Eye injury.pdf
6
Emergency department management of penetrating eye injuries Dan Lindfield BM MRCOphth (Speciality Trainee) * , Raja Das-Bhaumik MB BS MRCOphth (Specialist Registrar) Royal Eye Unit, Kingston Hospital, Galsworthy Road, Kingston upon Thames, Surrey, UK Received 7 October 2008; received in revised form 13 January 2009; accepted 13 January 2009 KEYWORDS Nursing; Ophthalmology; Eye; Vision; Visual loss; Trauma; Injury; Emergency department (ED); A&E; Penetrating; Ocular Abstract Penetrating injuries are rare but important for the patient both visually and socio- economically. This guide intends to provide a structure for emergency department personnel to enable targeted history taking, effective examination, appropriate investigation and timely referral for those presenting with penetrating eye trauma. ª 2009 Elsevier Ltd. All rights reserved. Introduction Any disease or process which can adversely affect vision has many sequelae including ability to work, capacity to drive and psychosocial effects. Penetrating eye injuries occur most commonly in the 20–40 years old age group and accu- rate detection is vital to facilitate subsequent specialist in- put (McCormack, 1999). Non-detection of a serious eye injury has potential to jeopardise a potentially treatable sight-threatening condition in addition to the medico-legal problems for the healthcare workers involved. Penetrating eye injuries are thankfully rare especially after legislation enforcing compulsory seatbelt use in cars (Hall et al., 1985). Incidence is currently estimated at 0.16 cases per 100,000 in the UK with a huge male predilection. The most common mechanism being hammering metallic objects (62% of total) (Imrie et al., 2008). Very severe cases of ocular trauma can be immediately apparent and the extent of the injury easy to determine but other cases may be very subtle. Early detection of this subgroup can markedly im- prove visual outcomes (Punnonen and Laattikainen, 1989). The traumatised eye is often very difficult to examine. The patient is usually in pain and agitated, family/friends are often very concerned. In addition, the eyelids can be very swollen and patients are reluctant to cooperate; 1755-599X/$ - see front matter ª 2009 Elsevier Ltd. All rights reserved. doi:10.1016/j.ienj.2009.01.003 * Corresponding author. Address: Ophthalmology, Conquest Hospital, St. Leonards on Sea, Sussex, UK. Tel.: +44 7726 025852. E-mail addresses: danlindfi[email protected] (D. Lindfield), [email protected] (R. Das-Bhaumik). International Emergency Nursing (2009) 17, 155– 160 available at www.sciencedirect.com journal homepage: www.elsevierhealth.com/journals/aaen Copyright Agency Limited (CAL) licenced copy
Transcript of Eye injury.pdf

International Emergency Nursing (2009) 17, 155–160
ava i lab le a t www.sc iencedi rec t . com
journal homepage: www.elsevierheal th .com/ journals /aaen
Emergency department management ofpenetrating eye injuries
Dan Lindfield BM MRCOphth (Speciality Trainee) *,Raja Das-Bhaumik MB BS MRCOphth (Specialist Registrar)
Royal Eye Unit, Kingston Hospital, Galsworthy Road, Kingston upon Thames, Surrey, UK
Received 7 October 2008; received in revised form 13 January 2009; accepted 13 January 2009
17do
*
Ho
ra
KEYWORDSNursing;Ophthalmology;Eye;Vision;Visual loss;Trauma;Injury;Emergency department(ED);A&E;Penetrating;Ocular
55-599X/$ - see front matti:10.1016/j.ienj.2009.01.00
Corresponding author. Aspital, St. Leonards on SeaE-mail addresses: danlin
[email protected] (R. Das-B
Copyright Agency Lim
er ª 2003
ddress:, Sussex,dfield@hhaumik)
ited (CAL
Abstract Penetrating injuries are rare but important for the patient both visually and socio-economically. This guide intends to provide a structure for emergency department personnel toenable targeted history taking, effective examination, appropriate investigation and timelyreferral for those presenting with penetrating eye trauma.ª 2009 Elsevier Ltd. All rights reserved.
Introduction
Any disease or process which can adversely affect vision hasmany sequelae including ability to work, capacity to driveand psychosocial effects. Penetrating eye injuries occurmost commonly in the 20–40 years old age group and accu-rate detection is vital to facilitate subsequent specialist in-put (McCormack, 1999). Non-detection of a serious eyeinjury has potential to jeopardise a potentially treatablesight-threatening condition in addition to the medico-legal
9 Elsevier Ltd. All rights reserved
Ophthalmology, ConquestUK. Tel.: +44 7726 025852.otmail.com (D. Lindfield),.
) licenced copy
problems for the healthcare workers involved. Penetratingeye injuries are thankfully rare especially after legislationenforcing compulsory seatbelt use in cars (Hall et al.,1985). Incidence is currently estimated at 0.16 cases per100,000 in the UK with a huge male predilection. The mostcommon mechanism being hammering metallic objects (62%of total) (Imrie et al., 2008). Very severe cases of oculartrauma can be immediately apparent and the extent ofthe injury easy to determine but other cases may be verysubtle. Early detection of this subgroup can markedly im-prove visual outcomes (Punnonen and Laattikainen, 1989).
The traumatised eye is often very difficult to examine.The patient is usually in pain and agitated, family/friendsare often very concerned. In addition, the eyelids can bevery swollen and patients are reluctant to cooperate;
.

156 D. Lindfield, R. Das-Bhaumik
especially when compounded by alcohol consumption whichis frequently significant in this patient group. Furthermore,due to many eye units having a dedicated ‘‘Eye A&E’’ thereis increasing paucity of knowledge regarding ophthalmicconditions as ED staff only see ophthalmic emergenciesinfrequently.
This article is designed to be a step by step guide to theinitial triage, examination, diagnosis and referral of pa-tients with confirmed or suspected penetrating eye injuries.
Anatomy
A working knowledge of the basic ocular anatomy is useful(Fig. 1).
History
Factual details are essential in determining the type of in-jury and enable rapid stratification of likely risk to theeye. Important factors include:
� When?: Timing of injury (and any delay to presentationwith reasons).� Where?: Occupational or assault-related injuries shouldbe carefully documented for medico-legal reasons.� How?:o Description of object causing injury
� Size.� Weight.� Velocity.� Direction (head-on or glancing impact).� Any object which is smaller in diameter than the
orbital rim can theoretically cause significant inj-ury as the ‘‘crash – helmet’’ (the strong anteriororbital impact area) may not have protected theorbital contents. Blunt but high force injury from asmall projectile can cause posterior blow-out rup-tures of the eye which can be missed if notsuspected.
o Potential infection/toxic risk
C
� Any penetrating injury causes a potential tract forinfection. Higher risk is carried with any organic
Figure 1 Basic ocular anatomy.
opyright Agency Limited (CAL) licenced copy
material. Metallic objects especially iron are oftenoculotoxic.
o Ocular protection
� Simple protective glasses or wrap-around goggles.Examination
Before embarking on examination of the eye, it is impera-tive that the patient is stable both haemodynamically andneurologically.
First things first: a drop of topical anaesthetic is a greataid to examination. Eyelids are very infrequently ‘‘too pain-ful to open’’. Eye drops containing preservatives are bestavoided as allergy can occur and they are retinotoxic if a pe-netrating injury is present. The following are commonlyavailable for ED use (British National Formulary, 2008):
� Benoxinate hydrochloride (0.4%).� Amethocaine hydrochloride (0.5% or 1%).� Lidocaine hydrochloride (4%).� Proxymetacaine (0.5%) (Note: must be keptrefrigerated).
Eyelids should never be forced apart. If topical anaesthesiaand verbal encouragement are not sufficient then examinationby a clinician with experience of ocular trauma is usually indi-cated. If the history is suspicious of penetration then this aloneshould require early specialist ophthalmic input.
A systematic approach to ocular examination is useful.This is helpful twofold: for yourself to ensure no componentof the examination is accidently omitted but it also servesas a logical structure useful for referring patients to oph-thalmic specialists. The following is suggested:
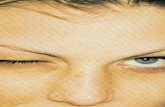
� First, assess pupillary reactions� The presence of a Relative Afferent Pupillary Defect(RAPD) indicates significant obstruction of the sensorypathway and is extremely useful in stratifying of injury.It cannot be caused by cataract or vitreous haemorrhagebut instead indicates more serious pathology (e.g. retinaldetachment, posterior globe rupture or optic nerveinjury) (Fig. 2).� Use the brightest light possible. A mains-voltage poweredophthalmoscope is best.� Shine the light into the affected eye: If the pupil con-stricts this is a normal ‘‘direct’’ response.� Next shine the light into the fellow eye whilst observingthe affected eye. If the pupil constricts in the affectedeye then a ‘‘consensual’’ response is present.� If direct and consensual responses are normal then aswinging light test is utilised to detect subtle differencesbetween the eyes. It is useful to assess the health of theoptic nerve by comparing the two pupils’ relativeresponse to light. Start by shining the light into theaffected eye and then swing the light to the unaffectedeye whilst observing the pupil of the affected eye. Ifthere is a difference between pupillary constrictionsdepending on which eye is receiving the light stimulusthen a (RAPD) is said to be present.

Figure 2 Relative Afferent Pupillary Defect (RAPD) illustrated.
Emergency department management of penetrating eye injuries 157
� Measure the visual acuity� All ED’s should have a Snellen visual acuity chart (Fig. 3).These should be used with the patient six metres awayand measuring the vision of one eye at a time.� If letters cannot be read then it is still useful to ascertainthe vision in terms of:1. No perception of light (termed ‘‘NPL’’).2. Perception of light (termed ‘‘PL’’).
Figure 3 Snellen chart for me
Copyright Agency Limited (CAL) licenced copy
3. Detection only of hand movements (‘‘HM’’).4. Ability to count fingers (‘‘CF’’).� If letters can be read record this as ‘‘6(metres) over(smallest line on chart read)’’.� E.g. patient reading the line marked ‘‘18’’ has visionrecorded as 6/18 (This corresponds to the patient seeingat 6 metres what the average person can see at 18 m).� Ocular motility (Fig. 4)
asurement of visual acuity.

Figure 5 Full thickness upper lid laceration involving the lidmargin.
158 D. Lindfield, R. Das-Bhaumik
� Assessment of eye movements is useful for determiningwhether there has been any damage to the bony orbitor extra-ocular muscles.� To test, keep the patient’s head in a straight-ahead posi-tion whilst asking them to follow a target (light). Movethe target up, down, left and right initially followed bydiagonal positions of gaze (top–left, bottom–right etc.).� Note any restrictions of movement in each eye.
Now move on to examining the eye itself. Remember,systematic and logical is the key. Think ‘‘front-to-back’’.Nature has also been kind to you by giving you anothereye to compare your findings with; don’t be afraid to useit if needed.
1. Start with the lids:� Lacerations can be deceptive. What appears to be a
superficial scratch can turn out to be a full thicknessinjury with retention of foreign body.
� The mode of injury, as determined by the history,should give a guide to potential examination findings.
� If lacerations are discovered, determine if they arepartial or full thickness (see Fig. 5). Penetrating lac-erations must increase your suspicion of penetratingocular injuries. Note that full thickness lacerationscan seal up leaving a foreign body in the orbit.
2. Anterior segment� Ideally this should be performed on the slit lamp. This
is sometimes not possible due to confounding injuriesbut this should be at the discretion of an ophthal-mologist. Trauma of significant force to render a pa-tient with orthopaedic injuries with concurrent ocularinjury should be fully assessed by a specialist andmay require the use of a hand-held slit lamp whereavailable.
� The slit lamp can be used to examine the cornea, thedepth of the anterior chamber and the iris.
� In particular look for:i. Lacerations to the cornea.ii. Hyphaema (blood in the anterior chamber).iii. Foreign body in the anterior chamber.iv. If the anterior chamber (space between the cor-
nea and the iris looks flat/non-formed (rememberto compare to the non-injured eye) then this is asign of aqueous loss and penetrating eye injury.
Figure 4 Ocular movements should be tested in all cardinalpositions of gaze.
Copyright Agency Limited (CAL) licenced copy
3. Posterior segment� Whilst examination of the posterior segment is crucial
it is usually very difficult without dim room lights andmydriatic drops (e.g. through a dilated pupil). Dilatingdrops are best instilled by ophthalmic specialists asthey carry a small but significant risk of inducing ac-ute angle closure glaucoma and will interfere withpupillary reaction measurement of routine neurolog-ical observations.
� Sometimes an adequate view of the posterior segmentcan be achieved with a direct ophthalmoscope. Startoff the lens-selection wheel in the ‘‘0’’ position butadjust up/down to sharpen the view. In particularlook for:i. Lens injury (is the lens still present? Is it cloudy?
Any foreign body embedded?).ii. Vitreous haemorrhage (can you see the retina? Is
blood in the way?).iii. Retinal detachment (‘‘curtain’’ of retina floating
freely).
Investigations
Investigations can help with the diagnosis as well as assistingwith the management of these patients later.
� Plain facial X-rays are useful for the detection of orbitalfractures but their role in cases of suspected intraocularforeign body has been contested (Saeed et al., 2008).Note should be made that radiolucent material is not vis-ible on plain films and again, the history should raise yoursuspicion of intraocular foreign body due to the mecha-nism of injury.� If intraocular foreign body is suspected the Royal Col-
lege of Radiologists still recommend plain X-rays asfirst line (Royal College of Radiologists, 1998) but re-cent evidence suggests that this 11 years old guidanceshould be re-evaluated following advances in CT tec-hnology. Many centres perform CT as first line inves-tigation of choice (Saeed et al., 2008).

Emergency department management of penetrating eye injuries 159
� The orbit is very fragile and susceptible to injury. Dou-ble vision and restricted eye movements would directyou to a possible orbital fracture. These can be app-arent on plain films but other features such as fluidlevels in sinuses can be the only sign. CT again is thegold standard (Salvolini, 2002).
� CT orbits:� This is useful for imaging the orbit in greater detail as
bony injuries are more apparent. The globe is welldefined and perforations can be detected more easily.It can also be used for detection of intraocular foreignbodies (Fig. 6) and globe contents within the orbitindicating perforation.
Emergency care
Penetrating eye injuries are very stressful to manage. Youare dealing with distorted anatomy, distressed patientsand potentially devastating consequences. If penetrating in-jury is suspected these simple do’s and don’ts may behelpful:
DO:
� Do not panic.� Protect the eye: use a Cartella shield (plastic shieldapplied with transpore or mepore tape). If not available– improvise. Gallipot or cut-down polystyrene drinkscup. Ensure it is securely attached.� Call the ophthalmologist immediately once you haveassessed the extent of the injury.� Keep patient nil by mouth.� Think about analgesia: topical/IM/IV (Note: topical ana-esthetics should be used sparingly as carry a risk of cor-neal toxicity).� Consider antiemetic.� Check tetanus status and give booster if necessary.
DONT:
� Try to remove embedded foreign bodies.� Pad the eye (increases eye pressure and can cause herni-ation of ocular contents).� Try to clean the eye as you may be inadvertently remov-ing ocular contents (e.g. iris or retina).
Figure 6 Radio-opaque foreign body situated within theglobe.
Copyright Agency Limited (CAL) licenced copy
� Put any creams or preservative-containing drops into theeye (toxic to internal structures).� Delay definitive referral – ophthalmologists expect to beinvolved with sight-threatening conditions or injuries.
Referral
As most of these injuries occur outside of clinic hours youwill most likely be referring to a non-resident ophthalmolo-gist. Therefore, knowing the extent of the injury and how todescribe it can make things much easier in the middle of thenight:
What to tell the on-call ophthalmologist:
� Mechanism of injury (e.g.: objects involved, velocity andproximity, when occurred, potential for foreign body).� Pupil reactions.� Visual acuity.� Your examination findings: see above.� What has been done so far?
E.g. ‘‘I would like to refer you a potential penetratingeye injury. Mrs. Jones was assaulted with a broken bottle2 h ago. She has no perception of light and on examinationthere is a corneal laceration with lens and iris disruption.She is otherwise fit and healthy with no other injuries’’.
Legal issues
As mentioned previously penetrating eye injuries are oftenas a result of assault or workplace accidents. Road trafficincidents causing eye injuries are much less common sincelegislation was passed regarding compulsory seatbelt wear(Hall et al., 1985). The police are often involved thereforeaccurate record keeping is essential. Photographs can beof additional use so the use of Polaroid photographs to doc-ument injuries is encouraged.
Post ED management
The main aims of ophthalmic care are to preserve visionwherever possible, restore normal anatomy and prevent fu-ture complications. Surgery is not always indicated but pri-mary repair is usually attempted to close the wounds even ifthe eye has very little or no visual potential. An intact eye ismuch better cosmetically. The alternative is evisceration(removing ocular structures but retaining the scleral shell)or enucleation (removing whole globe). Procedures are of-ten elected to be performed during normal working hoursto ensure that the required expertise, staff and equipmentare available.
Patients and their relatives are often very anxious andunderstandably want to know what will happen next. Whilsta detailed discussion is best left to the ophthalmic team thefollowing examples may be helpful as a guide to further care.
Laceration
The aim is to repair the laceration as soon as feasibly possi-ble. Corneal lacerations are repaired with fine nylon su-

160 D. Lindfield, R. Das-Bhaumik
tures. Scleral ruptures can be difficult to locate and visualoutcome depends on site of wound and the extent of dam-age to structures of the visual pathway. Restoration of nor-mal anatomy is ideal but not always possible.
Intra-ocular foreign body
Foreign bodies are usually surgically removed at the earliestpossible opportunity. Visual outcome is dependent uponwhich structures have been damaged and the nature ofthe foreign body. Wood for example confers a high risk ofinfection (especially fungal) in the eye. In contrast, a highvelocity metallic projectile carries a lower infection riskbut is usually more damaging to the anatomy.
Summary
Penetrating injuries are rare but important. Prompt andaccurate detection improves outcome. Hopefully this guidehas provided a structure for ED nurses to enable targeted
Copyright Agency Limited (CAL) licenced copy
history taking, effective examination, appropriate investi-gation and accurate referral.
References
BMA/Royal Pharmaceutical Society of Great Britain, 2008. BritishNational Formulary, <www.bnf.org>.
Hall, N.F., Denning, A.M., Elkington, A.R., Cooper, P.J., 1985. The eyeand the seatbelt in Wessex. Br. J. Ophthalmol. 69 (5), 317–319.
Imrie, F.R., Cox, A., Foot, B., Macewan, C.J., 2008. Surveillance ofintra ocular foreign bodies in the UK. Eye 22 (9), 1141–1147.
McCormack, P., 1999. Penetrating injury of the eye. Br. J.Ophthalmol. 83, 1101–1102.
Punnonen, E., Laattikainen, L., 1989. Prognosis of perforating eyeinjuries with intraocular foreign bodies. Acta Ophthalmol. 66,483–491.
Royal College of Radiologists, 1998. Making The Best Use of ClinicalRadiology, ISBN: 1-872599-370.
Saeed, A., Cassidy, L., Malone, D.E., Beatty, S., 2008. Plain X-rayand computed tomography of the orbit in cases and suspectedcases of intraocular foreign body. Eye 22 (11), 1373–1377.
Salvolini, U., 2002. Traumatic injuries: imaging of facial injuries.Eur. Radiol. 12 (6), 1253–1261.