Eye Emergencies and Trauma
36
EYE EMERGENCIES AND TRAUMA DEFITARIA PERMATASARI I11109005
-
Upload
yusufharkian -
Category
Documents
-
view
228 -
download
3
description
y
Transcript of Eye Emergencies and Trauma

EYE EMERGENCIES AND TRAUMA
DEFITARIA PERMATASARII11109005


Corneal abrasions• are the most common result of blunt injury• may follow injuries with foreign bodies, fingernails, or twigs.• Abrasions will be missed if fluorescein is not instilled.
Treatments
The aims of treatment are to ensure healing of the defect, prevent infection, and relieve pain. • Small abrasions : chloramphenicol ointment twice a day or eye
drops four times a day until the eye has healed and symptoms are gone.
• For larger or more uncomfortable abrasions : a double eye pad can be used with chloramphenicol ointment for a day or so until symptoms improve.
cycloplegic eye drops : cyclopentolate 1% or homatropine 2%Oral analgesia such as paracetamol or stronger non-steroidal anti-inflammatory drugs

Conjunctival Foreign bodies• it is essential to be on the lookout for a foreign body if a
patient has an uncomfortable red eye• It may be necessary to use local anaesthetic both to examine
the eye and to remove the foreign body• The upper lid must be everted to exclude a subtarsal foreign
body• Small loose conjunctival foreign bodies can be removed with
the edge of a tissue or a cotton wool bud or they can be washed out with water



Treatments for corneal foreign bodies• Apply topical anesthetic (e.g., proparacaine). Remove the
corneal foreign body with a foreign body spud or fine forceps at a slit lamp. Multiple superficial foreign bodies may be more easily removed by irrigation.
• Remove the rust ring as completely as possible on the first attempt. This may require an ophthalmic drill.
• Measure the size of the resultant corneal epithelial defect.
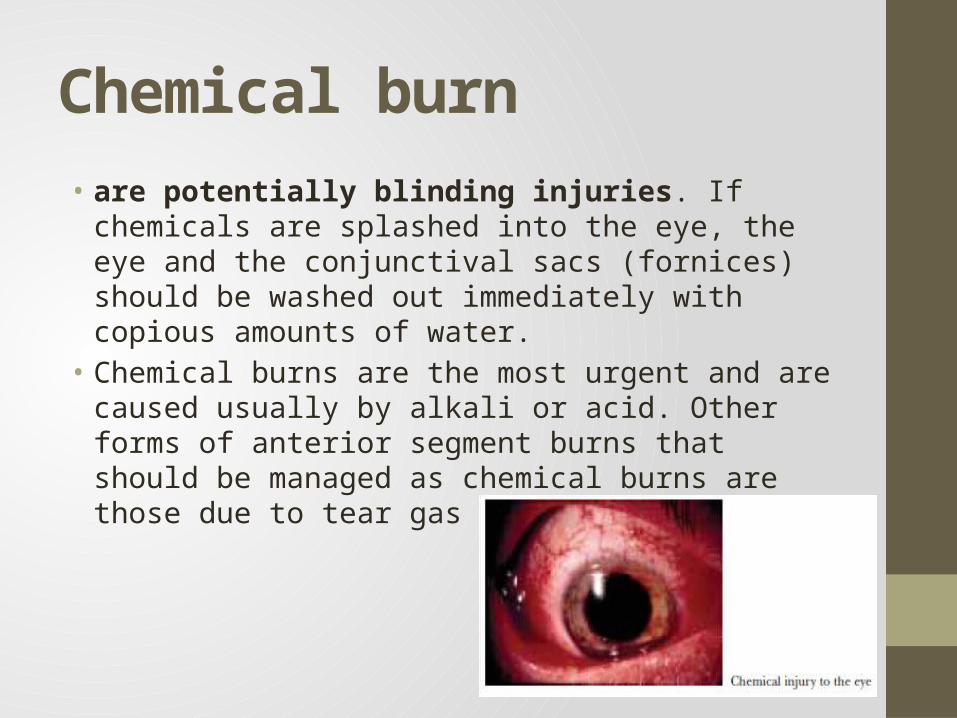
Chemical burn• are potentially blinding injuries. If chemicals are splashed into
the eye, the eye and the conjunctival sacs (fornices) should be washed out immediately with copious amounts of water.
• Chemical burns are the most urgent and are caused usually by alkali or acid. Other forms of anterior segment burns that should be managed as chemical burns are those due to tear gas and mace
• This includes alkali (e.g., lye, cements, plasters, airbag powder), acids, solvents, detergents, and irritants (e.g., mace).
• Treatment should be instituted IMMEDIATELY, even before testing vision, unless an open globe is suspected.
Alkali burn• Alkali burns are more severe than acid burns because of their
rapid penetration• Damage from alkali burns is related more to the degree of
alkalinity (pH) than to the actual cation• Permanent injury is determined by the nature and
concentration of the chemical as well as by the time lapsed before irrigation

Acid burn• such as those caused by battery acid, industrial cleaner
(H2SO4), laboratory glacial acetic acid or HCl, fruit and vegetable preservatives, bleach, refrigerant (H2SO3), industrial solvents, mineral refining agents, gas alkylation agents, silicone production agents, and glass etching agents (HFl)
• cause their maximum damage within the first few minutes to hours and are less progressive and less penetrating than alkaline agents
• Damage is therefore localized to the area of contact

Classification and prognosis• Classification and prognosis of the chemically burned eye is
most useful for alkali burns, but also extends to acid and toxic chemical injuries of the eye
I• Epithelial damage, no ischemia, good prognosis
II• Cornea hazy, iris detail seen, less than one-third
limbal ischemia, good prognosis
III• 100% epithelial loss and stromal haze blurs iris, one-
third to one-half limbal ischemia, guarded prognosis.
IV• Opaque cornea, greater than one-half limbal
ischemia, poor prognosis.
Thoft classificati
on

Treatment• Immediate treatment for chemical burns is copious irrigation
using the most readily available source of water (shower, faucet, drinking fountain, hose, or bathtub).
• The lids should be held apart and water irrigated continuously over the injured globe(s). The initial lavage at the site of the injury should continue for several minutes, so that both eyes receive copious irrigation.
• In the emergency room topical anesthetic is instilled immediately and q20 minutes to relieve some of the considerable pain, and immediate lavage is begun with at least 2,000 mL of normal saline 0.9% over a minimum period of 1 hour.

• Irrigation should be continued until pH paper reveals that the conjunctival readings are close to normal (pH between 7.3 and 7.7)
• the mydriatic–cycloplegics atropine 1% or scopolamine 0.25% should be instilled to dilate the pupil and prevent massive iris adhesions to the lens (posterior synechiae) as well as to reduce the pain secondary to iridociliary spasm
• antibiotics such as ciprofloxacin, ofloxacin, tobramycin, or polymyxin–bacitracin ointment should be started to protect against infection.
• For pain, systemic analgesics should be administered.
Flash burnHistory• Electric arc welding or sun lamp without eye protection with
symptoms appearing typically within several hours.• Symptoms are usually intense pain, red eye, blepharospasm
and tearing.Examination• Use topical anaesthesia in the examination.• Visual acuity.• Slit lamp – widespread superficial epithelial defects staining
with Fluorescein, often bilateral. There may be also conjunctival injection.
Treatment• Topical antibiotic (qid) and cycloplegic (e.g. Homatropine 2%
bd) for comfort for 3 days. Oral analgesia as required. Patients are informed to re-present if symptoms have not improved appreciably after 24 hours.
Follow up - When to refer?• Non-urgent - within 3 days.

Blunt injuries• large object hits the eye most of the impact is usually taken by
the orbital margin• smaller object hits the area the eye itself may take most of the
impactFindings:• Haemorrhage may occur and a collection of blood may be
plainly visible in the anterior chamber of the eye (hyphaema)• iris may also be damaged and the pupil may react poorly to
light
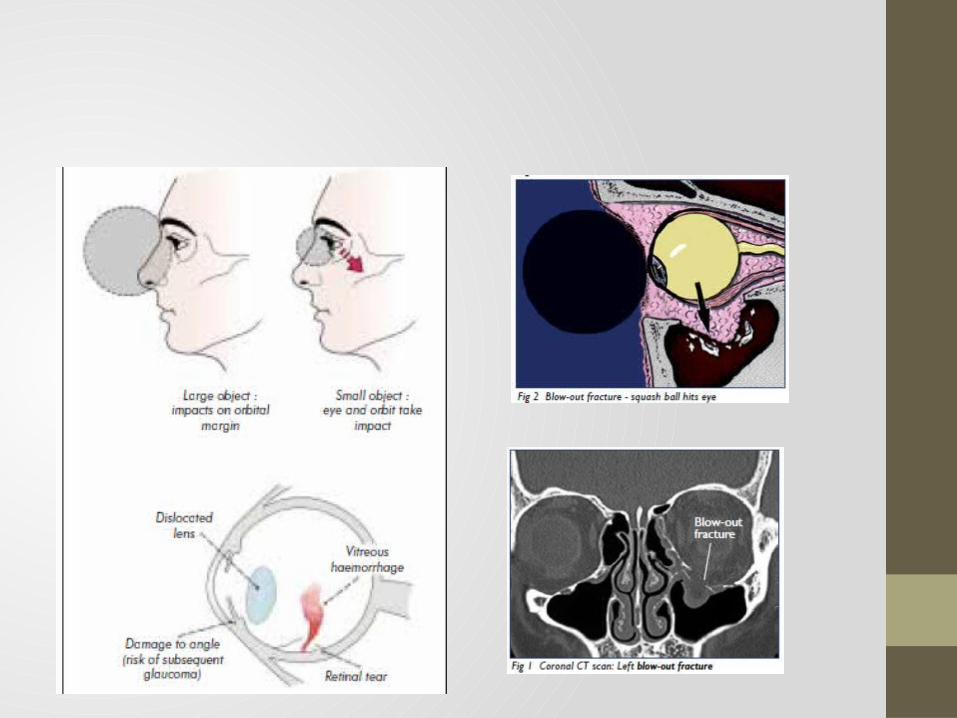

If the force of impact is transmitted to the orbit, an orbital fracture may occur.Clues of blowout fracture :Diplopia, a recessed eye, defective eye movements (especially vertical), an ipsilateral nose bleed, and diminished sensation over the distribution of the infraorbital nerve

Examintations:• Visual acuity.• Ocular movements – if there is considerable eyelid oedema,
carefully lift up the lid while viewing the eye to ensure there is no obvious rupture.
• Reduced movement may suggest ruptured globe or orbital wall fracture.

Examinations (2):• Slit lamp – looking for evidence of rupture (often at the
limbus). Examine for blood in the anterior chamber. Examine the eyelid for lacerations
• Ophthalmoscopy – Red reflex (missing in intraocular haemorrhage or retinal detachment). Look for any retinal pathology (after dilating the pupil)
InvestigationsCT scan (axial and coronal) for orbital wall fracture if indicatedFollow up - When to refer?Non-urgent referral within 3 days if the above findings are negative

Treatments• Topical antibiotic drops for superficial trauma. Usage is qid (4
times a day) and for 1 week• Suture any eyelid lacerations as indicated in eyelid trauma
section• Nasal decongestants for 7-10 days.• Instruct patient not to blow his or her nose. • Ice pack to the orbit for 24-48 hours.
Penetrating injuriesAny history of a high velocity injury (particularly a hammer and chisel injury)the eye should be examined very gently and no pressure should be brought to bear on the globeIt is possible to cause prolapse of intraocular contents and irreversible damage if the eye and orbit are not examined with great careSigns:distorted pupil, cataract, prolapsed black uveal tissue on the ocular surface, and vitreous haemorrhage.
Examination• Visual acuity.• Direct ophthalmoscopy – loss of red reflex may suggest retinal
trauma or detachment.• Slit lamp – looking for distorted anterior chamber structures
or corneal/scleral breaks.
Treatment• Ensure nil by mouth status. Strict bed rest. Injectable
analgesia/antiemetic if required. • CT scan of the orbit to exclude retained ocular/orbital foreign
body after discussion with ophthalmologist• Shield (not pad) the eye • No ointment for penetrating eye injury.• Check for tetanus immunisation status as per current protocol.• Commence broad spectrum IV antibiotics

Sympathetic ophthalmia, in which chronic inflammation develops in the normal fellow eye, is a potentially serious complication of any severe penetrating eye injury.The risk of this increases if a penetrating eye injury is left untreated
LacerationsHistoryFour basic questions are:which eye is injured? how did it happen? when did it happen? what are the symptoms?Examination• Wound examination – size and depth. • All wounds should be explored fully for extent of damage. • Visual acuity.• Superficial ocular examination with magnification to assess for
any corneal/conjunctival laceration or penetration.

Treatment/Investigation• Orbital X-Ray or CT if indicated for foreign bodies or orbital
fracture.• If superficial laceration:• Clean the area and surrounding skin with antiseptic such as
Betadine.• Subcutaneous anaesthetic with vasoconstrictor (2% Lignocaine
with Adrenaline).• Irrigate and debride the wound thoroughly with saline.• Identify foreign bodies if applicable.• Suture with a 6/0 non-absorbable suture.

Conjunctival LacerationSymptomsMild pain, red eye, foreign body sensation; usually, a history of ocular trauma.SignsFluorescein staining of the conjunctiva. The conjunctiva may be torn and rolled up on itself. Conjunctival and subconjunctival hemorrhages are often present.HistoryDetermine the nature of the trauma and whether a ruptured globe or intraocular or intraorbital foreign body may be present. Evaluate mechanism for possible foreign body involvement, including size, shape, weight, and velocity of object

Examinationsincluding careful exploration of the sclera (after topical anesthesia, e.g., proparacaine) in the region of the conjunctival laceration to rule out a scleral laceration or a subconjunctival foreign body.The entire area of sclera under the conjunctival laceration must be inspected. Since the conjunctiva is mobile, inspect a wide area of the sclera under the laceration. Use a proparacaine-soaked, sterile cotton-tipped applicator to manipulate the conjunctivaConsider a CT scan of the orbit to exclude an intraocular or intraorbital foreign body

Treatments• Antibiotic ointment (e.g., erythromycin or bacitracin t.i.d.) for
4 to 7 days. A pressure patch may be used for the first 24 hours.
• Most lacerations will heal without surgical repair. Some large lacerations (>1 to 1.5 cm) may be sutured with 8-0 polyglactin 910 (e.g., Vicryl). When suturing, take care not to bury folds of conjunctiva or incorporate Tenon capsule into the wound. Avoid suturing the plica semilunaris or caruncle to the conjunctiva.

Iridodialysis/Cyclodialysis• Iridodialysis: disinsertion of the iris from the scleral spur.
Elevated IOP can result from damage to the trabecular meshwork or from the formation of peripheral anterior synechiae (PAS).
• Cyclodialysis: disinsertion of the ciliary body from the scleral spur. Increased uveoscleral outflow occurs initially resulting in hypotony. IOP elevation can later result from closure of a cyclodialysis cleft, leading to glaucoma.
SymptomsUsually asymptomatic unless glaucoma develops. Large iridodialyses may be associated with monocular diplopia, glare, and pho-tophobia. Both are associated with blunt trauma or penetrating globe injuries. Typically unilateral.
SignCritical. Characteristic gonioscopic findings as described above.Other. Decreased or elevated IOP, glaucomatous optic nerve changes angle recession. Other signs of trauma including hyphema, cataract and pupillary irregularities.

Treatment• Sunglasses, contact lenses with an artificial pupil or surgical
correction if large iridodialysis and patient symptomatic.• If glaucoma develops, treatment is similar to that for primary
open-angle. Aqueous suppressants are usually first-line therapy. Miotics are generally avoided because they may reopen cyclodialysis clefts, causing hypotony. Strong mydriatics may close clefts, resulting in pressure spikes. Often these spikes are transient, as the meshwork resumes aqueous filtration.

Follow upCarefully monitor both eyes due to the high incidence of delayed open-angle and steroid-response glaucoma in the uninvolved as well as the traumatized eye