Fig. 2a Fig. 2b - Guerbet · 2010-21 Based on the fi ndings on CT scan and MRI, the diagnosis of...
3
2010-21 Fig. 2b Fig. 2a Fig. 1a Fig. 1b Fig. 1c Fig. 2c Fig. 2d Fig. 2e
Transcript of Fig. 2a Fig. 2b - Guerbet · 2010-21 Based on the fi ndings on CT scan and MRI, the diagnosis of...
2010-21
Fig. 2bFig. 2a
Fig. 1a Fig. 1b Fig. 1c
Fig. 2c Fig. 2d Fig. 2e
94620_RD Codali_2010-3_21.indd 2294620_RD Codali_2010-3_21.indd 22 30/05/11 11:2630/05/11 11:26
2010-21
Clinical history
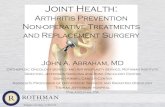
A 70-year-old Caucasian woman presented to an Ear-Nose and Throat (ENT) specialist with a painful swelling in the region of the right parotid gland. The clinical ENT exam revealed no abnormalities and the patient subsequently underwent a CT scan (Fig. 1) and MRI (Fig. 2) of the head, with focus on the right temporomanibular joint.
Imaging fi ndings
Figure 1: CT scan at the level of the temporomandibular joints (TMJ).Fig. 1a: Axial image.Fig. 1b: Reformatted image in the sagittal plane through the right TMJ.Expansile but localised lesion in the area of the right TMJ. Multiple, separate and unevenly dispersed small radiopacities in the vicinity of the mandibular condylar head.Fig. 1c: Reformatted image in the coronal plane, right TMJ (enlarged view).Thinning of the temporal bone with the lesion possibly extending to the middle cranial fossa.
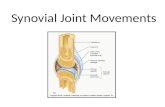
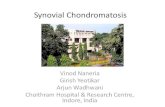
Figure 2: MRI of the brain and skull base, at the level of the TMJ.Fig. 2a: Axial T1-weighed image.Fig. 2b: Axial T2-weighted image.Fig. 2c: Coronal T1-weighed image.Fig. 2d: Coronal T2-weighed image at the level of the right TMJ.Fig. 2e: Sagittal T2-weighed image at the level of the right TMJ.Hydrops of the right TMJ and multiple particles within the capsula of the joint. These par ticles have a low signal intensity both on the T1- (Fig. 2a, 2c) and T2- (Fig. 2b, 2d and 2e) weighted images. Sagittal T2-weigthed image (Fig. 2e) shows, in concordance with the coronal T2-weighted image (Fig. 2d), synovial proliferation protruding into the base of the skull, extending to the tabula at the outer side of the medial fossa, but the medial fossa itself is not affected.
Dijk R.R. van, Rutten M.J.C.M.Department of Radiology, Jeroen Bosch Hospital, PO Box 90153, 5200 ME ‘s-Hertogenbosch, The Netherlands
94620_RD Codali_2010-3_21.indd 2394620_RD Codali_2010-3_21.indd 23 30/05/11 11:2630/05/11 11:26
2010-21
Based on the fi ndings on CT scan and MRI, the diagnosis of synovial chondromatosis of the temporomandibular joint was made.
Comment
Synovial chondromatosis (SC) of the temporomandibular joint (TMJ) was fi rst described by Axhausen in 1933. It occurs most commonly in middle-aged women. Clinical symptoms are pain, swelling, and limitation of motion. SC is uncommon, monoarthritic and generally affects the larger joints. It is characterised by the devel-opment of highly cellular metaplastic cartilaginous foci in the synovial membrane. It is believed that SC originates from embryonic mesenchymal remnants of the subintimal layer of the synovium that becomes metaplastic, calcifi es, and breaks off into the joint space. Although there are multiple reports of temporomandibular joint involvement in SC, cases involving base skull erosion to the middle cranial fossa are scarce.Radiographically, SC commonly demonstrates multiple juxtaarticular radiodensities. They range in size from a few millimetres to several centimetres and show varying degrees of mineralisation within each lesion. The cartilaginous foci may cause erosion of the adjacent bone and widening of the joint space. Although it is often misinterpreted as a sign of aggressiveness, this pattern is still compatible with a benign process. TMJ tumors are rare even though many types of bone or joint neoplasms have been described in this location. Benign bone tumors, including osteochondromas, osteomas, and giant cell tumors have been described. Of these, osteochondromas are the most common ones. Malignant bone tumors of the TMJ are particularly rare. Theoretically, a chondrosarcoma arising from synovial chondromatosis of the tem-poromandibular joint could appear.The articular calcifi cations are easily detected on CT scan of the skull base. MRI is well suited for detection of SC and particularly helpful in defi ning the tissue planes between the SC masses surrounding the soft tissue and the extension to the middle cranial fossa.
Key words
Temporomandibular joint - synovial chondromatosis – MRI
References
1. Axhausen G. Pathologie und Therapie des Kiefergelenks. Fortschr Zahnheilk 1933; 9: 171.2. Karlis V, Glickman RS, Zaslow M. Synovial chondromatosis of the temporomandibular joint with intrac-
ranial extension. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998; 86: 664-666.3. Herzog S, Mafee M. Synovial chondromatosis of the TMJ: MR and CT fi ndings. Am J Neuroradiol 1990;
11: 742-745.4. Ardekian L, Faquin W, Troulis MJ, et al. Synovial chondromatosis of the temporomandibular joint: report
and analysis of eleven cases. J Oral Maxillofac Surg 2005; 63: 941-947.
Dijk R.R. van, Rutten M.J.C.M.Department of Radiology,Jeroen Bosch Hospital, PO Box 90153, 5200 ME ‘s-Hertogenbosch, The Netherlands
94620_RD Codali_2010-3_21.indd 2494620_RD Codali_2010-3_21.indd 24 30/05/11 11:2630/05/11 11:26



![Synovial Chondromatosis of the TMJ: MR and CT Findings · Synovial Chondromatosis of the TMJ: ... often in larger joints, such as the ... and hip [1 , 2]. Synovial chondromatosis](https://static.fdocuments.in/doc/165x107/5adafbfc7f8b9a86378e15b7/synovial-chondromatosis-of-the-tmj-mr-and-ct-chondromatosis-of-the-tmj-often.jpg)