
Federal Health IT Public Policy Update
41
Federal Health IT Public Policy Update Innovative Ideas to Support Local Advocacy Friday, November 14, 2014
Transcript of Federal Health IT Public Policy Update
Federal Health IT Public Policy Update Innovative Ideas to Support Local Advocacy
Friday, November 14, 2014

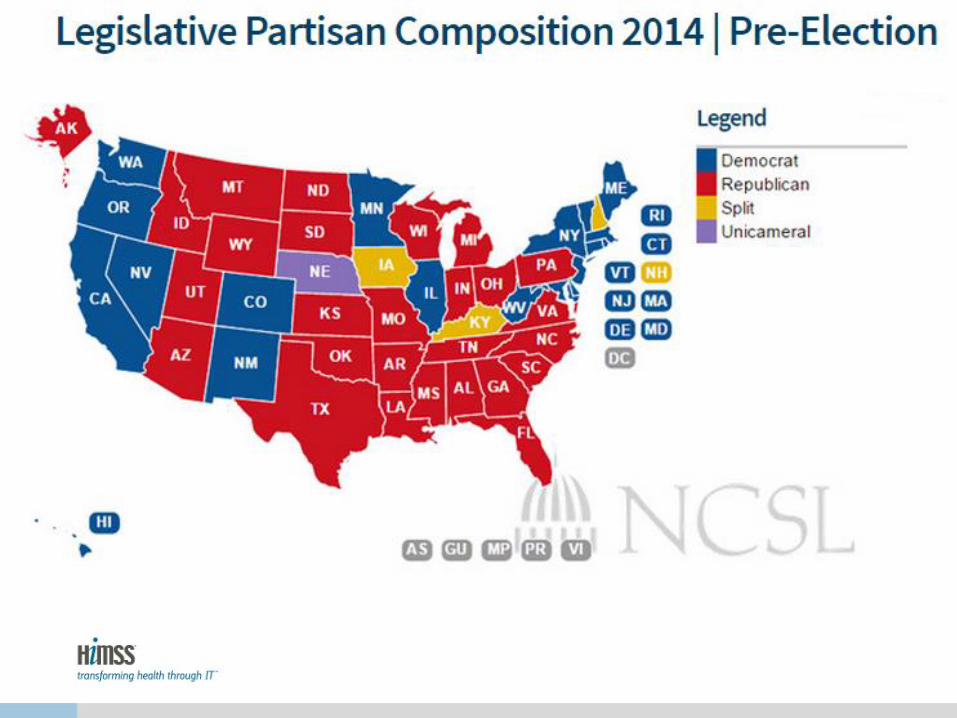
• 2014 Mid-Term Election Update
– Impact on Health IT
• Health IT Public Policy Initiatives Discussion
– Meaningful Use
– Interoperability
– Sustainable Growth Rate Formula Fix
– ONC Leadership Changes
• HIMSS State Government Affairs Update
– Innovative Approaches to Advocacy
Agenda
Federal Election Results and Their Impact on Health IT
Senate Election Results 2014
36 Senate Seats up for Re-election
– 33 regular races
– 3 special elections
Results Republican net gain of at least 8 seats
– 13 or more new Senators
• 11 Republicans
• 2 Democrats
– 53 Republicans
– 46 Democrats
– 1 undecided race
• Louisiana
House Election Results 2014
All 435 Seats up for Election
– 234 244 Republicans
– 199 184 Democrats
– 7 races still undecided
– 52 or more new House Members
• 36 Republicans
• 16 Democrats
Several Potential Avenues for Republican-Controlled Congress and Obama White House to Pursue
Willingness to Compromise
• Power evenly split between the legislative and executive branches can lead to more willingness to compromise
• Both parties temper their policies in order to achieve broad goals, or at least most of their goals
• Each side has an eye toward 2016 and securing as many legislative/policy victories as possible in order to enhance their campaign messages
Obstruct/More of the Same
• Each side could remain obstinate
and not willing to bend on policy
principles
• Each side would blame the other for
lack of progress and hope that they
could effectively assign blame to
the other in the public’s perspective
• For 2016, each side would
campaign on what they could do if
they controlled both branches of
government
Healthcare Changes on Agenda for Republican-Controlled Congress, Less So for President Obama Wholesale changes to the ACA are unlikely; Health IT in the picture for Republicans
• Possible areas of compromise on the ACA include eliminating the medical device tax
– Changes to the individual mandate are not open for discussion by the Administration
• In terms of health IT, the 2013 Senate Reboot Report will be on the agenda
– Portends possible changes to meaningful use
– Greater oversight of EHR incentive payments
– 2015 MU Reporting Period
• Sustainable Growth Rate Formula debate to occur in February/March
– Offsets will remain the key sticking point
• Cybersecurity and regulating health IT are bipartisan issues that could come to forefront
• House Republicans have passed many pieces of legislation to repeal in full or
in part the ACA
• With the Senate under GOP control, those bills may also have Senate floor
consideration
• Some may have bipartisan support such as repealing the medical device tax
• Others may be strongly opposed by the Senate Democrats such as changes to
risk corridors and reinsurance in the exchanges and subject to Democrat
filibuster
• Provisions likely to be considered include changing the 30 hour work week for
full time employees, risk corridors and reinsurance, and repealing IPAB
The Affordable Care Act will be Targeted by
the New Congress but will only Result in
Modest Changes
• The GOP may use reconciliation, which a special budget process
that allows the Senate to pass certain pieces of legislation with only
51 votes, to send legislation impacting the ACA to the President
• It is possible that the Senate GOP may find some Democrat
support for changes to the ACA, but not enough to overcome a 60
vote filibuster
• Items that may be targeted in reconciliation include the medical
device tax, health insurance tax, the individual mandate tax, and
the penalty on employers
Senate Reconciliation Procedure may be
Used to Send Legislation to the President

State Elections Overview

2014 Gubernatorial Election Results


Former State Legislators on their way to Washington U.S. House of Representatives
• Arkansas 4th – Bruce Westerman (R)
• Arizona 7th – Ruben Gallego (D)
• California 11th – Mark DeSaulnier (D)
• California 25th – Stephen Knight (R)
• California 33rd – Ted Lieu (D)
• California 35th – Norma Torres (D)
• California 45th – Mimi Walters (R)
• Georgia 1st – Buddy Carter (R)
• Georgia 11th – Barry Loudermilk (R)
• Hawaii 1st – Mark Takai (D)
• Illinois 10th – Robert Dold (R)
• Illinois 12th – Mike Bost (R)
• Michigan 4th – John Moolenaar (R)
• Michigan 8th – Mike Bishop (R)
• Minnesota 6th – Tom Emmer (R)
• Montana at-large – Ryan Zinke (R)
• New Hampshire 1st – Frank Guinta (R)
• Nevada 4th – Cresent Hardy (R)
• New Jersey 1st – Donald Norcross (D)
• New Jersey 12th – Bonnie Coleman (D)
• New York 1st – Lee Zeldin (R)
• North Carolina 7th – David Rouzer (R)
• North Carolina 12th – Alma Adams (D)
• Oklahoma 5th – Steve Russell (R)
• Pennsylvania 13th – Brendon Boyle (D)
• Virginia 10th – Barbara Comstock (R)
• West Virginia 2nd – Alex Mooney (R)
• West Virginia 3rd – Evan Jenkins (R)
• Wisconsin 6th – Glenn Grothman (R)

Former State Legislators on their way to Washington
U.S. Senate:
• Colorado – Cory Gardner (R)
• Iowa – Joni Ernst (R)
• Michigan – Gary Peters (D)
• North Carolina – Thom Tillis (R)
• South Dakota – Mike Rounds (R)
• West Virginia – Shelley Moore Capito (R)

Health IT Policy Initiatives Discussion

Meaningful Use Program Intent
• Improve quality, safety, efficiency, and reduce health
disparities
• Engage patients and families
• Improve care coordination
• Ensure adequate privacy and security protections for
personal health information
• Improve population and public health
Meaningful Use Program Intent
• Political Reality: Paving the Way for Healthcare
Reform
– Standards and Certification supporting information
gathering and sharing
– Quality reporting requirements for ACA
– Expand payment reform initiatives that capitalize
on health IT to improve quality, decrease cost of
care
Policy Challenges and HIMSS’s Responsibility
• MU originally envisioned to create the infrastructure to realize the Triple Aim via ACA
– Better care for individuals
– Better health for populations
– Reducing per-capita costs
• Quality and data collection and reporting too fluid
• Balancing stakeholder expectations and provider capabilities has not been achieved
• Policymakers and providers losing confidence in MU
Policy Challenges and HIMSS’s Responsibility
• Congress becoming impatient with $25B+ “paying for silos” and the pace/focus of change
• Debate about the pace of change:
– “You’re going too fast!” “Go faster!” “You’re asking for the wrong information!”
• Deep need for keeping government and private sector focused on practical and realistic achievement
• Our Nation is at a crossroads on the Meaningful Use Program
• The Flex-IT Act (HR 5481) tries to address the profound challenges associated with the transition to 2014 certified EHR technology and requirements for preparing data to be transmitted
– The legislation calls for an adjustment of the 2015 requirement to one three-month quarterly reporting period versus a full year
– Right now, EH, EPs, and CAHs not in their first year of the program have daunting requirements for 12 months of MU reporting in 2015
• The bill, introduced by Rep. Renee Ellmers (R-NC) and Rep. Jim Matheson (D-UT) is up to 17 cosponsors
• No companion bill in the Senate
• A legislative fix is more likely to be considered in the new 114th Congress in January than it is during the lame duck session this year
• HIMSS is working with a broad-based stakeholder coalition to generate more support in Congress for this issue
• HIMSS is also addressing this issue on the regulatory side by meeting with officials from HHS and CMS
– Little traction has developed in HHS to make changes to the current requirements
Flex-IT Act Addresses MU 2015 Full-Year Reporting Issue
• The original intention for Stage 3 was a focus on improving outcomes
• Specific ideas discussed for Stage 3
– Supports new model of care (e.g., team-based, outcomes-oriented, pop mgmt)
– Addresses national health priorities
– Broad applicability (since MU is a floor) across provider specialties and patient needs
– Address key gaps (e.g., information exchange, patient engagement, reducing disparities) in EHR functionality that the market will not drive alone, but are essential for all providers
– Use of mature standards widely adopted or could be widely adopted by 2017
• Tight timeline to publish the proposed rule and finalize it
– HIMSS recommends at least 18 months from publication of the final rule to the start of MU reporting period
MU Stage 3 Proposed Rule to be Released this Winter

Achieving Secure, Widespread, Interoperable Health Information
• ONC released Interoperability Vision Document in June 2014
– Identifies 5 core building blocks
1. Core technical standards and functions
2. Certification to support adoption and optimization
3. Privacy & security protections for health information
4. Supportive business, clinical, & regulatory environment
5. HIE governance
• HITPC and HITSC have weighed in on the vision document and offered ideas for a path forward
• In detailed comments, HIMSS recommended that ONC should:
– Work with stakeholder organizations to recognize and manage the complexity of a diverse healthcare system
– Focus on its convener role to drive consensus
– Consider incentives for providers that implement certified products
– Support the use of public and private policy levers beyond MU to foster interoperability and HIE
• Draft Roadmap expected to be released in January for public comment
Draft HHS Interoperability Roadmap V1.0 Currently in Formulation Stage
ONC’s Roadmap Drivers
HIMSS agrees with ONC’s Vision
• Developing a strong interoperable health IT ecosystem
• Coordination/Leadership structure balances federal resources
with stakeholder capabilities
• Navigating roadblocks essential to moving forward
• Focus on supporting the Triple Aim
• Certification and Standards key components to interoperability
across organizations & communities

HIMSS Recommendations
Working with all stakeholders, HIMSS will lead:
• Achieve baseline functionality for standards-based
interoperability
• Develop, harmonize, and disseminate standards
• Provide education & service offerings for providers to
advance interoperable product adoption
• Support and extend interoperability testing tools
• Leverage IHE, IHE certification
• Drive towards privacy and security end-states

Sustainable Growth Rate Formula Fix
• The current SGR patch expires at the end of March 2015 and Medicare physician payments will be cut by around 20+% on April 1st
• Despite strong Congressional interest in a permanent fix, finding the offsets to fund a $150 billion to $200 billion piece of legislation is extremely difficult
– The change in control of the Senate does not alter the chances for a permanent fix
• More likely a one-year patch is enacted before the SGR cut goes into effect
• Permanent SGR Fix Bill came close to getting through Congress earlier in 2014
– Bill focused solely on new policy around the SGR and did not include offsets. The provisions
included:
• Improved on existing fee-for-service system by rewarding value over volume and ensuring
payment accuracy
• Incentivizes movement to alternative payment models and PCMH
• Expands the use of Medicare data for transparency and quality improvement
• New Congress may have new dynamics that make agreement on even the policy around
an SGR fix difficult
One-Year SGR Patch Likely to Occur in
February/March 2015

ONC Leadership Changes

• On October 23, HHS announced that National HIT Coordinator Dr. DeSalvo was becoming Acting Assistant Secretary for Health
– Five days later, ONC backtracked and said that DeSalvo would still be heavily involved in ONC issues, such as HITPC, interoperability, and MU
– Lisa Lewis named acting national coordinator
• Deputy NC Dr. Jacob Reider announced his departure shortly after the original DeSalvo announcement
– Several additional ONC leaders have also moved on or intention to move on
• HHS has emphasized that ONC far more than one or two leaders
– The team is all part of HHS’ path toward delivery system reform and overall health improvement
• On November 3, HIMSS and CHIME sent a letter to HHS asking for Dr. DeSalvo back to ONC in a full-time capacity
– If not, ONC needs new leadership that appoint new ONC leadership immediately that can lead the agency on the host of critical issues that must be addressed
ONC Leadership in Transition Stage; Dr. DeSalvo Filling Two Roles in HHS, Other Leaders Moving on

HIMSS State Government Affairs Update and Innovative Approaches to Advocacy

HIMSS State & Local Advocacy
Advocacy is the “ability to plead in
favor of; support or urge by
argument; or recommend
publicly.”
Advocacy is the art of strategically
leveraging the best that HIMSS
has to offer to successfully
influence public policy to improve
healthcare for all.
• Educational Offerings (Papers & Webinars)
• Collaboration w/ State Associations
• State & Regional Event Support
• State HIT Dashboard
• Health IT Legislation Tracking
• Chapter Advocacy Roundtable (CAR)
• Regional Extension Centers (RECs)
• State Advisory Roundtable
• HIE & mHealth Policy Papers
• State Official Presence @ HIMSS
Conferences
• State Government Memberships
• State Legislator of the Year Award
Chapter Advocacy Roundtable
Chapter’s connection to state-level advocacy
Connect state officials with health IT subject matter experts in an effort to
educate and build relationships
Building relationships – A Journey
• State Health IT / Advocacy Days
• Testifying in support of legislation
• Outreach and education campaigns
• HIMSS State Government Membership
• Chapter Advocate Awards
• Chapter Advocate of the Year
• Chapter Levels of Advocacy

CARs
• Representatives of National HIMSS
• Organize visits to key state and Federal officials
• Connect with Chapter leadership
• Connect with other Chapter volunteers
• Connect with local media about key policy and advocacy issues
• Participate in monthly CAR calls
• Participate in CAR recognition program
Chapter Advocates = Chapter Connectors
Ohio Statehouse to HIMSS Innovation Center
HIMSS Innovation Center
Cleveland, Ohio
MCPc Telepresence
Ohio Statehouse
Columbus, Ohio
Health Information Technology Stakeholder Summit in Dallas, Texas
• Texas Legislature meets every other year
• Keep health IT fresh in the minds of legislators through targeted programming and a policy-driven guest list
• DFW HIMSS Partnered with local Stage 7 Facility – Children’s Medical Center
• 40 health IT stakeholders including federal, state, and local officials attended
• “To see first-hand Children’s advanced use of technology across its continuum of care and to gain a more thorough understanding of how incorporating health IT into healthcare can improve processes, drive efficiency, lower costs and deliver better patient care.”
WV Currently has 1 Stage 7
Hospital: West Virginia United
Health System (WVUHS) - Ruby
Memorial Hospital in
Morgantown, WV

HIMSS “Legislative Action Center”
• Use the Award-winning HIMSS Legislative Action Center as your personalized electronic tool to stay connected on key policy items and communicate directly with your elected officials.
• Use the “Key Issues” section to stay up to date on important issues, recent votes, and current legislation concerning health IT.
• Send a letter to your Member of Congress or State legislator by entering your zip code.
– http://cqrcengage.com/himss/home

• NHIT tentatively planned for October 5-9, 2015
• HIMSS plans NHIT activities and Policy Summit events
and Capitol Hill Day in Washington, DC
• HIMSS encourages chapters and other organizations to
hold their own events celebrating health IT around the
country
• WVHIMSS should consider holding a state-focused
event that leverages national coverage on this issue
Leverage National Health IT Week to Organize Events at the State and Local Level

How Your Efforts Can Impact Health IT
• Engage the newly elected officials – introduce yourself and place yourself as a subject matter expert for health IT.
• Remind the reelected legislators that you have appreciated their work in the past and look forward to bringing health IT to the forefront of 2015 and 2016 legislative sessions.
• Majority Party Change leads to change in committee chairmen and now is the time they’ll start deciding on their agenda.
• Begin building relationships early, engage the chairs and let them know you want to address health IT in their state.
Questions?


















