
Family-Based Therapy for Adolescent Drug Abuse: Knowns … · Family-Based Therapy for Adolescent...
30
Clinical Child and Family Psychology Review, Vol. 3, No. 4, 2000 Family-Based Therapy for Adolescent Drug Abuse: Knowns and Unknowns Timothy J. Ozechowski 1 and Howard A. Liddle 1,2 Family-based therapy is one of the most thoroughly studied treatments for adolescent drug abuse. Considerable empirical support exists for the efficacy of family-based therapy in curtailing adolescent drug use and cooccurring behavior problems. This article extends knowl- edge of the effects of family-based therapy for adolescent drug abuse by reviewing 16 controlled trials and 4 therapy process studies from a treatment development perspective. We articulate ‘‘knowns and unknowns’’ regarding the outcomes of treatment as well as the components, processes, mechanisms, moderators, and boundaries of effective family-based therapy for adolescent drug abuse. The review highlights areas of progress and future research needs within the specialty of family-based therapy for adolescent drug abuse. KEY WORDS: adolescent drug abuse; family-based therapy; treatment outcome; treatment devel- opment. Family-based therapy is one of the most thor- oughly studied treatment modalities for adolescent drug abuse (Weinberg, Rahdert, Colliver, & Glantz, 1998). Research reviews have documented ‘‘promis- ing but not definitive’’ (Liddle & Dakof, 1995a, p. 511) evidence of the efficacy of family-based therapy for treating adolescent drug abuse and associated behavior problems (Liddle & Dakof 1995a,b; Stan- ton & Shadish, 1997; Waldron, 1997). Family-based interventions have been supported across various sectors of the adolescent drug abuse treatment and research communities (Liddle, 1996). For instance, the American Academy of Child and Adolescent Psychiatry (AACAP) included family-based therapy within its recommended practice parameters for adolescent drug abuse treatment (AACAP, 1997). In the revised Treatment Improvement Protocol Series (TIPS) for adolescent substance abuse (CSAT, 1999), empirically supported family thera- 1 Center for Treatment Research on Adolescent Drug Abuse (M711), Department of Psychiatry and Behavioral Sciences, Uni- versity of Miami School of Medicine, PO Box 019132, 1400 NW 10th Avenue, Suite 1108, Miami FL 33136 USA. 2 Correspondence regarding this manuscript should be addressed to Howard A. Liddle, Ed.D. E-mail: [email protected] 269 1096-4037/00/1200-0269$18.00/0 2000 Plenum Publishing Corporation pies received prominent coverage. Clinical reviews of adolescent drug abuse treatment approaches have acknowledged family-based therapy as a core inter- vention modality (Crits-Cristoph & Sequeland, 1996; Gilvarry, 2000; Weinberg et al., 1998; Williams & Chang, 2000; Winters, Latimer, & Stinchfield, 1999). Family-based treatments are well represented among past and currently funded research projects in the National Institute on Drug Abuse (NIDA) and Center for Substance Abuse Treatment and Center for Substance Abuse Prevention portfolios, and new announcements that are inclusive of family- based treatments for adolescent drug problems are common in several agencies on the prevention and treatment research sections. 3 3 National Institute on Drug Abuse, PA-97-005 Research on Ado- lescent Drug Abuse; National Institute on Alcohol Abuse and Alcoholism, PA-97-055 Mechanisms of Adolescent Alcohol Abuse and Alcoholism; Center for Substance Abuse Treatment, TI-98-07 Adolescent Treatment Models; Center for Substance Abuse Prevention, SP-00-002 Family Strengthening. Announce- ments such as these are funding a new generation of theory-driven, manualized family-based treatment and prevention approaches. Also, the National Institute on Drug Abuse supports a research center and a research training program focusing on family-based treatments for adolescent drug abuse (Liddle & Hogue, in press).
-
Upload
vuonghuong -
Category
Documents
-
view
214 -
download
0
Transcript of Family-Based Therapy for Adolescent Drug Abuse: Knowns … · Family-Based Therapy for Adolescent...

Clinical Child and Family Psychology Review, Vol. 3, No. 4, 2000
Family-Based Therapy for Adolescent Drug Abuse:Knowns and Unknowns
Timothy J. Ozechowski1 and Howard A. Liddle1,2
Family-based therapy is one of the most thoroughly studied treatments for adolescent drugabuse. Considerable empirical support exists for the efficacy of family-based therapy incurtailing adolescent drug use and cooccurring behavior problems. This article extends knowl-edge of the effects of family-based therapy for adolescent drug abuse by reviewing 16controlled trials and 4 therapy process studies from a treatment development perspective.We articulate ‘‘knowns and unknowns’’ regarding the outcomes of treatment as well as thecomponents, processes, mechanisms, moderators, and boundaries of effective family-basedtherapy for adolescent drug abuse. The review highlights areas of progress and future researchneeds within the specialty of family-based therapy for adolescent drug abuse.
KEY WORDS: adolescent drug abuse; family-based therapy; treatment outcome; treatment devel-opment.
Family-based therapy is one of the most thor-oughly studied treatment modalities for adolescentdrug abuse (Weinberg, Rahdert, Colliver, & Glantz,1998). Research reviews have documented ‘‘promis-ing but not definitive’’ (Liddle & Dakof, 1995a, p.511) evidence of the efficacy of family-based therapyfor treating adolescent drug abuse and associatedbehavior problems (Liddle & Dakof 1995a,b; Stan-ton & Shadish, 1997; Waldron, 1997). Family-basedinterventions have been supported across varioussectors of the adolescent drug abuse treatment andresearch communities (Liddle, 1996). For instance,the American Academy of Child and AdolescentPsychiatry (AACAP) included family-based therapywithin its recommended practice parameters foradolescent drug abuse treatment (AACAP, 1997).In the revised Treatment Improvement ProtocolSeries (TIPS) for adolescent substance abuse(CSAT, 1999), empirically supported family thera-
1Center for Treatment Research on Adolescent Drug Abuse(M711), Department of Psychiatry and Behavioral Sciences, Uni-versity of Miami School of Medicine, PO Box 019132, 1400 NW10th Avenue, Suite 1108, Miami FL 33136 USA.
2Correspondence regarding this manuscript should be addressedto Howard A. Liddle, Ed.D. E-mail: [email protected]
269
1096-4037/00/1200-0269$18.00/0 2000 Plenum Publishing Corporation
pies received prominent coverage. Clinical reviewsof adolescent drug abuse treatment approaches haveacknowledged family-based therapy as a core inter-vention modality (Crits-Cristoph & Sequeland, 1996;Gilvarry, 2000; Weinberg et al., 1998; Williams &Chang, 2000; Winters, Latimer, & Stinchfield, 1999).Family-based treatments are well representedamong past and currently funded research projectsin the National Institute on Drug Abuse (NIDA)and Center for Substance Abuse Treatment andCenter for Substance Abuse Prevention portfolios,and new announcements that are inclusive of family-based treatments for adolescent drug problems arecommon in several agencies on the prevention andtreatment research sections.3
3National Institute on Drug Abuse, PA-97-005 Research on Ado-lescent Drug Abuse; National Institute on Alcohol Abuse andAlcoholism, PA-97-055 Mechanisms of Adolescent AlcoholAbuse and Alcoholism; Center for Substance Abuse Treatment,TI-98-07 Adolescent Treatment Models; Center for SubstanceAbuse Prevention, SP-00-002 Family Strengthening. Announce-ments such as these are funding a new generation of theory-driven,manualized family-based treatment and prevention approaches.Also, the National Institute on Drug Abuse supports a researchcenter and a research training program focusing on family-basedtreatments for adolescent drug abuse (Liddle & Hogue, in press).

270 Ozechowski and Liddle
This article extends previous reviews of the em-pirical literature on family-based therapy for adoles-cent drug abuse by evaluating existing research oncore criteria in contemporary intervention science(Kazdin, 1994a). Guidelines and blueprints for treat-ment development research have been articulatedwithin the psychotherapy research literature (seeCarrol & Rounsaville, 1990; Chambliss & Hollon,1998; Docherty, 1984; Kazdin, 1994a, 1997; Kazdin &Kendall, 1998; Onken, Blaine, & Battjes, 1997). Al-though not identical, taken together, these frame-works articulate standards and criteria for conductingprogrammatic research that would establish the com-ponents, processes, mechanisms, and boundaries ofeffective treatments for well-defined clinical prob-lems and patient populations. This review evaluatesresearch on family-based therapy for adolescent drugabuse from a treatment development perspective.Specifically, in specifying the knowns and unknownsabout the empirically supported family-based treat-ments for adolescent drug abuse, we aim to offer areport of the developmental status of this specialty.We highlight dimensions of treatment developmentprogress as well as areas that have been understudied,and we make recommendations about how coordi-nated research efforts on family-based therapy foradolescent drug abuse might be made to havemore impact.
The term family-based therapy for adolescentdrug abuse actually describes a collection of interven-tion models, some of which have been in develop-ment and testing since the late 1970s. Although eachmodel regards the family as a primary interventionunit, models vary in how extrafamilial influences orsystems are addressed. The review begins by high-lighting key theoretical and clinical components ofdifferent family-based treatments for adolescent drugand behavioral problems. Then, we outline theknowns and unknowns about how, for whom, andunder what conditions family-based therapy for ado-lescent drug abuse is effective. This interpretation isbased on the findings of existing controlled trials andprocess studies.
THEORETICAL FOUNDATIONS OF FAMILY-BASED THERAPY FOR ADOLESCENTDRUG ABUSE
Family Systems Theory
A conceptual cornerstone of all family-basedtreatments for adolescent drug abuse is family sys-
tems theory (Hoffman, 1981; Nichols & Schwartz,1998). Perhaps the most enduring and influential as-pect of this theoretical system is its emphasis on therelational and contextual nature of human behavior.From a family systems perspective, individual func-tioning is considered to be reciprocally intercon-nected to that of other individuals within one’s pri-mary relational context—the family. A hallmark ofthe systemic approach is the delineation of the recur-ring patterns and interactional sequences of interac-tion in which problems, such as drug abuse, are em-bedded (e.g., Stanton, Todd, & Associates, 1982). Afamily systems view of adolescent drug abuse focuseson the manner in which adolescent functioning isrelated to parental, sibling, and extended-family func-tioning, as well as to patterns of communication andinteraction within and between various family subsys-tems (e.g., parent–adolescent, parent–parent, par-ent–sibling). Specifically, a family systems orienta-tion considers the manner in which levels ofemotional connection and separation, harmony, andconflict among family members maintain and aremaintained by adolescent drug abuse and relatedproblem behaviors.
From a family systems perspective, clinical inter-vention should orchestrate emotional and cognitivechange within individuals and interactional changesbetween family members. Intervention strategies andtechniques derived from the ‘‘structural–strategic’’family therapy orientation (e.g., Haley, 1976; Mi-nuchin & Fishman, 1981) have been particularlyprominent within family-based therapy for adoles-cent drug abuse. The sine-qua-non of structural–strategic family therapy is the restructuring and reor-ganization of family functioning through in-session‘‘enactment’’ (Minuchin, 1974). Enactments are ther-apist-directed interactions among family membersduring the session. These interventions assess currentfamily processes and relational dynamics and createnew ways of interacting among family members. Forinstance, one type of enactment in family-based ther-apy for adolescent drug abuse might involve the ther-apist directing emotionally disengaged parents andadolescents to talk directly to one another about theirrelationship (Diamond & Liddle, 1999). Anothertype of enactment might entail the therapist assistingoverly permissive parents to take a firm stand againstthe adolescent’s behavior during the session. Tech-niques such as these are widely used in family-basedtherapy for adolescent drug abuse to establish norma-tive shifts in lines of authority, communication, andemotional connection within families of adolescent
Knowns and Unknowns 271
drug abusers. Here, the core hypothesis is that im-provements in family functioning are related to im-provements in functioning of the individual teenager,and make drug taking and other forms of problembehavior less likely (Diamond & Liddle, 1996).
Cognitive–Behavior Theory
In addition to structural–strategic family systemsapproaches, family therapy models that integrate tra-ditional family systems theory with principles andtechniques of individual cognitive–behavioral ther-apy (CBT) have been developed and tested for ado-lescent drug abuse (Azrin, Donohue, Besalel, Ko-gan, & Acierno, 1994; Waldron, Slesnick, Brody,Turner, & Peterson, 2000). Behavioral family-basedtherapy approaches view adolescent drug abuse as aconditioned behavior that is reinforced by cues andcontingencies within the family. For instance, drugabuse by adolescents may be directly modeled andreinforced by other family members. Alternatively,adolescent drug abuse may be tacitly reinforced byparents’ approval of the adolescent’s association withdrug-using peers, or by parental permissiveness to-ward the adolescent’s initial experimentation withdrugs. High levels of family conflict and stress mayalso serve as stimuli for adolescent drug abuse.
Intervention in behavioral family therapy for ad-olescent drug abuse entails the recalibration and themanagement of behavioral/interactional cues withinthe family such that the conditions and behaviorsthat are compatible with drug use are diminished andat the same time, those conditions that are incompati-ble with drug use are reinforced. Techniques includethe modeling and rehearsal of skills in family commu-nication, problem solving, and conflict resolution; im-proving parents’ behavior management and disci-pline practices; and implementing positive rewardsfor adolescents’ non-drug use behavior (e.g., schoolattendance and performance, church youth activ-ities).
Social Ecological and Developmental Theory
Social ecological family-based therapy modelsrepresent a new generation of adolescent drug abusetreatments that expand the boundaries of clinicalintervention beyond the family (Liddle, 1995).Multisystemic therapy (MST; Henggeler, Schoen-wald, Borduin, Rowland, & Cunningham, 1998) and
multidimensional family therapy (MDFT; Liddle,2000; Liddle, Dakof, & Diamond, 1991) are exam-ples of empirically supported treatments in thiscategory. Social ecological family-based therapymodels integrate classic family systems theory andsocial ecology theory (Bronfenbrenner, 1979). Indi-vidual behavior is considered within a nexus ofinterconnected and nested social systems includingthe individual, family, school, peer, neighborhood,community, and culture. A social ecological ap-proach toward adolescent drug abuse treatment isconsistent with basic research that has specified aninterconnected network of risk and protective fac-tors for drug abuse, and this network spans themultiple ecological systems in which teens live(Brook, Nomura, & Cohen, 1989; Hawkins, Cata-lano, & Miller, 1992; Petraitis, Flay, Miller, Torpy, &Greiner, 1998; Resnick et al., 1997). From a socialecological perspective, multiple risk factors are un-derstood to act independently and in combinationto compromise normal adolescent development,thereby giving rise to symptoms of drug abuse,delinquency, and other behavior problems (Baum-rind & Moselle, 1985; Lerner & Galambos, 1998).A developmentally grounded approach to assess-ment and intervention is emphasized in the MST(Henggeler et al., 1998) and MDFT models (Liddle,Rowe, Dakof, & Lyke, 1998; Liddle et al., 2000a).
Given the many factors involved in the creationand maintenance of adolescent drug abuse andassociated functional impairments, developmental/ecological family-based therapies espouse individu-alized, broad-based, comprehensive interventionstrategies (see Kazdin, 1994b; Miller & Prinz, 1990).Ecological family-based therapy depends on de-tailed and ongoing assessment of risk and protectivefactors within individual, familial, and extrafamilialsystems. These models assess functional areas thatare established empirically to be correlates of ado-lescent drug and behavior problems. Interventionsare tailored to work within each adolescent’s andfamily’s unique profile of developmental risk andprotection. The format and methods of clinicalintervention in ecological family-based therapy par-allel the scope and complexity with which adolescentproblem behaviors are understood. For instance,‘‘sessions’’ may occur in the home, school, or otherappropriate setting within the adolescent’s socialcontext rather than in a therapist’s office. Giventhe breadth and magnitude of the problems thatare addressed simultaneously in ecological family-based therapy, sessions are more frequent and inten-

272 Ozechowski and Liddle
sive than a traditional outpatient regimen of weekly1-hour service delivery units. Therapists may meetwith one or more members of the family on a dailybasis during the early stages of treatment and aretypically on-call to respond to crisis situations. Ther-apists spend varying but potentially significantamounts of time in individual and multiperson ses-sions with the adolescent, parents, siblings, extendedfamily, and extrafamilial system members includingschool teachers, probation officers, vocational spe-cialists, ministers, and so on. Members of the adoles-cent’s peer group may be involved in treatment aswell. Two or more therapists or a primary clinicianand therapist assistant may choreograph the servicesfor each case. The underlying clinical hypothesiswithin ecological family-based therapy is that ado-lescent drug abuse and problem behaviors will desistwhen therapists work closely with the adolescent,his or her family, and significant members of otherecological systems to construct and implement per-sonally meaningful, practical, and developmentallyfacilitative lifestyle changes.
Summary
Family-based treatments for adolescent drugabuse have evolved considerably since the early1980s. Earlier versions of these interventions, re-flecting their historical periods, focused on integ-rative combinations of structural and strategic familytherapies (Liddle, 1981; Henggeler, 1993) and fo-cused primarily on the family as the unit of interven-tion. These models changed over the years (Liddle,1995), and in Henggeler’s terms, interventions moved‘‘beyond family therapy’’ (Henggeler & Borduin,1990). The recent expansions of social ecological fam-ily-based therapy have broadened the boundaries ofadolescent drug abuse treatment well beyond thefamily. The expanded scope of family-based therapyis neither accidental nor random. These changes areclinically, theory, and research based. They are inaccord with recommendations that have been madefor some time (e.g., Kazdin, 1987). Also, these devel-opments relate to the increasing volume, relevance,and accessibility of research-based knowledge aboutthe development and continuation of adolescent drugabuse. Efforts to translate basic research on the etiol-ogy and progression of adolescent drug abuse intoclinical interventions have played a vital role in the
evolution of family-based drug therapy for adoles-cents (Dishion, Reid, & Patterson, 1988).
KNOWNS AND UNKNOWNS REGARDINGFAMILY-BASED THERAPY FORADOLESCENT DRUG ABUSE
The first generation of controlled outcome trialsand studies testing engagement strategies in familytherapy for adolescent substance abuse were con-ducted during the 1980s (Friedman, 1989; Joanning,Quinn, Thomas, & Mullen, 1992; Lewis, Piercy,Sprenkle, & Trepper, 1990; Liddle & Dakof, 1995a;Szapocznik, Kurtines, Foote, Perez-Vidal, & Hervis,1983, 1986; Szapocznik et al., 1988). Although stan-dards for what constitutes rigorous clinical researchhave evolved considerably since this earlier histori-cal period (see Docherty, 1984; Carroll & Rounsa-ville, 1990; Kazdin, 1994a), this first wave of studiesexemplified cutting-edge clinical research accordingto available standards at the time. Distinguishingfeatures of these studies include well-defined treat-ment and comparison conditions, the availability ofdocumented clinical procedures (treatment manualsin some cases), ongoing clinical supervision of thera-pists implementing the treatments, and standardizedassessments of drug use and other clinical outcomesat multiple time points. Some of these early studieswere implemented in community-based clinics—‘‘real world’’ settings that were worked with in away so that quality scientific research could beconducted. Research during this period establishedfamily-based therapy as a safe, acceptable, viable,and promising treatment for adolescent drugproblems.
Although it still lags behind adult treatmentaccording to virtually any metric (i.e., amount ofresearch dollars, number of studies, number oftrained investigators, focus of research training pro-grams to train investigators), the scientific qualityof family-based adolescent drug treatment researchcontinues to progress with considerable and broad-based federally funded research support (Weinberget al., 1998). A major advancement has been theextent to which the tested treatments can now bespecified. Treatment manuals specify theory-basedand principle-driven procedures of family and multi-ple systems–oriented interventions at high levels ofdetail (Henggeler et al., 1994; Liddle, 2000). Manualsfacilitate the dissemination and replication of family-

Knowns and Unknowns 273
based therapies in various adolescent treatmentand research settings [e.g., CSAT Cannabis YouthTreatment (CYT) Multisite Study4 (www.samhsa.gov/csat; or www.chestnut.org), see also Schoen-wald & Henggeler, in press). Other advances inthis specialty, each of which is essential to progressin any treatment research area, are assessment (Lec-cese & Waldron, 1994; Liddle & Rowe, 1998; McMa-hon & Metzler, 1998) and methodologies for evalu-ating therapist adherence to treatment protocols(Henggeler, Melton, Brondino, Scherer, & Hanley,1997; Hogue et al., 1998). Moreover, studying thera-pist adherence and performance has created newavenues for process research (e.g., Hogue, Liddle, &Rowe, 1996). Drawing on an events-based or task-analytic methodologic approach (Greenberg, Heath-erington, & Friedlander, 1996), family-based treat-ment researchers during the 1990s began observing
4The Cannabis Youth Treatment Study (CYT) was designed toadapt five promising adolescent treatments for use in clinicalpractice and then to field test their effectiveness in the largestrandomized experiment ever conducted with adolescent mari-juana users seeking outpatient treatment. Preliminary resultssuggest that all five treatments are more effective than currentpractice. Findings from the project are being posted atwww.chestnut.org/li/CYT and copies of the five treatment manu-als will be available this fall from CSAT at www.samhsa.gov/CSAT. Five promising manual-guided treatments were devel-oped by the CYT collaborating team for field testing to representreal programmatic and policy treatment options. They are:
1. Motivational Enhancement Therapy/Cognitive–BehavioralTherapy (MET/CBT5)—This is a five-session treatmentwith two individual sessions.
2. Cognitive Behavior Therapy 7 (CBT7)—This treatmentwas designed to follow MET/CBT5 and provides additionalgroup sessions.
3. The Family Support Network (FSN)—This treatment isdesigned to supplement MET/CBT or other types of treat-ment with additional support for families (home visits, par-ent education meetings) and case management.
4. The Adolescent Community Reinforcement Approach(ACRA)—This approach is composed of 14 individual ses-sions with the adolescent and/or the adolescent’s ‘‘con-cerned other.’’
5. Multidimensional Family Therapy (MDFT)—This is a 12-week, 15-session (individual, family, and multiple systemssessions) treatment that integrates substance abuse andfamily-focused and multisystems interventions.
The CYT project recruited 600 adolescent participants (as wellas their families) who were between the ages of 12-18, reportedusing marijuana in the previous 90 days, reported problemsrelated to marijuana abuse or dependence, and met placementcriteria for outpatient (vs. inpatient) substance-abuse treat-ment.
systematically how subtleties in therapist behaviorinfluence client responsiveness to manualized inter-ventions (Diamond & Liddle, 1999; Robbins, Alex-ander, Newell, & Turner, 1996). Process-outcomeresearch has begun to establish an empirical knowl-edge base about the ingredients and mechanismsof effective treatment. Thus, many factors, includingthe incorporation of more sophisticated treatmentmanuals, drug use assessment methods, treatmentoutcome and therapist adherence, data analytic ad-vances, methodological and procedural improve-ments in other areas such as clinician selectionand training, and the specification of inclusion andexclusion criteria for clinical cases enhance thequality of contemporary studies in this specialty.
Clearly, the same spirit of vitality that charac-terized the first wave of programmatic family-basedtreatment research with adolescent drug abusersis alive and well within today’s clinical researchprograms. Moreover, a new kind of synergy existsbetween the domains of research and clinical prac-tice in family-based therapy, and this bodes wellfor continued empirically rooted treatment develop-ment (see Henggeler, Schoenwald, & Pickrel, 1995;Liddle, 1999). Hoping to facilitate more progressof this kind, the remainder of this paper reviewsexisting outcome and process research on family-based therapy for adolescent drug abuse. We pres-ent the findings through a treatment developmentlens (see Kazdin, 1997; Kazdin & Kendall, 1998),and specify ‘‘knowns and unknowns’’ regarding (i)the effects of family-based therapy on adolescentdrug abuse and associated behavioral problems, (ii)the putative mediators and mechanisms of theseeffects, and (iii) moderators of and boundariesconditions on the effectiveness of family-based ther-apy for adolescent drug abuse. Finally, we highlightareas of treatment development in which significantresearch needs and opportunities exist.
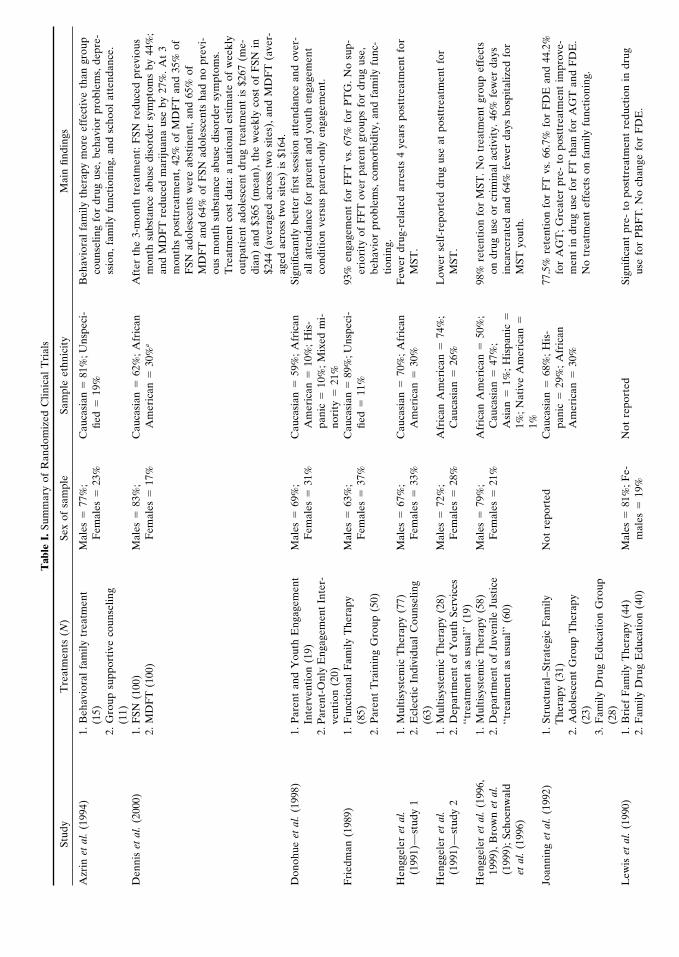
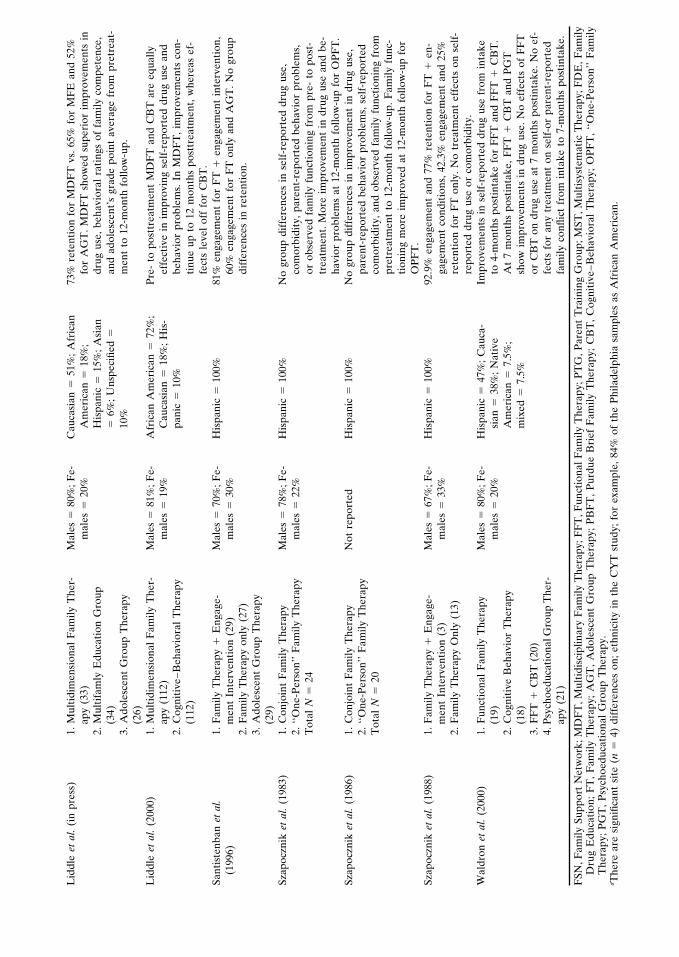
The reviewed studies include 16 clinical trialsand 4 process studies. Key features and findingsfrom the clinical trials are summarized in Table I,whereas Table II summarizes the process studies.The tables distinguish between the terms study andpaper. Study refers to the conduct of a specificempirical investigation, whereas paper refers to anymanuscript reporting on the findings of a study.Multiple papers that report on the same study arecombined within the same row in each of our tables.Likewise, separate studies that are reported withinthe same paper are described in different rowswithin our tables.
Tab
leI.
Sum
mar
yof
Ran
dom
ized
Clin
ical
Tri
als
Stud
yT
reat
men
ts(N
)Se
xof
sam
ple
Sam
ple
ethn
icit
yM
ain
findi
ngs
Azr
inet
al.
(199
4)1.
Beh
avio
ral
fam
ilytr
eatm
ent
Mal
es�
77%
;C
auca
sian
�81
%;U
nspe
ci-
Beh
avio
ral
fam
ilyth
erap
ym
ore
effe
ctiv
eth
angr
oup
(15)
Fem
ales
�23
%fie
d�
19%
coun
selin
gfo
rdr
ugus
e,be
havi
orpr
oble
ms,
depr
e-2.
Gro
upsu
ppor
tive
coun
selin
gss
ion,
fam
ilyfu
ncti
onin
g,an
dsc
hool
atte
ndan
ce.
(11)
Den
nis
etal
.(2
000)
1.F
SN(1
00)
Mal
es�
83%
;C
auca
sian
�62
%;
Afr
ican
Aft
erth
e3-
mon
thtr
eatm
ent:
FSN
redu
ced
prev
ious
2.M
DF
T(1
00)
Fem
ales
�17
%A
mer
ican
�30
%a
mon
thsu
bsta
nce
abus
edi
sord
ersy
mpt
oms
by44
%;
and
MD
FT
redu
ced
mar
ijuan
aus
eby
27%
.A
t3
mon
ths
post
trea
tmen
t,42
%of
MD
FT
and
35%
ofF
SNad
oles
cent
sw
ere
abst
inen
t,an
d65
%of
MD
FT
and
64%
ofF
SNad
oles
cent
sha
dno
prev
i-ou
sm
onth
subs
tanc
eab
use
diso
rder
sym
ptom
s.T
reat
men
tco
stda
ta:
ana
tion
ales
tim
ate
ofw
eekl
you
tpat
ient
adol
esce
ntdr
ugtr
eatm
ent
is$2
67(m
e-di
an)
and
$365
(mea
n),
the
wee
kly
cost
ofF
SNin
$244
(ave
rage
dac
ross
two
site
s),
and
MD
FT
(ave
r-ag
edac
ross
two
site
s)is
$164
.D
onoh
ueet
al.
(199
8)1.
Par
ent
and
You
thE
ngag
emen
tM
ales
�69
%;
Cau
casi
an�
59%
;A
fric
anSi
gnifi
cant
lybe
tter
first
sess
ion
atte
ndan
cean
dov
er-
Inte
rven
tion
(19)
Fem
ales
�31
%A
mer
ican
�10
%;
His
-al
lat
tend
ance
for
pare
ntan
dyo
uth
enga
gem
ent
2.P
aren
t-O
nly
Eng
agem
entI
nter
-pa
nic
�10
%;
Mix
edm
i-co
ndit
ion
vers
uspa
rent
-onl
yen
gage
men
t.ve
ntio
n(2
0)no
rity
�21
%F
ried
man
(198
9)1.
Fun
ctio
nal
Fam
ilyT
hera
pyM
ales
�63
%;
Cau
casi
an�
89%
;Uns
peci
-93
%en
gage
men
tfo
rF
FT
vs.
67%
for
PT
G.
No
sup-
(85)
Fem
ales
�37
%fie
d�
11%
erio
rity
ofF
FT
over
pare
ntgr
oups
for
drug
use,
2.P
aren
tT
rain
ing
Gro
up(5
0)be
havi
orpr
oble
ms,
com
orbi
dity
,an
dfa
mily
func
-ti
onin
g.H
engg
eler
etal
.1.
Mul
tisy
stem
icT
hera
py(7
7)M
ales
�67
%;
Cau
casi
an�
70%
;A
fric
anF
ewer
drug
-rel
ated
arre
sts
4ye
ars
post
trea
tmen
tfo
r(1
991)
—st
udy
12.
Ecl
ecti
cIn
divi
dual
Cou
nsel
ing
Fem
ales
�33
%A
mer
ican
�30
%M
ST.
(63)
Hen
ggel
eret
al.
1.M
ulti
syst
emic
The
rapy
(28)
Mal
es�
72%
;A
fric
anA
mer
ican
�74
%;
Low
erse
lf-r
epor
ted
drug
use
atpo
sttr
eatm
ent
for
(199
1)—
stud
y2
2.D
epar
tmen
tof
You
thSe
rvic
esF
emal
es�
28%
Cau
casi
an�
26%
MST
.‘‘t
reat
men
tas
usua
l’’(1
9)H
engg
eler
etal
.(1
996,
1.M
ulti
syst
emic
The
rapy
(58)
Mal
es�
79%
;A
fric
anA
mer
ican
�50
%;
98%
rete
ntio
nfo
rM
ST.
No
trea
tmen
tgr
oup
effe
cts
1999
),B
row
net
al.
2.D
epar
tmen
tof
Juve
nile
Just
ice
Fem
ales
�21
%C
auca
sian
�47
%;
ondr
ugus
eor
crim
inal
acti
vity
.46
%fe
wer
days
(199
9);
Scho
enw
ald
‘‘tre
atm
ent
asus
ual’’
(60)
Asi
an�
1%;
His
pani
c�
inca
rcer
ated
and
64%
few
erda
ysho
spit
aliz
edfo
ret
al.
(199
6)1%
;N
ativ
eA
mer
ican
�M
STyo
uth.
1%Jo
anni
nget
al.
(199
2)1.
Stru
ctur
al–S
trat
egic
Fam
ilyN
otre
port
edC
auca
sian
�68
%;
His
-77
.5%
rete
ntio
nfo
rF
Tvs
.66
.7%
for
FD
Ean
d44
.2%
The
rapy
(31)
pani
c�
29%
;A
fric
anfo
rA
GT
;G
reat
erpr
e-to
post
trea
tmen
tim
prov
e-2.
Ado
lesc
ent
Gro
upT
hera
pyA
mer
ican
�30
%m
ent
indr
ugus
efo
rF
Tth
anfo
rA
GT
and
FD
E.
(23)
No
trea
tmen
tef
fect
son
fam
ilyfu
ncti
onin
g.3.
Fam
ilyD
rug
Edu
cati
onG
roup
(28)
Lew
iset
al.
(199
0)1.
Bri
efF
amily
The
rapy
(44)
Mal
es�
81%
;Fe-
Not
repo
rted
Sign
ifica
ntpr
e-to
post
trea
tmen
tre
duct
ion
indr
ug2.
Fam
ilyD
rug
Edu
cati
on(4
0)m
ales
�19
%us
efo
rP
BF
T.
No
chan
gefo
rF
DE
.
Lid
dle
etal
.(i
npr
ess)
1.M
ulti
dim
ensi
onal
Fam
ilyT
her-
Mal
es�
80%
;Fe-
Cau
casi
an�
51%
;A
fric
an73
%re
tent
ion
for
MD
FT
vs.
65%
for
MF
Ean
d52
%ap
y(3
3)m
ales
�20
%A
mer
ican
�18
%;
for
AG
T.
MD
FT
show
edsu
peri
orim
prov
emen
tsin
2.M
ulti
fam
lyE
duca
tion
Gro
upH
ispa
nic
�15
%;
Asi
andr
ugus
e,be
havi
oral
rati
ngs
offa
mily
com
pete
nce,
(34)
�6%
;U
nspe
cifie
d�
and
adol
esce
nt’s
grad
epo
int
aver
age
from
pret
reat
-3.
Ado
lesc
ent
Gro
upT
hera
py10
%m
ent
to12
-mon
thfo
llow
-up.
(26)
Lid
dle
etal
.(2
000)
1.M
ulti
dim
ensi
onal
Fam
ilyT
her-
Mal
es�
81%
;Fe-
Afr
ican
Am
eric
an�
72%
;P
re-
topo
sttr
eatm
ent
MD
FT
and
CB
Tar
eeq
ually
apy
(112
)m
ales
�19
%C
auca
sian
�18
%;
His
-ef
fect
ive
inim
prov
ing
self
-rep
orte
ddr
ugus
ean
d2.
Cog
niti
ve–B
ehav
iora
lT
hera
pypa
nic
�10
%be
havi
orpr
oble
ms.
InM
DF
T,
impr
ovem
ents
con-
(112
)ti
nue
upto
12m
onth
spo
sttr
eatm
ent,
whe
reas
ef-
fect
sle
vel
off
for
CB
T.
Sant
iste
nban
etal
.1.
Fam
ilyT
hera
py�
Eng
age-
Mal
es�
70%
;Fe-
His
pani
c�
100%
81%
enga
gem
ent
for
FT
�en
gage
men
tin
terv
enti
on,
(199
6)m
ent
Inte
rven
tion
(29)
mal
es�
30%
60%
enga
gem
ent
for
FT
only
and
AG
T.
No
grou
p2.
Fam
ilyT
hera
pyon
ly(2
7)di
ffer
ence
sin
rete
ntio
n.3.
Ado
lesc
ent
Gro
upT
hera
py(2
9)Sz
apoc
znik
etal
.(1
983)
1.C
onjo
int
Fam
ilyT
hera
pyM
ales
�78
%;F
e-H
ispa
nic
�10
0%N
ogr
oup
diff
eren
ces
inse
lf-r
epor
ted
drug
use,
2.‘‘O
ne-P
erso
n’’
Fam
ilyT
hera
pym
ales
�22
%co
mor
bidi
ty,
pare
nt-r
epor
ted
beha
vior
prob
lem
s,T
otal
N�
24or
obse
rved
fam
ilyfu
ncti
onin
gfr
ompr
e-to
post
-tr
eatm
ent.
Mor
eim
prov
emen
tin
drug
use
and
be-
havi
orpr
oble
ms
at12
-mon
thfo
llow
-up
for
OP
FT
.Sz
apoc
znik
etal
.(1
986)
1.C
onjo
int
Fam
ilyT
hera
pyN
otre
port
edH
ispa
nic
�10
0%N
ogr
oup
diff
eren
ces
inim
prov
emen
tin
drug
use,
2.‘‘O
ne-P
erso
n’’
Fam
ilyT
hera
pypa
rent
-rep
orte
dbe
havi
orpr
oble
ms,
self
-rep
orte
dT
otal
N�
20co
mor
bidi
ty,
and
obse
rved
fam
ilyfu
ncti
onin
gfr
ompr
etre
atm
ent
to12
-mon
thfo
llow
-up.
Fam
ilyfu
nc-
tion
ing
mor
eim
prov
edat
12-m
onth
follo
w-u
pfo
rO
PF
T.
Szap
oczn
iket
al.
(198
8)1.
Fam
ilyT
hera
py�
Eng
age-
Mal
es�
67%
;Fe-
His
pani
c�
100%
92.9
%en
gage
men
tan
d77
%re
tent
ion
for
FT
�en
-m
ent
Inte
rven
tion
(3)
mal
es�
33%
gage
men
tco
ndit
ions
,42
.3%
enga
gem
ent
and
25%
2.F
amily
The
rapy
Onl
y(1
3)re
tent
ion
for
FT
only
.N
otr
eatm
ent
effe
cts
onse
lf-
repo
rted
drug
use
orco
mor
bidi
ty.
Wal
dron
etal
.(2
000)
1.F
unct
iona
lF
amily
The
rapy
Mal
es�
80%
;Fe-
His
pani
c�
47%
;C
auca
-Im
prov
emen
tsin
self
-rep
orte
ddr
ugus
efr
omin
take
(19)
mal
es�
20%
sian
�38
%;
Nat
ive
to4-
mon
ths
post
inta
kefo
rF
FT
and
FF
T�
CB
T.
2.C
ogni
tive
Beh
avio
rT
hera
pyA
mer
ican
�7.
5%;
At
7m
onth
spo
stin
take
,F
FT
�C
BT
and
PG
T(1
8)m
ixed
�7.
5%sh
owim
prov
emen
tsin
drug
use.
No
effe
cts
ofF
FT
3.F
FT
�C
BT
(20)
orC
BT
ondr
ugus
eat
7m
onth
spo
stin
take
.N
oef
-4.
Psy
choe
duca
tion
alG
roup
The
r-fe
cts
for
any
trea
tmen
ton
self
-or
pare
nt-r
epor
ted
apy
(21)
fam
ilyco
nflic
tfr
omin
take
to7-
mon
ths
post
inta
ke.
FSN
,Fam
ilySu
ppor
tN
etw
ork;
MD
FT
,Mul
tidi
scip
linar
yF
amily
The
rapy
;FF
T,F
unct
iona
lF
amily
The
rapy
;PT
G,P
aren
tT
rain
ing
Gro
up;M
ST,M
ulti
syst
emat
icT
hera
py;F
DE
,Fam
ilyD
rug
Edu
cati
on;
FT
,F
amily
The
rapy
;A
GT
,A
dole
scen
tG
roup
The
rapy
;P
BF
T,
Pur
due
Bri
efF
amily
The
rapy
;C
BT
,C
ogni
tive
–Beh
avio
ral
The
rapy
;O
PF
T,
‘‘One
-Per
son’
’F
amily
The
rapy
;P
GT
,P
sych
oedu
cati
onal
Gro
upT
hera
py.
a The
rear
esi
gnifi
cant
site
(n�
4)di
ffer
ence
son
;et
hnic
ity
inth
eC
YT
stud
y;fo
rex
ampl
e,84
%of
the
Phi
lade
lphi
asa
mpl
esas
Afr
ican
Am
eric
an.
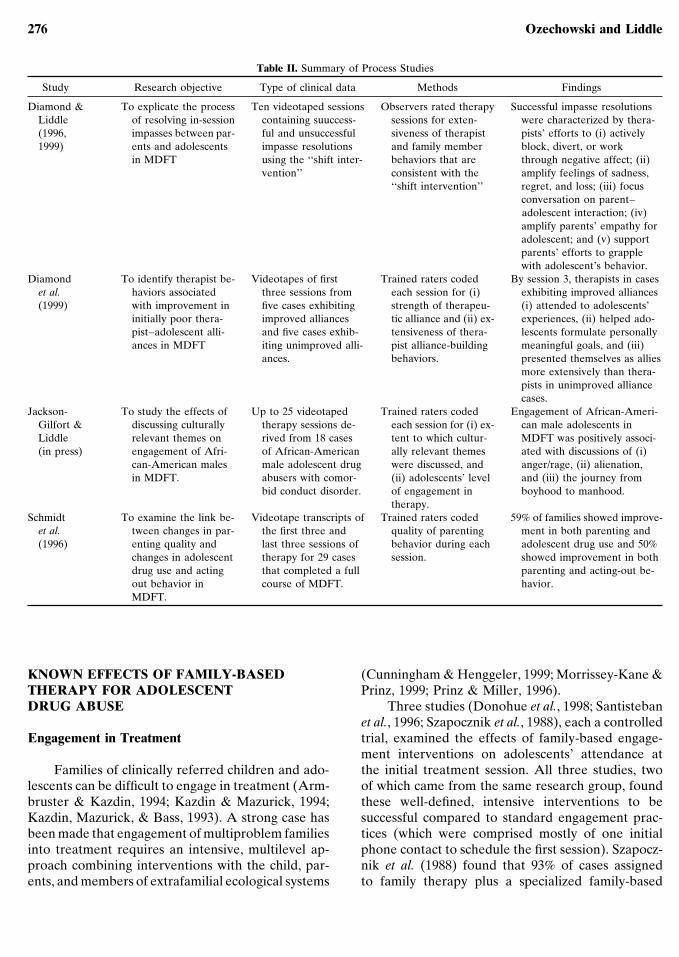
276 Ozechowski and Liddle
Table II. Summary of Process Studies
Study Research objective Type of clinical data Methods Findings
Diamond & To explicate the process Ten videotaped sessions Observers rated therapy Successful impasse resolutionsLiddle of resolving in-session containing suuccess- sessions for exten- were characterized by thera-(1996, impasses between par- ful and unsuccessful siveness of therapist pists’ efforts to (i) actively1999) ents and adolescents impasse resolutions and family member block, divert, or work
in MDFT using the ‘‘shift inter- behaviors that are through negative affect; (ii)vention’’ consistent with the amplify feelings of sadness,
‘‘shift intervention’’ regret, and loss; (iii) focusconversation on parent–adolescent interaction; (iv)amplify parents’ empathy foradolescent; and (v) supportparents’ efforts to grapplewith adolescent’s behavior.
Diamond To identify therapist be- Videotapes of first Trained raters coded By session 3, therapists in caseset al. haviors associated three sessions from each session for (i) exhibiting improved alliances(1999) with improvement in five cases exhibiting strength of therapeu- (i) attended to adolescents’
initially poor thera- improved alliances tic alliance and (ii) ex- experiences, (ii) helped ado-pist–adolescent alli- and five cases exhib- tensiveness of thera- lescents formulate personallyances in MDFT iting unimproved alli- pist alliance-building meaningful goals, and (iii)
ances. behaviors. presented themselves as alliesmore extensively than thera-pists in unimproved alliancecases.
Jackson- To study the effects of Up to 25 videotaped Trained raters coded Engagement of African-Ameri-Gilfort & discussing culturally therapy sessions de- each session for (i) ex- can male adolescents inLiddle relevant themes on rived from 18 cases tent to which cultur- MDFT was positively associ-(in press) engagement of Afri- of African-American ally relevant themes ated with discussions of (i)
can-American males male adolescent drug were discussed, and anger/rage, (ii) alienation,in MDFT. abusers with comor- (ii) adolescents’ level and (iii) the journey from
bid conduct disorder. of engagement in boyhood to manhood.therapy.
Schmidt To examine the link be- Videotape transcripts of Trained raters coded 59% of families showed improve-et al. tween changes in par- the first three and quality of parenting ment in both parenting and(1996) enting quality and last three sessions of behavior during each adolescent drug use and 50%
changes in adolescent therapy for 29 cases session. showed improvement in bothdrug use and acting that completed a full parenting and acting-out be-out behavior in course of MDFT. havior.MDFT.
KNOWN EFFECTS OF FAMILY-BASEDTHERAPY FOR ADOLESCENTDRUG ABUSE
Engagement in Treatment
Families of clinically referred children and ado-lescents can be difficult to engage in treatment (Arm-bruster & Kazdin, 1994; Kazdin & Mazurick, 1994;Kazdin, Mazurick, & Bass, 1993). A strong case hasbeen made that engagement of multiproblem familiesinto treatment requires an intensive, multilevel ap-proach combining interventions with the child, par-ents, and members of extrafamilial ecological systems
(Cunningham & Henggeler, 1999; Morrissey-Kane &Prinz, 1999; Prinz & Miller, 1996).
Three studies (Donohue et al., 1998; Santistebanet al., 1996; Szapocznik et al., 1988), each a controlledtrial, examined the effects of family-based engage-ment interventions on adolescents’ attendance atthe initial treatment session. All three studies, twoof which came from the same research group, foundthese well-defined, intensive interventions to besuccessful compared to standard engagement prac-tices (which were comprised mostly of one initialphone contact to schedule the first session). Szapocz-nik et al. (1988) found that 93% of cases assignedto family therapy plus a specialized family-based

Knowns and Unknowns 277
engagement intervention were successfully engagedin treatment, compared to a 42% engagement ratefor the family-based therapy without specializedengagement condition. In a replication study by thesame group, Santisteban et al. (1996) found thatfamily therapy plus a specialized engagement inter-vention resulted in an 81% rate of engagement intotreatment compared to a rate of 57% for family-based therapy only, and 62% for adolescent grouptherapy. Donohue et al. (1998) found that 89% ofcases receiving family-based engagement attendedthe first session, compared to 60% of cases receivingstandard parent-only engagement procedures. Over-all session attendance was also higher for the family-based treatment (83% vs. 57%).
Retention in Treatment
Treatment retention rates were reported in 12clinical trials. Retention rates for family treatmentswere high—typically between 70% and 90%. Heng-geler, Pickrel, Brondino, and Crouch (1996) re-ported that 57 out of 58 cases (98%) assigned toMST completed a full course of treatment lastingan average of 130 days. Waldron et al. (2000)reported that 56 out of 59 cases (95%) receivingeither FFT only or a combination of FFT pluscognitive–behavior therapy (CBT) were retained intreatment. Retention in certain intensive forms offamily-based therapy is dramatically higher than‘‘treatment as usual’’ (TAU) provided within thejuvenile justice system (Henggeler et al., 1991, 1996).Retention rate differences are less pronounced be-tween family-based therapies and other well-definedindividual and group therapies with specialized en-gagement strategies of their own (Azrin et al., 1994;Henggeler et al., 1991; Joanning et al., 1992; Liddleet al., in press). Several studies found no differencesin retention between family-based and alternativestate of the science, manualized treatments (Liddle,Turner, Tejeda, & Dakof, 2000; Santisteban et al.,1996; Waldron et al., 2000). Overall, these studiesindicate that most drug-abusing teens can be re-tained in treatments using assertive and labor-intensive recruitment of clients and their families.Furthermore, in several studies retention in family-based therapy is higher than in other well-estab-lished adolescent drug treatments (see Stanton &Shadish, 1997).
Drug Use
Thirteen clinical trials reported treatment effectson levels of adolescent drug use. All 13 studies mea-sured drug use by means of adolescent self-report.Six studies combined adolescent reports of drug usewith either parent reports or urinalysis, or in onecase, both. Nine of the 13 studies in this categoryincluded assessments of adolescents’ use of specificdrugs including alcohol, marijuana, cocaine, andother illicit drugs. However, no study in this reviewreported on treatment effects for specific substancesother than marijuana. Five studies distinguished be-tween ‘‘soft’’ (alcohol and marijuana) versus ‘‘hard’’(cocaine and other illicit substances) drug use, andthe other eight studies in this category define druguse as a summary or aggregate index of the use ofany illegal or illicit substance.
Consistent with previous reviews, strong and con-sistent empirical support exists for the efficacy of fam-ily-based therapy in reducing levels of adolescent druguse (Liddle & Dakof, 1995a,b; Stanton & Shadish,1997;Waldron, 1997)Significantpre- toposttreatmenteffects for family-basedtherapy wereobtained inall13clinical trials examining drug use outcomes betweenfamily-based and alternative conditions. Certain fam-ily-based therapies are efficacious in reducing alcoholand marijuana use as well the use of hard drugs includ-ing cocaine, heroin, and other narcotics (Azrin et al.,1994; Friedman, 1989; Henggeler, Pickrel, & Bron-dino, 1999; Lewis et al., 1990; Liddle et al., in press). Inseven studies family-based therapy was found to havesuperior pre- to posttreatment effects on levels of ado-lescent drug use compared to alternative treatmentsincluding individual therapy (Azrin et al., 1994; Heng-geler et al., 1991; Liddle et al., in press; Waldron et al.,2000), adolescent group therapy (Joanning, et al.,1992; Liddle et al., in press), and family psychoeduca-tional drug counseling (Joanning et al., 1992; Lewis etal., 1990; Liddle et al., in press). Family-based thera-pies were found to be equally effective compared to aparent-training group intervention (Friedman, 1989)and ‘‘one-person’’ family therapy intervention (Sza-pocznik et al., 1983, 1986).
There is evidence that the effects of family-basedtherapy on adolescent drug use endure beyond treat-ment termination. Drug use outcomes in family-ori-ented treatment were maintained 6 to 12 months aftertermination in six out seven studies in which posttreat-ment drug use outcomes were assessed. For example,Liddle et al. (in press) report sustained reductions indrug use at 6- and 12-months posttreatment among ad-

278 Ozechowski and Liddle
olescents in MDFT. These posttreatment effects weresuperior to those obtained for adolescent group ther-apy and a multifamily educational intervention. Simi-larly, Liddle et al. (in press) found that adolescent-re-ported drug involvement (marijuana and harder drugssuchascocaine)continuedtodecline6-and12-monthsposttreatment among adolescents in MDFT, whereasdecreases in drug involvement leveled off among ado-lescents in the comparison CBT treatment, a state ofthe science, manualized individual adolescent inter-vention. MDFT was also tested in the CYT study(Dennis et al., under review). In that study, MDFT re-duced days of marijuana use by 27%.
There was another treatment tested in CYT thathad a strong family intervention component. TheFamily Support Network (FSN; Hamilton, Brantley,Tims, Angelovich, & McDougall, 2000) was not devel-oped as a stand-alone treatment for adolescent drugabuse, but was designed and tested as a supplement tothe individually oriented Motivational EnhancementTherapy (MET)/Cognitive Behavior Therapy (CBT)(Sampl & Kadden, 2000; Webb, Scudder, Kaminer, &Kadden, 2000) that was also developed for the CYTexperiment. FSN was composed of 12 MET and CBTsessions with the adolescent (2 individual, 10 groupsessions) and 8 family sessions (multifamily group andindividual family sessions, and weekly case manage-ment services.5 After the 3 months of treatment, FSNreduced previous-month symptoms related to sub-stance abuse by 44%, and it worked more effectivelythan the comparison conditions with higher drug useseverity adolescents. At 3 months posttreatment, theabstinence rates for MDFT were42% and 35% for FSN
5There was another treatment in the CYT experiment that includedfamily interventions. The Adolescent Community ReinforcementApproach (Godley et al., 2000) is composed of 14 individual ses-sions with the adolescent and/or the adolescent’s ‘‘concernedother’’ (10 individual sessions with adolescent, 2 with the signifi-cant other/parent(s) alone, and 2 whole-family sessions). Basedon NIAAA-funded treatment research manuals, the focus is onlearning alternative skills to cope with problems and changingthe environmental contingencies related to continued substanceuse. Because of the relative proportion of individual to familywork in the ACRA model, the ACRA approach was not consid-ered a ‘‘family-based’’ treatment according to the definitions de-veloped for this review. At the same time, it should be notedthat the ACRA model, developed specifically for the CYT study,demonstrated effectiveness in having an impact on adolescentdrug abuse (Dennis et al., under review). The ACRA treatmentreduced days of use by 31% after its 3-month course of therapy.At 3 months posttreatment, 66% of the teens had no substance-abuse disorder symptoms for the previous month; also at the3-month posttest time point, 35% of ACRA adolescents wereabstinent from marijuana use.
adolescents, and at the 3-month postperiod, 65% ofMDFT and 64% of FSN adolescents had no previousmonth substance abuse disorder symptoms. Otherstudies have found sustained effects for family inter-ventions. Szapocznik et al. (1983, 1986) found sus-tained effects for structural–strategic family therapy6- and 12-months posttreatment, and Friedman (1989)found continued drug use effects for FFT 9 monthsposttreatment. Long-term treatment effects were re-ported by Henggeler et al. (1991), who found that ado-lescents in MST reported fewer drug-related arrests 4years posttreatment compared to adolescents in thetreatment-as-usual condition.
Overall, empirical evidence supports the efficacyof family-based therapy for reducing levels of adoles-cent drug abuse. Moreover, some evidence exists tosuggest that drug use reductions may be more pro-nounced in family-based therapy than in alternativenon-family-based treatments, and that these effectscan endure at least 6–12 months beyond the termina-tion of treatment.
Behavioral Problems Associated with Drug Use
Adolescent drug abuse tends to occur along withone or more other problem behaviors or symptomssuch as delinquency, aggressiveness, and antisocialbehavior (Patterson, Reid, & Dishion, 1992; Tildes-ley, Hops, Ary, & Andrews, 1995). Given the interre-latedness of drug and behavior problems, family- andmultiple systems–oriented adolescent drug abusetherapies have been designed not only to target ado-lescent drug use and abuse, but also to focus on thesecoexisting problem behaviors and to promote proso-cial behaviors (e.g., Henggeler et al., 1999; Lewis,Piercy, Sprenkle, & Trepper, 1989; Liddle, 1995).
Ten studies examined family treatment’s impacton behavioral problems associated with adolescentdrug abuse. Behavior problems were measured byparent reports on comprehensive behavior problemchecklists and inventories in eight of these studies.Three studies used both parent and adolescent re-ports of problem behavior. An adolescent-report de-linquency scale was used in conjunction with policearrest records in one study. Across these 10 studies,the term behavior problems generally refers to a col-lective or aggregate index of the number and severityof a wide range of behavioral symptoms. Specificmeasures of behavioral symptoms were obtained byDennis et al. (under review), who used the GlobalAppraisal of Individual Needs (GAIN; Dennis,

Knowns and Unknowns 279
1999), Liddle, Dakof, Turner, and Tejeda (2000) whoassessed externalizing and internalizing behaviorproblems separately, and Henggeler et al. (1999), whocollected adolescent reports and police records ofillegal activity.
Family-based therapy was found to be effectivein reducing problem behavior associated with adoles-cent drug abuse in each of the 10 clinical trials in thiscategory. The effects of family-based therapies werefound to be equivalent to those of alternative treat-ments in reducing problem behavior from pretreat-ment up to 6–12 months posttreatment in half ofthese studies (Freidman, 1989; Liddle et al., in press;Szapocznik et al., 1983, 1986, 1988). Three studiesprovide evidence that behavioral problems otherthan drug use may decrease more in family-basedtherapy than in alternative treatments. Azrin et al.(1994) found that the mean pre- to posttreatmentchange scores in parent-reported behavior problemswas higher in behavioral family therapy (BFT) thanin supportive group counseling. In addition, Heng-geler et al. (1999) found that during the period frompretreatment to 6 months posttreatment, adolescentsin MST had 46% fewer incarceration days and 50%fewer days in restrictive out-of-home placementsthan youth in the treatment as usual condition. Fi-nally, Liddle et al. (2000) found that parent reportsof externalizing behavior problems and adolescentreports of internalizing behavior problems improvedsignificantly from pretreatment to 12 months post-treatment among adolescents in MDFT, whereas im-provements on these variables leveled of from treat-ment termination to 12 months posttreatment amongadolescents in an individual adolescent CBT treat-ment. Overall, these studies provide support for theefficacy of family-based therapy in reducing problembehavior associated with adolescent drug abuse.Moreover, there is preliminary evidence that family-based therapy may be more effective than other typesof treatments in ameliorating problem behavior.
Psychiatric Comorbidity
Adolescent drug abuse is commonly accompa-nied by symptoms of psychiatric disorders suchas conduct disorder, attention-deficit hyperactivitydisorder, anxiety disorder, and depression (Brook,Cohen, & Brook, 1998; Greenbaum, Foster-John-son, & Petrila, 1996; Kandel et al., 1997; Weinberg &Glantz, 1999). Interventions in contemporary treat-ments try to decrease comorbid psychiatric symp-
toms as well as drug-using behaviors (AACAP,1997). Eight clinical trials included an assessmentof psychiatric symptoms in addition to substanceabuse or dependence. In all eight studies, symptomsof psychiatric comorbidity were measured on anadolescent self-report questionnaire. In two of theseeight studies, pretreatment psychiatric diagnoseswere made according to DSM-III-R or DSM-IVcriteria using standardized procedures. However,neither of these two studies examined posttreatmentchanges in diagnostic status. Six studies examinedpre- to posttreatment changes in psychiatric symp-tomatology, but none of these studies used a proce-dure to assign a psychiatric diagnosis. In four ofthese studies, psychiatric comorbidity was indexedby a summary or aggregate score across a broadrange of psychiatric symptoms. The Azrin et al.(1994) study examined change in a specific type ofcomorbid symptomatology—depression.
Family-based therapy was found to be effectivein decreasing psychiatric symptoms among adoles-cent drug abusers in all five studies that formallyassessed changes in psychiatric symptoms. Specifi-cally, Friedman (1989) found reduced adolescent-re-ported psychiatric symptoms in FFT and the controlcondition—parent-training group therapy. Likewise,Szapocznik et al. (1983, 1986, 1988) found reductionsin psychiatric symptoms for structural–strategic fam-ily systems therapy from pretreatment to 12 monthsposttreatment. As in the Friedman study, Szapoczniket al. (1983, 1986) found equivalent changes in thefamily-based control condition and the experimentalcondition, the innovative one-person family therapyexperimental condition. Differential treatment groupeffects were obtained by Azrin et al. (1994), whoreported a large pre- to posttreatment reduction inthe mean score for depression in the BFT condition,whereas the supportive group counseling conditionexhibited no change in depression. However, a con-found clouds the results obtained by Azrin et al.(1994). The mean pretreatment depression score inthe BFT condition was more than twice as high asthat within supportive group counseling (Azrin et al.,1994). Overall, the findings indicate that certain typesof family-oriented interventions can reduce psychiat-ric symptoms in samples of drug-abusing teens. Giventhe focus of some current studies in this area, theseprojects may shed light on the potential benefits ofincorporating psychiatric evaluation and medicationservices as adjuncts to family-based therapy for ado-lescent drug abuse (see Henggeler et al., 1999; Lid-dle, 2000).

280 Ozechowski and Liddle
School Attendance and Performance
Academic failure is another common correlate ofdrug abuse among adolescents (Ary et al., 1999; Ellick-son & Hays, 1992; Hawkins et al., 1992). Moreover,strong involvement in school is a buffering factoragainst teens’ involvement with drugs (Jessor, VanDen Bos, Vanderryn, Costa, & Turbin, 1995; Resnicket al., 1997). Accordingly, school bonding and aca-demic functioning is a core domain in which adoles-cent drug treatments should promote change. Family-based therapies are well-suited for influencing adoles-cent drug abusers’ involvement and performance inschool. School teachers and other personnel are oftendirectly involved inecologically orientedfamily-basedinterventions for adolescent drug abuse. In addition,attendance at school and academic performance areoften the focus of interventions between parents andteens in family-based adolescent therapies.
Four studies reported the effects of family-based therapy on adolescents’ school attendanceand performance. This focus is noteworthy becausetreatments must not only have an impact on symp-toms and negative functioning, but also demonstratechanges in empirically established prosocial anddevelopmentally adaptive competencies. In all ofthe studies reporting school-related outcomes, ado-lescents in the family-therapy condition evidencedmore improved academic functioning than those inalternative treatments. Liddle et al. (in press) foundthat adolescents in MDFT exhibited significantlyhigher increases in grade point average from intaketo 1 year posttreatment (on average, grades im-proved from failing to passing). Grades did notimprove for teens in either of the comparison treat-ments—adolescent group therapy or multifamilygroup education. Brown, Henggeler, Schoenwald,Brondino, and Pickrel (1999) reported that thepercentage of youth who were regularly attendingschool (based on combined self-reports, parent re-ports, and school records) increased more signifi-cantly among youth in MST compared to youth intreatment as usual from intake to 6 months posttermi-nation. Azrin et al. (1994) reported that BFT adoles-cents evidenced a greater increase in school atten-dance from intake to termination than adolescentsin supportive group counseling. Finally, Friedman(1989) found that mothers’ reports of their adoles-cent’s school problems exhibited a marginally sig-nificant decrease in FFT compared to the parent-training group condition. Overall, these findings pro-vide the first evidence of the efficacy of family-based
therapy in improving drug-abusing adolescents’involvement in school. Further research is neededto replicate these findings and identify the types ofinterventions that lead to improved school atten-dance and performance and the direct and/or mediat-ing mechanisms by which these changes occur.
Family Functioning
Improvements in family functioning are hypoth-esized to be a primary mechanism of change in family-based therapies for adolescent drug abuse. That is,a fundamental premise in family-based interventionsis that improvements in core dimensions of familyfunctioning (e.g., communication, cohesion, conflict,parenting practices) are mechanisms by which druguse and other behavioral symptoms subside. In orderto test hypotheses about the role of family function-ing as a mechanism in change, studies of family-basedtherapy for teen drug abuse should include assess-ments of family functioning. In our review, five stud-ies included self-report questionnaires, and five usedbehavioral observation measures [3 clinical trials, 2process studies (videotape ratings)] of family func-tioning.
The findings in all studies in this category suggestthat family-based interventions can improve familyfunctioning among adolescent drug abusers. In five ofseven clinical trials,6 family-based therapy was equallyeffective as alternative treatments in improving familyfunctioning. Friedman (1989) reported that parentand adolescent reports of the quality of the family en-vironment, family role–task behavior, and parent–adolescent communication improved from pretreat-ment to 9 months posttreatment in both FFT and thecomparison parent-training group condition. Like-wise,Szapoczniketal. (1983,1986)reportedsignificantimprovements in observational ratings of seven di-mensions of family functioning [structure, flexibility,resonance, developmental stage, IP-hood (i.e., identi-fied patienthood), conflict, and total functioning] frompretreatment to 12 months posttreatment for bothstructural–strategic and one-person family therapy.Joanning et al. (1992) found that adolescent reports ofthe quality of parent–adolescent communication im-proved significantly from pre- to posttreatment in
6The CYT study is not included in this section because the datato determine how the family-based therapies in CYT comparedto the non-family-based therapies were not available at the timeof the review.

Knowns and Unknowns 281
structural–strategic family therapy as well as in ado-lescent group therapy and family drug education. Fi-nally, Waldron et al. (2000) reported significant im-provements in average family conflict scores (basedon mean conflict scores combining ratings from the ad-olescent and primary caretaker) from intake to 7months postintake for a combined FFT � CBT condi-tion and for adolescent group treatment.
Two clinical trials found family-based therapy tobe superior to alternative treatments in improvingfamily functioning. Azrin et al. (1994) found that bothparent and adolescent reports of satisfaction with theparent–adolescent relationship improved more inBFTthaninsupportive groupcounseling.Also,Liddleet al. (in press) found that observational ratings ofglobal family health (positive, developmentally adap-tive family interactions) improved significantly frompretreatment to 12 months posttreatment among fam-ilies inMDFT, whereas improvements in family healthwere not observed among families in adolescent grouptherapy or multifamily drug education.
The link between improvements in family func-tioning and adolescent problem behavior in family-based therapy has also been studied. Specifically,Schmidt, Liddle, and Dakof (1996) investigated the re-lationship between observed changes in parenting be-havior and levels of adolescent drug abuse and exter-nalizing problem behaviors. Schmidt et al. (1996)conducted observational ratings of the quality of par-enting behavior exhibited during the first three andthe last three sessions of MDFT for 29 adolescent drugabuse cases completing 14–16 treatment sessions.They found significant improvements in the quality ofparenting behavior in 20 of 29 cases in MDFT. Fur-thermore, they found that the observed quality of par-enting behavior improved concurrently with adoles-cent drug use in 59% of MDFT cases and withadolescent acting-out behaviors in 50% of MDFTcases—both statistically significant associations.These findings, as well as those cited in the previousparagraph [the family-based MDFT treatment was as-sociated with observed changes in a family’s interac-tion (family health), whereas the non-family-based in-tervention conditions did not change the family’sfunctioning as rated in the videotapes], provide sup-port for a central tenet of family-based therapy—namely, that therapeuticchanges in family functioninglead to symptom reduction and improved adolescentfunctioning [studies from Henggeler’s group (Huey etal., 2000; Mann et al., 1990) also support the link be-tween behavioral changes in family functioning andchange in adolescent sympomatology].
These studies offer evidence that family func-tioning improves in family-based therapy for adoles-cent drug abuse. Moreover, the study by Schmidtet al. (1996) provides preliminary support for thehypothesis that improvements in family functioning,specifically in parenting behavior, may be a mecha-nism of change in adolescent drug use and behaviorproblems in family-based therapy. At the same time,the Schmidt et al. study did not have a non-family-based treatment comparison group; therefore, we donot know if changes in family functioning are mecha-nisms of change that are unique to family-based treat-ments. Clearly, there is a need for further study ofthe connection between changes in family function-ing and adolescent drug abuse in family-based andalternative treatments.
Treatment Cost and Cost Effectiveness
Little is known about treatment cost or the costeffectiveness of family-based therapy for adolescentdrug abuse. In one of two studies that examined costissues in our review, Schoenwald, Ward, Henggeler,Pickrel, and Patel (1996) found that the costs of pro-viding family-based therapy were approximately 50%higher than the costs of providing treatment as usual.However, during the year following treatment, youthwho received family-based therapy incurred 46%fewer days of incarceration and 64% fewer days ofinpatient psychiatric or residential treatment thanyouth in the alternative condition. Schoenwald et al.(1996) found that the cost savings stemming fromthese reduced incarceration rates offset approxi-mately 50% of the difference in direct costs betweenthe two conditions. Over time, it is possible that con-tinued cost savings resulting from lower rates of post-treatment out-of-home placements would completelyoffset the direct costs of providing family-based ther-apy. No such cost savings were noted for the alterna-tive treatment condition.
The National Treatment Improvement Study(NTIES; Center for Substance Abuse Treatment,2000; Gerstein & Johnson, 1999) is one of the fewstudies to provide formal cost estimates of adolescentoutpatient drug treatment. The NTIES study sur-veyed a nationally representative sample of adoles-cent treatment program directors who estimated thecosts of outpatient adolescent drug treatment. Denniset al. (under review) in the CYT study, the secondstudy in the reviewed articles to address cost issues,used NTIES data as a benchmark against which to
282 Ozechowski and Liddle
compare the five tested adolescent marijuana treat-ments. The economic cost of each treatment in theCYT was determined using the Drug Abuse Treat-ment Cost Analysis Program (DATCAP; French etal., under review). The average weekly cost of MDFT(Liddle, 2000) and FSN (Hamilton et al., 2000) wasless than the lower or upper7 weekly estimates fromthe program directors. The median weekly cost ofoutpatient adolescent drug treatment in the NTIESstudy was $267, and the weekly mean (average) treat-ment cost was $365. The weekly cost of FSN, a combi-nation of family intervention, case management, andCBT and MET interventions was $244, whereas theaverage weekly cost providing MDFT per adolescentwas $164. Both FSN and MDFT were delivered attwo different sites each (not the same sites becausethey were in different assignment arms in the con-trolled trial). FSN has negligible weekly cost differ-ences between the sites in St. Petersburg, Florida,($248) and Farmington, Connecticut ($241), butMDFT had significant cross-site cost differentials atthe two sites where MDFT was tested—MadisonCounty, Illinois ($113 a week per adolescent) andPhiladelphia ($208 a week). Given these treatmentcost findings, Dennis et al. (under review) concludethat these two treatments—MDFT, a stand-alonecomprehensive family-based treatment, and FSN, acomprehensive family-based treatment used as a sup-plement to individually focused adolescent drugabuse treatments—are sustainable under currentfunding levels. The cost-effectiveness data are beinganalyzed presently in the CYT study.
In-Session Processes Associated with Change
Process-outcome studies play an integral role intreatment development research (Diamond & Dia-mond, in press; Friedlander, Wildman, Heatherin-gton, & Skowron, 1994). Observational studies oftreatment processes can reveal essential informationabout how interventions activate mechanisms ofchange vis-a-vis drug and cooccurring problems. Illu-minating the interior of treatment, clinical processstudies inform manual development and therapisttraining and supervision. Moreover, process-outcomestudies can provide critical information about thecontexts and circumstances under which specific in-
7Dennis et al. (under review) use the median as the lower limitestimate and the mean as the upper limit estimate in theNTIES data.
terventions are most appropriate. This new knowl-edge informs decision rules and procedures about thesequencing and the timing of specific interventions.
Progress has been made in the family-basedtreatment process research area. A small numberof process studies have explicated key therapist andclient behaviors associated with successful interven-tion outcomes within specific stages and models oftreatment. For example, as part of the MDFT re-search program, Diamond and Liddle (1996, 1999)explored therapist behaviors associated with success-ful resolution of parent–adolescent impasses duringtreatment. This study found that resolving parent–adolescent impasses was facilitated by therapists’ ef-forts to (i) actively block, divert, or work throughnegative affect; (ii) amplify feelings of sadness,regret, and loss; (iii) solicit the adolescent’s thoughtsand feelings; (iv) focus conversations on parent–adolescent interaction; (v) amplify parents’ empathyfor the adolescent; and (vi) support parents’ efforts tograpple with adolescent behavior. In another MDFTprocess study, Diamond, Liddle, Hogue, and Dakof(1999) identified therapist behaviors associated withimprovements in initially poor therapist–adolescentalliances. In cases showing improved therapeutic alli-ances, therapists (i) attended to adolescents’ experi-ences, (ii) helped adolescents formulate personallymeaningful goals, and (iii) presented themselves as anally more extensively than therapists in unimprovedalliance cases. In another MDFT process study, Jack-son-Gilfort, Liddle and Dakof (in press) found thatengagement of African-American male adolescentsin MDFT is enhanced by discussion of specific cultur-ally relevant themes, including (i) anger and rage,(ii) alienation, and (iii) the teen’s ‘‘journey from boy-hood to manhood.’’
Observational process research methods havealso been applied to the study of therapist adherenceto manualized family-based procedures. Specifically,Hogue et al. (1998) developed the Therapist BehaviorRating Scale (TBRS), a 26-item process coding in-strument to rate therapist adherence to treatmentprotocols in MDFT. The TBRS is based on intensivereview of the MDFT manual and pilot coding of morethan 50 hours of clinical videotape material (Hogueet al.). Using the TBRS and observational processresearch methods, Liddle et al. (2000) demonstratedhigh levels of therapist adherence and treatment dif-ferentiation in their study of the efficacy of MDFTand CBT for adolescent drug abuse.
Process research has only begun to make a sub-stantive impact on the development of adolescent

Knowns and Unknowns 283
drug abuse therapies. Additional process-outcomestudies are needed in all phases of treatment. There isan acute need for the observation and coding of se-quences (see Bakeman & Gottman, 1997) of therapistinterventions as well as therapist–client interaction inthe kind of complex treatments described in this re-view. The sequential coding and analysis of therapist–client behavior is a promising frontier for enhancingknowledge of how interventions change over thecourse of family-based treatment, the manner in whichtherapist and client behaviors are reciprocally interre-lated, and how sequences of in-session behaviors re-late to specific immediate, medium range and perhapsmore distal outcomes in different outcome domains.
Summary
We should take encouragement in the researchfindings on the efficacy of family-based therapy foradolescent drug abuse. There is empirical evidencethat family-based therapies can (i) decrease to clini-cally significant levels adolescent drug use, externaliz-ing and internalizing behavior problems, and symp-toms indicative of psychiatric comorbidity and (ii)increase teens’ involvement with school, and improvetheir family’s functioning—well-established buffersagainst deviance. Intervention effects can endure atleast 12 months beyond the termination of treatmentwithin each of these domains. Furthermore, process-outcome studies have begun to explicate therapistbehaviors and interventions that give rise to thera-peutic success within specific phases of treatment in-cluding engagement and impasse resolution. Takentogether, these findings indicate that much progresshas been made toward developing and establishingfamily-based therapy as an empirically supportedtreatment for adolescent drug abuse. However, muchis yet to be learned about the effects of family-basedtherapies on adolescent drug abuse as well as themethods, mechanisms, and processes by which fam-ily-based therapies work. These treatments will con-tinue to evolve and improve as researchers explorefundamental unknowns.
UNKNOWNS REGARDING THE EFFECTS OFFAMILY-BASED THERAPY FORADOLESCENT DRUG ABUSE
Risky Sexual Behavior
High rates of sexual activity, including sex withmultiple partners and unprotected sexual activity, are
common among adolescent drug abusers (Hubbard,Cavanaugh, Craddock, & Rachal, 1985; Rounds-Bryant, Kristiansen, & Hubbard, 1999). In fact, stud-ies have shown that risky sexual behavior, along withantisocial behavior and academic failure, covarieswith drug abuse among adolescents, and togetherthese features may indicate a general tendency to-ward adolescent deviance (Ary et al., 1999; Tildeslyet al., 1995). Therefore, in addition to the clinicaloutcomes discussed previously, sexual activity andsexual relationships constitute an important focus foradolescent drug abuse treatments, and we are onlyat a beginning stage of understanding how this focalarea might be incorporated into general family-basedtreatments for teens (Liddle et al., 2000). Unfortu-nately, information about sexual activity among ado-lescent drug abusers was not provided in any studieswe reviewed. In fact, very few data exist on the impactof any form of drug abuse treatment on adolescentsexual activity. An exception is a recent study byJainchill, Yagelka, Hawke, and De Leon (1999)which demonstrated significant reductions from pre-treatment to 1 year posttreatment in some aspectsof high-risk sexual activity among both males andfemales following residential treatment for adoles-cent drug abuse.
The question of whether family-based therapycan target and demonstrate positive effects on riskysexual behavior among drug abusing teens remainsunanswered. However, there does seem to be oppor-tunities to examine these issues. Many of the primaryintervention targets in family-based therapy includ-ing parent–adolescent connectedness, open commu-nication between parents and adolescents about sex,and adolescent involvement in school may help fosterthe kind of attitudes toward sex that could diminishrisky sexual behavior (Dilorio, Kelley, & Hockenb-erry-Eaton, 1999; Resnick et al., 1997).
Association with Drug Use and Delinquent Peers
One of the most robust predictors of the onsetand maintenance of adolescent drug use is a teen’saffiliation with drug using peers. Several studies indi-cate that peer influences may be stronger than familyrelationships in predicting the trajectory of drug useduring certain stages of adolescence (Bailey & Hub-bard, 1990; Duncan, Duncan, Biglan, & Ary, 1998;Farrell & White, 1998; Wills & Cleary, 1999) and thatpeer effects mediate the relationship between familyvariables and adolescent drug use (Ary et al., 1999;

284 Ozechowski and Liddle
Blanton, Gibbons, Gerrard, Conger, & Smith, 1997;Dishion, Capaldi, Spracklen, & Li, 1995; Pattersonet al., 1992). Moreover, association with drug-usingpeers is a critical factor in relapse following adoles-cent substance abuse treatment (Brown, Vik, &Creamer, 1989). Thus, it is critical for adolescenttreatments to diminish teens’ involvement with drug-using peer groups and to build ties with non-drug-using peers.
Family-based therapies try to have an impact onpeer relationships in a number of ways. For example,increasing parental monitoring is a standard way ofreducing adolescents’ exposure and vulnerability todrug using peers. Improving parent–adolescent at-tachment and relationship quality attempts to reduceadolescents’ susceptibility to negative peer influ-ences. Contemporary therapies try to strengthen ado-lescents’ connection to prosocial institutions (e.g.,school, church, sports teams, community youth orga-nizations) in which ties with positive adult role mod-els and relationships with prosocial peers may de-velop. Although simple to state, succeeding withthese interventions is complex. Age, gender, and thenonmalleability of particular critical processes in anygiven individual or family will have an impact on theattempt to link a teen with nondeviant peers.
Although direct behavioral assessments of peerrelationships [e.g., observations of interactions withfriends (see Dishion et al., 1995)] were not conductedin any of the studies we reviewed, there is indirectevidence that family-based therapy reduces adoles-cents’ involvement with drug-using and delinquentpeers. For example, diminished externalizing and de-linquent behavior problems in family-based therapy(Henggeler et al., 1991; 1999; Liddle et al., 2000, inpress; Szapocznik et al., 1983, 1986) suggest a reduc-tion in adolescents’ affiliation with negative peersgiven the inherently social nature of these types ofbehavioral problems. Furthermore, connections tonormative peers may strengthen in family-based ther-apy by virtue of increased attendance and perfor-mance in school (Azrin et al., 1994; Brown et al., 1999;Friedman, 1989; Liddle et al., in press).
Although encouraging, these findings also revealhow much we do not know about this particular areaof intervention research with teens. A more directassessment and reporting of adolescent involvementwith drug-using and delinquent peers in the studieswould be helpful. There are a number of well-vali-dated instruments that researchers of family-basedtherapy may use in gathering data from adolescentsregarding levels of drug use among peer networks.
These include the Problem-Oriented Screening In-strument for Teenagers (POSIT; Rahdert, 1991), theAdolescent Drug Diagnosis (ADAD; Friedman &Utada, 1989), the National Youth Survey (Elliot,Huizinga, & Ageton, 1985), the Personal ExperiencesInventory (Winters & Henley, 1989), and the PeerModels of Drug Use Scale (Farrell, Danish, & How-ard, 1992). Moreover, the Problem Situation Inven-tory for Teens (Hall, 1990) may be used to assessadolescents’ susceptibility to peer pressure to usedrugs.
Long-Term Effects
Research has shown that patterns of adolescentdrug abuse tend to be quite stable over time (Brooket al., 1997; Stice, Myers, & Brown, 1998a), exertingnegative developmental effects extending into youngadulthood and beyond (Brook et al., 1998; New-comb & Bentler, 1988; Newcomb, Scheier, & Bentler,1993). Altering the powerful trajectory of drug abuseduring adolescence is an exceedingly difficult task,and relapse from certain types of drug abuse treat-ment is common among adolescents (Brown, Myers,Mott, & Vik, 1994; Brown et al., 1989; Spear, Ciesla, &Skala, 1999; Williams & Chang, 2000). In light ofthe perseverance of adolescent drug abuse and thetypically high rates of relapse from adolescent drugabuse treatment, the number of studies in this reviewdemonstrating sustained effects of family-based ther-apy 6 to 12 months beyond treatment termination isimpressive (Friedman, 1989; Henggeler et al., 1991;Liddle et al., 2000, in press; Szapocznik et al., 1983,1986). Nonetheless, there is much to be learned aboutthe long-term maintenance of treatment outcomes infamily-based therapy for adolescent drug abuse. Aprimary unknown is the duration or intensity of fam-ily-based treatment necessary to achieve lastingchange in drug use and behavioral functioning.Dose–response studies are virtually absent in thisarea. Another question is whether follow-up orbooster sessions improve the long-term durability oftreatment outcomes (see Bry & Krinsley, 1992). Fur-thermore, little is known about the types of environ-mental and contextual correlates of long-term post-treatment success and relapse in family-basedtherapy for adolescent drug abuse. Investigation ofthese and other unknowns pertaining to long-termeffects require follow-up periods of at least 1 yearbeyond the termination of treatment in studies of

Knowns and Unknowns 285
family-based therapy for adolescent drug abuse (Lid-dle & Dakof, 1995a).
Clinical Significance of Treatment Effects
Much attention has been devoted to establishingthe clinical significance of statistically significantchanges that occur as a result of treatment (Jacob-son & Traux, 1991; Jacobson, Roberts, Berns, &McGlinchey, 1999; Kazdin, 1994a, 1999; Kendall,Marrs-Garcia, Nath, & Sheldrick, 1999). Althoughprecise guidelines for the conceptualization and mea-surement of clinically significant change in psycho-therapy research are still evolving, generally acceptedcriteria for clinically significant change include (i)qualitative shift in individuals’ functional status (i.e.,chronic to mild drug use) and (ii) improvement inareas of social importance (e.g., lower crime, lesstruancy) (Kazdin, 1994a, 1999).
Both types clinically significant changes were re-ported in the studies we reviewed. Studies reportingimprovement in adolescents’ functional status in-clude Liddle et al. (in press), who found that a greaterpercentage of adolescents in MDFT compared to ad-olescent group therapy and multifamily educationdecreased their level of drug use to below the mini-mum level required for participation in the study.Similarly, Joanning et al. (1992) reported that agreater percentage of adolescent drug users in struc-tural–strategic family therapy were classified as notusing drugs at posttreatment compared to adolescentgroup therapy and family drug education. Likewise,Lewis et al. (1990) reported that a greater percentageof adolescents in family systems therapy comparedto those in family drug education made ‘‘clinicallyreliable’’ improvements in drug use based on stan-dardized change scores. With regard to the socialimpact of changes in adolescent symptoms, Heng-geler and colleagues reported that adolescents inMST experienced fewer drug-related arrests (Heng-geler et al., 1991) and fewer posttreatment incarcera-tions and out-of-home placements (Henggeler et al.,1999) than adolescents in treatment as usual. Also,Liddle et al. (in press) reported that the percentageof youth in MDFT who had at least a C grade pointaverage increased by 43% from intake to 12 monthsposttreatment compared to increases of 17% in ado-lescent group therapy and 8% in family drug edu-cation.
Although the current findings pertaining to clini-cal significance are a solid beginning, indices of clini-
cally significant change require much more attention.In particular, criteria must be developed for classify-ing reductions in adolescent drug use from clinicallevels to nonclinical or normative levels. The notionof identifying nonclinical or normative levels of ado-lescent drug use is in keeping with Marlatt’s applica-tion of the ‘‘harm reduction’’ model to adolescentsubstance abuse treatment (Baer, MacLean, & Mar-latt, 1998). The harm reduction model views levelsof drug use on a continuum ranging from excess tomoderation to abstinence. Any step toward the lowerend of the continuum is considered to be a positiveoutcome, and treatment need not culminate in absti-nence to be successful. Within the harm reductionmodel, decreases in drug use that result in substantialdiminution of harmful consequences and the restora-tion of adaptive functioning in everyday life are re-garded as clinically significant treatment outcomes.In fact, Marlatt and colleagues (1993) propose thatreduction and moderation may be more realistic aswell as developmentally appropriate treatment objec-tives than abstinence for adolescent substance abus-ers (Baer et al., 1998).
From the perspective of harm reduction, per-haps the best indication of clinically significantchange in adolescent drug use is the restoration ofadolescent functioning in everyday life. An emphasison the restoration of functioning as opposed tosymptom reduction per se is also in line withKazdin’s (1999) view of clinical significance. Thisperspective incorporates indices of adaptive func-tioning within multiple spheres of adolescent every-day life. Such indices may include attending school,improving grades, getting a job, participating inextracurricular activities or community youth orga-nizations, and so on (see Jessor et al., 1995). Reduc-tions in symptoms of drug use, comorbidity, andbehavior problems could be considered to be clini-cally significant to the extent that they are accompa-nied by improvements in areas of adolescentdaily functioning.
Mechanisms of Change in Family-Based Therapy
Knowledge about treatment effectiveness entailsunderstanding the pathways or mechanisms throughwhich treatments produce clinical outcomes. Family-based therapies hypothesize that changes within coredomains of adolescent life, especially the family, areresponsible for clinical outcomes in drug use andcooccurring symptomatology (see Gorman-Smith,

286 Ozechowski and Liddle
Tolan, Loeber, & Henry, 1998; Huey et al., 2000). Anumber of different findings in this review providepreliminary support for putative mechanisms ofchange in family-based therapies. First, as previouslydiscussed, particular forms of family-based therapypromote improvement in one or more functional do-mains that are supposed mechanisms of change.These domains include self-reported and behavior-ally rated family functioning, connection to and per-formance in school, and peer-related delinquent be-havior. Second, several studies showed thatimprovements in putative change mechanisms werein fact accompanied by reductions in drug use (Azrinet al., 1994; Friedman, 1989; Liddle et al., 2000, inpress; Szapocznik et al., 1983, 1986). Moreover,Schmidt et al. (1996) established a direct link betweenimprovements in parenting quality in MDFT and re-ductions in adolescent drug use.
Further studies are needed to establish causativeconnections between drug use outcomes and im-provements according to hypothesized mechanismsof change. We have several recommendations to en-hance the study of change mechanisms in family-based therapy for adolescent drug abuse. First, re-searchers should conduct comprehensive assessmentsof change over time within the individual, family,school, and peer domains hypothesized to producechanges in adolescent drug use and associated symp-toms. Second, researchers should demonstrate that(i) family-based therapy produces change drug useand in functional domains presumed to be mecha-nisms of change, (ii) improvements in hypothesizedchange mechanisms temporally precede changes indrug use, (iii) improvements in change mechanismsare directly related to reductions in drug use, and (iv)the effects of family-based therapy on hypothesizedchange mechanisms mediate or account for a substan-tial portion of treatment effects on drug use (seeBaron & Kenny, 1986). Along these same lines, weencourage researchers in this area to begin using ana-lytical techniques capable of modeling direct and me-diational effects among multiple variables over time.Longitudinal structural equation modeling (Farrell,1994) and latent growth curve modeling (Willett &Sayer, 1994) are examples of analytical approacheswell-suited for testing hypotheses about mechanismsof change.
Moderators of Treatment Effects
Moderators of treatment effects refer to child,family, parent, therapist, and contextual factors that
influence the impact treatment has on specific out-come variables (Holmbeck, 1997). By and large, mod-erators of the effectiveness of child and adolescenttreatments have not been studied systematically(Kazdin & Weisz, 1998). We found the same to betrue regarding research on the effects of family-basedtherapy for adolescent drug abuse. In fact, analysesof factors that moderate or interact with the effectsof family-based therapy for adolescent drug abuseare virtually absent in the studies we reviewed.
Research on moderators of clinical outcomes isessential for the development and refinement of fam-ily-based therapies. In particular, knowledge aboutmoderators of treatment effectiveness may provideclues for appropriately matching specific types of ado-lescent drug abusers to family-based versus alterna-tive treatments (see Longabaugh, Wortz, DiClem-ente, & Litt, 1994; Miller & Cooney, 1994). Perhapsmore importantly, research on moderator variablesmay illuminate the manner in which family-basedtherapy should be tailored to address the needs ofspecific subtypes of adolescent drug abusers. The nextsection identifies a number of potentially influentialmoderator variables.
Gender
Male and female adolescent drug abusers havebeen shown to differ in ways that may have importantimplications for how family-based therapy should ad-dress gender-related symptoms and risk factors. Mostnotably, female adolescent drug abusers are morelikely than their male counterparts to exhibit symp-toms of depression and anxiety, in addition to levelsof externalizing behavior equivalent to male drugabusers (Dakof, 2000; Hops, Davis, & Lewin, 1999;Khoury, 1998; Opland, Winters, & Stinchfield, 1995;Rounds-Bryant, Khristiansen, Fairbank, & Hubbard,1998; Scheier & Botvin, 1996a). These contrastingbehavioral profiles suggest possible gender differ-ences in the nature and etiology of adolescent drugabuse that may have important treatment implica-tions. Specifically, some investigators believe thatfamily-based therapy for female adolescent drugabusers requires a special focus on emotional andpsychological distress in addition to the managementof drug use and externalizing behavior (Dakof, 2000).
In the only study to examine treatment by gen-der interactions in family-based therapy, Henggeleret al. (1999) found that MST was highly effectivecompared to treatment as usual in decreasing drug

Knowns and Unknowns 287
use among female adolescents from pre- to posttreat-ment. However, by 6 months posttreatment, drug useamong female adolescents in family-based therapyhad deteriorated substantially. No such effects wereevident for males in either condition or females inthe comparison condition. This finding supports thecontention that female adolescents may have differ-ent treatment needs than males in family-based ther-apy (Dakof, 2000). Further studies are needed offemale adolescent drug abusers’ clinical needs as wellas the types of family-based interventions that aremost effective for females.
Ethnicity
Research is needed on the role of culturally spe-cific risk and protective factors among adolescents ofdifferent ethnic backgrounds in family-based therapyfor adolescent drug abuse. Studies have shown thatlevels of drug use among Hispanic adolescents covarywith levels of acculturation (Brook, Whiteman,Balka, Win, & Gursen, 1997; Vega, Gil, & Wagner,1998). It is believed that because Hispanic childrentend to acculturate more quickly and thoroughly thantheir parents, family conflicts arise when acculturatedadolescents do not conform to their parents’ moreethnocentric ways. In turn, parent–adolescent con-flicts stemming from acculturation differences mayincrease the risk of substance abuse among His-panic adolescents.
Levels of acculturation may influence the effec-tiveness of family-based interventions among His-panic adolescents and their families. For example,Santisteban et al. (1996) found that non-Cuban His-panic families were significantly more likely to en-gage in treatment than more acculturated Cuban His-panic families. The manner in which acculturationissues should be addressed within family-based ther-apy for Hispanic teens needs further investigation. Itmay be that family interventions are most effectiveamong Hispanic adolescents when intergenerationalconflicts and communicational barriers over culturalidentity issues can be addressed. Moreover, interven-tions to strengthen adolescents’ sense of identifica-tion with their Hispanic cultural roots may help toalleviate low self-esteem that often stems from asense of cultural displacement among U.S.-born His-panic adolescents (Vega et al., 1998).
Likewise, more research is needed on the role ofcultural factors in family-based therapy with African-American adolescent drug abusers. Research consis-
tently demonstrates lower drug use levels among Af-rican-American adolescents than among adolescentsof most other ethnic groups (Costa, Jessor, & Turbin,1999; Kilpatrick et al., 2000; Wallace & Bachman,1991). Studies suggest that African-American adoles-cents may be insulated against drug use by relativelystronger identification with moral and religious pro-hibitions against drug use, as well as by generallymore strict parental monitoring (Biafora & Zimmer-man, 1998; Taylor et al., 1999). However, as African-American adolescents get older, their risk for druguse tends to increase. Some investigators believe thisis due to culturally conditioned feelings of mistrust,hopelessness, and an impoverished outlook of thefuture (Scheier & Botvin, 1996b). Cultural mistrustand hopelessness often manifest themselves in theform of aggression and sensation-seeking behaviorthat in turn increase the risk of substance abuseamong African-American adolescents. Family-basedtreatment may be most effective for African-Ameri-can adolescents when moral and religious valuesagainst drug abuse are emphasized. Moreover, asshown by Jackson-Gilfort et al. (in press), discussionof culturally specific themes including mistrust, angerand rage, alienation, respect, and the journey fromboyhood to manhood may enhance the effectivenessof family-based therapy among African-Americanadolescent drug abusers (see Jackson-Gilfort & Lid-dle, in press, for the clinical intervention).
Psychiatric Comorbidity
Adolescent drug abusers often manifest comor-bid psychiatric disorders including conduct dis-order, ADHD, and depression (Brook et al., 1998;Greenbaum, Foster-Johnson, & Petrila, 1996; Kandelet al., 1997). Although a high degree of comorbiditywas present among adolescents in several of the stud-ies we reviewed, the moderating effect of psychiatriccomorbidity within family-based therapy for adoles-cent drug abuse was not examined. Adolescents withcomorbid psychiatric disorders are generally moredifficult to treat and may be less responsive to family-based therapy than adolescent drug abusers withoutcomorbid disorders (see Myers, Stewart, & Brown,1998; Stice, Myers, & Brown, 1998b; Weinberg et al.,1998). Integrating family-based therapy with pharma-cologic treatments may enhance treatment outcomesfor dually diagnosed adolescent drug abusers (seeKaminer, Tarter, Bukstein, & Kabene, 1992).

288 Ozechowski and Liddle
Motivation for Treatment
Adolescents’ pretreatment level of motivationand readiness for change has been shown to stronglypredict retention in treatment and drug use outcomeswithin residential and outpatient treatment modal-ities (Cady, Winters, Jordan, Solberg, & Stinchfield,1996; Melnick, De Leon, Hawke, Jainchill, & Kressel,1997). Accordingly, highly motivated adolescentsmay be more amenable to family-based therapy thanadolescents who are relatively less motivated fortreatment. Several studies (Diamond et al., 1999; San-tisteban et al., 1996; Szapocznik et al., 1988) demon-strate how motivation for treatment is malleable.These studies devised and tested specialized engage-ment and alliance-building interventions to facilitatetreatment process and outcome. For instance, effec-tive alliance establishing procedures include at-tending to the adolescent’s experiences, formulatingpersonally meaningful treatment goals, and pres-enting the therapist as an ally to the adolescent—andmaking sure of all of this before change strategiesare proposed (Diamond et al., 1999). In addition,Monti and colleagues (1997) outline motivational in-terviewing techniques that may be useful in family-based therapy with resistant adolescent drug abusers.
Parental and Sibling Substance Abuse
Substance abuse among parents and siblings in-creases adolescents’ risk for abusing drugs (Brook,Kessler, & Cohen, 1999; Hoffman & Su, 1998; Wong,Zucker, Puttler, & Fitzgerald, 1999). A strong par-ent–adolescent attachment (normally a protectivefactor against adolescent drug abuse) may actuallyhave a detrimental effect on adolescents with drug-abusing parents (Andrews, Hops, & Duncan, 1997;Fleming, Brewer, Gainey, Haggerty, & Catalano,1997). These findings suggest that family-based ther-apy for adolescent drug abuse may be differentiallyeffective based on levels of parent and sibling drugabuse. Incorporating drug abuse interventions forparents and siblings may be instrumental in at-tempting to achieve success with teens in family-based treatments (Catalano, Gainey, Fleming, Hag-gerty, & Johnson, 1999).
Transportability
A major consideration in evaluating the effec-tiveness of any treatment is its capacity for successful
implementation by therapists in community-basedclinical settings (Backer, David, & Soucy, 1995; Insti-tute of Medicine, 1998; Sobell, 1996). A number ofstudies in this review indicate that family-based treat-ments can be administered successfully in communitysettings, albeit under well-controlled and closely su-pervised conditions (Friedman, 1989; Henggeler etal., 1991; Liddle et al., 2000, in press). Important find-ings exist about the transportability of family-basedtherapy into more naturalistic clinical settings. Heng-geler et al. (1999) investigated the effects of imple-menting MST in community-based clinics without di-rect supervision from the developers of MST.Specifically, two therapists and one supervisor withina community-based clinical facility were providedwith 40 hours of initial training in MST. Thereafter,therapists received 1.5 hours of weekly supervisionfrom the clinic supervisor, rather than from expertsin MST from the research team. Henggeler et al.(1999) found this effort to transfer MST from thehands of the model developers to those of clinic staffresulted in markedly weaker drug use and delin-quency outcomes than in previous studies by Heng-geler and colleagues (1997). Specifically, Henggeleret al. (1999) found that adolescents in MST exhibitedmodest improvements in self-reported drug use andcriminal activity that were equivalent to those of ado-lescents in treatment as usual who received far fewerand less comprehensive services than adolescents inMST. Moreover, Henggeler et al. found that levelsof therapist adherence were lower in the currentstudy than in previous studies of MST, and that levelsof therapist adherence were associated with drug useoutcomes in the current study. A major conclusionof this study was that the absence of direct supervi-sion from the MST research team resulted in lowerlevels of therapist adherence, which in turn damp-ened the effectiveness of MST in reducing adolescentdrug use and delinquent behavior.
Further studies of the effectiveness of family-based therapy in typical clinical settings and treat-ment circumstances are urgently needed. Thesewould include (i) studies of family-based therapy im-plemented as a stand-alone treatment and (ii) studiesof family-based therapy as a component that is inte-grated within existing community-based clinical ser-vices (see McLellan et al., 1993). In particular, effec-tiveness research should investigate the acceptabilityof ecological family-based treatment methods amongcommunity-based therapists. It remains to be seenwhether treatment systems can support and whethercommunity-based therapists are receptive to main-

Knowns and Unknowns 289
taining daily contact with cases and to providing treat-ment in the home and other sites within the adoles-cent’s social ecology. Effectiveness research shouldalso examine the manner in which skills for workingsimultaneously with members of multiple social sys-tems can be imparted among community-based clini-cians. Moreover, we do not know the amount andtype of training needed for supervisors within com-munity clinics to provide effective supervision in fam-ily-based therapy.
Cost Effectiveness
Another boundary condition with implicationsfor treatment development is the cost effectivenessof clinical services (French, 1995; Yates, 1994; Zarkin,French, Anderson, & Bradley, 1994). Two fundamen-tal cost-related questions to consider are as follows:(i) Is the cost of providing family-based therapyworth the outcome? and (ii) Is family-based therapymore cost effective than other forms of treatment foradolescent drug abuse? Answers to questions such asthese require that cost–benefit and cost-effectivenessanalyses be incorporated into family-based treatmentdevelopment research (see French, 1995; Yates,1997). Briefly, cost–benefit analyses compare thecosts of providing treatment services with the mone-tary value of the benefits accrued as a result of treat-ment, thereby indicating the value of a particulartreatment. Cost-effectiveness analyses examine thecosts of treatment per unit of outcome (e.g., days ofabstinence, number of readmissions). The expendi-tures required for two or more programs to achievethe same outcome can be compared in a cost-effec-tiveness analysis.
Additional research is needed on the costs andbenefits of family-based therapy relative to othercommon adolescent drug-abuse treatment modal-ities such as inpatient and residential services, partialhospitalization and day treatment programs, thera-peutic communities, group treatments, and individ-ual outpatient services. We recommend researchersfocus the economic evaluation of family-based ther-apy on two somewhat distinct categories of benefits,including benefits to society and benefits to health-care service programs. Benefits to society includereduced numbers of drug abusers, reduced crimeand incarceration rates, higher productivity in workand school, reductions in drug-related health care
expenditures, and so on.8 In contrast, benefits toservice programs tend to be more circumscribedthan benefits to society and include factors suchas fewer repeat admissions, fewer hours of serviceconsumed per client, greater numbers of clientsserved, improved clinical outcomes, reductions inthe restrictiveness of services provided, and so on.Benefits to society are particularly appealing toofficials and administrators from local and federalgovernments who are concerned with social costsof adolescent drug abuse. However, managed careproviders and mental health care administratorsmay be more motivated by program-level economicbenefits. We recommend that researchers of family-based therapy for adolescent drug abusers tailorcost–benefit and cost-effectiveness analyses to theneeds, concerns, and motivations of the intendedconsumers of cost-related data.
Regardless of the purpose of particular cost–benefit and cost-effectiveness analyses, researchersof family-based therapy should study the costs andbenefits of treatment at both the client and the pro-gram levels. At the client level, comparisons can bemade between the types, amounts, and costs of ser-vices used by adolescents in family-based versus alter-native treatments. A useful instrument for document-ing client-level service utilization is the TeenTreatment Services Review (T-TSR; Kaminer, Blitz,Burleson, & Sussman, 1998). At the program level,researchers may want to study the overall costs ofservices within particular drug treatment programsbefore and after the integration of family-based ther-apy into existing services. French, Dunlap, Zarkin,McGeary, and McClellan (1997) developed the DrugAbuse Treatment Cost Analysis Program (DAT-CAP; see also www.DATCAP.com), which computesthe cost of a range of services provided over a fixedperiod of time within specific drug treatment pro-grams.
CONCLUSIONS AND FUTURE DIRECTIONS
Tremendous strides have been made toward es-tablishing family-based therapy as an empirically de-veloped and supported treatment for adolescent drugproblems. Theory- and research-oriented family-
8Although our focus is on tangible costs related to service utiliza-tion, it is also worthwhile to consider the value of relatively lesstangible changes in physical and emotional well-being. See French,Rachal, and Hubbard (1993) for a review.

290 Ozechowski and Liddle
based interventions have been formulated, manu-alized, and tested within a variety of clinical trialsand process studies. Solid empirical support existsfor the efficacy of family-based therapy in ameliorat-ing drug abuse, externalizing and internalizing behav-ioral problems, and symptoms of psychiatric comor-bidity among drug-abusing adolescents. Moreover,empirical support has been obtained for hypothe-sized mechanisms of change within family-based ther-apy for adolescent drug abuse, including improvedfamily functioning, involvement in school, and reduc-tions in peer-associated delinquent behavior. In addi-tion, process studies have illuminated ingredients ofintervention effectiveness within key stages of treat-ment. These areas of progress are signs that family-based therapy for adolescent drug abuse has evolvedinto a bona fide clinical and research specialty. In-deed, the progress that has taken place within thisspecialty exemplifies what Berscheid (1999) calls ‘‘thegreening of relationship science’’ (p. 206).
According to several indicators, the specialty offamily-based therapy for adolescent drug abuse isentering a new stage of development. Federal re-search support for family-based therapy for adoles-cent drug problems is at an all-time high. Innovativestudies, including practice research projects that aretesting the transportation of research-based interven-tions into community settings, are underway. Whencompleted, these studies will reveal the possibilitiesand problems of adapting and transferring existingand effective family-based therapies to nonresearchsettings. Beyond expanded federal support and a newwave of practice research studies, however, lies theissue of how new and existing studies and research,and the new knowledge that these efforts create canbe organized to enhance information yield and appli-cability. An organizing framework for synthesizingexisting findings and informing new generations ofstudies would help to consolidate and clarify progresswithin this specialty. In this review, we attempt tobegin defining and articulating a framework for treat-ment development research in family-based therapyfor adolescent drug abuse. Specifically, based on thefew existing but solid treatment development re-search guidelines in the psychotherapy literature, wehave articulated a set of knowns and unknowns re-garding the status of family-based therapy as an em-pirically developed and supported treatment for ado-lescent drug abuse. This treatment developmentperspective is intended to facilitate the identificationof components, mechanisms, moderators, processes,and boundary conditions of effective treatment. Prior
to this review, these dimensions of treatment devel-opment had not been comprehensively evaluatedwith regard to family-based therapy for adolescentdrug abuse. Hence, this review offers a characteriza-tion of the current state-of-the-science and some rec-ommendations for future treatment development re-search within this specialty.
Implementing a comprehensive treatment devel-opment research agenda in family-based adolescentdrug abuse therapy requires studies that thus far havebeen rare. In particular, dismantling and constructiveresearch designs are needed to compare the effective-ness of different versions of family-based therapy andpinpoint the effects of specific treatment componentsor combinations of components (see Kazdin, 1994a,1998). Moreover, parametric strategies (e.g., dose–response studies) are needed to identify the amount,frequency, duration, and intensity of family-basedtherapy necessary for producing particular outcomes.In addition, as discussed previously, process–out-come research is essential within all phases and stagesof family-based therapy to sharpen our understand-ing of how manualized interventions should be imple-mented and how therapist behavior is linked tochanges in adolescent and family functioning.
Therapist variables merit more focused attentionin treatment development research on family-basedtherapy for adolescent drug abuse. In particular,factors related to the quality of the therapist–adolescent/family relationship and its associationwith treatment retention and outcome in family-based interventions for adolescent drug problemshave been understudied. In addition, levels of thera-pist adherence and competence should be studied asmechanisms of treatment effectiveness and as out-comes in their own right. Issues pertaining to definingand measuring therapist competence have been dis-cussed in the psychotherapy research literature(Elkin, 1999; Waltz, Addis, Koerner, & Jacobson,1993). Developing standards and criteria for assessingtherapist competence within and across models offamily-based therapy for adolescent drug abuse rep-resents an important frontier for treatment develop-ment research (Hogue et al., 1996, 1998).
Treatment development research on family-based therapy has been hampered by inconsistentconceptualization and measurement of core outcomedomains such as drug use, behavior problems, andcomorbidity. By and large, measurements withinthese domains have suffered from what Kazdin andKagan (1994) refer to as ‘‘construct ambiguity’’ (p.42) or the operationalization of constructs in overly

Knowns and Unknowns 291
global terms. For example, measurements of druguse (or the way they are described and reported) instudies of family-based therapy generally have notdistinguished between different types of drugs or thewidely varying amounts, frequencies, combinations,and circumstances in which adolescents use them. Bythe same token, measures of ‘‘behavior problems’’and ‘‘comorbidity’’ in studies of family-based therapyfor adolescent drug abuse have not delineated treat-ment effects on specific types of behavioral and psy-chiatric symptoms. As is the case across the entirefield of substance abuse treatment, a greater level ofconceptual specificity and precision of measurementwould enhance family-based theory and interventiondevelopment. In addition, establishing consensusamong researchers on a core battery of outcome mea-sures would promote consistency and facilitate meta-analytic comparisons across studies (see Stanton &Shadish, 1997; Weisz & Hawley, 1998).
Family-based therapy development for adoles-cent drug abuse can be advanced by returning to afoundational measurement and research method infamily research—observation-based details aboutchanges in family functioning. However, most studieswithin this area either have not assessed family func-tioning or have measured change in family function-ing using self-report instruments. In addition toproviding a unique level of depth and richness, obser-vational measures are useful for describing patternsand sequences of family interaction (and family–therapist interaction)—primary targets of family-based interventions. Excellent guidelines for con-ducting observational assessments of family function-ing are provided by Alexander, Newell, Robbins, andTurner (1995), Margolin et al. (1998), and Markmanand Notarius (1987).
The transportation of family-based therapy intointegrated adolescent drug-abuse treatment servicesystems has profound implications for future treat-ment development research. (Schoenwald & Heng-geler, in press). More than ever before, family-basedtreatment development research requires collabora-tive partnerships among researchers, administrators,and providers within clinical service delivery systems(Altman, 1995; Backer et al., 1995; IOM, 1998; Sobell,1996). Family-based treatment development researchwill become more integrated into community-basedsubstance abuse treatment settings, and the treat-ment system itself (treatment administration and or-ganization, including the financing of treatment) willbe a focus of investigation. Researchers will studyfamily-based treatment models that have been tai-
lored to fit the clinical and administrative contingen-cies of different treatment systems (see Strosahl,1998). In addition to adolescent and family outcomes,researchers will assess organizational and system-level variables pertaining to family-based treatmentimplementation and service utilization (McGrew,Bond, Dietzen, & Salyers, 1994). Types of importantvariables relevant within family-based disseminationresearch include the size of therapists’ caseloads; thenumber and frequency of therapist contacts with theadolescent, family, and members outside the family;the amount and types of services families receivein addition to family-based therapy; and the cost offamily-based services. Moreover, researchers will as-sess levels of readiness, receptivity, and commitmentamong administrative and clinical staff toward theimplementation of family-based treatment methods(Brown, 1995; Backer, 1995; Corrigan et al., 1998).Researchers will also study the effectiveness of differ-ent methods and strategies for training clinical serviceproviders to implement manualized family-based in-terventions for adolescent drug abuse (see Keller &Galanter, 1999; Sorensen, Hall, Loeb, & Allen, 1988).Studying the transportation and dissemination offamily-based therapy will be facilitated by importingmethods of applied services research within tradi-tional psychotherapy research designs (Hendrick,Bickman, & Rog, 1993; Schoenwald & Henggeler,in press). Qualitative interviews, needs assessments,ethnographic field observations, and focus groups areexamples of services research strategies that will be-come important components of treatment develop-ment research on family-based therapy for adolescentdrug abuse.
Treatment development efforts should continueto be informed by basic research on the onset andmaintenance of adolescent drug abuse (see Kazdin,1997; Kazdin & Kendall, 1998). For example, inter-ventions targeting peer-related drug influences couldbe crafted based on Dishion and colleagues’ studiesof the types of peer conversations that predict adoles-cent drug abuse (Dishion et al., 1995; Dishion,McCord, & Poulin, 1999), as well as Scheier andBotvin’s (1998) research showing how personal com-petencies (academic self-esteem, decision-makingskills, self-management, and assertiveness) coupledwith high social skills buffer adolescents against peer-related invitations and pressures to use drugs. Ad-vances such as these in the basic research aspectsof adolescent drug abuse along with innovations intreatment efficacy, effectiveness, process, and ser-vices research can strengthen the scientific founda-
292 Ozechowski and Liddle
tion of family-based therapy for adolescent drugabuse. We hope this review facilitates cross-fertiliza-tion of these research domains and adds greaterorganization and momentum to the emergence of atreatment development research agenda within fam-ily-based therapies for adolescent drug abuse.
ACKNOWLEDGMENTS
Preparation of this article was supported bygrants from the National Institute on Drug Abuse(P50 DA07697, P50 DA11328, and 2 T32 DA07297-06), and from the Center for Substance Abuse Treat-ment (1 KD1 TI11871-01 and 5UR4 TI11323).
REFERENCES
Alexander, J. F., Newell, R. M., Robbins, M. S., & Turner,C. W. (1995). Observational coding in family therapy processresearch. Journal of Family Psychology, 9, 355–365.
Altman, D. G. (1995). Sustaining interventions in community sys-tems: On the relationship between researchers and communi-ties. Health Psychology, 14, 526–536.
American Academy of Child and Adolescent Psychiatry (1997).Practice parameters for the assessment and treatment of chil-dren and adolescents with substance use disorders. Journalof the American Academy of Child and Adolescent Psychiatry,36, 140S–156S.
Andrews, J. A., Hops, H., & Duncan, S. C. (1997). Adolescentmodeling of parent substance use: The moderating effect ofthe relationship with the parent. Journal of Family Psychol-ogy, 11, 259–270.
Armbruster, P., & Kazdin, A. (1994). Attrition in child psychother-apy. In T. H. Ollendick and R. J. Prinz (Eds.), Advances inclinical child psychology (Vol. 16, pp. 81–108). New York:Plenum Press.
Ary, D. V., Duncan, T. E., Biglan, A., Metzler, C. W., Noell, J.W., & Smolkowski, K. (1999). Development of adolescentproblem behavior. Journal of Abnormal Child Psychology,27, 141–150.
Azrin, N. H., Donohue, B., Besalel, V. A., Kogan, E. S., & Acierno,R. (1994). Youth drug abuse treatment: A controlled outcomestudy. Journal of Child and Adolescent Substance Abuse, 3,1–16.
Backer, T. E. (1995). Assessing and enhancing readiness forchange: Implications for technology transfer. In. T. E. Backer,S. L. David, & G. Soucy (Eds.), Reviewing the behavioralscience knowledge base on technology transfer. NIDA Re-search Monograph No. 155. Rockville, MD: National Instituteon Drug Abuse.
Backer, T. E., David, S. L., & Soucy, G. (Eds.). (1995). Reviewingthe behavioral science knowledge base on technology transfer.NIDA Research Monograph No. 155. Rockville, MD: Na-tional Institute on Drug Abuse.
Baer, J. S., MacLean, M. G., & Marlatt, G. A. (1998). Linkingetiology and treatment for adolescent substance abuse: To-ward a better match. In R. Jessor (Ed.), New prespectives onadolescent risk behavior (pp. 182–220). New York: CambridgeUniversity Press.
Bailey, S. L., & Hubbard, R. L. (1990). Developmental variation
in the context of marijuana initiation among adolescents. Jour-nal of Health and Social Behavior, 31, 58–70.
Bakeman, R., & Gottman, J. M. (1997). Observing interaction:An introduction to sequential analysis 2nd ed. New York:Cambridge University Press.
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediatorvariable distinction in social psychological research: Concep-tual, strategic, and statistical considerations. Journal of Per-sonality and Social Psychology, 51, 1173–1182.
Baumrind, D., & Moselle, K. A. (1985). A developmental perspec-tive on adolescent drug abuse. Advances in Alcohol and Sub-stance Abuse, 4, 41–67.
Berscheid, E. (1999). The greening of relationship science. Ameri-can Psychologist, 54, 260–266.
Blanton, H., Gibbons, F. X., Gerrard, M., Conger, K. J., & Smith,G. E. (1997). Role of family and peers in the developmentof prototypes associated with substance use. Journal of FamilyPsychology, 11, 271–288.
Biafora, F., & Zimmerman, R. (1998). Developmental patterns ofAfrican-American adolescent drug use. In W. A. Vega, A. G.Gil, and Associates, Drug use and ethnicity in early adolescence(pp. 149–175). New York: Plenum Press.
Bronfenbrenner, U. (1979). The ecology of human development:Experiments by nature and design. Cambridge, MA: HarvardUniversity Press.
Brook, J. S., Balka, E. B., Gursen, M. D., Brook, D. W., Shapiro,L., & Cohen, P. (1997). Young adults’ drug use: A 17-yearlongitudinal inquiry of antecedents. Psychological Reports,80, 1235–1251.
Brook, J. S., Cohen, P., & Brook, D. W. (1998). Longitudinalstudy of co-occurring psychiatric disorders and substance use.Journal of the American Academy of Child and AdolescentPsychiatry, 37, 322–330.
Brook, J. S., Kessler, R. C., & Cohen, P. (1999). The onset ofmarijuana use from preadolescence and early adolescence toyoung adulthood. Development and Psychopathology, 11,901–914.
Brook, J. S., Nomura, C., & Cohen, P. (1989). A network ofinfluences on adolescent drug involvement: Neighborhood,school, peer, and family. Genetic, Social, and General Psychol-ogy Monographs, 115, 123–145.
Brook, J. S., Whiteman, M., Balka, E. B., Win, P. T., & Gursen,M. D. (1997). African-American and Puerto Rican drug use:A longitudinal study. Journal of the American Academy ofChild and Adolescent Psychiatry, 36, 1260–1268.
Brown, B. S. (1995). Reducing impediments to technology transferin drug abuse programming. In T. E. Backer, S. L. David, &G. Soucy (Eds.), Reviewing the behavioral science knowledgebase on technology transfer. NIDA Research Monograph No.155. Rockville, MD: National Institute on Drug Abuse.
Brown, S. A., Myers, M. G., Mott, M. A., & Vik, P. W. (1994).Correlates of success following treatment for adolescent sub-stance abuse. Applied and Preventative Psychology, 3, 61–73.
Brown, S. A., Vik, P. W., & Creamer, V. A. (1989). Characteristicsof relapse following adolescent substance abuse treatment.Addictive Behaviors, 14, 291–300.
Brown, T. L., Henggeler, S. W., Schoenwald, S. K., Brondino,M. J., & Pickrel, S. G. (1999). Multisystemic treatment ofsubstance abusing and dependent juvenile offenders: Effectson school attendance at posttreatment and 6-month follow-up. Children’s Services: Social Policy, Research, and Practice,2, 81–93.
Bry, B. H., & Krinsley, K. E. (1992). Booster sessions and long-term effects of behavioral family therapy on adolescent sub-stance abuse and school performance. Jornal of BehaviorTherapy and Experimental Psychiatry, 23, 183–189.
Cady, M. E., Winters, K. C., Jordan, D. A., Solberg, K. B., &Stinchfield, R. D. (1996). Motivation to change as a predictor
Knowns and Unknowns 293
of treatment outcome for adolescent substance abusers. Jour-nal of Child and Adolescent Substance Abuse, 5, 73–91.
Carroll, K. M., & Rounsaville, B. J. (1990). Can a technologymodel of psychotherapy research be applied to cociane abusetreatment? In L. S. Onken & J. B. Blaine (Eds.), Psychother-apy and counseling in the treatment of drug abuse. NIDAresearch Monograph 104. Rockville, MD: National Instituteon Drug Abuse.
Catalano, R. F., Gainey, R. R., Fleming, C. B., Haggerty, K. P., &Johnson, N. O. (1999). An experimental intervention withfamilies of substance abusers: One-year follow-up of the focuson families project. Addiction, 94, 241–254.
Chambliss, D. L., & Hollon, S. D. (1998). Defining empiricallysupported therapies. Journal of Consulting and Clinical Psy-chology, 66, 7–18.
Costa, F. M., Jessor, R., & Turbin, M. S. (1999). Transition intoadolescent problem drinking: The role of psychosocial riskand protective factors. Journal of Studies on Alcohol, 60,480–490.
Corrigan, P. W., Williams, O. B., McCracken, S. G., Kommana,S., Edwards, M., & Brunner, J. (1998). Staff attitudes thatimpede the implementation of behavioral treatment pro-grams. Behavior Modification, 22, 548–562.
Crits-Cristoph, P., & Siqueland, L. (1996). Psychosocial treatmentfor drug abuse: Selected review and recommendations fornational health care. Archives of General Psychiatry, 53,749–756.
CSAT [Center for Substance Abuse Treatment]. (1999). Treat-ment of adolescents with substance use disorders. TreatmentImprovement Protocol (TIP) Series 32. Rockville, MD: U.S.Department of Health and Human Services.
CSAT [Center for Substance Abuse Treatment]. (2000). The Na-tional Treatment Improvement Evaluation Study: Adolescentsand young adults in treatment. [Online]. Available: http://www.health.org/nties/young/yungall.htm.
Cunningham, P. B., & Henggeler, S. W. (1999). Engaging multi-problem families in treatment: Lessons learned throughoutthe development of multisystemic therapy. Family Process,38, 265–286.
Dakof, G. A. (2000). Understanding gender differences in adoles-cent drug abuse: Issues of comorbidity and family functioning.Journal of Psychoactive Drugs, 32, 1–24.
Dennis, M. L. (1999). Global Appraisal of Individual Needs(GAIN): Administration guide for the GAIN and related mea-sures. Bloomington, IL: Chestnut Health Systems. [Online].Available: http://www.chestnut.org/li/gain/gadm1299.pdf.
Dennis, M. L., Titus, J., Diamond, G., Babor, T., Donaldson, J.,Godley, S. H., Tims, F., & Webb, C. (under review). TheCannabis Youth Treatment (CYT) Experiment: A multi-sitestudy of five approaches to outpatient treatment for adoles-cents. Journal of Substance Abuse Treatment.
Diamond, G. S., & Diamond, G. M. (in press). Studying coremechanisms of change: An agenda for family-based processresearch. In H. Liddle, H. Santisteban, Levant, D., Bray, J.(Eds.), Family psychology science. Washington, DC: Ameri-can Psychological Association Press.
Diamond, G. S., & Liddle, H. A. (1996). Resolving a therapeuticimpasse between parents and adolescents in MultidimensionalFamily Therapy. Journal of Consulting and Clinical Psychol-ogy, 64, 481–488.
Diamond, G. S., & Liddle, H. A. (1999). Transforming negativeparent–adolescent interactions: From impasse to dialogue.Family Process, 38, 5–26.
Diamond, G. M., Liddle, H. A., Hogue, A., & Dakof, G. A. (1999).Alliance building interventions with adolescents in familytherapy: A process study. Psychotherapy: Theory, Research,Practice, and Training, 36, 355–368.
Dilorio, C., Kelley, M., & Hockenberry-Eaton, M. (1999). Commu-
nication about sexual issues: Mothers, fathers, and friends.Journal of Adolescent Health, 24, 181–189.
Dishion, T. J., Capaldi, D., Spracklen, K. M., & Li, F. (1995).Peer ecology of male adolescent drug use. DevelopmentalPsychopathology, 7, 803–824.
Dishion, T. J., McCord, J., & Poulin, F. (1999). When interventionsharm: Peer groups and problem behavior. American Psycholo-gist, 54, 755–764.
Dishion, T. J., Reid, J. B., & Patterson, G. R. (1988). Empiricalguidelines for a family intervention for adolescent drug use.Journal of Chemical Dependency Treatment, 1, 189–224.
Docherty, J. P. (1984). Implications of the technology model ofpsychotherapy. In J. B. W. Williams & R. L. Spitzer (Eds.),Psychotherapy research: Where are we and where should wego? New York: Guilford.
Donohue, B., Azrin, N., Lawson, H., Friedlander, J., Teicher, G., &Rindsberg, J. (1998). Improving initial session attendance ofsubstance abusing and conduct disordered adolescents: A con-trolled study. Journal of Child and Adolescent SubstanceAbuse, 8 (1), 1–13.
Duncan, S. C., Duncan, T. E., Biglan, A., & Ary, D. (1998). Contri-bution of the social context to the development of adolescentsubstance use: A multivariate latent growth modeling ap-proach. Drug and Alcohol Dependence, 50, 57–71.
Elkin, I. (1999). A major dilemma in psychotherapy outcome re-search: Disentabgling therapists from therapies. Clinical Psy-chology Science and Practice, 6, 10–32.
Ellickson, P. L., & Hays, R. D. (1992). On becoming involvedwith drugs: Modeling adolescent use over time. Health Psy-chology, 11, 377–385.
Elliot, D. S., Huizinga, D., & Ageton, S. S. (1985). Explainingdelinquency and drug use. Beverly Hills, CA: Sage.
Farrell, A. D. (1994). Structural equation modeling with longitudi-nal data: Strategies for examining group differences and recip-rocal relationships. Journal of Consulting and Clinical Psy-chology, 62, 477–487.
Farrell, A. D., Danish, S. J., & Howard, C. W. (1992). Relationshipbetween drug use and other problem behaviors in urban ado-lescents. Journal of Consulting and Clinical Psychology, 60,705–712.
Farrell, A. D., & White, K. S. (1998). Peer influences and druguse among urban adolescents: Family structure and parent–adolescent relationship as protective factors. Journal of Con-sulting and Clinical Psychology, 66, 248–258.
Fleming, C. B., Brewer, D. D., Gainey, R. R., Haggerty, K. P., &Catalano, R. F. (1997). Parent drug use and bonding to parentsas predictors of substance use in children of substance abusers.Journal of Child and Adolescent Substance Abuse, 6, 75–86.
French, M. T. (1995). Economic evaluation of drug abuse treat-ment programs: Methodology and findings. American Journalof Drug and Alcohol Ause, 21, U111–135.
French, M. T., Dunlap, L. J., Zarkin, G. A., McGeary, K. A., &McLellan, A. T. (1997). A structured instrument for estimat-ing the economic cost of drug abuse treatment. Journal ofSubstance Abuse Treatment, 14, 445–455.
French, M. T., Rachal, J. V., & Hubbard, R. L. (1991). Conceptualframework for estimating the social cost of drug abuse. Journalof Health and Social Psychology, 2, 1–22.
French, M. T., Roebuck, M. C., Dennis, M. L., Babor, T., Diamond,G., Godley, S. H., Tims, F., & Herrell, J. (under review). Theeconomic cost of outpatient marijuana treatment for adoles-cents: Findings from a multisite field experiment. Journal ofSubstance Abuse Treatment.
Friedlander, M. L., Wildman, J., Heatherington, L., & Skowron,E. A. (1994). What we do and don’t know about the processof family therapy. Journal of Family Psychology, 8, 390–416.
Friedman, A. S. (1989). Family therapy vs. parent groups: Effectson adolescent drug abusers. The American Journal of FamilyTherapy, 17, 335–347.
294 Ozechowski and Liddle
Friedman, A. S., & Utada, A. (1989). A method for diagnosingand planning the treatment of adolescent drug abusers: TheAdolescent Drug Abuse Diagnosis (ADAD) Instrument.Journal of Drug Education, 19, 285–312.
Gerstein, D. R., & Johnson, R. A. (1999). Adolescent and youngadults in the national treatment improvement evaluation study(National Evaluation Data Services Report). Rockville, MD:Center for Substance Abuse Treatment.
Gilvarry, E. (2000). Substance abuse in young people. Journalof Child Psychology and Psychiatry and Allied Disciplines,41, 55–80.
Godley, S. H., Godley, M. D., & Dennis, M. L. (in press). Theassertive aftercare protocol for adolescent substance abusers.In E. Wagner & H. Waldron (Eds.), Innovations in adolescentsubstance abuse interventions. New York: Elsevier ScienceLtd.
Godley, S. H., Meyers, R. J., Smith, J. E., Godley, M. D., Titus,J. M., Karvinen, T., Dent, G., Passetti, L., & Kelberg, P.(2000). The Adolescent Community Reinforcement Approach(ACRA) for Adolescent Cannabis Users (Vol. 4 of the Canna-bis Youth Treatment (CYT) manual series). Rockville, MD:Center for Substance Abuse Treatment, Substance Abuse andMental Health Services Administration. (http://www.samhsa.gov/csat/csat.htm).
Gorman-Smith, D., Tolan, P. H., Loeber, R., & Henry, D. B.(1998). Relation of family problems to patterns of delinquentinvolvement among urban youth. Journal of Abnormal ChildPsychology, 26, 319–333.
Greenbaum, P. E., Foster-Johnson, L., & Petrila, A. (1996). Co-occuring addictive and mental disorders among adolescents:Prevalence research and future directions. American Journalof Orthopsychiatry, 66, 52–60.
Greenberg, L. S., Heatherington, L., & Friedlander, M. L. (1996).The events-based approach to couple and family therapy ther-apy research. In D. H. Sprenkle & S. M. Moon (Eds.), Re-search methods in family therapy. New York: Guilford Press.
Haley, J. (1976). Problem solving therapy. San Fransisco: Jos-sey-Bass.
Hall, J. A. (1990). Problem Situation Inventory for Teens. Unpub-lished manuscript. University of California, San Diego.
Hamilton, N., Brantley, L., Tims, F., Angelovich, N., & McDougall,B. (2000). Family Support Network (FSN) for Adolescent Can-nabis Users (Vol. 3 of the Cannabis Youth Treatment (CYT)manual series). Rockville, MD: Center for Substance AbuseTreatment, Substance Abuse and Mental Health Services Ad-ministration. (http://www.samhsa.gov/csat/csat.htm).
Hawkins, J. D., Catalano, R. F., & Miller, J. Y. (1992). Risk andprotective factors for alcohol and other drug problems inadolescence and early adulthood: Implications for substanceabuse prevention. Psychological Bulletin, 112, 64–105.
Hendrick, T. E., Bickaman, L., & Rog, D. J. (1993). Applied re-search design: A practical guide. Newbury Park, CA: Sage Pub-lications.
Henggeler, S. W. (1993). Multisystemic treatment of serious juve-nile offenders: Implications for the treatment of substance-abusing youths. In L. S. Onken, J. D. Blaine, & J. J. Boren(Eds), Behavioral treatments for drug abuse and dependence(NIDA Research Monograph No. 137, NIH Publication No.93-3684 ed., pp. 181–200). Rockville, MD: National Instituteon Drug Abuse.
Henggeler, S. W., & Borduin, C. M. (1990). Family therapy andbeyond: A multisystemic approach to treating the behaviourproblems of children and adolescents. Pacific Grove, CA:Brooks/Cole Publishing.
Henggeler, S. W., Borduin, C. M., Melton, G. B., Mann, B. J.,Smith, L. A., Hall, J. A., Cone, L., & Fucci, B. R. (1991).Effects of multisystemic therapy on drug use and abuse inserious juvenile offenders: A progress report from two out-
come studies. Family Dynamics of Addiction Quarterly, 1,40–51.
Henggeler, S. W., Melton, G. B., Brondino, M. J., Scherer,D. G., & Hanley, J. H. (1997). Multisystemic therapy withviolent and chronic juvenile offenders and their families: Therole of treatment fidelity in successful dissemination. Journalof Consulting and Clinical Psychology, 65, 821–833.
Henggeler, S. W., Pickrel, S. G., & Brondino, M. J. (1999). Multi-systemic treatment of substance abusing and dependent delin-quents: Outcomes, treatment fidelity, and transportability.Mental Health Services Research, 1, 171–184.
Henggeler, S. W., Pickrel, S. G., Brondino, M. J., & Crouch, J. L.(1996). Eliminating (almost) treatment dropout of substanceabusing or dependent delinquents through home-based multi-systemic therapy. American Journal of Psychiatry, 153,427–428.
Henggeler, S. W., Schoenwald, S. K., Borduin, C. M., Rowland,M. D., & Cunningham, P. B. (1998). Multisystemic treatmentof antisocial behavior in children and adolescents. New York:Guilford Press.
Henggeler, S. W., Schoenwald, S. K., & Pickrel, S. G. (1995).Multisystemic therapy: Bridging the gap between university-and community-based treatment. Journal of Consulting andClinical Psychology, 63, 709–717.
Henggeler, S. W., Schoenwald, S. K., Pickrel, S. G., Brondino,M. J., Borduin, C. M., & Hall, J. A. (1994). Treatment manualfor family preservation using multisystemic therapy. Columbia,SC: SC Health and Human Services Finance Commission.
Hoffman, L. (1981). Foundations of family therapy. New York:Basic Books.
Hoffman, J. P., & Su, S. S. (1998). Parental substance use disorder,mediating variables and adolescent drug use: A non-recursivemodel. Addiction, 93, 1351–1364.
Hogue, A., Liddle, H. A., & Rowe, C. (1996). Treatment adherenceprocess research in family therapy: A rationale and somepractical guidelines. Psychotherapy, 33, 332–345.
Hogue, A., Liddle. H. A., Rowe, C., Turner, R. M., Dakof, G., &LaPann, K. (1998). Treatment adherence and differentiationin individual versus family therapy for adolescent substanceabuse. Journal of Consulting and Clinical Psychology, 45,104–114.
Holmbeck, G. N. (1997). Toward terminological, conceptual, andstatistical clarity in the study of mediators and moderators:Examples from the child–clinical and pediatric psychologyliteratures. Journal of Consulting and Clinical Psychology,65, 599–610.
Hops, H., Davis, B., & Lewin, L. M. (1999). The development ofalcohol and other substance use: A gender study of family andpeer context. Journal of Studies on Alcohol, 13 (Supp), 22–31.
Hubbard, R. L., Cavanaugh, E. R., Craddock, S. G., & Rachal, J.V. (1985). Characteristics, behaviors, and outcomes for youthin the TOPS. In A. S. Friedman & G. M. Beshner (Eds.),Treatment services for adolescent substance abusers. Rockville,MD: National Institute on Drug Abuse.
Huey, S. J., Henggeler, S. W., Brondino, M. J., & Pickrel, S. G.(2000). Mechanisms of change in multisystemic therapy: Re-ducing delinquent behavior through therapist adherence andimproved family and peer functioning. Journal of Consultingand Clinical Psychology, 68(3), 451–467.
Institute of Medicine (1998). Bridging the gap between practiceand research: Forging partnerships with community-baseddrugs and alcohol treatment. Washington, DC: National Acad-emy Press.
Jackson-Gilfort, A., Liddle, H. A., & Dakof, G. (in press). Usingculturally specific themes to enhance engagement of African-American males in family therapy: A process study. Journalof Black Psychology.
Jackson-Gilfort, A., & Liddle, H. A. (in press). Culturally specific
Knowns and Unknowns 295
interventions to enhance engagement of African Americanmales in therapy. American Journal of Orthopsychiatry.
Jacobson, N. S., Roberts, L. J., Berns, S. B., & McGlinchey, J.B. (1999). Methods for defining and determining the clinicalsignificance of treatment effects: Description, application, andalternatives. Journal of Consulting and Clinical Psychology,67, 300–307.
Jacobson, N. S., & Traux, P. (1991). Clinical significance: A statisti-cal approach to defining meaningful change in psychotherapyresearch. Journal of Consulting and Clinical Psychology,59, 12–19.
Jainchill, N., Yagelka, J., Hawke, J., & De Leon, G. (1999). Adoles-cent admissions to residential drug treatment: HIV risk behav-iors pre- and posttreatment. Psychology of Addictive Behav-iors, 13, 163–173.
Jessor, R., Van Den Bos, J., Vanderryn, J., Costa, F. M., & Turbin,M. S. (1995). Protective factors in adolescent problem behav-ior: Moderator effects and developmental change. Develop-mental Psychology, 31, 923–933.
Joanning, H., Quinn, Q., Thomas, F., & Mullen, R. (1992). Treatingadolescent drug abuse: A comparison of family systems ther-apy, group therapy, and family drug education. Journal ofMarital and Family Therapy, 18, 345–356.
Kaminer, Y., Blitz, C., Burleson, J. A., & Sussman, J. (1998).The Teen Treatment Services Review (T-TSR). Journal ofSubstance Abuse Treatment, 4, 291–300.
Kaminer, Y., Tartar, R. E., Bukstein, O. G., & Kabene, M. (1992).Comparison between treatment completers and noncomplet-ers among dually diagnosed substance abusing adolescents.Journal of the American Academy of Child and AdolescentPsychiatry, 31, 1046–1049.
Kandel, D. B., Johnson, J. G., Bird, H. R., Canino, G., Goodman,S. H., Lahey, B. B., Regier, D. A., & Schwab-Stone, M. (1997).Psychiatric disorders associated with substance use amongchildren and adolescents: Findings from the Methods for theEpidemiology of Child and Adolescent Mental Disorders(MECA) study. Journal of Abnormal Child Psychology, 25,121–132.
Kazdin, A. E. (1987). Child and adolescent dysfunction and pathstoward maladjustment: Targets for intervention. Clinical Psy-chology Review, 12, 795–817.
Kazdin, A. E. (1994a). Methodology, design, and evaluation inpsychotherapy research. In A. E. Bergin & S. L. Garfield(Eds.), Handbook of psychotherapy and behavior change (4thed., pp. 19–71). New York: John Wiley & Sons.
Kazdin, A. E. (1994b). Psychotherapy for children and adolescents.In A. E. Bergin & S. L. Garfield (Eds.), Handbook of psycho-therapy and behavior change (4th ed., pp. 543–594). NewYork: John Wiley & Sons.
Kazdin, A. E. (1997). A model for developing effective treatment:Progression and interplay of theory, research, and practice.Journal of Consulting and Clinical Psychology, 26, 114–129.
Kazdin, A. E. (1998). Research design in clinical psychology (3rded.). Needham Heights, MA: Allyn & Bacon.
Kazdin, A. E. (1999). The meanings and measurement of clinicalsignificance. Journal of Consulting and Clinical Psychology,67, 332–339.
Kazdin, A. E., & Kagan, J. (1994). Models of dysfunction in devel-opmental psychopathology. Clinical Psychology: Science andPractice, 1, 35–52.
Kazdin, A. E., & Kendall, P. C. (1998). Current progress andfuture plans for developing effective treatments: Commentsand perspectives. Journal of Clinical Child Psychology, 27,217–226.
Kazdin, A. E., & Mazurick, J. L. (1994). Dropping out of childpsychotherapy: Distinguishing early and late dropout overthe course of treatment. Journal of Consulting and ClinicalPsychology, 62, 1069–1074.
Kazdin, A. E., Mazurick, J. L., & Bass, D. (1993). Risk for attrition
in treatment of antisocial children and families. Journal ofClinical Child Psychology, 22, 2–16.
Kazdin, A. E., & Weisz, J. R. (1998). Identifying and developingempirically supported child and adolescent treatments. Jour-nal of Consulting and Clincial Psychology, 66, 19–36.
Keller, D. S., & Galanter, M. (1999). Technology transfer of net-work therapy to community-based addictions counselors.Journal of Substance Abuse Treatment, 16, 183–189.
Kendall, P. C., Marrs-Garcia, A., Nath, S. R., & Sheldrick, R. C.(1999). Normative comparisons for the evaluation of clinicalsignificance. Journal of Consulting and Clinical Psychology,67, 285–299.
Khoury, E. (1998). Are girls different? A developmental perspec-tive on gender differences in risk factors for substance useamong adolescents. In W. A. Vega, A. G. Gil, and Associates,Drug use and ethnicity in early adolescence (pp. 95–123). NewYork: Plenum Press.
Kilpatrick, D. G., Acierno, R., Schnurr, P. P., Saunders, B., Re-snick, H. S., & Best, C. L. (2000). Risk factors for adolescentsubstance abuse and dependecne: Data from a national sam-ple. Journal of Consulting and Clinical Psychology, 68, 19–30.
Leccese, M., & Waldron, H. B. (1994). Assessing adolescent sub-stance use: A critique of current measurement instruments.Journal of Substance Abuse Treatment, 11, 553–563.
Lewis, R. A., Piercy, F. P., Sprenkle, D. H., & Trepper, T. S.(1989). The Purdue brief family therapy model for adolescentsubstance abusers. In T. Todd & M. Selekman (Eds.), Familyapproaches with adolescent substance abusers. New York:Gardner.
Lewis, R. A., Piercy, F. P., Sprenkle, D. H., & Trepper, T. S.(1990). Family-based interventions for helping drug-abusingadolescents. Journal of Adolescent Research, 5, 82–95.
Lerner, R. M., & Galambos, N. L. (1998). Adolescent develop-ment: Challenges and opportunities for research, programs,and policies. Annual Review of Psychology, 49, 413–446.
Liddle, H. A. (1981). Keeping abreast of developments in thefamily therapy field: The use of ‘‘concept cards’’ in clinicalpractice. In A. Gurman (Ed.), Questions and answers in familytherapy: Vol. 1. New York: Brunner/Mazel.
Liddle, H. A. (1995). Conceptual and clinical dimensions of amultidimensional, multisystems engagement strategy in fam-ily-based adolescent treatment. Psychotherapy: Theory, Re-search, and Practice, 32, 39–58.
Liddle, H. A. (1996). Family-based treatment for adolescent prob-lem behaviors: Overview of contemporary developments.Journal of Family Psychology, 10(1), 3–11.
Liddle, H. A. (1999). Theory development in family-based therapyfor adolescent drug abuse. Journal of Clinical Child Psychol-ogy, 28, 521–532.
Liddle, H. A. (2000). Multidimensional family therapy treatmentmanual for the Cannabis Youth Treatment Multisite Collabora-tive Project. Rockville, MD: Center for Substance AbuseTreatment.
Liddle, H. A., & Dakof, G. A. (1995a). Efficacy of family therapyfor drug abuse: Promising but not definitive. Journal of Maritaland Family Therapy, 21, 511–544.
Liddle, H. A., & Dakof, G. A. (1995b). Family-based treatmentsfor adolescent drug abuse: State of the science. In E. Rahd-ert & D. Czechowicz (Eds.), Adolescent drug abuse: Clinicalassessment and therapeutic interventions (NIDA ResearchMonograph No. 156, pp. 218–254). Rockville, MD: NationalInstitute on Drug Abuse.
Liddle, H. A., Dakof, G. A., & Diamond, G. (1991). Adolescentsubstance abuse: Multidimensional family therapy in action.In E. Kaufman & P. Kaufman (Eds.), Family therapy of drugand alcohol abuse (2nd ed., pp. 120–171). Needham Heights,MA: Allyn & Bacon.
Liddle, H. A., Dakof, G. A., Parker, K., Diamond, G. S., Barrett,K., & Tejeda, M. (in press). Multidimensional Family Therapy
296 Ozechowski and Liddle
for adolescent drug abuse: Results of a randomized clinicaltrial. American Journal of Drug and Alcohol Abuse.
Liddle, H. A., & Hogue, A. (in press). Multidimensional familytherapy: Pursuing empirical support through planned treat-ment development. In E. Wagner and H. Waldron (Eds.),Adolescent substance abuse. Needham Heights, MA: Al-lyn & Bacon.
Liddle, H. A., & Rowe, C. L. (1998). Family measures in drugabuse prevention research. In R. Ashery (Ed.), Drug abuseprevention through family interventions (NIDA ResearchMonograph 177, pp. 324–372) Rockville, MD: National Insti-tute on Drug Abuse.
Liddle, H. A., Rowe, C., Diamond, G. M., Sessa, F., Schmidt,S., & Ettinger, D. (2000a). Towards a developmental familytherapy: The clinical utility of adolescent development re-search. Journal of Marital and Family Therapy, 26, 491–506.
Liddle, H. A., Rowe, C., Dakof, G., & Lyke, J. (1998). Translatingparenting research into clinical interventions for families ofadolescents. Clinical Child Psychology and Psychiatry, 3,419–443.
Liddle, H. A., Turner, R. M., Tejeda, M. J., & Dakof, G. A.(2000b). Treating adolescent substance abuse: A comparisonof cognitive behavioral therapy and multidimensional familytherapy. Manuscript submitted for publication.
Longabaugh, R., Wirtz, P. W., DiClemente, C. C., & Litt, M.(1994). Issues in the development of client-treatment match-ing hypotheses. Journal of Studies on Alcohol, 12 (Suppl.),46–59.
Mann, B. J., Borduin, C. M., Henggeler, S. W., & Blaske,D. M. (1990). An investigation of systemic conceptualizationsof parent–child coalitions and symptom change. Journal ofConsulting and Clinical Psychology, 58, 336–344.
Margolin, G., Oliver, P. H., Gordis, E. B., O’Hearn, H. G., Medina,A. M., Ghosh, C. M., & Moreland, L. (1998). The nuts andbolts of behavioral observation of marital and family interac-tion. Clinical Child and Family Psychology Review, 1,195–213.
Markman, H. J., & Notarius, C. I. (1987). Coding marital andfamily interaction: Current status. In T. Jacob (Ed.), Familyinteraction and psychopathology: Theories, methods, and find-ings (pp. 329–390). New York: Plenum Press.
Marlatt, G. A., Larimer, M. E., Baer, J. S., & Quigley, L. A. (1993).Harm reduction for alcohol problems: Moving beyond thecontrolled drinking controversy. Behavior Therapy, 24,461–503.
McGrew, J. H., Bond, G. R., Dietzen, L., & Salyers, M. (1994).Measuring the fidelity of implementation of a mental healthprogram model. Journal of Consulting and Clinical Psychol-ogy, 62, 670–678.
McLellan, A. T., Arnndt, I., Metzger, D., Grossom, G., Woody,G., Luborsky, L., & O’Brien, C. (1993). The effects of psy-chosocial services in substance abuse treatment. Journal ofthe American Medical Association, 269, 1953–1959.
McMahon, R., & Metzler, C. (1998). Selecting parenting measuresfor assessing family based prevention interventions. In R.Ashery (Ed.), Drug abuse prevention through family interven-tions (NIDA Research Monograph 177, pp. 294–323). Rock-ville, MD: National Institute on Drug Abuse.
Melnick, G., De Leon, G., Hawke, J., Jainchill, N., & Kressel, D.(1997). Motivation and readiness for therapeutic communitytreatment among adolescent and adult substance abusers.American Journal of Drug and Alcohol Abuse, 23, 485–506.
Miller, W. R., & Cooney, N. L. (1994). Designing studies to investi-gate client-treatment matching. Journal of Studies on Alcohol,12(Suppl.), 38–45.
Miller, G. E., & Prinz, R. J. (1990). Enhancement of social learninginterventions for childhood conduct disorder. PsychologicalBulletin, 108, 291–307.
Minuchin, S. (1974). Families and family therapy. Cambridge, MA:Harvard University Press.
Minuchin, S., & Fishman, H. C. (1981). Family therapy techniques.Cambridge, MA: Harvard University Press.
Monti, P. M., Colby, S. M., Spirito, A., Barnett, N. P., Rohsenow,D. J., Myers, M., Woolard, R. H., & Lewander, W. J. (1997).Treating alcohol dependence. New York: Guilford Press.
Morrissey-Kane, E., & Prinz, R. J. (1999). Engagement in childand adolescent treatment: The role of parental cognitions andattrubutions. Clinical Child and Family Psychology Review,2, 183–198.
Myers, M. G., Stewart, D. G., & Brown, S. A. (1998). Progressionfrom conduct disorder to antisocial personality disorder fol-lowing treatment for adolescent substance abuse. AmericanJournal of Psychiatry, 155, 479–485.
Newcomb, M. D., & Bentler, P. M. (1988). Impact of adolescentdrug use and social support on problems of young adults: Alongitudinal study. Journal of Abnormal Psychology, 97,64–75.
Newcomb, M. D., Scheier, L. M., & Bentler, P. M. (1993). Effectsof adolescent drug use on adult mental health: A prospectivestudy of a community sample. Experimental and Clinical Psy-chopharmacology, 1, 215–241.
Nichols, M. P., & Schwartz, R. C. (1998). Family therapy: Conceptsand methods (4th ed.). Needham Heights, MA: Allyn &Bacon.
Onken, L. S., Blaine, J. D., & Battjes, R. J. (1997). Behavioraltherapy research: A conceptualization of a process. In S. W.Henggeler & S. B. Santos (Eds.), Innovative approaches fordifficult-to-treat populations (pp. 477–485). Washington, DC:American Psychiatric Press.
Opland, E. A., Winters, K. C., & Stinchfield, R. D. (1995). Examin-ing gender differences in drug-abusing adolescents. Psychol-ogy of Addictive Behaviors, 9, 167–175.
Patterson, G., Reid, J., & Dishion, T. (1992). Antisocial boys.Eugene, OR: Castalia.
Petraitis, J., Flay, B. R., Miller, T. Q., Torpy, E. J., & Greiner, B.(1998). Illicit substance use among adolescents: A matrix ofprospective predictors. Substance Use and Misuse, 33, 2561–2604.
Prinz, R. J., & Miller, G. E. (1996). Parental engagement interven-tions for children at risk for conduct disorder. In R. D. Pe-ters & R. J. McMahon (Eds.), Preventing disorders, substanceabuse, and delinquency. Thousand Oaks, CA: Sage.
Rahdert, E. R. (1991). The Adolescent Assessment/Referral SystemManual. Rockville, MD: U.S. Department of Health and Hu-man Services.
Resnick, M. D., Bearman, P. S., Blum, R. W., Bauman, K. E.,Harris, K. M., Jones, J., Tabor, J., Beuhring, T., Sieving,R. E., Shew, M., Ireland, M., Bearinger, L. H., & Udry, J. R.(1997). Protecting adolescents from harm: Findings from theNational Longitudinal Study on Adolescent Health. Journalof the American Medical Association, 278, 823–831.
Robbins, M. S., Alexander, J. F., Newell, R. M., & Turner, C. W.(1996). The immediate effect of reframing on client attitudein family therapy. Journal of Family Psychology, 10, 28–34.
Rounds-Bryant, J. L., Kristiansen, P. L., & Hubbard, R. L. (1999).Drug Abuse Treatment Outcome Study of Adolescents: Acomparison of client characteristics and pretreatment behav-iors in three treatment modalities. American Journal of Drugand Alcohol Abuse, 25, 573–591.
Rounds-Bryant, J. L., Kristiansen, P. L., Fairbank, J. A., & Hub-bard, R. L. (1998). Substance use, mental disorders, abuse,and crime: Gender comparisons among a national sampleof adolescent drug treatment clients. Journal of Child andAdolescent Substance Abuse, 7, 19–34.
Sampl, S., & Kadden, R. (2000). A 5 session Motivational Enhance-ment Therapy and Cognitive Behavioral Therapy (MET-CBT-5) for adolescent cannabis users (Vol. 1 of the Cannabis Youth
Knowns and Unknowns 297
Treatment (CYT) manual series). Rockville, MD: Center forSubstance Abuse Treatment, Substance Abuse and MentalHealth Services Administration. (http://www.samhsa.gov/csat/csat.htm).
Santisteban, D. A., Szapocznik, J., Perez-Vidal, A., Kurtines, W.M., Murray, E. J., & LaPerriere, A. (1996). Efficacy of inter-vention for engaging youth and families into treatment andsome variables that may contribute to differential effective-ness. Journal of Family Psychology, 10, 35–44.
Scheier, L. M., & Botvin, G. J. (1996a). Psychosocial correlates ofaffective distress: Latent-variable models of male and femaleadolescents in a community sample. Journal of Youth andAdolescence, 26, 89–115.
Scheier, L. M., & Botvin, G. L. (1996b). Purpose in life, cognitiveefficacy, and general deviance as determinants of drug abusein urban black youth. Journal of Child and Adolescent Sub-stance Abuse, 5, 1–26.
Scheier, L. M., & Botvin, G. J. (1998). Relations of social skills,personal competence, and adolescent alcohol use: A develop-mental exploratory study. Journal of Early Adolescence, 18,77–114.
Schmidt, S. E., Liddle, H. A., & Dakof, G. A. (1996). Changes inparental practices and adolescent drug abuse during Multidi-mensional Family Therapy. Journal of Family Psychology,10, 12–27.
Schoenwald, S. K., & Henggeler, S. W. (in press). Services researchand family based treatment. In H. A. Liddle, D. Santisteban,R Lavant, & J. Bray (Eds.), Family psychology interventionscience. Washington, DC: American Psychological Associ-ation.
Schoenwald, S. K., Ward, D. M., Henggeler, S. W., Pickrel,S. G., & Patel, H. (1996). Multisystemic therapy treatment ofsubstance abusing or dependent adolescent offenders: Costsof reducing incarceration, inpatient, and residential place-ment. Journal of Child and Family Studies, 5, 431–444.
Sobell, L. C. (1996). Bridging the gap between scientists and prac-titioners: The challenge before us. Behavior Therapy, 27,297–320.
Sorensen, J. L., Hall, S. M., Loeb, P., & Allen, T. (1988). Dissemina-tion of a job seekers’ workshop to drug treatment programs.Behavior Therapy, 19, 143–155.
Spear, S. F., Ciesla, J. R., & Skala, S. Y. (1999). Relapse patternsamong adolescents treated for chemical dependency. Sub-stance Use and Misuse, 34, 1795–1815.
Stanton, M. D., & Shadish, W. R. (1997). Outcome, attrition, andfamily-couples treatment for drug abuse: A meta-analysis andreview of the controlled, comparative studies. PsychologicalBulletin, 122, 170–191.
Stanton, M. D., Todd, T. C., & Associates. (1982). The familytherapy of drug abuse and addiction. New York: Guilford.
Stice, E., Myers, M. G., & Brown, S. A. (1998a). A longitudinalgrouping analysis of adolescent substance use escalationand de-escalation. Psychology of Addictive Behaviors, 12,136–146.
Stice, E., Myers, M. G., & Brown, S. A. (1998b). Relations ofdelinquency to adolescent substance use and problem use: Aprospective study. Psychology of Addictive Behaviors, 12,136–146.
Strosahl, K. (1998). The dissemination of manual-based psycho-therapies in managed care: Promises, problems, and prospects.Clinical Psychology: Science and Practice, 5, 382–386.
Szapocznik, J., Kurtines, W. M., Foote, F. H., Perez-Vidal, A., &Hervis, O. (1983). Conjoint versus one-person family therapy:Some evidence for the effectiveness of conducting family ther-apy through one person. Journal of Consulting and ClinicalPsychology, 51, 889–899.
Szapocznik, J., Kurtines, W. M., Foote, F., Perez-Vidal, A., &Hervis, O. (1986). Conjoint versus one-person family therapy:Further evidence for the effectiveness of conducting family
therapy through one person with drug-abusing adolescents.Journal of Consulting and Clinical Psychology, 54, 395–397.
Szapocznik, J., Perez-Vidal, A., Brickman, A. L., Foote, F. H.,Santisteban, D., Hervis, O., & Kurtines, W. M. (1988). Engag-ing adolescent drug abusers and their families in treatment:A strategic structural systems approach. Journal of Consultingand Clinical Psychology, 56, 552–557.
Taylor, W. C., Ayars, C. L., Gladney, A. P., Peters, R. J., Roy, J.R., Prokhorov, A. V., Chamberlain, R. M., & Gritz, E. R.(1999). Beliefs about smoking among adolescents—Genderand ethnic differences. Journal of Child and Adolescent Sub-stance Abuse, 8, 37–54.
Tildesley, E. A., Hops, H., Ary, D., & Andrews, J. A. (1995).Multitrait–multimethod model of adolescent deviance, druguse, academic, and sexual behaviors. Journal of Psychopathol-ogy and Behavioral Assessment, 17, 185–215.
Vega, W. A., Gil, A. G., & Wagner, E. (1998). Cultural adjustmentand Hispanic adolescent drug use. In W. A. Vega, A. G. Gil,and Associates, Drug use and ethnicity in early adolescence(pp. 125–148). New York: Plenum Press.
Waldron, H. B. (1997). Adolescent substance abuse and familytherapy outcome: A review of randomized trials. In T. H.Ollendick & R. J. Prinz (Eds.), Advances in Clinical ChildPsychology (Vol. 19, pp. 199–234). New York: Plenum Press.
Waldron, H. B., Slesnick, N., & Brody, J. L., Turner, C., & Pe-terson, T. (2000). Four- and seven-month treatment outcomesfor substance abusing youth. Manuscript submitted for publi-cation.
Wallace, J. M., & Bachman, J. C. (1991). Explaining racial/ethnicdifferences in adolescent drug use: The impact of backgroundand lifestyle. Social Problems, 38, 333–357.
Waltz, J., Addis, M., Koerner, K., & Jacobson, N. (1993). Testingthe integrity of a psychotherapy protocol: Assessment of ad-herence and competence. Journal of Consulting and ClinicalPsychology, 61, 620–630.
Webb, C., Scudder, M., Kaminer, Y., & Kadden, R. (2000). TheMET/CBT 5 Supplement: 7 Sessions of Cognitive BehavioralTherapy (CBT 7) for adolescent cannabis users. (Vol. 2 of theCannabis Youth Treatment (CYT) manual series). Rockville,MD: Center for Substance Abuse Treatment, SubstanceAbuse and Mental Health Services Administration. (http://www.samhsa.gov/csat/csat.htm).
Weinberg, N. Z., & Glantz, M. D. (1999). Child psychopathologyrisk factors for drug abuse: Overview. Journal of Clinical ChildPsychology, 28, 290–297.
Weinberg, N. Z., Rahdert, E., Colliver, J. D., & Glantz, M. D.(1998). Adolescent substance abuse: A review of the past10 years. Journal of the American Academy of Child andAdolescent Psychiatry, 37, 252–261.
Weisz, J. R., & Hawley, K. M. (1998). Finding, evaluating, refining,and applying empirically supported treatment for childrenand adolescents. Journal of Clinical Child Psychology, 27,206–216.
Willett, J. B., & Sayer, A. G. (1994). Using covariance structureanalysis to detect correlates and predictors of individualchange over time. Psychological Bulletin, 116, 363–381.
Williams, R. J., Chang, S. Y., and Addiction Centre AdolescentResearch Group (2000). A comprehensive and comparativereview of adolescent substance abuse treatment outcome.Clinical Psychology: Science and Practice, 7, 138–166.
Wills, T. A., & Cleary, S. D. (1999). Peer and adolescent substanceuse among 6th–9th graders: Latent growth analyses of influ-ence versus selection mechanisms. Health Psychology, 18,453–463.
Winters, K. C., & Henley, G. A. (1989). Personal Experience Inven-tory Test and Manual. Los Angeles: Western PsychologicalServices.
Winters, K., Latimer, W., & Stinchfield, R. (1999). Adolescenttreatment. In P. J. Ott, R. E. Tartar, & R. T. Ammerman

298 Ozechowski and Liddle
(Eds.), Sourcebook on substance abuse: Etiology, epidemiol-ogy, assessment, and treatment (pp. 350–361). Boston: Al-lyn & Bacon.
Wong, M. M., Zucker, R. A., Puttler, L. I., & Fitzgerald, H. E.(1999). Heterogeneity of risk aggregation for alcohol prob-lems between early and middle childhood: Nesting structureand variation. Development and Psychopathology, 11,727–744.
Yates, B. T. (1994). Toward the incorporation of costs, cost-effec-tiveness analysis, and cost–benefit analysis into clinical re-
search. Journal of Consulting and Clinical Psychology, 62,729–736.
Yates, B. T. (1997). From psychotherapy research to cost–outcomeresearch: What resources are necessary to implement whichtherapy procedures that change what processes to yield whichoutcomes? Pcychotherapy Research, 7, 345–364.
Zarkin, G. A., French, M. T., Anderson, D. W., & Bradley, C. J.(1994). A conceptual framework for the economic evaluationof substance abuse interventions. Evaluation and ProgramPlanning, 17, 409–418.


















