Facial Pain, Cervical Pain, and Headache Cedars-Sinai, 444 ... Pain.pdf · Facial Pain, Cervical...
14
Facial Pain, Cervical Pain, and Headache Steven B. Graff-Radford, DDS ABSTRACT Purpose of Review: This review discusses the role of musculoskeletal structures of the jaw and neck in perpetuating or triggering primary headache. Because treat- ments aimed at these structures often reduce headache, a better understanding of their role in headache is needed. Recent Findings: Central sensitization may result in changes in the afferent path- ways, making communication from cervical and temporomandibular nociceptive neurons to the trigeminal nucleus possible. This provides the pathophysiologic basis for directing therapy to the neck or temporomandibular joint to alleviate primary headache. Summary: Clinicians should recognize the significant role that musculoskeletal structures of the head and neck play in the perpetuation of headache and the im- portance of evaluating every patient for temporomandibular disorders and cervical abnormalities. Continuum Lifelong Learning Neurol 2012;18(4):869–882. INTRODUCTION Pain presentations in the head and neck may involve neurologic, vascular, and musculoskeletal structures. These structures influence each other, and their interrelationships are not always clear. Many patients have coexisting chronic head, neck, and face pain be- cause of the nociceptive barrage, cen- tral sensitization may account for the referral to distant sites. The close proximity of the trigeminal nucleus and upper cervical afferent pathways may account for the cross-referral from neck to face. As nociceptive inputs become chronic, central neurons are sensitized, reducing the threshold for activation and thereby making the response to afferent stimulation more sensitive, which may cause the recep- tive field to enlarge. Because of this in- terrelationship, individualized care to each pathologic system is necessary. Reviews that have studied the associa- tion between cervical dysfunction and migraine, as well as between cervical dys- function and temporomandibular disor- ders (TMDs), find no clear cause-effect relationship between these disorders. 1,2 TEMPOROMANDIBULAR DISORDERS The relationship between TMD and primary headache is important to under- stand, as treating one may affect the other (Case 9-1). TMD as a collective term may include a number of different clinical entities, including myogenous and arthrogenous components. Pain in the temporomandibular joint (TMJ) may occur in 10% of the US population, and TMD has been reported in 46.1% of the US population. 5,6 Studying the epidemiology of TMD has not allowed the differentiation of headache from fa- cial pain. Very few patients with either clicking or popping or intermittent pain Address correspondence to Dr Steven B. Graff-Radford, The Pain Center at Cedars-Sinai, 444 South San Vicente Boulevard, Suite 1101, Los Angeles, CA 90048, Steven.Graff-Radford @cshs.org. Relationship Disclosure: Dr Graff-Radford serves as a member of the speakers’ bureau or as a consultant for Allergan, Inc.; MAP Pharmaceuticals, Inc.; Nautilus Pharma; NuPathe, Inc.; Pfizer, Inc.; and Zogenix, Inc. Dr Graff-Radford has served as an expert witness and has performed medical record review. Unlabeled Use of Products/Investigational Use Disclosure: Dr Graff-Radford discusses the unlabeled use of amitriptyline, selective serotonin-norepinephrine reputake inhibitors, and antiepileptic drugs for the treatment of temporomandibular disorders. * 2012, American Academy of Neurology. 869 Continuum Lifelong Learning Neurol 2012;18(4):869–882 www.aan.com/continuum Review Article Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Transcript of Facial Pain, Cervical Pain, and Headache Cedars-Sinai, 444 ... Pain.pdf · Facial Pain, Cervical...
Facial Pain, CervicalPain, and Headache
Steven B. Graff-Radford, DDS
ABSTRACTPurpose of Review: This review discusses the role of musculoskeletal structuresof the jaw and neck in perpetuating or triggering primary headache. Because treat-ments aimed at these structures often reduce headache, a better understanding oftheir role in headache is needed.Recent Findings: Central sensitization may result in changes in the afferent path-ways, making communication from cervical and temporomandibular nociceptiveneurons to the trigeminal nucleus possible. This provides the pathophysiologic basisfor directing therapy to the neck or temporomandibular joint to alleviate primaryheadache.Summary: Clinicians should recognize the significant role that musculoskeletalstructures of the head and neck play in the perpetuation of headache and the im-portance of evaluating every patient for temporomandibular disorders and cervicalabnormalities.
Continuum Lifelong Learning Neurol 2012;18(4):869–882.
INTRODUCTIONPain presentations in the head andneck may involve neurologic, vascular,and musculoskeletal structures. Thesestructures influence each other, andtheir interrelationships are not alwaysclear. Many patients have coexistingchronic head, neck, and face pain be-cause of the nociceptive barrage, cen-tral sensitization may account for thereferral to distant sites. The closeproximity of the trigeminal nucleusand upper cervical afferent pathwaysmay account for the cross-referral fromneck to face. As nociceptive inputsbecome chronic, central neurons aresensitized, reducing the threshold foractivation and thereby making theresponse to afferent stimulation moresensitive, which may cause the recep-tive field to enlarge. Because of this in-terrelationship, individualized care toeach pathologic system is necessary.Reviews that have studied the associa-
tion between cervical dysfunction andmigraine, as well as between cervical dys-function and temporomandibular disor-ders (TMDs), find no clear cause-effectrelationship between these disorders.1,2
TEMPOROMANDIBULARDISORDERSThe relationship between TMD andprimary headache is important to under-stand, as treating one may affect theother (Case 9-1). TMD as a collectiveterm may include a number of differentclinical entities, including myogenousand arthrogenous components. Pain inthe temporomandibular joint (TMJ)may occur in 10% of the US population,and TMD has been reported in 46.1%of the US population.5,6 Studying theepidemiology of TMD has not allowedthe differentiation of headache from fa-cial pain. Very few patients with eitherclicking or popping or intermittent pain
Address correspondence toDr Steven B. Graff-Radford,The Pain Center atCedars-Sinai, 444 SouthSan Vicente Boulevard,Suite 1101, Los Angeles, CA90048, [email protected].
Relationship Disclosure:Dr Graff-Radford servesas a member of the speakers’bureau or as a consultantfor Allergan, Inc.; MAPPharmaceuticals, Inc.; NautilusPharma; NuPathe, Inc.;Pfizer, Inc.; and Zogenix,Inc. Dr Graff-Radford hasserved as an expert witnessand has performed medicalrecord review.
Unlabeled Use ofProducts/InvestigationalUse Disclosure:Dr Graff-Radford discussesthe unlabeled use ofamitriptyline, selectiveserotonin-norepinephrinereputake inhibitors, andantiepileptic drugsfor the treatment oftemporomandibular disorders.
* 2012, American Academy ofNeurology.
869Continuum Lifelong Learning Neurol 2012;18(4):869–882 www.aan.com/continuum
Review Article
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Case 9-1A 56-year-old woman presented with jaw, neck, and head ache. Pain was localized to the righttemporomandibular joint (TMJ) radiating into the masseter. She described the pain as mostly dull andachywith associated cracking in her jaw joint. At times she had limitedmouth opening and had tomake herjaw click to open. She described this as locking. The pain worsened as the day progressed and causedheadache and neck pain. The pain radiated from the cervical region into the upper shoulder and down theright arm and was associated with a sensation of tingling in her hand. She denied weakness in the upperextremity. The arm pain was described as intermittent, achy, and dull. Headache was described asintermittent with a throbbing quality and with tenderness over the left superficial temporal artery. Noassociated nausea, vomiting, photophobia, or phonophobia was present. When having a headache, shepreferred to be sedentary. She reported that her jaw had made a clicking noise for years, accompaniedby pain that worsened with function such as chewing or talking. She also reported a history of migrainewith aura occurring 1 to 2 times per year. She used four hydrocodone and diazepampills daily. Examinationshowed limited jaw range of motion and pain on palpation over the TMJ. Her neck range of motion waslimited, and movement increased the neck pain and often triggered a headache. The superficial temporalartery was very tender to palpation. Brain MRI was normal; MRI of the neck was positive forfacet arthropathy; and the temporomandibular MRI showed disk displacement without recapture. Furthertesting included erythrocyte sedimentation rate and C-reactive protein, which were normal.
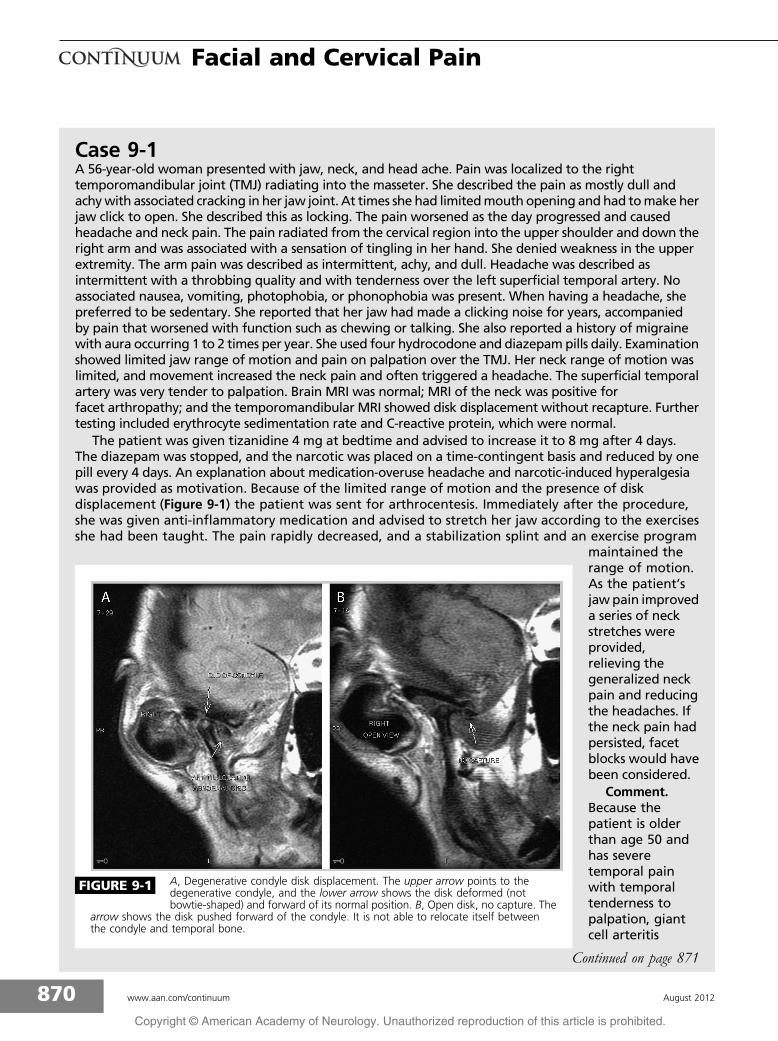
The patient was given tizanidine 4 mg at bedtime and advised to increase it to 8 mg after 4 days.The diazepam was stopped, and the narcotic was placed on a time-contingent basis and reduced by onepill every 4 days. An explanation about medication-overuse headache and narcotic-induced hyperalgesiawas provided as motivation. Because of the limited range of motion and the presence of diskdisplacement (Figure 9-1) the patient was sent for arthrocentesis. Immediately after the procedure,she was given anti-inflammatory medication and advised to stretch her jaw according to the exercisesshe had been taught. The pain rapidly decreased, and a stabilization splint and an exercise program
maintained therange of motion.As the patient’sjaw pain improveda series of neckstretches wereprovided,relieving thegeneralized neckpain and reducingthe headaches. Ifthe neck pain hadpersisted, facetblocks would havebeen considered.
Comment.Because thepatient is olderthan age 50 andhas severetemporal painwith temporaltenderness topalpation, giantcell arteritis
FIGURE 9-1 A, Degenerative condyle disk displacement. The upper arrow points to thedegenerative condyle, and the lower arrow shows the disk deformed (notbowtie-shaped) and forward of its normal position. B, Open disk, no capture. The
arrow shows the disk pushed forward of the condyle. It is not able to relocate itself betweenthe condyle and temporal bone.
Continued on page 871
870 www.aan.com/continuum August 2012
Facial and Cervical Pain
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
require treatment. It is estimated that75% of the population has a sign orsymptom during their lifetime, butfewer than 5% need therapeutic inter-vention. Because both headache andTMD are so common, they may bereported as unified or separate entities.The TMJ and associated orofacial struc-tures can be considered as triggeringor perpetuating factors for migraine.Ciancaglini and Radaelli7 report thatheadache occurs significantly more fre-quently in patients with TMD symptoms(27.4% versus 15.2%). Ignoring the TMJ,muscles, or other orofacial structures asperipheral triggers of headache willoften result in a poor clinical outcome.The trigeminal nerve is the final conduitof face, neck, and head pain.8 Manage-ment of pain in the first division may beinfluenced by therapy aimed at struc-tures innervated by the second or thirdtrigeminal divisions.
EtiologyInflammation within the joint accountsfor TMD pain, and the dysfunction iscaused by a disk-condyle incoordina-tion. The etiology for TMD may includeparafunctional behaviors, macrotrau-mas or microtraumas, changes in theocclusion, and behavioral influences.Treatments aimed at the occlusion andmasticatory system have been success-
ful at treating the headache associatedwith TMD. However, the cause-and-effect relationship remains unknown.Randomized controlled trials in whichheadache is treated by modifying theocclusion show no scientific supportfor this treatment. A literature meta-analysis does not support occlusion asa factor in headache etiology. Sensoryinnervation of the TMJ is mediatedthrough the mandibular division ofthe trigeminal nerve. Pain-sensitiveelements within the TMJ include thejoint capsule, the posterior attachmenttissues, and the discal ligaments. Theposterior attachment is highly inner-vated, richly vascularized, and frequentlyimplicated in the pathophysiology ofjoint pain. In contrast, the intraarticulardisk is largely devoid of neural orvascular tissue but plays a vital role inmaintaining condylar stability duringmandibular movement.
Trauma to the TMJmay result in acutecapsulitis, but this inflammatory processtends to resolve quickly without com-plication. Chronic joint disorders aremore frequently associated with pain-ful derangement of the TMJ. Articulardisk displacement frequently underliesthe mechanism of joint derangement,but the etiology is unclear. The remark-able adaptive capacity of the TMJ is welldocumented.8 Failure of this mecha-nism may lead to tissue destruction
KEY POINTS
h Because both headacheand temporomandibulardisorder are common,they may be reported asunified or separateentities.
h Inflammation withinthe temporomandibularjoint accounts fortempomandibulardisorder pain; thedysfunction is causedby disk-condyleincoordination.
h A literature meta-analysisprovides no support forocclusion as a factor inheadache etiology.
should be considered. Giant cell arteritis (International Classification of Headache Disorders, SecondEdition 6.4.1)3 should be suspected in patients older than 50 years who present with persistentheadache centered on one or both temples that worsens with cold temperatures and is associated withjaw claudication. The examination may reveal an enlarged, tender temporal artery. Laboratoryinvestigation should include erythrocyte sedimentation rate and/or C-reactive protein.4 A temporalartery biopsy may be required to confirm the presence of giant cells. Treatment is usually withcorticosteroids and is urgent because blindness secondary to granulomatous occlusion of the vesselsmay be rapid. This case illustrates the need to be aware that patients with primary headache may behelped by being aware of the role temporomandibular disorders and cervical abnormalities may play inperpetuating or triggering headache.
Continued from page 870
871Continuum Lifelong Learning Neurol 2012;18(4):869–882 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
and disk displacement and may be af-fected by age, stress, sex, systemic ill-ness, and previous trauma. However,acute and chronic disk displacement isnot always painful.
The TMJ has a bilateral location,with an upper and lower compartmentseparated by a fibrocartilaginous disk.This diarthrodial structure allows forboth rotatory and translational move-ment of the mandible. Although theTMJ is subject to the same pathologicdisorders that affect other synovialjoints, it is unique in certain anatomicaspects. Both joints move as a func-tional unit and are lined by a fibrousconnective tissue that is more resistantto degenerative change and has agreater capacity for repair. The masti-catory system includes the articulationof the upper and lower dentition thatmay limit or support joint function andstability. Major components of TMDare joint noise and incoordination ofthe disk-condyle relationship, whichpresents as noise in the joint with orwithout locking or the inability to openwith a normal range of motion. Thiscondition is often referred to as an in-
ternal derangement. Known as a diskderangement disorder, articular diskdisplacement is the most common tem-poromandibular arthropathy and ischaracterized by an abnormal relation-ship or misalignment of the articulardisk relative to the condyle.9 It is clas-sified as disk displacement with reduc-tion or disk displacement withoutreduction (Table 9-1 and Table 9-2).10
In disk displacement with reduction,during mouth opening, the disk thatbegins in a misplaced position reducesor improves its structural relationshipwith the condyle. As it reduces, a soundoften described as clicking or poppingis heard. When themouth closes, a sec-ond sound called a reciprocal click maybe audible as the disk moves off thecondyle just before the teeth cometogether. Usually the closing noise is ofless magnitude. Clicking sounds arenot necessarily a sign of degenerationor an indication for treatment. Morethan one-third of an asymptomatic sam-ple can have moderate to severe de-rangement as seen on imaging,11 andas many as 25% of clicking joints shownormal or slightly displaced disks.12
KEY POINTS
h The right and lefttemporomandibularjoints move as afunctional unit and arelined by a fibrousconnective tissue that ismore resistant todegenerative changeand has a greatercapacity for repair.
h Articular diskdisplacement is themost commontemporomandibulararthropathy and ischaracterized by anabnormal relationshipor misalignment of thearticular disk relative tothe condyle.
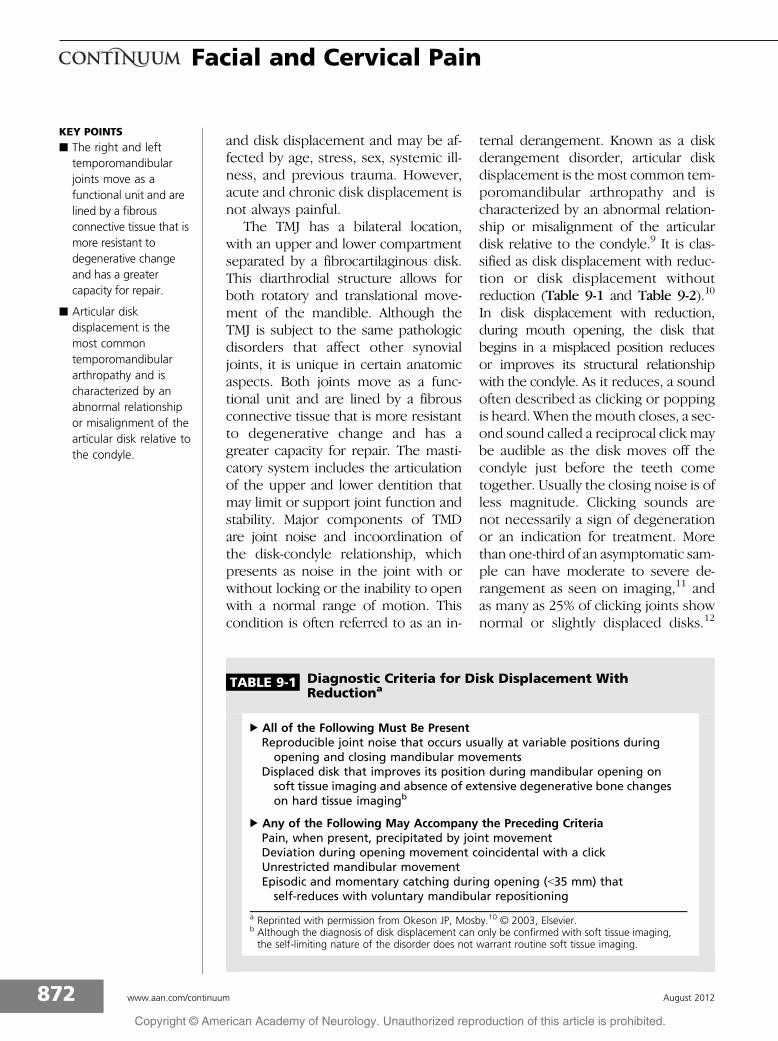
TABLE 9-1 Diagnostic Criteria for Disk Displacement WithReductiona
b All of the Following Must Be PresentReproducible joint noise that occurs usually at variable positions duringopening and closing mandibular movements
Displaced disk that improves its position during mandibular opening onsoft tissue imaging and absence of extensive degenerative bone changeson hard tissue imagingb
b Any of the Following May Accompany the Preceding CriteriaPain, when present, precipitated by joint movementDeviation during opening movement coincidental with a clickUnrestricted mandibular movementEpisodic and momentary catching during opening (G35 mm) thatself-reduces with voluntary mandibular repositioning
a Reprinted with permission from Okeson JP, Mosby.10 B 2003, Elsevier.b Although the diagnosis of disk displacement can only be confirmed with soft tissue imaging,the self-limiting nature of the disorder does not warrant routine soft tissue imaging.
872 www.aan.com/continuum August 2012
Facial and Cervical Pain
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Asymptomatic clicking does not requiretreatment.
A disk displacement without reduc-tion, also referred to as a closed lock,occurs when the out-of-place disk re-mains out of place during movementof the mandible. This is usually associ-ated with limited range of motion.
Myofascial PainFrequently pain associated with TMDis muscular in origin. The most com-mon diagnosis is myofascial pain. Char-acterized by a regional muscle pain,myofascial pain has been described asdull or achy and is associated with thepresence of trigger points in muscles,tendons, or fascia.13Y17 It is a commoncause of persistent regional pain in-volving the neck, shoulder, head, andorofacial regions. Although the preciseetiology of myofascial pain is unclear,it may be associated with stress andoral habits (developmental factors) orpoor sleep, postural abnormalities, anddepression (perpetuating factors).18,19
The major characteristics of myofascialpain include trigger points in musclesand local and referred pain. The trig-ger points may present clinically asactive or latent. When active, digitalpalpation produces pain referral to adistant site. When latent, local tender-ness to palpation may be present, butno distant referral occurs. Myofascialpain is not confined to a single derma-tomal, myotomal, or visceral divisionbut may expand beyond these limits.Clinically, the tender points appear intensemuscles in which active or passivestretching produces increased painassociated with decreasedmotion. Max-imal pain is produced when the muscleis contracted against fixed resistance.Clinical examination reveals a nodularor ropelike band under the skin that isassociated with the tender points. Pal-pation may result in a visible move-ment by the patient called a jumpssign.20 Moving the fingers over thenodule in a direction opposite to themuscle fiber orientation may elicit a
KEY POINTS
h Asymptomatic clickingdoes not requiretreatment.
h Frequently painassociated withtemporomandibulardisorder is muscular inorigin.
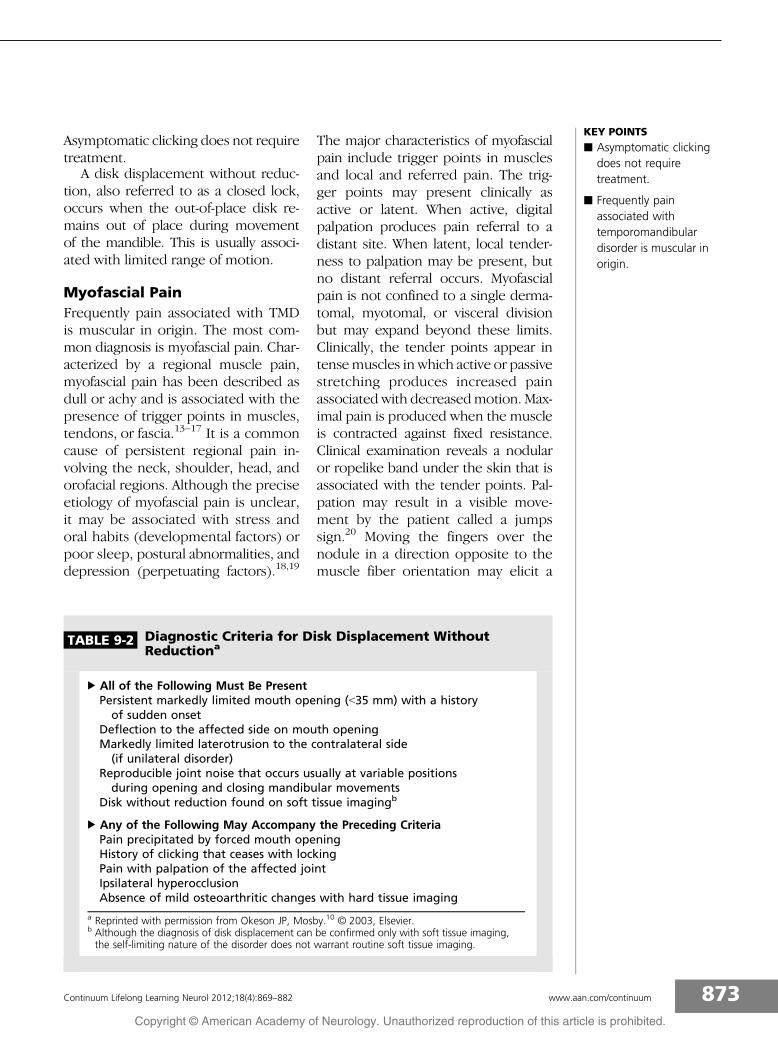
TABLE 9-2 Diagnostic Criteria for Disk Displacement WithoutReductiona
b All of the Following Must Be PresentPersistent markedly limited mouth opening (G35 mm) with a historyof sudden onset
Deflection to the affected side on mouth openingMarkedly limited laterotrusion to the contralateral side(if unilateral disorder)
Reproducible joint noise that occurs usually at variable positionsduring opening and closing mandibular movements
Disk without reduction found on soft tissue imagingb
b Any of the Following May Accompany the Preceding CriteriaPain precipitated by forced mouth openingHistory of clicking that ceases with lockingPain with palpation of the affected jointIpsilateral hyperocclusionAbsence of mild osteoarthritic changes with hard tissue imaging
a Reprinted with permission from Okeson JP, Mosby.10 B 2003, Elsevier.b Although the diagnosis of disk displacement can be confirmed only with soft tissue imaging,the self-limiting nature of the disorder does not warrant routine soft tissue imaging.
873Continuum Lifelong Learning Neurol 2012;18(4):869–882 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
twitch called the twitch response. Thepain is elicited in a characteristic patternspecific for each muscle. The referredpain may be accompanied by referredtenderness thatmay initiate furthermus-cle pain and satellite trigger points.
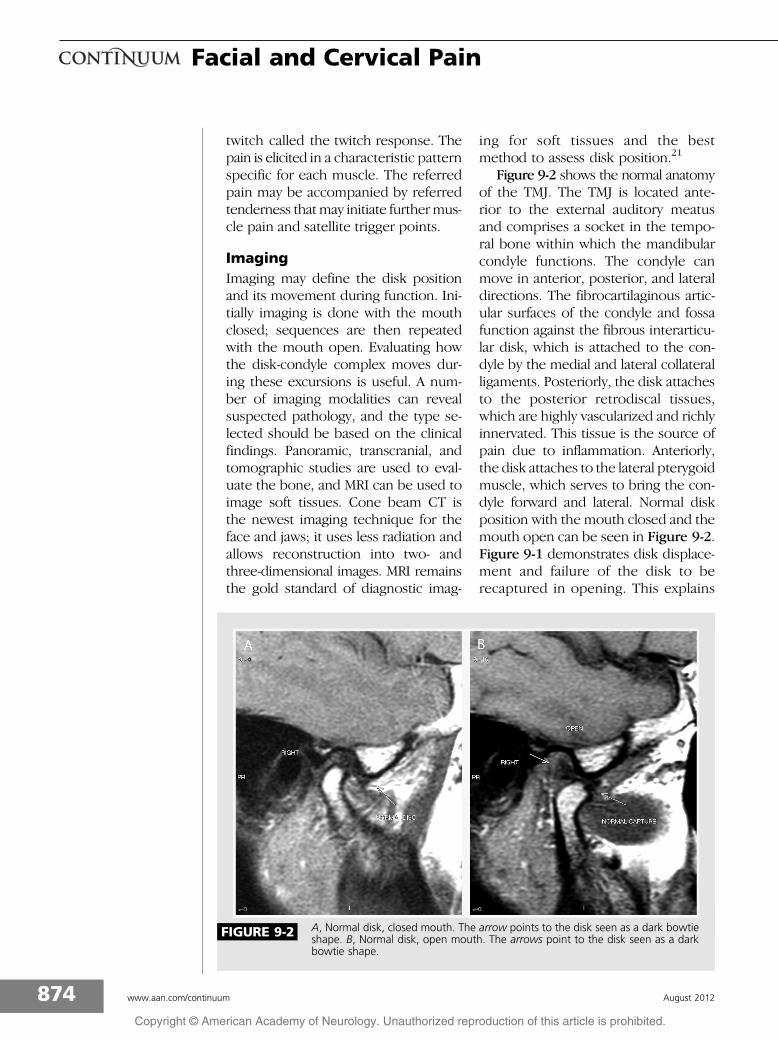
ImagingImaging may define the disk positionand its movement during function. Ini-tially imaging is done with the mouthclosed; sequences are then repeatedwith the mouth open. Evaluating howthe disk-condyle complex moves dur-ing these excursions is useful. A num-ber of imaging modalities can revealsuspected pathology, and the type se-lected should be based on the clinicalfindings. Panoramic, transcranial, andtomographic studies are used to eval-uate the bone, and MRI can be used toimage soft tissues. Cone beam CT isthe newest imaging technique for theface and jaws; it uses less radiation andallows reconstruction into two- andthree-dimensional images. MRI remainsthe gold standard of diagnostic imag-
ing for soft tissues and the bestmethod to assess disk position.21
Figure 9-2 shows the normal anatomyof the TMJ. The TMJ is located ante-rior to the external auditory meatusand comprises a socket in the tempo-ral bone within which the mandibularcondyle functions. The condyle canmove in anterior, posterior, and lateraldirections. The fibrocartilaginous artic-ular surfaces of the condyle and fossafunction against the fibrous interarticu-lar disk, which is attached to the con-dyle by the medial and lateral collateralligaments. Posteriorly, the disk attachesto the posterior retrodiscal tissues,which are highly vascularized and richlyinnervated. This tissue is the source ofpain due to inflammation. Anteriorly,the disk attaches to the lateral pterygoidmuscle, which serves to bring the con-dyle forward and lateral. Normal diskposition with the mouth closed and themouth open can be seen in Figure 9-2.Figure 9-1 demonstrates disk displace-ment and failure of the disk to berecaptured in opening. This explains
FIGURE 9-2 A, Normal disk, closed mouth. The arrow points to the disk seen as a dark bowtieshape. B, Normal disk, open mouth. The arrows point to the disk seen as a darkbowtie shape.
874 www.aan.com/continuum August 2012
Facial and Cervical Pain
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
locking. Understanding the pathophysi-ology is important, as it will alter thetreatment.
CERVICOGENIC PAINWhile cervical pain has been describedin many primary headaches, some arecaused by cervical pathology. The po-tential for cervical dysfunction to causeheadache is recognized under the clas-sification of cervicogenic headache(Table 9-3), and the pain typicallymanifests within the dermatomes ofthe trigeminal and upper cervical (C2,C3) nerves.3 Cervical structures thatinnervate the trigeminocervical com-plex or nucleus include the C1-C3 nerveroots and their branches, the occiput-C3 joints, the alar and transverseligaments, the prevertebral and post-vertebral muscles, the trapezius, thesternocleidomastoid muscles, the cer-vical dura mater, and the vertebral andcarotid arteries.1,22Y24
EpidemiologyEstimates of the prevalence of cervi-cogenic headache range from 0.4%
to 2.5% of the general population andincrease to 15% to 20% in a populationwith chronic headache. Cervicogenicheadaches affect women more oftenthan men in a 4:1 ratio. The averageage of patients with cervicogenic head-ache is in the forties.25
PathogenesisDiseases or dysfunctions of the cervi-cal region may cause pain when thepathology involves pain-sensitive struc-tures that refer in a physiologicallybased pattern. The local pain-sensitivestructures include the facet joints, peri-osteum, ligaments, muscles, cervicalnerve roots and nerves, and the verte-bral arteries.26Y28 Cervical causes ofheadache include developmental anom-alies of the craniovertebral junction andupper cervical spine, tumors, Paget dis-ease, osteomyelitis, rheumatoid arthritis,ankylosing spondylitis, retropharyngealtendonitis, and cervical dystonias. Cer-vical spina bifida does not cause head-ache unless it is associated with otheranomalies, such as Chiari malforma-tions. Cervical disk disease is commonbut is not usually accepted as a cause
KEY POINTS
h The potential for cervicaldysfunction to manifestas headache isrecognized under theclassification ofcervicogenic headache.The pain is typicallyperceived within thedermatomes of thetrigeminal and uppercervical (C2, C3) nerves.
h Diseases or dysfunctionsof the cervical regionmay cause pain whenthe pathology involvespain-sensitive structuresthat refer in aphysiologicallybased pattern.
h The structures knownto cause pain includethe facet joints,periosteum, ligaments,muscles, cervical nerveroots and nerves, andvertebral arteries.
TABLE 9-3 International Classification of Headache Disorders,Second Edition, Criteria for Cervicogenic Headachea,b
Diagnostic Criteria:A. Pain referred from a source in the neck and perceived in one or more
regions of the head and/or face, fulfilling criteria C and D.B. Clinical, laboratory, and/or imaging evidence of a disorder or lesion within
the cervical spine or in the soft tissues of the neck known to be, orgenerally accepted as, a valid cause of headache.
C. Evidence that the pain can be attributed to the neck disorder or lesion,based on at least one of the following criteria:1. Demonstration of clinical signs that implicate a source of pain in the neck.2. Abolition of headache following diagnostic blockade of a cervical
structure or its nerve supply using placebo or other adequate controls.D. Pain resolves within 3 months after successful treatment of the causative
disorder or lesion.
a Previously used terms for cervicogenic headache include cervical headache and headacheattributed to disorder of the cervical spine.
b Adapted from Headache Classification Subcommittee of the International Headache Society,Cephalalgia.3 B 2004, with permission from SAGE. cep.sagepub.com/content/24/1_suppl/9.long.
875Continuum Lifelong Learning Neurol 2012;18(4):869–882 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
of headache. Should they be impli-cated, herniations involving the uppercervical segments (C1-C3) would beexpected. Another controversial causeof headache is cervical whiplash injury.Pain is usually self-limiting, resolvesin weeks, and is likely due to injury ofligaments and muscles. Evidence dem-onstrates that chronic pain in this set-ting may be secondary to shearing oflong axons in the brainstem and uppercord that causes centrally mediatedpain and headache.29Y31 Sjaastad andBovim32 have suggested that patientswith cervicogenic headache report afairly uniform headache profile, withthe implication that the pain emanatesfrom cervical structures. They empha-size that this is not a disease but rathera reaction pattern. The profile they de-scribe includes (1) unilaterality begin-ning in the neck and radiating to theoculofrontal area, (2) moderate non-throbbing pain, intermittent or contin-uous, and provoked by neckmovementor sustained awkward postures, (3) non-
radicular pattern, (4) reduced rangeof motion in the cervical spine, (5) pre-dominantly female, (6) history of trauma,and (7) transient relief with cervicalblock or C2 root block. Other migraine-associated symptoms or autonomic fea-tures are not necessary.32,33
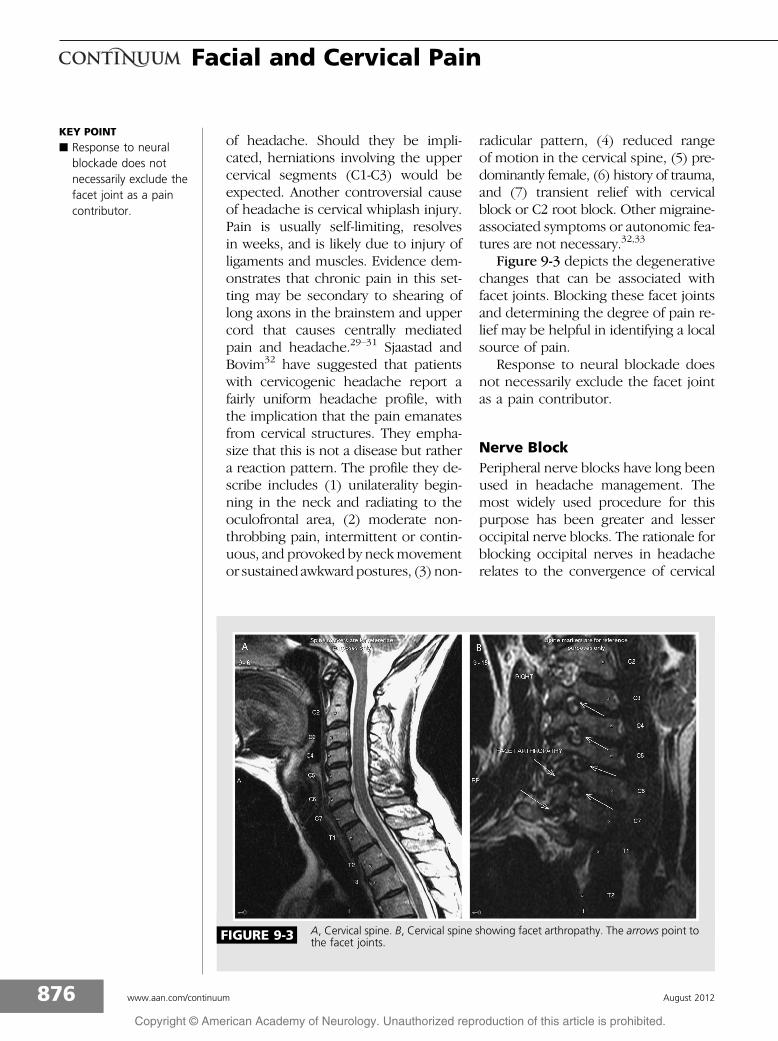
Figure 9-3 depicts the degenerativechanges that can be associated withfacet joints. Blocking these facet jointsand determining the degree of pain re-lief may be helpful in identifying a localsource of pain.
Response to neural blockade doesnot necessarily exclude the facet jointas a pain contributor.
Nerve BlockPeripheral nerve blocks have long beenused in headache management. Themost widely used procedure for thispurpose has been greater and lesseroccipital nerve blocks. The rationale forblocking occipital nerves in headacherelates to the convergence of cervical
KEY POINT
h Response to neuralblockade does notnecessarily exclude thefacet joint as a paincontributor.
FIGURE 9-3 A, Cervical spine. B, Cervical spine showing facet arthropathy. The arrows point tothe facet joints.
876 www.aan.com/continuum August 2012
Facial and Cervical Pain
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

and trigeminal fibers in the trigeminalnucleus caudalis. The region aroundthe nerve is usually infiltrated with alocal anesthetic (lidocaine, bupivacaine,or both), and a corticosteroid is some-times added. Several studies suggestthe efficacy of greater and lesser occipi-tal nerve block in the treatment of mi-graine, cluster headache, and chronicdaily headache. However, few of thosestudies are controlled and blinded.34
Cervical nerve root blocks have beenperformed since the late 19th century,and with the improvement of imag-ing, the procedure has been increasingin popularity over the past decade.35,36
Cervical nerve root blocks are used tomanage or treat spinal pain, radicularpain, and complex regional pain syn-dromes. Such blocks are usually per-formed in outpatient clinics, with orwithout imaging guidance such as fluo-roscopy or CT.
Diagnostic and therapeutic selectivenerve root blocks may be useful in thediagnosis of patients with headacheand radiculopathy. A reduction in painafter nerve block with local anestheticmay indicate the irritated root is causingthe headache. Using local anestheticselective nerve root blocks, Perssonand colleagues37 concluded that a directrelationship exists between degenera-tive change causing nerve root compres-sion in the upper and lower cervicalspine and headache.
It is common for cervical facet orzygapophyseal joint pathology to con-tribute to neck pain; therefore, man-agement with intraarticular injections,blocking the medial branches that in-nervate the joint, or performing medialbranch neurolysis may successfully re-duce chronic neck pain.
Neural RadiofrequencyProceduresA review of the literature on interven-tions aimed at the facet shows benefit
that may vary in duration.38 Boswelland colleagues38 concluded that therewas moderate evidence for neurotomyin short-term and long-term outcome,whereas the blocks alone producedlittle, if any, long-term benefit.
Physical TherapyCervical manipulation and mobiliza-tion have been evaluated for headachemanagement in several systematic re-views, case series, and controlled stud-ies. Mobilization and manipulationare similar terms that are frequentlyused interchangeably in the literature.Both terms refer to passive movementtechniques used to restore normal mo-tion to a joint. Manipulation occurswhen a high velocity thrust is appliedat the end range of motion. Mobiliza-tion implies passive movement, usuallyrhythmic in nature, that varies in am-plitude but never exceeds the joint’snormal motion.39 A Cochrane DatabaseReview40 reported high-quality evi-dence for manipulation in the man-agement of migraine compared withamitriptyline. Generally the literaturedoes not support cervical manipula-tion for the prevention or acute careof migraine.41Y43 The mobilization ofthe upper cervical joint using differenttechniques seems to be relatively safeand helpful for cervical headache, butthe small sample size (10 patients) andlength of follow-up (only 4 weeks) arelimitations of the study. Great cautionshould be exercised in providing mobi-lization, and in particular manipulation,because in rare cases stroke and verte-bral artery dissection may occur.
More than 100 cases of serious com-plications from chiropractic manipula-tion have been reported, and it can beassumed that a fairly large number ofsimilar complications go unreported.44
The potential serious complicationsare increased risk of vertebral arterydissection and approximate sixfold
KEY POINT
h Great caution should beexercised in providingmobilization, and inparticular manipulation,because in rare casesstroke and vertebralartery dissection mayoccur.
877Continuum Lifelong Learning Neurol 2012;18(4):869–882 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

increase in stroke or TIA. It is appro-priate to inform patients about thesepotentially serious complications of cer-vical chiropractic manipulation.
MANAGEMENT OFTEMPOROMANDIBULARDISORDERSThe biggest gap in TMD-headachestudies is the lack of clear diagnosis.Further, it is uncertain whether thecause of headache can be connectedto or correlated with TMD if treatingthe TMD reduces the headache. It isclear that primary headache is a CNSissue and that treating an existing TMDin the presence of primary headachemay reduce the pain intensity and fre-quency. This, however, should not bemisconstrued as cause and effect. Thefive basic areas considered in TMD ther-apy are summarized in Table 9-4.
Patient Education and Self-CareIt is essential to keep inmind that TMDsare self-limiting. Because the TMJ iscovered with fibrocartilaginous mate-rial, it has the propensity to remodel. Inmost patients, the disorder will resolvewithin 7 years.45,46 Typically, patients re-spond to conservative, noninvasive in-tervention unless nonreducing diskdisplacements are limiting function. Thisexplanation lessens patient fear of thedisorder. Patients should be instructed
to avoid chewy foods, especially chew-ing gum. They can be taught to avoidclenching their jaws during the day, toapply heat or ice, and to perform jaw-stretching exercises.
Cognitive-BehavioralInterventionsBehavioral modification of maladaptivehabits is an important component inthe management of TMD. This may beaccomplished with simple exercises orwith the help of a structured programfacilitated by a specialist in behavioralmodification. This type of programmay include lifestyle counseling, pro-gressive relaxation, biofeedback, andhypnosis. Treatments should be indi-vidualized to the patient.47
Pharmacologic TherapyPharmacologycanpromotepatient com-fort and healing when it is incorporatedas part of a comprehensive therapy. ForTMD, the most common medicationsinclude nonsteroidal anti-inflammatorydrugs and muscle relaxants. The useof tricyclic antidepressants, selectiveserotonin-norepinephrine reuptake in-hibitors, and antiepileptic drugs are alsoimportant in pain management.48
Physical TherapiesPhysical therapies include posture train-ing, exercise, joint mobilization, and
KEY POINT
h Temporomandibulardisorders areself-limiting.
TABLE 9-4 Basic Principles of Management of TemporomandibularDisorders
b Patient education and self-careb Cognitive-behavioral interventionsb Pharmacologic management (eg, analgesics, nonsteroidal
anti-inflammatory drugs, muscle relaxants, sedatives, and antidepressants)b Physical therapies (eg, posture training, stretching exercises, mobilization,
physical modalities, appliance therapy, and occlusal therapy)b Surgery
878 www.aan.com/continuum August 2012
Facial and Cervical Pain
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

the use of physical agents or modalities.The goal is to reduce the pain and simul-taneously improve the joint movementby altering nociceptive input, reducinginflammation, decreasing coordinatingand strengthening muscle activity, andallowing regeneration of tissues. InCase 9-1, physical therapy and appli-ance therapy were initiated and wererecommended because of the lockingand arthrocentesis. The patient wasasked to continue with her stabilizationappliance, and stretching exerciseswere provided along with the use of avapocoolant spray to maintain the gainsafter arthrocentesis.
The type of splint used in TMD iscontroversial. Fricton and colleagues49
reviewed 42 studies involving intraoralsplints. Generally, in patients with moresevere TMDs, splints are beneficial inrelieving TMD pain compared with pla-cebo, and stabilization splints are themost effective with the least potentialfor adverse effects. Because many dif-ferent splint designs are available, asummary of the conclusions from thisreview will provide a guideline for splintuse.
In severe TMDs, stabilization splints(splints that cover all maxillary or man-dibular teeth, do not alter the jaw pos-ition, and are worn at night only) reduceTMD pain when compared with non-occluding splints. Studies of headacheswith specific diagnoses are limited, anddefinitive conclusions cannot be con-firmed.When compared to physicalmedi-cine techniques, cognitive-behavioraltherapies, and acupuncture, stabiliza-tion appliances are equivalent. Onestudy claims that splint therapy maybe better than pharmacotherapy.50
Evidence shows that anterior posi-tioning splints (hard splints that coverall the maxillary and mandibular teethand hold the lower jaw in a forwardposition) and soft splints (splints thatcover all the maxillary and mandibular
teeth and hold the lower jaw in a for-ward position) reduce TMD when com-pared with placebo.
Anterior positioning splints areequally or more effective than stabili-zation splints in the management ofTMJ clicking and locking. The use ofthese appliances may lead to occlusalchanges, so they should be used withcaution.
Compared with stabilization appli-ances, there is no evidence supportingthe use of anterior bite planes, such asthe nociceptive trigeminal inhibitionreflex device (NTI) (a hard splint thatcovers only the central incisors on themaxilla and central and lateral incisorson the bottom, holding the mandibleforward), in headache. Potential sideeffects, including swallowing, possibleaspiration, tooth movement, and bitechange, make this splint undesirable. Acomprehensive review of controlledtrials by Stapelmann and Turp51 con-cluded that the NTI might be usefulin TMD and bruxism, but the potentialnegatives should be carefully consid-ered. Despite the evidence that splinttherapy is useful, splints should not beused in isolation but rather as part of anintegrated therapy program.52
Occlusal adjustment was once con-sidered beneficial for TMD; however, noevidence supports its use. A CochraneDatabase review53 and other system-atic reviews concluded that evidence isinsufficient to support ongoing use of oc-clusal adjustment as a treatment of TMD.
Miscellaneous physical therapies.Electrotherapy. Electrotherapy is pos-tulated to modify muscle hyperactivityand tissue swelling, change circula-tion, and reduce trigger point activity.Electrogalvanic stimulation uses a high-voltage, low-amperage, monophasiccurrent of varied frequency. The use oftranscutaneous electrical nerve stimula-tion (TENS) in the head is controversialfor the fear of creating epileptogenic
879Continuum Lifelong Learning Neurol 2012;18(4):869–882 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
effects. TENS uses a low-voltage, low-amperage, biphasic current of variedfrequency and is designed primarily forsensory counterstimulation in painfuldisorders. Little evidence is available forits effectiveness in the head.
Ultrasound. When transmittedthrough the tissue with a high-frequencyoscillating transducer head, ultrasoundproduces heat that can reach a depthof 5 cm. It is a frequently used physicaltreatment modality for musculoskeletalproblems. When used to deliver medi-cation into the tissue, the process iscalled phonophoresis, although themechanism and efficacy of drug deliv-ery are unknown.
Iontophoresis. Iontophoresis is atechnique to enhance the transportof drug ions across the skin into thedeeper tissue using a weak current. Re-cent studies question the efficacy of thismodality to provide pain relief.
Laser treatment. Low-level laser ther-apy may have biostimulating (biostim-ulation involves the modification ofthe environment to stimulate existingtissue capable of bioremediation) andanalgesic effects through direct irradia-tionwithout causing a thermal response.Several studies investigating the efficacyof laser therapy in TMDs are inconclu-sive because of poor methodology orsmall sample size. Further research isneeded to support the use of low-levellaser therapy in TMD treatment.
Surgery. TMJ surgery is effective forspecific articular disorders and may in-clude arthrocentesis, arthroscopy, ar-throtomy, and joint replacement. Mostpatients respond to simple intraarticularirrigation with or without steroids. Thisprocedure is effective in patients withacute closed lock and will likely resultin improved range of motion. It canalso be used for patients with degen-erative arthritides. In patients withdisk displacement, arthrocentesis canbe helpful.
REFERENCES1. Robertson BA, Morris ME. The role of cervical
dysfunction in migraine: a systematic review.Cephalalgia 2008;28(5):474Y483.
2. Olivo SA, Bravo J, Magee DJ, et al. Theassociation between head and cervicalposture and temporomandibular disorders:a systematic review. J Orofac Pain2006;20(1):9Y23.
3. Headache Classification Subcommittee ofthe International Headache Society. TheInternational Classification of HeadacheDisorders. 2nd edition. Cephalalgia2004;24(suppl 1):9Y160.
4. Villa-Forte A. Giant cell arteritis: suspect it,treat it promptly. Cleve Clin J Med 2011;78(4):265Y270.
5. LeResche L. Epidemiology oftemporomandibular disorders: implicationsfor the investigation of etiologic factors.Crit Rev Oral Biol Med 1997;8(3):291Y305.
6. Glass EG, McGlynn FD, Glaros AG, et al.Prevalence of temporomandibular disordersymptoms in a major metropolitan area.Cranio 1993;11(3):217Y220.
7. Ciancaglini R, Radaelli G. The relationshipbetween headache and symptoms oftemporomandibular disorder in the generalpopulation. J Dent 2001;29(2):93Y98.
8. Piovesan EJ, Kowacs PA, Tatsui CE, et al.Referred pain after painful stimulation ofthe greater occipital nerve in humans:evidence of convergence of cervicalafferences on trigeminal nuclei.Cephalalgia 2001;21(2):107Y109.
9. Scapino RP. The posterior attachment: itsstructure, junction, and appearance inTMJ imaging studies. Part 1. J CraniomandibDisord 1991;5(2):83Y95.
10. Okeson JP.Managementof temporomandibulardisorders and occlusion. 5th edition.St. Louis, MO: Mosby, 2003.
11. Kircos LT, Ortejndayhl DA, Mark AS,Arakawa M. Magnetic resonance imagingof the TMJ disc in asymptomatic volunteers.J Oral Maxillofac Surg 1987;45(10):852Y854.
12. Devant YTSI, Greene CS, Perry HT,Lautenschlager EP. A quantitativecomputer-assisted analysis of the discdisplacement in patients with internalderangement using sagittal view magneticresonance imaging. J Oral MaxillofacSurg 1993;51(9):974Y979.
13. Rivner MH. The neurophysiology ofmyofascial pain syndrome. Curr PainHeadache Rep 2001;5(5):432Y440.
880 www.aan.com/continuum August 2012
Facial and Cervical Pain
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

14. Gerwin RD. Classification, epidemiology,and natural history of myofascial painsyndrome. Curr Pain Headache Rep2001;5(5):412Y420.
15. Simons DG, Travell JG, Simons LS. The triggerpoint manual, vol 1. 2nd ed. Baltimore, MD:Lippincott Williams & Wilkins, 1998.
16. Fricton JR. Masticatory myofascial pain:an explanatory model integrating clinical,epidemiological and basic science research.Bull Group Int Rech Sci Stomatol Odontol1999;41(1):14Y25.
17. Graff-Radford SB. Myofascial pain: diagnosisand management. Curr Pain HeadacheRep 2004;8(6):463Y467.
18. Fricton JR, Olsen T. Predictors of outcomefor treatment of temporomandibulardisorders. J Orofac Pain 1996;10(1):54Y65.
19. Graff-Radford SB, Reeves JL, Jaeger B.Management of chronic head and neckpain: effectiveness of altering factorsperpetuating myofascial pain. Headache1987;27(4):186Y190.
20. Kraft GH, Johnson EW, LaBan MM. Thefibrositis syndrome. Arch Phys Med Rehabil1968;49(3):155Y162.
21. Emshoff R, Innerhofer K, Rudisch A, et al.Clinical versus magnetic resonance imagingfindings with internal derangement of thetemporomandibular joint: an evaluationof anterior disc displacement withoutreduction. J Oral Maxillofac Surg 2002;60(1):36Y41.
22. Bartsch T, Goadsby P. Increased responses intrigeminocervical nociceptive neurons tocervical input after stimulation of the duramater. Brain 2003;126(pt 8):1801Y1813.
23. Bartsch T, Goadsby PJ. The trigeminocervicalcomplex and migraine: current conceptsand synthesis. Curr Pain Headache Rep2003;7(5):371Y376.
24. Bogduk N. Anatomy and physiology ofheadache. Biomed Pharmacother 1995;49(10):435Y445.
25. Haldeman S, Dagenais S. Cervicogenicheadaches: a critical review. Spine J2001;1(1):31Y46.
26. Bogduk N, Marsland A. The cervicalzygapophysial joints as a source of neckpain. Spine 1988;13(6):610Y617.
27. Bogduk N. Cervicogenic headache: anatomicbasis and pathophysiologic mechanisms.Curr Pain Headache Rep 2001;5(4):382Y386.
28. Bogduk N. The anatomy andpathophysiology of neck pain. Phys MedRehabil Clin N Am 2003;14(3):455Y472.
29. Hawkins GW. Flexion and extension injuriesof the cervicocapital joints. Clin Orthop1962;24:22Y33.
30. Zwart JA. Neck mobility in different headachedisorders. Headache 1997;37(1):6Y11.
31. Weiss RD, Stern BJ, Goldberg J.Post-traumatic migraine: chronic migraineprecipitated by minor head or neck trauma.Headache 1991;31(7):451Y456.
32. Sjaastad O, Bovim G. Cervicogenic headache.The differentiation from common migraine.An overview. Funct Neurol 1991;6(2):93Y100.
33. Sjaastad O. Reliability of cervicogenicheadache diagnosis. Cephalalgia1999;19(9):767Y768.
34. Ashkenazi A, Levin M. Greater occipitalnerve block for migraine and otherheadaches: is it useful? Curr Pain HeadacheRep 2007;11(3):231Y235.
35. Oeppen RS. Discovery of the first localanaestheticVCarl Koller (1857Y1944).Br J Oral Maxillofac Surg 2003;41(4):243.
36. Kozak LJ, DeFrances CJ, Hall MJ. Nationalhospital discharge survey: 2004 annualsummary with detailed diagnosis andprocedure data. Vital Health Stat 2006;13(162):1Y209.
37. Persson LC, Carlsson JY, Anderberg L.Headache in patients with cervicalradiculopathy: a prospective study withselective nerve root blocks in 275 patients.Eur Spine J 2007;16(7):953Y959.
38. Boswell MV, Colson JD, Sehgal N, et al.A systematic review of therapeutic facetjoint interventions in chronic spinal pain.Pain Physician 2007;10(1):229Y253.
39. Schoensee S, Jensen G, Nicholson G, et al.The effect of mobilization on cervicalheadaches. J Orthop Sports Phys Ther1995;21(4):184Y196.
40. Brønfort G, Nilsson N, Haas M, et al.Non-invasive physical treatments forchronic/recurrent headache. CochraneDatabase Syst Rev 2004;(3):CD001878.
41. Biondi DM. Physical treatments forheadache: a structured review. Headache2005;45(6):738Y746.
42. Bronfort G, Assendelft WJ, Evans R, et al.Efficacy of spinal manipulation for chronicheadache: a systematic review. J ManipulativePhysiol Ther 2001;24(7):457Y466.
43. Graff-Radford SB, Mauskop A. Alternativeheadache treatments. In: Standards of carefor diagnosis and treatment of headache.4th edition. Chicago, IL: National HeadacheFoundation, 2004.
881Continuum Lifelong Learning Neurol 2012;18(4):869–882 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
44. Mauskop A. Alternative therapies inheadache. Is there a role? Med ClinNorth Am 2001;85(4):1077Y1084.
45. Apfelberg DB, Lavey E, Janetos G, et al.Temporomandibular joint disease: resultsof a ten year study. Postgrad Med1979;65(5):167Y169, 171Y172.
46. Okeson JP, Hayes DK. Long-term resultsof treatment for temporomandibulardisorders: an evaluation of patients.J Am Dent Assoc 1986;112(4):473Y478.
47. Turner JA, Keefe FJ. Cognitive-Behavioraltherapy for chronic pain. In: Max M, editor.Pain 1999Van updated review. Seattle,WA: IASP Press, 1999:523Y533.
48. Sharav Y, Singer E, Schmidt E, et al. Theanalgesic effect of amitriptyline on chronicfacial pain. Pain 1987;31(2):199Y209.
49. Fricton J, Look JO, Wright E, et al. Systematicreview and meta-analysis of randomizedcontrolled trials evaluating intraoral
orthopedic appliances for temporomandibulardisorders. J Orofac Pain 2010;24(3):237Y254.
50. Schokker RP, Hansson TL, Ansink BJ. Theresult of treatment of the masticatorysystem of chronic headache patients.J Craniomandib Disord 1990;4(2):126Y130.
51. Stapelmann H, Turp JC. The NTI-tssdevice for the therapy of bruxism,temporomandibular disorders, andheadacheVwhere do we stand? Aqualitative systematic review of theliterature. BMC Oral Health 2008;8:22.
52. Dao TT, Lavigne GJ. Oral splints: the crutchesfor temporomandibular disorders andbruxism? Crit Rev Oral Biol Med 1998;9(3):345Y361.
53. Koh H, Robinson PG. Occlusal adjustmentfor treating and preventingtemporomandibular disorders. CochraneDatabase Syst Rev 2003;(1):CD003812.
882 www.aan.com/continuum August 2012
Facial and Cervical Pain
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.