (Winter
et al. 2011). The prevalence of the non-traumatic SCI has not been reported due to lack of
documentation, different reasons etc. (Winter et al. 2011). In the USA, approximately 183-
230 000 people live with traumatic SCI (McDonald et al. 2002).
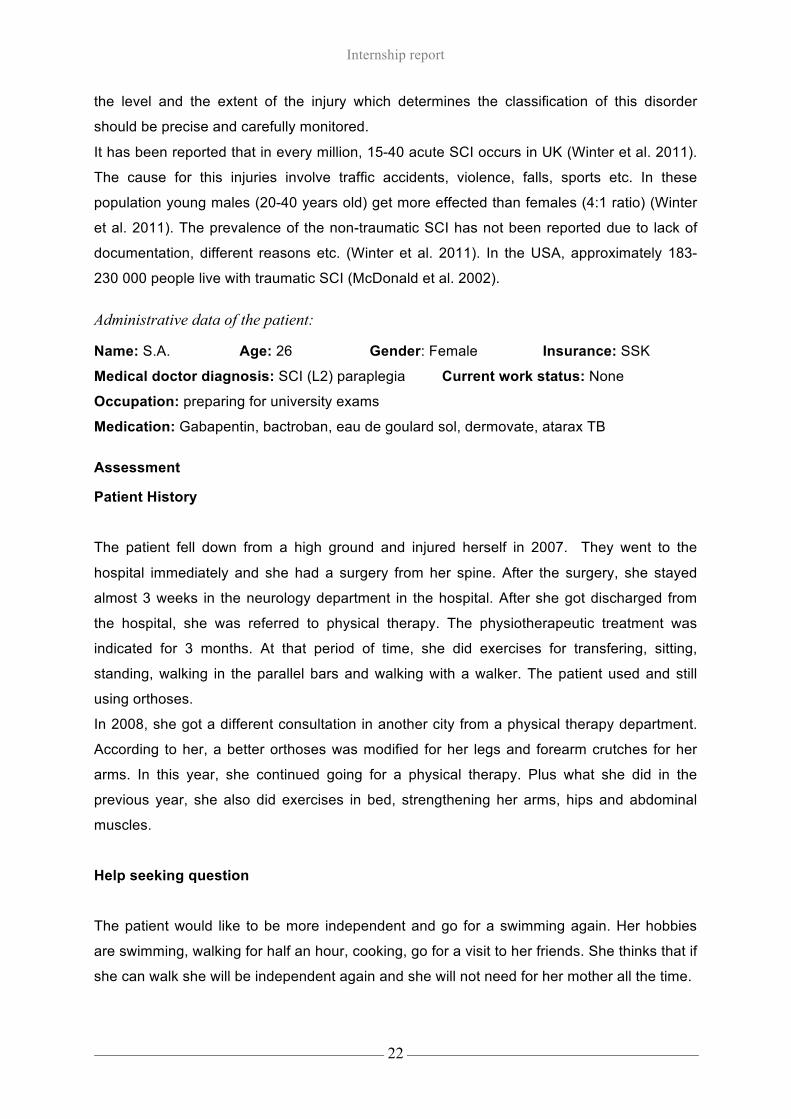
Administrative data of the patient:
Name: S.A. Age: 26 Gender: Female Insurance: SSK
Medical doctor diagnosis: SCI (L2) paraplegia Current work status: None
Occupation: preparing for university exams
Medication: Gabapentin, bactroban, eau de goulard sol, dermovate, atarax TB
Assessment
Patient History
The patient fell down from a high ground and injured herself in 2007. They went to the
hospital immediately and she had a surgery from her spine. After the surgery, she stayed
almost 3 weeks in the neurology department in the hospital. After she got discharged from
the hospital, she was referred to physical therapy. The physiotherapeutic treatment was
indicated for 3 months. At that period of time, she did exercises for transfering, sitting,
standing, walking in the parallel bars and walking with a walker. The patient used and still
using orthoses.
In 2008, she got a different consultation in another city from a physical therapy department.
According to her, a better orthoses was modified for her legs and forearm crutches for her
arms. In this year, she continued going for a physical therapy. Plus what she did in the
previous year, she also did exercises in bed, strengthening her arms, hips and abdominal
muscles.
Help seeking question
The patient would like to be more independent and go for a swimming again. Her hobbies
are swimming, walking for half an hour, cooking, go for a visit to her friends. She thinks that if
she can walk she will be independent again and she will not need for her mother all the time.
Internship report
23
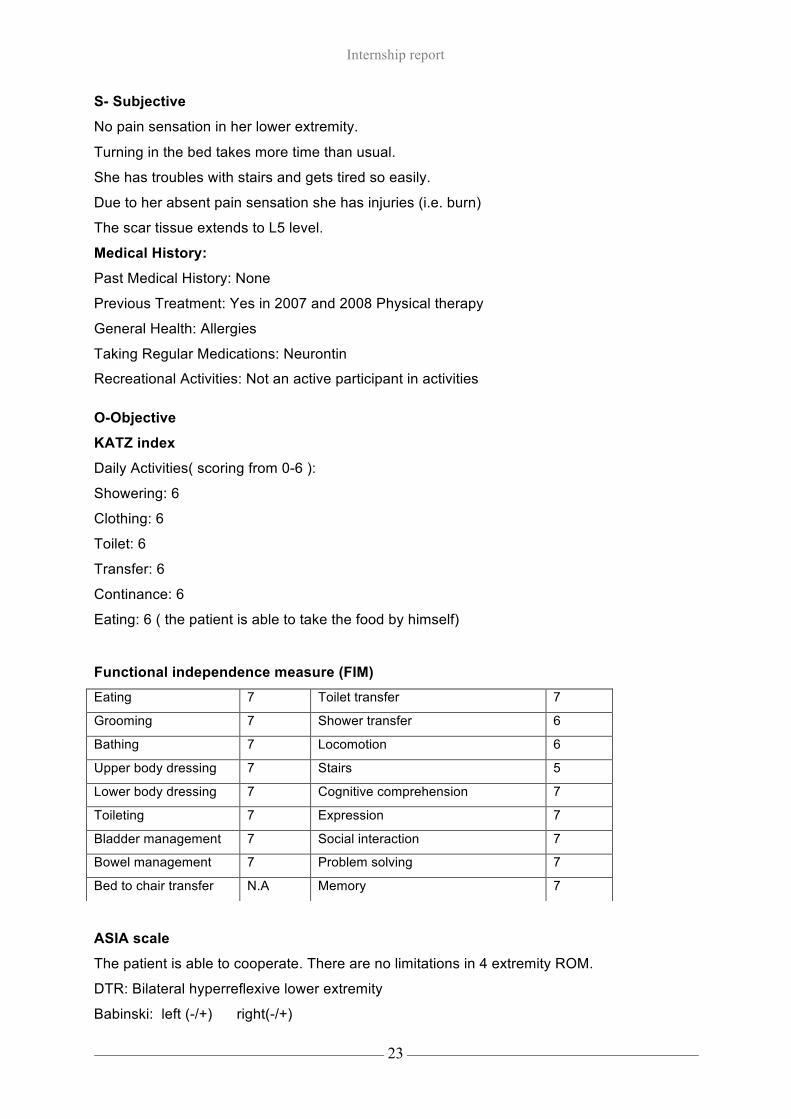
S- Subjective
No pain sensation in her lower extremity.
Turning in the bed takes more time than usual.
She has troubles with stairs and gets tired so easily.
Due to her absent pain sensation she has injuries (i.e. burn)
The scar tissue extends to L5 level.
Medical History:
Past Medical History: None
Previous Treatment: Yes in 2007 and 2008 Physical therapy
General Health: Allergies
Taking Regular Medications: Neurontin
Recreational Activities: Not an active participant in activities
O-Objective
KATZ index
Daily Activities( scoring from 0-6 ):
Showering: 6
Clothing: 6
Toilet: 6
Transfer: 6
Continance: 6
Eating: 6 ( the patient is able to take the food by himself)
Functional independence measure (FIM)
ASIA scale
The patient is able to cooperate. There are no limitations in 4 extremity ROM.
DTR: Bilateral hyperreflexive lower extremity
Babinski: left (-/+) right(-/+)
Eating 7 Toilet transfer 7
Grooming 7 Shower transfer 6
Bathing 7 Locomotion 6
Upper body dressing 7 Stairs 5
Lower body dressing 7 Cognitive comprehension 7
Toileting 7 Expression 7
Bladder management 7 Social interaction 7
Bowel management 7 Problem solving 7
Bed to chair transfer N.A Memory 7
Internship report
24
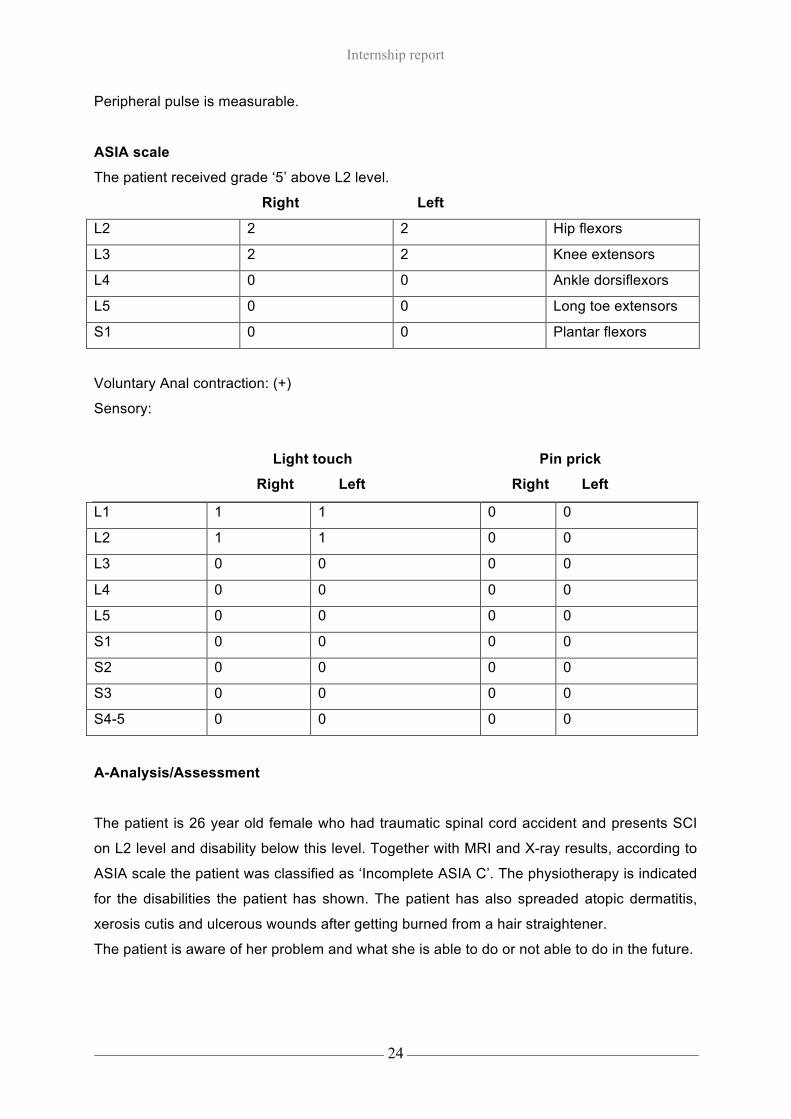
Peripheral pulse is measurable.
ASIA scale
The patient received grade ‘5’ above L2 level.
Right Left
L2 2 2 Hip flexors
L3 2 2 Knee extensors
L4 0 0 Ankle dorsiflexors
L5 0 0 Long toe extensors
S1 0 0 Plantar flexors
Voluntary Anal contraction: (+)
Sensory:
Light touch Pin prick
Right Left Right Left
L1 1 1 0 0
L2 1 1 0 0
L3 0 0 0 0
L4 0 0 0 0
L5 0 0 0 0
S1 0 0 0 0
S2 0 0 0 0
S3 0 0 0 0
S4-5 0 0 0 0
A-Analysis/Assessment
The patient is 26 year old female who had traumatic spinal cord accident and presents SCI
on L2 level and disability below this level. Together with MRI and X-ray results, according to
ASIA scale the patient was classified as ‘Incomplete ASIA C’. The physiotherapy is indicated
for the disabilities the patient has shown. The patient has also spreaded atopic dermatitis,
xerosis cutis and ulcerous wounds after getting burned from a hair straightener.
The patient is aware of her problem and what she is able to do or not able to do in the future.

Internship report
25
P-Plan
Treatment goals Short term:
• Teaching transfering from shower to standing or to similar activities.
• Teaching how to walk through the stairs.
• Prevention of getting injured (i.e. burn) by giving feedback and strategies.
Reasoning: The patient is having problems with transfering herself from getting into shower
to standing or the other way around. This may be a big burden for the patient because it
might take time. Walking through the stairs is important for her because she has stairs at
home. Ulcerous injuries might be a long lasting problem and should be prevented by giving
feedback and reminders.
SMART short term goals
1.
S Teaching transfering from shower to standing or to similar activities.
M Functional independence measure (FIM), mobility section
A The examples will be shown and guided by the therapist to the patient
R Getting independent is important for the patient to socialize with her environment
T 2-4 weeks
2.
S Teaching how to walk through the stairs
M Functional independence measure (FIM), locomotion section
A The examples will be shown and guided by the therapist to the patient
R Walking to the stairs is important because she has stairs at home
T 2-4 weeks
3.
S Prevention of ulcers, giving feedback and education
M Getting info from the patient about her environment to create a safe environment and
answering the questions from the patient about her condition
A Giving brochures and electronic reminder to make her use while she is in a
dangerous environment
R Prevention of ulcers is important not to cause a secondary complication while doing
the therapy
T 3 weeks
Internship report
26
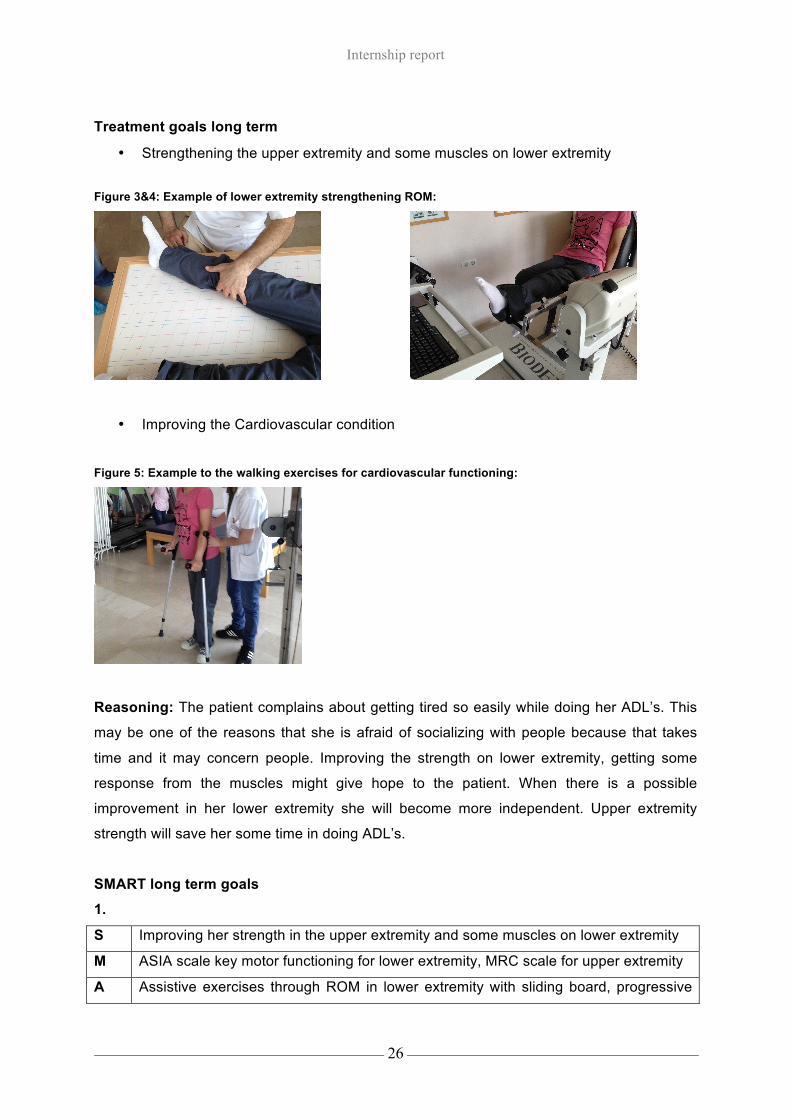
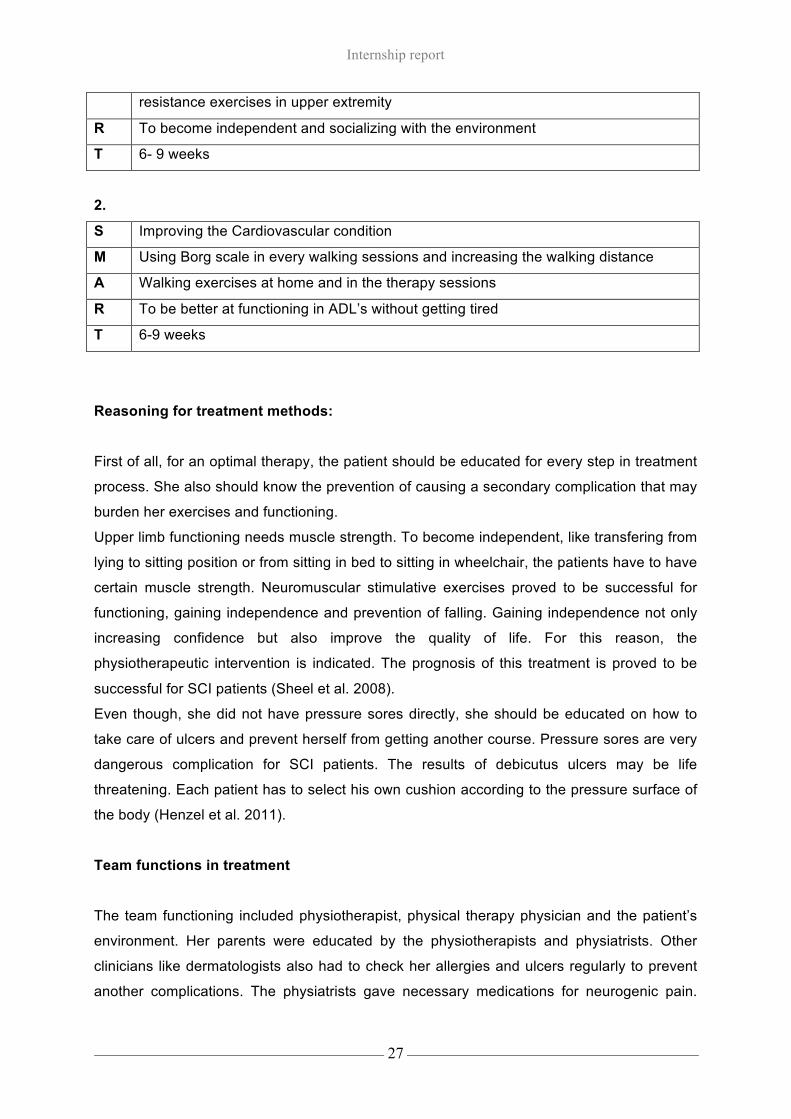
Treatment goals long term
• Strengthening the upper extremity and some muscles on lower extremity Figure 3&4: Example of lower extremity strengthening ROM:
• Improving the Cardiovascular condition
Figure 5: Example to the walking exercises for cardiovascular functioning:
Reasoning: The patient complains about getting tired so easily while doing her ADL’s. This
may be one of the reasons that she is afraid of socializing with people because that takes
time and it may concern people. Improving the strength on lower extremity, getting some
response from the muscles might give hope to the patient. When there is a possible
improvement in her lower extremity she will become more independent. Upper extremity
strength will save her some time in doing ADL’s.
SMART long term goals
1.
S Improving her strength in the upper extremity and some muscles on lower extremity
M ASIA scale key motor functioning for lower extremity, MRC scale for upper extremity
A Assistive exercises through ROM in lower extremity with sliding board, progressive
Internship report
27
resistance exercises in upper extremity
R To become independent and socializing with the environment
T 6- 9 weeks
2.
S Improving the Cardiovascular condition
M Using Borg scale in every walking sessions and increasing the walking distance
A Walking exercises at home and in the therapy sessions
R To be better at functioning in ADL’s without getting tired
T 6-9 weeks
Reasoning for treatment methods:
First of all, for an optimal therapy, the patient should be educated for every step in treatment
process. She also should know the prevention of causing a secondary complication that may
burden her exercises and functioning.
Upper limb functioning needs muscle strength. To become independent, like transfering from
lying to sitting position or from sitting in bed to sitting in wheelchair, the patients have to have
certain muscle strength. Neuromuscular stimulative exercises proved to be successful for
functioning, gaining independence and prevention of falling. Gaining independence not only
increasing confidence but also improve the quality of life. For this reason, the
physiotherapeutic intervention is indicated. The prognosis of this treatment is proved to be
successful for SCI patients (Sheel et al. 2008).
Even though, she did not have pressure sores directly, she should be educated on how to
take care of ulcers and prevent herself from getting another course. Pressure sores are very
dangerous complication for SCI patients. The results of debicutus ulcers may be life
threatening. Each patient has to select his own cushion according to the pressure surface of
the body (Henzel et al. 2011).
Team functions in treatment
The team functioning included physiotherapist, physical therapy physician and the patient’s
environment. Her parents were educated by the physiotherapists and physiatrists. Other
clinicians like dermatologists also had to check her allergies and ulcers regularly to prevent
another complications. The physiatrists gave necessary medications for neurogenic pain.
Internship report
28
The patient and his family also recommended to have psychological consultation if it is
necessary.
It was thought how to use the leg orthoses and forearm crutches to the patient.
This patient was taken care of by multiple physiotherapists in the hospital. Each
physiotherapist had the aim to accelerate the recovery process.
Treatment sessions and social contact
Our 26 year old patient has been following rehabilitation for 9 weeks in Baskent University
Hospital. She has a sister and also a very caring parents. According to her family, they were
sad in the begining about her daughter’s situation but after years they realized that they have
to make their daughter’s life easier by helping and motivating her. The patient and her family
were unaware of some of the situations in the begining of the treatment sessions. The patient
showed great confidence after 4 weeks. She did not have problems with her accepting the
situation and wanted to get better as soon as possible. Her parents have the same
psychological progress like their daughter towards the injury. They accepted the
consequences and try to get as much feedback as possible from physicians and
physiotherapists.
I personally knew that this type of injury and its consequences that is why I have dealt with
this patient successfully both mentally and physically.
Evaluation in treatment and prognosis
The patient was evaluated every week by physiotherapist and every 10 sessions by the
physiatrists. During these evaluations, the ASIA scale and functional independence score
were used. These process were very important for the patient to be able to get functional as
soon as possible. Due to fact that she had ulcers and allergies it took more time for her to be
active in treatment sessions. These secondary complications resulted in delayed progress of
the sessions. According to her dermatologist, electrotherapy could be the triggering reason
for getting allergies, therefore; after 4th weeks of treatment, application of the Galvanic and
Faradic currents were stopped. The exercises in the sliding board was a challenge for this
patient because of her ulcerous wounds. Therefore, some of her movements were adjusted
by using a small cloth underneath her feet to ease the movement in a preventive manner.
Even though she had the contradictory response from her body, there was an improvement
in her gait and cardiovascular state after 6th week. The prognosis of the treatment program
showed to be successful despite the secondary complications.

Internship report
29
The structures assessed and compared every week below:
Ø The flexors, extensors, abductors and internal, external rotators of the hip
Ø The extensors of the knee and 1st toe.
Ø The plantar flexors of the foot.
Ø Gait (Walking and steps for pre-walking in the stairs)
Ø Ulcerous wound healing.
Ø The psychological load and carriability.
Critical reflection
1.a. The physiotherapist as a healthcare worker: assessing, diagnosing, planning
In this competency, I felt so lucky that i could follow the assessment throughly. Despite the
fact that physiotherapist can not work with physicians officially, I had the opportunity to work
with one of the mand gained great knowledge and confidence. The experience in assessing
the patient throughly and make a differential diagnosis were achieved successfully. I have
improved myself in this competency through working with a physiatrist. I have used SOAP
notes for documentation.
In my previous internships, I have already achieved varoius treatment techniques, including
electrotherapy, therefore; treatment has always been success for me. I have treated
orthopedics, neurological, cardiopulmonary and pediatrics patients. Especially, I have
improved my treatment skills in neurological and orthopedics patients. I have always worked
independently with or without a supervision in level 3.
1.b. The physiotherapist as a healthcare worker: therapeutic measures In this competency, I have gained applied various treatment skills into practice. I have
applied EPM, kinesiotaping, mobilization and gave home exercises to the patients. I have
also recommended my thesis project outcome to the physiotherapists. I have recommended
McConnell taping in patients with PFPS.
All aspects that were achieved in level 3, therefore; I have had high scores in therapeutic
approach.
I have had all my smart goals for therapy without having any problems. When I had the
patients, I could follow every step in the treatment sessions. This competency level resulted
in a high level of working behaviour. This working behaviour between the physiotherapists
reflected upon getting a level 3 competency.

Internship report
30
1.c. The physiotherapist as a healthcare worker- Preventative measures
I have applied the necessary preventative measures in almost every patient. Because the
patients did not know exactly what condition they have. The feedback was given about their
condition, precautions before they do home exercises or or necessary actions while applying
the therapy. This competency was a success, therefore; I have gained a level 3 competency.
I believe that this is due to the positive experience in my past internships which I was thought
for preventative care.
2.a. The physiotherapist as a manager- organizing In this competency, I already have had a lot of knowledge in health care system, therefore; I
could apply my knowledge in physiotherapeutic documentation and organize myself
efficiently. The physiatrists used the health care system different than physiotherapists. They
had codes for every condition and they were classified by the government.
I have used the time extensively which had to be done according to the working system in
the hospital. I believe that I have applied my skills in organizing efficiently, thus i have
achieved level 3 competence.
2.b. The physiotherapist as a manager- business undertaking This competency level requires a lot of practice and skills. Even though, this competency
was hard to accomplish, I could learn beneficial skills from my CI. What i had to was
precisely organized and i applied these skills into practice. I was able to gain some good
skills in advertising the hospital and this resulted in having more patients. I could work in
level 3 in this competency.
3.a. The physical therapist as a profession developer- Conducting research
I used the evidence based literature on my reports and my thesis as a profession developer.
This has resulted in a positive outcome in the clinic. I have used my knowledge into practice
in level 3.
3.b. The physiotherapist as professional developer-innovation This competency was one of the hardest competencies to accomplish. Innovation requires
knowledge in every competence above. Not only the physiotherapeutic approach but also the
patients’ contribution to the treatment process is important. Team work should be optimal to
gain and apply the innovative skills into practice. I have had this opportunity up to a certain
amount and this has resulted in level 3 competence.

Internship report
31
Hour Justification
From week 1 to week 14:
Every week from 8.30 till 18.00 : 9.30hr x5= 46.5 Lunch break: 1.5hr x5=7.5 46.5-7.5=39
working hours
39x 14= 546hrs (14 weeks) Ommission days: 3
546hrs- 30hrs= 516 working hrs in total (excluding the hours for preparing reports)
General Conclusions
During this entire internship, I have gained necessary knowledge for my career in this field. I
have practiced assessment and observed most of the time due to the regulations. I have
learned more on therapy techniques that I will apply when I become a physiotherapist.
Not only this internship was about education but also about having enjoyable times during
working and after the working hours in a professional manner.
Overall, I am glad that I have had my last internship in this clinic.

Internship report
32
References
Andersen NH, Soybjerg JO, Johannsen HV, Sneppen O. Self-training versus physiotherapist-supervised rehabilitation of
shoulder in patients treated with subacromial decompression: A clinical randomized study. J shoulder elbow surg. 1999;
8:99-101.
Henzel MK, Bogie, KM, Guihan M, Ho CH. Pressure ulcer management and research priorities for patients with spinal cord
injury: consensus opinion from sci queri expert panel on pressure ulcer research implementation. 2011;48(3);11-31.
Kamkar A, Irrgang JJ, Whitney SL. Nonoperative management of secondary shoulder impingement syndrome. J Orthop
Sports Phys Ther. 1993; 17(5):212-24.
Koman LA, Smith BP, Shilt JS. Cerebral Palsy. 2004; 363(9421):1619-1631.
Kwon JY, Chong HJ, Lee JY, Ha Y, Lee PK, Kim YH. Effects of hippotherapy on gait parameters in children with bilateral
spastic cerebral palsy. 2011; 92(5): 774-9.
Lewis JS. Rotator cuff tendinopathy. Br J Sports Medicine. 2009; 43: 236-241.
McDonald JW, Sadowski C. Spinal cord injury. 2002; 359(9304): 417-425.
Sheel AW, Reid WD, Townson A, Ayas N, Konnyu KJ. Effects of exercise training and inspiratory muscle training in spinal
cord injury: a systematic review. 2008;31(5):500-508.
Tempelhof S, Rupp S, Seil R. Age related prevalence of rotator cuff tears in asymptomatic shoulders. 1999;8(4): 296-9.
Winter B, Pattani H. Spinal cord injury. 2011;12(9):403-5.

Hogeschool van Amsterdam
Amsterdam School of Health Professions
European School of Physiotherapy
Tafelbergweg 51
1105 BD Amsterdam
The Netherlands