Ffederasiwn Dyfed o Gynghorau Iechyd Cymuned ... proposals 1-15.pdfFfederasiwn Dyfed o Gynghorau...
76
Ffederasiwn Dyfed o Gynghorau Iechyd Cymuned 103 Heol Awst Caerfyrddin SA31 3AP Dyfed Federation of Community Health Councils 103 Lammas Street Carmarthen SA31 3AP Dear Minister Please find attached responses from the three CHCs within the Hywel Dda area. As in our original response there is agreement over aims and aspirations but not on the structure to achieve these. There is broad consensus between Carmarthenshire and Pembrokeshire as outlined in the list of agreed principles. Their responses differ in language and emphasis but not in the direction of travel. Ceredigion CHC has not agreed to the idea of a regional CHC with an executive committee, wishing to retain all rights, duties and powers at county level but proposes a strengthening of the federation to deal with regional issues. The Chairs and Chief officers have tried to develop a universally acceptable model that meets the seemingly conflicting demands of local representation in a regional setting, within the guidelines received from the Minister and Chief Executive of the NHS in Wales. It is a shame that only two of the three CHCs could agree to the proposed model. As Chair of the federation I am sorry not to be able to deliver what the Minister asked of all Chairs, but we remain a Member led organisation. I hope enough common ground has been found to establish a way forward for these three counties, as the agreement from Carmarthenshire and Pembrokeshire was for a model encompassing all three CHCs. We all agree that our task is to monitor and work constructively with the Hywel Dda LHB for the benefit of the populations we jointly serve. Yours sincerely Jack Evershed Chair of Dyfed federation of CHCs
Transcript of Ffederasiwn Dyfed o Gynghorau Iechyd Cymuned ... proposals 1-15.pdfFfederasiwn Dyfed o Gynghorau...

Ffederasiwn Dyfed o Gynghorau Iechyd Cymuned 103 Heol Awst
Caerfyrddin SA31 3AP Dyfed Federation of Community Health Councils 103 Lammas Street Carmarthen SA31 3AP
Dear Minister Please find attached responses from the three CHCs within the Hywel Dda area. As in our original response there is agreement over aims and aspirations but not on the structure to achieve these. There is broad consensus between Carmarthenshire and Pembrokeshire as outlined in the list of agreed principles. Their responses differ in language and emphasis but not in the direction of travel. Ceredigion CHC has not agreed to the idea of a regional CHC with an executive committee, wishing to retain all rights, duties and powers at county level but proposes a strengthening of the federation to deal with regional issues. The Chairs and Chief officers have tried to develop a universally acceptable model that meets the seemingly conflicting demands of local representation in a regional setting, within the guidelines received from the Minister and Chief Executive of the NHS in Wales. It is a shame that only two of the three CHCs could agree to the proposed model. As Chair of the federation I am sorry not to be able to deliver what the Minister asked of all Chairs, but we remain a Member led organisation. I hope enough common ground has been found to establish a way forward for these three counties, as the agreement from Carmarthenshire and Pembrokeshire was for a model encompassing all three CHCs. We all agree that our task is to monitor and work constructively with the Hywel Dda LHB for the benefit of the populations we jointly serve. Yours sincerely Jack Evershed Chair of Dyfed federation of CHCs

CONSULTATION UPON THE FUTURE OF CHC’S IN WALES – PRINCIPLES / FUNDAMENTALS (agreed by Carmarthenshire
and Pembrokeshire CHCs)
• Form a West Wales CHC and 3 divisions, one in each county. • Administered by an ‘executive committee’ of 18 members
• Sovereignty to WWCHC executive • 6 members from each county division on executive committee – 18 in
total
• Chairman appointed annually from the 18 and to be the
link/representative with LHB/Wales Board of CHC’s etc • Budget held and administered centrally by WWCHC
• Work direction etc determined by WWCHC • Lead Officer, part time, on rota from within the existing CHC Chief
Officer group • Central Planning Committee formed • Longer term administration office located near to the Hywel Dda LHB
headquarters • Longer term dedicated full time Lead Officer and support staff in central
office to include PPI • Advocacy service retained but transferred to budget and coordination
of Wales CHC Board with accountability retained at WWCHC level
• Each division to have 20 full members and additional co-options as necessary
• Local council meetings held in public as at present • Sub committees maintained within divisions as at present
• Local external stakeholder representation to committees as at present • Permanent office base to be maintained in each county to include
access to meeting rooms

• Appropriate staff in each of the three divisions
• Divisions to develop additional citizen engagement (PPI) models
○ Focus Groups ○ Internet survey groups








1
PEMBROKESHIRE COMMUNITY HEALTH COUNCIL RESPONSE TO THE CONSULTATION UPON THE FUTURE OF COMMUNITY HEALTH COUNCILS IN WALES AIM This document outlines the proposals by the Pembrokeshire Community Health Council for effective joint working between the constituent three CHCs in West Wales. These proposals will provide a robust way of representing the interests of the public and patient in the restructured health service. They will ensure that by 1 October 2009 we will have in place a working mechanism that achieves the Minister’s five key principles for the CHCs, within existing resources. INTRODUCTION The Carmarthenshire, Pembrokeshire and Ceredigion CHCs have successfully worked together on a federated basis for a number of years. On this basis the Pembrokeshire CHC wholeheartedly welcomes the opportunity to further develop and formalise this three county relationship, with the Minister’s five key principles at the heart of our philosophy. The fundamental principle is to provide an effective structure to better represent the interests of the public and patient within the Hywel Dda LHB designated area operating on three levels:
a. National Level. To work coherently and effectively within the overarching CHC framework for Wales;
b. Regional/Strategic Level. To hold the Hywel Dda LHB to account through the scrutiny of services;
c. Local Level. To further develop this critical activity through effective citizen engagement and systematic gathering of local views.
We intend to form a single West Wales CHC (WWCHC) coterminous with the Hywel Dda LHB, which will consist of an executive committee and three county divisions. The executive committee will be responsible for strategic national and regional issues while the balance between these issues and effective local participation will be fulfilled through the development of the three county Divisions, each operating within the boundaries of the existing three local authorities. At the heart of the county function will be effective and constant citizen engagement, informing of health care plans and gathering local views and concerns across this large diverse area. Whilst we can deliver the Minister’s main principles by 1 October 2009 by developing our federated structure within existing resources, this is a major constraint and further capability can only be developed as the structure matures and when additional resources are provided.

2
DETAILS National Level The WWCHC will maintain close links to the National CHC Board. Membership of the CHC Board by the WWCHC Chair formalises this relationship. Regular contact between WWCHC and the CHC Board is essential and this committed participation will allow regional issues or concerns to be debated on an all Wales basis and appropriate action sought from key organisations such as the National Advisory Board or National Delivery Group. The WWCHC would readily accept the corporate governance obligations that this entails, adhering to consistent procedures and data capture, whilst maintaining sensible freedom of movement to address local concerns effectively. Regional Level – the WWCHC The WWCHC will work closely and constructively with the Hywel Dda LHB; it will hold it to account for the delivery of healthcare within the region and will also be intimately involved in the planning of services at the earliest stages. In order to facilitate effective communication and liaison there should, in addition to three county divisional offices, eventually be one regional administrative headquarters for the WWCHC, located close to the main LHB headquarters. In the longer term there will also be one dedicated WWCHC Lead Officer/Chief Executive with appropriate support staff, but this cannot be achieved by 1 October 2009 due to lack of resources. Until that time this role will be undertaken on a part time rotational basis by one of the three Chief Officers from the county divisions. The WWCHC membership will consist of 60 equal members who will elect an executive committee of 18 members. This Committee will be composed of equal representation from the Carmarthenshire, Ceredigion and Pembrokeshire county Divisions, each of whom will annually elect 6 of its members to the WWCHC executive committee. The Chair of each Division will automatically have a place on the WWCHC executive committee, with the other fifteen, five from each division, elected by the division and reflecting the makeup of the Divisions, i.e., representatives from the Local Authority, Voluntary organisations and Assembly appointees. The Executive Committee will hold regular meetings in public. It will be the decision making body for the West Wales CHC and its decisions will be binding. The meetings schedule of the WWCHC will be organised once the administrative structure and meeting schedule of the LHB are known. The Chair, supported by the Lead Officer, would attend all Hywel Dda LHB Board public meetings and be permitted speaking rights (but not voting, to retain independence) and allowed to present agenda items - as at present. The Budget and expenditure plans will be approved by the executive committee and administered by the regional Lead Officer and funds will be devolved as appropriate to the constituent Divisions.

3
The Chair of the WWCHC will be the representative on the Board of CHCs. The Executive Committee of the WWCHC will set the Annual Plan and Work Programme for the Divisions building on best practice and feedback from the divisions. The Executive Committee of the WWCHC will also set basic strategy for the Divisions; the divisions will feed back information and findings to the Executive Committee. The WWCHC will be responsible for establishing a coherent Citizen Engagement (PPI/PPE) strategy. It will also form close links with the LHB’s citizen engagement strategy to ensure there is no duplication of effort or confusion regarding the roles and responsibilities of the proposed Stakeholder Reference Group. It will also coordinate the scrutiny role of the Divisions and maintain close contact with Health Inspectorate Wales. Full WWCHC involvement in all Hywel Dda LHB planning matters is essential. The continuance of the Three Counties Planning Forum is therefore vital since this has proved to be very effective in involving all stakeholders early in the NHS planning stages in a constructive and effective manner. Local Level – CHC County Divisions Each Division will be composed of 20 full CHC members. New members will be appointed to the Divisions (not direct to the WWCHC) The membership composition will be as at present, with representatives from the local authority, the voluntary sector and Assembly appointees. Each Division will elect a Chair, and two Vice Chairs from amongst its membership. Co-opted membership to each county Division will be coordinated by the Divisional Chief Officer and ratified by the WWCHC executive committee. The county Divisions will be the critical public interface of the WWCHC ensuring effective citizen engagement across a large and diverse area. They will also be most effective in engaging with Local Authorities, developing partnership working and examining ways to establish effective communication networks across health and social care. Due to the geography and large rural spread of the WWCHC it is deemed essential for the county Divisions to retain office premises (and access to conference facilities) in each county area - with a Divisional Chief Officer and appropriate staff. Meetings will also need to be held locally as appropriate. The Divisions will carry out the PPI and scrutiny role of the WWCHC and provide feedback to the executive committee The Divisions will also ensure that the executive committee is informed of local issues that need to be addressed at higher level.

4
The elected chairman of the division and five other members elected from each Division will have regional responsibility through the executive committee of the WWCHC. All 20 members in each county will also have a clearly defined portfolio of responsibilities, to include delegated and active citizen engagement in their areas, as well as the scrutiny function. This local function will develop the community strategy so important to the new role of the LHB. Each division will ensure that local involvement with communities, partners and service users is expanded and that the involvement is on a long term basis. The WWCHC would be the initial point of contact for public consultations and would ensure the fullest, appropriate citizens engagement by the local Divisions. Public Patient Involvement/Engagement Strategy To engage fully and effectively with the citizens within the WWCHC boundary, sufficient resources, both funding and appropriately trained, capable members, are prerequisite. A coordinated, regional approach across the three counties would be achieved by the executive committee supported by PPI staff. Sufficient investment in training should be made to enable members tasked with PPI responsibilities to develop and build intimate links with the community. It will be the responsibility of the executive committee to liaise with the LHB’s citizen engagement function whilst preserving the CHC’s independence and statutory remit, particularly with regard to the current Interim Consultation guidelines. The executive committee will also be tasked with improving the level of citizen engagement by evolving procedures which will assist the divisions in improving their performance. Initial thoughts would include developing Health Focus Groups, developing links to existing groups (Community Councils, Pensioners Clubs, Hard of Hearing, WI and so on and then moving towards engagement with others who are not represented by established groups or social networks(through links with drop-in centres, night shelters, mental health advocates and so on). Advocacy The CHC Advocacy Service must be strengthened and then coordinated and financed by the CHC Board, but continue to be delivered locally from one regional base as at present. Advocacy represents a source of vital intelligence and must be adequately resourced to provide a credible, timely service to the benefit of the public/patient and NHS. CHC advocacy will be a vital element in the NHS Redress Measures to be implemented in 2010. Accountability for the advocacy function should remain with the WWCHC with advocates, as at present, deploying into the local divisions as and when required to meet clients.

5
Partnership Working (see also Scrutiny below) Developing links with Local Authority Health and Social Care and the voluntary sector is critical and it is anticipated that this work will continue to develop across the three divisions through the Health, Social Care and Wellbeing Partnerships. It is also important to build on existing examples of good practice. Where CHC relationships with Local Authority Health and Social Care Scrutiny Committees are already well established, experiences and lessons learned can be used to develop similar arrangements across the whole region. Further development in sectors such as dementia, DTOC, Care home scrutiny etc. is envisaged. Scrutiny The CHC visiting and monitoring functions will continue, but with Divisions reacting to local information and trends through a programme of unannounced visits in addition to routine inspections. It is important that the WWCHC should work in partnership with Health Inspectorate Wales (HIW) in order to increase the effectiveness and efficiency of these activities. There will also be a responsibility to ensure that all inspection programmes are coordinated with other agencies to avoid undue disruption and confusion. Scrutiny strategy will be coordinated by the WWCHC but delivered at Divisional level, with cross-LHB working where necessary. Insofar as HIW is concerned, the development of an information sharing protocol (particularly with regard to trends derived from CHC advocacy) and a Memorandum of Understanding will be needed. Working with HIW will not prejudice the CHC’s statutory independence. Membership The overall success of the WWCHC will be largely dependent upon the quality and commitment of its membership. Each member must receive adequate training in order to understand the role of the WWCHC and to undertake the portfolio of responsibilities that this will entail. Careful selection of members is vital, to ensure they have the time and ability to achieve the demands required of them. The membership composition in each county division must endeavour to ensure that all communities are adequately represented.

6
CONCLUSION Immediate Delivery. The above proposals will allow the Dyfed CHC Federation to deliver a workable joint strategy on 1 October 2009, but the full benefits of this new way of working cannot be achieved without additional financial resources. In the short term we have no other option than to nominate an existing Chief Officer as the Lead Officer on a rotational basis, but he/she will retain their normal county CHC responsibilities. Initially, to help with the demands of this role and as is the case at present, there will have to be sharing of regional responsibilities between county Chief Officers. We hope the Minister will find favour with this proposal by the Pembrokeshire Community Health Council as a sound and pragmatic vision of how our constituent CHCs will work within the new health structures, whilst retaining their solid local links in this largely rural corner of West Wales. This structure will need to be properly resourced both in terms of finance and members. There must be a duty on the LHB to both engage meaningfully at an early stage of the planning of service delivery and respond constructively to the results of citizen engagement and scrutiny. We welcome the opportunity to work constructively with the LHB for the benefit of the public whom we jointly serve. Mrs Christine Roberts Mr Ashley Warlow Chairman Chief Officer On behalf of the Pembrokeshire Community Health Council 28th July 2009

Cyngor Iechyd Cymuned Ceredigion
8 Ffordd Portland Aberystwyth
Ceredigion SY23 2NL
Ceredigion Community Health Council
8 Portland Road Aberystwyth
Ceredigion SY23 2NL
CEREDIGION RESPONSE TO THE CONSULTATION ON THE FUTURE OF COMMUNITY HEALTH COUNCILS IN WALES
INTRODUCTION We very much welcome the Minister’s statement of 12th May 2009 that CHCs will be retained and the clear commitment to local accountability in her statement is strong evidence that she accepts that the current pattern of CHCs should continue. We must therefore ensure that we create an innovative, vibrant and effective Council fully representing “locality” patient views and needs. We must respond to the Minister’s challenge to “reach out “to all groups interested in health issues within Ceredigion. We must retain our ability to “challenge”, scrutinise, have continuous engagement and achieve more local involvement within our County, with communities and with our partners in local government and voluntary bodies. We have looked at the Minister’s five challenges namely to:
Develop a strategic relationship with the new LHBs Achieve more local involvement within communities and with partners Ensure we are involved in continuous engagement with service issues and not just when
there is service change Scrutinise the way in which services are planned and delivered by LHBs, as well as those
services at the interface of health and social care service provision In challenging any proposed service change, consider the changes within the current
priorities, resources, statutory frameworks and governance structures, and make constructive and realistic contributions to the process. We would argue, however, that it is not the place of the CHC, as representatives of the patients, to take into account the LHB’s priorities and resources – that is their job; ours is to articulate what the patient needs.
and feel that we can deliver these within our model. AIM To outline the proposals by the Ceredigion Community Health Council, for effective joint working between the three CHCs in the Hywel Dda area. These proposals will provide a robust way of representing the interests of the public and patient in the restructured health service. They will
Ffôn | Tel: 01970 624760 Ffacs | Fax: 01970 627730
e-bost | e-mail: [email protected] gwefan | web: www.patienthelp.wales.nhs.uk/ceredigion
Cadeirydd | Chairman: Mr Jack Evershed Prif Swyddog | Chief Officers: Monica Williams Cathryn Brown

2
ensure that by 1 October 2009 we will have in place a working mechanism that meets the Minister’s five challenges for the CHCs, within existing resources and within the existing legframework (Minister’s statement 12 May 2009).
al
he Carmarthenshire, Pembrokeshire and Ceredigion CHCs have successfully worked together
he fundamental principle is to provide an effective structure to better represent the interests of
a. National Level:
Ton a federated basis for a number of years. Ceredigion CHC (as does the Dyfed Federation) wholeheartedly welcomes the opportunity to further develop and strengthen this three county relationship, with the Minister’s five challenges at the heart of our philosophy. Tthe public and patient within the Hywel Dda designated area, operating on three levels:
To work coherently and effectively within the national structure and
b.
strategy of the CHC movement across Wales. Regional/Strategic Level: To hold the Hywel Dda LHB to account through the scrutiny
c. l:of services; County Leve To further develop this critical activity through effective citizen
We envisage the 3 CHCs in the Hywel Dda area running as the current bodies looking out for
tuent
ocal
a Health Board has
on a
nisms.
ch by Hywel Dda, which reflects the
re
ywel Dda has thus planned a county – based structure, based on an Assistant Director of loped
engagement and systematic gathering of local views.
their own localities (LA areas) and being in charge of their own budgets as at present. The Federation of the 3 CHCs should be made to work more effectively by specifying the policy responsibilities which it will coordinate, and make it democratically accountable to the constiCHCs through the system of elected representation set out below. It will be responsible for strategic national and regional issues while the balance between these issues and effective lparticipation will be fulfilled through the individual local CHCs. At the heart of the county (local CHC) function will be effective and constant citizen engagement, informing of health care plans and gathering local views and concerns across this large diverse area. At a late stage in the consultation on CHC structures, the new Hywel Ddissued its own consultation paper on the way in which it plans to develop its organisational structures to provide healthcare services in the region. This recognises the diverse and dispersed nature of the 3 Counties within its area and sets out a suitable structure which provides for Acute, Community, Primary Care and Mental Health services to be delivered county basis across the region. They argue that “There is a clear separation of counties and supporting infrastructure across the existing LHBs. These clearly divide Carmarthenshire, Ceredigion and Pembrokeshire, driven by Local Authority structure and partnership mechaLHBs have achieved a strong county focus through their existing structures, and any new organisational structures will be based on the 3 counties”. We greatly welcome this enlightened and pragmatic approaphysical realities of the region. The Minister will be aware of the huge physical size of rural Mid Wales – Ceredigion alone is considerably larger than the whole of Gwent - and the distance compounded by the deficiencies of rural roads means that travelling times within the region ameasured in hours rather than minutes. HOperations in each County with the following 18 categories of functions integrated and deveat county level:

3
Partnership mechanisms and planning, including statutory requirements for HSCWB, community safety and Children and Young people support
Primary care management and planning including managed practices Hospital Management Community services including District Nursing, health Visiting and School health Intermediate care-out-of-hospital/community rehabilitation services AHP services Community Hospitals, health centres and clinics Community and salaried dentistry NHS Funded Nursing Care and Continuing Health care (retain operational delivery at
locality, but develop policy and common approaches more corporately) Chronic Condition Management teams Local Medicines management delivery, supporting practices and contractors Specialist community-based nursing services, including sexual health, the homeless, breast
care, stoma care and diabetes (and others) Continence services Health promotion (in partnership with Public Health Wales) Voluntary sector liaison Supporting Local publics engagement Patient Flow Hotel Facilities
The arguments which have prevailed within Hywel Dda are equally applicable to the CHCs, and it
e, in Ceredigion, also work and need to continue to work with Meirionnydd and Montgomery
e can meet the Minister’s five challenges by 1 October 2009 by developing our federated be
ETAILS
is thus at the county level that CHCs will need to interface with monitoring and consultation on these functional areas. WCHCs who represent their patients who use the healthcare facilities of the Hywel Dda hospital –Bronglais, in Aberystwyth. In fact, over half of residents within the catchment area of Bronglais are actually resident in Meirionnydd and Montgomery (outside the Hywel Dda boundary but not outside the area for which Hywel Dda provides health services). The Community hospitals at Machynlleth and Tywyn also provide services from the Bronglais hub. Wstructure within existing resources. This is a major constraint and further capability can only developed as the structure matures and when additional resources are provided. D
ational Level N
he Federation will maintain close links to the National Board of CHCs. Membership of the CHC
s a tters
TBoard by the Federation Chair formalises this relationship. Regular contact between Federation and the Board of CHCs is essential and this committed participation will allow regional issues or concerns to be debated on an all Wales basis and appropriate action sought from key organisations such as the National Advisory Board or National Delivery Group. There iconcern that regional representation at Board of CHCs will not be enough to ensure that ma

4
of particular concern to one county are brought fully to the Board’s attention and mechanisms of ensuring this have to be thought through. Regional Level – the Federation The Federation at the regional level – like the individual CHCs at county level - will work closely and constructively with the Hywel Dda LHB. It will hold it to account for the delivery of healthcare at the strategic level within the region and will also be intimately involved in the planning of services at the earliest stages. Health transport policy will be another role for the Federation since by its nature transport links often cross boundaries. The roles of Federation Lead Officer and Federation Chair will be undertaken on a part time rotational basis by one of the three Chief Officers and three Chairs from the local CHCs. The Federation joint committee membership will consist of 18 members composed of equal representation from the Carmarthenshire, Ceredigion and Pembrokeshire CHCs, each of whom will annually appoint 6 of its members to the Federation. The Chair of each CHC will automatically have a place on the Federation, with the other fifteen, five from each CHC, elected by the CHC at a duly constituted public meeting, and – together with the Chair of that CHC - reflecting the makeup of the CHC, i.e. representatives from the Local Authority, Voluntary organisations and Assembly appointees. The Federation will hold regular meetings in public. The meetings schedule of the Federation will be organised once the administrative structure and meeting schedule of the LHB are known. The Chair, supported by the Lead officer, will attend all Hywel Dda LHB Board public meetings and be permitted speaking rights (but not voting, to retain independence) and allowed to present agenda items - as at present. The Chair of the Federation will be the representative on the Board of CHCs. The CHCs will feed back information and findings to the Federation so that it can take a 3 County approach as appropriate to issues of finance, equity of funding and access to health services across the 3 counties. The Federation will be responsible for establishing a coherent Citizen Engagement (PPI/PPE) strategy. It will also form close links with the LHBs citizen engagement strategy to ensure there is no duplication of effort or confusion regarding the roles and responsibilities of the proposed Stakeholder Reference Group. It will also coordinate the scrutiny role of the individual CHCs within the Hywel Dda area and maintain close contact with Health Inspectorate Wales. Full Federation involvement in all Hywel Dda LHB planning matters is essential, the Federation coordinating the planning discussion with Hywel Dda LHB. The continuance of the Three Counties Planning Forum is therefore vital since this has proved to be very effective in involving all stakeholders early in the NHS planning stages in a constructive and effective manner. Representation from each CHC area is essential as local issues need to be raised and debated. One representative covering the Federation area will not have “hands on” information on 3 County issues and concerns.

5
Each CHC shall have the right to alter at a duly constituted public meeting of that CHC its elected representation on the Federation as it shall see fit, and shall be able to send substitutes for members unable to attend. County Level – CHCs Each CHC will be composed of 20 full CHC members and up to a third of its number in co-opted members. The membership composition will be as at present, with representatives from the local authority, the voluntary sector and Assembly appointees. Each CHC will elect a Chair, and two Vice Chairs from amongst its membership. The individual CHCs will ensure effective citizen engagement across a large and diverse area. They will also be most effective in engaging with Local Authorities, developing partnership working and examining ways to establish effective communication networks across health and social care. Due to the geography and large rural spread of the Hywel Dda community it is deemed essential for the CHCs to retain office premises (and access to conference facilities) in each county area - with a Chief Officer and appropriate staff. Meetings will also need to be held locally as appropriate. The CHCs will carry out the PPI and scrutiny role of the Federation and provide feedback. The CHCs will also ensure that the Federation is informed of local issues that need to be addressed at higher level and are of interest to the other two CHCs. The elected chairman of the CHC and five other members elected from each CHC will be responsible to the CHC for their involvement at regional level. All 20 members in each county will also have a clearly defined portfolio of responsibilities, to include delegated and active citizen engagement in their areas, as well as the scrutiny function. This local function will develop the community strategy so important to the new role of the LHB. Each CHC will ensure that local involvement with communities, partners and service users is expanded and that the involvement is on a long term basis. The Federation will be the initial point of contact for regional consultations. Members will be mandated to discuss the issues in detail with their own CHCs and ensure the fullest, appropriate citizens engagement by the local CHCs. The fact also remains that the LHB will be dealing with 3 Local Authorities and other County based stakeholders. The 3 LAs have different patterns of social care delivery due to 3 separate economies and the LHB will not be able to organise services unless it has a clear defined avenue of collaboration with 3 diverse LA systems. Public Patient Involvement/Engagement Strategy To engage fully and effectively with the citizens within the Hywel Dda boundary, sufficient resources, both funding and appropriately trained, capable members, are prerequisite. A coordinated, regional approach across the three counties would be achieved by the Federation supported by PPI staff. Sufficient investment in training should be made to enable members tasked with PPI responsibilities to develop and build intimate links with the community. It will be the responsibility of the Federation to liaise with the LHBs citizen engagement function whilst preserving the CHCs independence and statutory remit, particularly with regard to the
6
current Interim Consultation guidelines. The Federation will also be tasked with improving the level of citizen engagement by evolving procedures which will assist the CHCs in improving their performance. Initial thoughts would include developing Health Focus Groups, developing links to existing groups (Community Councils, Pensioners Clubs, Hard of Hearing, WI and so on and then moving towards engagement with others who are not represented by established groups or social networks (through links with drop-in centres, night shelters, mental health advocates and so on). Advocacy The CHC Advocacy Service is now a well respected service with clear, local access points in Carmarthenshire, Ceredigion and Pembrokeshire and must be strengthened and then coordinated and financed by the Board of CHCs but continue to be delivered locally. Advocacy represents a source of vital intelligence and must be adequately resourced to provide a credible, timely service to the benefit of the public/patient and NHS. CHC advocacy will be a vital element when the Redress Measure for Wales is implemented in 2010. Accountability for the advocacy function should remain with the Federation with advocates, as at present, deploying into the local CHCs as and when required to meet clients. The advocacy service is anticipated to grow to meet increasing demands and ultimately it may be expected that advocates will require to be permanently based in all three CHC areas. Partnership Working Developing links with Local Authority Health and Social Care, the voluntary sector and other stakeholders is critical and it is anticipated that this work will continue to develop across the three CHCs through the Health, Social Care and Wellbeing Partnerships. It is also important to build on existing examples of good practice. Where CHC relationships with Local Authority Health and Social Care Scrutiny Committees are already well established; experiences and lessons learned can by used to develop similar arrangements across the whole region. Further development in sectors such as dementia, DTOC, Care home scrutiny etc., is envisaged. Collaboration on certain office functions e.g. joint newsletters, leaflets and web pages can be explored in the interests of economy and effectiveness. Scrutiny The CHC visiting and monitoring functions will continue, members reacting to local information and trends through a programme of unannounced visits in addition to routine inspections. It is important that the CHC/Federation should work in partnership with Health Inspectorate Wales (HIW) in order to increase the effectiveness and efficiency of these activities. There will also be a responsibility to ensure that all inspection programmes are coordinated with other agencies to avoid undue disruption and confusion. Scrutiny strategy will be coordinated by the Federation but delivered at CHC level, with cross-LHB working where necessary. In so far as HIW is concerned, the development of an information sharing protocol (particularly with regard to trends derived from CHC advocacy, child and adult protection) and a Memorandum of Understanding will be needed. Working with HIW will not prejudice the CHC’s statutory independence.

7
Membership The overall success of the new order will be largely dependent upon the quality and commitment of its membership. Each member must receive adequate training in order to understand the role of the CHC and Federation and to undertake the portfolio of responsibility that this will entail. Careful selection of members is vital, to ensure they have the time and ability to achieve the demands required of them. The membership composition must endeavour to ensure that all communities are adequately represented. In particular ,it should reflect the fact that patients with severe disabilities, long term limiting illnesses etc constitute a far higher proportion of the patient body than those groups form in the population as a whole. CONCLUSION Immediate Delivery. The above proposals will allow the three CHCs comprising the Dyfed CHC Federation to deliver a workable joint strategy on 1 October 2009. It is understood that the other CHCs in the region have proposed a similar but more formal model with the formation of a West Wales CHC. We cannot, however, support this .Our proposals have been able to take account of the Organisational Structure proposed by Hywel Dda which fits well into the reality on the ground of providing accountable healthcare services in a sparse rural area. They also take into account our different needs for strategic involvement with other CHCs in Mid wales with whom we share an ongoing concern for acute services within the catchment area served by Bronglais General Hospital. In parallel with Hywel Dda’s proposals, therefore, we have based our proposals on a structure that retains the identity of the individual CHCs rather than merge them within an amorphous West Wales CHC which would lose both local accountability and the ability to represent patient’ concerns as regards healthcare service delivery. The sparse rural population of Ceredigion necessitates a strong individual voice to guard against possible inequalities in such health care delivery, particularly in the context of the enlarged area served by the Hywel Dda Local Health Board. It should be noted that Ceredigion has the lowest population density in the area and could thus be more prone to suffering such inequalities than the other counties. Our view is that the putative West Wales CHC has an over complex management structure and has not been properly costed out and cannot be formed within the existing legal framework and by 1st October as the Minister requests. We hope the Minister will find favour with this proposal as a sound and pragmatic vision of how our constituent CHCs will work within the new health structures, whilst retaining their solid local links in this largely rural corner of West Wales. This structure will need to be properly resourced both in terms of finance and members. We welcome the opportunity to work constructively with the LHB for the benefit of the patients and public which we jointly serve.

Final Draft 1
THE FUTURE OF COMMUNITY HEALTH COUNCILS IN WALES
A PROPOSAL FOR JOINT WORKING WITHIN THE NORTH WALES
COMMUNITY HEALTH COUNCILS
INTRODUCTION Community Health Councils (CHCs) in North Wales are in receipt of correspondence from the Minister for Health and Social Services and the Director of NHS Wales requesting further proposals for joint working to be submitted by the end of July 2009. These proposals should adhere to the principles outlined in the Minister’s Direction to CHC Chairs – SF/EH/0237/09 dated 14 May 2009. In response to the consultation, the North Wales CHCs’ Joint Committee submitted a proposal for a model which demonstrated how CHCs in North Wales could successfully interface with the new Betsi Cadwaladr University Local Health Board (BCULHB). This joint proposal was formulated on the basis that the North Wales CHCs’ Joint Committee has been an effective model for partnership working between the CHCs in North Wales. Subsequent to the letters received from the Minister and the Director of NHS Wales, the North Wales CHCs’ Joint Committee met on Wednesday 3 June 2009 to discuss the way forward. The North Wales CHCs’ Chief Officers again met on 30 June and 6 July to formulate a proposal, based on the discussions in the Joint Committee, for further consideration and ratification by the North Wales CHCs prior to submission to the Minister. It is with regret that following this series of meetings and discussions no consensus has been reached by the North Wales CHC members as to the way forward. However, the proposals have been agreed and accepted by Denbighshire, Flintshire, Wrexham, Gogledd Gwynedd, Meirionnydd and Ynys Môn CHC members and as such we submit the following proposal for consideration by the Minister. We understand that Conwy CHC intend to make an individual submission. This proposal can be implemented by 1st October 2009 and will provide a single coterminous mechanism for the CHCs in North Wales for the interface with the BCULHB. The proposal is within the current legal framework and within the original financial allocations and will:
• ensure continuity of services provided by the CHCs • achieve efficient and effective use of resources • be strategic as well as being representational • increase visibility to the public and partners • enhance local engagement • ensure a unified Citizen voice • promote a strong partnership culture through increased collaboration • be outcome focused in scrutinising equity of health care
This model is also flexible and adaptable with the ability to evolve over time through collaborative working. When vacancies arise and current leases expire,

Final Draft 2
we will explore the feasibilities of consolidating premises and further sharing resources. PROPOSED MODEL (See Appendix A) We propose to form a North Wales CHCs’ Joint Committee (‘the Joint Committee’) coterminous with the Betsi Cadwaladr University Local Health Board. The Joint Committee will comprise representation from:
• Clwyd CHC (Denbighshire Flintshire Wrexham Area Committees) • Conwy CHCs (East & West) • Gogledd Gwynedd CHC • Meirionnydd CHC • Ynys Môn CHC
Structure: The Joint Committee will be made up of
• Members providing equal representation from the CHCs. The Chair of each CHC will automatically have a place on the Joint Committee with the remainder elected to reflect the make-up of the CHCs i.e. Representatives from Local Authorities, Voluntary Organisations and Assembly Public Appointments.
• A dedicated Lead Officer with appropriate support staff who will be the main contact between the BCULHB and the North Wales CHCs. This however cannot be achieved by 1st October due to lack of resources and in the short term will be nominated from the existing CHC Chief Officers in North Wales.
• A Chair and Vice Chair of the Joint Committee to be elected by the membership of that Joint Committee and may serve a maximum of two years.
HOW WE WILL WORK On a National Level To work within the overarching CHC framework for Wales a member of the Joint Committee will be elected as the North Wales CHCs’ representative on the Board of CHCs. On a Regional Level To ensure that the Joint Committee is fully engaged with the planning and delivery of services there will be two mechanisms established under its umbrella:
a. Service Planning Committee (to include the BCULHB’s Director of Planning and other such Directors as deemed appropriate as well as members drawn from the Joint Committee. This newly established Committee will be the vehicle for ensuring CHC involvement from the onset in all aspects of planning and delivery of services in North Wales by:
o Securing a strong level of scrutiny o Ensuring that the BCULHB is responsive to the needs and
views of its citizens o Ensuring that the principles of the Interim Revised NHS
Consultation Guidance are adhered to.

Final Draft 3
o Ensuring that the Citizen Centred Governance principles are the core focus for the BCULHB
b. Operational Team which will comprise members and officers with interests
in specific areas of healthcare provision, for example rural health, primary care, neurology services, and which will meet at regular intervals. The Operational Team will be the information conduit to the Service Planning Committee. Sub Committees will be established which will feed into the Operational Team e.g. Communication, Equality & Diversity, Visiting Monitoring
It is vital that a balance is struck between the needs of local CHC communities and the needs of the regional community as a whole. The Service Planning Committee will be the vehicle for securing a strong level of scrutiny ensuring that the BCULHB is responsive to the needs and views of its citizens in the planning and delivery of health services. Further, this committee will need to assess the impact of proposed changes to the NHS and not take a partisan role. Engagement by CHCs at local level (identified below) will be fundamental in providing a firm foundation for determining and developing the Joint Committee’s strategic response to any proposals made by the BCULHB. Standing Orders for the Service Planning Committee will be drafted, identifying key responsibilities and an operating framework. The frequency of meetings will need to be co-ordinated and aligned with the BCULHB and the Board of CHCs in Wales. Meetings of the CHCs’ Committees will be co-ordinated and aligned to Joint Committee meetings. We propose that the Chair and Lead Officer of the Joint Committee should attend all BCULHB public meetings and should be permitted speaking rights, but no vote so as to safeguard independence. Identifying Issues to be addressed regionally The issues we would expect to be addressed jointly will relate to:
• Welsh Assembly Government policies • National & Regional Consultations • Standards of service delivery • Equity of service provision across North Wales
These will be identified by:
• Monitoring visits • Gathering feedback from the Complaints Advocates, members groups and
continuous public engagement. • Cross border service issues • Issues raised by CHCs in other areas outside North Wales
On a Local level Engagement at a local level will be fundamental in providing a firm foundation for determining and developing the Joint Committee’s strategic response to any proposals made by the BCULHB

Final Draft 4
The local CHCs will be the critical public interface of the Joint Committee to ensure continuing and effective Citizen Engagement across a large and diverse region. This will fulfil the Minister’s vision of placing CHCs firmly in the role of the “Voice of the Community” with an obligation to demonstrate how we have gathered and represented that voice. In addition, within that presence, would lie the Complaints Advocacy service and other enquiries received about service provision serving as a barometer for service improvement. The results of this engagement will be fed into the Joint Committee via the Operational Team to inform the Joint Committee’s direction of travel with the BCULHB. We have established strong and effective partnerships with our stakeholders in North Wales over the years. These will need to be maintained and strengthened to enable continuous engagement with: § The Health, Social Care & Well Being Partnerships § Children and Young People’s Partnerships § Clinical Networks § County Voluntary Councils § Citizens Advice Bureaux § County, Town and Community Councils § Citizens Panels § AMs and MPs § Social networks § Communities First § Individuals not represented by established groups or social networks (This list is not exhaustive and is for example only)
It is recognised that we will need to become more proactive in engaging with the hard to reach, ethnic and diverse groups. North Wales CHCs are individually and collectively committed to expanding our conversation with and inclusion of under-represented groups but we realise that this cannot be done instantly and requires planning and imagination. We understand the key role of various initiatives across North Wales and have identified how these already link in to our communities. The thinking behind ‘Building Strong Bridges’ – which links the voluntary sector to the NHS and Local Authority - can be adopted and implemented by North Wales CHCs. We need to have continuous and effective engagement with groups such as the Homeless and Domestic Abuse Forum as well as strong links with the North Wales Race Equality Network. We will be more robust in gathering and reflecting the citizens’ voice and encouraging CHC members to build upon their existing links with local community groups. Investment in training and empowering members with the PPI and communications portfolio supported by their local Chief Officers will enable them to develop their existing links and forge new links within the communities. It will be essential to develop close liaison with the BCULHB’s PPI and communications functions.

Final Draft 5
Identifying Issues to be addressed locally Where local proposals / issues need to be discussed, the relevant local CHC will liaise directly with the designated officer or person of the BCULHB who has the responsibility for the provision of health care services for the relevant locality. Conversely if the Health Board wishes to discuss local issues, contact should be made with the Chair/Chief Officer of the relevant CHC via the Lead Officer. It proposed that each of the CHCs will be composed of 16 full CHC members. Scrutiny and Partnership Working Scrutiny will be co-ordinated by the Joint Committee and undertaken at local CHC level. CHC visiting and monitoring functions will remain to enable us to address urgent issues and monitor trends collectively. The development of Memoranda of Understanding with HIW, other inspecting bodies and BCULHB will be formulated. Resolution of disputes between CHCs The purpose of establishing the Joint Committee is to encourage and facilitate closer working across all the CHCs of North Wales. It is inevitable that from time to time disagreements may arise so it is important to establish a clear process for dealing with such issues as quickly as possible. The purpose of these guidelines is to explain how the Joint Committee will resolve any disagreements. Resolution of differences The Joint Committee makes it clear that all members have the right to raise concerns, be listened to positively and receive a response. Members can raise concerns individually or on behalf of their Community Health Council. The process for addressing disagreements is as follows: Stage1: Where the Joint Committee has failed to reach an agreement all parties should meet in the first instance to clarify the situation. Stage 2: If an agreement cannot be reached at stage 1, contact should be made with the Board of Community Health Councils to request an independent person (Director or Chair of another Community Health Council) to meet with the Joint Committee to review all information available, look at what steps have been taken to address the concern and suggest actions which could be taken to resolve the disagreement. The independent person will make recommendations and present these to a meeting of the Joint Committee. Stage 3: If the disagreement is still not resolved by the end of stage two, the independent person may recommend referral to a review panel made up of representatives from the Board of CHCs. The panel should be chaired by a representative from outside of North Wales and will look at the evidence to see if all parties have received a fair hearing, and/or if there is an alternative way to resolve the disagreement. It will make recommendations to the Joint Committee. The Review Panel will make recommendations based on:

Final Draft 6
• A review of available documentation • The procedures followed to date • Consultation on how disagreement may be resolved resulting in
written agreement/action plan • Feedback into wider CHC membership on how relationships may be
reviewed/improved The decision of the Review Panel will be binding. Conclusion This proposal gives an excellent opportunity for the CHCs in North Wales to collectively identify further innovative solutions for streamlining our functions and tackling issues jointly e.g. pooling knowledge/resources and developing a single communication and engagement strategy for North Wales.
In the short term and within the current legal framework and resources we will have to nominate an existing Chief Officer as the Lead Chief Officer but he/she will retain their individual CHC responsibilities. Initially, to assist with the demands of the Lead Chief Officer role and, as is the case at present, there will have to be sharing of regional responsibilities and a reassignment of tasks between local CHC Chief Officers. VISION FOR THE FUTURE As previously stated, our proposal will ensure that by 1st October 2009 we will have in place a working mechanism that achieves the Minister’s five key principles for CHCs and our aim is for the model outlined in appendix A to work successfully. We see this as an evolving model which will be developed through collaborative working. Consideration can be given also in the future to regulatory changes to the current statutory Federations of Conwy and Clwyd to enable operational restructuring if deemed necessary towards a Federated model which retains solid local links. We would aim to work towards the implementation of the model shown in appendix B by March 2012. The North Wales CHCs bring together a diverse range of staff and volunteers with a wealth of experience of health services and patient focus and public involvement. From this strong base, we have the opportunity to evolve a shared culture and organisational identity that is grounded in the strengths of the past and looks positively and creatively to the future. The values of the North Wales CHCs include commitments to: § Patient and public involvement including people from all equality groups, in
the development of all aspects of healthcare § Acknowledge and celebrate success and build upon skills and experience § A solutions-focused ‘can do’ culture where CHC members and staff work in
mutually supportive teams § Value members and staff, and their ‘expertise by experience’

Final Draft 7
§ Work across local and regional boundaries so that we have the skills of the right person, in the right place, at the right time
§ A ‘learning as growing’ organisation that values ability and offers opportunities to develop
As an organisation we will make a difference to the effectiveness of citizen engagement and thereby influence the strategic direction of the NHS in North Wales. Both members and staff are committed to make that difference a reality. Document agreed on 28 July 2009
Signed by Roy B. Davies, Clwyd CHC Federation Chair on behalf of the Chairs of Clwyd CHC (Wrexham, Flintshire & Denbighshire Area Committees) Gogledd Gwynedd CHC Meirionnydd CHC Ynys Môn CHC

Final Draft 8
Clwyd Community Health Council Administrative Office
Conwy West CHC
Gogledd Gwynedd
CHC
Operational Team
Sub Committees
Appendix A: Organisational Structure of the North Wales CHC’s from 1st October 2009
BETSI CADWALADR UNIVERSITY HEALTH BOARD
North Wales Community Health Councils Joint Committee Members representing local CHC’s
Lead Chief Officer
Services Planning Group
Conwy East CHC
Meirionnydd CHC
Ynys Mon CHC
Denbighshire Area
Committee
Flintshire Area
Committee
Wrexham Area
Committee

Final Draft 9
Appendix B: Organisational Structure of the ‘Vision of the Future’ for North Wales CHC’s
North Wales CHC’s (Regional Administrative Office(s)) Support Staff
Advocacy Service PPI Staff
Conwy CHC
Flintshire CHC
Denbighshire CHC
Wrexham CHC
Gogledd Gwynedd
CHC
Ynys Môn CHC
North Wales Community Health Councils Joint Committee Lead Chief Officer
Regional Chair Chairs of CHC’s and Members
Operational Team
Services Planning Group
BETSI CADWALADR UNIVERSITY HEALTH BOARD
Meirionnydd CHC
Sub Committees

Chairman: Mr M J Graham 30 July 2009 Mr Steve Davies Patient Experience Team Quality, Standards and Safety Improvement Directorate Department for Health and Social Services Welsh Assembly Government Cathays Park Cardiff CFlO 3NQ Dear Mr Davies Re: Brecknock and Radnor CHC Response to the Minister's Statement on the Future of Community Health Councils We are pleased to forward the proposals of our Community Health Council to the document. However, my colleague Mr John Howard, is on sick leave at the present time and we are, therefore, unable to put together a Federation response. Having said that, my Chairman, Mr Monty Graham, met with the Chairman of Montgomery CHC today and there would appear to be a good working relationship developing between them. As a result of their efforts a Federation meeting is likely to be called over the next couple of weeks where representatives of both councils will look to come to a conclusion on the best organization for CHCs in Powys. You will consequently be receiving another document which represents the views of both CHCs. Yours sincerely Bryn Williams Chief Officer

POWYS FEDERATION OF COMMUNITY HEALTH COUNCILS Consultation on the Future of Community Health Councils in Wales In response to the Minister’s, Mrs Edwina Hart MBE, letter of 14 May 2009 and the letter from Paul Williams, OBE Director General Department of Health and Social Services, regarding the future of Community Health Councils in Wales the following represents the Powys Federation of CHC’s proposals. The Brecon and Radnor and Montgomery CHCs have now had the opportunity to discuss the way forward in Powys which reflects on current practice and follows the guidance set out by the Minister. “ensuring a strategic relationship with the new LHB”
- This will be achieved through the formal meetings with Senior Officers of the Powys LHB, also with the Powys LHB Planning Officer and the Powys Federation of CHCs on a quarterly basis as set out in the original consultation document.
- The two Chief Officers will attend the Powys LHB Board meetings as at
present and other strategic/policy groups as appropriate, again as at present.
- CHC Members will continue to serve on Powys LHB planning groups.
- Establishing a Powys Federation of CHCs that fits into the Powys LHB and Powys Local Authority.
- Ad hoc meetings with Senior Officers that are specific to the CHC area.
- Continue the policy/strategic involvement with the LHB on the
interrelationship with out side commissioners and providers. “achieving more local involvement within communities and partners”
- This will be achieved through the Local Health Focus and Patient Participation groups already established in the small local towns in Powys and continue to develop the philosophy and perspective – for details see attached document.
- Agreeing a work plan in conjunction with the Powys LHB Patient & Public
Involvement Committee at CHC organised meetings and issues to be discussed at the Health Focus Groups.
- Attendance of LHB officers as necessary to discuss issues relating to the
proposed changes to NHS services.

2
- Feedback from Health Focus Groups activities to the Powys LHB PPI
Committee and local authority.
- Continue process of seeking the local peoples views on consultation documents..
“ensuring continuous engagement with service issues and not just when there is a service change”
- This will be done through the bi-monthly meetings of the Health Focus Groups as at present, embracing future and present services in an interactive and proactive way which creates the environment of cooperation.
- Feedback from LHB meetings and Planning Officer quarterly meetings to the
Health Focus Groups.
- As part of the CHC and LHB PPI work plan.
- As part of the CHC members being on the LHB Planning Groups and feedback to the Health Focus Groups.
“scrutinising the way in which services are planned and developed by LHB’s as well as those services at the interface of health and social care service provision”
- By continued membership of CHCs on planning groups, integrated workforce planning and development networks.
- By continued membership and participation on policy groups such as health
and social care joint executive committees.
- The CHC has established groups who conduct an agreed annual work plan to visit a range of NHS service provision and premises eg hospitals, both in Powys and bordering hospitals; GP Practices/Health Centres, Day Services, Pharmacies, Dentist Practices, Nursing Homes, etc.
- As CHC membership on Health, Social Care developments in Powys eg
Builth Wells, Llanidloes, Knighton Project Boards.
- Through County Council members on the CHC, relating to Social Care Services and changes.
- As members of the LHB groups to visit hospitals to look at issues such as
cleanliness, food, etc.
- By quarterly meetings of the Federation with the LHB Planning Officer.

3
- As a CHC member of the Partnership Board with LHB, Local Authority and
Voluntary Sector, etc.
- Through the CHC Advocacy Services who visit and talk to people in health and social care settings and feedback into the CHC Advocacy Management Group.
“in challenging any proposed service change considering those changes with the current priorities, resources, statutory framework and governance structures and make constructive and realistic contributions to the process.
- Through the continued CHC membership of the LHB Planning Groups it would be hoped to influence the outcome of proposed changes at this level. Participation and logical debate follow the process in pluralistic outcomes.
- These changes would be part of the work plan of the Health Focus Groups and
their views will be represented back to the Planning Group and to the meetings of the Federation and Planning Officer meetings.
- The CHC would expect as at present to discuss future changes and plans at the
quarterly meetings of Senior Officers of the LHB.
- Peoples views would be taken back via the CHC representatives on the LHB PPI Committee.
- By CHC involvement in the planning process CHCs would wish to make
constructive and realistic contributions based upon the views of the local population.
- As part of the meeting with Senior Officers of the LHB, the CHC would
continue to discuss current priorities and resource availability.
- The two CHCs already have a good working relationship with the Chairman, Chief Executive and Senior Officers of the LHB and local authority, meeting on a regular basis to discuss health related matters.

Proposal Draft
Powys Federation of Community Health Councils
Brecknock & Radnor
And
Montgomery
Community Health Councils
Contents
Page
1 Outline of structure of Community Health Councils in Powys
2 Powys Federation of Community Health Councils 3 Two Community Health Councils in Powys Brecknock & Radnor and Montgomery CHCs 4 Health Focus Groups

Outline of Structure of Community Health Councils in Powys
Powys Federation of Community Health Councils
Montgomery Brecknock and Radnor Community Health Council Community Health Council Local Health Focus Groups Local Health Focus Groups Montgomery Brecknock and Radnor

Powys Federation of Community Health Councils
Membership - Chair, Senior Vice Chair and Vice Chair + 2 members of Montgomery and Brecknock & Radnor CHC
- 2 Chief Officers of (Montgomery and Brecknock & Radnor CHC) Meetings - To meet on a bi-monthly basis in Llandrindod Wells with agenda, minutes,
etc.
Chair - 1 year Brecknock and Radnor with Vice Chair Montgomery alternating year Montgomery Chair, Vice Chair Brecknock & Radnor.
Secretariat to be shared by both Chief Officers. Role and Function - To collectively respond to strategic consultation documents as
necessary.
- To collectively respond to Powys LHB on Powys wide consultation Documents as necessary.
- To respond collectively to Welsh Assembly Government consultation documents as necessary.
- To respond collectively to other appropriate consultation
documents as necessary. - To agree agenda items and issues to be discussed at quarterly
meetings with the LHB and attend meetings. - To agree agenda items and issues to be discussed at quarterly
meetings with the Powys LHB Planning Officer and attend meetings.
- To agree annual work plan for the Federation. - To produce an annual report of the Federation work - To agree Vice Chair of Federation to attend Board meetings and be
responsible for feeding back to committee. - To share best practice across the two CHCs. - To look at joint working practices between the 2 CHC offices and
to look at best use of resources.

Two Community Health Councils in Powys
Montgomery CHC Brecknock & Radnor CHC 1 Chief Officer + office support staff 1 Chief Officer + office support staff Office in Newtown Office in Brecon 1 Chair, 1 Senior Vice Chair 1 Chair, 1 Senior Vice Chair, 1 Vice Chair + 17 members 1 Vice Chair + 17 Members 1 Complaints Advocate 1 Complaints Advocate To meet on a bimonthly basis To meet on a bimonthly basis or more frequently if necessary or more frequently if necessary. Role and Function of Each CHC - To be overall responsible for the work of the local CHC - To agree the work plan of the local CHC - To respond as appropriate to consultation documents as it effects the local CHC and its
residents. - To oversee the work and running of the local Health Focus Groups and work closely with
the Powys LHB PPI Committee. - To work closely with the Federation and have regular feedback between the Federation
and each CHC. - To contribute local CHC views into Federation responses to consultation documents. - To receive reports from quarterly meetings with the Powys LHB and Powys LHB
Planning Officer meetings. - Each local CHC be responsible for their local CHC budget. - Be responsible for the work of the local Complaints Advocacy service.

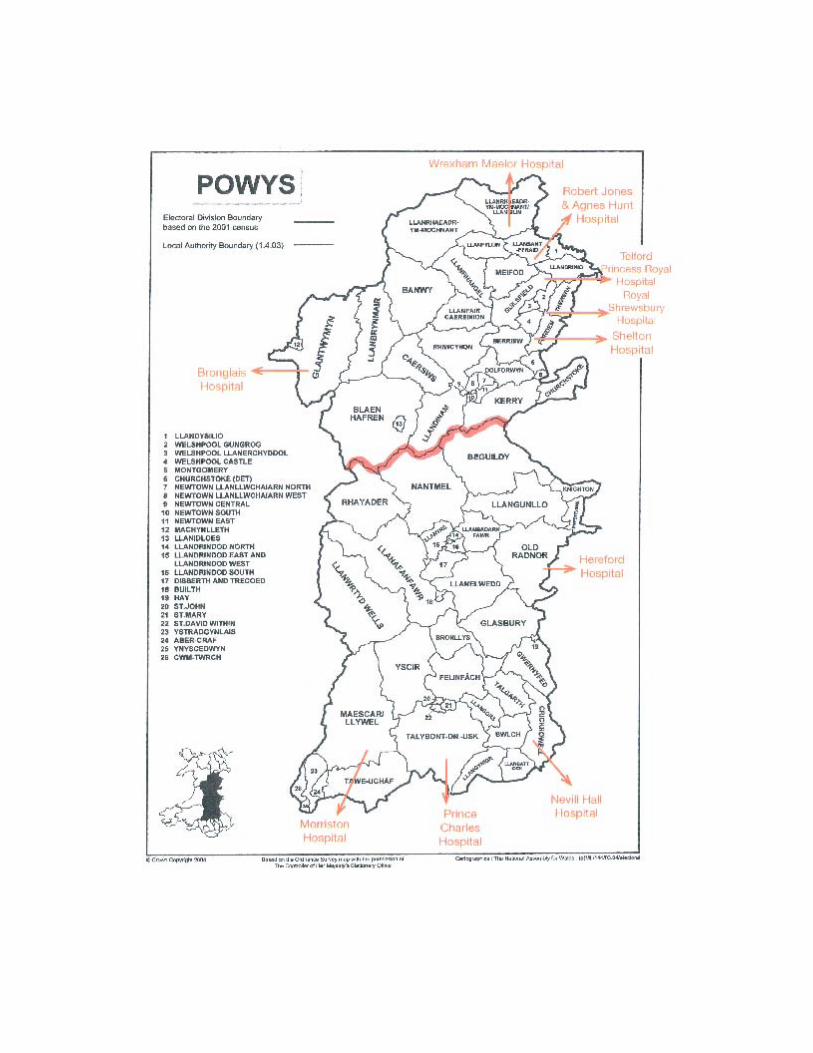
Health Focus Group (HFG) Health Focus Groups have been set up and running for a number of years in: Ystradgynlais Builth Wells Brecon Rhayader Crickhowell Knighton Hay-on-Wye Llandrindod Wells Talgarth (Include Montgomery Groups) The role of the HFGs is to enable members of the local communities to have an opportunity to:
1 Make their views known on the delivery of NHS service in Powys.
2 Be made aware of changes in the way the NHS services are or may be changed both locally and nationally.
3 Be engaged and make their views known on health related consultation documents
both locally and nationally.
4 Presentation by senior officers of Powys LHB where the Health Focus Group wish to have information on services or intended future developments. Also, when Powys LHB wish to seek the views of the general public.
5 Raise issues they wish the CHC to bring to the attention of the Powys LHB and Local
Authority.
6 Be engaged in the process for any significant service changes at the local community hospitals.
7 Express their views on GPs Primary Care services which the CHC can take up with
GP Practices or Director of Primary Care, Powys LHB. Practice Managers attend the meetings if requested to discuss local GP services.
8 To be engaged with the Powys LHB planning process at a very early stage not at the
end stage.
9 Speak to senior officers of the LHB as and when required for regular rapport and creation of informal/formal relationships with the CHC.
10 To make the Brecknock & Radnor Montgomery CHCs aware of issues that are
important to them about the NHS in Powys, bordering DGHs, also across social and environmental issues affecting the wellbeing of the population.

Funding/Accountability The Powys LHB part fund the Brecknock & Radnor and Montgomery Health Focus Groups to the tune of £10,000 for each CHC. The Chairs and Chief Officers attend and report back to the Powys LHB PPI Committee on the activities of the HFGs. In addition the CHC and the PPI Committee agree work plans for issues the LHB would wish the HFG to be involved. Members of the LHB Board attend some of the HFGs to discuss issues and listen to the views of the people attending the HFGs. The groups meet on a bimonthly basis in a local community, eg School, Town or Community Hall, etc. Minutes and agenda are sent out with supporting paper to those who regularly attend with approximately 20 to 30 being circulated. The meetings are open to all members of the community and can and are held both in the afternoon and evenings and last about 1½ to 2 hours. The meetings are publicised in the locality. The following topics are just part of the agenda items discussed by the above HFGs with responses being made available to the statutory agencies and reflected in outcomes.
- Non Emergency Patient Transport - Cross Border NHS services - Podiatry/nail cutting - Diabetic Retinopathy Screening Services - Shropdoc Out of Hours services - Health Inspectorate Wales Reports - Delayed Transfers of Care (DToC) - Delivery of the New NHS for Wales Consultation Documents - CHC Reorganisation - Consultation - Minor Injury Units Powys - Welsh Affairs Committee Cross Border Services in Wales - Unscheduled Care – Pat Roberts and Donna Bale presentation by LHB - Safe Solutions for Rural Wales - Hospital food - Hospital cleanliness audits - Delivering non-surgical cancer services South East Wales - Update on Builth Hospital working parties - Health Inspectorate Wales draft work programme - Powys LHB reports:
• Executive Team Reports • Partnership Planning update

• Financial performance update • Governance Risk Management
- Bowel Screening Wales - First Responder/Hearstart - 1000 Lives Campaign - Home Maintenance Adaptations for older people - Management of Mental Health & Learning Disabilities services - Presumed Consent for Organ Donation - Hereford Hospital services - Nevill Hall Hospital services/Clinical Futures - Stroke Services Powys - Satellite Unit for South East Wales - Paying for Care in Wales – consultation - Eating Disorders Pathway for Wales - Ambulance Service and performance in Powys/Wales - GP services and results of Patient Questionnaires - Out of Hours/Emergency Care - Immunisation and vaccination update action plan - All Wales review of the Management of Patients with Diarrhoea and Vomiting - Feedback from CHC hospital visits - Circulation of Powys LHB Health Focus newsletter - Powys LHB Infection Control Strategy 2008-2011 - Transitional Project Board Terms of Reference and Membership. - Bronglais Hospital - Robert Jones & Agnes Hunt Hospital

POWYS FEDERATION OF COMMUNITY HEALTH COUNCILS
FOCUS ON HEALTH GROUPS
TERMS OF REFERENCE 1. AIM
To establish independent focus on health groups to: (i) enable local people to input to the Local Health Board (LHB) and others on
health and related matters; (ii) provide local people with opportunities to review the services
commissioned or provided by the LHB; (iii) to ensure a partnership approach to providing a good quality health care
and access to services and to build upon the mutual trust and respect of those partners;
(iv) support the LHB to be responsive and accountable to the community it serves and monitor the duty to involve and consult
(v) actively engage in the planning or any changes being considered by Powys LHB and DGHs who provide services to Powys residents, eg Shrewsbury, North Wales LHB, Aneurin Bevan LHB, and Hereford.
2. OBJECTIVES
2.1 To offer local residents, or those registered with a GP in the area a means of influencing the planning and provision of health care services;
2.2 To support meaningful public involvement by:
taking a broad and inclusive approach to membership of focus groups; enabling members to develop their skills, understanding and
effectiveness; developing an action focus, working to improve the public’s health and
quality of life.
2.3 To draw on the skills and operating framework of the Community Health Council in establishing and developing the Health Focus Groups;
2.4 To work with health, voluntary and community organisations in the development of the Health Focus Groups;
2.5 To share experiences with other Health Focus Groups.

2.6 Involve key members of the locality
2.7 Attempt to include hard to reach groups, such as young people, etc;
2.8 Harness skills and experience already present in the locality and Community Health Council.
3. MEMBERSHIP
The membership to reflect a broad cross section of the community in age, social status, social and medical need.
4. PROCEDURES
4.1 The Focus Groups will meet as required but not less than bi-monthly.
4.2 The Forum will elect a Chair.
4.3 The CHC staff will administer and service the Focus Groups.
4.4 Senior NHS staff in Powys may be requested to attend Forum meetings with suitable advance notice.
5. WORK PROGRAMME
5.1 The Focus Groups will develop a work programme taking particular account of feedback from local people and of major changes/developments.
6. ACCESS
6.1 The Focus Groups will draw on the CHCs current rights of access to NHS services.
6.2 Focus Group members will not have access to individual patient information, including identifiable complaints, and will be required to observe patient confidentiality at all times. Neither will they have access to workforce information relating to individual members of staff, their remuneration and terms of service, or other personnel matters.
7. SERVICING, SUPPORT AND TRAINING

7.1 The CHC, by prior arrangement, will provide a suitable venue for Focus Group meetings.
7.2 The Focus Group will be serviced and supported by CHC staff: Chief Officer or other staff, including the production of reports or visits, surveys and other Focus Group activities.
7.3 Training opportunities will be identified, to increase member’s skills and understanding of how local health services are provided, and of local health issues. joint training will be provided between CHCs in Powys.
7.4 The LHB will nominate a senior member of staff to liaise with the CHC Chief Officer on a regular basis about Health Focus issues.
7.5 The chair of the Focus Group will be co-opted on to the CHC Council.
8. REPORTS
8.1 Regular reports and minutes of the Health Focus Group will be presented to the CHC for action. Relevant reports from CHC members will be passed to the Health Focus Group.
8.2 The LHB will receive and respond to written reports from the Focus Group.
8.3 Reports will also be made available to the Health and Local Authority Partnership.

Future of Community Health Councils in Bridgend, Neath Port Talbot and Swansea
Following the presentation on 12th May 2009 on the way forward as a result of
the consultation on the ‘Future of Community Health Councils in Wales’ by the
Health Minister, letters were sent on 14th May from the Minister and Director
General. Both letters requested joint proposals from CHCs falling within the
new LHB area. The relevant body being Abertawe Bro Morgannwg University
LHB (ABMU LHB).
Bridgend CHC members were circulated with the Minister’s statement,
Minister’s letter and Director General’s letter on 22nd May and the matters
discussed at the CHC’s Executive Committee meeting held on 2nd June 2009.
The meeting concluded that it would not be possible for a joint proposal from
the current structure to realise the challenges being laid down. It was resolved
to form proposals based on the Gwent CHC model.
The new structure could be called the Morgannwg Community Health Council.
The Attachment provides an outline of how the structure might look. The
structure would retain the identities of Bridgend, Neath Port Talbot and Swansea
in the form of Area Committees. It is important the Area Committees have equal
membership (16 each). These members would have full CHC status and be
recruited from the local area that they serve.
The CHC Executive Committee (see Attachment) will comprise the Chair and
Vice Chair of each Area Committee plus the Chair, Vice Chair and Junior Vice-
Chair of the CHC.
The members of the Area Committee will form the Morgannwg Community
Health Council (16 x 3 total 48). The Chair, Vice Chair and Junior Vice-Chair
would be elected from CHC membership. Similarly, the Chair and Vice-Chair
of each Area Committee would be elected by the local Area Committee body.
The Chair, Vice Chair and Junior Vice-Chair would not be officers of the Area
Committees, enabling them to take a strategic role for the CHC.
New CHC – Future of Community Health Councils 2009

The Chair of the CHC would represent the CHC on the newly-constituted Board
of CHCs in Wales as one of the 7 representatives.
Letter from Paul Williams – 14th May 2009
Having now described proposals above for the way forward for CHCs aligned
with the new ABMU LHB structure, it would be useful to indicate how the
proposed model could deal with the 8 bullet points raised in the Director
General’s letter.
1. Looking at the most effective way for CHCs to discharge their
functions and taking the opportunity to examine where these can be
streamlined/tackled jointly.
The Morgannwg CHC model would deal with this effectively as this
configuration could look at issues strategically across the new LHB area.
The CHC and its Executive Committee would tackle issues on an ABMU
LHB basis.
2. Practical and innovative proposals for the systematic gathering of
local views across the whole of the community.
It is envisaged that the proposed CHC would work closely with local
bodies such as the Council for Voluntary Services (CVS), Communities
First and Community Town Councils in looking at schemes for the
gathering of local views.
3. How will you identify which issues are to be addressed jointly?
Under the proposed model of one CHC this would not be a problem. The
Executive Committee would make recommendations to the CHC on how
issues would be addressed.
New CHC – Future of Community Health Councils 2009

4. How you intend to respond to proposals from LHBs on a local and
strategic level.
Area Committees would respond to local proposals and the Executive
Committee/CHC would respond to strategic issues.
5. The mechanism(s) you intend to use to effect the joint working
arrangements, whether through the creation of joint committee of
the CHCs or other methods.
It is proposed the new structure (see Attachment) is established, these
issues would not be relevant.
6. The selection method for membership of any joint committee.
Under one CHC there would be no requirement for joint committees.
7. The proposed proceedings (frequency of meetings, etc).
The 3 Area Committees would feed into the Executive Committee which
would make recommendations to the full CHC. It is proposed the area
Committees meet every 6 weeks, Executive Committee every 6 weeks
and full Council meetings quarterly.
8. How you intend to resolve disputes between CHCs.
Under the proposed structure, disputes between Area Committees would
be resolved at Executive Committee/CHC level.
We feel strongly that resolution of disputes under any joint committee
structure will not be realised.
New CHC – Future of Community Health Councils 2009

PROPOSAL RE THE CREATION OF
MORGANNWG JOINT COMMITTEE OF COMMUNITY HEALTH COUNCILS
INTRODUCTION Bridgend, Neath Port Talbot and Swansea Community Health Councils cover an area coterminous with that of the newly created Abertawe Bro Morgannwg University Local Health Board. This proposal is in response to the invitation to Chairs of CHCs in the Minister’s letter dated 14 May 2009 (as amplified by the Director General’s letter of the same date) to submit plans for effective joint working by the end of July 2009. BACKGROUND Federations were set up in April 2000 at the behest of the then Health Minister in the UK Government, Mr Alun Michael. The Morgannwg Federation followed the “loose federation” model whereby the constituent CHCs retained their separate statutory status while working together on issues of joint concern. A constitution was agreed with an Executive Committee whose members comprised the Chair plus two members of each CHC with Chief Officers in attendance. The secretariat for the Executive Committee is provided by the Federation Lead Officer (one of the CHC Chief Officers) with administrative support by his/her Office Manager. Membership of the Executive Committee is limited to a period of two years (or so long as the holder retains the chair of their own CHC). The Chair/Vice Chair of the Committee rotates each year between the three CHCs. The Executive Committee meets quarterly, while the Federation as a whole (comprising all members of all three CHCs) meets annually. The Annual Meeting takes the form of a seminar. They are themed with a presentation followed by a debate. Speakers in recent years have included the Director of the Stroke Association and the Director of the Board of CHCs in Wales.

2 In August to October 2000, the three CHCs moved into shared premises in Suite B, Britannic House, Llandarcy, the offices being equidistant in the area covered by the Federation. In April 2006, following agreement from Welsh Assembly Government, Bridgend CHC moved out to return to Bridgend where they had an office prior to the relocation to Llandarcy. It should be noted that while they have operated as a “loose” Federation, the CHCs have, of their own volition, worked jointly on matters such as the management and execution of the Hospital Patient Environment exercise and campaigning for the improvement of stroke services in Wales. The Federation also has a structured approach to the management of the Complaints Advocacy Service with bi monthly meetings of the complaints advocates with the Chief Officers and regular reporting/analysis of issues and trends. It is our belief that the current close working relationship of the three CHCs, the current Federation model can be developed so as to provide a revised model which meets the objectives set out in the aforementioned letters. The following is an extract from Swansea CHCs response to the Welsh Assembly Government’s proposals to change the structure of the NHS in Wales, which would strengthen the argument to retain separate CHCs:
• “While the new LHBs/Trusts will be providing secondary services to larger populations, community services will still be delivered locally by partnerships involving health bodies AND the locally based providers of social care – namely the elected Local Authorities and Voluntary Organisations. These social care providers, as elected and community based bodies, are closely in touch with the local electorate and their needs – as were the old Trusts and LHBs. There will be a need to strengthen the lines of communication between the local providers and the new health bodies. Again, Community Health Councils will be the appropriate organisation to assist communication between these community providers and the enlarged LHBs and to feed back the users’ experiences of community (health and social) care. In this way, it will be possible to take an overview of needs, plus the quality of local health services and social care services and how they affect families.

3 Rather than create a new and single Community Health Council which is not based on local communities, the Federation Model, which is currently in existence and works well, should be strengthened to provide a strategic role with the enlarged Local Health Boards. Community Health Councils should remain coterminous with local authorities, thus providing the link between the local providers and the new health bodies as outlined above.” (end of quote)
MEMBERSHIP OF THE CURRENT CHCs Currently, Bridgend and Neath & Port Talbot CHCs each have sixteen members, the proportion of First Minister, Voluntary Sector and local Authority members being as laid down in Regulations. Swansea CHC has twelve members but has applied for an increase to sixteen. It should be emphasised that Swansea CHC is the only statutory CHC with fewer than sixteen members, and that in order for this model to work and for Swansea CHC to discharge its core functions, Swansea’s application is strongly supported. There needs to be an early agreement to the increase as well as action by the Appointments Branch to fill the consequent vacancies and those being carried by the three CHCs. On this basis, we have constructed a model assuming the continuation of three CHCs each with sixteen members. THE PROPOSED MODEL It is proposed that a new joint committee, replacing the current Federation Executive Committee should be set up to take effect from 1 October 2009, i.e. the same day as the inception of the new Local Health Boards. The Joint Committee would comprise twelve members, four from each CHC, with the Chair and Vice Chair of each CHC as ex-officio members. The Joint Committee would be supported by a secretariat comprising the Federation Lead Officer and their Office Manager. The Committee would elect a Chair, Vice-Chair and Junior Vice-Chair to be rotated annually, with the Joint Committee Chair representing their Committee at meetings of the Board of Welsh CHCs and the Vice-Chair attending meetings of the Local Health Board (in what capacity is still to be clarified by the Welsh Assembly Government/Board of Welsh CHCs). Deputising would be Vice-Chair for Chair, Junior Vice-Chair for Vice-Chair etc. Chief Officers plus the Lead Officer and Office Manager would be in attendance at Joint Committee meetings which should be held on

4 alternate months to the scheduled CHC meetings i.e. February, April, June, August, October and December. As well as the Joint Committee having representation on the Local Health Board, there should be an annual meeting involving all members of the three CHCs with all available members of the LHB, to be organised jointly by the LHB/Joint Committee. The secretariat for this meeting could be alternated between the LHB/CHC. In terms of its constitution, we believe that the current constitution of the Federation Executive Committee would form a basis but we are open to suggestions should the BWCHC provide a template in order to ensure consistency across Wales. THE MINISTER/DIRECTOR GENERAL’S LETTERS To meet the objectives set by the Minister and to show compliance with the Director General’s letter we respond to each of the bullet points in the letter as follows:
• Looking at the most effective way for CHCs to discharge their functions and taking the opportunity to examine where these can be streamlined/tackled jointly
We believe we have addressed this point under “proposed model”. We would add that Neath & Port Talbot and Swansea CHCs are the only statutory CHCs in Wales currently sharing premises. The suite which houses the advocacy service as well as both CHCs is excellent value for money. The sharing of premises minimises overheads and that together with the exemption we have secured in relation to business rates saves the central pot many thousands of pounds per annum.
• Practical and innovative proposals for the systematic
gathering of local views across the whole community
We believe the gathering of local views should predominantly be the responsibility of individual CHCs. It would greatly facilitate this role if the Joint Committee were allowed to appoint a Public Involvement Officer.

5 • How you will identify which issues are to be addressed
jointly
Those issues identified as locality functions in the discussion paper on the ABMU LHB locality based management arrangements would fall to the individual CHCs. Strategic issues would be referred to the Joint Committee.
• How you intend to respond to proposals from LHBs on a local and strategic level
See previous bullet point
• The mechanism(s) you intend to use to effect the joint
working arrangements, whether through the creation of joint committee of the CHCs or other method
See under the “proposed model”
• The selection method for membership of any joint
committee
Through election by each CHC (but see reference to Chair and Vice-Chair of each CHC being ex-officio under the proposed model)
• The proposed proceedings (frequency of meetings etc)
See the “proposed model”
• How you intend to resolve disputed between CHCs
These would be referred initially to the Joint Committee. If not possible to resolve this, the Director of the Board of Community Health Councils would be asked to act as “honest broker”.
DETAILED WORKING The accountabilities/relationships are shown on the attached chart, (appendix 1), which is based on the Dyfed Federation model. It is suggested that each CHC would have its own ad hoc committees as required (i.e. Bridgend CHC’s Health Watch group) and that the

6 Joint Committee would also have ad hoc committees plus a standing Publicity Committee which would comprise the Chair and Chief Officer of each CHC. Exactly how members would work depends on agreements. But, for example we have been considering assigning members to some specialised areas of interest. If each CHC had a similar pattern of work this would result in three (or more) members from the three CHCs forming a group which would have particular knowledge across the ABMU area about say stroke or older people , or maternity services or sensory problems. They would form a small but knowledgeable group which could work closely together. It would be the responsibility of these groups to be proactive in seeking information and, for example, specifically to consult relevant expert bodies on local matters. These groupings could be disease based, population based (eg hard to reach populations) or service based (eg intermediate care) but they would be limited in number, say 6, and in time because they would change as issues demanded. For example, there could have been a short term grouping looking at Neurosurgery. DISPARITIES ACROSS CHCS IN WALES - BUDGET PER HEAD See attached Appendix 2 which clearly demonstrates how unequally resourced CHCs across Wales are. (See issues to be determined) OTHER MODELS It is noted that the Minister in her letter indicates that the Gwent CHC is not required to submit proposals and the Director General has referred to the “practices of Gwent CHC”. However, the model operated by Gwent is not the same as that which the Minister says she wishes to see. Gwent is a single statutory CHC with an internal federal structure, whereas what CHCs in “loose” federations are being asked to do is to show how within the existing statutory framework they can work together. If the creation through regulation of merged CHCs was what the Minister wanted, presumably she would have said so in her response. We would therefore require some further guidance from WAG/BWCHCs before responding to the suggestion about Gwent.

7
ISSUES TO BE DETERMINED There are a number of issues which need to be clarified by WAG/BWCHC before any model can be finalised. Not the least important of these is how the issue of the disparity in members, staffing and financial resources is to be addressed, as currently the resources available to individual CHCs and groups of CHCs, bear no relation to workload. Second, it is unclear given the way in which the Minister and Director General say they want CHCs to evolve, what will be the role of the proposed Stakeholder Reference Groups and how they and CHCs will relate. Third, loose Federations are based on the concept of a Lead Officer (being a Chief Officer from one of the constituent CHCs) having responsibility for the Federation secretariat. How is it envisioned this will work in relation to newly created joint committees which are meant to have an expanded role? NEATH & PORT TALBOT AND SWANSEA COMMUNITY HEALTH COUNCILS JULY 2009

Joint Committee of CHCs
Bridgend CHC(16 members)
Neath Port Talbot CHC(16 members)
Swansea CHC(16 members)
WAG
BOARD OF WELSH CHCS
12 members in total, Chairman and Vice Chair to be appointed on a
rotational basis from each division. Each division to provide 4 Members.
Chairman to be representative to Wales Board of CHCs
Annual meetings between Joint Committee and LHB.
Vice-Chair to represent Joint Committee on LHB Board.
Interface with LHBPublicity Committee Ad Hoc
Committee
Ad Hoc Committee
Ad Hoc Committee
Ad Hoc Committee
Ad Hoc Committee
Ad hoc/ Standing Committees
Ad hoc/ Standing Committees
Ad hoc/ Standing Committees
Appendix 1

Resources In this connection it is useful to compare financial resources available to CHCs across Wales. Since it cannot be disputed that population is the main determinant to workload (i.e. the greater the population the greater the number of patients) there should not be too great a disparity between the funding of different CHCs. In fact there are significant variations and these need to be addressed. The calculation of discretionary budgets divided by the population shows the following for 2008/2009:
CHC
Population Variable Budget
Budget per Thousand Population
£ Brecknock & Radnor 70,000 17,091 244 Bridgend 128,650 22,767 176 Cardiff 320,900 28,379 88 Carmarthenshire 177,600 23,936 134 Ceredigion 74,000 18,869 255 Clwyd 362,500 57,035 157 Conwy 111,900 29,049 260 Gogledd Gwynedd 75,000 19,560 261 Gwent 557,400 64,543 116 Meirionydd 34,000 17,031 501 Merthyr/Cynon 125,000 13,795 110 Montgomery 59,000 18,965 321 Neath Port Talbot 140,000 19,936 142 Pembrokeshire 113,700 23,544 207 Pontypridd/Rhondda 180,000 24,543 136 Swansea 223,000 19,288 86 Vale of Glamorgan 121,300 22,519 186 Ynys Mon 66,829 20,243 302
Appendix 2

A BALANCED APPROACH
Staying locally, looking strategically
Introduction This document is a response by Cwm Taf CHCs (Merthyr-Cynon Valley CHC and Pontypridd-Rhondda CHC) to the statement by the Minister for Health and Social Services on “The Future of Community Health Councils in Wales” in the National Assembly on 12 May 2009. The Minister asked Community Health Councils (CHCs) to develop joint proposals in each of the new Local Health Board (LHB) areas – with the exception of Gwent and Powys – for a stronger co-operative approach. In subsequent letters to CHCs, the Minister and the Director General of the Department of Health and Social Services set out (some of) the issues to be addressed in the proposals. For ease of presentation, the issues in the Director General’s letter have been utilised as the framework for these proposals (but an attempt has been made to link them with the issues raised in the Minister’s letter):
1. Looking at the most effective way for CHCs to discharge their functions and taking the opportunity to examine where these can be streamlined/tackled jointly;
2. Practical and innovative proposals for the systematic gathering of local views across the whole community;
3. Identifying which issues are to be addressed jointly; 4. Responding to proposals from the LHB at both a local and strategic level; 5. The mechanisms for effecting the joint working arrangements; 6. The selection method for membership of the joint committee; 7. The proposed proceedings of the joint committee; 8. The resolution of disputes.
Effective Discharge of Functions Following the merger of the two Trusts, which were coterminous with each of the two CHCs, the latter decided to explore how they would best work together with the new Trust. As a result the two CHCs, which have operated as the North Bro Taf Federation of CHCs for a number of years, set up a Joint Executive Group with the Trust. The Director of Strategy, who is also the Trust’s Deputy Chief Executive, normally represents the Trust (though the Chief Executive has attended on occasion) together with other senior officers as appropriate. The two CHCs are each represented by their Chairs, Vice-Chairs, Chief Officers and other members.

The Minister’s letter required CHCs to make sure there is “a strategic relationship with the new LHBs” as well as “ensuring continuous engagement with service issues, and not just when there is a service change”. In addition, CHCs are asked to scrutinise “the way in which services are planned and delivered by LHBs, as well as those services at the interface of health and social care service provision; and in challenging any proposed service change, considering those changes within the current priorities, resources, statutory frameworks and governance structures, and make constructive and realistic contributions to the process.” The Joint Executive Group meets every 2-3 months and considers issues that affect the whole of Cwm Taf. The fact that the Trust’s lead is the Director of Strategy helps to ensure the subject matter has a broad policy focus rather than an operational one, and that there is an on-going debate about issues as they emerge, options for further development and an appreciation of the constraints faced by the Trust. Though the Group is currently constituted with Cwm Taf Trust, it will be carried forward with the new Cwm Taf LHB. It is proposed that the Joint Executive Group would have the following functions:
(a) The planning of services. This would effectively be the service planning committee proposed in the consultation paper “Proposals on the Future of Community Health Councils in Wales” of which the LHB Director of Planning would be a member;
(b) Feeding into the formulation of plans the views of local communities and service users;
(c) Keeping the impact of the plans under review, their interface with social care and third-sector service provision, their costs and benefits.
There may be merit in re-naming the Group as the Joint Strategy and Review Group of the Cwm Taf LHB and CHCs. Other proposals to implement joint working and streamline services are: • the two CHCs full membership to meet twice a year to discuss policy and
strategy issues and to review the effectiveness of arrangements, including operational arrangements such as joint monitoring and visiting;
• review the current accommodation including the possibility of combined offices
if savings could be generated. (Outreach services could be established for advocacy with the possibility of an area office/s for local access);
• a single budget for the Federation with effect from 2010/11; • when retirements occur, or vacancies arise, review posts to see if it is feasible to
create a Federation-wide post, e.g. a whole-time Complaints Advocate instead of the current two 0.5 WTE Complaints Advocates; a Federation Chief Officer.

The latter would free up resources to create new posts such as a Deputy Chief Officer (as proposed in the consultation paper) and/or Patients and Public Involvement Officer;
• the re-naming of the current North Bro Taf Federation as the Cwm Taff CHCs
Federation to align it (or mark its alignment) with the Cwm Taf LHB. (It is proposed this take immediate effect. The existing CHCs would effectively be “area committees” of the Federation. Given the proposals in the previous paragraphs – i.e. the possibility of unified offices, a single budget and the appointment of a Federation Chief Officer – the Federation could be given the statutory status of a CHC with two area committees, i.e. the “Gwent model”.
The Board of CHCs is currently reviewing the arrangements for the monitoring and visiting of NHS premises with a view to streamlining and avoiding unnecessary duplication.
Systematic Gathering of Local Views across the Whole Community In response to the consultation document on “The Future of Community Health Councils in Wales”, Cwm Taf CHCs made the point that the Health Forum was a well-established mechanism with such bodies in Cynon Valley, Merthyr, Rhondda and the Taff-Ely area. With the possible exception of the latter, these bodies have had considerable success in engaging with the local communities, and it was felt that developing them (rather than re-inventing them in the form of Area Associations) was the preferred way forward. Cwm Taf CHCs intend to work with the new LHB to see how the Health Forum can strengthen community engagement. (At present, there is also a Patients Involvement Liaison Group which was part of the former North Glamorgan Trust, and a Patients Involvement Forum which is centred on the Royal Glamorgan Hospital. The new LHB plans to review the role of those bodies, and Cwm Taf CHCs would welcome being a part of that process and offer what support they can.) In addition, the CHCs plan to: • engage with Communities First (CF) groups to get local views of service users,
often people who are less likely to join “formal committees” • develop links with the Third Sector through its Health and Social Care Forum
• work with the Local Authority Children and Young People’s Champions and the
respective Local Authority Children and Young Persons Partnerships and Youth Fora to bring on board the views of the younger generation

• establish a patients and public involvement (PPI) team with Cwm Taf CHCs. This could be chaired by a CHC member with a particular role as “Champion” (much in the same way as the Vice-Chair of the new LHB has a specific primary sector role. In the event of the appointment of a Deputy Chief Officer, this could be one of the latter’s responsibilities.)
The Minister has proposed the creation of a Stakeholder Reference Group in each LHB area. No official guidance has yet been issued but this is an issue which will need to be addressed. As Cwm Taf CHCs see themselves having a key role in scrutiny, public engagement, involvement and consultation, and service planning, it is intended to initiate early discussions with the LHB. Identifying Issues to be Addressed Jointly These issues would be identified through the Federation Joint Executive Group which would probably have the same membership as the “CHC side” of the Joint Strategy and Review Group (see above). The Federation Executive could draw upon issues raised from Health Forum meetings, from developing contacts with CF co-ordinators so they can feed through issues their groups have, from its gathering of community views, patient and public involvement activities, complaints data, issues raised by CHCs in other areas, participation in the two Local Service Boards (LSBs), and also through the scrutiny processes within the two Local Authorities. Responding to Proposals from LHBs on a Local and Strategic Level The planning committee suggested in the consultation document is a positive proposal and, to a large extent, that has been incorporated in these proposals in the suggestion of the Joint Strategy and Review Group. It is suggested that this provision should be made in the Regulations. Other mechanisms have already been covered above, e.g. Health Forum meetings, PPI activities, LSBs, etc. Mechanisms to Effect (Practical and Innovative) Joint Working Meetings of the Federation Executive would be one of the means of initiating, exchanging and implementing innovative joint working. Other mechanisms would include joint visiting teams (primary, secondary and tertiary) – there are examples of this already with CAMHS monitoring which includes Abertawe and Bro Morgannwg, Cardiff and the Vale, and Cwm Taf CHCs. Joint training and development sessions, perhaps on a quarterly basis, would be another mechanism. CHC members could attend appropriate CF committees and/or other voluntary groups that deal with health and social care issues with a view to joint working with that sector.

Selection Method for Joint Committee Membership It is anticipated that the Federation Executive would consist of the Chairs, Vice-Chairs and Chief Officers together with perhaps an additional three members from each CHC as determined by each Council. Other officers of the CHCs to attend where appropriate. Proposed Proceedings of Meetings It is proposed that the Federation Executive would meet 4-6 times a year, and would be the key committee to deliver and develop the strategic direction of the Cwm Taf CHCs. The Executive would meet at least quarterly with the LHB Director of Strategic and Operational Planning who have the lead role from the LHB perspective in the Joint Strategy and Review Group. Other LHB Directors and managers would attend as appropriate, and it is suggested that the Chief Executive of the LHB would attend at least once a year. It is also proposed that the Federation Executive (or representatives) meet quarterly with representatives of the LSBs. Operational matters would be dealt with largely by individual CHCs except where there are overlapping issues, though the (full) membership of the two CHCs would meet twice a year. These meetings may coincide with the suggested joint quarterly training and development sessions. Resolution of Disputes between CHCs It would be desirable for there to be a common approach across Wales. Though it is not anticipated that disputes would be frequent, it is suggested the Board of CHCs be tasked with devising a procedure by April 2010 which would cover disputes between CHCs in different Federations or between Federations. CB/21/07/09

.CYNGOR IECHYD CYMUNED
COMMUNITY HEALTH COUNCIL
Cardiff Community Health CouncilGround Floor
Park HouseGreyfriars Road
Cardiff CF10 3AF
Tell Ffon: (029) 20377407
22ndJuly 2009
Vale of Glamorgan Community Health Council2 Stanwell Road
PenarthVale of Glamorgan CF64 3EA
Tell Ffon: (029) 20 350611
Mr Steve Davies
Patient Experience TeamQuality, Standards and Safety Improvement DirectorateDepartment for Health and Social ServicesWelsh Assembly GovemmentCathays ParkCardiff CFlO 3NQ
Dear Mr Davies
Re: CarditI and Vale of Glamorgan Response to the Minister's Statement on theFuture of Community Health Councils
We are pleased to enclose proposals that have been developed and agreed by Cardiff and theVale of Glamorgan Community Health Councils (CHCs) in response to the Minister'sStatement.
These proposals are fully endorsed by both councils and reflect the best model for deliveringthe CHC statutory responsibilities within the Cardiff and Vale of Glamorgan communities.
It is hoped that the document clearly sets out our proposals but should you wish to clarify anypoints in further detail, please do not hesitate to contact either Mr Martyn Jenkins or MrGordon Harrop.
Yours sincerely
~-~ .DrGwyneth"l::nt-Jones
Chairn1anCardiff Community Health Council
4 ( ~~~.Mrs Anita R Morgan
Chairman
Vale of Glamorgan Community HealthCouncll
Copies to: Mrs C Lamyman-Jones, Director, Board ofCommunity Health Councils in Wales
Cardiff Community Health Council Chair:Dr G Briwnant-Jones
Vale of Glamorgan Community Health Council Chair:Mrs A Morgan
Cardiff Chief Officer: Mr Martyn T Jenkins Vale of Glamorgan Chief Officer: Mr Gordon Harrop

1
CARDIFF AND VALE OF GLAMORGAN COMMUNITY HEALTH COUNCILS
RESPONSE TO THE MINISTER’S STATEMENT
Introduction This document is the response of the Cardiff and Vale of Glamorgan Community Health Councils (CHCs) to the statement made by the Minister for Health and Social Services on ‘Future of CHCs in Wales’ in the National Assembly on 12th May 2009. The Minister asked CHCs to develop joint proposals in each of the New Local Health Board (LHB) areas - with the exception of Gwent and Powys – for a stronger, co-operative approach. In subsequent letters to CHCs, the Minster and the Director General of the Department of Health and Social Services each set out a range of issues that should be addressed in the proposals. For ease of presentation the issues in the Director General’s letter have been used as a framework for the response. The issues to be addressed are:
• Looking at the most effective way for CHCs to discharge their functions and taking the opportunity to examine where these can be streamlined / tackled jointly
• Practical and innovative proposals for the systematic gathering of local views, across the whole community
• Identifying which issues are to be addressed jointly
• Responding to proposals from the LHBs on a local and strategic level
• The mechanism(s) for effecting joint working arrangements, whether through the creation of joint committee of the CHCs or other method
• The selection method for membership of any joint committee
• The proposed proceedings of the joint committee (frequency of meetings, etc)
• Resolution of disputes between CHCs

2
Historic Context It will be helpful to the reader if the context of our present situation is explained as CHCs have valuable organisational memory regarding how and why the Health Community has been organised in the past and also how it was most recently. Community Health Council Structure Pre-1996 Prior to 1996 the Cardiff and Vale of Glamorgan CHCs operated within a Federation model. Both CHCs were supported by a single secretariat working from office bases in both Cardiff and the Vale of Glamorgan. The NHS Organisational Structure Pre and Post 1996 NHS services pre 1996 were delivered through the South Glamorgan Health Authority. During this period the purchaser / provider split was introduced. This was a major change in the pattern of service planning and service delivery. Subsequently larger Health Authorities were established – namely the Bro Taf Health Authority in April 1996. In April 2002, Health Authorities were replaced by Local Health Boards (LHBs) in line with the Unitary Authority Structure in Wales. During this period the Government realised that the local voice was important and the establishment of LHBs was an attempt to commission services more locally and more responsive to the needs of local populations. The Local Authority Organisational Structure Pre and Post 1996 Local Authority Services were provided with an organisational structure that included the South Glamorgan County Council incorporating both the Cardiff and the Vale of Glamorgan communities. Cardiff and Vale of Glamorgan District Councils, on the other hand, provided a more local focus. Post 1996 the Unitary Authorities of Cardiff and the Vale of Glamorgan were established. This structure remains in place currently and both Local Authorities are key partners of the CHCs in each community. CHCs mirror Health, Social Care and Welfare providers. So an appreciation of how form has followed function enables the reader to place organisational proposals into context. When considering how the CHCs should respond to the Minister’s 2009 statement, current members recognised that the issues that were significant in the 1990s are still significant to CHCs in Cardiff and the Vale of Glamorgan today. From 1996 the model of two separate CHCs was the agreed way forward for the following key reasons. Firstly, because members join the CHC primarily to serve their local community. And secondly, Cardiff, as the capital city, is bigger and more demographically and socially complex than the Vale of Glamorgan. The two CHCs have operated successfully and with good effect since that time and the reasons to remain separate are still entirely

3
applicable. Cardiff generates more numerous demands which threaten to dominate the health community agenda. The Vale of Glamorgan’s issues are equally important but the likelihood of being subsumed by Cardiff issues is very real and a major concern. Having two CHCs has historically ensured that business is conducted in an equitable way and that our members (our unpaid workforce) will remain motivated to make a difference to patients’ services both locally and also strategically. Methodology and Guiding Principles In preparing these proposals and opinions, each CHC first identified common principles regarding how they could best support patients and their local populations. Members and staff all had an opportunity to contribute to this process and a joint meeting between the CHCs then approved the proposals in this document. The following principles emerged:
1 Both CHCs strongly believe that a ‘grass roots’ approach is essential if local populations are going to be engaged and treated as equals by the new LHB. CHCs must be accountable and responsive to their local communities. The consensus is for the retention of the two CHCs aligned to the Local Authority boundaries, with working premises in each area. It was felt that one CHC serving both local authority areas would become isolated from its population and a Committee structure of sub-areas would be over-whelmed by the Cardiff inner city agenda.
2 Agreement that the optimisation of both member and staff
resources, including skills and knowledge, was key to ensuring equity of CHC standards across the new LHB community
3 Agreement to work collaboratively and to structure the CHCs to
mirror the new Cardiff and Vale University LHB organisational structure where appropriate – to ensure CHC activity remains focussed both at a strategic and operational level. (The Vale CHC would also, in addition, continue to liaise with the ABM LHB and Bridgend CHC for its patients living in the Western Vale, until such time that services are no longer provided by that organisation).
4 Recognition of the important relationship with each separate Local
Authority – a relationship that must be developed as services are increasingly planned and delivered through joint mechanisms.
5 It was agreed that Public and Patient Involvement (PPI) activity
must be further developed to reflect the locality structure adopted by the new LHB. The development of public / stakeholder groups within each locality facilitated by the CHCs as part of the CHC role in generating the views of local population is a real opportunity for grass roots community engagement that could influence service

4
planning and delivery. This is an aspiration which requires to be funded.
This response has been subject to debate and discussion within the CHCs and the wider community – including Health Alliance meetings, Community Council meetings, Public Reference Groups and Carers Groups.
Effective Discharge of Functions
These cultural and organisational beliefs and activities are pertinent to each of the specific areas to which the paper responds later in our report. Both CHCs accept that there are four main statutory responsibilities placed upon them. To achieve effective delivery it is necessary to develop partnerships with a number of organisations including:
• New Local Health Board (LHB)
• Local Authority / Community Councils
• Councils for Voluntary Services / Voluntary Sector / Communities First
• Residual NHS Trusts
• Other CHCs / Board of CHCs in Wales The four key areas of CHC responsibility are:
• To hold to account the local NHS – both strategically and operationally from a public and patient perspective
• To provide an independent advocacy service for those who wish to complain about the NHS.
• To engage in the planning and consultation of changes / developments in NHS service delivery
• To enable local communities to influence the development of NHS services.
To enable the effective delivery of these functions the CHCs have agreed to:
1 To explore working towards the appointment of a Cardiff and Vale of Glamorgan CHCs joint Chief Officer, when opportunities arise through retirement, vacancies, etc.
2 To optimise member resources by developing a specialist Health
Team approach in line with the new LHB organisational structure, and not to just always monitor exclusively within local geographic boundaries. This concept is already in operation and membership will be extended to routinely include both CHCs. Examples of issues considered appropriate include Mental Health, Primary Care, Facilities and Cancer Services.
These Teams will have both a strategic and organisational focus which ensures that the CHCs exerts maximum influence on the

5
patients / publics experience and that member expertise will be available to CHCs throughout the new LHB community.
3 The provision of the Advocacy Service already operates across both CHCs and is a very good example of shared resource. Advocacy requires additional resources since uptake of service is proportional to levels of public awareness of the service and the CHCs will inevitably achieve a higher profile.
4 The administrative support activity can be reviewed to optimise the
staff resources where appropriate. However, the aspiration of the CHCs to develop their PPI activity (outlined later in this document) will require additional funding. Currently limited PPI activity in Cardiff is achieved by funding from Cardiff LHB, which will cease at the end of September 2009.
5 Both CHCs would strongly urge the Minister to retain the current
CHC regulation which gives Local Authorities flexibility in their nominations for membership of the CHC.
6 The strengthened role of CHCs cannot be realised by the
re-organisation of CHCs alone. The NHS must itself develop a new culture which builds upon the principles of honesty, transparency, accountability and engagement. These issues are an important element of strengthening the role and efficacy of CHCs.
7 The relationship with the new LHB has been fully considered. The
two CHCs already have positive communication mechanisms in place within the existing arrangements. Examples include – Trust Board, LHB Board, regular Liaison director level joint CHC meetings, regular director level attendance at CHC council meetings and Annual Review meetings. In addition, both CHCs are invited to attend a wide range of LHB, NHS Trust and Local Authority planning and operational meetings where their independence from NHS management hierarchies, and their duty to challenge, is so reassuring to patients and the public.
The two CHCs will work towards similar arrangements with the new LHB. The Director of the NHS in Wales has asked that, in particular, the consulted CHCs of each new LHB should consider the following points which appear in boxes in the text:
Looking at the most effective way for CHCs to discharge their functions and taking the opportunity to examine where these can be streamlined / tackled jointly
The format for CHC engagement with the new LHB and other partners, as follows, could be:

6
� 6-weekly Liaison Meeting of the Chairmen / Chief Executive of the New LHB and Chairman and Chief Officers of the CHCs.
� Strategic and operational Liaison meetings between the Director of
Planning, Director of Nursing, Director of Acute Services and Director of Community, Mental Health Services and representation of the CHCs to include Chairmen, Chief Officers, Chairs of an agreed number of CHC Health Groups (for example, CHC Mental Health Team).
� Annual Review Meeting with the New LHB Board � Maintenance of and development of CHC membership of appropriate
Local Authority committees - including Health Alliance; Health Social Care and Wellbeing Group; Local Service Board (LSB) Scrutiny Committee; and other Scrutiny Committees as appropriate; Advisory Planning Groups (APGs).
� Further develop engagement with Community Councils. � Further develop joint working with the Voluntary Sector including
Communities First projects. For example, CHC Public Reference Group in Butetown, which is a joint Cardiff CHC / Communities First project. And maintaining membership of the Health and Social Care Networks.
� Representation on a range of other Committees established within the
New LHB community.
Systematic gathering of local views, across the whole community
The gathering of local views across the Cardiff and Vale of Glamorgan community is an extremely difficult and time consuming exercise. Limited funding is made available to Cardiff CHC for the purpose of developing Public Reference Groups, based on the four parliamentary boundary areas. This funding allows Cardiff CHC to barely scratch the surface. Nevertheless, there are good examples of engagement – specifically working with Cardiff Communities First Butetown Project. The local residents have had a voice and been able to hold to account both the Cardiff LHB and Cardiff & Vale NHS Trust and Cardiff Local Authority during the planned regeneration of Loudoun Square. The Vale of Glamorgan PPI funding was withdrawn by the Vale of Glamorgan LHB some years ago and not reinstated. Public awareness events, major consultations and limited outreach to community groups are achieved at the expense of developing other core services. It is clear from the CHCs engagement during the transition process that the new LHB intends to plan and deliver services on a Local Authority area basis. Within this, the new LHB plans to develop Locality Teams and GP Co-operatives. Both CHCs recognise the opportunities that this will provide
7
for community / stakeholder engagement and both envisage the CHC having a key role in facilitating the process. To achieve this aspiration: The membership of both CHCs will need to be increased to provide the critical mass to work with the local communities which are planned. Cardiff CHC will need five members per locality and the Vale CHC seven members per locality. The rural nature of the Vale of Glamorgan being the reason for increased numbers per Locality Team. Therefore, Cardiff CHC will require 30 members (compared with the current 24) and the Vale of Glamorgan CHC 21 members (compared with 20 currently). In addition investment in staff resources will be required to support this activity. This will entail levels of unsociable hours of working – which increases the costs significantly under Agenda for Change. At least 2 Whole Time Equivalent (WTE) staff will be required to develop and sustain the required level of PPI activity.
Identifying which issues are to be addressed jointly
The CHCs in this community have an excellent record of working together. The Programme for Health Service Improvement (PHSI) Project has necessitated joint working and the modernisation agenda has been jointly considered and accepted by both CHCs. The structure outlined above, coupled with the Minister’s proposals that between them the Cardiff and Vale CHCs will elect just one member to the Board of CHCs, will build and develop the collaborative approach. Such collaborative working would include joint training and development events, which would be helpful in the identification of issues for joint consideration, responding to proposals from the new LHB at both local and strategic level.
Responding to proposals from the LHBs on a local and strategic level
• The mechanism(s) for effecting joint working arrangements, whether through the creation of joint committee of the CHCs or other method
A key aspect of the work being done by the CHCs in the community is to undertake operational activity that will assist the CHC to fully contribute to and inform the strategic discussions. The joint working structure outlined above will deliver robust CHC contributions at both levels.
The selection method for membership of the joint committee
It is anticipated that the various joint committees outlined above will ensure that consistent approaches and standards of delivery of CHC activity is achieved across the Cardiff and Vale of Glamorgan community.
The proposed proceedings of the joint committee (frequency of meetings, etc)

8
Both CHCs are in consensus of the need not to increase bureaucracy – but it is anticipated that a Federation Team will be established consisting of Chairs, Vice-Chairs and Chief Officers. This will meet at least quarterly and will be responsible for ensuring:
• Internal review mechanisms are consistent
• Standardisation of Annual Reports and Work Plans
• ‘Conversation with a Purpose’ with CHC members
• General review of progress of new LHB, NHS Trusts, Local Authority, Voluntary Sector, PPI activity, etc.
• Collaborative working - including joint training, development and at least one joint annual meeting of all members.
Resolution of disputes between CHCs
Both CHCs hold the view that they are statutory bodies responsible for bringing the views of their populations to the table. The process outlined above will, during early engagement, planning and consultation, identify potential issues that could become problematic. Early identification is key to this process as it allows time for full consideration to be given. There is no history of any dispute between CHCs in this community. Both Cardiff and the Vale CHCs have agreed to purposely work collaboratively and the practices outlined within this document will further reduce the risk of disputes. Conclusion This response has been developed to maximise the CHCs effectiveness across the new LHB community, whilst maintaining autonomy at a Local Authority level. The two CHCs believe strongly that they should each be accountable and responsive to their populations. There is concern amongst CHC members that to try to organise lay members as if they are paid employees of an NHS organisation will have a detrimental effect not only upon current membership but also on future recruitment. These proposals contain investment requirements and, furthermore, the current lack of funding for CHCs is a real issue. The current variable budget will not sustain an adequate level of CHC activity and will have a major impact upon the CHCs’ ability to undertake our statutory duties. The Minister’s statement about recognising the contribution of CHCs and strengthening this role initially boosted the morale of CHC members and staff. The new extraordinary financial restraint upon our ‘variable’ budgets and the possibility of new responsibilities being imposed without commensurate authority and resources is sadly now having a negative impact. The delicate balance that we have achieved locally over time in order to deliver effective

9
CHC activity will be difficult to maintain in the future if restructuring is not sensitive towards recognising what motivates members. Current membership / staff skills and knowledge must be retained if our communities CHCs are to remain effective. The proposals to be found throughout the document provide the best way forward for the CHCs belonging to our respective communities to maintain current services and also to develop. Cardiff and Vale of Glamorgan CHCs wish to continue to make a real difference in the planning and provision of health related public services within the separate communities of both Cardiff and the Vale of Glamorgan. July 2009