Family-Based Association Studies of Lipid Gene Polymorphisms in Coronary Artery Disease
4
Family-Based Association Studies of Lipid Gene Polymorphisms in Coronary Artery Disease Adrian Allen, PhD a , Christine Belton, BSc a , Chris Patterson, PhD b , Paul Horan, MD c , Paul McGlinchey, MD c , Mark Spence, MD c , Alun Evans, MD b , Damian Fogarty, MD a , and Pascal McKeown, MD a,c, * Dysfunction of lipid-metabolizing proteins is implicated in the pathogenesis of cor- onary artery disease. Single nucleotide polymorphisms in genes that encode sterol regulatory binding protein-1a, adenosine triphosphate binding cassette-A1, hepatic lipase, lipoprotein lipase, and cholesteryl ester transfer protein were assessed as potential markers of disease susceptibility in a family-based study of 1,012 patients from 386 families. Association between single nucleotide polymorphisms and coro- nary artery disease was tested by the combined transmission disequilibrium test/sib transmission disequilibrium test and pedigree disequilibrium test. After Bonferroni’s correction, the pedigree disequilibrium test demonstrated significant excess transmis- sion (p <0.0083) to affected patients of the hepatic lipase 514 T allele, which suggests that this may constitute a novel disease-susceptibility locus. © 2005 Elsevier Inc. All rights reserved. (Am J Cardiol 2005;96:52–55) Atherosclerosis is a complex, polygenic disease whose de- velopment is underpinned by the aberrant function of a plethora of factors from a variety of systems involved with cardiovascular function. These systems include the vascular endothelium, the thrombotic and antithrombotic systems, factors involved in mediation of inflammatory response, and those proteins responsible for the metabolism and transport of lipids in the blood. 1 This family-based study attempted to dissect out the genetic components of coronary artery dis- ease (CAD) by investigating the role of 6 single nucleotide polymorphisms (SNPs) in 5 genes involved in lipid metab- olism that have previously been associated with CAD or alteration of lipoprotein parameters. The position 36 de- letion SNP of sterol regulatory binding protein-1a is asso- ciated with the development of carotid plaques and with high levels of total cholesterol and low-density lipoprotein cholesterol. 2 The arginine 219 to lysine SNP in the adeno- sine triphosphate binding cassette-A1 gene has been re- ported to increase serum levels of high-density lipoprotein cholesterol and decrease the severity of CAD, 3 and the C/G SNP at position 17 of the gene promoter has also been associated with decreased incidences of CAD and athero- sclerosis. 4 The 514 C/T promoter SNP of the hepatic lipase gene has been associated with variations in high- density lipoprotein cholesterol levels 5 and decreased en- zyme activity associated with CAD. 6 The T/G SNP at po- sition 495 in intron 8 of the lipoprotein lipase gene has been associated with unfavorable lipid profiles and CAD, 7,8 and TT homozygosity has been associated with increased risk of multivessel disease. 9 The G/A SNP at position 277 of the cholesteryl ester transfer protein gene has been correlated with low-density lipoprotein levels 10 and associated with decreased high-density lipoprotein and enhanced coronary atherosclerosis in patients who have hypercholesterolemia. 11 ••• Subject recruitment and criteria used to define CAD were described by Spence et al. 12 Briefly, all subjects were Cau- casian whose parents and grandparents were born in Ireland. Each family was required to have 1 member affected with proved premature CAD (disease onset 55 years old for men and 60 years old for women) and 1 unaffected sibling and/or mother and father who were alive. The family structure and details with regard to age at CAD onset and study inclusion in affected and unaffected siblings are pre- sented in Tables 1 and 2, respectively. Affected siblings were recruited from patients who had been referred to the cardiology centers in the Royal Victoria and Belfast City Hospitals (Belfast, United Kingdom). Proved CAD was defined as the presence of 1 of the following: a history of acute myocardial infarction, a history of unstable angina (typical chest pain with dynamic elec- trocardiographic changes or minor increases in cardiac markers), or 70% luminal stenosis on coronary angiography. Unaffected siblings were required to be older than the affected sibling was at the onset of CAD, have no symptoms a Departments of Medicine and b Epidemiology and Public Health, Queen’s University Belfast, Belfast, Northern Ireland, United Kingdom; and c Regional Medical Cardiology Centre, Royal Victoria Hospital, Bel- fast, Northern Ireland, United Kingdom. Manuscript received September 9, 2004; revised manuscript received and accepted February 28, 2005. This research was supported by the Research and Development Office, Northern Ireland, a Royal Victoria Hospital Research Fellowship, the Northern Ireland Chest, Heart and Stroke Association, the Heart Trust Fund (Royal Victoria Hospital), and the Cardiac Research Fund (Royal Victoria Hospital), Belfast, Northern Ireland, United Kingdom. *Corresponding author. Tel.: 44-28-9063-4825; fax: 44-28-9031-2907. E-mail address: [email protected] (P. McKeown). 0002-9149/05/$ – see front matter © 2005 Elsevier Inc. All rights reserved. www.AJConline.org doi:10.1016/j.amjcard.2005.02.043
-
Upload
adrian-allen -
Category
Documents
-
view
212 -
download
0
Transcript of Family-Based Association Studies of Lipid Gene Polymorphisms in Coronary Artery Disease

AvpceftodepoalchcspcSa
Qaf2
NNFV
0d
Family-Based Association Studies of Lipid Gene Polymorphisms in CoronaryArtery Disease
Adrian Allen, PhDa, Christine Belton, BSca, Chris Patterson, PhDb, Paul Horan, MDc,Paul McGlinchey, MDc, Mark Spence, MDc, Alun Evans, MDb, Damian Fogarty, MDa, and
Pascal McKeown, MDa,c,*
Dysfunction of lipid-metabolizing proteins is implicated in the pathogenesis of cor-onary artery disease. Single nucleotide polymorphisms in genes that encode sterolregulatory binding protein-1a, adenosine triphosphate binding cassette-A1, hepaticlipase, lipoprotein lipase, and cholesteryl ester transfer protein were assessed aspotential markers of disease susceptibility in a family-based study of 1,012 patientsfrom 386 families. Association between single nucleotide polymorphisms and coro-nary artery disease was tested by the combined transmission disequilibrium test/sibtransmission disequilibrium test and pedigree disequilibrium test. After Bonferroni’scorrection, the pedigree disequilibrium test demonstrated significant excess transmis-sion (p <0.0083) to affected patients of the hepatic lipase �514 T allele, whichsuggests that this may constitute a novel disease-susceptibility locus. © 2005
Elsevier Inc. All rights reserved. (Am J Cardiol 2005;96:52–55)sldzsaTmcwda
SdcEpmssss
baPfotm
therosclerosis is a complex, polygenic disease whose de-elopment is underpinned by the aberrant function of alethora of factors from a variety of systems involved withardiovascular function. These systems include the vascularndothelium, the thrombotic and antithrombotic systems,actors involved in mediation of inflammatory response, andhose proteins responsible for the metabolism and transportf lipids in the blood.1 This family-based study attempted toissect out the genetic components of coronary artery dis-ase (CAD) by investigating the role of 6 single nucleotideolymorphisms (SNPs) in 5 genes involved in lipid metab-lism that have previously been associated with CAD orlteration of lipoprotein parameters. The position �36 de-etion SNP of sterol regulatory binding protein-1a is asso-iated with the development of carotid plaques and withigh levels of total cholesterol and low-density lipoproteinholesterol.2 The arginine 219 to lysine SNP in the adeno-ine triphosphate binding cassette-A1 gene has been re-orted to increase serum levels of high-density lipoproteinholesterol and decrease the severity of CAD,3 and the C/GNP at position �17 of the gene promoter has also beenssociated with decreased incidences of CAD and athero-
aDepartments of Medicine and bEpidemiology and Public Health,ueen’s University Belfast, Belfast, Northern Ireland, United Kingdom;
nd cRegional Medical Cardiology Centre, Royal Victoria Hospital, Bel-ast, Northern Ireland, United Kingdom. Manuscript received September 9,004; revised manuscript received and accepted February 28, 2005.
This research was supported by the Research and Development Office,orthern Ireland, a Royal Victoria Hospital Research Fellowship, theorthern Ireland Chest, Heart and Stroke Association, the Heart Trustund (Royal Victoria Hospital), and the Cardiac Research Fund (Royalictoria Hospital), Belfast, Northern Ireland, United Kingdom.
*Corresponding author. Tel.: 44-28-9063-4825; fax: 44-28-9031-2907.
aE-mail address: [email protected] (P. McKeown).002-9149/05/$ – see front matter © 2005 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2005.02.043
clerosis.4 The �514 C/T promoter SNP of the hepaticipase gene has been associated with variations in high-ensity lipoprotein cholesterol levels5 and decreased en-yme activity associated with CAD.6 The T/G SNP at po-ition 495 in intron 8 of the lipoprotein lipase gene has beenssociated with unfavorable lipid profiles and CAD,7,8 andT homozygosity has been associated with increased risk ofultivessel disease.9 The G/A SNP at position 277 of the
holesteryl ester transfer protein gene has been correlatedith low-density lipoprotein levels10 and associated withecreased high-density lipoprotein and enhanced coronarytherosclerosis in patients who have hypercholesterolemia.11
• • •ubject recruitment and criteria used to define CAD wereescribed by Spence et al.12 Briefly, all subjects were Cau-asian whose parents and grandparents were born in Ireland.ach family was required to have �1 member affected withroved premature CAD (disease onset �55 years old foren and �60 years old for women) and �1 unaffected
ibling and/or mother and father who were alive. The familytructure and details with regard to age at CAD onset andtudy inclusion in affected and unaffected siblings are pre-ented in Tables 1 and 2, respectively.
Affected siblings were recruited from patients who hadeen referred to the cardiology centers in the Royal Victoriand Belfast City Hospitals (Belfast, United Kingdom).roved CAD was defined as the presence of �1 of theollowing: a history of acute myocardial infarction, a historyf unstable angina (typical chest pain with dynamic elec-rocardiographic changes or minor increases in cardiacarkers), or �70% luminal stenosis on coronary angiography.Unaffected siblings were required to be older than the
ffected sibling was at the onset of CAD, have no symptoms
www.AJConline.org
oqtbtdc
mprSmsm
eawlp
piacawdcasdpcfTf
attn
TF
S
1111111
1
222222
3T
TAu
A
A
TPi
P
SAAH
L
C
s
TPi
S
S
A
A
H
L
C
53Coronary Artery Disease/Family Study of Lipid Gene Polymorphism
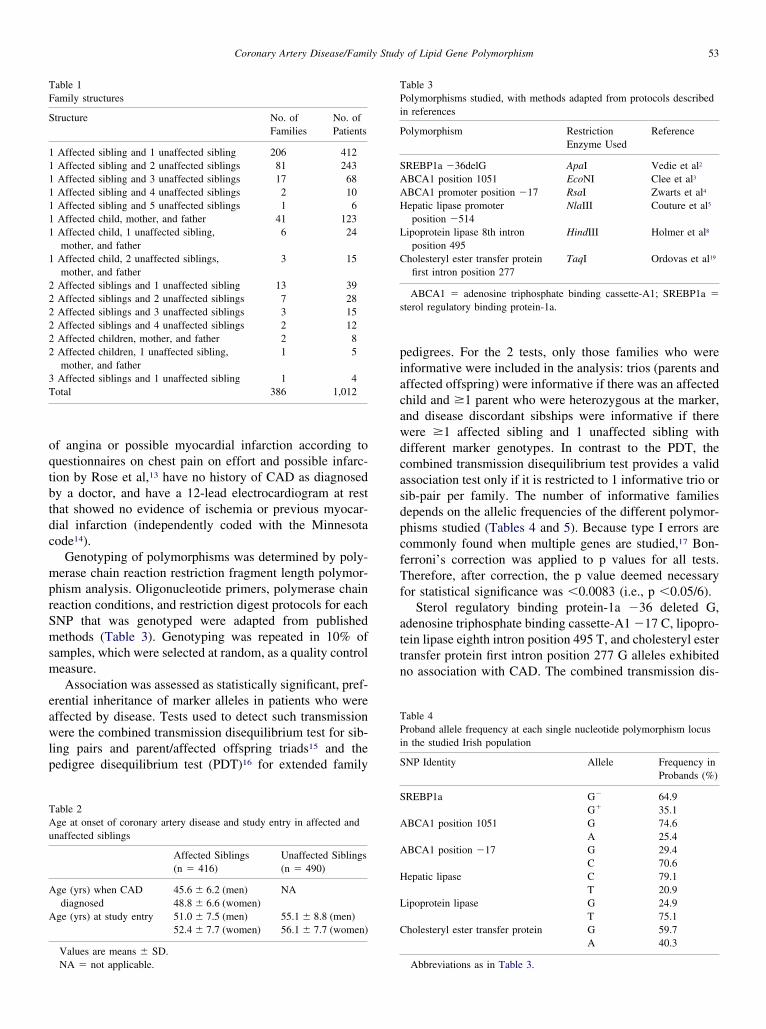
f angina or possible myocardial infarction according touestionnaires on chest pain on effort and possible infarc-ion by Rose et al,13 have no history of CAD as diagnosedy a doctor, and have a 12-lead electrocardiogram at resthat showed no evidence of ischemia or previous myocar-ial infarction (independently coded with the Minnesotaode14).
Genotyping of polymorphisms was determined by poly-erase chain reaction restriction fragment length polymor-
hism analysis. Oligonucleotide primers, polymerase chaineaction conditions, and restriction digest protocols for eachNP that was genotyped were adapted from publishedethods (Table 3). Genotyping was repeated in 10% of
amples, which were selected at random, as a quality controleasure.Association was assessed as statistically significant, pref-
rential inheritance of marker alleles in patients who wereffected by disease. Tests used to detect such transmissionere the combined transmission disequilibrium test for sib-
ing pairs and parent/affected offspring triads15 and theedigree disequilibrium test (PDT)16 for extended family
able 1amily structures
tructure No. ofFamilies
No. ofPatients
Affected sibling and 1 unaffected sibling 206 412Affected sibling and 2 unaffected siblings 81 243Affected sibling and 3 unaffected siblings 17 68Affected sibling and 4 unaffected siblings 2 10Affected sibling and 5 unaffected siblings 1 6Affected child, mother, and father 41 123Affected child, 1 unaffected sibling,mother, and father
6 24
Affected child, 2 unaffected siblings,mother, and father
3 15
Affected siblings and 1 unaffected sibling 13 39Affected siblings and 2 unaffected siblings 7 28Affected siblings and 3 unaffected siblings 3 15Affected siblings and 4 unaffected siblings 2 12Affected children, mother, and father 2 8Affected children, 1 unaffected sibling,mother, and father
1 5
Affected siblings and 1 unaffected sibling 1 4otal 386 1,012
able 2ge at onset of coronary artery disease and study entry in affected andnaffected siblings
Affected Siblings(n � 416)
Unaffected Siblings(n � 490)
ge (yrs) when CADdiagnosed
45.6 � 6.2 (men) NA48.8 � 6.6 (women)
ge (yrs) at study entry 51.0 � 7.5 (men) 55.1 � 8.8 (men)52.4 � 7.7 (women) 56.1 � 7.7 (women)
Values are means � SD.
NA � not applicable.edigrees. For the 2 tests, only those families who werenformative were included in the analysis: trios (parents andffected offspring) were informative if there was an affectedhild and �1 parent who were heterozygous at the marker,nd disease discordant sibships were informative if thereere �1 affected sibling and 1 unaffected sibling withifferent marker genotypes. In contrast to the PDT, theombined transmission disequilibrium test provides a validssociation test only if it is restricted to 1 informative trio orib-pair per family. The number of informative familiesepends on the allelic frequencies of the different polymor-hisms studied (Tables 4 and 5). Because type I errors areommonly found when multiple genes are studied,17 Bon-erroni’s correction was applied to p values for all tests.herefore, after correction, the p value deemed necessary
or statistical significance was �0.0083 (i.e., p �0.05/6).Sterol regulatory binding protein-1a �36 deleted G,
denosine triphosphate binding cassette-A1 �17 C, lipopro-ein lipase eighth intron position 495 T, and cholesteryl esterransfer protein first intron position 277 G alleles exhibitedo association with CAD. The combined transmission dis-
able 3olymorphisms studied, with methods adapted from protocols described
n references
olymorphism RestrictionEnzyme Used
Reference
REBP1a �36delG ApaI Vedie et al2
BCA1 position 1051 EcoNI Clee et al3
BCA1 promoter position �17 RsaI Zwarts et al4
epatic lipase promoterposition �514
NlaIII Couture et al5
ipoprotein lipase 8th intronposition 495
HindIII Holmer et al8
holesteryl ester transfer proteinfirst intron position 277
TaqI Ordovas et al19
ABCA1 � adenosine triphosphate binding cassette-A1; SREBP1a �terol regulatory binding protein-1a.
able 4roband allele frequency at each single nucleotide polymorphism locus
n the studied Irish population
NP Identity Allele Frequency inProbands (%)
REBP1a G� 64.9G� 35.1
BCA1 position 1051 G 74.6A 25.4
BCA1 position �17 G 29.4C 70.6
epatic lipase C 79.1T 20.9
ipoprotein lipase G 24.9T 75.1
holesteryl ester transfer protein G 59.7A 40.3
Abbreviations as in Table 3.

est
at1t�eha
idfT(Bpaeg
Ifutlchiatttit
stdwctabn
Tc
P
SAAHLC
isequil
54 The American Journal of Cardiology (www.AJConline.org)
quilibrium test and PDT analyses showed that there was notatistically significant excess transmission of these alleleso affected patients (Table 5).
The combined transmission disequilibrium test and PDTnalyses provided some indication of excess transmission ofhe adenosine triphosphate binding cassette-A1 position051 A allele (p � 0.038 and p � 0.046, respectively) andhe hepatic lipase position �514 T allele (p � 0.025 and p
0.004, respectively) to affected patients (Table 5). How-ver, after Bonferroni’s correction, only the PDT analysis ofepatic lipase �514 T showed a statistically significantllele transmission to affected offspring (Table 5).
A retrospective assessment of power was performed us-ng the method described for the combined transmissionisequilibrium test by Spielman and Ewens,15 in whichamilies that had minimal configuration were considered.he number of informative families varied from 140 to 188
Table 5). With 140 families of minimal configuration,onferroni’s corrected test (2-tailed) will have �80%ower to detect a deviation from 50% to 65% in the rate ofllele transmission to affected patients. The PDT would bexpected to have superior power by virtue of its use ofenotype information from more family members.16
• • •
n this study we found evidence of linkage and associationor the hepatic lipase position �514 T allele and CAD whensing the family-based PDT in a well-defined Irish popula-ion. Dugi et al6 reported that this SNP decreases hepaticipase activity and thus increases susceptibility to CAD. Inontrast, the T allele has been associated with high levels ofigh-density lipoprotein cholesterol.5 However, these stud-es have lacked the support of genetic and epidemiologicssociation studies such as this study. Our data suggest thathis locus is a potential disease susceptibility marker owingo its statistically significant, preferential inheritance inhose who develop CAD. However, replication of this resultn different populations will be necessary before confirming
able 5TDT and PDT analyses for transmission of disease-linked alleles from c
olymorphism (allele) cTDTPropAllel
Obse
REBP1a (G�) 158BCA1 position 1051 (A) 217BCA1 position �17 (C) 200epatic lipase position �514 (T) 185ipoprotein lipase 8th intron position 495 (T) 209holesteryl ester transfer protein 1st intron position 277 (G) 187
* p �0.05 2-tailed; † p �0.0083 (� 0.05/6) after Bonferroni’s correctiocTDT � combined transmission disequilibrium test; PDT � pedigree d
he validity of this hypothesis.
The tendency toward excess transmission of the adeno-ine triphosphate binding cassette-A1 position 1051 A alleleo affected patients (p � 0.038 by combined transmissionisequilibrium test and p � 0.046 by PDT) is at varianceith previous findings where it has been linked to a largely
ardioprotective effect.18 This disparity may be attributed tohe occurrence of a type I error, a common problem inssociation studies where multiple comparisons are made,17
ecause Bonferroni’s correction renders this finding nonsig-ificant.
1. Lusis AJ. Atherosclerosis. Nature 2000;407:233–241.2. Vedie B, Jeunemaitre X, Megnien JL, Atger V, Simon A, Moatti NA.
New DNA polymorphism in the 5= untranslated region of the humanSREBP-1a is related to development of atherosclerosis in high cardio-vascular risk population. Atherosclerosis 2001;154:589–597.
3. Clee SM, Zwinderman AH, Engert JC, Zwarts KY, Molhuizen HO,Roomp K, Jukema JW, van Wijland M, van Dam M, Hudson TJ, et al.Common genetic variation in ABCA1 is associated with altered li-poprotein levels and a modified risk for coronary artery disease.Circulation 2001;103:1198–1205.
4. Zwarts KY, Clee SM, Zwinderman AH, Engert JC, Singaraja R,Loubser O, James E, Roomp K, Hudson TJ, Jukema JW, et al. ABCA.1 regulatory variants influence coronary artery disease independent ofeffects on plasma lipid levels. Clin Genet 2002;61:115–125.
5. Couture P, Otvos JD, Cupples LA, Lahoz C, Wilson PW, Schaefer EJ,Ordovas JM. Association of the C-514T polymorphism in the hepaticlipase gene with variations in lipoprotein subclass profiles: the Fra-mingham Offspring Study. Arterioscler Thromb Vasc Biol 2000;20:815–822.
6. Dugi KA, Brandauer K, Schmidt N, Nau B, Schneider JG, Mentz S,Keiper T, Schaefer JR, Meissner C, Kather H, et al. Low hepatic lipaseactivity is a novel risk factor for coronary artery disease. Circulation2001;104:3057–3062.
7. Funke H, Klug J, Assman G. HindIII RFLP in the lipoprotein lipasegene, (LPL). Nucleic Acids Res 1987;15:9102.
8. Holmer SR, Hengstenberg C, Mayer B, Doring A, Lowel H, Engel S,Hense HW, Wolf M, Klein G, Riegger G, Schunkert H. Lipoproteinlipase gene polymorphism, cholesterol subfractions and myocardialinfarction in large samples of the general population. Cardiovasc Res2000;47:806–812.
9. Gambino R, Scaglione L, Alemanno N, Pagano G, Cassader M. Hu-man lipoprotein lipase HindIII polymorphism in young patients with
e genes
mission ofsease-linkedfected Patients
p Value(Z test result)
No. of InformativeFamilies
Expected cTDT PDT
150.7 0.380 0.238 180201.5 0.038* 0.046* 174200.5 0.947 0.552 179170.0 0.025* 0.004† 140198.3 0.169 0.068 171186.0 0.948 0.762 188
ibrium test. Other abbreviations as in Table 3.
andidat
Transosed Die to Af
rved
n.
myocardial infarction. Metabolism 1999;48:1157–1161.

1
1
1
1
1
1
1
1
1
1
55Coronary Artery Disease/Family Study of Lipid Gene Polymorphism
0. Goto A, Sasai K, Suzuki S, Fukutomi T, Ito S, Matsushita T, OkamotoM, Suzuki T, Itoh M, Okumura-Noji K, Yokoyama S. Cholesterylester transfer protein and atherosclerosis in Japanese subjects: a studybased on coronary angiography. Atherosclerosis 2001;159:153–163.
1. Kuivenhoven JA, Jukema JW, Zwinderman AH, de Knijff P, McPher-son R, Bruschke AV, Lie KI, Kastelein JJ. The role of a commonvariant of the cholesteryl ester transfer protein gene in the progressionof coronary atherosclerosis. The Regression Growth Evaluation StatinStudy Group. N Engl J Med 1998;338:86–93.
2. Spence MS, McGlinchey PG, Patterson CC, Belton C, Murphy G,McMaster D, Fogarty DG, Evans AE, McKeown PP. Family-basedinvestigation of the C677T polymorphism of the methylenetetrahydro-folate reductase gene in ischemic heart disease. Atherosclerosis 2002;165:293–299.
3. Rose GA, Blackburn H, Gillum RF, Prineas RJ. Cardiovascular SurveyMethods, 2nd Ed. Geneva: World Health Organisation, 1982.
4. Blackburn H, Keys A, Simonson E, Rautaharju P, Punsar S. Theelectrocardiogram in population studies: a classification system. Cir-
culation 1960;21:1160–1175.5. Spielman RS, Ewens WJ. A sibship test for linkage in the presence ofassociation: the Sib Transmission/Disequilibrium Test. Am J HumGenet 1998;62:450–458.
6. Martin ER, Monks SA, Warren LL, Kaplan NLA. Test for linkage andassociation in general pedigrees: the Pedigree Disequilibrium Test.Am J Hum Genet 2000;67:146–154.
7. Romero R, Kuivaniemi H, Tromp G, Olson J. The design, executionand interpretation of genetic association studies to decipher complexdisease. Am J Obstet Gynecol 2002;187:1299–1312.
8. Cenarro A, Artieda M, Castillo S, Mozas P, Reyes G, Tejedor D,Alonso R, Mata P, Pocovi M, Civeira F. Spanish FH group. A commonvariant in the ABCA1 gene is associated with a lower risk for prema-ture coronary heart disease in familial hypercholesterolaemia. J MedGenet 2003;40:163–168.
9. Ordovas JM, Cupples LA, Corella D, Otvos JD, Osgood D, MartinezA, Lahoz C, Coltell O, Wilson PW, Schaefer EJ. Association ofcholesteryl ester transfer protein-TaqIB polymorphism with variationsin lipoprotein subclasses and coronary heart disease risk—the Fra-
mingham Study. Arterioscler Thromb Vasc Biol 2000;20:1323–1329.