Femoro-Acetabular Impingement-Dr. M.N. Basu Mallick
19
DR M.N.BASU MALLICK ARTHROSCOPY AND SPORTS SURGERY APOLLO GLENEAGLES HOSPITAL, KOLKATA Femoro-Acetabular impingement Does Labrectomy have a role?
-
Upload
therightdoctors -
Category
Health & Medicine
-
view
422 -
download
1
Transcript of Femoro-Acetabular Impingement-Dr. M.N. Basu Mallick
DR M.N.BASU MALLICKA R T H R O S C O P Y A N D S P O R T S S U R G E R Y
A P O L L O G L E N E A G L E S H O S P I T A L , K O L K A T A
Femoro-Acetabular impingement
Does Labrectomy have a role?
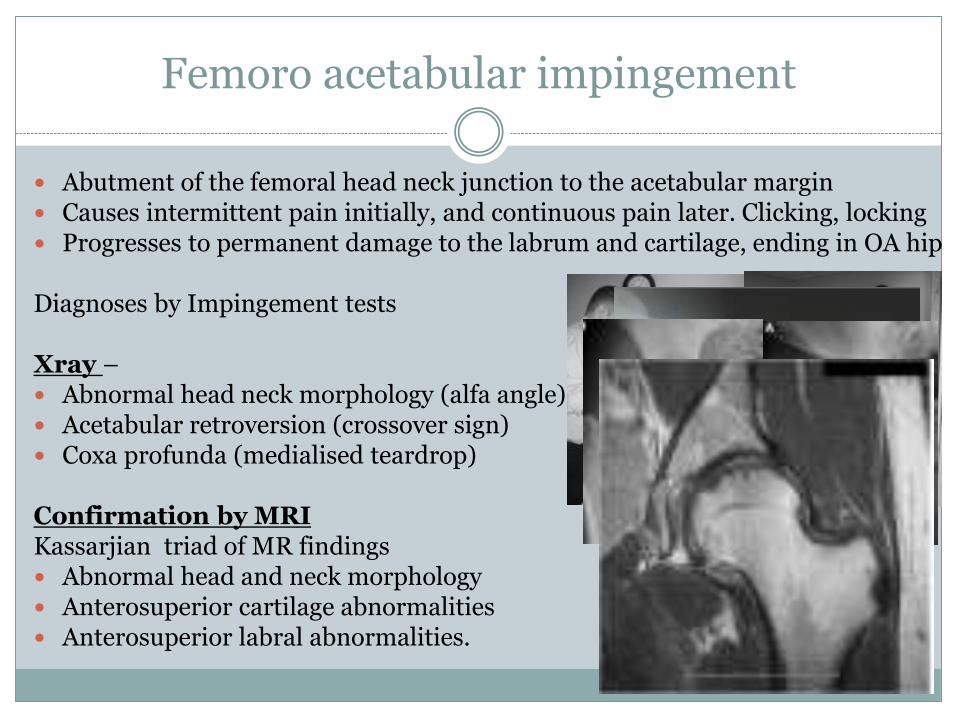
Femoro acetabular impingement
Abutment of the femoral head neck junction to the acetabular margin Causes intermittent pain initially, and continuous pain later. Clicking, locking Progresses to permanent damage to the labrum and cartilage, ending in OA hip
Diagnoses by Impingement tests
Xray – Abnormal head neck morphology (alfa angle) Acetabular retroversion (crossover sign) Coxa profunda (medialised teardrop)
Confirmation by MRIKassarjian triad of MR findings Abnormal head and neck morphology Anterosuperior cartilage abnormalities Anterosuperior labral abnormalities.
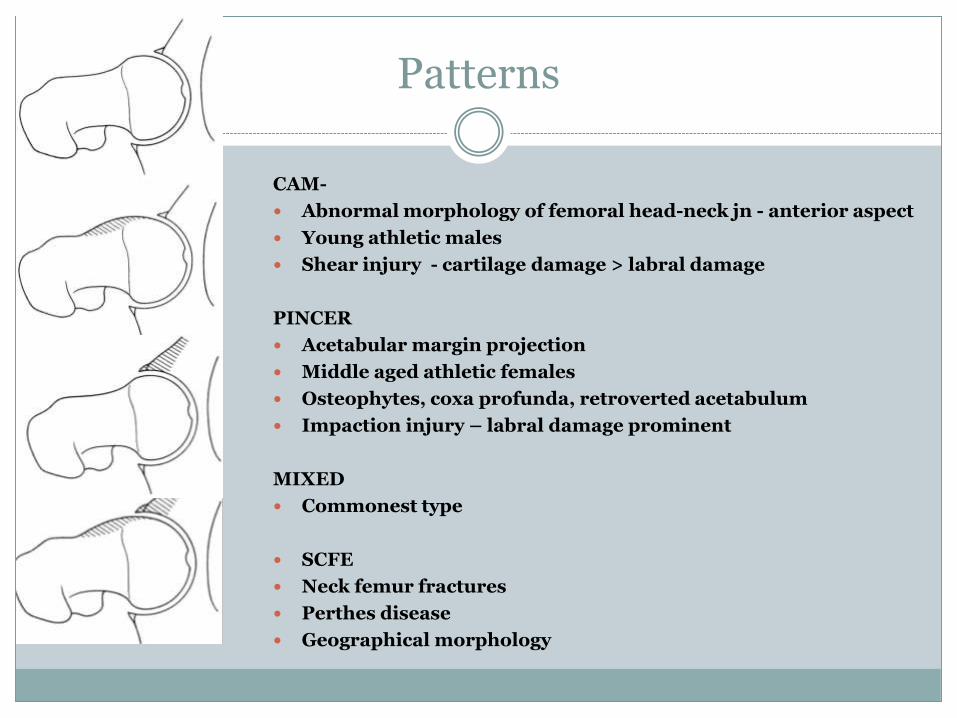
Patterns
CAM-
Abnormal morphology of femoral head-neck jn - anterior aspect
Young athletic males
Shear injury - cartilage damage > labral damage
PINCER
Acetabular margin projection
Middle aged athletic females
Osteophytes, coxa profunda, retroverted acetabulum
Impaction injury – labral damage prominent
MIXED
Commonest type
SCFE
Neck femur fractures
Perthes disease
Geographical morphology
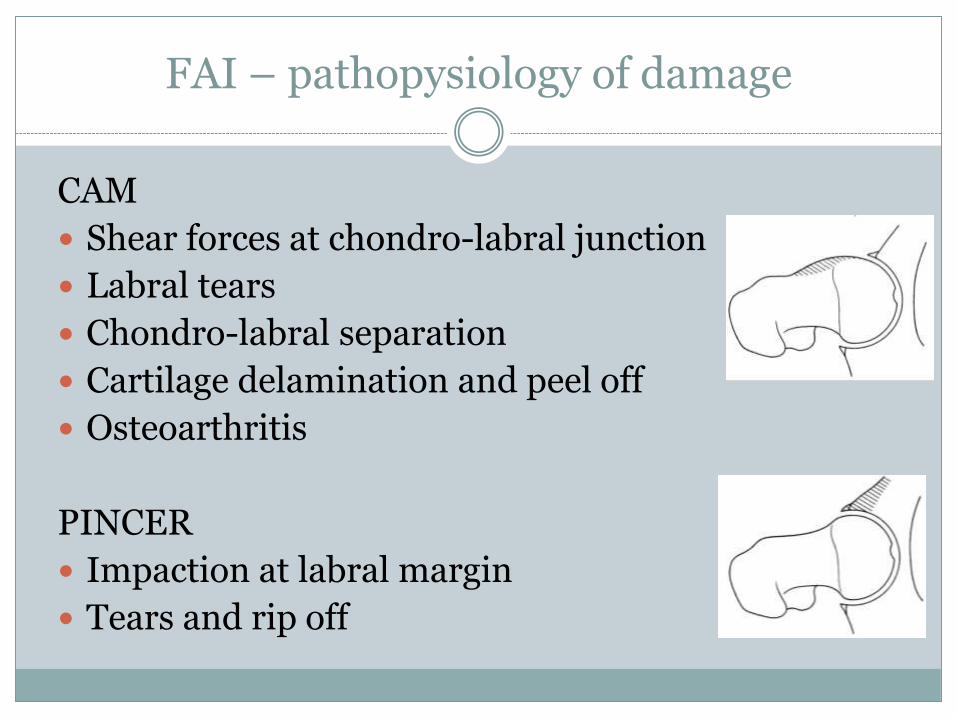
FAI – pathopysiology of damage
CAM
Shear forces at chondro-labral junction
Labral tears
Chondro-labral separation
Cartilage delamination and peel off
Osteoarthritis
PINCER
Impaction at labral margin
Tears and rip off
Treatment philosophy
Conservative
Restriction of inciting activity
Surgery
To restore normal roll and glide of the joint
Excision of the extra bone from the femoral head neck junction (cam)
Rim trimming of the acetabular margin (pincer)
Labrum is reattached if torn / surgically detached for rim trim
OPEN/ ARTHROSCOPIC/ ARTHROSCOPY+OPEN
The Labrum
Increases containment / inreases stability
Suction socket principle – creates a fluid film that prevents close contact within the joint
EVIDENCE
Routine repair of the labrum resulted in higher clinical scores in studies that compared labralrepair with without labral repair in the management of pincer-type FAI (Espinosa et al./ Larson et al.)
A case for LABRECTOMY
Role of labrum in containment and stability in non dysplastic hips – DOUBTFUL
Suction socket mechanism disrupted with damaged labrum, damaged cartilage, aspherical contour and inflammatory synovial fluid
Restoration of normal biomechanics in a repaired labrum – DOUBTFUL
Healing of labrum of limited vascularity - DOUBTFUL
A case for LABRECTOMY
EVIDENCE
Sustained improvement in clinical scores after isolated labral débridement of various patterns of labraldamage in patients without synovitis or arthritis (Byrd and Jones / Santori and Villar / Farjo et al/ Haviv and
O’Donnell )
In vitro biomechanical data suggest there is nil deleterious effect after the removal or detachment of small amounts of the labrum (Greaves et al/ Smith et al. )
Material And Method
10 hips, 8patients- 6males 2 females / Age 27-48
June 2011- June 2013 / follow up 13m – 36m
Diagnosis Pincer type 3 (osteophyte 3)
Mixed type 7 ( healed AVN 2/ ?healed perthes 1/ Idio 4)
Cam type 1 excluded from this study
Arthroscopic labral excision for pincer/mixed FAI
Cartilage status evaluated by OUTERBRIDGE SCALE
Post op follow up at 1m/2m/6m/6monthly
FU evaluated by Roles-modesly Score / Oxford Hip Score
Hip arthroscopic instrumentation/30 deg 4mm scope
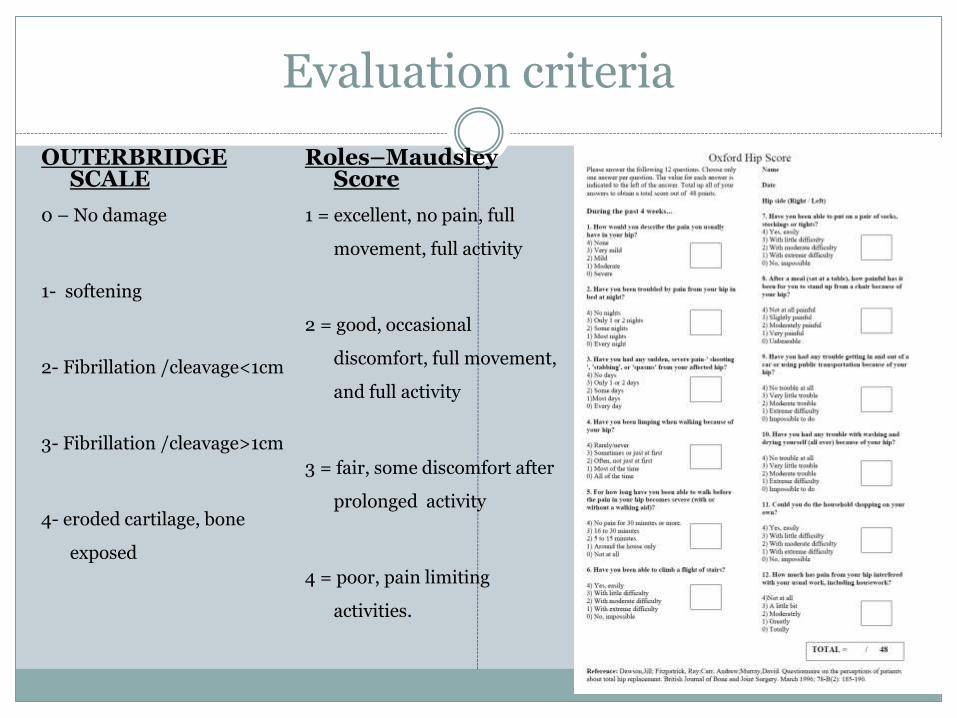
Evaluation criteria
OUTERBRIDGE SCALE
0 – No damage
1- softening
2- Fibrillation /cleavage<1cm
3- Fibrillation /cleavage>1cm
4- eroded cartilage, bone
exposed
Roles–MaudsleyScore
1 = excellent, no pain, full
movement, full activity
2 = good, occasional
discomfort, full movement,
and full activity
3 = fair, some discomfort after
prolonged activity
4 = poor, pain limiting
activities.
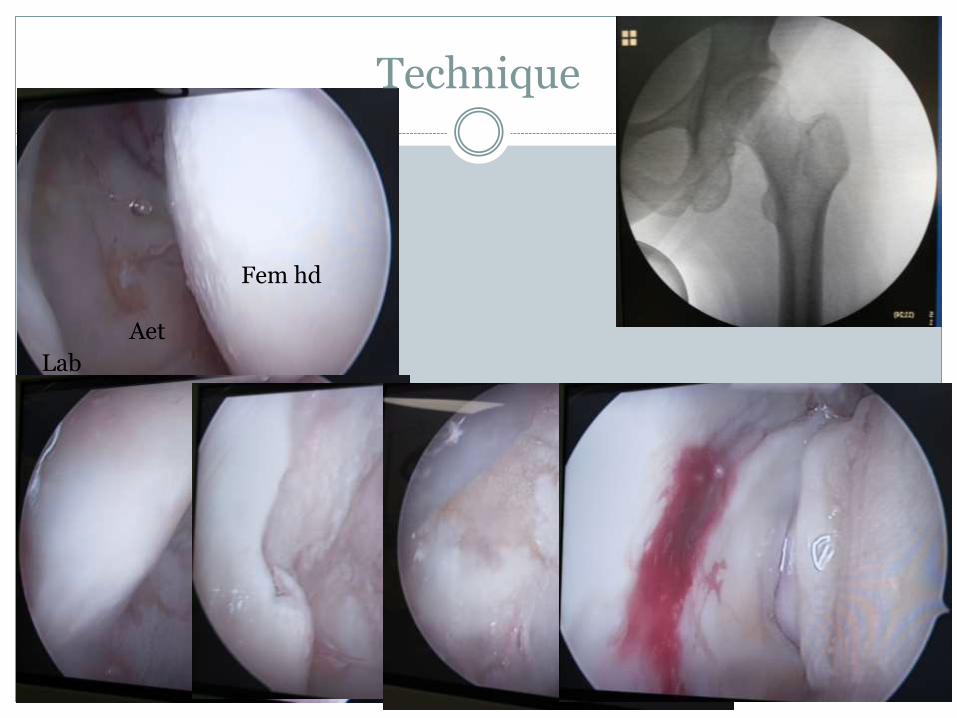
Technique
Fem hd
Lab
Aet
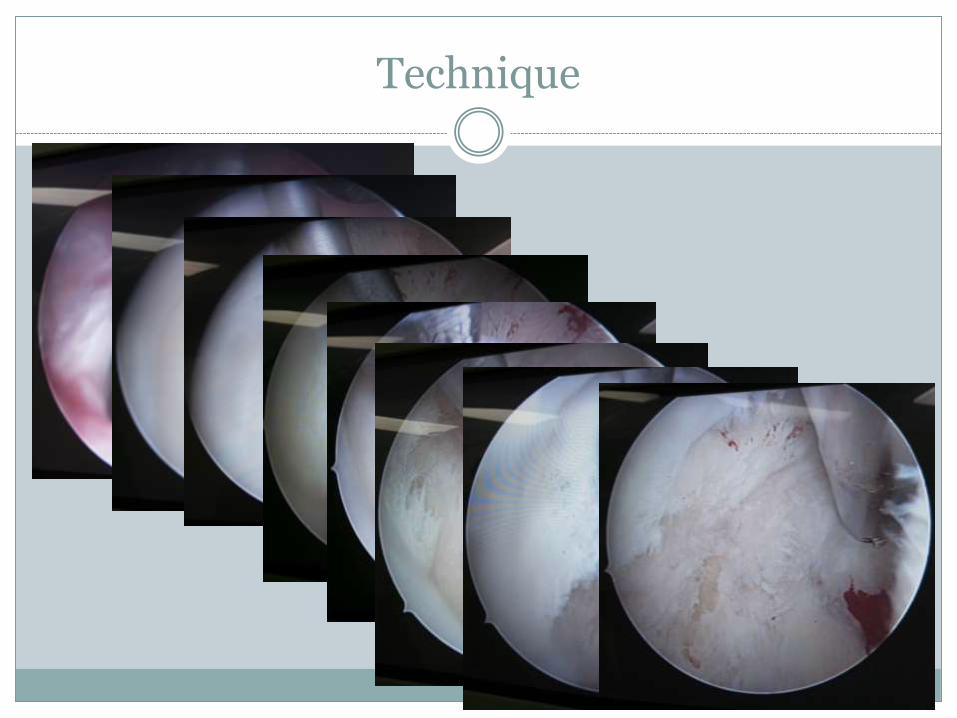
Technique
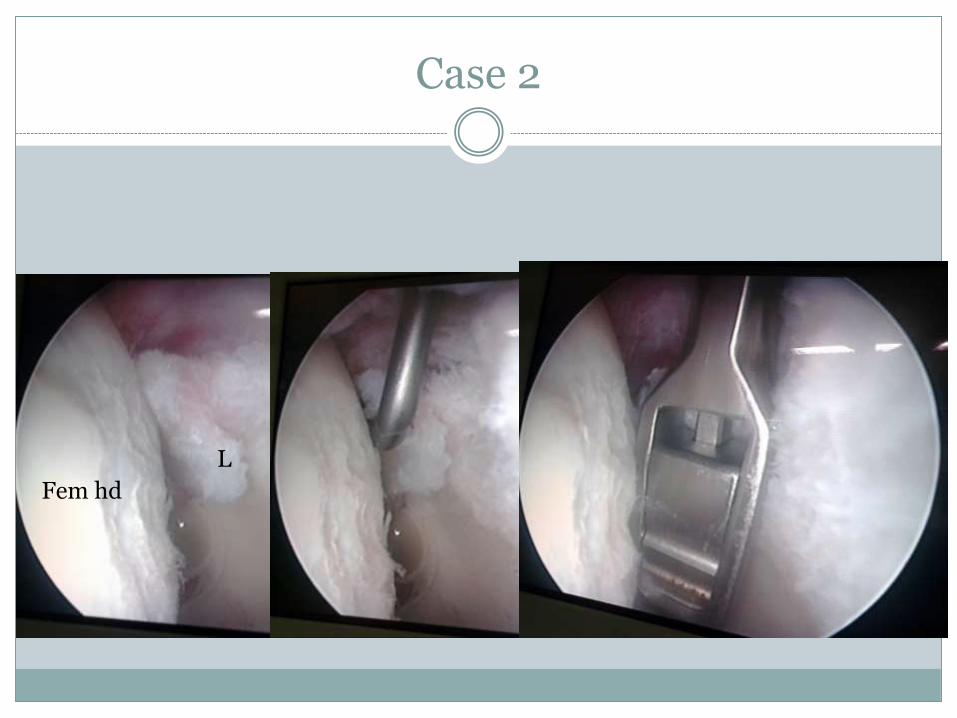
Case 2
Fem hd
L
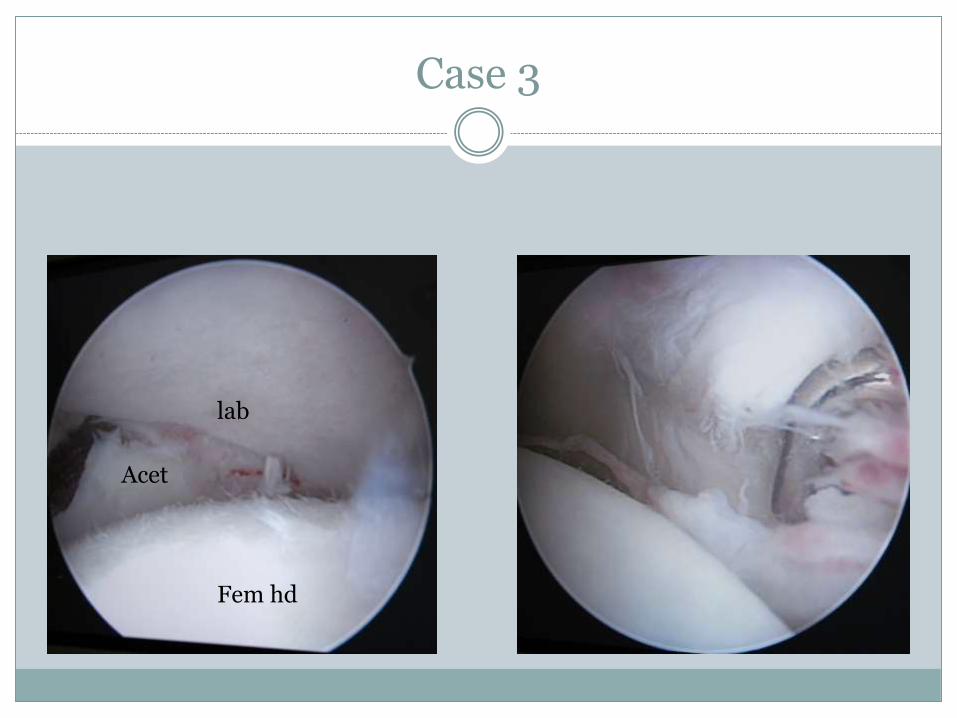
Case 3
Fem hd
lab
Acet
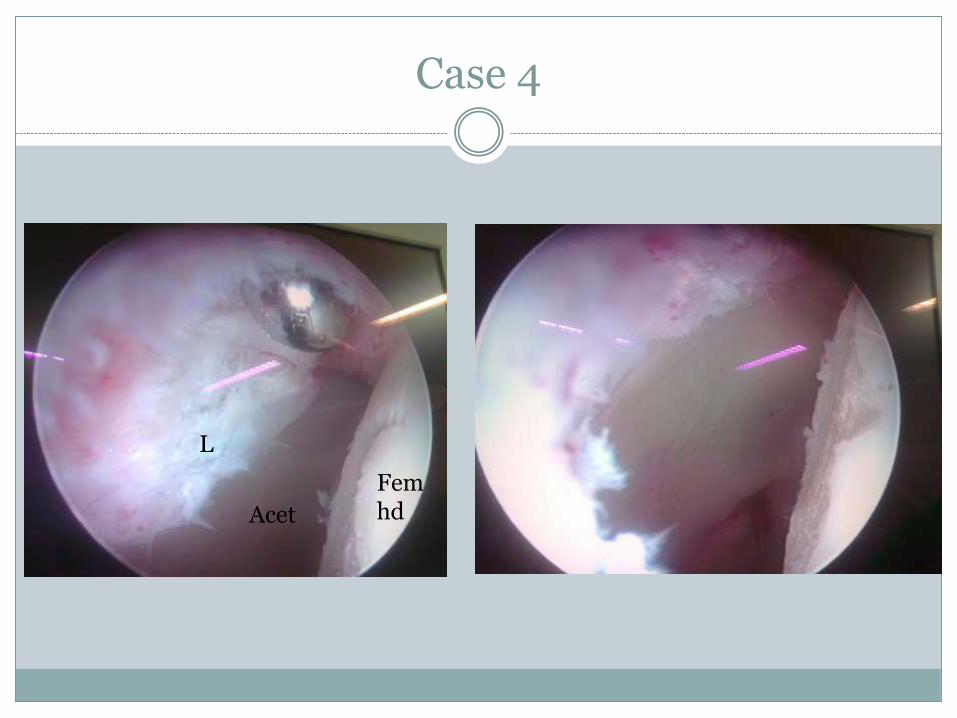
Case 4
Femhd
L
Acet
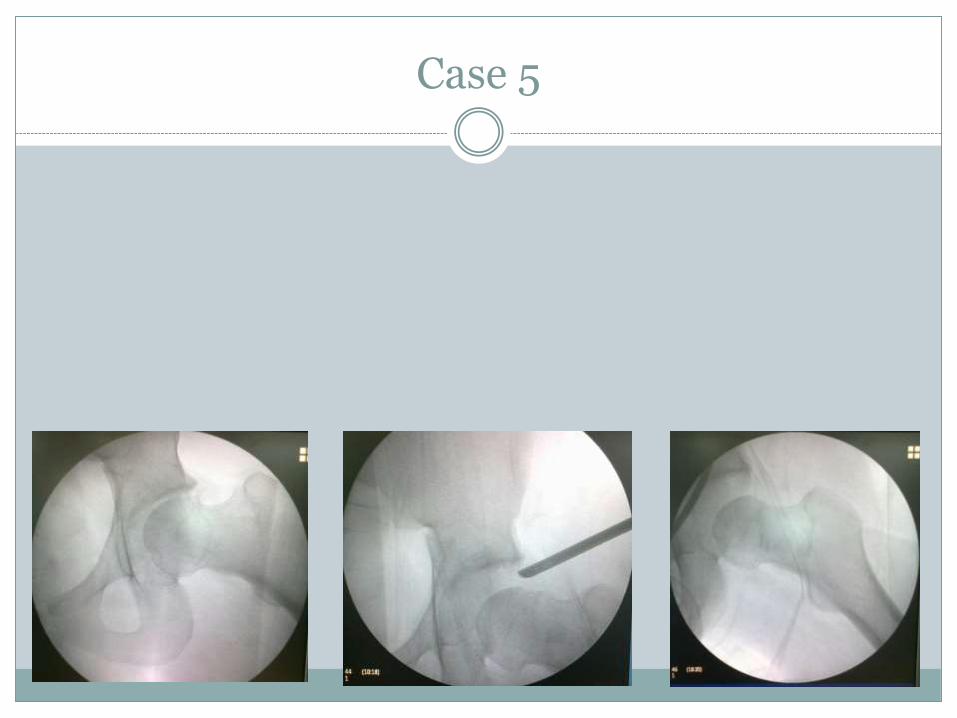
Case 5
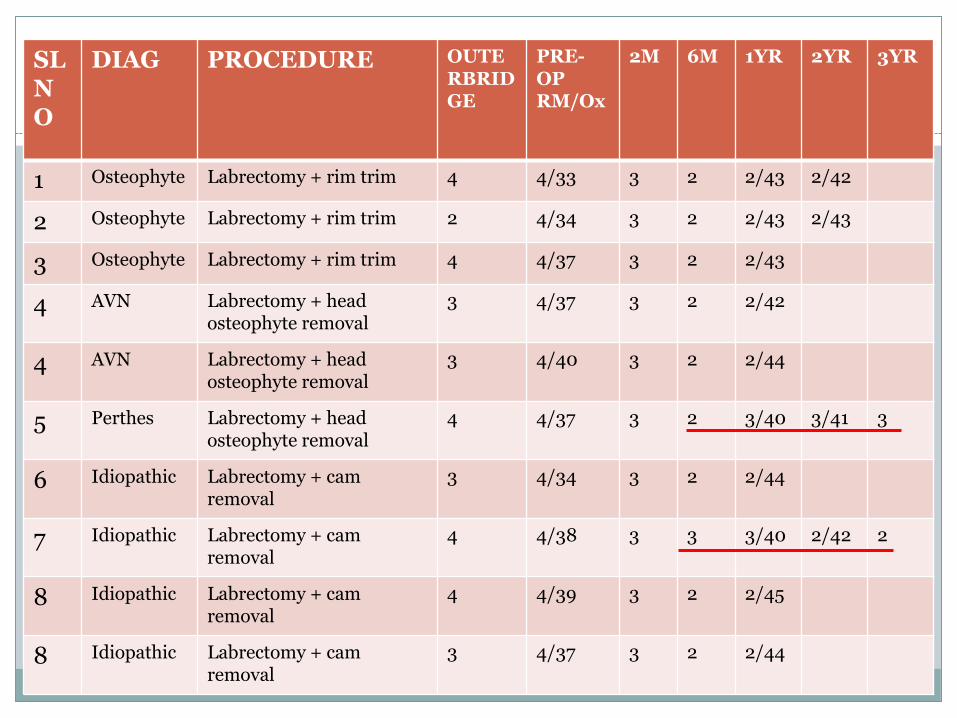
Results SL NO
DIAG PROCEDURE OUTERBRIDGE
PRE-OP RM/Ox
2M 6M 1YR 2YR 3YR
1 Osteophyte Labrectomy + rim trim 4 4/33 3 2 2/43 2/42
2 Osteophyte Labrectomy + rim trim 2 4/34 3 2 2/43 2/43
3 Osteophyte Labrectomy + rim trim 4 4/37 3 2 2/43
4 AVN Labrectomy + headosteophyte removal
3 4/37 3 2 2/42
4 AVN Labrectomy + headosteophyte removal
3 4/40 3 2 2/44
5 Perthes Labrectomy + headosteophyte removal
4 4/37 3 2 3/40 3/41 3
6 Idiopathic Labrectomy + camremoval
3 4/34 3 2 2/44
7 Idiopathic Labrectomy + camremoval
4 4/38 3 3 3/40 2/42 2
8 Idiopathic Labrectomy + camremoval
4 4/39 3 2 2/45
8 Idiopathic Labrectomy + camremoval
3 4/37 3 2 2/44
Discussion
The benefits of labral ‘repair’ in FAI is not clear and is done almost empirically. On the other hand a residual damaged labrum may continue to alter the hip biomechanics, causing continuing damage to the articular cartilage and early onset OA.
Labrectomy takes away one of the culprits and pain generators in FAI, and may be a better option biomechanically. However ‘labrectomy’ alone is not beneficial in the treatment for FAI and does not relieve pain or impingement in the presence of pathological bone (healed Perthes, AVN).
Labrectomy gives predictable favourable short term benefit in pincer and mixed type FAI
Maximal benefit is achieved in 6 months and is maintained thereafter
Grade 4 Outerbridge damage may not have long lasting benefit.
Limitation of the study
No sportsmen in the group
Labral pathology was not the only pathology that was tackled
All patients had some degree of cartilage damage (outerbridge 3/4
No cohort group of labral repair
Follow up less than 2-3 years. Long term outcome unknown.