
Pathology of extrahepatic biliary tract and pancreas MUDr. Helena Skálová.
Upload
frank-glennCategory
view
212download
0
EXTRAHEPATIC BILIARY-TRACT CANCER
FRANK GLENN, M.D., AND n”ALC0LM R. HILL, JR., M.D.
ALIGNANT tumors arising in the extra- M hepatic biliary tract are as yet not treated effectively by surgery. Because of the lack of advances in the therapeutic approach, there has been a trend toward resigned help- lessness on the part of the medical profession. Several factors have contributed to this, in- cluding the paucity of early symptoms pro- duced by biliary-tract neoplasms, the technical difficulties involved in radical regional exci- sion, and the short interval between establish- ment of the diagnosis and death. Indeed, here, as in other cancers, the absence of early symp- toms compounds the problem. The actual effectiveness of radical surgery at present leaves much to be desired. Palliative surgical procedures, although providing short periods of respite irom conditions such as obstructive jaundice, add little to survival expectancy. Because it has been repeatedly observed that carcinoma of the gallbladder is associated with cholelithiasis in the great majority of instances, we believe that there is something to be accomplished in the way of prevention by the early removal of the gallbladder con- taining stones.
Repeated evaluation of the accumulated ex- perience with Giliary-tract cancer should en- able us better to see how our results may be improved. Prevention, cure, and palliation are the objectives. Any approach that provides possible accomplishment in any one of these three categories merits full exploitation.
The experience gained at The New York Hospital-Cornell Medical Center from Sep- tember 1, 1932, through September 1, 1954, provides the data for this report (Fig. 3; Table 4). This also brings up-to-date previous reports of this series.5, 6
In extrahepatic biliary-tract cancer we in- clude that of the gallbladder, the hepatic and common bile ducts, and the ampulla of Vater, because of the anatomical relationship and morphological similarity of these tumors.22
From the Department of Surgery, The New York Hospital-Cornell Medical Center, New York, New York.
Presented at the Eighth Annual Cancer Symposium of the James Ewing Society, April 15, 1955.
Received for publication, May 6, 1955.
TABLE 1 AGE FACTOR I N THE INCIDENCE OF CANCER ENCOUNTERED IN OPERATIONS FOR BILI-
ARY-TRACT DISEASE* The Kew York Hospital-Cornell M e d i d Center-
September 1, 1932Septernbcr 1, 1954
Age, Y‘.
Less More than 50- 65- than 50 64 74 75
Total operative cases of bili-
Ca. of gallbladder or extra-
’% cancer among operative
ary-tract disease 2395 1478 339 59
hepatic bile ducts 6 46 31 7
cases 0.25 3 . 1 9.1 11.9
*Not including ampullary lesions.
I n our over-all experience in the surgical treat- ment of biliary-tract disease, the importance of this group of tumors would seem to be in- creasing because almost 10 per cent of persons more than 65 years of age are found to have associated cancer ok the gallbladder or bile ducts.? Furthermore, the proportion o€ our population in this older age group mounts decade by decade. Actual figures are difficult to establish. However, the Public Health Serv- ice reported 10,598 deaths from extrahepatic biliary-tract Lancer in 1948.10 Perhaps the in- cidence would be higher if statistics were based upon postmortem examinations. It has been estimated that 10 per cent of the adult popu- lation 01 the United States (110,000,000 more than 20 years of age) have gallstones. If this be a reasonable assumption and the incidence of cancer associated with gallstones (Table 1), particularly in the older age group, is correct, then we may anticipate that patients with these tumors will be more frequently encoun- tered in the future.
IDEALS AND OPTIMAL APPROACH
Carcinoma of the Gallbladder. Kadical cholecystectomy, to include wide resection of the liver bed, resection of the peritoneum over the hepatic ducts, the hepatic artery, the com- mon duct, and the associated portal vein down to the duodenum, is the optimal procedure in early, operable lesions. Postinflammatory at-
1218
No. 6 EXTRAHEPATIC BILIARY-TRACT CANCER * Glenn 6. Hill 1219
TABLE 2 OPERATIVE PROCEDURES PERFORMED ON 113 PATIENTS WITH CARCINOMA OF THE
EXTRAHEPATIC BILIARY TRACT The New York Hospital-Cornell Medical Center
September 1, 1932-September 1, 1954
Carcinoma Carcinoma Carcinoma of the of the of the
gallbladder extrahepatic ducts ampulla of Vater Total
Curutiua Proceduves
Cholecystectomy, rad. 0 13 Cholecystectomy, simple 6
Noncuratioe Procedures
Rad. pancreatoduodenectomy * 1
TOTAL CURATIVE PROCEDURES
Exploratory laparotomy & biopsy 39 Gastroenterostomy & biopsy 3 Cholecystostomy & biopsy 1 Choledochoduodenostorny & biopsy Cholecystogastrostomy & biopsy Partial choledochectomy with anastomosis
TOTAL NONCIJRATIVE PROCEDURES TOTAL OPERAIIVE CASES TOTAL NONOPERATIVE CASES (AUTOPSTT) 9
2 t
10 1
2
1
2
14t
36
2
1 1 3
64 100
2 13
"Including partial gastrectomy in all rases and cholecystectorny, splenectomy, transverse colectomy, and
+Including hepatic-arterp resection. $Including one radical pancreatoduodenectomy known to be noncurative at the end of the resection. §Including resection of hepatic tissue, lymph nodes, gastrohepatic ligament, etc.
right hemicolectomy in addition to the pancreatoduodenectomy in one or more cases.
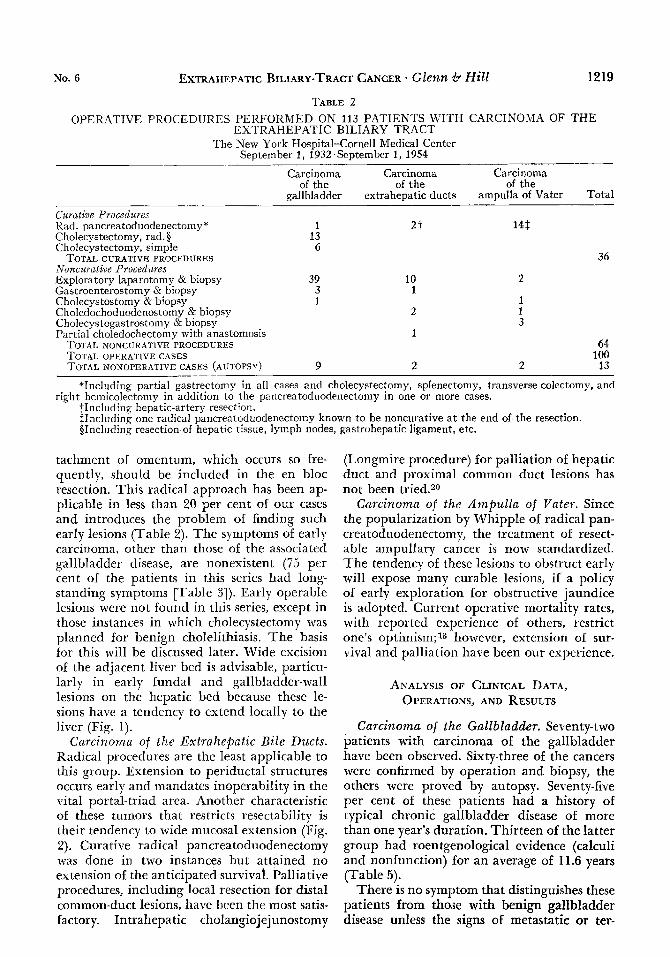
tachment of omentum, which occurs so fre- quently, should be included in the en bloc resection. This radical approach has been ap- plicable in less than 20 per cent of our cases and introduces the problem of finding such early lesions (Table 2). The symptoms of early carcinoma, other than those of the associated gallbladder disease, are nonexistent (75 per cent of the patients in this series had long- standing symptoms [Table 31). Early operable lesions were not found in this series, except in those instances in which cholecystectomy was planned for benign cholelithiasis. The basis for this will be discussed later. Wide excision 01 the adjacent liver bed is advisable, particu- larly in early fundal and gallbladder-wall lesions on the hepatic bed because these le- sions hate a tendency to extend locally to the liver (Fig. 1).
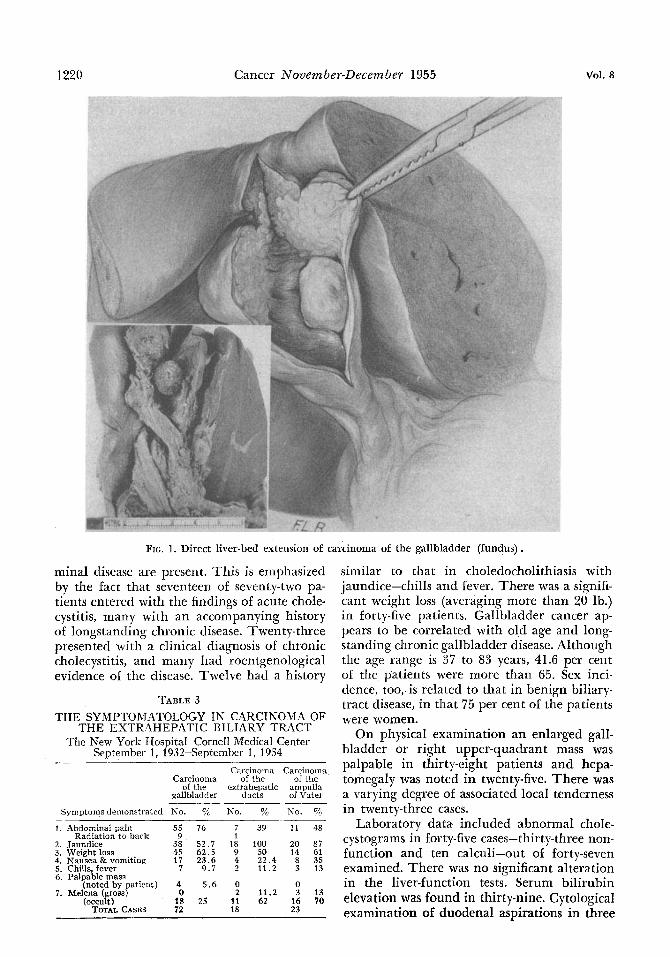
Carcinoma of the Extrahepatic Bile Ducts. Radical procedures are the least applicable to this group. Extension to periductal structures occurs early and mandates inoperability in the vital portal-triad area. Another characteristic of these tumors that restricts resectability is their tendency to wide mucosal extension (Fig. 2). Curative radical pancreatoduodenectomy was done in two instances but attained no extension of the anticipated survival. Palliative procedures, including local resection for distal common-duct lesions, have bren the most satis- factory. Intrahepatic cholangiojejunostomy
(Longmire procedure) for palliation of hepatic duct and proximal common duct lesions has not been tried.20
Corcinorna of the Ampzclla of Yuter. Since the popularization by Whipple of radical pan- creatoduodenectomy, the treatment of resect- able ampullary cancer is now standardized. The tendency of these lesions to obstruct early will expose many curable lesions, iE a policy of early exploration for obstructive jaundice is adopted. Current operative mortality rates, with reported experience of others, restrict one's optirnism;l3 however, extension of sur- vival and palliation have been our experience.
AKALYSIS OF CLINICAL DATA, OPERATIONS, AND RESULTS
Carcinoma of the Gallbladder. Seventy-two patients with carcinoma of the gallbladder have been observed. Sixty-three of the cancers were confirmed by operation and biopsy, the others were proved by autopsy. Seventy-five per cent of these patients had a history of typical chronic gallbladder disease of more than one year's duration. Thirteen of the latter group had roentgenological evidence (calculi and nonfunction) for an average of 11.6 years (Table 5) .
There is no symptom that distinguishes these patients from those with benign galIbladder disease unless the signs of metastatic or ter-
1220 Cancer Nouember-December 1955 Vol. 8
FIG. 1. Direct liver-bed extension of carcinoma of the gallbladder (fundus).
minal disease are present. This is emphasized by the fact that seventeen of seventy-two pa- tients entered with the findings of acute chole- cystitis, many with an accompanying history of longstanding chronic disease. Twenty-three presented with a clinical diagnosis of chronic cholecystitis, and many had roentgenological evidence of the disease. Twelve had a history
TABLE 3 T H E SYMPTOMATOLOGY I N CARCINOMA OF
THE EXTRAHEPATIC BILIARY TRACT The New York Hospital-CorneIl Medical Center
September 1, 1932-September 1, 1954 Carcinoma Carrinnma
Carcinoma of the of the of the extrahepatic ampulla
gallbladder ducts of Vater -- -- Symptoms demonstrated No. 7* No. yQ No. yo
1 . Abdominal pain 55 76 7 Radiation to back 9 1
2. Jaundice 38 5 2 . 7 18 3. Weight loss 4.5 62.5 9 4. Nausea&vomiting 17 23.6 4 5. Chills, fever 7 9 .1 2 6. Palpable mass
(noted by patient) 4 5.6 0 7. Melena (gross) 0 2
(occult) I8 25 11 TOTAL CASES 72 18
39 11 48
100 20 87 50 14 61 22.4 8 35 11.2 3 13
0 11.2 3 13 62 16 70
23
similar to that in choledocholithiasis with jaundice-chills and fever. There was a signifi- cant weight loss (averaging more than 20 lb.) in forty-five patients. Gallbladder cancer ap- pears to be correlated with old age and long- standing chronic gallbladder disease. Although the age range is 37 to 83 years, 41.6 per cent 01 the patients were more than 65. Sex inci- dence, too, is related to that in benign biliary- tract disease, in that 75 per cent of the patients were women.
On physical examination an enlarged gall- bladder or right upper-quadrant mass was palpable in thirty-eight patients and hepa- tomegaly was noted in twenty-five. There was a varying degree of associated local tenderness in twenty-three cases.
Laboratory data included abnormal chole- cystograms in forty-five cases-thirty-three non- function and ten calculi-out of forty-seven examined. There was no significant alteration in the liver-function tests. Serum bilirubin elevation was found in thirly-nine. Cytological examination of duodenal aspirations in three
No. 6 EXTRAHEPATIC BILIARY.?'RACT CANCER Glenn 6. Hill I221
FIG. 2. Mucosal extension (seeding) of the biliary tract from carcinoma of the gallbladder.
cases did not help in the preoperative diag- nosis.
Operative procedures were done on sixty- three patients (Table 2). In the others the diagnosis was not established until autopsy. The surgery was considered curative in twenty. One patient in this group had a pancreatoduo- denectomy; thirteen, radical cholecystectomy; and six, simple cholecystectomy. Other opera- tive procedures were done on forty-three pa- tients, including celiotomy and biopsy in thirty-nine, gastroenterostomy and biopsy in three, and cholecystostomy and biopsy in one.
The surgical follow-up of these patients re- vealed that of the twenty curative procedures done, nineteen patients were discharged from the hospital. Of the nineteen, sixteen were alive at six months, eleven at one year, and six at two years after surgery. Only two lived five or more years (Table 6). One patient died from chronic pyelonephritis with uremia at another hospital seven and a half years after surgery; there was no autopsy. She had had a laparot- omy for intestinal obstruction five years after cholecystectomy and no recurrent tumor was found. We have only one living patient now and he is four and a half years postoperative. In contrasting these twenty patients with the forty-three having noncurative operative pro- cedures, thirty-four in that group were dis-
charged from the hospital. OE those, seven were alive at six months and only one lived for two years.
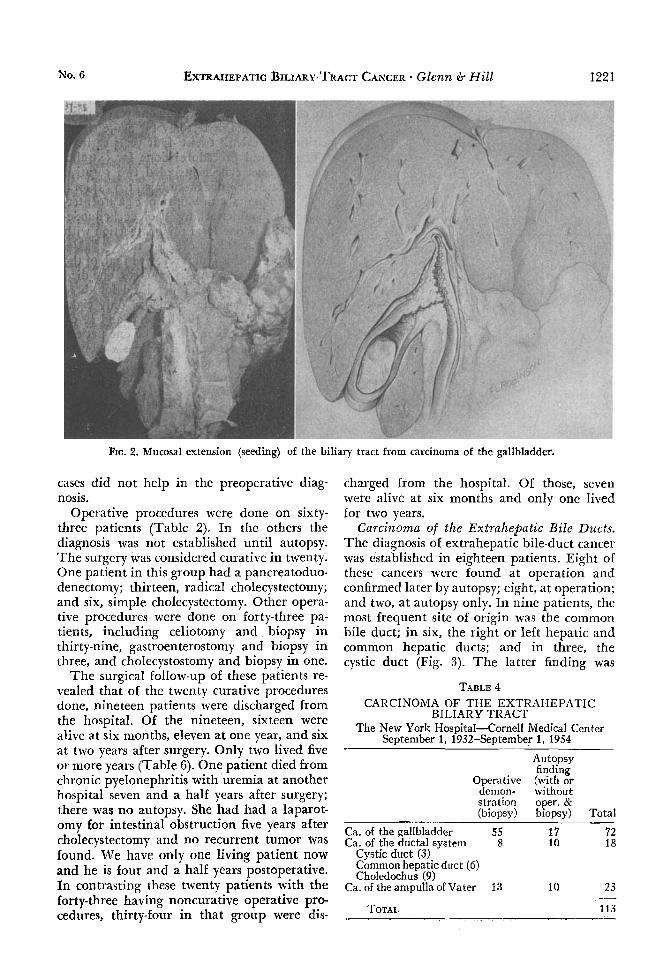
Carcinoma of the Extrahepatic Bile Ducts. The diagnosis of extrahepatic bile-duct cancer was established in eighteen patients. Eight of these cancers were found at operation and confirmed later by autopsy; eight, at operation; and two, at autopsy only. In nine patients, the most frequent site of origin was the common bile duct; in six, the right or left hepatic and common hepatic ducts: and in three, the cystic duct (Fig. 3). The latter finding was
TABLE 4 CARCINOMA OF THE EXTRAHEPATIC
BILIARY TKACT The New York Hospital-Cornell Medical Center
September 1, 1932-September 1, 1954
Autopsy finding
Operative (with or demon- without stration oper. & (biopsy) biopsy) Total
~
Ca. of the gallbladder 55 17 72 Ca. of the ductal systrm 8 10 18
Cystic duct (3) Common hepatic duct (6) Choledochus (9)
Ca. of the ampulla of Vater 13 10 23
TOTAL 113 --

Cancer hTovernber-Decernber 1995 Vol. 8 1222 TABLE 5
THE INFLUENCE OF SEX, AGE, AND A HIS-
HEPATIC BILIARY TRACT The New York Hospital-Cornell Medical Center
September 1, 1932-September 1, 1954
TORY OF BENIGN BILIARY-TRACT DISEASE IN CASES OF CARCINOMA OF THE EXTRA-
Ca. of Ca. of extra- Ca. of
bIadder ducts of Vater Total
Total no. of 72 18 23 113
gall- hepatic ampulla
patients studied
Sex ~~ ~
Male 18 12 16 Female 54 6 7
Age Less than
50 yr. 4 2 6
65 yr. or more 31 7 6
Av. age 62.5 60.7 57.6 Av. duration
of biliary- tract symp- tomatology 10.8 yr. 3.5 yr. Less than
50-64 yr. 37 9 11
1 yr. (5 cases)
X-ray f ind- ings of cho- l e c y s t i t i s (for at least 2 yr. prior to oper.*) 13 (17%) 4 0
*Autopsy in 9 cases.
more infrequent than the series would suggest. Jaundice was the most frequent complaint
on admission (eighteen patients), but it is interesting to note that seven of the group had abdominal pain as an initial symptom. Weight loss was mentioned by one half of the patients.
Physical examination showed hepatomegaly in ten patients and a definite right upper- quadrant mass in five.
Laboratory data provided help in that the stool guaiac examinations were positive in ten cases. Gastrointestinal series revealed distor- tion of the duodenum in five patients with sizable lesions. Liver-function tests showed impairment in six patients with longstanding obstruction. Biliary-drainage cytology was done on four patients and results varied from class I to 111 (Papanicolaou).
The ages of the patients in this group ranged from 30 to 78 years-an average of 60.7 years. The reversal of sex preponderance is unexplained (male, twelve cases, and female, six). Only 22 per cent of these patients had symptoms of gallbladder disease, averaging 3.4
years (one patient had had rholecystectomy and common duct exploration one year earlier, another had cholecystectomy for acute chole- cystitis with calculi twenty-four years earlier).
The surgical procedures done for extrahe- patic bile-duct cancer included two curative radical pancreatoduodenectomies, ten explora- tory laparotomies with biopsy, one gastroenter- 0s tomy, two sidetracking choledochoduode- nostomies, and one local tumor resection with end-to-end anastomosis over a T tube.
Follow-up of this group revealed that, of the two patients having curative surgery, one died postoperatively and the other lived for three years. Of the remaining patients, only eight were discharged from the hospital and seven died in less than six months. The one patient who had a local resection is living six months later. His hospital course was complicated by a postoperative duodenobiliary fistula that was controlled later by pyloric exclusion and gas- trojejunostomy. He is now gaining weight and is not jaundiced. He has an indwelling T tube that is clamped most of the time.
Carcinoma of the Ampulla of Vater. Ampul- lary carcinoma was proved in twenty-three cases. Thirteen of these cancers were found at operation, the other ten at autopsy in addi- tion to surgery.
Jaundice was the presenting symptom in twenty cases. Gross melena was admitted by four patients. Other prominent symptoms were fatigue and weight loss. A history of biliary- tract symptomatology, averaging one year in duration, was reported by 21.5 per cent.
9
23
FIG. 3. Sites of origin of biliary-tract cancer.

No. 6 EXTRAHEPATIC BILIARY-TRACT CANCER. Glenn d* Hill
TABLE 6 DURATION OF SURVIVAL IN PATIENTS WITH BILIARY-TRACT CARCINOMA
1223
The New York Hospital-Cornell Medical Center September 1, 1932-September 1, 1954
Patients Patients known to be alive after surgery Total discharged no. from hospital 6 mo. 1 yr. 18 mo. 2 yr. 3 yr. 5 yr
A . Patients Subjected to Curative Procedures Carcinoma of gallbladder 20 19 16 11 7 6 5 2* Carcinoma of extrahepatic ducts 2 1 1 1 1 1 1 0 Carcinoma of ampulla of Vater 14 9 9 t 8 6 6 4 31
Carcinoma of gallbladder 43 34 7 1 1 Carcinoma of extrahepatic ducts 14 8 1 0 0 Carcinoma of ampulla of Vater 7 3 3 3 1
B. Patients Subjected to Noncurative Procedures
*One patient is dead from other causes (seven and a half years after surgery). tIncluded is the one noncurative pancreatoduodenectomy. This patient died less than one year after
operation, $One of these patients developed fatal recurrence of carcinoma before the sixth year after operation. The
second died five and a half years after surgery. Autopsy revealed a gastrojejunal ulcer and acute cholangitis bu t no evidence of recurrent tumors.
Few consistent findings were of help in mak- ing a preoperative diagnosis. Guaiac-positive stools were noted in more than 80 per ccnt. Gastrointestinal series showed deformity indic- ative of nonresectability in four cases. Duo- denal aspiration for cells revealed no confirma- tory pattern in those studied. (The four cases examined had reports of class-I or -11 Papani- colaou.)
Male patients were found twice as often as
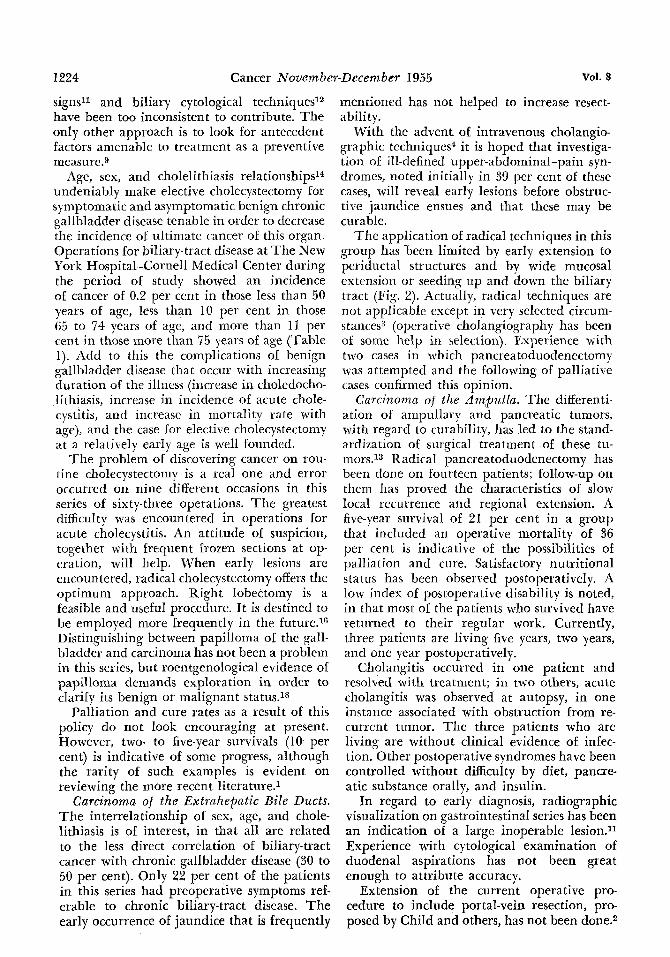
FIG. 4. Carcinoma of the ampulla of Vater.
female. The ages ranged from 38 through 80 years, with an average of more than 57 years.
Radical pancreatoduodenectomy (modified Wliipple procedure) was done in fourteen in- stances with an intent to cure. In one, how- ever, only palliation had been realized at the end of the procedure. Seven other patients had exploratory operations; three, cholecysto- gastrostomy; one, choledochoduodenostomy; and one, cholecystostomy.
I n terms of follow-up, the results in the ampullary tumors showed that, of the four- teen radical procedures, five postoperative deaths were recorded. These included one from bronchopneumonia, one from acute cho- langiohepatitis, onc from lower nephron syn- drome, one from anastomosis disruption and peritonitis, and one from coronary occlusion. Of the nine patients discharged, one died one year later, six were living at two years, and three lived for five years. Only three patients are now living: one at five years, another at two years, and one at one year.
DISCUSSION
Carcinoma of the Gallbladder. The record of this tumor as “inoperable” and “incurable” by the time there are early symptoms has con tinucd ~nchallenged.1~~ 17 ‘Turning to early diagnosis for hope in this cancer, as with many others, has found us looking for methods or clues in case finding. Specific symptoms are so lacking that they have not helped increase operability. The symptoms are similar to those of the chronic benign cholecystitis that is so frequently associated. Early roentgenographic
1224 Cancer November-December 1955 Vol. 8
signsll and biliary cytological techniques12 have been too inconsistent to contribute. The only other approach is to look for antecedent factors amenable to treatment as a preventive measure.9
Age, sex, and cholelithiasis relationships14 undeniably make elective cholecystectomy for symptomatic and asymptomatic benign chronic gallbladder disease tenable in order to decrease the incidence 01 ultimate cancer 01 this organ. Operations for biliary-tract disease at The New York Hospital-Cornell Medical Center during the period of study showed an incidence of cancer of 0.2 per cent in those less than 50 years of age, less than 10 per cent in those 65 to 74 years of age, and more than 11 per cent in those more than 75 years of age (Table 1). Add to this the complications of benign gallbladder disease that occur with increasing duration of the illncss (increase in choledocho- lithiasis, increase in incidence of acute chole- cystitis, and increase in mortality rate with age), and the case Tor elective cholecystectomy at a relatitely early age is well foundcd.
The problem of discovering cancer on rou- tine cholecystectomy is a real one and error occurred on nine different occasions in this series of sixty-three operations. The greatest difficulty was encountered in operations for acute cholecystitis. An attitude of suspicion, together with frequent frozen sections at op- eration, will hrlp. When early lesions are encountered, radical cholecystectomy offers the optimum approach. Right lobectomy is a feasible and ubeful procedure. Tt is destined to be employed more frequently in the future.16 Distinguishing between papilloma of the gall- bladder and carcinoma has not been a problem in this sex ies, but roentgenological evidence of papilloma demands exploration in order to clarify its benign or malignant status.18
Palliation and cure rates as a result of this policy do not look encouraging at present. However, two- to five-year survivals (10 per cent) is indicative of some progress, although the rarity of such examples is evident on reviewing the more recent literature.1
Carcinoma of the Extrahepatic Bile Ducts. The interrelationship of sex, age, and chole- lithiasis is of interest, in that all are related to the less direct correlation of biliary-tract cancer with chronic gallbladder disease (30 to 50 per cent). Only 22 per cent of the patients in this series had preoperative symptoms ref- erable to chronic biliary-tract disease. The early occurrence of jaundice that is frequently
mentioned has not helped to increase resect- ability.
With the advent of intravenous cholangio- graphic techniques4 it is hoped that investiga- tion of ill-defined upper-abdominal-pain syn- dromes, noted initially in 39 per cent of these cases, will reveal early lesions before obstruc- tive jaundice ensues and that these may be curable.
The application of radical techniques in this group has keen limited by early extension to periductal structures and by wide mucosal extension or seeding up and down the biliary tract (Fig. 2). Actually, radical techniques are not applicable except in very sclected circum- stances3 (operative cholangiography has been of some help in selection). Experience with two cases in which pancreatoduodenectomy was attempted and the following of palliative cases confirmed this opinion.
Carcinoma of the AmBulla. The differenti- ation of ampullary and pancreatic tumors, with regard to curability, has led to the stand- ardization of surgical treatment of these tu- mors.13 Radical pancreatoduodenectomy has been done on fourteen patients; follow-up on them has proved the characteristics of slow local recurrence and regional extension. A five-year survival of 21 per cent in a group that included an operative mortality of 36 per cent is indicative of the possibilities of palliation and cure. Satisfactory nutritional status has been observed postoperatively. A low index of postoperative disability is noted, in that most of the patients who survived have returned to their regular work. Currently, three patients are living five years, two years, and one year postoperatively.
Cholarigitis occurred in one patient and resolved with treatment; in two others, acute cholangitis was observed at autopsy, in one instance associated with obstruction from re- current tumor. The three patients who are living are without clinical evidence of infec- tion. Other postoperative syndromes have been controlled without difficulty by diet, panae- atic substance orally, and insulin.
In regard to early diagnosis, radiographic visualization on gastrointestinal series has been an indication of a large inoperable lesion.11 Experience with cytological examination of duodenal aspirations has not been great enough to attribute accuracy.
Extension of the current operative pro cedure to include portal-vein resection, pro- posed by Child and others, has not been done.2

No. 6 EXTRAHEPATIC BILIARY-TRACT CANCER . Glenn 6 Hill 1225
SUMMARY
The clinical data, surgical treatment, and current results in 113 cases of cancer of the extrahepa tic biliary tract are presented.
Conclusions from this series, as regards op- timal treatment of these lesions, are:
1. Prophylactic cholecystectomy will aid in better meeting the problem of carcinoma oE the gallbladder by preventing predictable can-
cer and helping to find early, curable lesions. 2. With present diagnostic and surgical ap-
proaches the treatment of extrahepatic bile- duct cancer is inadequate. Palliative proce- dures for carcinoma o f the ampulla of Vater offer some respite.
The results from radical surgery aimed at cure are sufficiently encouraging to warrant its rurther employment even though the opcrativc mortality has been high.
REFERENCES
1 . BOOHER, R. J., and PACK, G. T.: Cancer of the gallbladder; report of a five-year cnre of anaplastic carcinoma with metastases. Am. J. Surg. 78: 175-180, 1949.
2. CHILD, C. G., 111; HOLSWADE, G. R.; MCCLURE, R. D., JR.; C:ORE, A. L., and O’NEILL, E. A.: Pancreatico- duodenectorny with resection of the portal vein in the Macaca mulatta monkey and in man. Surg., Gynec. 6
3. GARLOCK, J. H.: Primary carcinoma of the common bile duct; resection: end-to-end anastomosis. Ann. Surg. 110: 474-476; disc. 476-479, 1939.
4. GLENN. F.: EVANS. 1.: HILL M., and MCCIENAHAN.
Obst. 94: 31-45, 1952.
J.: Intravenous diolaniiography. Ann. Surg. 140: 600: 612; disc. 612-614, 1954.
5. GLENN, F., and HAYS, D. M.: Carcinoma of the extrahepatic biliary tract. S. Clin. North America 33: 479-492, 1953.
6. GLENN, F., and HAYS, D. M.: The srope of radical surgery in the trcatment of malignant tumors of the extrahepatic biliary tract. Surg., Gynec. & Obst. 99:
7. GLENN, F., and HAYS, D. M.: The age factor in the mortality rate of patients undergoing surgery of the biliary tract. Surg., Gynec. & Obst. 100: 11-18, 1955.
8. GOLDCNBERG, I. S.: Carcinoma of the biliary tract. Am. J. Surg. 86: 292-300, 1953.
9. GRAH~M, E. A.: The prevention of carcinoma of the gall-bladder. Ann. Surg. 93: 317-322, 1931.
10. GRAY, H . K., and SHARPE, W. S.: Carcinoma of the gallbladder, extrahepatic bile ducts and the major duodenal papilla. S. Clin. North Arnerica 21: 1117-1127, 1941.
1 1 . HODES, P. J.; PENDERGRASS, E. P., and WINSTON, N. J.: Pancreatic, ductal, and vaterian neoplasms: their roentgen manifestations. Radiology 62: 1-15, 1954.
529-541, 1954.
12. LEMON, 11. M.: The clinical value of duodenal drainage in the diagnosis of carcinoma of the biliary tract and pancreas. Wew York State J . Med. 51: 2155- 2157; disc. 2157 2158, 1951.
13. LOGGAN, P. B., and KLEINSASSER, L. J.: Collective review; surgery of the pancrcas; the results of pan- creaticoduodendl resections reported in the literature. Internat. Abstr. Surg. 93: 521-543, 1951.
14. MOHARDT, J. H.: Carcinoma of the gall bladder; collective reviex. Internat. Abstr. Surg. 69: 440-451, 1939.
It;. NEIRLING, H. A.; DOCKERTY, M. B., and WAUCH, J. M.: y n o r n a of the extrahepatic bile ducts. Surg., Gynec. w Obst. 89: 429-438, 1949.
16. PACK, G. T., and BAKER, H. W.: Total right he- palic lobectomy; report of a case. Ann. Surg. 138: 253- 258, 1953.
17. SAINBURC, F. P., and GARLOCK, J. H.: Carcinoma of the gall bladder; report of seventy-five cases. Surgery
18. TABAH, E. J., and MCNEER, G., Papilloma of the gall bladder with in situ carcinoma. Surgery 34: 57-71, 1953.
19. UNITED STATES PUBLIC HEALTH SERVICE, FEDERAL SECURITY AGENCY: Deaths and death rates for selected causcs by age, race, and sex: United States, 1948. Vital Statistics, Special Reg., Nat. Surnm. 55: 315-345, 1950.
20. WADDELL, W. R., and BURHANK, C. B.: Cholan- giojejunostomy (Longmire operation) for relief of biliary obstruction due to carcinoma. New England J. M e d . 247: 929-932, 1952.
21. WHIPPLE, A. 0.; PARSONS, W. B., and MULLINS, C. R.: Treatment of carcinoma of the ampulla of Vater. Ann. Surg. 102: 763-776; disc. 776-779, 1935.
22. WILLIS, R. A.: Pathology of Tumours. St. Louis. C. 17. Mosby Co. 1948.
23: 201-205, 1948.


















