Favorable Outcome of Fournier Gangrene in Two Patients with ...
5
Advances in Peritoneal Dialysis, Vol. 30, 2014 Favorable Outcome of Fournier Gangrene in Two Patients with Diabetes Mellitus on Continuous Peritoneal Dialysis Fournier gangrene (FG), a form of necrotizing fasciitis of the perineum and genitals, with high morbidity and mortality in the general population, carries the additional risk of involvement of the peritoneal catheter tunnel and peritoneal cavity in patients on chronic peritoneal dialysis (PD). We describe two men with diabetes who developed FG in the course of PD. Computed tomography showed no extension of FG to the abdominal wall, and spent peritoneal dialysate was clear in both patients. Broad-spectrum antibiotic therapy with anaerobic coverage and early aggressive debridement followed by negative-pressure wound therapy and repeated debridement led to improvements in clinical status in both cases. Surgical closure and healing of the wound was achieved in one patient; the wound of the second patient is healing, but remains open. Both patients experienced prolonged hospitalization, with a serious decline in nutrition status. In patients on PD, FG can be treated successfully. However, additional measures are required to evaluate for potential involvement of the PD apparatus and the peritoneal cavity in the infectious process; and prolonged hospitalization, worsening nutrition, and multiple surgical interventions can result. Key words Fournier gangrene, diabetes mellitus, malnutrition, negative-pressure vacuum dressings Introduction Fournier gangrene (FG) is a synergistic polymicro- bial necrotizing fasciitis of the perineum and exter- nal genital organs primarily affecting men (1–3). Its histologic picture is characterized by obliterative endarteritis of the subcutaneous arteries and gan- grene of the subcutaneous tissue and the overlying skin (1–3). An acute surgical emergency, FG has a mortality rate of 24% – 45% (4). Extension of FG to the abdominal wall, chest, axillae, and thighs has been reported (3). Gangrene of the abdominal wall in patients on chronic peritoneal dialysis (PD) car- ries the added risk of extension of the necrotizing infectious process into the tunnel of the PD catheter and the peritoneal cavity. Only 1 case of FG in a patient on PD (5)—with a fatal outcome—was found in a bibliographic search. We report 2 men with diabetes who developed FG in the course of PD and survived. Their cases il- lustrate the diagnostic interventions, management, and follow-up of FG in PD patients. Case descriptions Both patients reported here were receiving PD for end-stage renal disease secondary to diabetic nephropathy. The PD schedule, which was exactly the same in the 2 patients, consisted of automated nocturnal 9-hour PD with 4 exchanges (3.0-L fill volume), plus two 2.5-L daytime exchanges, one with 7.5% icodextrin and one with dextrose. Peri- toneal transport was of the high-average type in both patients. Darlene Vigil, 1 Anil Regmi, 1,2 Reuben Last, 3 Brenda Wiggins, 1 Yijuan Sun, 1,2 Karen S. Servilla, 1,2 Joanna R. Fair, 4 Larry Massie, 5 Antonios H. Tzamaloukas 1,2 From: 1 Renal Section, Raymond G. Murphy VA Medical Center; 2 Department of Medicine, University of New Mexico School of Medicine; 3 Surgery Service, Raymond G. Murphy VA Medical Center, and Department of Surgery, University of New Mexico School of Medicine; 4 Radiology Service, Raymond G. Murphy VA Medical Center, and Department of Radiology, University of New Mexico School of Medicine; 5 Pathology Service, Raymond G. Murphy VA Medical Center, and Department of Pathology, University of New Mexico School of Medicine, Albuquerque, New Mexico, U.S.A.
Transcript of Favorable Outcome of Fournier Gangrene in Two Patients with ...

Advances in Peritoneal Dialysis, Vol. 30, 2014
Favorable Outcome of Fournier Gangrene in Two Patients with Diabetes Mellitus on Continuous Peritoneal Dialysis
Fournier gangrene (FG), a form of necrotizing fasciitis of the perineum and genitals, with high morbidity and mortality in the general population, carries the additional risk of involvement of the peritoneal catheter tunnel and peritoneal cavity in patients on chronic peritoneal dialysis (PD). We describe two men with diabetes who developed FG in the course of PD. Computed tomography showed no extension of FG to the abdominal wall, and spent peritoneal dialysate was clear in both patients. Broad-spectrum antibiotic therapy with anaerobic coverage and early aggressive debridement followed by negative-pressure wound therapy and repeated debridement led to improvements in clinical status in both cases. Surgical closure and healing of the wound was achieved in one patient; the wound of the second patient is healing, but remains open. Both patients experienced prolonged hospitalization, with a serious decline in nutrition status. In patients on PD, FG can be treated successfully. However, additional measures are required to evaluate for potential involvement of the PD apparatus and the peritoneal cavity in the infectious process; and prolonged hospitalization, worsening nutrition, and multiple surgical interventions can result.
Key wordsFournier gangrene, diabetes mellitus, malnutrition, negative-pressure vacuum dressings
IntroductionFournier gangrene (FG) is a synergistic polymicro-bial necrotizing fasciitis of the perineum and exter-nal genital organs primarily affecting men (1–3). Its histologic picture is characterized by obliterative endarteritis of the subcutaneous arteries and gan-grene of the subcutaneous tissue and the overlying skin (1–3). An acute surgical emergency, FG has a mortality rate of 24% – 45% (4). Extension of FG to the abdominal wall, chest, axillae, and thighs has been reported (3). Gangrene of the abdominal wall in patients on chronic peritoneal dialysis (PD) car-ries the added risk of extension of the necrotizing infectious process into the tunnel of the PD catheter and the peritoneal cavity.
Only 1 case of FG in a patient on PD (5)—with a fatal outcome—was found in a bibliographic search. We report 2 men with diabetes who developed FG in the course of PD and survived. Their cases il-lustrate the diagnostic interventions, management, and follow-up of FG in PD patients.
Case descriptionsBoth patients reported here were receiving PD for end-stage renal disease secondary to diabetic nephropathy. The PD schedule, which was exactly the same in the 2 patients, consisted of automated nocturnal 9-hour PD with 4 exchanges (3.0-L fill volume), plus two 2.5-L daytime exchanges, one with 7.5% icodextrin and one with dextrose. Peri-toneal transport was of the high-average type in both patients.
Darlene Vigil,1 Anil Regmi,1,2 Reuben Last,3 Brenda Wiggins,1 Yijuan Sun,1,2 Karen S. Servilla,1,2 Joanna R. Fair,4 Larry Massie,5 Antonios H. Tzamaloukas1,2
From: 1Renal Section, Raymond G. Murphy VA Medical Center; 2Department of Medicine, University of New Mexico School of Medicine; 3Surgery Service, Raymond G. Murphy VA Medical Center, and Department of Surgery, University of New Mexico School of Medicine; 4Radiology Service, Raymond G. Murphy VA Medical Center, and Department of Radiology, University of New Mexico School of Medicine; 5Pathology Service, Raymond G. Murphy VA Medical Center, and Department of Pathology, University of New Mexico School of Medicine, Albuquerque, New Mexico, U.S.A.

Vigil et al. 121
Patient 1A 68-year-old man on PD for 41 months presented with excruciating pain and swelling of the left groin and scrotum of 5 days’ duration. He had experienced no episodes of peritonitis or exit-site or tunnel infec-tion in the past, but had experienced an episode of urinary tract infection 1 year before the development of scrotal swelling and pain. Weekly Kt/V urea varied between 1.82 and 2.43.
At presentation, the patient’s temperature was 38°C, his heart rate was 113 bpm, and his respiratory rate was 23/min. His body mass index was 29.0 kg/m2. The left side of the scrotum was swollen and indurated, with extreme tenderness along the course of the left epididymis, and crepitus in the perineum and left hemiscrotum. Pertinent laboratory values (6) included serum sodium 133 mmol/L (glucose 286 mg/dL); potassium 4.5 mmol/L; creatinine 11.86 mg/dL; total CO2 20 mmol/L; hematocrit 33.5%; and white cell count 15.2×103/mm3, with 87% neutrophils.
Computed tomography (CT) showed scrotal wall thickening, prominent soft-tissue thickening, and subcutaneous gas posterior to the left inguinal canal, consistent with necrotizing fasciitis involving the left inguinal and intertriginous regions. The process did not involve the abdominal wall.
The patient was treated with aggressive hydration, parenteral vancomycin and piperacillin–tazobactam, and urgent wound debridement. Histologic exami-nation of the excised tissue revealed subcutaneous tissue necrosis and inflammation. Tissue cultures revealed mixed urogenital flora. Anaerobic and fungal cultures of the excised tissue were negative. A urinary tract infection was also present. Spent peritoneal dialysate contained 56 cells per cubic milliliter, with negative cultures.
The patient’s hospital course was complicated by severe hypotension that lasted 6 days, and atrial fibrillation with a rapid ventricular rate requiring cardioversion. Three surgical explorations with debridement were performed, and the wound was treated with negative-pressure wound therapy. Dur-ing this patient’s hospitalization, PD was continued using the established schedule, and spent PD fluid was monitored. Repeated effluent cell counts and cultures were negative.
The patient was discharged after 17 days of hos-pitalization. During hospitalization, he lost 6.2 kg of body weight. By 6 weeks after presentation, his wound
was healed, and he had regained his lost weight. His serum albumin was 4.2 g/dL before hospitalization, declined to 3.3 g/dL during hospitalization, and in-creased to 4.4 g/dL at 6 months after discharge.
Patient 2A 54-year-old man on PD for 30 months was admitted with generalized weakness, fever, and scrotal swell-ing and pain for 1 day. In the preceding months, his weekly Kt/V urea had fluctuated between 1.66 and 1.92. He had experienced 1 episode of peritonitis with coagulase-negative Staphylococcus 14 months before the current admission, but no exit-site or tunnel infec-tion. A perineal abscess had been drained 5 months before admission, and 2 months before admission, he had experienced the onset of persistent diarrhea which, after admission, proved to be secondary to Clostridium difficile infection.
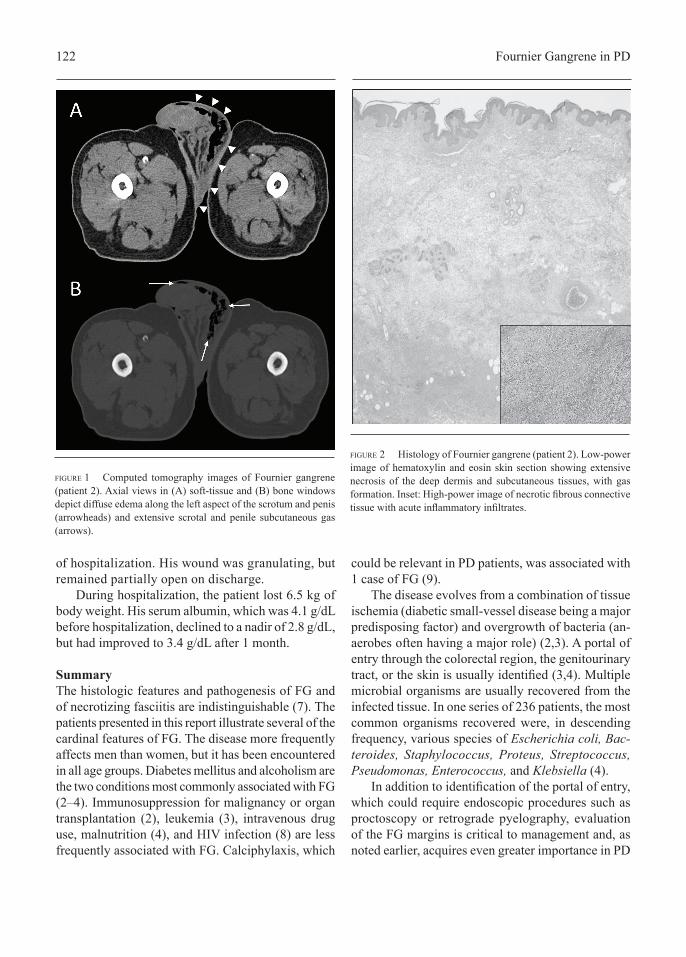
On admission, the patient’s temperature was 38.6°C, his heart rate was 93 bpm, and his respiratory rate was 21/min. His body mass index was 34.3 kg/m2. Examination of the scrotum revealed erythema, exquisite tenderness, and crepitus, particularly of the left hemiscrotum. Pertinent laboratory studies (6) in-cluded serum sodium 136 mmol/L (glucose 268 mg/dL); potassium 4.0 mmol/L; creatinine 15.78 mg/dL; total CO2 24 mmol/L; hematocrit 26.9%; and white cell count 20.7×103/mm3, with 92% neutrophils. Blood cultures were negative, and spent dialysate was clear. Imaging with CT revealed diffuse edema and subcutaneous emphysema in the left scrotum, extend-ing into the perineum and the penis (Figure 1), but not involving the abdominal wall.
On the day of admission, the patient underwent excision of the dead skin and debridement of the scrotum and was placed on a combination of vanco-mycin, piperacillin–tazobactam, and metronidazole. Histologic examination of the excised scrotal tissue revealed extensive inflammation and necrosis involv-ing the soft tissue under the skin and the adipose tissue (Figure 2).
After the surgical intervention, the patient’s clinical status improved, but he required two more sessions of debridement of the surgical wound, which was treated with negative-pressure wound therapy. During his hospitalization, PD was contin-ued on the established schedule. Physical debility and a need for systematic physical therapy delayed the patient’s discharge, which occurred after 38 days
122 Fournier Gangrene in PD
of hospitalization. His wound was granulating, but remained partially open on discharge.
During hospitalization, the patient lost 6.5 kg of body weight. His serum albumin, which was 4.1 g/dL before hospitalization, declined to a nadir of 2.8 g/dL, but had improved to 3.4 g/dL after 1 month.
SummaryThe histologic features and pathogenesis of FG and of necrotizing fasciitis are indistinguishable (7). The patients presented in this report illustrate several of the cardinal features of FG. The disease more frequently affects men than women, but it has been encountered in all age groups. Diabetes mellitus and alcoholism are the two conditions most commonly associated with FG (2–4). Immunosuppression for malignancy or organ transplantation (2), leukemia (3), intravenous drug use, malnutrition (4), and HIV infection (8) are less frequently associated with FG. Calciphylaxis, which
could be relevant in PD patients, was associated with 1 case of FG (9).
The disease evolves from a combination of tissue ischemia (diabetic small-vessel disease being a major predisposing factor) and overgrowth of bacteria (an-aerobes often having a major role) (2,3). A portal of entry through the colorectal region, the genitourinary tract, or the skin is usually identified (3,4). Multiple microbial organisms are usually recovered from the infected tissue. In one series of 236 patients, the most common organisms recovered were, in descending frequency, various species of Escherichia coli, Bac-teroides, Staphylococcus, Proteus, Streptococcus, Pseudomonas, Enterococcus, and Klebsiella (4).
In addition to identification of the portal of entry, which could require endoscopic procedures such as proctoscopy or retrograde pyelography, evaluation of the FG margins is critical to management and, as noted earlier, acquires even greater importance in PD
figure 1 Computed tomography images of Fournier gangrene (patient 2). Axial views in (A) soft-tissue and (B) bone windows depict diffuse edema along the left aspect of the scrotum and penis (arrowheads) and extensive scrotal and penile subcutaneous gas (arrows).
figure 2 Histology of Fournier gangrene (patient 2). Low-power image of hematoxylin and eosin skin section showing extensive necrosis of the deep dermis and subcutaneous tissues, with gas formation. Inset: High-power image of necrotic fibrous connective tissue with acute inflammatory infiltrates.

Vigil et al. 123
patients. Imaging, which also assists in making the diagnosis in difficult cases, is used to determine the extent of FG (10). Plain radiography, ultrasonography, CT, and magnetic resonance imaging have all been applied for this purpose (10). Imaging by CT was reported to be superior to that by plain radiography or ultrasonography (11). Magnetic resonance imag-ing is accurate in identifying the extent of disease and the point of origin (12). Given those reports, CT or magnetic resonance imaging, whichever is readily available, should be considered the imaging procedure of choice in FG.
The high mortality in FG has led to efforts to develop prognostic indicators that might be used to evaluate various therapeutic modalities. The FG severity index is calculated using stratified (high and low) values of body temperature; heart and respira-tory rates; serum sodium, potassium, creatinine, and bicarbonate; and hematocrit and white cell count (6). High index values were found in several studies to predict mortality with reasonable accuracy (13–15). Other clinical factors that were found to be associated with mortality were hepatic dysfunction, older age, colorectal origin (3), extent of the disease (2), and delays in surgical intervention (16).
Early recognition of FG is imperative (17). Man-agement has two prongs that should both be applied as soon as the diagnosis is made. First, parenteral antibiotics with broad coverage, including anaerobic agents, should be initiated, and hemodynamic stabili-zation should be pursued. At the same time, aggressive surgical debridement should also be performed (17). The wound should initially be treated with topical antiseptics and frequent dressing changes, and the edges of the wound should be carefully monitored for signs that the FG has advanced. After the first 2 days, treatment with negative-pressure wound therapy to promote granulation and closure has been found to be effective (18). Hyperbaric oxygen treatment has also been applied (2,4). Repeated debridement is usually necessary, until FG is found to be no longer advancing and causing tissue necrosis.
Perineal and scrotal soft-tissue defects can be extensive; they frequently lead to chronic wounds that can require reconstructive surgery. If fecal con-tamination of the wound becomes problematic, an enterocutaneous stoma might become necessary to divert stool from the wound (19). Colectomy has also been performed in patients with severe colonic disease
(19). Physical and mental debility might persist for a long period after discharge (19). In patients on PD who develop FG, imaging should address the potential for involvement of the abdominal wall proximally to the PD catheter tunnel and of the catheter exit site or tunnel. Spent dialysate should be monitored for signs of infection. In the absence of signs of peritoneal involvement, PD can continue. As has been reported with other severe infectious processes affecting PD patients (20), FG has a large effect on nutrition. Nutrition and physical rehabilitation require special attention in patients with FG.
AcknowledgmentThis work was supported by the Raymond G. Murphy VA Medical Center.
DisclosuresThe authors of this report declare that they have no financial conflicts of interest.
References 1 Fournier JA. Fulminating gangrene of the penis
[French]. Med Pract Paris 1883;4:589–97. 2 Smith GL, Bunker CB, Dinneen MD. Fournier’s gan-
grene. Br J Urol 1998;81:347–55. 3 Ekke N. Fournier’s gangrene: a review of 1726 cases.
Br J Surg 2000;87:718–28. 4 Vick R, Carson CC 3rd. Fournier’s disease. Urol Clin
North Am 1999;26:841–9. 5 Charboneau H, Pème F. A crackling priapism related to
Fournier’s gangrene in a patient on chronic peritoneal dialysis. J Infect 2010;61:274–5.
6 Laor E, Palmer LS, Tolia BM, Reid RE, Winter HI. Out-come prediction in patients with Fournier’s gangrene. J Urol 1995;154:89–92.
7 Efem SE. The features and aetiology of Fournier’s gangrene. Postgrad Med J 1994;70:568–71.
8 Elem B, Ranjan P. Impact of immunodeficiency virus (HIV) on Fournier’s gangrene: observations in Zambia. Ann R Coll Surg Engl 1995;77:283–6.
9 So A, Bell D, Metcalfe P, Gupta R. Calciphylaxis of the penis: a unique cause of Fournier’s gangrene. Can J Urol 2001;8:1377–9.
10 Rajan DK, Scharer KA. Radiology of Fournier’s gan-grene. AJR Am J Roentgenol 1998;170:163–8.
11 Levenson RB, Singh AK, Novelline RA. Fournier gan-grene: role of imaging. Radiographics 2008;28:519–28.
12 Kickuth R, Adams S, Kirchner J, Pastor J, Simon S, Lier-mann D. Magnetic resonance imaging in the diagnosis of Fournier’s gangrene. Eur Radiol 2001;11:787–90.

124 Fournier Gangrene in PD
13 Ersay A, Yilmaz G, Akgun Y, Celik Y. Factors affecting mortality of Fournier’s gangrene: review of 70 patients. ANZ J Surg 2007;77:43–8.
14 Corcoran AT, Smaldone MC, Gibbons EP, Walsh TJ, Davies BJ. Validation of Fournier’s gangrene severity index in a large contemporary series. J Urol 2008;180:944–8.
15 Kabay S, Yucel M, Yaylak F, et al. The clinical fea-tures of Fournier’s gangrene and the predictivity of the Fournier’s gangrene severity index on the outcomes. Int Urol Nephrol 2008;40:997–1004.
16 Sigihara T, Yasunaga H, Horiguchi H, et al. Impact of surgical intervention timing on the case fatality rate for Fournier’s gangrene: an analysis of 379 cases. BJU Int 2012;110:E1096–100.
17 Norton KS, Johnson LW, Perry T, Perry KH, Sehon JK, Zibari GB. Management of Fournier’s gangrene: an eleven year retrospective analysis of early recognition, diagnosis, and treatment. Am Surg 2002;68:709–13.
18 Silberstein J, Grabowski J, Parsons JK. Use of a vacuum-assisted device for Fournier’s gangrene: a new paradigm. Rev Urol 2008;10:76–80.
19 Czymek R, Kujath P, Bruch HP, et al. Treatment, out-come and quality of life after Fournier’s gangrene: a multicentre study. Colorectal Dis 2013;15:1529–36.
20 Fox L, Tzamaloukas AH, Murata GH. Metabolic dif-ferences between persistent and routine peritonitis in continuous ambulatory peritoneal dialysis. Adv Perit Dial 1992;8:346–50.
Corresponding author: Antonios H. Tzamaloukas, md, Renal Section (111C), Raymond G. Murphy VA Medical Center, 1501 San Pedro SE, Albuquerque, New Mexico 87108 U.S.A.E-mail: [email protected]