Fibromuscular Dysplasia PowerPoint Presentation for - FMDSA
59
Fibromuscular Dysplasia (FMD)
Transcript of Fibromuscular Dysplasia PowerPoint Presentation for - FMDSA

Fibromuscular Dysplasia (FMD)
0506-0653801
1
Table of Contents
•Fibromuscular Dysplasia Overview–Histology–Components of Vascular System–Pathology–Etiology–Clinical Presentation–Associated Diseases
•FMD Discussion by Arterial Involvement–Renal Arterial Involvement•Mechanisms of Hypertension•Natural History•Diagnosis•Treatment

0506-0653801
2
Table of Contents (Continued)
•FMD Discussion by Arterial Involvement (cont.)–Carotid Arterial Involvement•Natural History•Diagnosis•Treatment•Associated Conditions
–Non-Renal Abdominal Viscera Presentation and Treatment–Peripheral Artery Disease
•Case Studies
0506-0653801
3
Fibromuscular Dysplasia (FMD)
• Nonatherosclerotic, noninflammatory disease• More common in women and younger individuals– The incidence of FMD in children is unknown.
• Described in almost every vascular bed1
– Renal arteries (60-75%)– Cervicocranial arteries (25-30%)– Non-renal visceral arteries (9%)– Arteries in the extremities (5%)– Others including pulmonary and coronary arteries
• Multiple vascular beds in 28% of patients2
1Gray BH et al In Peripheral Vascular Diseases 1996, 2Lüscher TF et al Nephron 1986
0506-0653801
4
FMD - Histology of Arteries
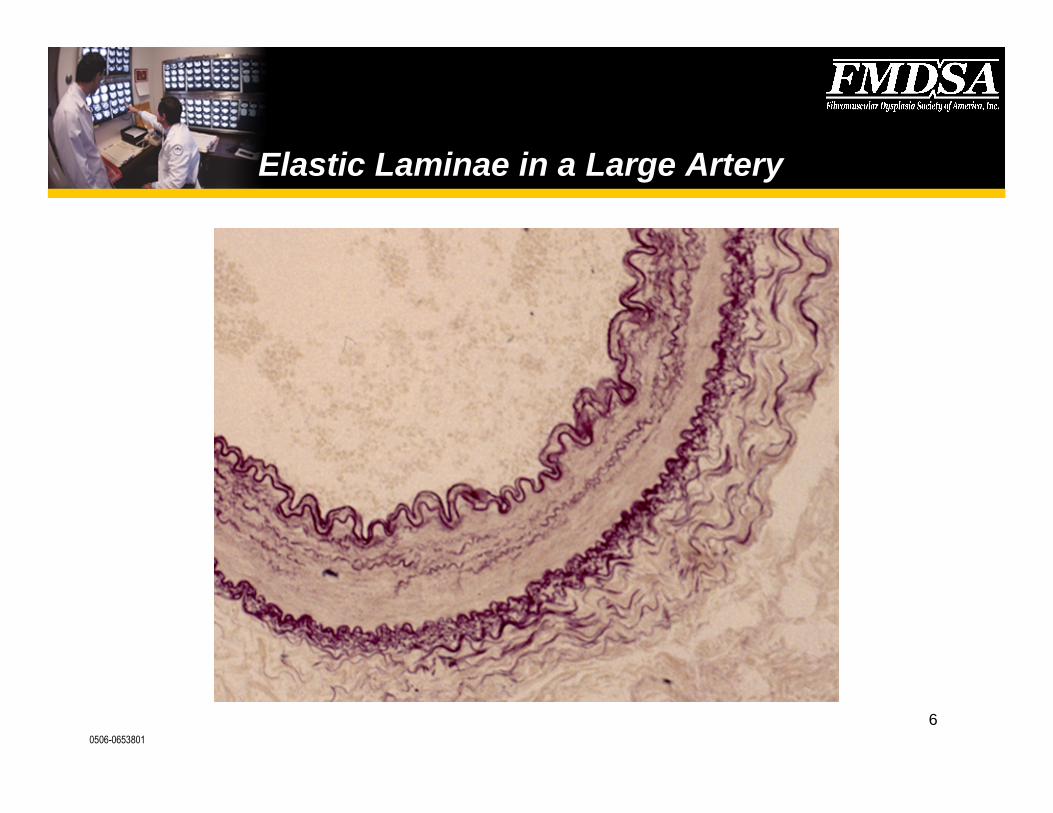
•Lumen•Endothelium (basal lamina)• Intima• Internal elastic lamina•Media•External elastic lamina•Adventitia

0506-0653801
5
Components of the Vascular System
0506-0653801
6
Elastic Laminae in a Large Artery

0506-0653801
7
FMD - Pathologic Classification
• Intimal fibroplasia (less than 10%)•Medial dysplasia–Medial fibroplasia (80%)–Perimedial fibroplasia (10-15%)–Medial hyperplasia (1-2%)
•Adventitial (periarterial) fibroplasia
Harrison EG Jr and McCormack LJ Mayo Clinic Proc 1971
0506-0653801
8
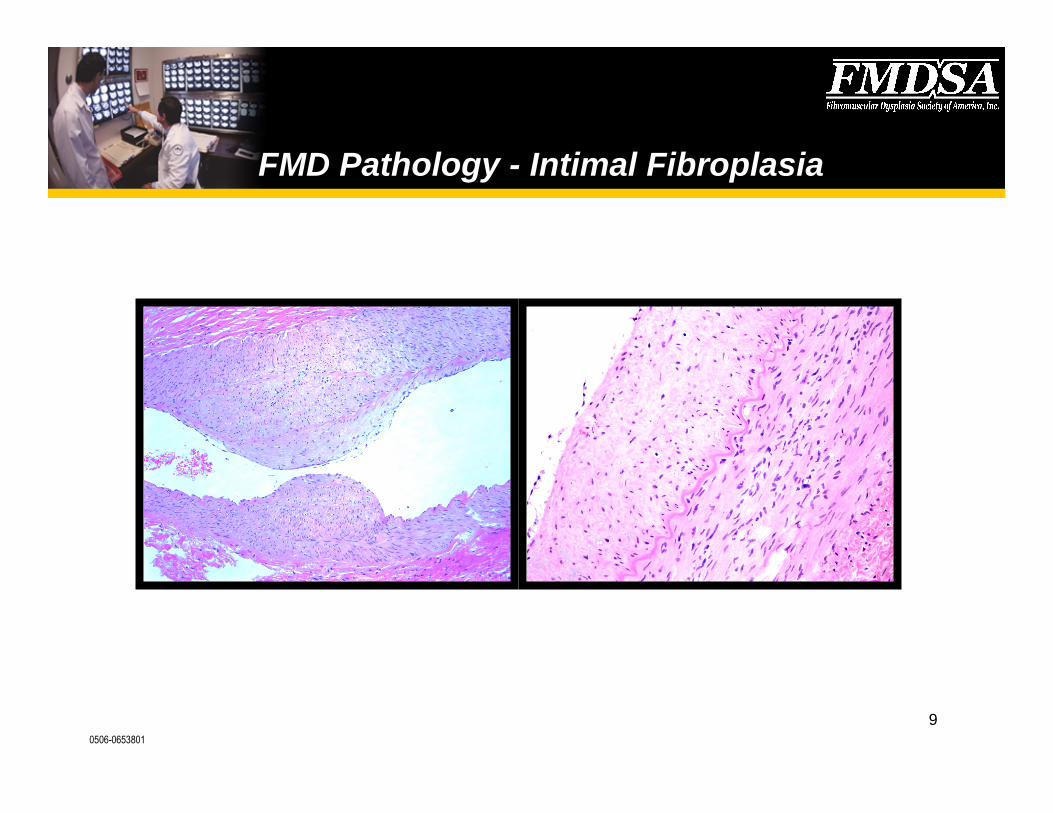
FMD Pathology - Intimal Fibroplasia
•Children and young adults•Circumferential deposition of collagen in the intima, often
projecting into lumina• Internal elastic lamina may be duplicated or disrupted
but can be identified•Long, irregular (tubular) or focal, smooth (concentric
band) stenoses1
1Stanley JC et al Arch Surg 1975
0506-0653801
9
FMD Pathology - Intimal Fibroplasia

0506-0653801
10
FMD Pathology - Medial Fibroplasia
• 25-50 year old women• Thickened media alternating with thinned media aneurysmal
dilatation–“String of beads”
• Thickened media is replaced by collagen• Internal elastic lamina may be thinned or fragmented– May lead to macroaneurysm formation1
• Frequently affects the renal arteries bilaterally
1Stanley JC Arch Surg 1975
0506-0653801
11
FMD Pathology- Perimedial Fibroplasia
•15- 30year old women•Collagen deposition in the outer half of the media
replacing the external elastic lamina; intact adventitialconnective tissue–“String of beads”–Can result in severe stenosis
•Often associated with collateral circulation•Preferentially affects the renal artery (mid portion)
0506-0653801
12
FMD Pathology - Adventitial (periarterial) Fibroplasia
• Adventitial (periarterial) fibroplasia– Very rare– Collagen replaces the fibrous adventitia– May extend beyond artery

0506-0653801
13
FMD - Etiology
•Genetic–Autosomal dominant with variable penetrance in 60% of cases
based on“clinical symptoms”1
–11% prevalence angiographically2
•Hormonal–No difference in gravidity or parity rates, effect on disease
progression3
–Oral contraceptive pill use?4,5,
1Rushton AR Arch Intern Med 1980, 2Pannier-Moreau I et al J of Hypertens 1997, 3Stanley JC et alArch Surg 1975, 4Sang CH et al Hypertension 1989, 5Hardy-Godon S et al J of Neuroradiol 1979

0506-0653801
14
FMD - Etiology
•Mechanical–Ptosis of the right kidney1
–Repetitive trauma such as hyperextension and rotation of theneck1
•Mural ischemia–Occlusion of the vasa vasorum2
–Vasospasm (ergotamines, methysergide)3
–Tobacco use4
1Lüscher TF et al Mayo Clin Proc 1987, 2Sottiurai V et al J of Surg Res 1978,3Fievez ML Med Hypotheses 1984, 4Sang CN et al Hypertension1989
0506-0653801
15
FMD - Clinical Presentation
•Asymptomatic•Nonspecific symptoms–Headaches, altered mentation, tinnitus, vertigo, carotidynia
•Neurologic symptoms–Transient ischemic attacks, cerebral infarctions, subarachnoidhemorrhages, syncope, Horner’s syndrome, cranial nerve palsies
Mettinger KL and Ericson K Stroke 1982, Houser OW et al Radiology 1971
0506-0653801
16
FMD - Associated Diseases
• Turner’s syndrome• Alport’ssyndrome• Neurofibromatosis• Coarctation of the aorta• Moyamoya disease
• Cystic medial necrosis• Hypertrophic cardiomyopathy• Heterozygous α1- antitrypsin
deficiency• Pheochromocytoma
0506-0653801
17
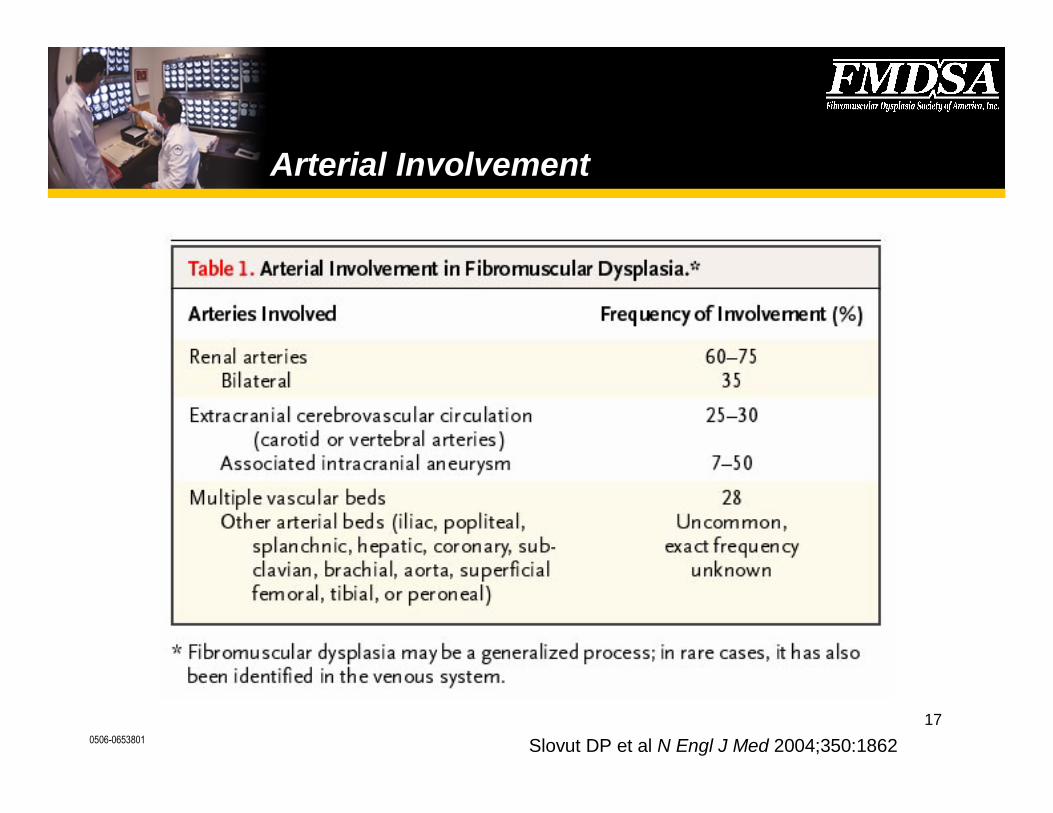
Arterial Involvement
Slovut DP et al N Engl J Med 2004;350:1862
0506-0653801
18
Renal Arteries
• Leadbetter and Burkland (1938) reported the first case of FMD1
• 40% of all patients with renovascular disease have FMD2
• Symptomatic patients present with hypertension– Onset of hypertension before age 30– Epigastric bruit (systolic/diastolic)3
• Less frequently develop ischemic renal atrophy and chronic renalfailure
1Leadbetter WF and Burkland CE J Urol 1938, 2 Olin JW and Novick ACIn Peripheral Vascular Diseases 1996, 3Eipper DF et al Am J of Cardiol 1976

0506-0653801
19
Renal Arteries
Panel A shows string of beads. Panel B shows gadolinium-enhancedMRA revealing bilateral medial fibroplasiaof the renal arteries.
0506-0653801
20
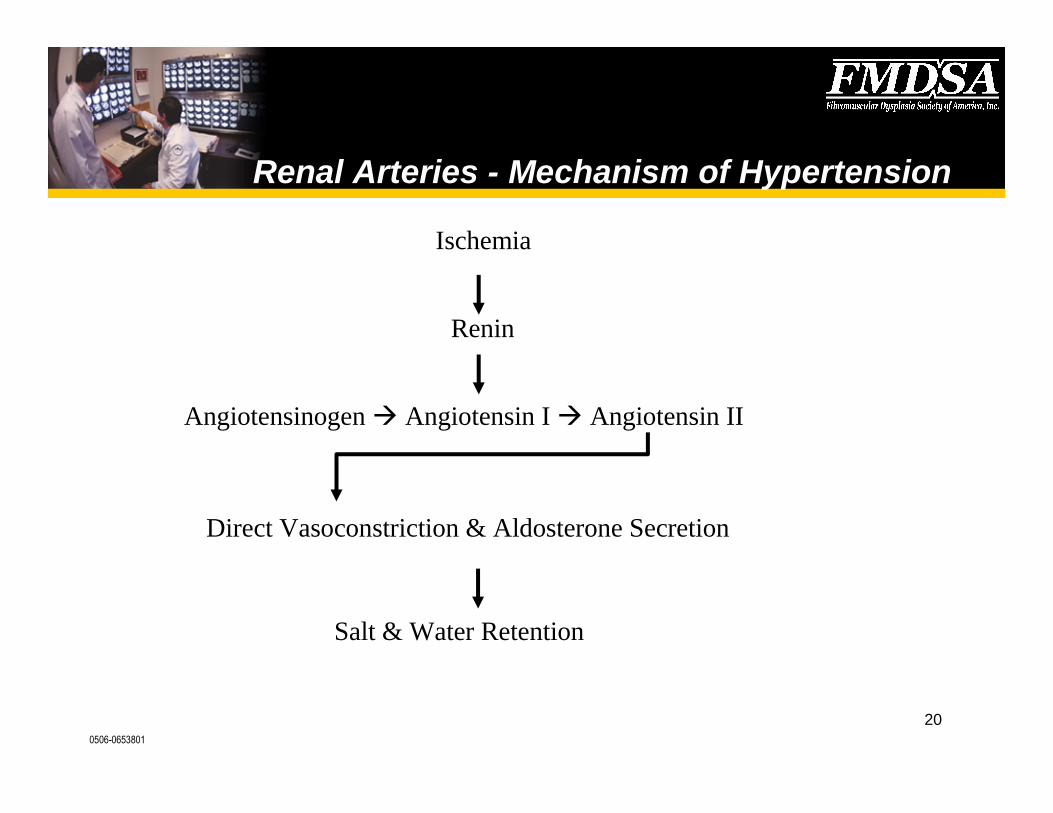
Renal Arteries - Mechanism of Hypertension
Ischemia
Renin
Angiotensinogen Angiotensin I Angiotensin II
Direct Vasoconstriction & Aldosterone Secretion
Salt & Water Retention

0506-0653801
21
Upper Percentiles ofBlood Pressure forGirls
The Fourth Report on the Diagnosis, Evaluation, andTreatment of High Blood Pressure in Children andAdolescents Pediatrics 114(2) Part 3 of 3 August 2004.
0506-0653801
22
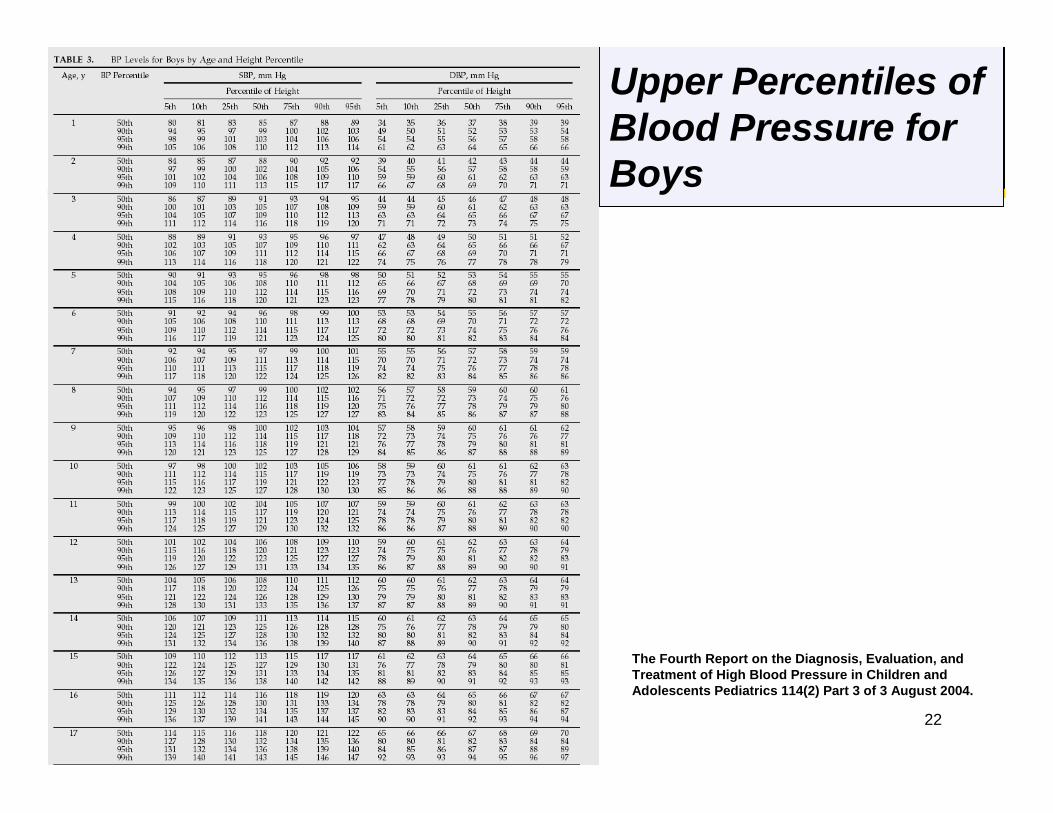
The Fourth Report on the Diagnosis, Evaluation, andTreatment of High Blood Pressure in Children andAdolescents Pediatrics 114(2) Part 3 of 3 August 2004.
Upper Percentiles ofBlood Pressure forBoys

0506-0653801
23
Renal Arteries - Natural History
•Angiographically- proven progression–Goncharenko (1981) 42/42 patients•Follow-up 1–136 months•75% bilateral, 29% medial FMD, 62% change in kidney size
0.5 cm
–Schreiber (1984) 66 patients with medial FMD•Follow-up 45 months angio, 104 months clinical•33% progression–9% increase in creatinine, 27% atrophy of
ipsilateral kidney (1.5 cm)
Goncharenko V et al Radiology 1981, Schreiber MJ et al Urol Clin of North Am 1984

0506-0653801
24
Renal Arteries - Natural History
• Clinically-proven progression– Cragg (1989)–71 potential kidney donors (f/up 49)
•26.6% developed hypertension at 7.5 years (30 w/o nephrectomy)•26.3% developed hypertension at 4.4 years (19 with nephrectomy)•6.1% age and sex-matched controls developed hypertension at 7.1
years
• Clinical progression may reflect the development of concomitantdevelopment of essential hypertension or atherosclerosis
Cragg AH et al Radiology 1989
0506-0653801
25
Renal Arteries - Diagnosis
•Captopril renography (functional)•Spiral CT angiography1
–Transverse sections and maximum-intensity projections
•MR angiography2
•Duplex Ultrasonography–Color power angio
•Angiography
1Beregi J-P et al AJR 1999, 2Leung DA et al Hypertension 1999
0506-0653801
26
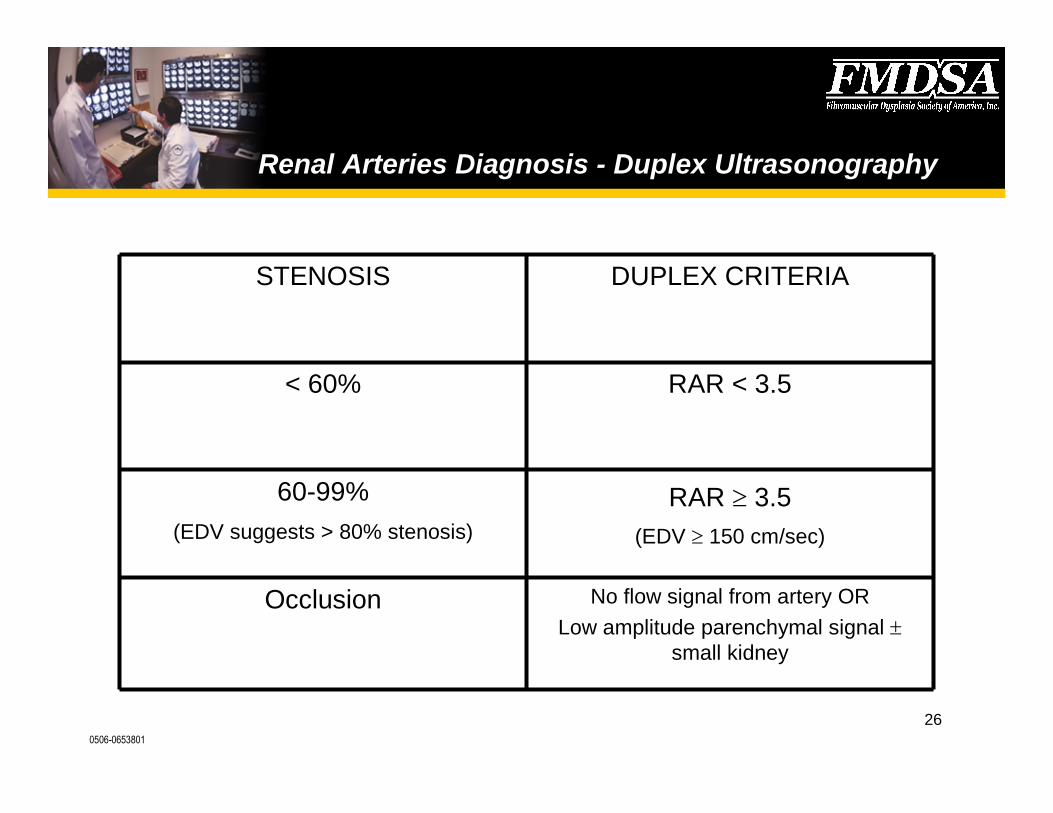
Renal Arteries Diagnosis - Duplex Ultrasonography
No flow signal from artery ORLow amplitude parenchymal signal
small kidney
Occlusion
RAR 3.5(EDV 150 cm/sec)
60-99%(EDV suggests > 80% stenosis)
RAR < 3.5< 60%
DUPLEX CRITERIASTENOSIS

0506-0653801
27
Renal Arteries - Treatment
•Stop smoking•Antiplatelet therapy•Medical therapy following JNC- VI guidelines1 and The
Fourth Task Force Report2
–Unilateral diseaseangiotensin-converting enzyme inhibitor,angiotensin II antagonist
–Bilateral diseasediuretic/calcium channel blocker
1JNC-VI Guidelines Arch Intern Med 1997 2The Fourth Report Pediatrics 114(2) Part 3 of 3 August 2004
0506-0653801
28
Renal Arteries - Indications for Intervention
•Blood pressure cannot be controlled despite threeantihypertensive medications at maximal doses
•The individual is intolerant to the medications•Compliance is an issue•An alternative to lifelong dependency on a medication in
a relatively young individual
0506-0653801
29
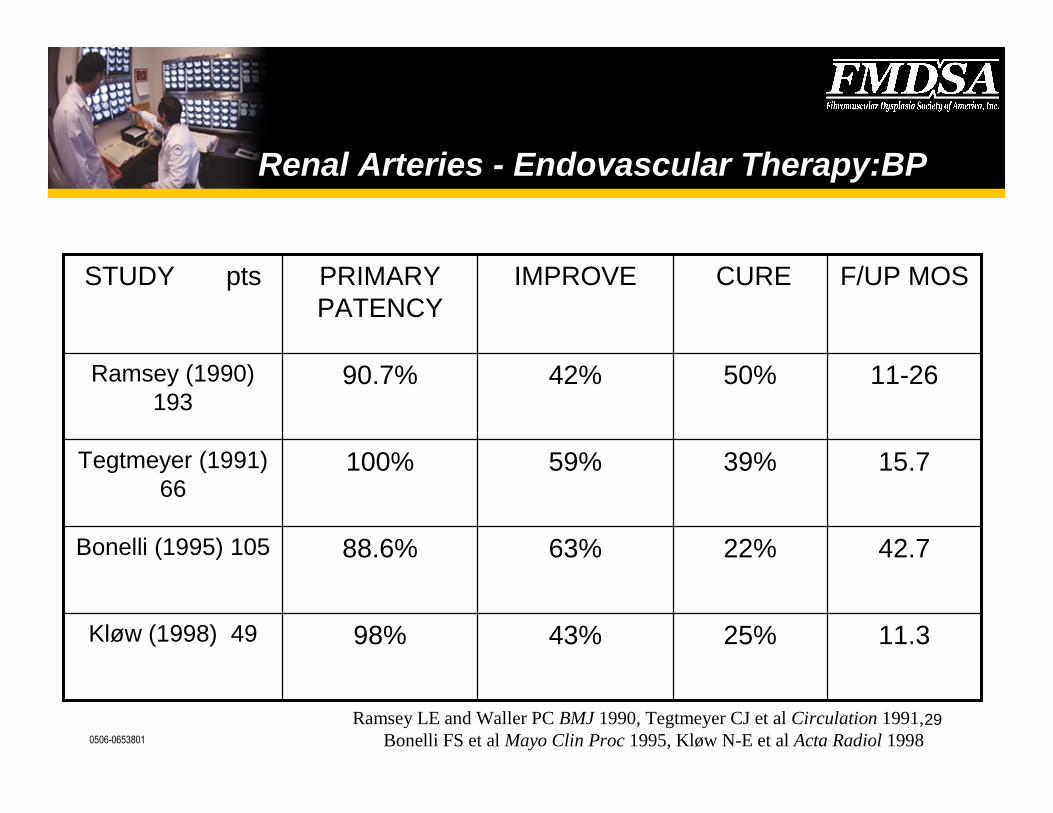
Renal Arteries - Endovascular Therapy:BP
11.3
42.7
15.7
11-26
F/UP MOS
25%43%98%Kløw (1998) 49
22%63%88.6%Bonelli (1995) 105
39%59%100%Tegtmeyer (1991)66
50%42%90.7%Ramsey (1990)193
CUREIMPROVEPRIMARYPATENCY
STUDY pts
Ramsey LE and Waller PC BMJ 1990, Tegtmeyer CJ et al Circulation 1991,Bonelli FS et al Mayo Clin Proc 1995, Kløw N-E et al Acta Radiol 1998

0506-0653801
30
Renal Arteries - Endovascular Therapy: CRI
(2) 14†PTS NOTIMPROVE
(12) 86*PTS IMPROVE
291.72.4CREATININE
3924.640.4BUN
IMPROVE (%)POST-PTA(mg/dl)
PRE-PTA(mg/dl)
Tegtmeyer CJ et al Circulation 1991

0506-0653801
31
Renal Arteries - Endovascular Therapy:Branch Lesions
•Segmental renal arteries are affected in 30- 56% ofpatients with FMD
•Cluzel (1994)–20 patients with 25 arteries–Technical success rate 84%–91% patency rate at 6 months–Hypertension cure•Post-PTRA 70%, 6-month 76%, long-term 68%
–Hypertension improved•Post-PTRA 25%, 6-month 24%, long-term 16%
Cluzel P et al Radiology 1994

0506-0653801
32
Renal Arteries –Intervention Complications
• Puncture site– AVF, pseudoaneurysm, bleeding/hematoma, femoral nerve injury,
infection
• Catheter-related– Dissection, perforation/rupture, AED, balloon rupture, thrombosis, renal
artery spasm
• Contrast Media– ARF, anaphylaxis
• Medical
0506-0653801
33
Renal Arteries –Predictors of Cure ofHypertension in FMD
• Younger patients with milder hypertension of a shorter duration weremost likely to be cured.
• Some patients with an extremely low chance of cure might bemanaged with a trial of medical therapy
• FMD is unlikely to progress to renal failure

0506-0653801
34
Renal Arteries - Surgery
• Indications– Lack of endovascular expertise, recurrent disease, inaccessible branch
lesions• Approaches– Aortorenal bypass, extracorporeal revascularization &
autotransplantation, spleno- or hepato-renal• Blood pressure– 36-63% cure, 30-50% improvement
• Outcomes– Low morbidity and mortality
Hansen KJ et al J Vasc Surg 1992, Novick AC et al JAMA 1987, Reiher L et al Eur J Endovasc Surg 2000

0506-0653801
35
Renal Arteries - Surgery
• 45 children with renovascular FMD, 17 with aortic involvement• Average age at diagnosis was 9 years• Three with renal failure• Twenty-three of the 45 had bilateral vessel involvement• A variety of surgical approaches were used depending on the
pathology encountered• Thirty-eight patients underwent revascularization, seven underwent
primary nephrectomy, five underwent primary partial nephrectomy,and 12 had aortoaortic bypass performed
• Seventy percent were cured, 26% improved; and 4% did notrespond to treatment with up to 16 years of follow-up
• There was no mortality.
O'Neill JA Jr.Long-term outcome with surgical treatment of renovascular hypertension. Pediatr Surg 1998;33(1):106-11

0506-0653801
36
Carotid Arteries
•Palubinskas and Ripley (1964) described a case of FMDinvolving the extracranial internal carotid artery1
•Carotid arteries (95%) frequently bilaterally2
•Vertebral involvement is rare and usually associated withcarotid involvement3
•Predominately affects extracranial segments
1Palubinskas AJ and Ripley HR Radiology 1964, 2Healton EB In Stroke:Pathophysiology,Diagnosis, and Management 1986, 3Osborn AG and Anderson RE Stroke 1977
0506-0653801
37
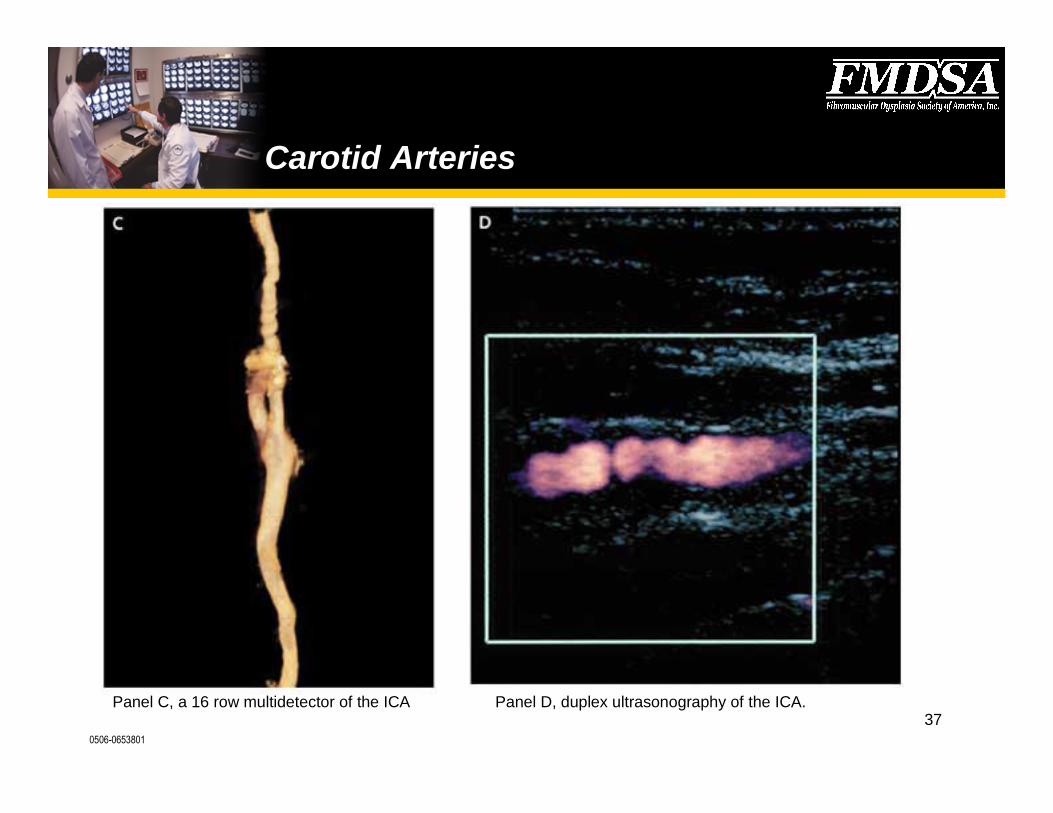
Carotid Arteries
Panel C, a 16 row multidetector of the ICA Panel D, duplex ultrasonography of the ICA.

0506-0653801
38
Carotid Arteries
See Examples of FMD:
Panel A–severe concentric stenosisin the ICA.
Panel B–ICA after percutaneousangioplasty.
Panel C–shows sever redundancy &a kink in the distal ICA.

0506-0653801
39
Carotid Arteries - Natural History
•Look at clinical outcome, not angiographic progression–Corrin (1981) 79 patients, 3 strokes (3.8%)•13 TIA/CVA, 10 SAH, TX [4 OR, 11 med]
–Wells (1982) 17 patients, 2 strokes* (13%)•9 TIA, TX [1 OR, 3 med]
–Stewart (1986) 45 patients, 0 strokes (0%) in the 35 who did nothave an operation•10 OR <3mos, 23/35 TIA/CVA only 1 symptomatic
Corrin LS et al Arch Neurol 1981, Wells RP and Smith RRNeurosurgery 1982, Stewart MT et al J Vasc Surg 1986

0506-0653801
40
Carotid Arteries - Diagnosis
• Angiography remains the gold standard– “String of beads”, smooth tubular stenoses, diverticula, well-
defined webs or septations1
– FMD has been associated with carotid kinks2
• Carotid duplex ultrasonography3
• Magnetic resonance angiography4
1Osborn AG and Anderson RE Stroke 1977, 2Schneider PA and Rutherford RB In Vascular Surgery 2000,3Boespflug OJM Neuroradiology 1985, 4Heiserman JE et al AJNR 1992

0506-0653801
41
Carotid Arteries - Treatment
• Stop smoking• Antiplatelet therapy• Intervention– Surgery including a resection with end-to-side anastomosis (or
interposition graft), endarterectomy, carotid-middle cerebral arterybypass
– Graduated intraluminal dilatation– Percutaneous transluminal angioplasty
0506-0653801
42
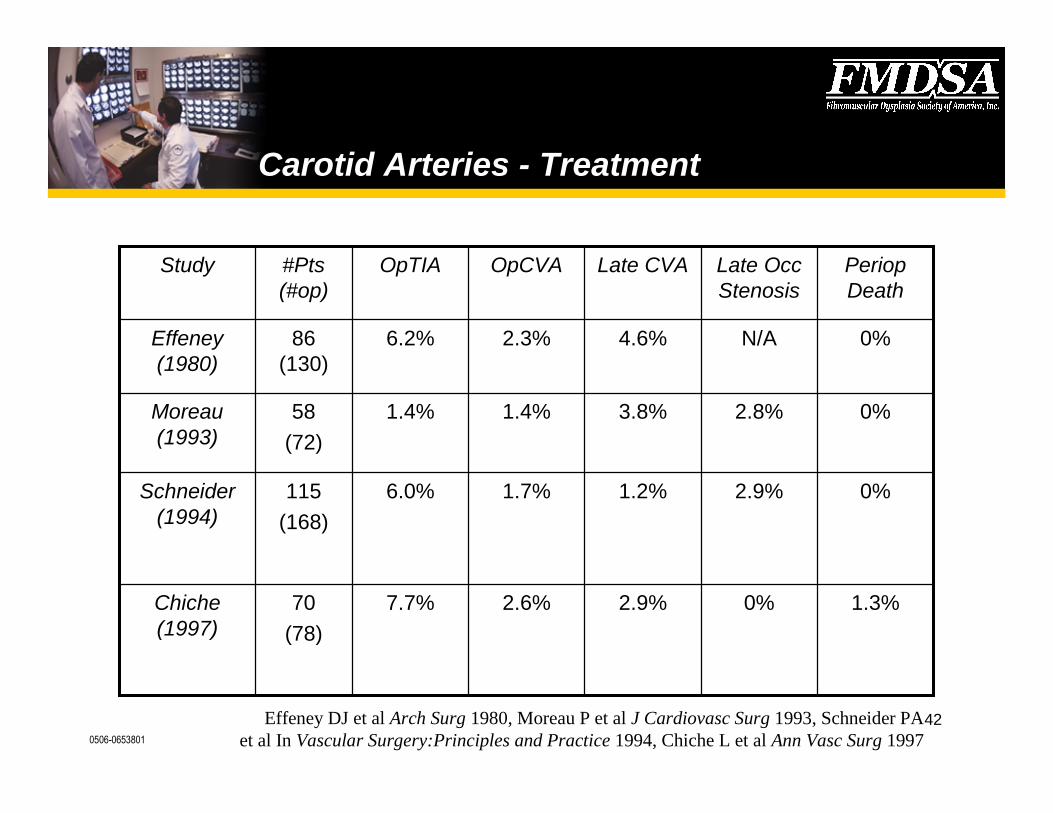
Carotid Arteries - Treatment
1.3%0%2.9%2.6%7.7%70(78)
Chiche(1997)
0%2.9%1.2%1.7%6.0%115(168)
Schneider(1994)
0%2.8%3.8%1.4%1.4%58(72)
Moreau(1993)
0%N/A4.6%2.3%6.2%86(130)
Effeney(1980)
PeriopDeath
Late OccStenosis
Late CVAOpCVAOpTIA#Pts(#op)
Study
Effeney DJ et al Arch Surg 1980, Moreau P et al J Cardiovasc Surg 1993, Schneider PAet al In Vascular Surgery:Principles and Practice 1994, Chiche L et al Ann Vasc Surg 1997

0506-0653801
43
Carotid Arteries - Associated Conditions
•Intracranial “berry” aneurysms– Incidence 21% to 51%1
–Multiple, found predominately in the internal carotid and middlecerebral arteries2
–Obtain a MRA for screening
•Dissections3
•Arteriovenous fistulas4
1Healton EB In Stroke:Pathophysiology, Diagnosis, and Management 1986, 2Mettinger KL Stroke1982, 3Müller BT et al J Vasc Surg 2000, 4Hieshima GB et al Neurosurgery 1986
0506-0653801
44
Non-Renal Abdominal Viscera
•Celiac, superior mesenteric, inferior mesenteric, hepatic,and splenic arteries
•More typically appear as long tubular stenoses1
•Component of a systemic process mimicking vasculitis(intimal FMD)
1Lüscher TF et al Mayo Clin Proc 1987

0506-0653801
45
Non-Renal Abdominal VisceraPresentation & Treatment
• Asymptomatic• Mesenteric ischemia1
– postprandial pain, weight loss, epigastric bruit
• Abdominal pain due to ruptured aneurysm2
• Bowel infarction is rare3
• Treatment with percutaneous transluminal angioplastyor surgical revascularization
1Yamaguchi R et al Am J Gastro 1996, 2Jones HJ et al J Rheumatol 1998,3Hamed RMA and Ghandour K J Pediatr Surg 1997

0506-0653801
46
Peripheral Arterial Disease
•Lower extremities–External iliac, femoral popliteal, tibial, peroneal–Digital ischemia, intermittent claudication, acute limb ischemia1
•Upper extremities–Subclavian, axillary, brachial, radial, ulnar–Arm claudication, paresthesias, subclavian steal syndrome,
weakness, ischemic digits (hypothenar hammer syndrome)
1Sauer L et al J Vasc Surg 1990

0506-0653801
47
Summary
•FMD can occur in almost any arterial bed•Angiography remains the diagnostic test of choice but
other, less invasive techniques may be useful•All patients must stop smoking and be treated with an
antiplatelet agent• Intervention should be reserved for symptomatic patients

FMD Case Studies
0506-0653801
49
• MF a 14 year old male• Routine physical examination
found to have hypertension• No symptoms or signs by
history or on examination
• BP 170/105 mmHg on repeatmeasurements
• EKG/ECHO–LV+• Metabolic panel normal
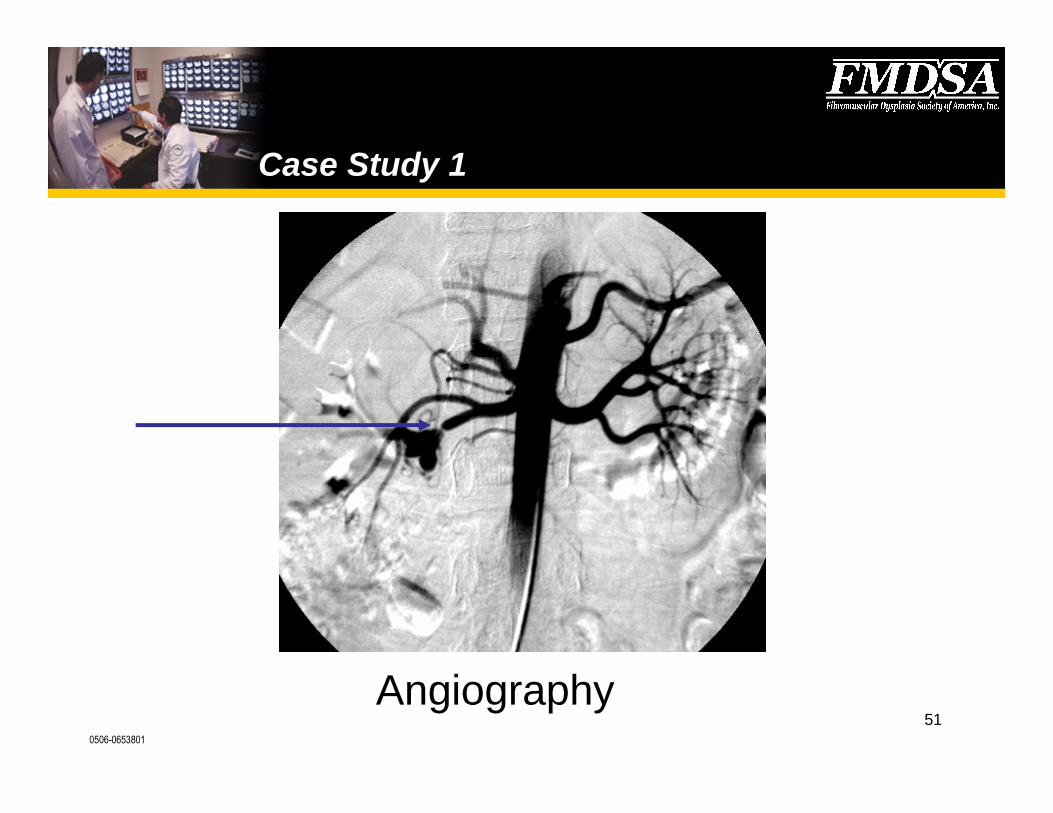
Case Study 1

0506-0653801
50
DMSA showsno scarring withequal uptake byboth kidneys
Case Study 1
0506-0653801
51Angiography
Case Study 1
0506-0653801
52
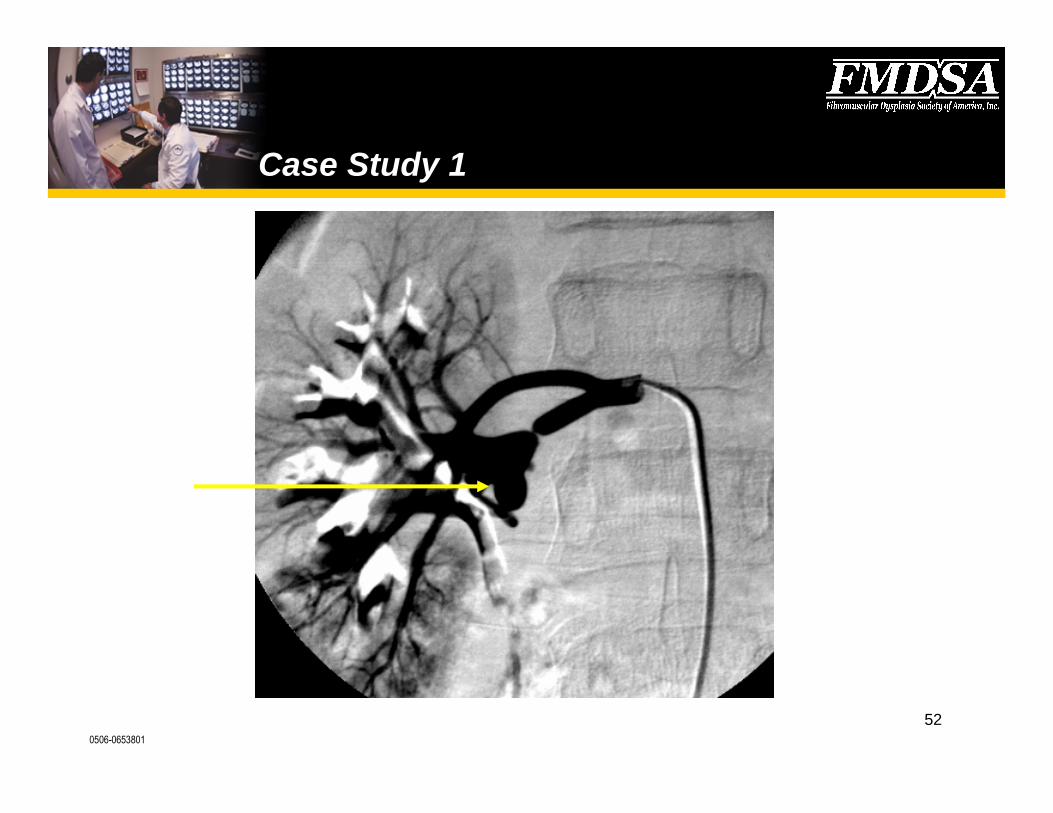
Case Study 1

0506-0653801
53
•Management–Antihypertensives–Right nephrectomy after failed repair to a large thin walled extra-
parenchymal aneurysm
•Follow- up–No further hypertension, off all medications. No indication of any
further vessel involvement after 36 months follow up.
Case Study 1
0506-0653801
54
Case Study 2
• GB 13 year male• Presented with severe hypertension• Found by routine school screening• Poorly functional right kidney, small size , severe right renal artery
stenosis• Normal left kidney and normal vessels• Right nephrectomy–off blood pressure medications
0506-0653801
55
Case Study 2
• GB now 15 years old• Severe hypertension recurred• Left kidney now with stenosis• Repeated balloon dilatation• Ongoing need for blood pressure medication

0506-0653801
56
Gerard Burns
Left kidney withtrident renal arterysub-branchinvolvement
Case Study 2

0506-0653801
57
• Patient JB• Found to have HTN on routinePediatrician’s visit
• Past history of trauma to the rightflank and back related tobaseball
• BP elevated to 160/100 mmHg
• LVH• Non-functional right kidney with
severe right renal arterynarrowing
• Unilateral Nephrectomy• No HTN after 3 years of follow up
Case Study 3
0506-0653801
58
For more information
A voluntary, not-for-profit health organization dedicated toimproving the lives of those affected by FibromuscularDysplasia (FMD) by building awareness and raising funds topromote research towards new medical treatments anddiagnostic tools.
P.O. Box 999, Hudson, OH 44236-0999
(330) 653-8416
www.fmdsa.org [email protected]