Facial Bones Power Point
14
Facial Bone Radiography A five minute guide to what the radiologist and clinician really need.
-
Upload
zhyema-zhyedee -
Category
Documents
-
view
214 -
download
0
description
test
Transcript of Facial Bones Power Point
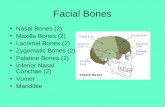
Facial Bones
Facial Bone Radiography
A five minute guide to what the radiologist and clinician really need.
Facial Bone Radiography
Severe trauma to the facial area usually proceeds to CT with 2D and possibly 3D reconstructions.
Facial radiographs remain a useful screening tool for lesser trauma with the advantages of lesser cost and radiation.
If you dont perform these often and are faced with the exam on the night shift dont despair here is your guide.
A good facial bone exam is based primarily on three projections:
Lateral
True Waters
Modified Caldwell
A SMV view is added in some protocols.
The key to a good exam is to take the images correctly and produce the expected view of the anatomy.
THE LATERAL PROJECTION
The lateral view should be taken upright if possible. A cross table lateral without turning the head is the next best choice.
Turning the patients head is not a good plan with acute trauma but, more importantly, a rotated projection can mask clues to a basilar skull fracture and doesnt allow a correct view of the cervical/cranial junction.
Right and Left laterals are not as important as a patient with a suspected skull Fx will get a CT.
This lateral view was taken with the head turned to the side on the table.
An air-fluid level in the sphenoid sinus is a clue to a possible basilar skull fracture which would be missed as the fluid would spread out in the dependant portion of the sinus.
This correctly positioned lateral displays well the relationship of the skull base to the cervical spine.
An air fluid level in the sinuses would be evident.
Another good lateral. Did you note the air-fluid levels in the maxillary sinuses? These can be due to sinusitis but in the setting of acute trauma may be a clue to bleeding and an orbital floor fracture.
THE WATERS VIEW
A waters view by definition should show the entire maxillary sinuses. Faces are different! A common mistake is to plug in a standard angle which ends up being too shallow. If a standard angle does not show the entire sinuses, it should be repeated. This view shows the anterior orbital rims (not the orbital floor) and gives the radiologist a good view of the zygomatic arches, zygomas and orbital roofs. Differentiation between an orbital rim Fx and an orbital floor Fx is important to the clinician.
Correctly positioned Waters. Z=zygoma, OR=orbital rim, ZA= zygomatic arch and ms=maxillary sinus. Note that the entire maxillary sinus is displayed.
THE CALDWELL PROJECTION
The Caldwell view is the only projection to visualize the true orbital floor where blowout fractures and sometimes entrapment of the extraocular muscle occurs. The standard Caldwell will not show the orbital floor well and a modified Caldwell with steeper angle is needed. In most patients, this is around 22 degrees. The ideal projection places the petrous ridges just below the orbital floor.
This standard, 15 degree Caldwell shows the petrous ridges (PR) above the lower orbit and obscures detail of the true orbital floor. It should be repeated with additional angle of around 8 degrees.
Modified Caldwell
This is the anatomic view you want to produce for a good modified Caldwell. A lesser angle obscures the orbital floor and a steeper angle approaches a Waters and shows the orbital rim instead of the floor.
If an orbital floor fracture is found, patients should proceed to CT to evaluate possible muscle entrapment and fragment position. This CT coronal image shows a left orbital floor depressed fracture with entrapment of the inferior rectus muscle. The patient went to surgery to relieve the entrapment and diplopia.
A case can be made for a facial bone protocol using just the previous three well positioned images. Our present protocol also includes a submental vertex view which gives the radiologist an additional look at the zygomatic arches.
GOOD POSITIONING
MAKES EVERYONE HAPPY!