FAO Nutrition Country Profile Brazil (2000)
36
Nutrition Country Profiles – BRAZIL - October, 2000 FAO Rome FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS FAO - NUTRITION COUNTRY PROFILES BRAZIL BRAZIL
-
Upload
nauber-gavski-da-silva -
Category
Documents
-
view
235 -
download
3
description
Nutrition Country Profile Brazil
Transcript of FAO Nutrition Country Profile Brazil (2000)
-
Nutrition Country Profiles BRAZIL - October, 2000 FAO Rome
FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED
NATIONS
FOOD AND AGRICULTURE ORGANIZATION
OF THE UNITED NATIONS
FAO - NUTRITION COUNTRY PROFILES
BRAZILBRAZIL
-
Nutrition Country Profiles - BRAZIL 1
Note for the reader The objective of the Nutrition Country Profiles (NCP) is to provide concise analytical summaries describing the food and nutrition situation in individual countries with background statistics on food-related factors. The profiles present consistent and comparable statistics in a standard format. This pre-defined format combines a set of graphics, tables and maps each supported by a short explanatory text. Information regarding the agricultural production, demography and socio-economic level of the country are also presented. In general, data presented in the NCP are derived from national sources as well as from international databases (FAO, WHO...). Technical notes giving detailed information on the definition and use of the indicators provided in the profile can be obtained from ESNA upon request. An information note describing the objectives of the NCP is also available. Useful suggestions or observations to improve the quality of this product are welcome.
For more information please contact:
E-mail: [email protected]
Nutrition Country Profile of Brazil
prepared by: Maria Antonia M. Galeazzi for the Food and Agriculture Organization the United Nations in collaboration with Rosanne Marchesich (FAO-ESNA).
The designations employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of the Food and Agriculture Organization of the United Nations concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers .
FAO, 2000
-
Nutrition Country Profiles - BRAZIL 2
Table of contents
SUMMARY-------------------------------------------------------------------------------------------------------3
TABLE 1: GENERAL STATISTICS OF BRAZIL -----------------------------------------------------4
I. OVERVIEW ---------------------------------------------------------------------------------------------------5
1. Geography ....................................................................................................................... 5 2. Population........................................................................................................................ 5 3. Level of development: poverty, education and health.................................................. 6 4. Agricultural production, land use and food security..................................................... 7 5. Economy.......................................................................................................................... 8
II. THE FOOD AND NUTRITION SITUATION ----------------------------------------------------------9
1. Trends in energy requirements and energy supplies .................................................. 9 2. Trends in food supplies ................................................................................................10 3. Food consumption ........................................................................................................13 4. Infant feeding practices..................................................................................................15 5. Anthropometric data ......................................................................................................16 6. Micronutrient deficiencies .............................................................................................21
REFERENCES ---------------------------------------------------------------------------------------------- 25
MAPS are presented after the
- General map of Brazil.
- Map 1: Population density by state in 1996.
- Map 2: Prevalence of poverty by state in 1990 (hunger map)
- Map 3: Prevalence of underweight in children under five years of age by state from 1989 to 1992.
- Map 4: Prevalence of stunting among children under five years of age by state from 1989 to 1992.
- Map 5: Prevalence of chronic energy deficiency among women of fertile age by Macro-Region in 1996. Graphs, tables and maps can be visualised by clicking on the words in bold and underline, only in the Full profile pdf file.
-
Nutrition Country Profiles - BRAZIL 3
SUMMARY
The diversification of food patterns in Brazil is strongly related to differences in access to food and food habit. Except for the Amazon region and the arid northeast area of Serto, no large differences in terms of agro-ecological characteristics or agricultural production throughout the country exist. This implies that the main food items, which provide most of the dietary energy supply, are similar from one region to another.
The national prevalence of underweight among children under five years in 1996 was of 6%, which showed an important decrease compared to the 18% in 1975 and the 7% in 1989.The prevalence was higher in rural areas with 9% of underweight compared to urban areas where there were only 5 % of underweight children. In 1992, among the nine states composing the northeast region, Maranho and Piau had the highest prevalence of underweight among children under five years (MOH, 1996; UNICEF, 1995) (Map 3).
Among the northeast states, Maranho and Piau showed the highest prevalences of stunting which corresponded to a high and medium prevalence in these states (Map 4 ). Wasting was not a public health problem
in Brazil: 5% in 1975, 2% in 1989 and 1996 (MOH, 1996; Monteiro, 1991; Monteiro, 1992).
Information concerning the prevalence of overweight showed a decrease from 8% in 1975 to 5% in 1996 (MOH, 1996; Monteiro et al., 1992). The improvement observed in the nutritional status of children under five years of age, between 1975 and 1989, can partly be explained by the important economic growth, the decrease of absolute poverty, as well as the improvement of health services, education and infrastructures.
The prevalence of chronic energy deficiency (BMI
-
Last updated: 16/06/00Indicator () Year Unit Indicator () Year Unit
A. Land in use for agriculture G. Average Food Supply1. Agricultural land 1995 ha per person 1.5392. Arable and permanent crop land 1995 ha per person 0.411 1. Dietary Energy Supply (DES) 1996-98 kcal/caput/day 2960
B. Livestock1. Cattle 1996-98 thousands 1563962. Sheep & goats 1996-98 thousands 306703. Pigs 1996-98 thousands 276734. Chickens 1996-98 millions 868
C. Population1. Total population 1998 thousands 1658502. 0-5 years 1998 % of total pop. 11.63. 6-17 years 1998 % of total pop. 24.74. 18-59 years 1998 % of total pop. 56.25. >= 60 years 1998 % of total pop. 7.56. Rural population 1998 % of total pop. 19.97. Annual population growth rate, Total 1995-2000 % of total pop. 1.98. Annual population growth rate, Rural 1995-2000 % of rural pop. -6.29. Projected total population in 2030 2030 thousands 236100
10. Agricultural population 1995 % of total pop. 19.411. Population density 1995 pop. per km2 18.6
D. Level of Development1. GNP per capita, Atlas Method 1997 current US$ 47902. Human Development Index rating (new) 1997 min[0] - max[1] 0.7393. Incidence of poverty, Total 1990 % of population 174. Incidence of poverty, Rural 1990 % of population 33 % Energy from:5. Life expectancy at birth (both sexes) 1998 years 66.9 2. Protein 1996-98 % of total energy 10.66. Under-five mortality rate 1998 per 1,000 live births 42 3. Fat 1996-98 % of total energy 24.9
E. Food Trade 4. Proteins 1996-98 g/caput/day 76.71. Food Imports (US $) 1996-98 % of total imports 7.8 5. Vegetable products 1996-98 % of total proteins 48.62. Food Exports (US $) 1996-98 % of total exports 15.8 6. Animal products 1996-98 % of total proteins 51.43. Cereal Food Aid (100 t) 1996-98 % of cereals imports 0.0
H. Food InadequacyF. Indices of Food Production 1. Total population "undernourished" 1995-97 millions 16.21. Food Production Index 1996-98 1989-91=100 131.0 2. % population "undernourished" 1995-97 % of total pop. 10.02. Food Production Index Per Capita 1996-98 1989-91=100 118.3
TABLE 1: GENERAL STATISTICS OF BRAZIL
... no data available see References for data sources used
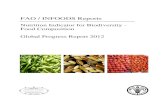
Percentage of DES by major food groups
30.7%
4.8%
19.0%6.0%
4.8%
10.9%
7.9%2.8%
1.6%
11.0%
Cereals (excl. beer)
Starchy roots
Sweeteners
Pulses, nuts, oilcrops
Fruits & Vegetables
Vegetable oils
Animal Fats
Meat & offals
Fish & seafood
Milk & Eggs
Other
Note: Value not indicated if below 1%
-
Nutrition Country Profiles - BRAZIL 5
BRAZIL
I. OVERVIEW
1. Geography
The Federal Republic of Brazil is located in the centre of South America and is bordered by Argentina, Uruguay, Paraguay, Bolivia, Peru, Colombia, Venezuela, Guyana, Suriname, French Guyana and the Atlantic Ocean. Its land area is of 8 511 965 km, with land boundaries adding up to 14 691 km and its coastline stretching to 7408 km. Brazil occupies 48% of the South American continent.
Brazil consists of 5 regions: north, northeast, centerwest, southeast and centersouth; 26 states; a Federal District in the centerwest, where the capital Brasilia is located. There are 5507 municipalities whose political, fiscal and administrative autonomy is enshrined in the Brazilian Constitution of 1988. The number of municipalities in a state varies widely, ranging from 15 in the state of Roraima to 853 in Minas Gerais.
Much of the country consists of hilly uplands, plateau and low mountains, with the Upper Amazon Basin being the largest plain. Three major rivers drain the Highlands, the largest being the Amazon. Four main kinds of vegetation are found in Brazil: tropical rain forests in the Amazon Basin and along the Atlantic coast; semi-deciduous forests from the south part of the state of Natal until Porto Alegre; scrubby thorn woodlands in the northeast and woodland savannah in the interior.
The climate is mainly tropical but presents important differences between regions. The north region is mainly humid with dry seasons, due to the high concentration of water from the Amazonas forest and rivers. The northeast region, which has few perennial rivers, is considered to be the hottest and driest part of the country with recurring drought. The climate in the southeast and centersouth region is mainly sub-tropical with low temperatures at high altitude. The centerwest has mainly tropical rains.
2. Population
In 1998, the Brazilian population was estimated to have almost 166 million inhabitants (UN, 1999) (Table 1). With an estimate total growth rate of 1.9%, from 1995-2000, the expected total population for 2030 is projected to reach 236 million (UN, 1998). The growth rate decreased from 2.7% in 1990-1995 to 1.9% in 1995-2000 (UN, 1999). The rural population decreased due to two main migration periods. The first took place from 1950 to 1970 and was directed towards the southeast and important metropolitan areas, while the second occurred from 1970 to 1990, mainly due to the modernisation of agriculture. Consequently, the overall rural population fell from 50% in 1965 to 20% in 1998. The rural growth rate from 1995 to 2000 was of -6.2%, and the rural population is expected to drop to 11% by 2030 (UN. 1999) (Table 1 and Table 2). The outcome will be a demographic explosion in developed areas and in the main cities.
The populations of the municipalities vary widely. Half of them have fewer than 10 000 inhabitants and account for only 9% of the Brazilian population, while 28 municipalities (under 1%) have more than 500 000 inhabitants, which account for 27% of the population. In 1997, 79% of the
-
Nutrition Country Profiles - BRAZIL 6
population lived in urban areas (ranging from 89% in the southeastern to 74% in the northeast) (PAHO/WHO, 1999). The north represents 45% of the countries total area and includes 7% of the total population. At the state level, the lowest demographic densities are in the north and centerwest regions (with the exception of the Federal District). The highest density is in the southeast, and in particular in Rio de Janeiro and So Paulo. The north and northeast regions respectively host 58% and 61% of the rural area-living people. The most uninhabited areas of the north are occupied by small population groups living on wood cutting, mining extraction and indigenous reserves (IBGE DPE/DEPIS, 1997) (Map 1).
The population distribution by age in 1998 indicates that 36% of the population was under 17 years old, 56% was between 18-59 years and 8% was above 60 years. Life expectancy at birth was 66.9 years for both sexes, from 19952000 (UN, 1999) (Table 1). However, there are differences at the subnational level. Life expectancy in the northeast and south regions was 58 and 65 years respectively. The fertility rate in 1999 was 2.2 (UNICEF, 2000).
The official language of Brazil is Portuguese. Data from the National Household Survey (PNAD) in 1996 indicated that 55% of the total population was white, 6% black, 38% mulatto, the others representing less than 1%).
3. Level of development: poverty, education and health
The Gross National Product (Atlas method) in 1997 was of US$ 4790. In 1990, the national percentage of the population living below the poverty line was of 17%. The rural prevalence was of 33% and the urban prevalence was of 13% (WB, 2001).
In 1996, 7% of the population was unemployed. Unemployment was found to be highest in the centerwest region (8%) (IBGE/PNAD,1996). In the northeast and rural areas the prevalence of poverty was the highest (39%). Poverty in the more industrialised areas (chiefly in the southeastern region) is described as increasingly urban or metropolitan (Rocha, 1996). Based on income distribution, 20% of the Brazilian population with the highest income held 63% of the wealth and the poorest 20%, held only 3% of the wealth (PAHO/WHO,1999).
The adult literacy rate from 19951999 was of 86% for males and of 85% for females (UNICEF, 2000). Regional differences exist: 88% in the north, 61% in the northeast, 87% in the centerwest and 91% in the south and southeast. High illiteracy rates were also found among those over 65 years: 40% of men and 48% of women. The average number of study years is 4.5 among men and 4.6 among women (UNICEF, 2000). In 1997, the Human Development Index (HDI) of Brazil was of 0.739 (UNDP, 1999).
From 1995-1999 all males and 96% of the females were enrolled in primary school. The attendance rate was of 93% for males and of 94% for females. Only 75% of the children completed grade five (UNICEF, 2000).
The under five mortality rate decreased from 177 deaths per 1000 live births in 1960 to 42 deaths per 1000 live births in 1998 (UNICEF, 2000) The decrease was greater in urban areas than in rural areas (INEI, 1996). Infant mortality rate decreased from 115 deaths per 1000 live births in 1960 to 34 deaths per 1000 live births in 1999 (UNICEF, 2000). In particular, from 1990 to 1995 the decline in the infant mortality rate was greater in urban areas, which increased the gap between rural and urban areas. In 1996, the northeast region had the highest prevalence of infant and under five mortality rates. The south region had the lowest prevalence for both rates (INEI, 1996).
Eighty three percent of the national population had improved drinking water in 1999 however there were large urban and rural differences with 89% in urban and only 58% in rural areas.
-
Nutrition Country Profiles - BRAZIL 7
For the same year, seventy two percent of the total population had adequate sanitation facilities with 81% in urban areas and only 32% in rural areas (UNICEF, 2000).
One hundred percent of routine EPI (expanded programme on immunization) vaccines were financed by the government in 1997-1999. Children under one year who were fully immunized against tuberculosis (TB) diphtheria (DPT), polio and measles were 99%, 94%, 96% and 96%, respectively (UNICEF, 2000).
Chronic diseases are slowly replacing infectious and parasitic diseases as the principal cause of mortality. The maternal mortality rate in 1999 was 160 per 100 000 live births (UNICEF, 2000). Maternal mortality, although difficult to estimate, is decreasing as a result of improved access and quality to health services and programmes. Pregnant women immunized against tetanus represented 20% of all pregnant women, from 1997-1999 (UNICEF, 2000). Overall, national access to health services has increased since the late 1980s: an increase in prenatal care coverage from 74% to 85% of expectant mothers, and of deliveries in health establishments from 80% to 91% (PAHO/WHO, 1999). However, the northeast and north regions, especially rural areas, lack available health infrastructures.
4. Agricultural production, land use and food security
In 1996, the agricultural sector generated 10% of GDP (PAHO/WHO, 1999). Brazil is the worlds largest sugar producer accounting for about 13% of world production. Large alcohol stocks, and increases in domestic sugar consumption due to demographic and economic growth, and expanding sugar exports are boosting sugar production.
Brazilian agriculture has maintained an average annual growth rate of about 5% during the last 40 years. In 1999, Brazil was one of the three largest producers of soybean (30 904 232 t), maize (32 178 276 t), cacao (205 899 t), oranges (22 772 180 t), sugarcane (333 314 400 t), cassava (20 932 514 t), banana (55 591 720 t), cashew nuts (124 773 t), pepper (34 581 t), beef (6 182 400 t), chicken (4 905 200 t) and castor seed (25 623 t). The country is among the ten largest producers of pork (1 751 600 t), eggs (1 524 500 t), honey (18 200 t), peanuts (1760 t), rice (11 778 807 t) and milk (22 636 000 t) (FAOSTAT, 1999). About 80% of crop and livestock production is concentrated in the central and southern zones: So Paulo, Mato Grosso do Sul, Sergipe, Rio de Janeiro, Minas Gerais, Bahia, Rio Grande do Sul and Gois. In addition, new agricultural borders, towards the north and centerwest, have increased the annual production of grain (cereals and pulses) over the last 10 years (1989-1999) by 9%. Rice and bean production have remained constant in the last 10 years, however, soy and corn production have increased by 22% and 8% respectively (EIU, 2000).
Brazil's 1999/2000 soybean crop production is being threatened by prolonged dryness. The southern states of Mato Grosso do Dul, Parana and Rio Grande do Sul are lagging behind in soybean production due to the ongoing drought. Vegetation conditions during 1999 were worse than in 1997 and 1998 in the states of Mato Grosso do Sul, Parana, and Rio Grande do Sul, which jointly produce about 51% of Brazil's soybeans (USDA/FAS, 1999).
Land use in Brazil can be broken down into the following categories: arable land (5%), permanent crops (1%), permanent pastures (22%), forests and woodland (58%) and other (14%). The countrys fishing potential, despite its vast coastline, has not been fully utilised (EIU, 2000). In 1995, 1.539 ha per person was agricultural land and 0.411 ha per person was arable and permanent crop land (FAOSTAT, 1999).
-
Nutrition Country Profiles - BRAZIL 8
Despite increased agricultural production, food insecurity is still a problem in Brazil. The main underlying causes are economic access to food, especially in urban areas and were land is insufficient. The problem of food insecurity is party due to the rural crisis and migration to cities as a result of the farm modernisation programme which led to an increase in the basic food prices. In addition, lack of infrastructure in certain areas, led to an increase in transportation and communication costs, resulting in high market prices. Efforts to stabilize the food supply, and include small farmers in the market, are still needed. The acceleration of the agrarian reform and the formulation of a new food supply policy are priority, together with actions to decrease unemployment and decrease income distribution inequalities (EIU, 2000).
In 1990, the Map of Hunger (Map 2) (Peliano, 1993) showed that 32 million people in Brazil were food insecure, which corresponds to 22% of the population. This group had an annual income of about US$170, which is insufficient to buy a food basket. Those who suffer from food insecurity are equally distributed between urban (metropolitan and non-metropolitan) and rural areas. However, non-metropolitan areas are more affected than metropolitan areas, 11.2 and 4.4 million respectively. The northeast and north regions, with the lowest GDP in 1995, present the worst social indicator of Brazil.
The northeast region concentrates the highest number of indigenous people (17.2 million) and the highest number of food insecure (10 million). Rural poverty is usually associated with a less developed infrastructure and poor access to health services. At the state level, Bahia and Minas Gerais present the highest number of food insecure. They are followed by the states Cear of So Paulo, Pernambuco, Paran and Rio de Janeiro (Peliano, 1993).
5. Economy
The Real Plan, implemented in July 1994, resulted in hyperinflation since the plan exposed imbalances in public finances. From 1995-1999 the public sector was not able to generate a primary surplus. This resulted in a proposal to cut public spending, particularly wages and pensions.
Brazil faced a currency crisis that had an impact in early 1999, but a swift policy response allowed the economy to recover more quickly than anticipated, with a growth for 1999 at almost 1%. In Brazil, high domestic interest rates in the second half of 1998 added to the government debt and, alongside lower tax revenues in the wake of the economic slowdown.
The Brazilian exchange rate devaluated after massive losses of reserves. Brazils devaluation, uncertainties in the run-up to elections, and a tighter U.S. monetary policy spread the economic downturn in 1999. The Brazilian devaluation worsened the external environment for many countries in the region. Prices of key commodities exported by Brazil (coffee, soybeans, and sugar) fell sharply in the first half of the year at the same time that Brazilian import demand collapsed, significantly reducing export revenues in a number of countries. However, the expected economic outcome for Brazil is likely to be much better than envisioned and should keep the decline in the regions GDP to about -0.6%. (World Bank, 2000).
-
Nutrition Country Profiles - BRAZIL 9
II. THE FOOD AND NUTRITION SITUATION
1. Trends in energy requirements and energy supplies
Per caput energy requirements1 increased from 1965 to 1997 but are expected to decrease by 2030. At the national level, trends in food requirements reflect the changes in population structure and in particular in the age, sex and urban-rural distribution of the population. The growth in per caput requirements is expected to drop because urbanisation is increasing. The percentage of people living in urban centres has increased by more than half from 1965 and 1997, and the total population almost doubled in the same time period. The per caput dietary energy supply (DES) has followed population growth and the trends in energy requirements, increasing from 2330 kcal/day in 1965 to 2960 kcal/day in 1997, exceeding per caput energy requirements (Table 2) (FAOSTAT, 1999). Table 2: Total population, urbanisation, energy requirements and dietary energy supplies (DES) per person and per day in 1965, 1997 and 2030
*Three-year average calculated for 1964-66 and 1996-98 (Source: FAOSTAT)
The share of fat in total DES has increased from 16% to 25% in the period 1964-1998 while the percentage of carbohydrates decreased from 74% to 65% during the same period. The share of protein in total DES remained the same at 11% during the 32 year period (FAOSTAT, 1999) (Figure 1).
1 Per caput energy requirements are calculated on the basis of the sex and age distribution of the population, using
references for body size, physical activity levels (higher among the rural population, lower among the urban), energy needs for pregnancy and lactation. The method of calculation is derived from James & Schofield (1990). The requirements are exp ressed per average person of the country. Thus requirements are low in young and/or urbanized populations and higher in older or rural populations.
Year 1965 1997 2030
Total population (thousands) 84351 161533 225161
Percentage urban (%) 50.4 79.0 88.9
Per caput energy requirements (kcal/day) 2096 2328 2167
Per caput DES (kcal/day)* 2330 2960 __
-
Nutrition Country Profiles - BRAZIL 10
Figure 1: Share of protein, fat and carbohydrate in Dietary Energy Supply Trends from 1964-66 to 1996-98
64.565.268.669.471.573.373.7
10.6 10.3 9.8 9.6 9.8 9.810.615.7 16.4 18.8
21.0 21.625.0
24.9
0
500
1000
1500
2000
2500
3000
1964-66 1969-71 1974-76 1979-81 1984-86 1989-91 1996-98
DE
S k
cal/c
aput
/day
Carbohydrates Protein Fat Source: FAOSTATBrazil
2. Trends in food supplies
Quantity - Many food groups presented an increase in quantity during the period of 196466 to 199698, in particular fruits and vegetables and milk and eggs, which reached 145 kg/caput/year and 125 kg/caput/year respectively and represent the major food items in Brazil. The supply of cereals also increased slightly over the entire time period but peaked from 19791986. Cereals are now the third major food item. Starchy roots which was the major food group item from 19641971 (123 kg/caput/year) but continually decreased and in 1996-1998, it was the fifth major food item (69 kg/caput/year). This contributes to the overall observed decrease in DES of carbohydrates. Meat and offal, sweeteners and other food groups also increased gradually during the 32 year time period.
Food groups with the lowest availability are pulses, nuts and oilcrops, fish and seafood, vegetable oils and animal fats. Fish and seafood, vegetable oils and animal fats have remained fairly constant over the 32 time period, whilst the pulses, nuts and oilcrops group decreased from 31 kcal/caput/year to 22 kg/caput/year for the same time period (Figure 2).
-
Nutrition Country Profiles - BRAZIL 11
Figure 2: Supplies of major food groups (in kg/caput/year)Trends from 1964-66 to 1996-98
0
25
50
75
100
125
150
1964-66 1969-71 1974-76 1979-81 1984-86 1989-91 1996-98
kg/c
aput
/yea
r
Cereals (excl. beer)
Starchy roots
Sweeteners
Pulses, nuts, oilcrops
Fruits & Vegetables
Vegetable oils
Animal Fats
Meat & offals
Fish & seafood
Milk & Eggs
Other
Energy Through out the entire period, cereals and sweeteners have been the two main food groups as a share of DES, although the first tends to decrease and the second to increase. Cereals have been the main source of energy in Brazil from 196466 to 19961998 from 36% to 31%, respectively (mainly rice). This is followed by sweeteners (mainly sugar) (16% to 19%), meat and offals (5% to 11%), vegetable oils (4% to 11%) and milk and eggs (6% to 8%). The DES of fruits and vegetables and fish and seafood remained constant at 5% and under 1%, respectively, for the entire time period (Figure 3).
Sugar consumption is increasing in Brazil due to population growth as well as to greater consumption of sugar-containing products such as soft drinks, ice cream and candy, which have been stimulated by the Real Plan.
The percent of energy from animal products increased from 13% to 21% and the percent of protein from animal products also increased from 32% to 51%, which can be attributed to the increase in meat and offal consumption. However, the percentage of fat from animal products remained constant at 50%. The percentage of energy from vegetable products decreased from 87% to 79% which can be attributed to the decrease consumption of cereals and starchy roots (11% to 5%) and pulses, nuts and oilcrops (12% to 6%). The percentage of protein from vegetable products decreased from 69% to 49% and the percentage of fat from vegetable products remained constant at 50% (FAOSTAT, 1999).
-
Nutrition Country Profiles - BRAZIL 12
Figure 3: Share of major food groups in Dietary Energy SupplyTrends from 1964-66 to 1996-98
0
500
1000
1500
2000
2500
3000
1964-66 1969-71 1974-76 1979-81 1984-86 1989-91 1996-98
kcal
/cap
ut/d
ay
Cereals (excl. beer)
Starchy roots
Sweeteners
Pulses, nuts, oilcrops
Fruits & Vegetables
Vegetable oils
Animal Fats
Meat & offals
Fish & seafood
Milk & Eggs
Other
Brazil Source: FAOSTAT
Major food imports and exports: Contribution of food import expressed as a percent of DES increased from 11% in 196466 to 21% in 199698. This growth is mainly due to the increase of imported food, in particular cereals (wheat and barley for processing), as a consequence of the open market. In 199698 the import of cereals accounted for 9 616 448 t/year. Until 1979, cereals (mainly wheat) represented total import contribution, however, after 1979, oils crops and eventually vegetable oils and milk and products contributed to the total DES of imports (FAOSTAT, 1999) (Figure 4).
Figure 4: Major food imports as a percentage of Dietary Energy SupplyTrends from 1964-66 to 1996-98
0
5
10
15
20
25
1964-66 1969-71 1974-76 1979-81 1984-86 1989-91 1996-98
% o
f DE
S
Cereals (excl. beer)
Oilcrops
Vegetable Oils
Milk & products
Brazil Source: FAOSTAT
-
Nutrition Country Profiles - BRAZIL 13
Brazil is the worlds largest sugar exporter, accounting for about 13% of world production and 19% of exports (EIU, 2000). Since 1989-91 sugar exports have more than tripled from 4% to 14% of total DES in 199698 or 7 004 892 t/year. There is concern that the financial crisis in eastern Asian markets will reduce some of the Brazilian sugar export potential (FAS, 1998) in the future.
In 19961998 vegetable oils (mainly soybean oil) and oil crops represented 7% of total DES for both groups. Fruits (mainly oranges) represented 4% of total DES or 15 346 080 t/year. Up until 1976, Brazil exported some cereals but since 1979 it has represented less than 1% of the total DES. The export of meat and offals has increased since 19641966 but still only represented 1% of total DES in 19961998 (FAOSTAT, 1999) (Figure 5).
Figure 5: Major food exports as a percentage of Dietary Energy Supply
Trends from 1964-66 to 1996-98
0
10
20
30
40
1964-66 1969-71 1974-76 1979-81 1984-86 1989-91 1996-98
% o
f DE
S
Cereals (excl. beer)
Sweeteners
Oilcrops
Fruit (excl. wine)
Vegetable oils
Brazil Source: FAOSTAT
3. Food consumption
The diversification of food patterns in Brazil are strongly related to differences in access to food and food habits. In fact, except for the Amazon region and the arid northeast area of Serto, no large differences in terms of agro-ecological characteristics or agricultural production throughout the country exist. This implies that the main food items, which provide most of the DES, are similar from one region to another. However, the remote areas listed above consume and produce mostly local traditional foods.
Differences among socio-economic groups are highlighted in the national food consumption study carried out from 197475 as part of the National Survey of Domestic Expenses (ENDEF). This survey was carried out on 55 000 households countrywide and included a seven day weighted food intake. The results indicated that the basic food items for meals were beans, cassava and rice. Cassava was found to be characteristic of the poorest 14% of the population; mainly in rural areas and urban northeast. Rice, on the other hand was the most common food item among affluent populations in the urban and rural areas. Consumption of other food items such as meat, milk, wheat products and fish, were strongly influenced by food habits and food access. In the north and centrewest fish was consumed more often than in other areas (ENDEF, 1975).
In 1974/75, the average energy intake was found to be 1900 kcal/caput/day in the north and northeast and 2400 kcal/caput/day in the south, southeast and centrewest. Protein intake varied from
-
Nutrition Country Profiles - BRAZIL 14
59 g in the southeast to 72 g in the south. Beans were the main source of protein among low income households (ENDEF, 1975).
In the last ten years, fast urbanisation and industrialisation; have contributed to changes in the food habits. In 1987 food consumption data were made available from the Household Expenditure Survey (POF). Results could not be compared to the 1975 survey because of the different methodologies used. One limitation of this study is that the fluctuation in food prices over the 15 year time period may have decreased the accuracy of the food consumption data for this study (IBGE, 1987)
The main findings are that cereals were the principal source of energy intake (17-24% of total DES), followed very closely by sweeteners (13-19% of total DES) and oils/fats (15-21% of total DES). Also, a generally low energy intake was observed, varying from 1616 kcal/caput/day in Goinia to 1754 kcal/caput/day in Curitiba (IBGE, 1987).
In 1996 the Ministry of Health supported a Household Food Consumption survey which included the cities of Braslia, Goinia, Ouro Preto, Campinas and Rio de Janeiro, and in 1997 included Curitiba and Belem. The survey used a methodology, which combined frequency monthly records of food consumption and food expenses. The results, when compared to the 1987 surveys, showed an increase in protein and energy intake. The share of total energy intake of cereals, sweeteners and oils/fats decreased while meat and offals, chicken and eggs and milk increased their share of total energy intake. As a percent of total DES, cereals still occupied the first place (15-18%), except in Rio de Janeiro and Ouro Preto where oils/fats (12%) and sweeteners (18%) exceeded cereals. The consumption of fish was highest in the regions closest to sea shore or to rivers such as Belem in the north (13.3 kg/caput/year) and Rio de Janeiro (11.4 kg/caput/year) close to the Atlantic sea (Table 3) (Galeazzi et al., 1998).
-
Nutrition Country Profiles - BRAZIL 15
Table 3: Food consumption surveys
Source SampleYear of survey Location Number
householdsSex Age
(years)Average food intake
Major Food Groups (kg/caput/year)
CerealsRoots/ Tubers
PulsesFruits/
VegetablesOils/Fats Meat Fish Milk products Sweeteners
Chicken & Eggs
Other
Galeazzi et al. 1998 Rio de Janeiro ... M/F All 66.5 31.6 20.1 253.9 14.6 29.7 11.4 75.5 40.2 31.67 78.7
MOH, 1996 Campinas ... M/F All 75.0 22.0 12.3 172.4 12.7 38.8 4.7 88.7 36.1 27.63 94.7
Ouro Preta ... M/F All 77.3 21.5 18.9 109.5 13.3 29.7 1.6 55.3 40.1 21.68 60.5
Goiania ... M/F All 67.9 18.4 15.2 241.2 21.3 37.2 2.4 79.1 30.9 24.82 58.6
Curitiba ... M/F All 51.9 12.9 13.2 86.1 12.6 11.8 2.6 9.8 35.7 10.24 30.0
Belem ... M/F All 58.7 38.8 13.8 145.0 10.3 48.5 13.3 10.4 31.6 29.19 38.7
Brasila ... M/F All 71.9 20.9 12.9 169.6 17.1 37.8 3.5 74.0 37.6 34.11 55.5
Nutrient Intake (person/day)
Energy (kcal)
% Protein % FatProtein
(g)
% from Animal
products
Fat (g)
% from Animal
products
Galeazzi et al. 1998 Rio de Janeiro ... M/F All 2589 15 26 90 57 69 35
MOH, 1996 Campinas ... M/F All 2279 14 28 82 59 72 42
Ouro Preta ... M/F All 2384 12 27 67 54 65 38
Goiania ... M/F All 2354 13 30 79 56 80 35
Curitiba ... M/F All 2174 14 26 39 33 43 13
Belem ... M/F All 2228 14 24 80 59 61 31
Brasila ... M/F All 2267 13 42 76 56 106 52
Share of major food groups in total energy intake (% kcal)
CerealsRoots/ Tubers
PulsesFruits/
VegetablesOils/Fats Meat Fish Milk products Sweeteners
Chicken & Eggs
Other
Galeazzi et al. 1998 Rio de Janeiro ... M/F All 24.3 4.0 7.7 11.1 12.8 5.2 1 8.6 16.9 4.83 3.3
MOH, 1996 Campinas ... M/F All 28.4 2.5 4.8 7.8 12.9 8.0 1 10.0 16.0 4.41 4.4
Ouro Preta ... M/F All 31.7 2.6 5.7 5.1 14.3 7.1 0 7.9 19.4 3.61 2.4
Goiania ... M/F All 26.5 2.7 5.8 12.5 17.1 7.7 0 8.2 13.2 3.82 2.3
Curitiba ... M/F All 31.7 2.8 6.4 5.6 18.7 3.9 1 2.7 24.1 1.67 2.0
Belem ... M/F All 23.0 13.0 5.5 14.0 9.9 10.3 1 4.1 15.0 2.22 1.7
Brasila ... M/F All 29.1 3.1 5.1 7.1 15.5 8.6 0 8.8 17.1 20.8 2.1
Note: ... Data not available
4. Infant feeding practices
Ninety three percent of the children are breast-fed in Brazil. Among them, 71% are breast-fed during their first day of life. The average duration of breast-feeding is 7 months; however duration varies in different geographical locations. In Rio de Janeiro, the north and the centerwest, the average length of breast-feeding is 10 months, while in the centereast it is 4.4 months. The education level of the mother was not identified as a strong determinant of the differences observed in breastfeeding duration.
Sixty percent of infants under one month were being breast-feed exclusively and it dropped to 34% for infants two to three months old and to 20% for infants from four to six months. A positive correlation was found between the duration of exclusive and increased socio-economic status. The longest duration of exclusive breast-feeding is in urban areas and in the south region. Mothers with a higher education level exclusively breast-fed for longer than mothers who were less educated. Still, the duration of exclusive breast-feeding among infants is short when compared to the WHO recommendations of six months.
Among infants under three months of age, complementary feeding consists mainly of liquids. Solid foods are introduced around 4 months. Roots and tubers are introduced to 19% of infants
-
Nutrition Country Profiles - BRAZIL 16
between the age of four and six months. Infants who were not breastfed receive infant formula. These infants receive solid food and animal proteins within the first four months of life. Cereals are consumed by 17% of bottle fed infants; which is twice as much as breast-fed infants (UNICEF, 1994).
5. Anthropometric data
Anthropometry of children
The nutritional status of children under five years is commonly assessed using three indices: weight-for-height which reflects acute growth disturbances, height-for-age which reflects long-term growth faltering and weight-for-age which is a composite indicator of both long and short term effects. Weights and heights of children are compared with the reference standards (NCHS/CDC/WHO) and the prevalence of anthropometric deficits is usually expressed as the percentage of children below a specific cut-off point such as minus 2 standard deviations (SD) from the median value of the international reference data (WHO, 1983).
The sources of anthropometric data used to describe the nutritional status of the population are the following:
The ENDEF (Estudo Nacional da Despesa Familiar) is a nationwide nutritional survey that was carried out in 1975. It was based on a national probability sample of 36 969 children under five years selected from urban and rural districts from five geographical regions of the country: north, northeast, south, centerwest, southeast. The rural area of both the north and centerwest regions, which in 1980 represented 2% and 3% of the total population respectively, were not included in the sample (Monteiro et al., 1992).
The PNSN (Pesquisa Nacional sobre Sade e Nutrio) is a survey on health and nutrition which was conducted in 1989 on a 7314 children under five years selected within the five previously mentioned geographical regions of the country, excluding the rural area of the north (Monteiro et al., 1991).
In 1996, DHS (Demographic and Health Survey) carried out a survey on 3 815 children under five years. The study included both urban and rural areas (excluding rural areas in the north) of seven predefined macro-regions (north, northeast, south, centerwest, centereast and the states of Rio de Janeiro and So Paulo (MOH, 1996).
The national prevalence of underweight among children under five years in 1996 was 6%, showing a decrease compared to 18% in 1975 and 7% in 1989. In 1996, males (6%) are more affected than females (5%). The highest prevalence was in rural areas (9%) (MOH, 1996; Monteiro et al., 1991; 1992).
In 1992, among the nine states composing the northeast region, Maranho and Piau had the highest prevalence of underweight among children under five years (UNICEF, 1995) (Map 3).
According to the information available on child anthropometry an important improvement occurred between 1975 and 1996 in the nutritional status of children under five at national, regional and state level. The prevalence of stunting decreased from 32% in 1975 to 15% in 1989. However, in 1996, stunting was still the main nutrition problem affecting children under five years, with a prevalence of 11% at the national level and 19% in the rural area (MOH, 1996; Monteiro et al., 1991; 1992) (Table 4a).
-
Nutrition Country Profiles - BRAZIL 17
Still, in 1996, important differences existed between regions, the highest prevalence of stunting was in the northeast (18%) and the lowest prevalence of stunting was in the south (5%). Rio de Janeiro had an even lower prevalence of 3%. (MOH, 1996) (Table 4a).
Among the northeast states in 1992, Maranho and Piau showed the highest prevalences of stunting which corresponded to a high and medium prevalence in these states (UNICEF, 1995) (Map 4).
The differences in income level between regions influence the differences in the level of stunting both directly and indirectly. Nevertheless, it appear that for the same income level, regional disparities in childrens nutritional status persist indicating that factors other than income play an important role in determining regional disparities. These factors relate to education and health.
-
Nutrition Country Profiles - BRAZIL 18
Looking at the situation in the rural and urban area of each region the highest prevalence of
stunting in 1996 was in the rural northeast (25%). However no data are available for the rural area of the north. The 1975 data shows that the rural populations both in the northeast and the centersouth have a much higher prevalence of stunting than in the urban areas of these regions.
In Brazil, the national prevalence of wasting was 5% in 1975 and 2% in 1989 and 1996. At the regional level the prevalence was very low in 1996; 1% in the northeast and less than 1% in the centersouth (MOH, 1996). The prevalence increased slightly for children under 6 months and 6-11 months; 3% and 4%, respectively (BEMFAM, 1997). However, Rio de Janeiro showed a wasting prevalence of 5% (MOH, 1996; Monteiro et al., 1991; 1992) (Table 4a).
Information concerning the prevalence of overweight showed a decrease from 8% in 1975 to 5% in 1989 and 1996. The prevalence of overweight for both sexes in 1975 was slightly higher for males than females (8% and 7%, respectively). In 1996 the prevalence of overweight was 5% for both genders. In 1975 rural areas showed a slightly higher prevalence of overweight than urban areas (8% and 7%, respectively) however, in 1996 the prevalence of overweight was 5% for both areas (MOH, 1996; Monteiro et al., 1992) (Table 4a).
The improvement observed in the nutritional status of children under five between 1975 and 1996 can partly be explained by the important economic growth, the decrease of absolute poverty, as well as the improvement in health services, education and infrastructures, which characterised the 1970-1988 period. In less developed regions improvements were less significant because of limited access to these regions.
No studies were carried out in Brazil to determine adolescent (10 to 19 years old) anthropometry.
-
Nutrition Country Profiles - BRAZIL 19
Table 4a: Anthropometric data on children
Source/ Location Sample
Year of survey Size Sex Age (years)
Percentage of Malnutrition
Underweight Stunting Wasting Overweight% W/A % H/A % W/H % W/H
< -2SD* < -2SD* < -2SD* > +2SD*MOH, 1996 National 3,815 M/F < 5 5.7 10.5 2.3 4.9DHS, 1996 National 1,926 M
-
Nutrition Country Profiles - BRAZIL 20
Anthropometry of adults
The nutritional status of adults was assessed using the body mass index (BMI) calculated as weight (kg) over height squared (m2). For classifying individuals according to their nutritional status, cut-off levels of BMI have been proposed. Adults with a BMI under 18.5 kg/m2 are considered to suffer from chronic energy deficiency (CED). A BMI of more than 25 kg/m2 but under 29.9 kg/m2 indicates overweight and over 30 kg/m2 indicates obesity.
In 1996, the prevalence of CED among women between the ages of 15 to 49 years was 6%. A decrease in the prevalence of CED was observed in the northeast and centersouth region. In 1996, the highest prevalences of CED were found in the rural areas (8%), especially the northeast rural area (9%). Rio de Janeiro also had a prevalence of 9% (Map 5) (BEM FAM, 1997).
While CED decreased, overweight and obesity in this population group increased. The prevalence of overweight at the national level increased from 19% in 1975 to 27% in 1989, while obesity increased from 7% to 12% during the same period. Although not presented in Table 4b, it appears than women are more affected by overweight and obesity than men (Sichieri et al, 1996). In 1989 urban area had a higher prevalence of both overweight and obesity than rural area (BEMFAM, 1997).
In 1996, the mean BMI shows a trend towards overweight and obesity since values are concentrated in the upper limit of the recommended range (24.0 kg/m at the national level). A difference was observed between regions, with the lowest mean BMI found in the northeast (23.4 kg/m) and the highest in the more developed regions of the south (24.8 kg/m) and So Paulo (24.8 kg/m) (BEMFAM, 1997). However, in 1996, the prevalence of both overweight and obesity were higher in rural areas than in urban areas. Overweight and obesity are considered to be a public health problem in Brazil.
-
Nutrition Country Profiles - BRAZIL 21
Table 4b: Anthropometric data on adults Body Mass Index
(kg/m2)Overweight
% BMIObesity % BMI
mean SD median < 18.5 25.0-29.9 >30.0
BEMFAM, 1997 National 2951 F 15-49 24.0 ... ... 6.3
DHS, 1996 Urban 2325 F 15-49 24.1 ... ... 5.8 18.8 6.9
Rural 626 F 15-49 23.6 ... ... 7.8 20.4 7.9
Northeast 927 F 15-49 23.4 ... ... 7.7 15.4 4.8
Northeast urban ... F 15-49 ... ... ... 6.3 ... ...
Northeast rural ... F 15-49 ... ... ... 8.8 ... ...
Centersouth ... F 15-49 24.8 ... ... 5.8 ... ...
Centersouth urban ... F 15-49 ... ... ... 5.8 ... ...
Centersouth rural ... F 15-49 ... ... ... 6.1 ... ...
Rio de Janeiro 258 F 15-49 23.9 ... ... 8.8 ... ...
So Paulo 588 F 15-49 24.8 ... ... 6.4 ... ...
BEMFAM, 1997PNSN, 1989 National 17168 F >18 ... ... 5.8 26.6 11.8
Urban 9325 F >18 ... ... 4.8 27.9 12.6Rural 6565 F >18 ... ... 8.6 21.6 8.8
Northeast ... F >18 ... ... ... 8.4 8.9Northeast urban 1850 F >18 ... ... 5.2 25.4 4.3Northeast rural 1937 F >18 ... ... ... 12.2 17.1 ...Centersouth ... F >18 ... ... ... 4.7 ... 14.3Centersouth urban1742 F >18 ... ... 4.6 ... ...Centersouth rural 1823 F >18 ... ... ... 5.1 ... ...
BEMFAM, 1997ENDEF, 1975 National 65169 F >18 ... ... ... 9.7 18.8 6.9
Urban ... F >18 ... ... ... ... ... ...Rural ... F >18 ... ... ... ... ... ...Northeast ... F >18 ... ... ... 11.8 ... ...Northeast urban ... F >18 ... ... ... 10.8 ... ...Northeast rural ... F >18 ... ... ... 13.3 ... ...Centersouth ... F >18 ... ... ... 7.8 ... ...Centersouth urban ... F >18 ... ... ... 7.1 ...Centersouth rural ... F >18 ... ... ... 9.6 ... ...
Chronic Energy Deficiency
% BMI
Notes: ... Data not available
6. Micronutrient deficiencies
Iodine Deficiency Disorders (IDD):
Iodine deficiency disorders (IDD) include the clinical and sub-clinical manifestations of iodine deficiency. Iodine deficiency in pregnant women may cause irreversible brain damage in the developing foetus, whereas in infants and young children it may cause psychomotor retardation and intellectual impairment. Total goitre rate (TGR) is the proportion of the population with a prevalence of goitre for all grades combining both palpable and visible goitre.
Iodine deficiency was assessed in 1975 through a national survey conducted on 421 756 children from 7 to 14 years of age. The results indicated a national prevalence of TGR of 14% (not in Table). At the state level, the highest prevalences were in Bahia, Minas Gerais, Maranho and Rondonia and prevalences varied from 25% to 33%. These corresponded to moderate to severe prevalences of IDD in Brazil at the different state levels (WHO, 1982). Later, in 1984, school children from the states of Goias, Par, Maranho, Minas Gerais and Bahia were found to have a prevalence of TGR that was greater than 30%.
In 1994/95 a national survey was carried out among school children from 6 to 14 years from 428 municipalities. The results showed a national TGR prevalence of 4%. The most prevalent levels were detected in the States of Mato Grosso do Sul and Roraima (20% for both).
-
Nutrition Country Profiles - BRAZIL 22
Since 1983 the Ministry of Health has closely monitored the mandatory iodization of table salt. In 1996, measurements carried out by the DHS on salt iodization found that more than 95% of household salt was iodized. The smallest values (90-92%) were found in the rural area and in the north region (UNICEF, 1998).
Iron Deficiency anaemia (IDA):
The consequences of iron deficiency anaemia (IDA) include reduced physical work capacity and productivity, impaired cognitive functions and brain metabolism and reduced immuno-competence. The causes of IDA include low dietary intake in relation to the recommended dietary allowances (RDA), poor bio-availability of iron in the diet, malaria and a high prevalence of parasitic infestations.
In 1998, 590 children under five years from the state of Pernambuco were studied using a heamoglobin cut off point of under 11 g/dL. A 48% prevalence of IDA was found and the prevalence was higher in the rural areas (56%) than in the urban areas (41%) (INAN/MS - IMIP - DN/UFPE - SES/PE, 1998).
In 1992, in the state of So Paulo (southeast), 2992 children from 6 to 24 months of age were examined using a haemoglobin cut-off point of 11 g/dL. The results, considered representative for the state, indicated a 59% prevalence of IDA (Torres de Almeida, 1992). In the same year, 363 pregnant women were screened by the health department of the district of Butantan (So Paulo City) and a 12% prevalence of IDA was determined using a haemoglobin cut-off point of 11 g/dL (Guerra et al., 1992). There is no information available on the actions carried out to control iron deficiency in Brazil (Table 5).
Vitamin A Deficiency (VAD):
Vitamin A is an essential micronutrient required for normal health and survival. It is involved in several critical functions in the body including vision, immune system, reproduction, growth and development. Children under five years are most susceptible to VAD. The consequences of VAD are tragic: they include night blindness, irreversible blindness, growth retardation and increased susceptibility to infections. Pregnant women are also prone to VAD and their children are likely to become deficient.
Several studies on VAD have been carried out during the last 20 years. They are all locally based surveys, which mainly concern states and cities and/or particular area or population groups.
In the northeast region VAD was reported in several studies in the past decades. Among them, the most significant are described below and were carried out in the states of Paraiba, Bahia , Pernambuco, Cear and Rio Grande do Norte.
In the state of Paraba, an epidemiological survey was conducted in 1981/82 on 5561 children under 12 years from six localities representative of the three different ecological regions of the state (Santos et al, 1983). Clinical signs of VAD were found only in the semiarid region (Serto). Prevalence of Bitot spot (X1B) was 0.6% and the prevalence of corneal scars (X3) was 0.1%, both being above the critical level and confirming VAD to be a public health problem in Serto (WHO, 1995). School children (five to under twelve years) had a higher prevalence of Bitot spots (0.9%) and night blindness (XN) (1.8%) than children under five years (0.3% and 0.2%, respectively). When comparing the harvest seasons results with the interharvest season results, the study shows seasonal variation, with a higher prevalence of xerophthalmia during the interharvest period and most prominent in the Serto area compared to the other areas studied (Table 5)
-
Nutrition Country Profiles - BRAZIL 23
These data were confirmed in a successive study carried out in the same state among children under six years. Moreover, this survey demonstrated that severe xerophthalmia occurred mainly among very young children, even among infant below six months of age living in the Coastal region. Mild xerophthalmia affected mostly older children from the semi-arid area of Serto. In the first case, breast-feeding practices may have played an important role in the development of VAD, since in the area, 21% of children were never breast-fed and infants were often weaned during the second month of life. In the second case, VAD could be explained mainly by irregularity in crop production and the low availability of fruits and green leafy vegetables (DAns et al, 1987; 1988).
A similar study was undertaken in 1989 among 563 children under five years in the urban area (7 small towns) of the semi-arid zone of the state of Bahia. No clinical sign of deficiency were registered but more than 5% of serum retinol levels where below the cut-off point of under 0.70mol/L. Therefore VAD was classified as a public health problem in the seven localities investigated (WHO, 1982). A 24 hours food consumption survey carried out at the same time revealing that only 8% of children had an adequate intake of vitamin A; 66% received under half of the recommended daily intake (Santos et al, 1996).
In the same year, levels of serum retinol were measured in 2619 children from 2 to 6 years of age from a representative sample of the city of Recife (state of Pernambuco) and the prevalence of VAD was 34% (Santos et al, 1996).
In 1986, 6291 children under five years from 3 towns of the semi-arid area of the state of Rio Grande do Norte were screened for clinical signs of VAD. The prevalence of Bitots spot was found to be 0.6% confirming that VAD in this particular area is a public health problem (Mariath et al., 1989) (Table 5).
In the same year, in the southeast region, a study was carried out in health units located in the poor areas of the city of Rio de Janeiro. The prevalence of VAD on the basis of the serum retinol levels under 0.70g/L varied from 14% in pregnant women to 56% in new-borns.
In the north region, a study was carried out in 1998 among children under five years from the city of Belm (state of Par). The results found a 12% prevalence of VAD. In the same year, in the southeast region, a study was carried out in health units located in the poor areas of the city of Rio de Janeiro. The prevalence of VAD on the basis of the serum retinol level varied from 14% in pregnant women to 56% in new-borns (Teixeria, 1998).
-
Nutrition Country Profiles - BRAZIL 24
Table 5: Surveys on micronutrient deficiencies
Source/ Deficiency Location Sample %Year of survey Size Sex Age Years
Iron
Torres de Almeida, 1992
1992 Hb < 11 g/dL State of So Paulo 2992 M/F 0.5 - 2 59.0
Guerra et al., 1992
1992 Hb < 11 g/dL So Paulo city (2) 363 F pregnant women 12.0
INAN/MS - IMIP - DN/UFPE State of Pernambuco
SES/PE, 1998 Hb < 11 g/dL Total 590 M/F < 5 48.0
" Urban 249 M/F < 5 41.0" Rural 251 M/F < 5 56.0
Vitamin A
Santos et al, 1983 State of Paraba
1981/1982 XN Serto (Semi-arid area) 4991 M/F
-
Nutrition Country Profiles - BRAZIL 25
REFERENCES
BEMFAM. 1997. Sade da Mulher e da Criana, in : Pesquisa Nacional Sobre Demografia e Sade-PNDS 1996. Rio de Janeiro.
DAns, C., Dricot, J., Diniz, A.S., Mariath, J.G.R. & Santos, L.M.P. 1988. Geographic distribution of xerophthalmia in the state of Paraiba, northeast Brazil. Ecology of Food and Nutrition 1988; 22: 131-138.
D'Ans, C., Dricot, J.M. & Mariath, J.G. 1987. Vitamin A periodic dosing in the state of Paraiba, Northeast Brasil. Xeroph Club Bull 1987;35:3-4.
EIU (Economist Intelligence Unit). 2000. Brazil Country Profile, 2000. Website at: http://db.eiu.com/report_dl.asp?mode=pdf&valname=CP9BRA
ENDEF. 1975. Estudo Nacional de Despesad Familiares-1975 Instituto Brasiuleiro de Geografica e estadstica (IBGE).Brazil.
FAOSTAT. 1999. FAO web page. Statistics database. FAO, Rome.
FAS ( Federation of American Scientists ). 1998. Brazilian Sugar Production and Exports Set Records ( http://www.fas.usda.gov/htp2/sugar/1998/98-05/may98cover.html )
Galeazzi. M.A. M. & Falchoni, P. Jnr. 1998. Inqurito de Consumo Alimentar da rea Metropolitana de Braslia- Relatrio Tcnico-Secretaria de Sade de Braslia.
Guerra, E.M. 1992. Prvalencia de deficincia de ferro em gestante de primera consulta em centros de sade de rea metropolitana- Ver. Sade pblica 26(2):88-95.
IBGE (Instituto Brasileiro de Geografia e Estatstica). 1987. Pesquisa de Oramentos Familiares (POF). Brazil.
IBGE DPE/DEPIS. 1997. Projees Populacionais: Brasil e Grandes Regies. Brazil.
IBGE/PNAD. 1996. Pesquisa Nacional por Amostra de Domiclios. Brazil.
INAN/MS IMIP DN/UFPE SES/PE. 1998. - Sade, nutrio, alimentao e condies socioeconmicas no Estado de Pernambuco. Brazil.
INEI. 1996. Encuesta Demogrfica y de Salud Familiar 1996 (ENDES). Brazil.
James, W.P.T. & Schofield, E,C. 1990. Human Energy Requirements. A manual for planners and nutritionists. FAO & Oxford Medical Publications. New York.
-
Nutrition Country Profiles - BRAZIL 26
Lira, P.I.C., Cartagena, H.A., & Mello, R. 1985. Estado nutricional de crianas menores de seis anos, segundo posse da terra, em areas rurais do estado de Pernambuco, nordeste do Brasil. Arch Latinoam Nutr 1985; 35(2):247-57.
Mariath, J.G.R. et al., 1989. Vitamin A activity of buriti (Mauritia vinifera Mart) and its effectiveness in the treatment and prevention of xerophthalmia. Am J Clin Nutr 1989;49;849-853.
MOH ( Ministry of Health ). 1996. Pesquisa nacional sobre demografia e sade 1996 (relatorio preliminar ). Demographic and health surveys. Rio de Janeiro, Brasil.
Monteiro, C.A. 1987. Estudos das condies de sade das crianas do Municpo de So Paulo (1984/85). V. Anemia. Rev. Sade pbl., 21 (3): 255-60.
Monteiro, C.A., Benicio M.H. & Gouveia, N.C. 1991. Growth and nutrition status of t he Brazilian children: findings from the 1989 National Health and Nutrition Survey. Country Studies on Nutrition Anthropometry NUT/ANTREF/1/91. World Health Organization. Geneva, Switzerland.
Monteiro, C.A., Benicio, M.H., Iunes R., Gouveia, N.C. Taddei, J.A. & Cardosos, M.A. 1992. Nutrition status of Brazilian children: trends from 1975 to 1989. Bulletin of the World Health Organization 1992:70:657-666.
PAHO/WHO. 1999. Health Systems and Services Profile for Brazil, Washington DC, USA.
Peliano, M.T.M. 1993. O Mapa da Fome: Subsdios Formulao de uma Poltica de Segurana Alimentar. Rio de Janeiro: IPEA, March, 1993 (Documento de Poltica, 14).
Rocha, S. 1996. Poverty Studies in Brazil, Review. IPEA (Instituto de Pesquisa Econmica Aplicada ) Rio de Janeiro.
Santos, L.M., Assis, M.O. & Martins, M.C. 1996. Nutritional status of pre-school children in the semi-arid region of Bahia (Brasil): II Vitamin A deficiency. Rev. Sade Pblica, 30 (1): 67-74.
Santos, L.M.P., Dricot, J.M., Ascuitti, L.S. & D'Ans C. 1983. Xerophthalmia in the state of Paraiba, northeast of Brazil: clinical findings. Am. J. Clin. Nutr. 38, 139-144.
Sichieri, R., Mathias, T. & Moura, A.S. 1996. Stunting, high weight-for-height, anemia and dietary intake among Brazilian students from a rural community. Nutrition Research, Vol. 16. No. 2, pp. 201-209.
Texeiea, D.E.T.A. 1998. Determinaco dos nveis sricos de retinol e ferro em criancas menores de 5 anos na cidade de Belm. Universidade Federal do Par, Belm. Mimeo.
-
Nutrition Country Profiles - BRAZIL 27
Torres M.A.de Almeida. 1992. Anaemia Carencial Ferropriva No Estado de So Paulo : Situao Actual e Formas de Interveno- Secretaria do Estado da Sade So Paulo, Brasil.
UN. 1998. World Urbanisation Prospects. 1996 Revision. United Nations Population Division. New York.
UN. 1999. World Urbanisation Prospects Database 1950-2050. The 1998 Revision. United Nations Population Division. New York.
UNDP (United Nations Development Programme). 1999. Human Development Report. Oxford University Press. New York.
UNICEF. 1994. Diagnstico de sade materno infantil no estado de sergipe. Governo de SERGIPE. Brazil.
UNICEF. 1995. Sade e Nutrico das Criancas Nordestinas. Pesquisas estaduais 1987-1992. Brazil.
UNICEF. 1998. A Infncia Brasilera nos Anos 90. Braslia Brasil.
UNICEF. 2000. The state of the worlds children 2000. United Nations Childrens Fund. Oxford University Press. New York.
USDA/FAS. 1999
WHO. 1982. Joint WHO/UNICEF/USAID/HKI/IVACG meeting. Control of vitamin A deficiency and xerophthalmia. Jakarta, 1980. Report. Geneva, 1982. (WHO Technical Report Series, 672).
WHO. 1983. Measuring change in nutritional status. Geneva, Switzerland
World Bank. 2000. The World Development Indicators 1999 CD-ROM. Win*STARS System Version 4.0. World Bank, Washington, D.C.
World Bank. 2001. The World Development Indicators 2000 CD-ROM. Win*STARS System Version 5.0. World Bank, Washington, D.C.
-
Nutrition Country Profiles - BRAZIL 28
References of data presented in Table 1, unless otherwise stated:
Source: Indicator:
FAOSTAT. 1999 A.1-2, B, C.10-11, E.1-3, F, G
UN. 1998/1999 rev. C.1-9, D.5
World Bank. 1999. D.1,
WB. 2001. D.3-4
UNDP. 1997. D.2
UNICEF. 2000. D.6
SOFI. 1999. H
-
Nutrition Country Profiles - BRAZIL 29
NCP of BRAZIL MAPS
- General map of Brazil. - Map 1: Population density by state in 1996. - Map 2: Prevalence of poverty by state in 1990 (hunger map). - Map 3: Prevalence of underweight among children under five years of age by state in 1989-1992. - Map 4: Prevalence of stunting among children less than five years of age by state in 1989-1992. - Map 5: Prevalence of chronic energy deficiency among women of fertile age by Macro-Region in 1996.
-
General Map of Brazil
Scale 1:28 000 000 (approx.)
Geographic Projection (Lat/Long)
N
EW
S
Brazil
FAO-GIS (SDRN)/ESNA, March 1998
The designations employed and the presentation of the material in the maps do not imply the expression
of any opinion whatsoever on the part of FAO concerning the legal or constitutional status of any country,
territory or sea area, or concerning the delimitation of frontiers.
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
Boa Vista
Manaus
Porto Velho
Rio Branco
Cuiaba
Campo Grande
Goiania
Belo Horizonte
Vitoria
Salvador
Aracaju
Maceio
Recife
Joao Pessoa
Natal
Fortaleza
Teresina
Palmas
Belem
Macapa
Sao Paulo
Curitiba
Florianopolis
Porto Alegre
Rio de Janeiro
Brasilia
State
#
Main Cities
Main Rivers
&V
&V Capital
-
BAHIA
SAO PAULO
PIAUI
MARANHAO
CEARA
RIO GRANDE DO NORTE
PARAIBA
PERNAMBUCO
ALAGOAS
SERGIPE
AMAZONAS
PARA
AMAPA
RORAIMA
RONDONIA
ACRE
MATO GROSSO
TOCANTINS
GOIAS
MINAS GERAIS
ESPIRITO SANTO
MATO GROSSO DO SUL
PARANA
SANTA CATARINA
RIO GRANDE DO SUL
RIO DE JANEIRO
&V
&V
Capital
Source: IBGE DPE/DEPIS, 1997
Map 1: Population density by State in 1996
The designations employed and the presentation of the material in the maps do not imply the expression
of any opinion whatsoever on the part of FAO concerning the legal or constitutional status of any country,
territory or sea area, or concerning the delimitation of frontiers.
Population / Km
0 - 9,9
10,0 - 49,9
50,0 - 99,9
100,0 - 199,9
>= 200,0
Scale 1:28 000 000 (approx.)
Geographic Projection (Lat/Long)
N
EW
S
Brazil
FAO-GIS (SDRN)/ESNA, March 1998
-
Source: Peliano, 1993 (IPEA)
Map 2: Prevalence of poverty by state in 1990 (Hunger map)
The designations employed and the presentation of the material in the maps do not imply the expression
of any opinion whatsoever on the part of FAO concerning the legal or constitutional status of any country,
territory or sea area, or concerning the delimitation of frontiers.
BAHIA
SAO PAULO
PIAUI
MARANHAO
CEARA
RIO GRANDE DO NORTE
PARAIBA
PERNAMBUCO
ALAGOAS
SERGIPE
AMAZONAS
PARA
AMAPA
RORAIMA
RONDONIA
ACRE
MATO GROSSO
TOCANTINS
GOIAS
MINAS GERAIS
ESPIRITO SANTO
MATO GROSSO DO SUL
PARANA
SANTA CATARINA
RIO GRANDE DO SUL
RIO DE JANEIRO
1.419.603
87.293
105.320
2.573.571
1.718.408
546.943
208.921
5.127.772
4.900.216
1.752.919
32.432.027
9.096.924
15.606.971
11.525.866
2.633.200
6.427.695
2.312.310
3.236.088
7.181.242
2.418.107
1.401.811
2.504.154
13.929.217
4.437.013
9.020.119
&V
&V Distrito Federal
Note: The State of Tocantins was still in 1990 part of the State of Goias.
% of food insecure
population
No data available
0 - 1.9
2.0 - 4.9
5.0 - 9.9
10.0 - 14.9
Scale 1:28 000 000 (approx.)
Geographic Projection (Lat/Long)
N
EW
S
Brazil
FAO-GIS (SDRN)/ESNA, March 1998
-
BAHIA
SAO PAULO
PIAUI
MARANHAO
CEARA
RIO GRANDE DO NORTE
PARAIBA
PERNAMBUCO
ALAGOAS
SERGIPE
AMAZONAS
PARA
AMAPA
RORAIMA
RONDONIA
ACRE
MATO GROSSO
TOCANTINS
GOIAS
MINAS GERAIS
ESPIRITO SANTO
MATO GROSSO DO SUL
PARANA
SANTA CATARINA
RIO GRANDE DO SUL
RIO DE JANEIRO
Source: UNICEF, 1995
Map 3: Prevalence of underweight among children
less than 5 years by state in 1989-1992
The designations employed and the presentation of the material in the maps do not imply the expression
of any opinion whatsoever on the part of FAO concerning the legal or constitutional status of any country,
territory or sea area, or concerning the delimitation of frontiers.
% weight for age < -2 SD
No data available
< 5.0
5.0 - 9.9
10.0 - 14.9
15.0 - 19.9
&V
Capital
&V
Scale 1:28 000 000 (approx.)
Geographic Projection (Lat/Long)
N
EW
S
Brazil
FAO-GIS (SDRN)/ESNA, March 1998
-
BAHIA
SAO PAULO
PIAUI
MARANHAO
CEARA
RIO GRANDE DO NORTE
PARAIBA
PERNAMBUCO
ALAGOAS
SERGIPE
AMAZONAS
PARA
AMAPA
RORAIMA
RONDONIA
ACRE
MATO GROSSO
TOCANTINS
GOIAS
MINAS GERAIS
ESPIRITO SANTO
MATO GROSSO DO SUL
PARANA
SANTA CATARINA
RIO GRANDE DO SUL
RIO DE JANEIRO
The designations employed and the presentation of the material in the maps do not imply the expression
of any opinion whatsoever on the part of FAO concerning the legal or constitutional status of any country,
territory or sea area, or concerning the delimitation of frontiers.
Map 4: Prevalence of stunting among children
less than 5 years by state in 1989-1992
% height for age < -2 SD
No data available
< 5.0
5.0 - 9.9
10.0 - 19.9
20.0 - 29.9
30.0 - 39.9
Source: UNICEF, 1995
Note: State of CEARA ( 0-36 months )
&V
Capital
&V
Scale 1:28 000 000 (approx.)
Geographic Projection (Lat/Long)
N
EW
S
Brazil
FAO-GIS (SDRN)/ESNA, March 1998
-
SUL
RIO DE JANEIRO
SAO PAULO
CENTRO-LESTE
CENTRO-OESTE
NORDESTE
NORTE
The designations employed and the presentation of the material in the maps do not imply the expression
of any opinion whatsoever on the part of FAO concerning the legal or constitutional status of any country,
territory or sea area, or concerning the delimitation of frontiers.
Source: Bemfam, 1997
Map 5: Prevalence of chronic energy deficiency among women
of fertile age (*) by Macro-Region in 1996
% BMI < 18.5 (kg/m)
No data available
2.5 - 4.9
5.0 - 6.9
7.0 - 9.9
(*) - mothers (15-49 years)
&V
Capital
&V
Scale 1:28 000 000 (approx.)
Geographic Projection (Lat/Long)
N
EW
S
Brazil
FAO-GIS (SDRN)/ESNA, March 1998
BRAZILSUMMARYTABLE 1: GENERAL STATISTICS OF BRAZILI. OVERVIEW1. Geopgraphy2. Population3. Level of development: poverty, education and health4. Agricultural production, land use and food security5. Economy
II. THE FOOS AND NUTRITION SITUATION1. Trends in energy requirments and energy supplies2. Trends in food supplies3. Food consumption4. Infant feeding practices5. Anthropometric data6. Micronutrient deficiencies
REFERENCESMAPSOctober, 2000