Faculty of nursing CHEM 203 Biochemistry UNIT VII Amino acids, Protein chemistry and metabolism Part...
20
Faculty of nursing CHEM 203 Biochemistry UNIT VII Amino acids , Protein chemistry and metabolism Part Dr. Ola Fouad Talkhan
-
Upload
tatum-joseph -
Category
Documents
-
view
216 -
download
0
Transcript of Faculty of nursing CHEM 203 Biochemistry UNIT VII Amino acids, Protein chemistry and metabolism Part...

Faculty of nursing
CHEM 203 Biochemistry
UNIT VII
Amino acids , Protein chemistry and metabolism
Part Dr. Ola Fouad Talkhan

Protein digestion The process of digestion is defined as the
‘process by which macromolecules in food are broken down into their component small-molecule subunits’.
The macromolecules are the proteins or polypeptides themselves, and the subunits are the amino acids.
The bonds holding the subunits together are peptide bonds

Protein Digestion
the degradation of proteins by cellular enzymes enzymes in a process called hydrolysis.
Protein digestion takes place in two different phases:◦In the stomach◦In the small intestine
Both of these phases of digestion are based on several types of enzymes that are called proteinases and proteases.


In the Stomach : start of protein Digestion
Gastrin-stimulates Parietal cells to secrete HCL; Chief cells of the gastric glands to secrete pepsinogen
Hydrochloric acid-Denatures protein structure-Activates pepsinogen (zymogen) to pepsin
Pepsin -hydrolyzes proteins to smaller polypeptides and some free amino acids.
Proteins proteoses + peptones Pepsin , H+ pH 1-2

In the intestine The remainder of protein digestion occurs in the small intestine as the
result of the action of enzymes such as1- trypsin , chemotrypsin and carboxypeptidase (secreted by the
pancreas)
proteoses polypeptides + A.A. peptones aminopeptidase polypeptides di, and tripeptidase + A.A. carboxypeptidase
2- peptidases ( aminopeptidase ,dipeptidase and tripeptidase ) (located in the cells that line the small intestine).
Trypsin, chemotrypsinHCO3 , pH 8.0
di, and tripeptidase dipeptidase A.A. tripeptidase

Amino acids absorbed
Proteins are broken down to◦ Tripeptides◦ Dipeptides◦ Free amino acids
Free amino acid small intestine(villi)Liverblood circulation

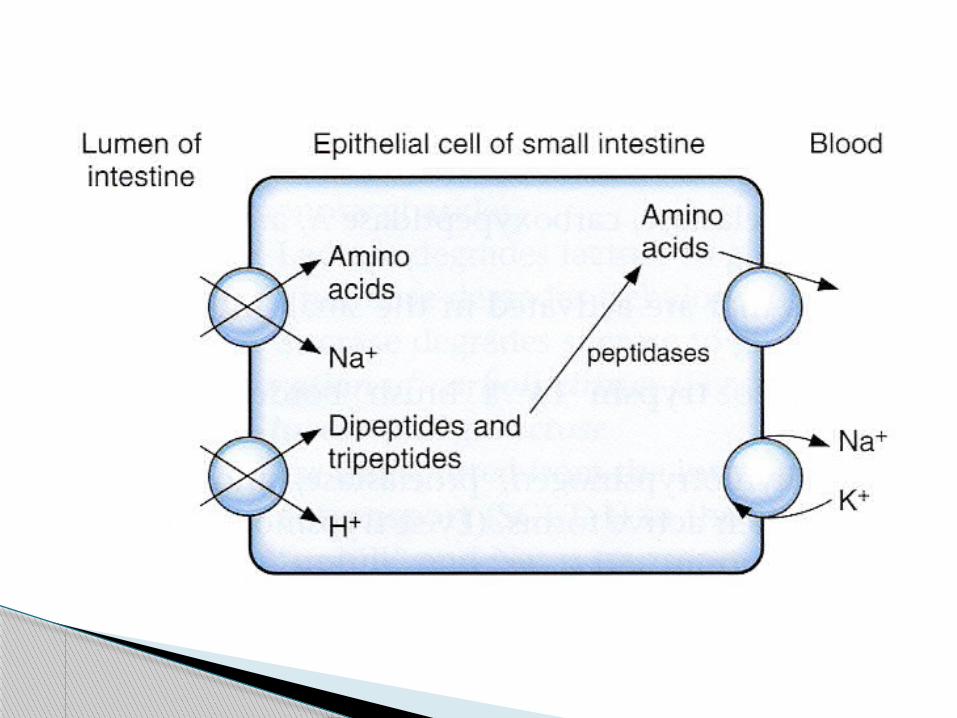
Peptide AbsorptionForm in which the majority of
protein is absorbed
More rapid than absorption of free amino acids
Active transport◦ Energy required
Metabolized into free amino acids in enterocyte
Only free amino acids absorbed into blood

Amino Acid Degradation and Synthesis
The catabolism of the amino acids involves the removal of α-amino groups (NH3), followed by the breakdown of the resulting carbon skeletons.
These pathways converge to form seven intermediate products:oxaloacetate, pyruvate, α-ketoglutarate, fumarate, succinyl coenzyme A (CoA), acetyl CoA, and acetoacetate.
these will enter in the synthesis of glucose or lipid or in the production of energy through their oxidation to CO2 by the citric acid cycle

Nonessential amino acids can be synthesized from the intermediates of metabolism or, as in the case of
cysteine and tyrosine, from essential amino acids

Fate of NH3 produced in deamination
Ammonia produced from deamination of A.A. are very toxic to the brain and nervous tissues so, it is rapidly removed by :
1. Urea : Formation of urea in the liver is quantitatively the most important disposal route for ammonia.
Urea travels in the blood from the liver to the kidneys, where it passes into the glomerular filtrate.

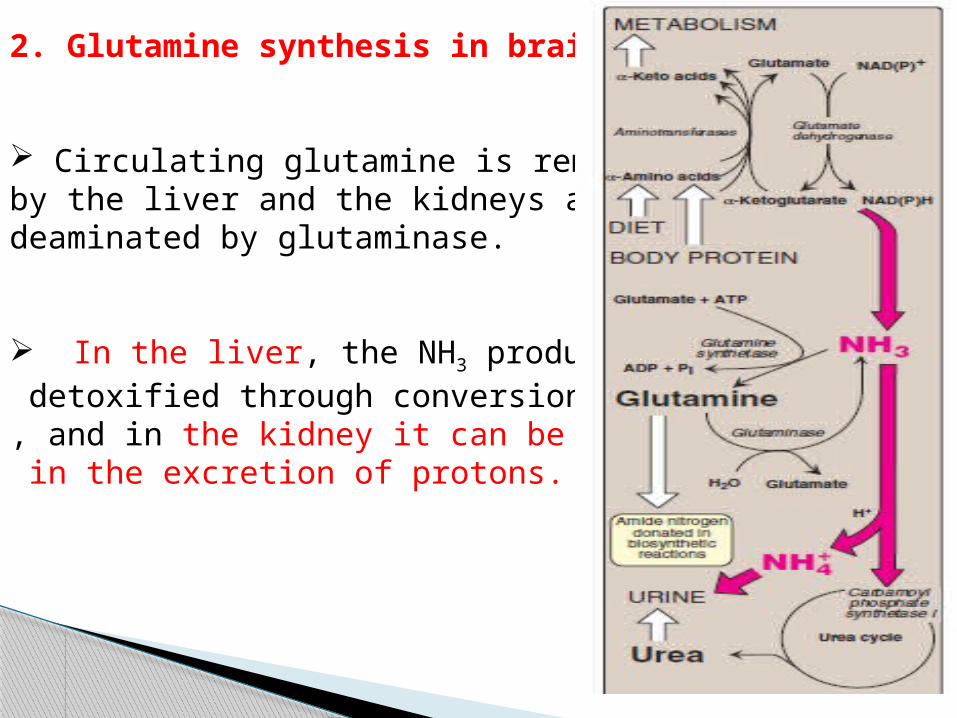
2. Glutamine synthesis in brain and liver
Circulating glutamine is removed by the liver and the kidneys and deaminated by glutaminase.
In the liver, the NH3 produced is detoxified through conversion to urea, and in the kidney it can be used in the excretion of protons.

HyperammonemiaThe capacity of the hepatic urea cycle exceeds the normal rates of ammonia generation, and the levels of serum ammonia are normally low (5–35 μmol/L).
However, when liver function is compromised, due either to genetic defects of the urea cycle or liver disease, blood levelscan rise above 1,000 μmol/L.
Such hy per ammon emia is a medical emergency, because ammonia has a direct neurotoxic effect on the CNS
the symptoms of ammonia intoxication, 1-tremors, slurring of speech, somnolence, vomiting, cerebral edema, and blurring of vision.
2-At high concentrations, ammonia can cause coma and death.

The two major types of hyperammonemia are:
1. Acquired hyperammonemia:
Liver disease is a common cause of hyperammonemia in adults, and may be due, for example, to viral hepatitis or to hepatotoxins such as alcohol
2. Congenital hyperammonemia: Genetic deficiencies of each of the five enzymes of the urea cycle have been described

METABOLIC DEFECTS IN AMINO ACID METABOLISM
1- Phenylketonuria (PKU).
A deficiency in phenylalaninehydroxylase results in the disease
phenylketonuria (PKU).
Phenylketonuria (PKU), caused by a deficiency of phenylalanine hydroxylase

Characteristics of classic PKU:1-Elevated phenylalanine:Phenylalanine is present in elevated concentrations in tissues, plasma, and urine.
2-CNS symptoms: Mental retardation, failure to walk or talk,seizures, hyperactivity, tremor, microcephaly, and failure to grow are characteristic findings in PKU.
3-Hypopigmentation: Patients with phenylketonuria often show a deficiency of pigmentation (fair hair, light skin color, and blue eyes).

2- Maple syrup urine disease(MSUD) is a rare (1:185,000), autosomal recessive disorder in which there is a partial or complete deficiency in branched-chain α-keto acid dehydrogenase, an enzyme complex that decarboxylates leucine, isoleucine, and valine
Accumulation of these A.A. in the blood, causing a toxic effect that interferes with brain functions.
Characteristics of Maple syrup urine disease feeding problems, vomiting, dehydration, severe
metabolic acidosis, and a characteristicmaple syrup odor to the urine. If untreated, the disease leads to mental retardation,
physical disabilities, and even death.

3- HomocystinuriaThe homocystinurias are a group of disorders involving defects in the metabolism of homocysteine. The diseases are inherited as autosomal recessive illnesses,due to a defect inthe enzyme cystathionine β-synthase,
Characteristics of Homocystinuria high plasma and urinary levels of homocysteine and methionine and low levels of cysteine.
ectopia lentis (displacement of the lens of the eye), skeletal abnormalities, a tendency toform thrombi (blood clots), osteoporosis, and neurological deficits.
Patients can be responsive or nonresponsive to oral administration of pyridoxine (vitamin B6)