Featured Articles - NCCN - Evidence-Based Cancer ... 8_Suppl_1_Multiple_Myeloma.pdf · As the...
44
JNCCN Volume 8 Supplement 1 Journal of the National Comprehensive Cancer Network NCCN.org SUPPLEMENT Addressing Challenges in Multiple Myeloma Management in an Era of New Therapeutics Sundar Jagannath, MD; Kenneth Anderson, MD; Ashraf Badros, MD; Jacob P. Laubach, MD; Constantine Mitsiades, MD, PhD; Ruben Niesvizky, MD; Paul Richardson, MD; and Robert L. Schlossman, MD Featured Articles The Role of Maintenance Therapy in the Treatment of Multiple Myeloma Ashraf Badros In the Age of Novel Therapies, What Defines High-Risk Multiple Myeloma? Ashraf Badros Complications of Multiple Myeloma Therapy, Part 1: Risk Reduction and Management of Peripheral Neuropathy and Asthenia Paul Richardson, Jacob Laubach, Robert L. Schlossman, Constantine Mitsiades, and Kenneth Anderson Complications of Multiple Myeloma Therapy, Part 2: Risk Reduction and Management of Venous Thromboembolism, Osteonecrosis of the Jaw, Renal Complications, and Anemia Ruben Niesvizky and Ashraf Badros This activity is sponsored by MediCom Worldwide, Inc. This activity was supported by an educational grant from Millennium Pharmaceuticals, Inc. CE Provided by MediCom Worldwide, Inc.
Transcript of Featured Articles - NCCN - Evidence-Based Cancer ... 8_Suppl_1_Multiple_Myeloma.pdf · As the...

JNCCN Volume 8 Supplement 1 Journal of the National Comprehensive Cancer Network
NCCN.org
S U P P L E M E N T
Addressing Challenges in Multiple Myeloma Management in an Era of New TherapeuticsSundar Jagannath, MD; Kenneth Anderson, MD; Ashraf Badros, MD; Jacob P. Laubach, MD; Constantine Mitsiades, MD, PhD; Ruben Niesvizky, MD; Paul Richardson, MD; and Robert L. Schlossman, MD
Featured ArticlesThe Role of Maintenance Therapy in the Treatment of Multiple MyelomaAshraf Badros
In the Age of Novel Therapies, What Defines High-Risk Multiple Myeloma?Ashraf Badros
Complications of Multiple Myeloma Therapy, Part 1: Risk Reduction and Management of Peripheral Neuropathy and AstheniaPaul Richardson, Jacob Laubach, Robert L. Schlossman, Constantine Mitsiades, and Kenneth Anderson
Complications of Multiple Myeloma Therapy, Part 2: Risk Reduction and Management of Venous Thromboembolism, Osteonecrosis of the Jaw, Renal Complications, and AnemiaRuben Niesvizky and Ashraf Badros
This activity is sponsored by MediCom Worldwide, Inc.
This activity was supported by an educational grant from Millennium Pharmaceuticals, Inc.
CE Provided by MediCom Worldwide, Inc.


Volume 8 Supplement 1 Journal of the National Comprehensive Cancer Network
JNCCNNCCN Member InstitutionsCity of Hope Comprehensive
Cancer Center Los Angeles, California
Dana-Farber/Brigham and Women’s Cancer Center| Massachusetts General Hospital Cancer Center Boston, Massachusetts
Duke Comprehensive Cancer CenterDurham, North Carolina
Fox Chase Cancer Center Philadelphia, Pennsylvania
Huntsman Cancer Institute at the University of Utah Salt Lake City, Utah
Fred Hutchinson Cancer Research Center/ Seattle Cancer Care Alliance Seattle, Washington
The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Baltimore, Maryland
Robert H. Lurie Comprehensive Cancer Center of Northwestern University Chicago, Illinois
Memorial Sloan-Kettering Cancer Center New York, New York
H. Lee Moffitt Cancer Center & Research Institute Tampa, Florida
The Ohio State University Comprehensive Cancer Center – James Cancer Hospital and Solove Research Institute Columbus, Ohio
Roswell Park Cancer Institute Buffalo, New York
Siteman Cancer Center at Barnes-Jewish Hospital and Washington University School of Medicine St. Louis, Missouri
St. Jude Children’s Research Hospital/University of Tennessee Cancer Institute Memphis, Tennessee
Stanford Comprehensive Cancer Center Stanford, California
University of Alabama at Birmingham Comprehensive Cancer Center Birmingham, Alabama
UCSF Helen Diller Family Comprehensive Cancer Center San Francisco, California
University of Michigan Comprehensive Cancer Center Ann Arbor, Michigan
UNMC Eppley Cancer Center at The Nebraska Medical Center Omaha, Nebraska
The University of Texas M. D. Anderson Cancer Center Houston, Texas
Vanderbilt-Ingram Cancer Center Nashville, Tennessee
For more information, visit www.NCCN.org
JNCCN is dedicated to improving the quality of cancer care locally, nationally, and internationally while enhancing the collaboration between academic medicine and the community physician. JNCCN is further committed to disseminating information across the cancer care continuum by publishing clinical practice guidelines and reporting rigorous outcomes data collected and analyzed by experts from the world’s leading care centers. JNCCN also provides a forum for original research and review papers focusing on clinical and translational research and applications of the NCCN Guidelines in everyday practice, as well as correspondence and commentary.
Mission Statement
The National Comprehensive Cancer Network (NCCN), a not-for-profit alliance of 21 of the world’s leading cancer centers, is dedicated to improving the quality and effectiveness of care provided to patients with cancer. Through the leadership and expertise of clinical professionals at NCCN Member Institutions, NCCN develops resources that present valuable information to the numerous stakeholders in the health care delivery system. As the arbiter of high-quality cancer care, NCCN promotes the importance of continuous quality improvement and recognizes the significance of creating clinical practice guidelines appropriate for use by patients, clinicians, and other health care decision-makers. The primary goal of all NCCN initiatives is to improve the quality, effectiveness, and efficiency of oncology practice so patients can live better lives. For more information, visit www.NCCN.org.
About the NCCN
NCCN
275 Commerce Drive
Suite 300
Fort Washington, PA 19034
215–690–0300
www.NCCN.org

Volume 8 Supplement 1 Journal of the National Comprehensive Cancer Network
JNCCNFaculty
Kenneth Anderson, MDKraft Family Professor of Medicine Harvard Medical School Chief of the Division of Hematologic Neoplasia Dana-Farber/Brigham and Women’s Cancer Center Boston, MA, USA
Ashraf Badros, MD Associate Professor of Medicine University of Maryland Greenebaum Cancer Center Bone Marrow Transplant Program Baltimore, MD, USA
Sundar Jagannath, MDChief Multiple Myeloma Program and
Bone Marrow and Blood Stem Cell Transplantation Program Attending Physician Medical Oncology St. Vincent’s Comprehensive Cancer Center New York, NY, USA
Jacob P. Laubach, MDInstructor in Medicine Department of Medical Oncology Dana-Farber Cancer Institute Department of Medicine Harvard Medical School Boston, MA, USA
Constantine Mitsiades, MD, PhDInstructor in Medicine Department of Medical Oncology Dana-Farber Cancer Institute Department of Medicine
Harvard Medical School Boston, MA, USA
Ruben Niesvizky, MDAssociate Professor of Medicine Weill Cornell Medical College Associate Attending Physician New York-Presbyterian Hospital New York, NY, USA
Paul G. Richardson, MDAssociate Professor of Medicine Harvard Medical School Dana-Farber Cancer Institute Boston, MA, USA
Robert L. Schlossman, MDDepartment of Medical Oncology Dana-Farber Cancer Institute Boston, MA, USA
Addressing Challenges in Multiple Myeloma Management in an Era of New Therapeutics
DisclosuresIn accordance with the Accreditation Council for Continuing Medical Education (ACCME), ACPE and California Board of Nursing, MediCom Worldwide, Inc. requires that all program planners, faculty, and providers who are in a position to control the content of a CE activity are required to disclose any relevant financial relationships they may have or have had within the last 12 months with the commercial supporter or the manufacturer(s) of any commercial device(s) discussed in this educational activity. Accordingly, the following disclosures were made.
Faculty DisclosuresThe presenting faculty reported the following:
Dr. Kenneth Anderson has received preclinical and clinical research support from Millennium Pharmaceuticals, Inc., and having served as an advisory board member for Millennium Pharmaceuticals, Inc.
Dr. Ashraf Badros has received research support from Proteolix, Inc., Millennium Pharmaceuticals, Inc., Celgene Corporation, and Novartis AG.
Dr. Sundar Jagannath has received consultant fees from Celgene Corporation, Merck & Co., Inc., and Millennium Pharmaceuticals, Inc.
Dr. Jacob Laubach has disclosed that he has no significant relationships with the grantor Millennium Pharmaceuticals, Inc. or any other commercial company whose products and services may be related to his material.
Dr. Constantine Mitsiades reports having participated in funded or unfunded research for OSI Pharmaceuticals, Inc.; Amgen Inc.; AVEO Pharmaceuticals, Inc.; EMD Serono, Inc.; and Sunesis Pharmaceuticals, Inc., and having participated as an advisory board member, speakers’ bureau member, expert witness, or consultant for Millennium Pharmaceuticals, Inc.; Novartis AG; Bristol-Myers Squibb; Merck & Co., Inc.; and Pharmion Corp. (now Celgene Corporation).
Dr. Ruben Niesvizky has received consultant fees and grant/research support from Celgene Corporation, Proteolix, Inc., and Millennium Pharmaceuticals, Inc. He has received honoraria related to speakers’ bureau activities from Celgene, Millennium, and Ortho Biotech (now Centocor Ortho Biotech Inc.).
Dr. Paul Richardson has received honoraria related to speakers’ bureau and advisory board activities from Millennium Pharmaceuticals, Inc. and Celgene Corporation.
Dr. Robert Schlossman has received honoraria related to speakers’ bureau activities from Celgene Corporation and Millennium Pharmaceuticals, Inc.
Provider DisclosuresThe individuals listed below from MediCom Worldwide, Inc. reported the following for this activity: Joan Meyer, executive director; Jacqui Brooks, MBBCH, MRCPsych, VP medical education; Gene Tombler, PhD, medical director; and Faith Reidenbach, medical writer, have nothing to disclose.
Conflict of Interest ResolutionTo resolve identified conflicts of interest, the educational content was fully peer reviewed by members of the MediCom Content Review Committee. The resulting certified activity was found to provide educational content that is current, evidence-based, and commercially balanced.

Volume 8 Supplement 1 Journal of the National Comprehensive Cancer Network
JNCCNCE Acceditation
CME CreditAccreditation Statement: MediCom Worldwide, Inc. is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical
education for physicians.Designation Statement: MediCom Worldwide,
Inc. designates this educational activity for a maximum of 2.5 AMA PRA Category 1 Credits™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
CPE CreditMediCom Worldwide, Inc. is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing
pharmacy education. Its CE programs are developed in accordance with the “Criteria for Quality and Interpretive Guidelines” of the ACPE. This program is acceptable for 2.5 contact hours of Continuing Education Credit.
Universal Program Number: 0827-000-10- 239-H01-P Disease State Management/Drug Therapy. Knowledge-based CPE activity.
Nursing CreditAccreditation Statement: MediCom Worldwide, Inc., 101 Washington Street, Morrisville, PA 19067 is approved by the California Board of Registered Nursing, Provider
Number CEP11380. MediCom designates this CNE activity for 2.5 contact hours. Program Number: 10-239-231.
Program OverviewMultiple myeloma (MM) remains the second most common hematologic malignancy in the United States, after non-Hodgkin lymphoma. Historically, MM has been a difficult and frustrating disease for patients and their health care providers. Since the reintroduction of thalidomide and the development of lenalidomide and bortezomib, outcomes have improved considerably, particularly when these newer agents are combined with conventional chemotherapeutic agents or with each other. Obviously, it is vitally important for today’s health care providers to understand the newer agents, but this is a challenge because the drugs have multiple functions (e.g., antiangiogenesis, immunomodulation, proteasome inhibition), have different toxicity profiles, and can be used in myriad combinations and sequences. Hematologists/oncologists have indicated a need to know more about choosing first-, second-, and third-line therapies; managing the side effects of the new agents; the role and timing of stem cell transplantation in the era of the new therapies; guidelines for maintenance therapy; and what new therapeutic combinations will be a major factor in treating myeloma in the coming years.
Continuing Education Information
Target AudienceThis activity is designed for physicians, pharmacists, physician assistants, nurses, nurse practitioners, and other health care professionals who have an interest in enhancing their knowledge and understanding of the management of multiple myeloma (MM).
Learning Objectives Upon completion of this activity, participants should be able to:• Evaluate the need for, and propose appropriate maintenance therapy options in, MM• Evaluate the current importance of assessing MM patients for risk, especially in the face
of emerging and novel agents, and integrate this knowledge into management plans• Describe the most appropriate techniques for monitoring treatment of MM• Formulate evidence-based management plans for patients with MM based on their age,
risk, and comorbiditiesThe opinions expressed in this publication are those of the participating faculty and
not those of the National Comprehensive Cancer Network, MediCom Worldwide, Inc., Millennium Pharmaceuticals, Inc., or the manufacturers of any products mentioned herein.
This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. The opinions expressed in the educational activity are those of the faculty. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings. Further, attendees/participants should appraise the information presented critically and are encouraged to consult appropriate resources for any product or device mentioned in this program.
Drs. Anderson, Badros, Laubach, Mitsiades, Niesvizky, Richardson, and Schlossman indicated that their materials would include the discussion of unlabeled uses of commercial products or investigational/unapproved products not yet approved by the FDA for certain uses in the United States.
Dr. Jagannath indicated that his material would not include the discussion of unlabeled uses of commercial products or investigational/unapproved products not yet approved by the FDA for any use in the United States.
Activity InstructionsThis activity is eligible for credit through February 15, 2011. After this date, this activity will expire and no further credit will be awarded.
Expected time to complete this activity as designed: 2.5 hoursThere are no fees for participating in this activity. All participants must read the
entire supplement and complete the Activity Evaluation Form. Participants must receive a minimum score of 70% on the self-assessment portion of the form to qualify for CE credit. Certificates will be mailed 4 weeks after receipt of a completed, qualified form.
Copyright 2010, National Comprehensive Cancer Network (NCCN). All rights reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from the NCCN.

Volume 8 Supplement 1 Journal of the National Comprehensive Cancer Network
JNCCN
S-1 Introduction: Addressing Challenges in Multiple Myeloma Management in an Era of New Therapeutics
Sundar Jagannath, MDHematologists, oncologists, and other physicians can expect to encounter an increasing number of patients with multiple myeloma. Historically, multiple myeloma has been a difficult and frustrating disease, but since the reintroduction of thalidomide and the development of lenalidomide and bortezomib, outcomes have improved considerably. This supplement is part of a 3-supplement series planned at a roundtable discussion held in 2009, and this introduction discusses the articles in this supplement as well as those in earlier and later planned publications not included in JNCCN.
S-4 Complications of Multiple Myeloma Therapy, Part 1: Risk Reduction and Management of Peripheral Neuropathy and Asthenia
Paul Richardson, MD; Jacob P. Laubach, MD; Robert L. Schlossman, MD; Constantine Mitsiades, MD, PhD; and Kenneth Anderson, MDPeripheral neuropathy and asthenia (fatigue) occur as both disease- and treatment-related complications in patients with multiple myeloma. Treatment-related peripheral neuropathy has an estimated incidence of 37% to 83% among patients with multiple myeloma, and asthenia is the most common adverse effect of cancer treatment, occurring in approximately 76% to 96% of patients receiving chemotherapy. These conditions are often dose-limiting, and they may interfere with optimal therapy and substantially affect patient quality of life. Regular screening and monitoring procedures, combined with patient education and effective management strategies, can reduce the risk of these treatment-related complications.
S-13 Complications of Multiple Myeloma Therapy, Part 2: Risk Reduction and Management of Venous Thromboembolism, Osteonecrosis of the Jaw, Renal Complications, and Anemia
Ruben Niesvizky, MD, and Ashraf Badros, MDVenous thromboembolism (VTE), osteonecrosis of the jaw, renal failure, and anemia are all common complications of multiple myeloma therapy. Many of these adverse events have been documented only in the past 5 to 10 years, in conjunction with the introduction of a series of the newer therapies thalidomide, bortezomib, and lenalidomide. This article discusses these complications in detail and provides strategies for health care providers to best prevent, identify, and manage them.
S-21 The Role of Maintenance Therapy in the Treatment of Multiple Myeloma
Ashraf Badros, MDMaintenance therapy in multiple myeloma has been under investigation for more than 3 decades, without evidence of clear benefit until recently. The role of the novel agents thalidomide, lenalidomide, and bortezomib as maintenance is emerging. Most reported maintenance studies have evaluated thalidomide, alone or in combination with a corticosteroid. Several of these studies suggest that thalidomide-based maintenance prolongs overall survival after autologous stem cell transplantation but important questions have not yet been resolved. Ongoing randomized trials are also evaluating lenalidomide and bortezomib maintenance therapies to better define the role of these drugs as maintenance in multiple myeloma.
S-28 In the Age of Novel Therapies, What Defines High-Risk Multiple Myeloma?
Ashraf Badros, MDMultiple myeloma is characterized by clinical and biologic heterogenicity. Recently, genetic analysis has provided predictable prognosis across different types of treatment. These advances have allowed patients to be categorized into different risk groups and have been particularly useful in defining a high-risk group. Preliminary studies have shown promising outcomes after the use of novel agents in high-risk patients. The application of risk-based therapy and the potential of the new agents to abrogate the influence of adverse prognostic features may improve outcomes in these patients.
S-35 CME Post-Test and Evaluation
Featured Articles
Addressing Challenges in Multiple Myeloma Management in an Era of New Therapeutics

Journal of the National Comprehensive Cancer Network Introduction
Sundar Jagannath, MDFrom St. Vincent’s Comprehensive Cancer Center, New York, New York.Correspondence: Sundar Jagannath, MD, St. Vincent’s Comprehensive Cancer Center, 325 West 17th Street, New York, NY 10011. E-mail: [email protected]
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-1
Introduction: Addressing Challenges in Multiple Myeloma Management in an Era of New Therapeutics
Hematologists/oncologists and other physicians can expect to encounter an increasing number of patients with multiple myeloma (MM) in the coming years. Between 1997 and 2006, the incidence rate of myeloma declined in the United States, but the burden (number of incident cases) increased.1 An analysis of population-based cancer registries in 9 countries detected modest increases in the incidence of MM in most between 1973 and 1992, with further increases projected by 2007.2 MM remains the second most common hematologic malignancy in the United States after non-Hodgkin’s lymphoma.3
Historically, MM has been a difficult and frustrating disease for patients and physicians. Since the reintroduction of thalidomide and development of lenalidomide and bortezomib, outcomes have improved considerably, particularly when these newer agents are combined with conventional chemotherapeutic agents or each other. Using the first-line regimens common in 1983, typical 2-year survival rates were 48% to 66%. In trials of triple combination therapy reported in 2008, the 2-year survival rates ranged from 83% to 90%.4 In the United States, the 5-year survival rate improved from 26% in 1975 to 1977 to 34% in 1996 to 2003, a statistically significant difference.5
Obviously, it is vitally important for today’s physicians to understand the newer agents, but this is a challenge because the drugs have multiple functions (e.g., antiangiogenesis, immunomodulation, proteasome inhibition), have different toxicity profiles, and can be used in myriad combinations and sequences. Hematologists/oncologists have indicated a need to know more about choosing first-, second-, and third-line therapies; side effects of the new agents; the role and timing of stem cell transplantation in the era of new therapies; guidelines for maintenance therapy; and what new therapeutic combinations will be major factors in treating myeloma in the coming years.6–8
This supplement is part of a 3-supplement series planned by myeloma experts via a roundtable discussion held April 24, 2009, in Philadelphia. Our charge was to develop outlines of 10 articles about myeloma therapy that would convey the information currently of most importance to community oncologists. The first 2 of the 4 articles in this supplement address risk reduction and management of the most common complications of myeloma therapy. Dr. Paul Richardson and colleagues focus on how thalidomide- and bortezomib-induced peripheral neuropathy usually can be effectively managed with dose reduction, schedule modification, optimized agent sequencing, or a combination of nonpharmacologic and pharmacologic therapy for symptom relief. They also discuss asthenia (fatigue), an important topic that is too infrequently addressed in myeloma reviews. The companion article, by Drs. Ruben Niesvizky and Ashraf Badros, explains the measures that oncologists should take to protect patients from a life-threatening complication, venous thromboembolism, the risk of which is elevated with thalidomide and lenalidomide. That article also reviews the latest data on osteonecrosis of the jaw, renal complications, and anemia.
Dr. Badros has contributed 2 additional articles to this supplement: one on maintenance therapy and the other on defining and treating high-risk myeloma. He explains that only recently, after 3 decades of investigation, have certain maintenance regimens shown promise in myeloma. In particular, several studies suggest that thalidomide, alone or with a corticosteroid, prolongs overall survival after autologous stem cell transplantation (ASCT). However, other studies have failed to support this

Introduction
February 2010
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-2
conclusion, and several important questions remain. Bortezomib- and lenalidomide-based maintenance therapies are being evaluated in ongoing randomized trials.
In the final article, Dr. Badros notes that advances in genetic analysis have allowed better estimates of prognosis for patients with myeloma. An effective means of risk stratification is required so that patients at high risk may be offered more aggressive treatment or be entered into clinical trials of investigational agents as first-line therapy. Dr. Badros discusses evolving risk stratification systems and the potential of the newer agents to improve outcomes in patients with newly diagnosed high-risk myeloma.
The first supplement in this series was published in Community Oncology. In the opening article on treatment goals, I review the indications for treating MM, help set goals for first-line treatment and treatment of relapsed/refractory disease, and suggest how to reconcile different schools of thought about treating MM.
In the second article in the Community Oncology supplement, Dr. Sergio Giralt reviews recent data on the use of novel therapies in the transplant setting and discusses why ASCT remains a standard of care in myeloma.
In the final article of the supplement, Dr. Donald Siegel and Elizabeth Bilotti discuss the investigational antimyeloma agents that are farthest along in clinical development.
The third supplement in this series, entitled “Essentials for Tailoring Multiple Myeloma Therapy,” will be published later this year by Oncology. It compares efficacy and safety data for the various therapies recommended for patients with newly diagnosed myeloma and those with relapsed/refractory disease. In it, Dr. Edward Stadtmauer provides guidance for choosing among the NCCN recommended regimens, with particular attention to patients who have cytogenetic abnormalities, renal disease, or other negative prognostic indicators. Dr. Niesvizky and colleagues discuss front-line treatment of patients with myeloma who cannot or choose not to undergo ASCT. Finally, Dr. Richardson and colleagues close the series by reviewing the treatment of relapsed/refractory disease.
An estimated 90% of oncology care in the United States is performed outside of academic medical centers,9 and data suggest that uptake of new evidence can be as fast in the community as at academic medical centers.10–13 The hope is that the information in these supplements will help community oncologists understand the latest standards for myeloma care and feel more confident about participating in this exciting, fast-changing field.
References 1. Horner MJ, Ries LA, Krapcho M, et al, eds. SEER Cancer Statistics Review, 1975–2006, National
Cancer Institute. Bethesda, MD. Based on November 2008 SEER data submission, posted to the SEER Web site 2009. Available at: http://seer.cancer.gov/csr/1975_2006. Accessed May 8, 2009.
2. Bray I, Brennan P, Boffetta P. Recent trends and future projections of lymphoid neoplasms—a Bayesian age-period-cohort analysis. Cancer Causes Control 2001;12:813–820.
3. American Cancer Society. Cancer Facts & Figures 2009. Available at: www.cancer.org/downloads/STT/500809web.pdf. Accessed May 20, 2009.
4. Durie BG. Myeloma therapy: 25 years forward—immune modulation then and now. J Clin Oncol 2008;26:4698–4700.
5. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin 2008;58:71–96.
6. Panel Intelligence. Multiple myeloma market assessment. A panel discussion among ten hematologists/oncologists. Cambridge, MA; March 2007. Available at: www.medpanel.com/reports/multiple_myleoma_therapy_market_assessment. Accessed February 11, 2009.

Introduction
Introduction
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-3
7. Panel Intelligence. Multiple myeloma: US market assessment. A survey of fifty community-based hematologist/oncologists. Cambridge, MA; March 2007. Available at: www.medpanel.com/reports/multiple_myeloma_us_market_assesment. Accessed February 11, 2009.
8. Myeloma Euronet International survey on barriers to myeloma diagnosis, treatment, and care 2006. February 2007. Available at: www.myeloma-euronet.org/en/survey/index.php. Accessed May 30, 2008.
9. PR Newswire. “Oncology World Congress survey finds wide gap between urban and rural oncologists in resource and information access” [press release]. September 20, 2004. Available at: www2.prnewswire.com/cgi-bin/stories.pl?ACCT=104&STORY=/www/story/09-20-2005/0004111294&EDATE. Accessed October 5, 2009.
10. Angermund R, Knauf W, Freund M, et al. Role of bortezomib in the treatment of multiple myeloma—first results from a representative multicentre treatment survey in Germany [abstract]. Blood 2005;106:Abstract 5156.
11. Cheung MC, Loutfy MR, Leitch HA, et al. Physician perceptions and preferences in the treatment of acquired immunodeficiency syndrome related lymphoma [abstract]. Blood 2006;108:Abstract 3331.
12. Tummala MK, Wajahath M, Kotlarewsky M, et al. Patterns of care regarding adjuvant hormonal agents and treatment of bone health in postmenopausal women with breast cancer in community and academic centers before and after the availability of ATAC (Adjuvant Tamoxifen, Arimidex or Combination) study [abstract]. J Clin Oncol 2007;25(Suppl 1):Abstract 6621.
13. McKibbin T, Kwan P, Simon J, Koeller J. Rapid adoption of chemotherapy regimens for advanced colorectal cancer (CRC) in the community oncology setting [abstract]. J Clin Oncol 2008;26(Suppl 1):Abstract 6563.

Supplement
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-4
This is a corrected copy of the article originally printed in the supplement to JNCCN. This corrected copy also includes additional material not in the original printed supplement.
Key WordsFatigue, neurotoxicity, thalidomide, bortezomib
AbstractPeripheral neuropathy (PN) and asthenia (fatigue) occur as both disease- and treatment-related complications in patients with mul-tiple myeloma (MM). Risk factors for treatment-related PN, which has an estimated incidence of 37% to 83% among patients with MM, include therapy duration, dose intensity, cumulative dose, and the presence of preexisting neuropathy. Asthenia is the most common adverse effect of treatment, occurring in approximately 76% to 96% of patients receiving therapy. The severity of PN and asthenia can range from mild to potentially debilitating. These conditions can be dose limiting; they may interfere with optimizing duration of therapy and may also substantially affect patient qual-
Peripheral neuropathy (PN) and asthenia (fatigue) are among the most commonly seen complications in patients undergoing multiple myeloma (MM) therapy. These potentially debilitating adverse effects are fre-quently dose limiting, and they may interfere with op-timal therapy and substantially affect patient quality of life as well as outcome. Effective strategies for prevent-ing and managing these complications of MM therapy are thus critical.
Peripheral Neuropathy
OverviewPN occurs in MM both as a disease-related complica-tion in newly diagnosed patients and as a side effect of MM therapy. The reported incidence is 1% to 20% in untreated patients with MM and 37% to 83% in previ-ously treated individuals; neurophysiologic evidence of neuropathy may be detected in 11% to 52% and 39% to 46% of these populations, respectively.1–6 Risk fac-tors for PN include treatment-specific characteristics, such as therapy duration, dose intensity, and cumulative dose, and patient-specific factors, such as age, comor-bidities (e.g., diabetes mellitus, alcoholism), and the presence of preexisting neuropathy.4,6–11
From Harvard Medical School, Dana-Farber Cancer Institute, Boston, Massachusetts.Dr. Richardson reports having participated in funded research for Celgene Corporation and Millennium and having participated as an advisory board member or consultant for Celgene Corporation; Millennium Pharmaceuticals, Inc.; and Johnson & Johnson. Dr. Laubach reports no potential conflicts of interest. Dr. Schlossman reports having served as a speakers’ bureau member for Celgene Corporation and Millennium Pharmaceuticals, Inc. Dr. Mitsiades reports having participated in funded research for OSI Pharmaceuticals, Inc.; Amgen, Inc.; AVEO Pharmaceuticals, Inc.; EMD Serono, Inc.; and Sunesis Pharmaceuticals, Inc., and having participated as an advisory board member for Millennium Pharmaceuticals, Inc.; Novartis International AG; Merck & Co.; and Pharmion Corporation. Dr. Anderson reports having received preclinical and clinical research support from Millennium Pharmaceuticals, Inc., Celgene Corporation, and Novartis, and having served as an advisory board member for Millennium Pharmaceuticals, Inc., Celgene Corporation, Novartis, and Merck & Co.Supported by an educational grant from Millennium Pharmaceuticals, Inc.Correspondence: Paul G. Richardson, MD, Harvard Medical School, Dana-Farber Cancer Institute, 44 Binney Street, Dana 1B02, Boston, MA 02115. E-mail: [email protected]
Complications of Multiple Myeloma Therapy, Part 1: Risk Reduction and Management of Peripheral Neuropathy and Asthenia
Paul G. Richardson, MD; Jacob P. Laubach, MD; Robert L. Schlossman, MD; Constantine Mitsiades, MD, PhD; and Kenneth Anderson, MD; Boston, Massachusetts
ity of life. Regular screening and monitoring, combined with pa-tient education and effective management strategies, can reduce the risk of these treatment-related complications, as well as their consequences. (JNCCN 2010;8[Suppl 1]:S4–S12)

Supplement
Peripheral Neuropathy and Asthenia
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-5
This is a corrected copy of the article originally printed in the supplement to JNCCN. This corrected copy also includes additional material not in the original printed supplement.
The incidence of thalidomide-induced PN varies among different patient populations, treatment regi-mens, and diagnostic criteria, but estimates range from 37% to 83%.1,5,9,13,15–21 Most cases are mild to moderate, classified as grades 1 to 2 (Table 1).22 Evidence from numerous studies indicates that the risk and severity of thalidomide-induced PN increases with cumulative dose or treatment duration, particularly when therapy extends beyond 6 months,1,5,7,15–17,19,23 although neuro-toxicity can also occur with short-term exposure.
Bortezomib-Induced PN (BiPN)Bortezomib-induced PN is predominantly a small-fiber sensory neuropathy, characterized by distal symmetric loss of all modalities in the lower limbs.3,9,24,25 Clini-cal signs and symptoms include burning dysesthesia, numbness, hyperesthesia, and pain; effects are typi-cally more pronounced in the lower limbs.9,25 Motor involvement is less likely with bortezomib than with thalidomide, but it may result in mild distal lower limb weakness.9 Autonomic dysfunction is frequently observed with bortezomib-induced PN; clinical mani-festations include gastrointestinal adverse effects (e.g., diarrhea, nausea, constipation, vomiting, anorexia) and hypotension.25,26 The neurotoxic effects of bort-ezomib therapy are generally reversible with dose re-duction or treatment discontinuation.3,4,11,14,24,27–31
The distinctive clinical features of bortezomib-associated neuropathy suggest fundamental differ-ences in its pathogenesis compared with thalidomide and other agents.9,24,25,28 Findings from recent in vitro
Clinical FeaturesTreatment-related PN depends on the agents used, as described subsequently, and is typically a length-dependent, axonal, sensory, or mixed sensorimotor neuropathy with symmetric, distal, and progressive signs and symptoms. Clinical manifestations are usu-ally agent-specific but range from temporary numb-ness, paresthesia, dysesthesia, hyperesthesia, loss of deep tendon reflexes, and muscle weakness or cramps to burning pain, muscle wasting, and paralysis. Au-tonomic involvement may result in orthostatic hy-potension, constipation/ileus, and urinary bladder or sexual dysfunction. In the most extreme cases, the manifestations of treatment-related PN can be life-threatening but this is, fortunately, very rare.7,9,12
Thalidomide-Induced PN (TiPN)Thalidomide has been shown to produce a small- and large-fiber sensory PN with distal symmetric loss of all modalities, primarily affecting the lower limbs. Asso-ciated clinical signs and symptoms typically include tingling or painful paresthesias and numbness in the feet and sometimes the hands.1,5,7,9,13 Motor neuropa-thy occurs infrequently with thalidomide treatment; if present, it is usually mild in severity.9,14 Autonomic manifestations are common, and include gastrointesti-nal (e.g., constipation, anorexia, nausea) as well as car-diovascular (e.g., hypotension, bradycardia) effects.15–17 Although the symptoms of thalidomide-induced PN are usually reversible after dose reduction or treatment stoppage, some effects may be permanent.15,17
Table 1 National Cancer Institute Common Toxicity Criteria (Version 3) for Peripheral Neuropathy
Adverse Event
Grade
0 1 2 3 4 5
Neuropathy: motor
Normal Asymptomatic; weakness on examination/testing only
Symptomatic; weakness interfering with function but not interfering with ADL
Weakness interfering with ADL; bracing or assistance to walk (e.g., cane or walker) indicated
Life threatening; disabling (e.g., paralysis)
Death
Neuropathy: sensory
Normal Asymptomatic; loss of deep tendon reflexes or paresthesia (including tingling) but not interfering with function
Sensory alteration or paresthesia (including tingling), interfering with function but not interfering with ADL
Sensory alteration or paresthesia interfering with ADL
Disabling Death
Abbreviation: ADL, activities of daily living. Adapted from National Cancer Institute. Cancer Therapy Evaluation Program, Common Terminology Criteria for Adverse Events v3.0 (CTCAE). Available at: http://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcaev3.pdf. Accessed August 28, 2009.

Supplement
Richardson et al.
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-6
This is a corrected copy of the article originally printed in the supplement to JNCCN. This corrected copy also includes additional material not in the original printed supplement.
and in vivo studies suggest that proteasome inhibitor-induced PN may be mechanism-based (a consequence of proteasome inhibition itself), with dorsal root gan-glia identified as a primary target leading to secondary peripheral nerve degeneration.32 However, a seperate preclinical study suggested that the dorsal root gan-glia lesions seen with bortezomib administration did not occur with carfilzomib, a second-generation pro-teasome inhibitor currently being investigated for the treatment of MM, although other studies have sug-gested carfilzomib, and agents in its class do in fact cause dorsal root ganglion abnormality.32,33 Further re-search is necessary to determine whether the mecha-nism underlying bortezomib-induced PN represents a class effect of proteasome inhibitors. However, clini-cal studies to date suggest this to be true, but with the degree of PN being less with carfilzomib.34
The reported incidence of treatment-emergent PN with bortezomib is 31% to 64%, with severe (grade 3 or 4) symptoms seen in 3% to 22% of pa-tients.3,4,6,11,27–31,35–37 Evidence of the dose-related and cumulative nature of bortezomib-induced neurotox-icity has been provided in several phase II and III studies, with reversibility also demonstrated in each of these.4,11,24,27–29,35,38
Assessment/MonitoringA comprehensive neuropathy assessment may in-volve a combination of patient history, clinical neu-rologic examination, and neurophysiologic testing. Diagnosis of any underlying conditions or comorbid-ities that may increase the risk of treatment-related PN is a critical part of this evaluation. PN severity should be characterized at each assessment to moni-tor neuropathy progression and determine whether a regimen change or some other type of interven-tion is indicated. Patient education is important for improving awareness and encouraging the reporting of symptoms. Neurotoxicity assessment tools (see an example in Figure 1) may be useful for quantifying PN severity based on patient self-reports.12
Patients should be evaluated for evidence of neu-ropathy at baseline, before initiating a change in thera-peutic regimen, in conjunction with new or worsening signs or symptoms, and periodically throughout treat-ment. Patient- or agent-specific risk factors may neces-sitate more aggressive or targeted assessments. For ex-ample, because the incidence of thalidomide-induced PN has been reported to increase with longer duration of administration; monthly evaluation of patients is
recommended during the first 3 months of treatment and regularly thereafter.15 In addition, neurophysi-ologic testing is suggested (e.g., sensory nerve action potential amplitudes) every 6 months for the detection of asymptomatic PN.15
Management StrategiesDose Reduction and Schedule Modification: For pa-tients with grade 1 PN, thalidomide therapy may be continued with a 50% dose reduction, particularly if no other treatment options are available.17 For grade 2 PN, thalidomide therapy should be discontinued until neuropathy has returned to baseline or less than a grade 1 severity; treatment may subsequent-ly be resumed with dosage levels reduced by half.17 Some recommend restricting thalidomide therapy to short-term use (e.g., < 6 months) or low-dose regimens (e.g., 50 mg/d).5,18 In general, a conserva-tive PN management approach is recommended for newly diagnosed MM patients, especially when treatment alternatives exist.17 Bortezomib dose mod-ifications should be made according to the directions in the prescribing information,25 which are based on PN severity and the degree of associated neuropathic pain or impaired function (Table 2). The benefits of dose modification were shown in the pivotal phase III trial of bortezomib, with resolution or improve-ment of grade 2 or higher PN observed in 68% of pa-tients who underwent a prespecified dose-reduction protocol, compared with 47% of those who did not.28
Therapeutic Intervention: Nonpharmacologic man-agement of sensory PN symptoms or neuropathic pain may involve the use of daily vitamins and nutritional supplements (e.g., multi-B complex vitamins [B1, B6, B12], folic acid, magnesium, potassium, vitamin E, acetyl l-carnitine, α-lipoic acid, l-glutamine; see Table 3 for dosing), emollient creams (e.g., cocoa butter, menthol, and eucalyptus-based creams), and physical therapy, as well as therapeutic massage.12,39–43 These recommen-dations are largely based on anecdotal evidence, and controlled studies are needed to confirm their efficacy. Moreover, use of supplements on the day of bortezomib administration is not recommended based upon pre-clinical data suggesting the possibility of antagonism, although this has not been confirmed clinically.44
If symptoms are inadequately controlled with nonpharmacologic intervention alone, pharmacologic therapy is advised. Because response is likely to vary substantially for each individual, a stepwise process may be necessary.41,45 Evidence of the therapeutic ben-

Supplement
Peripheral Neuropathy and Asthenia
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-7
This is a corrected copy of the article originally printed in the supplement to JNCCN. This corrected copy also includes additional material not in the original printed supplement.
For additional symptomatic relief, the tricy-clic antidepressant nortriptyline may be added at an initial dose of 25 mg every night at bedtime; dosing may be increased to 50 mg after 2 weeks, with further dose escalation of 25 mg monthly (as tolerated), up to a maximum of 100 mg every night at bedtime. If patient response remains inadequate, duloxetine, an antidepressant FDA approved for the treatment of neuropathic pain associated with diabetic peripheral neuropathy, may be prescribed at a dose of 20 to 60 mg every day. Topical lidocaine, which is FDA approved for postherpetic neuralgia, is sometimes helpful for the control of neuropathic pain in the feet and hands.
efits of many pharmacologic agents used in the treat-ment of neuropathic pain comes primarily from short-term clinical studies, so the long-term efficacy of such therapy has not yet been established.45
Among the pharmacologic agents recommended for the treatment of grade 1 or higher sensory PN or neuropathic pain are gabapentin, pregabalin, nor-triptyline, duloxetine, and topical lidocaine. Gaba-pentin, an anticonvulsant approved by the FDA for the treatment of neuropathic pain associated with postherpetic neuralgia, may be administered at an initial dose of 300 mg, 3 times daily, with titration as tolerated up to 1200 mg, 3 times daily.3
Figure 1 Tool for assessing severity of peripheral neuropathy.Republished with permission from Oncology Nursing Society. Tariman JD, Love G, McCullagh E, Sandifer S. Peripheral neuropathy associated with novel therapies in patients with multiple myeloma: consensus statement of the IMF Nurse Leadership Board. Clin J Oncol Nurs 2008;12(3 Suppl):29–36; permission conveyed through Copyright Clearance Center, Inc.
Instructions for Patients
By circling one number per line, please indicate how true each statement has been for you during the past seven days using the following scale.
0 = not at all1 = a little bit2 = somewhat3 = quite a bit4 = very much
I have numbness or tingling in my hands 0 1 2 3 4
I have numbness or tingling in my feet 0 1 2 3 4
I have discomfort in my hands 0 1 2 3 4
I have discomfort in my feet 0 1 2 3 4
I have joint pain or muscle cramps 0 1 2 3 4
I feel weak all over 0 1 2 3 4
I have trouble hearing 0 1 2 3 4
I get a ringing or buzzing in my ears 0 1 2 3 4
I have trouble buttoning buttons 0 1 2 3 4
I have trouble feeling the shape of small objects when they are in my hand 0 1 2 3 4
I have trouble walking 0 1 2 3 4
Instructions for Healthcare Professionals
This assessment tool is provided to help you evaluate peripheral neuropathy in patients receivingchemotherapy. Healthcare professionals may �nd discussion of patients’ responses helpful in determining the grade of neuropathy as de�ned by the National Cancer Institute Common TerminologyCriteria for Adverse Events (http://ctep.cancer.gov); however, no direct correlation exist between assessment scores and toxicity grades.

Supplement
Richardson et al.
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-8
This is a corrected copy of the article originally printed in the supplement to JNCCN. This corrected copy also includes additional material not in the original printed supplement.
Future DirectionsThe use of newer MM agents with improved neurotox-icity profiles can reduce the risk of treatment-related PN. Phase III trials have shown that with the potent thalidomide analogue lenalidomide, the incidence of grade 3 or 4 PN is less than 3%.46,47 The risk of treat-ment-emergent PN also appears to be decreased with the second-generation proteasome inhibitors carfilzo-mib (PR-171)48 and salinosporamide A (NPI-0052).49
The risk of treatment-related PN may also be re-duced by combining agents that have synergistic or neuroprotective effects. For example, a number of in-vestigations have provided evidence of the potential synergy between proteasome inhibitors and immu-nomodulatory agents in terms of anti-tumor effect.50 Importantly, while neuropathy as a treatment-relat-ed side effect is a concern with this combination, the severity of PN has been less than expected. Specifi-cally, studies have shown that the incidence of grade 3 PN is 5% to 10% with bortezomib/thalidomide/dexamethasone combination therapy.31,51–53 Impor-tantly, no occurrences of grade 4 PN and only 1 case of grade 3 PN have been seen in a phase I/II study of lenalidomide/bortezomib/dexamethasone (RVD) in 66 subjects with newly diagnosed MM.52 In a phase II trial of RVD treatment in 64 patients with relapsed and/or refractory MM, only 1 case of grade 3 PN was seen, which occurred despite bortezomib reduction and required treatment discontinuation but subse-quent improvement followed.54 This suggests that such combinations may favorably influence at least the severity of PN, perhaps through an anti-inflam-matory mechanism, as well as allowing dose reduc-tion without loss of therapeutic effect.
Initial findings suggest that the heat shock protein inhibitor tanespimycin may exhibit both synergistic
and neuroprotective effects when combined with bort-ezomib for treatment of MM. In a phase I/II study, no cases of grade 3/4 treatment-emergent PN were detect-ed in 72 patients treated with bortezomib plus tanespi-mycin for relapsed and refractory MM.55
AstheniaAsthenia, commonly referred to as fatigue, has been defined as a “distressing, persistent, subjective sense of physical, emotional, and/or cognitive tiredness or exhaustion” that is not proportional to recent activity, interferes with usual functioning, and is not relieved by rest.56,57 Its symptoms can also include generalized weakness, lack of energy, and malaise. Many MM pa-tients with asthenia have comorbidities such as de-pression, anxiety, and impaired psychosocial function-ing, which can be exacerbated by medication effects, especially in combination with glucocorticoids.
Asthenia is a highly prevalent condition among patients with cancer in general and the most common side effect of cancer treatment.58 Clinical trial data sug-gest that asthenia of any grade affects approximately 40% to 75% of patients with newly diagnosed disease, 60% to 93% of individuals treated with radiotherapy, and 76% to 96% of patients treated with chemo-therapy, depending on the type of primary neoplasia and treatment regimen.58–62 Examples of MM-specific rates in phase III trials are grade 3/4 asthenia has been reported by 15% of newly diagnosed patients receiv-ing thalidomide/dexamethasone,20 by about 6% of pa-tients with relapsed–refractory disease receiving bort-ezomib,29 by 6% of patients with relapsed–refractory disease receiving bortezomib/liposomal doxorubicin,63 and by 10% of newly diagnosed patients receiving lenalidomide/low-dose dexamethasone.64 The results
Table 2 Bortezomib Dose Modification Based on Severity of Bortezomib-Induced Peripheral NeuropathySeverity of Peripheral Neuropathy Modification of Dose and Regimen
Grade 1 (paresthesia or loss of reflex) without pain or loss of function No action
Grade 1 with pain or grade 2 (interferes with function but not with activities of daily living)
Reduce bortezomib dose from 1.3 to 1.0 mg/m2
Grade 2 with pain or grade 3 (interferes with activities of daily living) Withhold until toxicity resolves, then re-initiate bortezomib at 0.7 mg/m2 once weekly
Grade 4 (permanent sensory loss that interferes with function) Discontinue treatment
From Richardson PG, Xie W, Mitsiades C, et al. Single-agent bortezomib in previously untreated multiple myeloma: efficacy, char-acterization of peripheral neuropathy, and molecular correlations with response and neuropathy. J Clin Oncol 2009;27:3518–3525. Reprinted with permission. ©2009 American Society of Clinical Oncology. All rights reserved.

Supplement
Peripheral Neuropathy and Asthenia
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-9
This is a corrected copy of the article originally printed in the supplement to JNCCN. This corrected copy also includes additional material not in the original printed supplement.
7-day period, using a predefined scale. A comprehen-sive primary asthenia examination is recommended for all patients reporting moderate to severe fatigue. No standardized guidelines for diagnosis of asthenia have been established, but the Tenth Revision of the International Classification of Disease (ICD-10) in-cludes a proposed set of diagnostic criteria (Table 4).65
Management approaches for asthenia include 1) treatment of contributing factors (e.g., anemia, pain, depression/anxiety, systemic disorders, such as hypo-thyroidism, sleep disturbances, nutritional deficien-cies, and medication side effects); 2) patient education regarding the causes of asthenia and general strategies for fatigue self-management; 3) nonpharmacologic in-
of patient surveys suggest that asthenia exerts a more negative and longer-lasting effect on patients than pain, nausea, or depression, but that treatment is pre-scribed in as few as 14% to 40% of cases.59,62 This is true even though asthenia may persist for months or even years after treatment is completed.
According to the NCCN Clinical Practice Guide-lines in Oncology: Cancer-Related Fatigue (to view the most recent version of these guidelines, visit the NCCN Web site at www.NCCN.org), every cancer patient should be screened for asthenia at regular in-tervals, in conjunction with other vital-sign monitor-ing.56 During the initial screening, patients should be asked to assess their level of fatigue during the previous
Table 3 Suggested Doses of Some Commonly Used Vitamins/Supplements for PN*Vitamin/Supplement Dosing Regimen
Multi-B complex vitamins (with B1, B6, B12, folic acid and other)
B6 should be approximately 50 mg daily, not to exceed 100 mg per day. Folic acid should be 1 mg per day.
Vitamin E 400 IU daily
Vitamin D 400-800 IU daily
Fish oils (Omega-3 fatty acids [EPA and DHA]) 1–2 capsules daily with food (1 capsule is usually 1 g)
Magnesium Suggested doses include 250 mg twice a day, with prescription doses of 400 mgs daily, with dose frequency contingent on monitoring serum magnesium. May cause diarrhea in larger doses.
Potassium Either as provided by the treating physician or foods that are rich in potassium (eg, bananas, oranges and potatoes); serum K should be monitored.
Tonic water (i.e. selzer water with quinine) Drink one glass in evening and any other time cramping occurs.
Acetyl-L-carnitine 500 mg twice a day with food; Can take up to 2000 mg a day.
Alpha-lipoic acid 300 mg to 1000 mg a day with food.
Glutamine 1 g up to 3 times a day with food.
*For either thalidomide-induced peripheral neuropathy (TiPN) or bortezomib-induced peripheral neuropathy (BiPN) Please note: It is currently advised that patients do not take supplements on days of bortezomib infusions, and all supplements must be discussed with and approved by the treating physicians concerned. Supplements should be taken with food unless otherwise indicated. Additional Notes and Precautions:Nutritional supplements should be administered at low doses since there is preclinical evidence that the administration of pyridoxine (vitamin B6) and vitamin C at high doses may be harmful. Vitamin B6 can cause additional sensory neuropathy in patients with impaired renal function and in association with a protein-deficient diet. (Levine S, Saltzman A. Pyridoxine (vitamin B6) toxicity: enhancement by uremia in rats. Food Chem Toxicol 2002;40:1449–1451. Levine S, Saltzman A. Pyridoxine (vitamin B6) neurotoxicity: enhancement by protein-deficient diet. J Appl Toxicol 2004;24:497–500.)
Vitamin C may interfere with bortezomib metabolism and may also abrogate bortezomib-mediated inhibition of proteasome activity; therefore, its concomitant use with bortezomib should be avoided. (Catley L, Anderson KC. Velcade and vitamin C: too much of a good thing? Clin Cancer Res 2006;12:3-4. Perrone G, Hideshima T, Ikeda H, et al. Ascorbic acid inhibits antitumor activity of bortezomib in vivo. Leukemia 2009;23:1679–1686; Epub 2009 Apr 16.)
In preclinical studies, the anticancer activity of bortezomib has been shown to be blocked by the polyphenols. It is speculated that the vicinal diols in the polyphenols interact with the boronic acid of bortezomib and convert the active triangular boronic acid of bortezomib to an inactive tetrahedral boronate, thus inhibiting the anti-myeloma activity of bortezomib. The restriction of the intake of natural polyphenols in foods or vitamin supplements (such as in green tea) during bortezomib treatment in MM patients should be considered. (Kim TY, Park J, Oh B, et al. for the Korean Multiple Myeloma Working Party (KMMWP). Natural polyphenols antagonize the antimyeloma activity of proteasome inhibitor bortezomib by direct chemical interaction. Br J Haematol 2009;146:270–281.)

Supplement
Richardson et al.
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-10
This is a corrected copy of the article originally printed in the supplement to JNCCN. This corrected copy also includes additional material not in the original printed supplement.
terventions, including counseling, occupational ther-apy, cognitive behavioral therapy, exercise, dietary changes, and stress management; and 4) pharmaco-logic symptomatic therapy.56 Clinical trial data and anecdotal evidence suggest that psychostimulants, low-dose corticosteroids, and antidepressants may be helpful,66 but psychostimulants are investigational for this purpose and should be used with caution only af-ter treatment- and disease-specific morbidities have been characterized or excluded. The optimal dose and schedule have not been established for use of psycho-stimulants in cancer patients. Specific measures in MM patients include attention to hydration, evalua-tion of novel-agent specific–effects (such as those seen with bortezomib, thalidomide, and lenalidomide); ex-clusion of important co-morbidities (e.g., thyroid defi-ciency, amyloidosis), and care regarding the possibility of progressive disease.67
ConclusionsPeripheral neuropathy and asthenia are frequent complications of MM treatment. These complica-tions interfere with optimum therapy and adverse-ly affect patient outcomes as well as quality of life.
Among novel therapies associated with significant PN are bortezomib and thalidomide, both agents that have transformed the MM treatment paradigm through improvements in response rates, time-to-progression, and survival. Novel combination thera-pies for MM have the potential to reduce side effects, as well as enhance activity, thus improving the ther-apeutic index.68 In addition, effective management strategies are critical to reduce the risk of further treatment-related toxicities and improve the benefits of therapy in this otherwise incurable malignancy.
AcknowledgmentThe authors thank Kimberly Cohen for medical writing assistance and Katherine Redman for ad-ministrative support. The authors also gratefully ac-knowledge the input of Kathleen Colson, RN, and Deborah Doss, RN.
References 1. Plasmati R, Pastorelli F, Cavo M, et al. Neuropathy in multiple
myeloma treated with thalidomide: a prospective study. Neurology 2007;69:573–581.
Table 4 ICD-10 Criteria for Cancer-Related FatigueA. Six (or more) of the following symptoms have been present every day or nearly every day during the same 2-week period
in the past month, with at least 1 symptom (A1) being significant fatigue:
A1. Significant fatigue, diminished energy, or increased need to rest, disproportionate to any recent change in activity
A2. Complaints of generalized weakness or limb heaviness
A3. Diminished concentration or attention
A4. Decreased motivation or interest to engage in usual activities
A5. Insomnia or hypersomnia
A6. Experience of sleep as unrefreshing or nonrestorative
A7. Perceived need to struggle to overcome inactivity
A8. Marked emotional reactivity (e.g., sadness, frustration, or irritability) to feeling fatigued
A9. Difficulty completing daily tasks attributed to feeling fatigued
A10. Perceived problems with short-term memory
A11. Postexertional malaise lasting several hours
B. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning
C. Evidence from the history, physical examination, or laboratory findings shows that the symptoms are a consequence of cancer or cancer therapy
D. The symptoms are not primarily a consequence of comorbid psychiatric disorders such as major depression, somatization disorder, somatoform disorder, or delirium
Reprinted with permission from Cella D, Peterman A, Passik S, et al. Progress toward guidelines for the management of fatigue. Oncology 1998;12:369–377.

Supplement
Peripheral Neuropathy and Asthenia
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-11
This is a corrected copy of the article originally printed in the supplement to JNCCN. This corrected copy also includes additional material not in the original printed supplement.
2. Chaudhry V, Cornblath DR, Polydefkis M, et al. Characteristics of bortezomib- and thalidomide-induced peripheral neuropathy. J Peripher Nerv Syst 2008;13:275–282.
3. Richardson PG, Xie W, Mitsiades C, et al. Single-agent bortezomib in previously untreated multiple myeloma: efficacy, characterization of peripheral neuropathy, and molecular correlations with response and neuropathy. J Clin Oncol 2009;27:3518–3525.
4. Richardson PG, Briemberg H, Jagannath S, et al. Frequency, characteristics, and reversibility of peripheral neuropathy during treatment of advanced multiple myeloma with bortezomib. J Clin Oncol 2006;24:3113–3120.
5. Mileshkin L, Stark R, Day B, et al. Development of neuropathy in patients with myeloma treated with thalidomide: patterns of occurrence and the role of electrophysiologic monitoring. J Clin Oncol 2006;24:4507–4514.
6. Badros A, Goloubeva O, Dalal JS, et al. Neurotoxicity of bortezomib therapy in multiple myeloma: a single-center experience and review of the literature. Cancer 2007;110:1042–1049.
7. Wickham R. Chemotherapy-induced peripheral neuropathy: a review and implications for oncology nursing practice. Clin J Oncol Nurs 2007;11:361–376.
8. Wolf J, Richardson PG, Schuster M, et al. Utility of bortezomib retreatment in relapsed or refractory multiple myeloma patients: a multicenter case series. Clin Adv Hematol Oncol 2008;6:755–760.
9. Windebank AJ, Grisold W. Chemotherapy-induced neuropathy. J Peripher Nerv Syst 2008;13:27–46.
10. Palumbo A, Rajkumar SV. Treatment of newly diagnosed myeloma. Leukemia 2009;23:449–456.
11. Mateos MV, Richardson P, Schlag R, et al. Peripheral neuropathy with VMP resolves in the majority of patients and shows a rate plateau [abstract]. Presented at the XII International Myeloma Workshop; February 26–March 1, 2009; Washington, D.C. Abstract 172.
12. Tariman JD, Love G, McCullagh E, Sandifer S; for the IMF Nurse Leadership Board. Peripheral neuropathy associated with novel therapies in patients with multiple myeloma: consensus statement of the IMF Nurse Leadership Board. Clin J Oncol Nurs 2008;12(3 Suppl):29–36.
13. Mileshkin L, Prince HM. The troublesome toxicity of peripheral neuropathy with thalidomide. Leuk Lymphoma 2006;47:2276–2279.
14. Kannarkat G, Lasher EE, Schiff D. Neurologic complications of chemotherapy agents. Curr Opin Neurol 2007;20:719–725.
15. Thalomid package insert. Summit, NJ: Celgene Corporation; 2007. 16. Palumbo A, Facon T, Sonneveld P, et al. Thalidomide for treatment
of multiple myeloma: 10 years later. Blood 2008;111:3968–3977. 17. Ghobrial IM, Rajkumar SV. Management of thalidomide toxicity. J
Support Oncol 2003;1:194–205. 18. Offidani M, Corvatta L, Marconi M, et al. Common and rare
side-effects of low-dose thalidomide in multiple myeloma: focus on the dose-minimizing peripheral neuropathy. Eur J Haematol 2004;72:403–409.
19. Richardson P, Schlossman R, Jagannath S, et al. Thalidomide for patients with relapsed multiple myeloma after high-dose chemotherapy and stem cell transplantation: results of an open-label multicenter phase 2 study of efficacy, toxicity, and biological activity. Mayo Clin Proc 2004;79:875–882.
20. Rajkumar SV, Blood E, Vesole D, et al. Phase III clinical trial of thalidomide plus dexamethasone compared with dexamethasone alone in newly diagnosed multiple myeloma: a clinical trial
coordinated by the Eastern Cooperative Oncology Group. J Clin Oncol 2006;24:431–436.
21. Rajkumar SV, Rosiñol L, Hussein M, et al. Multicenter, randomized, double-blind, placebo-controlled study of thalidomide plus dexamethasone compared with dexamethasone as initial therapy for newly diagnosed multiple myeloma. J Clin Oncol 2008;26:2171–2177.
22. National Cancer Institute. Cancer Therapy Evaluation Program, Common Terminology Criteria for Adverse Events. Version 3.0 [Web page]. August 9, 2006. Available at: http://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcaev3.pdf. Accessed August 28, 2009.
23. Cavaletti G, Beronio A, Reni L, et al. Thalidomide sensory neurotoxicity: a clinical and neurophysiologic study. Neurology 2004;62:2291–2293.
24. Richardson P, Jagannath S, Colson K. Optimizing the efficacy and safety of bortezomib in relapsed multiple myeloma. Clin Adv Hematol Oncol 2006;4(5 Suppl 13):1–8.
25. Velcade package insert. Cambridge, MA: Millennium Pharmaceuticals, Inc; 2008.
26. Crocchiolo R, Ferrari S, Calbi V, et al. Effect of bortezomib on the autonomic nervous system [abstract]. Presented at the 2006 American Society of Hematology Annual Meeting; December 9–12, 2006; Orlando, Florida. Abstract 5101.
27. Richardson PG, Barlogie B, Berenson J, et al. A phase 2 study of bortezomib in relapsed, refractory myeloma. N Engl J Med 2003;348:2609–2617.
28. Richardson PG, Sonneveld P, Schuster MW, et al. Reversibility of symptomatic peripheral neuropathy with bortezomib in the phase III APEX trial in relapsed multiple myeloma: impact of a dose-modification guideline. Br J Haematol 2009;144:895–903.
29. Richardson PG, Sonneveld P, Schuster MW, et al. Bortezomib or high-dose dexamethasone for relapsed multiple myeloma. N Engl J Med 2005;352:2487–2498.
30. El-Cheikh J, Stoppa AM, Bouabdallah R, et al. Features and risk factors of peripheral neuropathy during treatment with bortezomib for advanced multiple myeloma. Clin Lymphoma Myeloma 2008;8:146–152.
31. Caravita T, Petrucci MT, Spagnoli A, et al. Neuropathy in multiple myeloma patients treated with bortezomib: a multicenter experience [abstract]. Presented at the 2007 American Society of Hematology Annual Meeting; December 8–11, 2007; Atlanta, Georgia. Abstract 4823.
32. Silverman L, Csizmadia V, Brewer K, et al. Proteasome inhibitor associated neuropathy is mechanism based [abstract]. Annual Meeting of the American Society of Hematology. 2008. Presented at the 2008 American Society of Hematology Annual Meeting; December 6–9, 2008; San Francisco, California. Abstract 2646.
33. Kirk CJ, Jiang J, Muchamuel T, et al. The selective proteasome inhibitor carfilzomib is well tolerated in experimental animals with dose intensive administration [abstract]. Presented at the 2008 American Society of Hematology Annual Meeting; December 6–9, 2008; San Francisco, California. Abstract 2765.
34. Jagannath S, Vij R, Stewart AK, et al. The Multiple Myeloma Research Consortium (MMRC). Initial results of PX-171-003, an open-label, single-arm, phase II study of carfilzomib (CFZ) in patients with relapsed and refractory multiple myeloma (MM) [abstract]. Blood 2008;112:Abstract 864.
35. Jagannath S, Barlogie B, Berenson J, et al. A phase 2 study of two doses of bortezomib in relapsed or refractory myeloma. Br J Haematol 2004;127:165–172.

Supplement
Richardson et al.
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-12
This is a corrected copy of the article originally printed in the supplement to JNCCN. This corrected copy also includes additional material not in the original printed supplement.
36. Richardson PG, Hideshima T, Mitsiades C, Anderson K. Proteasome inhibition in hematologic malignancies. Ann Med 2004;36:304–314.
37. Dhawan R, Delforge M, De Samblanx H, et al. Peripheral neuropathy as assessed in an international observational study of bortezomib [abstract]. Presented at the XII International Myeloma Workshop; February 26–March 1, 2009; Washington, D.C. Abstract 134.
38. San Miguel JF, Schlag R, Khuageva NK, et al. Bortezomib plus melphalan and prednisone for initial treatment of multiple myeloma. N Engl J Med 2008;359:906–917.
39. Colson K, Doss DS, Swift R, Tariman J. Expanding role of bortezomib in multiple myeloma: nursing implications. Cancer Nurs 2008;31:239–249.
40. Smith GG. Proteasome inhibition in cancer therapy. J Infus Nurs 2005;28:258–264.
41. Dworkin RH, O’Connor AB, Backonja M, et al. Pharmacologic management of neuropathic pain: evidence-based recommendations. Pain 2007;132:237–251.
42. Jensen TS, Finnerup NB. Management of neuropathic pain. Curr Opin Support Palliat Care 2007;1:126–131.
43. Colvin LA, Johnson PR, Mitchell R, et al. From bench to bedside: a case of rapid reversal of bortezomib-induced neuropathic pain by the TRPM8 activator, menthol. J Clin Oncol 2008;26:4519–4520.
44. Perrone G, Hideshima T, Ikeda T, et al. Ascorbic acid inhibits antitumor activity of bortezomib in vivo. Leukemia 2009;23:1679–1686
45. Zin CS, Nissen LM, Smith MT, et al. An update on the pharmacological management of post-herpetic neuralgia and painful diabetic neuropathy. CNS Drugs 2008;22:417–442.
46. Weber DM, Chen C, Niesvizky R, et al. Lenalidomide plus dexamethasone for relapsed multiple myeloma in North America. N Engl J Med 2007;357:2133–2142.
47. Dimopoulos M, Spencer A, Attal M, et al. Lenalidomide plus dexamethasone for relapsed or refractory multiple myeloma. N Engl J Med 2007;357:2123–2132.
48. Jagannath S, Vij R, Stewart K, et al. Final results of PX-171-003-A0, part 1 of an open-label single-arm, phase II study of carfilzomib in patients with relapsed and refractory multiple myeloma [abstract]. Presented at the 2009 American Society of Clinical Oncology Annual Meeting; May 29–June 2, 2009; Orlando, Florida. Abstract 8504.
49. Hofmeister CC, Richardson P, Zimmerman T, et al. Clinical trial of the novel structure proteasome inhibitor NPI-0052 in patients with relapsed/refractory multiple myeloma [abstract]. Presented at the 2009 American Society of Clinical Oncology Annual Meeting; May 29–June 2, 2009; Orlando, Florida. Abstract 8505.
50. Mitsiades N, Mitsiades CS, Poulaki V, et al. Apoptotic signaling induced by immunomodulatory thalidomide analogs in human multiple myeloma cells: therapeutic implications. Blood 2002;99:4525–4530.
51. Wang M, Giralt S, Delasalle K, et al. Bortezomib in combination with thalidomide-dexamethasone for previously untreated multiple myeloma. Hematology 2007;12:235–239.
52. Zangari M, Barlogie B, Burns MJ, et al. Velcade-thalidomide-dexamethasone for advance and refractory multiple myeloma: long-term follow-up of phase I-II trial UARK 2001-37: superior outcome in patients with normal cytogenetics and no prior thalidomide [abstract]. Presented at the 2005 American Society of Hematology Annual Meeting; December 10–13, 2005; Atlanta, Georgia. Abstract 2552.
53. Richardson P, Lonial S, Jakubowiak A, et al. Lenalidomide, bortezomib, and dexamethasone in patients with relapsed or relapsed/refractory multiple myeloma: encouraging efficacy in high risk groups with updated results of a phase I/II study [abstract]. Presented at the 2008 American Society of Hematology Annual Meeting; December 6–9, 2008; San Francisco, California. Abstract 92.
54. Richardson P, Jagannath S, Jakubowiak A, et al. Lenalidomide, bortezomib, and dexamethasone in patients with newly diagnosed multiple myeloma: encouraging response rates and tolerability with correlation of outcome and adverse cytogenetics in a phase II study [abstract]. Presented at the 2008 American Society of Hematology Annual Meeting; December 6–9, 2008; San Francisco, California. Abstract 1742.
55. Richardson PG, Chanan-Khan A, Lonial S, et al. Tanespimycin plus bortezomib in patients with relapsed and refractory multiple myeloma: final results of a phase I/II study [abstract]. Presented at the 2009 American Society of Clinical Oncology Annual Meeting; May 29–June 2, 2009; Orlando, Florida. Abstract 8503.
56. Berger AM, Abernethy AP, Atkinson A, et al. NCCN clinical practice guidelines in oncology: cancer-related fatigue, version 1.2009. Available at: http://www.nccn.org/professionals/physician_gls/PDF/fatigue.pdf. Accessed May 12, 2009.
57. Morrow GR, Shelke AR, Roscoe JA, et al. Management of cancer-related fatigue. Cancer Invest 2005;23:229–239.
58. Stasi R, Abriani L, Beccaglia P, et al. Cancer-related fatigue: evolving concepts in evaluation and treatment. Cancer 2003;98:1786–1801.
59. Curt GA, Breitbart W, Cella D, et al. Impact of cancer-related fatigue on the lives of patients: new findings from the Fatigue Coalition. Oncologist 2000;5:353–360.
60. Morrow GR. Cancer-related fatigue: causes, consequences, and management. Oncologist 2007;12(Suppl 1):1–3.
61. Hofman M, Ryan JL, Figueroa-Moseley CD, et al. Cancer-related fatigue: the scale of the problem. Oncologist 2007;12(Suppl 1):4–10.
62. Vogelzang NJ, Breitbart W, Cella D, et al. Patient, caregiver, and oncologist perceptions of cancer-related fatigue: results of a tripart assessment survey. Semin Hematol 1997;34(3 Suppl 2):4–12.
63. Orlowski RZ, Nagler A, Sonneveld P, et al. Randomized phase III study of pegylated liposomal doxorubicin plus bortezomib compared with bortezomib alone in relapsed or refractory multiple myeloma: combination therapy improves time to progression. J Clin Oncol 2007;25:3892–3901.
64. Rajkumar SV, Jacobus S, Callander N, et al. A randomized trial of lenalidomide plus high-dose dexamethasone vs lenalidomide plus low-dose dexamethasone in newly diagnosed multiple myeloma (E4A03): a trial coordinated by the Eastern Cooperative Oncology Group. Presented at the 2007 American Society of Hematology Annual Meeting; December 8–11, 2007; Atlanta, Georgia. Abstract 74.
65. Breitbart W, Alici-Evcimen Y. Update on psychotropic medications for cancer-related fatigue. J Natl Compr Canc Netw 2007;5:1081–1091.
66. Breitbart W, Alici Y. Pharmacologic treatment options for cancer-related fatigue: current state of clinical research. Clin J Oncol Nurs 2008;12(5 Suppl):27–36.
67. Laubach JP, Mitsiades CS, Mahindra A, et al. Novel therapies in the treatment of multiple myeloma. J Natl Compr Cancer Netw 2009;7:947–960.
68. Richardson PG, Mitsiades C, Schlossman R, et al. New drugs for myeloma. Oncologist 2007;12:664–689.

Supplement
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-13
Key WordsThalidomide, bortezomib, lenalidomide, deep vein thrombosis, pulmonary embolism, bisphosphonates, erythropoiesis-stimulating agents
AbstractVenous thromboembolism (VTE), osteonecrosis of the jaw, renal fail-ure, and anemia are all common complications of multiple myeloma therapy. Many of these adverse events have been documented only in the past 5 to 10 years, in conjunction with the introduction of a series of the newer therapies thalidomide, bortezomib, and lenalid-omide. This article discusses these complications in detail and pro-vides strategies for health care providers to best prevent, identify, and manage them. Preventive measures, such as VTE prophylaxis and appropriate dental hygiene, as well as patient education, dose adjustments, limited duration of drug treatment, and consideration of therapies that are associated with less burdensome adverse-event profiles, can contribute to substantially improved outcomes and quality of life. (JNCCN 2010;8[Suppl 1]:S13–S20)
and improved duration of response, but they have been associated with an increased risk of certain adverse events. Venous thromboembolism (VTE), osteonecro-sis of the jaw (ONJ), renal failure, and anemia are all common complications of MM therapy. Community oncologists should be familiar with these potential com-plications and the strategies for preventing, identifying, and managing them.
Venous ThromboembolismVTE typically manifests as deep vein thrombosis (DVT) or pulmonary embolism (PE). Both cancer and cancer treatments have been identified as discrete risk fac-tors.1 Current evidence indicates that cancer increases thrombosis risk 4.1-fold and chemotherapy increases the risk 6.5-fold.2 Other key VTE risk factors include older age, recent surgery, acute medical illness, and im-mobility or bed rest. The risk of VTE is typically cumu-lative.1 Therefore, even if an independent relationship between VTE and specific cancers such as MM were excluded, the advanced age of most MM patients and other factors common in MM patients would tend to place them at heightened VTE risk.3 A recent, retro-spective analysis of a managed care database of patients with MM (N = 1732) showed that 66.3% had at least 1 VTE risk factor and 48.3% had at least 2 risk factors.4
It has been posited that the hypercoagulable state typical with MM and other cancers provides a pro-thrombotic baseline environment. The prothrombotic state associated with MM may be due to multiple hemo-static abnormalities, including activation of coagulation pathways, reduced natural anticoagulation mechanisms,
Therapies such as thalidomide, bortezomib, and le-nalidomide have provided meaningful benefits in mul-tiple myeloma (MM), such as improved response rates
From aWeill Cornell Medical College, New York, New York, and bUniversity of Maryland, Greenebaum Cancer Center, Baltimore, Maryland.Dr. Niesvizky has disclosed that he has participated as an advisory board member, speakers’ bureau member, or consultant for Celgene Corp.; Millennium Pharmaceuticals, Inc.; and Proteolix, Inc. Dr. Badros has no interest, arrangement, or affiliation with the manufacturers of any products discussed in the article or their competitors.This work was supported by an educational grant from Millennium Pharmaceuticals, Inc.Correspondence: Ruben Niesvizky, MD, Weill Cornell Medical College, 520 East 70th Street, Starr 341, New York, NY 10021. E-mail: [email protected]
Complications of Multiple Myeloma Therapy, Part 2: Risk Reduction and Management of Venous Thromboembolism, Osteonecrosis of the Jaw, Renal Complications, and Anemia
Ruben Niesvizky, MD,a and Ashraf Z. Badros, MD,b New York, New York, and Baltimore, Maryland

Supplement
Niesvizky and Badros
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-14
is administered as a single agent.16,17 However, stud-ies have shown elevated VTE risk ranging from 8.5% to 15.0% when lenalidomide is combined with dexa-methasone.8,14,18,19 More recent trials have shown that lowering the dexamethasone dosage reduces the risk of VTE with lenalidomide substantially.20,21
Heightened VTE risk has also been associ-ated with the use of erythropoiesis-stimulating agents (ESAs), such as epoetin alfa and darbepo-etin alfa.12 Anemia is discussed in more detail in subsequent sections.
BortezomibThe proteasome inhibitor bortezomib does not ap-pear to increase VTE risk; in fact, it may exert anti-thrombotic actions. Proteasome inhibition is known to decrease expression of endothelial and vascular cell adhesion molecules; in addition, bortezomib has been shown to inhibit adenosine diphosphate–induced platelet aggregation.22 Two phase III studies indicate that bortezomib is associated with throm-bocytopenia rates ranging from 20% to 26% (grade 3) and 4% to 17% (grade 4), but a very low (1%) VTE rate.23,24
Treatment and Prophylaxis RecommendationsCurrent VTE prophylaxis guidelines from the American College of Chest Physicians (ACCP) recommend primary antithrombotic prophylaxis for patients with cancer only if they are bedridden or undergoing surgical intervention.1 However, as dis-cussed previously, without prophylaxis, the risk for VTE in treated MM patients is unacceptably high. In addition, PE is associated with a high case-fa-tality rate. One-week survival after PE is 71%, but one-quarter of all cases present as sudden death.25 Therefore, identifying high-risk patients and provid-ing them with appropriate prophylaxis is essential. Unfortunately, very few randomized studies have assessed the impact of anticoagulant prophylaxis in patients with cancer.
The International Myeloma Working Group (IMWG) recently published guidelines for prevent-ing VTE in myeloma.12 Primary data were lacking in many cases, so the IMWG recommendations are based on expert assessment or data extrapolation from studies not designed specifically to assess pro-phylaxis efficacy or safety. Therefore, they should not override the treating physician’s best judgment. Because VTE risk is frequently cumulative, patients
and an inflammatory milieu.5–8 Acquired resistance to activated protein C is a common coagulation ab-normality in MM, and it has also been associated with increased thromboembolism risk.5 Conditions that result in hypercoagulable states include immu-noglobulin interference with fibrin structure and paraprotein acting as an autoantibody against in-trinsic anticoagulants and phospholipids.9–11 A small recent study (N = 49) of patients with MM receiving thalidomide confirmed that most patients who sub-sequently experienced a thrombotic episode had an underlying hypercoagulability abnormality.7
Underlying VTE risk often escalates with thera-peutic intervention and is typically greatest after initial therapy. For example, approximately half of VTE events in patients with MM occur within 2 months of treatment initiation.5 Varying risk levels are associated with specific therapies and therapeutic combinations. In particular, VTE rates are high in patients receiving the immunomodulatory drugs tha-lidomide or lenalidomide in combination with high-dose dexamethasone, doxorubicin, or combination chemotherapy.12 Dexamethasone alone has also been shown to somewhat increase thrombosis risk.8,13,14
ThalidomideA recent systematic review and meta-analysis of 17 randomized, controlled trials found an overall VTE incidence of 11.7% in thalidomide-treated patients (95% CI, 8.1%–16.5%).15 This finding should be considered in the context of a systemic review by Zangari et al.,5 who assessed relapsed/refractory ver-sus newly diagnosed MM, as well as thalidomide monotherapy versus combination therapy, and found wide variation in VTE risk. Studies of thalidomide monotherapy showed VTE rates of less than 2% to 4% in both newly diagnosed patients and those with relapsed/refractory disease. Newly diagnosed patients receiving combination therapy had rates ranging from 17% to 28%. The rates of VTE in patients with relapsed/refractory MM who received combination thalidomide therapy tended to be lower (8% to 21%) but were still a cause for concern. The combination regimens evaluated included thalidomide/dexameth-asone, thalidomide/melphalan/prednisone, and tha-lidomide plus conventional chemotherapy.
LenalidomideAs with thalidomide, the risk for VTE with lenalido-mide is low, ranging from 0% to less than 5%, when it

Supplement
Complications of Multiple Myeloma Therapy
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-15
may present with a combination of disease-related and individual risk factors, as well as inherited and non-inherited risk factors. All of these must be considered alongside therapeutically mediated risk. Table 1 lists risk factors and related screening con-siderations for MM patients.2,12,26
According to the IMWG, selection of candidates for thromboprophylaxis should be based on the base-line VTE risk associated with each therapy.12 The IMWG recommends reducing VTE risk to less than 10% using the safest and least cumbersome prophy-laxis available. High-dose dexamethasone adminis-tration is considered an independent risk factor for VTE. At minimum, and coinciding with “black-box” warnings added recently to the prescribing informa-tion for thalidomide and lenalidomide, newly diag-nosed MM patients being treated with either of those drugs in combination with dexamethasone should receive thromboprophylaxis. Proposed prophylaxis strategies include the use of a low-molecular-weight heparin such as enoxaparin, warfarin, or aspirin. Clinical experience suggests that full-dose warfarin may be used as prophylaxis, but low-dose warfarin is not acceptable. Specific IMWG recommendations are summarized in Table 2.12
For patients receiving epoetin alfa, the FDA recommends administration of an anticoagulant prophylactic.27,28 The manufacturer of darbepoetin alfa does not recommend anticoagulant prophylaxis, but it specifies that the lowest dose needed should be used to reduce thromboembolism risk.29 The combi-nation of bortezomib with an ESA does not appear to increase the risk of VTE.30
Despite best efforts, prophylaxis cannot prevent all VTE incidents, and proper identification and management of VTE is critical. When DVT is sus-pected, the standard diagnostic test is compression ultrasonography. Suspected PE is typically investi-gated with imaging techniques, primarily CT pul-monary angiography. If this is contraindicated (due to baseline nephropathy, for example), magnetic resonance pulmonary angiography and/or nuclear medicine V/Q scan may be considered).12,31 In addi-tion, all patients should be provided with education regarding the clinical symptoms of VTE (i.e., skin redness, pain in the extremities or chest, shortness of breath, rapid heartbeat) and instructed to inform their physician promptly if any concerns arise. If DVT is confirmed, the overall goals of treatment are
symptomatic relief, prevention of emboli formation, and prevention of VTE recurrence.12 Proposed DVT treatment strategies are outlined in Figure 1.
Osteonecrosis of the JawA rare side effect recently documented in MM and other cancers, ONJ is linked to long-term use of bisphosphonates. The incidence of ONJ in bisphosphonate-treated MM patients is unknown. Manufacturer-sponsored epidemiologic studies re-
Table 1 Risk Factors to Consider When Screening Multiple Myeloma Patients for ThromboprophylaxisIndividual Factors
General patient characteristics
• Age
• Obesity and/or diabetes
• Cardiovascular or renal disease
• Acute infection
Inherited thrombophilic abnormalities
• Antithrombin III deficiencies
• Protein C and protein S deficiencies
• Acquired protein C resistance
• Factor V Leiden mutation
• Prothrombin gene (G20210A) mutation
• Elevated homocysteine levels
Central venous catheter use
Prior deep vein thrombosis, pulmonary embolism, or superficial vein thrombosis
Disease-Related Factors
Recent (< 3 mo) anesthesia, surgery, trauma, or hospital admission
Confinement (i.e., to a nursing home), immobilization, or sedentary lifestyle
Other malignant neoplasm, with or without chemotherapy
Hyperviscosity or other blood-clotting disorders
Neurologic disease with extremity paresis
Therapy-Related Factors
High-dose dexamethasone
Thalidomide, lenalidomide
Adjuvant doxorubicin for other cancer
Multiagent chemotherapies
Erythropoietin use
Data from Refs. 2, 12, and 26.

Supplement
Niesvizky and Badros
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-16
exposed bone in the jaw. The mandible is the main affected site, and most lesions occur posterior to the cuspid teeth.33,35,36
In a recent longitudinal study documenting the natural history of ONJ, 96 patients from the United States and Greece were followed up for 3.9 years af-ter ONJ diagnosis.35 Dental extractions preceded di-agnosis of ONJ in 47% of cases, and these procedures were more common in patients with a single episode of ONJ than in those with recurrent and nonhealing disease (58% vs. 30%). ONJ resolved in 62% of cases, recurred after healing in 12% (at the same or a new site) and did not resolve in 26% during 9 months of follow-up. The recurrence rate was higher among U.S. patients than Greek patients (22% vs. 7%, re-spectively). Discontinuation of bisphosphonate cor-related with increased bone pain in the Greek cohort and increased fracture rates in the U.S. cohort; U.S. patients were more likely to restart bisphosphonate than were their Greek counterparts. Recurrence of ONJ was precipitated by re-initiation of bisphospho-nate in 6 cases and dental treatment in 4 cases. The rate of MM relapse was higher in patients with recur-rent or unresolved ONJ than in those who experi-enced a single such episode.
Management of ONJ is controversial because there are so many unknowns. No evidence-based consensus guidelines exist. A cornerstone of man-agement is to attempt to prevent ONJ with good dental hygiene and avoidance of unnecessary den-tal procedures while on bisphosphonate therapy.
port an incidence ranging from 0.1% to 1.8%. By contrast, in independent epidemiologic reports from clinicians and the International Myeloma Founda-tion, the incidence estimates are higher, between 5% and 10%. In selected trials that focused on homog-enous MM patients, the incidence ranged between 3.2% and 10%. Although the pathogenesis of ONJ is not understood, indirect evidence suggests that it is multifactorial and is clearly linked to long-term bisphosphonate use. Based on the biologic activ-ity of bisphosphonates, ONJ is linked to adynamic bone, inhibition of angiogenesis, and microbial in-fections. ONJ typically occurs after dental proce-dures or local trauma, but it has also been shown to happen spontaneously.32,33
In the literature, the criteria used to diagnose ONJ have been inconsistent. Several associations and expert panels have provided consensus state-ments that include criteria for diagnosing ONJ; the details were recently reviewed.34 Bisphosphonate-related ONJ can be defined as an area of exposed bone in the maxillofacial region that has not healed within 8 weeks after identification by a health care provider in a patient who is receiving or has been ex-posed to a bisphosphonate without local evidence of malignancy and no prior radiotherapy to the affected region. Patients may present with pain or feelings of numbness or heaviness of the jaw. Other symptoms include soft-tissue swelling, loosening of teeth, and infection. In many cases, ONJ is asymptomatic and is detected by the examining physician, who finds an
Table 2 Recommendations for Thromboprophylaxis in Multiple Myeloma Patients Treated With Thalidomide or Lenalidomide• ≤ 1 VTE risk factor: aspirin (81–325 mg once daily)
• ≥ 2 risk factors: LMWH (equivalent to enoxaparin, 40 mg/d)
• LMWH is also recommended for all patients receiving thalidomide or lenalidomide plus high-dose dexamethasone or doxorubicin
• Barring contraindications in the front-line setting, treatment strategies using dexamethasone should use low-dose dexamethasone and include aspirin prophylaxis
• Full-dose warfarin (target INR 2–3) is an alternative to LMWH, although limited data exist to support this strategy
• Anticoagulant prophylaxis is recommended in patients with relapsed disease and a high risk for VTE
• It may be reasonable to deliver anticoagulant prophylaxis for 4 to 6 months; longer treatment periods may be considered in the presence of additional risk factors
• If VTE occurs in patients receiving thalidomide or lenalidomide, it is reasonable to briefly discontinue therapy and resume once proper anticoagulation has been established
Abbreviations: INR, International Normalized Ratio; LMWH, low molecular weight heparin; VTE, venous thromboembolism. Data from Palumbo A, Rajkumar SV, Dimopoulos MA, et al. Prevention of thalidomide- and lenalidomide-associated thrombosis in myeloma. Leukemia 2008;22:414–423.

Supplement
Complications of Multiple Myeloma Therapy
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-17
For patients who do develop ONJ, a conservative, “supportive,” nonsurgical approach has been rec-ommended: chlorhexidine 0.12% oral rinses, in-termittent systemic antibiotics, and careful seques-trectomy. Avoidance of bone curettage and surgical debridement is advised because most cases worsen after surgery. Ozone therapy, hyperbaric oxygen, and laser therapy have been used in several cases of ONJ, with mixed results.
In an effort to decrease the occurrence of ONJ, in 2007 ASCO updated its guidelines on the use of bisphosphonate in patients with MM.37 The guide-lines now recommend limiting the duration of bisphosphonate use to 2 years in patients with re-sponsive or stable MM, with drug resumption rec-ommended in the case of new-onset skeletal-related events. The guidelines also recommend that, before bisphosphonate initiation, patients should obtain a comprehensive dental examination, with particular attention to identifying active oral infections and sites at high risk for infection.
The incidence of ONJ may be lower in patients receiving 3-monthly bisphosphonate therapy versus monthly infusions;38 however, the data are prelimi-nary, and ongoing prospective clinical trials must be completed before such a schedule can be adopted.
Renal ComplicationsRenal impairment is common in patients with MM and may be present at diagnosis or a side effect of treatment. Bisphosphonates can cause renal func-tion deterioration in the form of tubular necrosis and focal segmental glomerulosclerosis. If renal impair-ment is secondary to bisphosphonate use, discontin-uation may lead to a partial recovery of function.39–41
The updated zoledronic acid prescribing infor-mation42 and the updated ASCO guidelines37 recom-mend a reduced dosage for patients with an estimated creatinine clearance between 30 and 60 mL/min. The dose should be administered over a period of no less than 15 minutes; administration time may be pro-longed for up to 30 minutes to decrease risk of renal toxicity.42 Zoledronic acid is not recommended for pa-tients with severe renal impairment (creatinine clear-ance < 30 mL/min). No dosing guidelines have been established for the use of pamidronate in patients with severe renal failure; however, ASCO recommends a reduced dosage.37 In general, bisphosphonates should
be used with extreme caution in MM patients with re-nal impairment, and all MM patients should be moni-tored for deterioration of kidney function.3
Monitoring of creatinine levels during MM treat-ment is strongly recommended, although no current guidelines have been validated. Dosing adjustments are necessary for patients who exhibit a change in kidney function.3 There is currently no standard def-inition of renal failure, but most recent studies have used a serum creatinine level of 2 mg/dL as a cutoff point. Another useful marker is glomerular filtration rate, which has been suggested to be a more accu-rate measurement of renal function, especially for patients with mild or moderate renal impairment.43
AnemiaAnemia may be present at the time of MM diagnosis, or it may develop subsequently. The most common trigger is the replacement of bone marrow by plasma cells, but anemia can also result from factors related to MM treatment, such as chemotherapy, radiation
Initiate therapy with LMWH*
Start oral anticoagulation within 24 hours (if concomitant thrombocytopenia risk is low)
Administer LMWH for a minimum of 5 days; do not stop treatment until INR is 2.0 to 3.0 for 2 consecutive days
Brie�y discontinue thalidomide or lenalidomide until full anticoagulation has been established
Optimal treatment duration is unknown; extended LMWH treatment should be considered based on cost-bene�t assessment
Optimal Dose, by LMWH Once Daily Twice DailyDeltaparin 200 U/kg 100 U/kgEnoxaparin 1.5 mg/kg 1 mg/kgNadroparin 171 U/kg 86 U/kg
Figure 1 Recommended approach to treatment of VTE in patients with multiple myeloma. Abbreviations: INR, international normalized ratio; LMWH, low-molecular-weight heparin; VTE, venous thromboembolism. *Treatment with unfractionated heparin is recommended for patients with renal failure.

Supplement
Niesvizky and Badros
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-18
the role and risk of ESAs in MM.All ESAs are contraindicated for patients with
uncontrolled hypertension.27–29 Revised FDA product labels for these drugs contain “black-box” warnings noting an increased risk of mortality, cardiovascular and thromboembolic events, and tumor progression or recurrence. In patients with renal failure, the FDA recommends individualized dosing with a goal of maintaining hemoglobin levels of 10 to 12 g/dL. In patients with cancer, ESAs are recommended for use only at the lowest doses and with concurrent chemo-therapy. They are not recommended when myelosup-pressive therapy is being used and a full recovery is expected.27–29 Based on these warnings, the NCCN recently released updated guidelines for the use of ESAs in cancer patients.52 The new guidelines elimi-nate hemoglobin level monitoring requirements and target hemoglobin ranges, reinforce the recommen-dation that only patients receiving chemotherapy should be treated with ESAs, and emphasize the risk for VTE with ESA administration.
For treatment with epoetin alfa, the FDA recom-mends administration of an anticoagulant prophylac-tic.27,28 Bortezomib combined with an ESA does not appear to be associated with increased VTE risk.30
ConclusionsThe identification over the past 10 years of new, more effective primary treatments for MM, such as bortezomib, lenalidomide, and thalidomide, has led to meaningful changes in patient outcomes. Howev-er, lenalidomide and thalidomide, used either alone or in combination, are associated with elevated VTE risk. Likewise, the treatment of MM-associated bony disease with bisphosphonate therapy provides clini-cal benefit but increases the risk for ONJ and renal impairment. Patients receiving MM therapy are also at heightened risk of anemia. The application of preventive measures, such as VTE prophylaxis, ap-propriate dental hygiene, and dose adjustments, can contribute to improved outcomes and quality of life for MM patients.
AcknowledgmentThe authors thank Caitlin Rothermel, MA, for med-ical writing assistance.
therapy, and B12 and folate deficiencies.44 Anemia often resolves when treatment for MM is swift and successful, but it will remain if the disease worsens.
Although anemia can be related to inadequate erythropoietin production,45 before initiating treat-ment, physicians should assess other possible causes. In particular, iron deficiency may be overlooked due to macrocytosis related to the treatment of MM.46 Patients with inadequate erythropoietin production may benefit from treatment with ESAs that mimic erythropoietin to stimulate red blood cell produc-tion.27–29 Treatment of anemia with ESAs has been successful in patients with a variety of cancer types, including MM.44 Studies specific to myeloma and lymphoma have shown improvement (response rates of 50%–70%) in anemia-related outcomes, such as quality of life, hemoglobin levels, and num-ber of required transfusions.45,47,48 If ESA use is not effective, the most likely causes are functional iron deficiency, infection, surgery, or plasma-cell bone marrow dysfunction.44
Unfortunately, recent evidence suggests that ESAs may contribute to solid tumor proliferation, thus reducing life expectancy. This was first noted in patients with breast or head and neck carcinoma.49 Research on ESA use in patients with MM has pro-duced conflicting results. In a retrospective analysis, Baz et al.50 identified a trend toward increased overall survival. A hazard ratio of 0.6 (P = .026; 95% CI, 0.38–0.94) was identified for all patients except those with stage 1 disease, as defined by the Southwest On-cology Group staging system. No effect was found for patients with stage 1 disease.50 However, another ret-rospective analysis conducted by Katodrikou et al.51 found that ESAs might have a detrimental effect on both median overall survival and progression-free survival in patients with MM. Median overall sur-vival was 31 months (95% CI, 25–37 months) for patients receiving ESAs and 67 months (95% CI, 55–79 months) for those not receiving ESAs. Me-dian progression-free survival was 14 months (95% CI, 12–16 months) for patients who received ESAs and 30 months (95% CI, 24–36 months) for patients who did not (P < .001 for both comparisons). The au-thors concluded that their results do not contravene the therapeutic value of ESAs but might indicate that their administration should be limited to MM patients in whom a good response can be predicted.51 A randomized, prospective trial is needed to clarify

Supplement
Complications of Multiple Myeloma Therapy
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-19
References 1. Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous
thromboembolism: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). Chest 2008;133(Suppl 6):S381–S453.
2. Heit JA, Silverstein MD, Mohr DN, et al. Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Intern Med 2000;160:809–815.
3. Anderson KC, Alsina M, Bensinger W, et al. NCCN clinical practice guidelines in oncology: multiple myeloma, v 2.2010. Available at www.NCCN.org. Accessed August 12, 2009.
4. Brandenburg NA, Goss TF, Knight T, et al. Evaluation of the relationship between venous thromboembolism risk factors and the use of antithrombotic prophylaxis in multiple myeloma patients treated with thalidomide and dexamethasone combination regimens [abstract]. Blood 2008;112:Abstract 2369.
5. Zangari M, Elice F, Fink L, Tricot G. Thrombosis in multiple myeloma. Expert Rev Anticancer Ther 2007;7:307–315.
6. Rickles FR, Patierno S, Fernandez PM. Tissue factor, thrombin, and cancer. Chest 2003;124(Suppl 3):S58–S68.
7. Talamo GP, Ibrahim S, Claxton D, et al. Hypercoagulable states in patients with multiple myeloma can affect the thalidomide-associated venous thromboembolism. Blood Coagul Fibrinolysis 2009;20:337–339.
8. Niesvizky R, Martinez-Banos D, Jalbrzikowski J, et al. Prophylactic low-dose aspirin is effective antithrombotic therapy for combination treatments of thalidomide or lenalidomide in myeloma. Leuk Lymphoma 2007;48:2330–2337.
9. Coleman M, Vigliano EM, Weksler ME, Nachman RL. Inhibition of fibrin monomer polymerization by lambda myeloma globulins. Blood 1972;39:210–223.
10. Spicka I, Rihova Z, Kvasnicka J, et al. Disturbances of anticoagulation and fibrinolytic systems in monoclonal gammopathies—another mechanism of M-protein interference with hemostasis. Thromb Res 2003;112:297–300.
11. Zangari M, Saghafifar F, Mehta P, et al. The blood coagulation mechanism in multiple myeloma. Semin Thromb Hemost 2003;29:275–282.
12. Palumbo A, Rajkumar SV, Dimopoulos MA, et al. Prevention of thalidomide- and lenalidomide-associated thrombosis in myeloma. Leukemia 2008;22:414–423.
13. Rajkumar SV, Rosinol L, Hussein M, et al. Multicenter, randomized, double-blind, placebo-controlled study of thalidomide plus dexamethasone compared with dexamethasone as initial therapy for newly diagnosed multiple myeloma. J Clin Oncol 2008;26:2171–2177.
14. Weber DM, Chen C, Niesvizky R, et al. Lenalidomide plus dexamethasone for relapsed multiple myeloma in North America. N Engl J Med 2007;357:2133–2142.
15. Gray KN, Chu D, Wu S, Lin RZ. Risk of venous thromboembolism with thalidomide in cancer patients: a systematic review and meta-analysis of randomized controlled trials [abstract]. Blood 2008;112:Abstract 3820.
16. Bennett CL, Angelotta C, Yarnold PR, et al. Thalidomide- and lenalidomide-associated thromboembolism among patients with cancer. JAMA 2006;296:2558–2560.
17. Sharma RA, Steward WP, Daines CA, et al. Toxicity profile of the immunomodulatory thalidomide analogue, lenalidomide: phase I clinical trial of three dosing schedules in patients with solid malignancies. Eur J Cancer 2006;42:2318–2325.
18. Niesvizky R, Jayabalan DS, Christos PJ, et al. BiRD (Biaxin [clarithromycin]/Revlimid [lenalidomide]/dexamethasone) combination therapy results in high complete- and overall-response rates in treatment-naive symptomatic multiple myeloma. Blood 2008;111:1101–1109.
19. Dimopoulos M, Spencer A, Attal M, et al. Lenalidomide plus dexamethasone for relapsed or refractory multiple myeloma. N Engl J Med 2007;357:2123–2132.
20. Boen M, McKoy J, West D, et al. Thalidomide (thal), lenalidomide (len), and dexamethasone (dex)-associated venous thromboembolism (VTE) and reported VTE rates pre- and post-FDA approval: optimal prophylaxis strategies are still unclear [abstract]. Blood 2008;112:Abstract 2403.
21. Jacobus S, Kumar S, Callander NS, et al. Effect of venous thrombotic events on overall survival in multiple myeloma: analysis of thrombotic events occurring in E4A03A randomized trial of lenalidomide plus high-dose dexamethasone (RD) versus lenalidomide plus low-dose dexamethasone (Rd) in newly diagnosed multiple myeloma, a trial coordinated by the Eastern Cooperative Oncology Group (ECOG) [abstract]. Blood 2008;112: Abstract 1740.
22. Zangari M, Guerrero J, Cavallo F, et al. Hemostatic effects of bortezomib treatment in patients with relapsed or refractory multiple myeloma. Haematologica 2008;93:953–954.
23. Richardson PG, Sonneveld P, Schuster MW, et al. Bortezomib or high-dose dexamethasone for relapsed multiple myeloma. N Engl J Med 2005;352:2487–2498.
24. San Miguel JF, Schlag R, Khuageva NK, et al. Bortezomib plus melphalan and prednisone for initial treatment of multiple myeloma. N Engl J Med 2008;359:906–917.
25. Heit JA, Silverstein MD, Mohr DN, et al. Predictors of survival after deep vein thrombosis and pulmonary embolism: a population-based, cohort study. Arch Intern Med 1999;159:445–453.
26. Bauer KA. The thrombophilias: well-defined risk factors with uncertain therapeutic implications [editorial]. Ann Intern Med 2001;135:367–373.
27. Epogen (epoetin alfa) for injection [package insert]. Thousand Oaks, CA: Amgen, Inc.; 2009.
28. Procrit (epoetin alfa) for injection [package insert]. Raritan, NJ: Ortho Biotech Products, L.P., 2009.
29. Aranesp (darbepoetin alfa) [package insert]. Thousand Oaks, CA: Amgen, Inc.; 2008.
30. Lonial S, Richardson PG, San Miguel J, et al. Characterisation of haematological profiles and low risk of thromboembolic events with bortezomib in patients with relapsed multiple myeloma. Br J Haematol 2008;143:222–229.
31. Bozlar U, Gaughen JR, Nambiar AP, Hagspiel KD. Imaging diagnosis of acute pulmonary embolism. Expert Rev Cardiovasc Ther 2007;5:519–529.
32. Badros A, Weikel D, Salama A, et al. Osteonecrosis of the jaw in multiple myeloma patients: clinical features and risk factors. J Clin Oncol 2006;24:945–952.
33. Migliorati CA, Casiglia J, Epstein J, et al. Managing the care of patients with bisphosphonate-associated osteonecrosis: an American Academy of Oral Medicine position paper. J Am Dent Assoc 2005;136:1658–1668.
34. Silverman SL, Landesberg R. Osteonecrosis of the jaw and the role of bisphosphonates: a critical review. Am J Med 2009;122(2 Suppl):S33–S45.

Supplement
Niesvizky and Badros
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-20
35. Badros A, Terpos E, Katodritou E, et al. Natural history of osteonecrosis of the jaw in patients with multiple myeloma. J Clin Oncol 2008;26:5904–5909.
36. Mehrotra B, Ruggiero S. Bisphosphonate complications including osteonecrosis of the jaw. Hematology Am Soc Hematol Educ Program 2006:356–360, 515.
37. Kyle RA, Yee GC, Somerfield MR, et al. American Society of Clinical Oncology 2007 clinical practice guideline update on the role of bisphosphonates in multiple myeloma. J Clin Oncol 2007;25:2464–2472.
38. Corso A, Varettoni M, Zappasodi P, et al. A different schedule of zoledronic acid can reduce the risk of the osteonecrosis of the jaw in patients with multiple myeloma. Leukemia 2007;21:1545–1548.
39. Desikan R, Veksler Y, Raza S, et al. Nephrotic proteinuria associated with high-dose pamidronate in multiple myeloma. Br J Haematol 2002;119:496–499.
40. Markowitz GS, Fine PL, Stack JI, et al. Toxic acute tubular necrosis following treatment with zoledronate (Zometa). Kidney Int 2003;64:281–289.
41. Markowitz GS, Perazella MA. Drug-induced renal failure: a focus on tubulointerstitial disease. Clin Chim Acta 2005;351:31–47.
42. Zometa (zoledronic acid) injection [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp.; 2008.
43. Dimopoulos MA, Kastritis E, Rosinol L, et al. Pathogenesis and treatment of renal failure in multiple myeloma. Leukemia 2008;22:1485–1493.
44. Blade J, Rosinol L. Complications of multiple myeloma. Hematol Oncol Clin North Am 2007;21:1231–1246.
45. Mittelman M. The implications of anemia in multiple myeloma. Clin Lymphoma 2003;4(Suppl 1):S23–S29.
46. Ludwig H, Rai K, Blade J, et al. Management of disease-related anemia in patients with multiple myeloma or chronic lymphocytic leukemia: epoetin treatment recommendations. Hematol J 2002;3:121–130.
47. Birgegard G. Managing anemia in lymphoma and multiple myeloma. Ther Clin Risk Manag 2008;4:527–539.
48. Seidenfeld J, Piper M, Flamm C, et al. Epoetin treatment of anemia associated with cancer therapy: a systematic review and meta-analysis of controlled clinical trials. J Natl Cancer Inst 2001;93:1204–1214.
49. Lyman GH, Glaspy J. Are there clinical benefits with early erythropoietic intervention for chemotherapy-induced anemia? A systematic review. Cancer 2006;106:223–233.
50. Baz R, Walker E, Choueiri TK, et al. Recombinant human erythropoietin is associated with increased overall survival in patients with multiple myeloma. Acta Haematol 2007;117:162–167.
51. Katodritou E, Verrou E, Hadjiaggelidou C, et al. Erythropoiesis-stimulating agents are associated with reduced survival in patients with multiple myeloma. Am J Hematol 2008;83:697–701.
52. Rogers GM, Becker PS, Bennett CL, et al. NCCN clinical practice guidelines in oncology: cancer- and chemotherapy-induced anemia, v 1.2009. Available at www.NCCN.org. Accessed August 12, 2009.

Supplement
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-21
Key WordsAutologous stem cell transplantation, interferon, thalidomide, bortezomib, lenalidomide
AbstractMaintenance therapy in multiple myeloma has been under in-vestigation for more than 3 decades, without evidence of clear benefit until recently. Chemotherapy maintenance offers no ben-efit after conventional or high-dose treatment. Interferon-based maintenance is associated with minimal improvements in clinical outcomes, but is poorly tolerated. Results of corticosteroid main-tenance studies have been conflicting; at least one randomized trial showed improved survival with prednisone maintenance after conventional chemotherapy. The role of the novel agents thalido-mide, lenalidomide, and bortezomib as maintenance is emerging. Most reported maintenance studies have evaluated thalidomide, alone or in combination with a corticosteroid. Several of these studies suggest that thalidomide-based maintenance prolongs overall survival after autologous stem cell transplantation. Impor-tant questions that have not yet been resolved include the op-timal dose and duration of thalidomide, whether clinical benefit depends on response to induction therapy and risk for relapse, and whether reported benefits are caused by cytoreduction or eradi-cation of minimal residual disease, especially with bortezomib maintenance. Ongoing randomized trials are evaluating lenalido-mide and bortezomib maintenance therapies to better define the role of these drugs as maintenance in multiple myeloma. (JNCCN 2010;8[Suppl 1]:S21–S27)
er, maintenance therapy practice patterns vary consid-erably because of conflicting data about its effectiveness. Currently, NCCN recommends thalidomide (category 1 recommendation) with or without prednisone (cat-egory 2B) for maintenance therapy; the roles of inter-feron and corticosteroids are less clear (category 2B).2 This article summarizes the results of many clinical tri-als that have been designed to evaluate maintenance af-ter conventional chemotherapy and high-dose therapy and identifies areas of current controversy in an effort to understand the role of maintenance therapy in manag-ing patients with newly diagnosed MM.
Maintenance After Conventional ChemotherapyBecause of the increased risk for acute myeloid leukemia with prolonged alkylating agent therapy, alternatives to this approach were being sought as early as the 1980s. Interferon-alpha was the subject of numerous trials that produced inconclusive results. Two meta-analyses, one performed using individual patient data and the other using published data, found a small but statistically sig-nificant survival benefit when interferon maintenance was used after conventional therapy.3,4 However, few patients can tolerate the substantial toxicities of inter-feron therapy, and therefore interferon maintenance is rarely used.
Several studies have evaluated corticosteroids, with or without interferon, as maintenance, but the data are insufficient to draw firm conclusions. When compared directly with interferon maintenance, dexamethasone, 20 mg/m2, given orally on days 1 to 4 of a 28-day cycle produced a similar median duration of remission, but significantly fewer patients treated with dexamethasone maintenance responded to repeat melphalan/dexa-methasone at relapse relative to those treated with in-
Maintenance therapy in multiple myeloma (MM) comprises any therapy given “following completion of induction treatment in responding or nonprogressing patients, with the goal of prolonging survival.”1 Howev-
From the Bone Marrow Transplant Program, Greenebaum Cancer Center, University of Maryland, Baltimore, Maryland.This work was supported by an educational grant from Millennium Pharmaceuticals, Inc.Correspondence: Ashraf Z. Badros, MD, University of Maryland, Greenebaum Cancer Center, Bone Marrow Transplant Program, 22 South Greene Street, Baltimore, MD 21201. E-mail: [email protected]
The Role of Maintenance Therapy in the Treatment of Multiple Myeloma
Ashraf Z. Badros, MD, Baltimore, Maryland

Supplement
Badros
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
22
Data on bortezomib-based maintenance strate-gies are beginning to emerge. A randomized phase III trial conducted by the Italian Multiple Myeloma Group is comparing bortezomib/melphalan/predni-sone/thalidomide (VMPT) induction followed by bortezomib/thalidomide maintenance to bortezo-mib/melphalan/prednisone (VMP) induction with-out maintenance in elderly patients with newly di-agnosed myeloma.11 Results presented at the 2008 American Society of Hematology Annual Meeting showed a higher response rate for VMPT relative to VMP (complete response [CR] rate, 31% vs. 16%; P = .003; very good partial response [VGPR] rate, 55% vs. 42%; P = .02) but no difference in OS at 3 years.
Maintenance After Autologous Stem Cell Transplantation
Chemotherapy and Interferon Maintenance After Autologous Stem Cell TransplantationAs with conventional induction regimens, chemo-therapy is not currently recommended as a mainte-nance strategy after autologous stem cell transplan-tation (ASCT).2 Interferon is currently considered a maintenance option in the NCCN Clinical Practice Guidelines in Oncology for Multiple Myeloma (to view the most recent version of these guidelines, vis-it the NCCN Web site at www.NCCN.org), based on low-level evidence and non-uniform NCCN consensus (category 2B).2 However, given the lack of clear activity and substantial toxicity associated with interferon and the availability of new agents, research into interferon maintenance has been largely abandoned.
Novel Agents After ASCTThalidomide is the best studied of the novel agents in the post-ASCT maintenance setting, although randomized clinical trials of bortezomib and lenalid-omide are underway (Table 1).12 Four randomized phase III trials have been completed to establish the role of thalidomide-based maintenance after ASCT (Table 2).13–16 In all 4 studies, improvements in re-sponse (CR) and PFS were seen. Of the 4 trials, 3 also reported significant improvements in OS, and a meta-analysis of these data showed a trend toward improved survival with maintenance thalidomide after ASCT (Figure 1).17 When the trial that in-
terferon maintenance (44% vs. 82%; P = .001).5 In the MY.7 study by the National Cancer Institute of Canada (NCIC), dexamethasone maintenance im-proved median progression-free survival (PFS) based on a hazard ratio (HR) of 0.61 (95% CI, 0.47–0.79), but not overall survival (OS; HR, 0.88; 95% CI, 0.65–1.18), relative to no maintenance.6 Similarly, when added to interferon, thrice-weekly prednisone, 50 mg, improved median PFS but not overall surviv-al (OS), relative to interferon alone in the SWOG 9028 trial.7
Only one trial, SWOG 9210, has shown a sur-vival benefit with corticosteroid maintenance thera-py.8 In this randomized trial, a prednisone regimen of 50 mg every other day significantly improved median PFS (14 vs. 5 months; P = .003) and OS (37 vs. 26 months; P = .05) relative to a physiologic dose regi-men (10 mg every other day). These data support the use of steroids in this setting, although the efficacy of the SWOG 9210 regimen has not been confirmed in another controlled clinical trial.
Recently, several trials have focused on the role of novel agents as maintenance therapy. Offi-dani et al.9 conducted a randomized comparison of maintenance with either thalidomide (100 mg/d) plus dexamethasone (20 mg/d for 4 days per month) or interferon thrice weekly plus dexamethasone in 103 patients who experienced response to induction therapy with ThaDD (thalidomide, dexamethasone, and pegylated liposomal doxorubicin). Both 2-year PFS and OS rates were significantly better with thalidomide-based maintenance (PFS, 63% vs. 32%; P = .024; OS, 84% vs. 68%; P = .030). The low-dose thalidomide regimen was generally well-tolerated, with peripheral neuropathy (6%) and constipation (4%) the most commonly reported grade 3/4 toxici-ties. More patients were compliant with thalidomide therapy long-term relative to interferon.
Preliminary data have been reported for mainte-nance therapy in elderly patients who experienced stable disease or better with thalidomide/dexameth-asone or melphalan/prednisone induction.10 A total of 111 patients with nonprogressive disease were randomized to maintenance with thalidomide, 100 mg daily, with thrice-weekly interferon or interferon alone. At a median follow-up of 17.2 months, me-dian survival from the start of maintenance was 53.1 months in the thalidomide/interferon arm and not yet reached in the interferon-alone arm (P = .49).

Supplement
Maintenance Therapy in Multiple Myeloma
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
23
cluded thalidomide during induction was excluded, the OS benefit became significant (HR, 0.49; 95% CI, 0.32–0.74).17 Peripheral neuropathy complicated the treatment course in all 4 studies, and, unsurpris-ingly, the incidence was highest when the duration of thalidomide maintenance was prolonged. None of the studies, however, determined the optimal dose or duration of thalidomide-based maintenance after ASCT.
A recent update to one of the trials, conducted at a median follow-up of 6 years, suggests that tha-lidomide may benefit patients with high-risk myelo-ma.18 The estimated OS rate at 5 years was 56% for patients with cytogenetic abnormalities treated with thalidomide versus 43% for those with cytogenetic
abnormalities in the control group (P = .02).Results from other randomized trials of thalido-
mide maintenance were presented at national meet-ings within the past year, none of which supports an improvement in OS. The United Kingdom Medical Research Council (MRC) Myeloma IX study evalu-ated thalidomide maintenance after primary treat-ment of myeloma (either ASCT or conventional chemotherapy, depending on the clinical situa-tion).19 A total of 820 patients were randomly as-signed to thalidomide maintenance (100 mg/d until relapse) or no maintenance, making this the largest trial conducted. Overall, PFS was numerically higher in the thalidomide arm, but the improvement was statistically significant only among patients who ex-
Table 1 Ongoing Randomized Phase III Trials of Maintenance Therapy After ASCT in Patients With Newly Diagnosed Multiple Myeloma
Clinical Trial and Accrual Goal Primary Treatment Maintenance Regimen(s)Primary End Point
NCIC MY.10 (N = 324) [NCT00049673]
ASCT •Thalidomide daily with alternate-day prednisone
•ObservationMaintenance × 4 y
OS
NHLBI/ BMTCTN0102 (N = 710) [NCT00075829]
Tandem transplantation (no HLA-matched sibling) or ASCT followed by mini-allogeneic SCT (HLA-matched sibling)
•Thalidomide/dexamethasone•ObservationMaintenance × 1 y; only administered to patients undergoing tandem transplantation
3-y PFS
CALGB 100104 (N = 462) [NCT00114101]
ASCT •Lenalidomide •PlaceboMaintenance continues as tolerated or until progression; only administered to patients with stable or responding disease after ASCT
TTP
IFM 2005-02 (N = 614) [NCT00430365]
ASCT •Lenalidomide•PlaceboDuration not specified
Duration of post-ASCT response
Gesellschaft für Medizinische Innovation (N = 194) [NCT00891384]
ASCT
Consolidation: lenalidomide, 25 mg, days 1–21 q4w × 6
•Lenalidomide, 5 mg, days 1–21 q4w•Lenalidomide, 25 mg/d, days 1–21 q4wMaintenance continues until disease progression
EFS
HOVON-65/GMMG-HD4 (N = 825)12
Induction: VAD vs. PAD Stem cell collection: CAD ASCT: HDM
•Thalidomide 50 mg/d•Bortezomib 1.3 mg/m2 q2wMaintenance × 2 y
PFS
PETHEMA GEM05 (N = 390) [NCT00461747]
Induction: VBMCP-VBAD-bortezomib vs. TD vs. VTD followed by ASCT
•Interferon•Thalidomide•Thalidomide plus bortezomibMaintenance × 3 y
Not stated
Abbreviations: ASCT, autologous stem cell transplantation; CAD, cyclophosphamide/doxorubicin/dexamethasone; EFS, event-free survival; HDM, high-dose melphalan; HLA, histocompatibility leukocyte antigen; OS, overall survival; PAD, bortezomib/doxorubicin/dexamethasone; PFS, progression-free survival; SCT, stem cell transplantation; TD, thalidomide/dexamethasone; TTP, time-to-progression; VAD, vincristine/doxorubicin/dexamethasone; VBMCP-VBAD, vincristine/carmustine/melphalan/cyclophosphamide/prednisone alternating with vincristine/carmustine/doxorubicin/dexamethasone; VTD, bortezomib/thalidomide/dexamethasone.

Supplement
Badros
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
24
salvage therapy. Two large studies have reported that the survival benefits with thalidomide were limited to patients who did not experience at least a VGPR, supporting the hypothesis that post-transplantation thalidomide provides additional cytoreduction rath-er than eradication or suppression of minimal re-sidual disease. Currently, however, initial response to therapy should not be used to guide maintenance treatment decisions.
Furthermore, the optimal dose and duration of maintenance thalidomide remains to be determined. The incidence of neuropathy is clearly cumulative and dose-related, partly leading to the recommenda-tion that thalidomide not be used throughout the en-tire treatment course. Doses of 200 mg daily or more are difficult to administer on a long-term basis.22,23 Lower-dose (100 mg/d) and time-limited therapy (6–12 months) were efficacious in studies by the Tu-nisian Multiple Myeloma Study Group (TMMSG) and Australasian Leukaemia and Lymphoma Group (ALLG), but the United Kingdom MRC Myeloma IX study did not show a survival benefit with a 100-mg daily thalidomide maintenance regimen.
Another intriguing issue is whether patients who begin maintenance treatment with less than a VGPR should discontinue therapy once they experi-ence VGPR or CR, given that those with VGPR/CR before maintenance therapy did not seem to benefit from additional therapy in some trials. The NCCN
perienced less than a VGPR with induction therapy (HR, 1.9; P = .007). OS was not significantly im-proved in any subgroup. Moreover, subgroup analy-ses showed that patients with 17p deletions had a significantly worse OS when treated with thalido-mide maintenance (HR, 4.55; P = .02), leading the researchers to conclude that 17p deletion is a contra-indication to thalidomide maintenance.
Two small studies presented at the XII Inter-national Myeloma Workshop in 2009 showed sig-nificant improvements in PFS, but not OS, with thalidomide-based maintenance. Mounier et al.20 compared an intermittent dexamethasone/thalido-mide maintenance regimen with no maintenance after ASCT in 108 patients and observed median event-free survival of 32 versus 17 months, respec-tively (P = .02). Maiolino et al.21 compared dexa-methasone maintenance with dexamethasone plus thalidomide, 200 mg daily, after ASCT in 212 pa-tients. Thalidomide significantly reduced the risk for progression relative to dexamethasone alone (HR, 2.43; P = .03), but OS was similar in the 2 arms (65% vs. 74% with dexamethasone and dexamethasone/thalidomide, respectively).
Therefore, although data support a role for thalidomide-based maintenance therapy after ASCT, several important questions remain, such as whether thalidomide given post-transplantation truly maintains response versus early initiation of
A
B
Studyor Sub-Category Log[HR] (SE)
HR (Random)95% Cl
HR (Random)95% Cl
Studyor Sub-Category Log[HR] (SE)
HR (Random)95% Cl
HR (Random)95% Cl
Barlogie13 2006 Attal14 2006 Spencer25 2006 Abdelke�15 2007
Total (95% CI) Test for heterogeneity: Chi² = 12.93, df = 3 (P = .005), I² = 76.8% Test for overall effect: Z = 1.93 (P = 0.05)
Barlogie13 2006 Spencer25 2006 Abdelke�15 2007
Total (95% CI) Test for heterogeneity: Chi² = 3.01, df = 2 (P = .22), I² = 33.6% Test for overall effect: Z = 3.38 (P = .0007)
Favors Thalidomide Favors Control
Favors Thalidomide Favors Control
0.20.1 0.5 1 2 5 10
0.20.1 0.5 1 2 5 10
0.98 [0.74, 1.30]0.56 [0.36, 0.86]0.32 [0.17, 0.58]0.69 [0.31, 1.54]
0.61 [0.37, 1.01]
-0.0182 (0.1451) -0.5805 (0.2207) -1.1476 (0.3086) -0.3757 (0.4126)
-0.5805 (0.2207)-1.1476 (0.3086)-0.3757 (0.4126)
0.56 [0.36, 0.86]0.32 [0.17, 0.58]0.69 [0.31, 1.54]
0.49 [0.32, 0.74]
Figure 1 Overall survival with maintenance thalidomide. (A) All trials. (B) Excluding Barlogie 2006.Abbreviations: HR, hazard ratio; OS, overall survival; SE, standard error. Adapted from Hicks LK, Haynes AE, Reece DE, et al. A meta-analysis and systematic review of thalidomide for patients with previ-ously untreated multiple myeloma. Cancer Treat Rev 2008;34:442–452, with permission from Elsevier.

Supplement
Maintenance Therapy in Multiple Myeloma
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
25
Tab
le 2
Pu
blis
hed
Ran
do
miz
ed T
rial
s o
f Th
alid
om
ide-
bas
ed M
ain
ten
ance
Th
erap
y A
fter
ASC
TSt
ud
yR
egim
ens
Thal
ido
mid
e R
egim
enEf
fica
cySa
fety
TT213
New
ly d
iag
no
sed
p
rog
ress
ive
or
sym
pto
mat
ic M
M,
≤ 75
y (
N =
668
)
Ind
uct
ion
: 4 c
ycle
s o
f ch
emo
ther
apy,
wit
h o
r w
ith
ou
t th
alid
om
ide
ASC
T: t
and
em t
ran
spla
nta
tio
n w
ith
mel
ph
alan
-bas
ed
pre
par
ativ
e re
gim
ens,
wit
h o
r w
ith
ou
t th
alid
om
ide
Co
nso
lidat
ion
: ran
do
miz
ed t
o 1
of
3 re
gim
ens,
wit
h
or
wit
ho
ut
thal
ido
mid
e M
ain
ten
ance
: IFN
tid
; wit
h o
r w
ith
ou
t th
alid
om
ide;
cy
cles
of
dex
amet
has
on
e, 4
0 m
g, g
iven
on
day
s 1–
4,
9–12
, 17–
20 q
3mo
fo
r 4
cycl
es, fi
rst
year
on
ly
Ind
uct
ion
: 400
mg
/d
ASC
T: 1
00 m
g/d
, in
itia
ted
af
ter
pla
tele
t re
cove
ry
Co
nso
lidat
ion
: 200
mg
/d
Mai
nte
nan
ce: 1
00 m
g/d
fo
r th
e fi
rst
year
an
d
50 m
g/d
th
erea
fter
Thal
ido
mid
e vs
. o
bse
rvat
ion
: C
R: 6
2% v
s. 4
3% ;
P <
.001
5-y
EFS:
56%
vs.
44%
; P
= .0
1M
ST a
fter
rel
apse
: 1.1
vs.
2.
7 y;
P =
.001
> G
rad
e 2
AEs
, th
alid
om
ide
vs.
ob
serv
atio
n:
Thro
mb
osi
s/em
bo
lism
: 30%
vs.
17
%; P
< .0
01PN
: 27%
vs.
17%
; P <
.001
Bo
wel
ob
stru
ctio
n: 1
4% v
s. 8
%;
P =
.02
Trem
or:
13%
vs.
6%
; P =
.003
Syn
cop
e: 1
2% v
s. 4
%; P
< .0
01
IFM
99-
0214
MM
wit
ho
ut
or
wit
h o
ne
adve
rse
pro
gn
ost
ic f
acto
r, <
65
y (N
= 7
08)
Ind
uct
ion
: VA
D ×
3–4
cyc
les
ASC
T: t
and
em t
ran
spla
nta
tio
n w
ith
mel
ph
alan
-bas
ed
pre
par
ativ
e re
gim
ens
Ran
do
miz
atio
n t
o m
ain
ten
ance
wit
h:
A)
no
mai
nte
nan
ce
B)
pam
idro
nat
e, 9
0 m
g, I
V q
4w u
nti
l pro
gre
ssio
n
C)
pam
idro
nat
e p
lus
thal
ido
mid
e
Mai
nte
nan
ce a
rm C
re
ceiv
ed t
hal
ido
mid
e,
400
mg
/d, w
ith
red
uct
ion
to
min
imu
m o
f 50
mg
/d
allo
wed
fo
r to
xici
ty;
thal
ido
mid
e g
iven
un
til
dis
ease
pro
gre
ssio
n
Arm
s A
vs.
B v
s. C
: B
est
resp
on
se a
fter
ra
nd
om
izat
ion
(P
= .0
01):
CR
/VG
PR: 5
5% v
s. 5
7% v
s.
67%
PR
: 37%
vs.
37%
vs.
30%
M
R: 7
.5%
vs.
5.5
% v
s. 3
%
3-y
pro
bab
ility
of
EFS:
36
% v
s. 3
7% v
s. 5
2%;
P <
.009
4-y
pro
bab
ility
of
OS:
77%
vs
. 74%
vs.
87%
; P <
.04
Gra
de
3/4
AEs
, arm
A v
s. B
vs.
C:
PN: 1
% v
s. 2
% v
s. 7
%; P
< .0
01Fa
tig
ue:
1%
vs.
2%
vs.
6%
; P
< .0
01C
on
stip
atio
n: 0
% v
s. 0
% v
s. 1
%;
P <
.001
Neu
tro
pen
ia: 0
% v
s. 1
% v
s. 6
%;
P =
.001
Car
dia
c: 0
% v
s. 0
% v
s. 1
%; P
= .0
4
TMM
SG15
Stag
e II/
III D
uri
e-Sa
lmo
n M
M,
< 6
0 y
(N =
202
)
Ind
uct
ion
: th
alid
om
ide
wit
h in
term
itte
nt
dex
amet
has
on
e A
SCT:
cyc
lop
ho
sph
amid
e/G
CSF
fo
r st
em c
ell
colle
ctio
n
Ran
do
miz
atio
n:
A)
Tan
dem
tra
nsp
lan
tati
on
wit
h m
elp
hal
an-
bas
ed p
rep
arat
ive
reg
imen
s; t
hal
ido
mid
e g
iven
at
pro
gre
ssio
n o
r re
lap
se
B)
Sin
gle
tra
nsp
lan
tati
on
wit
h m
elp
hal
an-
bas
ed p
rep
arat
ive
reg
imen
, wit
h t
hal
ido
mid
e m
ain
ten
ance
; sec
on
d A
SCT
at p
rog
ress
ion
or
rela
pse
Ind
uct
ion
: 200
mg
/d f
or
75 d
Ta
nd
em t
ran
spla
nta
tio
n:
salv
age
thal
ido
mid
e, 2
00
mg
/d
Sin
gle
tra
nsp
lan
tati
on
ar
m: 1
00 m
g/d
init
iate
d
3 m
o p
ost
-ASC
T an
d
con
tin
ued
fo
r 6
mo
Arm
A v
s. B
: C
R/V
GPR
:* 5
4% v
s. 6
8%;
P =
.04
PR:*
39%
vs.
27%
; P =
NS
MR
:* 3
% v
s. 3
% ;
P =
NS
3-y
PFS:
57%
vs.
85%
; P
= .0
23-
y O
S: 6
5% v
s. 8
5%;
P =
.04
Gra
de 3
/4 A
Es, s
alva
ge t
halid
omid
e (a
rm A
) vs.
mai
nten
ance
th
alid
omid
e (a
rm B
): PN
: 11%
vs.
4%
Fa
tig
ue:
6%
vs.
3%
C
on
stip
atio
n: 6
% v
s. 1
%
Infe
ctio
n: 0
% v
s. 1
%
ALL
G M
M616
New
ly d
iag
no
sed
, sy
mp
tom
atic
MM
, ≤
70 y
(N
= 2
69)
ASC
T: S
ing
le t
ran
spla
nta
tio
n w
ith
mel
ph
alan
-bas
ed
pre
par
ativ
e re
gim
en
Ran
do
miz
atio
n t
o:
A)
Pred
nis
olo
ne,
50
mg
, eve
ry o
ther
day
B
) Pr
edn
iso
lon
e p
lus
thal
ido
mid
e
Arm
B r
ecei
ved
100
mg
/d,
incr
ease
d t
o 2
00 m
g a
fter
14
day
s as
to
lera
ted
fo
r u
p
to 1
2 m
o
Arm
A v
s. B
: C
R/V
GPR
at
1 y:
40%
vs.
63
%; P
< .0
013-
y PF
S: 2
3% v
s. 4
2%;
P <
.001
3-y
OS:
75%
vs.
86%
; P
= .0
04
Gra
de
3/4
AEs
, arm
A v
s. a
rm B
: PN
: 0%
vs.
10%
; P <
.001
Co
nst
ipat
ion
: 0%
vs.
4%
; P =
.047
Ab
bre
viat
ion
s: A
Es, a
dve
rse
even
ts; A
LLG
, Au
stra
lasi
an L
euka
emia
an
d L
ymp
ho
ma
Gro
up
; ASC
T, a
uto
log
ou
s st
em c
ell t
ran
spla
nta
tio
n; C
R, c
om
ple
te r
esp
on
se; E
FS,
even
t-fr
ee s
urv
ival
; GC
SF, g
ran
ulo
cyte
co
lon
y-st
imu
lati
ng
fac
tor;
IFN
, in
terf
ero
n-a
lph
a; M
M, m
ult
iple
mye
lom
a; M
R, m
inim
al r
esp
on
se; M
ST, m
edia
n s
urv
ival
tim
e; N
S, n
ot
sig
nifi
can
t; O
S, o
vera
ll su
rviv
al; P
FS, p
rog
ress
ion
-fre
e su
rviv
al; P
N, p
erip
her
al n
euro
pat
hy;
PR
, par
tial
res
po
nse
; TT2
, To
tal T
her
apy
2; T
TMSG
, Tu
nis
ian
Mu
ltip
le M
yelo
ma
Stu
dy
Gro
up
; VA
D, v
incr
isti
ne/
do
xoru
bic
in/d
exam
eth
aso
ne;
VG
PR, v
ery
go
od
par
tial
res
po
nse
. *A
sses
sed
6 m
on
ths
afte
r se
con
d t
ran
spla
nta
tio
n in
arm
A a
nd
3 m
on
ths
afte
r th
alid
om
ide
mai
nte
nan
ce in
arm
B.

Supplement
Badros
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
26
AcknowledgmentThe author thanks Lori Keys Pender, MPH, BCOP, for medical writing assistance.
References 1. Anderson KC, Kyle RA, Rajkumar SV, et al. Clinically relevant
endpoints and new drug approvals for myeloma. Leukemia 2008;22:231–239.
2. Anderson KC, Alsina M, Bensinger W, et al. NCCN clinical practice guidelines in oncology: multiple myeloma. Version 2, 2010. Available at: http://www.nccn.org/professionals/physician_gls/PDF/myeloma.pdf. Accessed May 19, 2009.
3. Fritz E, Ludwig H. Interferon-alpha treatment in multiple myeloma: meta-analysis of 30 randomised trials among 3948 patients. Ann Oncol 2000;11:1427–1436.
4. Myeloma Trialists’ Collaborative Group. Interferon as therapy for multiple myeloma: an individual patient data overview of 24 randomized trials and 4012 patients. Br J Haematol 2001;113:1020–1034.
5. Alexanian R, Weber D, Dimopoulos M, et al. Randomized trial of alpha-interferon or dexamethasone as maintenance treatment of multiple myeloma. Am J Hematol 2000;65:204–209.
6. Shustik C, Belch A, Robinson S, et al. A randomized comparison of melphalan with prednisone or dexamethasone as induction therapy and dexamethasone or observation as maintenance therapy in multiple myeloma: NCIC CTG MY.7. Br J Haematol 2006;136:203–211.
7. Salmon SE, Crowley JJ, Balcerzak SP, et al. Interferon versus interferon plus prednisone remission maintenance therapy for multiple myeloma: a Southwest Oncology Group study. J Clin Oncol 1998:16:890–896.
8. Berenson JR, Crowley JJ, Grogan TM, et al. Maintenance therapy with alternate-day prednisone improves survival in multiple myeloma patients. Blood 2002;99:3163–3168.
9. Offidani M, Corvatta L, Polloni C, et al. Thalidomide-dexamethasone versus interferon-alpha-dexamethasone as maintenance treatment after ThaDD induction for multiple myeloma: a prospective, multicentre, randomised study. Br J Haematol 2008;144:653–659.
10. Ludwig H, Hajek R, Tóthová E, et al. Thalidomide-dexamethasone compared with melphalan-prednisolone in elderly patients with multiple myeloma. Blood 2009;113:3435–3442.
11. Palumbo A, Bringhen S, Rossi D, et al. A prospective, randomized phase III study of bortezomib, melphalan, prednisone and thalidomide (VMPT) versus bortezomib, melphalan and prednisone (VMP) in elderly newly diagnosed myeloma patients [abstract]. Presented at 2008 American Society of Hematology Annual Meeting; December 6–9, 2008; San Francisco, California. Abstract 652.
12. Sonneveld P, van der Holt B, Schmidt-Wolf IGH, et al. First analysis of HOVON-65/GMMG-HD4 randomized phase III trial comparing bortezomib, adriamycine, dexamethasone (PAD) vs VAD as induction treatment prior to high dose melphalan (HDM) in patients with newly diagnosed multiple myeloma (MM) [abstract]. Presented at the 2008 American Society of Hematology Annual Meeting; December 6–9, 2008; San Francisco, California. Abstract 653.
guidelines currently do not address the dose or dura-tion of maintenance thalidomide. Most centers cur-rently continue patients on thalidomide for 1 to 2 years, depending on the patient’s tolerance.
Finally, more research is needed to determine whether cytogenetics can be used to identify appro-priate candidates for post-transplantation mainte-nance. Subgroup analyses from Total Therapy 2 sug-gest that thalidomide maintenance reduced the risk for death in patients with metaphase cytogenetic ab-normalities, a well-known adverse prognostic factor, but not in those without these abnormalities.18 The IFM 99-02 trial showed that thalidomide was not effective in patients with del(13), and the United Kingdom MRC Myeloma IX trial showed that risk for death was significantly increased with thalido-mide maintenance in patients with del (17p).14
As these authors describe elsewhere in this sup-plement, increasing evidence suggests that the novel agents bortezomib and lenalidomide may overcome the poor prognosis associated with cytogenetic ab-normalities in myeloma.24 How these findings from the induction setting translate into the maintenance setting remains to be determined in appropriately designed clinical trials.
ConclusionsThe role of maintenance therapy after conventional chemotherapy remains to be determined, but there is a paucity of ongoing research in this setting. Much work is needed to evaluate maintenance therapy af-ter ASCT, yet the optimal treatment regimen has not been identified. Thalidomide is the first novel agent to be studied as a maintenance therapy and shows the most promise. However, it may work through a direct cytoreductive effect rather than a true maintenance effect, given that several trials showed benefit only in patients who had not experienced at least a VGPR before initiating maintenance treatment. The opti-mal dose and duration of thalidomide maintenance remains to be determined, as does the appropriate patient population for routine treatment. Moreover, whether thalidomide should be used as maintenance or at relapse remains a matter of debate. More robust results of trials with lenalidomide and bortezomib maintenance therapies are eagerly awaited.

Supplement
Maintenance Therapy in Multiple Myeloma
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
27
13. Barlogie B, Tricot G, Anaissie E, et al. Thalidomide and hematopoietic-cell transplantation for multiple myeloma. N Engl J Med 2006;354:1021–1030.
14. Attal M, Harousseau JL, Leyvraz S, et al. Maintenance therapy with thalidomide improves survival in patients with multiple myeloma. Blood 2006;108:3289–3294.
15. Abdelkefi A, Ladeb S, Torjman L, et al. Single autologous stem-cell transplantation followed by maintenance therapy with thalidomide is superior to double autologous transplantation in multiple myeloma: results of a multicenter randomized clinical trial. Blood 2008;111:1805–1810.
16. Spencer A, Prince HM, Roberts AW, et al. Consolidation therapy with low-dose thalidomide and prednisolone prolongs the survival of multiple myeloma patients undergoing a single autologous stem-cell transplantation procedure. J Clin Oncol 2009;27:1788–1793.
17. Hicks LK, Haynes AE, Reece DE, et al. A meta-analysis and systematic review of thalidomide for patients with previously untreated multiple myeloma. Cancer Treat Rev 2008;34:442–452.
18. Barlogie B, Pineda-Roman M, van Rhee F, et al. Thalidomide arm of Total Therapy 2 improves complete remission duration and survival in myeloma patients with metaphase cytogenetic abnormalities. Blood 2008;112:3115–3121.
19. Morgan GJ, Jackson GH, Davies FE, et al. Maintenance thalidomide may improve progression free but not overall survival; results from the Myeloma IX Maintenance Randomisation [abstract]. Presented
at the 2008 American Society of Hematology Annual Meeting; December 6–9, 2008; San Francisco, California. Abstract 656.
20. Mounier MM, Arnulf B, Jaccard A, et al. Intermittent dex/thal as pretransplantation and maintenance treatment in de novo MM: a randomized trial. Presented at the XIIth International Myeloma Workshop; February 26–March 1, 2009; Washington, DC.
21. Maiolino A, Barros JC, Tanaka P, et al. Thalidomide plus dexamethasone after ASCT improves PFS in MM: a Brazilian randomized trial. Presented at the XIIth International Myeloma Workshop; February 26–March 1, 2009; Washington, DC.
22. Feyler S, Rawstrom A, Jackson G, et al. Thalidomide maintenance following high-dose therapy in multiple myeloma: a UK myeloma forum phase 2 study. Br J Haematol 2007;139:429–433.
23. Chang JE, Juckett MB, Callander NS, et al. Thalidomide maintenance following high-dose melphalan with autologous stem cell support in myeloma. Clin Lymphoma Myeloma 2008;8:153–158.
24. Badros A. In the age of novel therapies, what defines high-risk multiple myeloma? J Natl Compr Cancer Netw 2010;8(Suppl 1):S28–S34.
25. Spencer A, Prince M, Roberts AW, et al. First analysis of the Australasian Leukaemia and Lymphoma Group (ALLG) trial of thalidomide and alternate day prednisolone following autologous stem cell transplantation (ASCT) for patients with multiple myeloma (ALLG MM6) [abstract]. Blood 2006;108:Abstract 58.

Supplement
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-28
Key WordsChromosomal abnormalities, risk stratification, thalidomide, bortezomib, lenalidomide, allogeneic stem cell transplantation
AbstractMultiple myeloma is characterized by clinical and biologic hetero-genicity. Recently, genetic analysis has provided predictable prog-nosis across different types of treatment. These advances have al-lowed patients to be categorized into different risk groups and have been particularly useful in defining a high-risk group with short survival after standard- and high-dose chemotherapies. Pre-liminary studies have shown promising outcomes after the use of novel agents, such as bortezomib, thalidomide, and lenalidomide in high-risk patients, including those eligible for autologous stem cell transplantation and those who cannot or will not undergo transplantation. The application of risk-based therapy and the po-tential of the new agents to abrogate the influence of adverse prognostic features may improve outcomes in these patients. (JNCCN 2010;8[Suppl 1]:S28–S34)
The use of nonchemotherapeutic antimyeloma agents is also driving efforts for improved prognostication. Re-cent data suggest that agents such as thalidomide, bort-ezomib, and lenalidomide may neutralize the effects of negative prognostic factors. An effective means of risk stratification is required so that patients with poor risk may be offered more aggressive treatment or be entered into clinical trials of novel agents as first-line therapy. This article discusses evolving systems for risk stratifica-tion and the potential of novel agents to improve out-comes in high-risk patients newly diagnosed with MM.
Evaluation of Genetic ChangesPlasma cells in MM harbor multiple and complex chro-mosomal abnormalities. Studies in the past 7 to 8 years have shown the prognostic value of genetic aberrations, and the assessment of chromosomal abnormalities is an additional parameter that can refine the identification of high-risk patients.
The different techniques currently used to detect genetic aberrations are conventional karyotyping, fluo-rescence in situ hybridization (FISH), and microarray technology.5 Nearly all patients with MM have abnor-mal chromosomes according to FISH (deletions, an-euploidy, and translocations), but standard metaphase analysis identifies aberrant karyotypes in approximately 30% of patients.6 Any abnormality detected conven-tionally identifies a subgroup with a higher proliferative rate and worse prognosis.
Several chromosomal changes have been associated with shorter survival. The most widely recognized poor prognosticators of survival are deletions of chromosome 13 or its long arm (del[13]), translocations of the heavy-chain gene on chromosome 14 (t[4;14] or t[14;16]), and deletion of p53 on chromosome 17p13 (del[17p]). Deletion or structural anomalies of chromosome 13 are
Multiple myeloma (MM) is a clinically and patho-physiologically heterogeneous disease, as evidenced by variable response to treatment and variation in survival from a few months to more than 10 years. Nationwide U.S. data show that approximately 20% of patients survive longer than 10 years, irrespective of therapy.1,2 Genetic variations among myeloma cells appear to un-derlie much of the heterogeneity in clinical outcomes.
Several groups have reported on the prognostic ca-pability of genetic information in MM, which has led to re-evaluation of the definition of high-risk disease.3,4
From the Bone Marrow Transplant Program, Greenebaum Cancer Center, University of Maryland, Baltimore, Maryland.This work was supported by an educational grant from Millennium Pharmaceuticals, Inc.Correspondence: Ashraf Badros, MD, University of Maryland, Greenebaum Cancer Center, Bone Marrow Transplant Program, 22 South Greene Street, Baltimore, MD 21201. E-mail: [email protected]
In the Age of Novel Therapies, What Defines High-Risk Multiple Myeloma?
Ashraf Badros, MD, Baltimore, Maryland

Supplement
High-Risk Myeloma
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-29
platform and widespread availability, and thus is not easily translated into clinical practice.
Risk StratificationGenetic changes display such a high prognostic value that myeloma experts have recently recommended including cytogenetic and FISH evaluations in a risk stratification system (Table 1).4,14 Routine molecular genetic testing is recommended for all patients with MM to identify the 25% with high-risk disease in whom conventional therapies perform poorly. The recommended basic test panel includes FISH detec-tion of t(4;14), t(14;16), and del(17q); cytogenetic detection of del(13); and determination of serum β2M, lactate dehydrogenase, or plasma cell labeling index as surrogate markers of tumor cell proliferation.
This risk-stratification model in Table 1 forms the basis of the Mayo Stratification of Myeloma and Risk-Adapted Therapy (mSMART), an evidence-based algorithm of treatment decision-making that was developed at the Mayo Clinic for patients with newly diagnosed MM.15 In general, these high-risk features define a population of 25% to 30% of pa-tients who have median survival of 2 to 3 years, even with stem cell transplantation, compared with
detected in approximately 50% of patients with an abnormal karyotype and in 10% to 20% of patients overall. Patients with chromosome 13 anomalies in their metaphase cells have shorter survival and lower treatment response rates. The effect of del(13) on prognosis is greater when it is detected with karyo-type analysis in metaphase cells than with interphase FISH.5,7–9 Recent data suggest that the prognostic significance of del(13) may depend on its association with t(4;14), del(17p), or a high serum level of β2-microglobulin (β2M).9
Chromosome translocations involving the im-munoglobulin heavy-chain gene locus are detect-able in 60% to 75% of patients with MM accord-ing to FISH. Translocations that have prognostic significance include t(4;14), t(14;16), t(11;14), and t(6;14). Of these, t(4;14) (detected in 15%–20% of patients) and t(14;16) (present in 2%–10% of patients) are unfavorable prognostic factors for pa-tients with MM treated with either conventional or high-dose therapy (HDT).5,6,8,10 By contrast, t(11;14) (detected in 15%–20% of patients) charac-terizes a group of patients with neutral or somewhat favorable prognosis.8,9
Deletion of chromosome 17p13, present in 10% of patients, confers poorer survival. Patients with this deletion who undergo HDT followed by autolo-gous stem cell transplantation (ASCT) have signifi-cantly shorter progression-free and overall survival than patients without this deletion.6–8
Aneuploidy occurs frequently in MM cells, and ploidy status has a significant impact on prognosis. Hypoploidy is associated with more aggressive disease and shorter survival. Hyperdiploid MM has a lower frequency of immunoglobulin heavy-chain translo-cations and is associated with good prognosis.5,9
Although chromosomal anomalies have a high impact on survival, they must be evaluated in the context of other parameters, especially the β2M lev-el. For example, subsets of patients with high-risk ge-netics, such as t(14;4) or del(17p), but with low β2M level may have a similar or only marginally worse prognosis than other patients.9
A few teams have recently investigated the role of gene expression profiling (GEP) in the prognos-tication of myeloma, and several molecular classi-fication systems have been proposed based on this technique.11–13 Although GEP is useful for risk strati-fication, it is currently limited by a lack of a uniform
Table 1 Recommended Classification of High-Risk MyelomaHigh Risk (25%) Good Risk (75%)*
Any of the following:
t(4;14) according to FISH
t(14;16) or t(14;20) according to FISH
Del 17q13 according to FISH
Deletion 13 or aneuploidy according to metaphase analysis
Plasma cell labeling index > 3%
Absence of high-risk features and presence of any of the following:
Hyperdiploidy
t(11;14) according to FISH
t(6;16) according to FISH
Abbreviations: FISH, fluorescence in situ hybridization. *Patients should be considered to be truly low-risk if genetic markers are accompanied by a β2-microglobulin level less than 5.5 mg/L, lactate dehydrogenase less than 250 U/L, and/or a plasma cell labeling index less than 1%. Similarly, the presence of β2-microglobulin level less than 3.5 mg/L may favorably modify the course for patients with otherwise high-risk genetics. Reprinted with permission from Macmillan Publishers Ltd. Stewart AK, Bergsagel PL, Greipp PR, et al. A practical guide to defining high-risk myeloma for clinical trials, patient counseling and choice of therapy. Leukemia 2007;21:529–534.

Supplement
Badros
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-30
Table 2 Selected Studies of New Agents in Newly Diagnosed High-Risk Patients Eligible for High- Dose Therapy/Autologous Stem Cell TransplantationFirst Author No. of Patients Patient Population Treatment Results
Bortezomib
Dispenzieri et al.19
44 Patients with high-risk newly diagnosed myeloma (del[13q], PCLI > 1%, t[4;14] or β2M > 5.5 mg/L)
Bortezomib for induction and maintenance
Response rate (> PR):•All = 48%•PCLI > 1%: 47%•β2M > 5.5 mg/L: 45%•del(13q): 33%•t(4;14): 50%After median follow-up of 41.6 months:•1-y PFS/OS: 50%/88%•2-y PFS/OS: 28%/76%
Knop et al.20 200 Newly diagnosed myeloma β2M: 3.75 ± 3.38 mg/Ldel(13): 55 (28%) del(17p): 20 (10%) t(4;14): 16 (8%)
Bort-dex-cyclophosphamide
Response rate on day 63 ORR: 84% Normal cytogenetics: 86% Abnormal cytogenetics: 82% del(13): 82% del(17p): 70% t(4;14): 94%
Lenalidomide
Kapoor et al.21 100 High-risk: at least 1 of the following: hypodiploidy, del(13), del(17p), t(4;14), t(4;16), or PCLI ≥ 3% Standard-risk: absence of all high-risk features
Len-dex (low- or high-dose)
Response rates:•CR + VGPR: high-risk, 38%; standard-risk, 45%•≥ PR: high-risk, 81%; standard-risk, 89%Median PFS: high-risk, 18.5 months; standard-risk, 36.5 months Median OS: not reached for either group
Zonder et al.22 198 AK Len-dex: 13/54 Dex: 12/43FISH-defined HRCA (del[13] or del[17p]) Len-dex group: 8/37 Dex group: 11/45
Len-dex vs. placebo-dex
Estimated 1-y PFS (with AK vs. without):•Len-dex: 54% vs. 86% (P = NS)•Dex: 27% vs. 67% (P = .008)Estimated 1-y PFS (with HRCA vs. without):•Len-dex: 100% vs. 71% (P = NS)•Dex: 55% vs. 57% (P = NS)Estimated 1-y OS (with HRCA vs. without):•Len-dex: 80% vs. 100% (P = NS)•Dex: 88% vs. 100% (P = NS)
Kapoor et al.23 125 High baseline PCLI (≥ 1%) vs. low baseline PCLI (< 1%)
Len-dex vs. TD Median PFS (high PCLI vs. low PCLI)•Len-dex: 2.3 vs. 3.1 y (NS)•TD: 1.3 vs. 2.3 y (P = .01)Median OS•Len-dex: not reached for either group•TD: 2.3 vs. 6.9 y (P = .02)
Thalidomide
Zangari et al.24
Waheed et al.25
668 Patients with or without cytogenetic abnormalities by metaphase analysis
TT2 protocol (induction, tandem transplantation, consolidation, maintenance) with thal vs. TT2 protocol without thal
5-y follow-up (TT2 + thal vs. TT2 without thal) Median EFS:•With CA: 3.7 vs. 2.5 y (P = .03)•Without CA: 6.3 vs. 5.4 y (P = .04)Median OS:•With CA: NR vs. 4.1 y (P = .04)•Without CA: NR vs. NR81-month follow-up (TT2 + thalidomide vs. TT2 without thalidomide) 6-y EFS•With CA: 38% vs. 20% (P = .008)•Without CA: 56% vs. 45% (P = .02)6-y OS•With CA: 53% vs. 35% (P < .001)•Without CA: 70% vs. 68% (P = NS)
Combinations
Cavo et al.26 474 (464 evaluable)
ISS II + III: 54%–56% del(13): 46%–47% t(4;14): 19%–20% del(17p): 7%–8%
VTD vs. TD
≥ nCR rate after induction:•ISS III: VTD, 24%; TD, 6% (P = .03)•del(13q): VTD, 39%; TD, 12% (P < .001)•t(4;14): VTD, 40%; TD, 9% (P < .001)•del(17p): VTD, 27%; TD, 0% (P < .001)

Supplement
High-Risk Myeloma
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-31
patients are therefore considered appropriate can-didates for alternative approaches, including early incorporation of novel agents. Clinical trial data suggest that in patients with MM who are eligible for transplantation, newer agents may be able to overcome the adverse influence of cytogenetic ab-normalities (Table 2).19–29
Two major combinations have emerged as treat-ment options for elderly patients and others who will not undergo transplantation: melphalan-prednisone (MP) plus an immunomodulatory agent, and MP plus bortezomib. Both of these approaches have re-sulted in outcomes superior to those with MP alone and are recommended induction therapies (NCCN category 1 recommendation) in patients ineligible for transplantation.17 These new combinations have also shown efficacy in high-risk patients ineligible for transplantation (Table 3).30–33
Role of ASCTThe introduction of reduced-intensity conditioning
more than 6 to 7 years for patients with standard-risk MM.16 Furthermore, identifying the other 75% of patients as standard risk allows them to receive appropriate treatment with minimal toxicity.
Emerging data suggest that novel therapies and combinations may ameliorate the adverse influence of these poor-risk features, underscoring the impor-tance of including genetics into risk-stratification schemes. Current NCCN guidelines include cytoge-netic and FISH evaluation as part of the initial diag-nostic workup but note that further data are needed before cytogenetic information can be incorporated into patient management.17
Outcomes With Novel AgentsA major application of genetic stratification is in the selection of candidates for HDT-ASCT. Several large studies have shown that patients defined as be-ing at high risk genetically do not develop durable responses to HDT as currently practiced, and many experience early relapse after ASCT.7–9,18 High-risk
Table 2 Selected Studies of New Agents in Newly Diagnosed High-Risk Patients Eligible for High- Dose Therapy/Autologous Stem Cell Transplantation (cont.)First Author No. of Patients Patient Population Treatment Results
Combinations (cont’d.)
Pineda-Roman et al.27
303 ISS II: 32% ISS III: 21% CA: 33% GEP-defined high risk: 15% GEP subgroup MS: 11%
TT3 protocol (induction and consolidation with VTD-PACE; maintenance with VTD) vs. TT2 protocol (historical controls)
2-y outcomes (TT3 vs. TT2 + thalidomide) CR duration•Low-risk: 95% vs. 84% (P = .01)•High-risk: 61% vs. 54% (P = NS)•MMSET risk subgroup: 89% vs. 46% (P = .004)EFS•Low-risk: 89% vs. 85% (P = .04)•High-risk: 60% vs. 35% (P = NS)•MMSET risk subgroup: 84% vs. 57% (P = NS)OS•Low-risk: 90% vs. 89% (P = NS)•High-risk: 70% vs. 46% (P = NS)•MMSET risk subgroup: 97% vs. 67% (P = .01)
Richardson et al.28
63 Patients with newly diagnosed MM ISS II/III: n = 31 del(13): n = 7 t(4:14): n = 10
Len + bort + dex for up to eight 21-day cycles
Response ORR/≥ VGPR after median of 10 cycles All patients: 98%/71% del(13)+: 86%/57% del(13)–: 100%/75%t(4;14)+: 100%/70% t(4;14)–: 98%/73%ISS I: 97%/51%, ISS II : 100%/57%, ISS III: 100%/80%
Landau et al.29 34 Patients with high-risk MM
Bort + liposomal dox + dex followed by thal + dex
Any response:del(13)+: 91% del(13)–: 70%t(4;14)+: 100% t(4;14)–: 75%del(p53)+: 100% del(p53)–: 76%
Abbreviations: AK, abnormal karyotype; β2M, β2-microglobulin; bort, bortezomib; CA, chromosomal abnormality; CR, complete response; dex, dexamethasone; dox, doxorubicin; EFS, event-free survival; FGFR3, fibroblast growth factor receptor 3; FISH, fluorescence in situ hybridization; GEP, gene expression profiling; HRCA, high-risk cytogenetic abnormality; ISS, International Staging System; len, lenalidomide; MM, multiple myeloma; MMSET, multiple myeloma SET domain; nCR, near complete response; NR, not reported; NS, not significant; ORR, overall response rate; OS, overall survival; PACE, cisplatin, doxorubicin, cyclophosphamide, etoposide; PCLI, plasma cell labeling index; PFS, progression-free survival; PR, partial response; thal, thalidomide; TD, thalidomide-dexamethasone; VGPR, very good partial response; VTD, bortezomib-thalidomide-dexamethasone.

Supplement
Badros
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-32
regimens with reduction in immediate transplantation-related mortality and stable engraftment has rekin-dled interest in allogeneic transplantation. In patients with poor-risk disease, nonmyeloablative condition-ing regimens (mini-allogeneic transplantation) with or without donor lymphocyte infusions have resulted in excellent responses and stable engraftment, with lower transplantation-related mortality, although acute and chronic graft-versus-host disease remains a troubling complication.34,35 In a prospective trial, the Intergroupe Francophone du Myélome studied ASCT followed by nonmyeloablative allotransplantation in patients with newly diagnosed MM who had both el-evated β2M and del(13),36 then compared the results with data on patients with the same high-risk features but had no donor and had undergone tandem ASCT.37 The median duration of overall (35 vs. 41 months) and progression-free survival (25 vs. 30 months) did not differ significantly between the regimens.36
Encouraging long-term follow-up results were recently reported for 102 patients who underwent ASCT followed by nonmyeloablative allogeneic he-matopoietic stem cell transplantation from a human leukocyte antigen-identical sibling.38 After a median
follow-up of 6.3 years, the median overall survival was not reached, and estimated 5-year overall and progres-sion-free survival were 64% and 36%, respectively. Although cytogenetic studies were not performed at specific times or using uniform methods, the authors reported that cytogenetics had no effect on the risk for relapse, suggesting that allogeneic transplantation may overcome adverse genetic prognostic features. A recent analysis of the prognostic impact of the most frequent genetic abnormalities in patients who under-went allogeneic transplantation showed that del(17p) was the only significant prognostic factor, with a negative impact on complete response and length of event-free survival.39 In multivariate analyses, only del(13) and del(17p) significantly influenced the rate of relapse, whereas for event-free survival, only age and del(17p) remained negative prognostic factors. Major findings were that t(4;14) was not associated with a worse complete response rate or shorter event-free or overall survival, suggesting that the negative effect of t(14;4) might be overcome with allogeneic transplantation. These results may have implications for risk-adapted strategies.
Abbreviations: β2M, β2-microglobulin; bort, bortezomib; CR, complete response; EFS, event-free survival; NS, not significant; ISS, International Staging System; KPS, Karnofsky performance status; OS, overall survival; TTP, time to progression.
Table 3 Selected Studies of New Agents in Patients With Newly Diagnosed High-Risk Disease Ineligible for High-Dose Therapy/Autologous Stem Cell Transplantation
First AuthorNo. of Patients Patient Population Treatment Results
Mateos et al.30,31 60 Elderly patients del(13): n = 13 IgH translocation: n = 8
Bort-melphalan-prednisone
Response rate: Rb del: 100% No Rb del: 66% IgH tr: 88% No IgH tr: 82% TTP (months): β2M < 3.5 mg/L: 23 β2M ≥ 3.5 mg/L: 29ISS stage I/II: 27 ISS stage III: 24 Rb del: 25 No Rb del: NR (IgH tr–)/no RB del: 29 (IgH tr)+/Rb del: 23
San Miguel et al.32 682 Elderly patients ISS I: 19% ISS II: 47% ISS III: 34%–35% KPS ≤ 70%: 33%–35% Bort group: High-risk cytogenetics [t(4;14)/t(14;16)/del(17p)]: n = 26 Standard-risk: n = 142
Bort-melphalan-prednisonevs.melphalan-prednisone
Bort group: High-risk vs. standard-risk patients: CR: 28% in both TTP: P = .55OS: P = .99
Palumbo et al.33 54 Elderly patients Median age: 71 y ISS I: 34% ISS II: 32% ISS III: 32% β2M ≥ 3.5 mg/mL: 57%del(13): 38% Data missing: 21%
Lenalidomide-melphalan-prednisone
1-y EFS: β2M < 3.5: 100% β2M ≥ 3.5: 86% (P = .02)del(13): 85% No del(13): 95% (P = NS)t(4;14): 83% No t(4:14): 87.5% (P = NS)

Supplement
High-Risk Myeloma
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-33
4. Stewart AK, Bergsagel PL, Greipp PR, et al. A practical guide to defining high-risk myeloma for clinical trials, patient counseling and choice of therapy. Leukemia 2007;21:529–534.
5. Fonseca R, Barlogie B, Bataille R, et al. Genetics and cytogenetics of multiple myeloma: a workshop report. Cancer Res 2004;64:1546–1558.
6. Dewald, GW, Therneau T, Larson D, et al. Relationship of patient survival and chromosome anomalies detected in metaphase and/or interphase cells at diagnosis of myeloma. Blood 2005;106:3553–3558.
7. Chang, H, Qi XY, Samiee S, et al. Genetic risk identifies multiple myeloma patients who do not benefit from autologous stem cell transplantation. Bone Marrow Transplant 2005;36:793–796.
8. Gertz MA, Lacy MQ, Dispenzieri A, et al. Clinical implications of t(11;14)(q13;q32), t(4;14)(p16.3;q32), and -17p13 in myeloma patients treated with high-dose therapy. Blood 2005;106:2837–2840.
9. Avet-Loiseau H, Attal M, Moreau P, et al. Genetic abnormalities and survival in multiple myeloma: the experience of the Intergroupe Francophone du Myélome. Blood 2007;109:3489–3495.
10. Chang, H, Sloan S, Li D, et al. The t(4;14) is associated with poor prognosis in myeloma patients undergoing autologous stem cell transplant. Br J Haematol 2004;125:64–68.
11. Shaughnessy JD Jr, Zhan F, Burington BE, et al. A validated gene expression model of high-risk multiple myeloma is defined by deregulated expression of genes mapping to chromosome 1. Blood 2007;109:2276–2284.
12. Zhan F, Barlogie B, Mulligan G, et al. High-risk myeloma: a gene expression based risk-stratification model for newly diagnosed multiple myeloma treated with high-dose therapy is predictive of outcome in relapsed disease treated with single-agent bortezomib or high-dose dexamethasone. Blood 2008;111:968–969.
13. Decaux, O, Lode L, Magrangeas F, et al. Prediction of survival in multiple myeloma based on gene expression profiles reveals cell cycle and chromosomal instability signatures in high-risk patients and hyperdiploid signatures in low-risk patients: a study of the Intergroupe Francophone du Myélome. J Clin Oncol 2008;26:4798–4805.
14. International Myeloma Workshop. Guidelines for risk stratification in multiple myeloma. Report of the 2008 International Myeloma Workshop Consensus Panel 2. Available at http://www.mw-delhi09.com/spargoDocs/Consensuspaneltwo.pdf. Accessed June 10, 2009.
15. Dispenzieri, A, Rajkumar SV, Gertz MA, et al. Treatment of newly diagnosed multiple myeloma based on Mayo Stratification of Myeloma and Risk-adapted Therapy (mSMART): consensus statement. Mayo Clin Proc 2007;82:323–341.
16. Rajkumar SV, Kyle RA. Multiple myeloma: diagnosis and treatment. Mayo Clin Proc 2005;80:1371–1382.
17. Anderson KC, Alsina M, Bensinger W, et al. NCCN clinical practice guidelines in oncology: multiple myeloma, v2.2010. Available at www.nccn.org. Accessed July 31, 2009.
18. Fonseca R. Strategies for risk-adapted therapy in myeloma. Hematology Am Soc Hematol Educ Program 2007;304–310.
19. Dispenzieri, A, Jacobus S, Vesole DH, et al. Primary therapy with bortezomib—the role of induction, maintenance, and re-induction in patients with high risk myeloma: update of results from E2A02 [abstract]. Presented at the 2008 American Society of Hematology Annual Meeting; December 6–9, 2008; San Francisco, California. Abstract 1738.
ConclusionsDefining a high-risk cohort of patients with MM with short survival regardless of treatment will be helpful in guiding management decisions. With the demon-strated adverse influence of chromosomal changes, various groups have endorsed a new risk stratifica-tion model that incorporates recently defined inde-pendent prognostic markers of underlying myeloma cell biology. Efforts have focused on defining a high-risk group that might merit a different management approach, such as early treatment with novel agents. The proposed risk stratification system remains a global stratification and is not therapy-based, al-though ongoing trials may uncover risk factors spe-cific for individual therapies. The general agreement is that no definitive treatment can currently be man-dated based on the presence of risk factors.14 The use of genetic information for stratifying risk and making treatment decisions continues to be explored in clin-ical trials and will likely play a greater role in patient care in the near future.
New therapies with novel mechanisms of action may benefit patients for whom other therapies fail. Preliminary reports from several groups show high response rates with use of bortezomib, lenalidomide, and thalidomide in both the transplantation and nontransplantation settings in high-risk patients, suggesting that these new agents may ameliorate the effects of adverse prognostic factors. Long-term follow-up and confirmation in prospective, com-parative trials will be required to determine whether clinical benefit can be sustained.
AcknowledgmentThe author thanks Meher M. Dustoor, PhD, for medical writing assistance.
References 1. Rajkumar SV, Buadi F. Multiple myeloma: new staging systems for
diagnosis, prognosis and response evaluation. Best Pract Res Clin Haematol 2007;20:665–680.
2. Horner MJ, Ries LAG, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2006. Available at: http://seer.cancer.gov/csr/1975_2006. Accessed May 8, 2009.
3. Stewart AK, Fonseca R. Prognostic and therapeutic significance of myeloma genetics and gene expression profiling. J Clin Oncol 2005;23:6339–6344.

Supplement
Badros
© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-34
20. Knop S, Liebisch P, Wandt H, et al. Bortezomib, IV cyclophosphamide, and dexamethasone (VelCD) as induction therapy in newly diagnosed multiple myeloma: results of an interim analysis of the German DSMM Xia trial [abstract]. Presented at the 2009 American Society of Clinical Oncology Annual Meeting; May 29–June 2, 2009; Orlando, Florida. Abstract 8516.
21. Kapoor P, Kumar S, Fonseca R, et al. Impact of risk stratification on outcome among patients with multiple myeloma receiving initial therapy with lenalidomide and dexamethasone. Blood 2009;114:518–521.
22. Zonder J, Crowley J, Bolejack V, et al. A randomized Southwest Oncology Group study comparing dexamethasone to lenalidomide + dexamethasone (LD) as treatment of newly diagnosed multiple myeloma: impact of cytogenetic abnormalities on efficacy of LD, and updated overall study results [abstract]. Presented at the 2008 American Society of Clinical Oncology Annual Meeting; May 30–June 3, 2008; Chicago, Illinois. Abstract 8521.
23. Kapoor P, Kumar S, Greipp PR, et al. Prognostic impact of the plasma cell labeling index (LI) in newly diagnosed myeloma patients treated with thalidomide-dexamethasone (thal/dex) or lenalidomide-dexamethasone (len/dex) [abstract]. Presented at the 2008 American Society of Hematology Annual Meeting; December 6–9, 2008; San Francisco, California. Abstract 1729.
24. Zangari M, van Rhee F, Anaissie E, et al. Eight-year median survival in multiple myeloma after total therapy 2: roles of thalidomide and consolidation chemotherapy in the context of total therapy 1. Br J Haematol 2008;141:433–444.
25. Waheed S, Shaughnessy J, Szymonifka, J, et al. Benefit of thalidomide in Total Therapy 2 (TT2) of multiple myeloma exhibiting both cytogenetic abnormalities and low risk by gene expression profiling [abstract]. Presented at the 2009 American Society of Clinical Oncology Annual Meeting; May 29–June 2, 2009; Orlando, Florida. Abstract 8590.
26. Cavo, M, Testoni N, Terragna C, et al. Superior rate of complete response with up-front Velcade-thalidomide-dexamethasone versus thalidomide-dexamethasone in newly diagnosed multiple myeloma is not affected by adverse prognostic factors, including high-risk cytogenetic abnormalities [abstract]. Presented at the 2008 American Society of Hematology Annual Meeting; December 6–9, 2008; San Francisco, California. Abstract 1662.
27. Pineda-Roman M, Zangari M, Haessler J, et al. Sustained complete remissions in multiple myeloma linked to bortezomib in total therapy 3: comparison with total therapy 2. Br J Haematol 2008;140:625–634.
28. Richardson P, Lonial S, Jakubowiak A, et al. Lenalidomide, bortezomib, and dexamethasone in patients with newly diagnosed multiple myeloma: encouraging efficacy in high risk groups with updated results of a phase I/II study [abstract]. Presented at the 2008
American Society of Hematology Annual Meeting; December 6–9, 2008; San Francisco, California. Abstract 92.
29. Landau H, Hassoun H, Cohen A, et al. Sequential administration of bortezomib, liposomal doxorubicin and dexamethasone followed by thalidomide and dexamethasone results in rapid control of untreated high-risk multiple myeloma and improves depth of response [abstract]. Presented at the 2008 American Society of Hematology Annual Meeting; December 6–9, 2008; San Francisco, California. Abstract 3712.
30. Mateos MV, Hernandez JM, Hernandez MT, et al. Bortezomib plus melphalan and prednisone in elderly untreated patients with multiple myeloma: results of a multicenter phase 1/2 study. Blood 2006;108:2165–2172.
31. Mateos MV, Hernandez JM, Hernandez MT, et al. Bortezomib plus melphalan and prednisone in elderly untreated patients with multiple myeloma: updated time-to-events results and prognostic factors for time to progression. Haematologica 2008;93:560–565.
32. San Miguel JF, Schlag R, Khuageva NK, et al. Bortezomib plus melphalan and prednisone for initial treatment of multiple myeloma. N Engl J Med 2008;359:906–917.
33. Palumbo A, Falco P, Corradini P, et al. Melphalan, prednisone, and lenalidomide treatment for newly diagnosed myeloma: a report from the GIMEMA—Italian Multiple Myeloma Network. J Clin Oncol 2007;25:4459–4465.
34. Badros A, Barlogie B, Morris C, et al. High response rate in refractory and poor-risk multiple myeloma after allotransplantation using a nonmyeloablative conditioning regimen and donor lymphocyte infusions. Blood 2001;97:2574–2579.
35. Badros A, Barlogie B, Siegel, et al. Improved outcome of allogeneic transplantation in high-risk multiple myeloma patients after nonmyeloablative conditioning. J Clin Oncol 2002;20:1295–1303.
36. Garban F, Attal M, Michallet M, et al. Prospective comparison of autologous stem cell transplantation followed by dose-reduced allograft (IFM99-03 trial) with tandem autologous stem cell transplantation (IFM99-04 trial) in high-risk de novo multiple myeloma. Blood 2006;107:3474–3480.
37. Moreau P, Hullin C, Garban F, et al. Tandem autologous stem cell transplantation in high-risk de novo multiple myeloma: final results of the prospective and randomized IFM 99-04 protocol. Blood 2006;107:397–403.
38. Rotta M, Storer BE, Sahebi F, et al. Long-term outcome of patients with multiple myeloma after autologous hematopoietic cell transplantation and nonmyeloablative allografting. Blood 2009;113:3383–3391.
39. Schilling G, Hansen T, Shimoni A. et al. Impact of genetic abnormalities on survival after allogeneic hematopoietic stem cell transplantation in multiple myeloma. Leukemia 2008;22:1250–1255.

© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-35
Please print clearly.
Name:
Mailing Address:
City State:
Zip: Phone: Fax:
License Number/State:
Date of Completion:____________________
Professional Degree: MD DO PharmD RPh RN LPN NP PhD Other________________
Specialty: _____________________________Years in practice: ________
Number of myeloma patients seen per week: _________
I certify that I have completed this educational activity as designed.
Signature Date
Addressing Challenges in Multiple Myeloma Management in an Era of New Therapeutics
Release date: February 15, 2010Expiration date: February 15, 2011
Activity Evaluation Form
To obtain continuing education credit within 4 weeks after receipt of a completed form, please: 1) Complete the attached self-assessment and evaluation by February 15, 2011.2) Fax the form to 215-337-0959 or mail completed form to MediCom Worldwide, Inc., 101 Washington Street, Morrisville, PA 19067. Kindly remember to fax or mail both pages.3) All participants must achieve a minimum score of 70% on the self-assessment portion of the form to qualify for CE credit.4) The participant will be mailed the CE certificate within 4 weeks after receipt of the completed, qualified form.
To rECEivE CrEdiT, you MusT subMiT This ForM by FEbruAry 15, 2011.

© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-36
Self-Assessment Answer SheetPlease circle one answer per question. A score of at least 70% on the post-test is required.
1. a b c d 6. a b c d
2. a b c d 7. a b c d
3. a b c d 8. a b c d
4. a b c d 9. a b c d
5. a b c d 10. a b c d
ACTiviTy EvALuATioNAddressing Challenges in Multiple Myeloma Management in an Era of New Therapeutics
Please rate the activity by filling in the most appropriate circle. (A) Excellent (b) Good (C) Fair (d) Poor
1. Overall content A B C D
2. Format A B C D
How well did this activity achieve its educational objectives? A B C D
3. Evaluate the need for, and propose appropriate maintenance therapy options in multiple myeloma A B C D
4. Evaluate the current importance of assessing multiple myeloma patients for risk, especially in the face of emerging and novel agents, and integrate this knowledge into management plans A B C D
5. Describe the most appropriate techniques for monitoring treatment of multiple myeloma A B C D
6. Formulate evidence-based management plans for multiple myeloma patients based upon their age, risk, and comorbidities A B C D
7. Do you feel the activity was useful to you in your practice setting? Yes No
8. Do you feel that fair balance was maintained for all therapeutic options? Yes No
9. Would you participate in future self-study activities? Yes No
10. How long did it take you to complete this activity?
2 hours, 30 minutes 2 hours, 45 minutes 3 hours
Please provide detailed comments and suggestions for future activities. Please contact me regarding upcoming medical education opportunities.
Name:
For additional information on multiple myeloma, please visit www.ManagingMyeloma.com
Please circle the correct answer below.

© Journal of the National Comprehensive Cancer Network | Volume 8 Supplement 1 | February 2010
S-37
1. Which of the following is/are FALSE about peripheral neuropathy in patients with multiple myeloma (MM)?a. It occurs as both a disease-related complication
and a side effect of therapy.b. Its clinical manifestations are usually agent-
specific.c. It is not usually reversible.d. All of the above
2. If sensory peripheral neuropathy or neuropathic pain in patients with MM cannot be controlled nonpharmacologically, which of the following agents is/are recommended?a. Gabapentinb. Nortriptylinec. Topical lidocained. All of the above
3. Which of the following is/are TRUE about asthenia? a. It is the most common side effect of cancer
treatment.b. According to patient surveys, it is the third
most distressing side effect of MM therapy.c. According to NCCN guidelines, patients
with severe asthenia should be treated with a psychostimulant.
d. All of the above
4. The risk for venous thromboembolism in patients being treated for MM:a. Is greater with increased duration of
antimyeloma therapy.b. Is regimen-specific.c. Warrants anticoagulant prophylaxis except in
bedridden patients.d. All of the above
5. In their longitudinal study of osteonecrosis of the jaw in patients with MM, Badros et al. determined that more than half of cases:a. Were preceded by dental extractions.b. Resolved and did not recur.c. Recurred after healing.d. Did not heal during 9 months of follow-up.
6. What is the state of the evidence about whether use of erythropoiesis-stimulating agents (ESAs) leads to solid tumor proliferation in patients with MM?a. ESAs appear to be safe for MM patients younger
than 70 years.b. The evidence in MM is inconclusive.c. ESAs are clearly contraindicated in MM.d. This question has not been studied in MM.
7. Which of the following MM maintenance regimen(s) has/have a category 1 recommendation from the NCCN?a. Prednisoneb. Interferonc. Thalidomided. All of the above
8. Which of the following is NOT a current research issue regarding post-transplant MM maintenance therapy with thalidomide?a. Whether it is safe when combined with
prednisoneb. Its optimal dosagec. Whether it should be discontinued if complete
response is achievedd. Whether cytogenetics can be used to identify
appropriate candidates
9. Which of the following is/are TRUE about genetic aberrations detected conventionally (i.e., by karyotyping) in MM patients?a. They occur in approximately 30% of patients.b. They are associated with a higher proliferative
rate.c. They are associated with worse prognosis.d. All of the above
10. According to the recently developed Mayo Clinic algorithm, which of the following is/are NOT indicators for high-risk MM?a. Serum β2-microglobulin level ≥ 3.5 mg/Lb. t(4;14) by fluorescence in situ hybridizationc. Aneuploidy by metaphase analysisd. Plasma cell labeling index > 3%
Self-assessment Please circle the correct answer on the enclosed answer sheet.










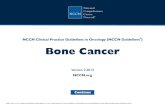





![[Ghiduri][Cancer]NCCN Pain Guidelines - Update](https://static.fdocuments.in/doc/165x107/55cf9686550346d0338c0f31/ghiduricancernccn-pain-guidelines-update.jpg)