Falls Safety Awareness
35
Falls Safety Awareness Please complete the above, in the blocks provided, as clearly as possible. Completing the details in full will ensure that your certificate bears the correct spelling and date. e date should be the day you finish & must be written in the DD/MM/YYYY format. Copyright Notice is booklet remains the intellectual property of Redcrier Publications L td e material featured in this document is subject to Redcrier Publications L td copyright protection unless otherwise indicated; any breach of this may result in legal action.Any other proposed use of Redcrier Publications L td material will be subject to a copyright licence available from Redcrier Publications L td .e information enclosed is not to be used, leased or lent to any one intending to use its contents for training purposes, neither is it to be stored on any retrieval systems for use at a later date. V10.0118.04 © Redcrier Publications Limited 2018 First name: Surname: Company: Date:
Transcript of Falls Safety Awareness

Falls Safety Awareness
Please complete the above, in the blocks provided, as clearly as possible.Completing the details in full will ensure that your certificate bears the correct spelling and date.
The date should be the day you finish & must be written in the DD/MM/YYYY format.
Copyright Notice This booklet remains the intellectual property of Redcrier Publications Ltd
The material featured in this document is subject to Redcrier Publications Ltd copyright protection unless otherwise indicated; any breach of this may result in legal action.Any other proposed use of Redcrier Publications Ltd material will be subject to a copyright licence available from Redcrier Publications Ltd.The information enclosed is not to be used, leased or lent to any one intending to use its contents for training purposes, neither is it to be stored on any retrieval systems for use at a later date.
V10.0118.04 © Redcrier Publications Limited 2018
First name:
Surname:
Company:
Date:

Falls Safety Awareness
2
Contents
Index. Page 2Learning outcomes. Page 3Fundamental standards. Pages 3 - 4Introduction. Page 5Unit One. Pages 6 - 8Identifying falls.Unit One Questions. Page 9Unit Two. Pages 10 - 17Causes and risk factors of falls.Unit Two Questions. Page 18Unit Three. Pages 19 - 23Care planning, reporting and assessment.Unit Three Questions. Page 24Unit Four. Pages 25 - 30Actions to reduce falls.Unit Four Questions. Page 31Unit Five. Pages 32 - 34Safety when dealing with a falling client.Unit Five Questions. Page 35
N.B: We are aware that official practice is to use the terms “service users” or “people using this service” to describe those receiving care. We prefer the term “client” and use it throughout our training package.
Key:
worksheet important
example

3
Falls Safety Awareness
Learning outcomes.
• Identify the main causes of falls.• Have knowledge of the impact of falls on clients.• Identify actions to reduce falls.• Understand the need for reporting and care planning.• Be able to ensure safety around a falling client.
Fundamental standards.
The fundamental standards are the standards by which CQC will inspect social care. The standards are based on the regulations from the Care Act 2014 and CQC have changed the focus for the purposes of inspection.
The fundamental standards are those standards that no care setting must fall below.
The standards are based on five areas as follows:Safe. People are protected from abuse and avoidable harm.
Effective. People’s care, treatment and support show quality of life and promote good outcomes, and providers should show evidence to prove it.
Caring. Care should be person centred involving dignity and respect, and compassion.
Responsive. Following correct working procedures as agreed by your workplace and as set out in the client’s care plan.
Well led. Management leadership and governance should ensure all of the above happens. Staff training should be recognised and openness and fairness be apparent.
These areas are known as key lines of enquiry or KLOES. Each KLOE has a set of criteria which CQC use to check whether the fundamental standards are being met.

Falls Safety Awareness
4
The fundamental standards are as follows:
Person centred care. Ensuring that those receiving the care are at the centre of all decisions.
Dignity and respect. Providing the client with dignity and respect in all aspects of their care.
Need for consent. Asking the client’s permission before carrying out tasks that affect them.
Safe care and treatment.
Following correct working procedures as agreed by your workplace and the client’s care plan.
Safeguarding service users from abuse.
Following agreed working and safeguarding procedures and being aware of signs and symptoms.
Meeting nutritional needs.
Being aware of dietary needs, working with the care plan, ensuring clients have the right equipment and conditions to eat.
Cleanliness, safety and suitability of premises and equipment.
Carrying out required checks of premises and equipment, implementing cleaning rotas and carrying out safety checks.
Receiving and acting on complaints.
Having a complaints policy and procedure in place that is accessible to all and act in accordance with the policy when dealing with complaints.
Good governance. Ensuring that all aspects of the workplace is overseen and policies and procedures are implemented and monitored regularly.
Staffing. Fit and proper persons employed.Fit and proper person requirement for Directors is followed.
Duty of candour. Relevant information must be volunteered to all persons who have or may have been harmed by the provision of services, whether or not the information has been requested and whether or not a complaint or a report about that provision has been made.
Our Redcrier manuals will provide your staff with training to support attainment of the fundamental standards.

5
Falls Safety Awareness
Introduction
Most of our daily life depends on the ability to move about freely as and when we want. Being mobile is of fundamental importance in maintaining independence.
It allows us to:
• Interact with our environment and carry out everyday activities such as washing, dressing, cooking, cleaning and shopping.
• Maintain social contact with friends and family. • Preserve our privacy.• Maintain dignity, self esteem and a feeling of self worth.
A fall can have a lasting impact on the life of a person. Not only are there the possible physical effects of a fall but also a loss of confidence. This in turn may lead to a restriction in activities and social isolation, which may further affect health and the quality of life.
Professor, and Nurse, Janice M. Morse, PhD (Nurs), PhD (Anthro), FAAN (Morse) has written widely in the areas of suffering and comforting, preventing patient falls (she is the author of the Morse Fall Scale, used internationally to triage the fall-prone patient), and developing qualitative methods. In 1997 she writes that: historically falls were considered an `accident’; an unavoidable problem of illness, disability, or just old age. We now know that although some falls will be unavoidable, in many cases we can put in place strategies and appropriate measures to help prevent them.
Preventing falls requires a planned and co-ordinated approach and may involve a team consisting of a number of professionals e.g. care staff, health services etc as well as relatives and the client themselves. All care home staff have a role to play in falls prevention, they need to have the necessary skills and knowledge and need to know the importance of their role within this team.
The aim of this manual is: to raise awareness of falls, identify the role carers play in helping to prevent falls and give them the knowledge to maintain safety when dealing with falls.

Falls Safety Awareness
6
Unit One
Identifying falls.
We are all potentially at risk of falling. Although it is not inevitable that we will have a fall as we get older, the likelihood of it happening will increase and the result may be more serious. Our bones will be more brittle and therefore broken or fractured bones are more likely.
According to Age UK.
Falls represent the most frequent and serious type of accident in people aged 65 and over.
Falls are the main cause of disability and the leading cause of death from injury among people aged over 75 in the UK.
Policies and guidelines on fall prevention.
In recent years several important government policies on the prevention and management of falls were produced in an attempt to address this problem.
In 2001 the Department of Health (DoH) introduced The National Service Framework for Older People (NSFOP). A key target set in Standard 6 of this framework was aimed at reducing the number of falls by highlighting the importance of falls prevention.
In 2004 The National Institute for Clinical Excellence (NICE) introduced a document called Falls: The assessment and prevention of falls in older people. In this recommendations for good practice based on the best available evidence of clinical and cost effectiveness in falls prevention are presented.
In June 2014 the Care Act became law and put safeguarding on a legal footing. The Care Act sets out the framework for future provision, including falls prevention, that local authorities must adhere to.
RIDDOR.
Reporting of Injuries, Diseases and Dangerous Occurrences Regulations.
Falls involving clients are reportable under RIDDOR if the client is taken to hospital from the workplace and the injury resulted from an action identified in the care plan, not being implemented correctly or if it occurred whilst the client was being hoisted. Where you are unsure if an incident.

7
Falls Safety Awareness
should be reported, ask for advice. Information can be found in the HSE RIDDOR Information sheet
Definitions and types of falls
Falls can happen for a number of reasons, but first let us define what we mean by a fall.
NICE (2004) defines a fall as:
An event whereby an individual comes to rest on the ground or another lower level, with or without loss of consciousness.
Although we are concentrating on falls, it is important that we don’t ignore near falls.
Near fall.
A near fall is usually defined as a sudden loss of balance which does not result in a fall or injury. It can include a person who slips, stumbles or trips but is able to regain control before falling. It is just as important that we record a near fall, as it identifies that the person may be at risk of falling and will help us to plan accordingly.
If we can identify the type of fall, this again will help us with our planning. Morse (1997) identifies three types of falls: Accidental, predicted and unpredicted and although most falls will probably be witnessed, there may be some that are not so it is important that accurate recording of all falls is undertaken to aid our care planning.
Accidental falls.
These are falls that are considered accidental and can be caused by the person slipping or tripping. This type of fall is often due to environmental factors for example spilled water on the floor, or a loose rug.
Predicted fall.
A fall that occurs where the individual has previously been identified as `at risk of falling’. Examples of this type of fall include: The individual may have poor mobility, be on several medications or have fallen before.
Unpredicted fall.
A fall that may be caused by sudden or unexpected conditions which could not be predicted or prevented. Examples of this type of fall could be having no previous history of falls, an unexpected seizure, a drop in blood pressure fainting, or dizziness.
Falls Safety Awareness
8
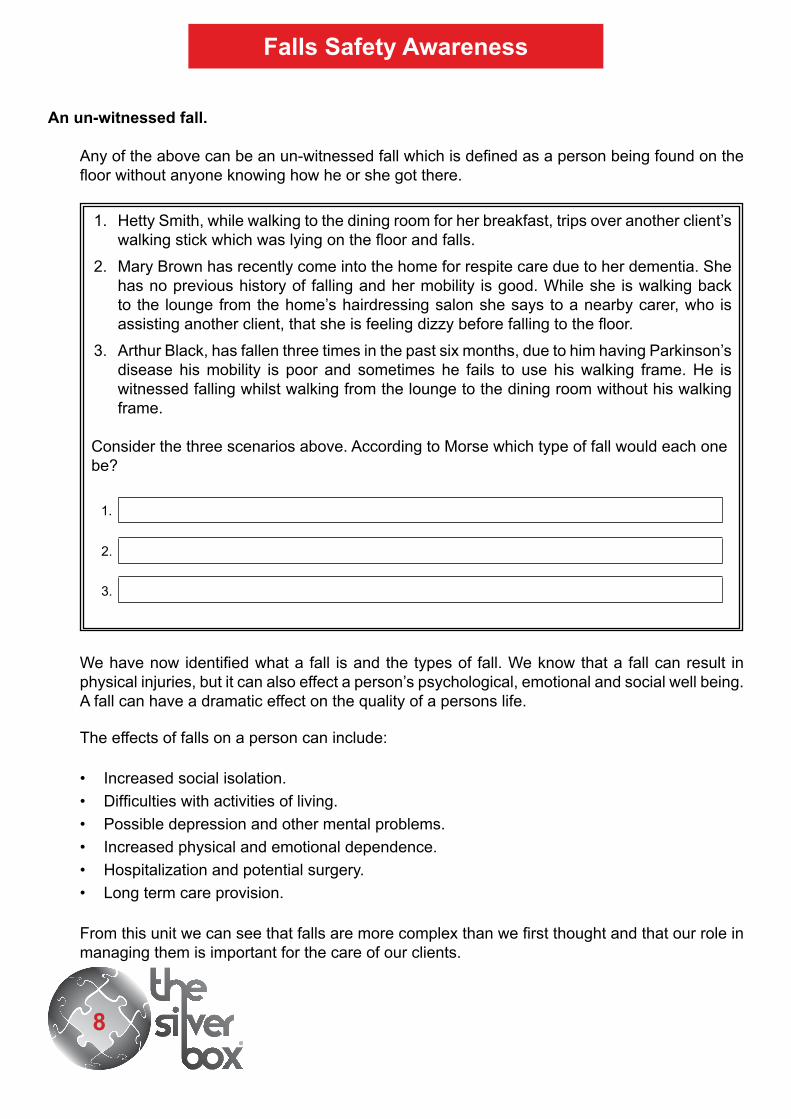
An un-witnessed fall.
Any of the above can be an un-witnessed fall which is defined as a person being found on the floor without anyone knowing how he or she got there.
1. Hetty Smith, while walking to the dining room for her breakfast, trips over another client’s walking stick which was lying on the floor and falls.
2. Mary Brown has recently come into the home for respite care due to her dementia. She has no previous history of falling and her mobility is good. While she is walking back to the lounge from the home’s hairdressing salon she says to a nearby carer, who is assisting another client, that she is feeling dizzy before falling to the floor.
3. Arthur Black, has fallen three times in the past six months, due to him having Parkinson’s disease his mobility is poor and sometimes he fails to use his walking frame. He is witnessed falling whilst walking from the lounge to the dining room without his walking frame.
Consider the three scenarios above. According to Morse which type of fall would each one be?
1.
2.
3.
We have now identified what a fall is and the types of fall. We know that a fall can result in physical injuries, but it can also effect a person’s psychological, emotional and social well being. A fall can have a dramatic effect on the quality of a persons life.
The effects of falls on a person can include:
• Increased social isolation.• Difficulties with activities of living.• Possible depression and other mental problems.• Increased physical and emotional dependence.• Hospitalization and potential surgery.• Long term care provision.
From this unit we can see that falls are more complex than we first thought and that our role in managing them is important for the care of our clients.

9
Falls Safety Awareness
Unit One Questions
What is the definition of a fall as defined by NICE?3.
Name two daily activities that being mobile allows us to do.1.
2.
1.
What are two possible effects on the person who has a fall?2.
2.
1.
What is an unpredicted fall?4.
What is a predicted fall?5.

Falls Safety Awareness
10
Unit Two
Causes and risk factors of falls.
We have identified that falls are a serious concern for clients, their families and health professionals. Often, more than one risk factor is involved. As the number of risk factors increase, so does the risk of falling and despite precautions being put in place many falls cannot be prevented. However with an assessment and prompt intervention, reducing the number and severity of potential injuries is possible.
Falls normally result from an interaction between two main types of risk factor, these are known as person specific risk factors and environmental risk factors.
Person specific are risk factors which relate to the specific individual and can include the following:
1. Problems with postural balance, mobility and walking (gait).• Lack of strength of muscles needed for walking.• Lack of exercise.• Neurological condition, such as a stroke.• Chronic illness such as multiple sclerosis.• Fainting, blackouts or loss of consciousness.• A hearing problem called tinnitus commonly known as `ringing in the ears’.• An injury caused by a previous fall.• Poorly fitting footwear and foot problems e.g. bunions, ingrowing toenails.• Injury or infection in the inner ear.• Loose clothing or bandages.• Ill fitting or badly adjusted mobility aids / assistive devices.• The inner ear is responsible for maintaining balance and any injury, blockage or infection
can cause balance problems.
2. Visual and hearing impairments.• Unable to judge distances properly.• Unable to manage steps.• Different levels on floors.

11
Falls Safety Awareness
• Difficulty moving between darkness and light.• Wearing bifocal glasses when walking.• Cataracts, glaucoma.• Unable to hear commands.
3. Hypotension (low blood pressure).• If a person’s blood pressure drops when they get up from a lying down or sitting position
they may be prone to falls. It can result from dehydration, poor nutrition, or conditions such as diabetes or certain medications.
4. Nutrition and hydration.• Poor nourishment can cause light headedness and confusion.• Poor hydration can cause dizziness, poor sleep patterns, poor balance.• A lack of calcium increases the risk of a fracture if a person has a fall.
5. Alcohol.• Consumption of alcohol can cause confusion, unsteadiness.
6. Medication.• Can have an effect where 4 or more medications a day are prescribed.
7. Confusion.• When a client is confused, even for a short time, it can sometimes lead to falls. Short term
confusion could be caused by being in an unfamiliar environment such as in the case of being a new client coming into a care home.
8. Urinary incontinence / constipation.• Older persons can be prone to urinary and bowel disorders. This can cause the person
to attempt to get to the toilet in a hurry without either calling for assistance or having the support of a care worker. Urinary infections can also cause confusion.
9. Medical conditions.• Chronic - stroke, arthritis, osteoporosis, depression, diabetes and neurological conditions
such as Parkinson’s disease. • Acute - chest infections and urinary tract infections.

Falls Safety Awareness
12
10. Dementia and cognitive impairment.
People with dementia are at greater risk of falling. This can be due to impaired judgment, memory loss, confusion and restlessness.
• Dementia can also affect the visual perception and the ability to recognise, understand and avoid potential hazards. Alterations in visual depth perception can make judging distances to and between objects, stairs and doorways very difficult. Alterations in a waking pattern due to the dementia can also increase the risk of falls.
Bill Hunt 78 years old, is a client in a care home. He has fallen twice in the past three months. He suffers from glaucoma in both eyes. He is currently on more than four medications a day including regular pain killers as he has arthritis.
Due to an enlarged prostate, Bill has a urinary catheter in place and he can experience constipation. Bill has been found playing with his catheter tubing, and his catheter bag is frequently found dragging on the floor while he’s walking.
Bill does not drink much fluid throughout the day, and eats only a small amount. His mobility and balance is generally poor but he is determined to walk with a walking frame. He will often get up from his chair without asking for assistance.
From this scenario identify 3 person specific risk factors.
1.
2.
3.
Environmental risk factors – areas within the environment that can present risks.
• Lighting poor or dim lighting especially on the stairs or corridors. Intensity and glare of very bright light is a risk. Shadows should also be avoided.
• Furniture, unstable items or improper use of devices such as bedside rails. • Stairs which are steep and / or have worn carpets.

13
Falls Safety Awareness
Flooring can cause falls where there are changes in floor surfaces either in texture or levels, loose or thick pile carpeting, movable rugs and highly polished floors or wet surfaces.
Toilet and bathroom areas without appropriate support such as grab rails. Chairs, toilets or beds being too high, low or unstable.
Temperature; a cold environment will be more likely to reduce the mobility of an individual.
New environments such as admission or relocation into a care environment could mean that the person is disorientated and confused.
Low staffing levels or lack of appropriately trained and experienced staff.
Wheelchairs inadequately maintained, loose sides or brakes not locking correctly.
Obstructions and objects lying on the floor; trailing wires, laundry, spilt liquids.
Pets. Small cats or dogs can easily get under the feet of an individual.
Jean Smith, 68 years old, lives in sheltered accommodation for people with a learning disability. Although she has mobility she finds walking for long distances difficult. She wears bifocal glasses. She has a walking stick which she uses sometimes. She has a dog who likes to sleep on the floor next to her feet.
Jean likes to read and has books and magazines scattered on the floor. She admits that she is not very physically active and does little exercise. Jean’s laundry is also strewn on the floors in the bedroom and bathroom. She has movable rugs in the bedroom and hall.
Jean has never had a fall before.
From this scenario identify 2 environmental risk factors.
1.
2.

Falls Safety Awareness
14
Physical effects.
When we think of falls we usually think of physical injury, broken or fractured bones, dislocation, bruising, cuts and grazes etc. Other physical injuries caused by falls include soft tissue damage, head injuries, skin wounds and skin tears.
Osteoporosis.
As we age, our bone strength and density reduces and therefore bones become more fragile. This may be increased by a condition called Osteoporosis which affects the skeleton. Although this condition does not cause a person to fall, if they do they are more likely to break a bone.
The bones that make up our skeleton are made of a thick outer shell and a strong inner honeycomb mesh, also made of bone. When Osteoporosis occurs, the inner bone structure becomes thin and more fragile or prone to break, even after a minor fall. The wrist, hip and spine are most commonly affected although it can affect any area of the body. Bone is alive and is constantly changing throughout our life. Having Osteoporosis does not mean your bones will break, just that they are more likely to. Bones that break because of Osteoporosis will still heal in the same time scale as bones not affected, which is usually 6-8 weeks.
Emotional social and psychological effects.
The consequence of a fall isn’t just physical injury it can affect a person in other ways, such as making them anxious about walking or frightened of falling again, This could cause them to withdraw from social activity and eventually lead to the development of low morale and low esteem.
These emotional effects of a fall can be contributory factors leading to depression and a low feeling of self worth.
The potential for further physical injury and resultant reduction in mobility can have a negative impact on the social element of a person’s life. People may be reluctant to visit family and friends, or to continue with hobbies or other pleasure activities because of the risk of falling.
For some people falls can induce a sudden state of confusion, this confused state can be compounded in the person who has pre existing dementia. For example the person may be frightened of falling again and refuse to stand or walk. Because of cognitive impairment they would not be able to communicate their anxieties and therefore instead exhibit their apprehension and alarm by becoming agitated or demonstrating challenging behaviour.
As you can see from all of the above a fall can result in emotional trauma and distress, resulting in loss of autonomy and involvement in the decision making process affecting their life. The result of all of this is known as post fall syndrome and it can affect an individual’s life dramatically.

15
Falls Safety Awareness
Post fall syndrome.
Post fall syndrome can be defined as a loss of confidence, leading to anxiety and in many cases has more of an impact than any injuries the client may receive. It can affect all aspects of the client’s life and indeed change their outlook on life. It is important that help is sought and measures put in place to limit these effects. Communication is important to try to understand the client’s fears and help them to overcome them and to deal with some of their emotions. Rebuilding their confidence will take time and patience. Telling them not to worry or not to be frightened is not helpful, but giving them opportunities to face their fears and anxieties through small tasks, social opportunities, simple exercises etc., and giving lots of encouragement and reassurance should start them on the path to regaining their confidence.
AnxietyDepression
Fear of fallingAnger / frustrationLoss of confidence
Stigma of having a fallFeeling of dependencyFeeling of usefulness
Loss of personal controlEmotional shock and distress
Social isolation and withdrawalPost fall syndrome
Falls Safety Awareness
16
Consequences of falls on care staff and the care organisation.
All care workers owe a ̀ duty of care’ in ensuring the clients health and safety. Having a client fall can affect care workers deeply. Care workers often regard it as being their fault that the client fell and question their care and practice. They may also experience feelings of guilt or distress, particularly if the fall resulted in a person being injured.
Care workers should be given opportunity to express these feelings so they can be recognised and discussed to prevent stress and negative feelings. Where appropriate, further training or changes to practice must be addressed.
For all care organisations, the clear objective must always be to provide high quality care for all its clients. However underlying this fundamental purpose is the need to maintain a reputable and trusted service. To further this, the management of falls must be addressed competently and correctly to the satisfaction of the clients, families and regulatory bodies such as the Care Quality Commission. Although the prevention of falls is the duty of every care worker, the overall process of assessment, monitoring and reduction of falls remains the responsibility of the organisation’s manager in order to comply with the Fundamental Standards.
All matters relating to the fall must be documented clearly by all concerned, records and other documentation must be kept up to date and appropriate measures put in place to reduce the risk of further falls.
Where other client’s have witnessed the fall, it is important to recognise this and the effect it may have on them.
Under each heading identify 3 effects of a fall.
Social. Emotional. Psychological.

17
Falls Safety Awareness
• They may be concerned about whether the person was hurt.• They may worry about having a fall themselves.• They may suffer symptoms of shock from what they have witnessed.
It is important to remain calm and give reassurance. Treat for shock if applicable, see the Basic Emergency Aid course for more detail. Talk to them about their concerns and fears, recognising they are very real to them, such as you or I having a fear of heights or lifts. Maintain regular checks on them to see they are alright and alert your colleagues, so they can keep an eye on them too.

Falls Safety Awareness
18
Give an example of how care staff may be affected by a client falling.3.
Unit Two Questions
Give two reasons why people with dementia are at risk of falling.4.
2.
1.
What are the two main types of risk factor that could cause a fall?1.
2.
1.
Give three examples of symptoms of post fall syndrome.5.
2.
1.
3.
Give two examples of how a client witnessing another client falling may be affected.2.
2.
1.

19
Falls Safety Awareness
Unit Three
Care planning, reporting and assessment.
Record keeping.
Accurate record keeping and documentation is important in all aspects of care. All accidents, including falls suffered by clients should be recorded in the approved accident book. Details of the fall and any actions should be made as entries in the persons care plan.
A care plan is a working document which identifies how we are going to meet the needs of an individual client. Each of your clients will have one, which will need to be updated to continue reviewing and identifying the changing needs of that individual. Each care plan will be different to reflect the care required for that person. See Redcrier’s Record Keeping manual for more detail.
Although each completed care plan will look different, the format will be similar. It should contain:
Basic information.
on the individual, age, height, weight etc.
Needs.
Including: mobility, continence, washing and dressing, social activities, communication, health / medication. Each of these areas will identify support needed, risk assessments carried out, any special requirements, equipment if required, identified along with techniques used.
Falls risk assessment.
Including: previous falls history, medications, medical conditions, visual or hearing impairments, mobility etc.
Where applicable it may also contain:
Outside services.
Required e.g. physiotherapist, chiropodist etc.
We should record as much information as possible to ensure that anyone reading the care plan can understand and meet the needs of that person. The care plan will need to be available to anyone providing care for them. All of the information in the plan should be looked at as a

Falls Safety Awareness
20
whole, so for instance if you are looking at assisting the client to move you would need to be aware of their risk of falling or if the client has been identified as at risk of falling this may impact on their independence in other areas, so risk assessments may need to be adapted to take account of it.
Every new client coming into your workplace should have a falls risk assessment carried out. Even an individual who has had no previous falls and has good mobility can become less confident when placed in a new environment.
Reporting falls.
As we have said reporting and recording falls is important as it can identify a person as being at risk of falling. However if we just record that they had a fall, it does not tell us very much. We need to look at the circumstances surrounding the fall and record as much detail as possible. When making records such as reports, it is important that we only record facts, so if we are not sure how the fall occurred, because we did not see it, we should only record what we see when we arrive on the scene and / or what we know e.g. medication they are on.
The post fall incident report should include the following information:
• Name, date of birth, date of fall, time of fall, was it witnessed.• Fall location, type of surface, was it wet, slippery etc. was their sufficient lighting (if applicable).• Mobility, were they using aids and if so were they using them correctly.• Type of fall – slip, trip, loss of balance, faint or collapse etc.• A description of the fall.
This should include how they fell, backwards, forwards etc. any warning prior to falling, footwear, glasses needed and were they wearing them, did the client know they were going to fall, had they taken any medication prior to fall, did they need first aid or medical attention, any injuries, were they seen by a doctor and was it reportable under RIDDOR.
If there were witnesses to the fall this should be recorded with their name/s contact details (if applicable) and a signature. The report should then be dated and signed. If there are no witnesses and the person who has fallen has provided information on what happened it may be appropriate for them to sign the report as well.
Falls assessment.
When looking at falls assessments as with all other aspects of their care, our focus should be on the individual. There are falls assessment tools which can help us to identify a person’s risk of falling but we need to remember that they are only part of the process, what is more important is that we look at the person individual risk factors. We need to:

21
Falls Safety Awareness
• Use our own knowledge of the person.• Gain information from relatives and the clients themselves. Collect previous history of falls
and causes.• Know current medical information for the client.• Check whether they have a fear of falling.• Carry out a hazard check of the area used by the client.
With all of this information we can make an informed decision about the individual’s risk of falling and put in place measures which will enable them to maintain an appropriate level of independence.
Clients who understand the reasons why they are at risk of falling may adopt their own strategies to prevent future falls and these should be taken into account and if appropriate, support given. Enabling individual choice may mean that in some cases the risk would still be there or a new risk may present itself. The risk would then need to be assessed and all discussions and decisions documented in the care plan.
Although relatives, care staff and health professionals may be involved in discussions, if the client has capacity and their health does not dictate otherwise, the ultimate decision will be theirs. See Redcrier’s Mental Capacity Act 2005 manual.
Falls assessment tools.
There are a number of falls assessment tools available to use, however as we have said, they should not be used in isolation of other relevant information and we must not lose sight of the fact that each person is an individual and therefore have their own risk factors to be considered.
Treating each person as an individual ensures an appropriate action plan is identified and implemented for them.
Two of the assessment tools available are STRATIFY and FRAT. Both of these use scoring systems, so will only give a general view of whether that person is at risk of falling, as we have said, there may be many reasons why a person may fall and many will be individual to that person.
Falls Safety Awareness
22
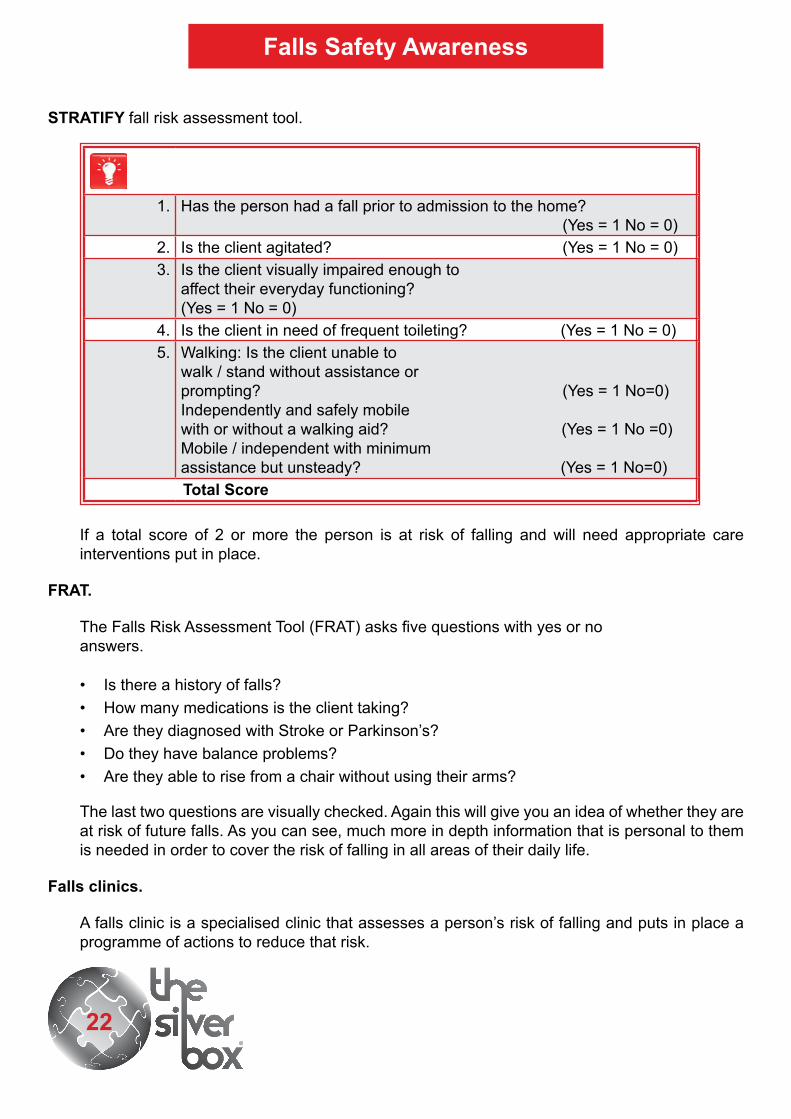
STRATIFY fall risk assessment tool.
1. Has the person had a fall prior to admission to the home? (Yes = 1 No = 0)
2. Is the client agitated? (Yes = 1 No = 0)3. Is the client visually impaired enough to
affect their everyday functioning?(Yes = 1 No = 0)
4. Is the client in need of frequent toileting? (Yes = 1 No = 0)5. Walking: Is the client unable to
walk / stand without assistance orprompting? (Yes = 1 No=0)Independently and safely mobilewith or without a walking aid? (Yes = 1 No =0)Mobile / independent with minimumassistance but unsteady? (Yes = 1 No=0)
Total Score
If a total score of 2 or more the person is at risk of falling and will need appropriate care interventions put in place.
FRAT.
The Falls Risk Assessment Tool (FRAT) asks five questions with yes or noanswers.
• Is there a history of falls?• How many medications is the client taking?• Are they diagnosed with Stroke or Parkinson’s?• Do they have balance problems?• Are they able to rise from a chair without using their arms?
The last two questions are visually checked. Again this will give you an idea of whether they are at risk of future falls. As you can see, much more in depth information that is personal to them is needed in order to cover the risk of falling in all areas of their daily life.
Falls clinics.
A falls clinic is a specialised clinic that assesses a person’s risk of falling and puts in place a programme of actions to reduce that risk.

23
Falls Safety Awareness
Who should attend a falls clinic?
Falls clinics are usually attended by people over 50 who are identified as being ata high risk of falling. Some clinics have set criteria for attendees. An example ofthese criteria is as follows:
• Multiple falls, more than one a year.• Unexplained fall with suspected balance problems.• A single fall with multiple risk factors.• An injury, especially all those who have suffered fractures such as a hip, wrist or arm.
Where ever appropriate a person considered to be at a high risk of falling must be offered a referral to the falls service provided by the National Health Service (NHS).
If a client is prone to falling or at risk, it may be helpful to keep a fall diary, this will help to identify any pattern developing.
An example of a falls diary.Name of Cient: Date of Birth:
Date of fall
Time of day
Where fall occurred Near miss Other factors Any injuries
Accident book
reference number
The falls diary can help to identify any developing pattern which can then be used to form the action plan for reducing future falls.
In this unit we have looked at what information we need to record and how we record it. We should remember that all information recorded should be factual and not based on opinion and should be clear and legible for anyone else picking it up. See Redcrier’s Record Keeping manual.

Falls Safety Awareness
24
Unit Three Questions
What is a care plan?1.
Name five things you would record on a falls incident report.4.
1.
2.
3.
4.
5.
Who should have a falls risk assessment carried out?2.
Why is it important to treat each person as an individual when carrying out a falls risk assessment?
3.
Why should every client have a falls risk assessment done?5.
What does a falls diary help us to do?6.

25
Falls Safety Awareness
Unit Four
Actions to reduce falls.
The manager has overall responsibility for falls, but it is the duty of all carers to ensure that any action plan that has been put in place is carried out. Ongoing assessment is important too so reporting and / or recording any changes you notice is also part of your role.
Assessing an individual client’s risk of falls as part of a comprehensive plan of care is the key to falls prevention and management in a care environment.
Post fall assessment.
Undertaking a ‘post fall’ assessment contributes to the overall management of falls. Collecting good information will help to spot patterns and the possible causes of falls. It provides evidence for other health care services such as the NHS fall services to make informative decisions and also the material allows feedback and discussion with other staff members. The post fall assessment should achieve the following:
• The assessment should identify the individual needs of the client.• The planning and delivery of care must ensure the welfare and safety of the client.
The information can also be used when discussing with the client and the family the circumstances and consequences of the fall. Any action plan to reduce the risk of future falls should be developed with the input and the agreement of the client and the family.
The post fall assessment should include information (where applicable) from the following sources.
• Post fall incident reports.• Post fall diaries.• Care plans.• Falls assessments conducted on admittance.• Checks for illness or medical problems.
With all of this information we will be able to identify the client’s personal risk factors and draw up a plan for that client to reduce their personal risks of falling. Once a plan has been put in place, it should be regularly monitored, reviewed and changed or adapted as required.

Falls Safety Awareness
26
When looking at a plan to reduce falls it is important to look at each risk factor and discuss what is needed to support it.
Risk Action Referral
History offalling.
Assess previous falls using information from
client family members, friends, and carers.
Descriptions of what happened.
Identify any links or causes of the falls.
Establish any emerging patterns.
Frequency of falls.
Confidence.
Refer to GP forreview.Referral to localfalls service forassessment.
MedicalHistory /medicalcondition.
Assess health history using previous medical history.
Look for clues which may have an effect on the person:• Recent weight loss.• Reduced appetite.• Increased tiredness.• Changes in bowel habit, urinary frequency.
Refer to GP fora review.
Medication.
Identify current medication, type and frequency?
Are all the medications necessary?
Identify any side effects.
Check medication is being taken at the right time,
correct method.
Check date of last medication review.
Discuss withGP / medicationreview.

27
Falls Safety Awareness
Risk Action Referral
Gait, mobilityand balance.
Ensure comprehensive assessment is completed.
Undertake moving and handling assessment. Identify any mobility difficulties including balance and transfers.
Use of any walking appliance.
Check equipment is in good working order.
Ensure adequate space for the person to mobilise with walking aid.
Consider environmental changes to increase safety.
Provide advice on how to manoeuvre safely, avoiding stooping, over stretching.
Promote independence where possible in functional activities.
Ensure regular supervised walking for those unsafe to walk independently.
Occupational therapist to assess functional capability.
Referral to GP /communityphysiotherapistor occupationaltherapist forassessment forgait, balanceand strengthexercises and orother walkingequipment.
Nutrition/ hydrationand alcoholintake.
If losing weight, perform nutritional assessment using MUST.
Weigh regularly.
Advise about importance of well-balanced diet, use of calcium and vitamin D for bone health.
Use of supplements.
Maintain adequate fluid balance, complete fluid / chart and monitor.
Monitor of swallowing problems, ensure dentures are used and well fitting.
Observe for sore gums / oral infections.
Advise on alcohol consumption of more than 1 unit per day and advise on the effects of alcohol including interactions with medications.
Refer to adietician.Refer tospeech andlanguage teamfor advice onswallowingdifficulties.Seek a dentalassessment.

Falls Safety Awareness
28
Risk Action Referral
Foot care / footwear.
Check foot wear is well fitting, non slip heels, no high heels or trailing laces.
Advise on dangers of walking bare foot, in socks or tights.
Consider slipper socks in bed for people at risk of falling out at night.
Advice on daily foot care.
Visual check for problems with feet or nails.
Observe any signs for poor circulation due to restricting hosiery. Consider use of soft-top (nonrestrictive socks).
Referral to apodiatrist forreview.
Vision& hearing.
Through comprehensive assessment, identify any visual or hearing problems. Identify any risks due to blurring / difficulty in judging distances.
Ensure good lighting. Recommend caution in new situations and on uneven floors. Areas free of clutter.
Spectacles are kept clean, fit well and used correctly.
People over the age of 65 are entitled to free eyes tests, ensure annual eye tests.
Check ear canal wax and hearing has been tested and correct as far as possible.
Ensure that if wearing a hearing aid, its working correctly and being used.
Referral toaudiology oroptician.

29
Falls Safety Awareness
Mobility equipment.
There is a range of equipment than can assist with mobility, e.g. walkers, wheelchairs, walking sticks. Prior to use many of these require adjustment and / or careful measuring in order to meet the person’s individual needs. For example, the height of a walking frame may need adjusting. The device itself could become a fall hazard if the measurements do not correctly match with the person using the device.
Risk Action Referral
Posturalhypotension.
Identify any episodes of dizziness on standing / sitting up / getting out of bed.Check lying and standing blood pressure.Medication review.Discuss coping techniques to reduce effects of standing up to quickly. Use of pillows to raise head.Frequent meals and fluids.
Review by GP/ review byfalls / syncopeclinic.
Urinaryincontinence.
Maintain good fluid intake, (1500mls daily).
Medical check up to identify infection.
High fibre diet to prevent constipation. Laxatives if necessary.
Ensure regular toileting; provide toileting aids, urine bottles, and bedside commodes.
Review by GP/ Bowel andbladderservicereview.
Cognitiveimpairment.
Identify cause through assessment and establish extent to which the person is affected.
Discuss with multidisciplinary team (MDT) possible options for management.
People in the early stages of dementia often respond well to balance and strength training and general exercise provision.
Increase in room checks and observation. Use of sitters to supervise and observe.
Initiate social activities to prevent wandering.
Review byGP.

Falls Safety Awareness
30
Exercises.
Simple exercises can help to strengthen muscles and help with balance, but also build confidence as the client sees what they are capable of. Exercise can be taken while seated in a chair. Simple exercises like flexing your fingers, bending your knees, pointing your toes carried out regularly can increase your suppleness and give you more flexibility and if done as a group it can be good fun as well. It may be necessary to look at what exercises would be suitable for each individual client and discussed with them to decide whether they would prefer one to one or in a group. Tai chi as a form of exercise may also be suitable for some clients as it is fairly gentle and again can build confidence and aids their physical and mental health.
Elsie Mann 82, has been admitted to the Park care home. In the past 6 months she has had two falls, which resulted in a broken left wrist. She has mild Alzheimer’s disease. She wears bifocal glasses and uses a walking frame. She has a poor appetite and may have lost weight. She wears slippers.
Reflective learning activity.
From the following three risk factors name two actions for each risk factor that would help reduce the risk of falling.
1.
2.
1.
2.
1.
2.
Gait, mobility and balance.1.
Nutrition / hydration.2.
Foot care.3.

31
Falls Safety Awareness
Unit Four Questions
Who has overall responsibility for the management of falls in the workplace?2.
Identify two pieces of mobility equipment.
2.
1.
1.
If the risk of a client falling was due to vision and hearing, give examples of two actions you could take?
5.
What is the key to falls prevention and management?3.
What should the post fall assessment achieve?4.
2.
1.

Falls Safety Awareness
32
Unit Five
Safety when dealing with a falling client.
Falls should not be treated lightly, although they may have no lasting physical effects such as injury, their impact on the person who has been subjected to the fall may be life changing. It’s also important to remember that there may be many risk factors involved.
Therefore, all care environments must have effective management policies in place that help reduce falls, protect the client from injury and supports the wellbeing and quality of life for its clients.
These policies and procedures must at all times meet legal requirements and follow best practice guidelines. Additionally, managers are responsible for ensuring that the environment is safe for the clients and employees and all staff are appropriately trained to meet the needs of the clients.
Identifying and assessing all those clients who are potentially at risk of falling is the first crucial step in identifying individualised effective methods in falls reduction and prevention.
Environmental interventions.
Actions that could help reduce a fall in the care environment include:
• Non-slip carpets, in the same colour where possible.• Good lighting and night lights for clients who need them.• Grab rails in corridors, bathrooms, toilets and if needed in the persons room.
On witnessing a fall, or finding a person who has fallen.
• It’s crucial that immediately following a fall, safe moving and handling and prompt appropriate care and attention is carried out. This is critical to the person’s chance of making a full recovery. Inappropriate response or actions could delay the treatment and could cause further harm to the person or cause risk injury to the care staff.
• All care establishments should have clear policies and procedures in the event of a fall and all staff are responsible for following these policies and procedures.
• The falling person presents a potential risk to the health and safety not only to themselves but also to the staff caring for them. Moving and handling equipment should be introduced to minimise the incidence of staff injuries from manual handling.

33
Falls Safety Awareness
• Back Care ( the National Organisation for Healthy Backs) in its Guide to the Handling of People suggests that `if a person is falling and is unable to regain balance, they must be lowered to the ground safely’.
• Any form of manual lift that is used in exceptional circumstances where there is no other possible option for example in a area that is inaccessible to hoists must be fully assessed, agreed and in line with your organisations policies and procedures.
• If the falling person is out of your reach, you will not have enough time to reach them, if possible remove any dangerous object that they might fall on.
• If the person is within your reach, you may be able to control the fall by getting behind the falling person, but always consider safety first. Maintain a stable base with flexed knees to help protect your back. (see Theory of Moving People Safely) and allow the person to slide to the floor supporting their head if possible. Do not take all of the person’s weight. When the person is sitting on the floor leaning against you, take a step back still supporting their head and maintaining their normal back position and gently lower them to the floor and allow them to recover. Please check the policies and procedures to determine whether this is appropriate in your workplace.
After a person has fallen carry out the following checks:
1. Upon finding a person who has fallen always check for ongoing hazards or dangers, it’s important to quickly summon help.
2. Check if the person is responsive and if so provide reassurance and comfort to the person. If not responsive, check the person’s airway and breathing.
3. If unresponsive, Cardiopulmonary Resuscitation (CPR) may be required if appropriate to the wishes of the person. If the person does not require resuscitating this should be clearly stated in their care plan and may be written as DNACPR: Do not attempt cardiopulmonary resuscitation.
4. An initial assessment to ascertain whether the person is injured should be undertaken by a senior member of staff. A survey is performed to identify potential injuries, for example complaint of pain, loss of sensation, loss of movement, visible injuries, obvious deformity, bruises, and skin tears.
5. Check for signs of nausea, confusion, drowsiness, or agitation.
6. A set of baseline observations should be performed such as blood pressure, temperature, pulse and respirations if appropriate. If you are just performing emergency first aid this will not be necessary. See Redcrier’s Basic Emergency First Aid manual.
Do not attempt to hold a person up or catch them if they are falling it is unsafe and could cause either the falling person or yourself harm.

Falls Safety Awareness
34
7. If head trauma, spinal damage or lower limb fracture is suspected make the person as comfortable as possible on the floor. DO NOT MOVE THE PERSON. If signs of injury are detected medical help should be sought as outlined in your organisations policies and procedures.
8. If a decision is taken that it would be appropriate to move the person then it’s important that all staff have the training and equipment to safely move the person back to their bed or chair ensuring privacy and dignity are respected.
9. Ensure an accident report and falls report are completed, record in care plan and inform next of kin as agreed in the care plan and if applicable report under RIDDOR.
10. Whenever possible, it’s important to explore what may have caused the fall and seek solutions to prevent further falls occurring.
11. Observe for any signs of nausea, vomiting or headache which could be a sign of a head injury. If head injury is suspected, always seek medical advice.
The preferred method for getting a person up from the floor should always be enabling them to get up themselves. Only if this is not possible should other methods be considered. If a person has fallen, you have completed the above checks and the person feels able to, they should always be encouraged to get themselves up, ensure they have had plenty of time to recover from the event, if necessary make them comfortable where they have fallen to allow time forrecovery. When they are ready talk them through the following procedure:
Encourage the person to bend up both knees (one at a time) and roll onto their side and then push up into a sitting position.
When ready ask them to roll onto all fours.
Bring a steady low table, chair or stool to within their reach and alongside them not in front. Then ask them to place their nearest hand on the seat to enable to push themselves up one leg at a time, using their other hand to push down on their raised knee and then swing round into a sitting position.
As we have shown throughout the manual falls are very common and can have many causes, you will not be able to prevent all falls, but hopefully we have shown how putting in place measures for each individual client will help to prevent those falls which would have been predictable and make you more aware of the causes and effects of falls and your role in supporting those who are at risk.
Except in exceptional or emergency situations, the manual lifting of all or most of a person’s weight is no longer accepted as a viable handling technique.

35
Falls Safety Awareness
Unit Five Questions
Give two examples of what you should not do if a person is falling.
2.
1.
1.
On finding a person who had fallen what would be the preferred way of getting them up off the floor?
2.
Give two examples of where you would record the fall.3.
What would you not do if you suspect an injury e.g. head, spine, fracture of a lower limb?
4.
Why should we never attempt to hold a person up or catch them if they are falling?5.
If you find someone who may have fallen, what two things should you do first?6.