Factors Influencing Bone Mineral Density in ARV-Naïve Patients at ...
5
175 ORIGINAL ARTICLE Acta Medica Indonesiana - e Indonesian Journal of Internal Medicine Factors Influencing Bone Mineral Density in ARV-Naïve Patients at Sanglah Hospital, Bali Sri Masyeni, Susila Utama, Agus Somia, Raka Widiana, Tuti P. Merati Department of Internal Medicine, Faculty of Medicine, Udayana University, Denpasar, Bali, Indonesia. Correspondence mail: Division of Tropical and Infectious Disease, Department of Internal Medicine, Faculty of Medicine, Udayana University. Jl. PB. Sudirman, Denpasar, Bali, Indonesia. email: [email protected]. ABSTRAK Tujuan: menilai faktor-faktor yang mempengaruhi densitas mineral tulang pada pasien yang belum pernah mendapat terapi ARV (ARV-naïve) di Rumah Sakit Sanglah, Bali. Metode: densitas mineral tulang atau bone mineral density (BMD) dinilai secara potong lintang dan diukur dengan mengunakan absorpsiometri sinar-X ganda di daerah lumbal / lumbal spine (LS) dan leher femur/femoral neck (FN) pada 73 pasien yang terinfeksi HIV tetapi ARV-naïve. Pasien yang terinfeksi HIV tersebut didapatkan dari poliklinik Rumah Sakit Sanglah secara berurutan sejak bulan Januari hingga Juni 2012. Kriteria inklusinya adalah pasien yang terinfeksi HIV dan ARV- naïve, berusia 13-50 tahun. Hubungan antara faktor-faktor yang mempengaruhi BMD, kadar CD4, RNA HIV, dan stadium HIV (WHO) dianalisis dengan ANOVA dan uji korelasi Spearman. Hasil: penelitian ini mengikutsertakan 73 pasien, 49 orang (65,2%) di antaranya adalah laki-laki. Usia rata-rata sampel penelitian adalah 33,08 ± 8,29. Nilai rata-rata CD4 adalah 144,71±143,40 sel/mmc dengan nilai CD4 terendah adalah 1. Nilai rata-rata beban virus atau viral load (VL) adalah 272.330±282.990 kopi/ml, VL terendah adalah ≤400 kopi/ml, dan tertinggi adalah ≥750.000 kopi/ml. BMD rendah ditemukan pada 32/73 subyek (43.8%). Osteopenia dan osteoporosis didiagnosis pada 26/73 subyek (35,6 %) dan 6/73 subyek (8,2%). Sekitar 13 kasus (40,6%) dengan BMD rendah terjadi pada kelompok usia 21-30 tahun. Ditemukan hubungan yang bermakna antara nilai BMD yang rendah dengan stadium HIV (r:0,337; p<0,001). Kesimpulan: pasien ARV-naïve dengan stadium HIV yang lebih tinggi mempunyai risiko yang lebih tinggi mengalami BMD yang rendah. Penelitian lebih lanjut dengan desain penelitian yang berbeda untuk menilai korelasi BMD yang rendah dengan faktor-faktor risiko tersebut. Kata kunci: infeksi HIV, kadar CD4, RNA HIV, stadium HIV, densitas mineral tulang. ABSTRACT Aim: to evaluate factors which influence bone mineral density in ARV-naïve patients in Sanglah Hospital, Bali. Methods: a cross-sectional BMD measured by dual X-ray absorptiometry at the lumbar spine (LS) and femoral neck (FN) in 73 ARV-naïve HIV-infected patients in out patient clinic of Sanglah Hospital, consecutively, from January to June 2012. Inclusion criteria are ARV-naïve HIV-infected patients age 13-50 year old. The relationship among factors influence BMD, CD4 level, HIV RNA, HIV stage (WHO) analysed with Anova and Spearman’s correlation test. Results: this study involved 49 males and 24 females. Mean age was 33.08±8.29. Mean CD4 was 144.71±143.40 cell/mmc with the lowest CD4 is 1. Mean viral load (VL) was 272.330±282.990 copies/ml, the lowest VL ≤400 copies/ml, and the highest ≥750 000 copies/ml. Low BMD found in 32/73 (43.8%). Osteopenia and osteoporosis were diagnosed in 26/73 (35.6 %) and 6/73 (8.2%). 13 (40.6%) of the low BMD cases occured on the age group 21-30 year. Significant correlation found between low BMD with HIV stage (r:0.337; p<0.001). Conclusion: patients with higher HIV stage have higher risk of low BMD in ARV-naïve patient. Further study is needed to evaluate correlation of low BMD with it’s risk factors. Key words: HIV infection, CD4 level, HIV RNA, HIV stage, bone mineral density.
Transcript of Factors Influencing Bone Mineral Density in ARV-Naïve Patients at ...

175
ORIGINAL ARTICLE
Acta Medica Indonesiana - The Indonesian Journal of Internal Medicine
Factors Influencing Bone Mineral Density in ARV-Naïve Patients at Sanglah Hospital, Bali
Sri Masyeni, Susila Utama, Agus Somia, Raka Widiana, Tuti P. MeratiDepartment of Internal Medicine, Faculty of Medicine, Udayana University, Denpasar, Bali, Indonesia.
Correspondence mail: Division of Tropical and Infectious Disease, Department of Internal Medicine, Faculty of Medicine, Udayana University. Jl. PB. Sudirman, Denpasar, Bali, Indonesia. email: [email protected].
ABSTRAKTujuan: menilai faktor-faktor yang mempengaruhi densitas mineral tulang pada pasien yang belum pernah
mendapat terapi ARV (ARV-naïve) di Rumah Sakit Sanglah, Bali. Metode: densitas mineral tulang atau bone mineral density (BMD) dinilai secara potong lintang dan diukur dengan mengunakan absorpsiometri sinar-X ganda di daerah lumbal / lumbal spine (LS) dan leher femur/femoral neck (FN) pada 73 pasien yang terinfeksi HIV tetapi ARV-naïve. Pasien yang terinfeksi HIV tersebut didapatkan dari poliklinik Rumah Sakit Sanglah secara berurutan sejak bulan Januari hingga Juni 2012. Kriteria inklusinya adalah pasien yang terinfeksi HIV dan ARV-naïve, berusia 13-50 tahun. Hubungan antara faktor-faktor yang mempengaruhi BMD, kadar CD4, RNA HIV, dan stadium HIV (WHO) dianalisis dengan ANOVA dan uji korelasi Spearman. Hasil: penelitian ini mengikutsertakan 73 pasien, 49 orang (65,2%) di antaranya adalah laki-laki. Usia rata-rata sampel penelitian adalah 33,08 ± 8,29. Nilai rata-rata CD4 adalah 144,71±143,40 sel/mmc dengan nilai CD4 terendah adalah 1. Nilai rata-rata beban virus atau viral load (VL) adalah 272.330±282.990 kopi/ml, VL terendah adalah ≤400 kopi/ml, dan tertinggi adalah ≥750.000 kopi/ml. BMD rendah ditemukan pada 32/73 subyek (43.8%). Osteopenia dan osteoporosis didiagnosis pada 26/73 subyek (35,6 %) dan 6/73 subyek (8,2%). Sekitar 13 kasus (40,6%) dengan BMD rendah terjadi pada kelompok usia 21-30 tahun. Ditemukan hubungan yang bermakna antara nilai BMD yang rendah dengan stadium HIV (r:0,337; p<0,001). Kesimpulan: pasien ARV-naïve dengan stadium HIV yang lebih tinggi mempunyai risiko yang lebih tinggi mengalami BMD yang rendah. Penelitian lebih lanjut dengan desain penelitian yang berbeda untuk menilai korelasi BMD yang rendah dengan faktor-faktor risiko tersebut.
Kata kunci: infeksi HIV, kadar CD4, RNA HIV, stadium HIV, densitas mineral tulang.
ABSTRACTAim: to evaluate factors which influence bone mineral density in ARV-naïve patients in Sanglah Hospital,
Bali. Methods: a cross-sectional BMD measured by dual X-ray absorptiometry at the lumbar spine (LS) and femoral neck (FN) in 73 ARV-naïve HIV-infected patients in out patient clinic of Sanglah Hospital, consecutively, from January to June 2012. Inclusion criteria are ARV-naïve HIV-infected patients age 13-50 year old. The relationship among factors influence BMD, CD4 level, HIV RNA, HIV stage (WHO) analysed with Anova and Spearman’s correlation test. Results: this study involved 49 males and 24 females. Mean age was 33.08±8.29. Mean CD4 was 144.71±143.40 cell/mmc with the lowest CD4 is 1. Mean viral load (VL) was 272.330±282.990 copies/ml, the lowest VL ≤400 copies/ml, and the highest ≥750 000 copies/ml. Low BMD found in 32/73 (43.8%). Osteopenia and osteoporosis were diagnosed in 26/73 (35.6 %) and 6/73 (8.2%). 13 (40.6%) of the low BMD cases occured on the age group 21-30 year. Significant correlation found between low BMD with HIV stage (r:0.337; p<0.001). Conclusion: patients with higher HIV stage have higher risk of low BMD in ARV-naïve patient. Further study is needed to evaluate correlation of low BMD with it’s risk factors.
Key words: HIV infection, CD4 level, HIV RNA, HIV stage, bone mineral density.

Sri Masyeni Acta Med Indones-Indones J Intern Med
176
INTRODUCTIONCo-morbidities normally thought to be
age related in populations that are not infected with Human Immunodeficiency Virus (HIV) are now being seen earlier in people with HIV. These are cardiovascular disease, metabolic disorder, neurocognitive disorders, liver and renal impairment, malignancies and bone disorders.1,2 Low BMD including osteopenia and osteoporosis is prevalent in HIV-infected subjects.3-11 Documented for at least two decades, bone loss is gaining recognition as major complication in HIV disease. Low BMD has been reported in many cross-sectional studies involving both younger4 and older3,10,12. A meta-analysis estimated that 67% of HIV-infected persons exhibited reduced BMD, and 15% had osteoporosis.9
The mechanisms underlying these changes are still unclear. Multiple factors associated with alterations in bone metabolism have been postulated and represent a complex interaction between HIV itself,13,14 traditional osteoporosis risk factors exacerbated by consequences of chronic HIV infection (poor nutrition and low weight), high rates of tobacco and alcohol use, low vitamin D levels, use of opioids, hypogonadism, steroid use and antiretroviral treatment (ART).15 In HIV infection, the viral protein itself increases osteoclast activity13, and decreases bone formation by promoting osteoblast apoptosis. Furthermore, chronic immune activation secretes high levels of proinflammatory cytokines e.g. Il-6, TNFα, IL-1β; all stimulate bone resorption.1,2 The relationship between prolonged antiretroviral therapy and bone loss is patent, although there are few data on the specific role of individual agents. Compared with ART-naïve patients, ART-treated individuals carry a 2.5-fold increased odds of having reduced BMD.9
Proteinase inhibitors (PI) containing regiments9,18, and tenofovir (TDF)19 have been reported associated with bone demineralization, although other studies have failed to confirm the association.20-22
The objectives of this study were to determine the profile, prevalence and factors influence BMD in ART-naïve HIV-infected patients.
METHODSFrom January to June 2012, 73 ART-naïve
HIV-infected outpatients consecutively were studied cross-sectionally in clinic of Sanglah Hospital. Inclusion criteria were ART-naïve HIV infected, age between 13-50 years, males and non menopausal females. Data regarding demographic characteristics including gender, age, BMI, risk factors for HIV-infection, stadium of HIV-infection according to WHO classification, immunovirological parameters including human T cell helper (CD4+) count, HIV ribonucleic acid (RNA) serum level, smoking, history of steroid use and alcohol consumption were recorded. A complete physical examination was performed. Written informed consent was obtained from all participants and the study was conducted in adherence with local ethic committee board of Udayana University.
Blood TestCell blood count levels, serum creatinine,
glutamic oxalacetic transaminases (GOT) and glutamic-pyruvic transaminases (GPT) were recorded. HIV- RNA serum levels were measured using brand chain deoxyribonucleic acid (b-DNA) technique (detection limit 400 copies/ml). CD4+ cell count was established using flow cytometry (BD FACS Count).
Bone Mineral DensityAll subjects underwent dual energy X-ray
absorptiometry (DEXA) scan (DEXA DPX;GE- Lunar USA) in the Radiologic Department and image both the anteroposterior lumbar spine (L1-L4) and femoral neck by the radiologist. Variables from the DEXA scan were considered as categorical value (normal values, osteopenia or osteoporosis). World Health Organization (WHO) classification was used for diagnostic purposes. Osteopenia was defined as a T score of between -1 and -2.5 SD, and osteoporosis was defined as a T score of less than -2.5 SD. The T score at the femoral neck makes it possible to quantitatively evaluate cortical bone tissue; the T score at the lumbar spine (L2-L4) makes it possible to quantitatively evaluate trabecular bone.
Statistical AnalysisStatistical summaries were prepared for the
main variables; DEXA scan results and clinical

Vol 45 • Number 3 • July 2013 Factors influencing bone mineral density in ARV-naive patients
177
and demographic characteristic are represented as graphs and tables. In the cross-sectional study, correlation test with Spearman’s correlation test and Anova test to correlate the effect of independent variables (clinical and demographic characteristic) with the DXA results. The P value for inclusion of a covariate in the model was set at P<0.05. The analysis was conducted using statistical package SPSS for Windows 16.0.
RESULTS
Demographic and clinical characteristics of our study population are summarized in Table 1. Males outnumbered females by a ratio of 2:1. BMI of the participants mostly (57.4%) is normoweight and 33.8% is underweight. The median of CD4+ is 59 (1-729) cell/mmc, HIV-RNA median is 168 160 (400-750 000) copies/ml. There is only 2 (2.7%) of the participants have an IVDU, while 44 subjects (60.8%) is a multipartner sexual, as a risk factor to get the HIV infection. In our study, we found 27 (37%) of the study population is homosexual. Almost fifty-percent of the participant was in HIV WHO stage IV.
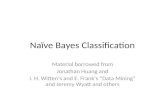
Almost a half of the study participant has low BMD. Low BMD was 32 subjects (43.8%), osteopenia found in 26 (35.6%) and osteoporosis 6 (8.2%). The lowest BMD was 13 (40.6%) in age group 21-30 years and 12 (37.5%) in age group 31-40, respectively. There is no significant correlation between low BMD and age of the cases. More than three-quarters of the low BMD was in HIV WHO stage IV. (Figure 1)
Correlation analysis using Spearman’s and Anova correlation test performed in order to find potential predictive factors of bone loss are summarized in Table 2.
DISCUSSIONOur observational study revealed a marked
prevalence of low BMD in ART-naïve HIV-infected persons. Almost 90% of participants presented some grade of low bone mass and approximately 10% had osteoporosis. Fausto et al. also found similar result with our study whereas low BMD found in 45.8% ARV-naïve
Table 1. Demographic and clinical characteristics (N=73)
Variables n (%)Sex
- Male 49 (65.2)
- Female 24 (34.8)
Age, mean,years (±SD) 33.08 (8.29)
History of smoking 23 (33.3)
History of alcohol used 10 (14.5)
History of IVDU 2 (2.7)
History of steroid use 6 (8.2)
Multipartner Sexual 44 (60.8)
Homosexual 27 (37)
BMI, kg/m2, mean (±SD) 20.32 (3.37)
CD4+, cell/mmc,mean (±SD) 144.71 (143.4)
HIV-RNA, copies/ml, mean (±SD) 272330 (282990)
HIV Stage (WHO)
- Stage I 4
- Stage II 18
- Stage III 19
- Stage IV 32
SD=standar deviation; BMI=body mass index; IVDU=intravenous drug user
Table 2. Correlation analysis of factors influence low BMD
Variables r p
Age -0.101 0.411
Male vs female* -0.304 0.267
History of smoking* -0.26 0.826
History of alcohol used* 0.74 0.546
CD4+ (≤200 vs >200) 0.203 0.85
HIV mRNA (≤100 000 vs >100000) -0.054 0.652
BMI -0.072 0.543
HIV- stage (WHO) (StageI-II vs III-IV) 0.337 0.0004
4
0 0
11
6
1
14
4
1
12
16
4
0
5
10
15
20
stage I stage 2 stage 3 stage 4
Normal Osteopenia Osteoporosis
Fre
qu
en
cy
Figure 1. Number of low BMD cases by HIV- stage (N=73)

Sri Masyeni Acta Med Indones-Indones J Intern Med
178
patient.16 These prevalence are lower than those reported by others authors3,4,7,8,9, but some of these differences may be due to different study characteristics (most included HIV- treated persons)8,9,17-20 and use different study design, commonly cohort study design with longitudinal follow-up.7,8,11 Brown et al. in a meta-analysis study estimated reduced BMD 67% of HIV-infected person and 15% had osteoporosis.9 Setyohadi et al. in Jakarta found reduced of BMD in ARV naïve HIV-infected patients was 26.2%.23 The most low BMD cases found in younger age, 21-30 years old. Arnsten et al. also reported a decrease of BMD in middle age women with HIV infection.4 It is also younger than normal population without HIV-infected person.24 In United States, the rate of osteoporosis will increase at the age of 50-59 year-old women and older in men.24 We found significant correlation between HIV stage (WHO) with low BMD. Bruera et al. found osteopenia and osteoporosis in naïve and in ART patients; these both group had lower BMD compared with healthy seronegative controls.22 We did not include healthy controls because several studies have definitively shown that HIV-infected persons have lower BMD compared to HIV-seronegative persons.3,8,9,11 The correlation among low BMD in more advance clinical conditions (WHO stage IV) may suggest a indirect effect HIV-infection through chronic immune activation effect on bone cells. The higher stage of HIV-infection, the higher level of proinflamatory cytokines are found in HIV-infected patients1,2 such as, tumor necrosis factor-alpha (TNF-α), interleukin (IL)-1, IL-6, IL-11 which is all stimulate bone resorption.25
No correlation found between traditional risk factors like age, BMI, smoking, sex, alcohol consumption, and viral load, level of CD4+ and HIV-RNA levels to low BMD. However, our result show a trend in CD4+ and HIV-RNA levels and low BMD. The reason of this finding may be explained by small sample size, and uneven sample distribution. We also were not able to investigate some variables that commonly influence low BMD in HIV-infected person and biochemical markers of bone metabolism such as serum and urinary calcium, osteocalsin,
parathyroid hormone, alkali phosphatases, 1,25 [OH]2-vitamin D and also free urinary cortisol, testosterone and estradiol levels.
CONCLUSIONWe found a high frequency of osteopenia
and/or osteoporosis in ARV-naive HIV-infected patients. Furthermore, the positive correlation between higher HIV stage and low BMD may suggest an indirect effect of HIV-infection through chronic immune activations. Therefore, clinical monitoring of BMD by DEXA scan should be considered as a priority in HIV-infected persons, to decrease risk of fracture. Prevention strategies such as lifestyle modification and management of abnormal scan according to general guidelines should also be encouraged.
REFERENCES1. Appay V, Sauce D. Immune activation and inflammation
in HIV-1 infection: causes and consequences. J Pathol. 2008;214:231-41.
2. Brown TT. The effect of HIV-1 infection on endocrine organs. Best Pract & Res Clin Endocrinol & Metabolism. 2011;25:403-13.
3. Arnsten JH, Freeman R, Howard AA, Floris-Moore M, Lo Y, Klein RS. Decreased bone mineral density and increased fracture risk in aging men with or at risk for HIV infection. AIDS. 2007;21:617–23.
4. Arnsten JH, Freeman R, Howard AA, Floris-Moore M, Santoro N, Schoenbaum EE. HIV infection and bone mineral density in middle-aged women. Clin Infect Dis. 2006;42:1014–20.
5. Kim TW, Alford DP, Malabanan A, Holick MF, Samet JH. Low bone density in patients receiving methadone maintenance treatment. Drug Alcohol Depend. 2006; 85:258–62.
6. Bolland MJ, Grey AB, Horne AM, et al. Bone mineral density remains stable in HAARTtreated HIV-infected men over 2 years. Clin Endocrinol (Oxf). 2007; 67:270–5.
7. Dolan SE, Kanter JR, Grinspoon S. Longitudinal analysis of bone density in human immunodeficiency virus-infected women. J Clin Endocrinol Metab. 2006; 91:2938–45.
8. Mondy K, Yarasheski K, Powderly WG, et al. Longitudinal evolution of bone mineral density and bone markers in HIV-infected individuals. Clin Infect Dis. 2003;36:482–90.
9. Brown TT, Qaqish RB. Antiretroviral therapy and the prevalence of osteopenia and osteoporosis: a meta-analytic review. AIDS. 2006;20:2165–74.

Vol 45 • Number 3 • July 2013 Factors influencing bone mineral density in ARV-naive patients
179
10. McComsey GA, Tebas P, Shane E, et al. Bone disease in HIV infection: a practical review and recommendations for HIV care providers. Clin Infect Dis. 2010;51(8):000-010.
11. Bonjoch A, Figueras M, Estany C, Perez-Avares N, Rosales J, del Rio L. High prevalence of and progression to low bone mineral density in HIV-infected patients: a longitudinal cohort study. AIDS. 2010;24;2827-33.
12. Sharma A, Flom PL, Weedon J, Klein RS. Prospective study of bone mineral density changes in aging men with or at risk for HIV infection. AIDS. 2010;24:2337-45.
13. Fakrudin JM, Laurence J. HIV-1 Vpr enhances production of receptor of activated NF-κB ligand (RANKL) via potentiation of glucocorticoid receptor activity. Arch Virol. 2005;150:67-78.
14. Kino T, Gragerov A, Kopp JB, et al. The HIV-1 Virion-associated protein Vpr is a coactivator of the human glucocorticoid receptor. Archive. 2009;189:51-62.
15. Cooper OB, Brown TT, Dobs AS. Opiate drug use: a potential contributor to the endocrine and metabolic complications in human immunodeficiency virus disease. Clin Infect Dis. 2003;37 (2 Suppl):S132–S136.
16. Fausto A, Bongiovanni M, Cicconi, et al. Potential predictive factors of osteoporosis in HIV-positive subjects. J Bone. 2006;38:893-897.
17. Ferna´ndez-Rivera J, Garcı´a R, Lozano F, et al. Relationship between low bone mineral density and highly active antiretroviral therapy including protease inhibitors in HIV-infected patients. HIV Clin Trials. 2003;4:337–46.
18. Grund B, Peng G, Gibert CL, et al. INSIGHT SMART Body Composition Substudy Group. Continuous antiretroviral therapy decreases bone mineral density.AIDS. 2009;23:1519–29.
19. Anastos K, Lu D, Shi Q, et al. The association of bone mineral density with HIV infection and antiretroviral treatment in women. Antiviral Therapy. 2007;12:1049-58.
20. Stelbrink HJ, Orkin C, Arribas JR, et al. Comparison of change in bone density and turn over with Abacavir-Lamivudin versus Tenofovir-Emtricitabine in HIV-infected adult : 48-week result from the ASSERT study. CID. 2010;51:963-72.
21. Young B, Dao CN, Buchacz K, Baker R, Brooks JT. Increased rate of bone fracture among HIV-infected person in the HIV outpatient study(HOPS) compare with the US general population, 2000-2006. CID 2010;52:1061-8.
22. Bruera D, Luna N, David DO, Bertoglio LM, Zamudio J, Decrease bone mineral density in HIV-infected patients is independent of antiretroviral therapy. AIDS. 2003;17:1917-23.
23. Setyohadi B, Mulansari NA, Sukamana N. Reduced bone mineral density and serum C-telopeptide concentration in Cipto Mangunkusumo Hospital. Acta Med Indones - Indones J Intern Med. 2009;41(4):191-4.
24. Srivastava M, Deal C. Osteoporosis in elderly: prevention and treatment. Clin Geriatr Med. 2002;18:529-55.
25. Haskelberg H, Carr A, Emery S. Bone turnover markes in HIV disease. AIDS Rev. 2011;13:240-50.