Failure to Collide -...
25
Failure to Collide Ebola and Modern Medicine, 2014 Paul Farmer, MD, PhD Harvard Medical School Brigham and Women’s Hospital Partners In Health Kapuscinski Development Lecture King’s College London April 20, 2015 Photo by Rebecca E. Rollins
Transcript of Failure to Collide -...

Failure to Collide
Ebola and Modern Medicine, 2014
Paul Farmer, MD, PhD Harvard Medical School
Brigham and Women’s Hospital
Partners In Health
Kapuscinski Development Lecture
King’s College London
April 20, 2015
Photo by Rebecca E. Rollins

Slow Plague vs. Fast Plague?
Zoonoses from equatorial Africa
• Marburg, Germany (1967)
• Yambuku, Zaire (1976)
• Nzara, Sudan (1976)
Photo by Lyle Conrad

Long DDx in Sub-Saharan Africa
• Malaria (“choleraic presentation”)
• Cholera
• Enteric fever due to S. typhi
• Lassa fever
• Dengue fever
• Yellow fever
• Relapsing fever
• Shigellosis
• Meningococcemia
• Listeriosis
• Staph/strep bacteremia
• Anthrax
• Measles
• Varicella
• Chikungunya virus
• Leptospirosis
• Toxic shock syndrome
• Fulminant viral hepatitis
• Influenza

Kikwit, 1995

Pathophysiology
• Enters through mucosa, breaks in skin, parenteral introduction (e.g needlestick);
environmental testing: no viable RNA on high-touch surfaces (e.g. bed rails, BR
tiles) but easily cultured from human remains for days to weeks
• Target cells include monocytes, macrophages, dendritic cells; then on to lymph
nodes, liver, spleen
• EBOV readily isolated from most bodily fluids (and ET suctioning) during
illness (begins 5-10 days after infection; earlier with direct inoculation)
• Infection of adrenal cortical cells; impaired synthesis of steroids, Na+
• ?Mechanism of GI involvement (?translocation of gut bacteria)
• Coagulopathy
• Autopsy studies/non-human primate models unremarkable for irreversible
vascular lesions (“infection of endothelial cells by Zaire Ebola virus was
infrequent and was mainly restricted to terminal stages of disease,” Feldmann
and Geisbert 2011)
Feldmann H, Geisbert TW. Seminar: Ebola Hemorrhagic Fever. Lancet 2011; 377: 849-862.

Slow vs. Fast Responses?
• Current (“25th recorded”)
outbreak of EVD thought to
begin in 12/2013 in Guinea Rain
Forest
• Patients not dx’d until epidemic
among HCWs
• Cases in all 3 countries by 4/2014
• WHO warns against “over-
reaction” in 4/2014
• MSF declares EVD “out of
control” in 6/2014
• As of 4/2015, 25,556 cases
Video source: WHO Ebola Response Team. Ebola Virus Disease in West Africa—The First 9 Months of the Epidemic and Forward Projections. NEJM
2014; 371: 1481-95.

Freetown, Sierra Leone
October 2014
Photo by Rebecca Rollins
How Did Ebola Spread So Quickly?
Ebola As Caregivers’ Disease

CDS (Clinical Datapenia Syndrome) in Ebola Epidemics
• Prodrome of fatigue/F/C/malaise/myalgias
• Predominance of GI symptoms (N/V/D, abdominal pain) f/b
hypovolemic shock and MSOF
• Hemorrhagic sx (petechiae, uncontrolled bleeding at venipuncture
site, hematemesis, melena) in minority of patients (1/44 in Kenema)
• Dizziness, headache common; delirium, stupor, meningo-encephalitis
in 10-15%; arthralgias also seen
• Little lab data except PCR. When reported: lymphopenia, plt,
transaminitis (AST>ALT); elevated BUN/Cr; acidosis common;
Na+, K+, Ca++; ?DIC
• Long-term sequelae (i.e. opthalmalhogic, neurologic, ?)

World Health Organization. Marburg Hemorrhagic Fever Fact Sheet 2014.
70.8%
0.0%
West Africans, 2014 Americans, 2014
CFR and “No-Overlap Syndrome”
The Collision of Modern Medicine and Hemorrhagic Viruses
22.6%
85.9%
Central Europe, 1967 Africa, 1968-2007
95% CI:
[0.0-0.0%]
(7/31) (462/538)
(0/10) (2,839/4,010)
• High mortality in Germany, Yugoslavia
• Grotesque mortality in sub-Saharan Africa,
even in cities (e.g. Angola, 2005)
• From Kikwit (82%) to Kenema (74%)
• All Americans have survived w/ proper care
Marburg Virus Disease, 1967 vs. Marburg Virus Since
Ebola Virus Disease in West Africa vs. US Hospitals
WHO Ebola Response Team. Ebola Virus Disease in West Africa—The First 9 Months of the Epidemic and Forward Projections. NEJM 2014; 371:
1481-95.

Clinical Course Revealed by the Collision (8/2)
Lyon GM, Mehta AK, Varkey JB, et al. Clinical Care of Two Patients with Ebola Virus Disease in the United States. NEJM 2014; 371: 2402-2409.
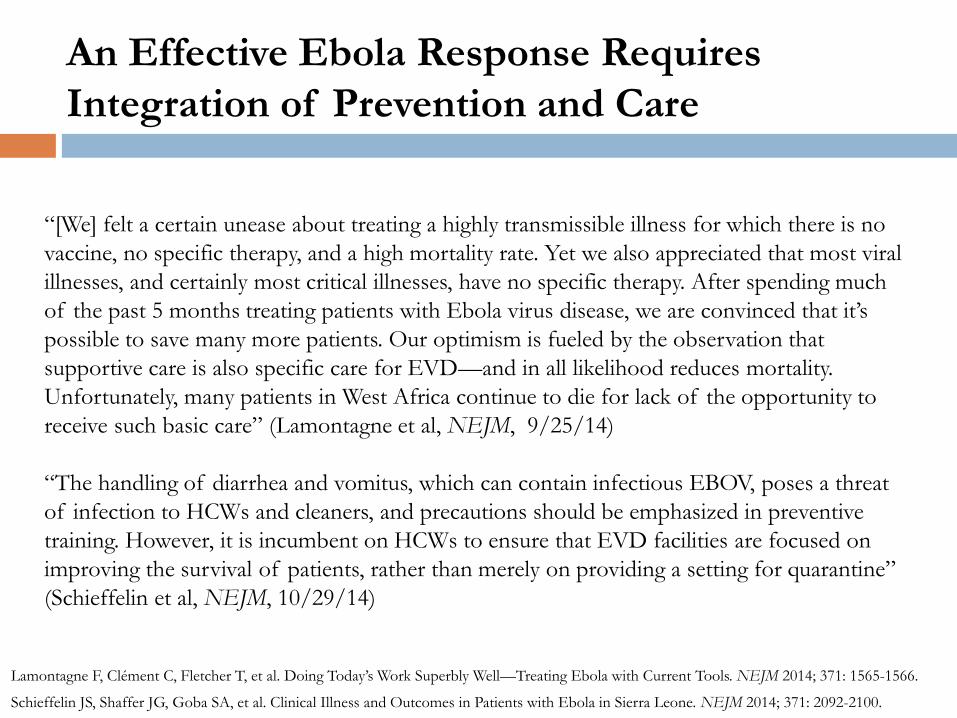
An Effective Ebola Response Requires
Integration of Prevention and Care
Lamontagne F, Clément C, Fletcher T, et al. Doing Today’s Work Superbly Well—Treating Ebola with Current Tools. NEJM 2014; 371: 1565-1566.
Schieffelin JS, Shaffer JG, Goba SA, et al. Clinical Illness and Outcomes in Patients with Ebola in Sierra Leone. NEJM 2014; 371: 2092-2100.
“[We] felt a certain unease about treating a highly transmissible illness for which there is no
vaccine, no specific therapy, and a high mortality rate. Yet we also appreciated that most viral
illnesses, and certainly most critical illnesses, have no specific therapy. After spending much
of the past 5 months treating patients with Ebola virus disease, we are convinced that it’s
possible to save many more patients. Our optimism is fueled by the observation that
supportive care is also specific care for EVD—and in all likelihood reduces mortality.
Unfortunately, many patients in West Africa continue to die for lack of the opportunity to
receive such basic care” (Lamontagne et al, NEJM, 9/25/14)
“The handling of diarrhea and vomitus, which can contain infectious EBOV, poses a threat
of infection to HCWs and cleaners, and precautions should be emphasized in preventive
training. However, it is incumbent on HCWs to ensure that EVD facilities are focused on
improving the survival of patients, rather than merely on providing a setting for quarantine”
(Schieffelin et al, NEJM, 10/29/14)

Preliminary Conclusion
• An effective Ebola response relies on
understanding epidemiology, pathophysiology,
and clinical course
• And needs staff, stuff, space, and systems for
safe supportive care
• Caregivers at greatest risk; survivors essential
part of response
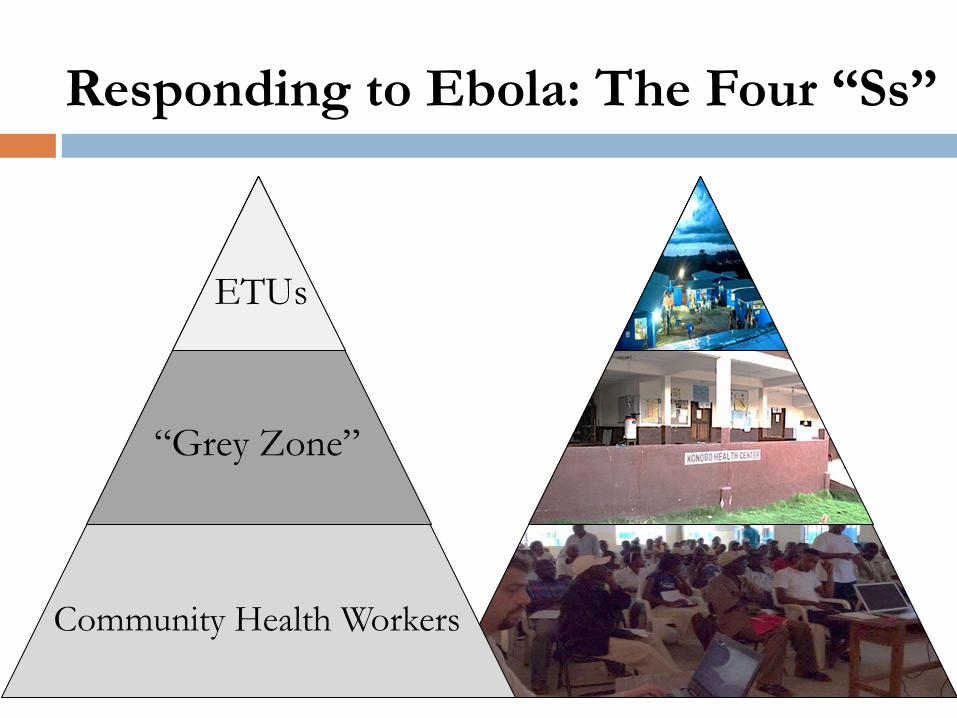
Responding to Ebola: The Four “Ss”
Community Health Workers
“Grey Zone”
ETUs

• RNs, MDs (esp. critical care)
• Nurses’ aides
• Psychosocial team
• Community health workers
• Logisticians
• Administrators/managers
• Researchers/epidemiologists
• Cleaners/sprayers
• Cooks
• Gardeners
• Plumbers
• Projectionists
• Priests Photo by Rebecca Rollins Photo by Rebecca Rollins
Staff: Two Tasks, One Team
Ebola Virus: For Want of
Rubber Gloves, Doctors Die
By Drew Hinshaw
August 16, 2014
1928 ad feat.
Margibi County,
Liberia
Stuff: Personal Protective Equipment

Stuff: Planes, Trains, and Automobiles
Photo by Partners In Health

Stuff: Preventives, Diagnostics, Therapeutics

Space: “One Way In, Two Ways Out”
Photo by Daniel Berehulak Photo by Jon Lascher

Systems: Respond to Ebola, Build/Rebuild Health Systems

0%
20%
40%
60%
80%
100%
1999 2002 2005 2008 2011 2014
WHO. Vaccine-Preventable Diseases Monitoring System: 2014 Update.
Hamilton J. “Ebola Is Preventing Kids from Getting Vaccinated in Liberia.” NPR: October 23, 2014.
UNFPA Sierra Leone Country Office. Impact of Ebola Outbreak on Reproductive Health and Proposed Mitigation Strategy. October 2014.
Children aged 12-23 months given
measles conjugate vaccine in Liberia
37,381
1,724
May-14 August-14May 2014 August 2014
Visits for short-term
family planning methods,
Marie Stopes International Sierra Leone
Systems: Respond to Ebola, Build/Rebuild Health Systems

0
500
1,000
1,500
2,000
2,500
1990 1995 2000 2005 2010 2015
Maternal deaths per 100,000 live births
Sierra Leone
Liberia
Guinea
WHO, UNICEF, UNFPA, and The World Bank. Trends in Maternal Mortality: 1990 to 2013. Geneva: WHO, 2014.
Hayden EC. Maternal Health: Ebola’s Lasting Legacy. Nature 2015; 519: 24-26.
Systems: Respond to Ebola, Build/Rebuild Health Systems

0
500
1,000
1,500
2,000
2,500
1990 1995 2000 2005 2010 2015
Maternal deaths per 100,000 live births
Sierra Leone
Liberia
Guinea
WHO, UNICEF, UNFPA, and The World Bank. Trends in Maternal Mortality: 1990 to 2013. Geneva: WHO, 2014.
Hayden EC. Maternal Health: Ebola’s Lasting Legacy. Nature 2015; 519: 24-26.
Systems: Respond to Ebola, Build/Rebuild Health Systems

What Never Happens with Emergency Responses?
• Health systems strengthening
• Training/capacity building
• Research
Photo by Clinton Foundation
$5.4B?
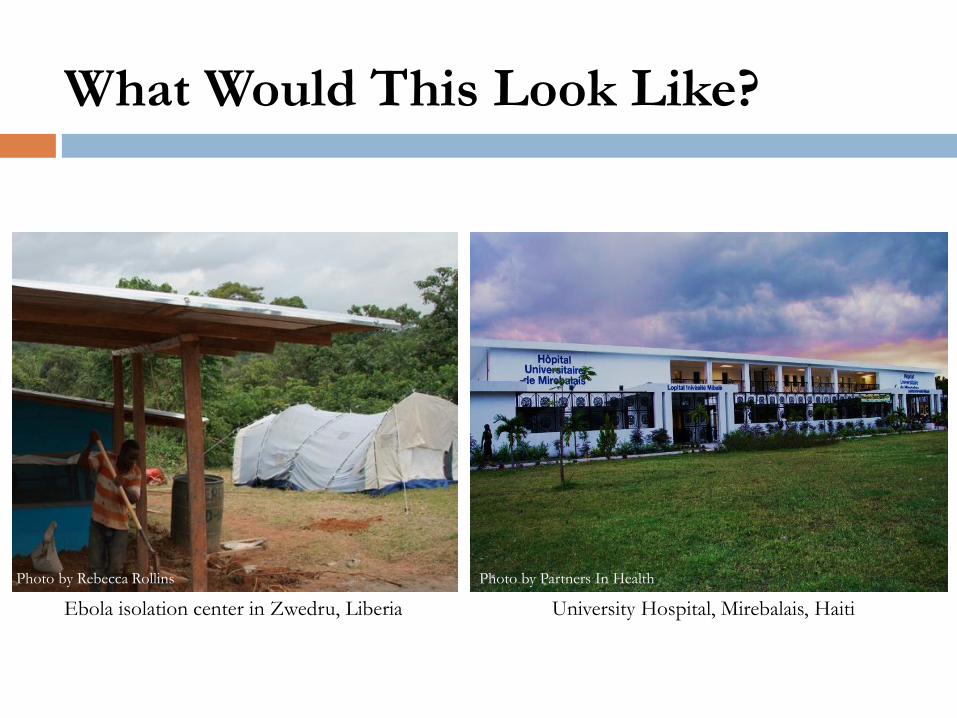
What Would This Look Like?
Photo by Rebecca Rollins Photo by Partners In Health
Ebola isolation center in Zwedru, Liberia University Hospital, Mirebalais, Haiti

Glenna Gordon, The Wall Street Journal
Monrovia, Liberia: September 29, 2014
Thank
You
`