Feasibility of Cardiac Resynchronization Therapy in a ... · Congenital heart disease,...
5
178 • HJC (Hellenic Journal of Cardiology) Hellenic J Cardiol 2010; 51: 178-182 Case Report Case Report Manuscript received: August 1, 2009; Accepted: January 9, 2010. Address: Ahmet Al Fagih Department of Adult Cardiology, Prince Sultan Cardiac Center, Riyadh, Kingdom of Saudi Arabia e-mail: [email protected] Key words: Congenital heart disease, dextrocardia, cardiac computed tomography. Feasibility of Cardiac Resynchronization Therapy in a Patient with Complex Congenital Heart Disease and Dextrocardia, Facilitated by Cardiac Computed Tomography and Coronary Sinus Venography AHMET AL FAGIH 1 , KHALED AL NAJASHI 2 , KHALED DAGRIRI 2 , ABDULMAJEED AL OTAY 2 , SALEH AHMED AL GHAMDI 2 1 Department of Adult Cardiology, 2 Department of Pediatric Cardiology, Prince Sultan Cardiac Center, Riyadh, Kingdom of Saudi Arabia We describe a case with pacemaker implantation for cardiac resynchronization therapy (CRT) in a patient with complex congenital heart disease, facilitated by cardiac computed tomography (CT) and coronary sinus (CS) venography. A 37-year-old male presented with congenitally corrected transposition of the great arter- ies and mesocardia, along with a history of two open heart surgeries (closure of atrial septal defects and a ventricular septal defect, and pulmonary valvectomy at age 7; mechanical tricuspid valve replacement at age 13). He showed symptoms of progressive heart failure (NYHA class III) with significant impairment of the systemic right ventricular function. He also developed permanent atrial fibrillation with a junctional rhythm at a rate of 45 beats per minute. Biventricular pacing without an atrial lead was considered to be the best option available. CRT implantation was facilitated by proper identification of CS anatomy utilizing cardiac CT and CS venography and was performed without any complications. At follow up, a postero-anterior chest X-ray showed the final position of the right-sided ventricular (left ventricular morphology) lead pointing to the apex and the left ventricular lead at the posterolateral aspect of the systemic ventricle (right ventricular morphology). A dult patients with congenital heart disease represent an expanding po- pulation that is growing at a rate of 5% per annum. 1 Ventricular dysfunc- tion is common in adult congenital heart disease patients who have a systemic right ventricle (RV) and is related to electrome- chanical dyssynchrony. 2-4 Over 25% of such individuals ultimately progress to symp- tomatic heart failure, which is occasionally refractory to drug therapy and is associated with substantial morbidity and mortality. 4 Therefore, identification of novel therapeu- tic strategies in these patients is of critical importance. Permanent pacemaker leads may be im- planted either epicardially or transvenously in infants as well as older children. 5 Patients with a systemic RV may require conven- tional pacemaker therapy, 6 which in the presence of ventricular dysfunction and con- duction disease may further compromise cardiac performance. 7,8 Hence, devices ca- pable of combining conventional pacing with modern functions geared towards ame- liorating ventricular function seem to offer an obvious advantage. Although cardiac resynchronization therapy (CRT) is rapidly emerging as an effective strategy for managing ventricular
Transcript of Feasibility of Cardiac Resynchronization Therapy in a ... · Congenital heart disease,...

178 • HJC (Hellenic Journal of Cardiology)
Hellenic J Cardiol 2010; 51: 178-182
Case ReportCase Report
Manuscript received:August 1, 2009;Accepted:January 9, 2010.
Address:Ahmet Al Fagih
Department of Adult Cardiology,Prince Sultan Cardiac Center, Riyadh, Kingdom of Saudi Arabiae-mail: [email protected]
Key words: Congenital heart disease, dextrocardia, cardiac computed tomography.
Feasibility of Cardiac Resynchronization Therapy in a Patient with Complex Congenital Heart Disease and Dextrocardia, Facilitated by Cardiac Computed Tomography and Coronary Sinus VenographyAhmet Al FAgih1, KhAled Al NAjAshi2, KhAled dAgriri2, AbdulmAjeed Al OtAy2, sAleh Ahmed Al ghAmdi2
1Department of Adult Cardiology, 2Department of Pediatric Cardiology, Prince Sultan Cardiac Center, Riyadh, Kingdom of Saudi Arabia
We describe a case with pacemaker implantation for cardiac resynchronization therapy (CRT) in a patient with complex congenital heart disease, facilitated by cardiac computed tomography (CT) and coronary sinus (CS) venography. A 37-year-old male presented with congenitally corrected transposition of the great arter-ies and mesocardia, along with a history of two open heart surgeries (closure of atrial septal defects and a ventricular septal defect, and pulmonary valvectomy at age 7; mechanical tricuspid valve replacement at age 13). He showed symptoms of progressive heart failure (NYHA class III) with significant impairment of the systemic right ventricular function. He also developed permanent atrial fibrillation with a junctional rhythm at a rate of 45 beats per minute. Biventricular pacing without an atrial lead was considered to be the best option available. CRT implantation was facilitated by proper identification of CS anatomy utilizing cardiac CT and CS venography and was performed without any complications. At follow up, a postero-anterior chest X-ray showed the final position of the right-sided ventricular (left ventricular morphology) lead pointing to the apex and the left ventricular lead at the posterolateral aspect of the systemic ventricle (right ventricular morphology).
A dult patients with congenital heart disease represent an expanding po-pulation that is growing at a rate
of 5% per annum.1 Ventricular dysfunc-tion is common in adult congenital heart disease patients who have a systemic right ventricle (RV) and is related to electrome-chanical dyssynchrony.2-4 Over 25% of such individuals ultimately progress to symp-tomatic heart failure, which is occasionally refractory to drug therapy and is associated with substantial morbidity and mortality.4 Therefore, identification of novel therapeu-tic strategies in these patients is of critical importance.
Permanent pacemaker leads may be im-planted either epicardially or transvenously in infants as well as older children.5 Patients with a systemic RV may require conven-tional pacemaker therapy,6 which in the presence of ventricular dysfunction and con- duction disease may further compromise cardiac performance.7,8 Hence, devices ca- pable of combining conventional pacing with modern functions geared towards ame-liorating ventricular function seem to offer an obvious advantage.
Although cardiac resynchronization therapy (CRT) is rapidly emerging as an effective strategy for managing ventricular

(Hellenic Journal of Cardiology) HJC • 179
Resynchronization in Complex Congenital Heart Disease
dysfunction and heart failure associated with congeni-tal heart disease, its usage in these patients is limited in terms of patient numbers and follow up.9 Experi-ence in transvenous CRT implantation is limited fur-ther by distorted coronary sinus (CS) anatomy and its tributaries due to previous surgeries and intractable heart failure. However, this route may be feasible for future lead implantation at a greater age.5
In this report, we described the feasibility of trans-venous CRT implantation in a patient with congenitally corrected transposition of the great arteries (ccTGA) and mesocardia, along with a history of two open heart surgeries.
Case presentation
A 37-year-old male presented with ccTGA and meso-cardia, along with a history of two open heart surger-ies. At the age of seven years, he underwent surgical closure of atrial septal defects and a ventricular septal defect, and pulmonary valvectomy. He also underwent mechanical tricuspid valve/systemic valve (TV) replace-ment at the age of 13 years. On follow up he showed symptoms of progressive heart failure with significant impairment of systemic RV (RV morphology) func-
tion. He also developed permanent atrial fibrillation with junctional rhythm at a rate of 45 beats per minute. In view of the slow ventricular response and concomi-tant severe heart failure (NYHA class III) symptoms, biventricular pacing without an atrial lead was consid-ered to be the best option available. It was anticipated that the abnormal CS anatomy would be more difficult in this particular patient, hence cardiac computed to-mographic (CT) angiography was performed as a road to implantation procedure (Figure 1).
CRT was performed as a two-step procedure in a single session. Firstly, CS angiography was performed through the right femoral vein approach using a pre-shaped long sheath (St. Jude Medical, SL3) and oc-clusive balloon (Medtronic, Attain) to plan for proper systemic ventricular lead positioning (Figure 2).10 Occlusive venography showed disturbed CS anatomy with only one suitable posterolateral branch, as well as the incidental finding of a fistula connecting the CS to the left atrium (Figure 2).
Subsequently, two axillary vein accesses were ob-tained, and then the RV lead (Medtronic, Sprint Qua-tro, 6947) was implanted in the right-sided ventricular apex (LV morphology). The LV delivery system (9F safe sheath CS Guide) was introduced into right
LV RV
IVC RA
LA
CS
TV
DAO
LV RV
RAIVC
CSDAo
LA
LV RV
RAIVC
CSDAo
LA
Figure 1. An axial computed tomography angiographic view depicting (A) artificial tricuspid valve (TV), right atrium (RA), inferior vena cava (IVC), small fistula into the left atrium (LA). In the three dimensional reconstruction (B) the coronary sinus is color coded in blue. DAO – descending aorta; LV – left ventricle; RV – right ventricle.

180 • HJC (Hellenic Journal of Cardiology)
A. Al Fagih et al
atrium, then into the CS with the help of a 6F Judkins right catheter and 0.035” terumo guide wire (Figure 3). Another CS venography was obtained through the safe sheath to rule out any dissection and to ensure
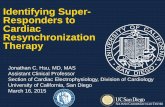
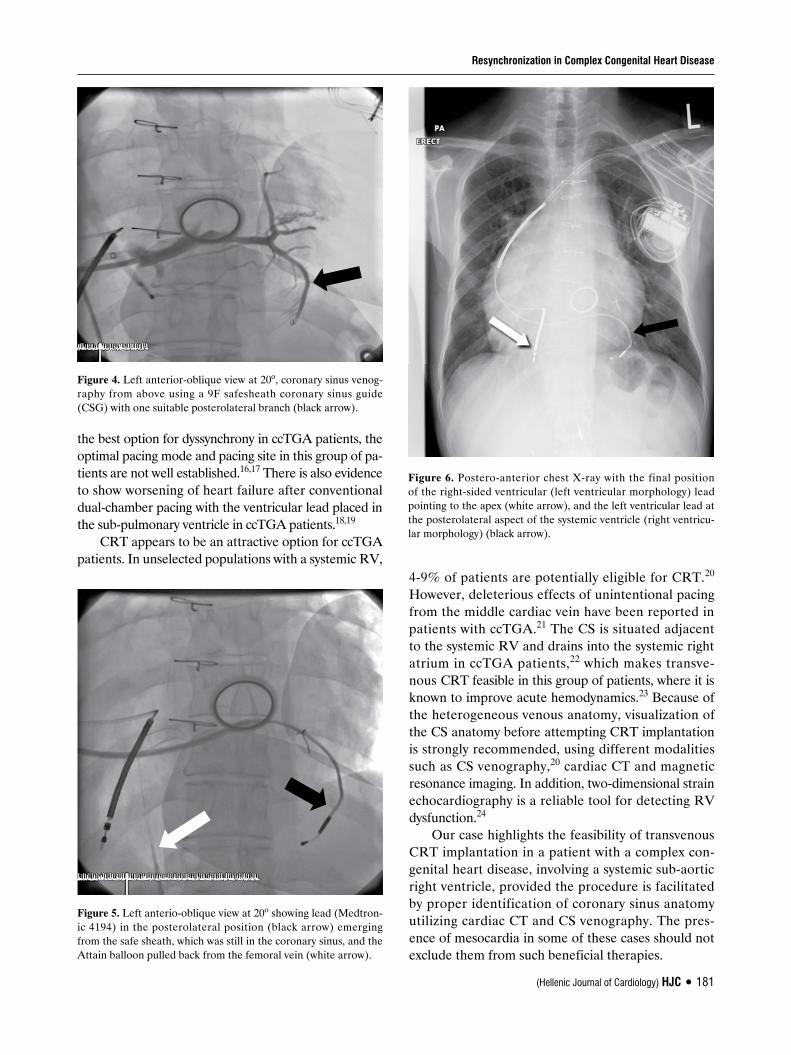
that the sheath was in the true lumen (Figure 4). A bipolar 4194 LV pacing lead (Medtronic) was then in-troduced into the target vein without much difficulty. The SL3 with the Attain balloon were pulled back through the femoral vein before the safe sheath was withdrawn under fluoroscopy guidance (Figure 5).
The procedure was then completed without any complications. At follow up, the postero-anterior chest X-ray showed the final position of the right-sided ven-tricular (LV morphology) lead pointing to the apex and the LV lead at the postero-lateral aspect of the systemic ventricle (RV morphology) (Figure 6).
Discussion
Congenitally corrected transposition of the great arter-ies accounts for 0.5% of all cases of congenital heart disease, of which 30% might be associated with me-socardia. Additional anomalies may be present, such as ventricular septal defect in 60-80%, sub-pulmonary ventricle outflow obstruction in 30-50% and TV ab-normalities in 14-56% of patients.11,12 Rhythm distur-bances can develop in up to 2% of this population per year, with or without surgical intervention.13,14 In most of these cases, failure of the sub-aortic ventricle usually appears in the third decade of life, with or without cor-rective or palliative surgeries.15
Although pacemaker implantation is considered
Figure 2. Left anterio-oblique view at 45o during occlusive coro-nary sinus venography shows the fistula (black arrow) and the posterolateral branch (white open arrow), as well as the metallic tricuspid valve (white arrow) and the right-sided ventricular tem-porary pacemaker (black open arrow).
Figure 3. Left anterio-oblique view at 25o during coronary sinus (CS) engagement using a 9F safesheath coronary sinus guide (CSG) (white arrow) with a 6F Judkins right catheter (black arrow) and 0.035” terumo guide wire. (a) Negotiating the CS ostium with the guide wire. (b) Guide wire, Judkins right and the safe sheath coronary sinus guide (CSG) inside the CS (striped arrow).
(Hellenic Journal of Cardiology) HJC • 181
Resynchronization in Complex Congenital Heart Disease
the best option for dyssynchrony in ccTGA patients, the optimal pacing mode and pacing site in this group of pa-tients are not well established.16,17 There is also evidence to show worsening of heart failure after conventional dual-chamber pacing with the ventricular lead placed in the sub-pulmonary ventricle in ccTGA patients.18,19
CRT appears to be an attractive option for ccTGA patients. In unselected populations with a systemic RV,
4-9% of patients are potentially eligible for CRT.20 However, deleterious effects of unintentional pacing from the middle cardiac vein have been reported in patients with ccTGA.21 The CS is situated adjacent to the systemic RV and drains into the systemic right atrium in ccTGA patients,22 which makes transve-nous CRT feasible in this group of patients, where it is known to improve acute hemodynamics.23 Because of the heterogeneous venous anatomy, visualization of the CS anatomy before attempting CRT implantation is strongly recommended, using different modalities such as CS venography,20 cardiac CT and magnetic resonance imaging. In addition, two-dimensional strain echocardiography is a reliable tool for detecting RV dysfunction.24
Our case highlights the feasibility of transvenous CRT implantation in a patient with a complex con-genital heart disease, involving a systemic sub-aortic right ventricle, provided the procedure is facilitated by proper identification of coronary sinus anatomy utilizing cardiac CT and CS venography. The pres-ence of mesocardia in some of these cases should not exclude them from such beneficial therapies.
Figure 4. Left anterior-oblique view at 20o, coronary sinus venog-raphy from above using a 9F safesheath coronary sinus guide (CSG) with one suitable posterolateral branch (black arrow).
Figure 5. Left anterio-oblique view at 20o showing lead (Medtron-ic 4194) in the posterolateral position (black arrow) emerging from the safe sheath, which was still in the coronary sinus, and the Attain balloon pulled back from the femoral vein (white arrow).
Figure 6. Postero-anterior chest X-ray with the final position of the right-sided ventricular (left ventricular morphology) lead pointing to the apex (white arrow), and the left ventricular lead at the posterolateral aspect of the systemic ventricle (right ventricu-lar morphology) (black arrow).

182 • HJC (Hellenic Journal of Cardiology)
A. Al Fagih et al
References
Brickner ME, Hillis LD, Lange RA. Congenital heart disease 1. in adults. First of two parts. N Engl J Med. 2000; 342: 256-263.Janousek J, Tomek V, Chaloupeck� VA, et al. Cardiac resyn-2. chronization therapy: a novel adjunct to the treatment and prevention of systemic right ventricular failure. J Am Coll Cardiol. 2004; 44: 1927-1931.Li W, Hornung TS, Francis DP, et al. Relation of biventricu-3. lar function quantified by stress echocardiography to cardio-pulmonary exercise capacity in adults with Mustard (atrial switch) procedure for transposition of the great arteries. Circulation. 2004; 110: 1380-1386.Piran S, Veldtman G, Siu S, Webb GD, Liu PP. Heart failure 4. and ventricular dysfunction in patients with single or systemic right ventricles. Circulation. 2002; 105: 1189-1194.Loukopoulou SN, Eleftherakis NG, Kourtesis AN, Thanopo-5. ulos BD. Combined epicardial and transvenous pacing in an infant with operated complex congenital heart disease and permanent epicardial DDD pacemaker as treatment of dys-function of the epicardial ventricular lead. Hellenic J Cardiol. 2009; 50: 68-72.Oechslin E, Jenni R. 40 years after the first atrial switch 6. procedure in patients with transposition of the great arteries: long-term results in Toronto and Zurich. Thorac Cardiovasc Surg. 2000; 48: 233-237.Janousek J, Tomek V, Chaloupecky V, Gebauer RA. Dilated 7. cardiomyopathy associated with dual-chamber pacing in in-fants: improvement through either left ventricular cardiac resynchronization or programming the pacemaker off allow-ing intrinsic normal conduction. J Cardiovasc Electrophysiol. 2004; 15: 470-474.Thambo JB, Bordachar P, Garrigue S, et al. Detrimental 8. ventricular remodeling in patients with congenital complete heart block and chronic right ventricular apical pacing. Circu-lation. 2004; 110: 3766-3772.Kiesewetter C, Michael K, Morgan J, Veldtman GR. Left 9. ventricular dysfunction after cardiac resynchronization thera-py in congenital heart disease patients with a failing systemic right ventricle. Pacing Clin Electrophysiol. 2008; 31: 159-162.Al-Khadra AS. Use of preshaped sheath to plan and facilitate 10. cannulation of the coronary sinus for the implantation of cardiac resynchronization therapy devices: preshaped sheath for implantation of biventricular devices. Pacing Clin Electro-physiol. 2005; 28: 489-492.Anderson KR, Danielson GK, McGoon DW, Lie JT. Eb-11. stein's anomaly of the left-sided tricuspid valve. Pathological anatomy of the valvular malformation. Circulation. 1978; 58: I87-91.Allwork SP, Bentall HH, Becker AE. Congenitally corrected 12.
transposition of the great arteries. Morphologic study of 32 cases. Am J Cardiol. 1976; 38: 910-912.Huhta JC, Danielson GK, Ritter DG, Ilstrup DM. Survival in 13. atrioventricular discordance. Pediatr Cardiol. 1985; 6: 57-60.McGrath LB, Kirklin JW, Blackstone EH, Pacifico AD, Kirk-14. lin JK, Bargeron LM. Death and other events after cardiac repair in discordant atrioventricular connection. J Thorac Cardiovasc Surg. 1985; 90: 711-728.Voskuil M, Hazekamp MG, Kroft LJ, et al. Postsurgical 15. course of patients with congenitally corrected transposition of the great arteries. Am J Cardiol. 1999; 83: 558-562.Karpawich PP. New directions in pacemaker therapy among 16. children and adult patients with congenital heart disease. Ex-pert Rev Cardiovasc Ther. 2007; 5: 611-613.Dubin AM, Janousek J, Rhee E, et al. Resynchronization 17. therapy in pediatric and congenital heart disease patients: an international multicenter study. J Am Coll Cardiol. 2005; 46: 2277-2283.Rodr�guez-Cruz E, Karpawich PP, Lieberman RA, Tanteng-18. co MV. Biventricular pacing as alternative therapy for dilated cardiomyopathy associated with congenital heart disease. Pacing Clin Electrophysiol. 2001; 24: 235-237.Van de Veire NR, Blom NA, Holman ER, Schalij MJ, Bax 19. JJ. Triplane tissue Doppler imaging to evaluate mechanical dyssynchrony before and after cardiac resynchronization in a patient with congenitally corrected transposition of the great arteries. J Cardiovasc Electrophysiol. 2007; 18: 222-225.Diller G-P, Okonko D, Uebing A, Ho SY, Gatzoulis MA. 20. Cardiac resynchronization therapy for adult congenital heart disease patients with a systemic right ventricle: analysis of feasibility and review of early experience. Europace. 2006; 8: 267-272.Przybylski A, Kowalski M, Maciag A, Szumowski L. Deleteri-21. ous effect of unintentional pacing from the middle cardiac vein in a patient with congenitally corrected transposition of the great arteries and ventricular septal defect. The beneficial effect of cardiac resynchronization therapy after heart sur-gery. J Interv Card Electrophysiol. 2009; 24: 67-70.Piran S, Veldtman G, Siu S, Webb GD, Liu PP. Heart failure 22. and ventricular dysfunction in patients with single or systemic right ventricles. Circulation. 2002; 105: 1189-1194.Diller G-P, Okonko D, Uebing A, Ho SY, Gatzoulis MA. 23. Cardiac resynchronization therapy for adult congenital heart disease patients with a systemic right ventricle: analysis of feasibility and review of early experience. Europace. 2006; 8: 267-272.Kalogeropoulos AP, Georgiopoulou VV, Giamouzis G, et al. 24. Myocardial deformation imaging of the systemic right ven-tricle by two-dimensional strain echocardiography in patients with d-transposition of the great arteries. Hellenic J Cardiol. 2009; 50: 275-282.




![Dextrocardia with Situs Inversus, Atrio-ventricular and ...dextrocardia to be associated with situs solitus in 64%, situs inversus in 27%, and situs ambiguous in 9% [2]. In our case](https://static.fdocuments.in/doc/165x107/608c25297b80eb7d6b550573/dextrocardia-with-situs-inversus-atrio-ventricular-and-dextrocardia-to-be-associated.jpg)