
F07311-Ch17.qxd 6/20/06 10:06 AM Page 32 NOSE AND ... · and sinusitis Foreign body Serosanguineous...
6
NOSE AND PARANASAL SINUSES 32 Symptoms, signs and investigations Symptoms It is vital to establish the precise complaint of the patient; thus, a full history is mandatory (Fig. 1). Nasal obstruction Nasal obstruction is probably the most common symptom, and may be due to anatomical abnormalities, disorders of the mucous membrane lining or stimulation of the autonomic nervous system (Table 1). An allergic aetiology is frequently volunteered by the patient where the symptoms manifest after contract with allergens such as grass pollen, feathers or animal furs. Viral infections, e.g. acute coryza and influenza, cause severe nasal obstruction but generally resolve rapidly over days. An overactivity of the parasympathetic as compared to the sympathetic nerve supply will cause dilatation of the vascular tree and hence engorgement. This is particularly noted by some patients in stress situations and with rupture of a blood vessel in the nasal mucous membrane. However, it is vital to exclude any bleeding disorders and neoplasms. If the discharge is offensive, it may indicate a bacterial infection, the presence of a foreign body or neoplasia. Sneezing Sneezing is a very frequent accompaniment of allergic and infective rhinitis. Commonly, patients with allergies to household dust and dust mite sneeze on awakening, as the bed mattress forms a huge reservoir of these allergens. Facial pressure/pain It is relatively uncommon to see facial pain due to a local cause such as nasal vestibulitis or herpes eruption. More frequently it is related to disease in the distribution of the trigeminal nerve, which supplies the sensory component to the face and the interior of the nose and paranasal sinus via the ophthalmic and maxillary nerves. Consequently, these anatomical sites require detailed examination in such cases (p. 53). Otological Any pathological process that disrupts the proper functioning of the Eustachian tube may give rise to aural symptoms. Nasal polyps, particularly of the antrochoanal variety, can physically block the pharyngeal end of the tube. Allergic diseases result in a similar problem by provoking oedema, and neoplasms may directly invade the Eustachian tube. The most frequent otological symptom is hearing loss caused by a middle ear effusion secondary to Eustachian tube dysfunction. Disorders of smell Anosmia, a total loss of sense of smell, is rare. Hyposmia, a reduced sense of smell, is more common. Cacosmia, which is an unpleasant smell detected mainly by others, may be caused by chronic nasal sepsis. Ozaena, a foul smell, is a common complaint in anaerobic infections seen in cases of atrophic rhinitis, but the presence of a foreign body and tumour must be excluded. Halitosis Poor dental hygiene and poor diet are the most common causes of halitosis. However, chronic sinusitis with purulent postnasal drip can also produce this symptom (p. 51). Signs A comprehensive approach to examination of the nose can only be acquired by practice. It is essential to examine both the exterior and interior of the nose, and also ancillary areas such as the ears and oropharynx. External Certain cosmetic deformities such as angulation of the bony nasal pyramid or a nasal hump may be obvious. A saddle deformity due to previous injury or infection is readily identified, and it is not unusual to find the septal Fig. 1 Symptoms in nasal and paranasal sinus disease. Otological (otalgia, hearing loss, crackling etc.) Facial pressure, discomfort Disorders of smell Halitosis Blockage Discharge Sneezing Postnasal drip alterations in ambient temperature and humidity. Neoplasia produces a progressive obstruction and may cause ocular and dental problems due to contiguous spread. Nasal discharge The specific character of a nasal discharge is very helpful in deciding aetiology (Table 2). Many patients describe this symptom as ‘catarrh’. However, if it produces a runny nose, the discharge should be described as rhinorrhoea and the term ‘catarrh’ (or postnasal drip) reserved for complaints of nasal discharge passing backwards into the nasopharynx. Epistaxis is defined as nasal haemorrhage and is most commonly due to spontaneous Table 1 Causes of nasal obstruction Variety Associated conditions Anatomical Septal deflection Adenoidal hypertrophy Neoplasia Choanal atresia Disorders of nasal lining Allergic and infective rhinitis Nasal polyps Autonomic nervous Vasomotor rhinitis system Table 2 Nasal discharge: its characteristics and significance Character of discharge Associated conditions Watery/mucoid Allergic, infective (viral) and vasomotor rhinitis Cerebrospinal fluid leak Mucopurulent Infective (bacterial) rhinitis and sinusitis Foreign body Serosanguineous Neoplasia Bloody Trauma, neoplasia, bleeding diathesis
Transcript of F07311-Ch17.qxd 6/20/06 10:06 AM Page 32 NOSE AND ... · and sinusitis Foreign body Serosanguineous...

NOSE AND PARANASAL SINUSES32
Symptoms, signs and investigations
Symptoms
It is vital to establish the precise complaint of the patient;thus, a full history is mandatory (Fig. 1).
Nasal obstructionNasal obstruction is probably the most common symptom,and may be due to anatomical abnormalities, disorders of themucous membrane lining or stimulation of the autonomicnervous system (Table 1). An allergic aetiology is frequentlyvolunteered by the patient where the symptoms manifest aftercontract with allergens such as grass pollen, feathers or animalfurs. Viral infections, e.g. acute coryza and influenza, causesevere nasal obstruction but generally resolve rapidly overdays. An overactivity of the parasympathetic as compared tothe sympathetic nerve supply will cause dilatation of thevascular tree and hence engorgement. This is particularlynoted by some patients in stress situations and with
rupture of a blood vessel in the nasalmucous membrane. However, it is vitalto exclude any bleeding disorders andneoplasms. If the discharge is offensive,it may indicate a bacterial infection, thepresence of a foreign body or neoplasia.
SneezingSneezing is a very frequentaccompaniment of allergic andinfective rhinitis. Commonly, patientswith allergies to household dust anddust mite sneeze on awakening, as thebed mattress forms a huge reservoir ofthese allergens.
Facial pressure/painIt is relatively uncommon to see facialpain due to a local cause such as nasalvestibulitis or herpes eruption. Morefrequently it is related to disease in thedistribution of the trigeminal nerve,which supplies the sensory componentto the face and the interior of the noseand paranasal sinus via the ophthalmicand maxillary nerves. Consequently,these anatomical sites require detailedexamination in such cases (p. 53).
OtologicalAny pathological process that disruptsthe proper functioning of theEustachian tube may give rise to auralsymptoms. Nasal polyps, particularlyof the antrochoanal variety, canphysically block the pharyngeal end ofthe tube. Allergic diseases result in asimilar problem by provoking oedema,and neoplasms may directly invade theEustachian tube. The most frequentotological symptom is hearing loss
caused by a middle ear effusionsecondary to Eustachian tubedysfunction.
Disorders of smellAnosmia, a total loss of sense of smell,is rare. Hyposmia, a reduced sense ofsmell, is more common.
Cacosmia, which is an unpleasantsmell detected mainly by others, maybe caused by chronic nasal sepsis.Ozaena, a foul smell, is a commoncomplaint in anaerobic infections seenin cases of atrophic rhinitis, but thepresence of a foreign body andtumour must be excluded.
HalitosisPoor dental hygiene and poor diet arethe most common causes of halitosis.However, chronic sinusitis withpurulent postnasal drip can alsoproduce this symptom (p. 51).
Signs
A comprehensive approach toexamination of the nose can only beacquired by practice. It is essential toexamine both the exterior and interiorof the nose, and also ancillary areassuch as the ears and oropharynx.
ExternalCertain cosmetic deformities such asangulation of the bony nasal pyramidor a nasal hump may be obvious. Asaddle deformity due to previousinjury or infection is readily identified,and it is not unusual to find the septal
Fig. 1 Symptoms in nasal and paranasal sinus disease.
Otological (otalgia, hearingloss, crackling etc.)
Facialpressure,
discomfort
Disorders of smell
Halitosis
Blockage
Discharge Sneezing Postnasal drip
alterations in ambient temperature andhumidity. Neoplasia produces aprogressive obstruction and may causeocular and dental problems due tocontiguous spread.
Nasal dischargeThe specific character of a nasaldischarge is very helpful in decidingaetiology (Table 2). Many patientsdescribe this symptom as ‘catarrh’.However, if it produces a runny nose,the discharge should be described asrhinorrhoea and the term ‘catarrh’ (orpostnasal drip) reserved for complaintsof nasal discharge passing backwardsinto the nasopharynx. Epistaxis isdefined as nasal haemorrhage and ismost commonly due to spontaneous
Table 1 Causes of nasal obstruction
Variety Associated conditions
Anatomical Septal deflection
Adenoidal hypertrophy
Neoplasia
Choanal atresia
Disorders of nasal lining Allergic and infective rhinitis
Nasal polyps
Autonomic nervous Vasomotor rhinitis
system
Table 2 Nasal discharge: its characteristicsand significance
Character of discharge Associated conditions
Watery/mucoid Allergic, infective (viral) and
vasomotor rhinitis
Cerebrospinal fluid leak
Mucopurulent Infective (bacterial) rhinitis
and sinusitis
Foreign body
Serosanguineous Neoplasia
Bloody Trauma, neoplasia, bleeding
diathesis
F07311-Ch17.qxd 6/20/06 10:06 AM Page 32

cartilage dislocated into the nasalvestibule (Fig. 2).
InternalA systematic examination is essentialto adequately visualize all areas. Theinferior turbinate is very prominentand often mistaken for a polyp.Common nasal polyps are white/greyin colour and painless on palpation.
Mucopus in the middle meatus mayindicate infection in the anterior groupof sinuses.
The postnasal space or nasopharynx isa difficult region to view with a headlight and mirror. However, modernflexible instruments and rigidendoscopes have eased the difficulties.The sites to visualize include theEustachian tube cushions, the posteriorchoanae, the roof of the nasopharynx,and the fossa of Rosenmüller which is arecess situated immediately posterior tothe Eustachian tube.
Examination of the paranasal sinusesis limited to palpation. In an acutefrontal sinusitis, there is localizedtenderness in the floor of the sinus.Maxillary tumours may cause expansionof the malar and deformities of theteeth-bearing alveolus.
Investigations
Clinical investigations should notreplace mandatory history taking andphysical examination. Many of theinvestigations are performed mainly toconfirm the diagnosis and rarely addmuch more information. Nevertheless,critical use and appraisal affords a usefuladjunct to history and examination.
Allergy testingThe simplest variety of allergy test is askin-prick performed on the volaraspect of the forearm. A wide varietyof allergens are possible, but the
33Symptoms, signs and investigations
Fig. 2 Functional and cosmetic deformities of the nose. (a) The caudal end of the nasal septum isdislocated into the right nostril. (b) Saddle deformity caused by excessive removal of septal cartilage.
Fig. 3 A skin-prick test illustrating multipleallergies.
Fig. 4 CT scan showing a malignant tumourof the maxillary sinus with bone erosion inthe nasal cavity and cheek.
■ Nasal obstruction is the commonestsymptom.
■ The characteristics of nasal dischargemay be suggestive of particular disease.
■ Nasal pathology may, via the trigeminalnerve, give rise to referred head and neckpain.
■ The internal nose is best examined usinga rigid endoscope.
■ Skin-prick tests for nasal allergy arerecommended for investigating rhinitis.
■ CT and MRI have replaced plainradiology in the detailed examination ofthe nose and paranasal sinuses.
Symptoms, signsand investigations
common ones include pollens, animaldander, household dust and dust mite.Controls such as saline and histamineshould be employed. A positiveresponse produces a wheal and flare(in about 20 minutes) which can begraded. However, a negative responsedoes not exclude allergy, and a positiveresponse is not absolute proof that thespecific allergen is causing symptoms(Fig. 3). The radioallergosorbent test(RAST) measures allergen-specificserum immunoglobulin E, but thistechnique is expensive and reservedfor special cases.
RadiologyPlain views of the sinuses have limitedvalue. CT scanning is the imaging ofchoice for the majority of nasal andsinus disease (Fig. 4). Soft tissue
abnormalities and tumours usuallyrequire magnetic resonance imaging(MRI) (Fig. 5). MRI distinguishesretained secretions from soft tissuemasses.
Mucociliary clearanceMucociliary clearance can be assessedin cases of suspected ciliary motilitydisorder, e.g. Kartagener’s syndrome. A pellet of saccharin placed on theanterior end of the inferior turbinateshould be tasted by the patient inabout 20 minutes. Prolongation of thistime occurs in some normals afternasal infections and in primary ciliarydyskinesia.
MiscellaneousRhinomanometry, which measuresnasal air flow and resistance, is ahighly specialized research tool. Nasalprovocation tests are more accuratethan skin tests, but are timeconsuming as only a single allergencan be tested at a time. Eosinophilia innasal smears and blood is supportiveof a diagnosis of allergic rhinitis.
(a) (b)
Fig. 5 MRI scan (T1) complementary toFigure 4: soft tissue detail is enhanced.
F07311-Ch17.qxd 6/20/06 10:06 AM Page 33

NOSE AND PARANASAL SINUSES34
Allergic and vasomotor rhinitis
The term ‘rhinitis’ implies an inflammatory response of thelining membrane of the nose and may be intermittent orpersistent. It is important to understand that such an eventcan occur as a consequence of both primary allergic andnon-allergic mechanisms (Fig. 1). In allergic rhinitis, specificallergens are responsible for a type 1 hypersensitivityreaction, and the symptom complex may be subclassified asbeing predominantly seasonal or perennial. Non-allergicpathologies include viral and bacterial infections (pp. 38, 50),as well as autonomic nervous system abnormalities whichcan result in vasomotor rhinitis.
should be interpreted only in relationto the history. Negative skin tests inthe face of obvious allergens are notinfrequent.
ManagementThe simplest treatment is avoidance ofknown allergens. In perennial allergicrhinitis, the quantity of dust and dust mite may be reduced in thebedclothes by:
■ changing a feather pillow to foam ■ washing the bedclothes twice weekly,
as the antigen is heat sensitive
■ using commercial sprays that inhibithouse dust mite
■ using a dust proof cover over themattress, duvet and pillows
■ avoiding carpets and heavy drapes inthe bedroom.
Suspected food allergens may beexcluded from the diet or replacedwith suitable alternatives. Removinganimal dander by giving up a pet may be emotionally upsetting butnecessary.
Desensitization injections may beoffered. These work on the principle ofproducing a blocking IgG antibodythat prevents antigen binding to IgE.Obviously, the treatment is only ofvalue if specific allergens can beidentified, and it is essential tocommence the series of necessaryinjections well in advance of theexposure. Due to the risk ofanaphylaxis, desensitization must bedone in a controlled environment withadequate resuscitation available.
Fig. 1 Causes of rhinitis.
Rhinitis
Non-allergic
Acute andchronic
infections
Allergic
Non-infective(drugsirritants
hormonalidiopathic)
Seasonalallergens
Perennialallergens
Occupational
Allergic rhinitis
Between 10 and 20% of the populationsuffer to some degree from nasalmanifestations of an antigen–antibodytype 1 hypersensitivity reaction (Fig. 2).In seasonal allergic rhinitis (hay fever),the allergens are inhaled, e.g. grass,pollens, weeds and flowers. Animaldander, household dust, the dust miteand feathers are the principal allergensin perennial allergic rhinitis and have noseasonal variation. Rarely, ingestedallergens are implicated in the perennialgroup, e.g. dairy products and wheat.
Clinical featuresThe clinical features of allergic rhinitisinclude the classic triad of:
■ nasal obstruction due to mucosalvasolidation and oedema
■ rhinorrhoea (runny nose) due toenhanced activity of glandularelements
■ paroxysms of sneezing due tomucosal stimulation.
The symptom complex is produced byallergen binding to immunoglobulin E(IgE), which in turn is bound to mastcells. This causes degranulation ofmast cells and the release of mediatorsubstances such as histamine,leukotrienes and SRSA.
Many patients have associatedevidence of atopy such as asthma,eczema, allergic dermatitis and drugallergies. Aspirin sensitivity is notinfrequent. Taking a detailed clinicalhistory may identify the allergensinvolved.
Typically, the nasal mucosa has aboggy, oedematous appearance (Fig. 3);it is covered by a thin layer of waterysecretion. Application of avasoconstrictor produces markedmucosal shrinking with improvementin the nasal airway. Skin-prick tests
Seasonalallergicrhinitis
Perennialallergicrhinitis
INHALED
INHALED
INGESTED
Pollen
Grasses
Weeds
House dust
Dust mite
Animal dander
Feathers
Wheat
Eggs
Milk
Nuts
Fig. 2 Common allergens in allergic rhinitis.
Fig. 3 Oedematous inferior turbinatesnarrowing the nasal airway in a patient withhay fever.
F07311-Ch18.qxd 6/20/06 10:08 AM Page 34
Drug therapyTherapy involving the use of bothtopical and systemic drugs has beendirected at either preventing mast celldegranulation or blocking the effect ofreleased mediators.
Topical sodium cromoglycatestabilizes the mast cell membrane andprevents the release of chemicalagents. It has provided effective reliefof asthmatic symptoms but has beenless successful in allergic rhinitis. Localdecongestants can be eithersympathomimetic agents or steroids.The former group includes ephedrinenose drops which provide dramaticshrinkage of nasal mucosa, but long-term use can lead to rhinitismedicamentosa. Locally-acting steroidnasal sprays, e.g. beclometasone,fluticasone, are highly effective againstblockage and rhinorrhoea. Regular usein a ‘course’ is important. Topicalantihistamines are an alternative.
Systemic drug therapy includesantihistamines which act by blockingthe H1 nasal mucosa receptors. Theirmajor drawback is drowsiness. Modernderivatives are less able to cross theblood–brain barrier, hence reducingside-effects. If sedation occurs,medication can be taken at night.
SurgerySurigical treatment (Fig. 4) is onlyinfrequently indicated, as mostpatients’ symptoms are controlled byconservative therapy. Turbinateresection, cautery or outfracture mayimprove nasal obstruction, butrhinorrhoea and sneezing areunaffected by surgical manipulations.
Intrinsic rhinitis(vasomotor rhinitis)
Intrinsic rhinitis is common (10–15%of the population). The symptoms are
35Allergic and vasomotor rhinitis
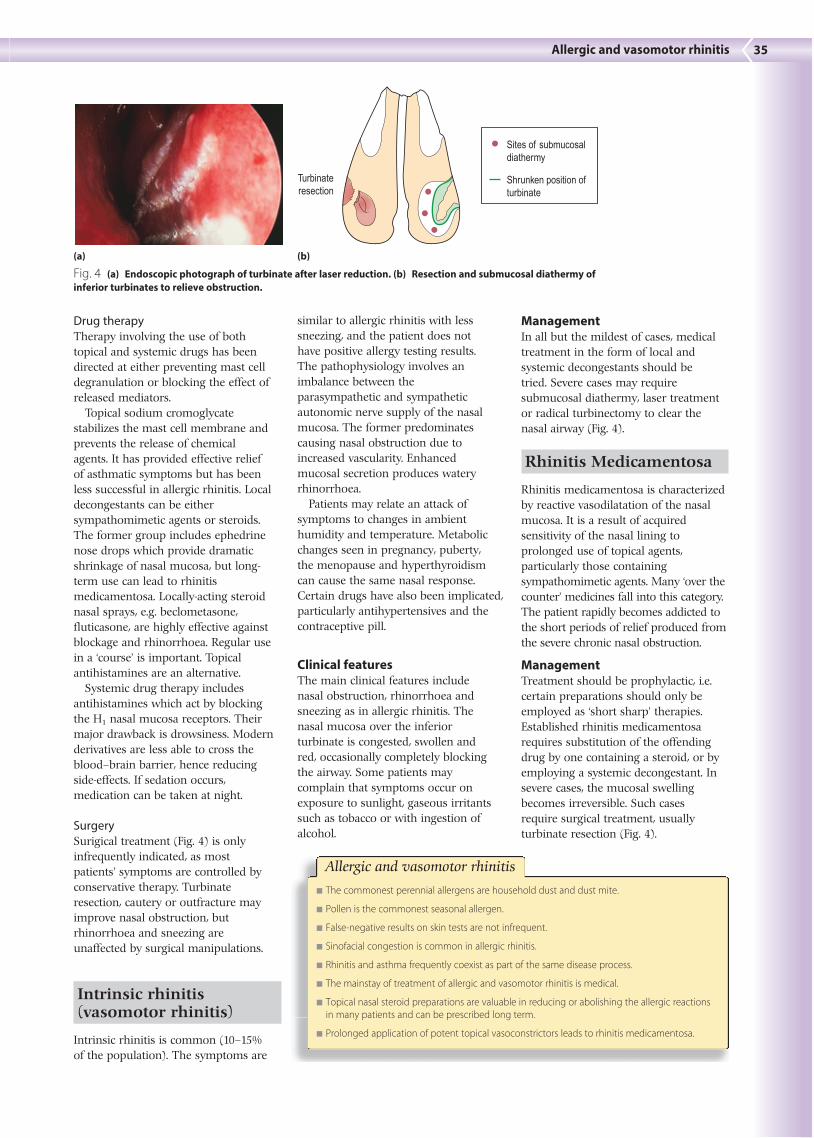
Fig. 4 (a) Endoscopic photograph of turbinate after laser reduction. (b) Resection and submucosal diathermy ofinferior turbinates to relieve obstruction.
■ The commonest perennial allergens are household dust and dust mite.
■ Pollen is the commonest seasonal allergen.
■ False-negative results on skin tests are not infrequent.
■ Sinofacial congestion is common in allergic rhinitis.
■ Rhinitis and asthma frequently coexist as part of the same disease process.
■ The mainstay of treatment of allergic and vasomotor rhinitis is medical.
■ Topical nasal steroid preparations are valuable in reducing or abolishing the allergic reactionsin many patients and can be prescribed long term.
■ Prolonged application of potent topical vasoconstrictors leads to rhinitis medicamentosa.
Allergic and vasomotor rhinitis
similar to allergic rhinitis with lesssneezing, and the patient does nothave positive allergy testing results.The pathophysiology involves animbalance between theparasympathetic and sympatheticautonomic nerve supply of the nasalmucosa. The former predominatescausing nasal obstruction due toincreased vascularity. Enhancedmucosal secretion produces wateryrhinorrhoea.
Patients may relate an attack ofsymptoms to changes in ambienthumidity and temperature. Metabolicchanges seen in pregnancy, puberty, the menopause and hyperthyroidismcan cause the same nasal response.Certain drugs have also been implicated,particularly antihypertensives and thecontraceptive pill.
Clinical featuresThe main clinical features includenasal obstruction, rhinorrhoea andsneezing as in allergic rhinitis. Thenasal mucosa over the inferiorturbinate is congested, swollen andred, occasionally completely blockingthe airway. Some patients maycomplain that symptoms occur onexposure to sunlight, gaseous irritantssuch as tobacco or with ingestion ofalcohol.
ManagementIn all but the mildest of cases, medicaltreatment in the form of local andsystemic decongestants should betried. Severe cases may requiresubmucosal diathermy, laser treatmentor radical turbinectomy to clear thenasal airway (Fig. 4).
Rhinitis Medicamentosa
Rhinitis medicamentosa is characterizedby reactive vasodilatation of the nasalmucosa. It is a result of acquiredsensitivity of the nasal lining toprolonged use of topical agents,particularly those containingsympathomimetic agents. Many ‘over thecounter’ medicines fall into this category.The patient rapidly becomes addicted tothe short periods of relief produced fromthe severe chronic nasal obstruction.
ManagementTreatment should be prophylactic, i.e.certain preparations should only beemployed as ‘short sharp’ therapies.Established rhinitis medicamentosarequires substitution of the offendingdrug by one containing a steroid, or byemploying a systemic decongestant. Insevere cases, the mucosal swellingbecomes irreversible. Such casesrequire surgical treatment, usuallyturbinate resection (Fig. 4).
Turbinateresection
Sites of submucosaldiathermy
Shrunken position ofturbinate
(a) (b)
F07311-Ch18.qxd 6/20/06 10:08 AM Page 35

NOSE AND PARANASAL SINUSES36
Nasal polyps and foreign bodies
Nasal polyps
The majority of nasal polyps areassociated with intrinsic rhinitis andallergy (Table 1), although only about25% of patients have positive skin-prick tests.
Nasal polyps are ‘bags’ ofoedematous mucosa and mostfrequently arise from the ethmoid cellsand prolapse into the nose via themiddle meatus. They are nearly alwaysbilateral. If allowed to grow they maypresent in the nasal vestibule (Fig. 1).The cardinal symptom is progressivenasal obstruction. Rhinorrhoea isfrequent and ocassionally a history ofrecurrent sinusitis due to ostialblockage is a feature. Otologicalsymptoms and hyposmia may occur.
Chronic sinus infection can result inpolypoid mucosal disease which,clinically, produces similar features toidiopathic nasal polyposis.
Clinical featuresExamination reveals single or multiplepale, grey polypoid masses which areinsensitive to palpation and do notbleed. Unilaterality and haemorrhageshould arouse the suspicion ofneoplasia. CT scans may reveal radio-opacity due to secondary infection, inthe paranasal sinuses, particularly ofthe maxillary antrum.
ManagementLarge polys are treated by pernasalremoval. Small polyps can be managedby topical nasal steroids. Short-termsystemic steroids are also occasionallyadministered. Recurrence rates may bereduced by long-term topical steroids,post-surgery. Any chronic sinusinfection should be treated inconjunction with nasal polypectomy.Rarely, an ethmoidectomy may be
required for frequent recurrences.Routine management strategies for theunderlying allergy or asthma shouldalso be instituted (pp. 34–35).
Antrochoanal polypThe antrochoanal polyp is uncommon.It is usually unilateral and commencesas oedematous lining in the maxillarysinus. This prolapses, usually via aposterior accessory ostium, into thenasal cavity and enlarges toward theposterior choana and naspoharynx. Thepatient, commonly a young adult,complains of unilateral nasalobstruction, which is worse onexpiration due to the ball valve effect ofthe polyp in the posterior choana. Ifsignificantly large it may block bothchoanae and cause otological symptomsdue to obstruction of the Eustachiantube (Fig. 2). Patients occasionallypresent so late that the polyp has
enlarged behind the soft palate andhangs visibly in the oropharynx.
Treatment is surgical by pernasalexcision with removal of the cysticantral portion endoscopically via anantrostomy. Recurrences may require aCaldwell–Luc approach to the antrumto remove the roots of the cyst.
Neoplastic polypsNeoplastic polyps (p. 110) are invariablyunilateral and cause progressivesymptoms: nasal obstruction, epiphora(blocking of the vasolacrimal duct),epistaxis and foul smelling nasaldischarge. They are frequently fleshy inappearance and bleed on palpation.Biopsy is mandatory.
Miscellaneous polypsNasal polyps are extremely rare inchildren. In this age group, carefulconsideration should be given to anyevidence of cystic fibrosis, and a sweattest should be performed.
Prolapse of the meninges(meningocele) or cerebrum(encephalocele) can occur through ananterior cranial fossa defect. Thisshould be excluded radiologically priorto excision or biopsy.
Nasal foreign bodies
Young children (and on occasion,psychiatric cases) are the main patientswho insert foreign bodies into thenose. The variety of foreign bodies isprotean (Fig. 3), but readily availableitems such as foam rubber, peas andsmall stones are frequent. Inorganicobjects may be in situ for long periods
Fig. 1 Bilateral nasal polyps presenting in the nasal vestibules (a). A polyp can easily beconfused with a normal inferior turbinate (b) especially if the turbinate is hypertrophic.
Table 1 Causes of nasal polyps
Infection
Rhinitis
Sinusitis — chronic paranasal infection
Nasal allergy, e.g. aspirin sensitivity, seasonal and
perennial allergic rhinitis
Idiopathic
Neoplasia
Association with other diseases
Asthma
Cystic fibrosis
Bronchiectasis
Fig. 2 Antrochoanal polyp. A surgicalspecimen showing the classic dumbbellappearance. This caused total unilateral nasalblockage.
Normal middle turbinate
Normal inferior turbinate
(a) (b)
F07311-Ch19.qxd 6/20/06 10:10 AM Page 36

before producing symptoms. However,organic objects, such as paper, wooland vegetable material, produce a briskmucosal reaction and hence rapidonset of symptoms (Fig. 4).
Clinical featuresThe child is usually calm, although priorclumsy attempts at removal may havecaused distress. Usually, the parentsprovide a sound history which an olderchild frequently denies. The cardinalsign is a unilateral nasal discharge whichis foul smelling if the foreign body hasbeen present for any length of time (Fig.4). Excoriation of the nasal vestibularskin and upper lip may be present. Theforeign body frequently impacts in thelower part of the nose and on ocassionssimply rests in the nasal vestibule.Unless there is a marked infection,visualization is usually possible in goodlight by elevating the nasal tip gentlywith the thumb.
ManagementIn a cooperative child, the foreign bodymay be either grasped by cuppedforceps or flicked out with a blunthooked probe. An adult may need torestrain a young child. The limbs areusually wrapped in a blanket and thehead held steady (Fig. 5). A general
37Nasal polyps and foreign bodies
Fig. 4 Unilateral nasal vestibulitis caused bya nasal foreign body. The patient presentedwith a 3-week history of foul odour.
anaesthetic will be required in all otherinstances, as inept attempts could pushthe object further back with thesubsequent risk of inhalation ortraumatic haemorrhage. In someinstances it is safer to deliver the objectvia the nasopharynx. The other nostrilmust be examined to exclude a secondforeign body.
RhinolithRhinolith is the term applied to a largeforeign body found in the nose of
some adults. It is composed ofdeposits of calcium and magnesiumon a nidus such as a piece of gauze orclotted blood. There is frequently ahistory of nasal packing for epistaxismany years previous (Fig. 6).
Clinical features and managementNasal obstruction and discharge arethe most common symptoms. Thelatter may be foul smelling and blood-stained due to the presence ofinfection and friable granulations.Examination reveals a mass that ishard to palpation. Plain radiology canconfirm the diagnosis.
Rhinoliths should preferably beremoved in one piece, but their sheerbulk may require piecemeal extraction.
(a) (b) (c) (d)
Fig. 3 A selection of removed nasal foreign bodies. (a) Piece of sofa sponge. (b) Piece of cotton wool. (c) Leaf. (d) Rubber pencil end.
Fig. 5 Restraining a young child whenremoving a nasal foreign body.
Fig. 6 Rhinolith. A large specimen extractedfrom a patient who had required nasal packing forepistaxis many years previous. The nidus(coloured red) was a remnant of the gauzeemployed.
■ The majority of nasal polyps are usually bilateral, secondary to rhinitis, and painless.
■ The prevalence of polyps increases with age.
■ Beware of unilateral bleeding polyps. They may be neoplastic and should be biopsied.
■ Nasal polyps are extremely rare in children.
■ A foul smelling unlateral nasal discharge in a child requires exclusion of a nasal foreign body.
■ Beware: foreign bodies can be inhaled.
■ Resort to removal under general anaesthesia if the patient is uncooperative, or removal isdifficult. The patient will thank you.
Nasal polyps and foreign bodies
F07311-Ch19.qxd 6/20/06 10:10 AM Page 37









![Neoplasia and Infection - Tumor Surgerytumorsurgery.org/Portals/0/PDF/Publications... · Neoplasia and Infection VIII GRBQ110-C37[1155-1200].qxd 6/3/06 1:53 AM Page 1155 Quark07 27B:GRBQ110:Chapters:CH-37:](https://static.fdocuments.in/doc/165x107/5aa919bd7f8b9a9a188c6378/neoplasia-and-infection-tumor-and-infection-viii-grbq110-c371155-1200qxd-6306.jpg)








