Eye Problems in General Practice MR Besharati MD Shahid Sadoughi University.
48
Eye Problems in General Practice MR Besharati MD Shahid Sadoughi University
-
Upload
wendy-west -
Category
Documents
-
view
223 -
download
2
Transcript of Eye Problems in General Practice MR Besharati MD Shahid Sadoughi University.

Eye Problems in General Practice
MR Besharati MD
Shahid Sadoughi University
Topics to be discussed
• Lacrimal disorders
• Blepharitis
• Degenerative changes of cornea and sclera
• Age related maculopathy
• Hypertensive eye disease
• Cataract
• Glaucoma
• Diabetic eye disease

Lacrimal system
• Stable tear film essential for maintenance corneal clarity
• Nutritional and protective functions
• Deficient tear film causes corneal and conjunctival damage


Tear film• Superficial lipid layer derived
from meibomian glands• Aqueous tears derived from
lacrimal gland contain immunoglobulins and lysozyme
• Thin mucus layer created by goblet cells allow adherence aqueous tears to cornea
• Tears flow from lacrimal gland to lacrimal puncta mainly along lower lid margin
• Upper lid has essential function in applying mucus to corneal surface and ensuring even spread of tears
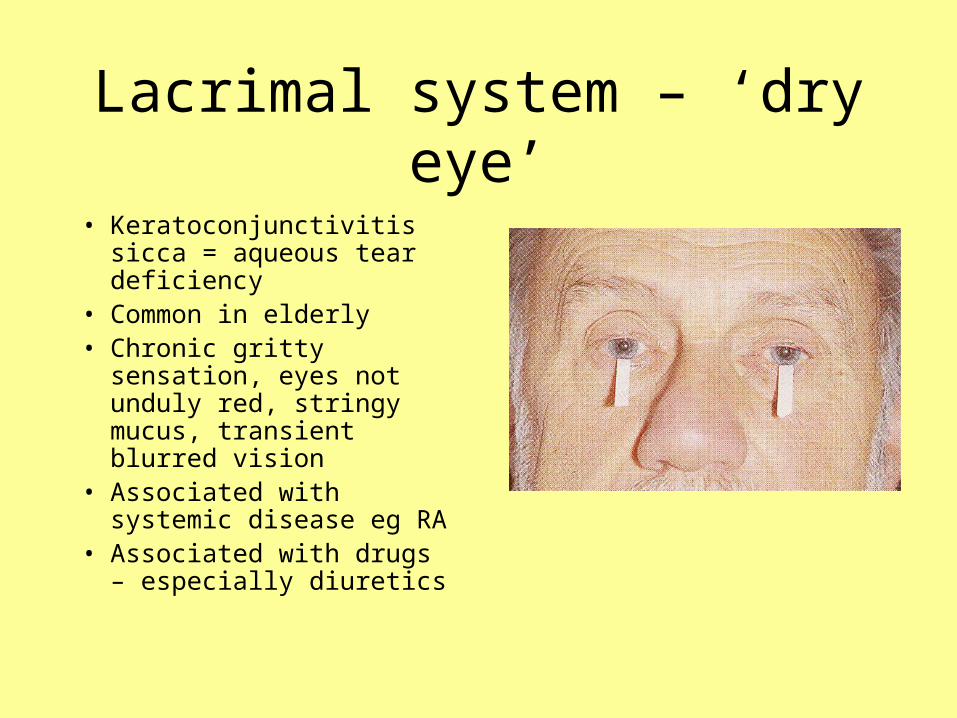
Lacrimal system – ‘dry eye’
• Keratoconjunctivitis sicca = aqueous tear deficiency
• Common in elderly• Chronic gritty sensation,
eyes not unduly red, stringy mucus, transient blurred vision
• Associated with systemic disease eg RA
• Associated with drugs – especially diuretics

Investigation of ‘dry eye’
• Tear film break up time (BUT)
• Rose bengal staining• Schirmer’s test –
absorbent paper strips placed in lower fornix, <10 mm wet in 5 minutes = deficiency

Treatment ‘dry eye’
• Artificial tear drops• Simple eye ointment
at night (prolonged lubrication)
• Acetylcysteine eye drops useful if filamentary keratitis
• Treat associated blepharitis

Lacrimal disorders – ‘watering eye’
• Tears are produced by lacrimal glands
• Flow along lid margins, spread by blinking
• Enter upper and lower puncta to lacrimal sac
• Flow down nasolacrimal duct to nose

‘watering eye’
• Excessive production of tears – can be paradoxical in dry eyes
• Punctal malposition• Punctal stenosis• Blockage of lacrimal sac
or nasolacrimal duct – syringing, -dacrocystorhinostomy

Blepharitis
• Generalised eyelid inflammation– Staphylococcal or
seborrheic dermatitis
• Itchy red burning eyelid margins
• Scales on lashes and crusty secretions on lids
• Recurrent and may be associated with bacterial conjunctivitis

Blepharitis
• Regular cleaning– Apply hot wet flannel
firmly against closed eye – Use moistened cotton
wool bud to wipe away secretions
• Local antibiotic –chloramphenicol or fusidic acid
• Add 1% hydrocortisone if persistent inflammation
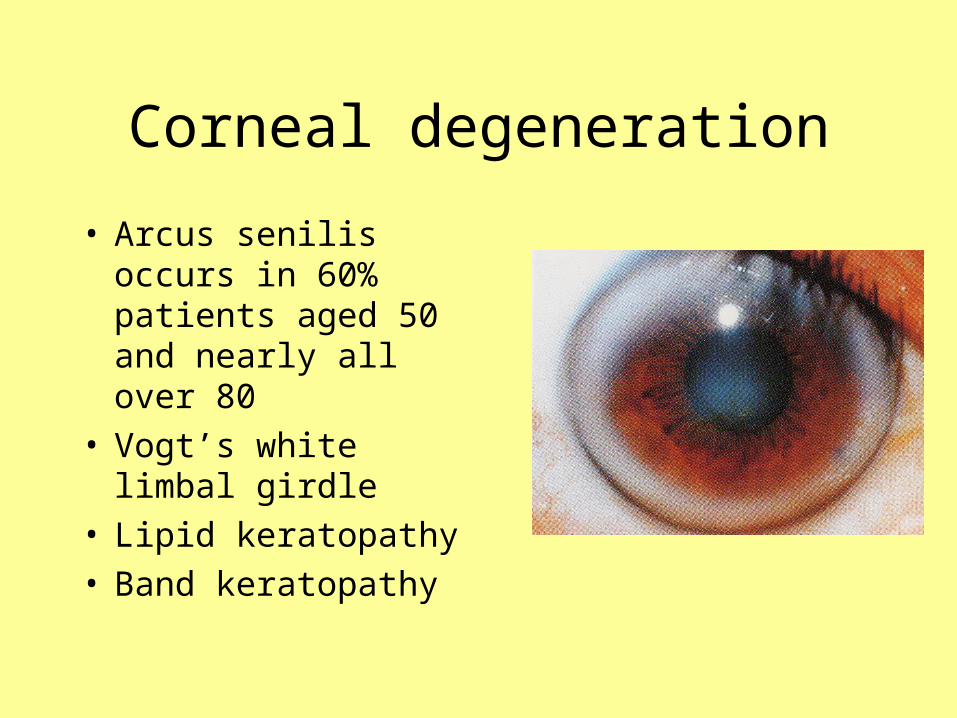
Corneal degeneration
• Arcus senilis occurs in 60% patients aged 50 and nearly all over 80
• Vogt’s white limbal girdle
• Lipid keratopathy• Band keratopathy


Age-related macular degeneration
• Leading cause of blindness in over 50s
• Over ½ million people in UK affected by AMD
• 190,000 new cases AMD in UK per year

What is AMD?
• Degenerative condition of central retina
• Dry AMD (85%) – atrophic form
• Wet AMD responsible for 15% sufferers but 90% blindness – neovascular form with new abnormal vessels at the macula
• High risk of second eye involvement within 5 years of first

AMD – risk factors
• Age (wet AMD usually presents in patients over 50)
• Genetics – hereditary link. Screening of blood relatives has debatable value
• Race/gender – white females• Smoking increases wet and dry
AMD• Hypertension• Post-menopausal women not on
HRT more likely to develop neo-vascularisation

AREDS (Age Related Eye Disease Study)
• Performed by National Eye Institute
• Antioxidants including Vit A and Vit E
• Zinc and copper• Beneficial in
preventing progression to sight-threatening AMD

Dry AMD• 85% cases
• Slow progression, not usually severe
• Difficulty with reading and fine visual tasks
• Distortion and metamorphosia uncommon
• Drusen, pigmentation and atrophy of retina
• No proven treatment
• Low vision services helpful

Wet AMD
• 15% cases• More severe, rapid visual loss,
3-6 months if untreated• Choroidal neovascularisation –
abnormal vessels leak fluid into macula, causing retinal surface to become uneven with blurring and distortion of central vision
• Scar tissue creates irreversible blind spots

AMD - symptoms
• Recent change in visual function, in particular ability to read, recognise faces, difficulty with changing light conditions
• On waking, dark patch in vision which quickly fades
• Distortion of the shape of familiar objects especially kinking of lampposts/windows (and not double vision or ghosting associated with cataract)

AMD -Signs
• Decreased acuity with Snellen chart
• No improvement in acuity with pinhole (in macular disease)
• Amsler grid testing
• Fundoscopy – subretinal fluid, exudate, haemorrhage or pigment epithelial elevation

Rehabilitation• Provision and training in use of
optical aids
• Increase wattage of household bulbs
• Mark cooker controls with tactile dots etc
• Registration as blind or partially sighted in order to access local social support
• Put in touch with community voluntary services or relevant support groups

Hypertensive eye disease
• Severity of hypertension– degree of hypertensive
vascular change
– retinopathy
• Duration of hypertension– degree of arteriosclerotic
vascular change
– retinopathy
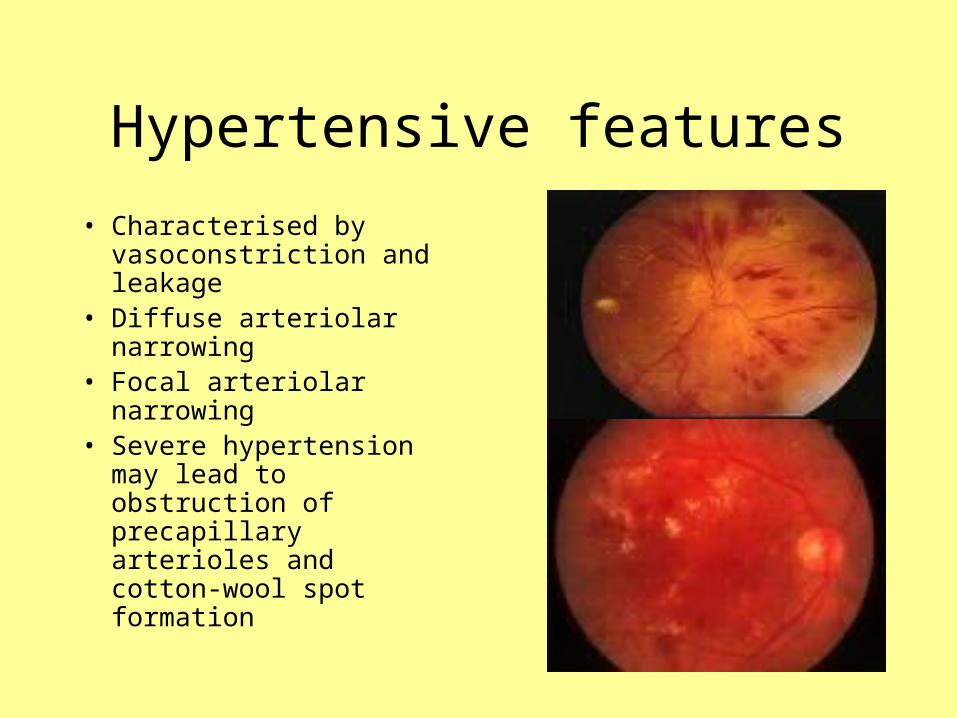
Hypertensive features
• Characterised by vasoconstriction and leakage
• Diffuse arteriolar narrowing
• Focal arteriolar narrowing• Severe hypertension may
lead to obstruction of precapillary arterioles and cotton-wool spot formation

Hypertensive features
• Abnormal vascular permeability leads to haemorrhages, retinal oedema and hard exudates
• Deposition of hard exudates around the fovea may lead to their radial distribution as a macular star
• Swelling of the nerve head occurs in malignant hypertension

Arteriosclerotic features
• Thickening of vessel wall with hyaline degeneration and narrowing of the lumen
• Arteriovenous crossing change / AV nipping
• Copper wiring
• Silver wiring – heightened reflex from opaque arterioles



Cataract
• A common cause of visual loss
• Most important cause of blindness worldwide
• Lens opacification

Symptoms of cataract
• Difficulty reading
• Vision worsens in bright light (especially with central opacity)
• Monocular diplopia
• Haloes around lights
• Improved near vision (nuclear sclerotic cataract can improve converging power of lens)

Signs of cataract
• Reduction in acuity (unilateral/bilateral)
• Diminished red reflex• Change in appearance
of lens

Types of cataract
• Senile • Traumatic• Metabolic• Toxic• Secondary• Hereditary


Treatment of cataract
• No effective medical treatment
• Decision to operate is a quality of life issue
• Various surgical options
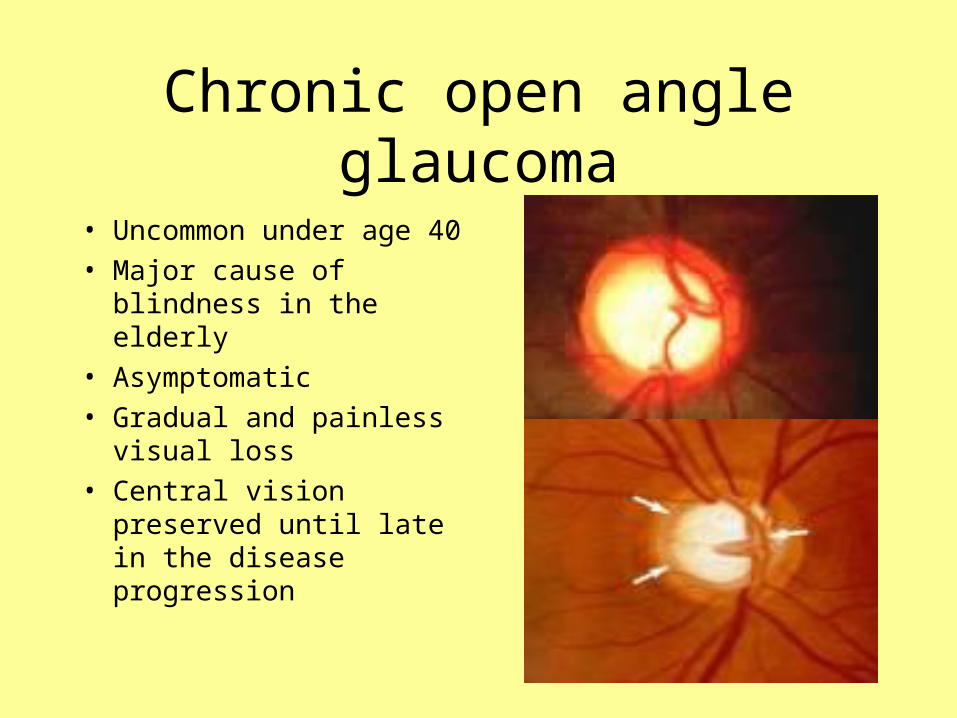
Chronic open angle glaucoma
• Uncommon under age 40
• Major cause of blindness in the elderly
• Asymptomatic
• Gradual and painless visual loss
• Central vision preserved until late in the disease progression

Signs of glaucoma
• Raised intraocular pressure ( >21 mmHg)
• Pathological cupping of optic disc – gradual loss of nerve fibres at disc resulting in a pale disc with an enlarged cup
• Visual field loss


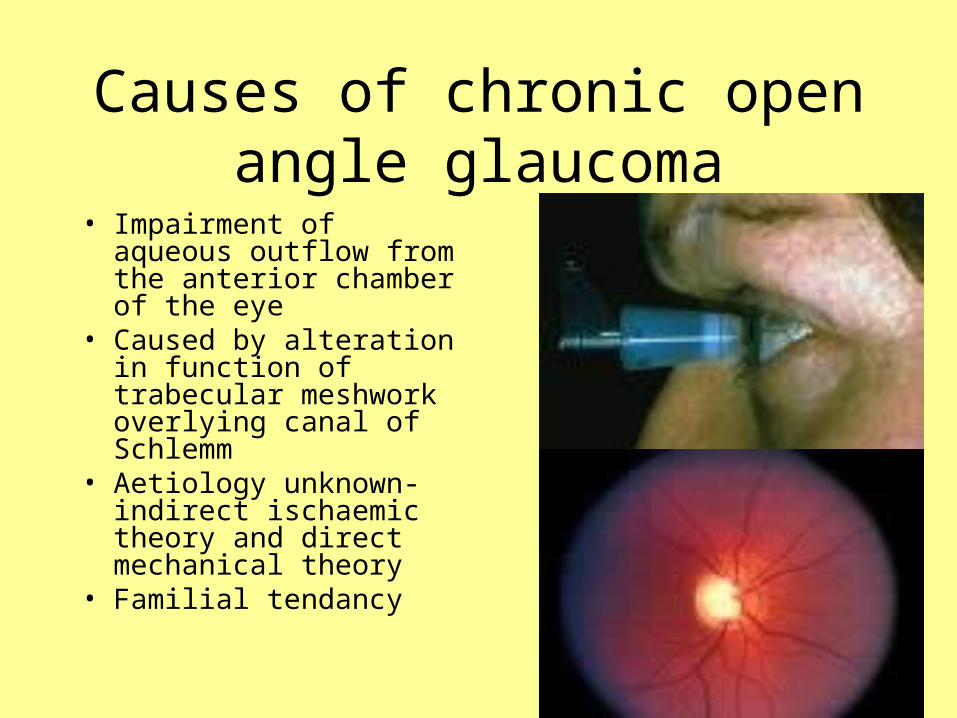
Causes of chronic open angle glaucoma
• Impairment of aqueous outflow from the anterior chamber of the eye
• Caused by alteration in function of trabecular meshwork overlying canal of Schlemm
• Aetiology unknown- indirect ischaemic theory and direct mechanical theory
• Familial tendancy

Medical treatment
• Pilocarpine drops 1-4% – act via ciliary muscle to open drainage channels
• Adrenaline drops 0.5-2% increase outflow aqueous humour
• Timolol drops 0.25-0.5 % and other beta blockers reduce aqueous humour production
• Acetozolamide capsules 250 mg reduce rate aqueous humour production

Laser / surgical options
• Laser trabeculoplasty – laser burns to trabecular meshwork result in increased aqueous flow
• Surgical drainage eg trabeculectomy – portion of sclera adjacent to the cornea is removed to create a fistula
• Long –term monitoring with applanation tonometry (= pressure gauge) and perimetry(=field testing)

Diabetic eye disease
• Background retinopathy
• Maculopathy• Proliferative
retinopathy

Diabetic background retinopathy
• Blot haemorrhages• Hard exudates
• Vision normal

Diabetic Maculopathy
• Hard exudate at fovea
• Vision irreversibly damaged

Diabetic proliferative retinopathy
• New vessel formation at optic disc in response to ischaemia
• Irreversible reduction in visual acuity
• Risks of vitreous haemorrhage and retinal detachment

Goals for treatment
• Good diabetic control can prevent new vessel formation
• Concurrent diseases such as hypertension, renal disease, anaemia, hyperlipidaemia, can accelerate retinopathy and need to be treated
• Pre-symptomatic screening and early photocoagulation

Screening for diabetic retinopathy
• Allows laser photocoagulation to be used for maculopathy and proliferative retinopathy
• May be done by regular eye examination
• Increasing use of retinal photography
• ?? Retinal photography in primary care