
Fast Track Chirurgie - ake-nutrition.at · Schlußfolgerung der Metaanalyse ¾There is no benefit...
45
Fast Track Chirurgie Die Chirurgie auf der Überholspur ? FRIEDRICH LÄNGLE Universitätsklinik für Chirurgie,Wien Abteilung für Allgemeinchirurgie
Transcript of Fast Track Chirurgie - ake-nutrition.at · Schlußfolgerung der Metaanalyse ¾There is no benefit...

Fast Track Chirurgie
Die Chirurgie auf der Überholspur ?
FRIEDRICH LÄNGLE
Universitätsklinik für Chirurgie,Wien
Abteilung für Allgemeinchirurgie

ELEKTIVE CHIRURGIEProblemstellung
• Postoperative Infektionsrate(Pneumonie, Abszess, Sepsis, HWI, Wundinfekt, …)
• Nicht – infektiöse Komplikationen(Anastomosendehiszenz, Blutung, Thrombose, …)
• Mortalität

ELEKTIVE CHIRURGIEPostoperative Komplikationen - Risikofaktoren
• Alter
• Immunsuppression, Tumorpatient
• Adipositas
• Diabetes mellitus
• Herz – und Lungenerkrankungen
• Ausmaß des katabolen operativen Streß
• Ernährungsstatus des Patienten
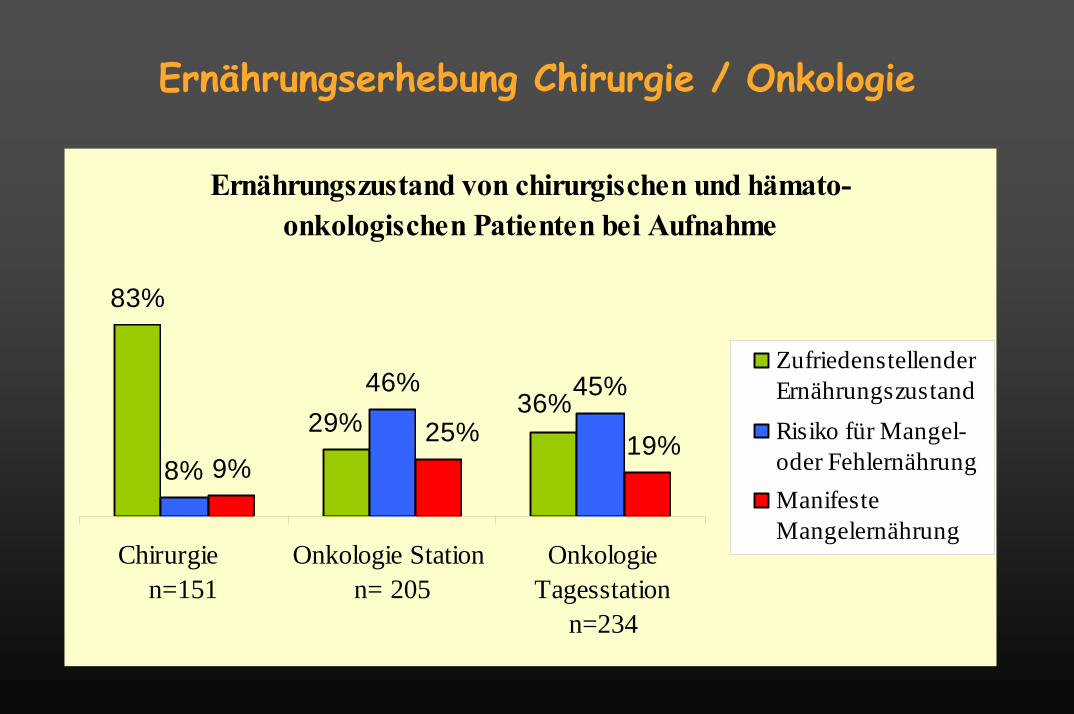
Ernährungserhebung Chirurgie / Onkologie
Ernährungszustand von chirurgischen und hämato-onkologischen Patienten bei Aufnahme
83%
8%
46% 45%
9%
36%29%
19%25%
Chirurgie n=151
Onkologie Station n= 205
OnkologieTagesstation
n=234
ZufriedenstellenderErnährungszustandRisiko für Mangel-oder FehlernährungManifesteMangelernährung

Protein-Energy Undernutrition Among Elderly Hospital PatientsSullivan D.H. JAMA (1999) 281, 21:2013-2019
497 Patineten, 65 Jahre oder älter
21% (102 Patienten: 62 Pat. auf chirurgischer Abteilung40 Pat. auf internistischer Abteilung) durchschnittliche tägliche Ernährung <50% als errechneter täglicher Energiebedarf
Outcome low Nutrient intake All Others Relative Risk
In-hospital mortality 12 (11.8%) 6 (1.5%) 8.0(2.8-22.6)Death <90 days of adm. 16 (15.7%) 23 (5.8%) 2.9 (1.4-6.1)

Nutrition Day / participation
NutritionDay 2006
• 23 languages• 25 countries• 748 units/wards• 16455 patients
Mangelernährung !?

Nutrition Day / Resources
Did you eat less last week?
0 10 20 300
20
40
60
80
100missingnormal< normal< 50%< 25%
LO S Hosp ita l (Days)
Patie
nts
in H
ospi
tal (
%)
6d

missing all
50%
25%
nothing
0
10
20
30
40
50
%
Lunch on Nutrition Day
all 1/2 1/4 nothing
x
Mortality
5.5 5.7%2.5%
1.3%
6.5 %

Nutrition therapyNutrition Day / Intervention
• Enteral 7.3%• Parenteral 4.0%• EN+PN 1.4%• Protein S. 5.4%

Grenzen Enterale ErnährungA clinical Pathway to Accelerate Recovery after Colonic Resection
L. Basse et al. Ann Surg 2000, Vol 232, N01,51-57
60 Patienten nach Colonresektion mitmultimodaler postoperativer Rehabilitation
Vermeidung einer routinem NasensondeEpiduralanästhesie für 48 hOpiodsparende AnalgesieFrüher oraler Kostaufbau
Bei 57 von 66 Patienten normale gastrointestinale Funktion48 Stunden post - operativ

Perioperative Traditionen
Preoperativ
– in-hospitalevaluation
– e.g.colonoscopy
– 1-2 fasting days– Bowel lavage
Operation Day
– opiates– Fluid loading– Drainages and
tubes– immobilisation
1.-x. POP-Day
– nasogastric tube– nil per mouth– parenteral nutrition– CV catheter– urinary cath.
Fasted – without glykogen-depots into „sport event“ ???

FAST Track = ERAS(Ehanced Recovery After Surgery)
Pathophysiologisches PrinzipMinimierung der Stressreaktion
ZielReduktion der Postoperativen Komplikationen
Rasche RekonvaleszenzKurzer Krankenhausaufenthalt
Ökonomische EffekteKosten einsparen

Perioperative Stressfaktoren• Angst• Operation• Schmerz• Hypothermie• Infusionsmenge• Hypoxie• Übelkeit, Erbrechen• Darmparalyse• Immobilisation• perioperatives Fasten• Stress induzierte Katabolie
immun function ↓
pulmonary function ↓
cardiac distress ↑
thrombembolism ↑

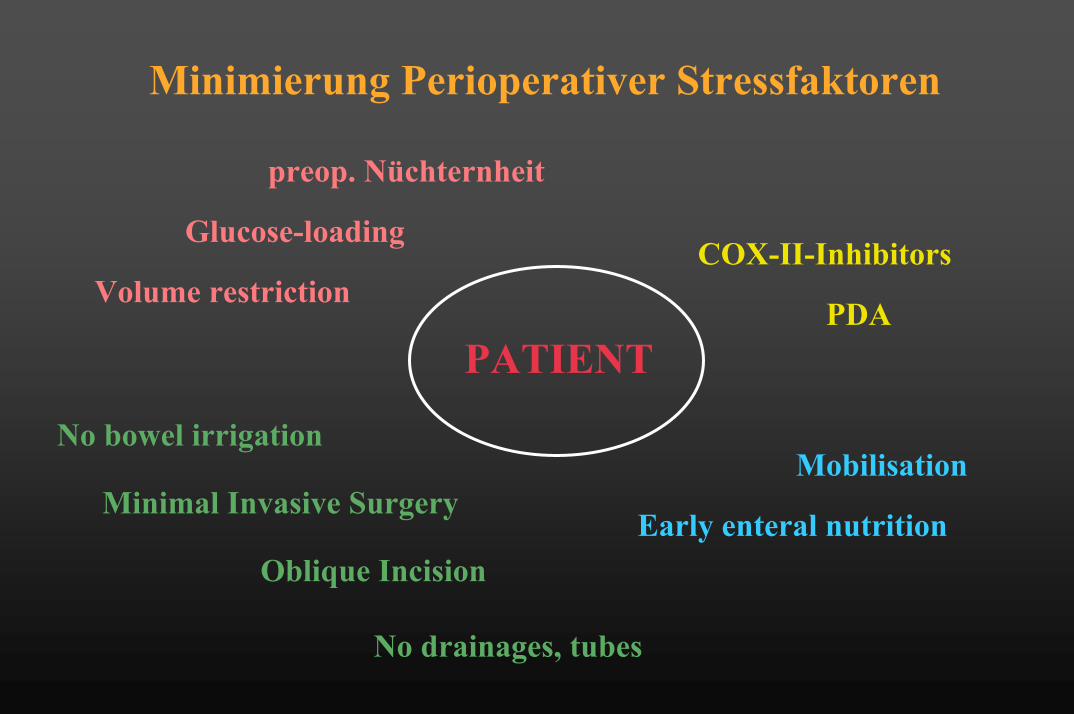
Minimierung Perioperativer Stressfaktoren
preop. Nüchternheit
COX-II-Inhibitors
PDA
Minimal Invasive Surgery
Oblique Incision
No bowel irrigation
Volume restriction
Early enteral nutrition
Mobilisation
OP-TRAUMA
Glucose-loading
No drainages, tubes

FAST Track = ERASPräoperative Nüchternheit - Fallbericht
Patientin hatte unter Chloroform-narkose Brandy aspiriert und verstarb
Simpson JY. Lancet 1848
Laryngealen Reflexe unter Narkose abgeschwächt, daher Gefahr der AspirationPräoperative Nahrungskarenz mit dem Ziel das Aspirationsrisiko zu senken
6 h präoperativ absolute Nahrungskarenz !

Spies CD et al. Anaesthesist 2003

Postoperative Insulinresistenz
P < 0.001, ANOVAn = 6-13
Insu
lin s
ensi
tivity
(%)
0
20
40
60
80
100
LapChol
Hernia Open Chol
Major Colorectal
Thorell et al: Curr Opin Clin Nutr Metab Care 1999

E.R.A.S.: Preoperativ Glucose loading
Nygren et al. Ann.Surg. 1995:222(6):728-734

Präoperative Glukose loading
Glycogen depot augmented
- Stress reaction (catecholamine) reducedBolder 1998
- Metabolic stress, insulin resistance reducedNygren, Thorell 1999
- Hunger, nausea, fatigue, anxiousness reducedHausel 2001
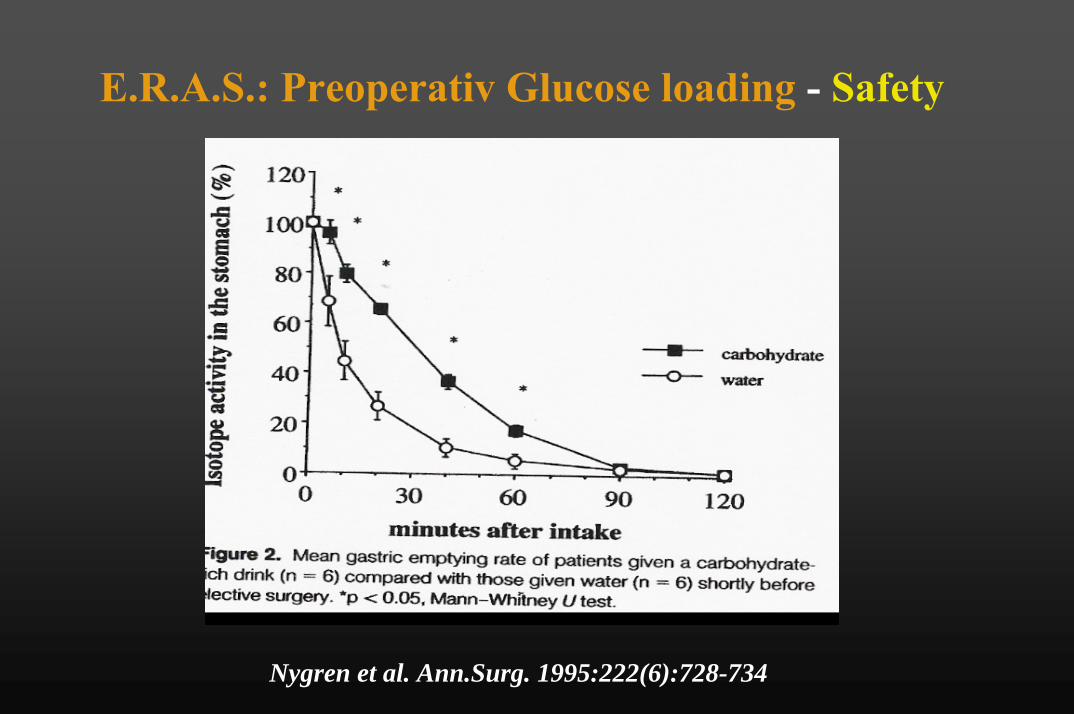
E.R.A.S.: Preoperativ Glucose loading - Safety
Nygren et al. Ann.Surg. 1995:222(6):728-734

Preoperative CarbohydratesHospital Stay
CH-Lsg. vs. NPO [Days] Reduction of LOS p
All Interventions -1.18 ±0.40 0.02Hip-Replacement -1.25±0.71 0.11Colorectal Surgery -2.1 ±1.36 0.152Open CHE -0.71±0.37 0.065
Ljungqvist et al Clin Nutr 1998:65

Meta-analysis of randomized clinical trials of colorectalsurgery with or without mechanical bowel preparation
Slim K., British Journal of Surgery 2004;91: 1125-1130
• 7 Untersuchungen• 1454 Patienten• 720 Patienten mit Darmvorbereitung• 734 Patienten ohne Darmvorbereitung• Primär: Anastomosenleaks
• Sekundär: Andere septische KomplikationenPostoperative Mortalität

AnastomosenleaksSlim K., British Journal of Surgery 2004;91: 1125-1130
• In allen Untersuchungen angegeben• Signifikant mehr Dehiszenzen in der
darmvorbereiteten Gruppe (p=0,032)
Darmvorbereitung keine Darmvorbereitung39/701 23/708

WundinfektionenSlim K., British Journal of Surgery 2004;91: 1125-1130
• In allen Untersuchungen angegeben• Mehr Wundinfekte in der darmvorbereiteten
Gruppe (n.s. P=0,175)
Darmvorbereitung keine Darmvorbereitung7,4% 5,7%

Postoperative MortalitätNicht septische KomplikationenSlim K., British Journal of Surgery 2004;91: 1125-1130
• Nur in 3 Untersuchungen angegeben
• Mortalität: Höher in der darmvorbereitetenGruppe (jedoch nicht signifikant)
• Komplikationene: Ebenfalls höher in der darmvorbereiteten Gruppe (nicht signifikant)

Klean-Prep
Die Darmreinigungslösung enthält: Macrogol 3350 (Polyethylenglykol)als abführende Komponente

Polyethylene glycolSlim K., British Journal of Surgery 2004;91: 1125-1130
• Anastomosenleaks signifikant höher 27/517 : 14/514
• Andere Darmvorbereitungen zeigen keine signifikante Erhöhung der Rate an
Anastomosendehiszenzen12/184 : 9/194

Oliveira L. et al. Dis Colon Rectum. 1997
• 90ml NaP (Fleet, Phospho-Soda) versus4 l PEG (GoLYTELY): 200 Patienten
• Randomisierte, geblindete Studie
1. Kein signifikanter Unterschied in der Qualität der Darmreinigung und der septischen bez. Anastomosenkomplikationen
2. 65% der Pat. würden eine Darmvorbereitung mit NaPnochmalig durchführen lassen / 25% der Pat. würden nochmalig PEG als Darmvorbereitung akzeptieren

Colon and Rectal Anastomoses do notRequire Routine Drainage
Urbach et al, Ann Surg 1999

A Meta-Analysis of Selective Versus Routine Nasogastric Decompression after Elective Laparotomy
Selective Routine p-value Rel RiskPatients 1986 - 1978Tubes replaced 103 36 0.0001 2.9 Complications 833 1084 0.03 0.76Pneumonia 53 119 0.0001 0.49Atelectasis 44 94 0.001 0.46Fever 108 212 0.02 0.51Vomiting 201 168 0.11 1.19Nausea 179 181 0.31 0.98Oral feeding (postop day) 3,5 4,6 0.04
CheathamML etal, Ann Surg 1995; 469-478

E.R.A.S.: Enhanced enteral nutrition
• Complication rate ↓infectionswoundhealing problemsLanastomotic dehiscence
• LOS ↓• Loss of muscle mass ↓• Fatigue ↓• Letality ↓• Quality of life ↑
Lewis et al. B.M.J. 2001:773

Early enteral feeding vs nil by mouthStephan JL. et al. BMJ. 2001; 323:6:1-5
P=0.080
P=0.036
P=0.045
P=0.15

Schlußfolgerung der Metaanalyse
There is no benefit in keeping patients „nil by mouth“ aftergastrointestinal surgery
Septic complications (RR 0.72) and length of hospital stay(signifc. reduction by 0.84 day) were reduced in those patientswho recieved early enteral feeding
In patients who recieved early enteral feeding there were no significant reductions in incidence of anastomotic dehiscence, wound infection, pneumonia, intra-abdominal abscess and mortality
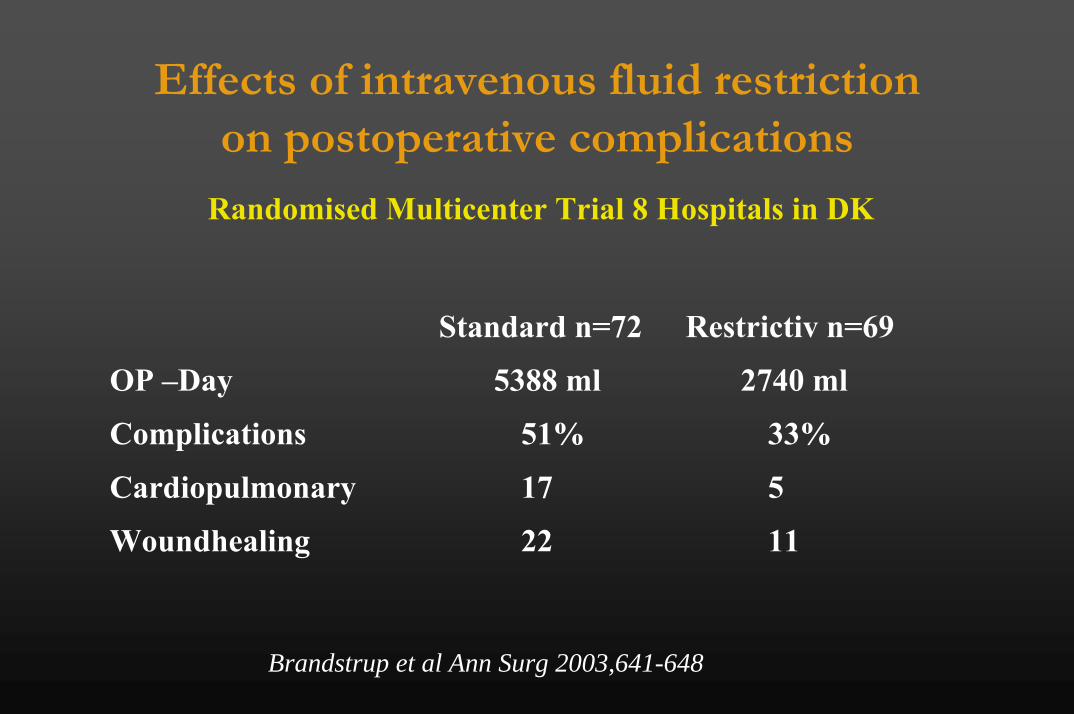
Effects of intravenous fluid restrictionon postoperative complications
Randomised Multicenter Trial 8 Hospitals in DK
Standard n=72 Restrictiv n=69
OP –Day 5388 ml 2740 ml
Complications 51% 33%
Cardiopulmonary 17 5
Woundhealing 22 11
Brandstrup et al Ann Surg 2003,641-648

Effect of salt and water balanceon recovery of
gastrointestinal function afterelective colonic
resection: a randomisedcontrolled trial
Lobo et alLancet, 25 May 2002, Pages 1812-1818








Fast Track -Perspectives
• Implementation als Standard in der Kolonchirurgie
• Evaluation in Pankreas, Leber-, Magenchirurgie
• Studien zur präop Glucose-loading, Darmvorbereitung, Infusionsregime und Darmtätigkeit
• Ökonomische Aspekte
• Evaluation psychologischer Aspekte
Minimierung Perioperativer Stressfaktoren
preop. Nüchternheit
COX-II-Inhibitors
PDA
Minimal Invasive Surgery
Oblique Incision
No bowel irrigation
Volume restriction
Early enteral nutrition
Mobilisation
PATIENT
Glucose-loading
No drainages, tubes



















