
Fetal_Deaths_in_the_United_States__Influence_of.7.pdf
7
Fetal Deaths in the United States: Influence of High-Risk Conditions and Implications for Management John C. Smulian, MD, MPH, Cande V. Anant h, PhD, MPH, Anthony M. Vintzileos, MD, William E. Scorza, MD, and Robert A. Knuppel, MD, MPH OBJECTIVE: To estimate the effect of specific maternal–fetal high-risk conditions on the risk and timing of fetal death. METHODS: This study examined 10,614,679 non-anomalous singleton pregnancies delivering at or beyond 24 weeks’ gestation, derived from the U.S. linked birth/infant death data sets, 1995–1997. Fetal death rates for pregnancies at low risk were compared with pregnancies complicated by chronic hypert ension, gestati onal hypertensive disord ers, diabetes, small for gestational age infants, and abruption. Adjusted relative risks as well as population-attributable risks for fetal death were derived by gestational age for each high-risk condition compared with low-risk pregnan- cies. RESULTS: The fetal death rate for low-risk pregnancies was 1.6 per 1000 births. Adjusted relative risk for fetal death was 9.2 (95% confidence interval [CI] 8.8, 9.7) for abrup- tion, 7.0 (95% CI 6.8, 7.2) for small for gestational age infants, 1.4 (95% CI 1.3, 1.5) for gestational hypertensive disorders, 2.7 (95% CI 2.4, 3.0) for chronic hypertension, and 2.5 (95% CI 2.3, 2. 7) for diabet es.Feta l dea th rates were lowest betwee n 38 and 41 weeks. The fetal death rate (per 1000 births) for these high-risk conditions was 61.4, 9.6, 3.5, 7.6, and 3.9, respectively. Almost two thirds of fetal deaths were attributable to the pregnancy complications exam- ined. CONCLUSION: High-risk conditions in pregnancy are associ- ated with an increas ed risk for fetal death, particular ly in the third trimester. Delivery should be considered at 38 weeks, but no later than 41 weeks, for these pregnancies. (Obstet Gynecol 2002;10 0:1183– 9. © 2002 by The Amer- ican College of Obstetricians and Gynecologists.) The risk for fetal death is increased in pregnancies com- plicated by chronic hypertension, hypertensive diseases of pregn ancy (preg nanc y-ind uced hyper tensio n, pre- eclampsia, and eclampsia) , diabetes, small for ges tat ion al age births, and placental abruption. 1,2 The presence of any of the se con dit ion s is common ly con sidere d an indica tion for antenatal fetal testing to assure fetal well- being. 3–6 Several different methods for monitoring fetal well-being are used in the United States. These include “kick count s,” which require only time and effort from the pregnant woman, as well as technology-dependent metho ds that include fetal heart rate moni torin g, ultra - sound examinations with biophysical profile evaluations and amniotic flu id volume assessments, and Doppler flow velocimetry. 3 The primary goal of fetal testing by any method is to prev ent fet al dea th. Tra dit ion all y, recommendations based on empirical evidence suggest initiating testing around 32 weeks’ gestation in the pres- ence of most high-risk conditions, 3,7 but there are no consistent recommendations as to when to discontinue testing and deliver the fetus. To make decisions about when to initiate and when to dis con tin ue fet al tes tin g, it is imp ort antto understand the influence of each high-risk condition on the timing of feta l deat h. There is li tt le av ai la bl e info rmat io n, if any, to describe the timing of fetal death in high-risk conditions in compar iso n wit h oth erwi se nor mal pre gna nci es, which would allow an appropriate judgment of how to time antepartum fetal testing. Therefore, this study was designed to determine whether the presence of specific high-risk conditions alters either the risk or timing of fetal death in the United States compared with appar- ently low-risk pregnancies without these conditions, and thereby to judge when to apply fetal surveillance tech- niques to prevent fetal death. MATERIALS AND METHODS Data for this study were derived from the US Perinatal Mor tal ity dat a sets compri sing liv e bir ths and fet al deaths from 1995 through 1997, assembled by the Na- From the Division of Maternal-Fetal Medicine and the Section of Epidemiology and Biostatistics, Department of Obstetrics, Gynecology and Reproductive Sciences, University of Medicine and Dentistry of New Jersey, Robert Wood Johnson Medical School/Saint Peter’s University Hospital, New Brunswick, New Jersey. Drs. Smulian and Ananth were supported in part through a grant from the National Institutes of Health (NICHD RO1-HD38902) and the National Birth Defects Prevention Study from the Centers for Disease Control and Prevention, Atlanta, Georgia. 1183 VOL. 100, NO. 6, DECEMBER 2002 0029-7844/02/$22.00 © 20 02 b y T he American Colle ge of O bstet ricians and Gyne colo gists . Published by Else vier Scie nce Inc. PII S002 9-784 4(02 )02389-0
-
Upload
jojolilimomo -
Category
Documents
-
view
214 -
download
0
Transcript of Fetal_Deaths_in_the_United_States__Influence_of.7.pdf

7/28/2019 Fetal_Deaths_in_the_United_States__Influence_of.7.pdf
http://slidepdf.com/reader/full/fetaldeathsintheunitedstatesinfluenceof7pdf 1/7
Fetal Deaths in the United States: Influence ofHigh-Risk Conditions and Implications for Management
John C. Smulian, MD, MPH, Cande V. Ananth, PhD, MPH, Anthony M. Vintzileos, MD, William E. Scorza, MD, and Robert A. Knuppel, MD, MPH
OBJECTIVE: To estimate the effect of specific maternal–fetalhigh-risk conditions on the risk and timing of fetal death.
METHODS: This study examined 10,614,679 non-anomaloussingleton pregnancies delivering at or beyond 24 weeks’gestation, derived from the U.S. linked birth/infant deathdata sets, 1995–1997. Fetal death rates for pregnancies at low risk were compared with pregnancies complicated bychronic hypertension, gestational hypertensive disorders,diabetes, small for gestational age infants, and abruption.Adjusted relative risks as well as population-attributablerisks for fetal death were derived by gestational age for each high-risk condition compared with low-risk pregnan-cies.
RESULTS: The fetal death rate for low-risk pregnancies was1.6 per 1000 births. Adjusted relative risk for fetal death
was 9.2 (95% confidence interval [CI] 8.8, 9.7) for abrup-tion, 7.0 (95% CI 6.8, 7.2) for small for gestational ageinfants, 1.4 (95% CI 1.3, 1.5) for gestational hypertensivedisorders, 2.7 (95% CI 2.4, 3.0) for chronic hypertension,and 2.5 (95% CI 2.3, 2.7) for diabetes.Fetal death rates were
lowest between 38 and 41 weeks. The fetal death rate (per 1000 births) for these high-risk conditions was 61.4, 9.6, 3.5,7.6, and 3.9, respectively. Almost two thirds of fetal deaths
were attributable to the pregnancy complications exam-ined.
CONCLUSION: High-risk conditions in pregnancy are associ-ated with an increased risk for fetal death, particularly inthe third trimester. Delivery should be considered at 38
weeks, but no later than 41 weeks, for these pregnancies.(Obstet Gynecol 2002;100:1183–9. © 2002 by The Amer-ican College of Obstetricians and Gynecologists.)
The risk for fetal death is increased in pregnancies com- plicated by chronic hypertension, hypertensive diseasesof pregnancy (pregnancy-induced hypertension, pre-eclampsia, and eclampsia), diabetes, small for gestationalage births, and placental abruption.1,2 The presence of any of these conditions is commonly considered anindication for antenatal fetal testing to assure fetal well-
being.3–6 Several different methods for monitoring fetalwell-being are used in the United States. These include“kick counts,” which require only time and effort fromthe pregnant woman, as well as technology-dependentmethods that include fetal heart rate monitoring, ultra-sound examinations with biophysical profile evaluationsand amniotic fluid volume assessments, and Dopplerflow velocimetry.3 The primary goal of fetal testing byany method is to prevent fetal death. Traditionally,recommendations based on empirical evidence suggestinitiating testing around 32 weeks’ gestation in the pres-ence of most high-risk conditions,3,7 but there are noconsistent recommendations as to when to discontinuetesting and deliver the fetus.
To make decisions about when to initiate and when todiscontinue fetal testing, it is important to understand theinfluence of each high-risk condition on the timing of fetal death. There is little available information, if any, todescribe the timing of fetal death in high-risk conditionsin comparison with otherwise normal pregnancies,which would allow an appropriate judgment of how totime antepartum fetal testing. Therefore, this study wasdesigned to determine whether the presence of specifichigh-risk conditions alters either the risk or timing of fetal death in the United States compared with appar-ently low-risk pregnancies without these conditions, andthereby to judge when to apply fetal surveillance tech-niques to prevent fetal death.
MATERIALS AND METHODS
Data for this study were derived from the US PerinatalMortality data sets comprising live births and fetaldeaths from 1995 through 1997, assembled by the Na-
From the Division of Maternal-Fetal Medicine and the Section of Epidemiology and Biostatistics, Department of Obstetrics, Gynecology and Reproductive Sciences,University of Medicine and Dentistry of New Jersey, Robert Wood Johnson
Medical School/Saint Peter’s University Hospital, New Brunswick, New Jersey.
Drs. Smulian and Ananth were supported in part through a grant from the National Institutes of Health (NICHD RO1-HD38902) and the National Birth Defects Prevention Study from the Centers for Disease Control and Prevention,
Atlanta, Georgia.
1183VOL. 100, NO. 6, DECEMBER 2002 0029-7844/02/$22.00
© 2002 by The American College of Obstetricians and Gynecologists. Published by Elsevier Science Inc. PII S0029-7844(02)02389-0

7/28/2019 Fetal_Deaths_in_the_United_States__Influence_of.7.pdf
http://slidepdf.com/reader/full/fetaldeathsintheunitedstatesinfluenceof7pdf 2/7
tional Center for Health Statistics of the Centers forDisease Control and Prevention. These natality andmortality data files, produced annually, include statisti-cal data from birth and infant death certificates (up to 1year) that are provided to the National Center for HealthStatistics by individual states, and the District of Colum-
bia, Puerto Rico, Virgin Islands, and Guam, under the
Vital Statistics Cooperative Program.8
In addition, infor-mation from fetal death certificates is linked to data from
birth records so that the combined data set containsinformation about pregnancies having fetal deaths. Thedata conform to uniform coding specifications and have
passed statistical quality checks. They have been editedand reviewed and form the basis for official US birth anddeath statistics.
Analyses were restricted to singleton births deliveredat or beyond 24 completed weeks of gestation. Thetiming of fetal death was assigned using the gestationalage at delivery as a surrogate because the exact timing of
fetal death was not available. Gestational age assignmentwas predominantly based on the date of last menstrual
period (LMP). In about 5% of births, the date or monthof LMP was missing, and therefore it was imputed.9
Inconsistent gestational age for birth weight was replaced by a clinical estimate in a small fraction of births. Thegestational age imputations and the replacement of clin-ical estimate were performed by the National Center forHealth Statistics before public release of data.
The vital statistics data contain information on severalsociodemographic factors, as well as medical and obstet-ric complications of pregnancy. Sociodemographic char-
acteristics that were examined included maternal age,gravidity, marital status (married or unmarried), mater-nal education (years of schooling), cigarette use (yes orno), maternal race (whites, blacks, and other race/ethnic-ity), and prenatal care. Complications of pregnancy ex-amined were chosen because of their reported associa-tion with increased risk for fetal death and because thesehigh-risk conditions encompass the majority of the com-mon indications for antepartum testing and are riskfactors for fetal death. These included hypertensive dis-orders, diabetes, and placental abruption. All complica-tions of pregnancy are recorded on vital statistics data
using a check-box format,10
indicating the presence orabsence of the condition. Also included in the analysiswere small for gestational age infants, defined as birthweight below the 10th centile for gestational age, derivedfrom singleton births in the United States for 1995–1997(internally derived data).
Hypertensive diseases were classified as either chronichypertension, pregnancy-induced hypertension, oreclampsia. For purposes of analysis, the latter two werecombined into a category of gestational hypertensive
disorders. Chronic hypertension was recorded if thewoman had elevated blood pressures before pregnancy,or prior to 20 weeks’ gestation. The diabetes categoryincluded both pre-existing and gestational diabetes. Pla-cental abruption was defined as the complete or partialseparation of the placenta prior to delivery. A clinicaldiagnosis of this condition is usually confirmed at deliv-
ery. No data were available to determine when high-riskconditions were identified during pregnancy.
To determine the fetal death rate in pregnancies con-sidered low-risk for fetal death, an examination of fetaldeath was performed for pregnancies in the absence of vaginal bleeding, placenta previa, placental abruption,hypertensive disorders (chronic and gestational hyper-tension), diabetes, and small for gestational age births.
The risk of fetal death (per 1000 births) at each week of gestation (24 to 42ϩ completed weeks), as well as foreach high-risk condition, was calculated using the num-
ber of deaths at week “x” divided by the total number of
births (fetal death plus live births) at week “x.” Adjustedodds ratio and 95% confidence interval for fetal death ateach week of gestation were derived from multivariablelogistic regression models for each high-risk pregnancycomplication, including chronic hypertension, gesta-tional hypertensive disorders, diabetes, small for gesta-tional age births, and abruption using pregnancies at lowrisk for fetal death as the reference group.
Variables considered for adjustment as potential con-founders included maternal age, gravidity, marital sta-tus, cigarette use, maternal education, absence of prena-tal care, race/ethnicity, anemia, and intrapartum fever.
Nonlinear relationship between fetal deaths and mater-nal age was assessed by including a second-order poly-nomial for maternal age in the regression models. Thespecific variables included for adjustment are noted inthe Results section. Because odds ratio is not a goodapproximator of relative risk (RR) when the incidence of the outcome in the presence of a risk factor is h ig h, wetransformed the adjusted odds ratios to RRs.11 The
population attributable risk (percent) was derived foreach high-risk condition to assess the impact of eachcondition on fetal death.12
RESULTS
During 1995–1997, 11,885,214 pregnancies occurred inthe United States. Of these, 1,153,511 were excludedsequentially owing to either multiple births (n ϭ338,489), chromosomal abnormalities or congenital mal-formations (n ϭ 634,813), or those with birth weight lessthan 500 g or gestational age less than 24 weeks (n ϭ180,209). Furthermore, an additional 117,024 pregnan-cies with placenta previa or unexplained uterine bleeding
1184 Smulian et al Fetal Death in High-Risk Conditions OBSTETRICS & GYNECOLOGY

7/28/2019 Fetal_Deaths_in_the_United_States__Influence_of.7.pdf
http://slidepdf.com/reader/full/fetaldeathsintheunitedstatesinfluenceof7pdf 3/7
(without a diagnosis of abruption) were excluded, leav-ing 10,614,679 singleton births for analysis. The popula-
tion descriptions for low-risk pregnancies and each high-risk complication are shown in Table 1. Compared withthe low-risk pregnancies, infants of mothers with hyper-tensive diseases or abruption were delivered earlier andweighed less.
Gestational age–specific fetal death rates for low- andhigh-risk pregnancies are shown in Figure 1. Death ratesfor the examined complications are higher and roughly
parallel to the rates for low-risk pregnancies across theentire spectrum of gestational age. All fetal death ratesdecrease with advancing gestational age; however, thedeath rate related to abruption decreases much less
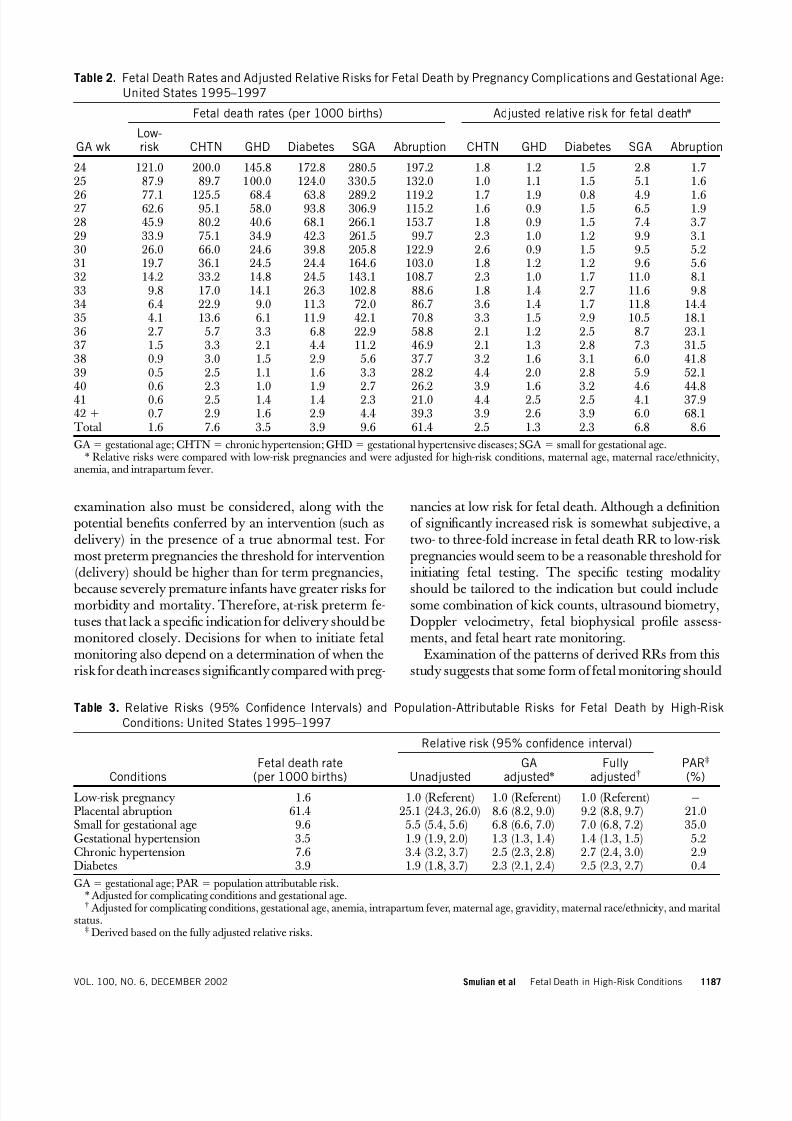
dramatically. Overall fetal death rates were lowest from38 to 41 weeks and increased thereafter for most condi-tions. The fetal death rates for low-risk pregnancies andthe adjusted RRs for fetal death by pregnancy complica-tion are reported for each week of gestation in Table 2.For all pregnancy complications examined, the RR forfetal death was increased across almost all gestationalages. The magnitude of increased risk was greatest for
pregnancies complicated by abruption, especially in thethird trimester, followed by the presence of a small forgestational age infant. For chronic hypertensive diseasesand diabetes, the magnitude of higher RR for fetal death
over low-risk pregnancies tended to increase two- tothree-fold near 34 weeks. The RR for fetal death forsmall for gestational age births remained elevated morethan four-fold throughout gestation. The proportion of all fetal deaths occurring at 38 weeks and beyond among low-risk pregnancies was 34.4% (4787 of 13,935); the
proportion of fetal deaths at or beyond 38 weeks among high-risk conditions was 28.2% (4442 of 15,735). Over-all, high-risk pregnancies accounted for 51.9% of the fetaldeaths at or beyond 38 weeks.
The overall unadjusted and adjusted RR for fetaldeath by high-risk condition is shown in Table 3. Abrup-
tion conferred the overall highest RR, followed by smallfor gestational age births, chronic hypertension, diabe-tes, and gestational hypertensive disorders. The popula-tion-attributable risks for fetal death by pregnancy com-
plications also are described in Table 3. The attributablerisks were adjusted for the other complicating condi-tions, as well as for gestational age at delivery, to isolatethe population risk conferred by each condition. Over50% of fetal deaths were attributable to either the pres-ence of a small for gestational age birth or abruption.Hypertensive diseases accounted for 8.1% and diabetesfor 0.4% of fetal deaths.
DISCUSSION
This large, population-based study demonstrates thatfetal death rates in pregnancies with and without high-risk conditions were lowest from 38 to 41 weeks’ gesta-tion. In the presence of hypertensive diseases, diabetes,small for gestational age births, and placental abruption,fetal death rates are dramatically increased comparedwith pregnancies without these complications. The in-creased risks persisted across all gestational ages, but
were highest for those with growth restriction and thosehaving abruption. The true magnitudes of elevated risk, particularly at later gestational ages, may be higher thanthose reported ( Table 2) because many of these pregnan-cies may have had fetal testing with obstetric interven-tion for abnormal tests. It is also possible that some
pregnancies were incorrectly categorized as low risk because of missing information about high-risk condi-tions. This would lead to further underestimates of theRR or fetal death.
Table 1. Description of Pregnancies With High-Risk Conditions: United States 1995–1997
Low-riskpregnancies
Chronichypertension
Gestationalhypertensive
disorders DiabetesSmall for
gestational agePlacentalabruption
Total births 8,938,313 68,639 387,831 220,621 940,923 58,352Number of fetal deaths 13,935 524 1358 850 9068 3581Fetal death rate
(per 1000)1.6 7.6 3.5 3.9 9.6 61.4
Age (y)* 26.9 (6.1) 30.3 (6.2) 26.5 (6.4) 29.8 (5.9) 25.7 (6.3) 27.3 (6.4)Race/ethnicity (%)
White 81 70 80 78 69 77Black 14 27 17 14 25 19Other 5 3 3 8 6 4
Gestational age (wk)* 39.1 (2.3) 38 (3.0) 38.2 (2.8) 38.6 (2.4) 39 (2.4) 36 (4.4)Birth weight (g)* 3455 (493) 3119 (769) 3131 (738) 3460 (642) 2529 (411) 2614 (904)*Data are presented as mean (standard deviation).
1185VOL. 100, NO. 6, DECEMBER 2002 Smulian et al Fetal Death in High-Risk Conditions

7/28/2019 Fetal_Deaths_in_the_United_States__Influence_of.7.pdf
http://slidepdf.com/reader/full/fetaldeathsintheunitedstatesinfluenceof7pdf 4/7
It is likely that many patients with the high-risk condi-tions may have been managed with antepartum testing,so our observations may not reflect “natural history.”
The fetal death rates may have been influenced by physicians’ decisions about the timing of testing andtiming of interventions. Even though there are no ran-domized controlled trials of antepartum fetal testing for
prevention of fetal death, there are other data that sug-gest that testing has reduced the fetal death rate in somesituations.13 Therefore, the fetal death rates for high-risk
conditions reported in this analysis may be biased to-ward an optimum lower rate. Although our results rep-resent fetal death risks under current management prac-tices in the United States, some additional inferencesregarding management may be justified by this analysis.
The consistently increased risk for fetal death in theexamined high-risk conditions suggests that antenatalfetal testing is justified in their presence. Decisions as towhen to start fetal testing should be based on the magni-tude of risk for fetal death. The risks of the false-positive
Figure 1. Fetal death rates by gestational age for low-risk pregnancies (filled circles) and those with placental abruption
(open circles), chronic hypertension (open triangles), gestational hypertension (open squares), diabetes (open diamonds),
and small for gestational births (asterisks).
Smulian. Fetal Death in High-Risk Conditions. Obstet Gynecol 2002.
1186 Smulian et al Fetal Death in High-Risk Conditions OBSTETRICS & GYNECOLOGY
7/28/2019 Fetal_Deaths_in_the_United_States__Influence_of.7.pdf
http://slidepdf.com/reader/full/fetaldeathsintheunitedstatesinfluenceof7pdf 5/7
examination also must be considered, along with the potential benefits conferred by an intervention (such asdelivery) in the presence of a true abnormal test. Formost preterm pregnancies the threshold for intervention(delivery) should be higher than for term pregnancies,
because severely premature infants have greater risks formorbidity and mortality. Therefore, at-risk preterm fe-tuses that lack a specific indication for delivery should bemonitored closely. Decisions for when to initiate fetalmonitoring also depend on a determination of when therisk for death increases significantly compared with preg-
nancies at low risk for fetal death. Although a definitionof significantly increased risk is somewhat subjective, atwo- to three-fold increase in fetal death RR to low-risk
pregnancies would seem to be a reasonable threshold forinitiating fetal testing. The specific testing modality
should be tailored to the indication but could includesome combination of kick counts, ultrasound biometry,Doppler velocimetry, fetal biophysical profile assess-ments, and fetal heart rate monitoring.
Examination of the patterns of derived RRs from thisstudy suggests that some form of fetal monitoring should
Table 2. Fetal Death Rates and Adjusted Relative Risks for Fetal Death by Pregnancy Complications and Gestational Age:
United States 1995–1997
GA wk
Fetal death rates (per 1000 births) Adjusted relative risk for fetal death*
Low-risk CHTN GHD Diabetes SGA Abruption CHTN GHD Diabetes SGA Abruption
24 121.0 200.0 145.8 172.8 280.5 197.2 1.8 1.2 1.5 2.8 1.725 87.9 89.7 100.0 124.0 330.5 132.0 1.0 1.1 1.5 5.1 1.6
26 77.1 125.5 68.4 63.8 289.2 119.2 1.7 1.9 0.8 4.9 1.627 62.6 95.1 58.0 93.8 306.9 115.2 1.6 0.9 1.5 6.5 1.928 45.9 80.2 40.6 68.1 266.1 153.7 1.8 0.9 1.5 7.4 3.729 33.9 75.1 34.9 42.3 261.5 99.7 2.3 1.0 1.2 9.9 3.130 26.0 66.0 24.6 39.8 205.8 122.9 2.6 0.9 1.5 9.5 5.231 19.7 36.1 24.5 24.4 164.6 103.0 1.8 1.2 1.2 9.6 5.632 14.2 33.2 14.8 24.5 143.1 108.7 2.3 1.0 1.7 11.0 8.133 9.8 17.0 14.1 26.3 102.8 88.6 1.8 1.4 2.7 11.6 9.834 6.4 22.9 9.0 11.3 72.0 86.7 3.6 1.4 1.7 11.8 14.435 4.1 13.6 6.1 11.9 42.1 70.8 3.3 1.5 2.9 10.5 18.136 2.7 5.7 3.3 6.8 22.9 58.8 2.1 1.2 2.5 8.7 23.137 1.5 3.3 2.1 4.4 11.2 46.9 2.1 1.3 2.8 7.3 31.538 0.9 3.0 1.5 2.9 5.6 37.7 3.2 1.6 3.1 6.0 41.839 0.5 2.5 1.1 1.6 3.3 28.2 4.4 2.0 2.8 5.9 52.1
40 0.6 2.3 1.0 1.9 2.7 26.2 3.9 1.6 3.2 4.6 44.841 0.6 2.5 1.4 1.4 2.3 21.0 4.4 2.5 2.5 4.1 37.942 ϩ 0.7 2.9 1.6 2.9 4.4 39.3 3.9 2.6 3.9 6.0 68.1 Total 1.6 7.6 3.5 3.9 9.6 61.4 2.5 1.3 2.3 6.8 8.6
GA ϭ gestational age; CHTN ϭ chronic hypertension; GHD ϭ gestational hypertensive diseases; SGA ϭ small for gestational age.* Relative risks were compared with low-risk pregnancies and were adjusted for high-risk conditions, maternal age, maternal race/ethnicity,
anemia, and intrapartum fever.
Table 3. Relative Risks (95% Confidence Intervals) and Population-Attributable Risks for Fetal Death by High-Risk
Conditions: United States 1995–1997
ConditionsFetal death rate
(per 1000 births)
Relative risk (95% confidence interval)
PAR‡
(%)UnadjustedGA
adjusted*Fully
adjusted†
Low-risk pregnancy 1.6 1.0 (Referent) 1.0 (Referent) 1.0 (Referent) —Placental abruption 61.4 25.1 (24.3, 26.0) 8.6 (8.2, 9.0) 9.2 (8.8, 9.7) 21.0Small for gestational age 9.6 5.5 (5.4, 5.6) 6.8 (6.6, 7.0) 7.0 (6.8, 7.2) 35.0Gestational hypertension 3.5 1.9 (1.9, 2.0) 1.3 (1.3, 1.4) 1.4 (1.3, 1.5) 5.2Chronic hypertension 7.6 3.4 (3.2, 3.7) 2.5 (2.3, 2.8) 2.7 (2.4, 3.0) 2.9Diabetes 3.9 1.9 (1.8, 3.7) 2.3 (2.1, 2.4) 2.5 (2.3, 2.7) 0.4
GA ϭ gestational age; PAR ϭ population attributable risk.* Adjusted for complicating conditions and gestational age.† Adjusted for complicating conditions, gestational age, anemia, intrapartum fever, maternal age, gravidity, maternal race/ethnicity, and marital
status.‡ Derived based on the fully adjusted relative risks.
1187VOL. 100, NO. 6, DECEMBER 2002 Smulian et al Fetal Death in High-Risk Conditions

7/28/2019 Fetal_Deaths_in_the_United_States__Influence_of.7.pdf
http://slidepdf.com/reader/full/fetaldeathsintheunitedstatesinfluenceof7pdf 6/7
be in place by 32–34 weeks for women with chronichypertension or diabetes. Because of the consistentlyhigh risk conferred by the presence of small for gesta-tional age, testing should be considered when a smallfetus (Ͻ10th centile) is diagnosed, especially when thereis an abnormal growth velocity or biometry is asymmet-ric. Based on the information provided from this study,
delivery should be considered as early as 38 weeks, butno later than 41 weeks, for all pregnancies with thesecomplications instead of continued surveillance. This isthe time when fetal death rates are at or near their lowestlevels and yet remain well above the fetal death rates formore normal pregnancies. Although we do not haveinformation from this cohort regarding the use or timing of antepartum testing in patients with high-risk condi-tions, it still seems reasonable to conclude that the riskfor fetal death in high-risk conditions is the lowest at38–41 weeks.
For women with gestational hypertensive disorders,
the RR for fetal death remains below 2 until 39 weeks. This may reflect the modifying effects of intervention bydelivery on the risk for death and not the true risks, perse. Certainly, women with the more advanced degrees of gestational hypertensive disorders (preeclampsia andeclampsia) should be considered for delivery at the timeof diagnosis, regardless of the fetal condition, because of the maternal risks.
The correct assignment of gestational age is importantfor calculating age-specific fetal death risks. Because fetaldeath always occurs prior to delivery, the use of deliverygestational age as a surrogate for age at fetal death will
likely overestimate the gestational age assigned for theactual death. This may result in some overestimation of the number of infants that are small for gestational age.Nevertheless, most fetal deaths are detected close to timeof death because mothers usually seek care when fetalmovements decrease or stop.14 It has been reported that,when managed expectantly, at least 90% of women willspontaneously develo p labor within 2 weeks of the diag-nosis of fetal demise.14 In recent years, the majority of
pregnancies with a demise are not managed expectantly, but are rather induced. Therefore, we believe that gesta-tional age at delivery is a reasonable estimate for gesta-
tional age of fetal death in most cases. The vital statisticsdatabase does not distinguish between antepartum andintrapartum fetal death, but because of the low rate of intrapartum death with current methods of fetal moni-toring during labor,15 the overwhelming majority of fetaldeaths recorded will be antepartum.
Of particular interest is the finding that over 50% of fetal deaths are attributable to either the presence of afetus that is small for gestational age or abruption. Thissuggests that it is mandatory to develop strategies di-
rected toward risk assessment and management of thesetwo conditions to reduce the number of fetal deaths.Fetuses that are at risk for being small for gestational agedue to uteroplacental insufficiency may be identified inthe second trimester using ultrasound Doppler velocim-etry screening of the uterine arteries.16 They also may beidentified from a history of previous growth restriction.
Similarly, women who are at high-risk for abruption may be identified by history or the presence of associatedat-risk conditions.17–20 Nevertheless, a widely accepteddefinition of high-risk status for abruption that carriesacceptable predictive values has not been established.Optimum testing modalities that would minimize false-
positive tests leading to unnecessary interventions alsoremain to be defined. It should be noted that by exclud-ing cases of unexplained vaginal bleeding, many cases of true abruption were not analyzed. This may have biasedthe results toward stronger associations between abrup-
tion and fetal deaths.It is important to acknowledge that recommendationsfor initiating testing to prevent fetal death that are in-ferred from these population-based data should be inter-
preted cautiously and may not substantially change cur-rent management of high-risk pregnancies in the UnitedStates. This is particularly true if most of such pregnan-cies are already managed using various testing modali-ties. It may not be possible to significantly improve fetaldeath rates before term if management is already opti-mized. Unfortunately, there are no population-basedstudies that describe the use of fetal testing in high-risk
pregnancies that describe variations in use or appropri-ateness of fetal testing; however, delivery as soon as a
patient reaches term, rather than continuation of preg-nancy for these conditions, would reduce an important
proportion of fetal death. Our data supports a strategy of consideration for delivery beginning around 38 weeks of
pregnancy, and certainly by 41 weeks, in the presence of high-risk conditions, because there is little additionalfetal benefit to be gained from pregnancy prolongation tooffset the persistently increased risk for fetal death. Thisappears to lend credence to traditional obstetric dogma
that women with high-risk conditions generally should be delivered by their due date.
REFERENCES
1. Kochenour NK. Other causes of fetal death. Clin ObstetGynecol 1987;30:312–21.
2. Fretts RC, Boyd ME, Usher RH, Usher HA. The chang-ing pattern of fetal death, 1961–1988. Obstet Gynecol1992;79:35–9.
1188 Smulian et al Fetal Death in High-Risk Conditions OBSTETRICS & GYNECOLOGY

7/28/2019 Fetal_Deaths_in_the_United_States__Influence_of.7.pdf
http://slidepdf.com/reader/full/fetaldeathsintheunitedstatesinfluenceof7pdf 7/7
3. American College of Obstetricians and Gynecology. Ante- partum fetal surveillance. 2000 compendium ACOG prac-tice bulletin no. 9. Washington, DC: American College of Obstetricians and Gynecologists, 1999:927–37.
4. Harman CR, Menticoglou SM. Fetal surveillance in dia- betic pregnancy. Curr Opin Obstet Gynecol 1997;9:83–90.
5. Snijders R, Hyett J. Fetal testing in intrauterine growthretardation. Curr Opin Obstet Gynecol 1997;9:91–5.
6. Sholl JS. Abruptio placenta: Clinical management in non-acute cases. Am J Obstet Gynecol 1987;156:40–51.
7. Antepartum fetal monitoring. In: Freeman RK, Garite TJ,Nageotte MP, eds. Fetal heart rate monitoring, 2nd ed.Baltimore: Williams & Wilkins, 1991:156–78.
8. MacDorman MF, Atkinson JO. Infant mortality statisticsfrom the linked birth/infant death data set—1995 perioddata. Natl Vital Stat Rep 1998;4 Suppl 2:1–220.
9. Taffel S, Johnson D, Heuse R. A method of imputing length of gestation on birth certificates. Vital Health Stat 21982;93:1–11.
10. Taffel SM,VenturaSJ, Gay GA. Revised U.S. certificate of birth—New opportunities for research on birth outcome.Birth 1989;16:188–93.
11. Zhang J, Yu FK. What’s the relative risk? A method of correcting the odds ratio in cohort studies of commonoutcomes. JAMA 1998;280:1690–1.
12. Eide GE, Gefeller O. Sequential and average attributablefractions as aids in the selection of preventive strategies. J Clin Epidemiol 1995;48:645–55.
13. Ananth CV, Smulian JC, Vintzileos AM. Epidemiology of antepartum fetal testing. Curr Opin Obstet Gynecol 1997;9:101–6.
14. Tricomi V, Kohl SG. Fetal death in utero. Am J ObstetGynecol 1957;74:1092–7.
15. Sheiner E, Hallak M, Shoham-Vardi I, Goldstein D,Mazor M, Katz M. Determining risk factors for intrapar-tum fetal death. J Reprod Med 2000;45:419–24.
16. Harrington K, Cooper D, Lees C, Hecher K, Campbell S.Doppler ultrasound of the uterine arteries: The impor-tance of bilateral notching in the prediction of preeclamp-sia, placental abruption or delivery of a small-for-gestation-al-age baby. Ultrasound Obstet Gynecol 1996;7:182–8.
17. Lockwood CJ. Heritable coagulopathies in pregnancy.Obstet Gynecol Surv 1999;54:754–65.
18. de Vries JIP, Dekker GA, Huijgens PC, Jakobs C,Blomberg BME, van Geijn HP. Hyperhomocysteinaemiaand protein S deficiency in complicated pregnancies. Br JObstet Gynaecol 1997;104:1248–54.
19. Kupfermic MJ, Eldor A, Steinman N, Many A, Bar-Am A, Jaffa A, et al. Increased frequency of genetic thrombophiliain women with complications of pregnancy. N Engl J Med1999;340:9–13.
20. Ananth CV, Savitz DA, Williams MA. Placental abruptionand its association with hypertension and prolonged rup-ture of the membranes: A methodologic review and meta-analysis. Obstet Gynecol 1996;88:309–18.
Reprints are not available. Address correspondence to: John C.Smulian, MD, MPH, UMDNJ-RWJMS/Saint Peter’s Univer-sity Hospital, 254 Easton Avenue, MOB– 4th Floor, NewBrunswick, NJ 08903-0591; E-mail: [email protected].
Received March 4, 2002. Received in revised form May 18, 2002. Accepted May 30, 2002.
1189VOL. 100, NO. 6, DECEMBER 2002 Smulian et al Fetal Death in High-Risk Conditions


















