Fibroids and infertility

of 24
-
Upload
drsathyabalasubramanyam -
Category
Health & Medicine
-
view
400 -
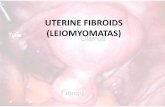
download
4
Transcript of Fibroids and infertility
- 1.FIBROIDS AND INFERTILITYCURRENT EVIDENCE Dr SATHYA
2. Fibroids are benign tumours of the uterusoccurring in up to 77% of women. Fibroids have been noted to occur more frequently in women with infertility. Retrospective studies have suggested the benefitof surgically removing fibroids to increase the fertility efficacy of both natural conception and assisted conception. 3. There are a variety of methods to surgicallyremove fibroids including laparotomy, laparoscopy and hysteroscopy. The relative advantages and disadvantages ofthese modalities in terms of fertility efficacy and side effects are unknown. 4. Cochrane review on surgical management of fibroids and infertility Objectives To determine the efficacy and safety of theremoval of uterine fibroids in subfertile women by laparotomy, laparoscopy or hysteroscopy when compared with expectant management or each other. 5. Selection criteria Randomised controlled trials (RCTs) in whichfibroids were removed via surgery for the treatment of infertility 6. Main results Only one randomized controlled study wasincluded (131 women) and this was probably underpowered. There was no evidence of a difference in outcome in terms of clinical pregnancy rate and live birth rate when fibroids were removed via laparotomy or laparoscopy for infertility. 7. There were some non fertility benefits ofremoval via laparoscopy including shorter hospital stay, less febrile illness and a smaller drop in preoperative haemoglobin concentration when compared to laparotomy. There were no randomised controlled studies comparing hysteroscopic removal or no intervention with other surgical modalities. 8. CONCLUSIONS OF COCHRANE There is limited evidence to suggest that there isno difference in fertility efficacy outcome if fibroids are removed via laparotomy when compared to laparoscopy. There is no good randomised controlledevidence to support hysteroscopic removal of fibroids compared to other surgical modalities for fertility efficacy. 9. COCHRANE REVIEWS Of 38 subfertility reviews currently or previouslypublished on the Cochrane Library from the Menstrual Disorders and Subfertility Group, 12 reviews concluded that there was evidence of effectiveness of the interventions studied. Implications: Very little good evidence is available for infertility and we are still dependent on substandard studies and expert opnions on deciding optimal management for a patient. 10. Types of fibroids 11. TYPES OF FIBROIDS 1. Submucos (SM): Fibroid distorting ut cavity. Type 0: pedunculated without intramural extension Type I: Sessile with intramural extension 50% 2. Intramural (IM): Fibroid not distorting the cavity & 50% protrudes out of the serosalsurface 12. Associated with infertility: 5- 10%. Only cause of infertility:2- 3% IVF provides a good model to assess the effect offibroid on implantation rate by excluding other factors such as tubal or male (Donnez & Jadoul, 2002). IVF cannot assess the effect of fibroid on spermmigration & ovum transport. 13. Type of fibroid and IVF preg rate SM: Most detrimental effect 9% IM: Modest impact 16% SS: Least impact on PR. 27% Control 30% 14. Donnez & Jadoul (2002). No difference in implantation or PR unless the uterine cavity itself was distorted by the myomas Fibroid preg rate% DISTORTED CAVITY 9% NOT DISTORTED CAVITY 34% CONTROL 40% 15. Size of fibroid No statistically significant difference inimplantation rate or pregnancy outcome