スライド 1 - Prince of Songkla...
11
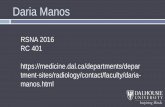
29/08/57 1 Confident Pathological Diagnosis of Interstitial Lung Diseases ~Differential Diagnosis between Idiopathic Interstitial Pneumonias and Chronic Hypersensitivity Pneumonitis and Connective Tissue Diseases~ Tamiko Takemura,MD, PhD. Department of Pathology, Japanese Red Cross Medical Center, Tokyo, Japan The 1578 th Chest Conference/ 3 rd Biennial Clnical-Radiologic-Pathologic Correlation Secondary lobule of Miller ILS, interlobular septum Perilobular fibrosis centriacinar Vein and lymphatic vessels in the interlobular septum(ILS) RB RB RB Br Br ILS ILS ILS RB Secondary lobule of Reid ●acinus, beneath the terminal bronchiole (Reid) Reid’ lobule composed of 3~5 acini ( 8 mm) ●Miller ‘s secondary lobule contain 1~3 lobules of Reid (Reid L. The pathology of Emphysema 1967) Centriacinar (RB and alveoli) 終末細気管支 Intralobular membranous bronchiole centrilobular Pleura Interlobular septum Interlobular vein Interlobular bronchus, Pulmonary artery Above mentioned structure Intralobular vein/venule Membranous bronchiole Terminal bronchiole/PA perilobular periacinar Pulmonary lobule and acinus (Matsumoto, 1977) PV PA Br PV PA acinus RB Centriacinar acinus perillobular 岡田慶夫. (図説肺のリンパ系と肺癌. 金芳堂. 1989 p 13) precap Post cap Distribution of Intrapulmonary lymphatic vessels (Okada) Subpleural lymphatics pleura Intralobular venule Capillary network Periarterial lymphatic Interlobular septum Lymphatics along ILS and vein Interlobular lymphatics RB TB Lymphatics along bronchus Interlobular vein Bronchus PA Pathological basis of interstitial pneumonia
Transcript of スライド 1 - Prince of Songkla...

29/08/57
1
Confident Pathological Diagnosis of Interstitial Lung Diseases
~Differential Diagnosis between Idiopathic Interstitial Pneumonias and Chronic Hypersensitivity
Pneumonitis and Connective Tissue Diseases~
Tamiko Takemura,MD, PhD.Department of Pathology, Japanese Red Cross Medical Center, Tokyo, Japan
The 1578th Chest Conference/3rd Biennial Clnical-Radiologic-Pathologic Correlation
Secondary lobule of Miller
ILS, interlobular septum
Perilobular fibrosis
centriacinar
Vein and lymphatic vessels in the interlobular septum(ILS)
RB
RB
RB
BrBr
ILS
ILS
ILS
RB
Secondary lobule of Reid
●acinus, beneath the terminal bronchiole (Reid)Reid’ lobule composed of 3~5 acini ( 8 mm)
●Miller ‘s secondary lobule contain 1~3 lobules of Reid(Reid L. The pathology of Emphysema
1967)
Centriacinar
(RB and alveoli)
終末細気管支
Intralobular membranous bronchiole
centrilobular
PleuraInterlobular septumInterlobular veinInterlobular bronchus, Pulmonary artery
Above mentioned structureIntralobular vein/venuleMembranous bronchioleTerminal bronchiole/PA
perilobular
periacinar
Pulmonary lobule and acinus (Matsumoto, 1977)
PV
PA
Br
PV
PA
acinus
RB
Centriacinar
acinus
perillobular
岡田慶夫. (図説. 肺のリンパ系と肺癌. 金芳堂. 1989 p 13)
precap
Post cap
Distribution of Intrapulmonary lymphatic vessels (Okada)
Subpleural lymphatics pleura
Intralobular venule
Capillarynetwork
Periarteriallymphatic
Interlobular septum
Lymphatics along ILS and vein
Interlobularlymphatics
RB
TB
Lymphaticsalong bronchus
Interlobular vein
Bronchus
PA
Pathological basis of interstitial pneumonia

29/08/57
2
RB
Back-to back alveoli
細血管は背中合わせ肺胞の稜の部分に存在
Lung parenchyma is composed of alveolar duct, alveolar sac, alveoli and air
AD
AD
AD
Interstitial pneumonia is usually defined as diffuse lung disease involving mainly alveolar septa with inflammatory cell infiltration and fibrosis.Ⅰ型
Ⅱ型
cellular~ fibrosingNSIP
normal
Basset F:Am J Pathol 1986; 122: 443-461
Intraluminal fibrosis
Basement membrane
Collagen fiber
Elastic fiber
Fibroblast/myofibrobalst
Type Ⅰpneumocyte
Type Ⅱpneumocyte
Regenerative epithelium
macrophage
Collagen globule
Intra-alveolar polypoid fibrosis (Masson body)
Alcian blue-PAS
Mural incorporation fibrosis of f0brosing NSIP
Obliterative fibrosis
DAD organizing ; proliferation of fibroblast and myofobrobalsts in the alveolar walls and alveolar lumina with ill-definedborder.

29/08/57
3
UIP is the basic pathological pattern of interstitial pneumonia
UIP pattern according to 2002 statement and 2011 guideline (AJRCCM 2002;165: 277-304, 2011; 183: 788-824)
1. Marked fibrosis with architecture distortion with or without
honeycombing in predominantly subpleural and paraseptal
distribution
2. Patchy involvement of fibrosis alternating normal alveoli
3. Presence of fibroblastic foci
4. Absence of features against diagnosis of UIP suggesting an
alternative diagnosis
① Hyaline membrane, ② Organizing pneumonia, ③ Granuloma
④Marked interstitial inflammatory cell infiltrate away from
honeycombing
⑤ Predominant airway centered fibrosis
⑥ Other features suggestive of an alternate diagnosis (sarcoidosis,
Lagerhans’ cell histiocytosis, asbetosis etc)
H.O
2001.5.17
63
UIP (小葉辺縁性病変)
65
Courtesy of Drs. Ogura and Itoh
Early phase of UIP :Perilobular, periacinar fibrosis
●Interlobular vein and artery running along the perilobular area●Intralobular bronchiole running along the periacinal region
MB MB TB
MB
Interlobular septum
Interacinar septum
S10
A
UIP in early phase:perilobular fibrosis → FF
MB
V
ILS
A
V
ILS
v
RB A
FF
v
Hyperplasia of smooth muscle in the fibrosis
Marked fibrosis at the pleuro-septal junction (wedge-shaped)

29/08/57
4
485
IPF/UIP
Fine nodular lesion arising from the pleura
Upper lobe image of the same case
RB
MBA
Fibrosis along the pleura, interlobular septa, and intralobularvein
UIP
V
V
V
V
Perilobular area
舌区先端の小葉間隔壁の模式図 (Reid)
L. Reid. The connective tissue septa in the adult humanlung. (Thorax 1959; 14: 138-145)
pleura
Broncho-vascular bundle
pleura
Minor septum
Larger septum
Major septum
(Connection bewwen ILS and bronchus)
(connection between pleura and bronchus)
Reconstruction of the arrangement of the connective tissue septa at the tip of the lingula
Minor septum
Connection between pleurae
Honeycombing
Autopsy lung of IPF/UIP
3~5 mm-sizdconcav-convex pleural surface
Histologically, collapsed alveoli, dilated alveolar ducts
in the cyst wall with smooth muscle hyperplasia.
Bronchiolar epithelium lining the cystic spaces
(bronchiolization)
Histology of honeycombing
(→alveolar tip)
MB

29/08/57
5
V
PVV
V
br
A
PA
ILS
A
V
MB
Pleural indentation at the interlobular septa wherealveoli are collapsed.
Microscopic honeycombing
Alveolar structure is simplified and dilated by periacinarfibrosis with atelectasis, developing to the clustered cystic
lesions. The dilated bronchioles connect to these cystic lesions.
v v
A
TB
Histopathological criteria for UIP pattern (2011)
UIP pattern
(All four criteria)
Probable UIP pattern
Possible UIP pattern (All three
criteria)
Not UIP pattern
(Any of the 6 criteria)
●Evidence of marked
f ibrosis/architectural distortion, ±honeycombing in a predominantly subpleural/paraseptaldistribution
●Presence of patchy involvement of lung parenchyma by fibrosis
●Presence of fibroblastic foci
●Absence of features against diagnosis of UIP suggesting an alternate diagnosis (see fourth column)
●Evidence of marked fibrosis/architectural distortion, ±honeycombing
●Absence of either patchy involvement orfibroblastic foci, but not both
●Absence of features against a diagnosis of UIP suggesting an alternate diagnosis (see fourth column)
or
● Honeycomb changes
only
●Patchy or diffuse involvement of lung parenchyma by fibrosis, with or without interstitial inflammation
●Absence of other criteria for UIP (see UIP pattern column)
●Absence of features against a diagnosis of UIP suggesting an alternate diagnosis (see fourth column)
●Hyaline membranes
●Organizing pneumonia
●Granuloma
●Marked interstitial inflammatory cell infiltrate away from honeycombing
●Predominant airway centered changes
●Other features suggestive of an alternate diagnosis
(Raghu G et al. AJRCCM, 183: 788-824, 2011)
HRCT Surgical lung biopsyPattern (when performed)
Diagnosis IPF?
UIP UIPProbable UIPPossible UIPNonclassifiable fibrosis
Not UIP
Yes
No
Possible UIP UIPProbable UIP
Possible UIPNonclassifiable fibrosis
Not UIP
Yes
Probable
No
Inconsistent with UIP
UIPProbable UIP
Possible UIPNon-classifiable fibrosisNot UIP
Possible
No
Combination of HRCT and surgical lung biopsy for the diagnosis of IPF
Key features for the pathologist in the 2011 evidence-based guidelines for IPF (Larsen & Colby : Arch Pathol Lab Med 2012; 136: 1234-41)
1. Surgical lung biopsy is no longer necessary for diagnosis of IPF; HRCT is acceptable instead
2. MDD is integral to the diagnosis and management of IPF
3. Pathologists should attempt to assign levels of confidence to the histologic diagnosis of UIP, but these levels are not validated and should be more conceptual than practical.
4. Acute exacerbation of IPF is an accepted phenomenon, and acute lung injury superimposed on a patchy fibrotic UIP-like background.
5. “Exclusionary” histologic features for diagnosis of UIP are imprecise, and there are no guideline that specifically define how they should be applied.
Summary of Update classification of IIPs
1. Idiopathic NSIP is accepted.
2. RB-ILD is clinico-radiologically diagnosed without surgical biopsy.
CPFE is recognized.
3. The behavior of IPF is acknowledged to be heterogeneous(stable, rapid progression, steady, acute exacerbation)
4. Acute exacerbation occurs in chronic fibrosing IP (IPF, NSIP)
5. Unclassifiable IIPs are recognized, often because of multiple mixed patterns of lung injury.
6. Clinical algorithm is necessary for classifying and managing IIP cases, especially when no biopsy is available.
7. Pleuroparenchymal fibroelastosis (PPFE) is recognized as a specific rare entity.
8. Molecular and genetic studies are necessary to diagnose and predict prognosis.

29/08/57
6
Revised ATS/ERS classification of IIPs: Multidisciplinary diagnoses (Travis, et al. AJRCCM 2013; 733-48)
Major idiopathic interstitial pneumoniasIdiopathic pulmonary fibrosisIdiopathic nonspecific interstitial pneumoniaRespiratory bronchiolitis-interstitial lung diseaseDesquamative interstitial pneumoniaCryptogenic organizing pneumoniaAcute interstitial pneumonia
Rare idiopathic interstitial pneumoniasIdiopathic lymphoid interstitial pneumoniaIdiopathic pleuroparencymal fibroelastosis
Unclassifiable idiopathic interstitial pneumonias
Fibrosing IP
Acute/subacute IP
Smoking-related IP
Important differential diagnosis
IIPs vs CHP and CTD
focusing on UIP pattern
Clinical phenotype of CHP(Yoshizawa, Y. J Allergy Clin Immunol 1999; 103: 315-320)
• Recurrent type; pulmonary fibrosis after repeated acute episodes
• Insidious onset ;chronic disease without acute episodes
*It is difficult to differentiate insidious-onset chronic HP from IPF.
* Up to 30 % of subjects with histologic HP have no identifiable antigen. (Travis et al. AJRCCM 2013; 188: 733-748)
*43 % of patients with IPF according to 2011 guideline had a subsequentdiagnosis of CHP. (Morell. Lancet Resp Med 2013 1; 685-94, 2013)
These data suggest many cases of CHP are managed as IPF.
Histologic diagnosis of CHP required presence of a bronchiolocentricchronic interstitial pneumonias and/or chronic bronchiolitis and poorly formed nonnecrotizing granulomatous inflammation confined to peribronchiolar interstitium. (Trahan et al. 2008; Chest 134; 126-132)
(31 specimens from 15 patients with clinical diagnosis of HP)
●1) Bronchiolocentric chronic interstitial pneumonia (83 %)
2) Interstitial pneumonia with a peripheral/subpleural and /or patchwork distribution (16%)
3) Fibroblastic foci (associated with honeycomb 13 %,
unrelated to OP or honeycomb 26 %)
4) Honeycomb change (16 %)
● 5) Lymphoid hyperplasia (79 %)
● 6) Chronic bronchiolitis (96 %)
7) Peribronchiolar fibrosis with bronchiolar metaplasia (54 %)
● 8) Isolated multinucleated giant cells (71 %)
● 9) Poorly-formed granulomas within peribronchiolar interstitium (58 %)
10) Organizing pneumonia (42 %)
Usual interstitial pneumonia-pattern fibrosis in surgical lung biopsies. Clinical, radiological and histopathological clues to aetiology. (Smith M, Dalurzo M, Panse P et al. J Clin Pathol 2013; 66: 896-903)
Radiological features Histopathological features
●Reticular pattern with traction bronchiectasis●Ground-glass opacities, common●Mid and upper lung zones commonly affected in a bronchovascular distribution with resulting micronodules●Non-basilar distribution common●Mosaic attenuation●Irregular bronchovascular bundles●Subpkleural honeycomb cysts, not always basilar
●Patchy fibrosis along the bronchovascularbundle with rare fibroblast foci●Individual interstitial giant cells, some with cholesterol clefts●Honeycomb cyst (lower and upper lobes)●Extensive peribronchiolar metaplasia●Bridging fibrosis across lobules
UIP in cHP
S2
FF v
RB
Bridging fibrosis
FF
Alcian blue
Chronic bird-related HP

29/08/57
7
Bridging fibrosislinear connection of fibrosis between centrilobular to perilobular area,
and centrilobular to centrilobular
① RB~Subpleural (41 %)
② RB~Interlobular septum (82 %)
③ RB~RB (65 %)
①
② ③
RB
ILS
v
RB
RB
RB
RBILS
Bridging fibrosis is seen in 70% of cHPcases.
Comparison of incidence of pathological features between chronic HP with UIP-like pattern and IPF/UIP
Pathological features Chronic HP (n=22) IPF/UIP (n=13) P value
Bronchiolitis 22 (100 %) 6 (46.2 %) 0.0003
Perilobular fibrosis 22 (100 %) 13 (100 %) 1.0000
Centrilobular fibrosis 22 (100 %) 6 (46.2 %) 0.0003
Bridging fibrosis 18 (81.8 %) 4 (30.8 %) 0.0042
Organizing pneumonia
18 (81.8 %) 3 (23.1 %) 0.0006
Fibroblastic foci 22 (100 %) 13 (100 %) 1.0000
Honeycombing 13 (59.1 %) 10 (76.9 %) 1.0000
Granuloma 14 (63.6 %) 0 0.0002
Giant cell 15 (68.2 %) 0 <0.0001
Isolated cyst with collagen deposition
3 (13.6 %) 0 0.2790
Lymphocytic alveolitis
19 (86.4 %) 4 (30.8 %) 0.0022
Lymphoid follicle 17 (77.3 %) 5 (38.5 %) 0.0268(Takemura Histopathology 2012: 61: 1026-35)
Patterns of fibrosis of CHP
Perilobular (periacinar) fibrosis UIP pattern
Centrilobular (centrilacinar) fibrosis
Bridging fibrosis
Insult to the respiratory bronchiole ~Alveolar duct → Intralumial and peribronchiolar fibrosis → obliteration, centriacinar(centrilobular)fibrosis
Diffusion of antigens to the peripheral alveoli → Macrophage and
lymphatic clearance → Perilobular accumulation, inflammation and
fibrosis
Connection between centrilobulra(centriacinar) and perilobular
/periacinar fibrosis, or centriacinar to centriacinar
Autopsy cases of chronic bird fancier’s disease
The patient had fed 300 chickens The patient had contact to birds in the park
Abundant exposure Small amount exposure
Comparison of Microscopic Features betweenCHP and IPF/UIP in autopsy cases
CHP (n=16) IPF/UIP (n=11)
UIP-like area Fibroblastic foci absent
present
Lymphoid follicle absent
present
2
6
2
14
0
9
0
11
F-NSIP like area absent
present
3
9
7
4
CLF absent
present
0
16
3
8 * p<0.03
Bridging fibrosis absent
present
8
8
10
1 * p<0.03
Atelectasis absent
present
10
6
5
6(Akashi ,Takemura Am J Clin Pathol 2009; 131:405-415)
Histopathological features of CHP autopsy lungs
UIP pattern
f-NSIP
pattern
CLF* Bridging fibrosis*
Atelectaticfibrosis
Cyst with collagen
deposit *
BFL
n=12
Insidious 11DAD 7
4 11 7 4 9
Recurrent
1 1 1 1 0 0
SHP
n=4
Insidious 2 2 2 1 2 1
Recurrent
2DAD 2
2 2 0 0 1
CLF; centrilobular fibrosis* CLF, bridging fibrosis, and cyst with membranous collagen deposit significantly present in CHP compared with IPF/UIP (p<0.03)

29/08/57
8
Three dimensional reconstruction ofcentrilobular and bridging fibrosis of CHPvs IPF/UIP
BronchiolePulmonary arteryFibrosis
CHP
IPF/UIP
IPF/UIP vs CTD/UIP
RA
RA 60’s M Arthralgia,Anti CCP Ab 753.9U/ml , RF 43.4 IU/ml
Honeycombing,Perilobular fibrosisLymphoid follicles with germinal center
UIP pattern
Usual interstitial pneumonia-pattern fibrosis in surgical lung biopsies. Clinical, radiological and histopathological clues to aetiology. (Smith M, Dalurzo M, Panse P et al. J Clin Pathol 2013; 66: 896-903)
Radiological features Histopathological features
●Reticular opacities with lobular distortion●Honeycomb cysts uncommon and fewer than
UIP in IPF●Traction bronchioloectasis●Airway-associated abnormalities●Pleural effusion, sometimes
●Fibrosis more haphazard and more airway-centerd●Nodular inflammatory(lymphoid) infiltration, often with germinal centers●NSIP-like alveolar septal fibrosis
common● Follicular bronchiolitis common● Bronchiolar remodeling common (peribronchiolar metaplasia)● Pleural inflammation and fibrosis common●Occasional fibroblast foci (always fewer than UIP in IPF)
UIP in rheumatic disease
Comparison of pathologic scores betweenCVD-UIP and IPF/UIP
Category CVD-UIP (n=39)
IPF/UIP (n=61) P value
Fibroblastic foci 1.56 ± 0.74 2.01 ± 0.81 0.007
Germinal centers 1.04 ± 1.07 0.33± 0.61 < 0.001
Total inflammation 2.10 ± 0.69 1.74 ± 0.66 0.010
Honeycomb (size) 1.71 ± 1.09 2.20 ± 1.09 0.034
Plasma cells 1.72± 0.68 1.43± 0.71 0.044
Organizing pneumonia
0.33 ± 0.53 0.38 ± 0.60 NS
Intraalveolar Mφ 0.76 ± 0.54 0.85 ± 0.45 NS
Pleural fibrosis, % of
affected cases
4 (10.5) 7 (11.5) NS
(Song JW Chest 2009; 136: 23-30)
Connective tissue disease-associated interstitial lung disease. A call for clarification (Lung-dominant CTD)
(Fischer A, e t al. Chest 2010; 138: 251-156)
1. Interstitial pneumonia(NSIP, UIP, LIP, OP, DAD) as determined by SLB or HRCT and2. Not definite connective disease and3. No identifiable alternative etiology for IP and 4. Any one of the following autoantibodies ot at least two of the
histopathology features:Autoantibodies
ANA(>1:x320), RF(>60 IU/ml), Nucleolar ANA, anti-CCP,
anti-Scl-70,anti-Ro, anti-LA, anti-dsDNA, anti-Smith,anti- RNP, anti- t RNA synthetase(Jo-1, PL-7, PL-12, EJ) anti-PM-Scl, anti-centromere
Pathological features a) Lymphoid aggregates with germinal centersb) Extensive pleuritisc) Prominent plasmacytic infiltrationd) Dense perivascular collagen

29/08/57
9
Histopathological features of Lung dominant-CTD
Lymphoid follicle with germinal centerExtensive pleuritis
Prominent plasmacytic infiltrationDense perivascular collagen
Autoimmune-featured interstitial lung disease A distinct Entity (Vij, Chest 2011; 140: 1292-99)
Comparison between AIF-ILD(63 cases), IPF(58 cases), and known CTD-ILD(37 cases):
62 % of patients with AIF-ILD had UIP on CT
Lung Bx; UIP 81 %, NSIP 6 %,
Patients with AIF-ILD and IPF had similar survival, worse than those with CTD-ILD.
Patients with ILD may have features of an autoimmune disorder that do not meet the diagnostic criteria fro CTD.
Frequency and implication of autoimmune serologies in IPF (Moua T.Mayo Clin Proc 2014; 89: 319-326)
29 % of patients with biopsy-confirmed IPF have positive serologic tests.No survival difference was observed between cases with or without autoantibodies.
60’s MaleANA 640 x, RAPA 1280 x No apparent CTD, 4 years after biopsy
UIP pattern with lymphoid follicles
Idiopathic Pleuoparenchymal Fibroelastosis(PPFE)
Amitani’ s disease; idiopathic pulmonary upper –lobe fibrosis (1992)Frankel; Idiopathic pleuroparenchymal fibroelastosis(2004)
upper lobePleuroparenchymal fibroelastosis (PPFE)
●Pleural thickening with collagen●Parenchymal fibrosis (intraalveolar collagen deposition)
●Parenchymal elastosis (subpleuralelastosis)
High frequency of pneumothorax
Fibroblastic foci at the edge of elastofibrosis Intra-alveolar fibrosis with marked elastosis.

29/08/57
10
Clinical settings of PPFE
IdiopathicBone marrow transplantationDrugs(chemotherapy)RadiationGraft-vs-host disease
TuberculosisMycobacteriosis (MAC)Ankylosing spondylitisPulmonary Langerhans cell histiocytosisSarcoidosisChronic hypersensitivity pneumonitisPneumoconiosis(silicosis, asbestosis)Rheumatoid arthritis Neuromuscular disorders
Rare histologic patterns of IP
1. Acute fibrinous organizing pneumonia
This is a case of RA. AFOP can be seen in CTD, HP, and drug-induced lung disease.
(1) Intra-alveolar fibrin (2) OP (3) Patchy distribution
2. Bronchiolocentric patterns of interstitial pneumoniamay be associated with environmental and occupational exposures
Chronic bird-related HP Hard metal lung disease; Fibrosis confined to the respiratory bronchiole
Coexisting patterns
Multiple pathologic and /or HRCT patterns may be found in the same patient.
● Different patterns my be seen in a single biopsy or in biopsies from multiple sites, or when pathologic and HRCT patterns differ. (e.g.UIP-NSIP, discordant UIP)
● In smokers, multiple features may coexist, i.e.,
PLCH, RB, DIP, pulmonary fibrosis (UIP, NSIP), and emphysema.
●CPFE is an example of coexisting patterns (UIP, NSIP and
emphysema)
● When coexisting patterns occur, MDD may determine the clinical significance of individual patterns.
UIP+ f-NSIP

29/08/57
11
UIP+centrilobular cystic lesion and mucostasis (smoking-related change) Unclassifiable IIPs
1) Inadequate clinical, radiologic or pathologic data
2) Major discordance between clinical, radiologic, or pathologic findings in the following situations
a. previous therapy resulting in substantial alteration of radiologic or histologic findings. (e.g., DIP→ f-NSIP)
b. new entity, or unusual variant of recognized entity
c. multiple HRCT findings and pathologic patterns with IIP.
2(a) DIP steroid → f-NSIP
Fibroblastic focus (→)
Rt.S4
Rt.S9
2(b) new entity
Cystic lesion beneath the terminal bronchiole, destructive alveoli,Mucostasis, fibroblastic foci
(smoking related IP)
2(b) unusual variant of recognized entity C-NSIP background + acute lung injury
CK
Ill-defined border between alveolar septum and lumina
Epithelial shedding, fibrinous exudateMacrophage and mononuclear cell infiltration
1. Pathological diagnosis should be made in reference to the clinical relevance and course, and HRCT findings in each case.
2. The diagnosis and management of the IIPs require clinical-radiologic-pathologic correlations with a multidisciplinary discussion.
Summary