
Fear in the Womb: The E ects of ... - uni-bielefeld.de · the al-Aqsa Intifada.5 Using data from...
36
“Fear in the Womb”: The Effects of Terrorism on Birth Outcomes in Spain * Climent Quintana-Domeque University of Oxford and IZA Pedro Rodenas Universitat d’Alacant February 2014 Preliminary and Incomplete Abstract We study the effects of terrorism in Spain on birth outcomes, focusing on terror- ism perpetrated by ETA (Euskadi ta Askatasuna or Basque Homeland and Freedom), combining information on the number of ETA casualties from The Victims of ETA Dataset with the individual birth records from the national registry of live births in Spain, elaborated by the Instituto Nacional de Estad´ ıstica. We focus on live births conceived between January 1980 and February 2003 and find that in utero exposure to terrorism early in pregnancy (1st trimester), as measured by the number of ETA- bomb casualties, has detrimental effects on birth outcomes: in terms of average birth weight (lower), the prevalence of low birth weight (higher) and the fraction of normal babies (lower). Our results are robust to a battery of robustness checks (e.g., measur- ing exposure to terrorism using date of birth instead of estimated conception date). Crucially, and in support of our identification strategy, the number of ETA-bomb ca- sualties after birth does not predict any of the birth outcomes under analysis, and virtually the same estimates are obtained when controlling for economic conditions (as captured by total unemployment rates) in each of the trimester of pregnancy. We do not find evidence of migration responses (in terms of population responses to last year terrorist activity), but both the number of live births and the number of fetal deaths increase with the number of ETA-bomb casualties. Given the increase in fetal deaths, the estimated effects of terrorism on birth outcomes for live births are likely to be downward biased (if anything) due to selective mortality. JEL Classification Codes : I12, J13. Keywords : Stress, Pregnancy, Terrorism, Birth Weight, Spain. * Quintana-Domeque (corresponding author): University of Oxford, Department of Economics, Manor Road Building, Manor Road, Oxford OX1 3UQ, United Kingdom; [email protected]. The usual disclaimers apply.
Transcript of Fear in the Womb: The E ects of ... - uni-bielefeld.de · the al-Aqsa Intifada.5 Using data from...

“Fear in the Womb”:The Effects of Terrorism on Birth Outcomes in Spain∗
Climent Quintana-DomequeUniversity of Oxford and IZA
Pedro RodenasUniversitat d’Alacant
February 2014
Preliminary and Incomplete
Abstract
We study the effects of terrorism in Spain on birth outcomes, focusing on terror-ism perpetrated by ETA (Euskadi ta Askatasuna or Basque Homeland and Freedom),combining information on the number of ETA casualties from The Victims of ETADataset with the individual birth records from the national registry of live births inSpain, elaborated by the Instituto Nacional de Estadıstica. We focus on live birthsconceived between January 1980 and February 2003 and find that in utero exposureto terrorism early in pregnancy (1st trimester), as measured by the number of ETA-bomb casualties, has detrimental effects on birth outcomes: in terms of average birthweight (lower), the prevalence of low birth weight (higher) and the fraction of normalbabies (lower). Our results are robust to a battery of robustness checks (e.g., measur-ing exposure to terrorism using date of birth instead of estimated conception date).Crucially, and in support of our identification strategy, the number of ETA-bomb ca-sualties after birth does not predict any of the birth outcomes under analysis, andvirtually the same estimates are obtained when controlling for economic conditions(as captured by total unemployment rates) in each of the trimester of pregnancy. Wedo not find evidence of migration responses (in terms of population responses to lastyear terrorist activity), but both the number of live births and the number of fetaldeaths increase with the number of ETA-bomb casualties. Given the increase in fetaldeaths, the estimated effects of terrorism on birth outcomes for live births are likelyto be downward biased (if anything) due to selective mortality.
JEL Classification Codes : I12, J13.Keywords : Stress, Pregnancy, Terrorism, Birth Weight, Spain.
∗Quintana-Domeque (corresponding author): University of Oxford, Department of Economics, Manor Road Building,Manor Road, Oxford OX1 3UQ, United Kingdom; [email protected]. The usual disclaimers apply.

“The ordinary textual meaning of “terrorism” refers to extreme fear”.
Ben Saul. The Challenge of Defining Terrorism, 2012.
1 Introduction
Terrorism and birth outcomes. According to Saul (2012), the best definition of
terrorism confines to violence committed to intimidate a population or coerce government
or international organizations in the name of a political, religious or ideological purpose.
Terrorism is one of today’s most important challenges faced by governments (and societies)
around the world. Terrorists seek to spread fear, influence public opinion, disrupt the econ-
omy, and change government policies in their target countries. Not surprisingly, several
United Nations resolutions acknowledge that terrorism seriously undermines human rights,
jeopardizes political order and peaceful, deliberative politics, and can threaten (interna-
tional) peace and security.
Terrorism has not escaped economists’ attention. Indeed, economists have been studying
the “economic” consequences of terrorism (as well as its causes) for several years (e.g.,
Krueger, 2007). More recently (health) economists have been inquiring about other “non-
economic” consequences of terrorism, such as its impact on birth outcomes (e.g., Brown,
2012), prompted by the existing and still growing research field on the role of prenatal
shocks in predicting not only birth but also long-term outcomes (e.g., Almond and Currie,
2011). But why birth outcomes should be affected by terrorism?
Terrorist violence involves stress and anxiety responses (e.g., Nijdam et al., 2010), and
one particular vulnerable group to stress responses is that of pregnant women.1 Women
who experience stress in the early stages of pregnancy are at increased risk of having a low
birth weight child (e.g., Beydoun and Saftlas, 2008).2
1These responses may lead to significant psychiatric disorders (e.g., Danieli, Brom and Sills, 2005; Whal-ley and Brewin, 2007).
2Stress during pregnancy could have negative effects on the fetus through neuroendocrine changes,changes in immune function, and/or through behavioral channels (Dunkel-Schetter, 2011).
1

The connection between child health (or birth outcomes) and “terrorism” has been
investigated in very different contexts: landmine explosions in Colombia (Camacho, 2008),
the September 11 attacks in the United States (Brown, 2012; Eccleston, 2011), and armed
conflict in West Bank and Gaza (Mansour and Rees, 2012). Infants exposed to terrorist
attacks or armed conflict during the prenatal period tend to be smaller at birth, and low
birth-weight is a predictor of both child health (e.g., McCormick, 1985; Pollack and Divon,
1992) and long-term outcomes such as educational attainment, labor market outcomes,
and adult health (Behrman and Rosenzweig, 2004 ; Black, Devereux and Salvanes, 2007;
Currie and Hyson, 1999; Currie, Garces and Thomas, 2002; Case, Fertig, and Paxson, 2005;
Johnson and Schoeni, 2011).
This paper. We study the effects of terrorism in Spain on birth outcomes. In particular,
we focus on terrorism perpetrated by ETA (Euskadi ta Askatasuna or Basque Homeland and
Freedom), a terrorist organization who seeks to gain independence for a Basque homeland
in northern Spain and southern France, and who announced “the definitive cessation of
its armed activity” in October 2011. While no attack has been perpetrated by ETA since
then, the Barometro del CIS (2013) opinion polls show that ETA terrorism has been one
of the main worries of Spaniards during the last 30 years, only after unemployment and
sometimes ranking above it.
We combine information on the number of ETA casualties from The Victims of ETA
Dataset (2007), elaborated by de la Calle and Sanchez-Cuenca, with the individual birth
records from the national registry of live births in Spain, elaborated by the Instituto Nacional
de Estadıstica. We focus on live births conceived between January 1980 and February 2003,
a period characterized by attrition attacks3, and investigate the impact of ETA terrorism
(and in particular of the number of bomb casualties) in each trimester of pregnancy on a
3Attacks that took take place in more distant locations than the territory the terrorist group hopesto eventually govern and are aimed at exhausting the government economically, politically, and ultimatelypsychologically into agreeing to group demands (de la Calle and Sanchez-Cuenca, 2006; LaFree et al., 2012).Prior to 1980 the registry of live births does not provide information on birth weight. The upper limit avoidsMadrid train bombings (March 11 2004) interfering with our estimates.
2

battery of birth outcomes: birth weight (in grams), low birth weight (1 if birth weight less
than 2500 grams), normality (absence of complications of labor and delivery) and gender of
the child.
Our identification is based on a difference-in-differences strategy across provinces (50
geographical regions) and time (more than 275 conception month-years). In addition, our
most complete econometric specification include several socio-demographic and maternal
controls (mother’s age, order of birth, mother’s marital status, mother’s occupation, father’s
occupation, municipality size, place of birth) and province-specific linear (month-by-year)
time trends. It is important to highlight that one crucial part of our analysis is to identify
the relevant trimesters of pregnancy (if any).4
Our contribution in perspective. Several studies in the United States have inves-
tigated the consequences of September 11 on birth outcomes. Perhaps, one of the most
carefully executed analyses has been conducted by Brown (2012). He finds that children ex-
posed while in utero to the terrorist attacks of September 11 were born significantly smaller
and earlier than previous cohorts. However, the external validity of estimates based on these
attacks is questionable on many different grounds. First, September 11 was just one shock
event, while the attacks of ETA (and many others terrorist groups) are spread over a long
time span (in our analysis, more than 20 years). Second, and perhaps more importantly,
September 11 was not only a source of acute maternal stress but also had negative pollution
and resource shocks (Bram, Orr and Rapaport, 2002; Landrigan, 2001), which are known
to have negative consequences on child health. While Brown excludes residents of the at-
tacked areas to remove these other influences, part of the relevant effect of stress on birth
outcomes is missed by using this approach. In our context, these other potential channels
are negligible.
4The medical literature provides mixed evidence on the relative importance of early versus late pregnancystress exposure (Schulte et al., 1990; de Weerth and Buitelaar, 2005; Hedegaard et al., 1993; Schneider etal., 1999). Economists tend to find that sources of acute maternal stress tend to affect birth outcomesnegatively when they occur early in pregnancy.
3

Another piece of relevant research for understanding the contribution of our paper is
the one by Mansour and Rees (2012), who provide perhaps the first study on the effect of
intrauterine exposure to armed conflict on pregnancy outcomes. Their evidence comes from
the al-Aqsa Intifada.5 Using data from the Palestinian Demographic Health Survey 2004,
they find that an additional conflict-related fatality 9-6 months before birth is associated
with a modest increase in the probability of having a child who weighed less than 2500g.
While this is a very relevant study, and the most comparable to ours in that they
try to estimate the impact of number of casualties per trimester of pregnancy on birth
outcomes, it suffers from certain limitations that we can overcome. First, their sample size
is very small (hundreds or thousands), while here we use administrative records (millions).
Second, different to us, they do not observe gestational length, so that they measure exposure
by counting backwards from the date of birth, which means that exposure in the first
trimester is likely going to be assigned with measurement error for pre-term babies (Currie
and Rossin-Slater, 2013). Third, while the al-Aqsa Intifada inflicted intense psychological
damage on noncombatants living in the West Bank and Gaza, Mansour and Rees recognize
that other channels apart from stress, namely, malnutrition, physical exertion and limited
access to prenatal care, due to curfews, border closures and road blocks, could affect birth
weight.6 These channels are certainly negligible in our context. Finally, they only have 10
administrative districts, which makes difficult to use “standard” clustering methods. We
have instead 50 provinces, not a very large number, but larger than 42, the rule of thumb
in Angrist and Pischke (2009).
Last but not least, our study is unique in that it is the first to assess the effects of
terrorism on birth outcomes in a developed country by using administrative records (more
than 6 million live births) and keeping track of a terrorist process (more than 20 years). In
5The name commonly used to describe a series of violent clashes between the Palestinians and Israel inthe time frame between 2000 and 2004.
6For instance, they note that many women of reproductive age living in the Occupied Territories werenot consuming sufficient meat, poultry and dairy products at the height of the al-Aqsa Intifada. They tryto assess the importance of these channels.
4

addition, our study breaks new ground by extending the analysis of the effects of terrorism
in Spain to the realm of early life shocks, complementing the two main existing pieces
of research on the economic and political consequences of terrorism in Spanish soil: The
economic analysis of Abadie and Gardeazabal (2003) and the study by Montalvo (2011) on
the electoral consequences of the Madrid train bombings of March 11 of 2004.7
Findings. We find that in utero exposure to terrorism early in pregnancy (1st trimester),
as measured by the number of ETA-bomb casualties, has detrimental effects on birth out-
comes: in terms of average birth weight (lower), the prevalence of low birth weight (higher)
and the fraction of normal babies (lower). Our results are robust to measuring exposure
to terrorism using date of birth instead of estimated conception date. In support of our
identification strategy, the number of ETA-bomb casualties after birth does not predict any
of the birth outcomes under analysis, and virtually the same estimates are obtained when
controlling for economic conditions (as captured by total unemployment rates) in each of
the trimester of pregnancy. Excluding either the Basque Country (the region with the high-
est terrorist activity) or the “safe” provinces (regions without any ETA-bomb casualty), we
obtain similar results. Two other interesting results are: (i) the effects seem to be driven
by trimesters with intense terrorism (say 10 ETA-bomb casualties or more), rather than by
trimesters with some terrorism (say 1 ETA-bomb casualty or more), and (ii) the effects of
terrorism are more “intense” (albeit not statistically significant) for children born to moth-
ers whose husbands (partners) are members of the armed-forces. Finally, using aggregate
data, we investigate migration, fertility and (fetal) mortality responses. While we do not
find evidence of migration responses (in terms of population responses to last year terrorist
activity), we find that both the number of live births and the number of fetal deaths increase
with the number of ETA-bomb casualties. Given the increase in fetal deaths, the estimated
7Abadie and Gardeazabal find that, after the outbreak of ETA-terrorism, per capita GDP in the BasqueCountry declined about 10 percentage points relative to a region without terrorism, while Montalvo showsthat the Madrid train bombings of March 11 of 2004, the worst terrorist attack in Spain (with 191 deathsand more than 2000 injured), affected the electoral outcomes of the Spanish General Election celebrated 3days after.
5

effects of terrorism on birth outcomes for live births are likely to be downward biased (if
anything) due to selective mortality.
The rest of the paper proceeds as follows. Section 2 describes the main data sources
and provide some descriptive statistics. Section 3 contains the empirical strategy. Section
4 presents the results of our analysis of live birth outcomes and a battery of extensions
and robustness checks. Section 5 studies the effects on fertility and (fetal) mortality and
migration responses. Section 6 provides a conceptual framework to measure the “trade-off”
between terrorism and unemployment in the production of child health and an estimate of
it. Finally, Section 7 concludes.
2 Data
2.1 Main Sources
The national registry of live births in Spain (Instituto Nacional de Estadıstica).8
The unit of observation in this dataset is the live birth. For each live birth, we have in-
formation on its date of occurrence (month and year), gender, weight, gestational length,
and normality (whether there were complications during the pregnancy or labor). How-
ever, there is no information on other child health metrics such as Apgar score or head
circumference. In addition, there is some demographic information on the mother of the
child (province of residence, age, parity history (number of births that she has had), mari-
tal status, and occupational status), but not on her risky behaviors (smoking or drinking),
prenatal visits, educational attainment or (family) income. When appropriate, there is also
information on his spouse: age and occupational status.
We use information on around 6.5 million births conceived between January 1980 and
February 2003.9 Following previous work on the determinants of birth weight, we focus on
8http://www.ine.es9Since conception length is not available for all live births, as a robustness check we also measure exposure
using date of birth. We have almost 10 million births born between January 1980 and December 2003.
6

mothers aged 15-49, exclude multiple births and those newborns whose weight was either
under 500 grams or above 9,000 grams. Moreover, following Currie and Rossin-Slater (2013),
those with gestational length below 26 weeks are also excluded.
The Victims of ETA Dataset (de la Calle and Sanchez-Cuenca).10 The unit of obser-
vation in this dataset is the ETA-victim casualty. It contains information on all casualties
caused by ETA during the period 1960-2006. For each casualty, there is information on
the name of the victim, the region of occurrence, time (day, month and year) and type
of attack (e.g., bomb or shooting). Our analysis will be focused on ETA-bomb casualties,
because from the point of view of the average mother in the population, she is more likely
to be concerned about attacks with (more) collateral victims (bombs) than about targeted
attacks (shooting).
2.2 Descriptive Statistics
We begin our empirical analysis presenting some descriptive statistics (averages) on birth
outcomes (panel A) and mother-pregnancy characteristics (panel B) by exposure to ETA-
bomb casualties during pregnancy in Table 1. This table has three columns. Column (1)
displays the average of the corresponding variable in each row for children unexposed to
ETA-bomb casualties during pregnancy, while column (2) focuses on children exposed to at
least one ETA-bomb casualty during pregnancy. Column (3) contains the (mean) difference
between the previous two columns (and its standard error).
[Insert Table 1 about here]
Panel A shows that children exposed to ETA-bomb casualties during pregnancy are on
average 36 grams (or 0.7 standard deviations) thinner; they are also 0.6 percentage points (or
6 per 1,000 live births) more likely to be low birth-weight babies and 2 percentage points (or
16 per 1,000 live births) less likely to be normally delivered; they are 1 percentage points (1
10http://www.march.es/ceacs/proyectos/dtv
7

per 1,000 live births) less likely to be males. Note that neither the fraction of available birth
weights (non-missing values) nor the fraction of premature babies is related to exposure to
ETA-bomb casualties during pregnancy.
Taken at face value, the estimates from panel A are consistent with exposure to terrorism
while in utero affecting birth outcomes negatively. However, exposed and unexposed children
may be different in many other dimensions apart from their exposure to bomb-casualties.
This is confirmed in panel B. For instance, mothers of babies exposed to ETA-bomb casu-
alties are more than half a year older than mother of unexposed babies, and their order of
births are also different. In addition, these descriptive statistics are not informative about
the relative importance of the timing of exposure (trimester). It is then crucial to account
for the (precise) timing of exposure and to use a proper identification strategy in order to
identify the impact of terrorism on birth outcomes.
3 Empirical Strategy
3.1 Counting forward from date of conception
We use the number of ETA-bomb casualties as our measure of terrorism intensity and
estimate regressions of the form
Yi,p,t = α + β1Casualties1p,t + β2Casualties
2p,t + β3Casualties
3p,t
+δp + γt + (θp × t) + τXi,p,t + ui,p,t
(1)
where Yi,p,t is the birth outcome corresponding to newborn i, whose mother’s province
of residence is p, conceived in the year-month t, CasualtiesTp,t is the number of ETA-bomb
casualties in trimester T of pregnancy in province p, and ui,p,t is a random error term.
Year-month of conception is estimated using the approach in Brown (2012): month of birth
minus gestational age minus 2 weeks divided by 4, and increased by 12 if the difference is
8

less than 1. Conception year is then either the year of birth or the birth year less one if the
conception month is larger than the birth month.11
Our most naıve regressions include both mother’s province of residence fixed effects (δp)
and year-month of conception fixed effects (γt), while our most complete regressions include
a vector of control variables (Xi,p,t) –birth order (parity) categories, mother’s age categories,
mother’s marital status indicator, mother’s occupational categories, father’s occupational
categories (with one category if not father), indicator for delivery in a hospital or clinic,
and size of the municipality of residence categories– and province-specific linear time (year-
month of conception) trends. The vector of parameters of interest is β = (β1, β2, β3),
which measures the sensitivity of infant health to prenatal terrorist activity in each of the
trimesters of pregnancy. Standard errors are clustered at the province level (50 provinces).
3.2 Counting backward from date of birth
In addition, since gestational length is not available for all live births (it is missing for
32% of live births) and in many instances is not available to the researcher, we also follow the
standard approach of measuring exposure by counting backwards from month of birth (e.g.,
Bozzoli and Quintana-Domeque, 2014; Mansour and Rees, 2012). We estimate regressions
of the form
Yi,p,t = α + β8−6Casualties8−6p,t + β5−3Casualties
5−3p,t + β2−0Casualties
2−0p,t
+δp + γt + (θp × t) + τXi,p,t + εi,p,t
(2)
where Yi,p,t is the birth outcome corresponding to newborn i, whose mother’s province
of residence is p, born in the year-month t, CasualtiesC−Ap,t is the number of ETA-bomb
casualties in C to A months before birth in province p, and εi,p,t is a random error term.
112 weeks are subtracted because conception usually occurs 2 weeks after the last normal menstrualperiod.
9

Our most naıve regressions include both mother’s province of residence fixed effects (δp) and
year-month of birth fixed effects (γt), while our most complete regressions include a vector
of control variables (Xi,p,t) and province-specific linear time (year-month of birth) trends.
As before, the vector of parameters of interest is β = (β8−6, β5−3, β2−0), which measures
the sensitivity of infant health to prenatal terrorist activity in each of the “approximately
measured” trimesters of pregnancy.
4 Effects on Birth Outcomes for Live Births
4.1 Main Regressions
Table 2 displays the main results of this paper. It contains a series of regressions for
four different birth outcomes –birth weight (in grams), and low birth-weight, normal and
male (indicators)– on the number of ETA-bomb casualties in each trimester of pregnancy
grouped into three different panels (A, B, C). While birth weight and low birth-weight
are standard birth outcomes, as pointed out recently by Currie and Rossin-Slater (2013),
measured effects of stressful events on these measures may be sensitive to specification, and
it is preferable to use more sensitive indicators of newborn health, such as the probability
of abnormal conditions of the newborn (here we use normal). Finally, and following Brown
(2012), we also consider gender as a potential outcome of exposure to terrorism while in
utero, since maternal stress may impact the sex ratio by reducing male births (Catalano et
al., 2006).
[Insert Table 2 about here]
Starting with panel A, which includes mother’s province of residence fixed effects and
year-month of conception fixed effects, we can see that an additional ETA-bomb casualty
in the first trimester of pregnancy (on average) decreases birth weight by around 0.7 grams,
increases the expected number of low birth-weights by around 0.2 per 1,000 live births,
10

and decreases the predicted number of normal deliveries (without pregnancy or labor com-
plications) by about 0.6 per 1,000 live births. In panel B we include socio-demographic
controls –mother’s age, birth order categories, mother’s occupational categories, father’s
occupational categories, mother’s marital status indicator, medical center/hospital delivery
indicator, and municipality size categories– and obtain similar results, both qualitatively
and quantitatively. Finally, to soak up any province-specific time trends, panel C adds the
interaction of mother’s province of residence fixed effects with a time trend (year-month
of conception). Remarkably enough, the statistical significance of our estimates survive
to this stringent adjustment.12 All point estimates remain in the same ballpark, but the
one concerning average birth weight, which gets reduced to almost one third of its original
magnitude.
The main takeaway of table 2 is that in utero exposure to terrorism early in pregnancy
(1st trimester) has detrimental effects on birth outcomes. According to our most conserva-
tive estimates, ten additional ETA-bomb casualties would decrease average birth weight by
about 3 grams (around 0.006 standard deviations) and increase low birth weight by about
1.5 per 1,000 live births. A more naıve picture would suggest instead effects of almost 7
grams (around 0.012 standard deviations) and about 1.9 per 1,000 live births. Both the
magnitudes of estimated effects and the fact that they are found for the first trimester
of pregnancy is consistent with the estimates available in the literature (Camacho, 2008;
Brown, 2012; Mansour and Rees, 2012).
Finally, since conception length is not available for all live births, in Table 3 we estimate
the same regressions but using only information on the date of birth as a robustness check.
The new point estimates are qualitatively very similar, which is quite reassuring given both
the different methodologies (date of birth versus date of conception) and the sample size
discrepancies. It seems that, if anything, using date of birth rather than conception date
results in attenuated estimated effects of terrorism on birth outcomes, something expected
12What is more, a new point estimate –the one corresponding to the number of fatalities in the 2ndtrimester of pregnancy– becomes statistically significant for the normal delivery outcome.
11

under (classical) measurement error in the trimester of pregnancy casualties variables.
[Insert Table 3 about here]
4.2 Falsification Test: Does Terrorism After Birth predict Birth
Outcomes?
Table 4 presents our placebo or falsification tests. In this table we re-estimate our most
complete econometric specification in Table 2 (panel C) for each birth outcome adding
either the number of ETA-bomb casualties in the first trimester after birth or the number
of ETA-bomb casualties in the first nine months after birth. If we were identifying acute
maternal stress shocks due to (unexpected) terrorism casualties, we should not find that
casualties after birth affect birth outcomes. The results in Table 2 show basically the same
results as in Table 2 (panel C) and, reassuringly, none of the point estimates on the placebo
variables is statistically significant at any conventional level.
[Insert Table 4 about here]
4.3 Confounding Economic Factors: In Utero Unemployment
Given that previous research has documented the negative economic consequences of
ETA-terrorism in Spain (Abadie and Gardeazabal, 2003), it may well be the case that our
trimester casualty variables are picking up the influence of resource (“economic”) shocks
rather than stress shocks. We assess such a possibility in Table 5, where we include the (to-
tal) unemployment rate corresponding to each trimester of pregnancy using data from the
Encuesta de Poblacion Activa.13 Two results stand out in this table. First, our estimates
are (almost) identical to those in Table 2 (panel C). Second, babies exposed to high unem-
ployment rates (in the first trimester of pregnancy) have a reduced incidence of low birth
13http://www.ine.es/inebaseDYN/epa30308
12

weight –a finding consistent with the empirical evidence in the US by Deheija and Lleras-
Muney (2004)–, tend to have a higher average birth weight, and are more likely to have
a normal delivery (without complications). This finding is consistent with an opportunity
cost of time selection story: High-educated (or more broadly, high socioeconomic status)
women are more likely to conceive during bad economic times than in good economic times
(and the opposite prevails for their low-educated counterparts).
[Insert Table 5 about here]
4.4 Excluding either The Basque Country or “Safe” Provinces
One may wonder whether our estimates are driven by just one region (the Basque Coun-
try is the one with the highest level of terrorist activity) and its three provinces (Alava,
Guipuzcoa, Vizcaya), so that the other provinces do not play any role in our analysis.
Another observer could also raise the concern that “healthy people” (with better health
outcomes) may migrate in response to terrorism from the Basque Country to other regions,
so that those exposed to terrorism in the Basque Country would tend to be negatively se-
lected. If that were the case, we would be overestimating the effect of terrorism. Table
6 shows that none of these possibilities is borne out in the data. Excluding the Basque
Country, we still obtain the same empirical results as in Table 2 (Panel C).
[Insert Table 6 about here]
By a similar token, we may inquire about what happens if we just focus on provinces
with at least one ETA-bomb casualty, so that we exclude “safe” provinces. This amounts
to excluding 35 out of 50 provinces. While clearly now clustered standard errors must be
taken with a grain of salt, the point estimates are similar to the ones reported in panel C
of Table 2.
[Insert Table 7 about here]
13

4.5 Heterogeneous Effects: Armed-Forces
While terrorism is likely to stress mothers exposed to it, clearly, some mothers are
more likely to suffer or perceive higher risks from it, either because of individual or group
heterogeneity. Ceteris paribus, one group of mothers that should be expected to respond to
terrorism in a more intense way is that whose partners (husbands) are in the police forces.
Unfortunately, our dataset does not allow us to identify the occupation of the husband to
the police force category (or level). Still, it provides information on whether the husband is
a member of the armed forces (“profesionales de las fuerzas armadas”). In Table 8 we broke
down our sample by father’s armed-forces (occupation) status. The two subsamples are very
different in size (1 to 75), but the qualitative results are quite spectacular: 11 out of 12 point
estimates (albeit almost all of them very imprecisely estimated, and hence not statistically
significant) are much larger in magnitude for babies born to armed-forces fathers than their
counterparts. For example, the point estimates corresponding to ETA-bomb casualties in
the first trimester of pregnancy of birth weight is −1.2 for armed-forces fathers versus −0.25
for other fathers: a 5 to 1 difference. Although not statistically significant, the effects of
terrorism are more “intense” for children born to mothers whose husbands (partners) are
members of the armed-forces.
[Insert Table 8 about here]
4.6 Non-linearities: Terrorism Intensity
So far we have been restricting the effect of ETA-bomb casualties to be linear. We now
explore the effects of terrorism by intensity in Table 9. We replace our count ETA-bomb
casualties’ variables with variables taking value 1 if the number of ETA-bomb casualties in
the trimester is equal or higher than 10 (and 0 otherwise) in panel A, and with variables
taking value 1 if the number of ETA-bomb casualties in the trimester is equal or higher than
1 (and 0 otherwise) in panel B. The results reveal that babies exposed in the first trimester
14

of pregnancy to 10 casualties or more are on average (almost) 10 grams thinner. Similarly,
the number of babies that are low birth-weight increase by (almost) 7 per 1,000 live births
when exposed to 10 casualties or more during the first trimester of pregnancy. The evidence
reported in this table indicates that intense terrorism is the responsible for the previously
estimated effects.
[Insert Table 9 about here]
5 Effects on Mortality, Fertility and Migration
5.1 Effects on Mortality and Fertility Responses
The analysis conducted up to that point has investigated the impact of exposure to
terrorism on birth outcomes for live births. We now turn to the study the impact of
exposure to terrorism on mortality, and in particular, fetal deaths.14 We aggregate (count
the number of) fetal deaths at the year-month-province level, so that the total number of
observations is 13,900. The results are presented in Table 10.
[Insert Table 10 about here]
The first column shows that one additional ETA-bomb casualty in the first trimester of
pregnancy increases fetal deaths by 0.2, while the increase is around 0.15 if the extra casualty
happens in the third trimester of pregnancy. We obtain virtually the same estimates if we
control for unemployment rates in each of trimester of pregnancy, and consistent with our
previous findings, higher unemployment rates are associated with a smaller number of fetal
deaths. Given the increase in fetal deaths, our previous estimates of the effects of terrorism
on birth outcomes are likely to be downward biased (if anything) due to selective mortality
14We investigate fetal deaths because is a natural extension in terms of linking them to in utero terrorismexposure. Note that neonatal deaths or post-neonatal deaths are likely to be affected by terrorist activityafter birth. Late Fetal Deaths Microdata available at http://www.ine.es/prodyser
15

(Bozzoli, Deaton, and Quintana-Domeque, 2009). In that sense, our previous estimates on
live birth outcomes can be understood as lower bounds.
While the first two columns look at mortality (fetal deaths), in columns (3) and (4) we
inquire into fertility responses. An additional casualty translates into 20 to 30 extra live
births, depending on the trimester of pregnancy. Interestingly, the effect is present for all
trimesters of pregnancy. The effects of terrorism on both fetal deaths and live birth are of
a similar order of magnitude: around 0.05 and 0.06 standard deviations.
5.2 Migration responses
Migration could be interfering with our identification strategy (and our estimates) if
residents (and in particular pregnant mothers) decided to migrate because of terrorism
from a region with terrorist activity (say the Basque Country) to one without terrorist
activity. While our results are robust to either excluding the Basque Country or “safe”
regions (provinces without any ETA-bomb casualty over 1980-2003), we have no way to
track mothers in our administrative records, so that we cannot study mothers’ migration
behavior. We can nevertheless investigate whether population sizes at the province level
for a given year can be predicted by the number of ETA-bomb casualties in the same
province one year before.15 The result of this analysis is presented in Table 11. For the
sake of comparison, in column (1) we replicate our regressions for live births using log(live
births), which gives a sense of how to compare the magnitudes for the estimates on the
log(population) dependent variables. Columns from (2) to (4), for the age-prime group,
age-prime females, and age-prime males, show that the number of ETA-bomb casualties
does not predict (log) population size for any of these groups (or any others).16
[Insert Table 11 about here]
15Population data obtained from Estimaciones Intercensales de Poblacion (INE).16Results available upon request.
16

6 The trade-off between unemployment and terrorism
6.1 Conceptual Framework
(Child) health is a multidimensional concept. Suppose that we can classify babies as
being healthy (h = 1) or unhealthy (h = 0), and that h is a function of several (observable)
inputs, say x1 and x2, and several (unobservable to the econometrician) inputs, say η. In
other words, we postulate the following child health production function
h = f(x1, x2) + η (3)
While we do not observe h, we observe two measures of babies’ health, namely h1 (a binary
measure of non-low birth weight: 1 if normal weight, 0 if low-birth weight) and h2 (a binary
measure of normality: 1 if normal delivery/pregnancy, 0 if not), such that
h1 = g(h) + u1 (4)
h2 = v(h) + u2 (5)
Substituting (3) into (4) and (5), we obtain
h1 = g(f(x1, x2) + η) + u1 (6)
h2 = v(f(x1, x2) + η) + u2 (7)
So that, the marginal rate of technical substitution (MRTS) between inputs x1 and x2 (i.e.,
how much x1 have to decrease if x2 increases by one extra unit)
MRTS =
∂f∂x1
∂f∂x2
(8)
17

is overidentified, since∂h1
∂x1
∂h1
∂x2
=∂h2
∂x1
∂h2
∂x2
= MRTS (9)
6.2 Estimation
Under separability, conditional independence and linearity, the MRTS between
x1 and x2 can be consistently recovered. One can for instance simultaneously regress h1 (low
birth weight) and h2 (normality) on the main inputs at stake (i.e., terrorist intensity in each
trimester of pregnancy –Casualties1, Casualties2, Casualties3– and unemployment rate
in each trimester of pregnancy –Unemployment1, Unemployment2, Unemployment3) and
on the rest of control variables of panel C in Table 2 using seemingly unrelated regression
(SUR) and test for (9).
[Insert Table 12 about here]
Table 12 shows that we cannot reject the equality of the ratios of the marginal effects of
terrorism and unemployment in the first trimester of pregnancy for h1 and h2, so that
the “marginal rate of technical substitution” between terrorism and unemployment in the
production of child health is identified.
7 Conclusion
We estimate the effect of in utero exposure to ETA-bomb casualties on a range of birth
outcomes: birth weight, low-birth weight, normality, and gender. We find detrimental effects
in terms of average birth weight (lower), the prevalence of low birth weight (higher) and the
fraction of normal babies (lower). Our results are robust to a battery of robustness checks
(e.g., measuring exposure to terrorism using date of birth instead of estimated conception
date).
Crucially, and in support of our identification strategy, the number of ETA-bomb casu-
alties after birth does not predict any of the birth outcomes under analysis, and virtually
18
the same estimates are obtained when controlling for economic conditions (as captured by
total unemployment rates) in each of the trimester of pregnancy. We do not find evidence
of migration responses (in terms of population responses to last year terrorist activity), but
both the number of live births and the number of fetal deaths increase with the number of
ETA-bomb casualties. Given the increase in fetal deaths, the estimated effects of terrorism
on birth outcomes for live births are likely to be downward biased (if anything) due to
selective mortality.
Results are driven by exposure to terrorism in the first trimester of pregnancy, indicating
that ETA-bomb casualties are acting as acute maternal stress shocks. That stress early in
pregnancy (rather than in other periods) is bad for the fetus is consistent with recent studies
on the effects of “violence”, from terrorist attacks in the United States (Brown, 2012) to
homicide rates in rural Brazil (Foureaux and Manacorda, 2013).
19
References
Abadie, Alberto and Javier Gardeazabal. 2003. “The Economic Costs of Conflict: A Case
Study of the Basque Country.” American Economic Review 93 (1):113–132.
Almond, Douglas and Janet Currie. 2011. Human Capital Development before Age Five,
Handbook of Labor Economics, vol. 4, chap. 15. Elsevier, 1315–1486.
Angrist, J. and J-S. Pischke. 2009. “Mostly Harmless Econometrics.” Princeton University
Press .
Behrman, J. and M. Rosenzweig. 2004. “Returns to Birthweight.” Review of Economics
and Statistics 86 (2):586–601.
Beydoun, Hind and Audrey Saftlas. 2008. “Physical and Mental Health Outcomes of Pre-
natal Maternal Stress in Human and Animal Studies: A Review of Recent Evidence.”
Paediatric and Perinatal Epidemiology 22 (5):438–466.
Black, Sandra, Paul Devereux, and Kjell Salvanes. 2007. “From the Cradle to the La-
bor Market? The Effect of Birth Weight on Adult Outcomes.” Quarterly Journal of
Economics 122 (1):409–439.
Bozzoli, Carlos, Angus S. Deaton, and Climent Quintana-Domeque. 2009. “Adult Height
and Childhood Disease.” Demography 46:647–669.
Bozzoli, Carlos and Climent Quintana-Domeque. 2014. “The Weight of the Crisis: Evidence
from Newborns in Argentina.” Review of Economics and Statistics , forthcoming.
Bram, J., J. Orr, and C. Rapaport. 2002. “Measuring the Effect of the September 11 Attack
on New York City.” Federal Reserve Bank of New York Economic Policy Review 8:5–20.
Brown, Ryan. 2012. “The Intergenerational Impact of Terror: Does the 9/11 Tragedy
Reverberate into the Outcomes of the Next Generation.” Duke University, mimeo .
20

Camacho, Adriana. 2008. “Stress and Birth Weight: Evidence from Terrorist Attacks.”
American Economic Review, Papers & Proceedings 98 (2):511–15.
Case, A., A. Fertig, and C. Paxson. 2005. “The Lasting Impact of Childhood Health and
Circumstance.” Journal of Health Economics 24:365–389.
Catalano, R., T. Bruckner, A. Marks, and B. Eskenazi. 2006. “Exogenous Shocks to the Hu-
man Sex Ratio: the Case of September 11, 2001 in New York City.” Human Reproduction
21:3127–3131.
CIS. 2013. “Barometro de la Percepcion de los Principales Problemas de Espa˜a.” Available
at http://www.cis.es. Accessed 13/02/2014.
Currie, Janet and Rosemary Hyson. 1999. “Is the Impact of Health Shocks Cushioned
by Socioeconomic Status? The Case of Low Birthweight.” American Economic Review
89:245–250.
Currie, Janet and Maya Rossin-Slater. 2013. “Weathering the storm: Hurricanes and birth
outcomes.” Journal of Health Economics 32 (3):487–503.
Danieli, Yael, Danny Brom, and Joe Sills. 2005. The Trauma of Terrorism: Sharing Knowl-
edge and Shared Care. An International Handbook, vol. 1. Psychology Press.
de la Calle, Luis and Ignacio Sanchez-Cuenca. 2006. “The Production of Terrorist Violence:
Analyzing Target Selection Within the IRA and ETA.” Working Paper. Instituto Juan
March .
———. 2007. “The Victims of ETA dataset.” Available at
http://www.march.es/ceacs/proyectos/dtv. Accessed 13/02/2014.
de Weerth, C. and J. Buitelaar. 2005. “Physiological Stress Recreativity in Human Preg-
nancy. A Review.” Neuroscience and Behavioral Reviews 29:295–312.
21

Dehejia, Rajeev and Adriana Lleras-Muney. 2004. “Booms, Busts, and Babies’ Health.”
The Quarterly Journal of Economics 119:1091–1130.
Dunkel-Schetter, Chris. 2011. “Psychological science on pregnancy: Stress processes, biopsy-
chosocial models, and emerging research issues.” Annual Review of Psychology 62 (2):531–
558.
Eccleston, M. 2011. “In Utero Exposure to Maternal Stress: Effects of the September 11th
of terrorist attacks in New York City on Birth and Early Schooling Outcomes.” Harvard
University, mimeo .
Foureaux Koppensteiner, Martin and Marco Manacorda. 2013. “The Effect of Violence on
Birth Outcomes: Evidence from Homicides in Rural Brazil.” IDB Working Paper 416.
Garces, Eliana, Janet Currie, and Duncan Thomas. 2002. “Longer-Term Effects of Head
Start.” American Economic Review 92:999–1012.
Hedegaard, M., T. Henriksen, S. Sabore, and N. Secher. 1993. “Physiological Distress in
Pregnancy and Preterm Delivery.” British Medical Journal 307:234–239.
Johnson, Robert C. and Robert F. Schoeni. 2011. “The Influence of Early-Life Events on
Human Capital, Health Status, and Labor Market Outcomes Over the Life Course.” The
B.E. Journal of Economic Analysis & Policy 11:1–57.
Krueger, Alan. 2007. What Makes a Terrorist. Economics and the Roots of Terrorism.
Princeton University Press.
LaFree, Gary, Laura Dugan, Min Xie, and Piyusha Singh. 2012. “Spatial and Temporal
Patterns of Terrorist Attacks by ETA 1970 to 2007.” Journal of Quantitative Criminology
28:7–29.
Landrigan, P. 2001. “Health Consequences of the 11 September 2001 Attacks.” Environ-
mental Health Perspectives 109:A514–15.
22

Mansour, Hani and Daniel I. Rees. 2012. “Armed conflict and birth weight: Evidence from
the al-Aqsa Intifada.” Journal of Development Economics 99 (1):190–199.
McCormick, Marie C. 1985. “The Contribution of Low Birth Weight to Infant Mortality
and Childhood Morbidity.” New England Journal of Medicine 312 (2):82–90.
Montalvo, Jose G. 2011. “Voting after the bombings: A natural experiment on the ef-
fect of terrorist attacks on democratic elections.” Review of Economics and Statistics
93 (4):1146–1154.
Nijdam, Mirjam J., Berthold P. R. Gersons, and Miranda Olff. 2010. “Dutch politicians’
coping with terrorist threat.” The British Journal of Psychiatry 197 (4):328–329.
Pollack, Raphael and Michael Divon. 1992. “Intrauterine Growth Retardation: Definition,
Classification, and Etiology.” Clinical Obstetrics and Gynecology 35 (1):99–107.
Saul, Ben. 2012. “The Challenge of Defining Terrorism.” Available at
http://www.isn.ethz.ch. Accessed 13/02/2014.
Schneider, M., E. Roughton, A. Koehler, and G. Lubach. 1999. “Growth and Develop-
ment following Prenatal Stress Exposure in Primates: An Examination of Ontogenetic
Vulnerability.” Child Development 70 (2):263–274.
Schulte, H., D. Weisner, and B. Allolio. 1990. “The Cortricotropin Releasing Hormone
Test in Late Pregnancy: Lack of Adrenocorticotropin and Cortisol Response.” Clinical
Endocrinology 33 (1):99–106.
Whalley, Matthew G. and Chris R. Brewin. 2007. “Mental Health following terrorist at-
tacks.” The British Journal of Psychiatry 190:94–96.
23

Table 1. DESCRIPTIVE STATISTICS
Mean characteristics of live births for exposed and unexposed children (and their mothers) to ETA-bomb casualties during
pregnancy while in utero, and their difference.
No ETA-Bomb Casualty ETA-Bomb Casualties 1 Difference
A. Birth Outcomes
BW (Birth Weight: 500-6590 grams)
[N = 6,327,753] 3,291.64 3,255.78 35.86***
(8.28)
BW is available (per 1,000)
[N = 6,641,478] 953 953 0
(11)
LBW (Low Birth Weight) (per 1,000)
[N = 6,327,753] 51 57 6***
(1)
Premature (per 1,000)
[N = 6,641,478] 47 50 3
(4)
Normal (per 1,000)
[N = 6,641,478] 899 883 16*
(9)
Male (per 1,000)
[N = 6,641,478] 517 516 1*
(0.4)
B. Mother and Pregnancy Characteristics
Mother’s age (15-49 years old)
[N = 6,641,478] 28.8 29.4 0.6***
(0.2)
Mother is married (per 1,000)
[N = 6,641,478] 883 879 4
(9)
First pregnancy (per 1,000)
[N = 6,641,478] 519 508 11
(9)
Second pregnancy (per 1,000)
[N = 6,641,478] 364 347 17***
(6)
Note. Live births conceived between January 1980 and February 2003. Each difference is computed as the estimated coefficient on an indicator variable (1 if ETA-
bomb casualties during pregnancy 1, 0 otherwise) in a separate OLS regression (which includes a constant) for each variable. Low Birth Weight: 1 if BW 2,500
grams, 0 otherwise. Statistical significance associated to the t-test of the estimated coefficient on the indicator variable with standard errors clustered at the province level (50 clusters). *** p-value < 0.01, ** p-value < 0.05, * p-value < 0.1

Table 2. OLS Regressions of Birth Outcomes on ETA-Bomb casualties by trimester of in utero exposure
(counting forward from estimated date of conception)
BW
LBW Normal Male
(per 1,000) (per 1,000) (per 1,000)
A. Year-Month Fixed Effects & Province Fixed Effects
ETA-Bomb casualties 1st trimester of pregnancy 0.674*** 0.187** 0.631*** 0.138
(0.194) (0.834) (0.194) (0.123)
ETA-Bomb casualties 2nd trimester of pregnancy 0.504 0.118 0.287 0.379
(0.404) (0.148) (0.275) (0.230)
ETA-Bomb casualties 3rd trimester of pregnancy 0.392 0.017 0.252 0.276
(0.484) (0.105) (0.454) (0.212)
Number of live births 6,327,753 6,327,753 6,641,478 6,641,478
B. (A) & Socio-Demographic Controls
ETA-Bomb casualties 1st trimester of pregnancy 0.725*** 0.208** 0.571*** 0.130
(0.198) (0.088) (0.187) (0.126)
ETA-Bomb casualties 2nd trimester of pregnancy 0.489 0.119 0.173 0.376
(0.380) (0.154) (0.275) (0.232)
ETA-Bomb casualties 3rd trimester of pregnancy 0.411 0.025 0.392 0.274
(0.460) (0.106) (0.434) (0.214)
Number of live births 6,295,035 6,295,035 6,607,470 6,607,470
C. (B) & Province-Specific Linear Year-Month Trends
ETA-Bomb casualties 1st trimester of pregnancy 0.278** 0.145** 0.671*** 0.093
(0.122) (0.061) (0.179) (0.120)
ETA-Bomb casualties 2nd trimester of pregnancy 0.055 0.179 0.272*** 0.337
(0.202) (0.144) (0.098) (0.236)
ETA-Bomb casualties 3rd trimester of pregnancy 0.148 0.055 0.253 0.228
(0.250) (0.078) (0.174) (0.212)
Number of live births 6,295,035 6,295,035 6,607,470 6,607,470
Note. Live births conceived between January 1980 and February 2003. Year and month of conception. Province of mother’s residence. Socio-
demographic controls: mother’s age categories: 6 dummy variables; birth order categories: 3 dummy variables; mother’s occupational categories
(including non-labor market activities): 11 dummy variables; father’s occupational categories (including indicator NA): 12 dummy variables; mother’s marital status: 1 dummy variable (married or not); medical center/hospital delivery indicator: 1 dummy variable; municipality size categories: 5 dummy
variables. Standard errors clustered at the province level (50 clusters). *** p-value < 0.01, ** p-value < 0.05, * p-value < 0.1

Table 3. OLS Regressions of Birth Outcomes on ETA-Bomb casualties by in utero prenatal exposure period
(counting backwards from date of birth)
BW
LBW Normal Male
(per 1,000) (per 1,000) (per 1,000)
A. Year-Month Fixed Effects & Province Fixed Effects
ETA-Bomb casualties 6-8 months before birth –0.525** 0.075 –0.382*** –0.063
(0.227) (0.050) (0.130) (0.079)
ETA-Bomb casualties 3-5 months before birth –0.582* 0.038 0.155 –0.229
(0.309) (0.116) (0.263) (0.213)
ETA-Bomb casualties 0-2 months before birth –0.077 0.007 0.018 –0.226
(0.474) (0.117) (0.139) (0.207)
Number of live births 8,407,042 8,407,042 9,831,737 9,831,737
B. (A) & Socio-Demographic Controls
ETA-Bomb casualties 6-8 months before birth –0.607*** 0.113** –0.331** –0.063
(0.200) (0.053) (0.130) (0.080)
ETA-Bomb casualties 3-5 months before birth –0.618** 0.053 0.182 –0.225
(0.299) (0.119) (0.275) (0.215)
ETA-Bomb casualties 0-2 months before birth –0.094 0.022 0.079 –0.224
(0.452) (0.111) (0.145) (0.209)
Number of live births 8,368,967 8,368,967 9,789,870 9,789,870
C. (B) & Province-Specific Linear Year-Month Trends
ETA-Bomb casualties 6-8 months before birth –0.211* 0.067 –0.396* –0.040
(0.116) (0.058) (0.213) (0.088)
ETA-Bomb casualties 3-5 months before birth –0.193 –0.000 –0.018 –0.218
(0.149) (0.116) (0.180) (0.215)
ETA-Bomb casualties 0-2 months before birth 0.391 –0.034 –0.128 –0.210
(0.312) (0.104) (0.130) (0.203)
Number of live births 8,368,967 8,368,967 9,789,870 9,789,870
Note. Live births born between January 1980 and February 2003. Year and month of birth. Province of mother’s residence. See Table 2.

Table 4. PLACEBOS
OLS Regressions of Birth Outcomes on ETA-Bomb casualties by trimester of in utero exposure and placebos (after birth).
BW LBW
(per 1,000)
Normal
(per 1,000)
Male
(per 1,000)
(1) (2) (3) (4) (5) (6) (7) (8)
ETA-Bomb Casualties in the 1st trimester –0.271** –0.259** 0.142** 0.135** –0.671*** –0.660*** –0.090 –0.092
(0.119) (0.118) (0.063) (0.063) (0.182) (0.176) (0.120) (0.118)
ETA-Bomb Casualties in the 2nd trimester –0.054 –0.036 –0.179 –0.187 –0.272*** –0.261** –0.337 –0.337
(0.204) (0.216) (0.145) (0.149) (0.098) (0.105) (0.235) (0.240)
ETA-Bomb Casualties in the 3rd trimester 0.140 0.146 –0.053 –0.054 0.253 0.251 –0.232 –0.228
(0.242) (0.250) (0.076) (0.078) (0.175) (0.172) (0.211) (0.211)
Placebos
ETA-Bomb Casualties in the 1st trimester after birth 0.294 -- –0.087 -- 0.007 -- 0.103 --
(0.365) (0.132) (0.149) (0.069)
ETA-Bomb Casualties in the 1-9 months after birth -- 0.249 -- –0.119 -- 0.142 -- 0.004
(0.246) (0.085) (0.109) (0.078)
Number of live births 6,295,035 6,295,035 6,295,035 6,295,035 6,607,470 6,607,470 6,607,470 6,607,470
Mother’s Province of Residence Fixed Effects Yes Yes Yes Yes Yes Yes Yes Yes
Year-Month Fixed Effects Yes Yes Yes Yes Yes Yes Yes Yes
Socio-Demographic Controls Yes Yes Yes Yes Yes Yes Yes Yes
Province-Specific Linear Time (Y-M) Trends Yes Yes Yes Yes Yes Yes Yes Yes
Note. See Table 2.

Table 5. ACCOUNTING FOR THE RELATIONSHIP BETWEEN ECONOMIC CONDITIONS AND CHILD
HEALTH
OLS Regressions of Birth Outcomes on ETA-Bomb casualties and unemployment rates by trimester of in utero
exposure
BW
LBW Normal Male
(per 1,000) (per 1,000) (per 1,000)
ETA-Bomb casualties 1st trimester of pregnancy 0.251* 0.146** 0.618*** 0.090
(0.127) (0.059) (0.161) (0.120)
ETA-Bomb casualties 2nd trimester of pregnancy 0.038 0.181 0.246** 0.339
(0.188) (0.139) (0.108) (0.236)
ETA-Bomb casualties 3rd trimester of pregnancy 0.154 0.055 0.269 0.224
(0.231) (0.076) (0.203) (0.217)
Unemployment rates
Unemployment rate 1st trimester of pregnancy 0.628* 0.209** 0.721* 0.001
(0.315) (0.093) (0.394) (0.155)
Unemployment rate 2nd trimester of pregnancy 0.013 0.138 0.283* 0.241
(0.240) (0.111) (0.158) (0.236)
Unemployment rate 3rd trimester of pregnancy 0.399 0.015 0.603 0.100
(0.325) (0.099) (0.566) (0.152)
Number of live births 6,295,035 6,295,035 6,607,470 6,607,470
Mother’s Province of Residence Fixed Effects Yes Yes Yes Yes
Year-Month Fixed Effects Yes Yes Yes Yes
Socio-Demographic Controls Yes Yes Yes Yes
Province-Specific Linear Time (Y-M) Trends Yes Yes Yes Yes
Note. See Table 2.
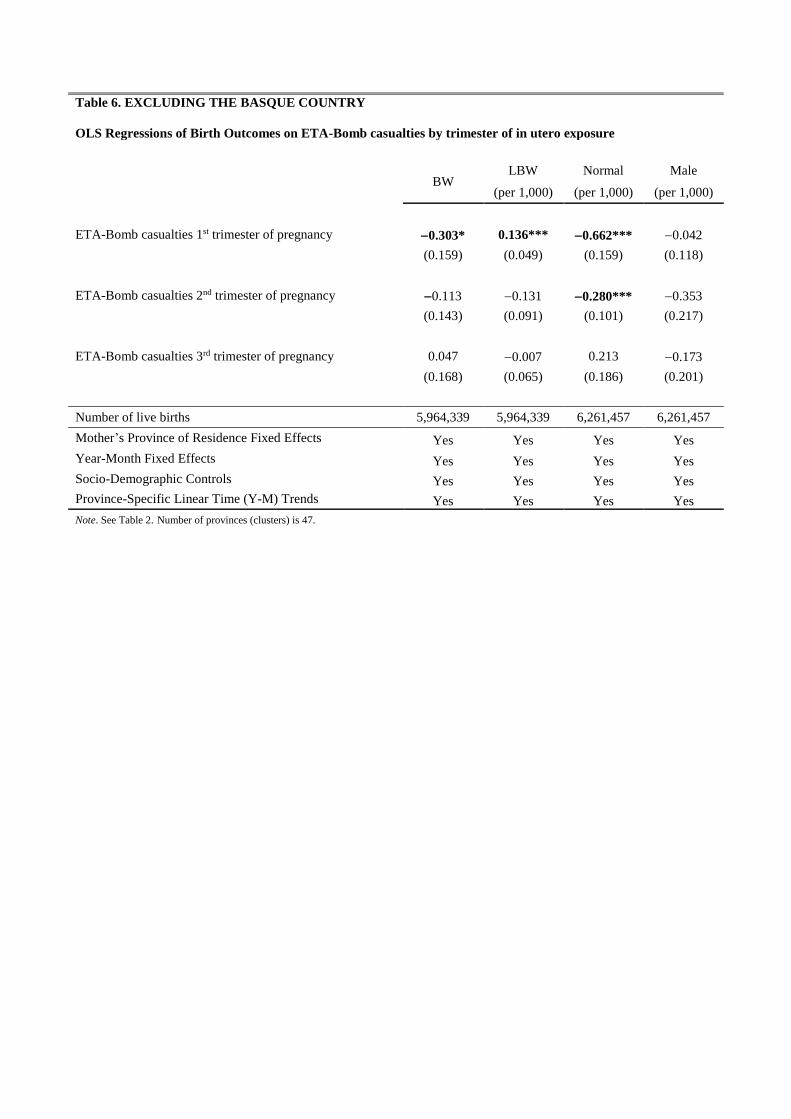
Table 6. EXCLUDING THE BASQUE COUNTRY
OLS Regressions of Birth Outcomes on ETA-Bomb casualties by trimester of in utero exposure
BW
LBW Normal Male
(per 1,000) (per 1,000) (per 1,000)
ETA-Bomb casualties 1st trimester of pregnancy 0.303* 0.136*** 0.662*** 0.042
(0.159) (0.049) (0.159) (0.118)
ETA-Bomb casualties 2nd trimester of pregnancy 0.113 0.131 0.280*** 0.353
(0.143) (0.091) (0.101) (0.217)
ETA-Bomb casualties 3rd trimester of pregnancy 0.047 0.007 0.213 0.173
(0.168) (0.065) (0.186) (0.201)
Number of live births 5,964,339 5,964,339 6,261,457 6,261,457
Mother’s Province of Residence Fixed Effects Yes Yes Yes Yes
Year-Month Fixed Effects Yes Yes Yes Yes
Socio-Demographic Controls Yes Yes Yes Yes
Province-Specific Linear Time (Y-M) Trends Yes Yes Yes Yes
Note. See Table 2. Number of provinces (clusters) is 47.

Table 7. EXCLUDING ALL PROVINCES WITHOUT ANY ETA-BOMB CASUALTY
OLS Regressions of Birth Outcomes on ETA-Bomb casualties by trimester of in utero exposure
BW
LBW Normal Male
(per 1,000) (per 1,000) (per 1,000)
ETA-Bomb casualties 1st trimester of pregnancy 0.348** 0.190** 0.541** 0.027
(0.125) (0.088) (0.228) (0.145)
ETA-Bomb casualties 2nd trimester of pregnancy 0.034 0.226 0.187 0.446*
(0.375) (0.183) (0.173) (0.222)
ETA-Bomb casualties 3rd trimester of pregnancy 0.368 0.208 0.297 0.278
(0.476) (0.157) (0.187) (0.196)
Number of live births 3,366,840 3,366,840 3,513,030 3,513,030
Mother’s Province of Residence Fixed Effects Yes Yes Yes Yes
Year-Month Fixed Effects Yes Yes Yes Yes
Socio-Demographic Controls Yes Yes Yes Yes
Province-Specific Linear Time (Y-M) Trends Yes Yes Yes Yes
Note. See Table 2. Number of provinces (clusters) is 15.

Table 8. HETEROGENEOUS EFFECTS: ARMED-FORCES FATHERS versus NON-ARMED-FORCES FATHERS
OLS Regressions of Birth Outcomes on ETA-Bomb casualties by trimester of in utero exposure.
BW LBW
(per 1,000)
Normal
(per 1,000)
Male
(per 1,000)
Armed-Force
Non-
Armed-
Force
Armed-Force
Non-
Armed-
Force
Armed-Force
Non-
Armed-
Force
Armed-Force
Non-
Armed-
Force
ETA-Bomb Casualties in the 1st trimester –1.20 –0.254** 0.377 0.142** –0.888 –0.662*** –0.458 –0.091
(1.11) (0.125) (0.670) (0.057) (1.34) (0.166) (1.0) (0.118)
ETA-Bomb Casualties in the 2nd trimester –0.109 –0.037 0.105 –0.186 –2.5*** –0.237** –2.6* –0.309
(0.739) (0.211) (0.258) (0.144) (0.63) (0.101) (1.5) (0.221)
ETA-Bomb Casualties in the 3rd trimester –1.04 0.173 0.875 –0.067 –2.7 0.296 2.3*** –0.259
(1.19) (0.254) (0.905) (0.724) (1.7) (0.180) (0.76) (0.226)
Number of live births 82,453 6,212,582 82,453 6,212,582 87,020 6,520,450 87,020 6,520,450
Mother’s Province of Residence Fixed Effects Yes Yes Yes Yes Yes Yes Yes Yes
Year-Month Fixed Effects Yes Yes Yes Yes Yes Yes Yes Yes
Socio-Demographic Controls Yes Yes Yes Yes Yes Yes Yes Yes
Province-Specific Linear Time (Y-M) Trends Yes Yes Yes Yes Yes Yes Yes Yes
Note. See Table 2.

Table 9. NON-LINEAR EFFECTS OF TERRORISM
OLS Regressions of Birth Outcomes on ETA-Bomb casualties by trimester of in utero exposure
BW
LBW Normal Male
(per 1,000) (per 1,000) (per 1,000)
A. Indicators for Trimesters with Intense Terrorism
1(ETA-Bomb casualties 1st trimester of pregnancy 10) 9.54*** 6.54*** 5.23** 0.29
(3.01) (0.87) (2.09) (4.66)
1(ETA-Bomb casualties 2nd trimester of pregnancy 10) 0.283 2.44 7.16** 7.77***
(3.71) (1.73) (3.28) (2.83)
1(ETA-Bomb casualties 3rd trimester of pregnancy 10) 2.65 2.65 11.16 5.02
(4.72) (2.87) (7.90) (3.03)
B. Indicators for Trimesters with Terrorism
1(ETA-Bomb casualties 1st trimester of pregnancy 1) 0.793 0.065 1.71 1.43
(0.996) (0.435) (1.03) (1.12)
1(ETA-Bomb casualties 2nd trimester of pregnancy 1) 1.36 1.10 2.30** 0.544
(1.64) (0.658) (1.09) (0.646)
1(ETA-Bomb casualties 3rd trimester of pregnancy 1) 2.06 0.787* 0.279 1.14
(1.47) (0.450) (1.30) (1.14)
Number of live births 6,295,035 6,295,035 6,607,470 6,607,470
Mother’s Province of Residence Fixed Effects Yes Yes Yes Yes
Year-Month Fixed Effects Yes Yes Yes Yes
Socio-Demographic Controls Yes Yes Yes Yes
Province-Specific Linear Time (Y-M) Trends Yes Yes Yes Yes
Note. See Table 2. 1() equals 1 if the condition within parenthesis is satisfied, and 0 otherwise.

Table 10. MORTALITY AND FERTILITY RESPONSES TO TERRORISM
OLS Regressions of Fetal Deaths and Live Births on ETA-Bomb casualties (and unemployment rates) by
trimester of in utero exposure
Fetal Deaths Live Births
(1) (2) (3) (4)
ETA-Bomb casualties 1st trimester of pregnancy 0.190** 0.188** 29.01** 28.91**
(0.072) (0.071) (11.52) (11.51)
ETA-Bomb casualties 2nd trimester of pregnancy 0.093 0.093 30.21** 30.20**
(0.083) (0.083) (12.32) (12.30)
ETA-Bomb casualties 3rd trimester of pregnancy 0.151*** 0.150*** 20.22*** 20.25***
(0.037) (0.038) (3.71) (3.70)
Unemployment rates
Unemployment rate 1st trimester of pregnancy -- 0.001 -- 0.734
(0.017) (1.82)
Unemployment rate 2nd trimester of pregnancy -- 0.036*** -- 0.278
(0.013) (0.846)
Unemployment rate 3rd trimester of pregnancy -- 0.029* -- 2.22
(0.017) (2.41)
Number of observations 13,900 13,900 13,900 13,900
Mother’s Province of Residence Fixed Effects Yes Yes Yes Yes
Year-Month Fixed Effects Yes Yes Yes Yes
Province-Specific Linear Time (Y-M) Trends Yes Yes Yes Yes
Mean of the dependent variable 2.10 477.8
SD of the dependent variable 2.96 620.4
Min of the dependent variable 0 2
Max of the dependent variable 25 5,899 Note. Each observation is the count of the dependent variable at the year-month-province cell. Standard errors clustered at the province level (50 clusters). *** p-value < 0.01, ** p-value < 0.05, * p-value < 0.1

Table 11. FERTILITY VERSUS MIGRATION RESPONSES TO TERRORISM
OLS Regressions of log (Live Births) and log(Population) on ETA-Bomb casualties (and unemployment rates) by
trimester of in utero exposure
Log(Population at year t in province p)
Log(Live Births) Total
25-54
Female
25-54
Male
25-54
ETA-Bomb casualties 1st trimester of pregnancy 0.015*** -- -- --
(0.005)
ETA-Bomb casualties 2nd trimester of pregnancy 0.013** -- -- --
(0.006)
ETA-Bomb casualties 3rd trimester of pregnancy 0.013*** -- -- --
(0.004)
ETA-Bomb casualties at year t1 in province p -- 0.0002 0.0003 0.0002
(0.0019) (0.0018) (0.0020)
Number of observations 13,900 1,200 1,200 1,200
Mother’s Province of Residence Fixed Effects Yes Yes Yes Yes
Year-Month Fixed Effects Yes No No No
Province-Specific Linear Time (Y-M) Trends Yes No No No
Year Fixed Effects -- Yes Yes Yes Note. For column (1) each observation is the count of the dependent variable at the year-month-province cell. For columns (2)-(4) each observation is the
count of the dependent variable at the year-province cell. Standard errors clustered at the province level (50 clusters). *** p-value < 0.01, ** p-value < 0.05,
* p-value < 0.1

Table 12. IDENTIFYING THE “MARGINAL RATE OF TECHNICAL SUBSTITUTION” BETWEEN
TERRORISM AND UNEMPLOYMENT IN THE 1ST TRIMESTER OF PREGNANCY
SUR Regressions of h1 (= 1 – LBW) and h2 (= Normal) on ETA-Bomb casualties and unemployment rates by
trimester of in utero exposure
h1 h2
ETA-Bomb casualties 1st trimester of pregnancy (𝐓𝟏) 0.146*
(0.087)
0.392***
(0.118)
ETA-Bomb casualties 2nd trimester of pregnancy (𝐓𝟐) 0.181**
(0.087) 0.038
(0.118)
ETA-Bomb casualties 3rd trimester of pregnancy (𝐓𝟑) 0.055
(0.088)
0.515***
(0.119)
Unemployment rate 1st trimester of pregnancy (𝐔𝟏) 0.209***
(0.075)
0.799***
(0.102)
Unemployment rate 2nd trimester of pregnancy (𝐔𝟐) 0.138
(0.098)
0.231*
(0.133)
Unemployment rate 3rd trimester of pregnancy (𝐔𝟑) 0.015
(0.075)
0.486***
(0.101)
Ratio of Coefficients
𝐓𝟏
𝐔𝟏
0.697
(0.480)
0.491***
(0.159)
Wald Test 2(1) = 0.17
p-value=0.6777
Number of live births 6,295,035
Mother’s Province of Residence Fixed Effects Yes Yes Yes Yes
Year-Month Fixed Effects Yes Yes Yes Yes
Socio-Demographic Controls Yes Yes Yes Yes
Province-Specific Linear Time (Y-M) Trends Yes Yes Yes Yes
Note. See Table 2. Standard errors (unadjusted) for clustering in parenthesis.


















