MRI scan shows a 3- cm low- density suprarenal mass on the right side.
© Schattauer 2014 Tierärztliche Praxis Kleintiere 1/2014
55
Key wordsFeline osteochondromatosis, cat, palliative treatment, osteocartilagi-nous lesion, FELV infection
SummaryObjective: To report palliative treatment in a case of multifocal feline osteochondromatosis in a feline leukaemia virus (FeLV) negative Euro-pean shorthair cat. Case: A 6-year-old spayed female European short-hair cat was presented because of a right forelimb lameness caused by an osteochondromatous lesion which had trapped tendons, vessels and nerves of the antebrachium. Several other lesions were present which did not cause the animal discomfort. The cat was tested nega -tive for FeLV. Palliative surgical removal of the mass was performed, resulting in a marked improvement of mobility with no local recur-rence. The cat developed a non-regenerative anaemia after surgery, however the underlying cause was not identified upon request of the owner. Overall survival after surgery was only 2 months. The cat was then euthanised due to severe progression of the anaemia. Con-clusion: Palliative surgical removal of osteochondromas may result in local improvement. However, owners need to be aware that it does not increase overall survival and that the prognosis is poor. Infection with FeLV is not necessarily associated with such lesions.
SchlüsselwörterFeline osteochondromatose, palliative Behandlung, osteokartilaginöse Läsion, Katze, FELV-Infektion
ZusammenfassungGegenstand: Beschrieben wird ein Fall multifokaler feliner Osteo-chondromatose bei einer FELV-negativen Europäisch-Kurzhaar-Katze. Fall: Die 6-jährige kastrierte Katze wurde mit einer deutlichen Lahm -heit der rechten Vordergliedmaße vorgestellt. Ursache war eine osteo-chondromatöse Zubildung am Antebrachium, die Sehnen, Nerven und Gefäße einbezogen hatte. An verschiedenen anderen Lokalisationen fanden sich weitere derartige Zubildungen, die dem Tier jedoch keine Probleme bereiteten. Eine FeLV-Infektion wurde weder im Serum noch in der Läsion festgestellt. Durch die palliative chirurgische Resektion der Neubildung am Unterarm bildete sich die Lahmheitssymptomatik vollständig zurück. Postoperativ entwickelte die Katze eine aregene -rative Anämie, deren ursächliche Abklärung der Besitzer verweigerte. Zwei Monate nach der Operation musste das Tier aufgrund der An-ämie euthanasiert werden. In dieser Zeit kam es zu keinem lokalen Rezidiv oder einer erneuten Lahmheit. Schlussfolgerung: Eine palli-ative Entfernung osteochondromatöser Zubildungen kann klinische Symptome verbessern, doch bleibt die Prognose bei multifokalen Lä-sionen vorsichtig. Eine FeLV-Infektion ist bei betroffenen Tieren nicht immer nachweisbar.
Correspondence toDr. Mirja Christine NolffChirurgische und Gynäkologische KleintierklinikLudwig-Maximilians-Universität MünchenVeterinärstraße 13, 80539 MünchenGermanyEmail: [email protected]
Feline Osteochondromatose bei einer FELV-negativen Europäisch-Kurzhaar-KatzeTierärztl Prax 2014; 42 (K): 55–59Received: September 21, 2012Accepted after revision: February 26, 2013
Feline osteochondromatosis in a FELV-negative European shorthair catM. C. Nolff1,2; C. Puff3; B. Länger1; M. Fehr1
1Small Animal Clinic, University of Veterinary Medicine Hannover, Foundation, Hanover, Germany; 2Clinic for Small Animal Surgery and Reproduction, Ludwig-Maximillians-University, Munich, Germany; 3Department of Pathology, University of Veterinary Medicine Hanover, Foundation, Hanover, Germany
Introduction
Osteocartilaginous exostoses have been reported in a number of species including man (3, 7), dogs (1, 2, 4), horses (5) and cats (6, 8– 10). While the disease seems to be a hereditary skeletal growth dis-turbance in dogs and horses (9, 11, 20), in cats a hereditary pattern has not been identified except for Scottish Fold cats which have a special form known as Scottish Fold Osteodystrophy (18, 21, 26, 27).
The histological appearance of the lesions is comparable throughout different species, showing a cancellous bone out-
growth which is capped by cartilaginous tissue (9, 10, 22, 25). In the cat two different forms of the disease have been reported. In the solitary form, exostoses of cartilage capped cancellous bone arise from cartilaginous caps located in the periosteum. The aver-age age of onset is around 6 years with no known gender predis-position (3, 5). The described localisations include the spine, long bones, head, ribs and pubis (2, 10, 16, 24, 25). The clinical symp-toms caused by the lesions depend on the localisation and the mechanical impact on the surrounding structures. The prognosis after treatment by surgical excision is good, but local re-growth is a
Case Report
For personal or educational use only. No other uses without permission. All rights reserved.Downloaded from www.tieraerztliche-praxis.de on 2017-06-21 | IP: 54.191.40.80

Tierärztliche Praxis Kleintiere 1/2014 © Schattauer 2014
56
common finding (5, 24). Malignant transformation may occur. Treatment options focus on local surgical debulking, but radiation therapy or amputation have been discussed (19). While the disease is well described, the underlying causes are not elucidated. A fre-quent association with a feline leukaemia infection is generally not discussed (28). The second form has been referred to as feline os-teochondromatosis. The average age of onset is around 2–3 years with no known gender predisposition (19).
Feline osteochondromatosis is characterised by multiple os-teocartilaginous outgrowths arising from the bone cortex at vari-ous sites – including scapulae, sternum, ribs, pelvis and lumbar vertebrae with a potential predisposition for Siamese cats (5, 16, 25). The exact etiology has not been elucidated but an underlying retroviral infection has been discussed since several reported cats have been tested FELV-positive and C-type particles have been found within the lesions (3, 8, 10). Controversially, a more recent publication did not identify an underlying FELV infection (16). We report an additional case of feline osteocartilagineous in a female European shorthaired cat that has been tested negative for FELV and a palliative attempt for treatment.
The prognosis for affected animals is poor with a mean survival below one year after onset and a potential for malignant trans-formation (5, 23).
Clinical reportPatient and history
A 6-year-old spayed female European shorthair cat was presented for investigation of multiple hard masses all over the body which had developed during the previous 6 months. During 4 weeks prior to presentation a lesion around the right forelimb had grown excess-ively to form a collar around the radius and ulna. The cat had de- veloped lameness and was treated by administration of meloxicam (0.1 mg/kg once daily, Metacam®, Boehringer Ingelheim GmbH, Basel, Switzerland). Otherwise, the cat did not show any signs of dis-comfort. According to the owners the cat was fed a conventional cat diet.
Clinical examination and laboratory findings
On presentation the cat was bright, alert and responsive. The physical examination was unremarkable despite several palpable hard masses all over the body which were connected to the under-lying bone and did not cause any pain: head (0.5 cm diameter), right scapula (4 x 10 cm), right pelvis (2 x 6 cm), right tibia (2 cm diameter) as well as a bony collar around the right radius and ulna (diameter 5 cm) and smaller lesions at the left forelimb (diameter 3 cm). The cat showed moderate right forelimb lameness. A neu -ro logic examination was unremarkable.
Haematological and biochemical blood analysis were within nor-mal limits. Serum FELV-antigen as well as feline immunodeficiency virus (FIV) antibodies were tested negative using a commercially
available ELISATest Kit (Snap® FIV/FeLV Combo Test, IDEXX GmbH Ludwigsburg, Germany). Analysis of Vitamin D3 revealed a 25-hydroxy-vitamin D3 serum level of 26.11 nmol/l (reference range 20–150 nmol/l) and a 1.25-dihydroxycholecalciferol serum level of 92 pg/ml (reference range < 30 pg/ml). The serum level of parathor-mone was 9 pg/ml (reference range 3–24 pg/ml).
Diagnostic imaging
Radiographs showed several dense lesions arising from the cortex of the pelvis, right scapula, sternum, skull, tibia, as well as moder-ate bony lesions which formed around the left radius and ulna and a severe bony callus-like collar around the right radius and ulna.
The owners were informed that curative treatment was unlikely to be successful and overall prognosis was poor. Since none of the lesions seemed to cause the cat discomfort except for the massive growth around the right radius and ulna that had recently caused lameness they opted for surgical debulking of this mass in order to see if it would result in pain relief for the cat, even if the prognosis was guarded.
A computed tomography scan was performed to evaluate which structures were involved in the lesion and whether surgical removal would be sensible. General anaesthesia was induced after premedication with glycopyrrolate (0.01 mg/kg i. m., Rubinol®, Riemser Arzneimittel AG, Riems, Germany) by intramuscular ad-ministration of ketamine (10 mg/kg i.m., Ketamin, Selectavet Dr. Otto Fischer GmbH, Weyarn-Holzolling, Germany) and midazo-lam (0.3 mg/kg i. m., Midazolam B. Braun, B. Braun Melsungen AG, Melsungen, Germany). Anaesthesia was maintained by ad-ministration of isoflurane (Isofluran CP, CP-Pharma, Burgdorf, Germany) delivered in 100% oxygen after endotracheal intu-bation. Vital functions were monitored and the CT scan was per-formed in ventral recumbency (Philips Brilliance CT 64-channel Scanner, Philips Deutschland GmbH, Hamburg, Germany).
The CT identified a bone hypodense lesion of 0.5 cm diameter dorsally on the skull at the midline between both orbitae. A soft tissue swelling which extended from the metacarpalia to the elbow and contained cloudy bone hypodense structures forming a collar around the antebrachium surrounded the right forelimb. The lesions involved tendons, vessels and nerves of the antebrachium (8.4 x 4.2 x 3.6 cm). Comparable lesions of a lesser extent were vis-ible at the left antebrachium. Additional bone hypodense lesions (6 x 3.7 x 3.2 cm) were located within the muscles surrounding the right scapula, within the mediastinum (2.7 x 1.2 x 0.7 cm) and at-tached to the cranial sternum (3.4 x 1.5 x 0.7 cm). A further lesion was found within the musculus longissimus lumborum at the height of the 11/12 intercostal space (1.3 x 0.5 x 0.3 cm) and cran-ially of the right ala ossis ilii (4.1 x 2.5 x 1.4 cm). The last two lesions were located at the left hind limb, one on the medial aspect of the left knee (1.2 x 1.1 x 1 cm) and at the medial aspect of the tarsus (1.5 x 1.2 x 1 cm). (▶ Fig. 1). Due to the masses formed around the contralateral limb the owners decided against ampu-tation as an option.
M. C. Nolff et al.: Feline osteochondromatosis in a FELV-negative cat
For personal or educational use only. No other uses without permission. All rights reserved.Downloaded from www.tieraerztliche-praxis.de on 2017-06-21 | IP: 54.191.40.80
© Schattauer 2014 Tierärztliche Praxis Kleintiere 1/2014
57
Surgical procedure
Surgery was performed directly after the CT Scan. Fentanyl (5 µg/kg, Fentanyl®-Janssen, Janssen-Cilag GmbH, Neuss, Ger-many) was injected intravenously for analgesia prior to surgery and maintained by continuous rate infusion throughout the surgi-cal procedure (10–20 µg/kg per hour to effect). The cat was pre-pared for surgery and positioned in ventral recumbency. After a dorsal approach to the radius the lesion including the incorporated fascia was slowly excised using a rongeur and a scalpel blade. Care
was taken to identify vessels, nerves and tendons within the lesion which were spared from excision. In the deeper areas where the lesion met the radius and ulna it was easily peeled off the bone. During surgery the wound showed excessive diffuse bleeding from the center of the lesion which was controlled by the use of electro -cautery. The remaining soft tissues were routinely closed in layers (PDS 3.0.) and the skin was closed after resection of a small piece in order to adjust to the new diameter of the antebrachium. Radio-graphs were taken after surgery to allow objective post surgical fol-low-up of regrowth (▶ Fig. 2).
Histopathology
For histopathological analysis, samples of the resected lesion were fixed in 10% neutral-buffered formalin, decalcified in EDTA sol-ution and embedded in paraffin wax. Tissue sections were stained with haematoxylin and eosin. Additional sections were used for immunohistochemistry by applying the avidin-biotin complex method using a primary antibody directed against feline leu- kaemia virus antigen (monoclonal anti-FeLV gp70; clone C11D8; Custom Monoclonals International, Sacramento, USA) with mi- nor modifications as described by Schwab et al. (26). Briefly, sec-tions were dewaxed and antigen was demasked by citrate treat-ment for 20 minutes.
Histological examination revealed a lobulated mass which was partly covered with a collagen-rich fibrous tissue (inter-preted as periosteal remnants). The mass consisted of an osteo-chondomatous proliferation, often with a peripheral arrange-ment of the cartilaginous part (▶ Fig. 3). The degree of cartilagi-nous versus osse ous differentiation varied depending on the lo-
M. C. Nolff et al.: Feline osteochondromatosis in a FELV-negative cat
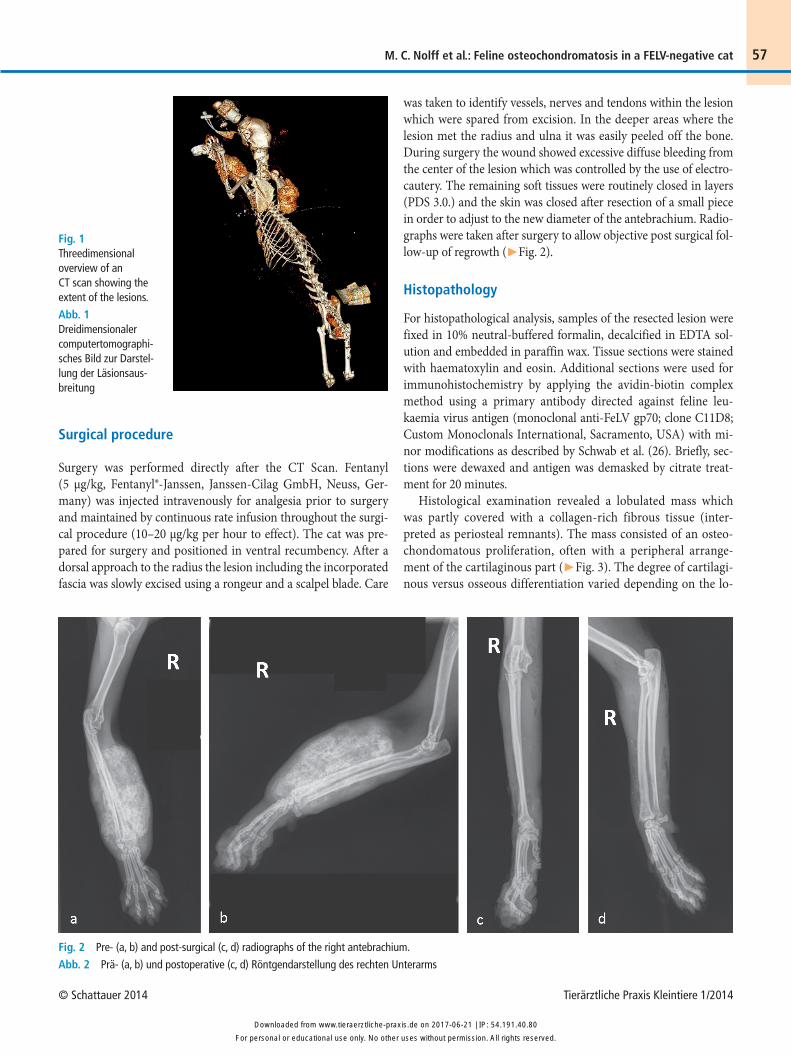
Fig. 1 Threedimensional overview of an CT scan showing the extent of the lesions.
Abb. 1 Dreidimensionaler computertomographi-sches Bild zur Darstel-lung der Läsionsaus-breitung
Fig. 2 Pre- (a, b) and post-surgical (c, d) radiographs of the right antebrachium.
Abb. 2 Prä- (a, b) und postoperative (c, d) Röntgendarstellung des rechten Unterarms
For personal or educational use only. No other uses without permission. All rights reserved.Downloaded from www.tieraerztliche-praxis.de on 2017-06-21 | IP: 54.191.40.80

Tierärztliche Praxis Kleintiere 1/2014 © Schattauer 2014
58
calisation examined. The cartilagenous tissue displayed a slightly irregular growth with a mild cellular pleomorphism. The well differentiated osseous part was primarily composed of trabecular bone. The intertrabecular marrow spaces contained a loose fi-brous connective tissue, mature adipocytes and islands of hae-matopoietic progenitor cells. There was no evidence of a malig-nant transformation and less than one mitotic figure per high power field was detected. Based on the multicenter character of the lesions and the histopathological features feline osteochon-dromatosis was diagnosed. Immunohistochemically, FeLV-anti -gen was not detected within the lesions.
Follow-up
The recovery from surgery was unremarkable. The cat was admin-istered cefazoline (2 mg/kg s. c. once daily, Excenel®, Pfizer AG, Zürich, Switzerland) and meloxicam (0.1 mg/kg once daily, Meta-cam®, Boehringer Ingelheim GmbH, Basel, Switzerland) for 7 days. Wound healing was uneventful and the cat showed full weight bearing and function of the affected limb directly after surgery.
A haematological control on the day after surgery showed anaemia with a packed cell volume (PCV) of 12% (before surgery PCV 30%, reference range 27–45%). The cat was given a whole blood transfusion (PCV after transfusion 18%), and further lab-oratory controls on days 2, 3 and 4 after surgery showed a stable PCV at 16% with no signs of regeneration. The cat was discharged 5 days after surgery and further follow-up care involving control of anaemia and re-growth were scheduled to be performed by the local veterinarian. On telephone request 2 weeks after surgery the
owners reported that the cat was doing well with full resolution of right forelimb lameness. However, 2 months after surgery the cat was euthanized due to recurrent severe anemia.
Discussion
Feline osteochondromatosis is a disease which is rarely docu-mented in cats, accounting for 20% of primary bone tumours in this species (6). Based on the literature the prognosis for the ani-mals is poor, with a reported survival time of less than one year after onset (2, 16). The presented case describes feline osteochon-dromatosis in a patient that has been tested negative for FELV and a palliative treatment approach.
While most of the lesions did not cause the animal pain, a rapid growth of osteocartilaginous tissue around the right radius and ulna which enclosed tendons, vessels and nerves of the antebra-chium caused right front limb lameness. Since the cat was not painful on palpation of the limb and no neurological impairment was detected, this lameness was most likely due to mechanical im-pairment.
Surgical debulking has been discussed as a possible palliative treatment approach for cats suffering from osteochondromatosis (5, 24) and other benign bone abnormalities such as osteomas (13). The purpose of surgical treatment was to reduce lameness and thus the quality of life for the cat. With some care taken to pre-serve vessels, nerves and tendons the lesion could be easily peeled off the underlying bone. However, the procedure was accompa-nied by substantial bleeding from the bone which necessitated a blood transfusion after surgery. Once the lesion was removed the bleeding was easily controlled. On admission the cat showed no anaemia and had a PCV of 30% (reference range 27–45%). The PCV dropped after surgery and was stable after blood transfusion (16%) but only a moderate increase in reticulocytes, indicating no regeneration was observed. Since the cat had been sent home 5 days after surgery and the owners did not carry out the advised controls we do not know if the post surgical anaemia persisted or resolved. However, given the short time between surgery and eu-thanasia it seems likely that the cat may never have fully recovered. There are numerous causes of anaemia in the cat including chronic inflammation, neoplasia, retroviral infection, iron defi-ciency, chronic blood loss, renal insufficiency, pure red cell aplasia, myelophthisis, myelofibrosis, myelonecrosis or myelodysplasia (5). Feline osteochondromatosis itself has not been directly linked to anaemia so far.
While the cat was hospitalized, findings suggesting iron defi-ciency or renal insufficiency have not been detected in blood and urine samples but none of these reasons can be excluded since no testing was performed at the time of death 2.5 months later.
Among the viral causes the FELV infection is one very common reason which has additionally been linked to the presence of multiple osteochondromas in the cat (8–10, 25). Infection of peri-ostal cells with the FELV is suspected as an aetiological source
M. C. Nolff et al.: Feline osteochondromatosis in a FELV-negative cat
Fig. 3 The osteochondromatous proliferations are covered by a collagen-rich fibrous tissue (interpreted as periosteal remnants) and display a peri -pheral arrangement of the cartilaginous part. (Haematoxylin and eosin; bar = 500 µm).
Abb. 3 Die osteochondromatösen Proliferationen sind von einem kolla-genreichen Bindegewebe bedeckt (interpretiert als periostales Restgewebe) und zeigen eine periphäre Ausrichtung des Knorpelanteils. (Hämatoxylin- Eosin; Balken = 500 µm).
For personal or educational use only. No other uses without permission. All rights reserved.Downloaded from www.tieraerztliche-praxis.de on 2017-06-21 | IP: 54.191.40.80

© Schattauer 2014 Tierärztliche Praxis Kleintiere 1/2014
59
since most of the initially reported cases were tested positive and viral particles could be found within the lesions (2, 10, 25). Atypi-cal feline fibrosarcoma virus as well as feline oncornavirus as an aetiological source have also been discussed (16, 23) but the exact mechanism has never been identified. We could not support this thesis since the cat presented in this study was tested negative for serum FeLV antigen and FeLV particles were not identified within the lesion. This finding is consistent with another more recent report of feline osteochondromatosis by Levitin et al. (16). With regard to the small number of published cases the aetiological role of FeLV remains questionable.
We also lack knowledge about predisposing factors or induc-tion of the disease and we know little about the differences and similarities of development between the various forms of osteo -cartilaginous outgrowths in different species. While age of onset, localisation and prognosis tend to differ between species, the lesions themselves seem remarkably comparable (1, 2, 10, 17, 20, 22). Typical findings are bony bases with cancellous bone covered by hyaline cartilage and a proliferative periostel response with thickening of the cambium layer. In some areas of the lesion en-chondral ossification is present, other areas show marrow spaces with adipocytes and even rarely haematopoietic cells (16, 25).
In man (12, 14, 15), dogs (9, 11) and horses (20) a hereditary pattern has been described which – according to Pool et al. (23) – could not be confirmed for the cat.
The prognosis for affected animals remains poor. Other authors reported a survival time of less than one year after onset of symp-toms due to proceeding functional impairment or malignant transformation of the lesions (20). The overall survival time of our cat after notification of the first lesion by the owners was 8.5 months. A direct etiological connection between feline osteo-chondromatosis and anaemia has not been published.
While the palliative surgery resulted in fast relief of lameness with no excessive regrowth at the surgical site within 2 months, the remaining lesions continued growing. The definite cause for an -aemia that ultimately caused death in the cat was not elucidated.
Conflict of interestThe authors confirm that they do not have any conflict of interest.
References1. Alexander JW. Selected skeletal dysplasias: craniomandibular osteopathy,
multiple cartilaginous exostoses, and hypertrophic osteodystrophy. Vet Clin North Am Small Anim Pract 1983; 13: 55–70.
2. Brown RJ, Trevethan WP, Henry VL. Multiple osteochondroma in a Sia-mese cat. J Am Vet Med Assoc 1972; 160: 433–435.
3. Carpenter JL, Andrews LK, Holzworth J. Tumors and tumor-like lesions. In Diseases of the Cat: Medicine and Surgery. Holzworth J, ed. Philadelphia Saunders 1987; 407–596.
4. Carrig CB. Growth abnormalities of the canine radius and ulna. Vet Clin North Am Small Anim Pract 1983; 13: 91–115.
5. Chandler EA, Gaskell RM, Gaskell CJ. Feline Medicine & Therapeutics, 3rd edn. Oxford: Blackwell 2004.
6. Cullen J. Viral carcinogenesis. In:Tumors in Domestic Animals, 4th edn. Meuten D, ed. Iowa, Iowa State Press 2002; 16–20.
7. Darilek S, Wicklund C, Novy D et al. Hereditary multiple exostosis and pain. J Pediatr Orthop 2005; 25: 369–376.
8. Essex M, Cotter SM, Carpenter JL. Feline virus-induced tumors and the immune response: recent developments. Am J Vet Res 1973; 34: 809–812.
9. Franch J, Font J, Ramis A et al. Multiple cartilaginous exostosis in a Golden Retriever cross-bred puppy. Clinical, radiographic and backscattered scan-ning microscopy findings. Vet Comp Orthop Traumatol 2005; 18: 189–193.
10. Gradner G et al. Use of latissimus dorsi and abdominal external oblique muscle for reconstruction of a thoracic wall defect in a cat with feline osteo-chondromatosis. J Feline Med Surg 2008; 10: 88–94.
11. Green EM, Adams WM, Steinberg H. Malignant transformation of solitary spinal osteochondroma in two mature dogs. Vet Radiol Ultrasound 1999; 40: 634–637.
12. Hameetman L, Szuhai K, Yavas A et al. The role of EXT1 in nonhereditary osteochondroma: identification of homozygous deletions. J Natl Cancer Inst 2007; 99: 396–406.
13. Hohdatsu T, Okada S, Ishizuka Y et al. The prevalence of types I and II fe-line coronavirus infections in cats. J Vet Med Sci 1992; 54: 557–562.
14. Jones KB, Piombo V, Searby C et al. A mouse model of osteochondroma -genesis from clonal inactivation of Ext1 in chondrocytes. Proc Natl Acad Sci USA 2010; 107: 2054–2059.
15. Ligon AH, Potocki L, Shaffer LG et al. Gene for multiple exostoses (EXT2) maps to 11(p11.2p12) and is deleted in patients with a contiguous gene syndrome. Am J Med Genet 1998; 75: 538–540.
16. Levitin B, Aroch I, Aizenberg I et al. Linear osteochondromatosis in a cat. Vet Radiol Ultrasound 2003; 44: 660–664.
17. Malik R, Allan GS, Howlett CR et al. Osteochondrodysplasia in Scottish Fold cats. Aust Vet J 1999; 77: 85–92.
18. Mathews KG et al. Resolution of lameness associated with Scottish fold os-teodystrophy following bilateral ostectomies and pantarsal arthrodeses: a case report. J Am Anim Hosp Assoc 1995; 31: 280–288.
19. Moore AS. Tumors of the skeletal system. In: Feline Oncology. Ogilvie GK, Moore AS, eds. Trenton: Veterinary Learning Systems 2001; 233–250.
20. Morgan JP, Carlson WD, Adams OR. Hereditary multiple exostosis in the horse. J Am Vet Med Assoc 1962; 140: 1320–1322.
21. Partington BP et al. What is your diagnosis? Scottish Fold osteodystrophy. J Am Vet Med Assoc 1996; 209: 1235–1236.
22. Pierz KA et al. Hereditary multiple exostoses: one center’s experience and review of etiology. Clin Orthop Relat Res 2002; 401: 49–59.
23. Pool RR. Osteochondromatosis. In: Disease Mechanism in Small Animal Surgery, 2nd edn. Bojrab MS, ed. Philadelphia: Lippincott Williams & Wil-kins 1993; 821–833.
24. Reidarson TH, Metz AL, Hardy RM. Thoracic vertebral osteochondroma in a cat. J Am Vet Med Assoc 1988; 192: 1102–1104.
25. Riddle WE, Jr., Leighton RL. Osteochondromatosis in a cat. J Am Vet Med Assoc 1970; 156: 1428–1430.
26. Schwab S, Herden C, Seeliger F et al. Non-suppurative meningoencephalitis of unknown origin in cats and dogs: an immunohistochemical analysis. J Comp Pathol 2007; 136: 96–110.
27. Simon D. Osteochondrodysplasie bei einer Scottish-Fold-Katze. Tierärztl Prax 2000; 28 (K): 86; 107–110.
28. Voss K. Diseases of bone. In: Feline Orthopedic Surgery and Musculosce -letal Disease. Montavon PM, Voss K, Langley-Hobbs SJ, eds. Phila delphia: Elsevier Limited 2009; 60–62.
M. C. Nolff et al.: Feline osteochondromatosis in a FELV-negative cat
ConclusionPalliative surgery may be an option for cats where mechanical dis-turbance by the lesions causes lameness. However, owners need to be aware of the overall prognosis of the disease and that no curative treatment is known to date. The true etiological role of FELV in cats developing feline osteochondromatosis remains speculative.
For personal or educational use only. No other uses without permission. All rights reserved.Downloaded from www.tieraerztliche-praxis.de on 2017-06-21 | IP: 54.191.40.80